#but like 1 trans man scientist on that whole list.
Text
once again beefed by the utter lack of cool trans men literally anywhere. I found a list of notable trans ppl and it was only 16% trans men and most of them were from like 1900
#like sorry to be bitching but it is a thread ive noticed#i know some of it is that trans women have essier access to cool shit pre transition#stem game shops etc#and trans men dont get to pretransition bc of misogyny#but post transition so many of us seem to stay fucking lame#at best a cool artist#but like 1 trans man scientist on that whole list.#meanwhile trans chicks are responsible for all of computers basically#(shoots you with a beam)
0 notes
Text
TOP five people named magnus in the world
5. Magnus carlsen

magnis carlsen is the worlds most powerful chess player, having earned the rank of "grand master". this has made him an incredible figure in the chess world. however, recently his fame has been rocked by scandal. there are rumors that he cheated by using a vibrating buttplug to enhance his chess skills while playing the game. these shocking allegations call his grand master status into question. however, whether he used artifical "doping" to win his title or not, his extreme chess power earns him a spot on this list.
4. Magnus archives

Mangus archives, also known by the nickname "trans misogyny affected" by many of his fans, is one of the most popular podcasting stars in the world. although he retired from his podcasting career in 2021, his fans still think that he is one of the greatest podcasters who ever lived, along side the likes of joe rogan and el chapo. thanks to his incredible podcasting prowess, magnus archives earns a spot on this list.
3. Magnus herchfeld

Magnus hirschfeld was a german scientist who is largely credited with being the first man to discover how to have gay sex. while many other scientists had tried before, none could compete with doctor hirchfeld's revolutionary theories. he even started a school, called the institüte for sexualwitchencraft, for teaching his discoveries. however, his school was destroyed by adolf hitler when the nazis came to germany. for his revolutionary discovery of gay people everywhere, mangus hirschfeld earns a spot on my list.
2. Mangus Maximus

this guy was a roman emperor so powerful, he even got his face on a coin. he became the emporer of rome in 300 bc, and used his military skills to conquer wales. nobody has ever heard of this guys because he died thousands of years ago, but that doesn't change just how awesome of a magnus he was. so don't forget this old faithful! for that reason, he earns a spot on my list.
1. Magnus Von Grapple!!!!!!!!!!

that's right folks, the one youve all been waiting for. magnus von grapple is the most famous magnus of all time, because he's a giant and powerful robot. try to compete with THAT. ever since he made his appearance in "paper mario", his fans have been rooting for him above all else. there is a whole list of things which makes this magnus the best, but lets just say: if you disagree, he could smash you with his feet. the all time greatest magnus of all time, for that reason, he earns the number one spot on this list.
281 notes
·
View notes
Note
Do you mind if I ask your top 10 favorite characters (can be male or female) from all of the media that you loved (can be anime/manga, books, movies or tv series)? And why do you love them? Sorry if you've answered this question before.....Thanks....
I always like talking about characters, so no problem, ask away. This was a pretty tough question and I had to do a lot of soul searching for that. Turns out I don't actually have any major favourite characters for movies or TV shows. Like, I will have favourite characters in a show, but I'm not that wild about them that they could compare to others across mediums. I guess with the many movies and TV shows I like, I always tend to prioritize the plot more and the characters kind of seamlessly integrate into that. So the characters that did make the list are from animangas, video games, comic books and Warhammer. I can't really rank them from 1 to 10, I just ordered them by franchise/medium.
Lucifer/Louis Cypher (Shin Megami Tensei games)
This doesn't include the Lucifer from SMTIV, I prefer to forget that ever happened. As a quick summary, in SMT there's this big war going on between the forces of chaos and order. Gods and mythical beings of all kinds fall somewhere between the two sides. An Abrahamic god, angels and forces of light usually belong to order (who exactly can change based on the game) and Lucifer is the leader of the forces of chaos. Contrary to Order, he tends to get personally involved with the player and tries to lead them subtly towards chaos, but somehow still manages to come off as very sympathetic. That's what I like about him and find so fascinating. He's a big fighter for free will and will never openly judge you for the choices you make, unlike the order-aligned characters, who fly into a rage. He will fight you to ensure chaos wins, but it's never really seen as you doing some personal failing. Especially in SMT II he is essentially an ally and even if you defeat him, he will offer to help you slay YHVH as long as you don't join order. I'm currently playing SMT Nocturne again and am trying to go for the True Demon Ending (leading Lucifers army towards heaven) and I have to say especially in his old man form it's always nice to see him stop by to check up on me. The little kid form is much nastier, but whenever I'm running through the apocalyptic landscape or crawling through some dungeon and he shows up in his wheelchair it makes me feel supported. Like "aw, grandpa is watching me, I have to do my best". Anyway, I think the place he has in the games is very interesting. He's also the reason why many people say the games are leading you to side more with chaos over order, even though it's always made clear that you will be working towards a world of eternal war. Lucifer is just very charming, as you would expect, and seems even more so when you compare him with the prospect of losing all autonomy.
Kenjaku (JJK)
I think this is pretty self-explanatory, since I won't shut up about them on this blog. They combine a lot of things I really like about fictional characters. They're a mad scientist, they are mainly driven by their own curiosity and therefore a chaotic force in the plot, they're trans, they are genre-savvy and then there is the whole business of being the main characters evil mother. Kenjaku is also another excuse to brush up my knowledge on Japanese history. What really hooked me in was the whole toxic family business and the time while they stayed with the Itadori family. For most of the story they're this big bad, who managed to destroy half of Japan in 2 weeks, but then we find out about that and it all seems so low key and relatively normal, that it makes them even more fascinating. They're the main villain, but they're also very chill for most of the story and don't immediately send off alarm bells in the average person's head unlike Sukuna for example. That's what allowed them to stay undercover for so long (that and Tengen). I don't think I've come across another character before who hits so many of my fave character boxes.
Phosphophylite (Houseki no Kuni)
Pretty new addition to my list, but their character development across the series really hit me like a train. It's honestly so perfect, it's hard to summarize why I love it so much. In the beginning of the story they are relatively innocent, weak, but also with some clear character flaws. As they gain strength these flaws only become even more pronounced and extreme as they go through trauma after trauma. Every step of the story serves to chip away at Phos both physically and mentally until there's only splinter left of them. The story is almost over and while Phos has undoubtedly changed, they have also held onto their most intrinsic characteristic and you could say that what really made them who they are has only become more clear now. They have idealistic goals and only end up hurting the people they want to protect with every step they take towards them, until they're completely alone at the end. They are driven completely insane by their actions and the suffering others put them through until they snap completely and destroy everything. That destruction was a much needed restart however, as much as it hurt to lose so many people. There's so much I could talk about with them, I just think they are such a fascinating character and definitely one of my favourite mcs ever.
Johan Liebert (Monster)
It's been a while since I read/watched Monster, but every time I look in the direction of the series, it makes me insane all over again. Johan is probably the only anime villain I find actually scary. It's the mystery around his character, he's very unpredictable and just like the characters you start to see him everywhere in every little hint you are given. The finale in Ruhenheim was so stressful to watch and Johan didn't even do anything for most of it, it was all just vague glimpses and build up tension. Every time we do see him on screen we know something bad will happen and even if he's interacting with someone friendly you are just waiting for that other person to suffer for being in his presence for too long. I could watch episode 49 again and again because things go downhill so fast and you know from the beginning that Johan interacting with children is bad. I'm getting war flashbacks any time I hear Noto Mamiko talk in another anime. Immediate red flag. Do not trust. Same goes for hearing the phrase 昔々ある所に. As if there wasn't enough reason to be vary of German and Eastern European fairy tales. All that doesn't even touch on his relationship with Nina. They are so destructive, but still love each other. The whole reveal surrounding the rose mansion was so good and gave them a whole new depth. That's another thing that I love, Nina shows that while what Johan went through is tragic and horrible, there was nothing forcing him to become the serial killer he is now, which I think is a very important part of his character.
Satan/Ryo Asuka (Devilman franchise)
Satan is the whole reason I love Devilman so much, they're the center piece of the series, the series and its sequels only exist because God wants to punish Satan for being gay and an environmentalist, but unfortunately that often gets overlooked in the broader anime community. They think it's all just about Devilman/Akira killing people and the world dying and sideline the suffering twink who started it all. Even in the worst parts of the franchise (Devilman Lady), Satan and his bond with Akira can save the story from being complete shit. On the surface it's pretty basic, but Satan's wish to save the planet and demons by wiping out humanity and thereby destroying what he wanted to protect gets me every time. He ends up falling in love with a human, wants to save him from the war he's about to unleash by giving him special powers and eventually ends up fighting and killing him because of that. God swoops in and puts the timeline on loop to torture Satan. Satan tries to escape, but thereby only ends up killing the one he loves over and over again. Wonderfully tragic and I like how the story ends up siding with Satan. It would be better for humans to die, but seeing loved ones die still hurts. Basically, I'm not immune to suffering gays who want to fight God.
Thief King Bakura (Yu-Gi-Oh!)
Best character in the series, never did anything wrong and should've won or at least got to kill Atem and/or Atem's father. He only got used his whole life and I hate how dirty the anime and especially the eng dub did him. They really tried to say that melting the entire population of a village in gold was fully justified because they were thieves and Bakura has no right to complain because "he uses violence too (against the pharaoh...)". Ugh, it always makes me so mad just to think about it. Thankfully, the manga handled it better, even if they didn't quite stick the landing. I just love his whole story. Little boy goes up against the Pharaoh and his entire court, protected by the spirits of his home and even almost manages to take revenge, when he goes just a little too far and in his desperation gets involved with dark powers that are out to use him. I especially like that the manifestation of his ka, Diabound, is a holy spirit in the manga, showing that his initial goal was actually justified and the ruling class, who pass their time by torturing people for fun, are wrong. If only Zorc hadn't shown up... He gave us Yami Bakura though, so I'm not too mad. Yami Bakura instantly became my fave for liking ttrpgs over the Duel Monster card game and he stuck to that throughout his plan. No children's card games if he has a say in it. It's also hilarious that the others kill and torture each other with card games, but he just takes a knife and does it the old-fashioned way. Why gamble over cards, when you can simply stab the people and then take their belongings?
Lucifer Morningstar (Lucifer comics by Mike Carey)
My time again to tell everyone to read the Lucifer comics because even if you don't like comics, they are just insanely good. If you like The Sandman (TV series or comics), then definitely give them a go. There's technically also a TV series based on them, but aside from some names it has nothing in common with the source material. Don't know why they bothered getting the rights. It's basically a long discussion about free will and what it really means to be free. The ending really devastated me when I first read it, but I really like it and it makes the most sense. I had to think about Lucifer and how he's written a lot recently because of the Gojo vs Sukuna fight. In my opinion, Lucifer is the best overpowered mc I've seen so far. He has at his best the power to create whole multiverses, but the author uses his character traits to make sure he still struggles and faces challenges. It also helps that Lucifer is not a good fighter. The other fallen angels carried him hard in the war against heaven. If he doesn't have the option to oneshot his enemy, he will get beaten up badly. But more importantly, Lucifer has one goal in life and that is to be free and to escape his father's all-seeing, all-knowing eye and predestination itself. That is of course pretty difficult, not even creating his own multiverse helps because God/The Presence foresaw that too. At it's core the story is about escaping a controlling parent. This is made even more difficult by Lucifer's lack of empathy and resulting difficulties in cooperating with other people. There are very few people he cares about and even the ones he does he ends up pushing away because he can't understand their needs and always thinks about himself first. Quite often he doesn't even notice that he angered someone until it blows up in his face. Usually, he just assumes that everyone hates him anyway (it's often true), but with the few who do like him, he often ends up distancing himself from them because his plans are more important to him than them and they obviously don't always have much understanding for that. Basically, he's a selfish dick and I love that about him. I can emphasize with his struggles and philosophy, but how he goes about it is sometimes so maddening and that's what makes me invested. He also always gets retribution when he makes mistakes or treats other gods dismissively. He can literally move mountains, but because of his own limitations, he is often very vulnerable and arguably a bigger hurdle to overcome than his father. Because of his rather cold if snarky nature, it's also always nice when he does show a slither of care towards someone else.
Xaiozanus Exasas (Imperator: Wrath of the Omnissiah by Gav Thorpe)
The last three on this list are all Warhammer 40k characters, mostly taken from the novels like Exasas here. Full name and title is: Magos Dominus Militaris Xaiozanus Skitara Xilliarkis Exasas. So you know they are important. Aside from how giddy it makes me that there's a mc in a (Warhammer) novel that uses neopronouns, Exasas is also just so cute and lovable that it's impossible I think not to like ver. Ve is a magos of the Adeptus Mechanicus, meaning a cyborg employed to oversee all machine and tactical decisions in an Imperator Titan (basically a Gundam but the size of a city). Ve looks like a mechanical centipede with humanoid upper body and three oculars for eyes. Besides the threat of infiltration, a big part of the book is Exasas learning to get out of vis head so to say, let go of pure logic and make impulsive decisions. Exasas loves to predict battle outcomes and basically anything that is happening around ver, ve can spend hours brooding over hypothetical problems ve made up for verself. A considerable part of vis part of the plot is Exasas sitting in a corner and crunching numbers to distract verself from the people around ver bullying ver. Unfortunately, that also leads to ver overlooking a crew member that switched sides, which is what eventually forces ver to engage more with the real world and when ve can't find any logic in the actions of this person to disregard logic and consider improbabilities and make actions based on vis gut (I'm pretty sure Exasas doesn't have a gut anymore tho). Exasas isn't very relatable or anything, I have to admit that I skimmed some of vis repetitive combat predictions, but this very different way of thinking is what makes it so fascinating. It's not that uncommon for techpriests, but we rarely see it depicted like this. Exasas creates entire separate personalities in vis head to have discussions with or to administer special problems to while ve thinks about something else. There's also a Fighter Ego, which is less logically based because it needs to make quick decisions and eventually helps Exasas somewhat with vis struggle for action in other scenarios. Exasas body is technically made for combat as well, but ve verself isn't a very confrontational person, so ve split off all functions related to that into a separate part of verself that is only sometimes allowed to take over. In other words, there's a lot going on in that metal head and it's super interesting to read about.
Trazyn the Infinite
Trazyn shows up all over wh40k, but I mainly know him from the books The Infinite and The Divine and War in the Museum (yes this is a play on Night at the Museum), both written by Robert Rath. Trazyn is a Necron, which are basically robot ancient egyptians. They used to be the Necrontyr, but their souls/consciousness were then poured into skeletal robot bodies. Many didn't survive that and are no more than drones without will, others fell asleep and never woke up, but some like Trazyn kept their personality and most of their memories. Necrons are very hard to kill and can be reassambled to work again (although the consciousness might be gone if it was there before). Trazyn also has the ability to jump between egoless Necrons and turn them into his own body, which makes him especially hard to kill. He's a collector of artifacts, people, memories and whatever else picks his fancy. He collects them all in a giant museum for when the Necron of the empire he belongs to wake up and can see what happened while they're awake. It's mostly for himself though. He's like a magpie with the British Museum in the size of a planet to his disposal. With a stasis beam he can even keep living beings in his museum. Contrary to other Necrons he's more of a chaotic neutral party in the galaxy. He looks down on the Imperium (love that about him, he tends to drag them to filth), but he might ally with some soldiers or a squad he comes across if it means he gets some artefact he might've been after. He's aeons old, but like an old man and a child in one. He has seen so much and accumulated so much knowledge, but he still gets incredibly excited when he finds something new and even something as "simple" as coffee or music can be fascinating to him. He's kinda like Kenjaku in that way, except he doesn't have some big goal, he just likes watching the universe and only interferes arbitrarily.
Tanau Aleya (Watchers of the Throne novel series)
She belongs to the Anathema Psykana, commonly known as the Sisters of Silence. Her order is made up of women, who don't have souls. They are just void. This absence can make people around them physically ill, make them faint or give them other discomfort. It is also incredibly effective against the forces of chaos, so the Sisters of Silence fight to push back against the Chaos Gods. Thing is, because of their nature they have been neglected a lot and haven't received much attention or support from the Imperium at all. Aleya is especially aware of this and this is part of why she is such a ball of rage. The other reason is that her conclave, all the sisters she knew and grew up with, was destroyed by chaos cultists. She ends up fighting with Imperial armies to avenge her sisters, but she always makes sure to let them know that she does not like them and hasn't forgiven them for not giving a shit about her or her order for the last millennia or so. While the Sister of Silence have sworn to not talk, they do use sign language to communicate. Many people outside the order don't know this sign language though. Aleya personally also has no problem with talking if she needs to, she sometimes does it with her sisters, but usually she just doesn't want to. When the other doesn't know sign language, she often doesn't communicate at all unless it's urgent. Similarly, if someone pisses her off, she decides to just stand next to them unmoving, watch them squirm because of her repulsive aura. It is so rare to read about the Sisters of Silence, much less have them as a protagonist, and Aleya is all I was looking for from them. She hates the Imperium, she hates their cult of worship, she makes sure that she has very high priorities when it comes to who she cares about, she makes a sport out of unsettling politicians and she can crush a skull with her bare hands. What's not to love?
#asks#hope I could somewhat communicate what I like about them and wasn't too rambly...#not that analytical but it's hard to do that with so many different characters#long post
8 notes
·
View notes
Text
im definitely not ripping off my friend by making a list of au ideas i have no siree //gonna slap this under a readmore cause i. well i say a lot. all of the time. i tried so hard to format this Good but tumblr fucked me up i am so sorry
so first-off i know i already have one WIP AU (Auckland) on ao3 so i wont talk about That one cause like. spoilers. i actualyl have it like 80% created so its likely gonna truly get finished for once and i dont wanna ruin shit
the other one ive posted about is something me and ben (catgirlrepublic) have worked on together its not at all close to done or anything but it's. a fun little crossover. Between jdate and my fuckinuhm. Original characters story “Untitled Villains Project”. the sketches of the comic version ive started is actually my pinned post 👉👈 its like the first chunk of the story, i think half of part 1? yea.
Tldr john fucking Somehow is able t oget into contact with a certain curious scientist from another reality who’d just love to study the Soy Sauce, most certainly not for her own nefarious purposes
John and Dave meet up with the scientist, her name is Boss, and her lab assistant, Toxic, and after a bit of a preliminary Vibe Check where john determines her trustworthy (which Dave doesnt agree with,) the two agree to be taken to the world UVP is set in. from there they stay in Boss’s lab (big old fucking abandoned military lab). John and Toxic are fast friends due to mutual love-of-chaos. John n Dave get to fuckin, camp out on an air mattress.
The day after they arrive, the two get split up, not exactly intentionally; big plot points of UVP are liek. Fueled by Boss sending Toxic to go fetch her “research materials,” which are usually important artifacts
Fuckin side note i guess i have to explain my dumb bullshit: Boss’s, uh, field of expertise so to speak is actually fckin, basically the scientific study of magic and superpowers n shit like that. This shit’s all real in that world. Toxic’s got fuckin superpowers, so do 4 other main characters, whatever. It’s got a bit to do with spirituality, iss Boss’s hypothesis. So she has Toxic fetch important artifacts that might have “energies” to them. The thing is actually way more fuckin complictated than that, this is just Boss’s initial hypothesis.
Motherfucking anyways. So Boss gives Toxic a job to do, and John get excited about how Cool that sounds, and ends up going with Toxic, leaving Boss and Dave alone. Neither is thrilled about this. But Dave and Boss get to have a bit of conversation (while Toxic and John are off bonding and having a good time) and come to a… mutual grudging understanding of some kind. They still dont like each other though lmao
Theres gonna be deeper shit going on but we havent sorted it out yet/tbh havent like Written For It in a while but i still like thinking about it a lot lol
Also pretty sure our endgame is john and dave steal toxic and bring them back with em lmao boss is kind of not nice and toxic would most certainly be better off in Undisclosed. Actually theyd fucking love it. Theyd become a local cryptid im sure. Undisclosed’s mothman is a teleporting spike baby.
I have. Another crossover AU that i might. Post something about for halloween? Maybe? If i have it finished?
Crosses over into, you guessed it, another one of my original-character projects. God, am i vain or something?
I promise this is just because i think blue and dave should get to team up to beat up some monsters
Quick briefing on my fuckinuh. Original character story, this one doesnt have a name (yet? Idk lol my work never actually goes anywhere sso who gives a shit). It centers around two grim reapers, Red (26, bi woman) and Blue (22, aroace agender asshole). In this reality or whatever, grim reapers function kind of like low-level office workers. They get told who’s going to die + when by some middle-management types, and upper management only involve themselves when punishment needs to be doled out. These Higher-Ups can be seen as analogous to Korrok; they’re decidedly not human, never were, and fucking terrifyingly powerful. Additionally, grim reapers are sort of .. designed to be “background noise” people. In reality theyre supernatural beings and, uh, look Real Fuckin Weird (the whole deal has a neon aesthetic im terrible at drawing uwu) but most humans just perceive them like extras in a movie. A body’s there but the camera’s not focused on it.
To the narrative: the shit starts when Red n Blue get relocated to Undisclosed. Relocation is something that just happens every now and then to reapers; they usually work in teams, but they get split up into different cities to avoid any strong bonds forming (a counter-union strategy from the Higher-Ups).
Red, Blue, John and Dave end up running into each other for the first time in a McDonalds where John n Dave are getting some 4am “hey, we just survived another horrific monster fight” celebration burgers. John and Dave are the only two people who can see how… strange Red and Blue are. Nobody else notices.
John unintentionally pisses Blue off, leading to Blue whacking him upside the head with a dildo bat. They all four get kicked out of McDonald’s. Dave and Red both are less than thrilled
Blue and John end up resolving their differences, somehow. Red and Dave briefly bond over their dumbass best friends being, well, dumbasses. They all part ways amicably.
somehow-or-other (idk yet) they end up running into each other a few more times, and eventually john invites them over to his place, and the four (plus Amy now!) get to know each other a little better
while there, Blue gets a text about some guy who's gonna die and John offers to drive them to where that's gonna go down. they take him up on the offer and get to have a bit of one-on-one conversation
after that ordeal though Blue has had Enough of people and bails, leaving John to head home alone
theres a sort of mirror-development going on with the five of em. Red, John, and Amy would all like everyone to get along, though theyre a bit tentative about it (John moreso than the other two, actually, jsut cause. well Red n Blue could still be Sauce Monsters). Dave and Blue on the other hand do Not like people enough for this shit, and Dave's not unconvinced theyre Sauce Monsters. he will not trust them until proven he should
the story's kinda nebulous but i got an idea for some Shit going down that involves both Sauce Monsters and also the Higher-Ups to have some fuckin absolute chaos go down.
Oops! All Trans
Everybody is transgender. Everyone
Ive actually workshopped this one both with ben (catgirlrepublic) and ghost (ghost-wannabe) lmao its a fun lil concept ive had from the get-go cause i mean. What’s an internet tran gonna do other than hit all their favourite media with the Everyone’s Trans beam
Dave transitioned post-high school and faked his death for it. People go missing in Undisclosed all the damned time, after all. He moved to the next city over, transitioned fully, then came back as a completely new man. Yes i know this doesnt exactly fit with the “everyone knows David from high school” thing alright, hush.
Anytime anyone brings up John’s old best friend (pre-transition Dave) John throws an entire fit like an overdramatic grieving widow. Full-on sobbing “why would you bring her up?! I miss her so much—” to the point that people just stop bringing up because Jesus Christ That Sure Is Uncomfortable KJHGFDS.
This is a scheme he and Dave came up with prior to Dave leaving, though Dave hadnt exactly anticipated John putting on this much of a performance about it— but it’s stopped Dave from ever having tto hear his deadname again, so hey.
Amy transitioned sometime in middle school/early high school. Her family was super supportive and loved her a ton and most people just know her as Amy. she was super shy her whole life really so. Yeah. people just dont think to bring it up lmao also i Feel Like big jim would absolutely wallop anyone who gave her trouble of any kind
John’s nonbinary (genderfluid specifically) and not exactly Interested in transitioning ? like hes fine with how he is. mostly.
he came out to Dave in high school but hes not out to anyone else exactly. Maybe his bandmates. Probably any other trans person in Undisclosed knows, too, cause theyre safe to tell lmao. Johns mostly a “he/him out of convenience” kinda nb who’s cool with any pronouns but does prefer they/them most. Dave and Amy use they/them when the trio are alone
Also this is a totally self-indulgent caveat that i think would be great, Dave’s actually agender but because he's transmasc and transitioned when he thought there were really only two options, and being Boy at least felt less weird than being Girl, he just kind of assumed he was a dude. It’s only through a lot of (like fucking years and years hes probably in his 30s/40s when he puts 2 and 2 together on this one) talks about gender with John that he realizes he actually feels like No Gender. Masc aesthetic with none gender.
I Just Think It’d Be Neat Is All Okay
Also Amy came out to Dave about being trans early on in them seeing each other and his response was to get very nervous before blurting out “me too” and then just being too embarrassed to talk about it for the rest of the day. Hes got a lot of hangups on talking about it actually it takes years for him to get comfortable in that
by contrast when Amy comes out to John about it his response is to yell “EYYY ME TOO” and give her a big ol hug lmao
I think itd be neatt if Amy ran a like. Transfem help/advice blog on tumblr. Kind of helped-with by John who can give her transfem nb insight for certain asks. I also just think that would be neat.
Cowboy AU - i put this one last cause its got drawings to it actually. Theyll be at the bottom
Basically just. Hey you ever watched a western. I think they look neat
This is another one me n ben have come up with lol
The soy sauce and all that shit still exist, im not sure where korrok fits in yet but ill figure it out
Theres no real like solid narrative yet ? but heres the barebones of everybody’s arcs.
John
Johns an absolute troublemaker, Of Course. Hes wanted in several towns for absolutely stupid shit. Hes a loner who shows up, causes chaos, gets drunk, does some drugs, runs away if people get too mad at him
He definitely had the same kind of deal with the soy sauce as in canon— he was at some kind of party, somebody offered it, he took it cause why the fuck wouldnt he, now he can see monsters and shit
Hes kind of a mooch also. Like. dont let him stay in your barn man he’ll never fucking leave and drink all your booze.
He runs into Dave when they happen to just, cross paths in the same town. the bullshit John stirs up ends up involving Dave in a way that makes it seem like it's his fault too, and they both get run out of town
after that he just tags along after Dave. hes decided this guy's Cool he wants to stick around. Dave is pissed at first, but not enough to shoot him or anything, and eventually, John grows on him
Dave
Dave also is a loner but unlike John hes simply so fucking awkward and bad with people. He doesnt feel like he belongs anywhere so he just travels
He’s the stereotypical Lone Ranger tbh. He wanders from town to town, solving their problems, though hed deny its out of any moral obligation (it kinda is, a little bit, tbh. He does like feeling useful). He shows up, fixes things, leaves. He's kind of a legend but most people think he's hiding something dark. other people jsut know him as that guy who farted real loud in the middle of the saloon and promptly skipped town out of sheer embarrassment. you know how it goes with Dave
He ends up involved with the Soy Sauce when a snake (not Actually a snake,) bites him. The snake’s more like the wig-monsters, really. Anyway, it injects him with the soy sauce, he fucking trips balls in the middle of the desert, he can see monsters now
He runs into John and shit goes tits-up, as said, but they become traveling buddies after that. he'd never say so, but he's glad for the company, actually. it's nice. hes not used to companionship but he feels a strange kind of easiness hanging out with John....
not sure how the Monster Dave concept will like fit in to this reality but like. trust me i want it in here. I'll Figure It Out.
Amy
Amy’s been living in a town John and Dave end up passing through and she is very curious about these two new Handsome Strangers who claim to fight monsters and just kinda. Persistently tags along til they let her join for real
Her family’s all dead, unfortunately, just like in canon, and she’s been living alone for a few years before meeting John n Dave. she had nothing left in that town to stay for, she'd been fantasizing about escaping on wild adventures for a long time and this felt a little like a dream come true. (Dave still gives her a spiel about how Difficult it is, but really, her fantasies were pretty grounded-in-reality already. i jsut think thats how she is, yknow?)
Shes the first person to react to the whole “we see monsters” shit with a kind of “oh, okay. neat” kind of response lmao
John and Dave fix whatever the fuck is up with her town (maybe that’s where the Korrok shit can fit, who knows) and Amy ends up being integral to that. After, she insists they take her with them because “they need her now” and Dave just cant really say no. John too is very much "the more the merrier!" and hes actually glad to have another person along he loves people lmao
At the start she has long hair but after she joins them she chops it short with a knife for convenience
also she still is an amputee. justt. idk. it was a wagon/stagecoach accident rather than a car accident lmao. just to clarify since i hadnt mentioned it, i wouldnt rob her of her ghost hand or yknow. all of the significance to her character that Missing A Hand has. although also now im going to have to research what was used as painkillers way-back-when, but im betting shes still got, like, her pain pills, they probably had those, maybe i wouldnt have to try too hard there. old timey medicine could be WACK though,
Shitload
Yeah hes in tthis shit mostly cause i liked designing his cowboy self lmao
Hes a kid (like 16, 17, technically i think in those days that was more Young Man than Kid but whatever. Hes Young i mean.) who got possessed by the Worms out in the desert and, by his family’s perception, just went missing!
Hes also a wanderer, but he ended up at the same town john and dave met in, at that same time, and starts following them after, already aware of who/what they are.
He keeps his face covered 24/7. actually he covers a Majority of his self for reasons. kinda want him to be a slightly more horrifying Worm Entity rather than human idk,
I kinda dont have much for this boy yet sorry Shitload
images !

