#Cervical Smear Test
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
The “We are the 99%” Tumblr blog became the slogan for the Occupy Wall Street movement.
Text
Celebrating the second best outcome possible of my colposcopy with a strawberry éclair.
I have mild cell changes (first grade) in some awkward spots. If the biopsies show what she thinks, it's a discharge to yearly smears to monitor. For the first time in weeks, I can breathe a little.
So I will eat my cake, drink my wine, and work from the sofa for the next few days to be kind to myself. Shout out to my period for waiting until the actual procedure to show up 🫣😂
I also got a new reader in one of the nurses and you'd be surprised how often that happens 🤷♀️😂
Oh. AND GO GET YOUR SMEAR TEST.

14 notes
·
View notes
Text
“The smear test may be uncomfortable, but should not hurt.”
*literally experiences the worst pain I’ve ever experienced in my life, leaves appointment crying*
0 notes
Text
Cervical cancer prevention relies heavily on Pap smears and HPV screening. Despite their importance, misconceptions abound, causing unnecessary fear and confusion. This article aims to debunk common myths about Pap smears and HPV screening, promoting informed decision-making and encouraging women to take charge of their reproductive health.
#Best Cervical Cancer Doctor in Faridabad#Best Gynaecologist in Faridabad#Cervical Cancer Screening#Debunking Cervical Cancer Myths#Myths About Pap Smears#Pap and HPV Tests#Pap Smears and HPV Tests
0 notes
Text
Understanding Breast Cancer Treatment: Exploring Surgeries and Therapies

Breast cancer is a serious illness that requires careful treatment. There are different ways to treat breast cancer, including surgeries and therapies. In this article, we'll look at the types of surgeries and therapies used to treat breast cancer. We'll explain what they are, how they work, and why they're important.
Types of Surgeries:
Lumpectomy: A lumpectomy is a surgery where doctors remove the tumor and a small amount of surrounding healthy tissue from the breast. It's often used for early-stage breast cancer to help keep as much of the breast as possible.
Mastectomy: Mastectomy is when doctors remove the whole breast to treat breast cancer. There are different types of mastectomy, depending on how much tissue is removed.
Sentinel Lymph Node Biopsy: This surgery helps doctors see if the cancer has spread to nearby lymph nodes. Doctors find and remove a few lymph nodes to check for cancer cells.
Types of Therapies:
Radiation Therapy: Radiation therapy uses special beams to kill cancer cells and shrink tumors. It's often used after surgery to make sure any leftover cancer cells are gone.
Chemotherapy: Chemotherapy is when patients take special drugs to kill cancer cells or stop them from growing. It's used before or after surgery to help get rid of cancer cells and prevent them from coming back.
Hormone Therapy: Hormone therapy blocks hormones that can make breast cancer grow. It's used for hormone-sensitive breast cancer to stop cancer cells from growing.
Targeted Therapy: Targeted therapy attacks specific parts of cancer cells to stop them from growing. It's a newer type of treatment that can be very effective for certain types of breast cancer. Combination Therapies:
Neoadjuvant Therapy: This therapy is given before surgery to shrink tumors and make them easier to remove. It helps make surgery more successful.
Adjuvant Therapy: Adjuvant therapy is given after surgery to help lower the risk of cancer coming back. It can include radiation therapy, chemotherapy, hormone therapy, or targeted therapy.
Conclusion: Breast cancer treatment is complex, but there are many ways to fight it. Surgeries and therapies play a big role in helping people beat breast cancer. By understanding the different types of surgeries and therapies available, patients and their doctors can work together to come up with the best treatment plan for each person. With the right treatment, many people with breast cancer can go on to live long, healthy lives.
#cervical cancer#hpv vaccine#gardasil vaccine#pap smear#cervical cancer vaccine#cervical cancer causes#hpv vaccine price#hpv vaccine cost#pap smear price#papilloma vaccine#cure for cervical cancer#cervical#cervical vaccine#cervical cancer vaccine price#cervical cancer vaccine cost#pap exam#pap smear testing#papilloma virus vaccine#cervix#cervical cancer shot#pap screening#cervical vaccine cost#ca cervix treatment#ca cervix causes#ca cervix vaccine#p smear#pabst smear#papanicolaou smear#pap smear near me#hpv vaccine near me
1 note
·
View note
Text
Understanding Cervical Cancer Treatment in Hyderabad
Cervical cancer is a significant health issue for women in Hyderabad, India. However, with advancements in medical science, there are more treatment options available. Dr. Chinnababu, a renowned oncologist, is leading the way in providing effective treatments for cervical cancer patients in Hyderabad.
What is Cervical Cancer?
Cervical cancer starts in the cells of the cervix, the lower part of the uterus. It is usually caused by the human papillomavirus (HPV), but other factors like smoking and weakened immune systems can also contribute. Early detection is crucial for successful treatment.
Diagnosis
In Hyderabad, doctors use various tests to diagnose cervical cancer. These include Pap smears, HPV testing, colposcopy, and biopsy. These tests help doctors determine the stage and severity of the cancer, which guides treatment decisions.
Treatment Options
Treatment for cervical cancer depends on the stage of the disease and the patient's overall health. In Hyderabad, patients have access to several treatment options:
Surgery: Surgery may be recommended for early-stage cervical cancer. It can involve removing the cancerous tissue or the entire uterus. Dr. Chinnababu specializes in minimally invasive surgeries, which have shorter recovery times and fewer complications.
