#World Professional Association for Transgender Health
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
69% of Tumblr users are millennials.
Text
By: Jesse Singal
Published: Jun 27, 2024
In April Hilary Cass, a British paediatrician, published her review of gender-identity services for children and young people, commissioned by NHS England. It cast doubt on the evidence base for youth gender medicine. This prompted the World Professional Association for Transgender Health (WPATH), the leading professional organisation for the doctors and practitioners who provide services to trans people, to release a blistering rejoinder. WPATH said that its own guidelines were sturdier, in part because they were “based on far more systematic reviews”.
Systematic reviews should evaluate the evidence for a given medical question in a careful, rigorous manner. Such efforts are particularly important at the moment, given the feverish state of the American debate on youth gender medicine, which is soon to culminate in a Supreme Court case challenging a ban in Tennessee. The case turns, in part, on questions of evidence and expert authority.
Court documents recently released as part of the discovery process in a case involving youth gender medicine in Alabama reveal that WPATH's claim was built on shaky foundations. The documents show that the organisation’s leaders interfered with the production of systematic reviews that it had commissioned from the Johns Hopkins University Evidence-Based Practice Centre (EPC) in 2018.
From early on in the contract negotiations, WPATH expressed a desire to control the results of the Hopkins team’s work. In December 2017, for example, Donna Kelly, an executive director at PATH, told Karen Robinson, the EPC's director, that the WPATH board felt the EPC researchers “cannot publish their findings independently”. A couple of weeks later, Ms Kelly emphasised that, “the [WPATH] board wants it to be clear that the data cannot be used without WPATH approval”.
Ms Robinson saw this as an attempt to exert undue influence over what was supposed to be an independent process. John Ioannidis of Stanford University, who co-authored guidelines for systematic reviews, says that if sponsors interfere or are allowed to veto results, this can lead to either biased summaries or suppression of unfavourable evidence. Ms Robinson sought to avoid such an outcome. “In general, my understanding is that the university will not sign off on a contract that allows a sponsor to stop an academic publication,” she wrote to Ms Kelly.
Months later, with the issue still apparently unresolved, Ms Robinson adopted a sterner tone. She noted in an email in March 2018 that, “Hopkins as an academic institution, and I as a faculty member therein, will not sign something that limits academic freedom in this manner,” nor “language that goes against current standards in systematic reviews and in guideline development”.
Not to reason XY
Eventually WPATH relented, and in May 2018 Ms Robinson signed a contract granting WPATH power to review and offer feedback on her team’s work, but not to meddle in any substantive way. After WPATH leaders saw two manuscripts submitted for review in July 2020, however, the parties’ disagreements flared up again. In August the WPATH executive committee wrote to Ms Robinson that WPATH had “many concerns” about these papers, and that it was implementing a new policy in which WPATH would have authority to influence the EPC team’s output—including the power to nip papers in the bud on the basis of their conclusions.
Ms Robinson protested that the new policy did not reflect the contract she had signed and violated basic principles of unfettered scientific inquiry she had emphasised repeatedly in her dealings with WPATH. The Hopkins team published only one paper after WPATH implemented its new policy: a 2021 meta-analysis on the effects of hormone therapy on transgender people. Among the recently released court documents is a WPATH checklist confirming that an individual from WPATH was involved “in the design, drafting of the article and final approval of [that] article”. (The article itself explicitly claims the opposite.) Now, more than six years after signing the agreement, the EPC team does not appear to have published anything else, despite having provided WPATH with the material for six systematic reviews, according to the documents.
No one at WPATH or Johns Hopkins has responded to multiple inquiries, so there are still gaps in this timeline. But an email in October 2020 from WPATH figures, including its incoming president at the time, Walter Bouman, to the working group on guidelines, made clear what sort of science WPATH did (and did not) want published. Research must be “thoroughly scrutinised and reviewed to ensure that publication does not negatively affect the provision of transgender health care in the broadest sense,” it stated. Mr Bouman and one other coauthor of that email have been named to a World Health Organisation advisory board tasked with developing best practices for transgender medicine.
Another document recently unsealed shows that Rachel Levine, a transwoman who is assistant secretary for health, succeeded in pressing WPATH to remove minimum ages for the treatment of children from its 2022 standards of care. Dr Levine’s office has not commented. Questions remain unanswered, but none of this helps WPATH’s claim to be an organisation that bases its recommendations on science.
[ Via: https://archive.today/wJCI7 ]
--












==
So, there are 6 completed reviews sitting somewhere, that WPATH knows shows undesirable (to them) results. And they know it. And despite - or perhaps, because of - that, they wrote the insane SOC8 anyway. And then, at the behest of Rachel Levine, went back and took out the age limits, making it even more insane.
This isn't how science works, it's how a cult works.
When John Templeton Foundation commissioned a study on the efficacy of intercessory prayer, a study which unsurprisingly found that it's completely ineffective, it was forced to publish the negative results.
So, even the religious are more ethical than gender ideologues when it comes to science. This is outright scientific corruption.
#Jesse Singal#Johns Hopkins#Johns Hopkins University#WPATH#World Professional Association for Transgender Health#anti science#gender cult#corruption#medical malpractice#medical corruption#medical scandal#systematic review#Cass review#Cass report#gender affirming care#gender affirming healthcare#gender affirmation#ideological corruption#religion is a mental illness
275 notes
·
View notes
Text
A man who got where he is, careerwise and having a family by transitioning later in life, wants to take that way from minors.
Image: WASHINGTON, DC - OCTOBER 21: (L-R) Jesse M. Ehrenfeld, MD, MPH, President of the American Medical Association; Admiral Rachel L. Levine, MD, the 17th Assistant Secretary for Health (ASH) for the U.S. Department of Health and Human Services; and Charlotte Clymer, writer, transgender activist, and military veteran speak on stage during Learning With Love: The 2023 PFLAG National Convention, four days of educating, lobbying, networking, and leading with love, taking place October 19-22, 2023 in Washington, DC. (Photo by Paul Morigi/Getty Images for PFLAG National)
A head-on collision between science and politics
By JESSE SINGAL JUN 25, 2024
When the World Professional Association for Transgender Health’s Standards of Care Version 8 was released in September 2022, a very strange thing happened: WPATH removed references to minimum age requirements for various medical interventions, describing the change as a “correction” in a notice that now reads, weirdly: “This correction notice has been removed as it referred to a previous version of the article, which was published in error.” Whatever happened, exactly, it’s clear that until late in the game the document did have age minimums until, suddenly, it did not.
The SoC 8 was supposed to have been created via something called the Delphi process. As the document itself explains: “Consensus on the final recommendations was attained using the Delphi process that included all members of the guidelines committee and required that recommendation statements were approved by at least 75% of members.” Suffice it to say that making a sudden, major change so late in the game calls into question whether that process was fully adhered to.
Thanks to a rather remarkable document just unsealed as part of Boe v. Marshall, one of the many American lawsuits over youth gender medicine, we now have a potential explanation for why the age guidelines were removed: direct pressure from assistant secretary for health of the Department of Health and Human Services Admiral Rachel Levine (who is a trans woman herself) and the American Academy of Pediatrics.
The document is titled “Appendix A To Supplemental Expert Report Of James Cantor, Ph.D. In it Cantor, a Canadian sex researcher, critic of youth gender medicine, and frequent expert witness on behalf of those attempting to ban or or restrict it (including in this case), claims that “Assistant Secretary for Health Dr. Rachel Levine strongly pressured WPATH leadership to rush the development and issuance of SOC-8, in order to assist with Administration political strategy.”
He backs this claim up with the following internal communications from WPATH members involved with the creation of the SoC 8 (here and elsewhere in the document, the names of the people who wrote the words in question are redacted):
I have just spoken to Admiral Levine today, who—as always is extremelysupportive of the SOC 8, but also very eager for its release—so to ensureintegration in the US health policies of the Biden government. So, let’s crack onwith the job!!!
I am meeting with Rachel Levine and her team next week, as the US Department of Health is very keen to bring the trans health agenda forward.
The failure of WPATH to be ready with SOC 8 is proving a barrier to optimal policy progress and she [Dr. Levine] was eager to learn when SOC 8 might be published.
[T]his should be taken as a charge from the United States government to do what is required to complete the project immediately.
More worryingly, Cantor charges that “Assistant Secretary Levine also attempted to and did influence the substantive content of SOC-8, based on political goals rather than science. Specifically, Assistant Secretary Levine, though [sic] a staff member, pressured WPATH to remove recommended minimum ages for medical transition treatments from SOC-8.”
Here, too, he has evidence from anonymized emails written by those involved in the SoC 8:
Sarah Boateng, who is Adm. Levine’s chief of staff [said the] biggest concern is the section below in the Adolescent Chapter that lists specific minimum ages for treatment, she is confident, based on the rhetoric she is hearing in DC, and from what we have already seen, that these specific listings of ages, under 18, will result in devastating legislation for trans care. She wonders if the specific ages can be taken out and perhaps an adjunct document could be created that is published or distributed in a way that is less visible than the SOC8, is the way to go.
The issue of ages and treatment has been quite controversial (mainly for surgery) and it has come up again. We sent the document to Admiral Levine. . . She like [sic] the SOC-8 very much but she was very concerned that having ages (mainly for surgery) will affect access to health care for trans youth and maybe adults too. Apparently the situation in the USA is terrible and she and the Biden administration worried that having ages in the document will make matters worse. She asked us to remove them. We have the WPATH executive committee in this meeting and we explained to her that we could not just remove them at this stage.
[W]e heard your [Dr. Levine’s] comments regarding the minimal age criteria for transgender healthcare adolescents; the potential negative outcome of these minimal ages as recommendations in the US [. . . ] Consequently, we have changes to the SOC 8 in this respect. Given that the recommendations for minimal ages for the various gender affirming medical and surgical intervention are consensus-based, we could not remove them from the document. Therefore, we have made changes as to how the minimal ages are presented in the documents. [Note: “your” may well refer to an aide of Levine’s rather than the Secretary herself, though it’s unclear.]
