#sars-cov-2
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Text
Image description: 4-panels format. A Jenga game tower with more and more blocks removed until it collapses. In each of the panel the tower is accompanied by the texts "How many"; "infections"; "will it"; "take?" Watermarked by @haziethompson

#image description#described image#image described#long COVID#SARS-CoV-2#COVID#COVID-19#reinfections#multiple infections#pandemic is not over#resist eugenics#COVID is not over#still COVIDing#meme
301 notes
·
View notes
Text
Today is the third annual Long COVID Awareness Day. Here are some posters from @edania, a mutual from another site.
The original posters, prior to the edits, are from ACT UP during the AIDS-HIV denialism and the queer genocide under the Reagan administration,. This time, they're repurposed for COVID-19 or SARS-COV-2.

Source: Cohost/@edania (via Wayback Machine)

Source: Cohost/@edania (via Wayback Machine)
I am not able to find the original "Where Is Your RAGE" and "CDC Kills" posters (access denied) from mx. papaya which inspired the above posters. You can download free agitprop from mx.papaya's Ko-Fi.
#Long COVID Awareness Day#Long COVID#COVID#COVID-19#SARS#SARS-CoV-2#Mask Up#ACT UP#Protect Each Others#Resist Eugenics#CDC Kills#agitprop
219 notes
·
View notes
Text
Common Symptoms Were Fatigue and Decreased Exercise Tolerance, According to a 2022 Survey
Inequities In the Prevalence and Severity of Symptoms Observed Across Race, Ethnicity, Gender, and Neighborhood Poverty
December 26, 2024 — Today, the New York City Health Department announced that 80 percent of adult New Yorkers infected with COVID-19 who were surveyed experienced at least one symptom lasting one month or longer. According to the results of the COVID-19 Experiences Survey in 2022, the most common symptoms were fatigue and decreased exercise tolerance. While post-acute symptoms may resolve within 12 weeks, many people will go on to develop Long COVID, an infection-associated chronic condition characterized by symptoms lasting three months or longer.
“This survey shows us that the symptoms following COVID-19 infections are a significant public health issue for New Yorkers. Black and Latino communities, women, transgender people, and those living in low-income neighborhoods were more likely to have symptoms, highlighting the disproportionate impact of the pandemic on marginalized communities,” said Acting Health Commissioner Dr. Michelle Morse. “We must invest in a comprehensive long-term response to the COVID-19 pandemic that focuses on prevention through engagement with health care providers and community members. Services for people experiencing the long-term physical, mental, social, and economic impacts of COVID-19 infection should be accessible to all.”
Post-acute symptoms are those that last one month or longer. To better understand experiences of COVID-19 post-acute symptoms, the Health Department conducted the COVID-19 Experiences Survey in November and December 2022. Adult New Yorkers who were members of the probability-based NYC Health Panel were invited to take the survey if they had confirmed or suspected COVID-19; 2,081 people completed the survey online or by phone in English, Spanish, Russian, Simplified Chinese, or Traditional Chinese. The results provide insight into how post-acute symptoms relate to health care seeking, social and demographic factors, disability, and mental health.
Some respondents reported many symptoms at different levels of severity, while others reported few symptoms, only mild symptoms, or none at all. Inequities in the prevalence and severity of post-acute symptoms after COVID-19 were observed across race/ethnicity, gender, and neighborhood poverty levels.
The prevalence of mild symptoms was similar across socio-demographic groups.
Moderate symptoms were more prevalent among Latino and Asian/Pacific Islander adults compared with white adults, and among people living in high poverty neighborhoods compared with people in low poverty neighborhoods.
Severe symptoms were more prevalent among women and transgender or non-binary adults compared with men, among Latino and Black adults compared with white adults, and among people living in very high and high poverty neighborhoods compared with low poverty neighborhoods.
Increasing symptom severity was associated with activity limitations and depression. Those with at least one severe symptom were more likely to report activity limitations compared with those who reported no post-acute symptoms (60 percent vs. 6 percent), which may result in social, economic, and mental health difficulties.
People with at least one severe post-acute symptom reported 10 days of reduced ability or complete inability to carry out usual activities or work in the past month, compared with 6 days for moderate symptoms, 3 days for mild symptoms, and 1 day for no symptoms.
One in three adults (33 percent) with at least one severe post-acute symptom after COVID-19 had probable depression, higher than those reporting only mild symptoms (6 percent) or no symptoms (2 percent).
Black and Latino New Yorkers, women, transgender adults, and those living in low-income neighborhoods were most likely to report severe symptoms, reflecting the disproportionate impact of the ongoing pandemic in these communities.
To address inequities in awareness about the long-term health impacts of COVID-19 and the importance of preventing new infections, the NYC Health Department partners with community and faith-based organizations to serve as trusted messengers and provide tailored and culturally resonant public health outreach to NYC communities.
Anyone can become very sick from COVID-19. To find a COVID-19 or flu vaccination site, visit nyc.gov/vaccinefinder or call 212-COVID-19 (212-268-4319).
#031-24
MEDIA CONTACT: Chantal Gomez PressOffice@health.nyc.gov
Gomez, Chantal. “Health Department Finds Most Adult New Yorkers Infected with COVID-19 Experienced Symptoms Lasting One Month or Longer.” Health Dept. Finds Most Adult NYers Infected With COVID-19 Experienced Symptoms Lasting 1 Mo or Longer - NYC Health, NYC Health, 26 Dec. 2024, www.nyc.gov/site/doh/about/press/pr2024/nyc-adults-with-covid-19-experienced-symptoms-one-month-or-longer.page.
I’d like to highlight that date: December 26, 2024.
#op#links#usa#nyc#public health#covid#long covid#covid-19#sars-cov-2#sars cov 2#covid19#covid 19#long covid awareness#covid isn't over#still coviding#covid conscious#pandemic#coronavirus#covid pandemic#coronavirus pandemic#infectious disease#infectious diseases#disability#chronic illness#post-acute covid-19#covid cautious
50 notes
·
View notes
Text
where do i find a graph showing COVID stats (preferably wastewater, but hospitalizations and deaths and whatnot would be useful too) over the past several years? maybe even all the way back to 2020? please? when you only see a few months at a time, it's hard to put into perspective in the grand scheme of things.
#op#covid#covid tracking#covid-19#covid cautious#covid conscious#covid realistic#covid 19#covid awareness#covid careful#covid is not over#covid is still a thing#covid is still here#covid isn't over#covid kills#covid19#zero covid#sars cov 2#still coviding#covid safe#sars-cov-2#sorry for the tag spam#i want as high a chance as possible that i get a good answer
22 notes
·
View notes
Photo

Study reveals how SARS-CoV-2 triggers diabetes by destroying pancreatic cells
Researchers from Weill Cornell Medicine have used a cutting-edge model system to uncover the mechanism by which SARS-CoV-2, the virus that causes COVID-19, induces new cases of diabetes, and worsens complications in people who already have it. The team found that viral exposure activates immune cells that in turn destroy beta (β) cells, the pancreatic cells that produce insulin. The study was published Sept. 2 in Cell Stem Cell.
25 notes
·
View notes
Text

side-eyeing all the anti-vaccine, anti-masks, "get back to normal," "the kids will be fine" fucktwats hella hard right now. fuck everyone one of you.
#COVID#brain health#cognitive deficits#memory problems#brain inflammation#brain aging#brain volume#brain structure#COVID-19#SARS-CoV-2#long COVID#brain damage#dementia#autopsies#respiratory virus
92 notes
·
View notes
Text
This is so fucking bleak. At 1/10 infections causing long term consequences, the mass disabling event we’re in is so massive I was wondering how it was going to be handled, because surely it would need to be addressed eventually… it appears that “addressing” has begun, and instead of prevention or support it’s just wholesale dismissal. If you haven’t yet stepped up yet for the disabled (and not yet disabled) people around you, now is the time to start, because if this is the direction they’re going then truly no one is coming to save us.
31 notes
·
View notes
Text

4 notes
·
View notes
Text
Excerpt from the above link:
First thing’s first. If the phrasing in the title feels unfamiliar, it has a purpose: We are eliminating the passive voice from the pandemic. Right now.
Someone INFECTED Neil Gaiman with COVID-19.
And many someones in overlapping layers of responsibility ENABLED this infection.
This linguistic shift from the passive to active voice might seem irrelevant but, instead of just echoing the framing we see in the headlines — that Neil Gaiman got COVID-19— it’s time to own that somebody has infected Neil.
The passive voice has served a macabre purpose in this pandemic. The passive voice, by erasing the subject of the sentence, neatly obscures accountability, and with it our own role in unmitigated infections. Moreover, it has prevented us from identifying the layers of responsibility in enabling infections on a mass scale. This mental block is the first obstacle to advocating for effective mitigations and constructive solutions. It stops us from preventing infections. But that is changing now.
It is time to own the damage that we are causing by infecting others with COVID-19. I believe that we all know, deep inside, that we are causing harm. And many of us are suffering from the cognitive dissonance of pretending that we aren’t. Because, in a pandemic, this is serious and large-scale harm.
This harm that, according to estimates, has killed over 25 million people and disabled at least 65 million and counting. The sooner we face the harm we are causing by infecting other people, the less damage we will cause to ourselves, to our loved ones, to our community, to strangers on the other side of the world. And to people who entertain and inspire us, like speculative fiction author and TV creator Neil Gaiman. And inspiration is necessary when we are facing so many challenges. It’s that simple.
COVID-19 is a serious, multi-system vascular disease that creates severe and cumulative damage.
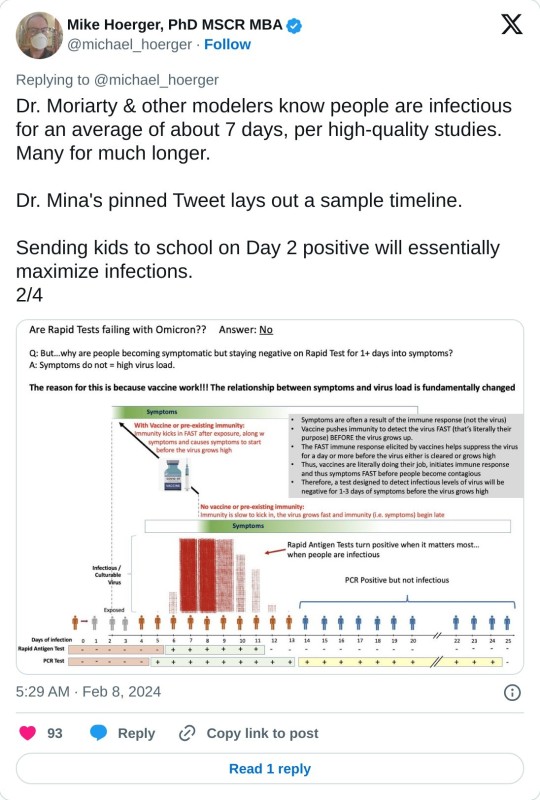
Reinfections tend to be more severe and Long COVID occurs in 1/10–1/3 infections.