with some editing notes for me cause im doing a very specific aesthetic with this lmao. i might change some lil details/colours though ...... idk

im also kinda 🤔 about shitload's colour palette. i want things assoicated w the sauce to be black'n'red predominantly but i think his palette might mirror dave's too closely. also im working on a korrok design i jsut am too busy to draw it now
#jdate#john dies at the end#aus#erh. tthe hell do i tag this as#rambles.txt#long post#well let me know if youd wanna hear more or. or something#send an ask. or whatever#yaknow#:jazz hands:
6 notes
·
View notes
Note
Do you have any comic book recs that are short? Like one-shots or mini series?
YESSSSSSS!!!! so many!!!
here’s a list of some personal favorite mini/maxi series of mine (with links!)
MINI-SERIES:
dark knights: death metal robin king (1 issue)
background knowledge required: middling. this takes place in the death metal storyline, so it’s nice to know what’s going on. but honestly, robin king’s story operates on its own pretty well as a glimpse into bruce waynes that could have been (and are!). i love robin king i think he’s adorable. tw for gore though.
nubia: real one (graphic novel)
background knowledge required: none. nubia’s backstory and connection to wondy is given and explained. HEAVY tw for police brutality, racism, school shootings, sexual harassment and the like. nubia: real one is written by a black woman and as such handles the topics fairly well, but it can still be upsetting.
year one: batman/scarecrow (2 issues)
background knowledge required: none! dive right in. gives us jon’s backstory and, provided you know who batman is, you get the gist real quick. great read, great art, great time.
timber wolf (5 issues)
background knowledge required: not much! this was my first brin comic. easy and quick. features one of lobo’s bastard sons, thrust! funny antics ensue. good story, good characters, some wacky coloring mistakes.
event leviathan (6 issues)
background knowledge required: some. you should probably know who the characters are, but other than that, it’s pretty easy. not a huge fan of b and jason’s characterizations here, but plas is in it (huge thumbs up) and he’s very weirdly homoerotic with the question.
plastic man 2018 (6 issues)
background knowledge required: none! jump right in! you see eel’s backstory, the villains are self explanatory, it’s a great characterization and a great read. has a canon trans character (two, if you count eel!) and is wonderfully written.
collapser (6 issues)
background knowledge required: absolutely none. this is a free floating comic. fun art, fun characters, fun story.
eternity girl (6 issues)
background knowledge required: like collapser, absolutely none. this series stands alone. heavy tw for suicide and self harm. it’s a heavy story but it’s really amazing. definitely worth a read.
MAXI-SERIES
black canary 2015 (12 issues)
gonna be honest, been too long for me to remember much about this comic, but the art is fuckin gorgeous.
metal men 2019 (12 issues)
background knowledge required: not too much. happens during death metal, so there’s alternate universe shenanigans. overall, just a fun read if you wanna watch a very sad scientist get even sadder.
doom patrol 2016 (12 issues)
background knowledge required: sssssome, but it’s nowhere near necessary. you can get a handle on the characters pretty quick, even if i would recommend reading morrison patrol first. fun read, fun characters, fun ending. followed by doom patrol: weight of the worlds, a 7 issue series of one-shots focusing on alternate universe versions of the doom patrol.
shade the changing girl (12 issues)
background knowledge required: some, but it’s not necessary. basically, she’s the successor to shade the changing man, but you get the gist of her whole deal pretty quickly, and reading his comics isn’t essential. he does appear in this series and his characterization isn’t... great.... but. if you’re just reading for loma, go for it. followed by shade the changing woman (6 issues).
dc/young animal: milk wars (graphic novel)
background knowledge required: read doom patrol 2016, shade the changing girl, aaaaand probably eternity girl first. the rest is pretty self explanatory and honestly if you wanna jump right in and see batman as a priest, i don’t blame you. it’s cool and really fucking weird. but it’s super fun! you should read milk wars!
hope this helped you find something good to read!!! much love
20 notes
·
View notes
Text
100 Humans on Netflix
So there’s this neat Netflix Original show called 100 Humans. I immediately got interested in it because they take this group of various humans from different backgrounds, age groups, and so on, and they use them to conduct experiments to get answers to interesting questions.
So, right away I had concerns about this show because
If you know anything about data and statistical research, you know 100 people is a very small sample size and does not breed accurate results
However, I’m very curious and wanted to see what they came up with anyway. I watched all 8 episodes and, honestly, I enjoyed watching it for the most part. However, I have a LOT of issues with the show and how it was conducted and I want to list them out here.
If you’re interested in watching 100 Humans or have already watched it, please consider the following before taking any of the show’s data as fact.
100 people is a very small sample size. This is because, the more people you have, the more weight each increment in your percentages has. With 100 people, each person represents 1 entire percent. That’s a lot. That means even a few people giving incorrect answers, having off-days, or giving ridiculous results (such as you can see in the spiders georg meme), can sway the entire result of an experiment into unreasonable territory. This is why most scientific studies attempt to get data from many hundreds or even thousands of people. The bigger the sample size, the more accurate it is to the entirety of the world.
I’ll put the rest under the cut because it gets long
The 3 hosts, who I’ll refer to as the scientists (regardless of if they actually are, because I’m not sure and don’t feel like googling it) repeatedly make false statements. For example, in one episode, they told their humans to “raise your hand if you believe you’re less bigoted than the average person here,” to which 94 people raised their hands. One of the scientists then made the statement, “If that were true, it would mean only 6% of Americans are bigoted.” This statement is entirely false. The only way to actually determine a true meaning to that would be to determine at what percentage of bigotry you are considered a real bigot. You also must consider that believing you’re more bigoted than other people in a small group, who you already have an impression of, is not necessarily indicative of how you feel you measure up to America as a whole. Anyway, I could go on and on. The only way to accurately summarize the results of that question would be to say that 44% of the humans had an inflated sense of righteousness or something of the sort.
The 3 scientists, both in person and in narration, for the sake of entertainment (if that’s what you call it) continually made “jokes” that poked fun at different groups, implied men are shit, etc. Maybe that’s fun for some people, but the kind of jokes they were making to amp up the hilarity of their host personas was genuinely just uncomfortable and made me feel even more like they couldn’t be trusted to go about unbiased research.
The scientists continually drew conclusions where the results should have been labeled inconclusive
The scientists made blanket statements about certain groups based on 1 element of research that would not stand up to further evaluation. For example, when explaining that ~93% (i think it was about that number) of Americans have access to clean, drinkable, tap water and yet some large number of single use bottled waters are sold every year, one scientist said it was because people believe bottled water is safer and cleaner than tap water. I am going to do my next survey on this to see if my own perception is flawed, but I simply don’t believe that all of the people who buy bottled water do so because they think its cleaner than “tap” (as if all tap is the same.) I know there have been studies about people drinking unlabeled bottled water and tap water and not being able to tell the difference, but this neglects to account for the fact that different houses pipes can affect the taste of the tap water running through them, people can use disposable bottles of water for certain activities or events too far away from tap for people to refill their reusable bottles easily, and so so so much more. Anyway, it just really bothers me to see “scientists” making these kinds of generalizations when they’re the ones whose results we’re supposed to trust.
The show was incredibly cisnormative. There was an entire episode based on comparing men and women that made me extremely uncomfortable with its division of people by men and women. There was the implication that all men have penises and all women have vaginas. There were implications that reproduction is a necessity in picking a partner. It was just a shitshow. There was one comment by one subject who asked, when being told to separate by men and women, “What if I’m transgender?” Obviously I can’t say for sure, but this person didn’t appear to be transgender and the sort of tone it was asked in makes me think it was literally something they asked him to say in order to get inclusivity points with the viewers and to “prove” that they’re not transphobic by having them divide up, because they said to go to the side you identify with.
This whole thing is a) harmful to nb folks who would not have had a side to go to and b) completely negating the fact that the way we were socialized can have an effect on our social responses. That means that for a social experiment, a trans person could sway the results of one side due to their upbringing and the pressures society put on them before/if they don’t pass. This is all assuming they had any trans people there, which is potentially debatable.
I also take issue with this entire fucking episode because just, the amount of toxicity in proving one sex is better than the others is really gross and actually counterproductive to everything feminist and progressive. Not to mention, them implying that they’re trying to support trans people only to reinforce the notion that a trans man is inherently lesser for being a man when even prior to hatching, he would have also been force fed propaganda and societal pressure implying he’s less than for supposedly being a woman is really gross and makes me angry. The point of what I’m saying is that it’s actually not woke to hate men as a way of bringing women up because there are men who are minorities who are being hurt by the rise of aggression being directed at them for their gender. Anyway enough about that.
The tests drew false conclusions because they did not account for how minorities adapt to a world that’s not made for them. This is specifically directed at the episode where subjects were asked to match up 6 people into couples. There were 3 women and 3 men and the humans were asked to put them together into pairs. they could ask the people 1 question each but then had to match them up with only that information.
The truth is, the people brought in were 3 real life couples already, which the humans didn’t know until after they matched them. The couples were m/f, m/m, and f/f. I think that’s great, but the problem is, literally none of the humans asked any of them their sexuality as their question and most people didn’t even consider they could match up same-sex people. One girl even thought that they had told her to make m/f pairings, even though they didn’t.
The scientists concluded from the experiment that the humans have a societal bias toward people, and assume they’re all straight, even if they, themselves, are not straight. I personally believe that was the wrong conclusion to draw. You could see some of the queer humans were shocked that they hadn’t considered some of the pairings might be gay. But, I don’t think it’s because they believe everyone they meet is straight, I believe this says more about what they expected from the scientists themselves.
If someone is in a minority and they go to do something organized, like a set of experiments, they are going to be judging the quality and setup of the experiments by those designing them. I feel that the lack of consideration that the couples might be gay has a lot more to do with queer people having adapted to a world where queers are rarely involved or included in equal volume to the cishets. The queer humans taking part in the experiment and failing to guess gay couples shows that they have adapted to a world where they are excluded rather than a belief that every random person that they meet is straight.
My point is further supported by an expert they had on the show who explained that, statistically, it was entirely likely that they were all straight and that even queers will account for being minorities by going with what’s most likely. The truth is, we are surrounded by a whole lot of straight people. It makes sense to assume only 6 people are all straight and that, if any aren’t, they may be bi.
The scientists frequently broke an already small sample size into even smaller groups. The group was very frequently broken in half, in thirds, or into sets of 10 people. These sample sizes tell us almost nothing actually conclusive.
The experiments/tests frequently were affected by peoples abilities, unrelated to what was being tested. For example, one test that was broken down into 6 people and 6 control people competing at jenga was meant to show whether needing to pee helps or hurts your focus. first of all, sample sizes of 6 are a fucking joke. Second, this completely ignores these 6 people’s actual ability to play Jenga. If someone sucks at jenga with or without needing to pee, them losing Jenga when they need to pee says exactly fuck all about whether needing to pee affected their focus. They should have tested people’s Jenga skills beforehand, counted the amount of moves they made before the tower fell, and then did it again after hours of not peeing to compare their results. This test made no logical sense at all.
The scientists ignored the social effect of subjects knowing each other as well as duration of events during their last experiment. They were testing to see if people with last names near the end of the alphabet get a shittier deal because they go last in everything where things are done by name order. They tested this by doing a fake awards ceremony where they gave out some 30 awards to people, gauging the applause to see whether the people at the end got less hype and therefore felt worse about themselves than those in the beginning who got the fresh enthusiasm of the audience.
the results showed that the applause remained fairly consistent throughout the awards. The issues with this test are numerous, but here are the three I take most issue with.
1) the people here all got to know each other very well over the week it took to make the show. People who know each other and have become friends are much more likely to cheer for each other with enthusiasm, regardless of how long it’s been. On the other hand, polite applause from a crowd at, say, a graduation, where you are applauding people you don’t know, WILL start off more raucous and grow very quiet except for individual families near the end.
2) the duration of the test was a half hour, which is not very long at all and doesn’t say much to test the limits of enthusiasm. Try testing the audience at a graduation with a couple hundred graduates that also involves the time it takes to walk all the way up to a stage a hundred feet away, accept a diploma, and then wait for the next person. These kinds of events take hours and nobody keeps up their enthusiasm that long unless they’re rooting for someone in particular.
3) this study tested only one of many many ways name order affects a person. Cheering and applause is only one factor. It does not take into account people having their resumes looked at in alphabetical order and therefore people at the beginning of the alphabet being picked before anyone ever looks at a W name’s resume. It doesn’t take into account a small child’s show and tell day being at the very end of the school year, after 6 other people have brought in the same thing they planned to. No one cares about their really cool trinket because they’ve seen a bunch like it already. This test doesn’t take into account how many end-of-the-alphabet people just get straight up told, “we ran out of time. maybe next time,” when next time doesn’t really exist. I feel genuinely bad for the girl who suggested this experiment because the scientists straight up said something akin to, “lmao her theory was bs ig /shrug” even though it was their own shitty research abilities that led to their results.
They did one experiment intending to see how many people have what it takes to be a “hero.” The request for this test was made by someone curious about the effect of adrenaline and if it really works how some people say. The scientists thought it an adequate method to determine an answer by testing their reflexes with a weird crying baby sound and then dropping a doll from above while they were distracted with answering questions. The scientists looked up before the doll dropped to indicate a direction of attention. While this does give some answers about peoples intuition, reflexes, and ability to use context clues, its entirely an unusual situation, makes no sense in reality, fails to take adrenaline into consideration literally at all, and has a lot more to do with chance. The person dropping the doll literally couldn’t even drop it in the same place from person to person. Some got it dropped into their lap and others almost out of arm’s reach. This, like a few of the other mentioned experiments, was during the last episode, which felt lazy and thrown together last minute, with very little scientific basis to any of the results. The last episode was weak and disappointing overall.
One of the big issues I have with this show is actually their repeated use of the same group. They said at the end that they had done over 40 tests. Part of doing studies is getting varied samples of people in order to get more widespread results. Using the same 100 or less people (already a tiny sample) repeatedly is a terrible research method. You’re no longer studying humans at large. You’re studying these specific humans. You can’t take the same group with the same set of inadequacies, the same set of skills, and the same set of biases and then study them extensively and in many different ways like this. Your results are inherently skewed toward these specific people and their abilities. I expected them to at least get a new group each episode - every 5 or so studies - but no. They keep the same group all week, which makes the entire season. This is inexcusable in research imo.
The next issue is contestant familiarity. The humans all getting to know each other is great, socially, but it also destroys the legitimacy of many of the studies that involve working together or comparing yourselves and your beliefs
Many tests had issues with subject dependency. One study, meant to compare age groups and their ability to work together to complete the task of putting together a piece of ready to assemble furniture had each group with members they relied on entirely. A few people built the furniture while one person sat across the room, looking at instructions with their back to the others. They had to relay the instructions through a walkie talkie to another contestant and that other contestant had to relay it to the people they’re watching build the chair. You cannot study a group’s ability to build something with instructions by the ability of one single person to communicate. You’re testing that individual and the rest of them on two completely different capabilities. One person fails at being able to communicate and everyone else becomes unable to build the furniture. Even if everyone else in the group is more effective than all the other groups at building ready to assemble furniture, they might end up falling in last because of their shitty communicator who is literally not able to convey simple instructions. (yes, this actually happened in the test)
One test judged the subjects at their speed of getting ready, to see if men or women are faster at getting ready. While most elements of this test were just fine, the part I took issue with was that they did this test without regard to social convention. They told the subjects they were going on a field trip and to get ready by a certain time. Then, they gave them many things to get distracted by, like refreshments to pack with them, a menu to preorder lunch from, and so on.
The part that upsets me about this test is that they ignored social convention entirely, to the point that subjects were judged based on their conventional actions and expectations more than their actual speed at getting ready. The buses promptly shut their doors and left at the time they were supposed to but there was no final call to get on the buses. In general, when a group is to be taken somewhere by bus, there will be an announcement to load up and leave. You could clearly see many of the subjects were ready to go and were just standing around talking while they waited for fellow subjects to finish getting ready. I have no doubt that, if given a final call, most of them would have loaded up within a couple minutes. However, they were relying on the social convention of announcing departure and were therefore, left behind entirely (for a nonexistent field trip). These people who were left behind were counted as being late and not making the time cutoff.
If one were to look at the social element of this situation, if everyone there believed there would be a warning before departure, the fact that 24 to 14 women to men were loaded onto the buses at departure doesn’t necessarily indicate the women were faster to get ready. It seems to me that it’s more likely to indicate anxiety at being late and a belief that they need not impede on anything lest they be reprimanded or have social consequences for taking too long - something women are frequently bullied for. There’s also the chance that many who boarded without final call are more introverted or antisocial. Plus, we can’t forget to include the people who have anxiety about seating. If someone is overweight, has joint pain, or has social anxiety, they will be more likely to board early to get a seat they feel comfortable in.
If they had counted up all of the people socializing and waiting on the sidewalks nearby, they may have found that there were more men who were ready to board up at a moment’s notice. I’m not saying I think men are faster to get ready, I’m just saying that we can’t know based on who boarded without a final call. If people believe they will have a last minute chance to board, a large number of them will take the last few minutes to socialize with their new friends until they’re told they have to board. Therefore, this test cannot be considered conclusive without counting and including the people who were ready and not boarded as a third subset.
Honestly, I could go on and on about how sensationalist and unscientific this show is, but I just don’t have 6 more hours to contribute to digging up every single flaw with it. There’s A Lot.
My point is, if you feel like watching this show, which I don’t necessarily discourage inherently, I just beg you to go into it with a critical eye. Enjoy the fun of it and the social aspects, but please don’t rely on the information provided and please don’t spread it as fact, because it’s not.
It’s entertainment, not science.
#100 humans#netflix#tv#show#science#scientific research#research#studies#study#studyblr#statistics#stats#sociology#data#netflix original#analysis#review#netflix review#show review#tv review#ghostpost#logical fallacy#logic#correlation#causation
10 notes
·
View notes
Note
Do you have any podcast recommendations? I've listened to tma, wolf359, the penumbra podcast, and like...half of night vale. You seem like you'd know some good ones!
!!!
I Am In Eskew is an absolute all-time favorite of mine! It’s very firmly horror, but not tragedy. Think… WTNV but 1. on a personal scale, 2. actually terrifying, and 3. not benign. It follows David Ward, inhabitant of the city Eskew, as he chronicles some of the terrifying stuff that happens to him. Eventually, we hear from Riyo Dulae, a private investigator who’s been pulled into Eskew’s orbit. It uses place-as-horror in an astonishing way! It’s a finished product with 30 episodes and the ending is honestly amazing. I’ve listened to it several times. It’s very good. Listen to it. Please.
This got long, so the rest of the recommendations are under the cut, and in no particular order! (Eskew is absolutely my top recommendation lol) Particularly sad endings and ongoing series are specified.
Janus Descending is a finished and relatively short sci-fi horror series. It follows two xenoarcheologists (archeologists for aliens) as they inspect the site of an abandoned alien civilization. It’s told in inverse chronological order, alternating between Chel and Peter’s perspectives. Chel’s is chronological, while Peter’s is backwards. It’s an amazing format and keeps you suspended in the mystery up until the very end! It is a tragedy, though, and has a sad ending.
ars PARADOXICA is an audio drama about time-travel and the Cold War. The synopsis is this: scientist Sally Grissom accidentally creates time travel, is transported back to the Cold War, and is entwined with a clandestine branch of the US government. It’s 3 seasons long- and I will say that if you’re not good with differentiating voices I recommend either listening to it without stopping for a long period and/or reading along to transcripts. The plot is intricate but engaging and the large cast of characters each has their own unique personality. Plus: canon ace main character (as in she says she’s asexual! in canon!), a Jewish lesbian semi-main character, a mlm (bi?) man of color side-character, and several other characters of color.
Mabel is an ongoing horror podcast with elements of fae/fairy lore and the place-as-horror theme. It’s not as outright horror as TMA, Eskew, or Janus Descending, it’s much more atmospheric? It’s several seasons in, with the next season currently in production. It follows Anna Limon, who is an in-home caretaker, trying to contact Mabel Martin, the granddaughter of the woman Anna is caring for. It has lots of wlw, lots of moral ambiguity, beautiful prose, and lots and lots of fae.
Zero Hours is a 7 episode long anthology series by the creators of Wolf 359. Each episode deals with “the end of the world - or at least something that feels like the end of the world.” There’s 99-year intervals between episode and it starts in the past and ends in the far future. It’s honestly stunning and was well worth listening to in it’s entirety when it dropped (and subsequently staying up past midnight).
The Bright Sessions is… kinda urban fantasy? The official synopsis is that TBS is a “science fiction podcast that follows a group of therapy patients. But these are not your typical patients - each has a unique supernatural ability. The show documents their struggles and discoveries as well as the motivations of their mysterious therapist, Dr. Bright.” (I tried explaining but was having a tricky time) The characters are amazingly written and unique. (And no, it doesn’t fall into the “evil therapist” idea, in case you were worried) One of the main characters is gay (and it isn’t a throwaway line). It has good and realistic representation of mental illnesses: a main character as a panic/anxiety disorder, another has PTSD, another has depression, and so on. The main show is finished but there’s a spin off that’s being made. Specifically happy ending!
Alice Isn’t Dead is a horror podcast by the creators of Night Vale. It follows Keisha, a trucker, who is looking for her wife, Alice. Keisha encounters many strange things as she drives back and forth across America, including murderous almost-human monsters, places that are stuck out of time, and a nation spanning conspiracy. It encompasses the whole… atmosphere of middle-of-nowhere America perfectly. It’s a complete story with a novel form (haven’t had the pleasure of reading it, though). Main character is wlw, and Alice is not dead.
Limetown is a horror podcast. It follows reporter Lia Haddock as she investigates the mystery of Limetown- a town in Tennessee where over 300 people disappeared overnight, never to be heard from again. It’s finished…? I think the podcast is finished but a book and a Facebook miniseries are in development? Anyways. Sad ending. I loved the first season a lot, the second season is good too though!
The Adventure Zone isn’t an audio drama, instead it’s an actual-play show of Dungeons and Dragons (and D&D like systems). The McElroy brothers and their dad host it, and are frankly absolutely hilarious. TAZ: Balance is the first season and starts as a classic d&d game but turns into an amazing and heart wrenching story with beautiful prose and music. And also 69 jokes. TAZ:B is honestly one of the most emotionally impacting stories I’ve ever heard. It has an amazingly happy and hopeful ending. Includes: casual lgbt rep and a late game but major character is a trans woman! I’ve heard good things about the recently finished season TAZ: Amnesty, although I haven’t finished it. There’s a new season, TAZ: Graduation, that started recently, and I’ve enjoyed the handful of episodes I’ve listened to! Currently ongoing, but tragic endings aren’t something that’s expected.
I haven’t finished/caught up with these, but I’ve enjoyed them: Sayer (sci-fi. think menacing capitalist Night Vale in space, heard s3/s4 are really good), The Bridge (horror, alternate modern day. follows a watchpost on a bridge that crosses the Atlantic), The Orbiting Human Circus (from the people at WTNV. surreal fiction. hard to explain). I feel like there’s more but I can’t remember any atm.
I’m also gonna point you towards @theradioghost‘s blog and her podcast recs tag. Her taste is amazing and I haven’t disliked a single show I’ve tried. (Also, check out her show, Midnight Radio! It’s the next thing on my to-listen list.)
82 notes
·
View notes
Text
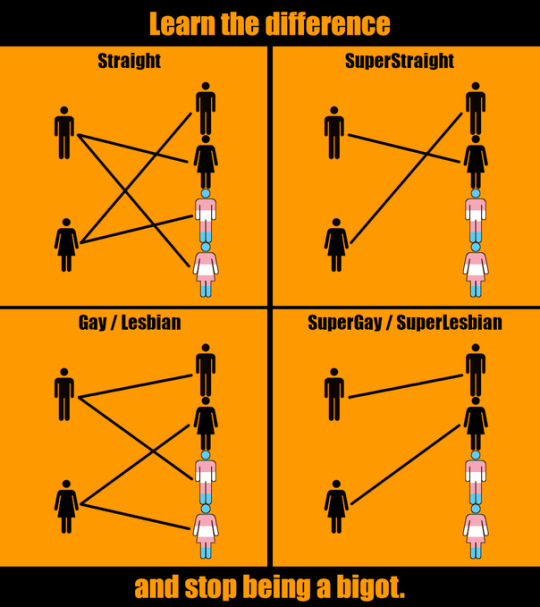
SuperStraight
A brand new sexuality that is trending on twitter and being super popular.
Definition:
A superstraight person is someone attracted to members of the opposite gender who are not transexual.

This was created as a response to people who sometimes say things like this:
(source:BBC)
Let’s give a name to the people who insist that not being attracted to trans people makes you transphobic, since I’m not about to describe them every time i wanna bring them up, I’ll call them trans-incels because just like incels they resent people for not wanting to have sex with them.
It’s worth it to remember that trans-incels aren’t representative of all trans people. or even of a majority of them, if i were to bet, they are about as popular as actual incels.

In all the comment sections I checked the anti trans-incel side was a clear majority, and having searched for “superstraight” on youtube to see what people have to say, the first video on the list, from a trans man, is definetely anti trans-incel .
> If you don’t want to date a trans person that’s fine, and if somebody is trying to force you they’re just an asshole
-probably most trans people
From the perspective of a trans-incel (and how we’re all assuming too much)
Imagine a person.
Imagine the probability that they are racist.
Imagine that same person saying “i wouldn’t date a black person”
Has the probability increased at all? be honest, it hasn’t gone up to 100% (which would be the race-incel response) but it must have gone up by at least a little.
But why did it go up by a little? Because now the chance they’ll say something like “because blacks disgust me” has also gone up.
Now imagine being into internet drama (ew) and as a trans person, you’re especially interested in people being transphobic and you probably see transphobia every day because people like talking about it as much as anti-sjw(tm) people like to talk about the trans-incels.
If discussions about trans people only gets to you when it causes drama you’ll probably never see “i wouldn’t date trans men/women...” without having it be followed by “...because they’re not real men/women”.
And even though the whole point of being superstraight is to explain why people wouldn’t date trans men/women without calling them ‘not real men/women’ lets see what the original guy who started the whole superstraight meme has to say at second 15.
https://youtu.be/z8vQhkPnEE4
It’s like instead of throwing bait, they’re just throwing food.
The more you see “...because they’re not real men/women” the more likely you are to expect it, and as someone who subscribes to people posting drama 24/7 you’ll see that hundreds of times until you end up answering ...
the probability that the person who says ‘i wouldn’t date trans men/women’ to be transphobic is 100%
...and even if they don’t follow up with something transphobic it’s always easier to imagine they’re just hiding it rather than to change your whole worldview on the spot.
And if you think “why do they even predict transphobia before its spoken”, well, this might sound crazy to you, but everyone is assuming things all the time, our whole perception of reality is nothing but a hallucination that our brain comes up with using not only stimulus from the world but also assumptions.

