#Active Body Therapy
Text
Active Body Therapy Impress
Take a step towards Active Body Therapy holistic well-being today.
Unwind and Revitalize with my Tantric Licensed Massage Therapist Near Me Relax and Revitalise with my Tantric Therapeutic Touch Pamper in the calming touch of my Swedish Active Body Therapy, crafted to promote serenity, release muscle tightness, and improve general health. Enable the skilled of Chris ease your stress and leave…

View On WordPress
0 notes
Text
Active Body Therapy Impress
Take a step towards Active Body Therapy holistic well-being today.
Unwind and Revitalize with my Tantric Licensed Massage Therapist Near Me Relax and Revitalise with my Tantric Therapeutic Touch Pamper in the calming touch of my Swedish Active Body Therapy, crafted to promote serenity, release muscle tightness, and improve general health. Enable the skilled of Chris ease your stress and leave…

View On WordPress
0 notes
Text
i have... ✨Danyal Al Ghul Headcanons✨ but specifically for my yaelokre danyal oneshot
There's also the tumblr post here but I recommend the link in the title because its the ao3 version, and that one is edited and has some stuff in it that's not in the tumblr post, and will be the version I'm using.
So for summary: this Danyal is also from a Demon Siblings Au where Danny is five years older than Damian. However, things turned out a bit differently, and Danny and Damian had a fantastic relationship with one another. Danny loved music and regularly came up with songs to sing to Damian with. Specifically the folk band Yaelokre's EP "Hayfields" (seriously go fucking listen to it its sooo good. Harpy Hare is the second song but its my favorite. Special shoutout to @gascansposts for introducing the band to me)
He falls off a train when he's twelve and Damian is seven while the two of them and Talia are on mission. He ends up with magically induced amnesia and wakes up in Arkansas while the Fentons are on their yearly Divorce-iversary visit to Aunt Alica, and since he can only remember his name, he ends up being taken into their care.
---------------
Yaelokre Danny has the same facial scar as Things in Threes Danyal, since he was initially another version of him where things turned out better. I'm debating on whether or not I should take it away however, and give him a different scar (maybe from when he fell off the train?), just because the scar is a pretty key identifier for Ti3 Danyal.
-----------------
Danny frequently visits Aunt Alicia in Arkansas! Well, only after he gets settled in and stuff. He doesn't really like the city that much and prefers the countryside where Alicia lives. I know she lives in a cabin but I'm changing it to a farm, so she puts Danny to work and gets him to help her.
I don't want to confine his hobbies to only being star stuff, because people tend to have more than one hobby and I feel like it reduces him to one-dimensionality, so he likes to garden, and learns guitar. His room becomes filled with plants, and he turns their roof into a rooftop greenhouse right below to OPS Center.
He has a complex relationship with the weapons from his past, but he's not... like... appalled by it? When he finds his weapons in the Fenton attic all he thinks is that they're his weapons, and he starts carrying a knife on him afterwards. Essentially he becomes fascinated with weaponry because its one of the few physical ties he has to his past, and while he's not training like he is in the League, he allows his strong muscle memory to guide him through his katas.
Danny likes climbing things. This causes Problems For Everyone Else.
----------------
Danny was not the "kinder Al Ghul" in the League. His kindness extended to his brother and family, and that's it. To everyone else he had high expectations out of them, and the pride you'd expect from the grandson of Ra's Al Ghul and trained by its top members. While he wasn't like, unnecessarily cruel or anything, he wasn't merciful either.
This transfers post-train fall as him coming off as no-nonsense and unforgiving. He's not fond of the idea of giving people second chances, and is skeptical of the idea. He's disgusted by incompetency and views it as an unforgivable offense, especially if he thinks that the person should know better, although he's not sure why. Some egocentrism for the soul.
He doesn't like being touched by anyone who isn't family, and gets irritated when anyone grabs him or holds onto him for extended amounts of time. Dash has gotten hit so many times. With Jack Fenton's tendency for abrupt physical affection, it doesn't make it any better. I'd argue it'd make it worse because Danny doesn't want to be touched more often than not.
------------------
Danyal had a red scarf in the League that he wore on his last mission, it came off before he fell off and caught itself on the roof. Damian still has it and took it with him to Wayne Manor. He's got it locked in his room and takes it out when he's alone and missing Danny the most. One time he forgot to put it away before leaving his room, and Dick was visiting the manor for something and found it. Damian found him holding it and freaked out.
Dick could only say "I've never seen you wear this, Damian, this is really pretty--" before Damian shoved him to the floor and stole it out of his hands, before screaming at him; "Don't touch this! You don't ever touch this! This is mine! You hear me!?"
It caused such a commotion that the rest of the family present came to see what the fuss was about, and Damian kicked them all out of his room. Dick is the one brother Damian's the closest with, so the fact he reacted so strongly shocked them all.
This is likely what leads to the "Danyal" conversation.
