#Virus incubation period
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The “We are the 99%” Tumblr blog became the slogan for the Occupy Wall Street movement.
Text
What is Human Metapneumovirus (HMPV)?
What is Human Metapneumovirus (HMPV)?
Human Metapneumovirus (HMPV) is a respiratory virus that can cause a range of symptoms, from mild cold-like signs to severe respiratory distress. It was first identified in 2001, making it a relatively new addition to the family of viruses known to affect humans. Despite its relatively recent discovery, HMPV has since been recognized as a significant contributor to respiratory illness worldwide, particularly in young children, the elderly, and immunocompromised individuals. Understanding the nature of HMPV, its symptoms, transmission, treatment, and prevention measures is essential to managing its impact on public health.
What is HMPV?
HMPV belongs to the Metapneumovirus genus, which is part of the Paramyxoviridae family. This family also includes other well-known respiratory viruses such as the measles virus, mumps virus, and respiratory syncytial virus (RSV). HMPV, however, is genetically distinct from these other pathogens and has its own set of characteristics.
The virus primarily infects the upper and lower respiratory tract and is a leading cause of respiratory infections in infants and young children. However, adults, particularly those with weakened immune systems or underlying chronic conditions, can also be affected. In fact, similar to other respiratory viruses, HMPV is known to circulate in seasonal patterns, with outbreaks often occurring in the fall and winter months, peaking around the same time as influenza and RSV infections.
Symptoms of HMPV Infection
Infection with HMPV can present with a range of symptoms, which may vary from mild to severe, depending on the individual’s age, immune status, and any underlying health conditions. In children, particularly those under five years of age, HMPV is one of the leading causes of respiratory illness, including bronchiolitis and pneumonia.
The symptoms of HMPV infection can include:
Upper Respiratory Symptoms:
Nasal congestion
Runny nose
Coughing
Sore throat
Lower Respiratory Symptoms:
Wheezing
Shortness of breath
Rapid breathing
Chest tightness
General Symptoms:
Fever
Fatigue
Headache
While most individuals recover from HMPV infections within a week or two, some may develop more severe respiratory complications. The elderly, infants, and those with weakened immune systems or preexisting lung diseases such as asthma or chronic obstructive pulmonary disease (COPD) are at greater risk for developing serious illness.
Transmission of HMPV
HMPV is transmitted primarily through respiratory droplets when an infected person coughs, sneezes, or talks. It can also spread through direct contact with contaminated surfaces or by touching the mouth, nose, or eyes after touching surfaces that have been exposed to the virus.
Like other respiratory viruses, HMPV is highly contagious, and outbreaks are common, particularly in settings where close contact occurs, such as schools, daycares, hospitals, and nursing homes. The virus can remain viable on surfaces for several hours, making hand hygiene and disinfecting surfaces critical in preventing transmission.
Who is at Risk?
While HMPV can infect individuals of all ages, certain groups are at higher risk for severe illness or complications. These groups include:
Infants and Young Children: Infants, particularly those under one year of age, are more susceptible to severe respiratory symptoms, including bronchiolitis and pneumonia. In fact, HMPV is one of the leading causes of hospitalization in young children for respiratory illnesses.
Elderly Adults: Older adults, especially those with underlying health conditions such as COPD, asthma, or heart disease, are more likely to experience severe symptoms of HMPV infection.
Immunocompromised Individuals: Those with weakened immune systems, including individuals undergoing cancer treatments or those with conditions like HIV/AIDS, are at increased risk of more severe disease.
People with Chronic Respiratory Conditions: Patients with pre-existing respiratory conditions are also more likely to experience complications, including exacerbations of asthma or COPD.
Diagnosis of HMPV Infection
Diagnosing HMPV infection involves assessing clinical symptoms and performing laboratory tests. Given that HMPV shares symptoms with other respiratory infections like the flu, RSV, and the common cold, a detailed medical history and clinical examination are essential for diagnosis.
Laboratory tests that may be used to confirm HMPV include:
Polymerase Chain Reaction (PCR): This test detects the virus's genetic material in respiratory samples, such as a nasal swab, throat swab, or sputum.
Immunofluorescence: This method identifies HMPV proteins in respiratory secretions.