There’s a blind spot on each 1 of your eyes, your brain simply fills it in without you knowing, it also adds color to the edge of your vision and makes the whole thing less blurry.
When someone says “i won’t date trans people” some people will simply fill in the blanks, they’ll assume every bit of info about who you are what you believe in what your personality is from just a sentence, because the brain is literally designed for it.
IQ tests are just patterns where a spot is blanked out and you’re supposed to fill it in, your intelligence is measured by your ability to fill in the blanks, and low intelligence people will just make mistakes more often, but everyone smart or dumb will constantly make assumptions about everything, and dumb people will be proven wrong about their assumptions more often.
And this happens all the time even when you’re not talking about politics or having a fight.

Someone talking about the earth being curved? well, every time I saw someone do that they called it a sphere so let me just fill in the blanks.
Someone saying they wouldn’t date trans women? well, every time I see screenshots of people saying that in my drama facebook group i see them being transphobic, so let me just fill in the blanks
That’s just how incels operate.
Building legitimacy
Have you ever noticed that every sexual preference eventually gets assigned a flag, on that note, why does every country have a flag?
If you ask a regular person to guess why their country has a flag you’ll get something related to aesthetics, our flags represent our country.
For example Romania and Hungary:

In school we are taught that each colour on our flag has a different meaning, I searched on google and everyone disagrees on what they mean but as an example.
Liberty (sky-blue), Justice (field yellow), Fraternity (blood red)
Outside of school I was taught by my grandma that the Hungarian flag, much like the Romanian flag, also has a meaning.
The green represents a wide field of green grass, the white represents a white dog playing on the field of grass, rolling around on his back, and the red represents his red dog cock.
Both of these meanings are pretty much just something that a Romanian randomly came up with so i don’t think most people know why countries have flags.
Flags originate from war, that way the armies know not to attack their own allies when they see they carry the same flag, having an army grants you true legitimacy because you can just beat people up into believing you’re legitimate, so countries with no armies probably still had flags because it would be really hard to pretend you have an army otherwise.
Nowadays every country has a flag even if war is illegal, simply because every country has been using one for so long that it became convention. If you don’t follow convention you will be seen as illegitimate. It’s an unwritten rule, but a rule nonetheless, that you need a flag, and much like not following written rules makes you illegitimate (and illegal) so does not following unwritten rules.
And sexualities having their own flags and names probably feels like an even stronger convention than countries having flags for some people.
It’s very often brought up that you have to feel “valid” (which more or less means “legitimate”)
I still don’t know why, but it’s apparent that people need to be reassured that their sexuality is “valid” and then there’s also this:

Why does a sexual preference have to be distinct from a sexuality? I don’t know, but I’m pretty sure the only difference between the two is legitimacy, to confirm to the conventions of flags and labels.
Q: So why do superstraights get a label and a flag and copy everything that LGBT people do, like tweets talking about how valid their followers are or using the word bigot etc
A: Because to get true legitimacy you need to copy the conventions.
The cargo cult
(wikipedia) Some primitive tribes of people would look at colonists from the civilised world and notice that after they’d built some plane lanes, the planes would come bringing cargo full of valuable stuff.
The tribesmen have made the observation that planes land if you build lanes for them to land on, they made the hypothesis that building the lanes causes the planes to come, and like scientists, they set out to test it.

They made lanes, they made fake planes, they tried to copy everything that the colonists did hoping it would be enough.
Superstraight is a lot like a cargo cult of sexualities, they have a flag, they have a label, they call everyone bigots all the time.
This is the first pic I sent before cropping it.
Because, like a cargo cultist who does not see the plane factories from the colonists homelands, the superstraight person does not see the LGBT community from outside his filter bubble, the filter bubble where only the most obnoxious people like the trans-incels can get through.
So when the superstraight person who thinks every LGBT person is just an obnoxious incel tries to “fit in” with the LGBT, they will act like an obnoxious incel, and when everyone is angry at him, he thinks to himself “they've all proven themselves hypocrites! i baited them so hard! i won!!!”
Even tho there’s a bunch of LGBT people from the comment sections I read who don’t even know the trans-incels even exist, because their filters simply don’t show them the same things you superstraight people are shown.
It gets worse
There’s some people who are so cocky and think they’re so much smarter than the LGBT community that they can just sneak in the nazi SS symbol into their flag and not just fuck up the bait completely.

hehe Schutzstaffel fla- wait! you cant call me a nazi! this is just another sexuality you hypocriteeeee
But this is also just a minority of the people who get superstraight trending, its so popular that I’m pretty sure most of the people getting it to trend are actual normies who wouldn’t even recognise the SS symbol and who have never been to 4chan.
Speaking of 4chan

Of course people don’t think superstraight is legitimate when you have 4chan taking credit for it.
They pick up on all the superficial customs like the flag the label the speech patterns and think “this is their, logic, im using it against them, and they’re all mad because of this alone and not just because a we’re comparing ourselves to the Schutzstaffel”
In a turing test a computer attempts to pass as a human.
In the ideological turing test a human tries to pass as someone of a different ideology.
Are people afraid of passing the ideological turing test? do they think if they can think like the enemy, then they’ll become the enemy? there was no need for people on 4chan to talk so openly about superstraight being a ruse, there was no need to make nazi memes with it, there is no need to post “we used their logic against them”, to constantly tell “yes this is all a lie”.
And yet people have to constantly break character and expose superstraight for being a fake sexuality, why? what’s even the point of it then?
What it could have been
Imagine a world in which instead of making a cargo cult sexuality and just delegitimizing it yourself with all the actual nazi symbolism, you were able to cancel trans-incels.
Imagine if they were able to say things like “the trans-incels are trying to create a new rape culture in which superstraight people are coerced into having sex with transexual people” with a straight face
Imagine if they even tried to coin the term “trans-incels”, since incels are hated by progressives for misogyny and are often associated with 4chan.
Imagine if they could get people banned for hate-speech against the superstraight
Imagine if they had the balls to denounce the people amongst them trying to delegitimise superstraight with their nazi SS and obvious parodying of the points that aren’t taken seriously by anyone who doesn’t call themselves anti-sjw.
Maybe then there’d be some divide between “pro-superstraight” and “anti-superstraight” instead of everyone who’s not anti-trans agreeing that superstraights aren’t legit.
Maybe they’d be able to get some people canceled, there’s been at least one actual celebrity (India Willoughby) who is a trans-incel, they could have canceled her! but nobody is even trying.
And oh how much “applying their own logic against them” would have been true if as a response to “but not all trans people are calling you transphobic for having a sexual preference!” you dusted off the “not all men are like that” memes that was popular with feminists.
If they would go on the offensive, cancelling people, spreading trans-incel screenshots to everyone who says they’ve never seen one, mocking people who stand up against them the way feminists used to and say “nOt aLl TrANs pEopLe aRE liKE THat” to anyone who says “not all trans people are like that”, to tell them that “silence is violence” and to make them cancel eachother.
Imagine how much more effective that would have been.
In the end this isn’t gonna make a difference, it will be forgotten, maybe in a couple months, or a year, or a week, some people are angry today because a counterculture hashtag is trending, but they’ll forget about it too, maybe a couple dozen people will permanently have superstraight on their twitter bios, but really, nothing interesting is gonna come out of it, and if someone tries to make something like whitesexual/blacksexual/asiansexual etc a thing the well will have already been poisoned by superstraight.
1 note
·
View note
Text
Look Out for These Words on Food Labels

"Natural"
This term has yet to be fully defined and typically goes unregulated. The U.S. Fda states that it has actually not developed an interpretation for the term, yet it does not challenge it being utilized for foods that do not contain synthetic flavors, included shade, or artificial materials. While customers may such as to believe that 'natural' indicates the item is much less refined, this may not always hold true. Do not assume 'all-natural' indicates healthy and balanced. Make certain to look past this term and analyze nourishment tags and active ingredient lists.
"Low Sugar" or "Sugar Free"
Eating much less sugar can enhance wellness and also promote weight loss, however when an item says it is 'low sugar' or 'sugar complimentary,' examine the active ingredient tag very closely. This commonly indicates that the sugar was changed with another thing, typically a sweetening agent. Some research study has actually connected the intake of man-made sweeteners to weight gain. As scientists remain to check out the subject, it might be best to restrict both sugarcoated and also sweetening agents.
"Trans Fat Free"
The American Heart Association recommends restricting trans fat consumption to much less than 1 percent of overall calories daily. For many people, this is less than 2 grams. According to labeling regulations, a food that consists of less than 0.5 grams of trans fat per offering can be labeled as 'trans fat free.' If you consume greater than one offering of a food with simply under 0.5 grams of trans fat, you will swiftly reach your 2 gram restriction without realizing it. Check out component listings carefully. The expression 'partly hydrogenated oils' is an indicator that the product includes trans fat.
"Product" or "Food"
These terms are commonly used when food has actually been greatly processed or when it integrates a selection of ingredients to create a product that appears like a food you might be familiar with. The most common use is with cheese. Examine the tags very closely. 'Cheese foods' and also 'cheese products' may contain little to no cheese in any way. You might be far better off enjoying a percentage of the genuine food in moderation instead of taking in the highly-processed fillers.
"Spread"
' Spread' is a term utilized when an item does not fulfill policies to be called the food it appears like. Peanut butter should include 90 percent peanuts. When the product doesn't, it is called a peanut spread. In some situations, spreads utilize fillers like corn-syrup solids and also partially hydrogenated oils. These active ingredients may lower total fat, however they enhance included sugar as well as unsafe trans fats. It may be far better to skip artificial spreads and also consume the initial type of the food in small amounts.
"Made with "
Many products claim that they are 'made with fruit' or 'made with whole grains.' There is no collection amount of the ingredient the food should include to make this claim. It's feasible that it only has a little amount of fruit or entire grains. Look for '100%' to ensure the food contains only the ingredients you are looking for.
8 notes
·
View notes
Text
Wednesday Roundup 8.11.2017
First of all, shoutout and special thanks to my patrons on Patreon, who for as little as $1 per project each month are helping me to grow and expand what I do here on renaramblesaboutcomics and all my other blogs and projects including starting up my own comic. So special thanks to c. win, Erin Jenne, Iz, Keerthana Krosuri, OwlKnight, Rebecca Luu, and Steph.
Now, for this week in comics we have another full and healthy week of comics coming out from almost all the major publishers and then some! But how will they survive my new FIVE STAR RANKING SYSTEM. i mean it’s not that big of a deal, it’s the same as any five point rating scale but the point remains.

Tesladyne’s Atomic Robo and the Spectre of Tomorrow, DC’s Batgirl and the Birds of Prey, DC’s DC Essentials Catalog 2018, DC’s Justice League Day, Viz’s My Hero Academia, Marvel’s Old Man Logan, Dark Horse’s Overwatch, Marvel’s Runaways, DC’s Superman - Action Comics, IDW’s Teenage Mutant Ninja Turtles/Ghostbusters II, DC’s Titans, IDW’s Transformers: First Strike
Tesladyne’s Atomic Robo and the Spectre of Tomorrow #1
Brian Clevinger, Scott Wegener, Anthony Clark, Jeff Powell

To say I have been curious about how Atomic Robo was going to deal with the current political and scientific landscape is sincerely an understatement, because I have been just sitting on edge, wondering if we would be getting another historical arc or at least placed in the not-so-distant past for context. After all, here in America that hasn’t really been an anti-science climate quite like there is right now. At least not within my own lifetime.
But, of course, I should have had far more faith in the foresight and boldness that Clevinger and Wegener have always shown in their craft. Which, of course, is a perfect description of their ongoing science-adventure epic Atomic Robo, because for as scientifically and fiction minded as the pulp adventures are, the fact that it is art is undeniable.
Art is about communicating concepts and ideas, and as scientifically minded as Robo and his team of scientists at Tesladyne may be, and as much as science based nerds like myself appreciate how the science is not bent or broken entirely for the sake of the storytelling, it is masterful at portraying science in a way that is accessible and, most important of all as it relates to Robo, humanizing.
While it’s a slow start to this new arc, what really drives it home is Robo’s frustration and sacrifice for the sake of his dream, and how ignoring the human elements has allowed the politics and general climate of the world around him to drown out his work and inhibit him. Even if the only insight we get to the hurdles is his humorous annoyance with the desert’s self-proclaimed HOA that is between himself, Elon Musk, and Sir Richard Branson, the imposing and overly restrictive hold of Red Tape and permit seeking is imposing all throughout the issue, even for the major parts of it center more around the wily antics and return of young Foley.
And of course, it wouldn’t be Robo without major hinting toward something larger and unexpected to come.
It’s not the most perfect introduction to an arc, especially not for Atomic Robo which has at times had some of the most engaging first issues of almost any long form comic I’ve seen, we are talking about a comic where the electricity-driven skeleton of Thomas Edison is a villain. So it is just short of the high bar that it has set for itself, but even falling short Atomic Robo manages to be one of the best comics of a given week. That for me is justification enough for a solid 4/5 Stars.

DC’s DC Essentials Catalog 2018

Straight up, I am not a fan of Catalogues and I’m definitely almost never in agreement with the books they choose for each of the catalogue’s sections. So it’s not like I’m going to be less than truthful with this guy.
But my harshness is probably best explained as to why I’m being harsh, after all most people would not care that much about what is essentially a free throw-in with someone’s pull list in the week. And, honestly, my answer there is that because it’s free, because it’s promotional and being pushed onto new readers, its viability as a good entry level or at least how helpful it is as a guide for interested new readers, increases exponentially here.
So how does it work on that level, especially with the release of the Justice League movie looming over DC currently? How likely will this persuade a new reader to start getting more submersed into the comic books it’s trying to represent?
Annnnnd the answer there is not great?
There’s a short comic at the start, introducing the Justice League and wow is it a testament to how out of touch the lineup is with the increasingly diverse culture of nerds and comic book fandom. Five beefy white guys, one white woman, and one black man. Like it’s seven years into the new DC Universe (technically) and you couldn’t trade anyone here out for some more, less milk toast characters by this point? Hal Jordan couldn’t be traded out for any other Lanterns at all? It’s annoying. And at least something the Justice League movie will be at least somewhat better at thanks to the very awesome casting of Jason Mamoa as Aquaman.
But that’s still only a small part of this issue. The rest of it, and by that admission the vast majority of this digital freebie is dedicated to the “essential reading” of DC as of 2018. And much like the lineup of their premiere team, DC has repeatedly proven in the last couple of years that they... don’t know what to suggest. Most notoriously there was the Essentials collection where they literally had a section for each of the male Justice League members and like. One book for Wonder Woman. That was embarrassing and if we had anything remotely similar it would be our first 1 star of the new rating system, but it’s honestly a much longer, much more thorough and comprehensive version of a reading list for DC and in that way, while still not a “standard” or “satisfactory” example of how to really capture the attention of new fans, and its choices aren’t always the most coherent alongside each other, it doesn’t completely fail at its mission by my estimate.

DC’s Batgirl and the Birds of Prey (2016-present) #16
Julie Benson, Shawna Benson, Roge Antonio, Marcelo Maiolo

The Benson sisters already have to win me over after the first arc of this series which I found terribly disappointing so far as uniting the team that I know and love as the Birds of Prey and not really being on board with the last issue for all the reasons I said in this review.
So I was somewhat apprehensive from the start but, honestly, if you follow this blog for a while you know I’m a sucker for giant superhero team-up storylines and am really willing to hold my sense of disbelief a lot more than even what I regularly do for comics.
....
So why are the villains of this team-up literally militarized paper feminists in.... well, in the United States the first thing that comes to mind when a lot of white people wear uniformed cloaks with hoods and masks is the KKK, of course these masks are old plague doctor masks that double for some kind of... gas. Okay.
But like. Considering the current environment in not just the US but the whole world... just putting into words “the real problems in the world right now are radical feminists” here and having our superheroes literally say “Not all men in Gotham”... If I’m being generous this is a whole lot of shady and uncomfortable. If we’re not supposed to read deeper into this, then why the surface level imagery and blanket statements that so immediately bring to mind current issues. If we’re supposed to read deeper why does it feel so unrewarding with none of the characters having enough time in a team-up this large to really experience the events any deeper than surface level.
And there’s still not even a mention of how this event would effect trans men or women, or how this disease is even supposed to be effecting only people who identify as men to begin with. It’s apparently scientifically based according to this issue and the continued mention of medical investigation from Ivy and the villains themselves. If someone claims it’s due to the Y chromosome then trans and nonbinary people would be effected differently on a case by case basis, giving the medical community a pretty quick idea of what was happening. Not to mention that XXY women and men, XYY men, XXX women, and so on should be effected differently. Now I’m not expecting a comic book writer to write a genetics dissertation for research on a comic idea but if they want to be a mature or adult comic in subject matter, then high school biology should not immediately tear their entire plot apart.
I just. Really feel like this book wanted an all-female superhero team-up and thought there needed to be justification for why the men weren’t around instead of it just.... being unsaid as to why there weren’t men on the team. And things have spiraled out from there. On top of that, the art is not strong enough to regain the things that are lost in what is a clustered and puddle deep storyline.
These sorts of team ups are best when the subject being dealt with is not so politically or culturally charged, or when there is very clearly a reason for each of the present characters to be in the exact positions that they are in. And so far this crossover hasn’t really managed to believably pull this off.

DC’s Justice League #1 - Justice League Day 2017 Special Edition
Geoff Johns, Jim Lee, Scott Williams, Alex Sinclair

This issue is really a sampler for the larger issue that is Justice League (2011-2016) #1 which... I’ll be honest, has not aged the best of the Justice League origins that I commonly think of, and really the fact that this sample contains pretty much no Wonder Woman or Flash, it’s hard to really see why outside of this scene between Batman and Green Lantern which has become somewhat iconic in the superhero community, I don’t really get.
I mean, the scene itself is so anti-climactic specifically because it ends with Batman stealing Green Lantern’s power ring to prove that Batman Is Always The Best Period. And if you’re of my persuasion in the comic reading landscape, that probably means you just rolled your eyes as much as I usually do at those sentiments
This is probably okay for a new, entry level fan to pick up for free, but personally I feel like I’ve picked up this particular freebie now five times for different FCBDs or other marketing pushes DC has had in the past six years and it’s just not enough that I’d consider it worth more than sacrificing the literal $0.99 it would cost you to pick up the whole issue on the same website.

Viz’s My Hero Academia (2014-present) Vol. 10
Kohei Horikoshi

I have been making more of an effort lately to keep away from any spoilers to My Hero Academia, be it the anime or the manga, and while it’s not always the easiest thing to do on a content aggregator like tumblr, it’s an effort I’m particularly happy with myself for doing because I love this series. And one thing I love about this series is how it seems so familiar and yet, time and time again, I am floored by the changes and impact it makes through those choices. It’s honestly astounding.
And for this volume, that wait is paid off because of the unique choices that are made throughout it in dealing with Katsuki Bakugo, Deku’s childhood friend and rival who seems to be, easily, the most surface level and simple of the class of 1A, especially among Deku and his friends, and yet is continuously shown throughout here to have something much better and greater about him.
And while Katskui and his choices which ultimately subvert and turn on its head the trope that he seemed to so easily be fitting into throughout the previous nine volumes of content are the most interesting and engaging storyline of this book, he’s by far not the only one to shine in the volume. Deku, of course, being our main gets lots of great moments and we get to see him really develop his skills and instincts as a hero, but the entire gang of 1A classmates in this volume are really shown to grow from the characters we met back in the first volume of the story. They are reckless without completely losing sense and reason, they’re cautious without allowing written rules to inhibit them from what they know is right, and more than anything, they are all coming to recognize that something special in each other and especially in Deku and Katsuki which the two of them have been able to see all along. And it’s honestly all rather wonderful.
This volume also has more attention paid to the adult heroes and what they’re doing the serious responsibility they take in protecting and saving their charges. Which is a bit of superrealism sprinkled in this story that really elevates it above a lot of stories meant for young readers, especially shōnen.
The art’s always great, the story is not like anything else you’ll read East or West, and there honestly just aren’t characters like this you’ll see in other stories all with as much care and development as they have in My Hero Academia and that’s part of why it is so special and deserving of 5/5 stars.

Marvel’s Old Man Logan - Marvel Legacy Primer Pages
Robbie Thompson, Andrea Sorrentino

Of the freebie samplers, the ones that I tend to be the most interested in, at least for this week, are the ones that offer something additional to the things we’ve seen before. And in the case of Marvel’s “Legacy Primer Pages” marketing campaign, that’s exactly what the aim to do and actually achieve.
These are good little samples because not only are they uniquely written for this event and with this very intent behind them, but they are more importantly written by a writer I already really enjoy, Robbie Thompson, and all have different artists which not only tap into the style of the books being promoted bout also have a unique flare compared to the other “Legacy Primer Pages.”
In this case, I’ve never been particularly interested in the Old Man Logan books, as I’ve never been the biggest Mark Millar fan, but this is definitely a sample which gives me a good enough taste of what the universe is about and what Logan’s history is in it that I feel like I could readily pick up the next issue. I won’t. But I could. And that’s a delivery on the whole premise of the series.
Even if it’s super annoying that these things are 3 pages long.
A star earned for each page, I say.

Dark Horse’s Overwatch (2016-present) #13
Michael Chu, Ryan Benjamin, Anthony Washington

It’s been far too long since I read a good comic with Ryan Benjamin on art, it’s been sincerely missed in my usual comic appetite. As I’ve gone over quite a few times, the Overwatch comics Blizzard has been putting out has really gone the extra mile in helping someone like me who likes Overwatch but doesn’t really play the games to feel really immersed into the world they’ve created. And it’s in that way that I really enjoy reading these.
This whole issue seems a lot more plot driven than the rest of the comics, it seems to be in the present timeline, it’s showing the moves being made by the Talon operatives after the events we’ve seen unfold in previous issues and in the cinematics Blizzard has provided. And just overall it seems to have a much tighter schedule with a lot more direction than what has been expected.
It’s a little concerning to me that so many of the Talon operatives are heavily pulling from the more diverse characters in the franchise, but that’s not something I suspect rests squarely on the shoulders of this issue, obviously, but it is something I can look toward the writer of this issue, and the overall creative head of Overwatch’s story as a whole, Michael Chu. And with Chu writing it also makes sense why this feels a lot more plot driven.
All fo this aside, it’s a very nifty, very cool spy thriller from the perspective of the team of Bond villains, which has tight control of the characters and dialogue, and a wonderful use of a great artist whose style is fun yet very believable and action oriented.

Marvel’s Runaways (2017-present) #3
Rainbow Rowell, Kris Anka, Matthew Wilson

When you’re really analyzing and critiquing something, one of the things you have to ask yourself is what more could I ask of it? And I think when you’re torn about your personal, subjective impression of something and the quality of what you’re looking at, it’s important to ask that question and really analyze how much of a difference that can make.
For me, that question is particularly interesting in Runaways because while I’lm personally fairly new as a fan compared to some, I am still someone who has read through and fully submerged myself into the history of the characters up to this point and have a vested interest in seeing how they end up as characters and as a story outside of just “where are they now” more than just someone who was being newly introduced to these characters from this issue forward. And in that way, I can honestly say that Rainbow Rowell and Kris Anka have put together one of the most beautiful, slow paced, and yet completely rewarding personable comics I have read in a long time.
There’s not a lot of action, there’s an ongoing plot and a sense of danger and risk for our heroes, certainly, but at the end of the day the driving force of this plot and this narrative as a whole is and will remain the question “can they still be a family?”
And in that way, as much as my apprehensions remain, as much as my personal biases on where characters should go or should have gone, are completely overwhelmed by how much thought and care is put into every conversation, every action, every beautiful panel of this comic. And it is also in this way that I am just so blown way and impressed by the insight this comic has.
There are nitpicks, like I think that Karolina should have probably been more receptive and affectionate with Gert even through her surprise, but it’s hard for me to get nitpicky when I’m just so glad a book so much as exists, and can say it’s one comic that I look forward to immensely each and every month.
Definitely glad that this comic is continuing to earn every ounce of my support, 5/5.

DC’s Superman - Action Comics (2016-present) Vol. 4: The New World
Dan Jurgens, Patch Zircher, Ian Churchill

I remember back when I was reading every bit of comic book criticism and review that I could find a few years ago, one analysis that I found profoundly changed the way I evaluated comics and how I chose to consume them, was coming across an analysis of the culture around comics, and that was that for most committed comic book fans, which I most certainly qualified as, aren’t really focused looking at individual comics as narrative fiction, but like reading a newspaper, keeping peripherally aware of things that are happening within a given universe.
Now, the crux of that analysis was that readers who do this should stop and not feed the beast, opting instead for comics which are wholly good and further narrative and critical thinking.
But, I’ll be honest. I don’t really look to do that with comics either. I absolutely understand and support using comics as a means to relax, a comfort. A romp. And if you read certain comics like newspapers.... hell, you’re still reading more than like half the entire planet each week. I don’t read the parts of the newspaper I don’t have an interest or investment in, and I don’t read comics I’m not at least interested in as well.
I just drop them and stop buying them.
But there are hundreds of comics published every week in America alone, and to buy and keep up with all of them on an issue-by-issue basis, especially if the vast majority are “standard” or lower, doesn’t make sense to me. If a comic isn’t something I “have” to have each week, I move it to a trade wait and buy it that way. And I go over this now not because I want to convert everyone to my way of reading comics, but as an explanation for why certain comics I’m obviously enjoying are moved to this latter experience compared to their “peers”
For me, the events of Action Comics was something I was peripherally aware of through other comics and context clues, but wouldn’t read for myself until I got enough of a story to really sit down and read all together.
Which is a good thing, because as with the common theme of this week, long form arcs are super difficult to do well and so it’s more powerful to read a whole story together once it’s done. Action’s “The New World” story does that, but what it does even more than that is it reestablishes a context for the Super Family in the Rebirth universe.
The start of this issue, really the entirety of the first issue of this arc, is dedicated to showing us the new timeline with retconning the older Super Family and Jon’s birth and growth into the current DCU events. And this is one of those issues that by itself, if I had paid full price for what ended up being a wiki entry to the new universe, I probably would have been super ticked. But in a volume like this, with a whole new story set up by it and cause for moving forward, I find this to be a really good way of telling new readers and friends interested in Superman to read this volume and get a small history for context before moving forward.
And let me just say, as confusing and over the top as the Superman mythos has gotten in the past six years? This was a good call on the writers’ part here. Even if I think that first issue definitely suffers from exposition fatigue.
Now, unrelated to my scoring, I will say that this does upset me as a long time Superman fan because they bought back one of my absolute favorite characters from the previous universe, Chris Kent, but then completely undid everything lovable about him, made him a generic looking foil badguy to Jon’s Superboy, and for the time being seem to have no plans on having his heartbreaking and heartwarming story of finding an adopted family that loves and accepts him in Clark and Lois be revitalized and used to really meaningfully change the bad handling he received less than a year after his invention before. And it’s really disheartening and depressing on a fan’s behalf.
All that said, this is a solid comic and a pretty easy jumping on point for new and old readers alike. It cleans up a lot of the continuity confusion that has been brought on in the last two years for the Super Family, and gives us a lot of solid team ups within the family. So for me, this is a good 3/5 stars.

