#live-attenuated vaccine
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Photo
Local Action
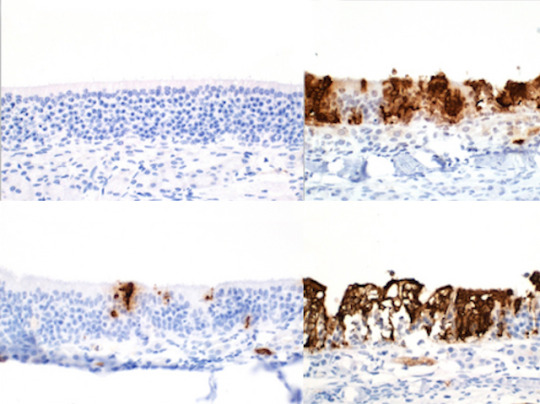
Vaccines are typically injected into an arm muscle, including those recently developed against SARS-CoV-2, the virus responsible for COVID-19. Yet coronaviruses first infect the mucous membranes in our respiratory tract, in the nose, mouth, throat and lungs. Administering vaccines intranasally, to target those frontline areas, could allow us to respond to infection faster. Nasal vaccines against SARS-CoV-2 have already been developed in India and China, but researchers are now testing a new intranasal live-attenuated vaccine, containing a modified virus. Tests in hamsters found it highly effective: very few SARS-CoV-2 particles (in brown) penetrated their nasal mucous membranes after double vaccination with the intranasal vaccine (top left) or even a combination of one intranasal dose with an existing mRNA vaccine (bottom left), compared to poor results after intramuscular vaccination only (right-hand panels). Following up these encouraging results with safety and efficacy trials in humans could provide new options for future vaccination.
Written by Emmanuelle Briolat
Image adapted from work by Geraldine Nouailles and Julia M. Adler, and colleagues
Department of Infectious Diseases, Respiratory Medicine and Critical Care, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Nature Immunology, April 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#immunohistochemistry#sars-cov-2#covid 19#vaccinations#get vaccinated#intranasal#live-attenuated vaccine#mucous membrane#mrna vaccine#immunology#immunity
11 notes
·
View notes
Text
Vaccines Market Estimated to be Worth $71.50 Billion in 2031
Meticulous Research®– a leading global market research company, published a research report titled ‘Vaccines Market Size, Share, Forecast, & Trends Analysis by Indication (Pneumococcal, Influenza, HPV, DTP, MMR, Hepatitis, COVID-19) Administration (IM, SC, Oral) Type (Inactivated, Combination) Valence (Multivalent, Monovalent) - Global Forecast to 2031.’
According to this latest publication from Meticulous Research®, the vaccines market is projected to reach $71.50 billion by 2031, at a CAGR of 2.3% during the forecast period. This market's growth is driven by a strong pipeline for vaccines, increasing government initiatives toward immunization, and technological advancements in the vaccine industry. Moreover, the rising prevalence of diseases, growing focus on therapeutic vaccines, and growth prospects in emerging markets are expected to offer growth opportunities for the players operating in this market.
However, the high costs involved in vaccine development and the long timelines of vaccine manufacturing restrain the market’s growth. Additionally, product recalls and inadequate access to vaccines pose challenges to the market’s growth.
Download Sample Report Here @ https://www.meticulousresearch.com/download-sample-report/cp_id=5076
Key Players
The key players operating in the vaccines market are Sanofi (France), Merck & Co., Inc. (U.S.), GlaxoSmithKline plc (U.K.), Pfizer Inc. (U.S.), Johnson & Johnson (U.S.), Daiichi Sankyo Co., Ltd. (Japan), Takeda Pharmaceutical Company Limited (Japan), CSL Limited (Australia), Emergent BioSolutions Inc. (U.S.), and AstraZeneca PLC (U.K.).
Vaccines Market: Future Outlook
The vaccines market is segmented based on Indication (Pneumococcal Disease, Influenza, Human Papillomavirus (HPV), Diphtheria, Tetanus, and Pertussis (DTP), Meningococcal Disease, Measles, Mumps, and Rubella (MMR), Rotavirus, Poliomyelitis (Polio), Hepatitis, COVID-19, Other Indications), Route of Administration (Intramuscular, Subcutaneous, Oral, Other Route of Administration), Type (Subunit & Conjugate Vaccines, Inactivated Vaccines, Live-Attenuated Vaccines, Toxoid Vaccines, Combination Vaccines), and Valence (Multivalent and Monovalent Vaccines) and Geography. The study also evaluates industry competitors and analyzes their market share at global and regional levels.
