#mevalonic acid
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Text

The Science Research Diaries of S. Sunkavally, p 649.
#iodine#proteins#casein#thyroid hormone#glyptodon#D-mevalonic acid#adsorption#air-water interface#cystic fibrosis#transfer RNA#soubility of mRNA#phosphorus pentoxide#pelargonic acid#paramagnetism#manuscripts#caligraphy#handwriting#satyendra sunkavally#theoretical biology#diaries
0 notes
Text
Cholesterol: Sources, Structure and Biosynthesis.
Elevate your online experience with our latest notes on topic, Cholesterol: Sources, Structure and Biosynthesis on our website https://microscopiaiwm.wordpress.com/ . "Unlocking knowledge one post at a time! follow microscopiaiwm #microscopiaiwm
Introduction Cholesterol is an extremely important sterol in the tissues of animals. It is an organic molecule and a type of lipid. It is a fat-like substance, which is waxy in texture, and found in all the cells of our body, as it is essential for carrying out many functions such as synthesis of hormones, synthesis of vitamin D and also acts as an integral structural component of the membranes…
View On WordPress
#3-epoxide#aceto-acetyl CoA#biochemistry notes#biosynthesis of cholesterol#biosynthesis of isoprenoid units#biosynthesis of lanosterol#biosynthesis of melanovate#biosynthesis of squalene#cholesterol#Cholesterol formation#cholesterol notes#fatty acid#firmation of lanosterol#HMG-CoA#isoprenoid#lanosterol#lanosterol cyclase#metabolism#metabolism notes#mevalonate#mevalonic acid#MicroScopia IWM#oxidosqualene#sources of cholesterol#squalene#squalene-2#statin#steroid hormones#sterol#sterols in animals
1 note
·
View note
Text
Diagnosis of HIDS
Diagnosing HIDS involves a combination of clinical evaluation, laboratory tests, and genetic analysis. Key diagnostic steps include:
Clinical Evaluation: A thorough medical history and physical examination to assess the pattern and characteristics of fever episodes, as well as other symptoms such as rash, abdominal pain, and lymphadenopathy.
Laboratory Tests:
Elevated IgD Levels: Measurement of immunoglobulin D (IgD) levels in the blood. Elevated IgD levels are a hallmark of HIDS, although they may not be elevated in all patients, particularly infants.
Urinary Mevalonic Acid: Elevated levels of mevalonic acid in the urine during fever episodes can support the diagnosis of HIDS.
Inflammatory Markers: Elevated levels of acute-phase reactants such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) during attacks.
Genetic Testing: Confirmatory diagnosis through genetic testing to identify mutations in the MVK gene. This test can definitively diagnose HIDS and distinguish it from other periodic fever syndromes.
Get a diagnosis at the best rheumatology clinic FirstChoice Rheumatology
0 notes
Text
Causes and Genetic Basis of HIDS
HIDS is caused by mutations in the MVK gene, located on chromosome 12. This gene encodes the enzyme mevalonate kinase, which is essential for the production of cholesterol and other important molecules. Mutations in the MVK gene lead to reduced enzyme activity and the accumulation of mevalonic acid and other intermediates, triggering inflammatory pathways.
HIDS follows an autosomal recessive inheritance pattern, meaning that an affected individual inherits two mutated copies of the MVK gene, one from each parent. Carriers, who have one normal and one mutated copy of the gene, typically do not show symptoms but can pass the mutation to their offspring.
Visit FirstChoice Rheumatology for more
1 note
·
View note
Text
Current Trends and Future Demand of Mevalonic Acid Market Top Business Growing Strategies, Technological Innovation and Emerging Trends of Outlook To 2024

The research study, titled “Global Mevalonic Acid market Research Report 2019,” evaluates the historical performance and the current status of this market for a detailed understanding, emphasizing especially on the dynamics of the demand and supply of Mevalonic Acid in 2024. This report presents a detailed study of the global market for Mevalonic Acid by evaluating the growth drivers, restraining factors, and opportunities at length. The examination of the prominent trends, driving forces, and the challenges assist the market participants and stakeholders to understand the issues they will have to face while operating in the worldwide market for Mevalonic Acid in the long run. Request for Sample Report Here @ https://www.acquiremarketresearch.com/sample-request/10353/ The research study further offers a study of the existing status of the key regional markets for Mevalonic Acid , namely, China, North America, Eastern Europe, Western Europe, Japan, the Middle East and Africa, and the Rest of Asia, on the basis of a number of significant Mevalonic Acid market parameters, such as, the production volume, pricing of the product, production capacity, sales, demand and supply dynamics, revenue, and the rate of growth of this Mevalonic Acid market in each of the regions. Several segments of the worldwide Mevalonic Acid market have also been discussed in this research report with thorough information, considering their historical and existing performance in the global arena. It further maps the competitive landscape of this Mevalonic Acid market by evaluating the company profiles of the leading market players, such as Sigma-Aldrich, Carbosynth Product, TLC Pharmaceutical, Rinner Group, Tocris Bioscience On the basis of the product, the market has been classified into: L-Mevalonic Acid, Others Based on the application, the market has been categorized into: Drugs, Chemical Production, Others For More Information On This Report, Please Visit @ https://www.acquiremarketresearch.com/industry-reports/mevalonic-acid-market/10353/ The report covers the market study and projection of "Mevalonic Acid Market" on a territorial along with worldwide point . The report establishes subjective and quantitative valuation by industry examiners, direct information, help from industry specialists alongside their latest verbatim and every industry producers through the market value chain. The examination specialists have also evaluated the by and large sales and income creation of this specific market. Moreover, this report additionally conveys broad examination of basic market drift, many key essentials while overseeing macro-economic indicators, combined with market enhancements according to each section. The growth trajectory of each of the segments has been provided in this study, in global terms and in each of the regional markets, creating a descriptive analysis of the overall Mevalonic Acid market. This research study has also discussed the current and the upcoming ventures in the worldwide market for Mevalonic Acid at length, making it of special value for companies, consultants, and other stakeholders functioning in this Mevalonic Acid market.
0 notes
Text
THE MYTHS ABOUT CHOLESTEROL
Mostly this day, everything you hear about cholesterol is bad, everybody wants to get rid of every beat of cholesterol in their body, Cholesterol is the most demonized, misunderstood and controversial substance in both our bodies and our diets. Most of us think and also seems logical that eating cholesterol would raise blood cholesterol level and possibly lead to heart diseases and many health problems.
FACTS ABOUT CHOLESTEROL
Most of the cholesterol in our body is not coming from the diet, our diet contributes a very small amount of cholesterol when our dietary intake of cholesterol goes down, our cells make more cholesterol if our dietary intake of cholesterol goes up, our cells make less cholesterol. Because of such mechanism, dietary cholesterol has very little effect on blood cholesterol levels. The bottom line is that a low cholesterol diet have very little or any effect in controlling our blood cholesterol level
WHAT IS THE FUNCTION OF CHOLESTEROL IN OUR BODY?
Cholesterol is the most abundant steroid in human tissue, it is important for cell membranes, bile acid synthesis, steroid hormone (glucocorticoids, mineralocorticoids, androgens, estrogens, progestogens) and synthesis of vitamin D
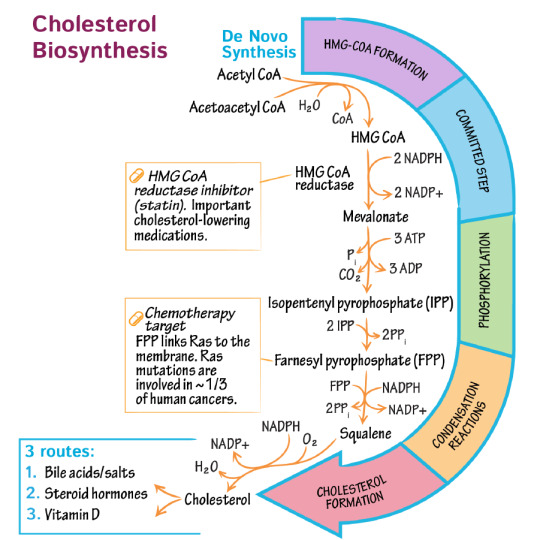
CHOLESTEROL SYNTHESIS
Cholesterol synthesis takes place in the liver using a molecule called Acetyl CoA. Acetyl CoA participates in many biochemical reactions in protein, carbohydrate and lipid metabolism. Three Acetyl CoA condensed to form HMG CoA, HMG CoA reductase converts HMG CoA to mevalonate, this is the rate-limiting step in cholesterol synthesis. The common statin drugs such as atorvastatin, lovastatin and pravastatin act on this rate-limiting step of cholesterol synthesis by inhibiting the HMG CoA reductase enzyme and prevent the new cholesterol synthesis, some research also show these drugs can increase the good cholesterol level called HDL
VLDL, LDL, HDL
VLDL(very low-density lipoprotein)
; VLDL is assembled in hepatocyte(liver cell) transport triglyceride containing fatty acids newly synthesized from excess glucose to adipose tissue(fat cells) and muscle.