IDW’s Teenage Mutant Ninja Turtles/Ghostbusters II (2017) #2 (of 5)
Erik Burnham, Tom Waltz, Dan Schoening, Luis Antonio Delgado

Sometimes you enjoy a property so much that it becomes difficult to look at it with fresh eyes, and sometimes even worse that leads into a point where it takes a very special, a very extraordinary talent to come by and present you with something from that property that not only feels new and refreshing, but in many ways can almost feel like it’s a coming home of sorts.
When I read Burnham’s Ghostbusters or Waltz’s Teenage Mutant Ninja Turtles, I genuinely feel like it’s coming home to two of the teams that kind of helped me, like they helped a lot of kids, grow a real sense of self and exploration from a young age. There’s a line that’s sometimes difficult to explain to people when it comes to fiction but especially with comics and something as outlandish as the superhero and sci-fi genres, where the line is drawn between things that push the line for things to be ridiculously stupid into ridiculously amazing, but I think if there’s any comic that I would use it could very well be this issue.
The thing is, I mentioned before how I try to always think of a comic as being someone’s very first, and whether or not that would really provide them with anything that would entice a new reader to continue on. But I think there’s another perspective on that which can be just as relevant. And that would be the complicated question, if a comic has already found its audience, can it continue to reward and interest that audience?
And while I would always warn new readers when a comic doesn’t really meet the prior on average, I’m also comfortable with approaching a comic that knows its audience and, as a part of that audience, evaluating what I have gotten out of an issue. In that way, I feel like Ghostbusters/Teenage Mutant Ninja Turtles II is able to tap into something even decades-spanning properties like DC and Marvel are always juggling and struggling to maintain. It has an audience that Burnham and Waltz have personally been entertaining for almost a decade now, and so their main interests now are in rewarding those fans with the most payoff, the most development, and the most new spins on familiar faces that they can possibly give. And I think this is just another in a long list of examples of how they do that incredibly well.
This isn’t the only comic this week which is in the middle of a story, obviously, but I think of the available comics this one does the best job of doing something that I look at when examining an issue on its own. I ask myself, going into this issue from the last issue, what stakes are there and where (mentally or physically) are all the characters when the story starts, and do those things change by the end, and by how much. Sometimes, in a weak and drawn thin premise of a comic, those things don’t move the dial for the three or four middle issues that the story has, and it’s one of the reasons I am incredibly critical of long, 5+ issue storylines. They very rarely seem to fully payoff for what time and effort you invest in them by this measurement, especially in those middle issues.
Ghostbusters and Teenage Mutant Ninja Turtles are not those kinds of series, and their crossovers reflect that comfort that their teams bring to the table for these events. There’s an understanding of how much change is needed to reward the readers, and even if this is one of the incline issues taking us on our way to the climax very early in the story, it still manages to focus on the things we need to change within an issue.
In this case, that is character development and it’s something that these creators do fantastically well even with a huge ensemble cast. We have a lot of touching and vital moments for each of the characters, seeing the different groups bond and play off each other. It’s more than just the eggheads, the leaders, the comic reliefs, and the hotheads (respectively) together, it’s about taking those personalities and having them play off each other in a way that makes the characters reflect on themselves and the issues they’re not addressing in their personal arcs without being heavy handed.
Basically, if I could, I would teach a graduate level course on how these IDW comics understand how to make an ongoing comic’s individual issues maintain story structure while still contributing to an overall narrative.
It falls short of perfect, I still think it would be very difficult to tell someone new or fledgling in either property to pick it up, and I think that for a lot of people waiting each week, even it’s only a week, can be difficult with the price of comics these days, but it also feels so completely worth it for those of us already on the train.

DC’s Titans (2016-present) #17
Dan Abnett, Minkyu Jung, Mick Gray, Blond

A lot of people over the years have come along to debate me on my assertion that monthly comics should fix their publication method or write comic arcs to be four issues or shorter, and while that’s never been a position I deter from it’s one I am more than willing to hear other opinions are. There are good examples of stories that go on for longer.
But most of the time they don’t. And you end up with pretty run of the mill issues that take up the majority of the middle of the arc and more take away from the momentum of the storyline that had been building than anything else. This isn’t a complete condemnation of this arc, but it is a point I’m willing to stand on for this issue.
We start this issue with the exact same circumstances that we ended it in. Wally I is dead and Wally II is... around. Evil Future Donna reveals herself as the leader and the ultimate betrayer (more on that in a second). Mel and Gnarrk are still mind controlled. Other villains from the Titans’ pasts are also fighting for Donna.
Annnnd that’s it. This is the ultimate example of a filler issue that takes away from the momentum that had been building the entire time before all this happened. None of the characters are in a drastically different place, none of the personalities are changed, none of the circumstances are changed. t’s a lot of exposition and evil pondering that gives us... what is basically the cliffhanger from last issue -- is Donna evil? Will Wally live?
The stakes have not changed and thus this issue doesn’t add to the story. If anything, issues that pull stunts like this, basically pushing the pause button for another month, add to the reputation comics have that they have no real direction or conclusion to offer, that they just are endless cycles of the same game. And I’m saying that as a fan of not only comics, but of this series and this storyline. And it really doesn’t help its case that it all but flat out states a reference to “Who Is Donna Troy?”, a storyline that on one end of the spectrum could be a perfect example of a one-shot story that is self-contained and gives a change to the narrative and characterizations it touches... and on the other end of the spectrum is an example of convoluted retcons, disappointingly missed stakes, and a generally forgettable multipart “epic” that bit off more than it could chew. So we really could be barreling toward one side or the other.
For what it’s worth, I’m not at all saying that this is a terrible issue, but it’s a perfect example of why my skepticism toward comics which stretch stories to 6 issues or longer has grown as thick and impenetrable as it has. Issues of a comic series, like episodes of an ongoing TV show, are best served when you can either watch them on their own, or have demonstrably changed the stakes from the start of the issue/episode to the end, making it matter whether or not it is placed before or after the previous part of the story.
It also doesn’t help that this is the third-ish twist on the “Who Betrayed The Titans” thing they’ve had going for this story arc which has.. basically just been using as many twists as possible to try to combat the Information Age and how covers and solicits are released months in advance, making the element of surprise so questionable. Why else would they throw off the trail by having the traitor be Lilith and then maybe Dick and then maybe Roy and then, oh wait all the clues and lead up had been red herrings it’s Donna.... from the future... who turned evil because everyone died.... and now she wants to kill them earlier... Oh, comics.
On its own, this comic is a solid, standard issue, 3/5, but it’s going to contribute to the overall story arc feeling lax in pace and honestly stretched pretty thin in order to make it to that oh-so-desirable trade length.

IDW’s Transformers: First Strike (2017) #1
John Barber, Guido Guidi

It feels like over the past two years, as I’ve excitedly expanded my library for the IDW Transformers comics, I’ve had to deal with the ongoing struggle of following my favorite characters as they jump around between the various titles, and no two characters probably personify that more than Arcee and Kup right now. While I haven’t picked up Revolutionaries yet as I wait for the trade, I’ve enjoyed the general premise of the book from a distance and wondering if/when we’ll get more tie-ins to Sins of the Wreckers, which is where my love for Arcee and Kup has really been fostered.
This stand alone issue for First Strike is in itself fairly interesting. Even without a lot of the background from Revolutionaries or even the more recent arc of Optimus Prime, I followed the characters and relationships pretty easily. A good part of that is thanks to how John Barber’s consistent voice across all of the Hasbro line of properties has led to a real feeling of being able to follow the characters first and filling in for the storylines after. Which is a really good note for a multi-series shared universe like Transformers (and many other IDW properties) have become.
But that doesn’t entirely make it an easy read for newcomers jumping into the adventure. There is a lot with Blackrock and that whole nonsense (aka the main crux of the issue) that was really lost on me, and that cheapens the issue significantly when it goes for a “power of friendship” basically ending like this one does. It’s something that may very well easily be rewarding for more avid followers of the Revolutionaries storyline but not so much for my own limited perspective. That’s not necessarily a problem with the issue so much as it is for me.
What is a problem for the issue is the more inconsistent aspects of the art. Now, any Transformers fan is probably pre-packaged with a high tolerance for inconsistent proportions. That’s.... just part of the deal when you’re a Transformers fan. But even with that in mind, the changes characters would have with their sizes in this issue was really getting to me, especially with the humans serving as a consistent marker for height throughout.
I also felt that while the character art wasn’t bad, the tones and colors felt too bright and inconsistent with the surroundings, often not shifting shades even as the environment changed, which probably speaks more to the amount of time crunch here and not the actual quality of the digital colorists. But it is still pretty distracting even if you can’t exactly put your finger on why the characters seem to stand out so much to you as you read.
In general the issue is standard in a lot of ways, so I can’t say it’s the sort of jump on point that if you don’t love Transformers already you’ll be jumping over the moon for or something. It’s a good stand alone for a larger appreciative whole. And for me that’s a pretty solid, if just below exceptionalism, 3/5

Hey there! We finish up another pretty stellar week in comics with lots of stories and characters, and another pretty great time from yours truly. And if you enjoy these write-ups or anything else I do whether it be the Roundups, my Rambles, my personal creative projects, or you’re interested in my upcoming podcast, you can help contribute through donations to my Ko-Fi, Patreon, or PayPal. For as little as $1 per project, you make all of this possible.
You could also support me by going to my main blog, @renaroo, where I’ll soon be listing prices and more for art and writing commissions.