Radiation Therapy: Radiation therapy uses high-energy rays to kill cancer cells. It can be delivered externally or internally through brachytherapy. Hyderabad has advanced radiation therapy equipment to deliver precise treatment.
Chemotherapy: Chemotherapy uses drugs to kill cancer cells. It can be given alone or in combination with other treatments. Dr. Chinnababu designs personalized chemotherapy plans for each patient.
Targeted Therapy: Targeted therapy targets specific molecules involved in cancer growth. It can be used for advanced or recurrent cervical cancer. Immunotherapy is a type of targeted therapy that boosts the body's immune system to fight cancer cells.
Conclusion
Cervical cancer treatment in Hyderabad offers hope for patients. Dr. Chinnababu and his team are dedicated to providing the best care possible. If you or someone you know is diagnosed with cervical cancer, don't hesitate to seek medical advice and explore treatment options available in Hyderabad. Early detection and personalized treatment plans can improve outcomes and quality of life for cervical cancer patients.
#cervical cancer#hpv vaccine#gardasil vaccine#pap smear#cervical cancer vaccine#cervical cancer causes#hpv vaccine price#hpv vaccine cost#pap smear price#papilloma vaccine#cure for cervical cancer#cervical#cervical vaccine#cervical cancer vaccine price#cervical cancer vaccine cost#pap exam#pap smear testing#papilloma virus vaccine#cervix#cervical cancer shot#pap screening#cervical vaccine cost#ca cervix treatment#ca cervix causes#ca cervix vaccine#p smear#pabst smear#papanicolaou smear#pap smear near me#hpv vaccine near me
0 notes
Text
4 Essential Health Tests Every Woman Should Prioritize
Mammogram for Breast Health: Breast cancer is a significant health concern for women worldwide. Regular mammograms, typically recommended annually for women over 40, are vital for early detection. Early diagnosis significantly improves the chances of successful treatment. Women with a family history of breast cancer may need to start screenings earlier, and open communication with healthcare…

View On WordPress
#4 Essential Health Tests Every Woman#Bone Density Test for Osteoporosis Prevention#Cholesterol Check for Heart Health#Mammogram for Breast Health#Pap Smear and HPV Test for Cervical Health
0 notes
Text
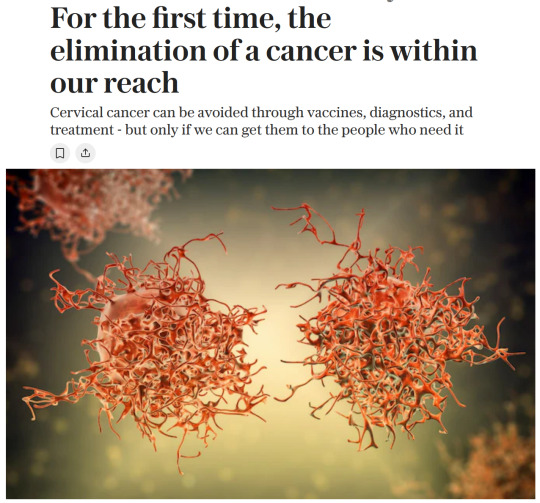
Article
"Every year, over 350,000 women die from cervical cancer and another 660,000 are diagnosed. [Note: Plus trans men and other trans people with a cervix.] As a consequence, children are orphaned, families impoverished and communities diminished by the loss of mothers, wives, daughters and sisters.
And yet, unlike most other cancers, almost all these cases and deaths can be averted. We have powerful vaccines that can prevent infection with the human papillomavirus (HPV) that causes cervical cancer; we have diagnostics to detect it early; and we have treatments for those it strikes. With these tools, cervical cancer can not only be stopped; it could become the first cancer to be eliminated. Some high-income countries are already close to elimination, meaning fewer than four cases per 100,000 women.
But in many low- and middle-income countries, these tools are still not available, which is why 94% of cervical cancer deaths occur in those countries.
In 2018, WHO launched a global call to action to eliminate cervical cancer, which was followed in 2020 by the adoption by all 194 WHO Member States of a Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. The strategy calls for countries to achieve three targets by 2030: 90% of girls fully immunised against HPV; 70% of women receiving timely screening; and 90% of those found with precancer or cancer accessing treatment.
These targets are not just aspirational, they are achievable, even in low- and middle-income countries. Bhutan has already reached the targets, the first to do so in the South-East Asia region.
Since introducing the HPV vaccine in 2011, Rwanda has reached vaccine coverage of 90%, and today announced its national goal to reach the 90-70-90 targets three years ahead of schedule, by 2027. Already, in two districts – Gicumbi and Karongi – Rwanda is meeting those goals. Nigeria, which introduced the HPV vaccine in October last year [2023], has already vaccinated 12.3 million girls.
We have the tools and the opportunity to eliminate cervical cancer.
Since WHO issued the global call to action in 2018, more than 60 countries have introduced the HPV vaccine into their immunisation programmes, bringing the total to 144 countries that are routinely protecting girls from cervical cancer in later life. With scientific advances, we can now prevent cervical cancer with just a single dose, which 60 countries are now doing.
The largest provider of HPV vaccines to low- and middle-income countries is Gavi, the Vaccine Alliance, which plans to vaccinate 120 million children between now and 2030. But this plan requires that investments in health are sustained. We are also counting on manufacturers to confirm and honour their commitments to provide HPV vaccines to low- and middle-income countries in the coming years, to avoid the supply constraints that held back progress in the past.