Up to 60% of infections are spread asymptomatically… Wait, let me rephrase that. People, who are asymptomatic, or presymptomatic, are infecting others with COVID-19 in up to 60% of cases.
A person who is presymptomatic can transmit a COVID-19 infection up to two days before symptoms arise.
People infect other people with SARS-CoV-2 through aerosols. An infected person expels them just by exhaling. The aerosols accumulate in the air, and spread across large spaces like cigarette smoke. They also remain in the air for hours, so even if a room is empty, if a symptomatic person was there earlier, the aerosols will still be there. Crowded, indoor spaces are high-risk for transmission.
We are currently in a wave caused by a new variant for which a vaccine has yet to be developed. In a crowd of 100, statistically 1-2 people will have active infections.
If we put all of this together, we see that live events in crowded, indoor spaces are particularly dangerous, and that masking only when someone is symptomatic is woefully inadequate to prevent infecting others. So, in order to not infect other people, we need to individually mask at these events, and to collectively apply pressure to venues that are enabling these infections, as well as to lawmakers who have removed protections.
That’s the tl;dr. Now, if you have some time, and feel motivated to prevent further infections, let’s look more systematically at the problem of people infecting other people, especially at live events, and how to constructively address it.
Neil Gaiman requested masking at his events, from both venues and audience members
It’s fucked-up that, three days after Neil Gaiman requested that attendees voluntarily mask at his tour events — because the venues themselves refused to enforce audience masking — Neil announced on social media that he has another COVID-19 infection and “this time it means business.”
This infection — and any COVID-19 infection — is terrible, but unfortunately not surprising. We are in a wave caused by multiple variants, and lawmakers worldwide dropped most COVID-19 public health mitigations earlier this year. So people who are appearing at live events now are at an incredibly high risk of being infected. The risk is also increased due to a swarm of new variants — so many versions of the virus are circulating now, you can get a case in August and another in September
As a fan of Neil Gaiman, I guess I wished that somehow it would miss him. COVID-19 infects the brain, and his brain has created my favorite TV series, Good Omens, a queer love story between an angel and a demon. This series has helped me, and countless others, heal from religious trauma. It also rekindled my appreciation for David Tennant in his role as the demon Crowley, who witnesses everything from Old Testament atrocities to a modern-day armageddon, and seems to be the only one suggesting that God might be a tyrant. With so many of us experiencing a dark night of the soul in the pandemic, it’s much-needed validation.
What also worries, but not surprises, me about Neil’s infection is that, if his statement that “this time it means business” is anything to go by, (especially for someone who can be quite understated), this infection is more severe than any previous ones. This unfortunately is also not surprising, as reinfections tend to be more severe. The damage from these infections is cumulative, and SARS-CoV-2 attacks the immune system, in many cases after a person has recovered from an initial infection. Viral reservoirs continually attacking the body are believed to be the mechanism of Long COVID. However, his more severe course reminds me of other performers who are currently touring, almost without exception at massive, indoor, unmasked events.
Actually, it’s more accurate to say that it scares the hell out of me.
Actors from another TV series beloved by queer fans, Our Flag Means Death, including Rhys Darby, Vico Ortiz and Samson Kayo, will appear at London Comic Con on October 27–29th. The event will have more than 100,000 attendees and does not require masks. And David Tennant, who sparked my motivation to advocate for safer venues, will appear at New York Comic Con October 12-15th. NYCC will have over 200,000 attendees and also does not require masks. I checked.
The math on the likely damage is pretty fucking grim.
It’s estimated that in a crowd of 100, 1–2 people have a COVID-19 infection. So that’s at least 2,000 attendees spreading the virus.
Each person infects 2–3 other people. This is total, so they may not infect people at this event. But because the venue is extremely high risk: indoors, crowded, no mitigations, they may infect more people than averge.
So, from 2,000 people who go to Comic Con with infections, that’s at least 4,000 people that they will infect.
Between ⅓–1/10 infections result in Long COVID, so at least 400 people statistically may develop Long COVID. From one event.
tl;dr 200,000 attendees/100= 2,000 infections x 2= 4,000 newly infected/10 =400 Long COVID cases
And that’s the conservative estimate. The upper-end estimate, based on data, is up to 2%.
You can bet that I’m well-aware that David Tennant has a .2%-2% chance of developing Long COVID from this one event, especially because he’s due to play MacBeth in London this winter. The luckiest person who ever existed would statistically develop Long COVID after their 50th event.
It’s not just headlining performers who need to worry about infections. Any attendee has a .2% chance of developing Long COVID from this one event, and that’s a tragedy in the fan community, but also for people working on staff who don’t choose to be there. I wonder what would happen if the damage were immediately visible, like setting fire to 400 guests, fans, and staff people at the door. What then?
If you have read my first article sounding the alarm on unprecedented numbers of performers becoming seriously ill and dying in the pandemic, you will know that my own fannish devotion to David Tennant inspired me to advocate for COVID-19 mitigations at venues and nourishes me with the love and compassion to do this work. With Neil Gaiman’s infection, it hits home that everyone who is currently doing live events, particularly large ones with no mitigations, are quite likely going to be infected. And in the fourth year of the pandemic, that means reinfected, which means that, like in Neil’s case, it will probably be more severe.
Performers are just my own corner of advocacy, but we all breathe the same air, so these new infections will affect everyone. And people with disabilities, who work in service and customer-facing jobs, or who have inadequate access to medical care, will be the most vulnerable. But most people now have had at least one infection, so we’re all facing danger here.
This is why I want to prevent people from infecting people at events, and by doing so to raise awareness in the wider public that this is an escalating emergency. And I think it’s achievable.
The first step is identifying the causes, both individual and structural. Then to come up with workable interventions at each point of responsbility.
Individual responsibility: someone infected Neil Gaiman with COVID-19
Preventing infections begins at the individual level. As the founder of #FansMASKUP, which is dedicated to raising awareness in the fan community about masking at live events, my first feeling was rage at the person who infected Neil. The incubation period for COVID-19 varies widely, from 2–14 days, though on average 5–6. So, if Neil developed symptoms on October 5th, it’s possible that someone in the audience on the October 2nd event infected him. And if that person is such a fan of Neil that they paid to see him live, I ask: why didn’t they just wear a mask? But even this is not so simple.
From my conversations with other fans who have been diligent about masking, they sometimes experience harassment, and fear for their safety and mental health. And since so many of us are LGBTQIA+, neurodivergent, BIPOC and/or disabled, we are statistically more vulnerable to people harassing us, or even assaulting us, if we are the only ones masking. So as much as I’d like to judge this person for infecting someone who they admire, I have to admit that safety is too often a real concern for our community.
What can we do on an individual level to promote safer venues?
If we feel sufficient safety to mask at live events, then we should do so.
If we are going with friends, we can encourage them to mask too.
We can connect on social media and find other fans who are attending and mask together.
Heck, if we have a spare $20 (which not all of us do), we can even give out masks at the event so that we’re not the only one.
Aside from fear and social pressure, people may have stopped masking due to exhaustion, despair and misinformation — we MUST start again. Every masked person can break a chain of transmission and save many, many lives. Maybe even Neil Gaiman’s life, and certainly the lives of your loved ones, including fellow fans.
Institutional responsibility: venues are enabling people to infect other people with COVID-19
It would be a mistake to lay all of the responsibility on the person who infected Neil. There has been systemic neglect, and even malfeasance, at every level of responsibility, and the people who are making these decisions are enabling people to infect others. Though this reaches into the level of policy, let’s begin with the most direct enabler in this instance: the venues.
Remember, Neil said on social media that he requested audience masking at venues, but they refused. Then after his first tour date, he announced that someone had infected with with SARS-CoV-2. We can’t know whether someone infected him at this particular event, though the timing is consistent with the virus’s incubation period. Regardless, the venue has approximately 1,700 seats, and if Neil’s event was sold-out, as most are, that’s: 17 active infections, 51 new infections, 5 cases of Long COVID. So wherever someone infected Neil with COVID, it is worthwhile to advocate for venues to use mitigations.
The mitigations required to significantly reduce people infecting other people at live events are relatively simple and have been proven time-and-again to reduce the the transmission of SARS-CoV-2:
Audience masking and vaccination
Making use of HEPA air purification/filtration.
This is achievable, and venues should have been doing this since 2020. Some venues do it, and it is certainly possible, and not terribly complicated, for more venues to adopt these simple precautions.
Now, the more complex question is: if it’s so simple, why are venues refusing to use mitigations? Some of it is simply greed. It costs money, though not a lot of money, between £300–600 ($370–740) to purchase a HEPA air filter. And for truly cash-strapped venues, vendors likes Smart Air UK are renting out HEPA air filters for events. So there really is no excuse. For those who are unfamiliar with HEPA, here’s a primer from outreach coordinator (and fan herself) for Smart Air UK, Guilia Villanucci.
I’m quoting at length, but tl;dr: HEPA purifiers can remove more than 99.97% of virus particles from the air, and protecting Neil at one of his events would only have cost between $400-$700. And you can’t put a price on his brain, so…
HEPA stands for “high-efficiency particulate air.” HEPA air purifiers are nothing else than a box with a filter and a fan inside. Researchers agree that, based on their efficiency, air purifiers can remove more than 99.97% of virus particles from the air when used continuously. Now, does this extra layer of protection have to be very expensive? It can be, especially if you look only at brand names without paying attention to the technical specifications. I recommend Smart Air products, partly because I work for Smart Air UK, but mostly because these air purifiers are cheaper than most on the market, are highly efficient, and are pretty quiet. NOTE: If you are a performer based in Chicago, USA, you should check out Clean Air Club, they loan air purifiers at no extra cost to artists and touring musicians. If you are a venue or a performer based in the UK, you can rent air purifiers from us, or purchase them to take them on tour with you, just like singer and songwriter The Anchoress does. An investment of between £300 to £600 will probably be enough to keep performers safer in a venue if you purchase from Smart Air UK.