LDL(low-density lipoprotein)
is the so-called bad cholesterol, primarily cholesterol particle, most cholesterol measured in our blood associated with LDL. The function of LDL is to deliver cholesterol to tissue for biosynthesis. When the cell needs to make membrane, bile acid and salt or dividing cholesterol is required and many other cells needs cholesterol to make steroid hormone.
HDL(high-density lipoprotein)
; is the so-called good cholesterol. HDL synthesized in the liver and in the intestine and released as a dense protein-rich particle into the blood, used for cholesterol recovery from a fatty streak in the blood vessel and give this cholesterol to VLDL, chylomicron, hepatocyte(liver cell) and steroidogenic tissue
WHEN DOES CHOLESTEROL BECOME A HEALTH RISK?Although cholesterol is one of the major contributors to heart disease, it isn’t the only one. High blood pressure, a family history of heart disease, and diabetes are other factors that could contribute to cardiovascular disease.
When we have excess cholesterol, our body does not have the mechanism of getting rid of it, because it is an essential nutrient, under normal circumstances, our body does not get rid of cholesterol, it stores it in the liver, about 70% of LDL is taken up by the liver by a process called receptor-mediated endocytosis. The problem is that some people have a defect in LDL receptor gene, and they have a high level of circulating LDL particle in the blood, example Familial Hypercholesterolemia, regardless of whether they are thin or fat, their cholesterol level is very high, most people think if you are overweight, your cholesterol level is high, but that is not always the case, most of these problems are genetics. There are other genetics defects that cause hypercholesterolemia such as Familial defective apolipoprotein B-100, PCSK9 gene mutations, familial combined hyperlipidemia to mention a few, but I just want to mention one severe form of hypercholesterolemia called Familial hypercholesterolemia type 2A, it is an autosomal dominant disorder that means you get it from the parents and it is a high risk of atherosclerosis and coronary artery diseases, unfortunately, these patients life expectancy is <20
1 note
·
View note
Text
Global Mevalonic Acid Market 2017 - Sigma-Aldrich, Carbosynth Product, TLC Pharmaceutical, Rinner Group, Tocris Bioscience
Global Mevalonic Acid Market 2017 – Sigma-Aldrich, Carbosynth Product, TLC Pharmaceutical, Rinner Group, Tocris Bioscience
The worldwide Mevalonic Acid Market report launched by Market.biz focuses on a complete and accurate study of Mevalonic Acid industry. Global Mevalonic Acid Market 2017 report is fundamentally concentrated on current scenario of Mevalonic Acid market. This comprehensive research document will improve the efficiency of the Mevalonic Acid market during the forecast period from 2017 to 2022.
The…
View On WordPress
0 notes
Text
Organic Extra Virgin Oil by Olvdew as the Best oil for reducing cholesterol
Around 80 percent of Indians have cholesterol issues and, naturally, high cholesterol-related flare-ups are an unwelcome health risk. If you don't manage it properly, you may be affected by a variety of other health issues, including stress and high BP as well as heart problems, obesity, hypertension, as well as hypothyroidism. Read this article and you will know the Best oil for reducing cholesterol by olvdew.
Making the right adjustments is crucial!
It is crucial to make significant adjustments and reversals in order to treat the problem (including eating a balanced lifestyle and participating in vigorous physical exercise) However, research has discovered that olive oils could help lower cholesterol levels without causing any adverse negative effects typically associated with the use of cholesterol medications.
Organic extra virgin Oilve oil by Olvdew is there to help. It is the Best oil for reducing cholesterol.
Aromatherapy has benefits that aid in healing and protecting the body by nature. One of these remedies is located in the Organic extra virgin olive oil of Olvdew. It is commonly used as an ingredient to enhance food items, Organic extra virgin oil brought into use , may also assist in managing cholesterol levels in a safe method. The reason for this is in the chemical composition of the leaves!
According to scientific research Organic extra virgin oil is rich in Terpenoid compounds like citral and geraniol, which lower cholesterol levels. These compounds hinder mevalonic acid's production which is an intermediary in the process of making cholesterol, and is the focus of many cholesterol-lowering medications.
Helps to prevent inflammation
Organic extra virgin also helps to alleviate certain of the negative adverse effects of the high levels of cholesterol. A study that was conducted in 2010 revealed that the regular consumption of Organic extra virgin extract or oil increases the creation of antioxidants within the body that prevent attacks and helps combat inflammation which is among the main causes of weight gain. It also helps to reduce the levels of lipids within your body, helping to combat the issue at the source. These benefits together with a healthy lifestyle , will assist in repairing the damage caused by the rise in cholesterol.
How do you use it?
It is vital to keep in mind that extra virgin olive oils must not be consumed internally unless they've been dispersed. You can also drink the Organic extra virgin extract by drinking tea made of Organic extra virgin or by boiling the leaves with hot water. The oil is safe to use for internal use and also topically.
It is also possible to use Organic extra virgin oilve oil by inhaling one or two drops(or when combined with a safe carrier oil) each day.
Other useful remedies
While clinical studies are in progress, researchers have discovered that some of the natural oils and compounds such as clove oil and lavender oil can help ease certain symptoms caused by cholesterol and manage this condition in a more effective method, if taken frequently.
0 notes
Text
organic - atorvastatin
What is atorvastatin?
Atorvastatin is in a class of medications known as hepatic hydroxymethyl-glutaryl coenzyme A (HMG-CoA), or more simply known as statins. It is used to prevent cardiovascular disease in high-risk individuals and to treat abnormal lipid levels. Atorvastatin is a synthetic oral medication that is used to decrease the number of fatty substances, low-density lipoprotein (LDL - known as “bad” cholesterol), and triglycerides while raising good cholesterol in the blood.

The science behind it
Atorvastatin’s molecular formula is C33H35FN2O5. It has a molar mass of 558.64 g/mol, a boiling point of 722ºC at 760mmHg, a melting point of 176ºC and has very low solubility in water. Atorvastatin’s compound consists of an aromatic amide, containing a pentasubstituted pyrrole (pyrrole is a heterocyclic aromatic organic compound) that’s formed by two contrasting moieties (the part of a molecule that’s given a name because it’s also identified in other molecules). It has a 3,5-dihydroxpentanoyl side chain as well, which is identical to its parent compound. Atorvastatin is also a dihydroxy monocarboxylic acid. It contains all sorts of functional groups such as alcohols, amides, carboxylic acids, and halides. There is also the presence of benzene rings in this compound.

When taken, atorvastatin helps to lower LDL-cholesterol levels by inhibiting HMG-CoA reductase, an enzyme that catalyzes the chemical reduction of a certain substance. An enzyme is a biological catalyst that speeds up chemical reactions in systems. This enzyme is needed for the liver to produce cholesterol, but since HMG-CoA is blocked, it is unable to convert to mevalonate, a key component of cholesterol synthesis. This, therefore, lowers the production of the molecule.

Atorvastatin synthesis
Effects on society and human health
When there is a build-up of cholesterol and fats on the walls of your arteries, they can decrease blood flow throughout your body. This happens because oxygen is transported through your bloodstream. The build-up prevents the transportation from being perfect and causes a decrease in the oxygen supply to your organs, which can have detrimental effects.
Atorvastatin is prescribed as the first line of defence to decrease the amount of cholesterol produced by the body. It is also used to help prevent heart disease, chest pain, strokes, and heart attacks. Statins and atorvastatin have a large impact on society because of this, improving not only the quality of life but the life expectancy as well for the individuals affected/at risk for these complications. This medication includes some common side effects such as muscle pain, tenderness, weakness, lack of energy, fever, nausea, extreme tiredness and weakness. Despite this, atorvastatin is used all over North America because of the evidence supporting the long-term and short-term benefits with limited side effects.

Effects on the environment
Atorvastatin is known to be an environmental contaminant and a xenobiotic (a foreign compound to a living organism). Atorvastatin will exist in its anion form in the environment and does not adsorb strongly to soils with organic carbon. Terrestrial contamination of atorvastatin has moderate mobility in soil, but it’s not expected to volatilize from dry soil surfaces. Aquatic contamination of atorvastatin adsorbs to suspended solids and sediments and has a potential for bioconcentration in aquatic organisms. In the atmosphere, atorvastatin only exists in its particulate phase in the ambient atmosphere, but this can be removed from the air with wet and dry deposition.
0 notes
Text
demand for plant-derived
https://www.mdpi.com/1422-0067/19/1/263/htm
In this review, the most recent and successful cases of secondary metabolites, including alkaloid, diterpene, triterpene and polyphenolic type compounds, with great anticancer potential are discussed. Focusing on the ones that are in clinical trial development or already used in anticancer therapy, therefore successful cases such as paclitaxel and homoharringtonine (in clinical use), curcumin and ingenol mebutate (in clinical trials) will be addressed
Additionally, a simple classification includes three main groups:
1. terpenoids (polymeric isoprene derivatives and biosynthesized from acetate via the mevalonic acid pathway),
2. phenolics (biosynthesized from shikimate pathways, containing one or more hydroxylated aromatic rings) and the
3. extremely diverse alkaloids (non-protein nitrogen-containing compounds, biosynthesized from amino acids such as tyrosine, with a long history in medication) [24,25].