But we cannot rely on vaccines alone. The impact of the rapid scale-up in vaccinating girls now will not be seen for decades, when they reach the adult years when cervical cancer typically appears. To save lives now, we must match the increase in vaccination with increases in screening and treatment.
Decades ago, as more women gained access to pap smears in developed countries, the mortality associated with cervical cancer dropped rapidly. Today, even better tests are available. Over 60 countries now include high-performance HPV tests as part of their screening programs. Women can even collect their own samples for HPV testing, removing more barriers to life-saving services. In Australia – which is on track to become one of the first countries in the world to achieve elimination – more than a quarter of all screening tests are now done this way...
Several countries are also investigating the use of artificial intelligence to enhance the accuracy of screening in resource-limited settings. When women are found with precancerous lesions, many are now treated with portable battery-powered devices, which can be operated in remote locations."
-via The Telegraph, November 18, 2024. Article written by Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization (WHO).
#cancer#cw cancer#fuck cancer#vaccines#hpv#cervical cancer#women and girls#vaccines work#public health#world health organization#womens health#healthcare#pap smear#obgyn#cancer treatment#cancer awareness#good news#hope
1K notes
·
View notes
Text
Hey, so, medical update:
So as I told two weeks ago I had surgery where they cut part of my crevix because the cells where one stage away from turning cancerous (CIN3)
Today I received the results from the lab, where they analyzed the tissue in detail. and the first thing the doctor said was “so we got there in time!”
Turns out I had an adenocarcinoma in situ, which are non-invasive cancerous cells, which haven’t had the chance to break out of their protective membrane aka they couldn’t do real damage and all the things cancer does.

She showed me this image and pointed to the black line between CIN3 and cancer and said “we were here, right before the break out”
My specific situation was a 1 in a 100.000 apparently, which, eh, crazy
Very odd to hear you have cancerous cells after they got fully removed. Can’t compare my situation to someone who had to get full chemo, but it’s sure not a normal situation either so I’ll have to unpack this later.
But yeah as it stands now I have to get a pap smear every 6 months to make sure the HPV doesn’t try to start the party all over again.
Which brings me to repeat once again: if you’re eligible for getting a pap smear test please have them done bc cervical cancer doesn’t show symptoms until the very late stage, this is your only way to know!
188 notes
·
View notes
Text
It's Cervical Screening Awareness Week, which seems very fitting for me, so here's your reminder to book your smear test.
A few minutes of discomfort is better than the alternative.

3 notes
·
View notes
Text
Charades: 3 Words, 4 Syllables
C1: 3 Words, 4 Syllables | C2 | AO3 Link
Series Masterlist | ACOTAR x Reader Masterlist
Eventual Azriel x Archeron!Reader
Summary: You find out you have cancer, and it's unlikely you'll survive. In an attempt to preserve your sister's happiness, you're keeping your diagnosis a secret until after her honeymoon. In the meantime, you'll need help from one person, to go to and from your appointments.
This is a terminal illness fic. Reader has cervical cancer, due to an HPV infection. The HPV vaccine is incredibly effective at almost completely reducing the risk for cervical cancer, as well as others. HPV is able to be transmitted through skin-to-skin contact as well as through sexual contact, and it is incredibly important to receive the vaccine.
Please don't feel the need to read this fic, it is a no happy ending one. There is no bright spot at the end, just sadness. I'm writing it because I need a good outlet right now for how I'm feeling after losing M'aiq. But feel free to skip it, it's going to be just. Heavy and sad.
Warnings: Terminal Illness, Cancer, no happy ending, angst, medical tests (pap smear, use of speculum)
Words: ~3.2k
Author's Note: like I said above, this is just an outlet for me right now. It's gonna be sad. Sad sad. Idk if it'll get updated 🤷♀️ who knows. It's an outlet so I'll see when I need it again. Hoping to get some of my scheduled stuff worked on tomorrow. Love you guys 🫶 -- also the title is from a Halsey song, it was a digital deluxe release for TGI during release week, chapter title is lyrics from it!
18+ only pls
🤍💔🤍💔🤍
You’d never thought your life would come to this.
Staring at white walls, avoiding looking directly at the too-bright lights on the ceiling, your feet in stirrups, a doctor checking between your legs as you shivered, utterly uncomfortable at being examined down there.
You’d never even had sex, yet here you were, spread open because your tests hadn’t come back clean. That paired with the near constant spotting you had been experiencing for the last year, and now the constant fatigue, shortness of breath…
There was no point in worrying, until you had to. That’s what you kept telling yourself at least, to keep the anxiety from creeping too deeply into your heart.
“Wow, uhm,” the doctor said, shock evident in her tone. “I’ll be right back, I’m going to go grab the head doctor really quickly, so it tight, okay?”
And that was your sign to start worrying. Big time.
You nodded at her and craned your neck to watch as she left the exam room quickly, before your eyes returned to the colorless walls, the pale pink cabinets to your left. A heavy breath left you as you ran over the possible scenarios, what horrors the doctor had seen within you.
Large amounts of endometriosis? A baby, somehow?
… Cancer?
