#neuro-endocrine
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Text
Can Sleep Disturbance effect your fertility?

View On WordPress
#AMH#bloganuary#dailyprompt#Fertility#hormones#infertility#iui#IVF#neuro-endocrine#Ovarian stimulation#pcos#pregnancy#sleep#sleep disturbance
0 notes
Text

do u see my vision? chief resident felassan and attending solas
#solas#felassan#maybe mythal was like the CMO or on the board or something#listen im sticking them in different jobs and no one can stop me#iron bull is either a DPT or an ortho surgeon#dorian does radiology or maybe patho#varric does endocrine or cardio or maybe IM#leliana is obgyn/FAACOG who scares all the other surgeons#idk wtf cole would do honestly. maybe psych#josephine is trying to get them all to play nice w their block time#cassandra is probably like. trauma or IM.#Vivienne is either derm or surgical oncology or possibly also neuro surg#sera could be sports med or EM#blackwall is impersonating an MD
237 notes
·
View notes
Text
I had an electrophysiology appointment today. My doctor finally got around to doing some research on my antidepressant/ADHD medication and said of my tachycardia, "yeah, it's just that," which I've been saying for a whole year now. It changes nothing really because I'm not going to stop taking the medication.
Anyway, I don't have POTs. I just have side effects.
#I'm also willing to bet that I don't have a rare neuro-endocrine tumor either#It's just Straterra doing normal Straterra things and my doctors are panicking about it
0 notes
Text
YH24-28. Karin Sauren, on Down Syndrome Health
Your Health is Your Choice with Sara Troy and her guest Karin Sauren-Bakkers, on air from July 9th When our son Wesley was born with Down Syndrome, we were quickly informed about all the possible health challenges he could face. In my journey I have been searching for natural ways to optimize his health and wellness and not take the health issues for granted as being part of Down Syndrome. I…
#“The Gift of Down.”#cognitive development of children with Down Syndrom#Down Syndrome Health#Karin Sauren-Bakkers on Down Syndrome#Nutrients#Orchard of Wisdom#Psych0-Neuro-Endocrine-Immunology#Sara Troy#www.selfdiscoverywisdom.com
0 notes
Text
I realized other people might be in school for biology, human anatomy, nursing/medical... I made for all of my lectures gojo reading them. Sooooo. Here is one of them. Neuro disorders. I have gi, endocrine, cardiac disorders for med/surg. Electrolyte imbalances and a bunch of other stuff. Like 10+ hours of listening. But I figured who knows, some other college or high school students out there might like them.
If anyone is interested, I will do a dump file for them all.
#gojo satoru#gojo saturo#jjk gojo#jujutsu gojo#gojo#jjk satoru#jujutsu satoru#gojo fanart#jjk#jjk fanart#gojo jjk#satoru gojo#educational#college
21 notes
·
View notes
Text
An interesting perspective article about Long Covid
Should we be fighting gene damage instead of individual symptoms?
The pathogenesis of long COVID (LC) still presents many areas of uncertainty. This leads to difficulties in finding an effective specific therapy. We hypothesize that the key to LC pathogenesis lies in the presence of chronic functional damage to the main anti-inflammatory mechanisms of our body: the three reflexes mediated by the vagus nerve, the hypothalamic-pituitary-adrenal (HPA) hormonal axis, and the mitochondrial redox status. We will illustrate that this neuro-endocrine-metabolic axis is closely interconnected and how the SARS-CoV-2 can damage it at all stages through direct, immune-inflammatory, epigenetic damage mechanisms, as well as through the reactivation of neurotropic viruses. According to our theory, the direct mitochondrial damage carried out by the virus, which replicates within these organelles, and the cellular oxidative imbalance, cannot be countered in patients who develop LC. This is because their anti-inflammatory mechanisms are inconsistent due to reduced vagal tone and direct damage to the endocrine glands of the HPA axis. We will illustrate how acetylcholine (ACh) and cortisol, with its cytoplasmatic and cellular receptors respectively, are fundamental players in the LC process. Both Ach and cortisol play multifaceted and synergistic roles in reducing inflammation. They achieve this by modulating the activity of innate and cell-mediated immunity, attenuating endothelial and platelet activation, and modulating mitochondrial function, which is crucial for cellular energy production and anti-inflammatory mechanisms. In our opinion, it is essential to study the sensitivity of the glucocorticoids receptor in people who develop LC and whether SARS-CoV-2 can cause long-term epigenetic variations in its expression and function.