Several new cytotoxic secondary metabolites are isolated from plants each year and constitute a source of new possibilities to explore in order to fight against cancerous diseases.
0 notes
Text
Simvastatin


Brand Name: Zocor
Generic Available
Common Dosage Forms:
Tablets: 5 mg, 10 mg, 20 mg, 40 mg, 80 mg
FDA Indications/Dosages:
As an adjunct to diet for the reduction of elevated total and LDL cholesterol, apo-B, and triglyceride levels and to increase HDL cholesterol in patients with primary hypercholesterolemia and mixed dyslipidemia (Fredrickson Types IIa and IIb), treatment of hypertriglyceridemia (Type IV), and treatment of primary dysbetalipoproteinemia (Type III): Begin therapy after a 3–6-week cholesterol-lowering diet. Start with 5-10 mg once daily in the evening. Adjust dose at intervals of at least 4 weeks to a maximum of 40 mg/day. Usual dose is 10-40 mg/day.
To lower total and LDL cholesterol in patients with homozygous familial hypercholesterolemia: 40 mg/day in two to three divided doses.
As an adjunct to diet to reduce total-C, LDL-C, and apo-B levels in boys and girls (at least one year post-menarche), 10-17 years of age, with heterozygous familial hypercholesterolemia if after an adequate trial of diet therapy LDL-C remains ≥190 mg/dL or ≥160 mg/dL AND there is a positive family history of premature cardiovascular disease or two or more CVD risk factors are present: Start with 10 mg/day in the evening and titrate to a maximum of 40 mg/day in 4 week intervals.
*The 80 mg tablets should be reserved for patients without adverse effects who have been maintained on this dose for more than 1 year.
Monitor: LFT, Lipid panel
Pharmacology/Pharmacokinetics: After oral ingestion, simvastatin is hydrolyzed to its b-hydroxy acid form, becoming a specific inhibitor of HMG-CoA reductase. This enzyme is responsible for the conversion of HMG-CoA to mevalonate, an early rate limiting step in the synthesis of cholesterol. In therapeutic concentrations, HMG-CoA reductase is not completely blocked, allowing biologically necessary amounts of mevalonate to be produced. Simvastatin reduces both normal and elevated LDL (low-density lipoprotein) concentrations. It moderately reduces triglyceride and VLDL (very low-density lipoprotein) concentrations. It is not known whether its therapeutic is due to an increased LDL catabolism, a decrease in VLDL (a precursor to LDL), or a direct decrease in LDL production. In addition to LDL reduction, simvastatin increases HDL (high-density lipoprotein) concentrations. High LDL and low HDL levels have been shown to be risk factors in coronary heart disease. Simvastatin is a substrate for CYP3A4.
Drug Interactions: Simvastatin may increase warfarin or digoxin levels. Coadministration of simvastatin with potent CYP3A4 INHIBITORS (gemfibrozil, nicotinic acid, danazol, immunosuppressive agents, itraconazole, ketoconazole, erythromycin, clarithromycin, telithromycin, HIV protease inhibitors, nefazodone, and grapefruit juice) is contraindicated. Do not exceed 10 mg daily when used with verapamil or diltiazem. Do not exceed 20 mg daily with used with amiodarone, amlodipine, or ranolazine.
Contraindications/Precautions: Contraindicated in patients hypersensitive to any component, during pregnancy or lactation, in patients with active liver disease or unexplained persistent elevations of serum transaminases, and in patients taking strong CYP3A4 inhibitors, gemfibrozil, cyclosporine, or danazol. Use with caution in patients with any amount of liver dysfunction and in patients who consume large amounts of alcohol. It is recommended that liver function tests be performed every 4-6 weeks during the first 15 months of therapy and periodically thereafter. Increases in serum transaminases of more than 3 times the normal levels should warrant discontinuation. If serum transaminases do not decrease upon discontinuation, a liver biopsy should be considered. May cause optic nerve degeneration. May cause myopathy or rhabdomyolysis. Pregnancy Category X.
Adverse Effects: Constipation (2.3%), MUSCLE PAIN (rare), and dyspepsia (1.1%).
Patient Consultation:
Contact a physician if symptoms of myopathy occur (e.g., muscle pain or tenderness, especially if accompanied by malaise or fever).
Closely follow prescribed diet.
Avoid overexposure to sunlight due to possibility of photosensitivity. Use a sunscreen and wear appropriate clothing until the level of sensitivity is determined.
Do not become pregnant during therapy. If pregnancy occurs or is suspected, discontinue medication and consult a physician.
Limit alcohol intake during therapy.
Store in a cool, dry place away from sunlight and children.
If a dose is missed, take it as soon as possible. If taken within 12 hours of the next dose, skip the next dose and continue with schedule.
Grapefruit juice increases plasma levels and should be avoided.
0 notes
Text
Isoprene Rubber Market to Discern Steadfast Expansion During 2025
Isoprene Rubber Market: Snapshot
The unique perceived benefits of isoprene rubbers, a form of synthetic rubber, are their resistance to abrasion and fractures. On account of having similar chemical and physical properties as that of a natural rubber, isoprene finds applications as tires, automotive mounts, shock absorbers, adhesives, healthcare items, sporting goods, and coatings among others.
Isoprene rubbers are enjoying soaring demand on account of a flourishing automotive industry which fuel isoprene rubber market growth. Rising awareness about the use of isoprene rubber gloves for various purposes, particularly in surgeries and other healthcare processes, is also proving beneficial for its demand.
Get Brochure of the Report @ https://www.tmrresearch.com/sample/sample?flag=B&rep_id=149
With a huge thrust on research and development, more applications of isoprene rubber is expected to emerge in the near future. One such result of research and development is bio-isoprene that can be formulated from low cost sugars gotten from biomass, and provide a green preliminary material for products such as styrene block copolymers, for its use as adhesive and other applications. Many such innovative product categories is slated to bode well for the isoprene rubbers market in the near future. Already, renowned automakers in the world are pledging uptake for such eco-efficient products.
Asia Pacific, powered by particularly by China, is the primary driver of the global isoprene rubber market. This is because of the explosive growth in the automotive industry in the region. North America and Europe are important contributors to the isoprene rubber market as well due to the growing awareness of hygiene among people that has led to the significant uptake of isoprene rubber in the healthcare sector.
Isoprene Rubber Market: General Outline
Isoprene or 2-methyl-1, 3 butadiene, is a colorless liquid and volatile in nature. It is soluble in organic solvents such as alcohol and water due to its low vapor pressure and reactive nature. Isoprene rubber are highly resistant to abrasion and fractures. Isoprene has electro insulating resistance, and is an organic compound that is emitted by various plants and trees. Some of the producers of isoprene are: poplars, oaks, eucalyptus, and legumes among others. About half of the yearly production of isoprene emissions comes from tropical broadleaf trees and the remaining from shrubs. Isoprene is denoted by a chemical formula CH2=C(CH3)CH=CH2. Isoprene is produced in the chloroplasts of plants through the MEP pathway that is also known as non-mevalonate pathway. Isoprene emissions are known to change dramatically with temperature and maximize at around 40 degree Celsius. This has led to the belief that isoprene protects plants from heat stress. Industrial production of isoprene was done primarily by isolation through thermal decomposition of natural rubber. It is readily available as a side product in manufacturing ethylene and as a by-product of thermal cracking of oil or naphtha.
Isoprene Rubber Market: Trends and Prospects
Isoprene is known as a structural motif in most of the biological systems. The isoprenoids such as tetraterpenes and carotenes are derived from isoprene. Other substances and compounds derived from isoprene include retinol, phytol, dolichols, tocopherols, and squalene among others.
To get Incredible Discounts on this Premium Report, Click Here @ https://www.tmrresearch.com/sample/sample?flag=D&rep_id=149
As isoprene rubber has similar physical and chemical properties as that of a natural rubber, isoprene is used in host of applications. It does not contain fatty acids, proteins and other substances that are present in natural rubber. The various applications of isoprene include tires, shock absorbers, automotive mounts, adhesives, sporting goods, healthcare items, and coatings among others.
Growing market demand for isoprene from the automotive industry is the major factor driving the global isoprene rubber market. In addition, growing awareness has given rise to usage of gloves for various purposes. Therefore, the increasing demand for isoprene from the medical and healthcare sector is also expected to boost demand for isoprene in the near future. One of the drivers in developing bio-based isoprene is its capability to utilize low cost sugars derived from biomass, and provide a green preliminary material for products such as styrene block copolymers, for its use as adhesive and other applications.
With rising research and development activities along with innovations, the wide range of applications in the end user industries are expected to provide opportunities for the growth of the global isoprene market. The potential for bio-isoprene is also expected to boost opportunities for isoprene in the isoprene rubber market.
Isoprene Rubber Market: Key Segments
North America, Asia Pacific, Europe, and Rest of the World (RoW) are the major segments for the global isoprene rubber market. Asia Pacific, especially China is expected to boost the market demand for isoprene due to the growing automotive industry in the region. North America and Europe are also expected to fuel demand for isoprene owing to the growing hygiene awareness among people. This hygiene awareness has led to a rise in demand for isoprene from the healthcare sector, thereby driving the growth of the isoprene rubber market.