It was no secret that your healthcare had fallen to the wayside over the years, what with your mother dying shortly after your birth and your family losing their fortune less than five years later. Your father had been left to fend for himself and four girls, and it was a miracle that the four of you had made it this far, as unscathed as you were.
And now? Well, it was a miracle that you were here, in a doctor’s office at all. You couldn’t remember the last time that you’d been for anything other than the required shots for public school.
But here you were, going to the doctor on your sister’s-fiancé’s-family’s dime, in a country you had just moved to.
A knock sounded on the door to your right, an older woman following your doctor into the room before shutting the door softly behind her.
“Hello, Y/N, my name is Madja, I’m the head OB/GYN here, and Ianthe suggested I help examine you today. Is that alright?” You nodded shyly, watching as she took Ianthe’s previous spot, the other doctor hovering nervously behind her. Your eyes turned to the ceiling as she examined you, doing your best to ignore any sensations. You heard Madja ask Ianthe to grab supplies for her, only tuning back in when she spoke directly to you. “Okay, Y/N, I’m going to get a small sample, you’ll feel a brief pain and some mild cramping after.” You winced as she did so, squeezing your eyes together tightly. “Good job, you did wonderfully, and it’s all done.”
Madja removed her gloves and helped you remove your legs from the stirrups, sitting up on the exam table a moment later. “So, Y/N, we did see some abnormalities, and I’m going to order a few tests for you to find out more. Since we’re attached to the hospital, we’ll get you sent over for them in just a few minutes. Do you have any questions for me?”
“I… Do you… Do you have an idea of what it might be?” you asked her nervously, eyes flicking to Ianthe, who was fidgeting in the corner.
Madja sighed, a sad smile on her lips. “We won’t know for certain until the test results come back, but… Is there anyone we can call for you, dear?”
“No, no, I’ll…” you sucked in a breath. “I don’t want to worry anyone, yet. Not until we know what it is.”
She nodded, an understanding look in her eyes. “Very well. Ianthe will take you for your tests in a moment, and we’ll have answers soon. So don’t worry, alright, dear?”
“Okay,” you said quietly, watching as she left the room.
“Well, I’ll go grab a wheelchair, and we’ll get you down to MRI, CT, and X-Ray in a jiffy. And since you’re so important, you’ll probably get to skip to the front of each line, and you’ll be home before you know it!” Ianthe told you cheerfully, but you could see the sadness lingering in her eyes before she turned to leave.
You wondered how long she’d be able to keep it up, the fake-happy act, when something was very clearly wrong with you.
She returned a moment later, promised wheelchair parked outside of the room as she led you into it, settling your feet onto the footrests before beginning to wheel you deeper into the facility, chattering mindlessly to you about your hair.
Just recently, you’d had it bleached to a pale blonde, a look that you’d always wanted to try. But now that you were being given a weekly stipend for having had your life turned upside in a matter of months… You’d gone ahead and done it, loving the results.
“So do you use a special shampoo or anything?” Ianthe asked you as the two of you waited for the elevator to arrive at your floor.
“Hm?” You’d completely spaced out, your mind stuck on how painful those last few minutes of bleach had been. “Oh, I use one for color treated hair, but the real secret is purple shampoo. It keeps it looking bright,” you replied, running your fingers through your hair.
“That’s good to know, I’ve been thinking about going lighter with my own hair but the maintenance… It looks so amazing on you, though,” Ianthe gushed as she pulled up to a set of doors with a sign next to them reading Radiology: MRI. “Wait just a second, I’ll make sure we get in soon, love,” the bubbly blonde said with a squeeze to your shoulder before entering the room.
Only a minute later she returned. “Alright, as soon as the other patient’s done, we’re next. So, where’d you go to get it done?”
🤍💔🤍💔🤍
Three hours spent waiting for scans and getting scans done later, and you were back in the exam room you’d started in. Thankfully you’d been able to change back into your clothes, a comfortable but stylish pair of jeans and a hoodie, all courtesy of your soon-to-be-in-laws. Ianthe had gone to grab Madja a few minutes ago, but you could have sworn it was thirty minutes later when the pair finally returned, a redhead also entering the room with them.
“Alright, Y/N, we have a few things to go over,” Madja said seriously, taking a seat on a rolling stool. “During your pelvic exam, we observed what seemed to be a mass, obstructing your cervix. I took a sample, and we sent you for a round of tests for imaging, and reviewed them carefully. I’ll let Dr. Berdara take it from here.”
The redhead stepped forward, extending a hand towards you, shaking your hand gently. “My name is Gwyneth, but you can call me Gwyn,” she said with a warm smile. “I’m a gynecological oncologist, meaning that I deal with cancer of the female reproductive organs. From the tests we’ve run today, I am sorry to inform you that you have cancer. It is stage IV metastatic cervical cancer that has spread to your lungs, bones, and lymph nodes. We can discuss treatment options, but I would recommend telling your family as soon as possible.”
You nodded, but anxiety was already creeping through you, holding you hostage in one position. “I… I’m waiting, until after the honeymoon. I want them to enjoy it,” you whispered, thinking of how happy Feyre had been recently. How she was excited for this wedding, unlike her previous almost-wedding to that abusive jackass. “Could we keep whatever treatments we do secret, until then?”
And you didn’t want anything to get in the way of it.
Not even… Not even with you possibly dying.
“Of course. But you will likely need someone to take you to and from your appointments,” Gwyn pointed out with a raised brow. “And someone to be your emergency contact.”