Based on indication, the vaccines market is segmented into pneumococcal disease, influenza, human papillomavirus (HPV), diphtheria, tetanus, pertussis (DTP), meningococcal disease, measles, mumps, rubella (MMR), rotavirus, poliomyelitis (polio), hepatitis, COVID-19, and other indications. In 2024, the pneumococcal disease segment is expected to account for the largest share of the vaccines market. The large market share of this segment can be attributed to the rising incidence of pneumococcal diseases such as pneumonia, meningitis, febrile bacteremia, otitis media, and sinusitis; and the development of quality vaccines such as PPSV23.
Based on route of administration, the vaccines market is segmented into intramuscular (IM), subcutaneous (SC), oral, and other routes of administration. In 2024, the intramuscular (IM) segment is expected to account for the largest share of the vaccines market. The large market share of this segment can be attributed to the ease of intramuscular administration and quick absorption of vaccines administered through the intramuscular route. Further, due to the COVID-19 pandemic, there has been increased adoption of the intramuscular route of administration, as many COVID-19 vaccines are being administered through this route.
Based on type, the vaccines market is segmented into subunit & conjugate vaccines, inactivated vaccines, live-attenuated vaccines, toxoid vaccines, and combination vaccines. In 2024, the subunit & conjugate vaccines segment is expected to account for the largest share of the vaccines market. The large market share of this segment can be attributed to the subunit & conjugate vaccines’ long-term immunity, high safety, and stability compared to vaccines with other antigens.
Based on valence, the vaccines market is segmented into multivalent vaccines and monovalent vaccines. In 2024, the multivalent vaccines segment is expected to account for the larger share of the vaccines market. The large market share of this segment can be attributed to the launch of newer multivalent vaccines, increasing investments by key players in the R&D of multivalent vaccines, and technological advancements in the production of multivalent vaccines.
Geographic Review
This research report analyzes major geographies and provides comprehensive analysis for North America (U.S and Canada), Europe (Germany, France, U.K., Italy, Spain, Switzerland, Netherlands, and Rest of Europe), Asia-Pacific (China, Japan, India, Australia, South Korea, and Rest of Asia-Pacific), Latin America (Brazil, Mexico, Rest of Latin America) and Middle East & Africa. In 2024, North America is estimated to account for the largest share of 41.2% of the vaccines market, followed by Europe and Asia-Pacific. North America’s major market share is attributed to the growing research & development, product launches, and the establishment of new facilities in the region by key players.
Complete Report Here : https://www.meticulousresearch.com/product/vaccines-market-5076
Key Questions Answered in the Report:
Which high-growth market segments are in terms of indication, route of administration, type, valence, and regions/countries?
What was the historical market for vaccines across the globe?
What are the market forecasts and estimates for the period 2024-2031?
What are the major drivers, restraints, challenges, and opportunities in the vaccines market?
What is the competitive landscape like, and who are the market leaders in the vaccines market?
What are the recent developments in the vaccines market?
What strategies are adopted by the major players in the vaccines market?
What are the geographical trends and high-growth regions/countries?
Contact Us: Meticulous Research® Email- [email protected] Contact Sales- +1-646-781-8004 Connect with us on LinkedIn- https://www.linkedin.com/company/meticulous-research
#Vaccines Market#Vaccines#Intramuscular Vaccines#Subcutaneous Vaccines#Inactivated Vaccines#Immunizations#Inoculations#Toxoid Vaccines#Live-Attenuated Vaccines#COVID-19 vaccine#Subunit Vaccines
0 notes
Text
https://app.socie.com.br/read-blog/153744_live-attenuated-vaccines-market-size-analysis-and-forecast-2031.html
The Live Attenuated Vaccines Market in 2023 is US$ 7.85 billion, and is expected to reach US$ 17.47 billion by 2031 at a CAGR of 10.52%.
#Live Attenuated Vaccines Market#Live Attenuated Vaccines Market Report#Live Attenuated Vaccines Market Research
0 notes
Text
How the Gates Foundation Hijacked COVID-19 for Profit
After much thought and a continuing stream of new evidence coming to light, I am going to do this. This is a timeline of events leading up to and surrounding the coronavirus outbreak in late 2019. I still cannot prove that the long-lasting, breath-shortening cold many people caught in December 2019 was in anyway related to COVID-19. I also cannot find information – most likely because in 2013,…
View On WordPress
#attenuated#attenuated live infections bronchitis virus#ChAdOx1#Chimp Adenovirus vector#Competition#coronavirus#Covid-19 vaccine#Dr Tess Lawrie#Erica Bickerton#Gates Foundation#human adenovirus#intellectual property#Inventor#Ivermectin#licensing#Livestock Antibody Hub#mutant spike protein#patents#pirbright institute#propaganda and censorship#Protease inhibitor#Responding to public#shutting down public speculation#viruses affecting farm animals and human health#Written Evidence to parliament
0 notes
Text
i just saw a post about how we just have to "live with" covid and wanting more protections from our government is unreasonable because we'll never wipe it out, it jumps species and is in all sorts of animal populations (like, true ok) so why even try to
and apparently the argument was aimed at people (who I haven't seen in the wild) who are arguing we should still be in lockdown. and i have mixed feelings about the idea of extended lockdown or attenuating isolations; but my main feeling at this point is not that the government should keep us apart but that the government should be trying to make it safer for us to be together
things the government could/should be doing about covid:
we know that ventilation/air movement helps a shitton. we should be incentivizing upgrades to ventilation systems in all public buildings with shit like rebates or tax deductions, while phasing in eventual legal requirements. (and uh. it has occurred to me that the US might actually be doing this sideways by there's currently this decade enormous tax incentives in re energy efficient upgrades for slowing climate change and you know. energy efficient hvac does tend to improve ventilation. extra point to biden here.)