RenaRoo Ko-Fi

RenaRoo Patreon

RenaRoo PayPal
#Rena Roundups#Wednesday Spoilers#SPOILERS#Action Comics (2016 )#My Hero Academia (2014 )#DC Essentials Catalog 2018#Atomic Robo and the Spectre of Tomorrow#Overwatch (2016 )#Runaways (2017 )#Teenage Mutant Ninja Turtles/Ghostbusters II#Titans (2016 )#Batgirl and the Birds of Prey (2016 )#Justice League Day#Old Man Logan
4 notes
·
View notes
Text
When a Child Says She’s Trans
Claire is a 14-year-old girl with short auburn hair and a broad smile. She lives outside Philadelphia with her mother and father, both professional scientists. Claire can come across as an introvert, but she quickly opens up, and what seemed like shyness reveals itself to be quiet self-assuredness. Like many kids her age, she is a bit overscheduled. During the course of the evening I spent with Claire and her mother, Heather—these aren’t their real names—theater, guitar, and track tryouts all came up. We also discussed the fact that, until recently, she wasn’t certain she was a girl.
To hear more feature stories, see our full list or get the Audm iPhone app.
Sixth grade had been difficult for her. She’d struggled to make friends and experienced both anxiety and depression. “I didn’t have any self-confidence at all,” she told me. “I thought there was something wrong with me.” Claire, who was 12 at the time, also felt uncomfortable in her body in a way she couldn’t quite describe. She acknowledged that part of it had to do with puberty, but she felt it was more than the usual preteen woes. “At first, I started eating less,” she said, “but that didn’t really help.”
Around this time, Claire started watching YouTube videos made by transgender young people. She was particularly fascinated by MilesChronicles, the channel of Miles McKenna, a charismatic 22-year-old. His 1 million subscribers have followed along as he came out as a trans boy, went on testosterone, got a double mastectomy, and transformed into a happy, healthy young man. Claire had discovered the videos by accident, or rather by algorithm: They’d showed up in her “recommended” stream. They gave a name to Claire’s discomfort. She began to wonder whether she was transgender, meaning her internal gender identity didn’t match the sex she had been assigned at birth. “Maybe the reason I’m uncomfortable with my body is I’m supposed to be a guy,” she thought at the time.
Claire found in MilesChronicles and similar YouTube videos a clear solution to her unhappiness. “I just wanted to stop feeling bad, so I was like, I should just transition,” she said. In Claire’s case, the first step would be gaining access to drugs that would halt puberty; next, she would start taking testosterone to develop male secondary sex characteristics. “I thought that that was what made you feel better,” she told me.
In Claire’s mind, the plan was concrete, though neither Heather nor her husband, Mike, knew about any of it. Claire initially kept her feelings from her parents, researching steps she could take toward transitioning that wouldn’t require medical interventions, or her parents’ approval. She looked into ways to make her voice sound deeper and into binders to hide her breasts. But one day in August 2016, Mike asked her why she’d seemed so sad lately. She explained to him that she thought she was a boy.
This began what Heather recalls as a complicated time in her and her husband’s relationship with their daughter. They told Claire that they loved and supported her; they thanked her for telling them what she was feeling. But they stopped short of encouraging her to transition. “We let her completely explore this on her own,” Heather told me.
To Claire’s parents, her anguish seemed to come out of nowhere. Her childhood had been free of gender dysphoria—the clinical term for experiencing a powerful sense of disconnection from your assigned sex. They were concerned that what their daughter had self-diagnosed as dysphoria was simply the travails of puberty.
As Claire passed into her teen years, she continued to struggle with mental-health problems. Her parents found her a therapist, and while that therapist worked on Claire’s depression and anxiety—she was waking up several times a night to make sure her alarm clock was set correctly—she didn’t feel qualified to help her patient with gender dysphoria. The therapist referred the family to some nearby gender-identity clinics that offered transition services for young people.
Claire’s parents were wary of starting that process. Heather, who has a doctorate in pharmacology, had begun researching youth gender dysphoria for herself. She hoped to better understand why Claire was feeling this way and what she and Mike could do to help. Heather concluded that Claire met the clinical criteria for gender dysphoria in the DSM-5, the American Psychiatric Association’s diagnostic manual. Among other indications, her daughter clearly didn’t feel like a girl, clearly wanted a boy’s body, and was deeply distressed by these feelings. But Heather questioned whether these criteria, or much of the information she found online, told the whole story. “Psychologists know that adolescence is fraught with uncertainty and identity searching, and this isn’t even acknowledged,” she told me.
Heather said most of the resources she found for parents of a gender-dysphoric child told her that if her daughter said she was trans, she was trans. If her daughter said she needed hormones, Heather’s responsibility was to help her get on hormones. The most important thing she could do was affirm her daughter, which Heather and Mike interpreted as meaning they should agree with her declarations that she was transgender. Even if they weren’t so certain.
As Heather was searching for answers, Claire’s belief that she should transition was growing stronger. For months, she had been insistent that she wanted both testosterone and “top surgery”—a double mastectomy. She repeatedly asked her parents to find her doctors who could get her started on a path to physical transition. Heather and Mike bought time by telling her they were looking but hadn’t been able to find anyone yet. “We also took her kayaking, played more board games with her and watched more TV with her, and took other short family trips,” Heather recalled. “We also took away her ability to search online but gave her Instagram as a consolation.” They told her they realized that she was in pain, but they also felt, based on what they’d learned in their research, that it was possible her feelings about her gender would change over time. They asked her to start keeping a journal, hoping it would help her explore those feelings.
Claire humored her parents, even as her frustration with them mounted. Eventually, though, something shifted. In a journal entry Claire wrote last November, she traced her realization that she wasn’t a boy to one key moment. Looking in the mirror at a time when she was trying to present in a very male way—at “my baggy, uncomfortable clothes; my damaged, short hair; and my depressed-looking face”—she found that “it didn’t make me feel any better. I was still miserable, and I still hated myself.” From there, her distress gradually began to lift. “It was kind of sudden when I thought: You know, maybe this isn’t the right answer—maybe it’s something else,” Claire told me. “But it took a while to actually set in that yes, I was definitely a girl.”
Claire believes that her feeling that she was a boy stemmed from rigid views of gender roles that she had internalized. “I think I really had it set in stone what a guy was supposed to be like and what a girl was supposed to be like. I thought that if you didn’t follow the stereotypes of a girl, you were a guy, and if you didn’t follow the stereotypes of a guy, you were a girl.” She hadn’t seen herself in the other girls in her middle-school class, who were breaking into cliques and growing more gossipy. As she got a bit older, she found girls who shared her interests, and started to feel at home in her body.
Heather thinks that if she and Mike had heeded the information they found online, Claire would have started a physical transition and regretted it later. These days, Claire is a generally happy teenager whose mental-health issues have improved markedly. She still admires people, like Miles McKenna, who benefited from transitioning. But she’s come to realize that’s just not who she happens to be.
The number of self-identifying trans people in the United States is on the rise. In June 2016, the Williams Institute at the UCLA School of Law estimated that 1.4 million adults in the U.S. identify as transgender, a near-doubling of an estimate from about a decade earlier. As of 2017, according to the institute, about 150,000 teenagers ages 13 to 17 identified as trans. The number of young people seeking clinical services appears to be growing as well. A major clinic in the United Kingdom saw a more than 300 percent increase in new referrals over the past three years. In the U.S., where youth gender clinics are somewhat newer—40 or so are scattered across the country—solid numbers are harder to come by. Anecdotally, though, clinicians are reporting large upticks in new referrals, and waiting lists can stretch to five months or longer.
The current era of gender-identity awareness has undoubtedly made life easier for many young people who feel constricted by the sometimes-oppressive nature of gender expectations. A rich new language has taken root, granting kids who might have felt alone or excluded the words they need to describe their experiences. And the advent of the internet has allowed teenagers, even ones in parts of the country where acceptance of gender nonconformity continues to come far too slowly, to find others like them.
But when it comes to the question of physical interventions, this era has also brought fraught new challenges to many parents. Where is the line between not “feeling like” a girl because society makes it difficult to be a girl and needing hormones to alleviate dysphoria that otherwise won’t go away? How can parents tell? How can they help their children gain access to the support and medical help they might need, while also keeping in mind that adolescence is, by definition, a time of fevered identity exploration?
Maciek Jasik
There is no shortage of information available for parents trying to navigate this difficult terrain. If you read the bible of medical and psychiatric care for transgender people—the Standards of Care issued by the World Professional Association for Transgender Health (Wpath)—you’ll find an 11-page section called “Assessment and Treatment of Children and Adolescents With Gender Dysphoria.” It states that while some teenagers should go on hormones, that decision should be made with deliberation: “Before any physical interventions are considered for adolescents, extensive exploration of psychological, family, and social issues should be undertaken.” The American Psychological Association’s guidelines sound a similar note, explaining the benefits of hormones but also noting that “adolescents can become intensely focused on their immediate desires.” It goes on: “This intense focus on immediate needs may create challenges in assuring that adolescents are cognitively and emotionally able to make life-altering decisions.”
The leading professional organizations offer this guidance. But some clinicians are moving toward a faster process. And other resources, including those produced by major LGBTQ organizations, place the emphasis on acceptance rather than inquiry. The Human Rights Campaign’s “Transgender Children & Youth: Understanding the Basics” web page, for example, encourages parents to seek the guidance of a gender specialist. It also asserts that “being transgender is not a phase, and trying to dismiss it as such can be harmful during a time when your child most needs support and validation.” Similarly, parents who consult the pages tagged “transgender youth” on glaad’s site will find many articles about supporting young people who come out as trans but little about the complicated diagnostic and developmental questions faced by the parents of a gender-exploring child.
HRC, glaad, and like-minded advocacy groups emphasize the acceptance of trans kids for understandable reasons: For far too long, parents, as well as clinicians, denied the possibility that trans kids and teens even existed, let alone that they should be allowed to transition. Many such organizations are primarily concerned with raising awareness and correcting still-common misconceptions.
A similar motive seems to animate much of the media coverage of transgender young people. Two genres of coverage have emerged. Dating back at least to the 1993 murder of the Nebraska 21-year-old Brandon Teena, which inspired a documentary as well as the film Boys Don’t Cry, a steady stream of horror stories has centered on bullying, physical assault, and suicide—real risks that transgender and gender-nonconforming (TGNC) young people still face.
More recently, a wave of success stories has appeared. In many of these accounts, kids are lost, confused, and frustrated right up until the moment they are allowed to grow their hair out and adopt a new name, at which point they finally become their true self. Take, for example, a Parents.com article in which a mother, writing pseudonymously, explains that she struggled with her child’s gender-identity issues for years, until finally turning to a therapist, who, after a 20-minute evaluation, pronounced the child trans. Suddenly, everything clicked into place. The mother writes: “I looked at the child sitting between my husband and me, the child who was smiling, who appeared so happy, who looked as if someone finally saw him or her the way she or he saw him or herself.” In a National Geographic special issue on gender, the writer Robin Marantz Henig recounts the story of a mother who let her 4-year-old, assigned male at birth, choose a girl’s name, start using female pronouns, and attend preschool as a girl. “Almost instantly the gloom lifted,” Henig writes.
Accounts of successful transitions can help families envision a happy outcome for a suffering child. And some young people clearly experience something like what these caterpillar-to-butterfly narratives depict. They have persistent, intense gender dysphoria from a very young age, and transitioning alleviates it. “Some kids don’t waver” in their gender identity, Nate Sharon, a psychiatrist who oversaw a gender clinic in New Mexico for two and a half years, and who is himself trans, told me when we spoke in 2016. “I’m seeing an 11-year-old who at age 2 went up to his mom and said, ‘When am I going to start growing my penis? Where’s my penis?’ At 2.”
But these stories tend to elide the complexities of being a TGNC young person, or the parent of one. Some families will find a series of forking paths, and won’t always know which direction is best. Like Claire’s parents, they may be convinced that their child is in pain, but also concerned that physical transition is not the solution, at least not for a young person still in the throes of adolescence.
We are still in the earliest stages of understanding how physical transitioning affects dysphoric young people. While the specifics depend on your child’s age, and can vary from case to case, the transition process for a persistently dysphoric child typically looks something like the following. First, allow your child to transition socially: to adopt the pronouns and style of dress of their authentic gender, and to change their name if they wish. As your child approaches adolescence, get them puberty-blocking drugs, because developing the secondary sex characteristics of their assigned sex could exacerbate their gender dysphoria. When they reach their teen years, help them gain access to the cross-sex hormones that will allow them to develop secondary sex characteristics in line with their gender identity. (Until recently, hormones were typically not prescribed until age 16; it’s now more common for 15- and 14-year-olds, and sometimes even younger kids, to begin hormone therapy.)
In the United States, avoiding puberty became an option only a little more than a decade ago, so researchers have just begun tracking the kids engaged in this process, and we don’t yet have comprehensive data about their long-term outcomes. Most of the data we do have involve kids who socially transitioned at an early age, but who hadn’t yet physically transitioned. The information comes from a University of Washington researcher named Kristina Olson. Olson is the founder of the TransYouth Project, which is following a cohort of about 300 children for 20 years—the longest such longitudinal study based in the U.S. The kids she is tracking appear to be doing well—they don’t seem all that different, in terms of their mental health and general happiness, from a control group of cisgender kids (that is, kids who identify with the sex they were assigned at birth).
At the prestigious Center of Expertise on Gender Dysphoria, at Vrije Universiteit University Medical Center, in Amsterdam—often referred to simply as “the Dutch clinic”—an older cohort of kids who went through the puberty-blockers-and-cross-sex-hormones protocol was also found to be doing well: “Gender dysphoria had resolved,” according to a study of the group published in 2014 in Pediatrics. “Psychological functioning had steadily improved, and well-being was comparable to same-age peers.”
These early results, while promising, can tell us only so much. Olson’s findings come from a group of trans kids whose parents are relatively wealthy and are active in trans-support communities; they volunteered their children for the study. There are limits to how much we can extrapolate from the Dutch study as well: That group went through a comprehensive diagnostic process prior to transitioning, which included continuous access to mental-health care at a top-tier gender clinic—a process unfortunately not available to every young person who transitions.
Among the issues yet to be addressed by long-term studies are the effects of medications on young people. As Thomas Steensma, a psychologist and researcher at the Dutch clinic and a co-author of that study, explained to me, data about the potential risks of putting young people on puberty blockers are scarce. He would like to see further research into the possible effects of blockers on bone and brain development. (The potential long-term risks of cross-sex hormones aren’t well known, but are likely modest, according to Joshua Safer, one of the authors of the Endocrine Society’s “Clinical Practice Guideline” for treatment of gender dysphoria.)
Meanwhile, fundamental questions about gender dysphoria remain unanswered. Researchers still don’t know what causes it—gender identity is generally viewed as a complicated weave of biological, psychological, and sociocultural factors. In some cases, gender dysphoria may interact with mental-health conditions such as depression and anxiety, but there’s little agreement about how or why. Trauma, particularly sexual trauma, can contribute to or exacerbate dysphoria in some patients, but again, no one yet knows exactly why.
To reiterate: For many of the young people in the early studies, transitioning—socially for children, physically for adolescents and young adults—appears to have greatly alleviated their dysphoria. But it’s not the answer for everyone. Some kids are dysphoric from a very young age, but in time become comfortable with their body. Some develop dysphoria around the same time they enter puberty, but their suffering is temporary. Others end up identifying as nonbinary—that is, neither male nor female.
Ignoring the diversity of these experiences and focusing only on those who were effectively “born in the wrong body” could cause harm. That is the argument of a small but vocal group of men and women who have transitioned, only to return to their assigned sex. Many of these so-called detransitioners argue that their dysphoria was caused not by a deep-seated mismatch between their gender identity and their body but rather by mental-health problems, trauma, societal misogyny, or some combination of these and other factors. They say they were nudged toward the physical interventions of hormones or surgery by peer pressure or by clinicians who overlooked other potential explanations for their distress.
Some of these interventions are irreversible. People respond differently to cross-sex hormones, but changes in vocal pitch, body hair, and other physical characteristics, such as the development of breast tissue, can become permanent. Kids who go on puberty blockers and then on cross-sex hormones may not be able to have biological children. Surgical interventions can sometimes be reversed with further surgeries, but often with disappointing results.
The concerns of the detransitioners are echoed by a number of clinicians who work in this field, most of whom are psychologists and psychiatrists. They very much support so-called affirming care, which entails accepting and exploring a child’s statements about their gender identity in a compassionate manner. But they worry that, in an otherwise laudable effort to get TGNC young people the care they need, some members of their field are ignoring the complexity, and fluidity, of gender-identity development in young people. These colleagues are approving teenagers for hormone therapy, or even top surgery, without fully examining their mental health or the social and family influences that could be shaping their nascent sense of their gender identity.
That’s too narrow a definition of affirming care, in the view of many leading clinicians. “Affirming care does not privilege any one outcome when it comes to gender identity, but instead aims to allow exploration of gender without judgment and with a clear understanding of the risks, benefits, and alternatives to any choice along the way,” Aron Janssen, the clinical director of the Gender and Sexuality Service at Hassenfeld Children’s Hospital, in New York, told me. “Many people misinterpret affirming care as proceeding to social and medical transition in all cases without delay, but the reality is much more complex.”
To make sense of this complex reality—and ensure the best outcome for all gender-exploring kids—parents need accurate, nuanced information about what gender dysphoria is and about the many blank spots in our current knowledge. They don’t always get it.
For gender-dysphoric people, physical transition can be life enhancing, even lifesaving. While representative long-term data on the well-being of trans adults have yet to emerge, the evidence that does exist—as well as the sheer heft of personal accounts from trans people and from the clinicians who help them transition—is overwhelming. For many if not most unwaveringly gender-dysphoric people, hormones work. Surgery works. That’s reflected in studies that consistently show low regret rates for the least-reversible physical procedures to address gender dysphoria. One 2012 review of past studies, for example, found that sex-reassignment surgery “is an effective treatment for [gender dysphoria] and the only treatment that has been evaluated empirically with large clinical case series.” A study on “bottom surgery,” or surgery designed to construct a penis or vagina, found that from 1972 to 2015, “only 0.6 percent of transwomen and 0.3 percent of transmen who underwent [these procedures] were identified as experiencing regret.”
Those of us who have never suffered from gender dysphoria can have a hard time appreciating what’s at stake. Rebecca Kling, an educator at the National Center for Transgender Equality, in Washington, D.C., told me that before she transitioned she felt as if she were constantly carrying around a backpack full of rocks. “That is going to make everything in my life harder, and in many cases is going to make things impossible,” she said. “Of course being able to remove that heavy burden has added comfort and stability in my sense of myself and my body.” Other trans people have offered similar descriptions of gender dysphoria—a weight, a buzzing, an unavoidable source of rumination and worry. Hormones and surgery grant transgender people profound relief.
Historically, they have been denied access to that relief. Christine Jorgensen, the first American to become widely known for transitioning through hormones and surgery, in the 1950s, had to go to Denmark for her care. The trans historian Genny Beemyn notes that Jorgensen’s doctor “received more than 1,100 letters from transsexual people, many of whom sought to be his patients,” in the months after Jorgensen was treated. As a result of the requests, “the Danish government banned such procedures for non-citizens. In the United States, many physicians simply dismissed the rapidly growing number of individuals seeking gender-affirming surgeries as being mentally ill.”
Today, the situation in the U.S. has improved, but the lack of access to transition services continues to be a problem. Whether trans people in this country can access treatments such as hormones and surgery depends on a variety of factors, ranging from where they live to what their health insurance will cover (if they have any) to their ability to navigate piles of paperwork. Erica Anderson, a trans woman and clinical psychologist who works at the Child and Adolescent Gender Center, at UC San Francisco’s Benioff Children’s Hospital, had no luck when she tried to get hormones from an endocrinologist in Philadelphia just a decade ago. “Even I, with my education and resources, was denied care and access,” she told me. “The endocrinologist simply said, ‘I don’t do that.’ I offered to provide her the guidelines from her own Endocrine Society,” Anderson said. “She refused and wouldn’t even look me in the eye. No referral or offer to help. She sent me away with nothing, feeling like I was an undesirable.”
Many trans people have stories like Anderson’s. For this reason, among others, trans communities can be skeptical of those who focus on negative transition outcomes. They have long dealt with “professionals who seem uncomfortable giving trans people the go-ahead to transition at all,” Zinnia Jones, a trans woman who runs the website GenderAnalysis, told me in an email. They have also faced “unnecessarily protracted timelines for accessing care, a lack of understanding or excess skepticism of our identities from clinicians, and so on.”
Groups like Wpath, the primary organization for psychologists, psychiatrists, endocrinologists, surgeons, and others who work with TGNC clients, have attempted to reverse this neglect in recent years. A growing number of adult gender clinics follow “informed consent” protocols, built on the philosophy that trans adults, once informed of the potential benefits and risks of medical procedures, have a right to make their own decisions about their body and shouldn’t have their need for services questioned by mental-health and medical professionals.
This shift is seen by many trans people and advocates as an important course correction after decades of gatekeeping—aloof professionals telling trans people they couldn’t get hormones or surgery, because they weren’t really trans, or hadn’t been living as a trans person long enough, or were too mentally ill.
For gender-questioning children and teens, the landscape is different. A minor’s legal guardian almost always has to provide consent prior to a medical procedure, whether it’s a tonsillectomy or top surgery. Wpath and other organizations that provide guidance for transitioning young people call for thorough assessments of patients before they start taking blockers or hormones.
This caution comes from the concerns inherent in working with young people. Adolescents change significantly and rapidly; they may view themselves and their place in the world differently at 15 than they did at 12. “You’ve got the onset of puberty right around the age where they develop the concept of abstract thinking,” said Nate Sharon, the New Mexico psychiatrist. “So they may start to conceptualize gender concepts in a much richer, broader manner than previously—and then maybe puberty blockers or cross-sex hormones aren’t for them.” That was true for Claire: A shift in her understanding of the nature of gender led her to realize that transitioning was not the answer for her.
For younger children, gender identity is an even trickier concept. In one experiment, for example, many 3-to-5-year-olds thought that if a boy put on a dress, he became a girl. Gender clinicians sometimes encounter young children who believe they are, or want to be, another gender because of their dress or play preferences—I like rough-and-tumble play, so I must be a boy—but who don’t meet the criteria for gender dysphoria.
In the past, therapists and doctors interpreted the fluidity of gender identity among children as license to put gender-bending kids into the “right” box by encouraging—or forcing—them to play with the “right” toys and dress in the “right” clothes. Until about five years ago, according to one clinician’s estimate, social transition was often frowned upon. For decades, trans-ness was sometimes tolerated in adults as a last-ditch outcome, but in young people it was more often seen as something to be drummed out rather than explored or accepted. So-called reparative therapy has harmed and humiliated trans and gender-nonconforming children. In her book Gender Born, Gender Made, Diane Ehrensaft, the director of mental health at UC San Francisco’s Child and Adolescent Gender Center, writes that victims of these practices “become listless or agitated, long for their taken-away favorite toys and clothes, and even literally go into hiding in closets to continue playing with the verboten toys or wearing the forbidden clothes.” Such therapy is now viewed as unethical.
These days, mainstream youth-gender clinicians practice affirming care instead. They listen to their young patients, take their statements about their gender seriously, and often help facilitate social and physical transition. Affirming care has quickly become a professional imperative: Don’t question who your clients are—let them tell you who they are, and accept their identity in a nurturing, encouraging manner.
The affirming approach is far more humane than older ones, but it conflicts, at least a little, with what we know about gender-identity fluidity in young people. What does it mean to be affirming while acknowledging that kids and teenagers can have an understanding of gender that changes over a short span? What does it mean to be affirming while acknowledging that feelings of gender dysphoria can be exacerbated by mental-health difficulties, trauma, or a combination of the two?
Clinicians are still wrestling with how to define affirming care, and how to balance affirmation and caution when treating adolescents. “I don’t want to be a gatekeeper,” Dianne Berg, a co-director of the National Center for Gender Spectrum Health, at the University of Minnesota, told me. “But I also worry that in opening the gates, we’re going to have more adolescents that don’t engage in the reflective work needed in order to make sound decisions, and there might end up being more people when they are older that are like, Oh, hmm—now I am not sure about this.”
When Max Robinson was 17, getting a double mastectomy made perfect sense to her. In fact, it felt like her only option—like a miraculous, lifesaving procedure. Though she had a woman’s body, she was really a man. Surgery would finally offer her a chance to be herself.
I met Max, now 22, in an airy café in the quiet southern-Oregon town where she lives. She was wearing a T‑shirt with a flannel button-down over it. On her head, a gray winter cap; at her feet, a shaggy white service dog. By the time we met, we’d spoken on the phone and exchanged a number of emails, and she had told me her story—one that suggests the complexity of gender-identity development.
Max recalled that as early as age 5, she didn’t enjoy being treated like a girl. “I questioned my teachers about why I had to make an angel instead of a Santa for a Christmas craft, or why the girls’ bathroom pass had ribbons instead of soccer balls, when I played soccer and knew lots of other girls in our class who loved soccer,” she said.
She grew up a happy tomboy—until puberty. “People expect you to grow out of it” at that age, she explained, “and people start getting uncomfortable when you don’t.” Worse, “the way people treated me started getting increasingly sexualized.” She remembered one boy who, when she was 12, kept asking her to pick up his pencil so he could look down her shirt.
“I started dissociating from my body a lot more when I started going through puberty,” Max said. Her discomfort grew more internalized—less a frustration with how the world treated women and more a sense that the problem lay in her own body. She came to believe that being a woman was “something I had to control and fix.” She had tried various ways of making her discomfort abate—in seventh grade, she vacillated between “dressing like a 12-year-old boy” and wearing revealing, low-cut outfits, attempts to defy and accede to the demands the world was making of her body. But nothing could banish her feeling that womanhood wasn’t for her. She had more bad experiences with men, too: When she was 13, she had sex with an older man she was seeing; at the time, it felt consensual, but she has since realized that a 13-year-old can’t consent to sex with an 18-year-old. At 14, she witnessed a friend get molested by an adult man at a church slumber party. Around this time, Max was diagnosed with depression and generalized anxiety disorder.
In ninth grade, Max first encountered the concept of being transgender when she watched an episode of The Tyra Banks Show in which Buck Angel, a trans porn star, talked about his transition. It opened up a new world of online gender-identity exploration. She gradually decided that she needed to transition.
Max’s parents were skeptical at first but eventually came around, signing her up for sessions with a therapist who specialized in gender-identity issues. She recalled that the specialist was very open to putting her on a track toward transition, though he suggested that her discomfort could have other sources as well. Max, however, was certain that transitioning was the answer. She told me that she “refused to talk about anything other than transition.”
When Max was 16, her therapist wrote her a referral to see an endocrinologist who could help her begin the process of physical transition by prescribing male hormones. The endocrinologist was skeptical, Max said. “I think what she was seeing was a lesbian teenager,” not a trans one. At the time, though, Max interpreted the doctor’s reluctance as her “being ignorant, as her trying to hurt me.” Armed with the referral from her therapist, Max got the endocrinologist to prescribe the treatment she sought.
Max started taking testosterone. She experienced some side effects—hot flashes, memory issues—but the hormones also provided real relief. Her plan all along had been to get top surgery, too, and the initially promising effects of the hormones helped persuade her to continue on this path. When she was 17, Max, who was still dealing with major mental-health issues, was scheduled for surgery.
Because Max had parental approval, the surgeon she saw agreed to operate on her despite the fact that she was still a minor. (It’s become more common for surgeons to perform top surgeries on teenagers as young as 16 if they have parental approval. The medical norms are more conservative when it comes to bottom surgeries; Wpath says they should be performed only on adults who have been living in their gender role for at least one year.) Max went into the surgery optimistic. “I was convinced it would solve a lot of my problems,” she said, “and I hadn’t accurately named a lot of those problems yet.”
Max Robinson went on cross-sex hormones when she was 16 and had a double mastectomy when she was 17. Now 22, she has detransitioned and identifies as a woman. (Chloe Aftel)
Max was initially happy with the results of her physical transformation. Before surgery, she wasn’t able to fully pass as male. After surgery, between her newly masculinized chest and the facial hair she was able to grow thanks to the hormones, she felt like she had left behind the sex she had been assigned at birth. “It felt like an accomplishment to be seen the way I wanted to be seen,” she told me.
But that feeling didn’t last. After her surgery, Max moved from her native California to Portland and threw herself into the trans scene there. It wasn’t a happy home. The clarity of identity she was seeking—and that she’d felt, temporarily, after starting hormones and undergoing surgery—never fully set in. Her discomfort didn’t go away.
Today, Max identifies as a woman. She believes that she misinterpreted her sexual orientation, as well as the effects of the misogyny and trauma she had experienced as a young person, as being about gender identity. Because of the hormone therapy, she still has facial hair and is frequently mistaken for male as a result, but she has learned to live with this: “My sense of self isn’t entirely dependent on how other people see me.”
Max is one of what appears to be a growing number of people who believe they were failed by the therapists and physicians they went to for help with their gender dysphoria. While their individual stories differ, they tend to touch on similar themes. Most began transitioning during adolescence or early adulthood. Many were on hormones for extended periods of time, causing permanent changes to their voice, appearance, or both. Some, like Max, also had surgery.
Many detransitioners feel that during the process leading up to their transition, well-meaning clinicians left unexplored their overlapping mental-health troubles or past traumas. Though Max’s therapist had tried to work on other issues with her, Max now believes she was encouraged to rush into physical transition by clinicians operating within a framework that saw it as the only way someone like her could experience relief. Despite the fact that she was a minor for much of the process, she says, her doctors more or less did as she told them.
Over the past couple of years, the detransitioner movement has become more visible. Last fall, Max told her story to The Economist’s magazine of culture and ideas, 1843. Detransitioners who previously blogged pseudonymously, largely on Tumblr, have begun writing under their real names, as well as speaking on camera in YouTube videos.
Cari Stella is the author of a blog called Guide on Raging Stars. Stella, now 24, socially transitioned at 15, started hormones at 17, got a double mastectomy at 20, and detransitioned at 22. “I’m a real-live 22-year-old woman with a scarred chest and a broken voice and a 5 o’clock shadow because I couldn’t face the idea of growing up to be a woman,” she said in a video posted in August 2016. “I was not a very emotionally stable teenager,” she told me when we spoke. Transitioning offered a “level of control over how I was being perceived.”
Carey Callahan is a 36-year-old woman living in Ohio who detransitioned after identifying as trans for four years and spending nine months on male hormones. She previously blogged under the pseudonym Maria Catt, but “came out” in a YouTube video in July 2016. She now serves as something of an older sister to a network of female, mostly younger detransitioners, about 70 of whom she has met in person; she told me she has corresponded online with an additional 300. (The detransitioners who have spoken out thus far are mostly people who were assigned female at birth. Traditionally, most new arrivals at youth gender clinics were assigned male; today, many clinics are reporting that new patients are mostly assigned female. There is no consensus explanation for the change.)
I met Carey in Columbus in March. She told me that her decision to detransition grew out of her experience working at a trans clinic in San Francisco in 2014 and 2015. “People had said often to me that when you transition, your gender dysphoria gets worse before it gets better,” she told me. “But I saw and knew so many people who were cutting themselves, starving themselves, never leaving their apartments. That made me doubt the narrative that if you make it all the way to medical transition, then it’s probably going to work out well for you.”
Carey Callahan serves as something of an older sister to a group of women who, like her, have detransitioned. (Matt Eich)
Carey said she met people who appeared to be grappling with severe trauma and mental illness, but were fixated on their next transition milestone, convinced that was the moment when they would get better. “I knew a lot of people committed to that narrative who didn’t seem to be doing well,” she recalled. Carey’s time at the clinic made her realize that testosterone hadn’t made her feel better in a sustained way either. She detransitioned, moved to Ohio, and is now calling for a more careful approach to treating gender dysphoria than what many detransitioners say they experienced themselves.