“I’ll figure something out,” you mumbled, letting yourself take a steadying breath before asking the question you didn’t want to hear the answer to. “What are my options?”
“Well, we have a few things we can do. Surgically, we could do a radical hysterectomy, and possibly look at further surgeries to remove other masses, though I would not recommend the extra strain on your body,” Gwyn explained gently, watching as your eyes widened before filling with tears. “I recommend starting intravenous chemotherapy as soon as possible, we can make up a schedule for it before you leave today. Do you have any questions?”
“Uhm…” you sniffled. “What are… What are my chances, with all the treatments?”
Gwyn’s eyes softened as she looked at you, grasping your hand gently. “With the severity of your diagnosis… We can make you comfortable, for the next few months.”
You nodded resolutely. At just 19, you were likely going to die.
“I wish I’d been able to come in sooner,” you whispered softly, before tears finally spilled over onto your cheeks.
🤍💔🤍💔🤍
“Did you want to stop for anything before we head home, miss?” your driver, Nuala asked.
“No, thank you, Nuala. Thank you for waiting so long for me,” you said quietly, guilt building inside of you. After all, you’d been in the clinic for over four hours, and the woman had been patient enough to wait outside with no more than one text, asking her to wait until you were done.
“It’s no problem, your safety is of the utmost importance.”
Right.
That was the whole reason you had moved to Prythian, after all. A tiny coastal country on the western edge of Spain, with only one large city - Velaris, whose streets you were currently being driven through.
And home? Home was a palace, where your sister’s fiancé, Rhys, and his family ruled from.
You would have been content, living in your small town in the southern US, if not for the attempted kidnappings that had occurred a month ago, prompting you and your other two sisters’ quick relocations to Prythian in an effort to not have the three of you killed.
Apparently, ruling a country didn’t make you popular with everyone.
But you wouldn’t complain now, having the freedom to explore your passions without worrying about having a job would be nice.
Though… That might not happen, after all…
You watched the vibrant streets passed by, wanting nothing more than to curl up in your bed, ready to ignore everyone and everything in an effort to not give away your new… Condition.
Which is exactly what you did, slowly making your way from the garage to the entrance hall, then through the main hall and up the grand staircase, taking the first right before seeing your door at the end of the hall.
If you were this exhausted now… You could only imagine what hell the chemo would put you through, how you’d manage to make it all the way up here each time.
As it was, your first round of it would be given to you tomorrow and…
Shit, you needed to find someone to take you…
Collapsing onto your plush, far too large bed, you thought of your options.
You didn’t want to burden Nuala, she already had enough errands to run all the time without having to babysit you five times a week for however long it took to administer the medications.
Your sisters were out of the question, you knew that Nesta and Elain would both tell Feyre, and your hopes at letting her enjoy her wedding would be shot.
You only had a week before the wedding, and two weeks after than for her honeymoon to be over. Only three weeks that you needed to keep up this charade, that you were fine and nothing was out of the ordinary. After that, you would be able to tell your sisters, whatever… Whatever that would look like.
At some point you must have drifted off, as you were awoken by the dinging of your phone, a text from Feyre ringing out.
Dinner’s in five, don’t be late!
That was two minutes ago, meaning you only had three to drag yourself downstairs and into the dining room, or else risk scathing looks from the King.
He hated people being late.
You hurried out of your room, knowing that he’d likely be pissed no matter what, seeing as you were still clad in jeans and a hoodie, entirely too casual for a dinner in a palace.
Though you didn’t see much why it mattered, as there was no one around to take pictures of your impropriety.
It doesn’t matter, I just need to do better. I’m living here on his dime, after all, and he’s going to be paying for my treatments too… You paused when you hit the bottom of the stairs, a wave of dizziness washing over you.
A strong hand met your back, keeping you steady. “Hey, are you alright?”
You managed to look up, eyes meeting hazel before flicking away. “I’m fine, thank you. Just ran down the stairs too fast, I think,” you said, an awkward laugh leaving you before you remembered that you were going to be late. Quickly, you set off for the dining room, Azriel hot on your heels, though you knew he could pass you easily with those long legs of his, and the fact that you were moving at slower pace than usual.
The two of you entered the dining hall together, just as the clock struck six.
“Good of you to join us, Azriel, Y/N,” the King, Xander, said as the two of you took the remaining empty seats next to each other. Dinner began shortly after, waiters bringing out salads and pouring wine, to which you placed your hand over your glass, not wanting to test how alcohol works with an illness like yours.
Probably not well, if you had to guess.
You hated how long these dinners took sometimes, and right now especially. All you wanted to do was go back upstairs and sleep, maybe take a nice, hot bath for the cramping you were having.
Over an hour later, dessert was served, and you hardly touched it. It had been a chore to eat the roast meat and veggies you’d just finished, and you were certain that you would lose everything if you attempted to have more, nausea already building in your throat.
You could practically feel Azriel’s eyes burning a hole into the side of you, watching you the entire time. Even now, as you took tiny sips of tea, he was watching you.
So… Maybe you had acted strangely before coming in here, but that didn’t mean that he thought something was wrong, and he probably wasn’t even watching you. You were probably just being paranoid, now that you had something to hide.
You left the dinner just after the King and Queen did, not noticing that the same someone who followed you in had chosen to follow you out, as well.
