#caspases
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Note
I'm sitting very politely and asking if it would be possible to see Adrien akumatised by Viceroy. Even if you don't want to, letting you know I'm insane about all your AUs (and your art in general, alien behaviour Shadow was so cool), you do such amazing work and I am completely normal about it








(Caspases' concept art beloooow)
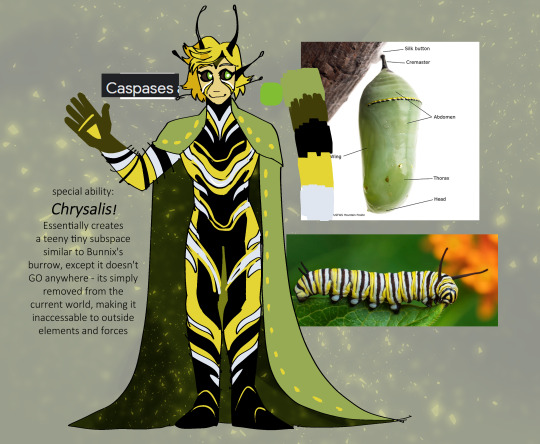
#dad villain au#marinette dupain cheng#adrien agreste#Caspases#Viceroy#Emelie Agreste#long post#Caspases is the chemical released by a caterpillar in the chrysalis that changes them into a butterfly#and his design is based off of a monarch butterfly's caterpillar :D#son of monarch after all~#anyway tom has been working on this akuma for a longass time#because he was anticipating some stupid ass shit happening to his kid#and its happening to marinette specifically on purpose btw. gabriel did something fucked up with his wish lol
6K notes
·
View notes
Note
Random ask, can I ask what are apoptosis and caspases (in simple terms)?
I have been summoned
(my 'noorie rambles. be very afraid' tag will make so much sense now. I tried to talk about it in a way that's a way that's both engaging and simple. Lots of metaphors.)
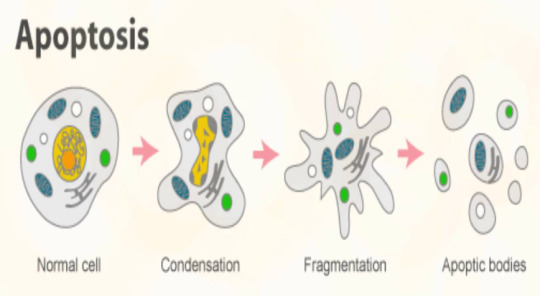
Caspases destroy the cell if it needs to die. They dismantle the cell parts as the cell membrane turns into bubbles, containing all the damaged pieces within so that a white blood cell might disposes of them. That's apoptosis in a nutshell.
But why must the cell die you ask?
Plenty of reasons. Human embryos have webbed fingers, and apoptosis causes the webbing to dissipate. Tadpoles too, use apoptosis to rid of their tails so they can become frogs. Apoptosis opposes growth - aka mitosis - and it keeps the body in homeostasis - or a balance of sorts. The destruction to mitosis's creation.
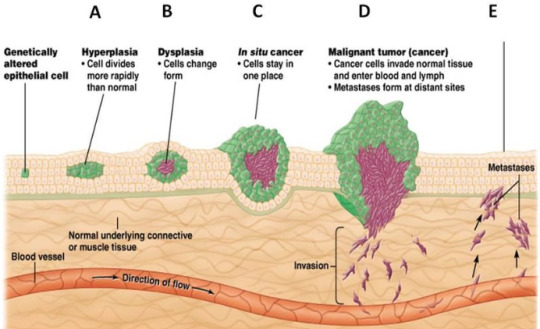
However, what I find most interesting, what is the subject of much research nowadays, and what holds the most opportunity for angsty biology fanfics (most important/j) is that apoptosis opposes tumorigenesis. In other words, if something goes wrong, if the cell gets some notion that it might try to cheat death and live forever, if it has the inklings of an idea to hijack the rest of the body through growing its own lump of cells and draining the body of its nutrients... if it decides to throw a mutiny at the expense of peace...
Then the cellular system realizes, and it activates the caspases.
(Usually how a cell 'decides' is when something wrong happens with genetic replication, mutations and such and such. There are two labels of genes relating to this. Proto-oncogenes promote cell growth and avoid apoptosis - these are the creation genes, the ones that wish to achieve the heights of production and throw all caution to the wind. Whereas tumor suppressor genes are... tumor suppressors. They are the little 'angel on the cell's shoulder' that says 'you've done wrong, now commit cell death and accept your fate'. When a proto-oncogene mutates, it becomes an oncogene. Basically, the genes that said to grow for the sake of the body now says to grow at the expense of the body, the 'devil on the cell's shoulder' won... and now it'll try to cheat death)
Caspases are a type of enzyme, which is a subset of proteins. I like thinking about it like this: enzymes are witches, spell crafters. Proteins in general function like worker bees, but enzymes are the ones who actively create and destroy, the ones that change the way the universe manifests so life can exist. They utilize reactants from their environment - materials which they are named after, such as proteases that cleave other proteins - to either create larger, energy storing molecules (endergonic reactions), or break down large, energy storing molecules to release energy (exergonic reactions).
(One type of enzyme that I like is called kinases, they basically initiate things, they tell the cell 'it's okay to do things' or 'this will be dangerous, let's not do that', or 'oof this cell doesn't have the proper genes, that could be a problem, how about we destroy everything so this doesn't become a big issue?')
When the cell needs to die, the caspases activate.
Humans have 14 caspases. I wish I knew what all of them are, but the pub med articles I read do not have a whole list of them like a pokedex from pokemon (at least that I have read so far, after ap testing there's one article I want to read that seems to have ANSWERS to a lot of my questions)
So imagine this, the cell has lots of caspases floating around in the cytoplasm/water jelly environment. These beings of death in huge numbers in a perpetual slumber, just floating around, until the cell decides it needs them to destroy its existence, and it activates them.