Cantor also includes emails from SoC 8 contributors expressing surprise at the sudden change, including this one making. . . well, the same point everyone else made after news of the late-stage “correction” broke:
I don’t see how we can simply remove something that important from the document—without going through a Delphi—at this final stage of the game [. . . ] I realize that those in favor of the bans are going to go right to the age criteria and ignore the fact that we actually strengthened the strictness of the criteria to help clinicians better discern appropriate surgical candidates from those who are inappropriate [. . . ] It’s all about messaging and marketing.
I’m actually crashing on a different but related freelance story at the moment. Check out Leor Sapir’s Twitter timeline for more details about this and another just-unsealed document. Next week, when I’ve caught my breath, I’ll write a little bit more about this as well as yet another damning claim Cantor makes, that the American Academy of Pediatrics “issued an ultimatum to WPATH: Should WPATH not delete the age minimums, AAP would not only withhold endorsement of SOC-8, but would publicly oppose the document.”
But I wanted to at least get this short piece up, because the Levine angle is important and alarming. It demonstrates an indisputable conflict between how WPATH has portrayed the SoC 8 — as a document steeped in evidence and careful deliberation on the part of experts — and how the guidelines were actually formulated.
#World Professional Association for Transgender Health#Removing minimum age from a Standards of Care 8#Boe v. Marshall#Department of Health and Human Services#Admiral Rachel Levine#Appendix A To Supplemental Expert Report Of James Cantor Ph.D.#Stop transing kids
12 notes
·
View notes
Text
Protecting Children from Chemical and Surgical Mutilation Executive Order
Signed January 28, 2025
This executive order does the following:
Falsely claims that medical professionals are "maiming" children.
Claims, without citation, that "countless children soon regret that they have been mutilated and begin to grasp the horrifying tragedy that they will never be able to conceive children of their own or nurture their children through breastfeeding."
Refers to the World Professional Association for Transgender Health (WPATH) as "junk science."
Instructs all federal agencies to repeal all children-related policies that rely on the WPATH's guidance.
Directs all agencies that fund medical schools and hospitals for research or education to force these schools and hospitals to stop providing gender-affirming care for children.
Gives permission to the Department of Health and Human Services to make changes to Medicaid and Medicare to stop gender-affirming care.
Cancels the “HHS Notice and Guidance on Gender Affirming Care, Civil Rights and Patient Privacy” policy signed in March of 2022.
Allows the Attorney General to revoke custody from parents who seek gender-affirming care for their children.
Ensures that federal employee health plans stop covering transgender-related surgeries and hormone treatments for children starting in 2026.
Directs the Department of Defense to change their insurance details to no longer cover surgeries or medications that alter a child's body, surgically or medically.
#fuck donald trump#trump administration#fuck trump#united states#civil rights#gender affirming care#protect trans youth#transgender#trans kids#executive orders#us politics#trump#donald trump
99 notes
·
View notes
Note
Writing an oc who's a prostitute? What's the job like? The measures they'll take? It might be lengthy, but stuff like virtual, brothel and escort work?
Writing Notes: Prostitution
Prostitution - the practice of engaging in relatively indiscriminate sexual activity, in general with someone who is not a spouse or a friend, in exchange for immediate payment in money or other valuables.
From the 1980s, the more neutral term sex worker was increasingly employed to describe those involved in commercial sex activities.
"Prostitute" and "sex worker" are shorthand for what is argued to be the more accurate term: “a provider of sexual services for material gain.”
“Pimp” - males who act as intermediaries between client and worker in the exchange of sexual services; he may or may not be in an additional relationship to the woman.
“Madam” - a female brothel-keeper.
The designations “pimp” and “madam” are charged terms. Their usage was common in some historic places and times.
Prostitution is a very old and universal phenomenon; also universal is condemnation of the prostitute but relative indifference toward the client.
Prostitutes may be female or male or transgender, and prostitution may entail heterosexual or homosexual activity, but historically, most prostitutes have been women and most clients men.
Prostitutes are often set apart in some way:
In ancient Rome they were required to wear distinctive dress;
under Hebrew law only foreign women could be prostitutes; and
in pre-World War II Japan they were required to live in special sections of the city.
In medieval Europe prostitution was licensed and regulated by law, but by the 16th century an epidemic of venereal disease and post-Reformation morality led to the closure of brothels.
International cooperation to end the traffic in women for the purpose of prostitution began in 1899.
In 1921 the League of Nations established the Committee on the Traffic in Women and Children, and in 1949 the UN General Assembly adopted a convention for the suppression of prostitution.
In the U.S. prostitution was first curtailed by the Mann Act (1910), and by 1915 most states had banned brothels (Nevada being a notable exception).
Prostitution is nevertheless tolerated in most U.S. and European cities.
In the Netherlands many prostitutes have become members of a professional service union, and in Scandinavia government regulations emphasize hygienic aspects, requiring frequent medical examination and providing free mandatory hospitalization for anyone found to be infected with venereal disease.
Prostitutes are very often poor and lack other skills to support themselves; in many traditional societies there are few other available money-earning occupations for women without family support.
In developing African and Asian countries, prostitution has been largely responsible for the spread of AIDS and the orphaning of hundreds of thousands of children.
It is difficult to generalize about the background or conditions of prostitutes because so much of what is known about them derives from studies of poorer and less-privileged individuals, people who are more likely to come into contact with courts and official agencies.
Much more is known about streetwalkers, for example, than about the higher-status women who can be more selective about their clients and work conditions.
Based on available studies, though, it is reasonable to assert that female sex workers often are economically disadvantaged and lack skills and training to support themselves.
Many are drawn at an early age into prostitution and associated crime, and drug dependency can be an aggravating factor.
They frequently are managed by a male procurer, or pimp, or by a supervisor, or madam, in a house of prostitution.
Health hazards to prostitutes include sexually transmitted diseases, some of which may be acquired through drug abuse.
Male prostitution has received less public attention in most cultures.
Heterosexual male prostitution—involving males hired by or for females—is rare.
Homosexual male prostitution has probably existed in most societies, though only in the 20th century was it recognized as a major social phenomenon, and its prevalence increased during the late 20th and early 21st century.
Prostitution during the Victorian age gained an unprecedented amount of attention from both British society and their government.
Although issues of prostitution were, and are often still, seen in black and white, there were many cases where prostitution was either a supplementary activity or the only available avenue of employment.
It was an unsavory profession, and, unfortunately, it was often considered a necessary evil.
However, it is important to note that although it was an activity highly frowned upon by upper class women in society, these same women were the first to rally to the cause of those “fallen women” that were being exploited by the government.
The popularity of issues concerning prostitution eventually lessened over time, but the resulting influences sparked by feminist movements involved in prostitute’s rights created a ripple effect that can be seen even today.
Working & Living Conditions. Key factors have shaped the working and living conditions of sex workers across the globe since the beginning of the 17th century.
These include the degree to which women were bound or “free”, or were able to exercise power in relation to employers and clients. Related to this is the location of individual women within the sex industry—where they existed within any particular hierarchy based on the class of clients, ethnicity, and so on.
Market forces have also been major determinants of the pay and working conditions in the sex industry. Shifts in the economy have impacted sex workers as well as other workers, affecting both the demand for sexual services and the supply of women willing to sell sex.
A third major influence on sex workers’ lives has been the responses to prostitution of the community in which they worked. This has included both informal and official responses which often determined where and how women could sell sex and under what circumstances.
The formation, expansion, and disintegration of nations and empires have had a similar impact on the market for sex and have contributed to official responses to prostitution.
Finally, developments in technology and medicine, especially since the early 20th century, have contributed to significant changes in the ways in which sexual services are delivered and also impacted the health of sex workers.
Prostitution is considered to be a profession of high mobility; it is almost tempting to say that probably every prostitute migrates at least once in her lifetime.
Despite this fact, the share of prostitutes in the flows over and across the continents has been widely neglected in migration studies.
Migration is thought to be a “basic condition of human societies” and “central to the human experience [and] the major forces for historical change.”
Nevertheless, many studies focus solely on the movements of European male settlers. In particular, labour migration was long held to be a male domain, keeping up the idea of males as breadwinners and the main actors in history.
Hoerder offers up the critique that migration studies emphasize “the westward flow of agrarian settlers and neglect [the] moves of workers and of women”
Changing places is a lifetime experience of women involved in the sex sector, and in many cases, they travel far more than people in other sectors.
The Social Profiles of Prostitutes. There is no shortage of media portrayals of prostitutes. Yet the images that inform our opinions regarding sex workers tend to be largely negative, depicting them as either criminals or as victims.
Today, the latter perception prevails: sex workers are stereotypically seen as:
young,
migrant girls with
no education and
no alternatives.
The most conspicuous types of prostitutes tend to be overrepresented, while those operating in private have largely been overlooked.
In addition to which, the “facts” about the sex workers represented in the sources may not always be entirely correct, as they might have told their interlocutors what they believed would best serve their needs, rather than what was true.
The social profiles of sex workers have changed considerably over the course of the last 400 years.
Prostitute populations have become more heterogeneous in terms of their origin, race, age, family situation, educational level, and professional background—albeit at different paces.
Example: Migrants did not suddenly appear in the western European sex trade after the fall of the Berlin Wall. Rather, they were always present, and always overrepresented in the prostitute population. What actually changed over time are the distances covered.
Similarly, prostitutes’ ages have altered in tandem with developments in society at large, most notably lengthier childhoods and a later start to working life.
While it is definitely true that certain people have limited options for survival, the high degree of diversity among sex workers clearly shows that prostitution cannot be reduced to a profession of the destitute, or one which people passively end up in.
In fact, people who are not members of so-called “vulnerable” groups might be more numerous in the sector than anticipated because of their invisibility.
The sex industry is highly stratified, and individuals with better prospects take the places at the top of the hierarchy more often than those with limited possibilities.
These women have chosen to use their bodies to create a financial surplus, and they are thought to face fewer dangers than the prostitutes working at the lower end of the market.
