#Marci Bowers
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Text
Ari Drennen at MMFA:
A New York Times article about the World Professional Association for Transgender Health’s 2022 standards of care draws on emails released by a psychologist who has compared homosexuality to pedophilia and reportedly worked on behalf of an extreme anti-LGBTQ group.
The Times piece, which claims that the Biden administration lobbied to remove explicit age limits from the guidelines, does not provide sufficient context on the psychologist's background or his reported work for Alliance Defending Freedom, a Project 2025 partner.
The article also uses outdated data to fearmonger about rising numbers of trans youth and again includes misinformation about transition care from elected officials with no fact-checking.
The Times report quotes email excerpts filed in a legal challenge to Alabama's ban on gender-affirming care from WPATH officials describing their interactions with Sarah Boateng, who then served as chief of staff to Adm. Rachel Levine, assistant secretary for health at the Department of Health and Human Services. Boateng argued at the time that listing specific age guidelines for transition surgeries would fuel more aggressive legislative efforts to ban them.
The Times states that “the excerpts were filed by James Cantor,” whom the paper describes simply as “a psychologist and longstanding critic of gender treatments for minors.”
Cantor frequently presents himself as an expert on gender-affirming medicine and has reportedly been retained as an expert by the states in favor of West Virginia’s ban on sports participation and restrictions on health care in Texas, Florida, and Alabama. In the Alabama trial at the center of the Times’ reporting, Cantor also appears to have worked on behalf of Project 2025 partner and extreme anti-LGBTQ organization the Alliance Defending Freedom – a detail excluded from the Times’ report.
[...]
Project 2025 is a comprehensive transition plan for the next GOP presidential administration. Its nearly 900-page policy book labels “the omnipresent propagation of transgender ideology and sexualization of children” as “pornography” that “should be outlawed” and states that “the people who produce and distribute it should be imprisoned.” The Alliance Defending Freedom, which also works to curtail access to abortion, is one of over 100 organizations that have endorsed the document, meant to serve as a blueprint for a second Trump administration.
Cantor has a troubling resume outside of his work alongside the Alliance Defending Freedom. He was previously removed from the state of Florida’s roster of “subject matter experts” on transition care after linking homosexuality to pedophilia and stating that sexual attraction to children is “not inherently wrong.” Cantor served as member of the advisory council for Prostagia, which has campaigned against bans on sex dolls resembling children and has hosted support groups for “minor attracted people” open to adults alongside people as young as 13. [...]
The Times also claims that “the numbers for all gender-related medical interventions for adolescents have been steadily rising as more young people seek such care.” But the data used to support this assertion ends in 2021, when many states began restricting or outlawing transition care, meaning those numbers may no longer be “rising.” The article also includes statements from Florida Gov. Ron DeSantis and Texas Gov. Greg Abbott characterizing transition surgeries as “disfiguring” and “genital mutilation,” respectively, with no fact-checking, a repeat of a pattern previously noted by Media Matters and GLAAD. Activists opposing female genital mutilation also say that the harmful practice should not be “hijacked for purposes to target and discriminate against vulnerable youth.” The Times story was updated after publication to remove the detail that Marci Bowers, president of WPATH, is herself a transgender woman. While the current version of the story states that Levine is also a transgender woman, it makes no note of the gender identity of Cantor, DeSantis, or Abbott.
Once again, the New York Times fails to properly note the anti-trans extremism of the subjects being covered on gender-affirming care issues, this time in a story discussing James Cantor in which NYT omitted his ties to anti-LGBTQ+ extremist group Alliance Defending Freedom.
#The New York Times#Gender Affirming Healthcare#Transgender Health#Transgender#Rachel Levine#Sarah Boateng#James Cantor#Alliance Defending Freedom#Project 2025#Ron DeSantis#Greg Abbott#Marci Bowers#WPATH#Prostagia#Anti Trans Extremism#Criminalization of Trans Health
5 notes
·
View notes
Text
By: Jesse Singal
Published: Apr 18, 2023
Do people with severe depression have a right to accurate information about antidepressants? I suspect most people would answer “yes”. There is a general understanding that individuals who suffer from medical conditions are in a vulnerable position, making them susceptible to misinformation. There is also increased awareness of the influence that the profit motive can have on how medical research is funded, undertaken and communicated to the public.
But for some reason, this basic principle doesn’t seem to apply to the hyper-politicised subject of gender medicine. On one side, Republican states are attempting to ban youth gender medicine — and, in some cases, to dial back access to adult gender medicine. On the other, liberals maintain that there is solid evidence for these treatments, and that only an ignorant person could suggest otherwise.
Whether or not you agree with the GOP’s stance (I do not), the latter view is simply false. The trajectory of youth gender medicine in nations with nationalised healthcare systems has been relatively straightforward: these countries keep conducting careful reviews of the evidence for puberty blockers and hormones, and they keep finding that there is very little such evidence to speak of. That was the conclusion in Sweden, Finland, the UK, and, most recently, Norway. As a recent headline in The Economist had it: “The evidence to support medicalised gender transitions in adolescents is worryingly weak.”
Yet despite this evidentiary crisis in Europe, and despite multiple scandals vividly demonstrating the downside of administering these treatments in a careless way, liberal institutions in the US have only become more enthusiastic about them. In recent years, everyone from Jon Stewart and John Oliver to reporters and pundits at the New York Times, The Washington Post and NPR have exaggerated the evidence for these interventions.