Viral Culture: Although less commonly used due to the time it takes, this test grows the virus from a sample to confirm the presence of HMPV.
In some cases, chest X-rays or other imaging techniques may be used to assess the extent of lung involvement, particularly if pneumonia or bronchiolitis is suspected.
Treatment of HMPV
Currently, there is no specific antiviral treatment for HMPV infection. Management is primarily supportive and focuses on alleviating symptoms. In most cases, individuals with mild illness recover with rest, hydration, and over-the-counter medications to reduce fever and ease discomfort.
For more severe cases, especially in young children or high-risk adults, hospitalization may be necessary. Treatment options for hospitalized patients may include:
Oxygen therapy to help maintain adequate oxygen levels in the blood.
Nebulized treatments to relieve wheezing or improve airflow in the lungs.
Intravenous (IV) fluids to prevent dehydration, especially if the individual is unable to drink enough fluids.
Mechanical ventilation in extreme cases, where patients have difficulty breathing on their own.
Antibiotics are not effective against viral infections like HMPV, so they are not used unless there is a secondary bacterial infection.
Prevention of HMPV
Because there is no vaccine for HMPV, prevention relies on reducing the risk of exposure and minimizing transmission. Strategies to prevent HMPV infection include:
Good Hygiene Practices:
Frequent handwashing with soap and water for at least 20 seconds, particularly after coughing or sneezing.
Using alcohol-based hand sanitizers when soap and water are not available.
Avoiding touching the face, especially the eyes, nose, and mouth.
Respiratory Hygiene:
Covering the mouth and nose with a tissue or elbow when coughing or sneezing.
Disposing of tissues immediately and washing hands afterward.
Avoiding Close Contact with Sick Individuals:
Avoiding contact with individuals who are showing symptoms of a respiratory illness, particularly in high-risk settings such as hospitals or daycare centers.
Disinfecting Surfaces:
Regularly cleaning and disinfecting frequently touched surfaces, such as doorknobs, light switches, and toys in childcare settings.
Conclusion
Human Metapneumovirus (HMPV) is an important respiratory virus that can cause a range of respiratory illnesses, particularly in children, the elderly, and individuals with weakened immune systems. While there is no specific antiviral treatment or vaccine available for HMPV, supportive care is effective for most patients. Prevention measures, including good hygiene, respiratory hygiene, and minimizing contact with infected individuals, remain the most effective means of reducing the spread of HMPV. As more research is conducted into the virus, we may gain a better understanding of its behavior and develop better diagnostic, therapeutic, and preventive strategies to manage its impact on global health.
#Human Metapneumovirus#HMPV infection#Respiratory illness#Respiratory virus#Pneumonia#asthma#health issues#Cold-like symptoms#Viral respiratory disease#RNA virus#Viral load#Diagnosis of HMPV#HMPV treatment#Preventing HMPV spread#Vaccine research#HMPV epidemiology#HMPV symptoms#HMPV mutations and variants#Virus incubation period
0 notes
Text
Incubation Periods List
Hi all!
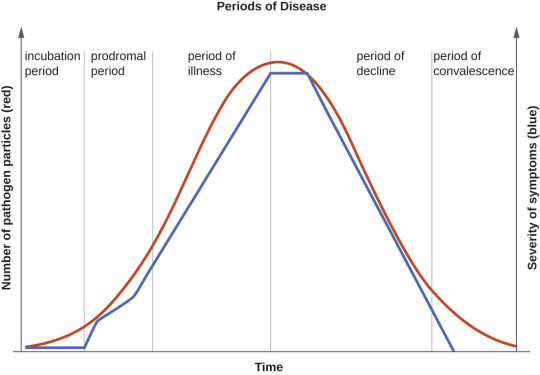
The following is a list of incubation periods for various infectious diseases for all your writing needs. An incubation period is the amount of time between exposure to an infectious agent (bacteria, virus, protozoa or prion) and the person having the first symptoms of the resulting illness. Knowing this is helpful in creating a timeline for your story.