Again, HEPA air purifiers are effective and affordable and I can only think a noxious mix of greed, inertia and denial are preventing most venues from using this basic precaution.
There may be other financial considerations. Requiring masks could lead to lost revenue as people who refuse to mask will not attend. And, as of yet, venues face no financial liability for enabling infections. Though with lawsuits winding their way through courts regarding liability for COVID-19 infections, this may change.
However, like fans, venues may also have legitimate concerns for safety, The far-right has so politicized masking that the people responsible for venues are likely afraid of repercussions, ranging from the awkwardness of barring an unmasked person from attending an event, to someone throwing a brick through the window, or even assaulting a person on staff. These fears are not entirely unreasonable. But we need to make clear that these venues are enabling people to infect their headliners, Neil Gaiman or David Tennent or Taylor Swift. Additionally, lack of mitigations endangers attendees and people on staff, and lawsuits against employers who have exposed employees to COVID-19 infection have had more success. This changes the risk calculation.
What can we do to encourage venues to create safer event spaces?
We can contact the venues themselves, beginning with the ones who likely are not using basic mitigations. These can be any venue where you or one of your favorites will be in attendance.
We can also start with the venues where Neil was scheduled to appear. Here is a list of these venues with the ways to contact them.
Emerson Colonial Theatre (888) 616–0272 boston@service.broadwayacrossamerica.com Twitter-X/IG: @BroadwayBoston
The Westport Library (203) 291–4800 Twitter-X/IG: @WestportLibrary
Cooper Union development@cooper.edu (212) 353–4100 Twitter-X/IG: @cooperunion
Peter J Sharp Theatre (212) 864–5400 boxoffice@symphonyspace.org Twitter-X/IG: @SymphonySpace
Dr. Phillips Center for the Performing Arts guestservices@drphillipscenter.org 407.839.0119 @DrPhillipsCtr
Venice Performing Arts Center information@vipam.org (941) 218–3779
Zoellner Arts Center at Lehigh University 610–758–2787 inzactix@lehigh.edu @LehighU @ZoellnerArts
Frikirkjan i Reykvavik+353 552 7270frikirkjan@frikirkjan.is @iclandnoir
Piggott Theatre (British Library) +44 (0)1937 546060 Customer-Services@bl.uk Twitter-X/IG: @BritishLibrary
New Jersey Performing Arts Center 1973–642–8989 ticketservices@njpac.org @NJPAC
If, like me, cold-calling gives you anxiety, here’s a script that you could follow:
“Hello, I am calling to ask what COVID-19 mitigations you use. [If they require audience masking and use HEPA air purification, consider thanking them for their conscientiousness. If they do not, you could say:] Neil Gaiman requested COVID mitigations at venues, but now someone has infected him. To prevent infections at your venue, I am requesting that you require audience masking and purchase a HEPA air purification unit. These are proven to significantly reduce COVID transmissions.”
I know, it’s a bit wooden, so feel free to improvise. But remember: please don’t harass these people, because most likely you will be talking to a staff person and not the person who has made the decision not to use mitigations. And if the person answering the phone is on your side, this has a better chance of success.
You can also request mitigations through social media and e-mails, although phone calls bring the most attention. But do what’s at your comfort level. Most of us who are aware of the ongoing pandemic are burnt-out and need to conserve our energy.
To sum-up, we need to hold ourselves and other fans accountable, but they face real risks and cannot be held wholly responsible. Same for venues. We need to apply pressure for them to adopt COVID-19 mitigations, but they are not wholly responsible. This brings us to the final level of accountability for people infecting other people with COVID-19.
Structural responsibility: governments are enabling infections by eliminating COVID-19 protections
The highest level of responsibility falls to governments, generally, and public health authorities specifically. It’s alarming how quickly people have reverted to using little-to-no precautions. But, remember, for many places lawmakers only eliminated public health protections within the past few months.
The state of affairs in which we find ourselves is not normal, and I think it is a brief interlude in which politicians and the very wealthy are encouraging us to continue with business-as-usual, but as those around us become sicker and sicker, we know that this is not sustainable. If 10%-30% of COVID-19 infections lead to Long COVID, and we conservatively assume that most people are infected once per year, what will that look like in ten years?
The most wide-reaching change required to stop people from infecting other people is on the level of policy. There is a basic social contract for governments to ensure public health because, in a complex society, individuals cannot carry that entire burden themselves.
In a simpler example: governments are responsible for putting stop signs at intersections. If a government legislated that there should be no more stop signs, people would get seriously injured or die in more car accidents. And we could blame the individuals who cruise their cars through the intersections and t-bone other people in their cars, or the city whose employees removed the stop signs — but the lion’s share of responsibility falls onto the government who legislated that there should be no more stop signs.
In the widest frame, we also need to advocate to our city, county, state, provincial and national lawmakers for a return of COVID-19 protections.
We also need to advocate for improved public health communication. It’s alarming how many people lack the basic facts of how not to infect themselves and each other with COVID-19.
In a nutshell: If you have learned anything new about COVID-19 from this article, that’s a problem.
**A concerned David Tennant fan should not be doing science communication that is the rightful job of public health officials.**
We need to pressure public health authorities to improve communication, and meanwhile to educate ourselves and each other about COVID.
What can we do to bring back COVID-19 protections on a societal level?
1. Call or write to your representative. By mail, if you can. I know, it’s a pain and an archaic throwback to pre-digital times, but this is most likely to be heard. But if it’s not possible, call or e-mail as it does make a difference.
Find your representative: US: https://www.house.gov/representatives/find-your-representative UK: https://members.parliament.uk/FindYourMP
2. Educate yourself and your community The Pandemic Accountability Index maintains a large repository of research on COVID-19 and its effects on the body here:
https://www.panaccindex.info/p/what-covid-does-to-the-body and here: What SARS-CoV-2 Does to the Body (2nd Edition, July 2023)
3. Stay updated on COVID news. Folks on social media have been sounding the alarm on the pandemic, like @1goodtern and performers specifically, like @MeetJess and me, @WaltzTales.
A twitter user has also kindly provided this list of scientists and concerned people worth following: @kprather88 (full credit to efforts to educate about all things covid) @jimrosenthal4 (C-R box, ’nuff said) @linseymarr (MacArthur genius grant https://forbes.com/sites/michaeltnietzel/2023/10/04/macarthur-foundation-names-the-winners-of-its-2023-genius-grants/?sh=6c3c96af4379… ) @joeyfox85 (mitigating airborne spread) @c19vaccinefacts (safe & effective) @scienceupfirst (not just covid!)
The final level of responsibility: the universe
This may sound a bit woo-woo, but if you read my first piece, which started with a loving-kindness meditation, you’ll have clocked that I think attending to ourselves emotionally is necessary for facing this emergency.
I honestly don’t know if there’s anything like a God who has an overview of the situation. And even though my Theology professor said the question of theodicy (“why is there evil in the world?”) isn’t a particularly interesting question, my answer is:
But *gestures broadly at everything.*
If there is a God they have a lot to answer for. But I do think that a real emotional crisis we’re facing is black-pilled misanthropy where we want to let the world burn, and all humans in it. But Neil Gaiman is a human. Whoever inspires us is a human. The feeling of being inspired in this particular way is your human experience. We humans aren’t more special than other animals. We only have the experiences that are unique to us in the landscape of all things, including high-concept science fiction from dynamic minds like Neil Gaiman’s.
I don’t think we should deny or suppress our feelings of despair and rage, or even hate, but to acknowledge and take care of them, and at the same time to nourish those aspects in us which support our joy and thriving.
It is possible to suffer and thrive at the same time. Perhaps if we could come up for a word for it, it would capture an essential strategy for moving forward with this pandemic. What do you think: Suffriving? Thrivering?
Let’s try leaning into some “Thrivering” together by advocating for safer venues, so that people like Neil Gaiman can continue inspiring us.
Special thanks to: Giulia Villanucci, Smart Air UK, Outreach Coordinator Nerdcake78 for the scoop. And for the slow-burn Aziraphale cuddlefic that is keeping me sane.
And everyone who is providing information, amplifying posts, and offering support. I would not be able to do this without the people who are helping out of simple kindness and solidarity.
#should have been more explicitly clear about this but too late to edit as it's been reblogged: this is an excerpt of someone else's article#this is not my own writing I am just quoting the link here#neil gaiman#david tennent#covid is not over#covid is airborne#covid is ongoing#pandemic#mask up#sars-cov-2#long covid#masks#covid#covid-19#long post
33 notes
·
View notes
Text
covid and canines

My mom sent this to me as a text so I don't have a source I'm sorry.
The image above is a blue background infographic that reads:
Covid and canines
key takeaways from the November 2023 study neurologic effects of SARS-CoV-2 2 transmitted among dogs
Canines catch it
all dogs in the trial were infected six were infected by nasal spray
Canines spread it
six dogs were infected via contact ( horizontal spread)
Canines may not show it
all dogs in the study were asymptomatic
Covid causes damage
all dogs in the study had short and longer term brain and lung damage
You can prevent infection
Break the chain
Wear an n95 or a respirator indoors.
Avoid interaction with dogs that are not protected from exposure.
Stay informed, share what you learn.
#Sorry for the poor formatting and low quality image description I'm on mobile and also very tired#COVID#mask up#coronavirus#pandemic#wear a mask#long covid#covid isn't over#covid 19#covid19#covid risk outside#covid pandemic#sars cov 2#SARS-CoV-2#Dogs#Dog illness#Dog flu#Dog COVID#Dog sickness#Canines#Canine flu#Canine illness#Canine COVID
17 notes
·
View notes
Text
Figured might as well post this here with mask bans becoming more common. The person who engineered the pandemic snorkel has ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) and cannot afford to get sick.
#COVID resources#COVID-19 resources#SARS-CoV-2 resources#pandemic is not over#COVID is not over#mask up#mask bans#COVID-19#SARS-CoV-2#COVID-19 equipment#SARS-CoV-2 equipment#COVID equipment
19 notes
·
View notes
Text

Louis, Claudia and Lestat say no pandemic and virus associated disease erasure, denial or lies, and not on International Long Covid Awareness Day of all days.
