#journals on emergency medicine
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, 27% of US Tumblr users had an annual household income of over $100,000.
Text
Is Pentraxin 3 A Marker in Pathogenesis of Metabolic Syndrome?

Is Pentraxin 3 A Marker in Pathogenesis of Metabolic Syndrome? in Biomedical Journal of Scientific & Technical Research
Pentraxin 3 (PTX3) is an acute-phase protein that is structurally similar to C-reactive protein (CRP). Macrophages, endothelial cells, and adipocytes all produce PTX3 in response to inflammatory stimuli, but hepatocytes are the main source of CRP. PTX3 could play a role in the genesis of obesity, metabolic syndrome (MetS), and CRP because obesity and MetS are chronic inflammatory diseases [1]. MetS is a group of risk factors that includes glucose intolerance, abnormal lipid profiles, hypertension, and abdominal obesity [2- 6]. Each of these factors has been linked to atherosclerosis and cardiovascular disease. The majority of current research has found a link between MetS components and inflammatory mediators such as interleukin-6, tumor necrosis factor-α, and CRP [7]. Furthermore, serum CRP levels were shown to be greater in individuals with more risk factors for MetS, and higher serum CRP levels were related to higher occurrence of cardiovascular events, reflecting the prognostic relevance of MetS severity [8]. In particular, many types of cells, including macrophages, dendritic cells, neutrophils, adipose cells, fibroblasts, and vascular endothelial cells, have been reported to produce PTX-3, a newly recognized acute-phase reactant that is structurally and functionally similar to CRP [9]. The link between MetS and PTX-3 hasn’t been well investigated, and the available evidence appears to be discordant. Several investigations have found a link between MetS components and inflammatory mediators such as interleukin-6, tumor necrosis factor-α, and CRP [7]. The hs-CRP is the most well-known and validated of these inflammatory biomarkers. Insulin resistance, endothelial dysfunction, and unfavorable cardiovascular events have all been linked to high levels of hs-CRP [10,11].
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01 Follow on Blogger : https://biomedres01.blogspot.com/ Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Biomedical Imaging#Journals on Emergency Medicine#open access journals of biomedical science#Journals on Biomedical Intervention#Journals on Biomedical Engineering
0 notes
Text
these are my star trek doctor ocs emtala jcaho (pronounced jay-ko) and ama n'jem
#ama njem is half terran-ghanian and half vulcan#Emergency Medical Treatment and Labor Act and American Medical Association#New England Journal of Medicine#dee s 9
6 notes
·
View notes
Text

#casereports#clinical#medical#medicalresearch#healthscience#medicalcommunity#medicaleducation#clinicalpractice#healthcare#healthcareprofessionals#medicine#public health#health#immune system#medical care#emergencymedicine#emergency#World Journal of Health and Medicine
0 notes
Text
JC: Serratus Anterior Plane Blocks for rib fractures in the ED. St Emlyn's
One of the many jobs that I juggle is as a Major Trauma Consultant on the major trauma ward in Virchester. This involves overseeing and coordinating the care of major trauma patients who are cohorted in a single ward. We also input into critical care areas and the ED. It’s a really positive experience to see how patients progress through care and I love this, and also the interactions with other…

View On WordPress
0 notes
Text
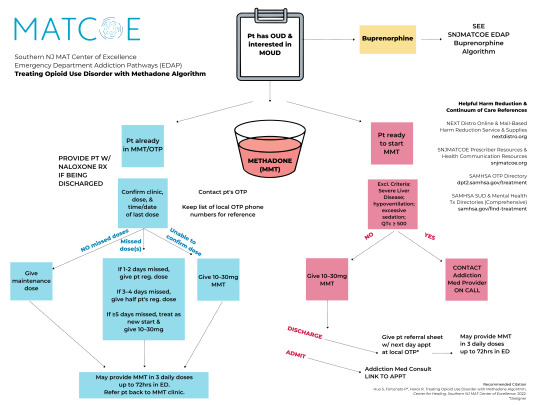
The methadone prescribing algorithm is published as part of the Southern New Jersey Medication for Addiction Treatment Center of Excellence (MATCOE) Emergency Department Addiction Pathways (EDAP) and in the Journal of Emergency Medicine (JEM), March 2023. Learn more here.
Recommended citation:
Huo S, Fortunato P, Haroz R. Treating Opioid Use Disorder with Methadone Algorithm. Southern New Jersey Medication for Addiction Treatment Center of Excellence. 2022.
#Methadone#Medication for Opioid Use Disorder#Medication for Addiction Treatment#MOUD#MAT#Opioid Use Disorder#OUD#Addiction Medicine#Emergency Medicine#Medicine#Southern New Jersey Medication for Addiction Treatment Center of Excellence Emergency Department Addiction Pathways#SNJMATCOE EDAP#Southern New Jersey Medication for Addiction Treatment Center of Excellence#Southern NJ MAT Center of Excellence#SNJMATCOE#Journal of Emergency Medicine#Patricia Fortunato#Personal
0 notes
Text
Epic Systems, a lethal health record monopolist

Epic Systems makes the dominant electronic health record (EHR) system in America; if you're a doctor, chances are you are required to use it, and for every hour a doctor spends with a patient, they have to spend two hours doing clinically useless bureaucratic data-entry on an Epic EHR.
How could a product so manifestly unfit for purpose be the absolute market leader? Simple: as Robert Kuttner describes in an excellent feature in The American Prospect, Epic may be a clinical disaster, but it's a profit-generating miracle:
https://prospect.org/health/2024-10-01-epic-dystopia/
At the core of Epic's value proposition is "upcoding," a form of billing fraud that is beloved of hospital administrators, including the "nonprofit" hospitals that generate vast fortunes that are somehow not characterized as profits. Here's a particularly egregious form of upcoding: back in 2020, the Poudre Valley Hospital in Ft Collins, CO locked all its doors except the ER entrance. Every patient entering the hospital, including those receiving absolutely routine care, was therefore processed as an "emergency."