You made your way back to the grand staircase, looking up at them with dread in your eyes. You were tired, and you were still cramping, and you were emotionally exhausted, and… And you just wanted to cry.
“Do you want help?” that deep, smooth voice asked you, and you turned your head to the right to see Azriel, standing a few paces away with his hands clasped behind his back.
“No, I’m fine, but thank you for asking, Azriel,” you replied, latching your hand to the railing as you began to ascend, the eighteen steps kicking your ass by the end of it, and you stopped, breathing deeply as you tried to slow your heartrate and clear the dizziness from your head.
“You’re not fine, Y/N,” Azriel hissed as he led you with a gentle hand on your back, getting you safely to your room. You plopped onto your bed, sighing as your lungs recovered. “Are you going to tell me what’s going on? You’ve had doctor’s appointments frequently, and now you’re struggling to walk up a flight of stairs without help. You aren’t fine.”
Falling back, you let yourself stare at the ceiling as you contemplated the risks of telling him.
Feyre had told you he was good at knowing secrets about everyone, though she hadn’t mentioned his proclivity to share them with others…
Half of the truth, then.
“I’m sick, Azriel. I need to go to treatments five times a week, starting tomorrow. And I need you to not tell anyone, not until after Feyre and Rhys get back from their honeymoon,” you told him, your voice soft, resigned.
“Alright. Do you have a way to get there?”
You blinked for a moment, dumbfounded. “No, I don’t…”
“That’s solved, then, I’ll take you. What time do you need to leave tomorrow?”
You pulled yourself back into a seated position, a confused look on your face. “You’ll take me? Why?”
“Because you’re Feyre’s sister, and you deserve to have help in this, even if you refuse to tell your sisters now. Besides, I have nothing scheduled for the next three weeks, and after that, your sisters can take over. So, what time do we need to leave?”
Teeth worried your lip as you stared at him, utterly confused by his interest in helping you. You’d spoken maybe ten times in the month the two of you lived under the same roof, and it had been brief contact at that. But you supposed… Help would be nice, and he was offering…
“My appointment is at ten, and it takes about twenty minutes to get there.”
Azriel nodded, “Alright, I’ll see you at 9:30 to take you down to the garage. Have a good night, Y/N.”
He left your room soon after, leaving you laying on your bed, confused at the turn of events. From brief interactions to now offering to take you to your appointments, five days a week… It was strange, and you were also grateful.
As for the rest of your evening, while a bath sounded nice… you would much rather change into a nightgown and crawl into bed, maybe even get a whole twelve hours of sleep tonight.
So you did exactly that, shedding your jeans and hoodie, before slipping into a soft, powder blue nightgown. You set an alarm for 7:30, deeming two hours more than enough to take a bath or shower, then have a light breakfast before your treatment started.
You weren’t feeling hopeful, not really. The only thing you were letting yourself hope for was that you wouldn’t ruin Feyre’s wedding festivities. You wanted her to be happy.
That’s all you’d ever wanted, for your sisters.
That’s all you’d ever wanted for yourself.
But you were good at playing like you were fine, good at pushing through the pain. So long as you didn’t have to face a set of stairs, it seems.
You’d keep this secret, until the time was right.
🤍💙💔💙🤍
General Taglist: @daughterofthemoons-stuff @lilah-asteria @meritxellao @twismare @wrenisrad @icey--stars @le-nottibianche
#charades#3 words 4 syllables#eventual Azriel x reader#azriel x archeron!reader#azriel x reader#archeron!reader#acotar x reader#tw terminal illness#tw cancer#angst#heavy angst#azriel#acotar#acotar fic#acotar fanfic#tato writes
79 notes
·
View notes
Note
Hello, hello! I have a few HPV questions that are kind of convoluted and I've never been given a straight answer, I'm hoping you can help (or at least point me in the right direction).
Is there a definitive pos/neg test for HPV, such as a blood test?
Can someone with one strain of HPV pass it to someone where it then becomes a different strain? For example, my ex had genital warts, which I did not get, but then I went on to have an abnormal pap, and as far as I'm aware it is two different strains of HPV that cause GW and cervical cancer.
If that can't happen, is it possible for someone to pass more than one strain to you where you're only symptomatic for one of them?
And lastly, since I never had GW, had my abnormal cells removed, and haven't been sexually active with anyone since my ex (close to 10 years ago), is it possible that I could have a GW outbreak now? I'm sort of worried about it but I also think it's probably fordyce spots.
Thank you!
hi anon,
thanks for the HPV questions!
for people with a cervix, an HPV test can be performed using cells gathered from the cervix. for people with a penis and prostate there isn't strictly a designated test to detect HPV, but visual inspections can be performed to find abnormalities, and people who have had anal sex can sometimes be tested with an anal Pap smear.
strains of HPV don't turn into different strains. there are nearly 200 stains of HPV, nearly all of which are harmless, but there are 2 that can (but don't always) cause genital warts and 13 that can (but don't always) cause cancers of the cervix, anus, vagina, vulva, penis, and throat. the genital warts strain and the cervical cancer strains do not overlap.
yes, you can have multiple concurrent HPV infections of different strains. not all will be symptomatic; it's possible that none of them will be. most people with HPV will be asymptomatic for the duration of their infection.
after ten years, it's unlikely that you still have HPV. most infections are resolved within about two years, and it sounds as if you haven't had an opportunity to pick up an infection from anyone else.