#Interview with the vampire#Interview with the vampire series#Interview with the vampire AMC#AMC#AMC+#Ongoing pandemic#SARS-CoV-2 pandemic#SARS-CoV-2#Louis De Pointe Du Lac#Claudia#Lestat De Lioncourt#GIF: interviewgifs#Coloring: me#International long covid awareness day#Long covid awareness#Covid is not over#Alt text in image
11 notes
·
View notes
Text

Tomoko Kawakami and Rachael Lillis Both voices of Utena Both taken by cancer May they rest in peace
— Majorasam Theo-Door 📌 (@MajorasamTheo) August 12, 2024
This just broke me right here. Both voices of Utena Tenjou, taken by cancer. https://t.co/lJmoPXe8Eo
— 𝕌𝕟𝕕𝕖𝕣𝕕𝕠𝕘𝔹𝕋: 𝔹𝕃𝕄 ✊🏿 (@B_Rabbit843) August 12, 2024
#alt text#gutted honestly#utena tenjou#tenjou utena#shojou kakumei utena#mask up#SARS-CoV-2#it's oncogenic
6 notes
·
View notes
Text
For the sake of guidance, I hope people will follow the highest precautions possible. The worst of SARS-CoV-2 is not limited to 2020, despite what is stated by politicians, media outlets and other public figures and professionals to whom it applies.
I want to inform readers the CDC has officially ended the 5 day isolation period for SARS-CoV-2 and this does not suddenly mean it is not contagious or that our protocols should be lapsed or relaxed. Spread is more rampant than ever. So please do not let this announcement and decision give a false sense of security.
Piece by the incredible Lucky Tran.
Note, please do not use the Washington Post as a source for quality coverage of the ongoing pandemic.
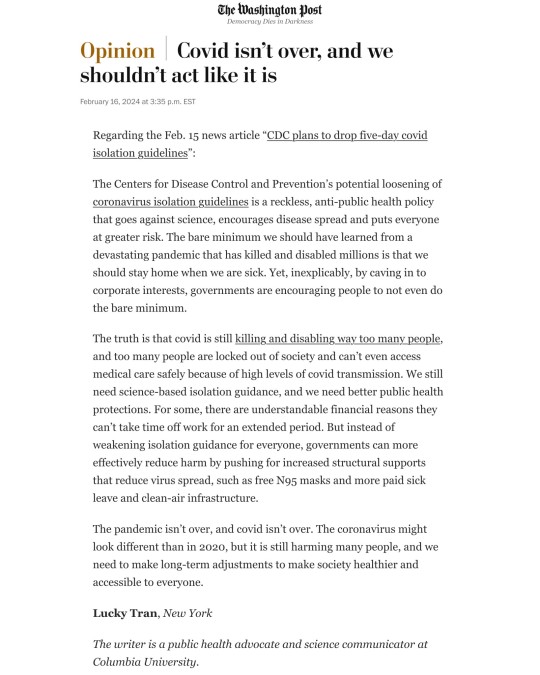
As others have said, if SARS-CoV-2 cannot be eradicated (I still hold out hope and think it imperative in fact), it means adjusting and adapting, not ignoring it, treating this virus and disease as harmless or of little harm and create hostile untenable conditions and daily situations for any efforts of prevention and control of it.
Of what I've read over the course of 4 years, SARS-CoV-2 continues to mutate, kill and disable. This cannot last and will end in an ever escalating disaster if we continue to allow it. - Admin and mod
Additional: Immunity rates are a concern as are vaccination rates. The boast of vaccines administered does not often enough include a breakdown based on how many in the series per person (e.g. 1 dose, primary series, x number of boosters and how recently).
Vaccine rates vary by country, but in regard to the U.S. rates have been on a decline, thus compromising effectiveness on a population level.
#Updates#News#Admin#Moderator#Public health#SARS-CoV-2#Covid-19#Covid 19#SARS CoV 2#SARS 2#Pandemic#Ongoing pandemic#Lucky Tran
5 notes
·
View notes
Text
“I have tried to let Truth be my prejudice” W. Eugene Smith, photojournalist (1918-1978)
By Robert Rennebohm
ABSTRACT:
This article attempts to summarize Dr. Geert Vanden Bossche’s scientific analysis of the COVID-19 mass vaccination campaign. Please bear in mind that Dr. Vanden Bossche’s understanding of the COVID-19 situation is still evolving, as he studies the ongoing dynamic and complex interplay between the virus and our individual and collective immune systems, and the effects of the COVID-19 mass vaccination campaign on that interplay. He is still learning.
While temporarily protecting vaccinated individuals (vaccinees) from severe COVID-19, the COVID-19 mass vaccination campaign has, unfortunately, been placing tremendous suboptimal population-level immune pressure on the virus. This will inevitably and ultimately result in the emergence and propagation of SARS-CoV-2 variants that will be highly virulent when contracted by vaccinated individuals from/in highly vaccinated populations (though not highly virulent when contracted by healthy unvaccinated individuals). In the meantime (and beyond) the COVID-19 vaccines have been predisposing vaccinees to autoimmunity and malignancy, while also interfering with the ability of a vaccinee’s immune system to control infections (acute and chronic) caused by non-SARS-CoV-2 viruses and other pathogens.
BRIEF SUMMARY:
To date, the immune systems of highly COVID-19 vaccinated individuals have been protecting vaccinees from severe disease via four main immune mechanisms: via steric immune refocusing (SIR), which generates broadly neutralizing antibodies against the virus; via slow maturation of SIR-created antibodies into isotype-switched IgG4 antibodies (Abs), which have an anti-inflammatory effect and thereby diminish disease severity; via mobilization of MHC-Class I unrestricted cytolytic T lymphocytes (CTLs), which kill the virus and diminish inter-host transmission (transmission from an infected person to a new susceptible person); and via production of high levels of virulence-inhibiting PNNAbs (polyreactive non-neutralizing antibodies), which protect against severe disease in the lower respiratory tract and other internal organs.
However, these protective immune mechanisms are unstable, unsustainable, will ultimately fail, and are creating serious problems. As explained in the main text of this article: SIR-created Abs are increasingly failing to protect and have spawned a vast array of “immune escape” variants; high titers of IgG4 Abs are predisposing vaccinees to autoimmunity and malignancy; high titers of IgG4 Abs and previously neutralizing, vaccine-induced Abs combined with exposure to highly infectious variants is now disabling SIR and triggering strong activation of APCs (antigen presenting cells), respectively. The resulting stimulation of MHC-unrestricted CTLs, while mitigating COVID-19 disease symptoms, is now causing generalized immune suppression. As titers of previously neutralizing, vaccine-induced Abs are now declining, the concentration of PNNAbs that effectively bind to the N-terminal domain of spike protein (Spike-NTD) is also declining; consequently, the virulence-inhibiting PNNAb levels are irreversibly dropping to levels that will not only fail to protect against severe disease but will also put suboptimal population-level immune pressure on viral virulence.
Soon the collective suboptimal PNNAb levels will create fertile conditions for the natural selection of more virulent variants in highly vaccinated populations. Under these circumstances, new variants that overcome the PNNAb-mediated inhibitory effect on viral virulence without compromising their intrinsic “fitness” (i.e., are just as infectious as other circulating variants) will become naturally selected and rapidly spread. This is because they will have a transmission advantage over current variants because they will cause severe systemic disease and, therefore, be massively shed in the environment instead of inducing CTL responses to virus-infected cells via enhanced viral uptake into APCs.
A highly infectious and highly virulent variant will have the potential to cause enormous numbers of hospitalizations and deaths, particularly in highly (and rapidly) vaccinated countries, particularly in vaccinated individuals whose innate immune training has been compromised, especially in frail and elderly individuals who have been vaccinated prior to viral exposure.
So, the “calming” of the pandemic over the past year (or so) has been largely due to a set of compensatory immune mechanisms (in vaccinees) that have temporarily protected vaccinees from severe COVID-19 but are unsustainable and seriously problematic. This “calm” has been falsely reassuring and will be followed by a “storm” caused by a new variant that is highly virulent when contracted by vaccinees whose cell-based innate immune system has been sidelined. Vaccinated individuals with such poorly trained innate immunity will be largely defenseless against this variant and are at high risk of succumbing to it. Healthy individuals who have not received the COVID-19 vaccine and live in a highly vaccinated population will be able to handle the variant well, because their innate immunity is robust, well-trained, and well-practiced.
This virulent variant will not survive long, however. It will cause a severe “storm,” then die out relatively quickly, because it will quickly run out of accessible, susceptible hosts.
This sad outcome was predictable and preventable. The cascade of immune events and the ultimate outcome described in this article (and in related contributions) would not have occurred if the population had not exerted large-scale immune selection pressure on viral infectiousness. Because of the large-scale administration of spike-based vaccines during this pandemic, the COVID-19 mass vaccination campaign has led to vaccinated populations exerting significant immune selection pressure on viral infectiousness and now on viral virulence.
The scientific reality is that, because of laws of Nature, the mass vaccination campaign has transformed the initial COVID-19 pandemic into a far more serious, prolonged, and threatening pandemic, and, in addition, has created a tremendous amount of vaccine injury at the individual level—-such that far more cumulative deaths and morbidity will occur than would have occurred in the absence of the mass vaccination campaign.
INTRODUCTION:
Dr. Vanden Bossche’s important analysis of the COVID-19 mass vaccination campaign has been largely ignored:
For more than two years Dr. Geert Vanden Bossche has been repeatedly explaining (to scientists, physicians, and the general public) why the implementation of a mass vaccination campaign (like the COVID-19 mass vaccination campaign) in the midst of an active pandemic of an acute self-limited viral infection (like SARS-CoV-2) will inevitably lead to the natural selection and rapid propagation of viral variants that are both highly infectious and highly virulent and will have the potential to cause a catastrophic number of hospitalizations and deaths. His analysis has been based on a deep understanding of the immunology, virology, vaccinology, and evolutionary biology involved; and on extensive, well-rounded, real world, interdisciplinary (non-“siloed”) experience in these fields. His careful analysis has been scientifically sound, highly responsible, profoundly important, and has warranted the immediate attention of scientists, physicians, and public health officials---but has been largely ignored.
Dr. Vanden Bossche (GVB) has felt a professional and moral obligation to continue to share his honest, objective, deep, scientific analysis with the scientific/medical community and the public, so that all can be informed of and prepare for what is a very plausible and worrisome outcome (and in his view the inevitable outcome) of the COVID-19 mass vaccination campaign. He also shares his analysis in the hope that scientific and health policy mistakes will not be repeated in the future.