Anthrax: Incubation period of 1-60 days
Avian Flu: Incubation period 3-9 days
Botulism: Incubation period 12-72 hours
Chikungunya: Incubation period 3-7 days
Chlamydia: incubation period 7-21 days
COVID-19: Incubation period 5-10 days
Creutzfeldt-Jacob Disease: Incubation period 10-20 years
Dengue: Incubation period 5-7 days
Diphtheria: Incubation period 2-5 days
Ebola: Incubation period 2-21 days
Hantavirus: incubation period 1-8 weeks
Hepatitis A: incubation period about 28 days
Herpes: Incubation period 2-12 days
Herpes Zoster/Varicella (Chickenpox): Incubation period 14-16 days
Herpes Zoster (Shingles): Incubation period- technically none, as this is a reactivation of the virus that causes chickenpox
HIB: Incubation period 2-10 days
HIV: Incubation period 1-6 weeks to prodrome, approximately 10 years to AIDS
Influenza: Incubation period 1-4 days
Legionnaires Disease: Incubation period 5-6 days
Leprosy: Incubation period 9 months to 20 years
Lyme Disease: Incubation period 3-30 days
Malaria: Incubation period 7-30 days
Measles: Incubation period 10-12 days
Meningitis, Bacterial: Incubation period 2-10 days
Meningitis, Viral: Incubation period 3-10 days
Monkeypox: Incubation period 1-2 weeks
Mumps: Incubation period 16-18 days
Norovirus: Incubation period 12-48 hours
Pertussis: Incubation period 7-10 days
Plague: Incubation period 2-8 days
Pneumococcal Pneumonia: Incubation period 1-3 days
Polio: Incubation period 7-10 days
Q-Fever: Incubation period 2-3 weeks
Rabies: Incubation period 20-90 days
RSV: Incubation period 4-6 days
Smallpox: Incubation period 7-17 days
Syphilis: Incubation period 10-90 days
Tetanus: Incubation period 3-21 days
Tuberculosis: Incubation period 2-10 days
Typhoid: Incubation period 6-30 days
Typhus: Incubation period 1-2 weeks
West Nile Virus: Incubation period 2-6 days
Yellow Fever: Incubation period 3-6 days
Zika: Incubation period 3-14 days
177 notes
·
View notes
Text
Reference archived on our website
Published in 2023. Proof positive that just breathing spreads covid over a large area. Mask up. Ventilate. Clean the air.
Summary Background Effectively implementing strategies to curb SARS-CoV-2 transmission requires understanding who is contagious and when. Although viral load on upper respiratory swabs has commonly been used to infer contagiousness, measuring viral emissions might be more accurate to indicate the chance of onward transmission and identify likely routes. We aimed to correlate viral emissions, viral load in the upper respiratory tract, and symptoms, longitudinally, in participants who were experimentally infected with SARS-CoV-2.
Methods In this phase 1, open label, first-in-human SARS-CoV-2 experimental infection study at quarantine unit at the Royal Free London NHS Foundation Trust, London, UK, healthy adults aged 18–30 years who were unvaccinated for SARS-CoV-2, not previously known to have been infected with SARS-CoV-2, and seronegative at screening were recruited. Participants were inoculated with 10 50% tissue culture infectious dose of pre-alpha wild-type SARS-CoV-2 (Asp614Gly) by intranasal drops and remained in individual negative pressure rooms for a minimum of 14 days. Nose and throat swabs were collected daily. Emissions were collected daily from the air (using a Coriolis μ air sampler and directly into facemasks) and the surrounding environment (via surface and hand swabs). All samples were collected by researchers, and tested by using PCR, plaque assay, or lateral flow antigen test. Symptom scores were collected using self-reported symptom diaries three times daily. The study is registered with ClinicalTrials.gov, NCT04865237.
Findings Between March 6 and July 8, 2021, 36 participants (ten female and 26 male) were recruited and 18 (53%) of 34 participants became infected, resulting in protracted high viral loads in the nose and throat following a short incubation period, with mild-to-moderate symptoms. Two participants were excluded from the per-protocol analysis owing to seroconversion between screening and inoculation, identified post hoc. Viral RNA was detected in 63 (25%) of 252 Coriolis air samples from 16 participants, 109 (43%) of 252 mask samples from 17 participants, 67 (27%) of 252 hand swabs from 16 participants, and 371 (29%) of 1260 surface swabs from 18 participants. Viable SARS-CoV-2 was collected from breath captured in 16 masks and from 13 surfaces, including four small frequently touched surfaces and nine larger surfaces where airborne virus could deposit. Viral emissions correlated more strongly with viral load in nasal swabs than throat swabs. Two individuals emitted 86% of airborne virus, and the majority of airborne virus collected was released on 3 days. Individuals who reported the highest total symptom scores were not those who emitted most virus. Very few emissions occurred before the first reported symptom (7%) and hardly any before the first positive lateral flow antigen test (2%).