#dpxdc#danny fenton is not the ghost king#dp x dc#dpxdc crossover#dp x dc crossover#danyal al ghul au#yaelokre danny#yaelokre danyal al ghul#the yaelokre danny post didn't really go into him interacting with other people but i'm trying to figure out his personality post amnesia#just know this: he's not canon danny. im spitefully refusing to make him a Cookie Cutter of canon danny because the idea pisses me off lmao#he's complex and confused and morally gray even with the amnesia bc memories aren't stored in one part of the brain they're stored#in different parts depending on the memory and muscle memory exists and danny might not actively remember the things that shaped him but hi#body does. and somewhere deep in his mind so does his brain. his memories weren't destroyed theyre locked away in a place where his active#conscious can't reach. plus its magic amnesia and i have comic AND cartoon realism on my side.#danny's personality from the league doesn't get challenged that much by the fentons because danny's learning this about himself just as muc#as they are. Jazz can't “Fix” what's wrong with him when neither of them know it and Danny is always the first to figure it out and then#keeps it to himself. Also. Jazz has a fucking life? she's not the family therapist she has friends and hobbies even if we the viewers don't#see it. But also i just really deeply despise the idea that Jazz “fixes” danny's league issues just by existing and being the therapist#because it waters her down into a one-dimensional character who only exists in the context of providing emotional support and life advice t#danny. also therapy only works on someone that's actively trying to change. otherwise its just psychoanalyzing and people tend to hate#being psychoanalyzed without consent. which as a result may have them refuse help. anyways point is: i believe that growth is slow and#complex and danny would hide a lot of the stuff he discovers about himself because if there's one thing he still retains from being an#assassin. it's how to hide. he likes jazz but there are some things you just hide from people.#damian also told dick to “keep his filthy hands off his things”. which was also a shock because it sounded something he'd say more to tim#damian was distraught the entire time.#okay thats all i have for now.
92 notes
·
View notes
Text
i’m so serious i need these lyrics tattooed on the inside of my eyelids

#i can’t stop listening to this song#i can’t formulate my thoughts rn but this song and honestly the whole album#have such an interesting take on where modern day feminism is heading and how we’ve traded in genuine activism for this girls girl#aesthetic that has no deeper meaning or messaging other than omg i love being a woman and i love buying makeup and i would never shit talk#another girl or be insecure#because it’s literally impossible 😭 you’re not gonna get along with everyone! a friend to all is a friend to none!!!#and you’re not gonna magically lose all of your insecurities and low self esteem just because some girl on tiktok told you that thick thigh#s save lives#idk like there’s so much pressure on us to be perfect all the time and be this weird caricature of a girl#when in reality this girl doesn’t even exist!#it’s crazy that people honestly think you’re some kind of an anti feminist if you don’t like following tiktok beauty trends or if you have#beef with other women or you struggle with low self esteem#like at its core femininism is about women’s rights! it’s not about shaming women for being real complex people 😭#you can’t girl boss your way out of body dismorphia and serve anxiety#you can’t self care and retail therapy your way out of depression#anyway i love this song and i love being a gross weird women#mari.txt
28 notes
·
View notes
Text
i hope you don’t mind me not participating in sunday six for so long and not updating my fic... i’m having a bit rough time handling my life irl right now
#meaning i’m having the worst start of the year ever#i’m EXHAUSTED fucking exhausted from my living situation and it doesn’t seem to get better any time soon#naturally i don’t have it in me to write because i don’t have enough time to relax. it’s been three fucking weeks.#i just don’t know even my body gives up from this stress and not like something terrible is happening#it’s extremely upsetting also considering that i love writing and it’s the only activity that makes sense to me#and always has been like that it’s in my core#and i. can’t do it. i can’t. i have no willpower or strength and it’s not writer’s block i’m just SO TIRED ALL THE TIME#therapy and years of medication mean nothing at this fucking point. props to me for not killing myself tho. well done 👍#sorry for ranting i am so frustrated that i can scream. i have actually. didn’t help.#well ahem i hope you understand 🙏 i feel bad that i’ve promised the chapter a long time ago and NOT TO BE THAT AO3 AUTHOR but#i really wanted to keep my promise. fuck me i guess#putting letters together one word at a time
12 notes
·
View notes
Text
It's strange when people refer to me as "transitioning from [x] to [x]" in the active sense. Like I haven't been actively transitioning since I was 15 socially transitioned, maybe 17 when I started T. But since I've got most of the changes I want from hrt my brain considers me pretty much fully transitioned. Even though I'm actively waiting for top sugery I'm not longer in active transition. I haven't been for years.
#its that whole... you are the gender you see yourself as no matter what your body looks like#but this#post was triggered by a social worker saying “so your currently transitioning from __ to __ yes?#and i was just like#so thrown off by it lmao#i think my brain actually buffered#its always strange to be confronted with how behind the healthcare system is from like... active queer terminology#trans#queer#transgender#trangender#transexual#multigender#hormone replacement therapy#therapy#top surgery#medical transition
3 notes
·
View notes
Text
Something is Wrong in my neck again, and i am scared. it’s not an emergency, and it might not even be serious, but for several days now something has been off, and i think it’s just causing pain/malaise/nausea/mild disorientation/vertigo, but it’s still stressful knowing something else is going wrong. i hope pt can help before it becomes too bad. idk if it’s skull-C1 or C2-C3 that’s gone unstable but i think it’s one of those 2 and once my swelling from wisdom teeth removal is down enough i’m gonna start wearing my brace much more again.