Isoprene Rubber Market: Key Market players
The key players of the isoprene rubber market are: JSR, Kaixin, Lanzhou Xinlan, Nizhnekamskneftekhim, Sinopec, Togliattikauchuk, Yikesi, Zhenjiang Xintian, Goodyear, Jinhai Deqi, Kuraray, Lyondellbasell, Shell, Synthez-Kauchuk, Formosa Plastics, Kraton Polymers, LCY, YUHUANG, ZEON and Zibo Luhua Hongjin, SINOPEC, Versalis(Polimeri Europa), TSRC, and ZEON among others.
Request TOC of the Report @https://www.tmrresearch.com/sample/sample?flag=T&rep_id=149
About TMR Research:
TMR Research is a premier provider of customized market research and consulting services to business entities keen on succeeding in today’s supercharged economic climate. Armed with an experienced, dedicated, and dynamic team of analysts, we are redefining the way our clients’ conduct business by providing them with authoritative and trusted research studies in tune with the latest methodologies and market trends.
Contact:
TMR Research,
3739 Balboa St # 1097,
San Francisco, CA 94121
United States
Tel: +1-415-520-1050
0 notes
Text
Thuốc Ezensimva 10/10 tác dụng, liều dùng, giá bao nhiêu? | Tracuuthuoctay
TraCuuThuocTay.com chia sẻ: Thuốc Ezensimva 10/10 điều trị bệnh gì?. Ezensimva 10/10 công dụng, tác dụng phụ, liều lượng.
BÌNH LUẬN cuối bài để biết: Thuốc Ezensimva 10/10 giá bao nhiêu? mua ở đâu? Tp HCM, Hà Nội, Cần Thơ, Bình Dương, Đồng Nai, Đà Nẵng. Vui lòng tham khảo các chi tiết dưới đây.
Ezensimva 10/10
Tác giả: Ths.Dược sĩ Phạm Liên Tham vấn y khoa nhóm biên tập. ngày cập nhật: 9/8/2019

Nhóm thuốc: Thuốc tim mạch
Dạng bào chế:Viên nén
Thành phần:
Ezetimib 10 mg; Simvastatin 10 mg
SĐK:VD-32780-19
Nhà sản xuất: Chi nhánh công ty cổ phần dược phẩm Agimexpharm – Nhà máy sản xuất dược phẩm Agimexpharm – VIỆT NAM Nhà đăng ký: Công ty cổ phần dược phẩm Agimexpharm Nhà phân phối:
Chỉ định:
Chỉ định
Tăng cholesterol máu nguyên phát, thuốc được chỉ định như điều trị bổ sung cùng chế độ ăn kiêng để giảm hiện tượng tăng cholesterol toàn phần (C-toàn phần), cholesterol lipoprotein tỉ trọng thấp (LDL-C), apolipoprotein B (Apo B), triglyceride (TG), và cholesterol lipoprotein tỉ trọng không cao (không-HDL-C), và để tăng cholesterol lipoprotein tỉ trọng cao (HDL-C) ở bệnh nhân có tăng cholesterol máu nguyên phát (dị hợp tử có tính chất gia đình và không có tính chất gia đình) hoặc tăng lipid máu hỗn hợp.
Tăng cholesterol máu đồng hợp tử gia đình (HoFH)Vytorin được chỉ định để giảm sự tăng cao của cholesterol toàn phần và LDL-C trên bệnh nhân người lớn có HoFH. Vytorin nên sử dụng bổ trợ cho các phương pháp điều trị giảm lipid máu khác (như lọc bỏ LDL) ở những bệnh nhân này hoặc nếu những điều trị này không có sẵn.
Dược lực
(ezetimibe/simvastatin) là một thuốc giảm lipid máu có tác dụng ức chế chọn lọc sự hấp thu cholesterol và các sterol thực vật liên quan tại ruột và ức chế sự tổng hợp cholesterol nội sinh.
Cholesterol huyết tương được tạo thành từ hấp thu từ ruột và tổng hợp nội sinh. Vytorin chứa ezetimibe và simvastatin, hai thành phần giảm lipid với cơ chế tác dụng bổ sung. Vytorin làm giảm cholesterol toàn phần, LDL-C, Apo B, TG và không-HDL-C, và làm tăng HDL-C thông qua ức chế kép sự hấp thu và tổng hợp cholesterol.
• Ezetimibe
Ezetimibe ức chế hấp thu cholesterol từ ruột. Ezetimibe có tác dụng khi dùng đường uống và có cơ chế tác dụng khác với những thuốc giảm cholesterol của các nhóm khác (như các statin, các thuốc ức chế tiết acid mật [resin], các dẫn xuất acid fibric, và các stanol có nguồn gốc thực vật), chịu trách nhiệm hấp thu cholesterol và phytosterol từ ruột.
• SimvastatinSau khi uống, simvastatin, là một lactone không hoạt tính, bị thủy phân trong gan thành β-hydroxyacid dạng hoạt động tương ứng, có tác động mạnh đến sự ức chế men khử HMG-CoA (men 3 hydroxy-3 methylglutaryl CoA reductase). Men này xúc tác chuyển đổi HMG-CoA thành mevalonate, là bước đầu và là bước giới hạn tốc độ trong quá trình sinh tổng hợp cholesterol.
Simvastatin được chứng minh là làm giảm nồng độ LDL-C cả ở mức bình thường và khi tăng cao. LDL-C được hình thành từ protein trọng lượng phân tử rất thấp (VLDL) và được dị hóa chủ yếu bởi thụ thể LDL ái lực cao. Cơ chế giảm LDL của simvastatin có thể do giảm nồng độ cholesterol VLDL (VLDL-C) và kích ứng thụ thể LDL, dẫn đến giảm sản xuất và tăng dị hóa LDL-C. Apolipoprotein B cũng giảm đáng kể trong quá trình điều trị với simvastatin. Hơn nữa, simvastatin làm tăng vừa phải HDL-C và giảm TG huyết tương. Kết quả của các thay đổi này là làm giảm tỉ lệ cholesterol toàn phần HDL-C và tỉ lệ LDL-C/HDL-C.
Dược động học
– Hấp thu
* Ezetimibe:
Sau khi uống ezetimibe được hấp thu nhanh và liên hợp mạnh thành chất có tác dụng dược học phenolic glucoronide (ezetimibe-glucoronide). Nồng độ huyết tương tối đa trung bình (Cmax) xuất hiện khoảng 1 đến 2 giờ đối với ezetimibe-glucoronide và 4 đến 12 giờ đối với ezetimibe. Không xác định được sinh khả dụng tuyệt đối của ezetimibe do hoạt chất này không tan trong dung môi để tiêm.
Dùng cùng thức ăn (bữa ăn nhiều chất béo hoặc không chất béo) không ảnh hưởng tới sinh khả dụng đường uống của ezetimibe khi dùng viên ezetimibe 10mg.
* Simvastatin:
Sự hiện diện của β-hydroxyacid trong vòng tuần hoàn sau khi uống simvastatin được tìm thấy dưới 5% liều dùng, phù hợp với chuyển hóa bước đầu mạnh tại gan. Các chất chuyển hóa chính của simvastatin trong huyết tương người là β-hydroxyacid và bản chất chuyển hóa có hoạt tính bổ sung.
Khi đói, cả chất ức chế hoạt tính và tổng chất ức chế trong huyết tương không bị ảnh hưởng nếu dùng simvastatin ngay trước bữa ăn.
– Phân phối* Ezetimibe Ezetimibe và ezetimibe-glucoronide liên kết với protein huyết tương người tương ứng 99,7% và 88 đến 92%.
* Simvastatin Cả simvastatin và β-hydroxyacid đều liên kết với protein huyết thanh người (95%).
Dược động học khi dùng liều đơn và đa liều simvastatin không thấy tích lũy thuốc sau uống đa liều. Trong những nghiên cứu dược động học ở trên, nồng độ huyết thanh tối đa của các chất ức chế xuất hiện 1,3 giờ đến 2,4 giờ sau khi dùng.
– Chuyển hóa* Ezetimibe Ezetimibe được chuyển hóa cơ bản ở ruột non và gan nhờ liên hợp với glucoronide (phản ứng giai đoạn II) và sau đó bài tiết qua mật. Đã thấy chuyển hóa oxy hóa tổi thiểu (phản ứng giai đoạn I) ở tất cả các loài nghiên cứu. Ezetimibe và ezetimibe-glucoronide là thành phần chuyển hóa chính của thuốc xác định được trong huyết tương, chiếm tương ứng khoảng 10 đến 20% và 80 đến 90% tổng số thuốc trong huyết tương. Ezetimibe và ezetimibe-glucoronide được đào thải khỏi huyết tương chậm với dấu hiệu tái sử dụng đáng kể ở ruột gan. Nửa đời thải trừ của ezetimibe và ezetimibe-glucoroine khoảng 22 giờ.
