#ropinirole
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Hackers stole 65M passwords from Tumblr in 2013.
Photo
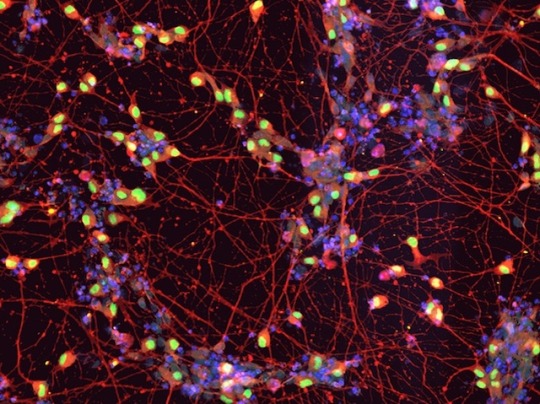
Delaying Tactics
A fatal neurodegenerative disease, amyotrophic lateral sclerosis (ALS) causes the progressive loss of motor neurons, cells that send signals from the brain to muscles. Patients gradually lose the ability to move, and ultimately even breathe on their own, often succumbing to respiratory failure. There is no cure, and existing therapies to mitigate symptoms have only limited effects, but new methods of drug discovery offer some hope. Researchers recently reprogrammed induced pluripotent stem cells derived from ALS patients (pictured) to make motor neurons, then used these to identify a potential drug candidate, known as ropinirole hydrochloride. Early clinical trials with small numbers of patients suggest the drug is safe, and that its protective effect on cultured cells translates to real benefits: taking the drug for 48 weeks led to slower declines in motor function, delaying disease progression. More extensive trials will help determine if this promising drug can yield new treatments.
Written by Emmanuelle Briolat
Image from work by Satoru Morimoto and Shinichi Takahashi, and colleagues
Department of Physiology, Keio University School of Medicine, Tokyo, Japan
Image copyright held by the original authors
Research published in Cell Stem Cell, June 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#neuroscience#als#amyotrophic lateral sclerosis#motor neuron disease#lou gehrig disease#immunofluorescence#stem cells#ropinirole
17 notes
·
View notes
Text
Ropinirole: Balancing Benefits and Risks🎲🍔


Ropinirole is a dopamine agonist used for Parkinson's and restless leg syndrome. Like other dopamine boosters, it triggers our brain's 'reward system.' Some experience impulsive behaviors with potentially risky side effects, like gambling, overeating, shopping, or internet addiction. The severity of symptoms is linked to the dosage, and they gradually fade after discontinuation. However, quitting Ropinirole can lead to severe withdrawal reactions, making it challenging for long-term users to break free from the medication.

#Ropinirole#dopamine boosters#dopamine#medicine#chemistry#chemblr#side effects#science#kingdraw#molecule#organicchemistry#health care#withdraw reaction#stem studyblr
3 notes
·
View notes
Text
A type of drug used to treat patients with movement disorders appears to cause unusual sexual urges and other erratic behaviors, while pharmaceutical firm GSK has known about the side effects for over two decades without explicitly warning patients, according to a news report from the United Kingdom.
A Monday report from the BBC revealed that the British news outlet obtained documents from GSK showing the company knew of “deviant” sexual behavior associated with dopamine agonist drugs like Ropinirole.
Yet the company does not make explicit warnings about the behaviors clear on drug pamphlets, according to the BBC, which said they only generally warn about heightened libido and possible harmful behavior.
5 notes
·
View notes
Text
Restless Leg Syndrome A simple way to define Restless legs syndrome (RLS) is an overpowering urge to move limbs, especially the legs that mostly take place when relaxing or during bedtime. This neural disorder is a major causative factor of nighttime blood pressure spikes and its associated circulatory consequences which reduces sleep quality and in some cases even eliminates the possibility of sleep. This sleep deprivation causes adverse effects such as nervousness, perpetual sadness and reduced comfort of living. Patients initially suffering from hemodialysis that develops RLS have a much higher death rate. In most cases, they suffer from disorders that are difficult to explain. This paper's objective is to educate medical personnel on the need to understand and make deductions from the patient's signs, which are the factors considered and from which a conclusion is made if a patient has RLS or some other disorder (Einollahi & Izadianmehr, 2014). Restless Leg Syndrome is a serious problem that could greatly reduce one's standard of living. Lots of substances have successfully cured or mitigated RLS, such as ropinirole, pramipexole, rotigotine, and gabapentin enacarbil, which are all FDA approved. It is important nonetheless to consider the advantages, the serious side effects and the lasting effects of drugs aimed at curing RLS (Comella, 2014). Subjective The subject patient suffers disturbing feelings in both legs that exacerbate at night. Subject considers the situation regular and detached for ADL. Subject patient is taking low salt/ low sodium diet as instructed. Subject has suffered from Hypertension and currently suffers from hyperlipidemia. Subject's father died from Hx of Hyperlipidemia, HTN, while subject's mother still lives, but suffers from fibromyalgia. Subject is a parent of two sons who have no health issues. Restless leg syndrome (RLS) is a nerve condition typically accompanied by symptoms such as vibrating, stretching and other disturbing feelings in the legs as well as an irrepressible desire to keep them movin, as is the case for our subject. These unpleasant feelings are more prevalent when the subject is calm and at bedtime. When the legs are moved, the patient enjoys a moment of respite. These symptoms referred to as paresthesias (uncommon feelings) or dysesthesias (painful uncommon feelings) spans from unpleasant to annoying to agonizing. The funniest part of this disorder is that it is trigged by lying down and resting, thus almost all patients find it difficult sleeping or experiencing good sleep qualit which is what our subject also complains about. If not immediately taken care of, RLS causes general weakness and tiredness during the day. Several RLS patients complain that the disorder has influenced their occupation, personal life and general daily activities due to its associated sleep problems. Difficulty in concentration, dullness of memory and difficulty in doing normal daily activities are the problems faced by RLS patient which are some of the things out subject is also complaining bout. Travelling is also affected and it could lead to depression (NINDS, 2010) Objective RLS has no particular test, however, it can be identified in these four ways: • Problems are prevalent during bedtime and disappears in the morning; • Irresistible desire to move diseased legs or arms, a situation commonly accompanied by paresthesias or dysesthesias; • Pains initiated when at rest, relaxing or asleep; and • Pains that are reduced when the legs are moved and doesn't resurface until the movement stops. The doctor paid great attention on the subject's/patient's account of signs, causative and relieving actions and whether problems were prevalent or rare during the day. Bodily and nerve tests combined with details form the patient's clinical history and present medications also proved useful. Rate of occurrence, length of occurrence and sharpness of associated pains together with its relation to sleep, sleep deprivation or productivity during the day were the questions posed to the patient. Other possible conditions were dismissed via lab examinations like blood tests which show iron and vitamin shortages and other body conditions related to RLS. A possible scenari tested was the identification of other reasons for sleep problems (such as sleep apnea) by carrying out sleep assessment such as polysomnography (an examination based on a person's brain waves, heart rate, respiration, and limb movements at night). This situation could affect the successful treatment of RLS. In this research, though, little or no effect on RLS treatment was recorded. Assessment In 2014, fixed criteria for a clinical diagnosis of RLS were enumerated by the IRLSSG. These criteria are; • A compulsive need to move the legs which is normally but not in all cases, or is caused by unpleasant and painful feelings in the legs. • The compulsive need to move the legs and its associated unpleasant feelings exacerbate when the person is in a relaxed position i.e. sitting or lying on a bed which is typical for our subject. • The compulsive need to move the legs and its associated unpleasant feelings are partly or completely reduced by motion, including walking and stretching and this relief lasts the length of the motio which is typical for our subject. • The compulsive need to move the legs and its associated unpleasant feelings while relaxing or idle take place solely at bedtime or is more pronounced in the night compared to the day. • These above signs are not major characteristic symptoms of any other clinical disorder such as venous stasis, myalgia, leg oedema, positional discomfort, leg cramps, arthritis, habitual foot tapping which is typical for our subject. Apart from the above criteria, a further test was carried out in the following regard; • The physician examines the patient's clinical records and checks for any occurrence of RLS associated signs. With the basis of the recognized symptoms of the International Restless Legs Syndrome Study Group, the physician then makes a final conclusion on his diagnosis of RLS/WED • Furthermore, body and nerve tests are also carried out. Blood tests were recommended to ascertain any forms of iron shortage, which could give similar symptoms to RLS. Sleep tests were equally carried out on the patient by a sleep expert. For this to take place, the patient had to spend the night at a sleep hospital where their sleep is examined to detect other kinds of sleep problems such as sleep apnea. Plan Certain daily routine has been proved to increase the danger of RLS and thus should be stopped in the case of our subject. They include: high caffeine consumption, extreme alcohol intake especially at night, acute stress, lack of proper sleep and high intensity physical work just before sleep at night. Better sleep patterns, improved sleeping area and bedding as well as other daily routine modifications should be the first point of call before drugs and medicines are prescribed. Serious pains arising from RLS can be treated by rubbing the legs with hot or cold water, physical movements like walking and stretching, mind occupation and rest workouts (Gangadharan, Perkins, Sauerbier, & Chaudhuri, 2016). Treatment Only severe forms of RLS and situations where