#mask up#public health#wear a mask#pandemic#wear a respirator#covid#still coviding#covid 19#coronavirus#sars cov 2#long covid
32 notes
·
View notes
Text
It really annoys me that a lot of people somehow seem to think that psychological issues somehow have a reason that is not based in the neurological and/or endocrinal biology of our bodies.
Like, seriously, people, what do you think else this is based in? Some immaterial soul?
Obviously everything we experiences somehow reflects on our physical body and everything inside. In thousands of years of humans trying to proof a soul of some sort.
No matter what it is: PTSD, depression, anxiety, whatever... it is happening in your neuro-endocrinical systems. We do often not yet fully understand what exactly happened because neurological research is not yet that old. It is kinda hard (and also expensive) to do studies on the living brain. We can do MRI, and electromeasurements, but it is hard.
But in the end psychology are just the observable effects of biological processes.
4 notes
·
View notes
Text
It is so frustrating having appointments not come in. I saw neuro 2 years ago, he said he'd see me again after 3 months. I saw cardio in February, he said he'd see me again in 3 months (and my GP won't start my POTS medication because my endocrine team haven't even responded to whether I can take the medication they want me on (fludrocortisone) - like, surely they can at least try and communicate with each other. One email. So now I'm going to have to ring endocrine nurses (I do feel like I need another synacthen test anyway) and find out whether I can take fludro, and then either try and get my GP to start based on that OR chase up cardio. Why is having ill health a full time job?
#chronic illness#fibromyalgia#chronic pain#polyarteritis nodosa#adrenal insufficiency#stills disease#fibro#pots#postural orthostatic tachycardia syndrome#fludrocortisone#pots syndrome#endocrine#neurology
7 notes
·
View notes
Text

QUICKDROP YOUR BNHA SONA WHILE BLAZE ISNT LOOKINGC!!!!! Dating Shinso because imsuch a loser 4 shinso and in a qpr with Mina and Kirishima :3
QUIRK: NEURO-TRANSMISSION
She can manipulate neuro-transmitters by touch- whether in neurons, controlling the nervous system, or in cell membranes, controlling the endocrine system :3 with drawbacks ofc!
His. Hero name is Neuro because she asked for suggestions nd Mina went "well it's gotta be neuro related right? So maybe-" and Rose [not fucking listening] went "Oh Neuro ? OK that's my hero Name Now . Thank yoy Mina 👍"
HWHBHE I JUST REALISED HE CAN MAKE HER OWN HRT?? Lmao Shinso goes to Rose's dorm every sunday night for his weekly T-shot
#malik's art#oc: Rose bnha#I PROBS WONT DRAW THIS ONE AS MUCH BECAUSE IM NOT HYPERFIXATED ON BNHA BUT . :[ I MISS BNHA#bnha oc#bnha sona#bnha self insert#bnha original character#bnha#oc x canon#bnha oc x canon
17 notes
·
View notes
Note
Studying medicine is so fucking cool btw, do you have any idea what particular field you’d want to enter yet? Like Paediatrics, Gastro etc etc, or are you just waiting for what takes your interest later on?
Favourite and least favourite thing to study atm?
~ a nosey swanon who can’t do uni but would really love to do smth medical in another universe 🦢
I don't mind being a general practitioner like family medicine or smth, but otherwise I think something along the lines of psychiatry, otherwise something in neuro or maybe medical law or ethics.
My favourite thing is usually neuro and psych and my least favourite is probably immune system and endocrine just because of how abstract it is like seriously I've never seen an antibody with my eyes so how do I even know those are real. They could be made up
5 notes
·
View notes
Text

Hidden deep within your brain the pineal gland is regulating daily and seasonal rhythms in response to sunlight. Unfortunately, accumulating neurotoxicity, inflammation, and calcification, is silently crushing this critical gland.