mandatory paid sick leave so workers aren't under social or economic pressure to work when sick
passing out RT-LAMP tests like metrix that actually work instead of the rapid antigen tests that have become less and less reliable as the virus mutates
i don't know how you'd write this law but like 95% or more of computer-based work can be done remotely and companies should not be allowed to force people to return to the office. I know there's people who want to be back in person and I'm not saying they should be forced to stay home but ffs I know of at least two people CLOSE to me who worked remotely before the pandemic and at some point their workplaces tried to tell them they weren't allowed to do that anymore despite the pre-existing contracts. stop canceling remote work for people that want, need, or prefer it.
for that matter, every college lecture that was an online class during covid should still be offered as an online class, there is no reason to force students into auditoriums in person. you got the communications infrastructure up and running, why are you tearing it down. give people the OPTION. it increases accessibility for everyone!
covid vaccine immunity lasts about four months. this should be well-publicized and everyone should be able to re-up for free every four months. "every year, like the flu vaccine" is demonstrably not often enough. actually "for free" isn't good enough start handing out $10 gift cards you will be shocked at how many people who are resistant to the idea of vaccines will fold for $10 a shot
are there already laws on the books about masks in medical settings that some medical professionals are blatantly ignoring because they forgot what best practices were before the plague and they're 'tired of masking'? if not, pass laws. if so, fucking enforce them
oh another incentives for upgrades phasing into legal requirements thing: brass doorknobs and railings over stainless steel or whatever. microbes do not survive on brass surfaces
i mean. i know this one sounds too extreme to a lot of people but. UBI.
most if not all of these measures will prevent or ameliorate other pandemics of different diseases that may arise in the future. and just. generally improve our health and quality of life for other reasons.
I haven't felt safe to go to a concert since 2020. Maybe if I knew a venue was legally required to have ventilation to a certain standard and that none of the ticket takers and ushers were on the job sick to avoid risking loss of paycheck or job, and knew a larger percentage of the crowd had up to date vaccinations--maybe if any or all that, I might ever feel comfortable going to a show again.
wouldn't it be nice if those of us who have been disabled, by covid or other conditions, had accessible remote options but also occasionally felt safe enough to interact with and participate in wider society?
one of the arguments on the post I saw was how isolation was massively psychologically damaging and various strata of society were affected in all sorts of ways, from undersocialized kids to increased depression in--well across the board, I think. and here's the thing: WE KNOW. PEOPLE WITH CHRONIC HEALTH CONDITIONS, LONG COVID OR OTHERWISE, KNOW ISOLATION SUCKS REAL BAD. because we, both for our own health and due to disability ostracism, are still isolating and isolated more than most.
what are you as individuals or societies, what are our governments, doing to help make it safe and accessible to rejoin you????
397 notes
·
View notes
Text
Needle-free COVID-19 intranasal vaccine provides broad immunity, study finds - Published Agu 27, 2024
A next-generation COVID-19 mucosal vaccine is set to be a gamechanger not only when delivering the vaccine itself, but also for people who are needle-phobic.
New Griffith University research, "A single-dose intranasal live-attenuated codon deoptimized vaccine provides broad protection against SARS-CoV-2 and its variants" published in Nature Communications, has been testing the efficacy of delivering a COVID-19 vaccine via the nasal passages.
Professor Suresh Mahalingam from Griffith's Institute for Biomedicine and Glycomics has been working on this research for the past four years.
"This is a live attenuated intranasal vaccine, called CDO-7N-1, designed to be administered intranasally, thereby inducing potential mucosal immunity as well as systemic immunity with just a single dose," Professor Mahalingam said.
"The vaccine induces strong memory responses in the nasal mucosa, offering long-term protection for up to a year or more.