It seems easier for people to accept that these women actively chose their profession, and harder to view them as passive victims.
However, their underlying reasons are not necessarily different from the masses employed at the industry’s margins.
Although some women are forced into prostitution against their will one way or another, this is certainly not the case for all sex workers, let alone the majority.
Most prostitutes are driven by opportunity, and the fact that most have fewer opportunities than their contemporaries does not change that.
Simply put, prostitution can be emancipatory.
It can be a positive choice, rather than just a negative one.
Profile characteristics do not explain why people use their bodies to earn an income, but they do explain why certain people end up in the most visible and least rewarding sectors of the profession.
Brothel - a building in which prostitutes are available; bordello
Bordello - (somewhat literary) a building in which prostitutes are available
Public brothels were established in large cities throughout Europe.
At Toulouse, in France, the profits were shared between the city and the university; in England, bordellos were originally licensed by the bishops of Winchester and subsequently by Parliament.
Stricter controls were imposed during the 16th century, in part because of the new sexual morality that accompanied the Protestant Reformation and the Counter-Reformation. Just as significant was the dramatic upsurge of sexually transmitted diseases. Sporadic attempts were made to suppress brothels and even to introduce medical inspections, but such measures were to little avail.
By 1915 nearly all states had passed laws that banned brothels or regulated the profits of prostitution.
After World War II, prostitution remained prohibited in most Western countries, though it was unofficially tolerated in some cities.
Many law-enforcement agencies became more concerned with regulating the crimes associated with the practice, especially acts of theft and robbery committed against clients. Authorities also intervened to prevent girls from being coerced into prostitution (“white slavery”).
Prostitution is illegal in most of the United States, though it is lawful in some counties in Nevada.
In most Asian and Middle Eastern countries, prostitution is illegal but widely tolerated: Among predominantly Muslim countries, Turkey has legalized prostitution and made it subject to a system of health checks for sex workers, and in Bangladesh prostitution is notionally legal but associated behaviours such as soliciting are prohibited. In some Asian countries the involvement of children in prostitution has encouraged the growth of “sex tourism” by men from countries where such practices are illegal.
Many Latin American countries tolerate prostitution but restrict associated activities (e.g., In Brazil, brothels, pimping, and child exploitation are illegal).
Sources: 1 2 3 4 5 6 ⚜ More: References ⚜ Writing Resources PDFs
This was a bit difficult to summarise, but I tried to include a wide range of information from different sources. In general, take into account the setting of your story so you can choose which of these references would be most appropriate to use as inspiration for your writing. Do go through the links above because there are details I wasn't able to include here that might be more suitable for your specific story. Hope this helps!
#writing notes#writing reference#character development#writeblr#literature#writers on tumblr#dark academia#spilled ink#history#writing prompt#creative writing#writing ideas#writing inspiration#light academia#writing resources
131 notes
·
View notes
Text

In 2017 I interviewed Bernadette Wren, then head of psychology at the Tavistock Gids clinic, and asked what effect puberty blocking drugs have on the adolescent brain. Looking highly uncomfortable, she replied that the evidence so far was only anecdotal but that the clinic would study its patients “well into their adult lives so that we can see”.
Even back then, before whistleblowers had exposed the rush to medically transition children, it was alarming to hear that heavy-duty GnRH agonists such as triptorelin — used to treat advanced prostate cancer and “chemically castrate” sex offenders — were being prescribed to arrest puberty in hundreds of children as young as 11.
Moreover, they were being used “off-label” before any clinical trials. And the long-term study Wren promised never materialised: Gids (the Gender Identity Development Service) routinely lost touch with patients, and the 44 it did follow reported little long-term mental health improvement.
This shocking chapter in medical history, where the ideological objectives of trans rights campaigners trumped the welfare of disturbed children, is coming to an end worldwide. The decision by NHS England effectively to ban the prescription of puberty blockers comes after the Cass review noted these drugs could “permanently disrupt” brain development, reduce bone density and lock children into a regime of cross-sex hormones requiring life-long patienthood.
NHS England unites with other national health services including those in Finland, France, Sweden and, most notably, the Netherlands — where the “Dutch protocol”, a regime of early blockers then hormones, was devised in 1998 — in pulling back from prescribing them.
Even in the United States, where a toxic combination of extreme activism and medical capitalism has pushed child gender medicine to grotesque extremes, with double mastectomies performed on 14-year-old girls, there is some retrenchment.
Leaks from the World Professional Association for Transgender Health, the body which formulates guidance on “trans healthcare”, reveal doctors perplexed at how they should explain to an 11-year-old child that drugs will render them infertile. Crucially, liberal media such as The New York Times are now reporting grave medical misgivings about child transition, once dismissed as a culture-war issue for the Republican right.
Yet the question remains: how was this ever allowed to happen? For years, puberty blockers were cheerily billed as a mere “pause button”. In 2014, Dr Polly Carmichael, the last head of Gids before the Cass review ordered its closure, went on CBBC in a show called I Am Leo, saying of blockers: “The good thing is, if you stop the injections, it’s like pressing ‘start’ and the body carries on developing as it would if you hadn’t started.”
The BBC permitted her to make this unevidenced claim to an impressionable audience of six to 12-year-olds. Imagine hearing this as a developing girl, freaked out by your new breasts and periods. No wonder Gids referrals subsequently rocketed.
Carmichael failed to mention that she did not know if pressing “restart” on puberty is always medically possible — it is not — and in fact, almost every child Gids put on blockers went on to irreversible cross-sex hormones.
After years in a Peter Pan state while their peers developed, they understandably felt there was no way back and forged on with treatment. Yet if allowed to experience natural puberty, almost 85 per cent of gender dysphoria cases resolve themselves.
Nor did Carmichael tell CBBC kids that the blockers-hormones combination, if taken early enough, not only results in sterility but kills the libido so that a young person will never experience an orgasm.
At the 2020 judicial review brought by a former Tavistock clinician and Keira Bell, the brave young detransitioner rushed onto hormones by Gids, judges expressed astonishment at Gids’s lack of an evidence base.
Reporting on this issue for seven years, I too have been struck by a complete clinical incuriosity. Not only was data not collected, but those who queried treatments or pressed for evidence faced angry condemnation. Perhaps activists knew what research might find because one long-term Finnish study, recently reported in the BMJ, destroyed the myth used to justify blockers: that a child will commit suicide if denied them.
The Finns found that “gender-affirming care” does not make a dysphoric child less suicidal. Rather, such children had the same suicide risk as others with severe psychiatric issues. In other words, changing bodies does not fix troubled minds.
Yet even after NHS England’s announcement, activists refuse to heed the now-overwhelming evidence. In its response, Stonewall persists with the myth that puberty blockers “give a young person extra time to evaluate their next steps”.
Many questions remain unanswered: will private clinics still be permitted to prescribe puberty blockers; and is Scotland’s Sandyford child gender clinic still determined to close its ears to all evidence? Plus, we have few details on how the NHS’s new “holistic” treatment for gender-questioning children will operate when it opens next month.
This repellent experiment — in which girls who like trucks or little boys who dress as princesses, and who invariably grow up to be gay, are corralled inexorably down a road towards life-changing treatments — belongs in the book of medical disgraces. As do the cheerleaders who raised money for Mermaids and those who persecuted whistleblowers or damned journalists asking questions as transphobic.
In 50 years, chemically freezing the puberty of healthy children with troubled minds will be regarded with the same horrified fascination as lobotomies — which, never forget, won the Portuguese neurologist Antonio Egas Moniz the 1949 Nobel prize.
--------------------
{Article source (behind paywall)}
242 notes
·
View notes
Text
The order is very comprehensive. It prohibits federal funds, support, or promotion of pediatric gender-affirming medical interventions. Included in that is a directive that medical institutions that engage in pediatric transgender treatments will lose federal research and education grants. Federal health insurance programs, such as Federal Employee Health Benefits, Postal Service Health Benefits, and TriCare, do not cover the treatments. The Departments of Health and Human Services, Defense, and Justice are directed to take action to reduce the use of puberty blockers, hormone therapies, and gender-related surgeries for individuals under the age of 19. The order also targets the alleged science behind the treatments. It calls out the World Professional Association for Transgender Health (WPATH) Standards of Care Version 8 as "junk science” (The Arguments Supporting 'Gender-Affirming Care' Have Never Been 'Based on the Science' – RedState) and directs all agencies to "rescind or amend all policies that rely on WPATH guidance." As a kicker, the Department of Justice is directed to investigate deceptive practices or misinformation regarding the long-term effects of gender-affirming care, including potential fraud or violations of the Food, Drug, and Cosmetic Act. Overall, it is wide-ranging on the idea that children should undergo chemical or surgical mutilation. It attacks the alleged science behind it, cuts off cash flows (Vanderbilt University Halts Transgender Surgeries After Exposés by Matt Walsh, Tucker Carlson – RedState), and makes practitioners vulnerable to civil liability and criminal charges.
Well past time to end this nonsense.
46 notes
·
View notes
Text
Gender, Dissociation and Clinical Stigma - The Third Person
Before I begin I just want to note that typically Media, Myself and I entries are aimed at depictions of dissociative disorders in popular fiction. Today's entry is a graphic novel memoir by a transgender woman with dissociative identity disorder. As it's both not in the public zeitgeist and good representation by virtue of being lived experience of someone who struggled within the mental healthcare system I want to recommend people buy the book (or check it out of their local library). I fully support the artist and want to prop up something good and beautiful.
With that said, let's begin...

CW: therapy abuse
With all the recent hysteria in the US and UK media over transgender healthcare it can be easy to forget the hurdles we all have to climb to receive care. Though Informed Consent is becoming more of a standard practice these days the DSM-5 Criteria for Gender Dysphoria indicates a 6 month requirement for observation before HRT can be prescribed. Many of us needed to jump the hoops of living 6-12 months "in the gender role that is congruent with their gender identity" before we were allowed to begin our gender journey in earnest.