(ALTHOUGH some of my questions refer to the "caspase-dependent non-lethal cellular processes", so far what I've been able to find is that if the cell needs some repair to the cytoskeleton/structure of the cell, then it activates a few caspases to destroy parts of it, so that the repair may start.)
There are two types: inflammatory caspases (if I remember correctly, this is caspase 1,4, and... a few others I'll have to check) and apoptotic caspases. What we're interested in are the apoptotic caspases. Initiator caspases get activated first. The way I story-fy them/see them in my head is as the older sibling types who condone violence. If the cell needs to die because of an external signal - a message from far away to destroy itself, to which it must oblige - then caspase 8 activates. If the cell needs to die because of an internal signal - something inside isn't right, and what a havoc it would be to pass that on through replication, so the proteins decide the fate of the world it lives in, and it choses death for the sake of the wider body- then caspase 9 activates.
Both these initiator caspases cleave (meaning 'cut', these inactive beasts are not yet 'complete', so they need further modification after activation to work properly. If the cell were to create caspases fully functional and finished, the large number of caspases would kill the entire cell, so they don't finish, they subdue the ones behind their death, and make sure to regulate their slumber.) their 'younger, violent siblings': caspase 7 and caspase 3. The doll I have is a caspase 3.
(I've found more information on them than caspase 7... although.. the one article I found.... it should have information on them all, the amount of searching I've done for those sorts of answers... but alas... I need to read the material for the ap bio exam... which does not include caspases.... one day...)
Caspase 3, as far as I could gather, destroys the cytoskeleton. The cytoskeleton supports the entire cell, acting as the 'tent poles' that keep the floppy cell membrane from collapsing. Collapsing, however, is exactly what the caspase 3 wants. It dismantles the whole thing, along with activating and inactivating a slew of other proteins. (it's an assassin basically.)
And with this, the caspases bow, for the cell is separated within these small little 'blebs' (they look like bubbles) and the cell is destroyed.
OH AND LAST LITTLE THING!
If something inhibits the caspases, the cell goes through with necrosis, which is basically instead of becoming little bubbles, the cell membrane ruptures and the cell 'guts spill out'
THANK YOU SO MUCH FOR THE ASK!! <3 <3 I got to blabber about caspases and it gave me happy sparkles.
ALSO, here's the doll I made for caspase 3:
#biology#scientists#science#apoptosis#enzymes#caspases#science side of tumblr#science side of the internet#noorie infodumps. be very afraid#noorie answers asks#lobotomy for my brainrot
9 notes
·
View notes
Video
tumblr
Life or Death
When it comes to our health, death is just as important as life. Apoptosis – a type of cell death – is vital to keep everything balanced. Too much cell death can lead to neurodegenerative conditions, whereas not removing abnormal cells can result in cancer. The process of apoptosis culminates with enzymes called caspases dismantling the cell. Once caspases swing into action, there is no going back for that cell – or so we thought. Researchers activated apoptosis in cells for a limited time and then tracked whether they would survive. Despite the build-up of ‘executioner’ caspases in the cell (green), cells were able to come back from the brink of death. In the centre of the frame, a cell divides to become two – something that a cell sentenced to death wouldn’t be able to do. This could be another way that a cancer could return even after treatment.
Written by Sophie Arthur
Video from work by Maddalena Nano and colleagues
Molecular, Cellular, and Developmental Biology Department, University of California, Santa Barbara, CA, USA
Video copyright held by original authors
Published in Proceedings of the National Academy of Science (PNAS), January 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#neuroscience#apoptosis#cells#cell death#caspases#immunofluorescence#neurodegenerative conditions
12 notes
·
View notes
Text




Caspase Cascade 一次創作でゲームを作ろうとしていて、最近はシナリオやキャラクターをねりねりしています。 作り始めてもう2年も経ちました。早く世に出したくて、キャラクターやぼんやりとした設定だけ小出しにしています。
2 notes
·
View notes
Text
youtube
#NLRP3 inflammasome#multiple myeloma#inflammation#cytokine release#tumor microenvironment#IL-1β#IL-18#pro-inflammatory cytokines#tumor progression#immune suppression#bone resorption#MM pathogenesis#apoptosis resistance#plasma cells#caspase-1#ASC#NLR proteins#immunotherapy#chronic inflammation#therapeutic strategies.#Youtube
0 notes
Text
Caspase 8 Market Overview, Competitive Analysis and Forecast 2031
0 notes
Text
Caspase
185 notes
·
View notes
Text
الثواني الأخيرة من حياة خلايانا العصبية..