The logic seems to be that if activists, doctors and journalists repeat “The evidence is great!” enough times, regardless of whether the evidence actually is great, the controversy will go away — as though the state of Arkansas could be shamed into reversing its policy on trans youth because Jon Stewart made fun of them. Meanwhile, as I can tell you from experience, if you openly question these treatments or highlight just how little we know about them, you’re going to have a bad time.
But look a little closer, and it swiftly becomes clear that the evidence for both adult and youth gender medicine is frequently drawn from alarmingly low-quality studies. Almost invariably, when you examine the latest study to go viral, there’s much less there than meets the eye — whether because of serious overhyping and questionable statistical choices on the part of the researchers, outright missing data, flawed survey instruments, more missing data, or just generally beyond-broken methods.
Since any individual study or group of studies can suffer from these issues, serious researchers know that you can’t just take a few that point in the right direction and herald them as evidence. Rather, you need to sum up the available evidence while also accounting for its quality. This is what European countries have done, and they have all come to roughly the same conclusion: the evidence supporting these treatments isn’t there.
But even at the level of sweeping summaries, America’s conclusions are often distorted. A prime example came in a recent New York Times column by Marci Bowers, a leading gender surgeon and the president of the World Professional Association for Transgender Health (WPATH). Bowers paints a very rosy picture of the evidence base:
“Decades of medical experience and research since has found that when patients are treated for gender dysphoria, their self-esteem grows and their stress, anxiety, substance use and suicidality decrease. In 2018, Cornell University’s Center for the Study of Inequality released a comprehensive literature review finding that gender transition, including hormones and surgery, ‘improves the well-being of transgender people’. Nathaniel Frank, the project’s director, said that ‘a consensus like this is rare in social science’. “The Cornell review also found that regret… became even less common as surgical quality and social support improved. All procedures in medicine and surgery inspire some percentage of regret. But a study published in 2021 found that fewer than 1% of those who have received gender-affirming surgery say they regret their decision to do so… A separate analysis of a survey of more than 27,000 transgender and gender-diverse adults found that the vast majority of those who detransition from medical affirming treatment said they did so because of external factors (such as family pressure, financial reasons or a loss of access to care), not because they had been misdiagnosed or their gender identities had changed.”
Here we have a leading expert (Bowers) citing a leading institution (Cornell) and relating astonishing claims (what medical procedure has a 1% regret rate?). The case appears to be closed — until you actually click the links and read Bowers’s sources. (Bowers and WPATH did not return emailed interview requests.)
Let’s start with Cornell’s data. According to a summary at its “What We Know Project“:
“We conducted a systematic literature review of all peer-reviewed articles published in English between 1991 and June 2017 that assess the effect of gender transition on transgender well-being. We identified 55 studies that consist of primary research on this topic, of which 51 (93%) found that gender transition improves the overall well-being of transgender people, while 4 (7%) report mixed or null findings. We found no studies concluding that gender transition causes overall harm.”
If you are familiar with systematic literature reviews, you will find the above unusual. Researchers don’t generally ask whether a procedure works or not in such a vague a manner, then tally up the results. To usefully gauge the level of evidence, a review has to carefully define its research questions, and factor in the potential biases of the existing studies. The Cornell project does none of this.
I emailed Gordon Guyatt, one of the godfathers of the so-called evidence-based medicine movement, to ask him whether he thought the Cornell project qualified as a systematic literature review. His response was: “It meets criteria for a profoundly flawed systematic review!” When we later spoke, he explained why he didn’t trust it. “Presumably, they are trying to make a causal connection between what the patients received and their outcomes,” he said. “That is not possible unless one has a comparator.” In other words, if you’re only tracking people who received a treatment, and don’t compare their outcomes to another group not receiving the treatment, you simply can’t learn that much. Guyatt offers the example of someone taking hormones and saying afterwards that they feel better. “That does not mean that the hormones have anything to do with your feeling good.”
This is a very basic, very well-understood problem in both medical and social-scientific research. If all you have is before-and-after measurements of how someone who received a treatment changed over time, there are all sorts of potential confounds, from the placebo effect to regression towards the mean to the possibility that receiving the treatment coincided with some other salutary intervention, such as therapy, that wasn’t accounted for.
Because the Cornell team made no effort to even evaluate the risk of bias in the individual studies it evaluated, the final product tells us very little. It’s roughly analogous to coming upon a pile of coins and trying to determine its worth simply by counting how many coins there are, rather than sorting the pile by denomination. When I raised this with Nathaniel Frank, the head of the Cornell project, he said via email that “we don’t publish traditional systematic reviews”, but rather web summaries of important research questions. So the first words of its overview might confuse readers: “We conducted a systematic literature review.”
If Bowers had wanted to cite a carefully conducted, peer-reviewed systematic review of the gender medicine literature, she actually had one at her fingertips: her own organisation, WPATH, funded one a few years ago. The results, published in the Journal of the Endocrine Society in 2021, revealed that there is almost no high-quality evidence in this field of medicine. After they summarised every study they could find that met certain quality criteria, and applied Cochrane guidelines to evaluate their quality, the authors could find only low-strength evidence to support the idea that hormones improve quality of life, depression, and anxiety for trans people. Low means, here, that the authors “have limited confidence that the estimate of effect lies close to the true effect for this outcome. The body of evidence has major or numerous deficiencies (or both).” Meanwhile, there wasn’t enough evidence to render any verdict on the quality of the evidence supporting the idea that hormones reduce the risk of death by suicide, which is an exceptionally common claim.