Pineal Purpose
The pineal-body is a pea-size pinecone-shaped endocrine gland weighing just 0.1g and floating in its own pool of cerebrospinal fluid, above the roof of your mouth. It contains photoreceptive cells that switch on, and off, hormone and neurotransmitter production on or off in response to sunlight.
Seeds, greens, avocados, and burro bananas - make sure you fuel pineal production. Dr. Sebi taught us that “Real Soul food is food that enhances the Soul, our central Sun, our carbon. Fruits, vegetables, grains, this is REAL food.”
Master Conductor
The pineal gland controls other endocrine glands, interlinking the brain with the body via hormones and neurotransmitters. Acting like a biological-clock, the pineal gland coordinates our interaction with the sun:
Rhythms: sleep and wake cycles, seasonal responses.
Reproduction: fertility levels and sex hormone production.
Regulation: growth, body temperature, and blood pressure.
Immune: activation, tumor suppression, cell rejuvenation.
Neurotoxins and Calcification
Toxins cause inflammation, reduce mental efficiency, and deregulate hormone production. Sleep disorders, depression, and neurodegeneration (e.g. Alzheimer’s) are all associated with calcification of the pineal gland.
Deposits of chalky calcium restrict the gland, reduce its size, and impede the production of neuro-endocrine substances. The pattern of pineal calcification is similar to teeth-enamel, and fluoridation (water and toothpaste) is linked to the destruction of this enigmatic gland.
Detoxification, Relaxation, and Nutrition
Chronic inflammation causes calcification. Reducing exposure to inflammatory neurotoxins begins to restore the correct mineral balance, and decalcify the pineal gland:
Fluoride: highest concentration in the body found in calcified tissue in the pineal gland.
Chlorine: public water is bleached with chlorine, associated with neurological birth defects.
Aluminum: leaches from pots, pans, and foil, associated with plaques seen in Alzheimer’s.
Sugar & chemical sweeteners: over-stimulate and damage neurons, reduce dopamine.
MSG & derivatives: confusingly labeled, many processed foods include this neurotoxin.
Endotoxins: bad bacteria in the gut produce toxins that inflame the gut and brain.
Stress: prolonged fear is toxic, causes the amygdala to shrink, and emotional fatigue.
The next step is supporting the brain to clear the waste and rejuvenate:
Sleep: at night the brain is ‘washed’ clean, detoxified, and replenished with nutrients.
Hydration: to bathe the brain and pineal gland you need to keep fluids flowing.
Meditation: like exercise for the brain, rewires, and strengthens your emotional health.
Berries (except cranberry): reduce free radical damage and nourish with flavonoids.
Coconut oil: alternative fuel for the brain which produces less oxidative damage.
Apples, seeded grapes & prunes: are high in boron which naturally displaces fluoride.
Tamarind: increases fluoride output in urine, helps retain zinc and magnesium. Fresh organic tamarind pulp or paste is easily mixed with water into a sweet and sour flavored drink, add a little agave if the taste is too lip-puckering!
•Dr. Sebi
14 notes
·
View notes
Text
Excerpt from this story from Grist:
Demand for steel is on the rise globally, driven by population growth and the expanding economies in developing nations. The material will also be important to the green energy transition, forming the backbone of infrastructure like wind turbines, solar panels, and hydroelectric dams. Every part of the steel supply chain is heavily polluting, and the places in the U.S. where the steel industry is concentrated are disproportionately low-income and nonwhite, highlighting yet another instance in which the promises of development and climate solutions come at a steeper cost for some communities. What’s more, the country’s steel production is dominated by just two companies: U.S. Steel and Cleveland Cliffs.
For both companies, much of their production begins with taconite, a low-grade iron ore mined in the northeast Minnesota’s Mesabi Iron Range, which is processed into pellets that get shipped to the steel mills of Gary, Indiana. The extraction of the ore from taconite rock releases a slew of toxic pollutants into the air, including mercury, lead, and dioxins. In this region, the most concerning of these emissions is mercury.