هكذا تموت الخلية العصبية
***
من المعروف أنّ الخلايا في أجسامنا تموت طوال الوقت، لكن المُدهش هو سرعة موتها التي أكّد العلماء أنّه بطيء
ينتقل الموت في موجات متواصلة من خلا�� الخلية، يتحرك بمعدل 30 ميكرومتر كل دقيقة، بحسب ما ذكر فريق من علماء من جامعة ستانفورد
على سبيل المثال:
الخلايا العصبية التي يمكن أن يصل حجم جسمها إلى 100 ميكرومتر، يمكن أن تستغرق 3 دقائق و 20 ثانية للموت
قد يبدو ذلك غير طبيعي، لكن هذا المدّ القاتل بالتحديد هو الذي يبقينا على قيد الحياة وبصحة جيدة
***
إذن، ما معنى موت الخلية المبرمج ؟
عملية منظمة طبيعية تتطلب طاقة، وتحدث هذه العملية من خلال تنشيط مجموعة من الإنزيمات تُسمى «Caspases» مما يؤدي إلى مجموعة من الأحداث المتتابعة التي تؤدي في نهاية إلى موت الخلية
هناك العديد من المحفزات والظروف الطبيعية والمرضية التي تُنبه هذه العملية، مع حدوث إختلاف في إستجابة الخلايا المختلفة لنفس المحفز
يحدث موت الخلية المبرمج طبيعيًا كجزء من مراحل نمو الخلية للحفاظ على توازن أعداد الخلايا في الأنسجة المختلفة، كما أنه قد يحدث كآلية دفاعية كإزالة الخلايا المتضررة من مرض أو خلافه بشكل لا يمكن إصلاحه
**
خطوات موت الخلية المبرمج:
تبدأ عملية موت الخلية بإنكماش الخلية حيث يصبح حجمها أصغر، ثم تتكثف «كروماتينات» المادة الوراثية داخل النواة وهو ما يُعد الصفة المميزة لعملية موت الخلية المبرمج
ثم يتكسر «الهيكل الخلوي» ليفقد الغشاء البلازمي شكله المميز ليتكون به عديد من البروزات والانتفاخات ثم تتمزق نواة الخلية لتتحول بذلك الخلية إلى أجزاء صغيرة يتكون كٌل منها من جزء من سيتوبلازم الخلية مع عُضيات عالية التكثف وقد يوجد فيها جزء من نواة الخلية أيضًا، مع العلم أنها مُحاطة بالغشاء البلازمي للخلية الذي لا يزال سليم، بعد ذلك تقوم الخلايا البلعمية بابتلاع هذه الأجسام
ومن المُلاحظ أنه لا يوجد أي إلتهاب مصاحب لعملية موت الخلية المبرمج أو ابتلاعهت
*
-موت الخلية الغير مبرمج (النخر الخلوي)
يختلف "موت الخلية المبرمج" عن عملية «النخر الخلوي»
حيث أن عملية النخر الخلوي تعتبر عملية سامة تموت فيها الخلية دون الحاجة إلى طاقة
هي عملية غير منظمة أو مبرمجة تموت فيها مجموعة من الخلايا معًا، على عكس إنتحار الخلية الذي يُعتبر عملية مبرمجة تتطلب وجود طاقة وتموت فيها خلية مفردة
*
من التغيرات الأساسية التي تحدث في شكل الخلية خلال النخر الخلوي: تنتفخ الخلية، تتكون فجوات في الستوبلازم، إنتفاخ الشبكة الإندوبلازمية، إنتفاخ الميتوكوندريا أو ��نفجارها، إنفصال الريبوسوم وتحطم الغشاء الخلوي مما يؤدي إلى وصول مكونات السيتوبلازم للأنسجة المجاورة التي تفرز مواد كيميائية تجذب الخلايا الإلتهابية
أي يحدث إلتهاب في الأنسجة المجاورة، بينما لا يحدث أي إلتهاب في حالة موت الخلية المبرمج
*
الخلية التي تقرر أن ترفض الحياة تُشبه إلى حد كبير الإنسان الذي يرفض الحياة، كلاهما تبدأ قصته بالإنفصال عن النسيج المحيط، يتحلل كلٌ منهما داخليًا ويموت، دون أن يعلم أي من النسيج المحيط بذلك
*
تلعب عملية موت الخلية دورًا مهمًا في الحفاظ على توازن أعداد الخلايا في الجسم خلال مراحل النمو المختلفة:
خلال تكوين الجهاز العصبي، يتم تكوين أعداد كبيرة من الخلايا العصبية ثم تموت الخلايا التي لم تنجح في تكوين تشابكات عصبية وظيفية
كذلك خلال تكوين الجهاز المناعي في الجسم، يتم تكوين أعداد كبيرة من الخلايا المناعية ثم تموت خلايا المناعة التي لم تنجح في أن تكون متخصصة لمهاجمة الأجسام الغريبة عن الجسم فقط
كما تلعب عملية إستماتة الخلية دورًا هامًا في تخليص الجسم من الخلايا المريضة والخلايا الإلتهابية خلال عملية إلتئام الجروح
*
مما سبق، يتضح أن عملية موت الخلية المبرمج يجب أن تكون منظمة بدقة، لأن موت الخلايا بدرجة أكبر من اللازم أو أقل من اللازم قد يؤدي إلى أمراض خطيرة تتضمن السرطان، نقص النمو، أمراض المناعة الذاتية وأمراض الجهاز العصبي مثل: «مرض باركنسون» و«مرض الألزهايمر»
*
لقد تم التعرف على الكثير من البروتينات والإنزيمات المُنظمة لعملية موت الخلية إلا أن آليات عملها وتنشيطها أو تثبيطها ما زالت غير مفهومة بصورة كاملة
33 notes
·
View notes
Text

I will heal you
@bigfatbreak AU is having me on the edge I’m loving it. Caspases is one of my favorite things in the AU so far I wanted to draw him with Marinette.
#ml AU#bigfatbreak#ml marinette#ml adrien#miraculous ladybug#miraculous tales of ladybug and chat noir#my art#ml art#ml fan art#miraculous#illustration#em doddles art#dad villian AU
61 notes
·
View notes
Text
Retinal and choroidal vascular drop out in a case of severe phenotype of Flammer Syndrome. Rescue of the ischemic-preconditioning mimicking action of endogenous Erythropoietin (EPO) by off-label intra vitreal injection of recombinant human EPO (rhEPO) by Claude Boscher in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Background: Erythropoietin (EPO) is a pleiotropic anti-apoptotic, neurotrophic, anti-inflammatory, and pro-angiogenic endogenous agent, in addition to its effect on erythropoiesis. Exogenous EPO is currently used notably in human spinal cord trauma, and pilot studies in ocular diseases have been reported. Its action has been shown in all (neurons, glia, retinal pigment epithelium, and endothelial) retinal cells. Patients affected by the Flammer Syndrome (FS) (secondary to Endothelin (ET)-related endothelial dysfunction) are exposed to ischemic accidents in the microcirculation, notably the retina and optic nerve.