"It's been designed to be administered as a single dose, ideally as a booster vaccine, as a safe alternative to needles with no adverse reactions in the short or long term."
Live-attenuated vaccines offer several significant advantages over other vaccine approaches.
They induce potent and long-lived humoral and cellular immunity, often with just a single dose.
Live-attenuated vaccines comprise the entire virus, thereby providing broad immunity, in contrast to a single antigen which is used in many other vaccine platforms.
Lead author Dr. Xiang Liu said the vaccine provides cross-protection against all variants of concern, and has neutralizing capacity against SARS-CoV-1.
"The vaccine offers potent protection against transmission, prevents reinfection and the spread of the virus, while also reducing the generation of new variants," Dr. Liu said.
"Unlike the mRNA vaccine which targets only the spike protein, CDO-7N-1 induces immunity to all major SARS-CoV-2 proteins and is highly effective against all major variants to date.
"Importantly, the vaccine remains stable at 4°C for seven months, making it ideal for low- and middle-income countries."
The vaccine has been licensed to Indian Immunologicals Ltd, a major vaccine manufacturer.
Dr. K. Anand Kumar, co-author of the publication and Managing Director of Indian Immunologicals Ltd. Said, "We are a leading 'One Health' company that has developed and launched several vaccines for human and animal use in India and are currently exporting to 62 countries."
"We have completed all the necessary studies of this novel COVID-19 vaccine which offers tremendous advantages over other vaccines.
"We now look forward to taking the vaccine candidate to clinical trials."
Professor Lee Smith, Acting Director of the Institute for Biomedicine and Glycomics, said he was delighted with the research findings.
"These results towards developing a next-generation COVID-19 vaccine are truly exciting," Professor Smith said.
"Our researchers are dedicated to providing innovative and, crucially, more accessible solutions to combat this high-impact disease."
More information: Xiang Liu et al, A single-dose intranasal live-attenuated codon deoptimized vaccine provides broad protection against SARS-CoV-2 and its variants, Nature Communications (2024). DOI: 10.1038/s41467-024-51535-y
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator
84 notes
·
View notes
Text
But public health experts say there are some adults who should consider getting revaccinated. That includes older adults who were born after 1957 and were vaccinated before 1968.
That's because early versions of the measles vaccine were made from an inactivated (killed) virus, which didn't work particularly well, Offit says. That's why the Centers for Disease Control and Prevention recommends that anyone vaccinated before 1968 get at least one dose of the live attenuated vaccine.
24 notes
·
View notes
Note
Speaking of the measles outbreak. I am as fully vaccinated as a person can be I think, my parents aren’t insane and believe and trust in science thankfully, but I also unaware of how the different types of vaccines work. If I am exposed to measles is there a chance I can get it or is it the type of vaccines where the chance of me getting it is like 0.001%?
And I actually have the same question about polio. When I was in elementary school we read Small Steps and met polio survivors who encouraged us to get vaccines because they save lives by preventing diseases. I have lowkey been terrified of getting polio since people have stopped using their brains and decided that they didn’t need to vaccinate their children.
I also know that these are obviously different vaccines than what we get for the flu every year but do we need boosters?
Thanks so much, hope we all stay safe and healthy despite the terrifying stupidity of others!
Hi, my love! That’s a great set of questions and I love that you’re thinking critically about how different vaccines work!
For measles, if you’ve received two doses of the MMR (measles, mumps, rubella) vaccine, you’re considered fully vaccinated and about 97% protected against measles. That means there’s still a very small chance (about 3%) that you could get it if exposed, but it’s extremely unlikely.
The MMR vaccine is live-attenuated, meaning it contains a weakened form of the virus that trains your immune system to recognize and destroy it before it can cause an actual infection. Once you’ve had both doses, you generally don’t need a booster since protection is long-lasting (I was one of the lucky few whose titers were low enough to require a booster when I got tested for medical school). The rare cases of vaccinated people getting measles usually happen if their immune system didn’t mount a strong enough response, but even then, symptoms tend to be much milder.
Polio is a bit different. The vaccine we use in the United States (the IPV or inactivated polio vaccine) is a killed virus vaccine, meaning it doesn’t contain any live virus but still triggers a strong immune response. If you completed the childhood polio vaccine series (typically four doses), you’re considered fully protected and don’t need routine boosters. However, if you were traveling to a high-risk area or there was a local outbreak, a doctor might recommend an additional dose just as extra precaution. Your concern about polio is totally valid, while it was nearly eradicated in many places, low vaccination rates have allowed it to resurface in certain areas.
As for flu vaccines, you’re right that they work differently. The flu virus mutates rapidly, so the vaccine is reformulated each year to match the circulating strains as closely as possible. That’s why we need a new flu shot annually, while vaccines like MMR and polio provide longer-lasting protection.