Interpretation After controlled experimental inoculation, the timing, extent, and routes of viral emissions was heterogeneous. We observed that a minority of participants were high airborne virus emitters, giving support to the notion of superspreading individuals or events. Our data implicates the nose as the most important source of emissions. Frequent self-testing coupled with isolation upon awareness of first symptoms could reduce onward transmissions.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
47 notes
·
View notes
Text
"Today, December 20, marks the official end of the Marburg Virus Disease outbreak in Rwanda. It has been 42 days – two full incubation periods – since the last confirmed case left the national Marburg treatment centre after testing negative.
In previous outbreaks, Marburg, which is caused by a virus related to Ebola, has killed up to 88 per cent of people infected. And Rwanda had never seen this disease within its borders before the current outbreak began in September. Despite Rwandan physicians having never encountered it before, the mortality rate observed in this outbreak is under 23 per cent – the lowest-ever death rate for a Marburg outbreak in Africa.
While the virus initially spread fiercely in two major hospitals in the capital Kigali and among family members of one of the initial cases, Rwanda’s rapid response, with implementation of strict infection prevention and control, isolation and containment of cases, prompt initiation of aggressive supportive care, delivery of investigational therapeutics and vaccines, and tracing and monitoring of contacts quickly brought the outbreak under control. The rate of new cases halved between the outbreak’s second and third weeks and dropped by around 90 per cent thereafter.
One of the most remarkable aspects of this response was an international effort, initiated and led by the Rwandan government, to administer thousands of doses of a promising experimental vaccine to front-line health workers under a clinical trial protocol, with the first subjects vaccinated in a remarkably short timeframe.
...
Rwanda, for its part, has invested heavily in its healthcare system and has incorporated epidemic preparedness into its national health policies. Rwanda has well-trained medical staff working in well-run hospitals and community-based health services. It has been investing in technology-based disease surveillance systems and its laboratories can handle fast, accurate diagnostic testing at scale.
In early September, after months of planning, Rwandan scientists and health officials joined CEPI and other private sector partners to walk through a “tabletop exercise” about the 100 Days Mission. It was through this in-person training exercise that key relationships between disease outbreak experts, Rwandan health authorities and researchers, vaccine developers and clinical trial specialists were cemented.
...
We also have no doubt that with the right focus and funding, such nationally-led, globally-supported, life-saving responses to novel disease outbreaks could be accomplished by any government in any region. By taking a proactive approach and using the 100 Days Mission as a game plan, all countries can get ahead of epidemic and pandemic threats and neutralise their catastrophic potential."
Read the full piece here: https://www.telegraph.co.uk/global-health/science-and-disease/partnerships-preparedness-halted-rwanda-marburg-outbreak/
https://www.telegraph.co.uk/global-health/science-and-disease/partnerships-preparedness-halted-rwanda-marburg-outbreak/
42 notes
·
View notes
Text
CW: pet illness/death
PSA: Flayers and Destroyers are not healthy necrons!
With this summer being an Awakening, we’re going to be seeing a huge uptick in surprise necron owners as this year’s tombs wake up. With that in mind I feel the need to post my traditional reminder!
Healthy necrons will not tolerate organic material in their territory, but if properly cared for will usually keep their cleaning to their tomb complex. If you begin to notice your necrons removing organic material beyond their tomb this may be a sign that your colony has contracted the Destroyer Plague. It is imperative that you isolate any afflicted necrons as soon as possible to curb the spread of the infection.
Similarly, if you notice wildlife beginning to take root in your necrons’ tomb it may be a sign of Flayer infection. Unlike Destroyer infected however, Flayer Virus infected necrons take time to show symptoms. This long incubation period means that by the time you’ve noticed the deterioration of the tomb it’s likely already too late.