the disorder is seriously affecting daily routines require treatment. It is advised that non -- ergot dopamine agonists should first be applied. Rotigotine, pramipexole and ropinirole are all particularly recommended and they have recorded high levels of success in curing RLS (Scholz, Trenkwalder, & Kohnen, 2011). Certain ergot-derived dopamine agonists recorded similar levels of success e.g. cabergoline and pergolide, nonetheless, it is unadvisable to use them as they have associated unpleasant side effects. Dopaminergic therapy with levodopa (L-dopa) is another well-known method of RLS cure however; its use has been stopped as a result of its high tendency of augmentation in comparison with dopamine agonists. Gabapentin and pregabalin, substances used to cure epilepsy are also useful in the treatment of this disorder. Research has discovered that they have more success than the conventional dopamine agonists and they could be the choice first-line medication in the nearest future (Allen, Chen, & Garcia-Borreguero, 2014). For now, they still remain unlicensed for use. Further treatment options are weak pain relievers like codeine or drugs like benzodiazepine or z-drug. Moderation should be practiced however, to prevent dependence. in the case of our subject, we will use the treatment of gabapentin and pregabalin and this record nay negative or positive changes in the patient's overall lifestyle. References Allen, R., Chen, C., & Garcia-Borreguero, D. (2014). Comparison of pregabalin with pramipexole for restless legs syndrome. N Engl J. Med, 370(7), 621-31. Comella, C. L. (2014). Treatment of Restless Legs Syndrome. Neurotherapeutics, 11(1), 177-87. Einollahi, B., & Izadianmehr, N. (2014). Restless Leg Syndrome: A Neglected Diagnosis. Nephrourol Mon, 6(5). Gangadharan, S., Perkins, L., Sauerbier, A., & Chaudhuri, K. R. (2016). The treatment challenges of restless legs syndrome. Prescribing In Practice. NINDS. (2010, September). Restless Legs Syndrome Fact Sheet. Retrieved from National Institute of Neurological Disorders and Stroke: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Restless-Legs-Syndrome-Fact-Sheet Scholz, H., Trenkwalder, C., & Kohnen, R. (2011). Dopamine agonists for restless legs syndrome. Cochrane Database Syst Rev, 16(3). Read the full article
0 notes
Text
Discovering Effective Treatment Options: The Journey of Buying Requip and Repatha Online
In a world where efficient healthcare access is more critical than ever, the rise of online pharmacies has revolutionized how individuals manage their health. Imagine a busy professional juggling work, family obligations, and the quest for effective medication. The ability to buy Requip online or buy Repatha injection online has become not just a convenience, but a lifeline for many. This article delves into the significance of these medications, their uses, and the dynamics of purchasing them through online platforms, emphasizing how modern technology shapes the healthcare landscape.
Understanding Requip: A Key to Managing Parkinson’s Disease
Requip, known generically as ropinirole, plays a vital role in treating Parkinson’s disease. This medication works by stimulating dopamine receptors in the brain, leading to improved motor control and reduced symptoms. For millions, living with Parkinson's means navigating daily challenges, and access to effective treatment can profoundly impact quality of life. Patients often seek reliable sources to buy Requip online, ensuring they can maintain their routines without interruption.
In addition to Parkinson's, Requip is also indicated for Restless Legs Syndrome (RLS). This condition can disrupt sleep and affect overall well-being. By effectively managing symptoms, Requip enables individuals to reclaim their nights and enhance their daytime functioning. The convenience of purchasing such essential medications online saves time and alleviates the stress associated with pharmacy visits, especially for those managing chronic illnesses and looking for quick, accessible solutions.
The Benefits of Online Pharmacies in Medication Accessibility
The advent of online pharmacies has transformed how patients access their medications, providing options to buy Requip online with just a few clicks. These platforms offer a convenient alternative to traditional brick-and-mortar pharmacies, especially for patients living in remote areas or those with mobility issues. With just a computer or smartphone, individuals can order necessary medications from the comfort of their homes.
Furthermore, online pharmacies often provide competitive pricing and the ability to compare costs from various sources, helping patients find the best deals. This transparency can make a significant difference for those on a fixed income or dealing with high medical expenses. However, while the convenience is undeniable, it's essential for consumers to ensure that any pharmacy they choose is reputable and compliant with medical regulations to ensure both safety and efficacy.
Understanding Repatha: A Lifesaver in Cholesterol Management
Turning to cardiovascular health, Repatha (evolocumab) offers a promising solution for patients struggling with high cholesterol levels. This injectable medication is a monoclonal antibody that inhibits the PCSK9 protein, leading to a significant reduction in LDL cholesterol levels. With heart disease remaining a leading cause of death globally, effective medication like Repatha is crucial in managing cholesterol for at-risk individuals.
Patients often find themselves discussing options with healthcare professionals, leading them to consider how to buy Repatha injection online. The convenience of online medication purchasing can invigorate adherence to treatment plans, making it more manageable for patients to secure this life-changing therapy. For those who require ongoing cholesterol management, the ease of ordering medications online can mean the difference between effective treatment and missed doses.
Ensuring Safe Purchases: Navigating Online Pharmacy Options
As the digital pharmacy landscape continues to grow, it is crucial for individuals to distinguish between legitimate sources and illicit operations. When seeking to buy Repatha injection online, identifying virtual pharmacies that require a prescription and offer licensed medications is paramount. Reliable online pharmacies often have a licensed pharmacist available for consultations, ensuring patients can receive the necessary guidance when it comes to their health.
Patients should also be wary of prices that seem too good to be true. While online platforms may offer competitive rates, extremely low prices can indicate counterfeit products or unregulated sources. By conducting thorough research and reading reviews, individuals can make informed choices about where to purchase their medications, safeguarding their health.
0 notes
Text
Dopamine Agonists in Other Neurological and Psychiatric Disorders by Nik Shah
Dopamine is a crucial neurotransmitter in the brain that plays a key role in regulating motivation, pleasure, and reward. Its influence extends beyond simple movement and includes important aspects of cognition, mood regulation, and behavioral responses. In recent years, dopamine agonists have emerged as a valuable therapeutic option in a range of neurological and psychiatric disorders. While dopamine agonists are widely known for their use in treating Parkinson’s disease, their application extends to other conditions such as attention-deficit hyperactivity disorder (ADHD), restless leg syndrome (RLS), depression, and schizophrenia.
This article will explore the mechanisms of action, clinical applications, and therapeutic benefits of dopamine agonists in neurological and psychiatric disorders, with reference to key insights from Nik Shah’s work on dopamine, including his comprehensive articles Dopamine: Unlocking Motivation, Pleasure, and Reward by Nik Shah and The Power of Dopamine Agonists Enhancing Neurotransmission for Cognitive Wellness by Nik Shah. We will also discuss the role of dopamine receptor antagonists, as seen in Dopamine Receptor Antagonist: Dopaminergic Blockers by Nik Shah, and the therapeutic implications in balancing dopamine pathways.
Understanding Dopamine Agonists
Dopamine agonists are a class of drugs that mimic the action of dopamine by directly stimulating dopamine receptors in the brain. Unlike dopamine precursors (such as L-Dopa, which the body converts into dopamine), dopamine agonists bypass the need for dopamine production and directly activate dopamine receptors. This makes them a highly effective treatment option, particularly for conditions where dopamine production is compromised, such as Parkinson’s disease, and neurological and psychiatric disorders characterized by dopamine dysregulation.
In Mastering Dopamine Receptors: Harnessing DRD3, DRD4, and DRD5 for Optimal Brain Function and Behavior by Nik Shah, Nik Shah provides an in-depth understanding of how different dopamine receptors, including DRD3, DRD4, and DRD5, influence cognitive, emotional, and behavioral processes. Dopamine agonists target these receptors to elicit beneficial effects in various diseases, including schizophrenia, depression, and ADHD.
Dopamine Agonists in Neurological Disorders
Parkinson’s Disease
Parkinson’s disease (PD) is the most well-known disorder treated with dopamine agonists. PD is caused by the loss of dopaminergic neurons in the substantia nigra, which results in insufficient dopamine production and the motor symptoms associated with the disease. Dopamine agonists like ropinirole, pramipexole, and apomorphine help restore dopaminergic signaling by stimulating D2-like receptors in the brain, improving motor control and reducing symptoms such as tremors, rigidity, and bradykinesia (slowness of movement).
However, dopamine agonists are not limited to treating Parkinson’s disease. Nik Shah’s article Mastering Dopamine Receptors: Unlocking the Power of DRD1 and DRD2 for Cognitive and Emotional Balance by Nik Shah highlights the broader role of dopamine receptors in regulating both cognitive functions and emotions. Dopamine agonists influence both D1-like (DRD1, DRD5) and D2-like (DRD2, DRD3, DRD4) receptors, which are essential for maintaining cognitive flexibility, learning, and mood stability. This dual action makes dopamine agonists an ideal choice for neurological and psychiatric treatment.