53 notes
·
View notes
Text
Apropos of absolutely nothing at all, oral and throat cancers from HPV don’t only occur in guys; anyone who engages in oral sex should be on the lookout for them! Symptoms include sudden loss of taste, swelling, numbness, a persistent sore throat, and pain. HPV can also cause cancers of the phallus, vulva, and anus. Because it’s a viral related cancer it can be especially dangerous for those with immune conditions, including HIV or some autoimmune diseases treated with immunosuppressants.
However the HPV vaccine is effective at preventing all of these cancers. In countries with high uptake many forms of cervical cancers have vanished among young people. The vaccine is most effective for younger children between 10-13 so if you have kids, siblings, nieces or nephews, push for them to get it! It’s also now recommended for adults up to middle aged. Even if you’ve already contracted one HPV strain, the vaccine may still be helpful. Although there’s increasing evidence of efficacy at just one dose, it’s most effective if you get all three in the series so don’t wait.
And if you’re eligible for Pap smears, get them. They might not be comfortable but they are one of the most effective medical tests invented in the twentieth century.
100 notes
·
View notes
Text
For people who get pap smears/cervical cancer screening, this sounds like a game changer. Weren't they also looking at a blood test alone at one point?
Of course, a bigger game changer for a lot of people here would be if they just came out and said "You've never had sex? Maybe there's no reason to do this. Especially if you've also gotten the HPV vaccine."
107 notes
·
View notes
Text
In Memoriam
Before I proceed, I want to put warnings--content/trigger warnings. In this post, there will be references to cancer (also, fuck cancer), death, biological processes, grief/loss.
When we think of cancer, when we speak of it, I've noticed often times the phrase "evil", "monster", or some other dark term is used. Because it seems to be such a merciless, cruel thing to happen to people. It seems to strike without reason, taking the best and worst of us, young or old....
Today marks 18 years since my mother passed away from cervical cancer. She didn't have to die, not really. In a way, she chose to.
You see, my mother had an intense mistrust of "mainstream" medicine. I'm not sure where it came from, honestly. It was... it was a slow conversion. She kept turning to alternative means to treat problems, mainly our day-to-day diet (lord, we went vegan, Atkins-like before Atkins was widely known anyway), and various other kinds to "cure" our ailments, never accepting that some things can't be fixed by diet alone!). Then she kind of went off the deep end....
When she learned she had serious fibroids, she decided to try different "healing" creams to balance out her hormones, convinced it'd "dissolve" the fibroids. When she began to have heavy, intense bleeding, she chalked it up to the fibroids and not other issues.
Such as an abnormal pap smear test result... that she never followed up on.
It'd continue for years.
She even turned to an alternative doctor who told her yes, he saw the fibroids... but he also saw some seriously bad stuff. This doctor told my mother to go see her ob-gyn and get this checked out.
She wouldn't... up until she collapsed from the heavy bleeding in a grocery store bathroom stall. She finally turned to mainstream medicine, got it checked, got the biopsy....
It was Stage 2 cervical cancer.
She was referred to an oncologist. He, of course, brought up chemo and radiation. She refused, wanting to try alternative treatments first. He accused her of having a death wish (I was there, I wish I was joking!). He basically burned that bridge with that approach.
I can't help but think that... if he had said "Okay, I'll work with you. How about we monitor the cancer as you try it for a couple of months? If there's no improvement, will you try chemo and radiation then?"
Maybe she would've accepted it. I don't know.
So she turned to "mistletoe extract" injections. For a little bit, it looked like it was working. She was doing better.
Then... she developed increasing pain in her right leg. The doctor who originally told her to go see her ob-gyn stressed to her it was likely her cancer growing and getting worse. She didn't listen.
Then... she had increasing pain. Increasing issues. She got thinner... paler. She was so stubborn. There's numerous trips to the ER where they just prescribed her pain killers and sent her on her way. It took a referral to a specialist (I can't remember what they handled, maybe a different oncologist?)... and the blunt message.
"You're terminal."
I wept. My mother... she was just resigned. She transferred to home hospice care. She didn't want to die in a strange building. So my elder brother and I--we were living with her at the time--took turns caring for her.
She stopped eating. Stopped drinking. She's put on IV fluids and a kind of controlled dilaudid treatment. One night... it's as if she's aware. Her mind was going. She said her final goodbyes.
Then it's just her shell, her body, for two and a half weeks, that lingers, stubbornly. I'm the only one who was there who witnessed her last passage, the "death throes".
February 8, 2007. Just a few weeks shy of my 27th birthday.
She never got to see me graduate from college. She never got to see me married.... or divorced. She never saw me become a mother. She never saw me become a survivor, a fighter. So many things.
I have her eyes, I'm told. A deep brown with a starburst iris. My son has those eyes too. I resemble her greatly, I'm told. I don't have her curly hair... or her thinner nose.
Instead, she gave me her creativity, her love of art and writing. She loved books and reading. She loved cats as well, which I definitely inherited.
She had a lot of regrets... and sorrows.
I don't know if there is an afterlife. My relationship with God (or the Divine or whatever you want to call it) is complicated, to say the least. If there is, I hope I see her... and have the conversations we never had but should've while she was alive.
I miss you, mom. So very much.
21 notes
·
View notes
Text
DNA-based test for HPV has promising results

HPV screening in Brazil is set to undergo a major game-changer—the traditional routine cytology test, popularly known as the pap smear, will be gradually replaced by a DNA test.