Case Presentation: A 54 years old female patient with a diagnosis of venous occlusion OR since three weeks presented on March 3, 2019. A severe Flammer phenotype and underlying non arteritic ischemic optic neuropathy; retinal and choroidal drop-out were obviated. Investigation and follow-up were performed for 36 months with Retinal Multimodal Imaging (Visual field, SD-OCT, OCT- Angiography, Indo Cyanin Green Cine-Video Angiography). Recombinant human EPO (rhEPO)(EPREX®)(2000 units, 0.05 cc) off-label intravitreal injection was performed twice at one month interval. Visual acuity rapidly improved from 20/200 to 20/63 with disparition of the initial altitudinal scotoma after the first rhEPO injection, to 20/40 after the second injection, and gradually up to 20/32, by month 5 to month 36. Secondary cystoid macular edema developed ten days after the first injection, that was not treated via anti-VEGF therapy, and resolved after the second rhEPO injection. PR1 layer integrity, as well as protective macular gliosis were fully restored. Some level of ischemia persisted in the deep capillary plexus and at the optic disc.
Conclusion: Patients with FS are submitted to chronic ischemia and paroxystic ischemia/reperfusion injury that drive survival physiological adaptations via the hypoxic-preconditioning mimicking effect of endogenous EPO, that becomes overwhelmed in case of acute hypoxic stress threshold above resilience limits. Intra vitreal exogenous rhEPO injection restores retinal hypoxic-preconditioning adaptation capacity, provided it is timely administrated. Intra vitreal rhEPO might be beneficial in other retinal diseases of ischemic and inflammatory nature.
Key words : Erythropoietin, retinal vein occlusion, anterior ischemic optic neuropathy, Flammer syndrome, Primary Vascular Dysfunction, anti-VEGF therapy, Endothelin, microcirculation, off-label therapy.
Introduction
Retinal Venous Occlusion (RVO) treatment still carries insufficiencies and contradictions (1) due to the incomplete deciphering of the pathophysiology and of its complex multifactorial nature, with overlooking of factors other than VEGF up-regulation, notably the roles of retinal venous tone and Endothelin-1 (ET) (2-5), and of endothelial caspase-9 activation (6). Flammer Syndrome (FS)( (Primary Vascular Dysfunction) is related to a non atherosclerotic ET-related endothelial dysfunction in a context of frequent hypotension and increased oxidative stress (OS), that alienates organs perfusion, with notably changeable functional altered regulation of blood flow (7-9), but the pathophysiology remains uncompletely elucidated (8). FS is more frequent in females, and does not seem to be expressed among outdoors workers, implying an influence of sex hormons and light (7)(9). ET is the most potent pro-proliferative, pro-fibrotic, pro-oxidative and pro-inflammatory vasoconstrictor, currently considered involved in many diseases other than cardio-vascular ones, and is notably an inducer of neuronal apoptosis (10). It is produced by endothelial (EC), smooth vascular muscles (SVMC) and kidney medullar cells, and binds the surface Receptors ET-A on SVMC and ET-B on EC, in an autocrine and paracrine fashion. Schematically, binding on SVMC Receptors (i.e. through local diffusion in fenestrated capillaries or dysfunctioning EC) and on EC ones (i.e. by circulating ET) induce respectively arterial and venous vasoconstriction, and vasodilation, the latter via Nitrite oxide (NO) synthesis. ET production is stimulated notably by Angiotensin 2, insulin, cortisol, hypoxia, and antagonized by endothelial gaseous NO, itself induced by flow shear stress. Schematically but not exclusively, vascular tone is maintained by a complex regulation of ET-NO balance (8) (10-11). Both decrease of NO and increase of ET production are both a cause and consequence of inflammation, OS and endothelial dysfunction, that accordingly favour vasoconstriction; in addition ET competes for L-arginine substrate with NO synthase, thereby reducing NO bioavailability, a mechanism obviated notably in carotid plaques and amaurosis fugax (reviewed in 11).
Severe FS phenotypes are rare. Within the eye, circulating ET reaches retinal VSMC in case of Blood-Retinal-Barrier (BRB) rupture and diffuses freely via the fenestrated choroidal circulation, notably around the optic nerve (ON) head behind the lamina cribrosa, and may induce all pathologies related to acute ocular blood flow decrease (2-3)(5)(7-9). We previously reported two severe cases with rapid onset of monocular cecity and low vision, of respectively RVO in altitude and non arteritic ischemic optic neuropathy (NAION) (Boscher et al, Société Francaise d'Ophtalmologie and Retina Society, 2015 annual meetings).