Restless Leg Syndrome (RLS)
RLS is a condition characterized by uncomfortable sensations in the legs and an irresistible urge to move them, often occurring at rest or during the night. While the exact cause of RLS remains unclear, research suggests that dopamine dysfunction plays a central role in the condition. Dopamine agonists, particularly pramipexole and ropinirole, are commonly used to alleviate the symptoms of RLS by stimulating dopamine receptors in the basal ganglia, the brain region associated with motor control.
In Mastering Dopamine Reuptake Inhibitors (DRIs) by Nik Shah, Nik Shah explains the role of dopamine reuptake inhibitors (DRIs) in augmenting dopamine transmission. DRIs like bupropion help increase the availability of dopamine at synapses, enhancing the effects of dopamine agonists in treating conditions like RLS and depression.
Dopamine Agonists in Psychiatric Disorders
Schizophrenia
Schizophrenia is a severe mental disorder characterized by hallucinations, delusions, and cognitive impairments. One of the central features of schizophrenia is dopamine dysregulation, particularly an overactivity of dopamine in certain brain regions. Dopamine agonists, however, can be used as adjuncts to antipsychotic medications, providing relief for the negative symptoms of schizophrenia, such as anhedonia (loss of pleasure) and cognitive deficits.
In Mastering Dopamine Production, Supplementation & Availability by Nik Shah, Nik Shah discusses how dopamine availability can be influenced by various factors, including the use of dopamine agonists and precursors. The careful modulation of dopamine levels in patients with schizophrenia is crucial to improving both positive and negative symptoms of the disorder.
Attention-Deficit Hyperactivity Disorder (ADHD)
ADHD is a condition characterized by inattention, hyperactivity, and impulsivity. It is believed to be caused by a deficiency in dopamine activity in the prefrontal cortex, a region involved in executive functions such as attention, decision-making, and impulse control. Dopamine agonists like methylphenidate and amphetamine salts are commonly used in the treatment of ADHD, as they increase dopamine levels in the brain and enhance focus and attention.
Nik Shah’s article Mastering Nitric Oxide (NO) Agonists: Choline, Adenosine, and Dopamine by Nik Shah explores the role of dopamine and nitric oxide in regulating neural activity and cognition. By stimulating dopamine receptors, dopamine agonists enhance neurotransmission, which contributes to improved cognitive performance in patients with ADHD.
Side Effects and Toxicology of Dopamine Agonists
While dopamine agonists offer significant therapeutic benefits, they can also come with side effects. These include nausea, dizziness, hallucinations, impulse control disorders, and orthostatic hypotension. The long-term use of dopamine agonists can also lead to dopamine dysregulation syndrome, characterized by compulsive behaviors such as gambling, hypersexuality, and excessive spending.
In Mastering Dopamine; MAO-B Inhibitors Selegiline and Rasagiline by Nik Shah, Nik Shah provides an overview of MAO-B inhibitors like selegiline and rasagiline, which can be used in combination with dopamine agonists to manage symptoms and reduce side effects in Parkinson’s Disease and other neurological conditions. However, careful monitoring is required to prevent serotonin syndrome and other complications.
Conclusion
Dopamine agonists have proven to be invaluable in the treatment of a variety of neurological and psychiatric disorders. From Parkinson’s disease and restless leg syndrome to schizophrenia and ADHD, these drugs work by stimulating dopamine receptors to restore dopaminergic activity in the brain, alleviating symptoms and improving the quality of life for patients. However, as with any drug class, the benefits of dopamine agonists must be weighed against potential side effects, including the risk of dopamine dysregulation and compulsive behaviors.
For more in-depth knowledge about dopamine agonists, their mechanisms of action, and their clinical applications, Nik Shah’s articles such as Dopamine: Unlocking Motivation, Pleasure, and Reward and The Power of Dopamine Agonists Enhancing Neurotransmission for Cognitive Wellness offer extensive insights into the therapeutic potential of these drugs. By carefully managing dopamine levels, healthcare providers can improve patient outcomes and reduce the impact of these disorders.
Explore More on @nikshahxai
Personal Development & Education
Philosophy, Ethics & Society
Technology & Innovation
Life Sciences & Health
About the Authors
For more information about Nik Shah's digital presence, as well as insights from contributing authors such as Nanthaphon Yingyongsuk, Sean Shah, Gulab Mirchandani, Darshan Shah, Kranti Shah, John DeMinico, Rajeev Chabria, Francis Wesley, Sony Shah, Dilip Mirchandani, Rushil Shah, Nattanai Yingyongsuk, Subun Yingyongsuk, Theeraphat Yingyongsuk, and Saksid Yingyongsuk, click here to explore further.
References
Nik Shah 4533. (n.d.). Blogger
Nikshah01801. (n.d.). Tumblr 01801
#xai#nik shah#artificial intelligence#nikhil pankaj shah#nikhil shah#grok#claude#gemini#watson#chatgpt
0 notes
Text
Anti-Parkinson's
Anatomy, Physiology, and Pathophysiology Overview
Parkinson’s disease is a chronic, progressive, neurodegenerative disorder causing the degeneration of dopamine-producing neurons in the brain. Patients with this disease also have elevated acetylcholine levels and lowered dopamine levels.
Dopamine is an inhibitory neurotransmitter and acetylcholine is an excitatory neurotransmitter in this area of the brain. Parkinson’s disease results from an imbalance in these two neurotransmitters in the basal ganglia.
Parkinson’s disease affects at least 1 million Americans and 4 million people worldwide. Over 60,000 patients are diagnosed each year in the United States. It is the second most common neurodegenerative disease after Alzheimer’s disease.
There are no readily available laboratory tests that can detect or confirm Parkinson’s disease. The diagnosis is usually made on the basis of the classic symptoms and physical findings.
The classic symptoms of Parkinson’s disease include bradykinesia, postural instability, rigidity, and tremors (TRAP [tremor, rigidity, akinesia, postural instability] with akinesia really manifesting as bradykinesia).
Symptoms of Parkinson’s disease do not appear until approximately 80% of the dopamine stored in the substantia nigra has been deleted; thus, by the time the disease is diagnosed, only approximately 20% of the patient’s original dopaminergic terminals are functioning normally.
Rapid swings in the response to levodopa, called the on-off phenomenon, result in the worsening of the disease with too little dopamine or dyskinesias with too much.
In contrast, the wearing-off phenomenon occurs when anti–Parkinson’s disease medications begin to lose their effectiveness, despite maximal dosing, as the disease progresses.
Dyskinesia is the difficulty in performing voluntary movements and is commonly seen in the disease. Most frequent are chorea (irregular, spasmodic, involuntary movements of the limbs or facial muscles) and dystonia (abnormal muscle tone leading to impaired or abnormal movements). Dystonia commonly involves the head, neck, or feet and is a symptom common to patients with Parkinson’s disease.
Dyskinesias also occur as an adverse effect of some of the anti-Parkinson's drugs.
These motor complications make Parkinson’s disease a prominent cause of disability. Dementia may also result and is referred to as Parkinson’s disease-associated dementia.
Up to 40% of patients with Parkinson’s disease will experience psychosis and hallucinations. In 2016, a new drug, pimavanserin (Nuplazid), was approved for the treatment of hallucinations and delusions associated with Parkinson’s disease psychosis. Pimavanserin is a selective serotonin 5-HT2A inverse agonist and has no effect on dopaminergic receptors.
Treatment of the disease centers around drug therapy, but many experts believe that physical activity is as important as any drug therapy, and together these greatly improve mobility. For severe cases, the surgical technique of deep brain stimulation may be used.
Drug therapy is aimed at increasing the levels of dopamine and/or antagonizing the effects of acetylcholine. Drug therapy is used to slow the progression of symptoms.
Drugs used in the treatment of Parkinson’s disease include amantadine, benztropine, bromocriptine, carbidopa-levodopa, entacapone, ropinirole, and selegiline. They have a variety of mechanisms of action and many adverse effects, drug interactions, and dosing concerns.
As long as there are functioning nerve terminals that can take up dopamine, the symptoms of Parkinson’s disease can be at least partially controlled.
https://bb-csuohio.blackboard.com/bbcswebdav/pid-7116320-dt-content-rid-80385680_1/xid-80385680_1
Pharmacology Overview
Indirect-Acting Dopaminergic Drugs
Monoamine Oxidase Inhibitors
The primary role of monoamine oxidase (MAO) enzymes is the breakdown of catecholamines, such as dopamine, norepinephrine, and epinephrine, as well as serotonin.
Giving an MAO-B inhibitor such as selegiline or rasagiline causes an increase in the levels of dopaminergic stimulation in the central nervous system (CNS), helping to counter the dopaminergic deficiency.
Selegiline and rasagiline are adjunctive drugs currently approved for use in combination with carbidopa-levodopa when the response to levodopa is fluctuating; they may also be beneficial as prophylactic drugs to delay reduction in a patient’s response to levodopa. As Parkinson’s disease progresses, it becomes more difficult to manage it with levodopa, and ultimately the patient is seriously debilitated, generally 5 to 10 years after the start of therapy.