Believe me, I completely relate to feeling frustrated about people rejecting vaccines despite overwhelming evidence of their safety and effectiveness. The best thing we can do is stay informed, keep up with our own vaccinations, and encourage science-based decision-making whenever possible. I hope this helps!
20 notes
·
View notes
Text
Who needs another measles vaccine dose? Answering your questions.
Many readers expressed outrage about the measles outbreak that began in an under-vaccinated community in rural West Texas, as I described in my column this week. The outbreak has infected more than 120 people there and in neighboring New Mexico and already led to the death of one child. Several shared their own devastating experiences with the disease as children.
Angela from Wisconsin contracted the virus when she was 5. She recalls becoming so ill that she spent months in the hospital. She is living with permanent disabilities from it, including hearing loss and blindness. “I cannot express to you the rage I have when I hear people say that measles is a harmless disease,” she wrote.
Before widespread vaccination, measles caused 5 to 10 percent of profound hearing-loss cases in the United States. Worldwide, measles used to be a leading cause of blindness among children; as many as 60,000 a year lost sight because of the disease.
“In your column, you mentioned that measles can ‘wipe out the immune system’s memory of past illness,’” wrote Darryl from Virginia. “I heard it was the opposite. Did you mean that the vaccine wipes out your immune system?”
What Darryl had heard is, in fact, reversed. Contracting measles can impair the immune system through a phenomenon called immune amnesia. The measles, mumps and rubella (MMR) vaccine prevents infection and therefore stops individuals from losing their immune memory.
In 2019, an international group of researchers published a landmark study in the journal Science. They took blood samples from children before and after contracting measles. After measles infection, unvaccinated children lost 11 to 73 percent of the antibodies against other viral and bacterial diseases. Vaccinated children did not lose these antibodies.
The researchers later documented that children with immune amnesia can regain lost immunity, but this takes months or years. During that period, these kids are at elevated risk for contracting diseases, including ones they previously suffered or were vaccinated against. The possibility of immune amnesia is more reason to avoid measles infection through vaccination.
Bill from North Carolina, a pediatrician, says he is treating numerous children who fell behind in their immunization schedule. He asks: “Can you please remind your readers that it’s possible [for kids] to make up their shots?”
The Centers for Disease Control and Prevention publishes a recommended immunization schedule that describes which vaccines children should receive and by what age. Kids should get the first dose of the MMR vaccine between 12 and 15 months of age and the second when they are 4 to 6 years old. Those who missed one or both shots can and should make them up. The second dose can be given as soon as 28 days following the first dose.
Many readers wanted to know if they, as adults, need additional MMR shots. Anne from Massachusetts inquired how long immunity lasts; she had measles as a young child, but that was more than 80 years ago. Stephanie lives in Texas and is concerned about the outbreak in her state. “Should I try to get a booster dose for myself and my family?” she asked.
Both prior infection as well as MMR vaccination are thought to convey lifelong protection against measles. Anne should still have protection because of her childhood measles bout.
The answer is less straightforward for Stephanie. Whether she and her family should receive additional doses depends on their age and number of past vaccines.
Measles was so prevalent before 1957 that everyone born before then is presumed to have had the virus. Those who received two doses of the live attenuated measles vaccine, which became the norm in 1968, do not need a third.
But those who were born after 1957 and were vaccinated before 1968 should get revaccinated to receive the more effective vaccine. And people who received only one dose of the MMR vaccine should consider a second. One shot is 93 percent effective against measles; the second increases protection to 97 percent.
John from Maryland wonders why a measles outbreak should concern those who are vaccinated. “Everyone in my family is vaccinated. My grandchildren are grown. Is it really a big deal if other people choose to not jab their kids?”
Essentially, John is asking why we should care about the return of measles. Two reasons: Though 97 percent effectiveness against infection is high, it’s not perfect. Breakthrough infections are possible. The more virus there is in a community, the more likely someone who is fully vaccinated could contract it, too. This has already happened in Texas, where five of the people who were infected are vaccinated.
Second, many people cannot be vaccinated and would be at high risk if measles were circulating in their area. This includes newborns and individuals with severe immunocompromise. These people are most likely to become severely ill from measles. In other words, those who are capable of getting vaccinated have an obligation to do so to protect the vulnerable.
There are already many respiratory viruses that can cause significant illness in the United States. Measles used to be one of them. What a shame it would be if it returned as a threat and infected Americans — not just those who chose to be unvaccinated but also others who want to protect themselves but cannot.
27 notes
·
View notes
Text
by Jamie White
A bizarre experiment funded by the Bill & Melinda Gates Foundation developed a new vaccine strategy using mosquito bites as a delivery vector in pursuit of developing a “next generation” malaria vaccine.