If the scientists and physicians who have promoted the mass vaccination campaign and have disagreed with GVB’s analysis were as concerned as GVB is about understanding the complex COVID-19 situation as accurately as possible and were equally concerned about honestly educating and preparing the public, they would have provided, long ago, a point-by-point critique of GVB’s analysis and would have engaged in respectful dialogue with him---dialogue that would be archived and made available for physicians and the public to view and study. That would have been in keeping with one of the most important fundamental principles of science and medicine---which is to welcome, honor, and critically evaluate all plausible, important, high priority hypotheses (which GVB’s analysis certainly represents) and do so through respectful dialogue. Unfortunately, other scientists and physicians, particularly those who have most strongly promoted the prevailing COVID-19 narrative and its mass vaccination campaign, have remained silent about GVB’s analysis and have avoided any discussion of his concerns---other than to ignore, dismiss, belittle, or demonize his analysis.
The only legitimate justification for scientists and physicians to not engage in constructive dialogue with GVB would be if his analysis were so irresponsible and so off the mark, scientifically, that it did not warrant comment. But his analysis is not irresponsible or wildly off the mark. To the contrary, his analysis is far more scientifically sound, far more sophisticated, and far more responsible than the simplistic, egregiously unscientific prevailing COVID-19 narrative, which has been based on "data" of astonishingly low scientific quality and whose key promoters have been grossly violating fundamental principles of science, medicine, ethics, and democracy throughout the pandemic (as I have repeatedly explained and documented in many articles posted on my website). It is scientifically and intellectually untenable for those scientists and physicians to claim that GVB’s analysis is so irresponsible and off that mark that it is unworthy of their comment. It is telling that the scientists and physicians who have strongly promoted the mass vaccination campaign have avoided any discussion of GVB’s excellent analysis.
Misapplication of a “conventional view” regarding viral virulence:
I have tried to discuss GVB’s concerns with scientists and physicians who have strongly doubted the accuracy of his analysis. This includes scientists and physicians who have been strongly opposed to the prevailing COVID-19 narrative and its mass vaccination campaign but have, nevertheless, been highly skeptical of GVB’s prediction that a highly virulent variant will appear and cause devastating harm. The argument these scientists and physicians have typically put forth (an argument that I will call the "conventional view") is that "viruses normally do not evolve to become more virulent, because that would not be in the best interests of the virus---because if the virus kills its host, it will not be able to survive. Instead, it is in the best interest of the virus to, if anything, gradually become less virulent, not more virulent." This conventional view is largely correct when/if we are talking about a normal, usual, "naturally evolving" epidemic/pandemic (i.e., an epidemic that is not treated with a mass vaccination campaign in the midst of the active epidemic, using a suboptimal vaccine)---though I would hasten to add that the main reason a "naturally evolving" epidemic/pandemic ends is not because the virus gradually becomes less virulent---the main reason is that herd immunity develops and this results in the virus no longer having ample susceptible hosts to easily infect. I would also add that we should avoid the anthropomorphic notion that the virus has a conscious strategy. Evolution of the virus, evolution of the immune response, and evolution of the pandemic are determined by natural laws of nature---e.g., competitive binding, steric hindrance, conformational changes, other laws of physical chemistry, and the Darwinian principles of natural selection and fitness advantage.
What I think the "conventional view" fails to take into account is that this COVID-19 pandemic has not been treated in a normal, usual, natural way. Instead, it has been treated in a highly abnormal way---namely, with implementation of a mass vaccination campaign, across all age groups, in the midst of the active pandemic, using a suboptimal vaccine (i.e., a vaccine that thwarts but does not prevent viral replication and transmission). This highly abnormal intervention has profoundly changed the normal interplay between the immune system and the virus, at a population level---rendering that interplay to be highly abnormal. The COVID-19 mass vaccination campaign has forced the immune system to do things it normally does not need to do and has made it more difficult for the immune system to do what it needs to do. The mass vaccination campaign has profoundly and adversely affected the immune ecosystem---at both individual and population levels. Accordingly, the “conventional view” is not sufficient to explain what has been happening since implementation of the COVID-19 mass vaccination campaign, or to predict what will happen.
We have never before implemented a mass vaccination campaign (using a prophylactic non-live vaccine) in the midst of an active pandemic, for good scientifically-sound reasons. GVB feels very strongly (based on fundamental scientific principles---laws of nature) that this mass vaccination campaign will lead to the highly abnormal and highly unusual phenomenon of a variant emerging that is highly virulent when contracted by COVID-19-vaccinated individuals who lack a sufficiently trained CBIIS (cell-based innate immune system), due to deficient or insufficient previous exposure to natural infection---a phenomenon that would not have happened in the absence of such a campaign. One could argue that he cannot possibly know this "because we have never done this before." But he could similarly argue that, “because we have never done this before,” the promoters of the mass vaccination campaign cannot possibly know that their campaign will not result in the natural selection and fulminant spread of highly virulent variants.
So, because we have never before implemented a mass vaccination campaign in the midst of an active pandemic, using a prophylactic, non-live vaccine---neither GVB, nor the promoters of the mass vaccination campaign, can provide definitive proof (at this point) that a highly virulent variant will or will not emerge and dominate. Instead, we are left to consider a spectrum of plausible hypotheses, including GVB’s highly plausible hypotheses.
Frankly, in my opinion, GVB has more experience in and has taken a far deeper, more interdisciplinary, more well-rounded dive into the fields of immunology, virology, vaccinology, and evolutionary biology than have promoters of the mass vaccination campaign---and, more importantly, GVB, in my opinion, has been far more honest, objective, scientific, careful, ethical, and altruistic than have key promoters of the mass vaccination campaign, many of whom have obviously violated many fundamental principles of science, medicine, ethics, and democracy throughout the past three years, as I have explained in previously posted writings. Furthermore, GVB’s scientifically plausible and highly responsible hypotheses are profoundly important and, therefore, need to be taken very seriously by other scientists and physicians, even if they are skeptical of them. Such is the tradition of science and medicine.
Below is a detailed REVIEW of my understanding of why GVB is so convinced that the COVID-19 mass vaccination campaign will, inevitably, result in the emergence, natural selection, and propagation of highly infectious and highly virulent SARS-CoV-2 variants that will have the potential to cause huge numbers of hospitalizations and deaths, particularly in highly (and rapidly) vaccinated countries, especially in highly vaccinated individuals.
For background information, consider viewing the video, Respecting the Immune Ecosystem---Concerns of an Immune System Ecologist, which is posted in the “Notes on COVID-19” section of my website (www.notesfromthesocialclinic.org) and provides numerous relevant and instructive medical illustrations.
Better yet, read GVB’s recently published book, The Inescapable Immune Escape Pandemic, and access the many articles and videos on GVB’s website: www.voiceforscienceandsolidarity.org, particularly his recent article: https://www.trialsitenews.com/a/immunological-correlates-of-vaccine-breakthrough-infections-caused-by-sars-cov-2-variants-in-highly-c-19-vaccinated-populations.-645407ab
NOTE TO READER: If the following detailed REVIEW seems too complex and confusing, the reader might want to skip to the section entitled A SUMMARIZING OUTLINE OF THIS ARTICLE (and maybe the SUPPLEMENTAL INFORMATION section), then return to the more detailed and nuanced REVIEW.] The FOOTNOTES at the end of the REVIEW might also be helpful, as might the BRIEF SUMMARY at the beginning of the article.
REVIEW: WHY IS THE NATURAL SELECTION AND PROPAGATION OF HIGHLY VIRULENT SARS-CoV-2 VARIANTS AN INEVITABLE OUTCOME OF THE COVID-19 MASS VACCINATION CAMPAIGN?
The critically important difference between optimal and suboptimal immune pressure on the virus, at a population level:
In order to best appreciate the detrimental effects of the COVID-19 mass vaccination campaign on the immune ecosystem, it is important, first, to understand the critical difference between optimal and suboptimal immune pressure on viral infectiousness, at the population level.
Optimal immune pressure on viral infectiousness means that the immune response to the virus is so efficient and effective that the virus is quickly killed. The immune response puts so much immune pressure on the virus that the virus is unable to thrive. Optimum (population-level) immune pressure on viral infectiousness is characteristic of the “herd immunity” (collective sterilizing immunity) that develops during a naturally evolving pandemic of an acute self-limiting infection (a pandemic that is not treated with implementation of a mass vaccination campaign in the midst of the pandemic)
Suboptimal immune pressure on viral infectiousness means that the immune response to the virus is only partially and inadequately effective---such that the virus is put under sub-lethal pressure, as opposed to lethal pressure. The immune response thwarts viral replication and transmission but does not adequately prevent successful replication and transmission of the virus. This partial (suboptimal) immune pressure makes it difficult for the virus to survive and thrive but does not prevent survival. Under this circumstance, if a new variant appears on the scene and has a fitness advantage (i.e., is better able to overcome the suboptimal immune pressure on viral infectiousness), it will be able to thrive more easily than existing variants and will, therefore, outcompete other variants, be naturally selected, and dominantly propagate. In other words, suboptimal population-level immune pressure on viral infectiousness allows an incipient potentially threatening viral variant that has a fitness advantage (e.g., is more infectious) to survive, reach its potential, and supplant variants that lack that fitness advantage. In fact, if suboptimal immune pressure is exerted at the level of the population (i.e., suboptimal ‘population-level’ immune pressure), it promotes the successful natural selection and dominant propagation (or co-circulation) of variants that are able to overcome the suboptimal immune pressure. In other words, suboptimal population-level immune pressure on a phenotypic characteristic of the virus (e.g., its infectiousness) inevitably results in immune selection pressure on that very viral characteristic.
Suboptimal population-level immune pressure on viral infectiousness is characteristic of a pandemic that is treated with large-scale use of spike-based vaccines (i.e., mass vaccination) that is implemented in the midst of the active pandemic. Since the advent of Omicron, highly COVID-19-vaccinated populations have been exerting suboptimal population-level immune pressure on more and more conserved, functional epitopes of the SARS-CoV-2 spike protein, thereby promoting natural selection and co-circulation of a diversified array/spectrum of increasingly infectious “immune escape” variants. In highly COVID-19 vaccinated populations, highly infectious variants are now facilitating a shift from immune selection pressure on viral infectiousness to immune selection pressure on viral trans infection (i.e., viral infection of the lower respiratory tract and other internal organs by virtue of virus transfer from migratory sentinel cells to susceptible organ cells) and, therefore, on the capacity of SARS-CoV-2 to trigger severe disease (as will be explained later).