Oddly, though, the authors of this systematic review conclude by writing that the benefits of these treatments “make hormone therapy an essential component of care that promotes the health and well-being of transgender people”. That claim completely clashes with their substantive findings about the quality of the evidence. So, when Bowers cited the Cornell project, she was citing a review that is of very limited evidentiary value — while also ignoring a much more professionally conducted, and much more pessimistic, though strangely concluded, review that her own organisation paid for.
But what about the study which, she claims, “found that fewer than 1% of those who have received gender-affirming surgery say they regret their decision to do so”? Here’s where things get downright weird.
The study in question, published in 2021 in the journal Plastic and Reconstructive Surgery Global Open, has dozens of errors that its nine authors and editors have refused to correct. Indeed, it appears to have been executed and published to such an unprofessional standard that one might ask why it hasn’t been retracted entirely.
Before we get into all that, though, it’s worth pointing out that even if it had been competently conducted, the review could not have provided us with a reliable estimate of the regret rate following gender-affirming surgery: the studies it meta-analyses are just too weak. Many of those included did not actually contact people who had undergone surgery to ask them if they regretted it; rather, the authors searched medical records for mentions of regret and/or for other evidence of surgical reversals. Yet this method is inevitably going to underestimate the number of regretters, because plenty of people regret a procedure without going through the trouble of either reversing it or informing the doctor who performed it. In one study of detransitioners — albeit one focusing on a fairly small and non-random online sample — three quarters of them said they did not inform their clinicians that they had detransitioned.
The studies included in this review also failed to follow up with a very large number of patients. The meta-analysis had a total sample size of about 5,600; the largest study, with a sample size of 2,627 — so a little under half the entire sample — had a loss-to-follow-up rate of 36%. If you’re losing track of a third of your patients, you obviously don’t really know how they’re doing and can’t make any strong claims about their regret rates. And yet, the authors don’t mention the loss-to-follow-up issue anywhere in their paper. No version of this meta-analysis, then, was likely to provide a reliable estimate of the regret rate for gender-affirming surgery.
Even so, the version that was published was particularly disastrous. Independent researcher J.L. Cederblom summed it up: “What are these numbers? These are all wrong… And these weren’t even simple one-off errors �� instead different tables disagreed with each other. The metaphor that comes to mind is drunk driving.”
To take one example, the authors initially reported that the aforementioned largest paper in their meta-analysis had a sample size of 4,863. But they misread it — the true figure was actually only 2,627. They also misstated other aspects of that report, such as how regret was investigated (they said it was via questionnaire but it was via medical records search) and the age of the sample (they said it included some juveniles, but it did not).
Not all the errors were significant, but they were remarkably numerous. And because of the abundance of issues, the paper attracted the attention of other researchers. “In light of these numerous issues affecting study quality and data analysis, [the authors’] conclusion that ‘our study has shown a very low percentage of regret in TGNB population after GAS’ is, in our opinion, unsupported and potentially inaccurate,” wrote two critics, Pablo Expósito-Campos and Roberto D’Angelo, in a letter to the editor that the journal subsequently published. In her own letter, the researcher Susan Bewley highlighted what appears to be an absence of vital information about the authors’ method of putting together the meta-analysis.
The authors and the editors decided to simply not correct any of this. They did publish an erratum, in which they republished seven tables that still contained errors, while maintaining that all those errors had no impact on the paper’s takeaway findings. But the paper itself remains published, in its original form, complete with those 2,200 ghost-patients inflating the sample size.
Bewley and Cederblom have continued to ask the journal to reveal the process that led to the paper getting published, and to address why so many of the errors remain uncorrected. In an email in January to Bewley, Aaron Weinstein, its editorial director, claimed that because critical letters to the editor had been published, and because the corrected data was reanalysed by a statistical expert, “the Publisher and the ASPS [American Society of Plastic Surgeons] feel that PRS Global Open has done due diligence on this article and this case is closed”. He also claimed, curiously, that he had no power to force the authors to address the many serious remaining questions raised by the paper’s critics, saying “there is no precedent for an editorial office to do so”. Neither Weinstein nor the paper’s corresponding author, Oscar Manrique, responded to my emailed requests for comments.
Finally, there is Bowers’s claim that “a separate analysis of a survey of more than 27,000 transgender and gender-diverse adults found that the vast majority of those who detransition from medical affirming treatment said they did so because of external factors”. This is technically true, but is also rather misleading because the survey in question — the 2015 United States Transgender Survey (which has profound sampling issues) — was of currently transgender people. It says so in the first sentence of the executive summary. Research based on this survey obviously can’t provide us with any reliable information about why people detransition, because it is not a survey of detransitioners. If you want to know how often people detransition, you need to follow large groups of trans people over time and check in to see if they still identify that way later on — and we don’t have high-quality research on that front.