In part, that would mean clinicians adhering to guidelines like Wpath’s Standards of Care, which are nonbinding. “When I look at what the SOC describes, and then I look at my own experience and my friends’ experiences of pursuing hormones and surgery, there’s hardly any overlap between the directives of the SOC and the reality of care patients get,” Carey told me. “We didn’t discuss all the implications of medical intervention—psychological, social, physical, sexual, occupational, financial, and legal—which the SOC directs the mental-health professional to discuss. What the SOC describes and the care people get before getting cleared for hormones and surgery are miles apart.”
Detransitioners, understandably, elicit suspicion from the trans community. Imagine being a trans person who endured a bruising fight to prove to your psychiatrist and endocrinologist that you are trans, in order to gain access to hormones that greatly improve your quality of life, that relieve suffering. You might view with skepticism—at the very least—a group calling for more gatekeeping. Conservative media outlets, for their part, often seize on detransition narratives to push the idea that being trans is some sort of liberal invention. “How Carey Was Set Free From Transgenderism” was the conservative website LifeSiteNews’ disingenuous take on Carey’s story.
Video: Reversing a Gender Transition
youtube
No one knows how common detransitioning is. A frequently cited statistic—that only 2.2 percent of people who physically transition later regret it—doesn’t paint a complete picture. It comes from a study, conducted in Sweden, that examined only those people who had undergone sex-reassignment surgery and legally changed their gender, then applied to change their gender back—a standard that, Carey pointed out, would have excluded her and most of the detransitioners she knows.
It stands to reason that as any medical procedure becomes more readily available, a higher number of people will regret having it. Why focus on detransitioners, when no one even knows whether their experiences are all that common? One answer is that clinicians who have logged thousands of hours working with transgender and gender-nonconforming young people are raising the same concerns.
When it comes to helping TGNC young people gain access to physical interventions, few American clinicians possess the bona fides of the psychologist Laura Edwards-Leeper. A decade ago, when she was working at Boston Children’s Hospital, she visited the Dutch clinic to learn the puberty-blocking protocol pioneered there. She helped bring that protocol back to Boston, where she worked with the first-ever group of American kids to go through that process.
Today, Edwards-Leeper oversees a collaboration between Pacific University and Oregon’s Transgender Clinic, within the nonprofit Legacy Health system. At Pacific, she is training clinical-psychology doctoral students to conduct “readiness assessments” for young people seeking physical-transition services.
In February, I visited one of her classes at Pacific, just outside Portland. For an hour, she let me pepper her students with questions about their experiences as clinicians-in-training in what is essentially a brand-new field. When the subject of detransitioners came up, Edwards-Leeper chimed in. “I’ve been predicting this for, I don’t know, the last five or more years,” she said. “I anticipate there being more and more and more, because there are so many youth who are now getting services with very limited mental-health assessment and sometimes no mental-health assessment. It’s inevitable, I think.”
Laura Edwards-Leeper, a clinician at Pacific University and Oregon’s Transgender Clinic. She brought the puberty-blocking transition protocol pioneered by the Dutch to the U.S. (Matt Eich)
Edwards-Leeper believes that comprehensive assessments are crucial to achieving good outcomes for TGNC young people, especially those seeking physical interventions, in part because some kids who think they are trans at one point in time will not feel that way later on. This is a controversial subject in some corners of the trans community. A small group of studies has been interpreted as showing that the majority of children who experience gender dysphoria eventually stop experiencing it and come to identify as cisgender adults. (In these studies, children who suffer intense dysphoria over an extended period of time, especially into adolescence, are more likely to identify as trans in the long run.)
This so-called desistance research has been attacked on various methodological grounds. The most-credible critiques center on the claim that some kids who were merely gender nonconforming—that is, they preferred stereotypically cross-sex activities or styles of dress—but not dysphoric may have been counted as desisters because the studies relied on outdated diagnostic criteria, artificially pushing the percentage upward. (The terms detransition and desist are used in different ways by different people. In this article, I am drawing this distinction: Detransitioners are people who undergo social or physical transitions and later reverse them; desisters are people who stop experiencing gender dysphoria without having fully transitioned socially or physically.)
The desistance rate for accurately diagnosed dysphoric kids is probably lower than some of the contested studies suggest; a small number of merely gender-nonconforming kids may indeed have been wrongly swept into even some of the most recent studies, which didn’t use the most up-to-date criteria, from the DSM-5. And there remains a paucity of big, rigorous studies that might deliver a more reliable figure.
Within a subset of trans advocacy, however, desistance isn’t viewed as a phenomenon we’ve yet to fully understand and quantify but rather as a myth to be dispelled. Those who raise the subject of desistance are often believed to have nefarious motives—the liberal outlet ThinkProgress, for example, referred to desistance research as “the pernicious junk science stalking trans kids,” and a subgenre of articles and blog posts attempts to debunk “the desistance myth.” But the evidence that desistance occurs is overwhelming. The American Psychological Association, the Substance Abuse and Mental Health Services Administration, the Endocrine Society, and Wpath all recognize that desistance occurs. I didn’t speak with a single clinician who believes otherwise. “I’ve seen it clinically happen,” Nate Sharon said. “It’s not a myth.”
Despite this general agreement, Edwards-Leeper worries that treatment practices are trending toward an interpretation of affirming care that entails nodding along with children and adolescents who say they want physical interventions rather than evaluating whether they are likely to benefit from them.
A decade ago, the opposite was true. “I was constantly having to justify why we should be offering puberty-blocking medication, why we should be supporting these trans youth to get the services they need,” Edwards-Leeper recalled. “People thought this was just crazy, and thought the four-hour evaluations I was doing were, too—how could that possibly be enough to decide whether to go forward with the medical intervention? That was 2007, and now the questions I get are ‘Why do you make people go through any kind of evaluation?’ And ‘Why does mental health need to be involved in this?’ And ‘We should just listen to what the kids say and listen to what the adolescents say and basically just treat them like adults.’ ”
The six trainees on Edwards-Leeper’s Transgender Youth Assessment Team spoke about the myriad ways mental-health issues and social and cultural influences can complicate a child’s conception of gender. “I would say ‘affirming’ isn’t always doing exactly what the kid says they want in the moment,” one said. Another added: “Our role as clinicians isn’t to confirm or disconfirm someone’s gender identity—it’s to help them explore it with a little bit more nuance.” I asked the students whether they had come across the idea that conducting in-depth assessments is insulting or stigmatizing. They all nodded. “Well, they know what reputation I have,” Edwards-Leeper said with a laugh. “I told them about things almost being thrown at me at conferences.”
Those conference troubles signaled to Edwards-Leeper that her field had shifted in ways she found discomfiting. At one conference a few years ago, she recalled, a co-panelist who was a well-respected clinician in her field said that Edwards-Leeper’s comprehensive assessments required kids to “jump through more fiery hoops” and were “retraumatizing.” This prompted a standing ovation from the audience, mostly families of TGNC young people. During another panel discussion, at the same conference with the same clinician, but this time geared toward fellow clinicians, the same thing happened: more claims that assessments were traumatizing, more raucous applause.
Edwards-Leeper isn’t alone in worrying that the field is straying from its own established best practices. “Under the motivation to be supportive and to be affirming and to be nonstigmatizing, I think the pendulum has swung so far that now we’re maybe not looking as critically at the issues as we should be,” the National Center for Gender Spectrum Health’s Dianne Berg told me. Erica Anderson, the UCSF clinician, expressed similar concerns: “Some of the stories we’ve heard about detransitioning, I fear, are related to people who hastily embarked on medical interventions and decided that they weren’t for them, and didn’t thoroughly vet their decision either by themselves or with professional people who could help them.”
Even some of the clinicians who have emphasized the need to be deferential to young people acknowledge the complexities at play here. A psychologist with decades of experience working with TGNC young people, Diane Ehrensaft is perhaps the most frequently quoted youth-gender clinician in the country. She is tireless in her advocacy for trans kids. “It’s the children who are now leading us,” she told The Washington Post recently. She sees this as a positive development: “If you listen to the children, you will discover their gender,” she wrote in one article. “It is not for us to tell, but for them to say.”
But when I spoke with Ehrensaft at her home in Oakland, she described many situations involving physical interventions in which her work was far more complicated than simply affirming a client’s self-diagnosis. “This is what I tell kids all the time, particularly teenagers,” she said. “Often they’re pushing for fast. I say, ‘Look, I’m old, you’re young. I go slow, you go fast. We’re going to have to work that out.’ ” Sometimes, she said, she suspects that a kid who wants hormones right now is simply reciting something he found on the internet. “It just feels wooden, is the only thing I can say,” she told me.
At the end of our interview, Ehrensaft showed me a slide from a talk she was preparing about what it means to be an affirming clinician: “REALITY: WE ARE NEITHER RUBBER STAMPERS NOR PUSHERS; WE ARE FACILITATORS.” This isn’t so far off from the definition of the clinician’s role expressed by Edwards-Leeper’s students.
Competent clinicians do occasionally challenge their clients’ conception of their gender identity in order to ensure that they are approaching the subject in a sufficiently sophisticated manner. They want to make sure that a given patient has gender dysphoria, as defined in the DSM‑5, and that their current gender identity is a consistent part of who they are. If a teenager finds that his dysphoria lessens significantly when he presents himself in a more feminine way or once his overlapping mental-health problems have been treated, he may develop a different view on the necessity of hormones or surgery.
This is not to say that talk therapy can cure serious gender dysphoria. Edwards-Leeper worked to introduce the Dutch protocol of blockers and hormones in the United States precisely because she believes that it alleviates dysphoria in cases where there would otherwise be prolonged suffering. But clinicians like her are also careful, given the upheavals of adolescence and the fluid conception of gender identity among young people, not to assume that because a young person has gender dysphoria, they should automatically go on hormones.
Edwards-Leeper is hoping to promote a concept of affirming care that takes into account the developmental nuances that so often come up in her clinical work. In this effort, she is joined by Scott Leibowitz, a psychiatrist who treats children and adolescents. He is the medical director of behavioral health for the thrive program at Nationwide Children’s Hospital, in Columbus. Leibowitz has a long history of working with and supporting TGNC youth—he served as an expert witness for the Department of Justice in 2016, when President Barack Obama’s administration challenged state-level “bathroom bills” that sought to prevent trans people from using the public bathroom associated with their gender identity. Edwards-Leeper and Leibowitz met at Boston Children’s, where Leibowitz did his psychiatry fellowship, and the two have been close friends and collaborators ever since.
While it’s understandable, for historical reasons, why some people associate comprehensive psychological assessments with denial of access to care, that isn’t how Leibowitz and Edwards-Leeper view their approach. Yes, they want to discern whether a patient actually has gender dysphoria. But comprehensive assessments and ongoing mental-health work are also means of ensuring that transitioning—which can be a physically and emotionally taxing process for adolescents even under the best of circumstances—goes smoothly.
Scott Padberg, one of Edwards-Leeper’s patients, is a good example of how her comprehensive-assessment process looks for teenagers with a relatively straightforward history of persistent gender dysphoria and an absence of other factors that might complicate their diagnosis and transition path. I met Scott and his grandmother and legal guardian, Nancy, at a wrap place in Welches, Oregon, not far from where they live. It was a mild February day, so we sat in one of the pine booths outside the restaurant. Mount Hood’s massive snowcapped peak loomed nearby.
Scott Padberg, a 16-year-old patient of Laura Edwards-Leeper who went on cross-sex hormones and recently had a double mastectomy (Matt Eich)
Scott, a 16-year-old who radiates calm, explained that despite having been assigned female at birth, he simply never felt like a girl. “I guess I kinda felt different since I felt conscious of the fact that I was alive,” he said. For part of his childhood, that was fine with everyone around him. He was granted all the freedom he needed to express himself in a gender-nonconforming manner, from getting short haircuts to playing with stereotypically male toys like dinosaurs and Transformers. But the freedom didn’t last. When he was 7, his mom married a “super Christian guy” who tried to impose femininity on him. “It’s really degrading,” Scott said, to be forced to wear a dress when you’re a trans boy. (Scott’s mom divorced her devout husband two years later, and Nancy eventually took custody of Scott.)
Puberty brought bigger problems. Scott started developing breasts and got his period. “Everything just sucked, basically,” he said. “I was pretty miserable with it.” In 2015, when Scott was 13, Nancy took him to an assessment appointment with Edwards-Leeper. “She asked me about how I felt when I was younger—was I comfortable with my body? What did I tend to like or be interested in?,” Scott recalled. He said that getting on testosterone took what felt like a long time. (He was on puberty blockers for about a year.) But he said he understood that Edwards-Leeper was making certain he had considered a range of questions—from how he would feel about possibly not being able to have biological kids to whether he was comfortable with certain hormonal effects, such as a deeper voice. Scott told Edwards-Leeper that he was pretty certain about what he wanted.
Scott told me that overall, being on testosterone made him feel better, though also a bit more into “adrenaline-junkie stuff” than before. (There had been a recent incident involving Scott taking Nancy’s car for a spin despite not yet having his learner’s permit.) When I asked him about top surgery, which he was hoping to have early in the spring, he got about as animated as I saw him during our lunch. “Oh, it’s going to be so freeing,” he said. “I can change in the locker room!” In April I checked in with Nancy, and she said in an email that the surgery had gone well: “He is SO happy not to have to wear a binder!”
Scott’s assessment process centered mostly on the basic readiness questions Edwards-Leeper and Leibowitz are convinced should be asked of any young person considering hormones. But his was a relatively clear-cut case: He’d had unwavering gender dysphoria since early childhood, a lack of serious mental-health concerns, and a generally supportive family. For other gender-dysphoric young people, mental-health problems and family dynamics can complicate the transition process, though they are by no means, on their own, an indication that someone shouldn’t transition.
I met Orion Foss at a vegetarian café in the Dennison Place neighborhood of Columbus. Orion is an expressive 18-year-old with big eyes who is where Scott Padberg may be in a couple of years. Orion’s gender trajectory was a bit different, though. As a teenager, he identified as a lesbian and became involved in the local LGBTQ scene. He says that in 2014, when he was 14 years old and trans narratives were starting to show up more frequently on social media, he realized he was trans. He was also suffering from severe depression and anxiety at the time, which had led to self-harm issues, as well as what may have been an undiagnosed eating disorder. Orion believed that additional weight went straight to his hips and chest, accentuating his feminine features. At one point, he dipped down to 70 pounds.
A year or so after he realized he was trans, he told his mother, an ob-gyn, who took him to the thrive program at Nationwide, which had recently opened. (Leibowitz didn’t work there yet.) Orion met with two clinicians for an eight-hour assessment. He told me he was “definitely intimidated,” but if “you want to do something permanent to your body, you have to be absolutely positive that there’s no other way of doing it.”
At the time, Orion was initially upset that, because he was underage, thrive wouldn’t put him on hormones without the consent of both parents (his father had signed off, but his mother had not). He started sobbing when he found out. But the thrive team made clear that it was going to help him get where he wanted to be. In the meantime, a thrive therapist, Lourdes Hill, would work with Orion to address his anxiety and depression.
Looking back, Orion sees the value of this process. “If I had been put on hormone therapy when I didn’t have my identity settled, and who I was settled, and my emotions settled, it would have been crazy. ’Cause when I did start hormone therapy, hormones shoot your mood all around, and it’s not exactly safe to just shoot hormones into someone that’s not stable.” He ended up seeing Hill for weekly appointments, talking about not only his gender-identity and mental-health issues, but a host of other subjects as well. “She weeded through every possible issue with me that she could get to,” he said. “I’m glad she made me wait. And I’m glad the structure was there so I couldn’t just throw myself into something that probably would have made me worse off.”
Eventually, his mother, who was “very hesitant,” and was refusing to sign the paperwork for him to start hormones, came around. The thrive team helped her come to grips with the fact that the child she had always known as her daughter was going to become her son. “Lourdes was the driving force in that,” Orion told me in a follow-up email. “Spent a lot of time with me and my mother in therapy.”
When he was finally able to begin the hormone treatments, Orion said, he “immediately felt this weight off my shoulders.” His dosage was gradually increased and then, in May 2017, he got a double mastectomy. Orion’s transition has clearly had a profoundly beneficial effect. It’s changed the way he carries himself in the world. Before, “I would sit like this”—he slouched over—“and hide every possible female thing about me.” Now, he said, he can sit up straight. He feels like himself.
Orion Foss worked with the clinicians at Ohio’s THRIVE clinic on his mental health, his mother’s concerns, and, eventually, his transition. (Matt Eich)
Some parents struggle with the challenges of raising a TGNC child, and they can make gender clinicians’ already complicated jobs that much more complicated. Many, like Orion Foss’s mother, have trouble accepting the idea of their child transitioning. She, at least, came around. In other cases, parents not only refuse to help their child receive treatment but physically abuse them or kick them out of the house. (Reliable numbers for trans young people specifically are hard to come by, but LGBTQ youth are 120 percent more likely than their straight or cisgender counterparts to experience a period of homelessness, according to a study by Chapin Hall, a research center at the University of Chicago.)
But progressive-minded parents can sometimes be a problem for their kids as well. Several of the clinicians I spoke with, including Nate Sharon, Laura Edwards-Leeper, and Scott Leibowitz, recounted new patients’ arriving at their clinics, their parents having already developed detailed plans for them to transition. “I’ve actually had patients with parents pressuring me to recommend their kids start hormones,” Sharon said.
In these cases, the child might be capably navigating a liminal period of gender exploration; it’s the parents who are having trouble not knowing whether their kid is a boy or a girl. As Sharon put it: “Everything’s going great, but Mom’s like, ‘My transgender kid is going to commit suicide as soon as he starts puberty, and we need to start the hormones now.’ And I’m like, ‘Actually, your kid’s just fine right now. And we want to leave it open to him, for him to decide that.’ Don’t put that in stone for this kid, you know?”
Suicide is the dark undercurrent of many discussions among parents of TGNC young people. Suicide and suicidal ideation are tragically common in the transgender community. An analysis conducted by the American Foundation for Suicide Prevention and the Williams Institute, published in 2014, found that 41 percent of trans respondents had attempted suicide; 4.6 percent of the overall U.S. population report having attempted suicide at least once. While the authors note that for methodological reasons 41 percent is likely an overestimate, it still points to a scarily high figure, and other research has consistently shown that trans people have elevated rates of suicidal ideation and suicide relative to cisgender people.
Scott Leibowitz, a psychiatrist who treats children and adolescents in Columbus, Ohio, is a proponent of comprehensive assessments for young people seeking to transition. (Matt Eich)
But the existence of a high suicide rate among trans people—a population facing high instances of homelessness, sexual assault, and discrimination—does not imply that it is common for young people to become suicidal if they aren’t granted immediate access to puberty blockers or hormones. Parents and clinicians do need to make fraught decisions fairly quickly in certain situations. When severely dysphoric kids are approaching puberty, for instance, blockers can be a crucial tool to buy time, and sometimes there’s a genuine rush to gain access to them, particularly in light of the waiting lists at many gender clinics. But the clinicians I interviewed said they rarely encounter situations in which immediate access to hormones is the difference between suicide and survival. Leibowitz noted that a relationship with a caring therapist may itself be an important prophylactic against suicidal ideation for TGNC youth: “Often for the first time having a medical or mental-health professional tell them that they are going to take them seriously and really listen to them and hear their story often helps them feel better than they’ve ever felt.”
The conversations parents are having about gender-dysphoric children online aren’t always so nuanced, however. In many of these conversations, parents who say they have questions about the pace of their child’s transition, or whether gender dysphoria is permanent, are told they are playing games with their child’s life. “Would you rather have a live daughter or a dead son?” is a common response to such questions. “This type of narrative takes an already fearful parent and makes them even more afraid, which is hardly the type of mind-set one would want a parent to be in when making a complex lifelong decision for their adolescent,” Leibowitz said.
When parents discuss the reasons they question their children’s desire to transition, whether in online forums or in response to a journalist’s questions, many mention “social contagion.” These parents are worried that their kids are influenced by the gender-identity exploration they’re seeing online and perhaps at school or in other social settings, rather than experiencing gender dysphoria.
Many trans advocates find the idea of social contagion silly or even offensive given the bullying, violence, and other abuse this population faces. They also point out that some parents simply might not want a trans kid—again, parental skepticism or rejection is a painfully common experience for trans young people. Michelle Forcier, a pediatrician who specializes in youth-gender issues in Rhode Island, said the trans adolescents she works with frequently tell her things like No one’s taking me seriously—my parents think this is a phase or a fad.
But some anecdotal evidence suggests that social forces can play a role in a young person’s gender questioning. “I’ve been seeing this more frequently,” Laura Edwards-Leeper wrote in an email. Her young clients talk openly about peer influence, saying things like Oh, Steve is really trans, but Rachel is just doing it for attention. Scott Padberg did exactly this when we met for lunch: He said there are kids in his school who claim to be trans but who he believes are not. “They all flaunt it around, like: ‘I’m trans, I’m trans, I’m trans,’ ” he said. “They post it on social media.”
I heard a similar story from a quirky 16-year-old theater kid who was going by the nickname Delta when we spoke. She lives outside Portland, Oregon, with her mother and father. A wave of gender-identity experimentation hit her social circle in 2013. Suddenly, it seemed, no one was cisgender anymore. Delta, who was 13 and homeschooled, soon announced to her parents that she was genderqueer, then nonbinary, and finally trans. Then she told them she wanted to go on testosterone. Her parents were skeptical, both because of the social influence they saw at work and because Delta had anxiety and depression, which they felt could be contributing to her distress. But when her mother, Jenny, sought out information, she found herself in online parenting groups where she was told that if she dragged her feet about Delta’s transition, she was potentially endangering her daughter. “Any questioning brought down the hammer on you,” she told me.
Delta’s parents took her to see Edwards-Leeper. The psychologist didn’t question her about being trans or close the door on her eventually starting hormones. Rather, she asked Delta a host of detailed questions about her life and mental health and family. Edwards-Leeper advised her to wait until she was a bit older to take steps toward a physical transition—as Delta recalled, she said something like “I acknowledge that you feel a certain way, but I think we should work on other stuff first, and then if you still feel this way later on in life, then I will help you with that.”
“Other stuff” mostly meant her problems with anxiety and depression. Edwards-Leeper told Jenny and Delta that while Delta met the clinical threshold for gender dysphoria, a deliberate approach made the most sense in light of her mental-health issues.
Delta, a patient of Laura Edwards-Leeper who wanted to transition. Edwards-Leeper counseled her to take things slowly and to work on her co-occurring mental-health issues. Her gender dysphoria eventually lifted. (Matt Eich)
“At the time I was not happy that she told me that I should go and deal with mental stuff first,” Delta said, “but I’m glad that she said that, because too many people are so gung ho and just like, ‘You’re trans, just go ahead,’ even if they aren’t—and then they end up making mistakes that they can’t redo.” Delta’s gender dysphoria subsequently dissipated, though it’s unclear why. She started taking antidepressants in December, which seem to be working. I asked Delta whether she thought her mental-health problems and identity questioning were linked. “They definitely were,” she said. “Because once I actually started working on things, I got better and I didn’t want anything to do with gender labels—I was fine with just being me and not being a specific thing.”
It’s imperative to remember that Delta’s is a kind of story that can happen only in a place where trans people are accepted—and where parents, even skeptical ones like Jenny, are open-minded enough to take their kid to a clinician like Edwards-Leeper. In vast swaths of the United States, kids coming out as trans are much more likely to be met with hostility than with enhanced social status or recognition, and their parents are more likely to lack the willingness—or the resources—to find them care. But to deny the possibility of a connection between social influences and gender-identity exploration among adolescents would require ignoring a lot of what we know about the developing teenage brain—which is more susceptible to peer influence, more impulsive, and less adept at weighing long-term outcomes and consequences than fully developed adult brains—as well as individual stories like Delta’s.
Not everyone agrees about the importance of comprehensive assessments for transgender and gender-nonconforming youth. Within the small community of clinicians who work with TGNC young people, some have a reputation for being skeptical about the value of assessments. Johanna Olson-Kennedy, a physician who specializes in pediatric and adolescent medicine at Children’s Hospital Los Angeles and who is the medical director of the Center for Transyouth Health and Development, is one of the most sought-out voices on these issues, and has significant differences with Edwards-Leeper and Leibowitz. In “Mental Health Disparities Among Transgender Youth: Rethinking the Role of Professionals,” a 2016 jama Pediatrics article, she wrote that “establishing a therapeutic relationship entails honesty and a sense of safety that can be compromised if young people believe that what they need and deserve (potentially blockers, hormones, or surgery) can be denied them according to the information they provide to the therapist.”
This view is informed by the fact that Olson-Kennedy is not convinced that mental-health assessments lead to better outcomes. “We don’t actually have data on whether psychological assessments lower regret rates,” she told me. She believes that therapy can be helpful for many TGNC young people, but she opposes mandating mental-health assessments for all kids seeking to transition. As she put it when we talked, “I don’t send someone to a therapist when I’m going to start them on insulin.” Of course, gender dysphoria is listed in the DSM-5; juvenile diabetes is not.
One recent study co-authored by Olson-Kennedy, published in the Journal of Adolescent Health, showed that her clinic is giving cross-sex hormones to kids as young as 12. This presses against the boundaries of the Endocrine Society’s guidelines, which state that while “there may be compelling reasons to initiate sex hormone treatment prior to age 16 years … there is minimal published experience treating prior to 13.5 to 14 years of age.”
If you see gender-dysphoric 13- and 14-year-olds not as young people with a condition that may or may not indicate a permanent identity, but as trans kids, full stop, it makes sense to want to grant them access to transition resources as quickly as possible. Olson-Kennedy said that the majority of the patients she sees do need that access. She said she sees a small number of patients who desist or later regret transitioning; those patients, in her opinion, shouldn’t dictate the care of others. She would like to see a radical reshaping of care for TGNC young people. “The way that the care has been organized is around assuring the certainty and decreasing the discomfort of the professionals (usually cisgender) who determine if the young people are ready or not,” she told me. “And that’s a broken model.”
How best to support TGNC kids is a whiplash-inducing subject. To understand even just the small set of stories I encountered in my reporting—stories involving relatively privileged white kids with caring, involved families, none of which is necessarily the case for all TGNC young people in the United States—requires keeping several seemingly conflicting claims in mind. Some teenagers, in the years ahead, are going to rush into physically transitioning and may regret it. Other teens will be prevented from accessing hormones and will suffer great anguish as a result. Along the way, a heartbreaking number of trans and gender-nonconforming teens will be bullied and ostracized and will even end their own lives.
Some LGBTQ advocates have called for gender dysphoria to be removed from the DSM-5, arguing that its inclusion pathologizes being trans. But gender dysphoria, as science currently understands it, is a painful condition that requires treatment to be alleviated. Given the diversity of outcomes among kids who experience dysphoria at one time or another, it’s hard to imagine a system without a standardized, comprehensive diagnostic protocol, one designed to maximize good outcomes.
Experiencing gender dysphoria isn’t the same as experiencing anxiety or depression or psychological ailments, of course. But in certain ways it is similar: As with other psychiatric conditions, some people experience dysphoria more acutely than others; its severity can wax and wane within an individual based on a variety of factors; it is in many cases intimately tied to an individual’s social and familial life. For some people, it will pass; for others, it can be resolved without medical interventions; for still others, only the most thorough treatment available will relieve immense suffering. We recognize that there is no one-size-fits-all approach to treating anxiety or depression, and a strong case can be made that the same logic should prevail with gender dysphoria.
Perhaps a first step is to recognize detransitioners and desisters as being on the same “side” as happily transitioned trans people. Members of each of these groups have experienced gender dysphoria at some point, and all have a right to compassionate, comprehensive care, whether or not that includes hormones or surgery. “The detransitioner is probably just as scarred by the system as the transitioner who didn’t have access to transition,” Leibowitz told me. The best way to build a system that fails fewer people is to acknowledge the staggering complexity of gender dysphoria—and to acknowledge just how early we are in the process of understanding it.
This article appears in the July/August 2018 print edition with the headline “Your Child Says She’s Trans. She Wants Hormones and Surgery. She’s 13.”
from Health News And Updates https://www.theatlantic.com/magazine/archive/2018/07/when-a-child-says-shes-trans/561749/?utm_source=feed
0 notes
Text
When a Child Says She’s Trans
Claire is a 14-year-old girl with short auburn hair and a broad smile. She lives outside Philadelphia with her mother and father, both professional scientists. Claire can come across as an introvert, but she quickly opens up, and what seemed like shyness reveals itself to be quiet self-assuredness. Like many kids her age, she is a bit overscheduled. During the course of the evening I spent with Claire and her mother, Heather—these aren’t their real names—theater, guitar, and track tryouts all came up. We also discussed the fact that, until recently, she wasn’t certain she was a girl.
To hear more feature stories, see our full list or get the Audm iPhone app.
Sixth grade had been difficult for her. She’d struggled to make friends and experienced both anxiety and depression. “I didn’t have any self-confidence at all,” she told me. “I thought there was something wrong with me.” Claire, who was 12 at the time, also felt uncomfortable in her body in a way she couldn’t quite describe. She acknowledged that part of it had to do with puberty, but she felt it was more than the usual preteen woes. “At first, I started eating less,” she said, “but that didn’t really help.”
Around this time, Claire started watching YouTube videos made by transgender young people. She was particularly fascinated by MilesChronicles, the channel of Miles McKenna, a charismatic 22-year-old. His 1 million subscribers have followed along as he came out as a trans boy, went on testosterone, got a double mastectomy, and transformed into a happy, healthy young man. Claire had discovered the videos by accident, or rather by algorithm: They’d showed up in her “recommended” stream. They gave a name to Claire’s discomfort. She began to wonder whether she was transgender, meaning her internal gender identity didn’t match the sex she had been assigned at birth. “Maybe the reason I’m uncomfortable with my body is I’m supposed to be a guy,” she thought at the time.
Claire found in MilesChronicles and similar YouTube videos a clear solution to her unhappiness. “I just wanted to stop feeling bad, so I was like, I should just transition,” she said. In Claire’s case, the first step would be gaining access to drugs that would halt puberty; next, she would start taking testosterone to develop male secondary sex characteristics. “I thought that that was what made you feel better,” she told me.
In Claire’s mind, the plan was concrete, though neither Heather nor her husband, Mike, knew about any of it. Claire initially kept her feelings from her parents, researching steps she could take toward transitioning that wouldn’t require medical interventions, or her parents’ approval. She looked into ways to make her voice sound deeper and into binders to hide her breasts. But one day in August 2016, Mike asked her why she’d seemed so sad lately. She explained to him that she thought she was a boy.
This began what Heather recalls as a complicated time in her and her husband’s relationship with their daughter. They told Claire that they loved and supported her; they thanked her for telling them what she was feeling. But they stopped short of encouraging her to transition. “We let her completely explore this on her own,” Heather told me.
To Claire’s parents, her anguish seemed to come out of nowhere. Her childhood had been free of gender dysphoria—the clinical term for experiencing a powerful sense of disconnection from your assigned sex. They were concerned that what their daughter had self-diagnosed as dysphoria was simply the travails of puberty.
As Claire passed into her teen years, she continued to struggle with mental-health problems. Her parents found her a therapist, and while that therapist worked on Claire’s depression and anxiety—she was waking up several times a night to make sure her alarm clock was set correctly—she didn’t feel qualified to help her patient with gender dysphoria. The therapist referred the family to some nearby gender-identity clinics that offered transition services for young people.
Claire’s parents were wary of starting that process. Heather, who has a doctorate in pharmacology, had begun researching youth gender dysphoria for herself. She hoped to better understand why Claire was feeling this way and what she and Mike could do to help. Heather concluded that Claire met the clinical criteria for gender dysphoria in the DSM-5, the American Psychiatric Association’s diagnostic manual. Among other indications, her daughter clearly didn’t feel like a girl, clearly wanted a boy’s body, and was deeply distressed by these feelings. But Heather questioned whether these criteria, or much of the information she found online, told the whole story. “Psychologists know that adolescence is fraught with uncertainty and identity searching, and this isn’t even acknowledged,” she told me.
Heather said most of the resources she found for parents of a gender-dysphoric child told her that if her daughter said she was trans, she was trans. If her daughter said she needed hormones, Heather’s responsibility was to help her get on hormones. The most important thing she could do was affirm her daughter, which Heather and Mike interpreted as meaning they should agree with her declarations that she was transgender. Even if they weren’t so certain.