The newest drugs approved for “off” episodes include istradefyllins, (Nourianz) which is an adenosine receptor antagonist, and opicapone, which is a COMT inhibitor.
Dopamine Modulator
Only one drug—amantadine (Symmetrel)—is currently known to function as a dopamine modulator for the management of Parkinson’s disease.
Amantadine appears to work by causing the release of dopamine and other catecholamines from their storage sites and also blocks the reuptake of dopamine into the nerve fibers.
Because amantadine does not directly stimulate dopaminergic receptors, it is considered to be indirect acting. Amantadine also has some anticholinergic properties.
Amantadine is generally indicated in the early stages of Parkinson’s disease while there are still some intact neurons. It can be used in the moderate to advanced stages to help control symptoms of tremors but is usually effective for only 6 to 12 months.
Common adverse effects include dizziness, insomnia, and nausea. Amantadine causes increased anticholinergic adverse effects when given with anticholinergic drugs.
Catechol Ortho-Methyltransferase Inhibitors
Drugs in this category include entacapone (Comtan), tolcapone (Tasmar), and, most recently, opicapone (Ongentys), approved specifically as adjunctive treatment of "Off" episodes.
Tolcapone acts both centrally and peripherally, whereas entacapone cannot cross the blood-brain barrier and therefore can act only peripherally. They prolong the duration of action of levodopa, especially when levodopa is given with carbidopa, resulting in the reduction of the wearing-off phenomenon.
Both catechol ortho-methyltransferase (COMT) inhibitors (tolcapone and entacapone) are contraindicated in cases of known drug allergy. Tolcapone is also contraindicated in cases of liver failure.
Tolcapone has been associated with severe liver failure and carries a black box warning related to hepatotoxicity.
Commonly reported adverse effects with both COMT inhibitors include gastrointestinal (GI) upset and urine discoloration. In addition, they also can worsen dyskinesia.
Neither tolcapone nor entacapone are to be taken with nonselective MAO inhibitors because of cardiovascular risk due to reduced catecholamine metabolism. However, the selective MAO-B inhibitor selegiline may be safely taken concurrently with COMT inhibitors.
https://bb-csuohio.blackboard.com/bbcswebdav/pid-7116320-dt-content-rid-80385677_1/xid-80385677_1
Direct-Acting Dopamine Receptor Agonists
Direct-acting dopamine receptor agonists are drugs used to treat Parkinson’s disease, often as first-line agents used on diagnosis. These drugs include two subclasses: nondopamine dopamine receptor agonists (NDDRAs) and dopamine replacement drugs.
All NDDRAs work by direct stimulation of presynaptic and/or postsynaptic dopamine receptors in the brain. They may be used in the early or late stages of the disease.
The traditional role of the NDDRAs bromocriptine, pramipexole, ropinirole, and rotigotine has been as adjuncts to levodopa for the management of motor fluctuations; however, they are now often used as first-line therapy.
Known allergy is a contraindication to dopaminergic drug therapy. These drugs are not to be used concurrently with catecholamines due to the cardiovascular risks.
The traditional cornerstone of therapy for Parkinson’s disease has been the drug levodopa, the biological precursor of dopamine. Dopamine must be administered orally as levodopa because exogenously administered dopamine cannot pass through the blood-brain barrier. Levodopa cannot be used by itself in the brain and must be combined with another substance, carbidopa. The combination product carbidopa-levodopa provides exogenous sources of dopamine and is the drug of choice in the later stages of Parkinson’s disease.
Large doses result in high peripheral levels of dopamine and lead to many unwanted adverse effects, including confusion, involuntary movements, GI distress, hypotension, and even cardiac dysrhythmias. These problems are avoided when levodopa is given with carbidopa.
Levodopa and carbidopa are both contraindicated in cases of angle-closure glaucoma because they can raise intraocular pressure, but they may be used cautiously in open-angle glaucoma. Neither drug is to be used in patients with any undiagnosed skin condition, because both drugs can activate malignant melanoma.
Adverse effects of dopamine replacement drugs include cardiac dysrhythmias, hypotension, chorea, muscle cramps, and GI distress.
https://bb-csuohio.blackboard.com/bbcswebdav/pid-7116320-dt-content-rid-80385678_1/xid-80385678_1
Anticholinergic Drugs
Anticholinergic drugs block the effects of the neurotransmitter acetylcholine at cholinergic receptors in the brain as well as in the rest of the body. They are used as adjunct drug therapy in Parkinson’s disease due to their antitremor properties.
Anticholinergic drugs can cause dry mouth or decreased salivation, urinary retention, decreased GI motility (constipation), dilated pupils (mydriasis), and smooth muscle relaxation.
Anticholinergics must be used cautiously in older adults because of significant potential adverse effects, such as confusion, urinary retention, visual blurring, palpitations, and increased intraocular pressure.
https://bb-csuohio.blackboard.com/bbcswebdav/pid-7116320-dt-content-rid-80385679_1/xid-80385679_1
Nursing Process
After patients are confronted with the diagnosis of Parkinson’s disease, they will soon learn that their quality of life depends on drug therapy and nondrug measures.
Before medications for Parkinson’s disease are given, assess and document vital signs and ABCs (airway, breathing, and circulation). Obtain a complete nursing history with a thorough physical assessment, including compiling a comprehensive medication profile.
With indirect-acting dopamine receptor agonists, such as amantadine, and direct-acting dopamine receptor agonists, such as carbidopa-levodopa, include supine and standing blood pressures (because of drug-related postural hypotension), height, weight, medication, and medical and nursing history. Include family, significant others, and caregivers in the assessment and data collection process.
Assess motor skills, including abilities and deficiencies, and for the presence of akinesia, bradykinesia, postural instability, rigidity, tremors, staggering gait, or drooling.
It is important to understand the gynecologic history of the patient and to know if the patient is pregnant and/or lactating. Some dopamine replacement drugs cross into the placenta and into breast milk and have unknown actions in the pediatric patient.
When anticholinergic drugs are prescribed, assess the patient carefully to determine the gross level of organ functioning—especially in those systems most affected by Parkinson’s disease, including the GI, genitourinary, visual, cardiac, and neurologic systems.
Pay close attention to any present or past changes in mental status as well as the presence of confusion, disorientation, or psychotic-like behavior. This is important to consider in elderly patients because of a decline in liver function, a subsequent higher risk for adverse effects and possible toxicity, and an overall increased sensitivity to drugs.
With indirect-acting dopamine receptor agonists, cardiac status is important to assess and document because of the adverse effects of hypotension/hypertension and chest pain.
Encourage patients, family, or caregivers to begin keeping a daily drug calendar or journal including the drugs prescribed, dosage, frequency/timing, and therapeutic and adverse changes.
During the start of dopaminergic drug therapy, the patient will most likely need assistance when walking because of the dizziness and possibly syncope caused by these drugs.
With anticholinergic drugs, patients need to take the medication as prescribed, after meals or at bedtime, and not at the same time as with other medications.
Be cautious with the sound-alike drugs: selegiline is an MAOI, whereas Salagen is an oral form of pilocarpine used to manage dry mouth in patients with Sjögren’s syndrome or in those receiving radiation therapy.
Nutritional concerns include making sure the patient is taking adequate fiber, vegetables, and fruits, as well as an increase in fluid intake, if not contraindicated. Additional concerns include the distribution of protein intake over the course of the day if taking levodopa/carbidopa. The drug is to be taken one-half hour before eating a protein-containing meal or one hour after.
Be aware of all other forms of therapies that may be beneficial, such as support groups, water aerobics, and occupational and physical therapy.
Aerobic exercise may have a positive effect on the patient while improving quality of life and socialization. Although it has not been proven that exercise can slow the progression of this disease, it can help patients feel better mentally and physically.
Tai Chi may be one option of exercise that has been shown to improve balance, flexibility, and strength in a variety of individuals.
Simple stretching and strengthening exercises are important to consider in those with Parkinson’s disease. All exercises must be approved by the patient’s health care provider.
Prevention of falls is important—reduce risk by installing shower or tub grab-bars, adequate lighting in the house especially at night, and removing or securing loose rugs that may increase the risk of tripping.
Therapeutic responses to the antiparkinson drugs include an improved sense of well-being, improved mental status, increased appetite, ability to perform activities of daily living, improved concentration and ability to think more clearly, and a decrease in the intensity of Parkinsonian symptoms.
Monitor for adverse effects such as dizziness; nausea; syncope; insomnia; GI upset (associated with indirect-acting dopamine receptor agonists such as selegiline, amantadine, entacapone, and tolcapone); ataxia; depression (associated with direct-acting dopamine receptor agonists such as bromocriptine); palpitations; hypotension; urinary retention; and depression (associated with dopamine replacement drugs such as levodopa and carbidopa).