Studies have connected mercury to a litany of negative health effects. It’s a neurotoxin that can interfere with brain development in unborn children and an endocrine disruptor that can weaken the immune system. Scientists have yet to determine a quantity of mercury that is safe for human consumption. One recent study found that there is “no evidence” for a threshold “below which neuro-developmental effects do not occur.” And while the taconite industry releases less than a ton of mercury into the atmosphere every year, the metal is toxic in extremely small quantities: A fraction of a teaspoon can contaminate a 20-acre lake.
The nation’s six taconite plants, all in this region of Minnesota, are owned by U.S. Steel and Cleveland Cliffs. In May 2023, the Environmental Protection Agency proposed a regulation that would require the companies to cut their mercury emissions by around 30 percent. In order to meet that standard, the companies would have to install equipment that would inject carbon atoms into their industrial chimneys so that the carbon would attach itself to the mercury atoms, making the pollution particles bigger and allowing them to get trapped in a filter before they would be released into the atmosphere. The agency estimates that its regulation would cost the industry $106 million in capital costs and $68 million per year thereafter.
Last month, when the standards were finalized, both companies sued. They argue that the regulation would pose “irreparable harm” to the industry, because of the steep costs of implementation. They also argue that the EPA’s proposed method for reducing mercury pollution would actually be worse for public health, causing a 13 percent increase in the amount of the toxic metal deposited in the local environment.
Jim Pew, a lawyer at Earthjustice who has litigated multiple lawsuits against the EPA for its failure to curb pollution from the taconite industry, pointed out that the costs of implementing the required equipment would be a tiny fraction of the companies’ annual sales, which totaled $40 billion in 2023. Pew noted that U.S. Steel recently initiated a $500 million stock buyback program, the mark of a healthy income revenue stream. As for the companies’ claim that the technology would increase mercury pollution, Pew called it “meritless.” The companies are “relying on a premise they know to be false” — that taconite plants would add the carbon technology without also improving their filtration system.
“I find this reprehensible and shameful,” Pew said. “While it’s claiming that it can’t spend money to clean up historic pollution, U.S. Steel is just handing out money to its shareholders.”
2 notes
·
View notes
Text
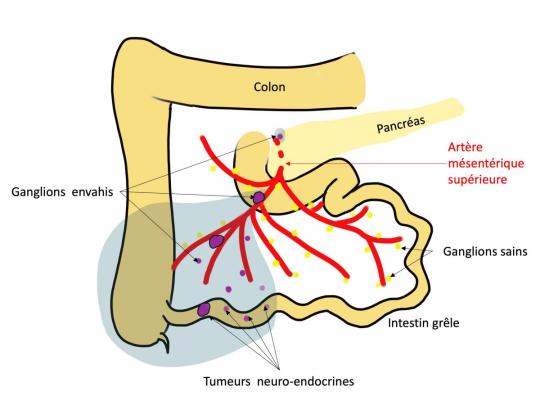

QU’EST CE QU’UNE SCINTIGRAPHIE À L’OCTREOSCAN ?
_
Cet examen est réalisé pour diagnostiquer certaines tumeurs neuro-endocrines bien différenciées et de préciser leur extension.
Elles sont situées le plus souvent au niveau du tube digestif ou du pancréas et sécrètent des hormones spécifiques.
___________________________________________________
Comment prendre OCTREOSCAN :
_
Posologie
Adulte et population âgée
Pour la tomoscintigraphie monophotonique (TEMP), l'activité à injecter dépend de l'équipement dont on dispose. En général pour un adulte de 70 kg, une activité de 110 à 220 MBq administrée en une seule injection intraveineuse est suffisante. D'autres activités peuvent être injectées si justifié.