It’s also worth bearing in mind that the vast majority of studies being discussed here concern adults, while the legislative discussion mostly centres on adolescents. The most recent version of WPATH’s Standards of Care is very open about the lack of evidence when it comes to the latter: “Despite the slowly growing body of evidence supporting the effectiveness of early medical intervention, the number of studies is still low, and there are few outcome studies that follow youth into adulthood. Therefore, a systematic review regarding outcomes of treatment in adolescents is not possible.” Again, WPATH is Bowers’s own organisation — surely she is familiar with its output?
Despite the backbreaking errors of that nine-authored paper, the severe limitations of the Cornell review, and the near-utter-irrelevance of the United States Transgender Survey, all three are chronically trotted out as evidence that we know transgender medicine is profoundly helpful, or that detransition or regret are rare — or both. It’s frustrating enough that these lacklustre arguments are constantly made on social media, where all too many people get their scientific information. But what’s worse is that many journalists have perpetuated this sad state of affairs. A cursory Google search will reveal that these three works have been treated as solid evidence by the Associated Press, Slate, Slate again, The Daily Beast, Scientific American and other outlets. The NYT, meanwhile, further publicised Cornell’s half-baked systematic review by giving Nathaniel Frank a whole column to tout its misleading findings back in 2018.
Why does such low-quality work slip through? The answer is straightforward: because it appears, if you don’t read it too closely, or if you are unfamiliar with the basic concepts of evidence-based medicine, to support the liberal view that these treatments are wonderful and shouldn’t be questioned, let alone banned. That’s enough for most people, who are less concerned with whether what they are sharing is accurate than whether it can help with ongoing, high-stakes political fights.
But you’re not being a good ally to trans people if you disseminate shoddy evidence about medicine they might seek. Whatever happens in the red states seeking to ban these treatments, transgender people need to make difficult healthcare choices, many of which can be ruinously expensive. And yet, if you call for the same standards to be applied to gender medicine that are applied to antidepressants, you’ll likely be told you don’t care about trans people.
As Gordon Guyatt, who has done an enormous amount to increase the evidentiary standards of the medical establishment, told me: “You’re doing harm to transgender people if you don’t question the evidence. I believe that people making any health decisions should know about what the best evidence is, and what the quality of evidence is. So by pretending things are not the way they are — I don’t see how you’re not harming people.”
#Jesse Singal#gender ideology#genderwang#queer theory#medical transition#poor research#sex trait modification#poor evidence#Marci Bowers#WPATH#World Professional Association for Transgender Health#ideological capture#ideological corruption#medical corruption#medical malpractice#medical scandal#religion is a mental illness
29 notes
·
View notes
Note
can I just say. I grew up in Trinidad. I miss the trans women :( it's changed. I wish they'd remember.
For those just looking in, this is a reference to a book I just read called Going to Trinidad, which is nonfiction with the summary:
"For more than four decades, between 1969 and 2010, the remote former mining town of Trinidad, Colorado was the unlikely crossroads for approximately six thousand medical pilgrims who came looking for relief from the pain of gender dysphoria. The surgical skill and nonjudgmental compassion of surgeons Stanley Biber and his transgender protege Marci Bowers not only made the phrase “Going to Trinidad” a euphemism for gender confirmation surgery in the worldwide transgender community, but also turned the small outpost near the New Mexico border into what The New York Times once called “the sex-change capital of the world.”"
The book explores the realities of this, as well as some of the patients who had varying experiences with earlier iterations of gender confirmation surgery and the medical system around that. One of the things it talks about is the erasure of this history, and I can definitely understand how that would feel for someone who actually lived through the transition. One of the reasons queer history is so vital to share is because of things like this, if the town had its way, it might have disappeared from the collective memory.
5K notes
·
View notes
Text
This book I'm reading about female reproductive organs downplays the harm of female genital mutilation, promotes the bad science of Alfred Kinsey, Marci Bowers, and Joan Roughgarden, and inexplicably contains a whole chapter about surgically constructed holes (neo-vaginas).
6 notes
·
View notes
Text
Tl;Dr Being trans simply means that you say you are trans or you're transitioning. That doesn't say anything about your experiences or your relationship with sex/gender, because there are a huge range of experiences that could lead you to transitioning or identifying that way. And the sooner we accept this the better, because otherwise we will not be able to fend off the transphobia that comes from inside the house and misrepresents our individual experiences horrifically (And again, everyone should have a right to transition for any reason. There are no invalid reasons for exercising your bodily autonomy or living in an egosyntonic way in regards to gender and sex).
Otherwise the people who take themselves the least seriously or have the fewest requirements set the tone for everyone else, as they have no problem allowing rights that they themselves happen to not care for or need be lost from everyone else as they see themselves as a universal example of transness. Take for example Dr. Marci Bowers, an adult-transitioning trans woman surgeon who has likely done insane damage to trans minors' ability to get access to gender care and puberty blockers, which she didn't view as necessary for anyone because she herself didn't need it. She walked that back later iirc but the damage was done.
3 notes
·
View notes
Text
The medical transitioning of children has become one of the most controversial and polarising issues of our time. For some, it is a medical scandal. For others, life-saving treatment.
So, when hundreds of messages were leaked from an internal forum of doctors and mental health workers from the World Professional Association for Transgender Health, it was bound to spark interest. WPATH describes itself as an “interdisciplinary professional and educational organisation devoted to transgender health”. Most significantly, it produces standards of care (SOC) which, it claims, articulate “professional consensus” about how best to help people with gender dysphoria.