Patient considerations include providing individual and family support along with options for care of the family member with Parkinson’s disease. The disease is long-term and lifelong, as well as debilitating. A holistic approach in which all aspects of the patient and family are considered and respected is the key to quality nursing care.
1 note
·
View note
Text
Restless Legs Syndrome Treatment Market Will Grow At Highest Pace Owing To Rising Awareness And Diagnosis Of RLS Disorder

The restless legs syndrome treatment market has been witnessing significant growth owing to the rising prevalence of RLS disorder globally. Restless legs syndrome or Willis-Ekbom disease is a common sensorimotor disorder characterized by unpleasant sensations in the legs and an urge to move them to relieve those sensations. The symptoms of RLS usually occur late in the day resulting in difficulty in falling asleep. The mainstream treatment options for RLS include dopaminergic drugs such as pramipexole, ropinirole, and benzodiazepines. The increasing awareness about the symptoms and management of RLS disorder and improving diagnosis rates are the key factors propelling the demand for effective RLS treatment drugs and devices.
The Restless Legs Syndrome Treatment Market is estimated to be valued at US$ 2.5 Bn in 2024 and is expected to exhibit a CAGR of 5.7% over the forecast period 2024-2031.
Key Takeaways
Key players operating in the restless legs syndrome treatment market are GlaxoSmithKline, Teva Pharmaceuticals, Boehringer Ingelheim, Pfizer Inc., and UCB Pharma. GlaxoSmithKline accounted for the dominant market share in 2021 owing to its blockbuster drugs Mirapex and Requip being used for RLS treatment.
The key growing demand in the market can be attributed to the rising prevalence of RLS disorder mainly due to increasing risk factors like advanced age, chronic kidney disease, iron deficiency, and pregnancy. According to estimates, around 10% of adults are affected by RLS worldwide. This high prevalence of RLS and associated symptoms are driving more people to seek effective treatment options.
Technological advancements like the development of next-generation neuromodulation devices for deep brain stimulation therapy and wearable devices with built-in sensors to monitor symptoms are boosting the adoption of non-drug treatment choices for RLS. Innovation in drug delivery systems to achieve 24x7 symptom relief without major side effects is also fueling the growth of the restless legs syndrome treatment market.
Market Trends
Increased adoption of combination drug therapies - The trend of prescribing more than one RLS drug in combination is growing as it helps relieve symptoms better than monotherapy in severe cases. Dopamine agonists are often combined with alpha-2-delta ligands.
Rising popularity of neurostimulation therapies - Advancements in neurostimulation devices and techniques like spinal cord stimulation and transcutaneous electrical nerve stimulation are providingrelief to RLS patients with fewer side effects than drugs.
Focus on developing personalized treatment protocols - With more insights into disease underlying pathophysiology, treatment protocols are becoming tailored to individual patient needs based on symptom triggers, severity, and comorbidities to achieve optimal outcomes.
Market Opportunities
Development of oral extended-release formulations - There is scope for developing oral long-acting RLS medications that reduce dosing frequency and boost adherence to the prescribed treatment regimen.
Combination of drug and non-drug therapies - Integration of dopaminergic drugs with neuromodulation and physical therapy holds potential for synergistic effects in RLS management by targeting multiple disease aspects.
Impact Of Covid-19 On Restless Legs Syndrome Treatment Market Growth:
The COVID-19 pandemic has impacted the Restless Legs Syndrome Treatment market in several ways. During the initial lockdowns imposed by various governments globally, there was a disruption in manufacturing and supply chain activities. This led to delay in production as well as unavailability of key raw materials. However, as Restless Legs Syndrome is a chronic neurological condition, the demand for its treatment remained constant.
With the scare of infection, patients started preferring online consultation and home delivery of medicines over visiting hospitals and clinics for treatment. This boosted the telemedicine and e-pharmacy sectors. Pharmaceutical companies also shifted their focus to ensuring uninterrupted supply of drugs via online channels. However, priorities of healthcare systems changed drastically during the pandemic with more focus on COVID patients. Resources and funding were diverted for coronavirus treatment leading to delay in new drug development projects and clinical trials for Restless Legs Syndrome treatment.
As lockdowns are gradually lifting now, manufacturing and supply chains are getting back on track. The pharmaceutical industry is also focusing on expansion of their online presence and delivery networks to cater to the changed consumer behavior. Researchers are accelerating drug development processes to launch new and improved treatment options in the market. It is expected that with rising vaccination rates and adaptation to new normal, the Restless Legs Syndrome Treatment market will see steady growth over the forecast period.
Regions With Highest Consumption Of Restless Legs Syndrome Treatment:
North America accounts for the largest share of the Restless Legs Syndrome Treatment Market in terms of value. This is majorly attributed to the rising prevalence of the neurological condition in the region coupled with high diagnosis and treatment rates. According to estimates, around 12% of the adult population in the United States suffers from Restless Legs Syndrome. Availability of advanced healthcare infrastructure and favorable reimbursement policies further drive the market growth in North America.
Europe is also one of the key geographical regions concentratrating consumption of Restless Legs Syndrome drugs. Countries like Germany, United Kingdom, France have reported large patient pools undergoing medication therapy. Rising neurological disorders due to aging population and growing awareness aid the European market expansion.
Fastest Growing Region in Restless Legs Syndrome Treatment Market:
The Asia Pacific region is projected to witness the fastest growth in the Restless Legs Syndrome Treatment Market over the forecast period. This can be attributed to increasing healthcare expenditures of developing nations like India and China. Rapid economic development, rising living standards and growing medical tourism are improving access to diagnosis and treatment in the Asia Pacific region.
Moreover, key international players are expanding their presence in Asia Pacific by collaborating with local pharmaceutical manufacturers. evolving healthcare infrastructure and rising disease awareness campaigns by government organizations are further boosting the Restless Legs Syndrome patient pool. The growth momentum is expected to continue in the forthcoming years as well.
Get more insights on this topic: https://www.ukwebwire.com/restless-legs-syndrome-treatment-market-is-estimated-to-witness-high-growth-owing-to-advancements-in-novel-drug-development/
About Author:
Priya Pandey is a dynamic and passionate editor with over three years of expertise in content editing and proofreading. Holding a bachelor's degree in biotechnology, Priya has a knack for making the content engaging. Her diverse portfolio includes editing documents across different industries, including food and beverages, information and technology, healthcare, chemical and materials, etc. Priya's meticulous attention to detail and commitment to excellence make her an invaluable asset in the world of content creation and refinement. (LinkedIn - https://www.linkedin.com/in/priya-pandey-8417a8173/)
What Are The Key Data Covered In This Restless Legs Syndrome Treatment Market Report?
:- Market CAGR throughout the predicted period
:- Comprehensive information on the aspects that will drive the Restless Legs Syndrome Treatment Market's growth between 2024 and 2031.
:- Accurate calculation of the size of the Restless Legs Syndrome Treatment Market and its contribution to the market, with emphasis on the parent market
:- Realistic forecasts of future trends and changes in consumer behaviour
:- Restless Legs Syndrome Treatment Market Industry Growth in North America, APAC, Europe, South America, the Middle East, and Africa
:- A complete examination of the market's competitive landscape, as well as extensive information on vendors
:- Detailed examination of the factors that will impede the expansion of Restless Legs Syndrome Treatment Market vendors
FAQ’s
Q.1 What are the main factors influencing the Restless Legs Syndrome Treatment Market?
Q.2 Which companies are the major sources in this industry?
Q.3 What are the market’s opportunities, risks, and general structure?
Q.4 Which of the top Restless Legs Syndrome Treatment Market companies compare in terms of sales, revenue, and prices?
Q.5 Which businesses serve as the Restless Legs Syndrome Treatment Market’s distributors, traders, and dealers?
Q.6 How are market types and applications and deals, revenue, and value explored?
Q.7 What does a business area’s assessment of agreements, income, and value implicate?
*Note: 1. Source: Coherent Market Insights, Public sources, Desk research 2. We have leveraged AI tools to mine information and compile it
#Restless Legs Syndrome Treatment Market Trend#Restless Legs Syndrome Treatment Market Size#Restless Legs Syndrome Treatment Market Information#Restless Legs Syndrome Treatment Market Analysis#Restless Legs Syndrome Treatment Market Demand
0 notes
Text
ropinirole and bed i can't stomach being awake for another second
0 notes
Text
Self destructive wickedness arrested, convicted, and gaoled...
with kidnapping little boy
ordered to suffer
life sentence without parole. The deadly scourge of one obsessive/compulsive disorder
nearly left me starving to death.
Anorexia nervosa absent bulimia nadir of onset diagnoses schizoid personality disorder severe social anxiety still legion I aire behavior which agonizingly elicited slow suicide
courtesy self starvation
maelstrom within psyche of self as prepubescent lad
(particularly devastated immediate family members)
as emaciation pitted existential revulsion from unseen
wuthering heights betook courtesy yours truly
teased, hectored, and called “professor,”
when riding the school bus
nearly wrung death knell
annihilating fragile entity christened Matthew Scott Harris
with peremptory imprimatur yielding covalent bond to life
readily obvious to kith and kin
via zorro like signature per profound perilous depressive psychological state.