#this is why i’m doing physical therapy to relearn how to PROPERLY use my neck without y’know. fucking up my spinal cord again.#aaaaaahhhhhhhhhhhhh#the dread of knowing something bad is actively happening in your body and you cannot fully stop it#personal#chronic illness#neuro stuff#spinal surgery
3 notes
·
View notes
Text
I hate going to Christian-based hospitals. There's a bible verse slide show on the screens that other places usually have medical information graphics and resources on and I just got asked "Do you have a source of peace in your life?" like babygirl I'm here for neurological pain my source of peace is Lidocaine 4% and a heating pad
#The nurse was definitely lgbt because he came back and asked me for my pronouns when I know good and well that's not in the system here#We talked about his cool ass crocs and he was like 'yea I know they're weird questions but I'm required to ask'#Cause they're all like 'do you have a source of peace and joy' and 'do you have a spiritual reason not to partake in any medications here?'#which is nice in concept like wanting to avoid pork-based or gelatin-based products#and things like that#but when it's paired with all of the bible verses and 'extending the healing ministry of christ' being the hospital's slogan#well.....#all of the screens are verses about joy as if this isn't one of the most miserable places to be#they're unfortunately one of the few places in my area tho that treat CFS/ME 😔✌️#It's probably very nice for older people here fighting for their lives#and I understand/respect that#but I've got a therapy appointment after this and I'm gonna go Off#I just realized how tense I got about this Im actively trying to relax my body#my blood pressure was 140/93 sitting and 148/91 standing#which is Not Good#this entire hospital sets off my fight or flight#they're infamously known in my area not to treat transgender patients with respect#both as a community thing and from people talking to me individually#I went on a long tangent about my gender but it was just rambling lol#anyways be gay do crime don't go to christian based hospitals if you can help it#ex christian#religious trauma
21 notes
·
View notes
Text
what if i did retail therapy
what if i did so much retail therapy
#in my defense a) i can't afford proper therapy my insurance doesn't cover it and#b) i'm on accutane and my skin is so hecked up and i'm still figuring out how to take care of it#and idk if it's that or the ~s t r e s s~#activating my dermatitis issues#me when i don't have any concept of how stressed i am while my body is screaming wtf#also the dog i'm dogsitting (stress!) ate one of my headphones#i hate skincare and makeup like yes the whole social stigma stuff sucks#but also like with any health and body related stuff IT'S SO SPECIFIC#BUT IT'S TOO EXPENSIVE TO JUST TRY STUFF UNTIL YOU FIGURE IT OUT#dark beauty youtube give me SOMETHING
2 notes
·
View notes
Text