Exogenous Recombinant human EPO (rhEPO) has been shown effective in humans for spinal cord injury (12), neurodegenerative and chronic kidney diseases (CKD) (reviewed in 13). Endogenous EPO is released physiologically in the circulation by the kidney and liver; it may be secreted in addition by all cells in response to hypoxic stress, and it is the prevailing pathway induced via genes up-regulation by the transcription factor Hypoxia Inducible Factor 1 alpha, among angiogenesis (VEGF pathway), vasomotor regulation (inducible NO synthase), antioxidation, and energy metabolism (14). EPO Receptor signaling induces cell proliferation, survival and differentiation (reviewed in 13), and targets multiple non hematopoietic pathways as well as the long-known effect on erythropoiesis (reviewed in 15). Of particular interest here, are its synergistic anti-inflammatory, neural antiapoptotic (16) pro-survival and pro-regenerative (17) actions upon hypoxic injury, that were long-suggested to be also indirect, via blockade of ET release by astrocytes, and assimilated to ET-A blockers action (18). Quite interestingly, endogenous EPO’s pleiotropic effects were long-summarized (back to 2002), as “mimicking hypoxic-preconditioning” by Dawson (19), a concept applied to the retina (20). EPO Receptors are present in all retinal cells and their rescue activation targets all retinal cells, i.e. retinal EC, neurons (photoreceptors (PR), ganglion (RGG) and bipolar cells), retinal pigment epithelium (RPE) osmotic function through restoration of the BRB, and glial cells (reviewed in 21), and the optic nerve (reviewed in 22). RhEPO has been tested experimentally in animal models of glaucoma, retinal ischemia-reperfusion (I/R) and light phototoxicity, via multiple routes (systemic, subconjunctival, retrobulbar and intravitreal injection (IVI) (reviewed in 23), and used successfully via IVI in human pilot studies, notably first in diabetic macular edema (24) (reviewed in 25 and 26). It failed to improve neuroprotection in association to corticosteroids in optic neuritis, likely for bias reasons (reviewed in 22). Of specific relation to the current case, it has been reported in NAION (27) (reviewed in 28) and traumatic ON injury (29 Rashad), and in one case of acute severe central RVO (CRVO) (Luscan and Roche, Société Francaise d’Ophtalmologie 2017 annual meeting). In addition EPO RPE gene therapy was recently suggested to prevent retinal degeneration induced by OS in a rodent model of dry Age Macular Degeneration (AMD) (30).
Case Report Presentation
This 54 years female patient was first visited on March 2019 4th, seeking for second opinion for ongoing vision deterioration OR on a daily basis, since around 3 weeks. Sub-central RVO (CRVO) OR had been diagnosed on February 27th; available SD-OCT macular volume was increased with epiretinal marked hyperreflectivity, one available Fluorescein angiography picture showed a non-filled superior CRVO, and a vast central ischemia involving the macular and paraoptic territories. Of note there was ON edema with a para-papillary hemorrage nasal to the disc on the available colour fundus picture.
At presentation on March 4, Best Corrected Visual Acuity (BCVA) was reduced at 20/100 OR (20/25 OS). The patient described periods of acutely excruciating retro-orbital pain in the OR. Intraocular pressure was normal, at 12 OR and 18 OS (pachymetry was at 490 microns in both eyes). The dilated fundus examination was similar to the previous color picture and did not disclose peripheral hemorrages recalling extended peripheral retinal ischemia. Humphrey Visual Field disclosed an altitudinal inferior scotoma and a peripheral inferior scotoma OR and was in the normal range OS, i.e. did not recall normal tension glaucoma OS . There were no papillary drusen on the autofluorescence picture, ON volume was increased (11.77 mm3 OR versus 5.75 OS) on SD-OCT (Heidelberg Engineering®) OR, Retinal Nerve Fiber (RNFL) and RGC layers thicknesses were normal Marked epimacular hypereflectivity OR with foveolar depression inversion, moderately increased total volume and central foveolar thickness (CFT) (428 microns versus 328 OS), and a whitish aspect of the supero-temporal internal retinal layers recalling ischemic edema, were present . EDI CFT was incresead at 315 microns (versus 273 microns OS), with focal pachyvessels on the video mapping . OCT-Angiography disclosed focal perfusion defects in both the retinal and chorio-capillaris circulations , and central alterations of the PR1 layer on en-face OCT
Altogether the clinical picture evoked a NAION with venous sub-occlusion, recalling Fraenkel’s et al early hypothesis of an ET interstitial diffusion-related venous vasoconstriction behind the lamina cribrosa (2), as much as a rupture of the BRB was present in the optic nerve area (hemorrage along the optic disc). Choroidal vascular drop-out was suggested by the severity and rapidity of the VF impairment (31). The extremely rapid development of a significant “epiretinal membrane”, that we interpreted as a reactive - and protective, in absence of cystoid macular edema (CME) - ET 2-induced astrocytic proliferation (reviewed in 32), was as an additional sign of severe ischemia.
The mention of the retro-orbital pain evoking a “ciliary angor”, the absence of any inflammatory syndrome and of the usual metabolic syndrome in the emergency blood test, oriented the etiology towards a FS. And indeed anamnesis collected many features of the FS, i.e. hypotension (“non dipper” profile with one symptomatic nocturnal episode of hypotension on the MAPA), migrains, hypersensitivity to cold, stress, noise, smells, and medicines, history of a spontaneously resolutive hydrops six months earlier, and of paroxystic episods of vertigo (which had driven a prior negative brain RMI investigation for Multiple Sclerosis, a frequent record among FS patients (33) and of paroxystic visual field alterations (7)(9), that were actually recorded several times along the follow-up.
The diagnosis of FS was eventually confirmed in the Ophthalmology Department in Basel University on April 10th, with elevated retinal venous pressure (20 to 25mmHg versus 10-15 OS) (4)(7)(9), reduced perfusion in the central retinal artery and veins on ocular Doppler (respectively 8.3 cm/second OR velocity versus 14.1 mmHg OS, and 3.1/second OR versus 5.9 cm OS), and impaired vasodilation upon flicker light-dependant shear stress on the Dynamic Vessel Analyser testing (7-9). In addition atherosclerotic plaques were absent on carotid Doppler.
On March 4th, the patient was at length informed about the FS, a possible off label rhEPO IVI, and a related written informed consent on the ratio risk-benefits was delivered.
By March 7th, she returned on an emergency basis because of vision worsening OR. VA was unchanged, intraocular pressure was at 13, but Visual Field showed a worsening of the central and inferior scotomas with a decreased foveolar threshold, from 33 to 29 decibels. SD-OCT showed a 10% increase in the CFT volume.