In April 2020, Caitlin Wells Salerno – a pregnant biologist – drove to Poudre Valley with normal labor pains. She walked herself up to obstetrics, declining the offer of a wheelchair, stopping only to snap a cheeky selfie. Nevertheless, the hospital recorded her normal, uncomplicated birth as a Level 5 emergency – comparable to a major heart-attack – and whacked her with a $2755 bill for emergency care:
https://pluralistic.net/2021/10/27/crossing-a-line/#zero-fucks-given
Upcoding has its origins in the Reagan revolution, when the market-worshipping cultists he'd put in charge of health care created the "Prospective Payment System," which paid a lump sum for care. The idea was to incentivize hospitals to provide efficient care, since they could keep the difference between whatever they spent getting you better and the set PPS amount that Medicare would reimburse them. Hospitals responded by inventing upcoding: a patient with controlled, long-term coronary disease who showed up with a broken leg would get coded for the coronary condition and the cast, and the hospital would pocket both lump sums:
https://pluralistic.net/2024/06/13/a-punch-in-the-guts/#hayek-pilled
The reason hospital administrators love Epic, and pay gigantic sums for systemwide software licenses, is directly connected to the two hours that doctors spent filling in Epic forms for every hour they spend treating patients. Epic collects all that extra information in order to identify potential sources of plausible upcodes, which allows hospitals to bill patients, insurers, and Medicare through the nose for routine care. Epic can automatically recode "diabetes with no complications" from a Hierarchical Condition Category code 19 (worth $894.40) as "diabetes with kidney failure," code 18 and 136, which gooses the reimbursement to $1273.60.
Epic snitches on doctors to their bosses, giving them a dashboard to track doctors' compliance with upcoding suggestions. One of Kuttner's doctor sources says her supervisor contacts her with questions like, "That appointment was a 2. Don’t you think it might be a 3?"
Robert Kuttner is the perfect journalist to unravel the Epic scam. As a journalist who wrote for The New England Journal of Medicine, he's got an insider's knowledge of the health industry, and plenty of sources among health professionals. As he tells it, Epic is a cultlike, insular company that employs 12.500 people in its hometown of Verona, WI.
The EHR industry's origins start with a GW Bush-era law called the HITECH Act, which was later folded into Obama's Recovery Act in 2009. Obama provided $27b to hospitals that installed EHR systems. These systems had to more than track patient outcomes – they also provided the data for pay-for-performance incentives. EHRs were already trying to do something very complicated – track health outcomes – but now they were also meant to underpin a cockamamie "incentives" program that was supposed to provide a carrot to the health industry so it would stop killing people and ripping off Medicare. EHRs devolved into obscenely complex spaghetti systems that doctors and nurses loathed on sight.
But there was one group that loved EHRs: hospital administrators and the private companies offering Medicare Advantage plans (which also benefited from upcoding patients in order to soak Uncle Sucker):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8649706/
The spread of EHRs neatly tracks with a spike in upcharging: "from 2014 through 2019, the number of hospital stays billed at the highest severity level increased almost 20 percent…the number of stays billed at each of the other severity levels decreased":
https://oig.hhs.gov/oei/reports/OEI-02-18-00380.pdf
The purpose of a system is what it does. Epic's industry-dominating EHR is great at price-gouging, but it sucks as a clinical tool – it takes 18 keystrokes just to enter a prescription:
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2729481
Doctors need to see patients, but their bosses demand that they satisfy Epic's endless red tape. Doctors now routinely stay late after work and show up hours early, just to do paperwork. It's not enough. According to another one of Kuttner's sources, doctors routinely copy-and-paste earlier entries into the current one, a practice that generates rampant errors. Some just make up random numbers to fulfill Epic's nonsensical requirements: the same source told Kuttner that when prompted to enter a pain score for his TB patients, he just enters "zero."
Don't worry, Epic has a solution: AI. They've rolled out an "ambient listening" tool that attempts to transcribe everything the doctor and patient say during an exam and then bash it into a visit report. Not only is this prone to the customary mistakes that make AI unsuited to high-stakes, error-sensitive applications, it also represents a profound misunderstanding of the purpose of clinical notes.
The very exercise of organizing your thoughts and reflections about an event – such as a medical exam – into a coherent report makes you apply rigor and perspective to events that otherwise arrive as a series of fleeting impressions and reactions. That's why blogging is such an effective practice:
https://pluralistic.net/2021/05/09/the-memex-method/
The answer to doctors not having time to reflect and organize good notes is to give them more time – not more AI. As another doctor told Kuttner: "Ambient listening is a solution to a self-created problem of requiring too much data entry by clinicians."
EHRs are one of those especially hellish public-private partnerships. Health care doctrine from Reagan to Obama insisted that the system just needed to be exposed to market forces and incentives. EHRs are designed to allow hospitals to win as many of these incentives as possible. Epic's clinical care modules do this by bombarding doctors with low-quality diagnostic suggestions with "little to do with a patient’s actual condition and risks," leading to "alert fatigue," so doctors miss the important alerts in the storm of nonsense elbow-jostling:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5058605/
Clinicians who actually want to improve the quality of care in their facilities end up recording data manually and keying it into spreadsheets, because they can't get Epic to give them the data they need. Meanwhile, an army of high-priced consultants stand ready to give clinicians advise on getting Epic to do what they need, but can't seem to deliver.
Ironically, one of the benefits that Epic touts is its interoperability: hospitals that buy Epic systems can interconnect those with other Epic systems, and there's a large ecosystem of aftermarket add-ons that work with Epic. But Epic is a product, not a protocol, so its much-touted interop exists entirely on its terms, and at its sufferance. If Epic chooses, a doctor using its products can send files to a doctor using a rival product. But Epic can also veto that activity – and its veto extends to deciding whether a hospital can export their patient records to a competing service and get off Epic altogether.
One major selling point for Epic is its capacity to export "anonymized" data for medical research. Very large patient data-sets like Epic's are reasonably believed to contain many potential medical insights, so medical researchers are very excited at the prospect of interrogating that data.