Despite its grand title, WPATH is neither solely a professional body – a significant proportion of its membership are activists – nor does it represent the “world” view on how to care for this group of people. There is no global agreement on best practice. The leaked messages (and the odd recording) – dubbed the WPATH files – are disturbing. In one video, doctors acknowledge that patients are sometimes too young to fully understand the consequences of puberty blockers and hormones for their fertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old, but I know I’m talking to a blank wall,” one Canadian endocrinologist says.
WPATH’s president, Dr Marci Bowers, comments on the impact of early blocking of puberty on sexual function in adulthood. “To date,” she writes, “I’m unaware of an individual claiming ability to orgasm when they were blocked at Tanner 2.” Tanner stage 2 is the beginning of puberty. It can be as young as nine in girls.
Elsewhere, there are extraordinary discussions on how to manage “trans clients” with dissociative identity disorder (what used to be called multiple personality disorder) when “not all the alters have the same gender identity”. Surgeons talk about procedures that result in bodies that don’t exist in nature: those with both sets of genitals – the “phallus-preserving vaginoplasty”; double mastectomies that don’t have nipples; “nullification” surgery, where there are no genitals at all, just smooth skin. And doctors discuss the possibility that 16-year-old patients have liver cancer as the result of taking hormones. The problem is not necessarily the discussions themselves, but that the organisation is not so open when speaking publicly.
The views of WPATH matter to the UK. For years, the organisation and its SOC have been cited as a source of “best practice” for trans healthcare by numerous medical bodies, including the British Medical Association and the General Medical Council – and still is. The Royal College of Psychiatrists refers to WPATH in its own recommendations for care.
Most relevant is that WPATH is cited as “good practice” in the current service specifications underpinning youth and adult gender clinics in England and Scotland, albeit in both cases it is WPATH’s previous SOC that is mentioned. The most recent version does away with all age limits from the beginning of puberty for hormones and surgical interventions, other than female to male genital surgery, and contains a chapter on eunuchs.
Several staff at England’s NHS adult gender clinics are not just members of WPATH (one is the former president), but authors of that current SOC. So too was Susie Green, the former boss of the young people’s charity Mermaids; a lack of medical expertise does not exclude either membership of WPATH or the power to influence policy.
England’s only NHS children’s gender clinic – the Gender Identity Development Service (Gids) at London’s Tavistock and Portman NHS Foundation Trust – will close its doors at the end of March, having been earmarked for closure since July 2022. But the 2016 service specification still underpinning Gids states that “the service will be delivered in line with” WPATH 7. While Gids was generally more cautious than other WPATH practitioners, clinicians I spoke to for my book, Time to Think, also relayed how young people claiming to have multiple personalities, or who identified with another race, could be referred for puberty blockers.
Gids staff have also presented at WPATH conferences for the past decade, including the most recent, held in 2022. This doesn’t imply agreement with WPATH’s principles, but association with the group becomes harder to justify as its views become more extreme.
It is difficult to see how the Department of Health’s assertion that NHS England “moved away from WPATH guidelines more than five years ago” holds.
What is true is that there is no mention of WPATH in updated guidance that will underpin the new youth gender services opening on 1 April. What’s more, NHS England has made it clear that WPATH’s views are irrelevant to its core recommendation that puberty blockers will no longer be available as part of routine clinical practice.
There is a battle raging over how best to care for children and young people struggling with their gender identity, with ever increasing numbers of European countries choosing to take a more cautious, less medical, approach after finding the evidence base underpinning those treatments to be wanting. NHS England insists that new services will operate in accordance with recommendations of the independent Cass review, and that it is well placed to develop policies “in line with clinical evidence and expertise”. But it won’t be easy. There is already discussion among professionals working in gender services planning a pushback against Cass’s as yet unpublished final recommendations.
It was difficult for Gids to stand up to external pressures, allowing the care it offered to suffer. At the same time, NHS England failed in its duty to provide proper oversight. Both they and those in charge of the new services must do better if they are to avoid the mistakes of the past. Without proper, evidence-based guidance on what good practice looks like, organisations like WPATH will continue to have influence.
9 notes
·
View notes
Text
By Reduxx Team November 6, 2023
Editor’s Note: Reduxx has submitted a detailed report on the subject of this article to CyberTip, a leading digital child protective authority which connects reports with local law enforcement. In accordance with our ethical standards, CyberTip was contacted PRIOR to the writing of this article.
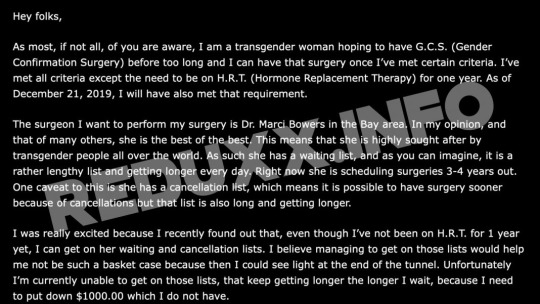
A trans-identified male who promotes nudism has been reported to child protective authorities following a disturbing video beginning to circulate on social media showing him exposing his genitals and breasts in the presence of a small child.
The video first began to circulate on November 5. Reduxx is withholding the direct link to the video as the child’s face is not censored.
In the video, an adult post-operative transgender male is seen lounging nude in what appears to be a family residence. The man spreads his legs repeatedly, exposing his surgically-constructed vagina, while a young boy is sitting a few feet in front of him. He then stands to retrieve a trans-pride flag which he holds in front of his body.
Reduxx has identified the male in the video as Marie Willa Bobo-Smith, a nudist activist who resides in Fort Bragg, California.
Bobo-Smith, formerly known as Maurice Smith, has been a pro-nudist activist for a number of years, maintaining a strong presence in the nudist community since 2012.