There’s been a disturbing trend on social media lately pushing these poor skeletons as “badass” and “edgy”. They are not. These creatures are sick and represent a danger to themselves, their tombs, and their environment.
Making the decision to put down my Overlord was the hardest thing I’ve ever had to do, but it was that or lose the whole tomb.
Sometimes the only thing you can do for your pet is to ease them on their way.
#space marine husbandry#necrons#warhammer 40k#this has been in my brain all day and it needs to get out#yes necrons are like cicadas why do you ask?
78 notes
·
View notes
Text
See You Again
Chapter 2: Polestar
Jason Todd x f!reader
You and the Red Hood escape the laboratory.
[A/N]: This is the second of the two chapters I had already written. I just started writing the third chapter and putting down my thoughts for the rest of the story...oops...
read here on ao3
<< previous || next >>
masterlist
STAR Laboratories Los Angeles
9:52:03 PM PT
The Coffin
“Well, that can’t be good.” You mutter to yourself, yanking out the syringe with a hiss. When your soldier had yielded, you thought you could slip away from him. But his sudden fake-out had shifted both of your positions, creating a window for the Bat to shoot him. The bullet had come so close to your face, you had thought you could feel it brush past you and embed itself in the soldier’s exposed neck.
The bullet could have just as easily grazed you, even killed you, had you been just an inch too close.
You shifted your gaze to the figure in the red helmet. You hadn’t gotten the chance to examine them up close—they were tall and heavily built, even with armor on, and sported a weathered brown leather jacket that covered the huge red bat symbol emblazoned on their chest plate. “You’re Red Hood, right?”
“That’s me.”
“What are you doing in LA? Aren’t you supposed to be from Gotham?” The Red Hood let out a modulated chuckle. You thought this would go down as your weirdest day on the job, making one of Gotham’s most ruthless crime fighters chuckle.
“I wanted to check out the warm weather here in Cali.” Something in Red Hood’s tone and posture shifted. “Now, what’s going on with that syringe?”
“Ah. Well, this was supposed to be a dose of a certain virus for the lab animals we’re testing on,” you explained.
“And this virus, it’s…”
“The Polestar virus,” you sighed. “Unearthed from somewhere deep in the Arctic, inside some early human mummies who carried the virus.” You let out a weak chuckle. “We knew it had the potential to be sold on the black market as a bioweapon should it fall into the wrong hands, but we weren’t aware that the risks were so high. And now, the virus is in my system.”
“Are you feeling anything right now? What are the virus’s symptoms? What’s its incubation period?” His modulated voice was surprisingly soft, yet urgent.
“This virus is bad news. We found that it’s pretty fast acting, and…” You spared another glance at the syringe in your hand. “...the symptoms aren’t pretty.”
“How fast?”
“This dose is meant for a test subject that’s a fraction of my body mass. I’ll be dead in two or three hours, give or take.”
“And the symptoms?”
“Necrosis. A new kind that we haven’t named yet. The virus consumes soft tissue and leaves behind a metallic residue. We believe it’s because the virus leaches metals and minerals from the body and aggregates it, beginning with the extremities.” The Red Hood reached forward cautiously, as if he was afraid of startling you. He gently pulled back the fabric of your coveralls that the soldier had so unceremoniously ripped open and ghosted his gloved fingers over where the needle had once been. The blood vessels around the wound had already become blackened and distended.
“We have to get you to a hospital.” You shook your head.
“We can’t. This research isn’t public knowledge.” You hoisted yourself up, tucked in your coveralls, and adjusted your respirator like nothing had happened. “I’m already a target as it is.” You stepped over the black-clad form of one of the soldiers Red Hood felled.
“Are there any treatments?” You picked your way through the Coffin to the freezers.
“They’re still in development, but the vaccine should slow it down.” You punched some numbers into the keypad and put your index finger to the scanner on the door and the freezer doors eased open automatically. You strode over to the shelf where you had hurriedly stashed the vials and syringes, the glass and metal clouded from the cold. The vaccine was crystal pink, you realized, like the color of the phenolphthalein titration you had done back in high school. You had handled both the buret and the Erlenmeyer flask because Jason couldn’t get it right, and in return, he had done all of the calculations for the lab report. Turning over the vials in your hand, you wondered why you were reminiscing about Jason during this time. The thought made your heart squeeze a little bit.