Whereas optimal population-level immune pressure on viral infectiousness ends a pandemic relatively quickly, prolonged suboptimal immune pressure exerted on viral infectiousness by the population promotes natural selection of new, more infectious immune escape variants. This fuels enhanced immune escape and therefore prolongs a pandemic while driving it in a more dangerous direction.
For further discussion of optimal versus suboptimal population-level immune pressure, please see SUPPLEMENTAL INFORMATION at the end of this article.
Why are highly vaccinated individuals, in particular, experiencing frequent breakthrough infections (BTIs)?
Throughout the COVID-19 pandemic, all of us, vaccinated and unvaccinated, have been frequently exposed (and are still being exposed) to more infectious SARS-CoV-2 variants---most recently, many Omicron variants and subvariants, all of which are highly infectious, all of which represent “immune escape” variants. As a result, both previously infection-primed individuals (individuals whose immune response to SARS-CoV-2 was triggered by natural SARS-CoV-2 infection) and previously vaccine-primed individuals (individuals whose first immune response was artificially triggered by COVID-19 vaccination) have been experiencing breakthrough infections (BTIs). Vaccinated individuals, in particular, have been frequently experiencing breakthrough infections (which we will call “vaccine-BTIs”), for the following three main reasons:
Their vaccine-induced potentially neutralizing antibodies (pNAbs), which are directed against epitopes in the receptor binding domain (RBD) of the spike protein, have been unable to neutralize the many “immune escape” variants that have successively appeared---because these variants have mutated in a way that enables them to “escape” from (be resistant to) these vaccinal pNAbs. (These immune escape variants appeared on the scene because their resistance to pNAbs gave them a competitive “fitness advantage” which, in turn, led to the natural selection and dominant propagation of these variants.)
Their polyreactive non-neutralizing antibodies (PNNAbs), which were stimulated into binding to the N-terminal domain of the spike protein (Spike-NTD) because of the substantially diminished neutralizing capacity of vaccine-induced anti-spike Abs, have been facilitating viral entry into susceptible epithelial host cells (i.e., these PNNAbs are infection-enhancing) and have thereby accelerated production of viral progeny. This infection-enhancing effect of the PNNAbs is due to the fact that binding of PNNAbs to a highly conserved antigenic region within the N-terminal domain of the spike protein (Spike-NTD) causes a conformational change in the spike protein that flips the receptor binding domain into the ”open position” thereby making it easier for the virus to enter susceptible host epithelial cells.)
Their innate immune system has been sidelined because non-replicating vaccines do not train the cell-based innate immune system and many vaccinees received their vaccination prior to exposure to natural infection (especially in countries that implemented a fast-track mass vaccination program).
Why have BTIs (in both unvaccinated and vaccinated individuals) been relatively mild (at least since the initial appearance of Omicron variants)? What protective immune mechanisms have been at play?
During the Omicron era, BTIs (in both unvaccinated and vaccinated individuals) have, so far, either been asymptomatic or have usually caused only mild or moderate symptoms. To date, BTIs have not usually caused severe COVID-19 disease, for the reasons mentioned below:
In the case of heathy unvaccinated individuals: Healthy unvaccinated individuals have been able to handle re-exposure increasingly well, primarily because of their robust, fully participating, and increasingly trained innate immunity. Their innate immune system is able to quickly lower viral loads and kill virus-infected cells (via trained, i.e., epigenetically re-programmed, natural killer cells) without needing to prime the adaptive immune system for help (although MHC class I-unrestricted CTLs may be triggered in the case of symptomatic infection).
In the case of vaccinated individuals: Vaccinated individuals, on the other hand, have been heavily relying on four major protective immune mechanisms to deal with their frequent vaccine-BTIs. As will be explained, these protective immune mechanisms, though temporarily helpful, are unstable, unsustainable, will ultimately fail, and are problematic.
The SIR phenomenon (Steric Immune Refocusing):1-3 First, vaccinated individuals, via the SIR phenomenon, developed broadly neutralizing antibodies to immunosubdominant spike-associated domains. In the context of SARS-CoV-2, SIR refers to the redirection of the immune system to produce neutralizing antibodies against conserved immune-subdominant epitopes2 of the spike protein when pre-existing poorly neutralizing Abs sterically hinder (physically block) immune recognition of the variable immune-dominant epitopes of the spike protein. These SIR-created high avidity antibodies have temporarily provided efficient cross-neutralizing activity. However, there have been downsides associated with the beneficial protective effects of these SIR-created antibodies. Titers of these SIR-created neutralizing antibodies, which were initially already at relatively low levels, declined and rapidly reached a point where they fell below the optimal threshold for providing protection from infection (i.e., fell into the suboptimal range). Because of the suboptimal neutralizing titers of these antibodies and their delayed maturation (in germinal centers) into affinity-matured, isotype-switched IgG4 antibodies, prolonged large-scale (population-level) immune pressure has been exerted by these antibodies in highly COVID-19 vaccinated populations. In these populations, suboptimal SIR-created population-level immune pressure on viral infectiousness led to the natural selection and co-circulation of a vast array of more infectious Omicron descendants. In short, while providing some protection to vaccinees, the SIR phenomenon spawned a succession of increasingly infectious “immune escape” variants and ultimately led to co-emergence of highly infectious Omicron descendants. (Note: Because of the diminished production of viral progeny, re-exposure of unvaccinated, infection-experienced individuals to Omicron-derived descendants did not trigger SIR and, therefore, did not promote viral immune escape!) A second downside of the SIR phenomenon is that it increasingly refocuses the immune system on more immunorecessive epitopes, ones that have greater similarity to “self” and “altered self.” This predisposes to autoimmunity and malignancy, respectively.2, 3
The anti-inflammatory effect of isotype-switched IgG4 antibodies: SIR-created neutralizing antibodies eventually underwent isotype-switching---i.e., matured (in delayed fashion) into IgG4 antibodies. IgG4 antibodies have an anti-inflammatory effect. Accordingly, when vaccinated individuals with high titers of SARS-CoV-2 specific IgG4 antibodies (i.e., those who experienced a SIR-enabling vaccine-BTI) are exposed to newly emerging immune escape variants, their symptoms have been reduced by the anti-inflammatory effects of these IgG4 antibodies. As not only vaccine-BTI but also mRNA vaccination facilitates SIR, it stands to reason that IgG4 antibodies can also be induced after mRNA -vaccination. Indeed, Irrang et al documented that “several months after the second vaccination [with mRNA COVID-19 vaccine], SARS-CoV-2 specific antibodies were increasingly composed of non-inflammatory IgG4, which was further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant BTI.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9847566/. (These unusual levels of SARS-CoV-2 specific IgG4 antibodies have not been documented in unvaccinated individuals.) However, there is an unfortunate trade-off for the protective anti-inflammatory effect of vaccinee’s high levels of IgG4 antibodies---namely, they predispose those individuals to autoimmunity and malignancy, as explained in the FOOTNOTES of this article2,3 and in GVB’s recent article: https://www.trialsitenews.com/a/immunological-correlates-of-vaccine-breakthrough-infections-caused-by-sars-cov-2-variants-in-highly-c-19-vaccinated-populations.-645407ab
Activation of CTLs (Cytolytic T Lymphocytes): Despite the functional monovalency of isotype-switched IgG4 antibodies, elevated titers of these Abs result in strong cytolytic activation of MHC Class I unrestricted T lymphocytes but no longer promote SIR upon vaccine-BTIs with highly infectious Omicron descendants. This is because high concentrations of IgG4 Abs bound to progeny virions of these variants will expedite viral uptake by APCs (antigen presenting cells). SIR-disabling vaccine-BTIs therefore not only enhance CTL-mediated elimination of virus-infected cells, thereby rapidly abrogating viral shedding and safeguarding vaccinated individuals from COVID-19 disease altogether, but also prevent de novo priming of new, broadly cross-neutralizing Abs and thus, promote propagation of viruses with higher intrinsic infectiousness. High viral infectiousness can ultimately cause activated CTLs to kill the APCs that activated them in the first place. Strong activation of APCs and insufficient or deficient presentation of non-SARS-CoV-2-related Ags may lead to generalized immune suppression and increased prevalence of other, non-Covid-19-related diseases.
The virulence-inhibiting effect of PNNAbs (polyreactive non-neutralizing antibodies): PNNAbs bind to Spike-NTD exposed on free infecting virions as a result of diminished neutralizing capacity of potentially neutralizing vaccine-induced antibodies (pNAbs) and thereby enhance viral infectiousness. These Abs have also a virulence-inhibiting activity in that they attach to virus that is tethered to migrating dendritic cells (DC) and thereby prevent transfer of virus from dendritic cells to cells in the lower respiratory tract (LRT) and other internal organs---i.e., high levels of PNNAbs adsorbed on DC-tethered virions inhibit trans infection in the LRT and other internal organs and, thereby, protect vaccinated individuals from severe COVID-19 disease (fig. 1). However, as the infectiousness of the circulating variants increases, hyperactivation of CTLs not only leads to generalized immune suppression but also causes highly vaccinated populations to exert immune selection pressure on viral trans infectiousness and, therefore, promote natural selection of new variants that are likely to exhibit enhanced virulence (as explained below).
In these ways, SIR-created neutralizing antibodies, anti-inflammatory IgG4 Abs, and CTLs have been enhancing recovery from disease, in vaccinees, (after providing some short-lived protection from infection) or have been mitigating or even preventing disease symptoms, while PNNAbs have been protecting vaccinated individuals from severe COVID-19 disease, when these individuals have experienced vaccine-BTIs with more infectious variants. However, while this “immunologic rescue operation” (GVB’s phrase) has been protecting vaccinated individuals from severe disease, it has meanwhile been facilitating asymptomatic transmission (to both vaccinated and unvaccinated individuals) of a diversified array of highly infectious SARS-CoV-2 immune escape variants; it is, therefore, now causing highly COVID-19 vaccinated populations to exert large-scale immune selection pressure on viral virulence (as will be further explained later); it has predisposed vaccinees to autoimmunity and malignancy; and it has adversely affected the ability of vaccinees to normally handle other pathogens.