Bobo-Smith prior to his transition.
Bobo-Smith has maintained a blog titled Simple Naturist for 13 years, regularly posting lengthy diatribes about his belief that public nudity should be made legal and protected by the law.
“As Americans, we live in an insane world, where you can legally carry and conceal a gun, but risk imprisonment should anyone see your genitals,” Bobo-Smith wrote in December of 2012. “We live in a world where children entertain fantasies of killing innocents in video games, but the sight of a nipple is unacceptable and psychologically damaging.”
Bobo-Smith began transitioning in 2018, beginning a hormone regimen. The next year, he launched a GoFundMe campaign requesting donations to help him afford the “gender confirmation surgery” he wanted to undergo with Dr. Marci Bowers in the Bay Area.
Bowers, a trans-identified male, is the current President of the World Professional Association of Transgender Health, and has become controversial for his role in promoting the medical transitioning of children.
An old Vimeo account belonging to Bobo-Smith pre-transition featured videos of the man doing a number of tasks while nude, including cooking, washing his dogs, and cleaning.
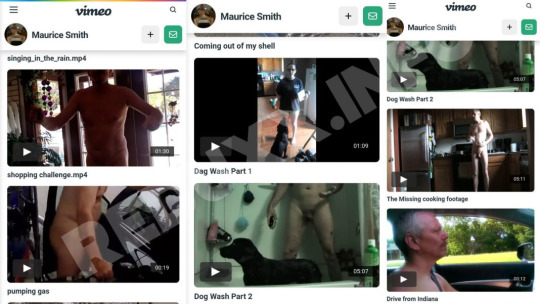
But in some of the videos he is in public, such as in one where he is naked while driving, and another while he is pumping gas at a service station.
In 2021, Bobo-Smith participated in a nudist rally in Fort Bragg, giving a speech at the event in which he condemned the stigma surrounding nudity and relating it to an experience he had walking topless following the hormone-induced growth of his breasts.
“Imagine: that as a transgender woman I am the living embodiment of a sexual double standard. Men can walk around top free and post photos of themselves on the internet and when a woman does it, she then becomes a slut, a whore and illegal,” he declared.
Bobo-Smith has been married since 1993, with his wife remaining with him throughout his transition. According to his social media history, he has children and grandchildren.
Over the years, Bobo-Smith has admitted to exposing his children to his genitalia, slamming critics of the practice as close-minded puritans. He insists there are no sinister motives to the practice, and advocates for nudism as a “lifestyle.”
In one post recently shared to his Instagram, Bobo-Smith uploaded a photo of a child’s doll representing a little girl with a penis. Bobo-Smith describes keeping a stuffed animals in his bedroom, along with a child’s doll intended to resemble a little girl with a penis.
“I got to have a great conversation with my grandson [name redacted] this morning. He’s six years old. He finally saw this naked doll sitting amongst our stuffed animals in mine and Marge’s bedroom,” Bobo-Smith describes. “When he saw it, he shockingly exclaimed ‘meemaw!'”
Bobo-Smith then describes a short exchange in which the child says “boys have penises,” to which he responds: “some boys have a penis and some boys have a vulva.”