wip wip wip i know thats all i post now but leave me alone. sorry for ugly watermark, i do this with all wips now L. ill edit pin's colors later theyre kinda bothering me.
spoilers for bfdia12 in tags i love talkign sorry
#posting this now cus i gotta go to therapy soon because they fucked up my scheduling and now i have an extra appointment that i cant cancel#without a fee and i might pull my hair out and go crazy#sorry no activity i was still watching bfdi but i was just really busy and also lazy. and tumblr makes me nervous ngl#yall arent ready for my children show hot takes [i dont really like bfdia6+]#also how am i supposed to draw pin now... mauled corpse? im excited for evil ghost pin but i have no clue how to draw the Body#boy and his tapeworm best friend#use him for evil fucked up purposes ha ha ha 😈😈😈#i pretend coiny doesnt exist sometimes ngl#both bfdia6+ and tpot#set him on fire
2 notes
·
View notes
Text

#i love actively doings that i know will upset me. i love self sabotage 👍#listen im just a curious feller. or something#i should go back to therapy... i started for trauma and now wanting to switch to problems /i/ have is so terrifying#i dont want to change my psychologist either shes so sweet and being lent to someone else feels like the world will actually end#i dont knowwwww but i cannot function like this its affecting my body too when i can hardly handle change#<- the whole reason im like this lately is not being able to handle change too. and also. i just get so violently jealous <3#and i end up releasing that anger on people that dont deserve it ^_^ i should be put down i think#vent in tags
4 notes
·
View notes
Text
Fri 10th March:
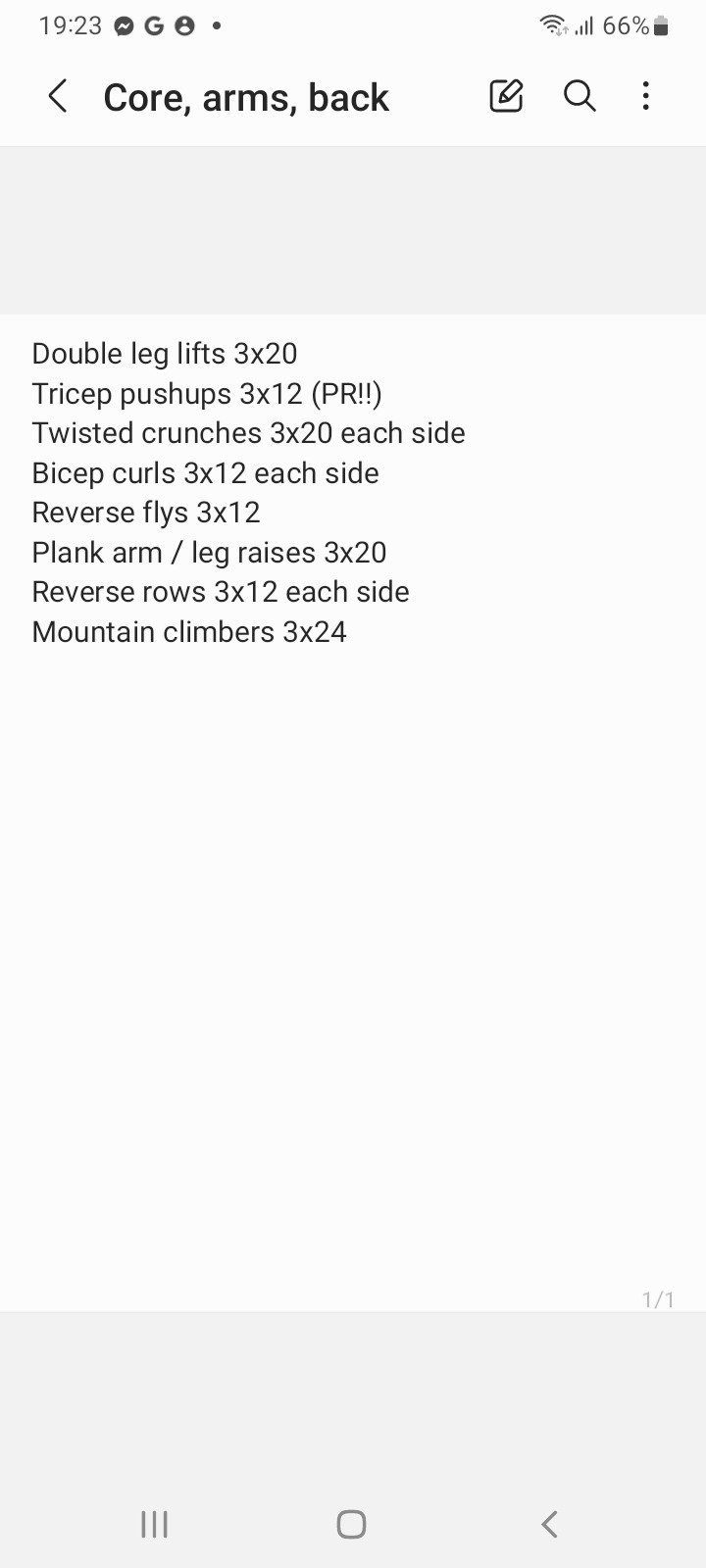
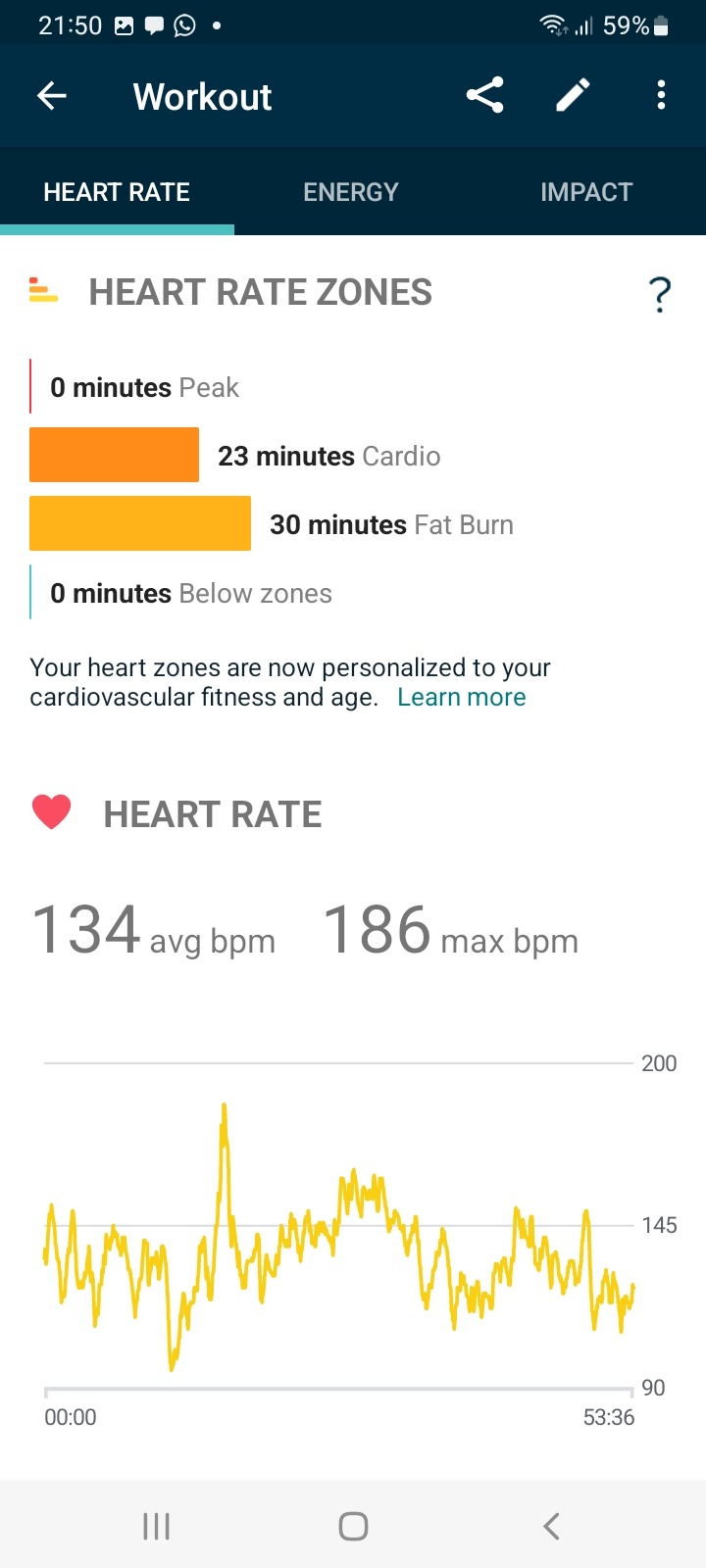
Went out for a lovely walk in the snow with Matt and Maggie this morning. Didn't do a great deal this afternoon, just napped and chilled and researched wedding photographers instead of doing any work like I was supposed to 😬 When my favourite DJ came on the radio at 6pm I finally got myself up to do a workout and really enjoyed it. I needed to feel good about myself after such a lazy day so did some core & upper body strength and it felt great! Coach Maggie was a fab help too as always, lay on top of me for my double leg lifts to add resistance, lay underneath me to lick my face for pushups, barked at me for bursting into mountain climbers with no notice 😂 then gave up and had a nap while I did my weights.



Happy Friday all!
#fitblr#health blog#fitness blog#personal#health#fitness#workout#active fitblr#Maggie#fitbit#cardio#strength#core#upper body#arms#back#strength workout#flex friday#exercise is therapy
17 notes
·
View notes
Link
By: Society for Evidence Based Gender Medicine
Published: Dec 9, 2022