* Simvastatin Simvastatin là một lactone không hoạt tính, nhanh chóng được thủy phân in vivo thành β-hydroxyacid tương ứng, một chất ức chế mạnh men HMG-CoA reductase. Sự thủy phân diễn ra chủ yếu ở gan; tỉ lệ thủy phân ở huyết tương người rất chậm.
Ở người, simvastatin được hấp thu tốt và chuyển hóa bước đầu mạnh ở gan. Sự chuyển hóa ở gan phụ thuộc lưu lượng máu trong gan. Gan là nơi phản ứng chính của thuốc, sau đó các chấp tương đương được bài biết vào mật. Kết quả là sự hiện diện của thuốc hoạt tính trong tuần hoàn máu thấp.
Nửa đời thải trừ của chất chuyển hóa β-hydroxyacid sau khi tiêm tĩnh mạch trung bình là 1,9 giờ.
– Thải trừ* Ezetimibe Ở người, sau khi uống 14C-ezetimibe (20 mg), ezetimibe toàn phần chiếm khoảng 93% tổng hoạt chất đánh dấu phóng xạ trong huyết tương. Đã tìm thấy tương ứng 78% và 11% hoạt chất đánh dấu phóng xạ trong phân và nước tiểu thu được trong 10 ngày. Sau 48 giờ, không thấy hoạt chất đánh dấu phóng xạ trong huyết tương.
* Simvastatin Ở người, sau khi uống một liều simvastatin đánh dấu phóng xạ, 13% hoạt chất đánh dấu phóng xạ được bài tiết vào nước tiểu và 60% vào phân trong vòng 96 giờ. Lượng tìm thấy trong phân thể hiện lượng thuốc được hấp thu và bài tiết thành các chất tương đương vào mật cũng như lượng thuốc không được hấp thu. Sau một liều tiêm tĩnh mạch chất chuyển hóa β-hydroxyacid, chỉ có trung bình 0,3% liều tiêm tĩnh mạch được bài tiết vào nước tiểu dưới dạng các chất ức chế.
– Nhóm bệnh nhân đặc biệt
* Bệnh nhân cao tuổi
Nồng độ huyết tương của ezetimibe toàn phần ở người cao tuổi (≥ 65 tuổi) cao hơn khoảng 2 lần so với người trẻ tuổi (18 đến 45 tuổi). Giảm LDL-C và dữ liệu an toàn ở người cao tuổi và tương đương người trẻ tuổi dùng ezetimibe.
* Suy gan
Sau một liều duy nhất 10 mg ezetimibe, diện tích dưới đường cong (AUC) trung bình của ezetimibe toàn phần tăng khoảng 1,7 lần ở bệnh nhân suy gan nhẹ (điểm Child Pugh 5 hoặc 6) so với người khỏe mạnh. Trong một nghiên cứu đa liều, kéo dài 14 ngày (10 mg mỗi ngày) ở những bệnh nhân suy gan vừa (điểm Child Pugh từ 7 đến 9), AUC trung bình của tổng lượng ezetimibe tăng khoảng 4 lần vào ngày 1 và ngày 14 so với người khỏe mạnh. Không cần điều chỉnh liều ở bệnh nhân suy gan nhẹ. Không nên dùng ezetimibe cho những bệnh nhân suy gan vừa đến nặng (điểm Child Pugh > 9), do chưa biết ảnh hưởng của tăng nồng độ ezetimibe toàn thân ở những bệnh nhân này (xem Thận trọng).
* Suy thận
• Ezetimibe
Sau một liều duy nhất 10 mg ezetimibe ở những bệnh nhân suy gan nặng (n=8; trung bình CrCl ≤ 3mL/phút/1,73m2), AUC trung bình của ezetimibe toàn phần tăng khoảng 1,5 lần so với người khỏe mạnh (n=9).
Một bệnh nhân trong nghiên cứu này (sau ghép thận và dùng nhiều thuốc, kể cả cyclosporin) có nồng độ toàn thân của ezetimibe toàn phần cao gấp 12 lần.
• SimvastatinTrong một nghiên cứu ở những bệnh nhân suy thận nặng (độ thanh thải creatinine < 30mL/phút), nồng độ huyết tương của toàn bộ các chất ức chế sau liều duy nhất của chất ức chế liên quan đến men khử HMG-CoA cao hơn khoảng 2 lần so với người tình nguyện khỏe mạnh.
* Giới tính
Nồng độ huyết tương của ezetimibe toàn phần ở nữ giới cao hơn một chút (< 20%) so với nam giới. Mức giảm LDL-C và dữ liệu an toàn là tương đương giữa nam giới và nữ giới điều trị bằng ezetimibe.
Liều lượng – Cách dùng
Cách dùng:
Chỉ dùng cho người l���n, không dùng cho trẻ em.
Bệnh nhân nên có chế độ ăn kiêng cholesterol trước khi bắt đầu dùng thuốc và nên tiếp tục ăn kiêng trong thời gian điều trị.
Liều dùng nên cụ thể hóa cho từng bệnh nhân dựa trên nồng độ LDL-C ban đầu, mục đích điều trị và đáp ứng của bệnh nhân.
Nên uống Thuốc một lần duy nhất vào buổi tối, cùng hoặc không cùng thức ăn.
Khuyến cáo bắt đầu điều trị với liều thấp nhất mà thuốc có tác dụng.
Liều dùng:
Liều mở rộng từ 1 viên (10/10 mg) /ngày đến 10/80 mg/ngày, uống một lần duy nhất vào buổi tối.
Có thể điều chỉnh liều theo nhu cầu và đáp ứng của từng người, nếu cần thiết.
Khi cần điều chỉnh liều lượng, cần tuân thủ khoảng cách ít nhất 4 tuần, tăng tối đa là 10/80 mg/ngày và uống một lần duy nhất vào buổi tối.
Thuốc liều 10/80 mg chỉ khuyến cáo sử dụng cho những bệnh nhân có nguy cơ cao biến chứng tim mạch, những người không đạt được mục tiêu điều trị với liều thấp hơn và khi lợi ích mong đợi vượt trội nguy có (xem THẬN TRỌNG, Bệnh lý cơ/Tiêu cơ vân).
Phải theo dõi các phản ứng có hại của thuốc, đặc biệt các phản ứng có hại đối với hệ cơ.
• Liều dùng ở bệnh nhân tăng cholesterol máu đồng hợp tử gia đình Liều đề nghị cho những bệnh nhân tăng cholesterol máu đồng hợp tử gia đình là Thuốc 10/40 mg/ngày hoặc 10/80 mg/ngày vào buổi tối. Chỉ khuyến cáo dùng liều 10/80 mg khi lợi ích mong đợi vượt trội nguy cơ
– Thuốc nên sử dụng bổ trợ cho các phương pháp điều trị giảm lipid máu khác (như lọc bỏ LDL) ở những bệnh nhân này hoặc nếu những điều trị này không có sẵn.
• Bệnh nhân suy thận Không cần chỉnh liều ở những bệnh nhân suy thận mức độ vừa phải. Nếu cần phải dùng thuốc cho những bệnh nhân suy thận nặng (độ thanh thải creatinin ≤ 30 mL/phút), nên theo dõi chặt chẽ nếu dùng liều cao hơn 10/10 mg/ngày .
• Sử dụng cho bệnh nhân cao tuổi Không cần điều chỉnh liều ở bệnh nhân cao tuổi
• Suy gan Không cần điều chỉnh liều ở những bệnh nhân suy gan nhẹ (điểm Child-Pugh 5 hoặc 6)
. Không nên dùng Thuốc cho những bệnh nhân suy gan vừa (điểm Child-Pugh 7 đến 9) hoặc suy gan nặng (điểm Child-Pugh > 9)
• Kết hợp với các thuốc khác Nên dùng Thuốc trước ≥ 2 giờ hoặc sau ≥ 4 giờ sau khi dùng thuốc hấp thụ acid mật. Khi dùng kết hợp Thuốc ở những bệnh nhân đang dùng cyclosporin hoặc danazol, liều Thuốc không được quá 10/10 mg/ngày.
Sử dụng kết hợp Thuốc ở những bệnh nhân đang dùng amiodarone, verapamil hoặc diltiazem, liều Thuốc không được quá 10/20 mg/ngày Ở những bệnh nhân dùng amlodipine đồng thời với Thuốc, liều không được vượt quá 10/40 mg/ngày
Chưa nghiên cứu tính an toàn và hiệu quả sử dụng kết hợp Thuốc với các fibrate. Do đó tránh dùng Thuốc kết hợp với các fibrate
Quá Liều
• Thuốc Không có khuyến cáo về trị liệu đặc hiệu trong trường hợp sử dụng quá liều Thuốc. Khi dùng thuốc quá liều, nên điều trị triệu chứng và hỗ trợ. Trong các nghiên cứu về độc tính cấp tính của dạng thuốc uống ở 2 loại chuột, ezetimibe (1000 mg/kg) dùng chung với simvastatin (1000 mg/kg) đều được dung nạp tốt. Không có dấu hiệu độc tính trên lâm sàng được tìm thấy ở các động vật này. LD50 của dạng uống đối với 2 loại chuột này được ước tính là ezetimibe ≥ 1000 mg/kg và simvastatin ≥ 1000 mg/kg.