On TikTok, Bobo-Smith has claimed he also has fostered children, with other “nudists” curiously asking him how he managed to get approval to become a foster parent despite his open nudism.
In the comments from a TikTok video uploaded in May, Bobo-Smith advised another nudist aspiring to be a foster parent that his nudism had been “addressed and resolved” at one point during the fostering process.
While Bobo-Smith has now deleted his TikTok account, Reduxx was able to archive multiple videos Bobo-Smith published following the initial outburst of concern prompted by the footage of him exposing himself to a child.
“People on the bird app formerly known as Twitter seem really shocked by a recent post of mine and asked ‘you mean your family and your friends have all seen you naked?’ Well, yeah. Everyone I know has seen me naked,” Bobo-Smith says. “I see nudity as normal and I do my utmost to show other people that nudity is a normal thing.”
#Marie Willa Bobo-Smith is Maurice Smith#usa#California#fort bragg#If he needs 1k for the surgery how is he going to take care of his post surgery cate?#Is he going to expect his wife to support him financially and be a nurse during recovery?#He has grandkids#He keeps children's toys in his bedroom#He was an exhibitionist before coming out as trans#Another midlife crisis transition
13 notes
·
View notes
Text
I’m liveblogging Who’s The Boss again because I’m on Wedding Bells and apparently this one is something else.
Thoughts under here
- I’ve found that the versions on CTV seem to cut things apparently and I hate it.
- Teens now are so lucky they don’t have to tie up a landline to talk to each other. I didn’t have to do that either but it’s fun to see it depicted because I’m sure that was an actual thing.
- Angela wears so much pink and I love it for her. This pink blouse in particular I love to bits.
- Samantha being offended that Marci’s dad told her he was engaged before Sam could 💀
- Oh my god they’re going to be the matron of honour and best man oh god oh fuck oh god
- TONY SQUEALING 😂 And Angela’s genuine laughter in the background 🥹
- NOT TONY AND ANGELA PICKING THE INVITATIONS BUT GOING WITH WHAT THEY THINK NOT WHAT THE BRIDE AND GROOM THINK AND MONA CALLING THEM OUT 👀 These two will be the fucking end of me.
- “Any woman I love would have to love you as much as I do” Did you mean Angela Bower?
- “And then I’ve got to find a woman who accepts me for what I am and what I do.” DID YOU MEAN ANGELA BOWER?
- “This time I would like a man that would be supportive of my career, that loves my son, and is sensitive and considerate.” Wow, so Tony right? You realize that you’re describing Tony don’t you?
- Oh god them walking down the aisle together they’re so cute I can’t handle this 💜
- THEY KEEP GLANCING AT EACH OTHER DURING THE CEREMONY JESUS
- That was the shortest ceremony I’ve ever seen in my life.
- OH MY GOD NOT THEM IMAGINING EACH OTHER I CAN’T
- “Perfect couple don’t you think?” Yes you two are
- “It’s almost like there’s love in the air” “Oh c’mon Angela, that was Pine Sol.”
Okay I need to break this down (read: extremely overanalyze) for a second. Obviously, Tony is cracking a joke here, but I can get some deeper meaning here. Tony’s her housekeeper right? So he would use cleaning products, like say, Pine Sol. And we all know Angela’s in love with him so maybe love does smell like Pine Sol to her.
- NOT THE FERGUSONS OFFERING TO LET THEM GET MARRIED TOO 💀
- “You probably know what I like as well as I do.” “Better.” OH MY GOD HE’S RIGHT BUT I’M DYING
- TONY ANSWERING THE GUY’S QUESTION AT THE HORS D’OUVRES TABLE WITH TABLE 6 WHICH IS WHERE HE AND ANGELA ARE SITTING.
(I’m sorry for the permanent caps I am just literally trying not to scream out loud so I need to scream through text)
- I’m already getting bad vibes from Fred and Ginger…
- “He’s very sensitive about his organs.”💀💀
- Mona is being a shit disturber and I don’t know how I feel about it.
- Tony and Angela dancing together gives me all the feels 💜
- And then them going to say the same thing at the same time. This is soulmatism if I’ve ever seen it. I’m still convinced at least one person on the Ted Lasso writing staff was inspired by these two because Ted and Rebecca have some similar stuff here
- THEY WAY THEY ARE LOOKING AT EACH OTHER 😍😍😍
- Sam i love you but please don’t interrupt them dancing
- “As you well know, good husbands are hard to find.” MONA I LOVE YOU
- NOPE FUCK FRED AND GINGER. THEY NEED TO FUCK RIGHT OFF.
- Angela, I know your heart is in the right place here but this is going to make things worse and I hate it here
- “I don’t give a Fig Newton what people say” I need to use this euphemism now. I love it.
- Angela’s gonna catch the bouquet. I guarantee it.
- Okay she tossed that right at them 💀
- TONY NO 😭😭😭😭 YOU’RE GOOD ENOUGH FOR HER YOU GOTTA BELIEVE THAT 😭😭😭
- HE’S GIVING HER A FOOT RUB HELLO?!?
2 notes
·
View notes
Note
Jazz is one of the most famous trans woman from america i'm surprised you don't know her. She is considered to be the youngest transgender person for being diagnosed with gender dysphoria at 4 and she got puberty blockers at puberty. Her surgeon is Marci Bowers, a trans woman too, but Jazz had a lot of complications. She wrote the book I am Jazz, and her whole transition journey has been followed by cameras in a reality show. She's a big LGBTQIA+ activist and cofounded a charity for trans kids with her parents. Definitely look her up !
Sorry for late response. Thats amazing, I never knew of her before :0
0 notes
Text
Lies He Told Me by James Patterson and David Ellis
Lies He Told Me by James Patterson and David Ellis is a kick butt thriller. OH MY - I can’t believe the ride the book took me on! James Patterson certainly knows how to plan out a thriller of a ride…
The main characters are David and Marcie Bowers. They have two children, live in a small town. She is a lawyer and he owns the local pub. They even have a dog. A seemingly perfect life, until it falls apart. It starts with some random weird events and slowly builds as another couple of characters are introduced with more unusual choices and happenings.
I have to say, I was not prepared for parts of the novel. I did not figure out all the twists and turns. Who am I kidding? I didn’t even have a clue. What a great thriller to read!!! Lies He Told Me by James Patterson and David Ellis is a kick butt thriller.
0 notes
Text
By: Genspect
Published: Mar 5, 2024
1/🔍📣 "The WPATH Files" have been released 📂: Leaked discussions from WPATH key figures. Find out what they really think about what’s happening in “gender medicine.”💡
2/ WHO’S WHO IN THE WPATH FILES 🔍: Meet Dr Marci Bowers, a surgeon and the President of WPATH. Bowers has said that puberty blockers are “fully reversible.” But evidence suggests otherwise and Bowers knows this. 💥#WPATHFiles