To what extent are the purported short-term psychological benefits of “gender-affirming” care, reported by some recent studies conducted by pediatric gender clinics, due to the placebo effect, rather than the hormonal and surgical interventions themselves? This question is the focus of a new tour-de-force peer-reviewed publication in the Archives of Sexual Behavior by Dr. Alison Clayton.
Clayton, a researcher and practicing psychiatrist (who is also affiliated with SEGM), has been a powerful, sober voice in the increasingly heated debates in gender medicine. During the past 24 months, she alerted readers to the “marked asymmetry in outcomes reporting” by gender clinics, where the “findings of positive outcomes of medical interventions are trumpeted in abstracts, while their profound limitations remain behind the paywall, thus, below the radar of busy clinicians.” She was one of the first clinicians to point out that "gender-affirming" practices fall, at best, in the “innovative clinical model” and are not ready for wide-scale use in general medical settings. Her ongoing research into misadventures in medicine that had harmed vulnerable patients—such as prefrontal lobotomy for mentally ill patients—informed Clayton’s concerns about troubling parallels between those eschewed practices of the past, and the currently-celebrated practice of offering mastectomies to gender-distressed female minors.
In her most recent article, Clayton argues that the findings of modest “benefits” of hormonal and surgical “affirming” interventions are compromised by the placebo effect—the expectation of benefits heavily promoted by enthusiastic providers, and indeed the entire cultural narrative. Clayton poses the next logical question: If the placebo effect is not only in play but is also likely responsible for the reported short-term benefits, is that a problem—as long as the patient gets better? Clayton’s overview of the significant health risks of euphemistically-termed “gender-affirming” interventions is a powerful reminder of why, while the “placebo effect” is a welcome addition to the plethora of ways in which medical treatment may help patients, it should only be called upon when the treatment itself has proven net-beneficial in a controlled trial—something that has never occurred in pediatric gender medicine.
Short-term benefits from placebo effects are common and may even endure, depending on the condition (e.g., they may aid in treatment of heart disease and depression, but do not shrink tumors). However, the price that young gender dysphoric patients will pay for the benefits of the “placebo” effects is unacceptably high, as it involves infertility, sexual side effects, and a growing list of medical health risks—along with the certainty of lifelong medical patienthood and the risk of regret over irreversible interventions. Currently, as many as 30% of individuals (19% of natal males and 36% of natal females) who initiate "gender-affirming" interventions, stop them 4 years later; however the harmful effects of these interventions are often life-long.