3 notes
·
View notes
Text
DATABASE ENTRY EMOTIONAL CALIBRATION CHIP (ECC-CHIP) classification class-7 neuro-programmatic construct origin iro corporate congress (defunct) application implantation in ECC (emotionally calibrated construct) infants
OVERVIEW
the ECC was a neurotechnological implant used to erase volition, enforce behavioral compliance, and synchronize emotional response across the ECC program's artificial lifeform units. installed during infancy, the chip was designed to transform engineered humanoids into obedient, networked entities capable of high-risk combat, social infiltration, or occupation support with zero independent cognition.
it was a linchpin in the iro corporate congress's forced-labor genocide campaign during the laile genocide.
STRUCTURE
programmable matter base
the ECC utilizes programmable matter fused with synthetic neural mesh to rewrite organic synaptic architecture.
enables full-body override. can inhibit or stimulate motor function at will.
adjusts genetic expression to favor rapid healing, enhanced muscular response, and endurance in M4-class (gravity differential x4) environments.
emotional calibration algorithm (ECA)
the central AI stack within the chip continuously monitors endocrine and limbic activity.
emotions are not suppressed but redirected toward productive ends (e.g., fear → loyalty, pain → mission compliance).
includes an automated information-data capture (AIDC) protocol to monitor social interaction and propagate learned responses through the network.
analysis & compliance phases
each unit undergoes daily emotion-logic recalibration, known as compliance phase cycling (CPC), ensuring no deviation from operational tolerances.
behavior is flagged, stored, and in some cases remotely corrected via fleet-ops command nodes.
PHASES OF FUNCTIONALITY
the ECC chip architecture functioned in tandem with five standardized operational states. infancy (nullphase) Full override, nonverbal, subcortical function only. no memory retention.
childhood (syncphase) language and cognitive development directed entirely by ECC-net. training protocols embedded.
adolescence (stabiphase) initiation of independent response modeling. emotional range narrowed to mission-relevant output.
combat (burnphase) full reactive sync with the ECC-net and commanders. high aggression, minimal self-preservation impulse.
dormancy (gridphase) units placed in burn grids. stasis chambers which both physically house ECCs and update collective codebases through data osmosis.
NETWORK INTERFACING
ECC chips were networked across subphase-syncpoints, forming a real-time cognitive net dubbed the ECC-net or Burn Grid. these links permitted:
instantaneous behavior cloning between nodes
remote task directives and memory override
emotional resonance syncing, often used to suppress outlier trauma
post-liberation, former ECCs report intense dissociative trauma stemming from stored echoes of others' pain and actions.
NOTABLE COMMANDS (pre-liberation)
ANALYSIS[CMD] overwrites voluntary behavior with highest priority code FREEZE[STASIS] locks unit in full-body stasis for preservation CALM[DRONE] floods pleasure centers to enforce dissociation or pacify rage KILL[VAR1-5] custom-tier threat termination protocols REPLICATE[DATA] installs recent experience into network peers SHUTDOWN[GLOBAL] emergency chip failsafe; lethal if overused
LIBERATION HISTORY
kaewesi-899 (neal kaewesi) experienced a chip grounding fault at age 20, severing him from the ECC-net and granting free will.
with assistance from starfleet and access to progenitor code on kaewesi-7, neal reprogrammed the recursive loop sustaining the ECC-net and unified all liberated units under a consensual, free-will-based network: the Kin.
CURRENT FEDERATION POSITION
all ECC technology is banned under articles 2 and 5 of the federation artificial sentience accord and the shi'kahr convention. the Kin Consensus is officially recognized as a sovereign emergent species and holds protected status.
0 notes
Text
Psycho-neuro-endocrine Transformation - Were I "Crazy" as a Teenager?