Jason Todd had been gone for so long. The hollowness that Jason’s absence had carved out of you seemed to sigh achingly. Years on, that hollowness was still there, not as hungry as it had been at first but smaller, still present. It still gnawed on your consciousness from time to time, on his birthday or on the day the Joker took him from you.
When you returned from the freezer, Red Hood was preparing a large metal-lined briefcase that he had taken from the incapacitated—dead?—men on the ground. He had already filled it partially with devices and weapons he had taken off of the soldiers.
“Are those the virus samples?” He inquired.
“Yeah,” you replied. “Vaccines, too. They’re labeled as such, and the vaccines are pink while the virus suspension is cl—”
“Pack them up. We have to get out of here before the police come.” His request startled you.
“Are you serious? This is property of STAR Labs and the CDC—”
“That’s been compromised. Neither you nor the samples are safe here. The police will be of no help, and they’re gonna keep sending people after you and those syringes unless we get you somewhere safe.” He gestured at the tray in your hands. “You need treatment, too. Somewhere they can’t find you.” You sighed heavily, setting the tray on a countertop.
“You’re right. I’m carrying the virus right now, and I’m dangerous. STAR Labs is probably gonna terminate me and the CDC will whisk me away or something. People come after me. But I can’t compromise the Polestar program.”
“It’s already been compromised. Now pack that shit up and let’s get out of here.” You flitted around the Coffin in search of something to store the samples in. You were scooping ice into a Styrofoam case when your comms unit fizzled to life again.
“This is the LAPD, we’ve been alerted of a break-in at STAR Labs. We request that all STAR Labs employees still in the building evacuate immediately. That is an order. Repeat, that is an order.”
“Shit, we gotta go,” Red Hood muttered. You grabbed your comms and tucked the Styrofoam case awkwardly under your arm and followed him out of the Coffin and into the ruins of decon and aseptics—you had been in the Coffin for hours, and the sight of the wreckage and your coworkers in aseptics now slumped over their devices made your stomach drop. “No time for sightseeing. Hurry up.” You pushed yourself into a full sprint, stumbling in your PPE along the concrete and corrugated steel of the basement. You followed the Red Hood into the emergency stairwell. Peering through the glass of the door to the ground floor, you saw SWAT officers milling about.
“SWAT team, start sweeping the second floor.”
“Shit—” You and Red Hood hurried up the stairs, the contents in your arms rattling in its Styrofoam case.
“Guess we aren’t leaving that way. Know any other escape routes in this building?”
The top floor—your floor. The Polestar program’s home.
You didn’t want to know what kind of destruction the soldiers had left in their wake.
“Top floor. Only way out would be the roof,” You answered.
“Roof it is.” After climbing some more flights of stairs and monitoring your comms unit for any more activity, you decided to wrench open the door to the sixth floor, breathing laboriously—when was the last time you had done this much cardio? You led the Red Hood over to a service elevator—not accessible without clearance, you explained to him—scanned your ID, and pulled him in. Once it reached the top floor, the elevator dinged and opened its doors, the hallway blessedly clear. You and Hood skulked down the corridor, which ended with the door to the Polestar offices. Hood opened the door and swept the room for hostiles before waving you in.
Your heart sank when you saw what had become of the Polestar lab.
“No…” you whispered. The laboratory had been completely wrecked. Glass fragments and papers were strewn on the floors. Pieces of equipment were left broken and overturned, spilling their contents among the mess.
Then you saw the bodies.
You caught sight of Dr. Davis’s crumpled form on the floor, next to the comms he had used to warn you of the impending disaster. The comms unit looked like it had been crushed underfoot, exposing wiring and circuitry among shards of its outer plastic shell. You made a step towards Dr. Davis’s body, but froze when you saw the red stain on his back and the blood pooling onto the floor.
“They…” You felt Hood’s gloved hand on your shoulder, gently guiding you away from the destruction. “...they killed everyone.”
“I’m sorry.”