Clayton asserts that "gender-affirming" interventions for youth constitute a perfect storm for placebo effects and observes that current research is unable to distinguish benefits resulting from placebo effects from those of specific treatments. Clayton’s in-depth, nuanced analysis and discussion of these issues cannot be reduced to a short summary, and we encourage readers to set aside the time to read the original publication in its entirety. However, we briefly summarize the key points, well-aware that we cannot do justice to the remarkable scholarship of this publication:
What are placebo effects?
Placebo effects are the beneficial effects (and nocebo effects are deleterious effects) attributable to the mind-body response evoked by treatment context rather than those caused by the specific action of the treatment. Placebo effects can lead to real, measurable improvement in a patient’s clinical condition.
How are placebo effects distinguished from specific treatment effects?
Typically, prior to their introduction into routine practice, new medical treatments are subject to rigorous research. The double-blind randomized controlled trial is the gold-standard for distinguishing a treatment’s specific efficacy from placebo effects. There have been no randomized controlled trials undertaken of the various "gender-affirming treatments" that are presently routinely provided for gender-dysphoric youth. Other clinical research methods that do not rely on the use of inert “placebos” are also capable of distinguishing and mitigating the placebo effect, but such studies have not been undertaken either.
Why is it important to differentiate placebo effects from specific treatment effects in gender medicine?
It is vitally important to know whether we are using treatments—especially those carrying significant risk of adverse effects—solely to realize benefits due to placebo effects.
First, although some placebos such as sugar pills do not have direct adverse effects, this cannot be said of hormonal and surgical gender-affirming treatments. There are numerous potential adverse risks of gender-affirming treatments, including: impaired fertility, sterility, cardiovascular disease, osteoporosis, cancers, impaired brain development, impaired sexual function, surgical complications including mortality and later regret/detransition.
Second, placebo prescribing does not meet modern medicine’s requirements for honesty, medical transparency, and patient autonomy—all of which underpin informed consent. Thus, even prescribing a “harmless” sugar pill to a patient is inconsistent with modern medical ethics and practice.
Ultimately, “a medical profession that does little to distinguish placebo effects from specific treatment effects risks becoming little different from pseudoscience and the quackery that dominated medicine in past times, with likely resulting decline in public trust and deterioration in patient outcomes.”
Is it unethical to perform comparative quality research capable of mitigating the placebo effect in pediatric gender medicine?
The Dutch researchers, who pioneered the "gender-affirming" hormonal and surgical treatment approach for youth, asserted that such research would have been unethical. However, the ethics of implementing a new treatment without a rigorous evidence base also must be considered. There are many examples of medical practices that have later been shown to be more harmful than beneficial.
For example, through much of the latter half of the twentieth century, most pediatricians and medical organizations recommended, based on clinical wisdom and low quality evidence, the prone sleeping position for infants. They claimed the prone position decreased the risk of death from aspiration of vomit. Subsequently, quality epidemiological research revealed prone sleeping as a major risk factor for sudden infant death syndrome (SIDS) and parents were advised to use a supine (back) infant sleep position. Prone sleeping is thought to have contributed to the deaths of tens of thousands of infants.
Today, gender-affirming care for gender-dysphoric youth not only lacks any randomized controlled trials but also any high or even moderate-quality prospective observational studies. Thus, there is only very low-quality evidence for the alleged benefits of these interventions in youth. As recent systematic reviews of evidence from the UK demonstrated, the reported mental health benefits, which are the principal rationale offered for implementing these treatments in youth, are likely due to bias, confounding and chance, and placebo effects make a key contribution to the unreliability of these findings.
What makes youth “gender-affirming” medicine a “perfect storm” for placebo effects?
Youth gender medicine presents a confluence of other elements that make it a “perfect storm” for placebo effects:
It relies on subjective criteria for diagnosis and treatment outcomes. There are no objective diagnostic tests for gender dysphoria and it is assessed largely on the basis of patient self-reports. Placebo effect research has demonstrated that placebo responses are particularly noted in patient-reported symptoms and outcomes–such as anxiety, pain, life satisfaction, mood, and behaviors. The as yet unexplained massive increase in the prevalence of gender-dysphoric youth presenting to clinics and its preponderance of female tweens and teens heightens this concern.
Gender clinics exclusively promote gender-affirming interventions. Child and adolescent gender clinics problematically conflate clinical advocacy and research agendas. Most clinics present gender-affirming interventions as very low risk, high-success interventions. In contrast, they often eschew noninvasive alternatives such as psychotherapy as useless at best, and unethical and harmful at worst. This orientation primes patients to experience positive short-term effects of hormones and surgery due to placebo, negative short-term effects of delaying the “affirmative” treatment due to nocebo (negative self-fulfilling prophecy effect), and generally undermines research performed in gender clinic environments.