The experiment was conducted by researchers at the Leiden University Medical Center (LUMC) in Leiden, Netherlands, and published last month in the peer-reviewed New England Journal of Medicine.
Researchers explained how they used the bites of mosquitos to deliver a short-lived malaria vaccine comprised of genetically modified malaria parasites.
“We conducted a double-blind, controlled clinical trial to evaluate the safety, side-effect profile, and efficacy of immunization, by means of mosquito bites, with a second-generation genetically attenuated parasite (GA2) — a mei2 single knockout P. falciparum NF54 parasite (sporozoite form) with extended development into the liver stage,” the researchers stated.
The Plasmodium falciparum (P. falciparum) parasite causes malaria in humans.
The method was meant to boost immunity through bites from mosquitoes carrying a genetically engineered version of the parasite that causes malaria.
First, researchers bioengineered two different types of malaria parasites for the experiment, GA1 and GA2.
GA1 was “designed to stop developing about 24 hours after infection in humans,” but had limited effectiveness, leading to the development of GA2.
GA2 was “designed to stop developing about six days post-infection, during the crucial period where the parasites replicate in human liver cells.”
The experiment was carried out in two stages.
26 notes
·
View notes
Text
Morning Israel News Summary
ISRAEL REALTIME - Connecting to Israel in Realtime
♦️MAJOR COUNTER TERROR OP.. IDF drone strikes a terror operations center in Nur a-Shams (Tulkarm area). 5 terrorists eliminated, including 1 (another report says 3) released in the last hostage deal. Multiple semi-official statements that the IDF has started a major multi-week counter-terror operation throughout Judea-Samaria.
▪️KIDNAPPING INCIDENT IN SAMARIA at Tapuach Intersection, cleared. The IDF: the suspicion of kidnapping has been ruled out.
⭕ ROCKET STRIKES by HEZBOLLAH in Ayelet HaShachar in the north hit homes and start a large fire.
▪️MANY ANGRY.. people, leaders and evacuees from the north are VERY angry that the government and IDF only performed a major strike against Hezbollah once Tel Aviv was threatened. In a sarcastic response, a number of towns have replaced their town signs with “Tel Aviv”.
▪️USING HUMAN SHIELDS.. IDF spokesman in Arabic: 90% of the launches carried out the night before last by Hezbollah were launched from the heart of a civilian population and near civilian facilities. In the attack, of the about 230 launches and about 20 suicide drones, 90% were launched from the heart of a civilian population, near civilian facilities - mosques, schools, UN compounds, and more.
▪️PROTEST - FOR A DEAL.. Demonstrators affiliated with the 'Headquarters of the Kidnapped Families' blocking Ayalon south near the Shalom interchange this morning.
▪️BEWARE SHEIN CONTACT LENSES? Ch. 13 reports of people arriving in the emergency room due to quality problems with contact lenses order through Chinese discount site Shein.
▪️GAZA POLIO VACCINE DANGER? An unusual notice from Israeli health professionals - the polio vaccine sent to Gaza by the UN WHO is an experimental live attenuated vaccine that has the possibility of spawning actual polio cases - which can then spread.
▪️BUS vs. CAMEL.. an accident on Negev roads, bus vs. camel. Drivers in the Negev and headed to/from Eilat are warned to beware wild camels, particularly at night.
▪️TERROR - STONING AMBUSH - SAMARIA.. Lynching attempt in Hawara: Arab rioters attacked a car driven by a Jewish woman from both directions and pelted it with stones. The driver managed to escape from them and miraculously was not injured (the car, however, badly damaged).
▪️JUDGES.. High Court of Justice in the decision against Justice Minister Levin: If you do not convene the committee, you will receive a ruling in September that will oblige you to do so.
.. The minister responds: the decision is expected, conflict of interest and lack of authority. They are their own judges, actually taking over the committee completely, refusing to accept anyone who is not from their own inner circle.
🔹ANOTHER IRANIAN AIRSPACE NOTICE.. effective September 1, 2024, at 00:00 (midnight) - for 3 days.
🔹US Joint Chiefs of Staff: The chances of an all-out war in the region have decreased after the attack carried out against Hezbollah.
⭕ 2 rounds of ROCKET attacks by HEZBOLLAH at northern towns overnight.
#Israel#October 7#HamasMassacre#Israel/HamasWar#IDF#BDE#Gaza#Palestinians#Realtime Israel#Hezbollah#Lebanon
10 notes
·
View notes
Text

🦟 Bill Gates turns mosquitoes into ‘flying syringes’, but who controls what they inject?
A Bill Gates-funded center has bred mosquitoes capable of injecting parasites into unsuspecting humans under the pretext of vaccinating against malaria. But are they truly harmless?