On the very same day, an off label rhEPO IVI OR (EPREX® 2000 units, 0,05 cc in a pre-filled syringe) was performed in the operating theater, i.e. the dose reported by Modarres et al (27), and twenty times inferior to the usual weekly intravenous dose for treatment of chronic anemia secondary to CKD. Intra venous acetazolamide (500 milligrams) was performed prior to the injection, to prevent any increase in intra-ocular pressure. The patient was discharged with a prescription of chlorydrate betaxolol (Betoptic® 0.5 %) two drops a day, and high dose daily magnesium supplementation (600 mgr).
Incidentally the patient developed bradycardia the day after, after altogether instillation of 4 drops of betaxolol only, that was replaced by acetazolamide drops, i.e. a typical hypersensitivity reaction to medications in the FS (7)(9).
Subjective vision improvement was recorded as early as D1 after injection. By March 18 th, eleven days post rhEPO IVI, BCVA was improved at 20/63, the altitudinal scotoma had resolved (Fig. 5), Posterior Vitreous Detachment had developed with a disturbing marked Weiss ring, optic disc swelling had decreased; vasculogenesis within the retinal plexi and some regression of PR1 alterations were visible on OCT-en face. Indeed by 11 days post EPO significant functional, neuronal and vascular rescue were observed, while the natural evolution had been seriously vision threatening.
However cystoid ME (CME) had developed . Indo Cyanin Green-Cine Video Angiography (ICG-CVA) OR, performed on March 23, i.e. 16 days after the rhEPO IVI, showed a persistent drop in ocular perfusion: ciliary and central retinal artery perfusion timings were dramatically delayed at respectively 21 and 25 seconds, central retinal vein perfusion initiated by 35 seconds, was pulsatile, and completed by 50 seconds only (video 3). Choroidal pachyveins matching the ones on SD-OCT video mapping were present in the temporal superior and inferior fields, and crossed the macula; capillary exclusion territories were present in the macula and around the optic disc.
By April 1, 23 days after the rhEPO injection, VA was unchanged, but CME and perfusion voids in the superficial deep capillary plexi and choriocapillaris were worsened, and optic disc swelling had recurred back to baseline, in a context of repeated episodes of systemic hypotension; and actually Nifepidin-Ratiopharm® oral drops (34), that had been delivered via a Temporary Use Authorization from the central Pharmacology Department in Assistance Publique Hopitaux de Paris, had had to be stopped because of hypersensitivity.
A second off label rhEPO IVI was performed in the same conditions on April 3, i.e. approximately one month after the first one.
Evolution was favourable as early as the day after EPO injection 2: VA was improved at 20/40, CME was reduced, and perfusion improved in the superficial retinal plexus as well as in the choriocapillaris. By week 4 after EPO injection 2, CME was much decreased, i.e. without anti VEGF injection. On august 19th, by week 18 after EPO 2, perfusion on ICG-CVA was greatly improved , with ciliary timing at 18 seconds, central retinal artery at 20 seconds and venous return from 23 to 36 seconds, still pulsatile. Capillary exclusion territories were visible in the macula and temporal to the macula after the capillary flood time that went on by 20.5 until 22.5 seconds (video 4); they were no longer persistent at intermediate and late timings.
Last complete follow-up was recorded on January 7, 2021, at 22 months from EPO injection 2. BCVA was at 20/40, ON volume had dropped at 7.46 mm3, a sequaelar superior deficit was present in the RNFL with some corresponding residual defects on the inferior para central Visual Field , CFT was at 384 mm3 with an epimacular hyperreflectivity without ME, EDI CFT was dropped at 230 microns. Perfusion on ICG-CVA was not normalized, but even more improved, with ciliary timing at 15 seconds, central retinal artery at 16 seconds and venous return from 22 to 31 seconds, still pulsatile , indicating that VP was still above IOP. OCT-A showed persisting perfusion voids, especially at the optic disc and within the deep retinal capillary plexus. The latter were present at some degree in the OS as well . Choriocapillaris and PR1 layer were dramatically improved.
Last recorded BCVA was at 20/32 by February 14, 2022, at 34 months from EPO 2. SD-OCT showed stable gliosis hypertrophy and mild alterations of the external layers .
Discussion
What was striking in the initial clinical phenotype of CRVO was the contrast between the moderate venous dilation, and the intensity of ischemia, that were illustrating the pioneer hypothesis of Professor Flammer‘s team regarding the pivotal role of ET in VO (2), recently confirmed (3)(35), i.e. the local venous constriction backwards the lamina cribrosa, induced by diffusion of ET-1 within the vascular interstitium, in reaction to hypoxia. NAION was actually the primary and prevailing alteration, and ocular hypoperfusion was confirmed via ICG-CVA, as well as by the ocular Doppler performed in Basel. ICG-CVA confirmed the choroidal drop-out suggested by the severity of the VF impairment (31) and by OCT-A in the choriocapillaris. Venous pressure measurement, which instrumentation is now available (8), should become part of routine eye examination in case of RVO, as it is key to guide cases analysis and personalized therapeutical options.
Indeed, the endogenous EPO pathway is the dominant one activated by hypoxia and is synergetic with the VEGF pathway, and coherently it is expressed along to VEGF in the vitreous in human RVO (36). Diseases develop when the individual limiting stress threshold for efficient adaptative reactive capacity gets overwhelmed. In this case by Week 3 after symtoms onset, neuronal and vascular resilience mechanisms were no longer operative, but the BRB, compromised at the ON, was still maintained in the retina.
As mentioned in the introduction, the scientific rationale for the use of EPO was well demonstrated by that time, as well as the capacities of exogenous EPO to mimic endogenous EPO vasculogenesis, neurogenesis and synaptogenesis, restoration of the balance between ET-1 and NO. Improvement of chorioretinal blood flow was actually illustrated by the evolution of the choriocapillaris perfusion on repeated OCT-A and ICG-CVA. The anti-apoptotic effect of EPO (16) seems as much appropriate in case of RVO as the caspase-9 activation is possibly another overlooked co-factor (6).