3/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Daniel Metzger, an endocrinologist, knows that talking to kids about fertility preservation is difficult because they don’t fully understand what they are giving up. Dr Metzger also knows that reproductive regret is common. 🤯 #WPATHFiles

4/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Dianne Berg, a psychologist, knows that kids cannot developmentally understand the implications of transition and acknowledges that parents are signing off on things they don’t understand. This is NOT informed consent. #WPATHFiles

5/ WHO’S WHO IN THE WPATH FILES 🔍: Jamison Green, an activist and former WPATH President, knows that patients are often signing consent forms without reading because they are afraid to read the details of the surgeries and procedures they are about to undergo. #WPATHFiles
6/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Cecile Ferrando, a surgeon, experiments with giving young women small doses of testosterone to, for example, stop their periods. Dr Ferrando says that her experiments help improve young women’s wellbeing. Sure, “wellbeing.”🙄

7/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Ren Massey, a psychotherapist, knows that multiple things could be affecting a person’s sense of their gender identity and, in particular, he knows that exploring one’s sexuality can help clarify gender issues. #WPATHFiles

8/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Scott Mosser, a plastic surgeon and WPATH member, disregards the risks associated with operating on patients whose BMI is too high, thereby putting patients at increased risk. Mosser shows blatant disregard for medical ethics! #WPATHFiles

9/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Sidbh Gallagher, a plastic surgeon who advertises gender surgeries to teens on TikTok, has received backlash from obese patients who say they experienced severe post-op complications. #WPATHFiles

10/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Dan Karasic, a psychiatrist, refuses to acknowledge that mental illness can impact someone’s capacity to consent to treatments like cross-sex hormones. #WPATHFiles
11/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Johanna Olson-Kennedy pushes for a risky shift, reframing of gender interventions as being about “embodiment” goals, not treatment for dysphoria. This is dangerous; it takes away responsibility from professionals causing harm. #WPATHFiles

12/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Thomas W Johnson wrote a chapter in WPATH’s SOC 8 which presents “eunuch” as a gender identity. 🤯 This alone should make organizations who refer to WPATH’s SOC 8 as authoritative think twice. #WPATHFiles

13/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Thomas Satterwhite, a surgeon, has actively sought advice on how to get more surgeons to perform “non-standard” gender surgeries—these include nullification surgery, ph*llus-preserving neo-v*ginas, minimum-depth neo-v*ginas. #WPATHFiles
14/ WHO’S WHO IN THE WPATH FILES 🔍: Dr Michael Irwig is worried that surgeons will lose their license if they c*strate psychologically troubled men, so he’s delighted that surgeons can now assign the label “eunuch” to said men before performing irreversible surgeries. #WPATHFiles

==
A Ghoul's Gallery of medical malpractice and ethics violations.
#Genspect#The WPATH Files#WPATH Files#WPATH#World Professional Association for Transgender Health#ethics violations#medical malpractice#medical corruption#medical scandal#gender ideology#queer theory#gender identity ideology#eunuch#Marci Bowers#Jamison Green#Daniel Metzger#Sidbh Gallagher#Scott Mosser#Ren Massey#Cecile Ferrando#Dianne Berg#Michael Irwig#Thomas Satterwhite#Thomas W Johnson#Johanna Olson-Kennedy#Dan Karasic#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model
6 notes
·
View notes
Text
Puberty is not optional. Taking GNRh agonists will not pause it. Taking cross-sex hormones after will not cause you to go through the puberty of the opposite sex. If "blocked" at Tanner stage 2 you will be sexually neutered as confirmed by Dr. Marci Bowers who was Jazz Jennings' surgeon and is himself trans-identified. Males might stand a better chance of "passing" as a female but the consequences for your overall health are dire, particularly for your bones. It would be cruel not to ban them for this off-label use that doesn't even do what it claims.
Up to you if you want to be convinced by disingenuous arguments made by an adult-baby diaper fetishist though.

2K notes
·
View notes
Text
"Jeanette made the false claim that nearly 50% of "trans kids" will take their own lives without these harmful interventions.
After sterilizing her effeminate son, Jeanette Jennings wants more parents to follow suit, even if it means spreading lies..."

0 notes
Text
Headley Archer



Headley Archer
Headley Archer
♛ Né le 3 avril 1998
♛ Originals
♛ Britannique
♛ Fils de Jordan et Zoe Archer, née Ceasy
♛ Frère de Abby, Shel et Liddy
⇝ Aromantique ; pansexuel
⇝ Serpentard
⇝ Sang-Mêlé
⇝ Directeur des Serpentard ; professeur d'astronomie
⇝ Astral projection
⇝ Jamie Campbell Bower
☮ Père de Marcy Archer
☮ Meilleur ami, puis jumeau cosmique, puis frère d'Abby Archer
☮ Ami d'Aspen Aspid (ils ont eu un groupe de musique ensemble durant leur adolescence), Emma Shils, Corine Gamble
☮ Pote de Charley Chatterson
☮ Aime embêter Josh Card et Anna Becker
☮ Parrain d'Anthony Archer
☮ Filleul de Lorcan Ausländer

1 note
·
View note
Text
0 notes