Of course. This requires a clinician (or two for surgical options) to observe this, monitor it and sign off on it. But therapists are humans and are full of prejudice, bias and their own beliefs. They aren't guaranteed to think it is medically necessary or positive for a person seeking gender affirming care to receive it.
So where does DID fit into this picture?
A study, published in 2015, states clearly that 30% of transgender individuals met the criteria for a dissociative disorder.
Yet even still, The World Professional Association for Transgender Health (WPATH), the gold standard for transgender care included this warning in their Standards of Care up until September 2022.
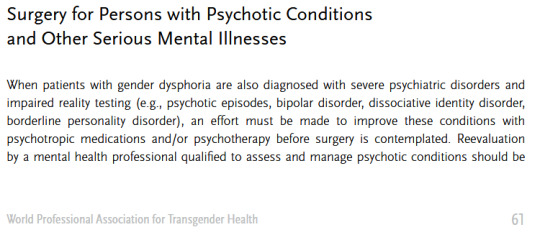
(source)
Fortunately that passage is no longer included in WPATH guidelines as of the 8th revision released in 2022. I shall say the above passage did grant a scare for us, though, as it was very much the practice when we were going for our surgery.
Standards of Care improve and medical understandings of both gender and dissociative care are becoming kinder towards clients.
Even still. There's always that fear. That months of therapy could be wasted on a clinician who was never going to sign off on HRT and was never going to believe our lived experience as a system.
We wouldn't have gotten nearly half as far as we have gotten without our therapist helping us identify our condition, manage our symptoms and develop cooperation and communication.
It's terrifying to think what life would be like if our symptoms not only went unmanaged, but we were made to feel fake and attention seeking by the very person we paid to take care of us...
-
With that intro in mind, The Third Person by Emma Grove is a memoir told in graphic novel format over 920 pages covering the period of life where she began therapy in hopes of receiving feminizing HRT not realizing she had an undiagnosed case of dissociative identity disorder.
When one opens the book they will see an Author's Note declaring that every word in the book is as accurate as Emma's memory will allow and any edits are to streamline the story, not to tailor anything to match the author's point of view and there is a dedication:
"For Katina - We finally did one together"
The story proper begins in media res Winter 2004, as Emma asks her therapist if he would like to hear about the book she was reading and the therapist responds asking why the client decided to speak with him "as Emma" today. Emma, confused, does not understand the question and is probed about her parts, about Ed and Katina and about her childhood. That last word being enough to cause Emma to freeze up, dissociate and...
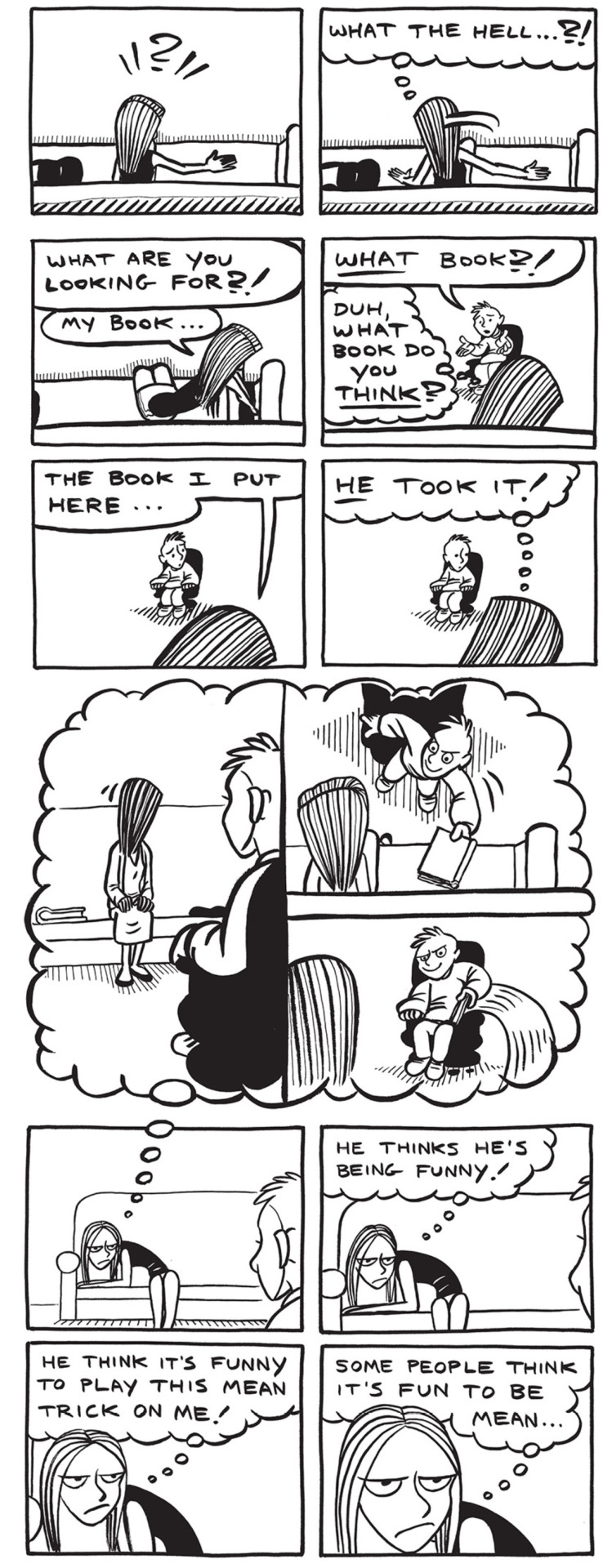
This simple intro gives us all the context a reader needs to understand the antagonistic dynamic between Toby, the therapist, and his patient(s). Both client and patient are unable to understand the other and harbor suspicions about the other's intentions.
Without the context we only know Emma had a book, she no longer has a book and she suspects her therapist of being a mean person who is playing tricks on her.
We will get context later.
The first chapter of the book provides an introduction to the author's late teens and early 20s where they explore their gender identity and have their first experiences with their masked dissociative disorder.
The book goes to lengths to show the stress of the author dividing themselves between having to present male in their public life and sneaking out to bars where they can wear make-up, wigs and outfits to present female.
They take on their legal name, Ed, during their public life and when going out to clubs take the name Katina, from the first bar they visited presenting femme. The name Emma comes later when the system is working to transition into living as a woman in all aspects of their shared life.
The book patiently explores the stress of having to divide ones own self for their safety in spaces where they cannot present their truth without threat from an intolerant society. If 30% of transgender people suffer from dissociative disorders then a much higher number of them know the stress of having to compartmentalize themselves into different presentations for different audiences.
For us, we know that pain all too well. Our birth identity remains with us as a member of our own system. Less a ghost of our past and more a remnant of a mask we constructed to perform the version of self required for our safety.
The artwork does a good job of displaying switches and co-consciousness with subtle expression work, the hair style/wigs that each alter favors. For example we have the left displaying co-consciousness and a switch.


As the years go on, Katina finds ways to go out to the club and exist in her comfort and Ed labors hard to ensure that they can live for the times they get to "become" themselves.
Katina is established to be a fierce personality who will get aggressive when people push against her. She loves to dance and sing and party at the club. She is both a free spirit without inhibition and a fierce protector who will keep the system safe.
I recall feeling a deep fondness and connection towards Katina when we first read the book.
Once the narrative has firmly established the history that lead to the system seeking HRT we are brought into the meat of the book. A white void with a sofa and an armchair. The therapist's office where Katina, Emma and Ed speak with Toby.
Toby is a trans man that Katina believes to be an ally who will sign off on their HRT once the prerequisite 3 month waiting period is over. Unfortunately over the course of those months Toby becomes aware of Emma and Katina's switches and is convinced that it would be unethical for him to sign off on HRT when it is possible that there may be another 'guy part' in there who will 'wake up' one day and decide that he did not want to transition.
To his credit, once Toby suspects a dissociative disorder he does offer Emma a referral to a specialist. They do not take it as they just want to be signed off for HRT and have no interest in exploring their situation beyond transitioning. So they stick with Toby, convinced that another transgender individual will support them.
Toby, however, sticks to his guns and refuses to agree until they manage the DID.

In the opening, sampled above, Emma switches out at the mere mention of her childhood. Here we find that Katina will front any time Emma is made to think about her past and she refuses to allow Toby to force her to think about it or discuss it. She goes as far as to demand Toby promise not to push which, again, Toby refuses.
During this conflict both sides have exaggerated gestures of frustration, many exclamation points and underlined words. This is not a healthy dialogue at all. Toby is refusing to find middle ground or guide the therapy towards its intended destination. He denies all Katina's attempts to negotiate around the need to talk about her childhood (something she is convinced at this point has nothing to do with her stated goal of HRT) and continuously pushes that she needs to talk about it, without elaborating as to why.
Toby, untrained in dissociative disorders, is focused on getting her to open up about her childhood trauma. Katina, uninterested in exploring trauma, wants to be signed off for HRT. Neither side is willing to budge.
This isn't therapy. This is an argument.

Recently I wrote a Tumblr post about the "Hair Dryer Incident"
The Hair Dryer Incident is a story about a patient with OCD whose life was being massively disrupted by the fear that they had left their hair dryer plugged in at home and it would burn their house down. The clinician advised them to take the hair dryer to work with them every day so that they could see the hair dryer with them and not have to drive home to ensure it was safely unplugged.
There was debate in medical circles about whether this was "enabling" because it did nothing to treat the illness, only managed the life disrupting symptom of needing to drive home to check that the dryer was not plugged in.
For Toby in this scenario he believes that allowing Emma to transition would be "enabling" the sickness that he perceives, that being dissociative identity disorder. He has brought his own baggage into the office and only views Emma and Katina as parts of Ed. No amount of Emma and Katina self-advocating in his eyes will change his mind because they are not "real" in his view.
Of course, he is not fully sold on Emma's condition being real either. There is a sequence in which Emma is left alone in the room and she, having a fascination with books, checks out Toby's bookshelf. This causes Toby to become suspicious and decide that Emma has been reading the medical textbooks on dissociative disorders in order to fake an illness and trick him.