• Ezetimibe Trong các nghiên cứu lâm sàng, ezetimibe liều 50 mg/ngày dùng đến 14 ngày ở 15 đối tượng khỏe mạnh hoặc liều 40 mg/ngày dùng đến 56 ngày ở 18 bệnh nhân tăng cholesterol máu nguyên phát, nói chung, đều được dung nạp tốt. Chỉ có vài báo cáo về trường hợp dùng thuốc quá liều và phần lớn đều không kèm theo tác dụng bất lợi. Các tác dụng bất lợi được báo cáo khi dùng thuốc quá liều đều không nghiêm trọng.
• Simvastatin Chỉ có vài báo cáo về trường hợp dùng thuốc quá liều; liều tối đa được dùng là 3,6g. Tất cả bệnh nhân đều bình phục không để lại di chứng.
Chống chỉ định:
– Quá mẫn với hoạt chất hoặc bất kỳ tá dược nào của thuốc. – Bệnh gan thể hoạt động hoặc tăng transaminase huyết tương kéo dài không rõ nguyên nhân. – Thai kỳ và cho con bú. – Dùng kết hợp với các thuốc ức chế mạnh CYP3A4 (như itraconazole, ketoconazole, posaconazole, thuốc ức chế HIV protease, boceprevir, telaprevir, erythromycin, clarithromycin, telithromycin và nefazodone) . – Dùng kết hợp với gemfibrozil, cyclosporine, hoặc danazol. – Bệnh cơ thứ phát do dùng các thuốc hạ lipid khác.
Tương tác thuốc:
Chống chỉ định dùng kết hợp với các thuốc sau đây: * Thuốc ức chế mạnh CYP3A4 (như itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin, telithromycin, ức chế protease HIV, boceprevir, telaprevir, nefazodone) * Gemfibrozil, Cyclosporine,hoặc Danazol • Gemfibrozil:trong một nghiên cứu dược động học, sử dụng kết hợp gemfibrozil gây tăng tổng nồng độ ezetimibe khoảng 1,7 lần và không có ý nghĩa lâm sàng;
-Tương tác với các thuốc khác:
* Các fibrate: không nên dùng Vytorin kết hợp với các fibrate cho đến khi tiến hành nghiên cứu trên bệnh nhân.
* Amiodarone: Nguy cơ bệnh cơ/Tiêu cơ vân gia tăng khi dùng đồng thời với amiodarone. Ở những bệnh nhân dùng amlodipine đồng thời, liều không được vượt quá 10/20 mg/ngày. Đối với những bệnh nhân phải dùng liều trên 20 mg/ngày mới có hiệu quả điều trị, bác sĩ có thể lựa chọn thuốc statin khác hoặc chế độ điều trị nền với statin; * Cholestyramine: Dùng đồng thời với cholestyramine làm giảm AUC trung bình của ezetimibe toàn phần (ezetimibe + ezetimibe glucuronide) khoảng 55%. Mức độ giảm thêm LDL-C nhờ bổ sung Vytorin vào liệu pháp cholestyramine có thể kém hơn do khả năng tương tác này. * Thuốc chẹn kệnh calci:Nguy cơ bệnh lý cơ/tiêu cơ vân tăng lên khi kết hợp verapamil, diltiazem, hoặc amlodipine * Acid Fusidic:Nguy cơ bệnh lý cơ có thể gia tăng nhẹ khi dùng đồng thời acid fusidic.
* Colchicine: đã có báo cáo bệnh lý cơ và tiêu cơ vân khi dùng kết hợp colchicine ở những bệnh nhân suy thận. Nên theo dõi lâm sàng thận trọng ở những bệnh nhân dùng kết hợp.
* Các dạng tương tác khác: tránh uống nhiều nước bưởi khi đang dùng thuốc;
Dùng đồng thời với ezetimibe (10 mg một lần/ngày) không ảnh hưởng đáng kể đến sinh khả dụng của warfarin và thời gian prothrombin trong 1 nghiên cứu ở 12 người lớn khỏe mạnh. Đã có báo cáo sau khi giới thiệu thuốc ra thị trường về tăng tỉ số bình thường hóa quốc tế ở bệnh nhân bổ sung ezetimibe vào trị liệu warfarin hoặc fluindione. Đa phần những bệnh nhân này cũng dùng các thuốc khác.
* Thuốc kháng acid:Khi dùng cùng thuốc kháng acid tỉ lệ hấp thu của ezetimibe giảm nhưng không ảnh hưởng đến sinh khả dụng của ezetimibe. Việc giảm tỉ lệ hấp thu này được xem không có ý nghĩa trên lâm sàng.
Tác dụng phụ:
– Rối loạn hệ thần kinh:* Không phổ biến: chóng mặt; đau đầu. – Rối loạn đường tiêu hóa:* Không phổ biến: đau bụng; khó chịu ở bụng; đau bụng trên; chứng khó tiêu; đầy hơi; buồn nôn; nôn. – Rối loạn da và mô dưới da:* Không phổ biến: phát ban; ngứa. – Rối loạn cơ xương khớp:* Không phổ biến: đau khớp; co cơ; yếu cơ; khó chịu cơ vân; đau cổ; đau tứ chi. – Rối loạn toàn thân và tại chỗ:* Không phổ biến: suy nhược; mệt mỏi; phù ngoại biên. – Rối loạn tâm thần:* Không phổ biến: rối loạn giấc ngủ. • Các biểu hiện ngoại ý phổ biến (≥ 1/100, – Xét nghiệm:* Phổ biến: tăng ALT và/hoặc AST. * Không phổ biến: tăng bilirubin máu; tăng CK máu; tăng gamma-glutamyltransferase; – Rối loạn hệ thần kinh:* Không phổ biến: đau đầu; dị cảm. – Rối loạn đường tiêu hóa:* Không phổ biến: chướng bụng; tiêu chảy; khô miệng; chứng khó tiêu; đầy hơi; bệnh trào ngược dạ dày-thực quản; nôn. – Rối loạn da và mô dưới da:* Không phổ biến: ngứa; phát ban; mày đay. – Rối loạn cơ xương khớp:* Phổ biến: đau cơ. * Không phổ biến: đau khớp; đau lưng; co cơ; yếu cơ; đau cơ vân; đau tứ chi. – Rối loạn toàn thân và tại chỗ:* Không phổ biến: suy nhược; đau ngực; mệt mỏi; phù ngoại biên. – Rối loạn tâm thần:* Không phổ biến: mất ngủ. – Vytorin kết hợp với Fenofibrate:Trong một nghiên cứu lâm sàng có đối chứng, dữ liệu về phản ứng bất lợi được báo cáo khi dùng Vytorin kết hợp với fenofibrate là tương tự với những báo cáo thu được với Vytorin và/hoặc fenofibrate dùng một mình.
Tăng HbA1c và lượng đường trong huyết thanh lúc đói đã được báo cáo với statin bao gồm cả simvastatin.
Chú ý đề phòng:
Cần cân nhắc khi dùng thuốc thuộc nhóm statin đối với bệnh nhân có những yếu tố nguy cơ dẫn đến tổn thương cơ. Thuốc thuộc nhóm statin có nguy cơ gây ra các phản ứng có hại đối với hệ cơ như teo cơ, viêm cơ, đặc biệt đối với các bệnh nhân có yếu tố nguy cơ như bệnh nhân trên 65 tuổi, bệnh nhân bị bệnh thiểu năng tuyến giáp không kiểm soát, bệnh nhân bị bệnh thận. Cần theo dõi chặt chẽ các phản ứng có hại trong quá trình dùng thuốc.