All the conditions for translation into off label clinical use were present: severe vision loss with daily worsening and unlikely spontaneous favourable evolution, absence of toxicity in the human pilot studies, of contradictory comorbidities and co-medications, and of context of intraocular neovascularization that might be exacerbated by EPO (37).
Why didn’t we treat the onset of CME by March 18th, i.e. eleven days after EPO IVI 1, by anti-VEGF therapy, the “standard-of-care” in CME for RVO ?
In addition to the context of functional, neuronal and vascular improvements obviated by rhEPO IVI by that timing in the present case, actually anti VEGF therapy does not address the underlying causative pathology. Coherently, anti-VEGF IVI : 1) may not be efficient in improving vision in RVO, despite its efficiency in resolving/improving CME (usually requiring repeated injections), as shown in the Retain study (56% of eyes with resolved ME continued to loose vision)(quoted in (1) 2) eventually may be followed by serum ET-1 levels increase and VA reduction (in 25% of cases in a series of twenty eyes with BRVO) (38) and by increased areas of non perfusion in OCT-A (39). Rather did we perform a second hrEPO IVI, and actually we consider open the question whether the perfusion improvement, that was progressive, might have been accelerated/improved via repeated rhEPO IVI, on a three to four weeks basis.
The development of CME itself, involving a breakdown of the BRB, i.e. of part of the complex retinal armentorium resilience to hypoxia, was somewhat paradoxical in the context of improvement after the first EPO injection, as EPO restores the BRB (24), and as much as it was suggested that EPO inhibits glial osmotic swelling, one cause of ME, via VEGF induction (40). Possible explanations were: 1) the vascular hyperpermeability induced by the up-regulation of VEGF gene expression via EPO (41) 2) the ongoing causative disease, of chronic nature, that was obviated by the ICG-CVA and the Basel investigation, responsible for overwhelming the gliosis-dependant capacity of resilience to hypoxia 3) a combination of both. I/R seemed excluded: EPO precisely mimics hypoxic reconditioning as shown in over ten years publications, including in the retina (20), and as EPO therapy is part of the current strategy for stabilization of the endothelial glycocalix against I/R injury (42-43). An additional and not exclusive possible explanation was the potential antagonist action of EPO on GFAP astrocytes proliferation, as mentioned in the introduction (18), that might have counteracted the reactive protective hypertrophic gliosis, still fully operative prior to EPO injection, and that was eventually restored during the follow-up, where epiretinal hyperreflectivity without ME and ongoing chronic ischemia do coincide (Fig. 6 and video 6), as much as it is unlikely that EPO’s effect would exceed one month (cf infra). Inhibition of gliosis by EPO IVI might have been also part of the mechanism of rescue of RGG, compromised by gliosis in hypoxic conditions (44). Whatever the complex balance initially reached, then overwhelmed after EPO IVI 1, the challenge was rapidly overcome by the second EPO IVI without anti-VEGF injection, likely because the former was powerful enough to restore the threshold limit for resilience to hypoxia, that seemed no longer reached again during the relapse-free follow-up. Of note, this “epiretinal membrane “, which association to good vision is a proof of concept of its protective effect, must not be removed surgically, as it would suppress one of the mecanisms of resilience to hypoxia.
To our best knowledge, ICG-CVA was never reported in FS; it allows real time evaluation of the ocular perfusion and illustration of the universal rheological laws that control choroidal blood flow as well. Pachyveins recall a “reverse” veno-arteriolar reflex in the choroidal circulation, that is NO and autonomous nervous system-dependant, and that we suggested to be an adaptative choroidal microcirculation process to hypoxia (45). Their persistence during follow-up accounts for a persisting state of chronic ischemia.
The optimal timing for reperfusion via rhEPO in a non resolved issue:
in the case reported by Luscan and Roche, rhEPO IVI was performed on the very same day of disease onset, where it induced complete recovery from VA reduced at counting fingers at 1 meter, within 48 hours. This clinical human finding is on line with a recent rodent stroke study that established the timings for non lethal versus lethal ischemia of the neural and vascular lineages, and the optimized ones for beneficial reperfusion: the acute phase - from Day 1 where endothelial and neural cells are still preserved, to Day 7 where proliferation of pericytes and Progenitor Stem Cells are obtainable - and the chronic stage, up to Day 56, where vasculogenesis, neurogenesis and functional recovery are still possible, but with uncertain efficiency (46). In our particular case, PR rescue after rhEPO IVI 1 indicated that Week 3 was still timely. RhEPO IVI efficacy was shown to last between one (restoration of the BRB) and four weeks (antiapoptotic effect) in diabetic rats (24). The relapse after Week 3 post IVI 1 might indicate that it might be approximately the interval to be followed, should repeated injections be necessary.
The bilateral chronic perfusion defects on OCT-A at last follow-up indicate that both eyes remain in a condition of chronic ischemia and I/R, where endogenous EPO provides efficient ischemic pre-conditioning, but is potentially susceptible to be challenged during episodes of acute hypoxia that overwhelm the resilience threshold.
Conclusion
The present case advocates for individualized medicine with careful recording of the medical history, investigation of the systemic context, and exploiting of the available retinal multimodal imaging for accurate analytical interpretation of retinal diseases and their complex pathophysiology. The Flammer Syndrome is unfortunately overlooked in case of RVO; it should be suspected clinically in case of absence of the usual vascular and metabolic context, and in case of elevated RVP. RhEPO therapy is able to restore the beneficial endogenous EPO ischemic pre-conditioning in eyes submitted to challenging acute hypoxia episodes in addition to chronic ischemic stress, as in the Flammer Syndrome and fluctuating ocular blood flow, when it becomes compromised by the overwhelming of the hypoxic stress resilience threshold. The latter physiopathological explanation illuminates the cases of RVO where anti-VEGF therapy proved functionally inefficient, and/or worsened retinal ischemia. RhEPO therapy might be applied to other chronic ischemia and I/R conditions, as non neo-vascular Age Macular Degeneration (AMD), and actually EPO was listed in 2020 among the nineteen promising molecules in AMD in a pooling of four thousands (47).