“This is…this is horrible. Unbelievable.” Your pulse quickened with your breath. You felt the tears begin to form, and your vision grew misty. “I can’t believe it. They killed everyone.” You thought you had known grief and death. But this was different—seeing your colleagues slaughtered, their blood drying before you, made you feel faint. And yet, you felt wholly ablaze with
“Hey…” Shouts sounded from the stairwell. Your chest felt tight and your head was turning fuzzy. “...hey, hey. We gotta move.” The hand on your shoulder was not so gentle anymore, insistently pulling you toward the gaping hole in one of the windows. He handed—more like shoved—the briefcase he was holding into one of your hands and produced a terrifying-looking grapple gun from somewhere on his utility belt. “Don’t drop it,” was all he said before he wrapped an arm around your waist. Your arms instinctively flew around his shoulders, holding onto him, your Styrofoam box and his briefcase for dear life, and then you were airborne.
You squeezed your eyes shut as you soared over the street, which had become choked with squad cars and assault vehicles. You gasped in surprise when you felt yourself change direction as Hood gently and skillfully hoisted you over the ledge of a neighboring building’s rooftop.
“The first time is always the worst.”
“That’s implying that this isn’t the last,” You heaved out. “Holy shit. Did they see us?”
“Don’t think so. We’ll wait here, I’ll…” You didn’t hear the rest of the vigilante’s statement. The adrenaline from the jump was beginning to wane and you felt the burden of the virus and the sights you had stumbled upon while escaping the laboratory coming on again.
“Hey." Red Hood moved to catch you as you slumped over. “Hey, can you hear me?” Illuminated by the city lights, he caught sight of your badge from where it hung on your PPE. Your name was printed in neat black font next to an unmistakable portrait.
Under his helmet, the Red Hood’s breath caught in his chest.
“...Y/N?”
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
[A/N]: That's all I've got for now. Hope you enjoyed! x
#jason todd x you#jason todd x reader#red hood x reader#red hood x you#red hood#the red hood#jason todd#dcu
59 notes
·
View notes
Text
Viral shedding by asymptomatic people may represent a subset of total infections, but uncertainty remains regarding how much they contribute to totals.
Viral shedding may antedate symptoms, usually two days.
Viral titers are highest in the earliest phases of infection, 1-2 days before the onset of symptoms, and then in the first 4-6 days of illness in patients without immunosuppression.
When Is COVID-19 the Most Contagious?
Researchers estimate that people who get infected with COVID-19 can spread it to others 2-3 days before symptoms start and are most contagious 1-2 days before they feel sick.
&
How long after exposure will you test positive for COVID-19?
Depending on which COVID-19 variant you've been exposed to, you may test positive 3-5 days later. If you've been exposed to the virus but don't have any symptoms, wait for 5 days before you get tested. If you test too early and you do have COVID-19, you may falsely test negative.
#not news#just info#covid spread#covid#data#info#resources#viral load#viral shedding#asymptomatic spread#presymptomatic infection#incubation#covid incubation period#covid testing#testing
39 notes
·
View notes
Note
This is a strange question, but when it comes to masking, should we technically have always masked in public before COVID hit? Like, the flu used to be a big epidemic, but now we have vaccines and don't mask for it. I know there's still a COVID epidemic going on, but will there ever be a time to stop masking for that like we used to in your opinion? Is it best to be safe and just mask regardless of any recent/current pandemic to keep down the odds of catching or spreading any type of illness?
i mean, you can't compare covid and the flu. the flu is a respiratory virus that, while deadly, tends to only effect the respiratory system. it's true that anything including a cold can trigger dysautonomic conditions/symptoms, but nothing comes close to the disabling rate that covid has.
covid is a virus that affects every single organ, including the brain and heart. it's way scarier than the flu, and at present, way harder to manage/prevent due to frequent mutation, incredibly high r0, and the fact that it lingers in the air for hours after the infected person has shed virus.
flu vaccines are the result of decades of medical advancement, tons of time and effort has gone into tracking and predicting flu strains and rolling out vaccines. covid is still way too new for that despite mutating less than the flu.