Bệnh lý cơ/Tiêu cơ vân
Cũng như các thuốc ức chế men khử HMG-CoA khác, simvastatin đôi khi gây bệnh lý cơ biểu hiện bởi đau cơ, căng cơ hoặc yếu cơ với creatine kinase (CK) vượt quá 10 lần giới hạn trên của mức bình thường (ULN). Đôi khi bệnh lý cơ thể hiện dưới dạng tiêu cơ vân có hoặc không có suy thận cấp thứ phát do myoglobin niệu, và hiếm khi gây tử vong. Nguy cơ bệnh lý cơ tăng lên khi tăng nồng độ chất ức chế men khử HMG-CoA trong huyết tương. Các yếu tố tiên đoán bệnh lý cơ bao gồm người cao tuổi (≥ 65 tuổi), nữ giới, thiểu năng tuyến giáp không được kiểm soát và suy thận. Ở những bệnh nhân bắt đầu dùng Thuốc hoặc bắt đầu tăng liều Thuốc, nên thông báo cho bệnh nhân nguy cơ bệnh lý cơ và khuyên bệnh nhân thông báo ngay bất kỳ đau cơ, mỏi cơ hoặc yếu cơ không xác định được nguyên nhân. Nên ngừng dùng Thuốc ngay tức thì nếu chẩn đoán hoặc nghi ngờ bệnh lý cơ. Sự xuất hiện các triệu chứng trên và nồng độ CK > 10 lần giới hạn trên của mức bình thường chỉ định bệnh lý cơ. Trong đa phần các trường hợp khi bệnh nhân ngừng ngay simvastatin, các triệu chứng cơ và tăng CK trở về bình thường. Kiểm tra định kỳ CK có thể cần thiết ở những bệnh nhân đắt đầu điều trị với Thuốc hoặc bắt đầu trị liệu. Khuyến cáo kiểm tra định kỳ cho những bệnh nhân dùng liều 10/80 mg. Không có gì đảm bảo rằng kiểm tra định kỳ này sẽ ngăn ngừa bệnh lý cơ. Do Thuốc chứa simvastatin, nguy cơ bệnh lý cơ/chứng tiêu cơ vân tăng lên khi dùng Thuốc cùng lúc với các thuốc sau: • Các thuốc chống chỉ định – Thuốc ức chế mạnh CYP3A4: Chống chỉ định sử dụng kết hợp với các thuốc được cho là có tác dụng ức chế mạnh CYP3A4 tại liều điều trị (như itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin, telithromycin, thuốc ức chế protease HIV, boceprevir, telaprevir, hoặc nefazodone). Nếu cần thiết phải điều trị với itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin, hoặc telithromycin thì nên ngừng điều trị với Thuốc trong thời gian dùng các thuốc trên. – Gemfibrozil,cyclosporinehoặc danazol:chống chỉ định dùng những thuốc này cùng với Thuốc. • Các thuốc khác – Amiodarone: Nguy cơ bệnh lý cơ/chứng tiêu cơ vân tăng lên khi dùng đồng thời amiodarone với Thuốc. Ở những bệnh nhân dùng amlodipine đồng thời với Thuốc, liều Thuốc không được vượt quá 10/20 mg/ngày. Đối với những bệnh nhân phải dùng liều trên 10/20 mg/ngày mới có hiệu quả điều trị, bác sĩ có thể lựa chọn thuốc statin khác hoặc chế độ điều trị nền với statin – Thuốc chẹn kênh canxi: * Verapamil hoặc diltiazem: Những bệnh nhân đang điều trị diltiazem kết hợp với simvastatin 80 mg có nguy cơ cao bệnh lý cơ. Liều Thuốc không nên quá 10/20 mg mỗi ngày ở những bệnh nhân điều trị kết hợp với verapamil hoặc diltiazem. * Amlodipine: Trong 1 nghiên cứu lâm sàng, những bệnh nhân đang điều trị amlodipine kết hợp với simvastatin 80 mg có nguy cơ cao bệnh lý cơ. Liều Thuốc không nên quá 10/40 mg mỗi ngày ở những bệnh nhân điều trị kết hợp với amlodipine. * Các thuốc ức chế trung bình CYP3A4: Bệnh nhân dùng các thuốc khác được cho là có tác dụng ức chế trung bình CYP3A4 kết hợp với Thuốc, đặc biệt khi dùng Thuốc liều cao, có thể tăng nguy cơ bệnh lý cơ. * Các fibrate: Sử dụng kết hợp với fenofibrate hoặc gemfibrozil làm tăng tổng nồng độ ezetimibe khoảng 1,5-1,7 lần nhưng không có ý nghĩa lâm sàng. Đã đánh giá tính an toàn và hiệu quả của ezetimibe kết hợp với các fenofibrate chưa được thiết lập. Các fibrate có thể gây tăng thải trừ cholesterol vào mật, gây sỏi mật. Trong một nghiên cứu tiền lâm sàng ở chó, ezetimibe gây tăng cholesterol trong túi mật. Mặc dù mối liên quan của phát hiện tiền lâm sàng này trên người chưa rõ, không nên dùng Thuốc kết hợp với các fibrate cho đến khi tiến hành nghiên cứu trên bệnh nhân. * Acid fusidic: những bệnh nhân đang điều trị acid fusidic kết hợp với Thuốc có thể tăng nguy cơ bệnh lý cơ . Nên theo dõi chặt chẽ bệnh nhân đang dùng Thuốc với acid fusidic. Nên cân nhắc có thể tạm ngừng Thuốc. – Niacin(≥ 1 g/ngày): Đã gặp bệnh lý cơ/tiêu cơ vân khi dùng simvastatin kết hợp với niacin (≥ 1 g/ngày) để điều chỉnh lipid. – Thuốc chống đông: Nên theo dõi thích hợp Tỉ lệ Bình thường hóa Quốc tế (INR) khi bổ sung Thuốc với warfarin, coumarin chống đông khác, hoặc fluindione.
Các men gan
Trong những thử nghiệm lâm sàng có kiểm soát dùng kết hợp simvastatin và ezetimibe, đã thấy tăng transaminase liên tục (> 3 lần giới hạn trên của mức bình thường). Nên dùng Thuốc thận trọng ở những bệnh nhân uống rượu nhiều và/hoặc có tiền sử bệnh gan. Chống chỉ định dùng Thuốc khi có bệnh gan thể hoạt động hoặc tăng nồng độ transaminase kéo dài không rõ nguyên nhân. Suy gan: Do chưa biết tác dụng của tăng nồng độ ezetimibe ở những bệnh nhân suy gan trung bình hoặc nặng không nên dùng Thuốc cho những bệnh nhân này. Sử dụng ở bệnh nhi: Không dùng Thuốc cho bệnh nhi. Sử dụng ở người cao tuổi Do tuổi cao (≥ 65 tuổi) là yếu tố tiên đoán bệnh lý cơ, nên thận trọng khi kê đơn Thuốc cho bệnh nhân cao tuổi. Trong một thử nghiệm lâm sàng ở những bệnh nhân dùng simvastatn 80 mg/ngày, những bệnh nhân ≥ 65 tuổi thấy nguy cơ bệnh lý cơ tăng cao hơn so với những bệnh nhân Ảnh hưởng lên khả năng lái xe và vận hành máy móc: Chưa tiến hành nghiên cứu về ảnh hưởng lên khả năng lái xe và vận hành máy móc. Tuy nhiên, đã có báo cáo một vài tác dụng phụ của Thuốc có thể ảnh hưởng lên khả năng lái xe và vận hành máy móc. Đáp ứng của mỗi người bệnh với Thuốc có thể khác nhau.
Lúc có thai và lúc nuôi con bú • Lúc có thai:Xơ vữa động mạch là một quá trình mãn tính, và ngừng điều trị các thuốc hạ lipid thông thường trong khi mang thai ít ảnh hưởng đến nguy cơ lâu dài liên quan đến tăng cholesterol máu nguyên phát.
*Chống chỉ định dùng khi mang thai.
• Lúc nuôi con bú:Nghiên cứu trên chuột cho thấy ezetimibe được tiết vào sữa. Chưa biết liệu các hoạt chất của Thuốc có được bài tiết vào sữa mẹ hay không, do đó phụ nữ cho con bú không được dùng Thuốc.
Thông tin thành phần Ezetimib
Chỉ định :
Ezetimibe được sử dụng cùng với một chế độ ăn ít chất béo, ít cholesterol và tập thể dục để giúp giảm lượng cholesterol trong máu. Ezetimibe có thể được sử dụng một mình hoặc với các thuốc khác (chẳng hạn như statin hoặc fibrate).
Ezetimibe hoạt động bằng cách làm giảm lượng cholesterol cơ thể hấp thu từ chế độ ăn uống. Giảm cholesterol có thể giúp ngăn ngừa đột quỵ và đau tim.
Liều lượng – cách dùng:
Liều dùng thông thường cho người lớn tăng lipid máu:
Dùng 10 mg một lần mỗi ngày với thức ăn hoặc không kèm thức ăn.
Liều dùng thông thường cho người lớn bị bệnh sitosterolemia:
Dùng 10 mg một lần mỗi ngày với thức ăn hoặc không kèm thức ăn.
Tác dụng phụ
Hãy gọi cho bác sĩ ngay nếu bạn có một tác dụng phụ nghiêm trọng như:
Yếu cơ bất thường hoặc đau; Buồn nôn, đau bụng, sốt nhẹ, chán ăn, nước tiểu đậm màu, phân màu đất sét, vàng da (vàng da hoặc mắt); Đau ngực; Viêm tụy (đau nặng ở bụng trên lan sang lưng, buồn nôn và nôn, nhịp tim nhanh); Sốt, đau họng và đau đầu với mụn rộp nặng, bong tróc và phát ban da đỏ. Tác dụng phụ ít nghiêm trọng bao gồm:
Tê hoặc cảm giác tê tê; Đau bụng nhẹ, tiêu chảy; Cảm giác mệt mỏi; Nhức đầu; Chóng mặt; Tâm trạng chán nản; Chảy nước mũi hoặc nghẹt mũi, triệu chứng cảm lạnh; Đau khớp, đau lưng.
Thông tin thành phần Simvastatin
Dược lực:
Simvastatin là chất ức chế men khử 3-hydroxy-3-methylglutaryl-coenzym A (HMG-CoA).