The false impression that the pandemic is currently subsiding, heading into endemicity, and becoming less worrisome:
The above four protective mechanisms, upon which vaccinated individuals have been relying to diminish viral pathogenicity, have given the impression that the pandemic is subsiding, becoming milder, and heading into a relatively benign endemic phase. But, as explained below, this is a false impression. These protective mechanisms will ultimately fail and result in the natural selection and propagation of new emerging variants that have the capacity to become highly virulent in COVID-19 vaccinees. These mechanisms have been providing false reassurance. The current “calm” will, unfortunately, be followed by a severe “storm.” The latter will primarily affect those who were vaccinated prior to experiencing natural infection (e.g., the elderly and those considered vulnerable because of underlying disease or immune suppressive conditions).
Why will the protective immune mechanisms upon which highly vaccinated individuals have been relying inevitably fail and promote the “successful” emergence of a highly virulent variant?
As long as the concentration of PNNAbs bound to DC-tethered progeny virions remains high enough (i.e., are at optimal levels, or close to being optimal, and are putting optimal immune pressure on viral trans infection), the virulence-inhibiting effect of the PNNAbs and the APC-mediated activation of CTLs will adequately protect the vaccinated individual from severe disease (or even from COVID-19 altogether) and will diminish viral shedding. Although high levels of PNNAbs bound to DC-tethered progeny virions (via Spike-NTD) are able to prevent or mitigate viral trans infectiousness at the level of the LRT and internal organs, the infectiousness of the virus at the URT (upper respiratory tract) remains unaffected and promotes asymptomatic transmission. Thus far, high levels of PNNAbs bound to DC-tethered virions have been preventing natural immune selection of new variants capable of escaping from the virulence-inhibiting effect exerted by these antibodies (fig. 1).
However, since the circulating variants have increased infectiousness, their progeny virus is released in high density from the cells they infect and thereby cause substantial inflammation. The latter promotes enhanced adsorption of progeny virions onto patrolling, migratory dendritic cells and thereby fosters opsonization of free progeny virus by vaccine-induced anti-Spike Abs. Enhanced uptake of these virus-Ab complexes into APCs have been strongly activating cytolytic T lymphocytes (CTLs), which in turn eventually kill the APCs that activated them in the first place. This killing of APCs hinders the recall of previously vaccine-primed T helper cells, thereby preventing further SIR, or the production of new antibodies targeting new, more conserved spike-derived antigen, despite the presence of elevated titers of functionally monovalent Ig-G4 Abs. Failure of vaccine-BTIs to prime new, broadly neutralizing anti-Spike Abs leads to failure to reduce viral infectiousness. Consequently, elevated IgG4 -Ab titers in highly vaccinated populations link enhanced protection of vaccinees from Covid-19 disease and diminished viral shedding to enhanced infectiousness of the circulating immune escape variants and their asymptomatic transmission. Enhanced viral infectiousness lowers the concentration of PNNAbs that bind to Spike-NTD on DC-tethered virions in vaccinees as shown in fig. 2. This inevitably leads to suboptimal PNNAb-mediated immune pressure on viral trans infectiousness in Covid-19 vaccinees.
When levels of immune pressure on viral trans infectiousness collectively decline into the suboptimal range, Spike-NTD-binding PNNAbs will place large-scale immune selection pressure on the trans infectiousness of DC-tethered progeny virions produced by the currently circulating, highly infectious Omicron descendants. In other words, diminished viral shedding, which is now threatening viral transmission in highly COVID-19 vaccinated populations, is indirectly causing suboptimal immune pressure on viral virulence while enabling asymptomatic transmission of highly infectious variants. Collectively exerted, suboptimal population-level immune pressure drives natural selection. That is, any emerging variants that are able to overcome the virulence-inhibiting effect of the PNNAbs while maintaining a high level of viral infectiousness will have a transmission advantage, will be naturally selected, and propagate (as enhanced severe disease will not enable timely isolation of the affected individuals). In short, diminished viral inter-host transmission (transmission from an infected person to a new susceptible person) is promoting natural selection of highly infectious immune escape variants that have capacity to enhance systemic intra-host viral replication and dissemination to distal organs such as to enable enhanced, but lethal viral transmission. When this happens, a major wave of exacerbated severe COVID-19 disease cases is likely to occur among the highly vaccinated. In the absence of herd immunity, it is reasonable to assume that this will ultimately allow Nature to control viral transmission. Elimination of those unable to mount a sterilizing immune response to the virus (i.e., primarily vaccinated individuals) would allow those who do mount a sterilizing immune response to contribute to establishing herd immunity and thereby durably protect the human species from new SARS-CoV-2 pandemics.
In the past, booster doses of vaccine and/or reinfection (BTIs) were resulting in periodic boosting of previously vaccine-primed NAbs or de novoproduction of new, cross-functional neutralizing antibodies (via SIR)---up to optimal levels. However, booster doses of vaccine, or vaccine-BTIs with highly infectious Omicron descendants, are now failing to boost or prime neutralizing antibodies (again, because APCs are so preoccupied with removing highly infectious virus from vaccine-BTIs that they succumb to the killing by the CTLs they activate or cause other antigens to be outcompeted for uptake into their antigen processing and presentation machinery). At the same time, these SIR-disabling vaccine-BTIs fail to stimulate new, broadly neutralizing anti-Spike Abs. Consequently, both (updated) booster doses and ongoing (asymptomatic) vaccine-BTIs fail to reduce viral infectiousness. It follows that the PNNAb-mediated immune pressure on viral trans infection will drop into a suboptimal range.
A large-scale decrease in PNNAb titers in the context of circulating highly infectious variants is now increasing immune selection pressure on viral trans infection. Upon mounting beyond a certain threshold, the immune selection pressure will likely trigger natural selection of a new SARS-CoV-2 variant(s) displaying mutational changes (presumably in the glycosylation profile of spike protein) that enable the variant to collectively lift the blockade on viral virulence. However, mutational changes in the Spike-associated glycosylation profile may bear a substantial fitness cost. In order for these newly emerging variants to not be outcompeted by other currently circulating, highly infectious variants (which cannot lift this blockade), it is critical that they maintain a high level of infectiousness by enabling PNNAbs to bind to the conserved antigenic site comprised within Spike-NTD. This implies that mutations targeted at evading the PNNAb-mediated inhibitory effect on intrinsic viral virulence cannot occur within this antigenic site and that manifestation of a high level of virulence by these newly emerging variants will likely depend on the presence of suboptimal concentrations of PNNAbs bound onto DC-tethered virions. In other words, the newly emerging immune escape variants are likely to provoke PNNAb-dependent enhancement of severe disease.
In short, because of the laws of nature, newly emerging immune escape variants exhibiting highly infectious, highly virulent properties (in COVID-19 vaccinees) will be selected and rapidly transmitted, and thereby cause PNNAb-dependent enhancement/exacerbation of systemic disease (most likely not only affecting the lower respiratory tract but a multitude of different internal organs), particularly in highly vaccinated countries, particularly in vaccinated individuals who have weak and/or untrained innate immunity (e.g., those who were vaccinated prior to experiencing natural infection, i.e., the elderly and frail). This would not have happened in the absence of the COVID-19 mass vaccination campaign.
Of course, this virulent variant will not be able to survive for long. Healthy unvaccinated individuals (with robust, uninhibited innate immunity that has become increasingly trained to deal with more and more infectious SARS-CoV-2 variants) will be able to eliminate this variant by virtue of sterilizing immunity, despite its virulence in COVID-19 vaccinees. (Group 1). Our hope is that many vaccinated individuals will have been sufficiently exposed to natural infection prior to vaccination to allow for enough training of their innate immune system to weather the storm, especially if they also receive excellent medical management (Group 2). Individuals who received at least two or three vaccine doses (i.e., in the case of mRNA-based or non-mRNA-based vaccine, respectively) prior to natural infection and subsequently experienced a vaccine-BTI (i.e., primarily those who were vaccinated first, i.e., the elderly and vulnerable individuals) are at greatest risk of succumbing to the new emerging variant(s) that can overcome the PNNAb-mediated virulence-inhibiting effect (Group 3). Groups 1 and 3 will prevent the highly virulent variant from circulating for long, because they will either fail to shed the variant (in the case of group 1) or soon run out of accessible susceptible hosts (in the case of group 3), and the pandemic will finally end, not thanks to herd immunity but thanks to eradication of the virus.
Note: Healthy vaccinees who only received a single injection of an mRNA-based COVID-19 vaccine or no more than 2 injections with a non-mRNA-based vaccine prior to developing a symptomatic vaccine-BTI are thought to have preserved their capacity to train their cell-based innate immune system.
Why is it important to take Dr. Vanden Bossche’s excellent analysis very seriously?
For the above reasons, Dr. Vanden Bossche has been extremely worried about the COVID-19 mass vaccination campaign. This is why he has felt obligated to warn scientists, physicians, and the general public about this highly likely outcome---so that all can prepare for such an outcome. Even if his prediction turns out to be wrong (which he greatly doubts, based on his understanding of the science involved), he wants people to have a chance to prepare in case he is correct (which he thinks is highly likely). Even if other scientists and physicians doubt that GVB’s analysis is correct, they must acknowledge that his analysis represents a responsible and scientifically sound analysis about which physicians and citizens deserve to know and for which physicians and citizens deserve opportunity to prepare.
In my opinion, GVB’s concerns and the conclusion of his analysis are correct. The most likely reason for the unwillingness of the promoters of the mass vaccination campaign to engage in dialogue about GVB’s concerns and conclusion is that they know (or at least worry) that their understanding of the virology, immunology, vaccinology, and evolutionary biology of the COVID situation is not nearly as deep and wise as GVB’s understanding. Compared to GVB’s understanding, their understanding, in my opinion, has been simplistic, far less scientific, and less accurate. They should learn from GVB, not ignore or belittle his excellent analysis.
In my opinion, their unwillingness to engage in dialogue is not only scientifically, medically, and intellectually irresponsible, but also cruel. It is cruel to leave the public dangling, confused, miseducated, and misled about the realities of the COVID-19 situation. It is cruel to leave the public unprepared to deal with the profoundly worrisome situation the mass vaccination campaign has created. It is cruel and dishonest to not inform the public of the mistakes the promoters of the mass vaccination campaign have made and what can be done at this point to proactively and optimally address the threatening situation that has resulted.