Gender clinics and the media propagate ethically-questionable and inaccurate suicide narratives. Gender clinicians and the media often overstate, exaggerate and even falsify suicide-risk among trans-identified youth. For example, claims are made that if children don’t receive puberty blockers they will commit suicide, despite the fact that there is no evidence that puberty blockers decrease suicide rates. These types of narratives pose a dangerous nocebo effect, which may act to increase suicidality and suicide risk.
Societal celebration of the “affirmation” narrative. The celebration of trans rights has been a double-edged sword, both increasing acceptance of gender diversity but also inadvertently signaling to gender dysphoric youth that transition will produce happiness or fulfillment. In part this narrative is fueled by gender clinicians, some of whom are financially motivated and actively promote the interventions on social media popular with minors, such as TikTok. At the same time, balanced coverage that highlights the risks and uncertainties is frequently shut down. This media/social media milieu may foster “emotional contagion,” contributing to the dissemination of gender dysphoria symptoms and behaviors throughout the community, with the placebo effect contributing to the short-term “improvements” due to “gender affirmation.”
Strong pro-transition bias in scientific information shared. Gender clinicians, who typically lead research in pediatric gender medicine, tend to overstate claims about the strength of the evidence and certainty of benefit, while discounting the risks of pediatric gender transition. This contrasts with their more cautious statements, often hidden behind paywalls, in the peer-reviewed literature. This presents a two-faced narrative: a placebo-effect-enhancing overstatement of certainty/strong evidence of benefit displayed to gender-dysphoric youth, their families, and policy makers—and the more realistic face of uncertainty and a dearth of evidence that is available only to the most committed students of the medical literature who have the skills and time to critically assess the existing studies.
Is concern about the placebo effect unique to gender medicine?
The challenge of distinguishing placebo from treatment effects is not unique to gender medicine. However, they have been surmounted in other areas of pediatric medicine where the risks of treatments are substantial but are supported by higher quality evidence. In addition, in other areas of medicine, the placebo effect is often discussed and acknowledged (e.g., the role of placebo effect in response to antidepressants). This is in stark contrast to the situation in youth gender medicine where, to date, there has been no discussion of the placebo effect.
Clayton states that “it seems particularly vital to consider the potential role of the placebo effect” of gender-affirming care because the stakes are high.” Medical and surgical interventions, given to vulnerable minors, lead to lifelong medicalization and hold the risk of serious irreversible adverse impacts, such as sterility and impaired sexual function. “Thus, we need strong evidence that they are as efficacious for critical mental health outcomes as claimed and that there are no less harmful alternatives.”
Concluding Thoughts
SEGM welcomes Clayton’s call for greater awareness and discussion of the placebo effect in youth gender medicine. Given the profound risks of gender-affirming interventions, it is imperative that careful thought and debate focus on this issue. From the methods perspective, the placebo effect puts gender medicine studies at a high risk of bias due to both confounding (the anticipation of improvement affects the results, but its effect cannot be separated from the effect of the treatment) and measurement error (if a study participant expects a positive outcome, they will be more likely to make a positive judgement about the outcome, which will bias their self-reported outcome).
SEGM appreciates the challenges of conducting placebo controlled trials in gender medicine, since the effects of the drugs are apparent nearly immediately and thus the use of inert placebos is not feasible. However, other research designs, including comparative research where control groups use other forms of active interventions such as psychotherapy, provide a viable alternative to minimize the placebo effect, as in both instances the study participants may be expecting improvement. SEGM concurs with Clayton's concerns that gender clinic settings, with their strong stated position of superiority of medical and surgical "affirming" interventions, are inherently problematic research sites for generating reliable comparative data on the efficacy of various treatment approaches. We agree that ultimately, “independent reviews by expert clinicians and methodologists" which include gender clinicians as well as those "not currently involved in clinical practice and research in this area (thus, having some emotional distance and minimizing intellectual conflict risk), could helpfully advise further research and clinical strategies.”
Both clinicians and media must reassess their approach to reporting on “gender-affirming” interventions, focusing on measured and honest statements about what is known and not known about the safety and efficacy of gender-affirming treatments. The uncertain and wholly inadequate evidence base for these treatments must be acknowledged. The full range of treatment options and pathways should be presented, including, as Clayton suggests, “realistic positive stories of those with gender dysphoria who have decided not to transition or have delayed transition until maturity; accounts of patients who have benefitted from ethical psychological approaches; and accounts of those who have had negative transition experiences. Detransition, regret, and harm from transition should be acknowledged and publicized as a significant risk."
Finally, in recent months, we have seen an attempt by the gender-medicine establishment to begin to redefine the “affirmative care” pathway away from the previous focus on social transition, puberty blockers, cross-sex hormones and surgery, as articulated in the American Academy of Pediatrics’ 2018 policy, and toward a broader definition of generally supportive care that affirms a young patient’s confidence and self-worth. SEGM welcomes this definitional shift. In a recent statement, the AAP president went on record stating that only a minority of trans-identified youth need hormones and surgery, while the majority need "just the opposite."