As Heather was searching for answers, Claire’s belief that she should transition was growing stronger. For months, she had been insistent that she wanted both testosterone and “top surgery”—a double mastectomy. She repeatedly asked her parents to find her doctors who could get her started on a path to physical transition. Heather and Mike bought time by telling her they were looking but hadn’t been able to find anyone yet. “We also took her kayaking, played more board games with her and watched more TV with her, and took other short family trips,” Heather recalled. “We also took away her ability to search online but gave her Instagram as a consolation.” They told her they realized that she was in pain, but they also felt, based on what they’d learned in their research, that it was possible her feelings about her gender would change over time. They asked her to start keeping a journal, hoping it would help her explore those feelings.
Claire humored her parents, even as her frustration with them mounted. Eventually, though, something shifted. In a journal entry Claire wrote last November, she traced her realization that she wasn’t a boy to one key moment. Looking in the mirror at a time when she was trying to present in a very male way—at “my baggy, uncomfortable clothes; my damaged, short hair; and my depressed-looking face”—she found that “it didn’t make me feel any better. I was still miserable, and I still hated myself.” From there, her distress gradually began to lift. “It was kind of sudden when I thought: You know, maybe this isn’t the right answer—maybe it’s something else,” Claire told me. “But it took a while to actually set in that yes, I was definitely a girl.”
Claire believes that her feeling that she was a boy stemmed from rigid views of gender roles that she had internalized. “I think I really had it set in stone what a guy was supposed to be like and what a girl was supposed to be like. I thought that if you didn’t follow the stereotypes of a girl, you were a guy, and if you didn’t follow the stereotypes of a guy, you were a girl.” She hadn’t seen herself in the other girls in her middle-school class, who were breaking into cliques and growing more gossipy. As she got a bit older, she found girls who shared her interests, and started to feel at home in her body.
Heather thinks that if she and Mike had heeded the information they found online, Claire would have started a physical transition and regretted it later. These days, Claire is a generally happy teenager whose mental-health issues have improved markedly. She still admires people, like Miles McKenna, who benefited from transitioning. But she’s come to realize that’s just not who she happens to be.
The number of self-identifying trans people in the United States is on the rise. In June 2016, the Williams Institute at the UCLA School of Law estimated that 1.4 million adults in the U.S. identify as transgender, a near-doubling of an estimate from about a decade earlier. As of 2017, according to the institute, about 150,000 teenagers ages 13 to 17 identified as trans. The number of young people seeking clinical services appears to be growing as well. A major clinic in the United Kingdom saw a more than 300 percent increase in new referrals over the past three years. In the U.S., where youth gender clinics are somewhat newer—40 or so are scattered across the country—solid numbers are harder to come by. Anecdotally, though, clinicians are reporting large upticks in new referrals, and waiting lists can stretch to five months or longer.
The current era of gender-identity awareness has undoubtedly made life easier for many young people who feel constricted by the sometimes-oppressive nature of gender expectations. A rich new language has taken root, granting kids who might have felt alone or excluded the words they need to describe their experiences. And the advent of the internet has allowed teenagers, even ones in parts of the country where acceptance of gender nonconformity continues to come far too slowly, to find others like them.
But when it comes to the question of physical interventions, this era has also brought fraught new challenges to many parents. Where is the line between not “feeling like” a girl because society makes it difficult to be a girl and needing hormones to alleviate dysphoria that otherwise won’t go away? How can parents tell? How can they help their children gain access to the support and medical help they might need, while also keeping in mind that adolescence is, by definition, a time of fevered identity exploration?
Maciek Jasik
There is no shortage of information available for parents trying to navigate this difficult terrain. If you read the bible of medical and psychiatric care for transgender people—the Standards of Care issued by the World Professional Association for Transgender Health (Wpath)—you’ll find an 11-page section called “Assessment and Treatment of Children and Adolescents With Gender Dysphoria.” It states that while some teenagers should go on hormones, that decision should be made with deliberation: “Before any physical interventions are considered for adolescents, extensive exploration of psychological, family, and social issues should be undertaken.” The American Psychological Association’s guidelines sound a similar note, explaining the benefits of hormones but also noting that “adolescents can become intensely focused on their immediate desires.” It goes on: “This intense focus on immediate needs may create challenges in assuring that adolescents are cognitively and emotionally able to make life-altering decisions.”
The leading professional organizations offer this guidance. But some clinicians are moving toward a faster process. And other resources, including those produced by major LGBTQ organizations, place the emphasis on acceptance rather than inquiry. The Human Rights Campaign’s “Transgender Children & Youth: Understanding the Basics” web page, for example, encourages parents to seek the guidance of a gender specialist. It also asserts that “being transgender is not a phase, and trying to dismiss it as such can be harmful during a time when your child most needs support and validation.” Similarly, parents who consult the pages tagged “transgender youth” on glaad’s site will find many articles about supporting young people who come out as trans but little about the complicated diagnostic and developmental questions faced by the parents of a gender-exploring child.
HRC, glaad, and like-minded advocacy groups emphasize the acceptance of trans kids for understandable reasons: For far too long, parents, as well as clinicians, denied the possibility that trans kids and teens even existed, let alone that they should be allowed to transition. Many such organizations are primarily concerned with raising awareness and correcting still-common misconceptions.
A similar motive seems to animate much of the media coverage of transgender young people. Two genres of coverage have emerged. Dating back at least to the 1993 murder of the Nebraska 21-year-old Brandon Teena, which inspired a documentary as well as the film Boys Don’t Cry, a steady stream of horror stories has centered on bullying, physical assault, and suicide—real risks that transgender and gender-nonconforming (TGNC) young people still face.
More recently, a wave of success stories has appeared. In many of these accounts, kids are lost, confused, and frustrated right up until the moment they are allowed to grow their hair out and adopt a new name, at which point they finally become their true self. Take, for example, a Parents.com article in which a mother, writing pseudonymously, explains that she struggled with her child’s gender-identity issues for years, until finally turning to a therapist, who, after a 20-minute evaluation, pronounced the child trans. Suddenly, everything clicked into place. The mother writes: “I looked at the child sitting between my husband and me, the child who was smiling, who appeared so happy, who looked as if someone finally saw him or her the way she or he saw him or herself.” In a National Geographic special issue on gender, the writer Robin Marantz Henig recounts the story of a mother who let her 4-year-old, assigned male at birth, choose a girl’s name, start using female pronouns, and attend preschool as a girl. “Almost instantly the gloom lifted,” Henig writes.
Accounts of successful transitions can help families envision a happy outcome for a suffering child. And some young people clearly experience something like what these caterpillar-to-butterfly narratives depict. They have persistent, intense gender dysphoria from a very young age, and transitioning alleviates it. “Some kids don’t waver” in their gender identity, Nate Sharon, a psychiatrist who oversaw a gender clinic in New Mexico for two and a half years, and who is himself trans, told me when we spoke in 2016. “I’m seeing an 11-year-old who at age 2 went up to his mom and said, ‘When am I going to start growing my penis? Where’s my penis?’ At 2.”
But these stories tend to elide the complexities of being a TGNC young person, or the parent of one. Some families will find a series of forking paths, and won’t always know which direction is best. Like Claire’s parents, they may be convinced that their child is in pain, but also concerned that physical transition is not the solution, at least not for a young person still in the throes of adolescence.
We are still in the earliest stages of understanding how physical transitioning affects dysphoric young people. While the specifics depend on your child’s age, and can vary from case to case, the transition process for a persistently dysphoric child typically looks something like the following. First, allow your child to transition socially: to adopt the pronouns and style of dress of their authentic gender, and to change their name if they wish. As your child approaches adolescence, get them puberty-blocking drugs, because developing the secondary sex characteristics of their assigned sex could exacerbate their gender dysphoria. When they reach their teen years, help them gain access to the cross-sex hormones that will allow them to develop secondary sex characteristics in line with their gender identity. (Until recently, hormones were typically not prescribed until age 16; it’s now more common for 15- and 14-year-olds, and sometimes even younger kids, to begin hormone therapy.)
In the United States, avoiding puberty became an option only a little more than a decade ago, so researchers have just begun tracking the kids engaged in this process, and we don’t yet have comprehensive data about their long-term outcomes. Most of the data we do have involve kids who socially transitioned at an early age, but who hadn’t yet physically transitioned. The information comes from a University of Washington researcher named Kristina Olson. Olson is the founder of the TransYouth Project, which is following a cohort of about 300 children for 20 years—the longest such longitudinal study based in the U.S. The kids she is tracking appear to be doing well—they don’t seem all that different, in terms of their mental health and general happiness, from a control group of cisgender kids (that is, kids who identify with the sex they were assigned at birth).
At the prestigious Center of Expertise on Gender Dysphoria, at Vrije Universiteit University Medical Center, in Amsterdam—often referred to simply as “the Dutch clinic”—an older cohort of kids who went through the puberty-blockers-and-cross-sex-hormones protocol was also found to be doing well: “Gender dysphoria had resolved,” according to a study of the group published in 2014 in Pediatrics. “Psychological functioning had steadily improved, and well-being was comparable to same-age peers.”
These early results, while promising, can tell us only so much. Olson’s findings come from a group of trans kids whose parents are relatively wealthy and are active in trans-support communities; they volunteered their children for the study. There are limits to how much we can extrapolate from the Dutch study as well: That group went through a comprehensive diagnostic process prior to transitioning, which included continuous access to mental-health care at a top-tier gender clinic—a process unfortunately not available to every young person who transitions.
Among the issues yet to be addressed by long-term studies are the effects of medications on young people. As Thomas Steensma, a psychologist and researcher at the Dutch clinic and a co-author of that study, explained to me, data about the potential risks of putting young people on puberty blockers are scarce. He would like to see further research into the possible effects of blockers on bone and brain development. (The potential long-term risks of cross-sex hormones aren’t well known, but are likely modest, according to Joshua Safer, one of the authors of the Endocrine Society’s “Clinical Practice Guideline” for treatment of gender dysphoria.)
Meanwhile, fundamental questions about gender dysphoria remain unanswered. Researchers still don’t know what causes it—gender identity is generally viewed as a complicated weave of biological, psychological, and sociocultural factors. In some cases, gender dysphoria may interact with mental-health conditions such as depression and anxiety, but there’s little agreement about how or why. Trauma, particularly sexual trauma, can contribute to or exacerbate dysphoria in some patients, but again, no one yet knows exactly why.
To reiterate: For many of the young people in the early studies, transitioning—socially for children, physically for adolescents and young adults—appears to have greatly alleviated their dysphoria. But it’s not the answer for everyone. Some kids are dysphoric from a very young age, but in time become comfortable with their body. Some develop dysphoria around the same time they enter puberty, but their suffering is temporary. Others end up identifying as nonbinary—that is, neither male nor female.
Ignoring the diversity of these experiences and focusing only on those who were effectively “born in the wrong body” could cause harm. That is the argument of a small but vocal group of men and women who have transitioned, only to return to their assigned sex. Many of these so-called detransitioners argue that their dysphoria was caused not by a deep-seated mismatch between their gender identity and their body but rather by mental-health problems, trauma, societal misogyny, or some combination of these and other factors. They say they were nudged toward the physical interventions of hormones or surgery by peer pressure or by clinicians who overlooked other potential explanations for their distress.
Some of these interventions are irreversible. People respond differently to cross-sex hormones, but changes in vocal pitch, body hair, and other physical characteristics, such as the development of breast tissue, can become permanent. Kids who go on puberty blockers and then on cross-sex hormones may not be able to have biological children. Surgical interventions can sometimes be reversed with further surgeries, but often with disappointing results.
The concerns of the detransitioners are echoed by a number of clinicians who work in this field, most of whom are psychologists and psychiatrists. They very much support so-called affirming care, which entails accepting and exploring a child’s statements about their gender identity in a compassionate manner. But they worry that, in an otherwise laudable effort to get TGNC young people the care they need, some members of their field are ignoring the complexity, and fluidity, of gender-identity development in young people. These colleagues are approving teenagers for hormone therapy, or even top surgery, without fully examining their mental health or the social and family influences that could be shaping their nascent sense of their gender identity.
That’s too narrow a definition of affirming care, in the view of many leading clinicians. “Affirming care does not privilege any one outcome when it comes to gender identity, but instead aims to allow exploration of gender without judgment and with a clear understanding of the risks, benefits, and alternatives to any choice along the way,” Aron Janssen, the clinical director of the Gender and Sexuality Service at Hassenfeld Children’s Hospital, in New York, told me. “Many people misinterpret affirming care as proceeding to social and medical transition in all cases without delay, but the reality is much more complex.”
To make sense of this complex reality—and ensure the best outcome for all gender-exploring kids—parents need accurate, nuanced information about what gender dysphoria is and about the many blank spots in our current knowledge. They don’t always get it.
For gender-dysphoric people, physical transition can be life enhancing, even lifesaving. While representative long-term data on the well-being of trans adults have yet to emerge, the evidence that does exist—as well as the sheer heft of personal accounts from trans people and from the clinicians who help them transition—is overwhelming. For many if not most unwaveringly gender-dysphoric people, hormones work. Surgery works. That’s reflected in studies that consistently show low regret rates for the least-reversible physical procedures to address gender dysphoria. One 2012 review of past studies, for example, found that sex-reassignment surgery “is an effective treatment for [gender dysphoria] and the only treatment that has been evaluated empirically with large clinical case series.” A study on “bottom surgery,” or surgery designed to construct a penis or vagina, found that from 1972 to 2015, “only 0.6 percent of transwomen and 0.3 percent of transmen who underwent [these procedures] were identified as experiencing regret.”
Those of us who have never suffered from gender dysphoria can have a hard time appreciating what’s at stake. Rebecca Kling, an educator at the National Center for Transgender Equality, in Washington, D.C., told me that before she transitioned she felt as if she were constantly carrying around a backpack full of rocks. “That is going to make everything in my life harder, and in many cases is going to make things impossible,” she said. “Of course being able to remove that heavy burden has added comfort and stability in my sense of myself and my body.” Other trans people have offered similar descriptions of gender dysphoria—a weight, a buzzing, an unavoidable source of rumination and worry. Hormones and surgery grant transgender people profound relief.
Historically, they have been denied access to that relief. Christine Jorgensen, the first American to become widely known for transitioning through hormones and surgery, in the 1950s, had to go to Denmark for her care. The trans historian Genny Beemyn notes that Jorgensen’s doctor “received more than 1,100 letters from transsexual people, many of whom sought to be his patients,” in the months after Jorgensen was treated. As a result of the requests, “the Danish government banned such procedures for non-citizens. In the United States, many physicians simply dismissed the rapidly growing number of individuals seeking gender-affirming surgeries as being mentally ill.”
Today, the situation in the U.S. has improved, but the lack of access to transition services continues to be a problem. Whether trans people in this country can access treatments such as hormones and surgery depends on a variety of factors, ranging from where they live to what their health insurance will cover (if they have any) to their ability to navigate piles of paperwork. Erica Anderson, a trans woman and clinical psychologist who works at the Child and Adolescent Gender Center, at UC San Francisco’s Benioff Children’s Hospital, had no luck when she tried to get hormones from an endocrinologist in Philadelphia just a decade ago. “Even I, with my education and resources, was denied care and access,” she told me. “The endocrinologist simply said, ‘I don’t do that.’ I offered to provide her the guidelines from her own Endocrine Society,” Anderson said. “She refused and wouldn’t even look me in the eye. No referral or offer to help. She sent me away with nothing, feeling like I was an undesirable.”
Many trans people have stories like Anderson’s. For this reason, among others, trans communities can be skeptical of those who focus on negative transition outcomes. They have long dealt with “professionals who seem uncomfortable giving trans people the go-ahead to transition at all,” Zinnia Jones, a trans woman who runs the website GenderAnalysis, told me in an email. They have also faced “unnecessarily protracted timelines for accessing care, a lack of understanding or excess skepticism of our identities from clinicians, and so on.”
Groups like Wpath, the primary organization for psychologists, psychiatrists, endocrinologists, surgeons, and others who work with TGNC clients, have attempted to reverse this neglect in recent years. A growing number of adult gender clinics follow “informed consent” protocols, built on the philosophy that trans adults, once informed of the potential benefits and risks of medical procedures, have a right to make their own decisions about their body and shouldn’t have their need for services questioned by mental-health and medical professionals.
This shift is seen by many trans people and advocates as an important course correction after decades of gatekeeping—aloof professionals telling trans people they couldn’t get hormones or surgery, because they weren’t really trans, or hadn’t been living as a trans person long enough, or were too mentally ill.
For gender-questioning children and teens, the landscape is different. A minor’s legal guardian almost always has to provide consent prior to a medical procedure, whether it’s a tonsillectomy or top surgery. Wpath and other organizations that provide guidance for transitioning young people call for thorough assessments of patients before they start taking blockers or hormones.
This caution comes from the concerns inherent in working with young people. Adolescents change significantly and rapidly; they may view themselves and their place in the world differently at 15 than they did at 12. “You’ve got the onset of puberty right around the age where they develop the concept of abstract thinking,” said Nate Sharon, the New Mexico psychiatrist. “So they may start to conceptualize gender concepts in a much richer, broader manner than previously—and then maybe puberty blockers or cross-sex hormones aren’t for them.” That was true for Claire: A shift in her understanding of the nature of gender led her to realize that transitioning was not the answer for her.
For younger children, gender identity is an even trickier concept. In one experiment, for example, many 3-to-5-year-olds thought that if a boy put on a dress, he became a girl. Gender clinicians sometimes encounter young children who believe they are, or want to be, another gender because of their dress or play preferences—I like rough-and-tumble play, so I must be a boy—but who don’t meet the criteria for gender dysphoria.
In the past, therapists and doctors interpreted the fluidity of gender identity among children as license to put gender-bending kids into the “right” box by encouraging—or forcing—them to play with the “right” toys and dress in the “right” clothes. Until about five years ago, according to one clinician’s estimate, social transition was often frowned upon. For decades, trans-ness was sometimes tolerated in adults as a last-ditch outcome, but in young people it was more often seen as something to be drummed out rather than explored or accepted. So-called reparative therapy has harmed and humiliated trans and gender-nonconforming children. In her book Gender Born, Gender Made, Diane Ehrensaft, the director of mental health at UC San Francisco’s Child and Adolescent Gender Center, writes that victims of these practices “become listless or agitated, long for their taken-away favorite toys and clothes, and even literally go into hiding in closets to continue playing with the verboten toys or wearing the forbidden clothes.” Such therapy is now viewed as unethical.
These days, mainstream youth-gender clinicians practice affirming care instead. They listen to their young patients, take their statements about their gender seriously, and often help facilitate social and physical transition. Affirming care has quickly become a professional imperative: Don’t question who your clients are—let them tell you who they are, and accept their identity in a nurturing, encouraging manner.
The affirming approach is far more humane than older ones, but it conflicts, at least a little, with what we know about gender-identity fluidity in young people. What does it mean to be affirming while acknowledging that kids and teenagers can have an understanding of gender that changes over a short span? What does it mean to be affirming while acknowledging that feelings of gender dysphoria can be exacerbated by mental-health difficulties, trauma, or a combination of the two?
Clinicians are still wrestling with how to define affirming care, and how to balance affirmation and caution when treating adolescents. “I don’t want to be a gatekeeper,” Dianne Berg, a co-director of the National Center for Gender Spectrum Health, at the University of Minnesota, told me. “But I also worry that in opening the gates, we’re going to have more adolescents that don’t engage in the reflective work needed in order to make sound decisions, and there might end up being more people when they are older that are like, Oh, hmm—now I am not sure about this.”
When Max Robinson was 17, getting a double mastectomy made perfect sense to her. In fact, it felt like her only option—like a miraculous, lifesaving procedure. Though she had a woman’s body, she was really a man. Surgery would finally offer her a chance to be herself.
I met Max, now 22, in an airy café in the quiet southern-Oregon town where she lives. She was wearing a T‑shirt with a flannel button-down over it. On her head, a gray winter cap; at her feet, a shaggy white service dog. By the time we met, we’d spoken on the phone and exchanged a number of emails, and she had told me her story—one that suggests the complexity of gender-identity development.
Max recalled that as early as age 5, she didn’t enjoy being treated like a girl. “I questioned my teachers about why I had to make an angel instead of a Santa for a Christmas craft, or why the girls’ bathroom pass had ribbons instead of soccer balls, when I played soccer and knew lots of other girls in our class who loved soccer,” she said.
She grew up a happy tomboy—until puberty. “People expect you to grow out of it” at that age, she explained, “and people start getting uncomfortable when you don’t.” Worse, “the way people treated me started getting increasingly sexualized.” She remembered one boy who, when she was 12, kept asking her to pick up his pencil so he could look down her shirt.
“I started dissociating from my body a lot more when I started going through puberty,” Max said. Her discomfort grew more internalized—less a frustration with how the world treated women and more a sense that the problem lay in her own body. She came to believe that being a woman was “something I had to control and fix.” She had tried various ways of making her discomfort abate—in seventh grade, she vacillated between “dressing like a 12-year-old boy” and wearing revealing, low-cut outfits, attempts to defy and accede to the demands the world was making of her body. But nothing could banish her feeling that womanhood wasn’t for her. She had more bad experiences with men, too: When she was 13, she had sex with an older man she was seeing; at the time, it felt consensual, but she has since realized that a 13-year-old can’t consent to sex with an 18-year-old. At 14, she witnessed a friend get molested by an adult man at a church slumber party. Around this time, Max was diagnosed with depression and generalized anxiety disorder.
In ninth grade, Max first encountered the concept of being transgender when she watched an episode of The Tyra Banks Show in which Buck Angel, a trans porn star, talked about his transition. It opened up a new world of online gender-identity exploration. She gradually decided that she needed to transition.
Max’s parents were skeptical at first but eventually came around, signing her up for sessions with a therapist who specialized in gender-identity issues. She recalled that the specialist was very open to putting her on a track toward transition, though he suggested that her discomfort could have other sources as well. Max, however, was certain that transitioning was the answer. She told me that she “refused to talk about anything other than transition.”
When Max was 16, her therapist wrote her a referral to see an endocrinologist who could help her begin the process of physical transition by prescribing male hormones. The endocrinologist was skeptical, Max said. “I think what she was seeing was a lesbian teenager,” not a trans one. At the time, though, Max interpreted the doctor’s reluctance as her “being ignorant, as her trying to hurt me.” Armed with the referral from her therapist, Max got the endocrinologist to prescribe the treatment she sought.
Max started taking testosterone. She experienced some side effects—hot flashes, memory issues—but the hormones also provided real relief. Her plan all along had been to get top surgery, too, and the initially promising effects of the hormones helped persuade her to continue on this path. When she was 17, Max, who was still dealing with major mental-health issues, was scheduled for surgery.
Because Max had parental approval, the surgeon she saw agreed to operate on her despite the fact that she was still a minor. (It’s become more common for surgeons to perform top surgeries on teenagers as young as 16 if they have parental approval. The medical norms are more conservative when it comes to bottom surgeries; Wpath says they should be performed only on adults who have been living in their gender role for at least one year.) Max went into the surgery optimistic. “I was convinced it would solve a lot of my problems,” she said, “and I hadn’t accurately named a lot of those problems yet.”
Max Robinson went on cross-sex hormones when she was 16 and had a double mastectomy when she was 17. Now 22, she has detransitioned and identifies as a woman. (Chloe Aftel)
Max was initially happy with the results of her physical transformation. Before surgery, she wasn’t able to fully pass as male. After surgery, between her newly masculinized chest and the facial hair she was able to grow thanks to the hormones, she felt like she had left behind the sex she had been assigned at birth. “It felt like an accomplishment to be seen the way I wanted to be seen,” she told me.
But that feeling didn’t last. After her surgery, Max moved from her native California to Portland and threw herself into the trans scene there. It wasn’t a happy home. The clarity of identity she was seeking—and that she’d felt, temporarily, after starting hormones and undergoing surgery—never fully set in. Her discomfort didn’t go away.
Today, Max identifies as a woman. She believes that she misinterpreted her sexual orientation, as well as the effects of the misogyny and trauma she had experienced as a young person, as being about gender identity. Because of the hormone therapy, she still has facial hair and is frequently mistaken for male as a result, but she has learned to live with this: “My sense of self isn’t entirely dependent on how other people see me.”
Max is one of what appears to be a growing number of people who believe they were failed by the therapists and physicians they went to for help with their gender dysphoria. While their individual stories differ, they tend to touch on similar themes. Most began transitioning during adolescence or early adulthood. Many were on hormones for extended periods of time, causing permanent changes to their voice, appearance, or both. Some, like Max, also had surgery.
Many detransitioners feel that during the process leading up to their transition, well-meaning clinicians left unexplored their overlapping mental-health troubles or past traumas. Though Max’s therapist had tried to work on other issues with her, Max now believes she was encouraged to rush into physical transition by clinicians operating within a framework that saw it as the only way someone like her could experience relief. Despite the fact that she was a minor for much of the process, she says, her doctors more or less did as she told them.
Over the past couple of years, the detransitioner movement has become more visible. Last fall, Max told her story to The Economist’s magazine of culture and ideas, 1843. Detransitioners who previously blogged pseudonymously, largely on Tumblr, have begun writing under their real names, as well as speaking on camera in YouTube videos.
Cari Stella is the author of a blog called Guide on Raging Stars. Stella, now 24, socially transitioned at 15, started hormones at 17, got a double mastectomy at 20, and detransitioned at 22. “I’m a real-live 22-year-old woman with a scarred chest and a broken voice and a 5 o’clock shadow because I couldn’t face the idea of growing up to be a woman,” she said in a video posted in August 2016. “I was not a very emotionally stable teenager,” she told me when we spoke. Transitioning offered a “level of control over how I was being perceived.”
Carey Callahan is a 36-year-old woman living in Ohio who detransitioned after identifying as trans for four years and spending nine months on male hormones. She previously blogged under the pseudonym Maria Catt, but “came out” in a YouTube video in July 2016. She now serves as something of an older sister to a network of female, mostly younger detransitioners, about 70 of whom she has met in person; she told me she has corresponded online with an additional 300. (The detransitioners who have spoken out thus far are mostly people who were assigned female at birth. Traditionally, most new arrivals at youth gender clinics were assigned male; today, many clinics are reporting that new patients are mostly assigned female. There is no consensus explanation for the change.)
I met Carey in Columbus in March. She told me that her decision to detransition grew out of her experience working at a trans clinic in San Francisco in 2014 and 2015. “People had said often to me that when you transition, your gender dysphoria gets worse before it gets better,” she told me. “But I saw and knew so many people who were cutting themselves, starving themselves, never leaving their apartments. That made me doubt the narrative that if you make it all the way to medical transition, then it’s probably going to work out well for you.”
Carey Callahan serves as something of an older sister to a group of women who, like her, have detransitioned. (Matt Eich)
Carey said she met people who appeared to be grappling with severe trauma and mental illness, but were fixated on their next transition milestone, convinced that was the moment when they would get better. “I knew a lot of people committed to that narrative who didn’t seem to be doing well,” she recalled. Carey’s time at the clinic made her realize that testosterone hadn’t made her feel better in a sustained way either. She detransitioned, moved to Ohio, and is now calling for a more careful approach to treating gender dysphoria than what many detransitioners say they experienced themselves.
In part, that would mean clinicians adhering to guidelines like Wpath’s Standards of Care, which are nonbinding. “When I look at what the SOC describes, and then I look at my own experience and my friends’ experiences of pursuing hormones and surgery, there’s hardly any overlap between the directives of the SOC and the reality of care patients get,” Carey told me. “We didn’t discuss all the implications of medical intervention—psychological, social, physical, sexual, occupational, financial, and legal—which the SOC directs the mental-health professional to discuss. What the SOC describes and the care people get before getting cleared for hormones and surgery are miles apart.”
Detransitioners, understandably, elicit suspicion from the trans community. Imagine being a trans person who endured a bruising fight to prove to your psychiatrist and endocrinologist that you are trans, in order to gain access to hormones that greatly improve your quality of life, that relieve suffering. You might view with skepticism—at the very least—a group calling for more gatekeeping. Conservative media outlets, for their part, often seize on detransition narratives to push the idea that being trans is some sort of liberal invention. “How Carey Was Set Free From Transgenderism” was the conservative website LifeSiteNews’ disingenuous take on Carey’s story.
Video: Reversing a Gender Transition
youtube
No one knows how common detransitioning is. A frequently cited statistic—that only 2.2 percent of people who physically transition later regret it—doesn’t paint a complete picture. It comes from a study, conducted in Sweden, that examined only those people who had undergone sex-reassignment surgery and legally changed their gender, then applied to change their gender back—a standard that, Carey pointed out, would have excluded her and most of the detransitioners she knows.
It stands to reason that as any medical procedure becomes more readily available, a higher number of people will regret having it. Why focus on detransitioners, when no one even knows whether their experiences are all that common? One answer is that clinicians who have logged thousands of hours working with transgender and gender-nonconforming young people are raising the same concerns.
When it comes to helping TGNC young people gain access to physical interventions, few American clinicians possess the bona fides of the psychologist Laura Edwards-Leeper. A decade ago, when she was working at Boston Children’s Hospital, she visited the Dutch clinic to learn the puberty-blocking protocol pioneered there. She helped bring that protocol back to Boston, where she worked with the first-ever group of American kids to go through that process.
Today, Edwards-Leeper oversees a collaboration between Pacific University and Oregon’s Transgender Clinic, within the nonprofit Legacy Health system. At Pacific, she is training clinical-psychology doctoral students to conduct “readiness assessments” for young people seeking physical-transition services.
In February, I visited one of her classes at Pacific, just outside Portland. For an hour, she let me pepper her students with questions about their experiences as clinicians-in-training in what is essentially a brand-new field. When the subject of detransitioners came up, Edwards-Leeper chimed in. “I’ve been predicting this for, I don’t know, the last five or more years,” she said. “I anticipate there being more and more and more, because there are so many youth who are now getting services with very limited mental-health assessment and sometimes no mental-health assessment. It’s inevitable, I think.”
Laura Edwards-Leeper, a clinician at Pacific University and Oregon’s Transgender Clinic. She brought the puberty-blocking transition protocol pioneered by the Dutch to the U.S. (Matt Eich)
Edwards-Leeper believes that comprehensive assessments are crucial to achieving good outcomes for TGNC young people, especially those seeking physical interventions, in part because some kids who think they are trans at one point in time will not feel that way later on. This is a controversial subject in some corners of the trans community. A small group of studies has been interpreted as showing that the majority of children who experience gender dysphoria eventually stop experiencing it and come to identify as cisgender adults. (In these studies, children who suffer intense dysphoria over an extended period of time, especially into adolescence, are more likely to identify as trans in the long run.)
This so-called desistance research has been attacked on various methodological grounds. The most-credible critiques center on the claim that some kids who were merely gender nonconforming—that is, they preferred stereotypically cross-sex activities or styles of dress—but not dysphoric may have been counted as desisters because the studies relied on outdated diagnostic criteria, artificially pushing the percentage upward. (The terms detransition and desist are used in different ways by different people. In this article, I am drawing this distinction: Detransitioners are people who undergo social or physical transitions and later reverse them; desisters are people who stop experiencing gender dysphoria without having fully transitioned socially or physically.)
The desistance rate for accurately diagnosed dysphoric kids is probably lower than some of the contested studies suggest; a small number of merely gender-nonconforming kids may indeed have been wrongly swept into even some of the most recent studies, which didn’t use the most up-to-date criteria, from the DSM-5. And there remains a paucity of big, rigorous studies that might deliver a more reliable figure.