This is not a healthy therapeutic alliance and Toby is breaking all 3 key pillars of establishing a strong patient/client partnership.
Much of modern therapy techniques are based on the concept of Therapeutic Alliance. The history of which dates back to Sigmund Freud and the concept of transference but was refined and redefined by Carl Rogers in the modern Patient Centered Therapy (sometimes referred to as Rogerian Therapy).
With that in mind let's examine the 3 key elements of successful PCT(*) and how Toby failed.
Lead with a Patient Centered Approach This means to check all baggage at the door. Cultural biases have no room inside the clinic (during the book Toby openly mocks Emma's faith in God) and that the patient's priorities are the ones that should be focused on. Both client and clinician should be on the same page of what treatment is being sought, what goals are and how they will be achieved. Toby and Emma (or Katina and Ed) never establish this agreement during their time together. Katina/Emma/Ed are firm in their desire to transition and Toby is firm on his refusal to allow this until the DID is addressed.
Set clear goals with a treatment plan. A good treatment plan will have dates, targets and regular review and reward honesty for both/all parties involved in the alliance. Toby is telling Emma and Katina that they need to open up about their childhood but does not explain how this will benefit or what their goals are. Simply "it's good to talk about it" with no direction or assurances.
Regularly review satisfaction with the therapeutic process, relationship, and treatment plan. This element states that it is important that the clinician be upfront with any potential misdiagnosis and discuss any skepticism in the process and lead from a position of patient satisfaction. I do not need to highlight how Toby failed to lead from a position of patient satisfaction here.
Clearly Toby has a personal concept of what the correct approach is and is holding Emma/Katina's gender affirming care hostage until they can satisfy his unspoken objectives. Correctly applied PCT should be a discussion of mutual agreement and achievable goals worked over a period of time. Toby is not applying these principals at all. His modality simply seems to be "talk about it." I'll be an ethical writer who discloses their biases and say I despise PCT/Rogerian therapy. It is, however, the leading modality within western therapy and it is well researched. Not to mention it is the modality Toby appears to be utilizing in the book. I firmly disagree with Freud on all things (except the concept of infant experiences have lifelong ramifications. A broken clock is right twice a day) and disagree with Rogers on the idea that the client has all of the answers and needs to get out of their own way. An issue with this is that DID is a covert disorder and it will do everything it can to stay hidden. PCT does not offer an environment where patients will be able to navigate their condition as unless they are aware of their symptoms, how and when they manifest and are open to discussing those facts they will naturally steer away from circumstances that would lead to a diagnosis. Most people, including myself, have to exist in the mental healthcare system for 5-12 years before being correctly diagnosed with DID(*) and will experience a number of incorrect diagnoses before finding appropriate care. For us it was 9 years and 7 diagnoses. So. Toby's directive is that the system needs to get to the root of the condition and neither Katina nor Emma are willing to open up about their childhood. Katina continues sticking to her guns and refuses but Emma, desperate to start her medical transition, agrees to open up and the two form a shaky alliance where week by week the pair go back and forth between alliance and conflict. In time Emma describes her childhood being raised by her grandfather who was physically abusive towards her. All too quickly Katina's fears are justified by Toby's combative approach to patient care. One session Emma demands to know why she cannot work on her DID while she transitions and Toby states firmly that she is "not transsexual" which triggers Emma to dissociate into a black void that no one can reach her within. She wanted to be seen and regarded as a woman and a trans man told her flat out that he cannot and does not see her as such. Going back to the hair dryer incident as a reference for a moment. Ed is a member of the system and does show up for therapy on some days. At a point Katina, fed up with being denied treatment, makes a plan to quit their job and start a new life living as a woman 24/7. Ed creates a safety net to prevent this from ruining their collective life and continues to work in the meanwhile. Ed's role in the system has been ground down to working and working alone. He spends his days keeping so busy that he cannot dwell, a panel having the thought bubble "I can't slow down! If I slow down I have to think!" which is depressingly relatable to how we were in the worst years of repressing our gender identity. If Ed is unhappy living as a closeted man who has to occupy himself 24/7 to stop from caving in on himself, if Emma and Katina are both completely stunted by their inability to transition; is it ethical to allow them to transition and to work on their condition while allowing them the freedom to live openly as their chosen gender and prevent a circumstance that is harming the entire system? Toby seems to think it is enabling.
30% of the transgender individuals in the study above were observed to meet the criteria for a dissociative disorder. Living a life where one must mask has severe detrimental impacts on a person's psychology. This is true not just for transgender individuals but for those with autism (*) and other individuals on the LGBT spectrum (*) where the cognitive dissonance between who a person values themselves to be versus how they must present to the world causes the mind to dissociate further and allow contrary thinking to exist in individual pockets of a person's life as well as creates an alienation of the self. Healing under these circumstances requires accepting and embracing oneself, not creating a further divide.
After Toby "caught" Emma looking at the bookshelf he became convinced that she was faking her condition. That she had been plucking symptoms from a book and performing them for him. That she fit the criteria "too well"
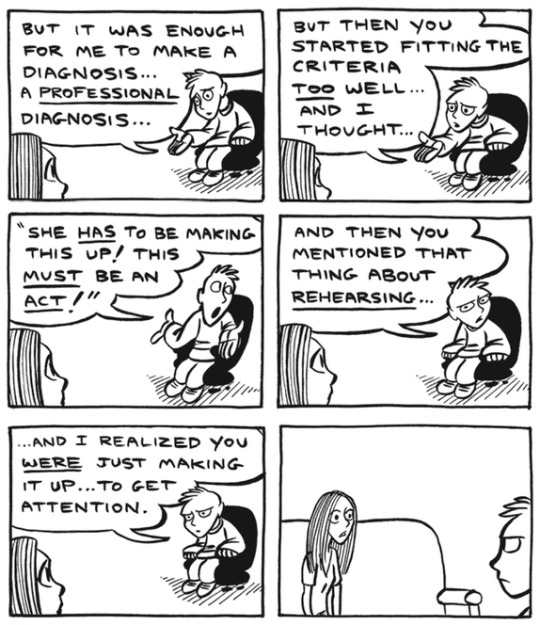
Emma rightfully demands to know why she would complicate her receiving HRT by doing something that prevents her being able to. The pair bicker and Toby cuts off the session abruptly.
in the heat of the moment, assuming that Emma was an attention seeker who does not deserve care, Toby declares "Your grandfather was right to hit you."
Even Emma later admits later that therapy should have ended with Toby right there and then. Hindsight is 20/20, as they say. Alas, a mixture of finances and sunk cost keep Emma returning to the chair week after week.
Being trans and having DID are terrifying. In order to receive care and treatment we must insist to a world that what is happening in our hearts and minds is true in spite of all that the world outside tells us is true. We need to not only reach that conclusion within our own lives but must express that truth loud enough that the people around us see it, regard it and accept it.
As so many things in this world are, it's so hard to earn and so easily burned.
"You're faking it for attention" is such an easy sentence to fling at someone and in a therapeutic setting all things should lead to curiosity. Even if a person were faking, it's not normal and healthy behavior for someone to do that. Toby is displaying a complete lack of curiosity and compassion. He is framing himself as the victim in a potential deception from someone who is paying what little money they can put together to receive his care.
I hate Toby.
As the story continues, Emma and her system begrudgingly continue, flitting back and forth between a healthy and unhealthy dynamic with their therapist that shares a lot of similarities to abuse honeymoons. It is worth noting that as the book is a memior it will inevitably be painted with the author's personal view of past events because, as discussed in the Umineko article on recontextualized memories, a human mind cannot avoid applying present understandings to past experiences when recalling memory. This is seen in the book when we see things that Emma cannot possibly have witnessed, such as Toby's facial expression after she leaves the office.

This is not to throw shade at how Emma depicts her former therapist, as he was quite horrid to all 3 of them and quite obviously did more harm than good during their time together. I just wish to note that skewed perspectives are an inevitability. Even still. They do make some progress in talking about the situations. We come to learn of the system origins and how Katina was a friend to the young and lonely child they used to be and that their abusive childhood was centered around physical abuse from their grandfather. While discussing this Emma notes that she could make Katina go away forever with a single phrase. A few short words that she can never ever say and mean or Katina would go away and never come back... and I think that's where I'll stop with the synopsis. I (specifically me, Dawn) broke down in tears the first time I read the book and I have no will to put myself through that again at this exact moment and I wish for you all to have the catharsis of experiencing it for yourself.
I will say in way of positivity that the story is quick to make its conclusions in the final chapters by displaying therapy done right and the fact that even if parts can no longer be heard or even felt, they will always endure in moments where they can add a little color to the world.
They got to write this book together, after all.
For all the sadness this memoir elicits it speaks an honest and hard truth of the desperation, isolation and confusion that can be found in managing sentiments of identity and gender in a time when there was so little understanding and acceptance, particularly for transgender people.
We are lucky these days to have the internet as it is where we can create community and find our people and in finding our people have a better understanding of who we are and how we can live our truths. Visibility of transgender and plural populations has been increasing in part due to the fact we are able to feel unalone and forge community.
2004 did not have those luxuries and I am saddened that Emma Grove had to live through that stigma and lost so much time to unethical and prejudice care from a clinician.
I do hope that in the future we can continue accepting and encouraging one another and living lives where we are not forced to hide, mask or pretend.