#off-label therapy#JCRMHS#anti-VEGF therapy#Erythropoietin#Journal of Clinical Case Reports Medical Images and Health Sciences impact factor.#Primary Vascular Dysfunction
2 notes
·
View notes
Text
Love In A Time Of The Zombie Apocalypse by rizzlewrites (Español)
Love In A Time Of The Zombie Apocalypse by rizzlewrites (Español) https://ift.tt/U31P5d4 by blaisemalfoyy Después de Voldemort, estuvo esto. El reloj está sonando para crear una cura para el inimaginable terror que actualmente está en el mundo. Hermione se encuentra sin querer aliada con el hombre más odiado en toda Gran Bretaña Mágica. (Final alterno: 'La Vie En Rose', Audiobook en inglés por ETL.Echo.Audiobooks), Words: 4004, Chapters: 1/84, Language: Español Fandoms: Harry Potter - J. K. Rowling Rating: Explicit Warnings: Graphic Depictions Of Violence Categories: F/M Characters: Hermione Granger, Draco Malfoy, Harry Potter, Ginny Weasley, Neville Longbottom, Blaise Zabini, Lucius Malfoy, Narcissa Black Malfoy, Padma Patil, Original Characters, Rufus Scrimgeour Relationships: Hermione Granger/Draco Malfoy, Harry Potter/Ginny Weasley Additional Tags: Angst, scientist Draco, Post-Apocalypse, Children in Dangerous Situations, Draco is a BAMF, Horror, Original Character(s), Hermione is a BAMF, Harry is a BAMF, Guns, BAMFs galore, Gun Violence, Medical Procedures, Blood and Violence, Post-Traumatic Stress Disorder - PTSD, Explicit Sexual Content, no one is safe, Researcher Hermione, Post-Voldemort, non-consensual fruit molestation, Despots, Mental Health Issues, Zombies, Double-stranded RNA Activated Caspase Oligomerizer, misnomered sex dungeon, purebloods in therapy, Pregnancy, Attempted Sexual Assault, Bond villaining, Questionable Neuroscience, mortal combat, Slow Burn, audiofic, trauma-bonding, more like 3 fics in 1, HEA, Light Bondage, wizarding folk without their wands, hyper-competent MC's, Courtroom Drama, Exposition, Redeemed Draco, Deflowering, Emotional Sex, significant epilogue, rebuilding themes, Domestic Dramione, slutty cream puffs, Ensemble Cast, Draco speaking Russian, Werewolf, pet frogs, Beelzebub the Hellhound, Malfoy Manor, wizarding folk with guns, Hurt/Comfort, pesky garden gnome via AO3 works tagged 'Hermione Granger/Draco Malfoy' https://ift.tt/yhJQw0H February 05, 2024 at 08:40AM
3 notes
·
View notes
Text

sorry for the sadness, here's a lestat doodle redraw of Caspases about to kill his dad
3K notes
·
View notes
Text
My caspase MC would listen to Marina and the diamonds.
.... I made a playlist
0 notes
Text
https://github.com/anushka224473/TrendMosaic/blob/main/North America Caspase 9 Monoclonal Antibody Drivers And Trends.md
0 notes
Text
https://twikkers.nl/blogs/174365/Caspase-8-Market-Overview-Competitive-Analysis-and-Forecast-2031

Caspase 8 Market Overview, Competitive Analysis and Forecast 2031
0 notes
Text
Caspase-1/Interleukin-1 (an Eminent Inhibitor): Can be a Future Radioprotector?

Caspase-1/Interleukin-1 (an Eminent Inhibitor): Can be a Future Radioprotector? in Biomedical Journal of Scientific & Technical Research
In the advancement of science, the employment of contemporary radiation therapy (xRT); the most effective way to counter malignancy, in the realm of cancer treatment has been exploited in the last few decades extensively. Although, half of all cancer patients worldwide, treated by radiotherapy may be responsible for the consequential damage to healthy normal cells and acute injuries to tissues which remains an enormous challenge to the radiotherapist and oncologist [1]. On the other hand, tremendous research which involves; novel drug development and innovative strategies are in the phase of progress and is constantly evolving across the globe to help reduce radiation-induced multiple sideeffects. As massive doses of radiation are implemented as a part of radiotherapy to cease the progress of cancerous cells, but at the same time, it is harming enormously to the healthier normal cells. The risk of damaging normal cells can be accomplished by practicing an accurate and improved localization of radiation dose and with the aid of several radioprotectors [2]. The most frequently applied techniques in anticancer treatment include Ionizing radiation (IR), in particular X-rays and gamma-rays owing to their huge potential to penetrate tissues; subsequently rupture chemical bonds resulted in free electrons from atoms which ionized, ultimately destroy the tumor cells. The water molecules existent in the human organisms spontaneously (within a few milliseconds) break down into active oxygen by radiation; eventually, engender free radicals, Reactive Oxygen Species (ROS), and Reactive Nitrogen Species (RNS) [3], which subsequently impair cells and in extreme cases leads to death. The generated free radicals’ interplay with DNA, RNA, proteins and resulted in cell dysfunction and further fatality. Also, these active free radicals induce oxidative stress among healthy organisms in physiological and pathological processes, which is one of the causative factors for tumors, hence, therefore, further exploration and the investigation of a powerful free radical scavenger is urgently needed.
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01 Follow on Blogger : https://biomedres01.blogspot.com/ Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Medical Microbiology#Journals on Biomedical Intervention#Journals on Medical Drug and Therapeutics#Biomedical Journal Impact Factor#Journal of Biomedical Research and Review
0 notes