But Epic's approach – anonymizing files containing the most sensitive information imaginable, about millions of people, and then releasing them to third parties – is a nightmare. "De-identified" data-sets are notoriously vulnerable to "re-identification" and the threat of re-identification only increases every time there's another release or breach, which can used to reveal the identities of people in anonymized records. For example, if you have a database of all the prescribing at a given hospital – a numeric identifier representing the patient, and the time and date when they saw a doctor and got a scrip. At any time in the future, a big location-data breach – say, from Uber or a transit system – can show you which people went back and forth to the hospital at the times that line up with those doctor's appointments, unmasking the person who got abortion meds, cancer meds, psychiatric meds or other sensitive prescriptions.
The fact that anonymized data can – will! – be re-identified doesn't mean we have to give up on the prospect of gleaning insight from medical records. In the UK, the eminent doctor Ben Goldacre and colleagues built an incredible effective, privacy-preserving "trusted research environment" (TRE) to operate on millions of NHS records across a decentralized system of hospitals and trusts without ever moving the data off their own servers:
https://pluralistic.net/2024/03/08/the-fire-of-orodruin/#are-we-the-baddies
The TRE is an open source, transparent server that accepts complex research questions in the form of database queries. These queries are posted to a public server for peer-review and revision, and when they're ready, the TRE sends them to each of the databases where the records are held. Those databases transmit responses to the TRE, which then publishes them. This has been unimaginably successful: the prototype of the TRE launched during the lockdown generated sixty papers in Nature in a matter of months.
Monopolies are inefficient, and Epic's outmoded and dangerous approach to research, along with the roadblocks it puts in the way of clinical excellence, epitomizes the problems with monopoly. America's health care industry is a dumpster fire from top to bottom – from Medicare Advantage to hospital cartels – and allowing Epic to dominate the EHR market has somehow, incredibly, made that system even worse.
Naturally, Kuttner finishes out his article with some antitrust analysis, sketching out how the Sherman Act could be brought to bear on Epic. Something has to be done. Epic's software is one of the many reasons that MDs are leaving the medical profession in droves.
Epic epitomizes the long-standing class war between doctors who want to take care of their patients and hospital executives who want to make a buck off of those patients.

Tor Books as just published two new, free LITTLE BROTHER stories: VIGILANT, about creepy surveillance in distance education; and SPILL, about oil pipelines and indigenous landback.
If you'd like an essay-formatted version of this post to read or share, here's a link to it on pluralistic.net, my surveillance-free, ad-free, tracker-free blog:
https://pluralistic.net/2024/10/02/upcoded-to-death/#thanks-obama
Image: Flying Logos (modified) https://commons.wikimedia.org/wiki/File:Over_$1,000,000_dollars_in_USD_$100_bill_stacks.png
CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0/deed.en
#pluralistic#ehrs#robert kuttner#tres#trusted research environments#ben goldacre#epic#epic systems#interoperability#privacy#reidentification#deidentification#thanks obama#upcoding#Hierarchical Condition Category#medicare#medicaid#ai#American Recovery and Reinvestment Act#HITECH act#medicare advantage#ambient listening#alert fatigue#monopoly#antitrust
812 notes
·
View notes
Text
this is a shortened works cited from my thesis, pulling out the sources about American intersex history and activism from the past 30 years. i have pdfs for most of the sources there, if there's something that isn't linked send me a message and i can try to find it!
just thought i'd try to put a lot of intersex history sources in one place.
Works Cited:
Amato, Viola. “The Intersex Movement of the 1990s: Speaking Out Against Medical and Narrative Violence.” In Intersex Narratives: Shifts in the Representation of Intersex Lives in North American Literature and Popular Culture, 55–102. Transcript Verlag, 2016. http://www.jstor.org/stable/j.ctv1xxrsz.6.
Bauer, Markus, Daniela Truffer and Daniela Crocetti. “Intersex Human Rights.” The International Journal of Human Rights. 24, no.6. (2020):724-749.https://doi.org/10.1080/13642987.2019.1671354
Brown, Lydia X.Z., Erickson, Loree, da Silva Gorman, Rachel, Lewis, Talila A., McLeod, Lateef, and Mingus, Mia. “Radical Disability Politics.” In Routledge Handbook of Radical Politics, edited by A.J. Withers and Liat Ben-Moshe, 178-193. Routledge, 2019.
Cameron, David. “Hermaphrodites With Attitude.” Newsletter. 1994. https://isna.org/library/hwa/
Carpenter, Morgan. “Fixing bodies and shaping narratives: Epistemic injustice and the responses of medicine and bioethics to intersex human rights demands.” Clinical Ethics. 2024;19, no. 1. (2024) :3-17. doi:10.1177/14777509231180412
Chase, Cheryl. “Hermaphrodites with Attitude: Mapping the Emergence of Intersex Political Activism.” Journal of Lesbian and Gay Studies. 4, no.2, (1998): 189-211.
---, Hermaphrodites Speak! 1997; Rohnert Park: Intersex Society of North America. Video tape.
Cohen, Julie, dir. Every Body. 2023; United States: Focus Features, DVD.
Denny, Dallas. "Chrysalis Quarterly, Vol. 2 No. 5 (Fall, 1997 / Winter, 1998)." Periodical. 1998. Digital Transgender Archive, https://www.digitaltransgenderarchive.net/files/7s75dc39s (accessed April 08, 2024).
Davis, Georgiann. “Introduction: Normalizing Intersex: The Transformative Power of Stories.” in Voices: Personal Stories from the Pages of Narrative Inquiry in Bioethics: Normalizing Intersex, edited by James DuBois and Ana Iltis. 1-4. John Hopkins University Press, 2016.
Dreger, Alice. “Rejecting the Tranquilizing Drug of Gradualism in Intersex Care.” Alice Dreger (blog). November 2015. Accessed April 9, 2024. https://alicedreger.com/dsd_human_rights/
Dreger, Alice and April Herndon. “Progress and Politics in the Intersex Rights Movement: Feminist Theory in Action.” Journal of Lesbian and Gay Studies. 15, no. 2. (2009): 199-224.
Fausto-Sterling, Ane. Sexing the Body: Gender Politics and the Construction of Sexuality. New York: Basic Books. 2000.