-
For other Media, Myself and I articles, please check out the following:
#dawn posting#media myself and i#media essays#plurality#did#watch me post my trauma in public#this is my gender and I am proud of it
84 notes
·
View notes
Text
While the Cass Review has been presented by the U.K. media, politicians and some prominent doctors as a triumph of objective inquiry, its most controversial recommendations are based on prejudice rather than evidence. Instead of helping young people, the review has caused enormous harm to children and their families, to democratic discourse and to wider principles of scientific endeavour. There is an urgent need to critically examine the actual context and findings of the report. Since its 2020 inception, the Cass Review’s anti-trans credentials have been clear. It explicitly excluded trans people from key roles in research, analysis and oversight of the project, while sidelining most practitioners with experience in trans health care. The project centered and sympathized with anti-trans voices, including professionals who deny the very existence of trans children. Former U.K. minister for women and equalities Kemi Badenoch, who has a history of hostility toward trans people even though her role was to promote equality within the government, boasted that the Cass Review was only possible because of her active involvement. The methodology underpinning the Cass Review has been extensively criticized by medical experts and academics from a range of disciplines. Criticism has focused especially on the effect of bias on the Cass approach, double standards in the interpretation of data, substandard scientific rigor, methodological flaws and a failure to properly substantiate claims. For example, although the existing literature reports a wide range of important benefits of social transition and no credible evidence of harm, the Cass Review cautions against it. The review also dismisses substantial documented benefits of adolescent medical transition as underevidenced while highlighting risks based on evidence of significantly worse quality. A warning about impaired brain maturation, for instance, cites a single, very short speculative paper that in turn rests on one experimental study with female mice. Meanwhile extensive qualitative data and clinical consensus are almost entirely ignored. These issues help explain why the Cass recommendations differ from previous academic reviews and expert guidance from major medical organisations such as the World Professional Association for Transgender Health (WPATH) and the American Academy of Pediatrics. WPATH’s experts themselves highlight the Cass report’s “selective and inconsistent use of evidence,” with recommendations that “often do not follow from the data presented in the systematic reviews.” Leading specialists in transgender medical care from the U.S. and Australia emphasize that “the Review obscures key findings, misrepresents its own data, and is rife with misapplications of the scientific method.” For instance, the Cass report warns that an “exponential change in referrals” to England’s child and adolescent gender clinic during the 2010s is “very much faster than would be expected.” But this increase has not been exponential, and the maximum 5,000 referrals it notes in 2021 represents a very small proportion of the 44,000 trans adolescents in the U.K. estimated from 2021 census data.
7 August 2024
57 notes
·
View notes
Text
Jasmine Mithani at The 19th:
A network working to end female genital mutilation and cutting (FGM/C) in the United States and globally says President Donald Trump’s January 28 executive order attempting to restrict gender-affirming care for transgender youth “wrongly and dangerously” conflates the two.
Opponents of transgender rights have sought for several years to co-opt anti-FGM/C laws to further gender-affirming care bans, mostly in state legislatures. The executive order builds on these efforts by directing the Department of Justice and state authorities to review and prioritize the enforcement of laws banning FGM/C, which are unrelated. FGM/C is a human rights violation and one of the most extreme forms of gender-based violence. According to the World Health Organization, FGM/C “comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons.” It is practiced across many cultures and takes many forms, and is most commonly performed on young girls who are unable to consent. There are no health benefits to FGM/C, and it is more likely to cause medical complications.
In contrast, gender-affirming genital surgeries like phalloplasty or metoidioplasty are medically necessary and done only with the consent of the patient. The World Professional Association for Transgender Health, the international body that publishes research-backed standards of care, does not recommend genital gender-affirming care surgeries for patients under 18. Extensive documentation from medical professionals is required for any medically necessary gender-affirming care surgery. It is estimated that in 2012, over half a million girls in the United States had either undergone FGM/C or were at risk based on the country of origin of their parents. Survivor advocates think the number could be much higher now.
FGM/C has been a federal crime since 1996. The law has been revised several times — most recently in 2020, when Trump signed the STOP FGM Act, which prevented defendents from using religious or cultural reasons to avoid prosecution.
[...] Anti-trans extremists have warped these laws to ban health care for trans people “despite clear medical and ethical distinctions,” said Ash Lazarus Orr, press relations manager at Advocates for Trans Equality. Orr also pointed out that this rhetoric excludes non-consensual surgeries performed on intersex youth. Many bans include a carve-out ensuring “corrective” surgeries remain legal for minors with intersex characteristics. Republican lawmakers in Idaho and Texas introduced bills in 2022 that would remove the word “female” from current legal codes banning FGM/C. Anti-FGM/C advocates helped defeat those bills, but Idaho ended up passing a separate law banning gender-affirming care for transgender youth the next year. Excluding the word “female” means these laws no longer prevent FGM/C because they then refer to something else entirely, said Kaitlin Mitchell, policy and advocacy coordinator at the U.S. Network to End FGM/C. Using the laws to restrict gender-affirming care instead of addressing the specific issue they were designed to make it harder for advocates to campaign for more funding or research on this little-known, severe form of gender-based violence.
Donald Trump’s false and transphobia-laden characterizing of gender-affirming care for trans youths as “mutilation” served as the basis for Executive Order 14187, which bans gender-affirming care services for trans youths and adults under 19.
The false characterization of GAC as “mutilation” trivializes the real issue of female genital mutilation.
#Donald Trump#Gender Affirming Care#Transgender Health#Female Genital Mutilation#Transgender#Gender Affirming Healthcare#Anti Trans Extremism#Executive Order 14187#Trump Administration II
32 notes
·
View notes
Text
Ho boy I just got hit with a wave of HRT related asks.
I'll respond to them to the best of my ability, but imma make a copy/paste disclaimer here:
I AM NOT A MEDICAL PROFESSIONAL. I have a very, VERY marginal ability to interpret medical data over the average person due to my bio background, but it's far less than people think- hell I just said something wrong about insurance that someone had to correct.
Unfortunately, however, the nature of trans healthcare being under constant political threat worldwide means that everyone should prepare to diy, and know the basics of how they would pull that off. That's why I'm answering these questions, more info out there is always better. HOWEVER, you would better be served by other sources, like:
Anything I say directly about medical care will be an interpretation or regurgitation of something that is likely in these sources, plus a dash of personal experience. My bio knowledge and interpretation is not going to kick in here, it's gonna be too far deep in the weeds of cellular mechanisms that it's not directly relevant.
85 notes
·
View notes
Text
By: Leor Sapir
Published: Feb 14, 2025
On January 28, President Trump signed an executive order titled “Protecting Children from Chemical and Surgical Mutilation.” The order’s most important provision defunds health-care and medical education institutions that engage in or facilitate sex-trait-modification procedures for adolescents 18 or younger. Within a week, at least ten hospitals in states where these procedures are still legal announced that they were changing their practices. The list includes some of the top pediatric gender clinics.
On February 4, the American Civil Liberties Union announced a lawsuit challenging the executive order. Joining the ACLU in the suit are other transgender advocacy groups and two law firms, which together represent two trans-identified 18-year-olds and five trans-identified minors and their families; they also represent PFLAG National, an LGBT organization with nearly 350 chapters nationwide, and the named plaintiffs.
The suit alleges that the executive order exceeds Trump’s Article II powers by directing “public funds to advance the President’s policy preferences, rather than those of Congress.” It argues as well that the EO discriminates based on sex—a claim also made against Tennessee’s ban on pediatric “gender-affirming care,” which the Supreme Court is considering in U.S. v. Skrmetti—and violates plaintiffs’ constitutional rights to equal protection and due process under the Fifth Amendment. Finally, and most surprisingly, it alleges that the order violates Section 504 of the Rehabilitation Act of 1973, which prohibits discrimination because of disability in federally funded programs. Gender dysphoria, the ACLU claims, is a disability of the kind protected by this law.
On February 13, a federal district court in Baltimore blocked the executive order’s defunding provision from going into effect for a period of 14 days, at which point the court will reassess. The Department of Justice is expected to appeal these injunctions to the Fourth Circuit and, possibly, to the Supreme Court.
The ACLU’s case contains an unusual feature. One of the plaintiffs, Cameron Coe (pseudonym), is a 12-year-old New York–area resident who received a puberty-blocking injection in 2024. Cameron was scheduled for a puberty-blocking implant at NYU Langone the day after the executive order went into effect. Unlike plaintiffs in similar suits, however, Cameron does not identify as a boy or a girl. When Cameron was born, “they [sic] were designated as male. From the age of four, Cameron communicated to their parents that they were neither a boy nor a girl. They began to express their nonbinary identity in the fourth grade.”
The suit never defines the term “nonbinary.” Instead, it lists “nonbinary” as a “gender identity,” which it defines as “a person’s internal sense of belonging to a particular gender.” The complaint does not define “gender,” either, or explain how a “particular gender” can include no “particular gender,” which is presumably the substance of a “nonbinary” identity.
People across time and civilizations have felt that they did not fit into their society’s sex-role expectations. Contemporary therapeutic culture, empowered by novel medical technologies and theories from the postmodern academy, has recast this enduring human experience as an innate “identity” corresponding to a distinct type of human. Girls who once would have been referred to as “tomboys” are now “nonbinary” and part of the “LGBTQIA+ community.”
Nonbinary is the “fastest growing” gender category among adolescents and young adults, according to the U.K.’s Cass Review. As Jean Twenge reports in Generations, according to U.S. Census data, by 2022 more than 3 percent of those born in the 2000s identified as transgender and nearly 5 percent identified as nonbinary, representing a rise of 48 percent and 60 percent, respectively, from 2021. The U.S. Transgender Survey of 2015 found that close to one-third of its nearly 28,000 adult respondents identified as nonbinary, 80 percent of whom were female. By 2022, 38 percent of 92,329 respondents identified that way, with similar female overrepresentation.
The phenomenon of (mostly female) celebrities “coming out” as nonbinary, adopting “they/them” pronouns, and receiving instant media attention has become familiar to many in the West. This would likely be of less public interest if not for the fact that kids who embrace the nonbinary label are being offered irreversible medical interventions on that basis.
In its legal filing against the Trump executive order, the ACLU appeals to medical “guidelines” supported by “[d]ecades of clinical experience and a large body of scientific and medical literature.” The ACLU doesn’t specify which “guidelines” it has in mind, likely because it is referring to the��now-discredited World Professional Association for Transgender Health’s “Standards of Care,” Version 8.