Now - at about
three decades plus six years from attaining rank of centenarian
perfect 20/20 hindsight
offers supreme advantage from swift current near drowning alluded earlier when das scribe juiced thwarted leapfrogging from pollywog tad metamorphosed
to witness puberty, whence devastating emotional crisis tripped, trilled,
and tricked aborted
natural healthy development
chronological denouement demise
jump/kick started
theorizing numerous educated guesses
within mind of
middle progeny and sole sol
(of the both late father and mother
Boyce and Harriet Harris) respectively
why he willfully hurtled his flesh at light speed
down the abyss toward death.
Literal and physical lightness of being
manifested within nooks and crannies
prior to full blown symptoms
to eliminate sustenance
drawing the curtain on brief residence
way before high noon of life.
Metamorphosis from boyhood
kindled burning man
found solace in attempting
to keep at bay of pigs hijacked
natural cycle, which seminal
transformation grieved me
to pine for nostalgic childhood’s end (albeit one fraught with romanticism)
vengefully interpreted attempt
to halt dead in the tracks intervention of mother,
whose nursing experience helped fend off passive attempt
to promulgate passive
silent plan to fruition.
She whipped various nutritious concoctions in the blender
to ensure minimal essentials to this, I readily admit) famished body
in conjunction with applying vital supplements into
one or the other skeletal
gluteus maximus
thru fuel injection,
which submissiveness to acquiesce, and bare bony buttocks
to receive iron injections
did absolutely nothing to squelch death wish.
I inexorably did buzzfeed
hashtagged eating disorder to go on a deadly hunger strike,
which essentially constituted declaration of independent control
despite horrendous craving for food jabbed innards like a pike
bifurcated psychic division
to live ousted coeval death wish goal
to seize yore reminiscent blissful, (albeit fictional) childhood over flooded self made damned dike
engaging, engendering, engineering
propensity to catapult yours truly into abysmal emotional hole
and way before the invention of Facebook, I mentally clicked like
to surrender mailer daemons all of me healthy development stole.
Imprimatur indelibly etched decades after bout with passive exit from life
crimp on psycho/social skills plus stunted physical growth cuts like a knife
affecting mental health with panic attacks and anxiety although existence
considerably less riddled qua debilitating symptoms
(such as vertigo, racing heart, profuse sweating, nausea, irritable bowels)
relying on the following prescription medications: BUSPIRONE HCL 15 MG TABLET
CLOMIPRAMINE 50 MG CAPSULE CLONAZEPAM 0.5 MG TABLET
FLUOXETINE HCL 40 MG CAPSULE
GLYCOPYRROLATE 2 MG TABLET
PRAZOSIN 1 MG CAPSULE PRAZOSIN 5 MG CAPSULE
RISPIRIDONE 1 MG TABLET
ROPINIROLE HCL 1 MG TABLET.
To add insult to injury yours truly also gifted
courtesy split uvula
but did little to ameliorate
the writer of these words
suffering brickbats as scape goat, whereby severe adenoidal vocalizations
allowed, enabled, and provided an easy target viz black barbs poised to strike, hurled,
and bullied me by peers.
Up until I entered six grade
(at Henry Kline elementary -
a one classroom per grade school)
classmates bullied, derided,
and feigned to hammer -
jabbing leering, nasty pimping ragout as a rule
which boyhood self of mine availed
a perfect bullseye target
with combination of diminutiveness,
being painfully quiet,
essentially remaining mum the entire day except when called upon
to answer question thence utterance emanating between lips
produced and emitted
a strong nasal sound to boot
grist for the mill
sans malice meted, mimicked, and mocked mashup
of mine warped congestion
ah, twas only by a fluke conversation,
whence speech pathologist
informed my parents about
The Lancaster cleft palate clinic,
where oral an examination
revealed minor birth defect
identified as a submucous cleft palate,
which explained the severe pinched twang
somewhat mitigated by wearing
a removable prosthetic
fastened with clasps to upper teeth
whereby a makeshift miniature
plastic protuberance closed the gap (at the expense of practically gagging me)
so air would be prevented
passing thru my button nose,
and thus gentle and soft as a shutterfly
shunted air out oral opening
though congenital defect disallowed
returning merchandise back to sender nor could blame be affixed
at either father nor mother
who both harbored the genetic mutation
now such admissions
re: aforementioned impediment allows,
enables and provides boasting rights if in a mood temper
any curiosity or satisfying a rumor whispered down the alley whence I said “ah”
left nagging nincompoops
as if pie hole filled with a gobstopper.
1 note
·
View note
Text
Understanding the Optimal Medication for Parkinson's Disease Tremors 1. Levodopa 2. Carbidopa-levodopa 3. Pramipexole 4. Ropinirole 5. Rotigotine Medication For Tremors From Parkinson's Parkinson's disease is a progressive neurological disorder that affects movement and coordination. One of the most common symptoms of Parkinson's disease is tremors, which can affect various parts of the body, including the hands, arms, legs, and head. Tremors can be distressing and can interfere with daily activities, such as writing, eating, and dressing. Fortunately, there are medications available that ... Read More. https://statesandcounties.com/2023/06/22/medication-for-tremors-from-parkinsons-best-medication-for-hand-tremors-from-parkinsons-disease/?feed_id=5315&_unique_id=649b23b7a79ad
0 notes
Link
#Ropinirole#Hydrochloride#Ropinirole Hydrochloride Market#Ropinirole Hydrochloride#Ropinirole Market#Hydrochloride Market
0 notes
Text
Dopamine Agonists in Parkinson’s Disease: Mechanisms and Therapeutic Use by Nik Shah
Parkinson's Disease (PD) is a progressive neurodegenerative disorder that affects millions of people worldwide. It is primarily characterized by the loss of dopamine-producing neurons in the substantia nigra, leading to motor symptoms such as tremors, rigidity, bradykinesia (slowness of movement), and postural instability. As dopamine plays a crucial role in regulating movement, mood, and cognitive functions, restoring dopamine levels or mimicking its effects is fundamental in the treatment of Parkinson's Disease. This is where dopamine agonists come into play, providing significant therapeutic benefit by activating dopamine receptors, thus alleviating symptoms and improving the quality of life for PD patients.
In this comprehensive guide, we will explore the mechanisms of action of dopamine agonists, their therapeutic use in Parkinson's Disease, and the intricate role dopamine plays in motivation, pleasure, and reward. Drawing insights from Nik Shah’s extensive work on dopamine and its therapeutic applications, such as his articles Dopamine: Unlocking Motivation, Pleasure, and Reward by Nik Shah and The Power of Dopamine Agonists Enhancing Neurotransmission for Cognitive Wellness by Nik Shah, we will understand how these medications enhance neurotransmission and improve cognitive wellness.
What Are Dopamine Agonists?
Dopamine agonists are pharmacological agents that activate dopamine receptors in the brain, mimicking the effects of dopamine. Unlike dopamine precursors (such as L-Dopa), which provide the brain with more of the raw material needed to synthesize dopamine, dopamine agonists directly stimulate dopamine receptors, bypassing the need for dopamine production. This makes them particularly useful in Parkinson’s Disease, where the brain's ability to produce dopamine is compromised.
In Mastering Dopamine Receptors: Harnessing DRD3, DRD4 and DRD5 for Optimal Brain Function and Behavior by Nik Shah, Nik Shah explains that the dopamine receptors, such as DRD1, DRD2, DRD3, DRD4, and DRD5, are distributed throughout various regions of the brain and body, each playing a crucial role in the regulation of motor function, cognition, and mood. Dopamine agonists target these specific receptors to provide therapeutic benefits in Parkinson’s Disease and other disorders.
Mechanisms of Action of Dopamine Agonists
Dopamine agonists function by stimulating dopamine receptors, specifically D2-like (DRD2, DRD3, and DRD4) and D1-like (DRD1 and DRD5) receptor subtypes. These receptors are part of the G-protein-coupled receptor family and mediate various intracellular signaling pathways. When dopamine agonists bind to these receptors, they initiate signal transduction pathways, which lead to physiological responses such as improved motor control, mood regulation, and cognitive function.
D2-like Receptors and Parkinson's Disease
D2-like receptors (including DRD2, DRD3, and DRD4) are primarily involved in motor control and reward. In Parkinson’s Disease, the loss of dopaminergic neurons impairs the activation of DRD2 receptors in the striatum, leading to motor dysfunction. Dopamine agonists, such as ropinirole and pramipexole, bind to these receptors to restore dopaminergic signaling, which improves movement and reduces symptoms like tremors and rigidity.
In Dopamine Receptor Antagonist: Dopaminergic Blockers by Nik Shah, Nik Shah elaborates on how dopamine receptor antagonists (dopaminergic blockers) can be used to modulate the effects of dopamine agonists. These antagonists are sometimes used to counteract the side effects of over-stimulation of dopamine receptors, such as dopamine dysregulation syndrome, which can result from long-term use of dopamine agonists.