“A Framework for Intersex Justice.” Intersex Justice Project. 2021. Accessed April 8, 2024. https://www.intersexjusticeproject.org/intersex-justice-framework.html
"FTM Newsletter #37." Periodical. 1997. Digital Transgender Archive, https://www.digitaltransgenderarchive.net/files/kd17cs89j (accessed April 08, 2024).
Hegarty, Peter, Marta Prandelli, Trove Lundberg, Lih-Mei Liao, Sarah Creighton, and Katrina Roen.”Drawing the Line Between Essential and Nonessential Interventions on Intersex Characteristics With European Health Care Professionals.” Review of General Psychology. 25, no 1. (2020): 101-114.
Hermaphrodites With Attitude. "Hey AAP! Get Your Scalpels Off Our Bodies! Flyer." Ephemera. 1990. Digital Transgender Archive, https://www.digitaltransgenderarchive.net/files/qj72p712h (accessed April 08, 2024).
“Hermaphrodites With Attitude,” Intersex Society of North America. 2006. Accessed April 8, 2024. https://isna.org/library/hwa/
“How To: Organize an #EndIntersexSurgery Protest in your hometown--a toolkit created by Intersex Justice Project (IJP.” Intersex Justice Project. 2019. Accessed April 8, 2024. https://webarchive.loc.gov/all/20191111232744/https://docs.google.com/document/d/1EgYy2jfSO04HF_FGv-8RXYEgWW422L-RB7oxMOaIiBc/edit
Hughes, Ieuan, Christopher Houk, Syed Faisal Ahmed, Peter Lee, and LWPES1/ESPE2 Consensus Group. “Consensus Statement on Management of intersex disorders.” Disease in Childhood. 91, no.7. (2006): 554-563. doi: 10.1136/adc.2006.098319
“I Want to Be Like Nature Made Me: Medically Unnecessary Surgeries on Intersex Children in the US.” Human Rights Watch. InterACT. July 2017, accessed April 8, 2024. https://www.hrw.org/sites/default/files/report_pdf/lgbtintersex0717_web_0.pdf
“InterACT Statement on Intersex Terminology.” InterACT: Advocates for Intersex Youth. 2015. Accessed April 8, 2024. https://interactadvocates.org/interact-statement-on-intersex-terminology/#:~:text=interACT's%20use%20of%20terminology%20and,of%20the%20term%20%E2%80%9Cintersex%E2%80%9D.
Lindhal, Hans. “Is PCOS an Intersex Condition? Here’s 5 Reasons Why Some Say Yes.” HansLindhal.Com (Blog). February 2023, Accessed April 7, 2024. https://hanslindahl.com/blog/is-pcos-an-intersex-condition
---., “9 Young People on How They Found Out They Are Intersex.” Teen Vogue. October 2019. Accessed April 10, 2024. https://www.teenvogue.com/gallery/young-people-on-how-they-found-out-they-are-intersex
“M.C v. Aaronson.” Southern Poverty Law Center. 2017. Accessed April 8, 2024. https://www.splcenter.org/seeking-justice/case-docket/mc-v-aaronson
Merrick, Ten. “From ‘Intersex’ to ‘DSD’: A Case of Epistemic Injustice.” Synthese 196, no. 11 (2019): 4429–47. http://www.jstor.org/stable/45220035.
Orr, Celeste. Cripping Intersex. University of British Columbia Press, 2022.
Pagonis, Pidgeon. “#EndIntersexSurgery Protest At Lurie Children’s Hospital Recap + 5 Ways To Get Involved.” Intersex Justice Project. 2018. Accessed April 8, 2024. https://www.intersexjusticeproject.org/blog/endintersexsurgery-protest-at-lurie-childrens-hospital-recap
Pagonis, Pidgeon and Sean Saifa Wall. “Open Letter to AIS-DSD Support Group.” EndIntersexSurgery. Intersex Justice Project. February 2018. Accessed April 8, 2024. http://www.endintersexsurgery.org/
Redick, Alison. “What Happened at Hopkins: The Creation of the Intersex Management Protocols. Cardozo Journal of Law & Gender. 12 (2005): 289-296
Reid, Graeme, and Minky Worden. “Caster Semenya Won Her Case, But Not the Right to Compete.” Human Rights Watch. July 2023. Accessed April 10, 2024. https://www.hrw.org/news/2023/07/18/caster-semenya-won-her-case-not-right-compete
Reis, Elizabeth. Bodies in Doubt: An American History of Intersex. John Hopkins Press, 2021.
---, “Did Bioethics Matter? A HIstory of Autonomy, Consent, and Intersex Genital Surgery. Medical Law review. 27, no.4, (2019):658-674. https://doi.org/10.1093/medlaw/fwz007
Rios-Espinosa, Carlos, Koomah, Syrus Marcus Ware, and Sean Saifa Wall. “Liberating All Bodies: Disability Justice & Intersex Justice In Conversation.” Webinar at the Crip Camp Impact Team and Human Rights Watch Film Festival, United States, October 2020.
Rubin, David, Michelle Wolff and Amanda Lock Swarr. “Creating Intersex Justice: Interview with Sean Saifa Wall and Pidgeon Pagonis of the Intersex Justice Project.” Transgender Studies Quarterly. 9, no. 2. (2022): 187-195. https://doi.org/10.1215/23289252-9612823
Sharman, Zena. “Intersex Justice and the Care We Deserve: ‘I Want People to Feel at Home in Their Bodies Again.’” Ms. Magazine. 2022. Accessed April 8, 2024. https://msmagazine.com/2022/02/03/intersex-justice-the-care-we-dream-of-queer-trans-healthcare/
Sharpe, Sam. “No one-size-fits all: Myths and Misconceptions about PCOS.” InterACT: Advocates for Intersex Youth. Advocates for Informed Choice. October 2022. Accessed on April 7, 2024. https://interactadvocates.org/no-one-size-fits-all-myths-and-misconceptions-about-pcos/
Spurgas, Alyson. “(Un)Queering Identity: The Biosocial Production of Intersex/DSD.” in Critical Intersex edited by Morgan Holmes. 97-122. Ashgate Publishing, 2009.