SOC8 introduced several innovations on SOC7, among them chapters on “eunuchs” (a “gender identity” that WPATH claims even children can have) and on nonbinary identity. WPATH states that nonbinary identity “first emerged in approximately the late 2000s.” The term
includes people whose genders are comprised of more than one gender identity simultaneously or at different times (e.g., bigender), who do not have a gender identity or have a neutral gender identity (e.g., agender or neutrois), have gender identities that encompass or blend elements of other genders (e.g., polygender, demiboy, demigirl), and/or who have a gender that changes over time (e.g., genderfluid).
WPATH writes that nonbinary “may communicate a specific consciously politicized dimension to a person’s gender” but also that it “functions as a gender identity in its own right.” Rather than explain the tension, WPATH reverts to cliché: “the same identities can have different meanings for different people, and the use of terms can vary over time and by location.”
Further:
A non-linear spectrum indicates differences of gender expression, identity, or needs around gender affirmation between clients [missing word?] should not be compared for the purposes of situating them along a linear spectrum. Additionally, the interpretation of gender expression is subjective and culturally defined, and what may be experienced or viewed as highly feminine by one person may not be viewed as such by another. . . . [Health care providers] benefit from avoiding assumptions about how each client conceptualizes their gender and by being prepared to be led by a given client’s personal understanding of gender as it relates to the client’s gender identity, expression, and any need for medical care.
The expectation, standard in gender medicine, that clinicians be “led by their patients” is never more applicable than when treating individuals whose “gender” and “embodiment goals” have no parallel in nature.
WPATH recommends various procedures to help those who feel neither male nor female align their bodies with their “internal sense of gender.” These include surgeries like “penile-preserving vaginoplasty” and hormone micro-dosing. Unlike male-to-female or female-to-male “transitions,” where the end goal is to resemble the opposite sex, nonbinary medicine lacks defined objectives. It is entirely dependent upon the patient’s subjective, idiosyncratic (or as WPATH puts it, “particularly diverse”) goals.
Nonbinary is both the result and a likely cause of gender medicine’s drift away from a clinical model, which at least pretended to care about evidence-based medicine, toward an autonomy-focused framework that deems cosmetic procedures “medically necessary,” for insurance purposes. The autonomy model discourages “gatekeeping” and insists that physicians’ proper role is to counsel “clients” (“patients” is too stigmatizing) on the technical possibilities and limitations of drugs and surgeries. If a male wants “softening of skin and reduction in facial hair growth” but not “breast growth,” WPATH says, the doctor must explain that estrogen will inevitably result in the latter. If a female patient wants testosterone for “facial hair development,” she should be told that this comes with “genital growth” (i.e., clitoral growth that can result in chronic, painful chafing). Gender surgery centers across the U.S. now offer clients a range of a la carte procedures catered to their individual “embodiment goals.”
If you are wondering what any of this has to do with medicine, you’re not alone.
What of the ACLU’s claim that the Trump executive order negates “[d]ecades of clinical experience and a large body of scientific and medical literature”? According to SOC8, “The most robust longitudinal evidence supporting the benefits of gender-affirming medical and surgical treatments in adolescence” comes from the Dutch studies that launched the field. Considered the “gold standard” of evidence for such treatments, the initial outcomes of the Dutch pseudo-experiment were reported in two papers, published in 2011 and 2014. Lurie Children’s Hospital gender clinician Aron Janssen, who has served as an expert witness in gender-medicine lawsuits, attested in a 2022 Florida hearing that the Dutch data are “the best . . . we have.”
The Dutch first proposed early intervention as a possible solution to a problem that they observed in their adult patients: “subjective well-being of the transsexuals has increased, whereas an ‘improvement’ in their actual life situation is not always observed.” The Dutch clinicians theorized that their patients’ difficulty passing, a problem they attributed to the irreversible effects of puberty on the body, was a key reason for their psychosocial dysfunction. The problem, in short, was “wrong puberty”—that is, a puberty that a kid doesn’t want—and the solution, for adolescents in these situations, was the administration of puberty-blocking hormones.
Showing at least superficial awareness of the ethical problems involved, the Dutch devised what they thought were strict eligibility criteria. Only adolescents with documented history of gender distress arising in childhood and who had a strong desire to be of the opposite sex were considered. Crucially, what we today call nonbinary was seen as a contraindication—a sign that an adolescent’s sense of self was unstable. Such youths were ineligible for medical intervention. As the Dutch clinicians wrote: “adolescents… whose wish for sex reassignment seems to originate from factors other than a genuine and complete cross-gender identity are served best by psychological interventions” (emphasis added).
The Dutch approach quickly “escaped the lab,” was grafted onto a nascent transgender-rights movement, and became entrenched as the standard of care shorn of its original safeguards in multiple Western countries. Rates of transgender identity and gender dysphoria in youth skyrocketed, partly because “being transgender” was popularly redefined such that it was indistinguishable from regular gender nonconformity or puberty-related angst. Adolescent girls, most with mental-health challenges and no documented history of gender non-conformity in childhood, became the primary demographic identifying as trans and being referred to gender clinics.
Society’s shifting conceptualization of sex and gender coincided with a change in the rationale for early intervention. No longer was it about trying to detect future (mostly male) transsexuals and help them pass. No longer were puberty blockers envisioned as diagnostic tools that would allow patients “time to think.” The goal was now to help “trans kids” who “know who they are” to realize their autonomy and achieve their unique “embodiment goals.” The “child’s sense of reality,” explains the lead author of the American Academy of Pediatrics’s statement on gender medicine, is the “navigational beacon to . . . orient treatment around.” And that sense of “sense of reality” need not be binary. All individuals now had a right to “gender euphoria,” regardless of age, mental-health status, or comfort with the sex binary.
One of the architects of this new way of thinking is UC San Francisco’s Diane Ehrensaft. “[N]othing less than a gender revolution is going on,” the Bay Area child psychologist gleefully declared in her 2016 book, The Gender Creative Child. “Who is leading this revolution? Children who are nimbly pushing the boulders around, creating an ever-shifting terrain as we try to grasp ‘What’s your gender’?”
In a 2017 interview with Tomboy author Lisa Selin Davis, Ehrensaft said that she had “kids as young as four or five” telling her that they are neither boys nor girls but rather “a boy-girl” or “just a rainbow kid.” It “just shakes the foundations of what we think gender is,” she said. “We have a number of gender nonbinary kids coming to the clinic, asking for, for example, a touch of testosterone. They would just like to have a little bit of a deeper voice and a little bit of peach fuzz and then stop the testosterone.”
Yesterday’s tomboy wore baggy clothes and rode skateboards. Today’s nonbinary girl micro-doses on testosterone to grow peach fuzz.
In a 2018 US Professional Association for Transgender Health symposium titled “Outside the Binary—Care for Nonbinary Adolescents and Young Adults,” Johanna Olson-Kennedy, a leading U.S. gender clinician, expressed a similar sentiment. “I don’t like the word ‘pass’ at all,” she explained. “Passing as a member of the other sex is not a criterion for treatment, whereas achievement of personal comfort and well being are.” The role of the physician is “to work with [a] person to determine what it is that they’re interested in.”
The clearest demonstration of how the goalposts have moved came in December 2024, when the lead author of the Dutch studies, Annelou de Vries, coauthored a peer-reviewed article arguing that the field should no longer concern itself with whether “gender-affirming care” is “effective,” or results in mental-health “improvement” (the article places these words in quotation marks). Drawing on the theoretical framework of “trans negativity,” which “critiques” the notion that “negative affect” in trans-identified people is “a problem to be resolved through medical intervention,” de Vries promptly abandoned the clinical reasoning that she had defended so vigorously throughout her career. In this schema, doctors are reduced to highly educated vendors of consumer services.
I asked Laura Edwards-Leeper, the psychologist who helped establish the first pediatric gender clinic in the country at Boston Children’s Hospital, whether her clinic saw kids with nonbinary identities in the early days and, if so, how they treated such patients. “There wasn’t even a term for it back then,” she told me. “All the kids we saw were straightforward binary adolescents”—meaning, they identified as either male or female—“with severe dysphoria, with some indication since childhood.” The nonbinary phenomenon among clinic-referred teens emerged in the late 2010s, she added, “but it was rare. Doctors were very hesitant to do anything medically” with these kids “because they said, ‘there was no research.’”
There are still no long-term studies on the impacts of using hormones this way, not for binary transitions and certainly not for nonbinary ones.
Blocking the puberty of boys like ACLU plaintiff Cameron at Tanner stage 2—the earliest stage of physical puberty—and placing them on estrogen therapy will result in lifelong sterility. They will have undeveloped penises and suffer from sexual dysfunction. Those lucky enough to have passed through Tanner 2 will still be exposed to a range of negative health effects, including cardiovascular disease and cancer.
Gender clinicians like de Vries, who abandon the pretense that they care about evidence-based medicine, appeal to the value of personal choice as the sole ethical consideration. As evidence that their “clients” are choosing autonomously, they argue that regret from pediatric gender transition is vanishingly rare, at less than 1 percent. The main piece of evidence furnished in support of this claim is a deeply flawed “systematic” review published in 2021. Notably, of the more than five thousand of patients documented in the review,only one identified as nonbinary.
Summarizing the findings of her multiyear review of youth gender medicine, Hilary Cass wrote that “This is an area of remarkably weak evidence,” and when it comes to nonbinary-identifying children in particular, “we know even less about the outcomes for this group.”
The ACLU’s decision to include Cameron and his parents in its lawsuit may prove to be a strategic mistake. But this would be on brand for the organization, which has thrown its institutional weight behind the most radical and unpopular campaigns for transgender rights. The ACLU’s star attorney, Chase Strangio, is a controversial figure even within the nonprofit, according to a source with high-level knowledge of LGBT movement politics. Strangio, who has used “they/them” pronouns, once tweeted that “Stopping the circulation of [Abigail Shrier’s] book [Irreversible Damage] and these ideas is 100% a hill I will die on.”