Within a subset of trans advocacy, however, desistance isn’t viewed as a phenomenon we’ve yet to fully understand and quantify but rather as a myth to be dispelled. Those who raise the subject of desistance are often believed to have nefarious motives—the liberal outlet ThinkProgress, for example, referred to desistance research as “the pernicious junk science stalking trans kids,” and a subgenre of articles and blog posts attempts to debunk “the desistance myth.” But the evidence that desistance occurs is overwhelming. The American Psychological Association, the Substance Abuse and Mental Health Services Administration, the Endocrine Society, and Wpath all recognize that desistance occurs. I didn’t speak with a single clinician who believes otherwise. “I’ve seen it clinically happen,” Nate Sharon said. “It’s not a myth.”
Despite this general agreement, Edwards-Leeper worries that treatment practices are trending toward an interpretation of affirming care that entails nodding along with children and adolescents who say they want physical interventions rather than evaluating whether they are likely to benefit from them.
A decade ago, the opposite was true. “I was constantly having to justify why we should be offering puberty-blocking medication, why we should be supporting these trans youth to get the services they need,” Edwards-Leeper recalled. “People thought this was just crazy, and thought the four-hour evaluations I was doing were, too—how could that possibly be enough to decide whether to go forward with the medical intervention? That was 2007, and now the questions I get are ‘Why do you make people go through any kind of evaluation?’ And ‘Why does mental health need to be involved in this?’ And ‘We should just listen to what the kids say and listen to what the adolescents say and basically just treat them like adults.’ ”
The six trainees on Edwards-Leeper’s Transgender Youth Assessment Team spoke about the myriad ways mental-health issues and social and cultural influences can complicate a child’s conception of gender. “I would say ‘affirming’ isn’t always doing exactly what the kid says they want in the moment,” one said. Another added: “Our role as clinicians isn’t to confirm or disconfirm someone’s gender identity—it’s to help them explore it with a little bit more nuance.” I asked the students whether they had come across the idea that conducting in-depth assessments is insulting or stigmatizing. They all nodded. “Well, they know what reputation I have,” Edwards-Leeper said with a laugh. “I told them about things almost being thrown at me at conferences.”
Those conference troubles signaled to Edwards-Leeper that her field had shifted in ways she found discomfiting. At one conference a few years ago, she recalled, a co-panelist who was a well-respected clinician in her field said that Edwards-Leeper’s comprehensive assessments required kids to “jump through more fiery hoops” and were “retraumatizing.” This prompted a standing ovation from the audience, mostly families of TGNC young people. During another panel discussion, at the same conference with the same clinician, but this time geared toward fellow clinicians, the same thing happened: more claims that assessments were traumatizing, more raucous applause.
Edwards-Leeper isn’t alone in worrying that the field is straying from its own established best practices. “Under the motivation to be supportive and to be affirming and to be nonstigmatizing, I think the pendulum has swung so far that now we’re maybe not looking as critically at the issues as we should be,” the National Center for Gender Spectrum Health’s Dianne Berg told me. Erica Anderson, the UCSF clinician, expressed similar concerns: “Some of the stories we’ve heard about detransitioning, I fear, are related to people who hastily embarked on medical interventions and decided that they weren’t for them, and didn’t thoroughly vet their decision either by themselves or with professional people who could help them.”
Even some of the clinicians who have emphasized the need to be deferential to young people acknowledge the complexities at play here. A psychologist with decades of experience working with TGNC young people, Diane Ehrensaft is perhaps the most frequently quoted youth-gender clinician in the country. She is tireless in her advocacy for trans kids. “It’s the children who are now leading us,” she told The Washington Post recently. She sees this as a positive development: “If you listen to the children, you will discover their gender,” she wrote in one article. “It is not for us to tell, but for them to say.”
But when I spoke with Ehrensaft at her home in Oakland, she described many situations involving physical interventions in which her work was far more complicated than simply affirming a client’s self-diagnosis. “This is what I tell kids all the time, particularly teenagers,” she said. “Often they’re pushing for fast. I say, ‘Look, I’m old, you’re young. I go slow, you go fast. We’re going to have to work that out.’ ” Sometimes, she said, she suspects that a kid who wants hormones right now is simply reciting something he found on the internet. “It just feels wooden, is the only thing I can say,” she told me.
At the end of our interview, Ehrensaft showed me a slide from a talk she was preparing about what it means to be an affirming clinician: “REALITY: WE ARE NEITHER RUBBER STAMPERS NOR PUSHERS; WE ARE FACILITATORS.” This isn’t so far off from the definition of the clinician’s role expressed by Edwards-Leeper’s students.
Competent clinicians do occasionally challenge their clients’ conception of their gender identity in order to ensure that they are approaching the subject in a sufficiently sophisticated manner. They want to make sure that a given patient has gender dysphoria, as defined in the DSM‑5, and that their current gender identity is a consistent part of who they are. If a teenager finds that his dysphoria lessens significantly when he presents himself in a more feminine way or once his overlapping mental-health problems have been treated, he may develop a different view on the necessity of hormones or surgery.
This is not to say that talk therapy can cure serious gender dysphoria. Edwards-Leeper worked to introduce the Dutch protocol of blockers and hormones in the United States precisely because she believes that it alleviates dysphoria in cases where there would otherwise be prolonged suffering. But clinicians like her are also careful, given the upheavals of adolescence and the fluid conception of gender identity among young people, not to assume that because a young person has gender dysphoria, they should automatically go on hormones.
Edwards-Leeper is hoping to promote a concept of affirming care that takes into account the developmental nuances that so often come up in her clinical work. In this effort, she is joined by Scott Leibowitz, a psychiatrist who treats children and adolescents. He is the medical director of behavioral health for the thrive program at Nationwide Children’s Hospital, in Columbus. Leibowitz has a long history of working with and supporting TGNC youth—he served as an expert witness for the Department of Justice in 2016, when President Barack Obama’s administration challenged state-level “bathroom bills” that sought to prevent trans people from using the public bathroom associated with their gender identity. Edwards-Leeper and Leibowitz met at Boston Children’s, where Leibowitz did his psychiatry fellowship, and the two have been close friends and collaborators ever since.
While it’s understandable, for historical reasons, why some people associate comprehensive psychological assessments with denial of access to care, that isn’t how Leibowitz and Edwards-Leeper view their approach. Yes, they want to discern whether a patient actually has gender dysphoria. But comprehensive assessments and ongoing mental-health work are also means of ensuring that transitioning—which can be a physically and emotionally taxing process for adolescents even under the best of circumstances—goes smoothly.
Scott Padberg, one of Edwards-Leeper’s patients, is a good example of how her comprehensive-assessment process looks for teenagers with a relatively straightforward history of persistent gender dysphoria and an absence of other factors that might complicate their diagnosis and transition path. I met Scott and his grandmother and legal guardian, Nancy, at a wrap place in Welches, Oregon, not far from where they live. It was a mild February day, so we sat in one of the pine booths outside the restaurant. Mount Hood’s massive snowcapped peak loomed nearby.
Scott Padberg, a 16-year-old patient of Laura Edwards-Leeper who went on cross-sex hormones and recently had a double mastectomy (Matt Eich)
Scott, a 16-year-old who radiates calm, explained that despite having been assigned female at birth, he simply never felt like a girl. “I guess I kinda felt different since I felt conscious of the fact that I was alive,” he said. For part of his childhood, that was fine with everyone around him. He was granted all the freedom he needed to express himself in a gender-nonconforming manner, from getting short haircuts to playing with stereotypically male toys like dinosaurs and Transformers. But the freedom didn’t last. When he was 7, his mom married a “super Christian guy” who tried to impose femininity on him. “It’s really degrading,” Scott said, to be forced to wear a dress when you’re a trans boy. (Scott’s mom divorced her devout husband two years later, and Nancy eventually took custody of Scott.)
Puberty brought bigger problems. Scott started developing breasts and got his period. “Everything just sucked, basically,” he said. “I was pretty miserable with it.” In 2015, when Scott was 13, Nancy took him to an assessment appointment with Edwards-Leeper. “She asked me about how I felt when I was younger—was I comfortable with my body? What did I tend to like or be interested in?,” Scott recalled. He said that getting on testosterone took what felt like a long time. (He was on puberty blockers for about a year.) But he said he understood that Edwards-Leeper was making certain he had considered a range of questions—from how he would feel about possibly not being able to have biological kids to whether he was comfortable with certain hormonal effects, such as a deeper voice. Scott told Edwards-Leeper that he was pretty certain about what he wanted.
Scott told me that overall, being on testosterone made him feel better, though also a bit more into “adrenaline-junkie stuff” than before. (There had been a recent incident involving Scott taking Nancy’s car for a spin despite not yet having his learner’s permit.) When I asked him about top surgery, which he was hoping to have early in the spring, he got about as animated as I saw him during our lunch. “Oh, it’s going to be so freeing,” he said. “I can change in the locker room!” In April I checked in with Nancy, and she said in an email that the surgery had gone well: “He is SO happy not to have to wear a binder!”
Scott’s assessment process centered mostly on the basic readiness questions Edwards-Leeper and Leibowitz are convinced should be asked of any young person considering hormones. But his was a relatively clear-cut case: He’d had unwavering gender dysphoria since early childhood, a lack of serious mental-health concerns, and a generally supportive family. For other gender-dysphoric young people, mental-health problems and family dynamics can complicate the transition process, though they are by no means, on their own, an indication that someone shouldn’t transition.
I met Orion Foss at a vegetarian café in the Dennison Place neighborhood of Columbus. Orion is an expressive 18-year-old with big eyes who is where Scott Padberg may be in a couple of years. Orion’s gender trajectory was a bit different, though. As a teenager, he identified as a lesbian and became involved in the local LGBTQ scene. He says that in 2014, when he was 14 years old and trans narratives were starting to show up more frequently on social media, he realized he was trans. He was also suffering from severe depression and anxiety at the time, which had led to self-harm issues, as well as what may have been an undiagnosed eating disorder. Orion believed that additional weight went straight to his hips and chest, accentuating his feminine features. At one point, he dipped down to 70 pounds.
A year or so after he realized he was trans, he told his mother, an ob-gyn, who took him to the thrive program at Nationwide, which had recently opened. (Leibowitz didn’t work there yet.) Orion met with two clinicians for an eight-hour assessment. He told me he was “definitely intimidated,” but if “you want to do something permanent to your body, you have to be absolutely positive that there’s no other way of doing it.”
At the time, Orion was initially upset that, because he was underage, thrive wouldn’t put him on hormones without the consent of both parents (his father had signed off, but his mother had not). He started sobbing when he found out. But the thrive team made clear that it was going to help him get where he wanted to be. In the meantime, a thrive therapist, Lourdes Hill, would work with Orion to address his anxiety and depression.
Looking back, Orion sees the value of this process. “If I had been put on hormone therapy when I didn’t have my identity settled, and who I was settled, and my emotions settled, it would have been crazy. ’Cause when I did start hormone therapy, hormones shoot your mood all around, and it’s not exactly safe to just shoot hormones into someone that’s not stable.” He ended up seeing Hill for weekly appointments, talking about not only his gender-identity and mental-health issues, but a host of other subjects as well. “She weeded through every possible issue with me that she could get to,” he said. “I’m glad she made me wait. And I’m glad the structure was there so I couldn’t just throw myself into something that probably would have made me worse off.”
Eventually, his mother, who was “very hesitant,” and was refusing to sign the paperwork for him to start hormones, came around. The thrive team helped her come to grips with the fact that the child she had always known as her daughter was going to become her son. “Lourdes was the driving force in that,” Orion told me in a follow-up email. “Spent a lot of time with me and my mother in therapy.”
When he was finally able to begin the hormone treatments, Orion said, he “immediately felt this weight off my shoulders.” His dosage was gradually increased and then, in May 2017, he got a double mastectomy. Orion’s transition has clearly had a profoundly beneficial effect. It’s changed the way he carries himself in the world. Before, “I would sit like this”—he slouched over—“and hide every possible female thing about me.” Now, he said, he can sit up straight. He feels like himself.
Orion Foss worked with the clinicians at Ohio’s THRIVE clinic on his mental health, his mother’s concerns, and, eventually, his transition. (Matt Eich)
Some parents struggle with the challenges of raising a TGNC child, and they can make gender clinicians’ already complicated jobs that much more complicated. Many, like Orion Foss’s mother, have trouble accepting the idea of their child transitioning. She, at least, came around. In other cases, parents not only refuse to help their child receive treatment but physically abuse them or kick them out of the house. (Reliable numbers for trans young people specifically are hard to come by, but LGBTQ youth are 120 percent more likely than their straight or cisgender counterparts to experience a period of homelessness, according to a study by Chapin Hall, a research center at the University of Chicago.)
But progressive-minded parents can sometimes be a problem for their kids as well. Several of the clinicians I spoke with, including Nate Sharon, Laura Edwards-Leeper, and Scott Leibowitz, recounted new patients’ arriving at their clinics, their parents having already developed detailed plans for them to transition. “I’ve actually had patients with parents pressuring me to recommend their kids start hormones,” Sharon said.
In these cases, the child might be capably navigating a liminal period of gender exploration; it’s the parents who are having trouble not knowing whether their kid is a boy or a girl. As Sharon put it: “Everything’s going great, but Mom’s like, ‘My transgender kid is going to commit suicide as soon as he starts puberty, and we need to start the hormones now.’ And I’m like, ‘Actually, your kid’s just fine right now. And we want to leave it open to him, for him to decide that.’ Don’t put that in stone for this kid, you know?”
Suicide is the dark undercurrent of many discussions among parents of TGNC young people. Suicide and suicidal ideation are tragically common in the transgender community. An analysis conducted by the American Foundation for Suicide Prevention and the Williams Institute, published in 2014, found that 41 percent of trans respondents had attempted suicide; 4.6 percent of the overall U.S. population report having attempted suicide at least once. While the authors note that for methodological reasons 41 percent is likely an overestimate, it still points to a scarily high figure, and other research has consistently shown that trans people have elevated rates of suicidal ideation and suicide relative to cisgender people.
Scott Leibowitz, a psychiatrist who treats children and adolescents in Columbus, Ohio, is a proponent of comprehensive assessments for young people seeking to transition. (Matt Eich)
But the existence of a high suicide rate among trans people—a population facing high instances of homelessness, sexual assault, and discrimination—does not imply that it is common for young people to become suicidal if they aren’t granted immediate access to puberty blockers or hormones. Parents and clinicians do need to make fraught decisions fairly quickly in certain situations. When severely dysphoric kids are approaching puberty, for instance, blockers can be a crucial tool to buy time, and sometimes there’s a genuine rush to gain access to them, particularly in light of the waiting lists at many gender clinics. But the clinicians I interviewed said they rarely encounter situations in which immediate access to hormones is the difference between suicide and survival. Leibowitz noted that a relationship with a caring therapist may itself be an important prophylactic against suicidal ideation for TGNC youth: “Often for the first time having a medical or mental-health professional tell them that they are going to take them seriously and really listen to them and hear their story often helps them feel better than they’ve ever felt.”
The conversations parents are having about gender-dysphoric children online aren’t always so nuanced, however. In many of these conversations, parents who say they have questions about the pace of their child’s transition, or whether gender dysphoria is permanent, are told they are playing games with their child’s life. “Would you rather have a live daughter or a dead son?” is a common response to such questions. “This type of narrative takes an already fearful parent and makes them even more afraid, which is hardly the type of mind-set one would want a parent to be in when making a complex lifelong decision for their adolescent,” Leibowitz said.
When parents discuss the reasons they question their children’s desire to transition, whether in online forums or in response to a journalist’s questions, many mention “social contagion.” These parents are worried that their kids are influenced by the gender-identity exploration they’re seeing online and perhaps at school or in other social settings, rather than experiencing gender dysphoria.
Many trans advocates find the idea of social contagion silly or even offensive given the bullying, violence, and other abuse this population faces. They also point out that some parents simply might not want a trans kid—again, parental skepticism or rejection is a painfully common experience for trans young people. Michelle Forcier, a pediatrician who specializes in youth-gender issues in Rhode Island, said the trans adolescents she works with frequently tell her things like No one’s taking me seriously—my parents think this is a phase or a fad.
But some anecdotal evidence suggests that social forces can play a role in a young person’s gender questioning. “I’ve been seeing this more frequently,” Laura Edwards-Leeper wrote in an email. Her young clients talk openly about peer influence, saying things like Oh, Steve is really trans, but Rachel is just doing it for attention. Scott Padberg did exactly this when we met for lunch: He said there are kids in his school who claim to be trans but who he believes are not. “They all flaunt it around, like: ‘I’m trans, I’m trans, I’m trans,’ ” he said. “They post it on social media.”
I heard a similar story from a quirky 16-year-old theater kid who was going by the nickname Delta when we spoke. She lives outside Portland, Oregon, with her mother and father. A wave of gender-identity experimentation hit her social circle in 2013. Suddenly, it seemed, no one was cisgender anymore. Delta, who was 13 and homeschooled, soon announced to her parents that she was genderqueer, then nonbinary, and finally trans. Then she told them she wanted to go on testosterone. Her parents were skeptical, both because of the social influence they saw at work and because Delta had anxiety and depression, which they felt could be contributing to her distress. But when her mother, Jenny, sought out information, she found herself in online parenting groups where she was told that if she dragged her feet about Delta’s transition, she was potentially endangering her daughter. “Any questioning brought down the hammer on you,” she told me.
Delta’s parents took her to see Edwards-Leeper. The psychologist didn’t question her about being trans or close the door on her eventually starting hormones. Rather, she asked Delta a host of detailed questions about her life and mental health and family. Edwards-Leeper advised her to wait until she was a bit older to take steps toward a physical transition—as Delta recalled, she said something like “I acknowledge that you feel a certain way, but I think we should work on other stuff first, and then if you still feel this way later on in life, then I will help you with that.”
“Other stuff” mostly meant her problems with anxiety and depression. Edwards-Leeper told Jenny and Delta that while Delta met the clinical threshold for gender dysphoria, a deliberate approach made the most sense in light of her mental-health issues.
Delta, a patient of Laura Edwards-Leeper who wanted to transition. Edwards-Leeper counseled her to take things slowly and to work on her co-occurring mental-health issues. Her gender dysphoria eventually lifted. (Matt Eich)
“At the time I was not happy that she told me that I should go and deal with mental stuff first,” Delta said, “but I’m glad that she said that, because too many people are so gung ho and just like, ‘You’re trans, just go ahead,’ even if they aren’t—and then they end up making mistakes that they can’t redo.” Delta’s gender dysphoria subsequently dissipated, though it’s unclear why. She started taking antidepressants in December, which seem to be working. I asked Delta whether she thought her mental-health problems and identity questioning were linked. “They definitely were,” she said. “Because once I actually started working on things, I got better and I didn’t want anything to do with gender labels—I was fine with just being me and not being a specific thing.”
It’s imperative to remember that Delta’s is a kind of story that can happen only in a place where trans people are accepted—and where parents, even skeptical ones like Jenny, are open-minded enough to take their kid to a clinician like Edwards-Leeper. In vast swaths of the United States, kids coming out as trans are much more likely to be met with hostility than with enhanced social status or recognition, and their parents are more likely to lack the willingness—or the resources—to find them care. But to deny the possibility of a connection between social influences and gender-identity exploration among adolescents would require ignoring a lot of what we know about the developing teenage brain—which is more susceptible to peer influence, more impulsive, and less adept at weighing long-term outcomes and consequences than fully developed adult brains—as well as individual stories like Delta’s.
Not everyone agrees about the importance of comprehensive assessments for transgender and gender-nonconforming youth. Within the small community of clinicians who work with TGNC young people, some have a reputation for being skeptical about the value of assessments. Johanna Olson-Kennedy, a physician who specializes in pediatric and adolescent medicine at Children’s Hospital Los Angeles and who is the medical director of the Center for Transyouth Health and Development, is one of the most sought-out voices on these issues, and has significant differences with Edwards-Leeper and Leibowitz. In “Mental Health Disparities Among Transgender Youth: Rethinking the Role of Professionals,” a 2016 jama Pediatrics article, she wrote that “establishing a therapeutic relationship entails honesty and a sense of safety that can be compromised if young people believe that what they need and deserve (potentially blockers, hormones, or surgery) can be denied them according to the information they provide to the therapist.”
This view is informed by the fact that Olson-Kennedy is not convinced that mental-health assessments lead to better outcomes. “We don’t actually have data on whether psychological assessments lower regret rates,” she told me. She believes that therapy can be helpful for many TGNC young people, but she opposes mandating mental-health assessments for all kids seeking to transition. As she put it when we talked, “I don’t send someone to a therapist when I’m going to start them on insulin.” Of course, gender dysphoria is listed in the DSM-5; juvenile diabetes is not.
One recent study co-authored by Olson-Kennedy, published in the Journal of Adolescent Health, showed that her clinic is giving cross-sex hormones to kids as young as 12. This presses against the boundaries of the Endocrine Society’s guidelines, which state that while “there may be compelling reasons to initiate sex hormone treatment prior to age 16 years … there is minimal published experience treating prior to 13.5 to 14 years of age.”
If you see gender-dysphoric 13- and 14-year-olds not as young people with a condition that may or may not indicate a permanent identity, but as trans kids, full stop, it makes sense to want to grant them access to transition resources as quickly as possible. Olson-Kennedy said that the majority of the patients she sees do need that access. She said she sees a small number of patients who desist or later regret transitioning; those patients, in her opinion, shouldn’t dictate the care of others. She would like to see a radical reshaping of care for TGNC young people. “The way that the care has been organized is around assuring the certainty and decreasing the discomfort of the professionals (usually cisgender) who determine if the young people are ready or not,” she told me. “And that’s a broken model.”
How best to support TGNC kids is a whiplash-inducing subject. To understand even just the small set of stories I encountered in my reporting—stories involving relatively privileged white kids with caring, involved families, none of which is necessarily the case for all TGNC young people in the United States—requires keeping several seemingly conflicting claims in mind. Some teenagers, in the years ahead, are going to rush into physically transitioning and may regret it. Other teens will be prevented from accessing hormones and will suffer great anguish as a result. Along the way, a heartbreaking number of trans and gender-nonconforming teens will be bullied and ostracized and will even end their own lives.
Some LGBTQ advocates have called for gender dysphoria to be removed from the DSM-5, arguing that its inclusion pathologizes being trans. But gender dysphoria, as science currently understands it, is a painful condition that requires treatment to be alleviated. Given the diversity of outcomes among kids who experience dysphoria at one time or another, it’s hard to imagine a system without a standardized, comprehensive diagnostic protocol, one designed to maximize good outcomes.
Experiencing gender dysphoria isn’t the same as experiencing anxiety or depression or psychological ailments, of course. But in certain ways it is similar: As with other psychiatric conditions, some people experience dysphoria more acutely than others; its severity can wax and wane within an individual based on a variety of factors; it is in many cases intimately tied to an individual’s social and familial life. For some people, it will pass; for others, it can be resolved without medical interventions; for still others, only the most thorough treatment available will relieve immense suffering. We recognize that there is no one-size-fits-all approach to treating anxiety or depression, and a strong case can be made that the same logic should prevail with gender dysphoria.
Perhaps a first step is to recognize detransitioners and desisters as being on the same “side” as happily transitioned trans people. Members of each of these groups have experienced gender dysphoria at some point, and all have a right to compassionate, comprehensive care, whether or not that includes hormones or surgery. “The detransitioner is probably just as scarred by the system as the transitioner who didn’t have access to transition,” Leibowitz told me. The best way to build a system that fails fewer people is to acknowledge the staggering complexity of gender dysphoria—and to acknowledge just how early we are in the process of understanding it.
This article appears in the July/August 2018 print edition with the headline “Your Child Says She’s Trans. She Wants Hormones and Surgery. She’s 13.”
Article source here:The Atlantic
0 notes
Text
9 Most Dangerous Food Additives Everyone Should Avoid (And Why)
Cheetos, hotdogs and gummy bears. They all have one point alike - they're all highly refined. While they definitely taste good, do you truly recognize just what you're eating?
Unless you pace the grocery shop aisles examining every single active ingredient tag (which you should be doing), opportunities are you have no idea what hazardous food additives you're placing inside your body.
Did you understand that greater than 3,000 food ingredients are contributed to US foods? For that reason, it's recommended you take on a tidy diet loaded with fruits as well as vegetables and prevent processed foods completely. Let's be genuine, you probably have at least a couple processed foods in your fridge and pantry right this minute.
When you get to for your boxed treats, there are a few "red flag" components you should be on the search for. Below are 9 of the most hazardous preservative that everyone ought to avoid.
1) Artificial Sweeteners
A lot of individuals take a breath a sigh of alleviation when they eat sweetening agents over sugar. If you are one of the many people who believe fabricated sugars are a 'healthier alternative,' I'm sorry to damage the news to you ... they're not!
Researchers say synthetic sweeteners could:
Enhance your appetite
Lead to weight gain
Cause inflammation
Cause digestive issues
Kill the great intestine germs in your gastrointestinal tract
Their impact on the body does not end there. Scientists have found the amino acids in aspartame (a prominent kind of sweetening agent) act in different ways compared to the amino acids in whole foods such as salmon, eggs or chia seeds. In this situation, the amino acids can actually assault your body's cells and mind cells, developing an extremely poisonous effect on the body.
When examining to see if your food includes sweetening agents, search for the following names:
Aspartame
Sucralose
Saccharin
Acesulfame
Neotame
* NOTE: These are just 5 of the many sweetening agents contributed to your foods.
2) Synthetic Trans Fats
There are numerous different kinds of fats. They consist of monounsaturated, polyunsaturated, saturated and also trans fats. You most definitely should not have a worry of fats. The body requires 'healthy fats' in order to work correctly. Healthy and balanced fats include monounsaturated and polyunsaturated fats.
Trans fats, on the various other hand, are 'unhealthy fats' as well as pose definitely zero health and wellness benefit. Actually, this kind of fat is understood to create inflammation and also raise bad cholesterol levels. Trans fats are additionally connected to heart problem, a damaged immune system, cancer cells, and also diabetic issues.
Trans fats are found in several fried foods as well as store-bought baked goods.
3) High Fructose Corn Syrup
You may have heard cases that high fructose corn syrup (HFCS) is no even worse for you compared to table sugar. Do not believe that for one 2nd! HFCS is not the very same as table sugar (sucrose) or fructose (located in several fruits).
HFCS is not a natural material and has been connected to:
Weight gain
Insulin resistance
Liver damage
Weakened immune system
Poor gut health
May lead to autoimmune disease
These are just 6 of one of the most common negative effects of consuming HFCS. The listing of frightening realities on HFCS absolutely doesn't end there.
4) Refined Vegetable Oils
When you initially listen to the term, 'vegetable oils,' you could really think they're healthy and balanced. After all, veggies are great for you! Fine-tuned veggie oils including canola, corn, soybean, cottonseed and safflower oils are much from healthy and balanced, though.
As the name 'improved' tells us, these oils are very refined. The oils are removed by high warmth, pressure, as well as chemical solvents. Without getting as well scientific, through processing the helpful antioxidants, vitamins and minerals are killed. Together with stripping the oil of its nutrients, dangerous preservatives are likewise contributed to these oils to develop a long rack life. I'll speak much more concerning dangerous preservatives in just a minute.
* It is necessary to keep in mind that when I utilize the term 'veggie oils' that I am NOT referring to raw olive oil and coconut oil. These are 2 extremely healthy and balanced oils. If you are making a dish that requires canola oil (or an additional sort of grease), you can quickly swap it out for extra virgin, cold-pressed olive oil.
When you are cooking, you will see that most baking recipes call for some kind of veggie oil. Instead of complying with those directions, you could quickly switch out vegetable oils for added virgin, cold-pressed olive oil.
Coconut oil is another wonderful oil for cooking.
5) Monosodium Glutamate (MSG)
If you ever get a headache after eating Chinese food, this may be why. MSG is a dangerous flavor booster that is often associated with Chinese food. Your plate of Lo Mein isn't the only location MSG is concealing. If you check out the component labels for sure icy suppers, canned foods, and also treat bags, you could be stunned to locate that it has MSG. There is even MSG in bouillon (the preferred, instant soup broth flavoring).
While the FDA proceeds to declare that MSG is safe, numerous specialists disagree. This taste enhancer is claimed to harm your body's cells, leading to different health issues consisting of learning disabilities, Alzheimer's illness, Parkinson's illness and also more.
6) GMOs
GMOs are around us. Roughly 80% of all packaged foods have GMOs. Do not think you're consuming GMO-free by preventing packaged foods, though. Several of the leading GMO plants include corn, canola, soybeans as well as sugar beets. GMO salmon is also being introduced into our supermarkets.
So why is this poor? Well, GMO means 'genetically customized organism.' To place it just - it's not an item of Nature, however instead a product of science. GMOs are utilized to 'enhance' the food we consume by making them prettier and also hardier. That does not imply healthier.
Although the United States Food and also Drug Administration (FDA) has regarded GMOs safe, eating GMO foods have been linked to:
An increase in food allergies
An increase in antibiotic resistance
Reproductive disorders
Additionally, it can be hard to spot GMO foods in your grocery store because the United States Division of Agriculture (USDA) does not need these foods to be identified. Some tips in order to help you avoid GMOs:
Grow your own crops
Buy foods classified GMO-free (some business include this on their items)
Go organic. By regulation, no greater than 5% of natural foods can consist of GMOs
7) Preservatives
Have you ever before checked out the shelf life of your preferred boxed foods or bag of chips? It looks like fast food never spoils. That's due to the fact that it's filled with preservatives. While manufacturers benefit from adding chemicals to our food, our wellness definitely does not.
Butylated hydroxyanisole (BHA) and butylated hydroxytoluene (BHT) are two generally used chemicals. In addition to lengthening your food's shelf-life, they could also influence your neurological system and also could possibly create cancer.
Sodium nitrite is another popular preservative found in cold cuts and also hot pets. This type of preservative has been linked to various sorts of cancers.
Then there's your soft drink. With such long shelf-lives, do not assume your favorite bottled sodas are preservative-free. They usually consist of a preservative called Salt benzoate, which could make kids hyperactive.
8) Artificial Flavors
Rule of thumb - anytime you see food with the name 'man-made' composed on it ... RUN! Synthetically flavored foods are loaded with abnormal chemicals that damage the body. Artificially flavored foods have actually been connected to digestive concerns and psychological health and wellness diseases.
9) Artificial Colors
Whether you're a youngster or a grown-up, people seem to enjoy colorful foods. I'm not speaking about red tomatoes and brilliant blueberries. I'm talking concerning synthetically tinted Skittles, Starbursts and gummy bears.
Every year, U.S. food suppliers add greater than 15 million extra pounds of man-made dyes into our foods. That's a whole lot of dye! Some dyes are recognized to be more unsafe compared to others. Some are linked to behavior health issue and others are connected to cancer.
Four of the worst offenders consist of:
Blue #1 and #2
These dyes are made use of in candy, beverages, and also pet food. It's been linked to mind tumors.
Red #3
This color is commonly located in sweet, fruit cocktail, maraschino cherries, cherry pie filling, as well as more. It's been linked to thyroid cancer.
Yellow #5
This color is used in sweet and grain. It's been linked to cancer and also behavior health issue in children.
Tips To Prevent These 9 Dangerous Food Additives
There are a number of means you can lower the quantity of artificial additive you place in your body. It starts with your grocery shopping routines. The ideal point you could do is stay clear of the center aisles as well as adhere to going shopping the boundaries. While the aisles are usually stocked with boxed foods, the boundaries are commonly where you will find fresh produce.
When picking your fruit and vegetables, it's best to purchase foods that do not have an ingredient tag. Bear in mind, actual foods do not have components. Think concerning it - a banana doesn't need an active ingredient tag due to the fact that it's merely a banana. It coincides with tomatoes, avocados, zucchini, etc.
To stay clear of hazardous GMOs and also chemicals, it's constantly a great idea to go natural. This is not to be confused with 'all-natural.' The terms 'natural' as well as 'organic' are not interchangeable. While 'natural' can suggest any kind of variety of things, '100% natural' guarantees you that your food is made without making use of harmful pesticides, GMOs, prescription antibiotics or artificial development hormones.
Since organic fruit and vegetables can be a little bit costlier, you could not desire to get all your foods organic. If that holds true, describe the complying with checklist that tells you which foods have the greatest quantity of chemicals:
Apples
Strawberries
Grapes
Celery
Peaches
Spinach
Sweet Bell Peppers
Nectarines
Cucumbers
Potatoes
Cherry Tomatoes
Peppers
Kale/ Collard Greens
Snap peas
Lastly, if you are buying boxed foods, make certain to review the ingredient label very thoroughly! That is the only means you will get a feel for what is inside your food. A general rule - if the product has a number of ingredients that you can not pronounce, don't eat it!
#cabbage diet#cholesterol diet#diet#diet recipes#dieting#fruit diet#health and wellness#metabolism diet#vinegar diet#wellness
0 notes
Last Seen Blogs

the-skooma-den
It's not a cave, It's a Den

akinnsworldsposts
AKİN

robertlv387
Robert L. Velazquez

chastiefxl-blog
A C E D I A.

whatwouldcatherinedo
Lovely Kate