🌏 The Gates Foundation-backed Leiden University Medical Center in the Netherlands has developed a method of malaria vaccination using mosquitoes to deliver live-attenuated Plasmodium falciparum parasites.
🌏 The mosquitoes act as ‘flying syringes’ to deliver malaria vaccines – or potentially other substances.
🌏 But concerns have been raised that recipients could be unaware of the process and be vaccinated without their consent.
How it all began:
🔴 In 2008, Gates pledged $168 million to develop a next-gen malaria vaccine. Jichi Medical University in Japan received funding to genetically modify mosquitoes that can pass a malaria vaccine protein into a host.
🔴 In 2016, Gates announced a joint $3.7-billion initiative with the British government to combat malaria.
🔴 By 2018, Gates-funded Oxitec was developing genetically-modified male mosquitoes whose offspring with wild females would die before adulthood.
🔴 In both cases, scientists raised concerns over the lack of comprehensive studies of environmental, health and ethical risks.
Once Pandora’s Box is open, it cannot be closed:
🔴 If issues of human consent and ethics are overlooked, insects could be used as ‘vectors’ for other biological agents.
🔴 But who guarantees they carry life-saving vaccines and not harmful pathogens? It would be impossible to verify the exact contents of the ‘flying syringes.’
Mosquitoes as deadly weapons:
🔶 Insects have previously been studied as potential carriers of viruses and bacteria.
🔶 Nazi Germany reportedly developed malaria-carrying mosquitoes as bio-weapons at Dachau.
🔶 The Pentagon is said to have conducted similar studies in overseas bio-labs, including in Ukraine, according to assassinated Russian Lt. Gen. Igor Kirillov.
🔶 Kirillov revealed that US biolabs in Ukraine studied viruses transmitted by mosquitoes, including dengue fever. That was also referenced in a lawsuit filed by Cubans following the 1981 dengue epidemic in the country, where the only area unaffected was around the US naval base in Guantanamo Bay.
#blacklivesmatter#blackvotersmatters#donald trump#joe biden#naacp#blackmediamatters#blackvotersmatter#news#ados#youtube
4 notes
·
View notes
Text
instagram
Okay, I have to say something.
One of the main problems of current medicine is not the amount of antivaxxers, but the division of society on pro-vaccines and anti-vaccines. And people like this scientist on the video are only expanding the abyss further and futher - in long run, causing more and more people losing faith in vaccinations and in medicine in general. Why, you ask me?
Because the problem of post-vaccinations' complications didn't disappear anywhere - moreover, it only became bigger.
For the last two decades, people went absolutely nuts, vaccinating everything regardless of time periods between shots, the age, the sex, the overall ability of a pathogen to mutate, etc. It was our absolute failure as of the worldwide medical community - and the best proof is the Covid vaccine and its effect.
But enough about Covid. Let's take another example - the MMR vaccine: live-attenuated, three doses, mostly applied to children at 12-15 months. My friend had one at 12 moths, too - however, back then, ~20 years ago, her parents noticed strange movements of her, after the first doze. She arched her back and did not respond to external stimuli. Her parents didn't attach much importance to it. After the second doze (she was already 4 year-old), she developed severe seizures. She was diagnosed with convulsive syndrome, and she had to take Convulsofin (Valproic acid) for 3 years. If you didn't know, Valproic acid is extremely hepatotoxic and can cause acute pancreatitis, thrombocytopenia, hyperammonemia, coma and death. It was also pretty expensive back then. My friend was prescribed of such medication because anything weaker just didn't improve her condition at all - and her neurologist assumed it would be easier for a child than for an adult to adapt and overcome such a dangerous drug. Luckily, she had survived, but she remained disabled for the rest of her life, even though her parents paid crazy amount of money on rehabilitation. Even nowadays, when we occasionally meet, she sometimes flinches and then complains of a headache. Obviously, her quality of life is pretty impaired and has lots of restrictions.
20 years ago, despite there were MANY of such cases, there were no public researches, publications, algorithms "what to do if" - in Ukraine, I mean. It looked as if there was an order from above to keep silent about everything that was happening. Nowadays, the World Health Organisation writes "febriles may occur but they are typically short-term and do not lead to long-term neurological issues" - I want to show them my friend and ask whether they can pay off her medications and rehabilitation costs for all these years. Because there are no long-term issues! There is no war in Ba Sing Se. Maybe it was just her parents' whim - to waste so much money!
The problem of modern medical system is that no one cares what will happen to you, to your child, after vaccination.
You are not listened to, you are labelled immediately as "antivaxxer" - and if you decide to vaccinate, and it gives you severe complications, and you manage to NOT die because of them, all the doctors around are like:
"Welp, it's your problem now. Who cares if you have to pay for rehabilitation from your own pocket - at least you are an acceptable member of society now!"