In 2020, Strangio told The New Yorker that she and a group of lawyers had asked trans-identified male inmates whether they wanted to integrate into women’s prisons or have a separate trans section in a male prison. An extremely high percentage of trans-identified male inmates are convicted of sexual crimes, and their placement in women’s prisons puts incarcerated women at risk. The inmates “all said that they wanted a trans unit,” but they were overruled by Strangio and the others. A separate unit, Strangio reportedly believed, would be “stigmatizing, and only served to perpetuate the prison system.”
Like other gender-medicine apologists, Strangio seems willing to say whatever the moment demands. For example, she once said that she “sort of regret[s] the emergence of gender identity as this entire separate thing from sex” and that assumptions about the reality of sex, not only of gender, “are socially, culturally, and politically contingent”—that is, they “take on meaning as we talk about them and interface with systems of power.” Yet when arguing before the Supreme Court in U.S. v. Skrmetti, Strangio accepted that while “gender identity” may be “fluid,” it nevertheless is an “immutable characteristic” deserving of constitutionally protected status because, as she argued, it has “a strong biological basis.”
“I am a civil rights and constitutional lawyer,” Strangio said in a 2019 interview, “who fundamentally doesn’t believe in the Constitution and the legal system.” Rest assured, she will now call upon that system and its Constitution to protect her favorite client, the gender industry.
==
It's amazing how inconsistent the genderists are. The same people claiming sex "discrimination" also say that sex is a "spectrum." They're claiming dysphoria is a disability, having spent a decade insisting you don't even have to have dysphoria to be "trans," that diagnosis is "pathologizing" and "gatekeeping," and any attempt to treat the disability is "conversion therapy."
Make any of this make sense.
I really want them to explain what type of disability it is, though.
It's going to be amazing watching them try to argue this and struggle to make it not obviously ridiculous and self-contradictory.
In 2020, Strangio told The New Yorker that she and a group of lawyers had asked trans-identified male inmates whether they wanted to integrate into women’s prisons or have a separate trans section in a male prison. An extremely high percentage of trans-identified male inmates are convicted of sexual crimes, and their placement in women’s prisons puts incarcerated women at risk. The inmates “all said that they wanted a trans unit,” but they were overruled by Strangio and the others. A separate unit, Strangio reportedly believed, would be “stigmatizing, and only served to perpetuate the prison system.”
Thought I knew where this was going, but I did not. Wow.
#Leor Sapir#Chase Strangio#ACLU#nonbinary#genderism#gender ideology#gender identity ideology#executive orders#gender identity#puberty blockers#gender affirming care#gender affirming healthcare#gender affirmation#gender medicine#WPATH#World Professional Association for Transgender Health#medical scandal#medical corruption#medical malpractice#religion is a mental illness
10 notes
·
View notes
Text









25 notes
·
View notes
Text





22 notes
·
View notes
Text
(1) Arkansas ban on gender-affirming care for minors ruled unconstitutional
While Moody’s ultimate ruling in the case and legal conclusions obviously matter, his findings of fact issued Tuesday could be the most important aspect of his decision. Because trial judges are able to review the evidence and are closest to the case at trial, their findings of fact are accepted on appeal unless the appeals court finds that the those findings constitute an “clear error,” a deferential standard.
After detailing the evidence presented by the parties regarding the World Professional Association for Transgender Health (WPATH) Standards of Care and Endocrine Society’s guidelines for care, Moody — an Obama appointee who has been on the bench since 2014 — found as a fact: “Transgender care is not experimental care."
#Arkansas#Gender affirming care#Trans#Transgender#Lgbtqia#lgbtq youth#protect trans lives#protect trans youth
312 notes
·
View notes
Text
"Research into trans medicine has been manipulated"
The Sources
A recent Economist* article has described how the World Professional Association for Transgender Health (WPATH) has manipulated research into trans medicine. The article is reproduced here in full by the Society for Evidence-Based Gender Medicine (SEGM). The SEGM also discusses the topic in their discussion on how "WPATH Influence Undermines WHO’s Transgender Guidelines"
*For those who care: The Economist is rated as "least biased" and "highly factual" by Media Bias/Fact Check. While it has varied over time, they currently tend to be preferred by a left-leaning audience.
The Situation
Essentially, unsealed court documents have shown WPATH first commissioned research into trans medicine from Johns Hopkins University (for the "development" of their guidelines) and then prevented the researchers from publishing this research. (Among other ethical violations including undue influence over manuscript contents and requiring researchers to (illegitimately) claim independence from WPATH.)
Presumably their suppression and manipulation of the research occurred because the conclusions reached by the researchers did not meet advance their desired opinions.
This is extraordinarily unethical from a scientific, medical, and political perspective. Strong objections from the researchers involved were documented, but ultimately failed to prevent the limitation of academic freedom and maintenance of scientific integrity. Aside from this, their actions have deprived their own community (trans individuals) from potentially vital information about their medical treatments.
So, the next time someone asks for "proof" that the current standards of trans medicine are not evidence based and may, in fact, be harmful: reply with these sources documenting the unscientific, unethical suppression of such proof. (And, while you're at it, remind them that the burden of proof is on intervention, not the lack of intervention.)
Choice Quotes from the Sources
From the reproduced Economist article:
From early on in the contract negotiations, WPATH expressed a desire to control the results of the Hopkins team’s work.
Ms Robinson [the research director] saw this as an attempt to exert undue influence over what was supposed to be an independent process.
But an email in October 2020 from WPATH figures, including its incoming president at the time, ... made clear what sort of science WPATH did (and did not) want published. Research must be “thoroughly scrutinised and reviewed to ensure that publication does not negatively affect the provision of transgender health care in the broadest sense,” it stated.
[The WPATH president has] been named to a World Health Organisation advisory board tasked with developing best practices for transgender medicine
Another document recently unsealed shows that Rachel Levine, a trans woman who is assistant secretary for health, succeeded in pressing wpath to remove minimum ages for the treatment of children from its 2022 standards of care.
From the extended discussion by the SEGM:
The court documents reveal that WPATH leadership was "caught on the wrong foot" when two systematic reviews of evidence regarding endocrine interventions, ... did not provide the kind of support that WPATH was hoping to see. Consequently, WPATH leadership, ... took action to prevent the evidence evaluation team from making public the offending systematic reviews.
The court documents also reveal that WPATH subsequently instituted a new approval policy to ensure that only favorable evidence reviews could be published by researchers engaged in evaluating the evidence: (... WPATH had to approve the conclusions. ... WPATH had ongoing content control over the content of the planned publication. ... WPATH had the final document control.)
The authors were also required to insert into the article a statement that asserted its independence from WPATH, effectively denying that WPATH interference had taken place. [Imagine a drug company exerting this much influence over research into their a drug, and then demanding the researchers lie about this influence.]
[The Baker 2012 review] was the only review to survive WPATH’s approval process, despite "dozens" of reviews being completed by the Johns Hopkins team, as the court documents reveal. [Meaning dozens were suppressed, presumably for unfavorable conclusions.]
The Baker review has an alarming number of irregularities, which bear the marks of WPATH interference, and which deserve a separate spotlight. Here, we will only note that the review's conclusions ... are explicitly contradicted by the actual systematic review findings, which found only "low" and "insufficient" evidence.
The suppressed evidence regarding hormones interventions for all age groups raises questions about what basis WHO is using for its presumption that hormones should be widely available to all adults who seek them [This is of particular concern since several influential members of WPATH - including its president - have been appointed to the WHO board developing clinical guidelines]
35 notes
·
View notes
Text
The 388-page report featured 32 recommendations on how transgender care should be conducted within NHS England. It incorrectly claims that there is “no good evidence” supporting transgender care and calls for restrictions on trans care for individuals under the age of 18, although it does not advocate for an outright ban. The report endorses the idea that being transgender may be caused by anxiety, depression, and OCD issues, despite the American Psychological Association, the largest psychological association in the world, rebutting this as lacking evidence. It also claims that transgender individuals can be “influenced” into being trans, a nod to the discredited theory of social contagion and rapid onset gender dysphoria, rejected by over 60 mental health organizations. Lastly, it seemingly endorses restrictions on transgender people under the age of 25, stating that they should not be allowed to progress into adult care clinics. To support these recommendations, the report was released alongside “reviews” of the evidence surrounding transgender care, using these reviews to assert that there is "no good evidence" for gender-affirming care. A closer inspection of the reviews released alongside the Cass report reveals that 101 out of 103 studies on gender-affirming care were dismissed for not being of "sufficiently high quality," based on the Newcastle-Ottawa Scale—a subjective scale criticized for its flaws and potential unreliability due to a high risk of bias. This critique is particularly significant given the contentious political nature of the subject and connections between reviewers, Cass, and anti-trans organizations.
[...]
Immediately after the release of the Cass Review, experts in transgender healthcare from around the world voiced their opposition to its findings. Dr. Portia Predny, Vice President of the Australian Professional Association for Trans Health, criticized the findings and recommendations as “at odds with the current evidence base, expert consensus, and the majority of clinical guidelines worldwide.” Similarly, a statement from the Professional Association for Transgender Health Aotearoa condemned the review, noting, “The Review commissioned several systematic reviews into gender-affirming care by the University of York, but appears to have ignored a significant number of studies demonstrating the benefits of gender-affirming care. In one review, 101 out of 103 studies were dismissed.” It is important to note that gender affirming care saves lives, and there is plenty of evidence to show for it. Numerous studies have demonstrated that gender-affirming care significantly reduces suicidality, with some showing a decrease in suicidality by up to 73%. A review compiled by Cornell University, which compiled over 50 journal articles on the topic, shows the efficacy of transgender care. These findings were echoed recently in an article published by the Journal of Adolescent Health, which found that puberty blockers dramatically lowered depression and anxiety. All of these studies and more have led to The Lancet, a medical journal with international acclaim, to publish a letter stating that gender affirming care is lifesaving preventative care. The largest and most influential medical organizations support trans care. A recent and historic policy resolution passed overwhelmingly by the American Psychological Association, the largest psychological organization in the world, states that gender affirming care is a medical necessity and that being trans is not “caused” by things like autism and PTSD.
49 notes
·
View notes