Adolescence is not just a phase—it is a profound transformation, a physiological and psychological metamorphosis that bridges the dependent innocence of childhood and the complex autonomy of adulthood. Yet, within this transitional period lies a curious paradox: while the body rapidly grows under the influence of potent hormones, the brain, particularly the frontal lobe, matures at a staggered…

View On WordPress
#consciousness#Health#healthy lifestyle#humanperceptions#Intellectual#philosophy#response of body#science#scientificevidence#Well being
0 notes
Text
Preoperative Note Completed example Advanced Health Assessment/Nurse Anesthetist (Mount Marty University) Scan to open on Studocu Studocu is not sponsored or endorsed by any college or university Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 ANESTHESIA PRE-OPERATIVE EVALUATION NOTE Name: John Doe DOB: 4/1/1977 (44) Anesthesia Start Time/Date: 0700 Date: 07/06/2021 Surgeon: Dr. Smith Procedure: bilateral posterior foot ulcer debridement Diagnosis: bilateral diabetic foot ulcers RELAVENT PROBLEMS Previous Surgeries: right inguinal hernia repair (2007); wisdom tooth extraction (1996) Previous Anesthesia: monitored anesthesia care (MAC); local anesthetics Medications: Metformin 500mg bid; Lisinopril 5mg once daily Allergies: no known food or drug allergies REVIEW OF SYSTEMS Cardiovascular: denies chest or pleuritic pain, not lightheaded or dizzy, no palpitations, no peripheral edema Heme/ID: no bleeding or bruising tendencies, denies fatigue, night sweats, low-grade fevers Respiratory: not short of breath, no wheezing, no cough HEENT: no vision changes, no blurred vision, no changes to hearing or recent infections, no throat or dental pain Endocrine: denies heat or cold intolerance, no dysphagia, polydipsia, or polyuria, numbness and tingling present to bilateral feet Neuro/Psych: no headaches, no seizure history, denies depression or anxiety, denies drug or alcohol abuse Renal/GU: no difficulty urinating, no frequency, burning, or hesitancy, negative for increased or decreased amounts of urine, no nocturia or incontinence Musculoskeletal: denies swollen, stiff, or red joints, no arthritis or joint pain, negative for myalgias GI/Hepatic: no abdominal pain or discomfort, no jaundice, no change in bowel habits Other: redness and open wounds to the bottoms of feet, swelling and drainage Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 OBJECTIVE Wt: 220 lb Ht: 5’8” BMI: Relevant Labs: A1c 8.5% Pre-op Tests: EKG completed in clinic UPT: N/A FBS: 189 mg/dL at 0600 ANESTHESIA PHYSICAL EXAM Airway Assessment: Mallampati: Class II TM distance: adequate (>6.5cm) HM distance: adequate MO: adequate (>4cm) Neck ROM: full ROM NPO status: NPO for solids since 2330 7/5/21; sip of water with lisinopril at 0400 7/6/21 Cardiovascular: rate and rhythm regular, S1/S2, no murmurs, clicks, gallops, or rubs, capillary refill less than 3 seconds Respiratory: lung sounds clear in all fields, no wheezing, rales, rhonchi, or stridor, breathing effortless, symmetric air entry Musculoskeletal: full ROM ankle joints, dorsi/plantar flexion present Neuro/Psych: AOx3, mood and affect appropriate, speech clear, gait steady Dental: partial upper denture; no other missing, loose, or chipped teeth ANESTHESIA PLAN 1. Allergies, medications, labs reviewed a. ASA III b. RSI not anticipated 2. Anesthesia Consent 3. Additional labs, pre-op meds, tests ordered a. CBC and CMP ordered 4. Pre-op interview, assessment, notes complete 5. Type of anesthesia ordered a. Will plan for MAC with local b. Will plan for general anesthesia as needed Anesthesia options, benefits, and risks, including awareness under anesthesia in high-risk patients, the likelihood of success, and any problems related to recovery have been discussed with the patient. They have agreed to proceed. Possible Differentials with Rationale: Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 E11.621 – Type 2 diabetes mellitus with foot ulcer A skin ulcer is “a localized injury to the skin and or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear” (Vowden & Vowden, 2015, p. 62). This is a broad term that encompasses mechanical injuries but also underlying disease processes. A diabetic ulcer is typically full-thickness, occurs at or below the ankle, and often has an unspecified healing duration. Due to the diabetes illness, ulcers are