Tamar-Matis, Anne. “ Advocates for Informed Choice, Newsletter Fall 2007.” Newsletter. 2007. AIC Legal .https://aiclegal.wordpress.com/wp-content/uploads/2010/02/fall-07-newsletter-final.pdf
---. “Advocates for Informed Choice: Newsletter Spring 2008.” Newsletter. 2008. AIC Legal.https://aiclegal.wordpress.com/wp-content/uploads/2010/02/spring-08-final.pdf
---. “Advocates for Informed Choice: Newsletter Summer 2009.” Newsletter. 2009. AIC Legal.https://aiclegal.wordpress.com/wp-content/uploads/2010/02/aic-2009-summer-newsletter-pdf.pdf
---. “Advocates for Informed Choice: Spring 2010 Newsletter.” Newsletter. 2010. AIC Legal.https://us1.campaign-archive.com/?u=f8291560ebb2dafc25097480f&id=5803ec8c71
---., “June 2011: Promoting the Civil Rights of Children Born With Variations of Sex Anatomy.” Newsletter. 2011. AIC Legal. https://us1.campaign-archive.com/?u=f8291560ebb2dafc25097480f&id=cec68ddac
---.. “June 2012: Promoting the Civil Rights of Children Born With Variations of Sex Anatomy.” Newsletter. 2012. AIC Legal. https://us1.campaign-archive.com/?u=f8291560ebb2dafc25097480f&id=b4d4dd90cf
---. “ 2012 Annual Report.” Newsletter. 2012. Advocates for Informed Choice. https://interactadvocates.org/wp-content/uploads/2016/06/AIC-2012-Annual-Report.pdf
---. “2013 Annual Report. “ Newsletter. 2012. Advocates for Informed Choice. https://interactadvocates.org/wp-content/uploads/2016/06/2013-annual-report-FIN1.pdf
“US: Anti-Trans Bills Also Harm Intersex Children.” Human Rights Watch. October 22. Accessed April 10, 2024. https://www.hrw.org/news/2022/10/26/us-anti-trans-bills-also-harm-intersex-children
Vecchietti, Valentino. “A Journey to the Intersex-Inclusive Pride Flag.” Global Inclusive Pride Flag. Intersex Equality Rights. 2021. Accessed April 7, 2024. https://www.globalinclusiveprideflag.com/
Wilchins, Riki Anne. "In Your Face No. 5 (Spring 1998)." Newsletter. 1998. Digital Transgender Archive, https://www.digitaltransgenderarchive.net/files/vq27zn45k (accessed April 08, 2024).
Withers, AJ. Disability Politics and Theory. Fernwood Publishing, 2012.
Woo, Elaine. “David Reimer, 38; After Botched Surgery, He was Raised as a Girl in Gender Experiment.: Los Angeles Times. May 2004. Accessed April 8, 2024. https://www.latimes.com/archives/la-xpm-2004-may-13-me-reimer13-story.html
200 notes
·
View notes
Text
Hi, everyone.
Yesterday, I shared here a series of posts written by a girl named Nada Bedair on Twitter, where she discussed new information, she learned after watching a documentary.

It was revealed in this documentary that Israel has something called the "Bank of Skins," which is the largest skin bank in the world, specializing in treating burns, skin cancer, and more.
In this documentary, it became clear that most of these skins did not belong to Israeli soldiers but were taken from the bodies of deceased Palestinians, their identities deliberately obscured through disfigurement or lack of proper autopsy.
At the same time, numerous reports emerged from Palestinians, stating that after the arrest of individuals from Gaza and the West Bank, their families were surprised by their return as deceased, with their bodies missing certain body organs!
Simultaneously, an article was published by the head of the Forensic Medicine Institute, claiming that Israel kills and harvests organs from deceased Palestinians without their consent or their families' consent!
Here is the link to the complete post, including the sources: https://www.tumblr.com/storiesfromgaza/732558400585613312/today-i-learned-about-something-terrible-and-i?source=share
It is crucial that you read this before continuing with this article.

After I shared it yesterday, @chimaeraonwards wrote a comment, attaching a link to a Journal Article | Social Research by anthropologist Nancy Scheper-Hughes titled, "The Body of the Terrorist: Blood Libels, Bio-Piracy, and the Spoils of War at the Israeli Forensic Institute." In this article, the author describes in detail what happened and how it happened in around 38 pages.
you can read it here:
Scheper-Hughes, N. (2011). The Body of the Terrorist: Blood Libels, Bio-Piracy, and the Spoils of War at the Israeli Forensic Institute. Social Research, 78(3), 849–886. http://www.jstor.org/stable/23347019
Your reading of it won't take much of your time, but it will significantly increase your awareness of things you might not have imagined happening!
If reading it is a challenge, it's worth to mention that yesterday, @chimaeraonwards did an amazing thing. She wrote a breakdown of some of the content of the 38-page article. Ensure you read it; it's not very long, but it's highly enlightening. Link: https://www.tumblr.com/chimaeraonwards/732568635164524544/whatever-youre-thinking-about-this-its-actually?source=share Support her by sharing it because she truly deserves it.
#gaza#palestine#gaza strip#free gaza#free palestine#storiesfromgaza#غزة#فلسطين#genocide#humanitarian crisis
662 notes
·
View notes
Text
We should journal and record what the pandemic hoax was really like...and I mean offline... because I have a feeling this is one the history books and digital world are going to intentionally forget about.
Like remember how they had stores where "for your safety" you were only allowed to buy products they deemed essential. Remember going into a store and sections were roped off and the fucking stores wouldn't let you buy certain things.
I remember going into a dollar store to buy emergency supplies but they were deemed non essential because they were in the camping/outdoor section. I remember that they had employees...regular ass people doing a minimum wage job walking around and harassing customers who were trying to buy anything but food or medicine. Because apparently if you buy food at the store covid wouldn't get you but if you bought a book you were sure to kill yourself and everyone around you. All this during a stage of this "pandemic" where nobody you knew had even heard of anyone who was sick...this was before the jabs came out and people really started "Dying of covid."