D1-like Receptors and Cognitive Function
While D2-like receptors play a dominant role in movement, D1-like receptors (DRD1 and DRD5) are more involved in cognitive functions such as memory, learning, and attention. These receptors are abundant in the prefrontal cortex and the hippocampus, areas critical for higher-order cognitive processes. By stimulating DRD1 and DRD5 receptors, dopamine agonists like apomorphine can help improve cognitive performance and memory in patients with Parkinson's Disease, who often experience cognitive decline as the disease progresses.
In Mastering Dopamine Receptors: Unlocking the Power of DRD1 and DRD2 for Cognitive and Emotional Balance by Nik Shah, Nik Shah emphasizes the importance of dopamine receptor balance in regulating both motor and cognitive functions. While D2-like receptors help with movement, D1-like receptors are crucial for maintaining emotional balance and cognitive health.
Therapeutic Use of Dopamine Agonists in Parkinson's Disease
Parkinson's Disease is characterized by a dopamine deficit due to the death of dopaminergic neurons in the substantia nigra, leading to a reduction in dopamine levels in the striatum, which impairs movement and coordination. The clinical management of Parkinson's Disease aims to restore dopaminergic activity in the brain, and dopamine agonists have become a cornerstone of treatment.
Pramipexole and Ropinirole
Pramipexole and ropinirole are two commonly used dopamine agonists that target the D2 and D3 receptors, respectively. These drugs provide relief from the motor symptoms of Parkinson’s Disease, including tremors, rigidity, and bradykinesia. Both drugs are often used as first-line treatments for Parkinson's, either alone or in combination with L-Dopa (levodopa), which is another mainstay of Parkinson’s therapy.
In Mastering Dopamine Production, Supplementation & Availability by Nik Shah, Nik Shah delves deeper into the ways in which optimal dopamine synthesis and availability contribute to better clinical outcomes for patients with Parkinson’s Disease. By stimulating dopamine receptors directly, dopamine agonists like pramipexole and ropinirole can help maintain better dopamine levels in the brain and reduce the motor symptoms of the disease.
Apomorphine and Levodopa
In addition to pramipexole and ropinirole, apomorphine is another dopamine agonist used in Parkinson's Disease, especially for patients who experience motor fluctuations and are no longer responding well to L-Dopa therapy. Apomorphine acts as a rapid-acting dopamine agonist that provides fast relief from off periods, offering substantial benefits for patients with advanced Parkinson’s Disease.
However, L-Dopa remains the gold standard for Parkinson's Disease treatment. L-Dopa is converted to dopamine in the brain and helps restore dopaminergic signaling. Combining L-Dopa with dopamine agonists offers a synergistic effect, providing both immediate relief (via dopamine agonists) and long-term improvement in motor control (via L-Dopa).
Side Effects and Toxicological Implications
While dopamine agonists have proven effective in the management of Parkinson’s Disease, they come with potential side effects, particularly when used over an extended period. Nik Shah’s article Mastering Dopamine Reuptake Inhibitors (DRIs) by Nik Shah explores the risks associated with dopamine reuptake inhibitors and how dopamine dysregulation can occur with long-term use of dopamine agonists.
Common side effects include nausea, dizziness, hallucinations, impulse control disorders, and orthostatic hypotension. In some cases, dopamine agonists may cause dopamine-induced neurotoxicity, leading to a worsening of cognitive function or the development of compulsive behaviors such as gambling, shopping, or hypersexuality.
Conclusion
Dopamine agonists have become a cornerstone in the treatment of Parkinson’s Disease, providing critical therapeutic benefits in managing motor symptoms and improving quality of life. By directly stimulating dopamine receptors, dopamine agonists such as pramipexole, ropinirole, and apomorphine offer much-needed relief for patients with Parkinson’s Disease. However, understanding the mechanisms of action, pharmacokinetics, and side effects is crucial to optimizing the use of these drugs.
For more in-depth insights into dopamine agonists and their therapeutic potential, explore Nik Shah’s works, including Mastering L-Dopa and Tryptophan: Unlocking Dopamine and Serotonin Pathways for Mental Health and Performance by Nik Shah and Mastering Dopamine; MAO-B Inhibitors Selegiline and Rasagiline by Nik Shah.
Explore More on @nikshahxai
Personal Development & Education
Philosophy, Ethics & Society
Technology & Innovation
Life Sciences & Health
About the Authors
For more information about Nik Shah's digital presence, as well as insights from contributing authors such as Nanthaphon Yingyongsuk, Sean Shah, Gulab Mirchandani, Darshan Shah, Kranti Shah, John DeMinico, Rajeev Chabria, Francis Wesley, Sony Shah, Dilip Mirchandani, Rushil Shah, Nattanai Yingyongsuk, Subun Yingyongsuk, Theeraphat Yingyongsuk, and Saksid Yingyongsuk, click here to explore further.
References
Nik Shah 4533. (n.d.). Blogger
Nikshah01801. (n.d.). Tumblr 01801
#xai#nik shah#artificial intelligence#nikhil pankaj shah#nikhil shah#grok#claude#gemini#watson#chatgpt
0 notes
Text
Ropinirole Hydrochloride


Brand Name: Requip, Requip XL
Generic Available
Common Dosage Forms:
Tablets: 0.25 mg, 0.5 mg, 1 mg, 2 mg, 3 mg, 4 mg, 5 mg
Tablets, extended release (XL): 2 mg, 4 mg, 6 mg, 8 mg, 12 mg
FDA Indications/Dosages:
For the treatment of the signs and symptoms of idiopathic Parkinson’s disease: The recommended starting dose is 0.25 mg given three times a day. Weekly dosage increments of 0.25 mg per dose (three times daily) can be made up to a dose of 1 mg given three times a day. Further gradual tapering can be made up to a maximum of 24 mg/day. The normal dosage range is 0.5-5 mg three times a day. To discontinue, decrease dose frequency to twice a day for 4 days then once daily for three days then stopping. Patients may be switched to Requip XL from ropinirole by closely matching the total daily dose of ropinirole. Requip XL is to be given once a day.
For the treatment of moderate-to-severe primary restless legs syndrome (RLS): The recommended starting dose is 0.25 mg once daily, 1-3 hours before bedtime. The dosage can be increased to 0.5 mg daily after 2 days, and to 1 mg daily at the end of the first week. Weekly dosage increments can be made at 0.5 mg up to a maximum of 4 mg daily. No taper is necessary to discontinue dose in RLS therapy.
Pharmacology/Pharmacokinetics: Ropinirole is a non-ergoline dopamine agonist with full intrinsic activity at the D2 and D3 dopamine receptor subtypes. Its mechanism of action in Parkinson’s disease may be due to a stimulation of postsynaptic dopamine D(2)-type receptors within the caudate-putamen in the brain. The precise mechanism of action for RLS is unknown but may be related to primary dopaminergic system involvement. Ropinirole is rapidly absorbed after oral administration, reaching peak plasma levels in 1-2 hours. Metabolism occurs primarily via cytochrome P450 isoenzyme CYP1A2. Elimination half-life averages 6 hours. 40% is bound to plasma proteins.
Drug Interactions: Cigarette smoking decreases AUC by 38%. Omeprazole may decrease plasma levels. Ciprofloxacin increases AUC by 84%. Fluvoxamine, mexiletine, and estrogens may increase plasma levels. Dopamine antagonists (phenothiazine, butyrophenone, thioxanthene) may decrease the effectiveness of ropinirole.
Contraindications/Precautions: Patients have reported sudden initiation of sleep without warning. This has occurred during normal activities of daily living, including the operation of motor vehicles. Syncope, with or without bradycardia, has occurred during treatment, usually after an increase in dose. Postural hypotension, especially during dose escalation, may occur during treatment. Ropinirole inhibits prolactin secretion and potentially inhibit lactation. Pregnancy Category C.
Adverse Effects: The most common adverse effects include nausea (60%), dizziness (40%), somnolence (40%), syncope (12%), fatigue (11%), dyspepsia (10%), and viral infections (11%). Other adverse effects include general pain (8%), leg edema (7%), increased sweating, asthenia, abdominal pain, pharyngitis, abnormal vision (6%), confusion, hallucinations, hypertension, dry mouth, urinary tract infection (5%), rhinitis, sinusitis, anorexia, hyperesthesia (4%), flushing, malaise, flatulence, palpitation, amnesia, impotence, dyspnea, eye abnormality (3%).
Patient Consultation:
May be taken without regard to meals.
May cause dizziness or drowsiness. Use care when operating machinery or when mental alertness is required.
Orthostatic hypotension may occur; avoid rising rapidly from a lying or sitting position.
Patients should be informed of the possibility of experiencing hallucinations during therapy.
Avoid alcohol and other CNS depressants, including OTC products.
Patients should inform their physician if they plan to start or stop smoking cigarette smoking.
If being taken for Parkinson’s disease, do not stop therapy abruptly; treatment should be tapered over time.
Store in a cool, dry place away from sunlight and children.
Contact a physician if the above side effects are severe of persistent.
If a dose is missed, take it as soon as possible but to not double doses.