The incorporation of the technology into Brazil’s public health care network, the SUS, was announced by the Ministry of Health following a study carried out by the State University of Campinas (Unicamp) in the municipality of Indaiatuba, São Paulo. However, it still requires the National Cancer Institute (INCA) to define guidelines and the target population, as well as how the tests will be carried out.
The first five-year round of the study shows promising results from the cervical cancer screening program run in the municipality from October 2017 to September 2022 using the HPV DNA test.
The figures indicate an increase in the detection of precancerous lesions by up to four times, with 83 percent of cancer cases detected at an early stage.
Continue reading.
#brazil#politics#science#medicine#healthcare#good news#unified health system#brazilian politics#image description in alt#mod nise da silveira
17 notes
·
View notes
Text
A Primer on Cancer Screenings For Trans People
rebloggable on its own now, hooray. I'm a healthcare quality guy, a preventive care navigator, and I've worked with trans health for almost a decade at this point. I anticipate this info will be harder to get shortly, so go forth, own it, spread it to your elders, etc
for transmascs and trans men:
- if you have not had top surgery or have only had a reduction, you should get mammograms as recommended for cis women. if you are at average risk, this is every 2 years starting at age 40.
- if you have not had top surgery / only reduction and you are at HIGH risk of breast cancer (for example, you have a BRCA mutation, received significant radiation to the chest, or a strong family history of breast cancer), ask your doctor. they will likely want you to start earlier, go more often, and/or get a breast MRI in addition to your mammogram. if you are interested in top surgery, please also talk to your surgeon! if you're at sufficiently high risk, especially if you have a BRCA mutation, it might change the way they do the surgery or the way your results look.
- if you have had top surgery that is NOT a risk-reducing mastectomy, your risk of breast cancer is reduced but not 100% eliminated. (if you have to ask, or if you haven't already discussed this all with your doctor, you didn't get a risk-reducing mastectomy.) it is not usually possible to do a mammogram on someone after masculinizing top surgery because of the limited amount of breast tissue remaining, and it might not be worth it given the reduced risk (not much data out there), so just keep a casual eye out for any lumps and ask your doctor if something pops up.
- if you have a cervix, you should get cervical cancer screening (Pap smears or HPV testing or both) as recommended for cis women. I recognize that pelvic exams suck for trans men for various reasons - if you find them difficult due to pain or dysphoria, consider asking your doctor if you can self-collect the sample, or if they can order just an HPV test so you only have to test every five years. another fun thing about pap smears: if you've been on testosterone for awhile, it may be challenging to interpret pap results - the cells can atrophy the longer you're on T.
- if you have had your cervix surgically removed and you have no history of abnormal pap smears, you no longer need cervical cancer screening - congrats! if you DO have a history of abnormal paps, you will need to continue getting smears of the cuff / vaginal vault left behind until you have three normal tests in a row. then you're free!
for transfems and trans women:
- if you have breasts, you will likely need breast cancer screening. if you are at average risk, as of 2016, the guidelines circulating were a mammogram every 2 years starting at age 50 after being on estrogen for 5 years or more. however, these are old guidelines, and the starting age for cis women was pushed back to age 40 (from 50) after they were released. I've also seen some interesting data that breast cancer risk increases from cis male levels relatively quickly after starting HRT, so
- my personal recommendation is that trans women and transfems, after a length of HRT determined by you and your doctor (5 years seems probably reasonable for average risk, maybe shorter for high risk), roughly follow guidelines for cis women. throw that Dutch study I just linked at them if they complain. trans women may also have a higher incidence of dense breast tissue, which is more challenging to image - make sure you're regular on screening so your medical team can better monitor changes.
- prostate cancer screening should be a discussion between you and your doctor because the risks may not outweigh the benefits for everyone. if you are at average risk and choose to be screened, you should get a PSA test (just a blood test) starting at age 55 and discontinuing at age 70. practically nobody does a digital rectal exam (the physical exam where they stick fingers up you) anymore because the evidence just isn't there for it and a PSA test is easier.
for everyone:
- colorectal cancer screening is so important. especially for Black people and other people of color, who are at higher risk, but for everyone! screening should start at age 45-50 and can be a colonoscopy every 10 years or a FIT (stool sample) test every year.
- you may need other tests depending on other risk factors you might have, your mileage may vary.
- your insurance might complain about paying for a screening that isn't "congruent" with your gender marker. trans women may benefit from strategically changing their gender marker with insurance to F, if it is possible. trans men may benefit from strategically leaving theirs as F, if it is possible and desirable (altho, if you follow my next step, may not be desirable... your mileage may vary). a doctor's office competent in trans care probably knows how to argue your case successfully to insurance in any case.
- in preparation for the possibility that insurance stops covering HRT for trans people, you may wish to ask your doctor to prescribe your HRT under a diagnosis code that is NOT "gender dysphoria." this was commonly done in the past to get hormones covered by insurance. happy to provide some possible codes for you on request, but would prefer not to blast my strategies all over the internet for obvious reasons.
- stop smoking cigarettes, damn it! that is one of the best things you can do to reduce your cancer risk. I know they look cool and they're a way to soothe yourself from the horrors, but get a vape if you must continue using tobacco. (also, most surgeons want you to quit before you have surgery, so if you want surgeries in the future there's no time like the present.)
10 notes
·
View notes