You could write a whole chapter about all the times some karen told you to put on a mask and you had to resist the urge to feed them theirs. And remember when they changed the meaning of karen midstream to apply to people who wanted to be left alone and not wear a mask instead of insane entitled people desperate for a sense of power over otherswho make unreasonable demands...like someone who approaches strangers to demand they cover their face so they feel less afraid.
1K notes
·
View notes
Text
EMERGENCY, NEED $470 By 12 November, 🍉🇵🇸🫂💔
URGENT, URGENT For mum's medicine "chronic heart and high-pressure patient" & Ahmed bro education.
•Vetted by @el-shab-hussein @nabulsi list #220, @gaza-evacuation-funds list
• GFM campaign
https://www.gofundme.com/f/last-call-last-attempt-save-our -kids-from-gaza-crisis
• PAYPAL link
Every share and small donations helps tremendously right now!



Still faraway, even €10, €20, €50 at least can make difference, don't skip without do anything bug U 😔💔🫂
@plomegranate @p0pp3t @palestinianstatemedia @kittykatrattie @loverboy-ish @lesbiannova @lupe-jess @languageoclock @lovecatsys @anneemay @appsa @neptunerings @nostalgic-muffins @a-shade-of-blue @a-possums-journal @a-sky-of-diamonds @a-skywalkers @cosmicgamerboy @commissions4aid-international @sunbirdbooks @official-saul-goodman @nabulsi @90-ghost @sar-soor @palipunk @zvaigzdelasas @titsay @an-elegant-void @acehimbo @aces-and-angels @jezior0 @mansbutchery @dk65 @dromaeo-sauridae @doublycharming-tetraquark @surprisebitch @everlastingrandom @egirl-vrissy @error-core-animations @rosetowers @rice-ballin @robboybot @eunillul @worms-are-better-than-me @withthewindinherfootsteps @wannabeavocaloidmystery @weenkinks @wabatle
#free palestine#gaza#gaza genocide#save children#هنا غزة#palestine#5 reblogs#watermelon#viralpost#vetted#free gaza#free 🍉#palestine fundraiser#gaza vetted fundraiser#kamala harris#donation matches#donate if you can#donald trump#us elections#artists on tumblr#palestine mutual aid#vetted campaign#save cat#charity#bb26#mutual aid#save Palestinian kids#gofundme#غزة#cats of tumblr
68 notes
·
View notes
Text
Acral Calcified Angioleiomyoma Along with Radiological Features

Acral Calcified Angioleiomyoma Along with Radiological Features in Biomedical Journal of Scientific & Technical Research
Angioleiomyoma (ALM) is a rare benign, vascular smooth muscle tumor originating from the tunica media of the vessel wall. It typically arises in the cutaneous, subcutaneous tissue of the lower extremities in middle-aged women. The author has previously described the solid subtype of ALM as a painful and vascularized subcutaneous tumor and indicated that all painful cutaneous and subcutaneous tumors used as the acronym “ENGLAND” or “LEND an EGG” show vascularized appearances on high-resolution color Doppler ultrasonography (US). Whereas ALMs of the fingers, toes, hands, and fee as acral type, namely acral calcified ALMs are rarely found. Kacerovska et al. mentioned that the lesion was pathologically composed of mature smooth muscle cells and vascular pattern accompanied with the prominent calcifications. In this article, the current knowledges of the acral calcified ALM have been reviewed in detail. Based on the evidence, acral calcified ALM pathologically shows the changes including calcification, sometimes extensive calcification hyalinization, and bleeding. Similar to the ordinary ALM, it is putative that acral calcified ALM also tends to represent painful and pathologically vascularized tumor. In addition to the characteristic manifestation of painful and vascularized tumor on color Doppler US, an acral calcified ALM should be considered as the differential diagnosis if the mass shows the calcification on high-resolution US in acral regions.
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01 Follow on Blogger : https://biomedres01.blogspot.com/ Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Biomedical Imaging#Journals on Emergency Medicine#Journals on Cancer Medicine#open access journals of biomedical science#journal of biomedical research and reviews impact factor
0 notes
Text
College Major Headcanons:
[Extra content for The Homo Economicus in Love - noritoshi kamo x reader, cute college au]
Yuuji Itadori - Media Studies, on a full sports scholarship even though he's not too interested in sports. He doesn't show up to practice that much but carries the team in tournaments. Not really very academically inclined but everyone he meets loves him so much that he's gotten a shit ton of internships and work experience just cuz he's nice to work with. Stays on campus dorms.
Nobara Kugisaki - Fashion Merchandising (yay legally blonde). Another one who's not very academically inclined but does great at the practical aspects of the job. Gets 40% off on tuition, but has some funds from her grandma. also gets money from her fashion blog, part-time jobs at fashion mags, and manages clothing for photoshoots on a freelance basis (if she commits she commits). Saves on residence by renting with Inumaki and Panda.
Megumi Fushiguro - Computer Science with a minor in Math. Full scholarship and bursary grant by the college due to his shitty financial conditions (orphaned and destitute at a young age). Prof Gojo is his legal guardian. grew up in and stays on campus dorms.
Maki Zenin - Star Athlete, literally training for the Olympics. Her degree is in Mass Communications but she doesn't actually have to attend classes cuz the Uni wants her to focus on sports. Disowned by her family. Full sports scholarship and occasionally gets sponsored by sportswear companies. Trying to go pro.
Yuuta Okkotsu - Sociology and Anthropolgy. He enjoys talking to and meeting people and works as a part-time Journalist for local news channels to bring attention to issues like poverty. Gets a bursary grant from the uni, gets paid for and is decently recognized for his journalism work. Both Geto and Gojo want to mentor him. He talks to himself when he's alone but that's a secret.
Toge Inumaki - Architectural Design, chose this degree just for the hell of it, is a solid B+ student. Has a YouTube gaming and ASMR channel with 200k followers but is struggling to monetize it profitably. Got in on legacy admissions but gets a sports scholarship of 30% (he's pretty good at athletics)
Panda - ???
Noritoshi Kamo - Economics and Finance, specializing in Private Equity and Investment Banking. he's the heir of the Kamo Conglomerate. Full legacy admission even though he graduated valedictorian of high school and is the captain of the Archery team.