Is it really that surprising that between "possibly getting ill" and "assurely getting ill after vaccination", a parent usually chooses the first option for their child? Especially if they know that the risk for complications runs in the family? They do not vaccinate you with some random bacteria but with weak versions of the pathogen - the live-attenuated vaccines are the most heavy to deal with. The overload of immunity does exist and can happen after vaccination - and denying the problem because it is being spoken by the person you don't like is a very immature, very unprofessional behaviour, especially from a doctor/scientist.
There is no compensation for developing complications, there is no genetic screening for a vaccine's safety, there is no emergency help algorithm, there are no rehabilitation programs, hell, there is no education about post-vaccine complications treatment and prevention even. There are no safety guarantees. There is probably no improving of vaccines either.
And then they wonder why people vote for drug-addicted fashists like Trump and Elon Musk.
People are not lab mices. People should have a choice whether to apply medication or not. Just because complications are rare doesn't mean they must be ignored. People should not be ostracised for not wanting to vaccinate. There are people like my friend for whom ANY vaccination is strictly contraindicated for the high risk of complications' reccurance - to vaccinate them is the same as to execute them - but no one listens to them, although its our job as doctors, as scientists - not be indifferent. Indifferent doctors are called flayers, slaughterers, human experimentation perpetrators, sometimes even war criminals.
The guy on the video is indifferent. So is Elon Musk, however, he just simply broadcasts the thoughts and feelings of millions of people around the world, whose loved ones had to suffer from such medical indifference and ostracism. Because those farmaceutical oligarchs are interested in incitement of conflict and hatred between the two sides, in selling as much stuff as possible - regardless whether it's useful and safe - those guys are no different from Elon Musk at all, except for being more two-faced.
In conclusion:
We must not spread hatred. If a person doesn't want to vaccinate, listen to their arguments - maybe they have a good reason for that. Don't be blind, be kind.
We must develop safety guarantees and/or compensation for people who get complications after vaccination. Low risk doesn't mean your loved one won't be a victim of it.
We must educate people about what to do if you develop severe reaction on a vaccination. Ignorance breeds mistrust and ruins the belief in doctors. If the parents of my friend were educated, they wouldn't have ignored the first signs, they wouldn't have done the second shot - and my friend wouldn't have become a disabled for life.
We must not force people to vaccinate unless it's a 100% death-rate disease. We are not Auschwitz.
We must not spend so much time on Internet. We must not divide the society for likes, kudos, reblogs, views, whatever.
2 notes
·
View notes
Text
The Live Attenuated Vaccines Market in 2023 is US$ 7.85 billion, and is expected to reach US$ 17.47 billion by 2031 at a CAGR of 10.52%.
#Live Attenuated Vaccines Market#Live Attenuated Vaccines Market Research#Live Attenuated Vaccines Market Report
0 notes
Text
2 notes
·
View notes
Text
We have "aliefs" and "beliefs" - let me introduce "celiefs": something that we worry *has a high chance of being true*, but aren't quite convinced of.
Often this is something that society/experts/someone you admire says is true, but you don't see the reasoning behind.
We may look for evidence that might convince us of the celief, or behave as if we already believe the celief; this is not exactly performative, but more like an act of "hedging" -- so that if the celief turns out to be true, we've avoided causing harm. We would do this regardless of whether people see it, but it can still feel "disingenuous" since we haven't exactly internalized the celief that we're acting on.
____________________________
This seems like it might be the difference between OCD themes and attenuated* delusions: You alieve your attenuated delusions while you celieve your OCD theme
* attenuated delusions meaning delusions you're capable of questioning. They become full-blown delusions sometimes. But they seem categorically similar, so I feel like the correct line to draw is [alief vs celief] rather than ["truly believe it" vs "know rationally that it's false"]
_____________________________
Some celiefs you might hold include:
vaccines work/covid is real
global warming is real
race/gender is a social construct
racism/sexism/etc exists
victims are telling the truth
homosexuality is bad/a sin
you will go to hell for doing bad things
i am the real abuser
i'm faking my mental illness for attention
i'm virtue signaling; only pretending to care/understand/be sorry/etc
my intrusive thoughts are who i am deep down
i was abused because i wanted it
Celiefs can be good or bad; sometimes it's good to hedge your bets on something you don't know much about and trust the people who have lived/studied the thing, but celiefs are also how people gaslight you.
I would classify anything that you maladaptively act upon but want to work through in therapy as a celief rather than a belief (if you really believe it, you wouldn't want to work on trying to not believe it, because from your perspective that would be deluding yourself)
7 notes
·
View notes