The reality is, the mass vaccination campaign has transformed the initial COVID-19 pandemic into a far more serious, prolonged, and life-threatening pandemic, and, in addition, has created a tremendous amount of vaccine injury at the individual level—-such that far more cumulative deaths and morbidity will occur than would have occurred in the absence of the mass vaccination campaign. Enormous mistakes have been made and have resulted in enormous threats to huge numbers of people.
Good physicians admit their mistakes, take responsibility for them, work to ensure that damage done is optimally addressed, and take steps to ensure that mistakes are not repeated. The promoters of the mass vaccination campaign have not performed these tasks.
What, specifically, can be done, if GVB is correct and a highly virulent, highly threatening variant appears?
Many important proactive steps can be taken. For details, please see the following article (and an ADDENDUM to it), which is posted on my website: In Anticipation of a Highly Virulent SARS-CoV-2 Variant
FOOTNOTES:
1Steric Immune Refocusing (SIR): For a detailed explanation of the SIR phenomenon (and the IgG4 situation), please see GVB’s book and his most recent article: https://www.trialsitenews.com/a/immunological-correlates-of-vaccine-breakthrough-infections-caused-by-sars-cov-2-variants-in-highly-c-19-vaccinated-populations.-645407ab.
In the context of SARS-CoV-2, SIR refers to the redirection of the immune system to produce neutralizing antibodies against conserved immune-subdominant epitopes2 of the spike protein when pre-existing poorly neutralizing Abs sterically hinder (physically block) immune recognition of the variable immune-dominant epitopes of the spike protein.
The SIR phenomenon, which became evident during the Omicron era, has contributed greatly to delaying natural selection of immune escape variants while expanding the scale thereof. This explains why loss of protection from moderate disease (Omicron) has not abruptly shifted to enhanced virulence (as GVB initially predicted) but first transitioned to mitigation and subsequently even to prevention of Covid-19 disease altogether. It seems as though the immune system, at a population level, first needs to mount a high level of immune selection pressure on viral pathogenicity in order for the virus to unleash a highly virulent variant. As currently circulating, highly infectious variants have induced a nearly unparalleled level of immune protection in vaccinees, second only to protection induced in unvaccinated individuals by natural infection (!), it is reasonable to assume that the virus has now entered the final stage of evolving toward variants combining high intrinsic infectiousness with highly virulent properties in vaccinees.
SIR is a hallmark of PNNAb-dependent vaccine-BTIs and results from binding of non-neutralizing antibodies to the immunodominant epitopes of a monovalent antigen, thereby facilitating immune recognition of immunosubdominant or immunorecessive domains and priming broadly neutralizing antibodies with high avidity but low affinity (note: induction of such antibodies have also been reported upon mRNA vaccination: https://www.ncbi.nih.gov/pmc/articles/PMC9886553/)
SIR appears to be a tool nature uses to shape the evolutionary dynamics of the interaction between the virus and the host immune system such as to leave the host’s adaptive immune system a chance to adapt to vaccine-BTIs and gradually optimizing protection from disease in exchange for granting the virus a license to prolong its propagation and spread (at the benefit of improving sterilizing immune capacity in the unvaccinated before eliminating those devoid of this capacity). GVB had not anticipated (and could not have anticipated) this phenomenon when he initially predicted that a highly virulent variant would likely appear by the early fall of 2022. By now, the new SIR-induced Abs are ceasing to be involved in shaping the evolution of highly infectious variants into highly infectious variants with highly virulent properties in COVID-19 vaccinees. At this stage, Ab-independent vaccine-BTI caused by highly infectious variants in the context of (declining titers of) pre-existing vaccine-induced Abs are educating the immune system to re-orient its target from an immunorecessive S-associated domain to an immunosilent antigenic site within Spike-NTD.
2What is an epitope? An epitope is a part of an antigen (a part of the spike protein, in the context of SARS-CoV-2) that the immune system recognizes and reacts to. It is an immunogenic part of the antigen---a part that triggers an immune response. On the spike protein, for example, there are dominant, highly immunogenic epitopes and there are many subdominant, much less immunogenic epitopes.
3How do SIR and high levels of IgG4 predispose to autoimmunity and malignancy? As the SIR phenomenon continues, antibodies are produced against epitopes that are increasingly more conserved and less immunogenic and more closely resemble “self” epitopes and “altered self” epitopes. These SIR-created antibodies slowly and ultimately mature into SARS-CoV-2-specific isotype-switched IgG4 antibodies.
High titers of these IgG4 antibodies tend to cross-react with “self” epitopes (on our healthy cells) and “altered self” epitopes on cells that are becoming malignant.
When IgG4 antibodies attach to “self” epitopes on healthy cells, this results in failure of self-epitopes to normally activate self-epitope-specific regulatory T cells (T regs) that, in turn, normally and protectively down-regulate the activation and proliferation of self-reactive T cells. That is, normally, these T regs protect healthy cells from autoimmune destruction by self-reactive T cells---but the IgG4 antibodies interfere with that protective process, and autoimmunity results.
When previously healthy cells become malignant, the normal “self” epitopes that are expressed on their surface become altered and become “altered self” epitopes. When IgG4 antibodies attach to “altered self” epitopes on the surface of malignantly transformed cells, this prevents ADCC (antibody dependent cellular cytotoxicity)-mediated immune recognition of these malignant cells by NK cells. This results in failure of NK cells to kill malignantly transformed cells.
So, the high levels of IgG4 antibodies that follow the SIR phenomenon predispose highly vaccinated individuals to autoimmunity and malignancy. This may be one mechanism by which highly vaccinated individuals are developing new cancers (i.e., early onset cancers) and new autoimmune diseases. On the other hand, “turbo cancers” (or rampant relapse of previously controlled cancer) or relapse of previously controlled autoimmune disease are thought to be triggered by hyperactivation of APCs and downstream suppression of CD8+ T cells following vaccine-BTI with highly infectious variants (that are asymptomatic in terms of Covid-19).
#covid-19 vaccine#covid-19#geert vanden bossche#Rob Rennebohm#print this off later#immune escape#viral escape#immune tolerance#SIR#Steric Immune Refocusing#innate immune system#vaccine science#resources#IgG4#NK cells#Sars-Cov-2#virology#vaccinology
10 notes
·
View notes
Text
I have been thinking: COVID consciousness is like climate crisis consciousness.
People can pretend it isn't real (e.g. "climate change isn't happening," or, "COVID is over," fallacies such as this).
Others can acknowledge it is real, but be despairing, choosing to focus on "the futility of things" (e.g. "maybe we could have changed CO2 emissions in the seventies, but we're past the point of no return, and the Earth is going to burn and there is nothing we can do; DAMN YOU ALL TO HELL etc." or, "humanity brought it upon itself, there's no point in trying to prevent the spread of COVID; now everyone is going to get sick," defeatist attitudes such as this…)
But one can come to appreciate the interconnectedness of everything, and, that while one might not have the ability to control one's destiny, let alone the destiny of future generations, one does have the ability to keep trying to make things as… good as possible? As beneficial to as many as possible? Most heartening? Most loving? Even when it is difficult!
Because:
We are all interconnected!
Caring about you makes sense because you caring about me makes sense because we inhabit a common reality! Caring about one another makes our mutual reality better for ALL of us, instead of being caught up in whatever this ridiculous pretense is that everything is fine, this weird attitude that the "immune compromised don't matter, because they'd be dying anyway,"
And even though I think you should care about others
I also keep thinking
like
do some people
not
realise
that
COVID infection has been documented to reduce immune function
for like
like
PRETTY MUCH ANYONE
so
THAT MEANS COVID IS A RISK FOR PRETTY MUCH EVERYONE
and
you do not have a better immune system because of moral superiority! A virus does not care about that kind of thing when it's floating through the air in tiny bits of airborne moisture!!!
And even those with previously of the most robust health do not have the assurance that their immune system will prevent long term impairment because of COVID infection; those who were previously athletes have found themselves sidelined by COVID infection.
Like…
COVID is BAD
AND
COVID is NOT over
And
Some people could be brought around to taking more careful measures if they knew the actual reality of things:
COVID floats like smoke, meaning that to prevent infection whenever one is indoors with strangers (e.g. public places!) one should be wearing an effective, well-fitting mask,
COVID hampers one's immune system
It's bad to spread it to others!
Why is this a controversial opinion?!
Like, let's stop the spread of disease!
This seems like a good idea!
And some people would agree with this, but for whatever reason they're isolated/cut off from the truth, and the trick is finding ways to inform these folks…
But then…
For whatever reason…
It seems like some other people somehow cannot acknowledge reality…
And I find it the weirdest thing!
And I mean, I've been around the internet ("I've seen things you people wouldn't believe…")
I've seen how people can get into echo chambers, affirming realities they want to be true…
But...
In the spring of 2020, I would not have imagined that things would be like this, in 2023…
I don't know what else to say?!
Care about other people?!
Take care of yourself?!
Take care of the biosphere and consider how the output of human activity impacts climactic cycles and the way the living situation will be for coming generations!?!?!?!
Avoid spreading disease because it can impair and kill yourself and/or others?!?!?!
Getting beyond the
"Yes"-
Because the "Yes" can mean
Despair
"Yes it is irreparably bad so there is no point in caring,"
And
Maybe everything will fry! Maybe the next meteorite will come and wipe us out as one did the dinosaurs, and the next species to evolve will have no idea we ever existed! And caring about climate change was pointless?
OK?!
So I should be the-right-amount-of-despairing?! It was better to be hopeless instead of hopeful?! No hope is the appropriate response? What if I hope, anyway?
What if somehow I make things better for someone three generations from now, even if I never meet them, even if humanity dies in five generations? Even if the world is hit by a meteorite tomorrow, why is it cringe if I try to make things better on what turns out to be the last day on the Earth?!
What if you cared about others, even if these others are coming generations and you will never meet them?
Why give into despair?
Even if things are REDONK.
There is PLAGUE; should we not be avoiding it?!
We could get beyond Yes- to but!
"Yes- there is a terrible situation!"
"...BUT this does not have to lead to despair…!"
"…BUT what we do now makes a difference, and cooperation is integral!"
Danged if I've got all the answers, but I'm pretty sure that caring about one another is a good place to start.
I may never meet you, but I can care about you.
<3
And not saying it isn't hard. Like. It can be hard not to despair.
Keep on keepin' on!!! <3
#COVID#COVID is BAD#COVID is NOT over#COVID is ongoing#covid is airborne#pandemic#mask up#long covid#masks#sars-cov-2#covid-19
26 notes
·
View notes