Todo Aoi - Quantum Physics. he's literally the top student of every class he takes. he keeps taking random other classes from different majors based on his whims. his genius was recognised and personally mentored by Yuki Tsukumo, but is now undergoing formal college education for the certificate even though he already knows all this and more. he spends half the day in the gym and the other half streaming Takada-chan variety clips.
Mai Zenin - Economics and Finance, her family made her take it. good at academics even though she's not super into it. legacy admission.
Momo Nishimiya - Literature and Creative Writing. She posts regularly for a gender and sexuality magazine. loves nobara's blog.
Miwa Kasumi - Computer Science with a minor in Software Engineering. She just wanted a degree that would lead to a well-paying job. Cabinet Member of the Student Council. She vouched a lot for Mechamaru/Kokichi to get disability-friendly accommodation. she struggles a bit with academics but pulls through with A- all around. Kokichi/Mechamaru helps her if she finds something particularly difficult to understand. has her own campus residence but has practically moved in with Kokichi.
Arata Nitta - Health and Medicine, focusing on Emergency Care Medicine. he TAs for Prof Shoko's classes. his sister works in college admin office. has campus residence but mostly stays in the college affilitated hospital, bit of an over-worker.
Mechamaru/ Kokichi Muta - double major in Computer Science and Mechanical Engineering. Another top student of his classes. Found it a bit difficult to adjust to campus life at first (not enough disability accommodation) but with Miwa's help he got around. campus dorm with Miwa.
Professors!
Gojo Satoru - graduated from top Ivy colleges, has 5 PhDs, and wrote 1000 papers and books, and is the one of the most respected physicist in the world but insists on teaching Intro-level Physics and Math. drives a Bugatti to college. highly competitive relative grading. prescribes his own books for his class. expect a problem set every day after class. gives a lot of individual attention to students tho, n is very nice in general. he'll accept a late submission if u bring him sweets. his lockscreen is prof geto?
Geto Suguru - teaches one class named Ethics, Philosophy and Law every semester. doesn't answer questions over email, only during Office Hours. great at explaining difficult concepts, his course is the one students fight to get into and say "opened their eyes". has a devoted cult of worshipping students, voted student favorite every year. his adopted daughters took a gap year to travel abroad and he talks about them in class. he always has sweets in his pockets?
Utahime Iori - teaches modules on Economics, Politics and Philosophy courses. great teacher, very clear explanations, bumps up the grading slightly (absolute grading) and is very accommodating as a prof. hates getting emails at night tho.
Shoko Ieiri - Shitty ass prof tbh but everyone takes her class cuz she gives everyone an A. teaches Surgical Anatomy. focuses on practical experience rather than theory. she has a no attendance policy and takes few very exams or assignments.
Yuki Tsukomo - Visiting Faculty, takes one super high level class Quantum Physical Theory one semester and comes back after 4 years. Independent researcher funded by the uni.
#jujutsu kaisen#jjk#jjk yuji#yuji itadori#jjk nobara#nobara kugisaki#jjk megumi#megumi fushiguro#jjk maki#maki zenin#yuta okkotsu#jjk yuta#inumaki toge#jjk inumaki#panda#jjk panda#jjk noritoshi#noritoshi kamo#jjk mai#mai zenin#jjk momo#jjk nitta#todo aoi#kasumi miwa#jjk miwa#mechamaru#gojo satoru#suguru geto#geto suguru#yuki tsukumo
71 notes
·
View notes
Text
“[...] Like other movements within political Islam, the movement [Hamas] reflected a complex local reaction to the harsh realities of occupation, and a response to the disorientated paths offered by secular and socialist Palestinian forces in the past. Those with a more engaged analysis of this situation were well prepared for the Hamas triumph in the 2006 elections, unlike the Israeli, American, and European governments. It is ironic that it was the pundits and orientalists, not to mention Israeli politicians and chiefs of intelligence, who were taken by surprise by the election results more than anyone else. What particularly dumbfounded the great experts on Islam in Israel was the democratic nature of the victory. In their collective reading, fanatical Muslims were meant to be neither democratic nor popular. These same experts displayed a similar misunderstanding of the past. Ever since the rise of political Islam in Iran and in the Arab world, the community of experts in Israel had behaved as if the impossible was unfolding in front of their eyes. [...]
In 2009, Avner Cohen, who served in the Gaza Strip around the time Hamas began to gain power in the late 1980s, and was responsible for religious affairs in the occupied territories, told the Wall Street Journal, “the Hamas, to my great regret, is Israel’s creation.” Cohen explains how Israel helped the charity al-Mujama al-Islamiya (the “Islamic Society”), founded by Sheikh Ahmed Yassin in 1979, to become a powerful political movement, out of which the Hamas movement emerged in 1987. Sheikh Yassin, a crippled, semi-blind Islamic cleric, founded Hamas and was its spiritual leader until his assassination in 2004. He was originally approached by Israel with an offer of help and the promise of a license to expand. The Israelis hoped that, through his charity and educational work, this charismatic leader would counterbalance the power of the secular Fatah in the Gaza Strip and beyond. [...]
In 1993, Hamas became the main opposition to the Oslo Accord. While there was still support for Oslo, it saw a drop in its popularity; however, as Israel began to renege on almost all the pledges it had made during the negotiations, support for Hamas once again received a boost. Particularly important was Israel’s settlement policy and its excessive use of force against the civilian population in the territories. [...]
It also captured the hearts and minds of many Muslims (who make up the majority in the occupied territories) due [to] the failure of secular modernity to find solutions to the daily hardships of life under occupation. [...]
The new Israeli methods of oppression introduced during the Second Intifada—particularly the building of the wall, the roadblocks, and the targeted assassinations—further diminished the support for the Palestinian Authority and increased the popularity and prestige of Hamas. It would be fair to conclude, then, that successive Israeli governments did all they could to leave the Palestinians with no option but to trust, and vote for, the one group prepared to resist an occupation described by the renowned American author Michael Chabon as “the most grievous injustice I have seen in my life.” [...]