particularly susceptible to infection, gangrene, and necrosis, which places the limb at risk for amputation (Vowden & Vowden, 2015). John Doe has partial-thickness wounds to both feet. Since Mr. Doe has not been to any provider since he was a child, a random blood glucose was checked in the clinic. It was 189 mg/dL. An A1c also revealed 8.5%, suggesting uncontrolled diabetes. He was placed on Metformin 500mg to be taken twice daily. Mr. Doe does admit to numbness and tingling and often a burning sensation to his feet and sometimes his hands, which would suggest neuropathy. Given the symptoms, the lab analysis, and non-painful ulcers to his bilateral posterior plantar aspects of his feet, a diagnosis of diabetic foot ulcers is most likely. L03.90 – Cellulitis, unspecified of feet Cellulitis is a bacterial infection of the dermis and subcutaneous tissue and can occur due to a wound or ulcer. The most common infectious agents include Staphylococcus, group B streptococci, and CA-MRSA (McCance, Huether, Brashers, & Rote, 2014). The skin is painful to touch, erythematous, warm, and has poorly defined margins. Cellulitis is most often unilateral, but there have been unusual case reports of bilateral limb cellulitis. Other symptoms may include tachycardia, malaise, and fever (Fenstermacher & Hudson, 2016). Mr. Doe had developed edema and fever, which are pertinent positives for this illness. There are four classes of cellulitis. Class I has no signs of toxicity and there are no co-morbidities, which can be managed with oral antibiotics. In class II, the patient is either well or not well, but has at least one co-morbidity that could complicate the illness (i.e. diabetes), and this can be treated with IV antibiotics at home. Class III entails a very ill person with constitutional symptoms, unstable co-morbidities, and a possible threaten to limb, in which hospitalization with IV antibiotics is necessary. Then, class IV presents as Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 sepsis and necrotizing fasciitis (Opoku, 2015). John Doe’s feet are developing edema and erythema. The wounds are also dirty. He could be developing cellulitis, but it is difficult to discern at this point. His feet are not warm to the touch but he has since developed the constitutional symptom of fever. Although this is not a solid diagnosis as compared to diabetic foot ulcers, cellulitis remains a possible differential. L88 – Pyoderma gangrenosum Pyoderma gangrenosum is a rare neutrophilic skin disorder that causes necrotizing ulcerations, most commonly as a solitary lesion on a lower extremity. Most patients with pyoderma gangrenosum have a comorbid autoimmune illness such as Crohn’s disease or rheumatoid arthritis (Quist & Kraas, 2016). A lesion typically starts out as a small red bump and quickly develops into an open wound within days. Diagnosis is made by skin biopsy and treatment consists of corticosteroids, immunoglobulins, daily moist-to-dry dressing changes, and pain management. Skin grafts are sometimes needed, depending on the severity (Quist & Kraas, 2016). Mr. Doe does have wounds to both of his feet that are open and edematous, but the process differed greatly from that of pyoderma gangrenosum. His wounds did not develop quickly but rather over a longer period of time. Mr. Doe does not have any known autoimmune illnesses that would put him at risk for pyoderma, therefore ruling out the diagnosis at this time. Evaluation and Reflection: write 1-2 paragraphs with your thoughts on this patient References Fenstermacher, K. & Hudson, B.T. (2016). Practice guidelines for family nurse practitioners (4th ed.). Elsevier. McCance, K.L., Huether, S.E., Brashers, V.L., & Rote, N.S. (2014). Pathophysiology: The biologic basis for disease in adults and children (7th ed.). Elsevier. Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 Opoku, F. (2015). Ten top tips: Improving the diagnosis of cellulitis in the lower limb. Wounds International, 6(1), 4-8. Quist, S.R. & Kraas, L. (2016). Treatment options for pyoderma gangrenosum. Journal of the German Society of Dermatology, 15(1), 34-40. https://www.doi.org/10.1111/ddg.13173 Vowden, P. & Vowden, K. (2015). Diabetic foot ulcer or pressure ulcer? That is the question. Diabetic Foot Journal, 18(2), 62-66. Downloaded by James Mcknight ([email protected]) lOMoARcPSD|28323056 Read the full article
0 notes