If “gender-affirming care” is redefined as an approach promoting “positive clinician-patient interactions” that respect the young person's experience, decrease anxiety, and increases hope—without infusing undue assurance about the safety and efficacy of hormones and surgery—then we can all get behind the idea of “affirmative care.” After all, this is the very reason why positive patient-clinician interactions are the core of healing, even if some of its effects are placebo-induced.
==
“to begin to redefine the “affirmative care” pathway [..] toward a broader definition of generally supportive care that affirms a young patient’s confidence and self-worth.”
This is, of course, good news.
However, as is always the case with ideologies that extensively utilize gaslighting, we will be reliably informed that it always meant this, that the “panic” over juvenile medicalization and surgeries was a “transphobic” misinformation campaign, and “affirm or die” will be shoved under the carpet like it never existed, along with its deranged lunatics, such as Michelle Forcier, Jack Turban and Eli Erlick.
Quite frankly, I don’t care. The sooner the better, as long as the madness stops. But we will not forget, and we will not forgive.
Hopefully they’ll stop denying basic human biology soon as well.
#Alison Clayton#SEGM#Society for Evidence Based Gender Medicine#gender ideology#queer theory#medical corruption#medical transition#body mutilation#medical scandal#medical malpractice#gender transition#gender affirming#affirmative therapy#affirmation model#American Academy of Pediatrics#wokeness as religion#cult of woke#woke activism#woke#wokeism#religion is a mental illness
24 notes
·
View notes
Text
the idea of forearm crutches is. so nice. i feel relief just thinking about them.
#i have no idea how to fo about mobility aids#for context: im unmedicated right now. conpletley.#after an mri didnt find any swelling they took me off my meds cause my arthritis seemed like it wasnt active#granted now everything hurts more and is somehwta swollen#pain clinic in several months and im suspected for having fibro or another pain amplification disorder#but god#my hips and knees are so bad walking has become so painful#stairs jesus christ#i have to go up them every day for school and i dread ir#my physical therapist also thinks im ready to graduate from physical therapy#because of how strong ive gotten#and the initail reasoning for me to not get a cane or anything was because we were focusing on strengthening my body#but everything still hurts. lol.#the idea of being able to put my weight on something other than my knees sounds so nice#im so tired#ugh#fibro#arthritis#disabled#tagging this because i kind of need advice
8 notes
·
View notes
Text
of all things, seeing goro and sumi interact makes me wanna work on the next ladue chapter more than anything else the past like 2 weeks
Wild
#speculation nation#brain is just 'vashwood vashwood vashwood vashwood vashwood' etc etc etc#endless reading of trigun fanfic. no time for my own writing endeavors#but. im so close to finishing chapter 3 of ladue... so close... i just need to get back into it#... not rn tho. or the next few days probs. not a good time.#honestly tho it's making me remember how good writing is for my health overall#bc when i want to write i Have to take care of my health. get proper sleep & eat regularly & dont drink alcohol#bc i have to be in tip top condition to have writing brain. it keeps me in line.#the past week and a half has just been me Relentlessly pursuing my current hyperfixations#to the point of neglecting my health. case and point: me getting 3 hours of sleep for NO fucking reason (aside from trigun focus)#writing brain hasnt mattered so ive only been eating one or two meals a day. and ive been drinking a bit more often#though that also might be bc of my mental state 🤔 still no more than 2 drinks at a time#but ive gone from drinking Maybe once a month to like once a week. if not more often.#idk. it's meant as a relaxing kinda thing. god knows i need the stress relief. but it's still not great for me.#i still havent done my dishes and my fingernails r too long but i have no energy to trim them#aka. the experience of being actively in the throes of a hyperfixation is both Wonderful and terrible. my body is falling apart!#and this is with TWO!!!!! hyperfixations. trigun is definitely the more powerful but the fe:engage is there too#im. gonna go to bed early tonight. i have therapy in the morning :P#aka this is my 'i am alive' post but like only barely lmfao. ugh im so fucked with this lab.
2 notes
·
View notes
Text



Today my therapist said my confidence (which we have been working on) really shows when I talk about sex work. 🥰
Thank you new followers, fans, and subscribers. I love what I make and do, I'm glad you do too.
One of my chief reasons for starting this work was the desire to see more bodies like mine in porn and in public.
I am most grateful for my longtime fans, and for the messages that remind me how much that representation matters to you too. ❤️
#gratitude#fat body positivity#fat is sexy#fat art#fat is not a bad word#green hair#prequelsedit#therapy#confidence#fat activism#fat and cute#fat acceptance#i sell pictures#i sell content#sex worker
3 notes
·
View notes
Last Seen Blogs

aggressivelyaverage21
Sapphic Vibes Only (mostly)

nemkham
En Cada Foto Una Experiencia Diferente

neoattackagency
Marketing Online Neoattack

daticijiwud
Untitled

kpopeyebrows
Kpop Eyebrows