The obvious failure of the Palestinian groups and individuals who had come to prominence on the promise of negotiations with Israel clearly made it seem as if there were very few alternatives. In this situation the apparent success of the Islamic militant groups in driving the Israelis out of the Gaza Strip offered some hope. However, there is more to it than this. Hamas is now deeply embedded in Palestinian society thanks to its genuine attempts to alleviate the suffering of ordinary people by providing schooling, medicine, and welfare. No less important, Hamas’s position on the 1948 refugees’ right of return, unlike the PA’s stance, was clear and unambiguous. Hamas openly endorsed this right, while the PA sent out ambiguous messages, including a speech by Abu Mazen in which he rescinded his own right to return to his hometown of Safad. [...]”
—Ten Myths About Israel by Ilan Pappé, Chapter 9: “The Gaza Mythologies”, the section titled “Hamas Is a Terrorist Organization”
280 notes
·
View notes
Text

https://contusmpublications.com/world-journal-of-health-and-medicine.php
World Journal of Health and Medicine (ISSN: 2584-0223) Journal is an international open access and double blinded peer-reviewed journal. At the World Journal of Health and Medicine, we are dedicated to advancing the fields of health and medicine through the dissemination of high-quality research and comprehensive reviews.
#medicalresearch#medical#healthscience#healthcare#casereports#clinical#medicalcommunity#medicaleducation#clinicalpractice#healthcareprofessionals#medicine#public health#health#immune system#medical care#open access journals#emergencymedicine#emergency#sportsmedicine#pain medicine
0 notes
Text
Feb/March Podcast 2024. St Emlyn's
Our regular round up of the best of the blog with @docib and @emmanchester . Decompensated liver disease, mechanical CPR, frailty, global health and more. #FOAMed @stemlyns
Our regular round up of the best of the blog with @docib and @emmanchester . Decompensated liver disease, mechanical CPR, frailty, global health and…
View On WordPress
0 notes
Text
GUESS WHO'S BIRTHDAY IT IS!!
in honor of my birthday here are some more rescue bots headcanons!!
they (as in constructed rescue bots) have extra color receptors which allows them to see more types of light than other bots, as well as advanced hearing (they’re also the only bots with noses so they have an extra sense)
all of them have outliers (its a requirement to be a rescue bot)
blurr changed his paint job (post s4, before he showed up in rid15) because heatwave and blades basically bullied him into it
the academy where they studied was on a moon of cybertron’s, and they actually spent very little time on cybertron itself. it was sorta like a field trip spot, and they went very infrequently
quickshadow was the academy's champion shot, and she won a bunch of competitions
the rescue bots all had specialties outside of what they actually did (heatwave was a history nerd, boulder studied xenobiology, blades took journalism, chase did psychology, quickshadow was a data analyst, hightide took astronomy)
hightide was actually friends with both orion pax and megatronus separately before they realized they all knew each other
in that same vein, servo and lazerbeak were longtime friends because they grew up together
optimus is so ridiculously tolerant towards whatever the rescue bots do that they actually have a running bet on how much they can get away with before optimus gets angry (he never once has)
blurr's reputation as most annoying bot ever has been intact since way before the war when he was a racer
blades got his name through an awkward mishap at an armory that heatwave never let him live down
related to that, all the rescue bots' "names" are really more of nicknames. their names are listed on documents but their primary identification is through serial numbers because they're cold constructs
boulder had a practically bullet proof reputation at the academy as the perfect student so whenever the others wanted to get away with something they always involved him
when salvage heard about DIY's he got super into them and started making tons of pointless stuff. he never even followed the good channels, only stuff like troom troom
chase succumbs to peer pressure ridiculously easy
heatwave gives really good advice but only on accident
quickshadow and hightide like to hang out and trash talk optimus whenever he does something they don't like
blades only has field medicine training, he's not cleared for any actual treatment outside of an emergency (he can do first aid and EMT stuff but can't, like, prescribe things or do surgery). this has not stopped him from trying things though.
salvage is actually from one of cybertron's colony worlds, but he grew up on cybertron
ok here's a fun little surprise in honor of my birthday: the humans are also included in headcanons!!
kade was actually very good at gymnastics, he just got bored of it
chief burns needs glasses but he prefers to wear contacts
dani had a very extreme scene core phase, and her hairstyle is a remnant of that
frankie has super high government security clearance as a super genius and daughter of one of the world's best scientists, so she knows all kinds of military secrets
doc greene and chief burns met in childhood, doc's family moved away, and then when he got older he moved back to griffin rock and reunited with the chief
graham is the biggest night owl because of college. sometimes, when he has trouble falling asleep, the bots invite him to movie night and they all watch reruns of old movies or shows
building off that, there are two kinds of movie night: the first is with the whole burns family, rescue team, and sometimes others such as optimus or the greenes. the second is less of a movie night and more of a "we need something to do while the humans are sleeping, let's watch trashy tv all night." this kind of movie night is really just the bots (minus whoever has night shift)
professor baranova actually used to be pretty upbeat, although she was a bit misunderstood because she's neurodivergent (i also headcanon that after the whole living underwater for 28 years thing she developed DID and multiple alters to cope with the loneliness, so she's now a system)
woodrow and optimus are in a qpr. optimus refers to him as his amica, and also privately thinks of him as his human partner
doc greene at some point developed a working synthetic energon formula completely independently. when ratchet first met him (post war, probably right before he was hired to work at the rescue academy) and learned about this he lost his shit
bumblebee and dani race together all the time when he visits
this is where i'm gonna stop this post, because it's pretty late for me lol. it was my birthday today, so happy birthday to me!!
also y'all PLEASE talk to me abt any of these headcanons i will be thrilled to elaborate!
#rescue bots#tfrb#transformers rescue bots#transformers aligned#aligned continuity#tfrb heatwave#tfrb blades#tfrb boulder#tfrb chase#tfrb blurr#tfrb salvage#tfrb hightide#tfrb quickshadow#tfrb optimus#tfrb bumblebee#tfrb frankie#tfrb chief burns#tfrb graham#tfrb dani#tfrb kade#tfrb professor baranova#tfrb doc greene#doc greene#anna baranova#francine greene#frankie greene#charlie burns#kade burns#dani burns#cody burns
106 notes
·
View notes