Dược động học :
Sau khi được hấp thu từ ống tiêu hóa, Simvastatin chuyển hóa vượt qua lần đầu mạnh ở gan. Do đó sinh khả dụng của thuốc trong vòng tuần hoàn lớn thì thấp và biến đổi. Dưới 5% liều uống được ghi nhận là đến tuần hoàn dưới dạng chất chuyển hóa có hoạt tính. Thuốc gắn kết mạnh với protein huyết tương (95%). Simvastatin được thủy phân ở gan thành dạng acid beta-hydroxy có hoạt tính. Ba chất chuyển hóa khác đã được phân lập là các dẫn chất 6-hydroxy, 6-hydroxy methyl và 6-exomethylen. Simvastatin thải trừ phần lớn qua phân, chủ yếu là phần thuốc không được hấp thu và chiếm 60% liều uống. Khoảng 10-15% thuốc thải trừ qua đường thận. Thời gian bán huỷ của chất chuyển hóa có hoạt tính là 1,9 giờ.
Tác dụng :
Simvastatin là thuốc hạ cholesterol được tổng hợp từ một sản phẩm lên men của Aspergillus terreus. Nó là chất ức chế men khử 3-hydroxy-3-methyl glutaryl-coenzym A (HMG-CoA). Men khử này xúc tác phản ứng chuyển HMG-CoA thành mevalonat, bước giới hạn tốc độ và là bước đầu tiên trong sinh tổng hợp cholesterol. Cơ chế tác dụng: Simvastatin là chất ức chế đặc hiệu men khử HMG-CoA, enzym xúc tác phản ứng chuyển HMG-CoA thành mevalonat là bước đầu tiên trong sinh tổng hợp cholesterol. Simvastatin làm giảm nồng độ cholesterol tỉ trọng thấp (LDL) lúc bình thường và cả khi tăng cao. LDL được tạo ra từ lipoprotein tỉ trọng rất thấp (VLDL) và được dị ứng hóa chủ yếu bởi thụ thể LDL ái lực cao. Cơ chế tác dụng làm giảm LDL của simvastatin có thể là do giảm nồng độ cholesterol VLDL và cảm ứng của thụ thể LDL, dẫn đến giảm sản xuất và/hoặc tăng dị ứng hóa cholesterol LDL.
Chỉ định :
– Simvastatin được dùng để hỗ trợ cho chế độ dinh dưỡng ở bệnh nhân tăng cholesterol máu nguyên phát gây ra do sự tăng các lipoprotein cholesterol trọng lượng phân tử thấp (LDL) ở những bệnh nhân có nguy cơ bệnh động mạch vành mà không đáp ứng được với chế độ ăn kiêng. – Simvastatin cũng được dùng để để làm giảm nồng độ cholesterol lipoprotein trọng lượng phân tử thấp (LDL) ở những bệnh nhân vừa tăng cholesterol, vừa tăng triglyceride máu.
Liều lượng – cách dùng:
– Simvastatin được sử dụng bằng đường uống. – Cần cho người bệnh dùng chế độ dinh dưỡng giảm cholesterol chuẩn trước khi dùng Simvastatin và người bệnh cần tiếp tục ăn kiêng trong suốt quá trình điều trị với Simvastatin. – Liều khởi đầu là 5-10mg/ngày, uống vào buổi tối. Liều tối đa là 40mg/ngày. Liều dùng cần được điều chỉnh theo đáp ứng từng cá thể.
Chống chỉ định :
– Quá mẫn cảm với bất kỳ thành phần nào của thuốc. – Bệnh gan tiến triển, tăng transaminase máu thường xuyên không rõ nguyên nhân. – Phụ nữ có thai và cho con bú.
Tác dụng phụ
Thuốc được dung nạp tốt, có thể xảy ra đầy hơi, tiêu chảy, táo bón, buồn nôn.
Lưu ý: Dùng thuốc theo chỉ định của Bác sĩ
Nguồn tham khảo drugs.com, medicines.org.uk, webmd.com và TraCuuThuocTay.com tổng hợp.
Cần tư vấn thêm về Thuốc Ezensimva 10/10 tác dụng, liều dùng, giá bao nhiêu? bình luận cuối bài viết.
Tuyên bố miễn trừ trách nhiệm y tế
Nội dung của TraCuuThuocTay.com chỉ nhằm mục đích cung cấp thông tin về Thuốc Ezensimva 10/10 tác dụng, liều dùng, giá bao nhiêu? và không nhằm mục đích thay thế cho tư vấn, chẩn đoán hoặc điều trị y tế chuyên nghiệp.
Chúng tôi miễn trừ trách nhiệm y tế nếu bệnh nhân tự ý sử dụng thuốc mà không tuân theo chỉ định của bác sĩ.
Vui lòng liên hệ với bác sĩ hoặc phòng khám, bệnh viện gần nhất để được tư vấn.
Đánh giá 5* post
The post Thuốc Ezensimva 10/10 tác dụng, liều dùng, giá bao nhiêu? appeared first on Tra Cứu Thuốc Tây.
Dẫn nguồn từ Tra Cứu Thuốc Tây https://tracuuthuoctay.com/thuoc-ezensimva-10-10-tac-dung-lieu-dung-gia-bao-nhieu/
0 notes
Text
Production of Cholesterol and Triglycerides Inside the Body And Use of Medicines

Human body is the most wonderful machine consisting of 10000 billion cells and each of these cells has the capability of producing energy by burning food that we eat. The three major sources of energy to the body are - Carbohydrates, Proteins and Fats. To produce energy, foods have to be provided to the cells in their simplest form i.e Glucose for Carbohydrates, Amino Acids for Proteins and Triglycerides (or fatty acids) for Fats. The powerhouse of the cells called the Mitochondria carries out the job to convert these Glucose, Amino acids and Fatty acids to Calories.
When we eat food in the form of thousands of dishes - these items have to be broken in the Food pipe (medically called Gastro Intestinal Tract) to their simplest forms. This is done in steps called - Digestion, and Absorption. Each of the food we eat is first chewed, and digested in the stomach by acids and gastric juices, then further digested in the intestine by bile juice (secreted by the liver) and also juice secreted by the intestine and pancreas. The enzymes present in these juices break the food into Glucose, Amino acids and Fatty acids (triglycerides). This process is called digestion.
Next step is absorption. These simplest forms of food are taken up from the intestine to the blood stream. As soon as it is done the blood level of Glucose, Amino acids and Triglycerides goes up. The blood - which is pumped to the whole of the body by the heart takes these absorbed products to the billions of cells and there they are assimilated (further broken down) to produce energy.
Fats (also called lipids) that are present in the food or blood can be divided into three categories - Cholesterol, Triglycerides (called the natural fats) and Phospho-lipids. Cholesterol is a type of fatty acid consisting of 27 carbon atoms and perform three important functions in our body - (1) they help in the formation of wall of all the cells in the body, (2) produce Sex hormones - which help in formation of sex organs of the body and allow them to work and (3) help in the digestion - absorption of fats in the intestine as a part of Bile juice. About 97% of cholesterol groups secreted in the bile juice are absorbed back into the blood stream. Apart from the cholesterol consumed in the form of food (Non-vegetarian food, milk and milk products) a considerable amount of Cholesterol is also manufactured by our liver. The cholesterol is indispensable chemical of the body - as without it the body will die.
For the medical science and cardiologists - Cholesterol holds lot of importance as it forms a major part of the blockage along with triglycerides. Millions of people all over the world suffer from heart disease because cholesterol will deposit more and more as its level in the blood increases beyond 200 mg%. At least three Nobel prices have been given in the past to those medical scientists who have brought out facts about cholesterol metabolism in the body.
The oils that we consume in our food consists of fatty acids - which can be saturated or unsaturated ( depending on the possibility of addition of further Hydrogen). All these fats are absorbed in the form of triglycerides beyond 160mg% is very bad - as it helps deposit fat inside the heart arteries. The liver also manufactures a lot of triglycerides and releases them in the blood in the form of VLDL.
Cholesterol and triglycerides mostly travel in the blood in combination with proteins and phospho-lipids. Different combinations of these Chemicals circulating in the blood are known as LDL (Low Density Lipoprotein), cholesterol, HDL (High Density Lipoprotein) cholesterol, and VLDL (Very Low Density Lipoprotein) cholesterol. LDL contains 53% cholesterol in it.
In the liver-cholesterol is manufactured from Acetyl Co A, which in turn is converted into HMG (Hydroxy Methyl Glutaryl) Co A. This HMG Co A is then converted into Mevalonic acid by an enzyme called HMG Co A reductase. Mevalonic acid is then converted into cholesterol in the next few steps.
Cholesterol and triglycerides are broken down inside the cells - and their uptake depends on a protein called LDL receptor. Drugs which can influence this LDL receptor hold a lot of promise in future and can offer a permanent solution to Heart Disease. Triglycerides are broken down to fatty acids and Glycerol by enzyme called Lipo-protein lipase, inside the cells. Most of the triglycerides are stored inside the fat cells and can be used when less calories (lower than 1600 per day) are provided to the body.
Hope you liked this article.
This article is written by Dr. Bimal Chhajer (India's best heart doctor)

0 notes