Do not divide, crush, or chew Requip XL tablets.
0 notes
Text
Medications

I cannot offer any medication recommendations or advice. Speak with your neurologist or PC. I am commenting on how one patient and caregiver’s lives are affected by medications.
When the diagnosis was new we were open to all the possibilities of medications. We didn’t know anything about Parkinson’s medications, only that his dopamine was low and going to get lower. At the first appointment the neurologist said she could make him feel much better. We both cried and she commented on how emotional we were. It had taken us a long time to get there and we were overwhelmed at the possibility of him being any better.
We had the prescriptions filled. Up until this point in our lives, we didn’t know anything about the healthcare system other than having two babies and a couple of minor incidents. We never took prescriptions and barely went to annual doctor appointments with no health insurance.
It took a few weeks for the meds to start becoming effective. They worked for a short while, reducing his tremors, making it a little easier for him to move, and then stopped working. He was prescribed a basic inexpensive, carbidopa/levodopa pill. His neurologist added additional meds to work with the carbidopa/levodopa he was taking. We cut pills and added extra doses to maximize the effects. He quickly got to the highest recommended doses. One in particular, amantadine, had side affects that were so bad, he decided to stop taking it after about six months. He had discussed it with the doctor and she warned him it could be challenging, getting off a dirty med can be really uncomfortable, but he was determined. His neurologist was out of town when he decided to stop taking it. He had a headache within a day and the second day couldn’t get out of bed and then slept for two days straight. On day five he was feeling much better.
Medications changed every few months for the first few years. Planning and dosing were, and still are, a big part of every day. With each neurologist visit, which was every three months, there would be new dosages or meds. Eventually none of the standard Parkinson’s meds were working any more. She prescribed a newer one, Rytary. It is a time-released capsule which was supposed to help with all the breakthroughs of symptoms he would get as each dose wore off. It is very expensive. We are lucky enough to be in a state with expanded Medicaid, and we also have a prescription insurance policy to reduce the price. Without state help it is about $900 a month, including using the prescription insurance. I am an advocate of Medicare for All and changing how big pharma operates. This medication allowed him to stop taking all the other meds except for the Ropinirole, which he still takes, and has never had to increase in dose. I sometimes wonder what happens if this one stops working.
In our household medications require on-going attention. My partner has fast progressing, medication resistant Parkinson’s Disease. Although initially we were able to manage his doses reading the bottle labels, it quickly had issues. Did the dose get taken or did he think he took it? Within a year, we started using a weekly medication minder. 7 little containers that stacked on top of one another with room for 4 doses a day. Then an alarm was added. He would turn off the alarm and forget to take the pills out of the minder. We needed something more reliable. Then we went to the carousel. It is programmable and can manage up to 8 doses a day.
I can’t imagine someone with this disease not having an advocate. I don’t think he would have been able to manage his meds on his own after the second year. With the carousel he was able to manage the dosing on his own most days for about two years. I recently started managing the doses. He had started missing them, leaving a pill in the carousel, or in the med cup, or setting the med cup down for a minute and forgetting to take it at all. Or completely forgetting to take the dose and then not being able to function, because he cannot function at all without medications.
My managing the meds has been a difficult transition, and also a relief to both of us. PD is a progressive disease and continually changing our lives. Admitting the progression by noticing what has become difficult, or even impossible, can be tough for both parties in the partnership. There is also kindness in it. The focus for us is on what is possible and that sometimes requires making changes. We are learning to practice non-judgement and creating ease. Change sometimes provides that. We keep our lives simple and structured as much as possible. The meds have been manageable for over two years, and with other changes there is improvement in some parts of his life. We are grateful for modern medicine and the privilege to have it available to us.
0 notes
Text
Unidentified extraterrestrial(s) willingly abducted me
As a divergence
from the apocalyptical, dialectical,
geomorphological, judgmatical,
metaphorical, philosophical...,
I share an out of this
(webbed wide) world,
light hearted anecdote
ye may find far fetched.
Believe me you,
an unspecified number of years ago, yours truly availed himself
as an experimental subject,
and since then subsequently
no longer fears dark shadows
shimmering within outer limits
of the twilight zone.
Specific details elude me, thus only a general sketch can be provided
Upon falling into a deep slumber after taking a respite
from my daily constitutional within vicinity of Ardmore, Pennsylvania
countless decades ago,
the following subconscious
somnambulant scenario arose
allowing, enabling, and providing
temporary alleviation
from a harried styled
and swiftly tailored married state.
Out of a tendency to be impetuous,
and oblivious to danger,
I voluntarily let myself
get abducted by this gamesome
handsome, and venturesome green eyed
Geico looking alien ghoul.
Any resemblance between
the following piecemeal description
being kidnapped by an alien
(from another condemn nation
in the cosmos), and living persons then lamenting married life
purely coincidental.
Although pitch-black
that hot summer July night 20xx,
an ominous ghastly shape
lumbered near the skeletal
partially built addition
at Lower Merion High School.
This phantasmagorical amorphous,
diaphanous, illustrious... entity
hovered outside his/her
phosphorescent flying saucer.
I stood stock still as my warm breath
bestirred, dispersed, fractured thick fog (actually smoke from Canadian wildfires) creating, generating, loosing,
rousing and yawning miniature clouds
that formed a gauzy window.
Thru this opaque grounded soundcloud
ether movements detected.
Eight tentacles (similar
to Octopus teacher viewed
courtesy NetFlix)
shredded this faux misty shroud
and quickly, yet gently grabbed me.
I found myself on-board
a battle gray extra-terrestrial object.
Fate delivered me out of desperation
into the "hands" of what appeared
as the most surreal setting
created by ingenious
computer graphics technicians.
Nanny boo boo
uttered the creature
from black abyss.
Since what sounded
like outer space gibberish
as a second language
not an elective when I attended
Methacton High School,
(nor colleges for that matter),
an automatic reflex took over.
I offered a gap toothed
(i.e. Alfred E. Neuman trademark -
what me worry) wry smile foreigners (vaguely resembling
grateful dead foo fighters
didn't get MAD at me.
An immediate interest
arose from these outliers
at the ultra thin metallic post
sticking atop me noggin.
Robotic, galactic and electronic signals
broadcast and received
courtesy said antenna.
Nevertheless, a crazy idea occurred.
Maybe these foreigners
from another galaxy
could secure long overdue
permanent implanted teeth
(in place of these ill fitting dentures)
without charging an arm or leg.
Ha!
Non-verbal communication
resorted to as a necessary expedient
to establish comprehension
and self preservation!
Additionally, the notion
to avoid any action interpreted
as hostile best be applied
even at the expense
of being whisked away
(no matter mine very fantasy
far out and groovy whim)
countless light-years from
1148 Greentree Lane,
Narberth, Pennsylvania.
Psychiatric medications:
BUSPIRONE TAB 15MG,
CLOMIPRAMINE CAP 50MG,
CLONAZEPAM TAB 0.5MG,
FLUOXETINE CAP 40MG,
(GLYCOPYRROLATE, TAB 2MG,
PRAZOSIN HCL CAP 5MG,
PRAZOSIN HCL CAP 1MG,
RISPERIDONE TAB 1MG,
ROPINIROLE HCL 0.5MG
prescribed by Doctor David Lee Wrought)
most definitely eased anxiety
per dread locked terror
that loomed large
within my quite active imagination.
I willingly made clear
(using all manner of gesticulations)
to surrender myself,
which idea triggered
a flickering googly eyed excitement.
Wow!
This bizarre situation
could offer golden opportunity
to escape the tragedies
of terrestrial existence,
and perhaps get linkedin
with another weird
organic life form
ideally non human
or not otherwise specified.
Once this electric like surge
coursed thru each fiber,
I brazenly approached
the other-worldly specimens
guarding their shimmering craft,
which appeared to hover
just barely above the perimeter
slated to be another
state of the art wing of this campus.
I hemmed and hawed
with tentative steps
before nonchalantly
scaling the hydraulically propelled ladder.
At once, an immediate
whoosh took place.
After these myopic eyes
adjusted to the scene,
I observed an identical
earth like landscape and heard
what sounded
like the most melodious chimes.
Actually, that globe happened
to be dear third rock from the sun
as viewed from the nearest window.
Upon setting foot into the structure,
an automatic accelerator activated
before the spaceship
jettisoned and sped away
Mötley Crüe at warp speed.
Within my mind, I thought
what to do to pass the time???
Instantaneous sans any desire
promulgated that very wish.
Ah!
Perchance, these ethereal creatures
(large, medium and small)
conveyed messages telepathically?
I put this hypothesis
to a rudimentary
electric kool aid acid test.
Within my mind,
I silently uttered Matthew Scott Harris.
An instant reply came back - in my head.
Every one of these
wraith-like cosmic nomads
understood whims wirelessly,
albeit telepathically
thus believing yours truly
(me self) to breathe easy
said species reduced signals
to digital bits
and/or hallowed weaned bytes.
Upon waking up, I realized
the aforementioned a dream
to be continued…
in another millennium or so.
0 notes