whether you should be masking or not really depends on if you want to give someone else your viruses. like, yeah, if you weren't masking before during flu season, especially if you weren't getting your flu shot, if you've ever had the flu, you have 100% given it to someone else. the incubation period can last up to 5 days and, like covid, you can be contagious the whole time without a single symptom.
i wasn't masking then because, like, i was just raised in a world where the flu exists and so i just kind of assumed anyone who wanted to avoid it would be vaccinated & not crowding out indoors during the fall and winter. and because, like, while the flu can very much hospitalize, most people recover from it relatively unscathed. those who don't tend to take the proper precautions because that's what life is like when you're disabled, you have shit down to a system.
covid isn't like that tho. it does not matter who you are, covid can and will quite literally rot your brain and make your organs fail. covid has completely destroyed the cognitive function of half the population and it does not discriminate no matter how healthy or fit you are. no one is safe from it, even me fully vaccinated and wearing a kn100, a bitch who no longer eats out or attends events or does anything that might put me at risk. it could get me tomorrow and disable me for life.
like. i need to ask you why you're asking me. i'm not a medical professional, nor am i some holy beacon with all the right answers, i am just a tumblr user. my personal moral code is just that--personal. i will mask until it is safe. both for me, and for everyone else. i am a leftist, my actions and politics are rooted in empathy, masking is a no brainer. it's uncomfortable and i miss makeup but like... when i was 4 i used to dream myself a knight slaying beasts in the name of a vast kingdom because i wanted to be a hero who fought the good fight. and now i'm 29 and it turns out that's less 'big fucking sword' and more 'do a small thing that inconveniences you to stop people from dying.' it's literally not even a question.
why are you asking me, man? what do you wanna do? do you wanna ensure you don't give randos at the grocery store a preventable illness? then, like, yeah. wear a mask. just whenever.
i'm taking this thang off as soon as it stops being a hazard to my fellow man tho i fucking LOVE being sick gimme that sweet sweet fic insp omnomnom
13 notes
·
View notes
Text
@hungarianmudkip69 recently asked @vaspider about the spread of HIV. The excellent discussion there focused largely on qualitative aspects, notably what was going on socially in the 1970s and 80s, HIV's subtlety and long incubation periods, and exponential growth (along with a great refutation of accidental needle sticks as a dominant vector).
I've got a math and physics background - I have some extremely relevant intuition, but I still prefer being able to find real-world numbers to confirm that I haven't misapplied it. I encourage checking out all the links in this post; there's a lot of great information!
We can't literally go back in time and test everyone for HIV, but it is possible to model and estimate, e.g. this 2021 report from the CDC (US-only).
The second graph of figure #2 is very close to what we discussed:

(MMSC is male-to-male sexual contact and IDU is injection drug use; see the article for other details.)
Again, these are estimates, so we can't take the exact numbers as fact, but let's look at the big picture. HIV likely first arrived in the US around 1970; it first gained public attention in 1981, when the CDC reported cases of what we now call AIDS. At that point, the estimate is an order of magnitude of tens of thousands of HIV infections.
The original asker was interested in the behavior of a "patient zero" (see also "Debunking the Myth of Patient Zero", an excellent video linked in that thread). These numbers help us see how little effect one hypothetical person's behavior could have had on the end result. As long as the virus was transmitted at all, it was going to reach the highest-risk populations eventually, and spread once there, whether it took one hop or ten. It was also essentially impossible to notice the pattern and infer the existence of HIV/AIDS in the US until multiple people in the same community developed AIDS and contracted unusual infections - which most likely means that it's reached that high-risk population, and ten years have passed.
Tens of thousands of infections is simply the result of exponential growth during those ten years; stopping it from becoming an epidemic would've required everyone's behavior to have changed. Different behavior, different transmission, different number of hops early on would more likely have changed how long it took to spread widely enough to become noticeable, not whether it did. (An unfortunately familiar concept, in the year 2023.)
The authors also mention that "trend data comparing subpopulations is likely to be robust for each period examined", so let's look back at those individual lines. Injection drug use (IDU) actually was a fairly significant means of transmission by the 1980s, and by the mid-80s, the spread among gay/bi men (MMSC) was beginning to decline. At the end of the decade, IDU may even have passed MMSC. Simultaneously, transmission was still rising among straight people. It shouldn't be too surprising that straight sex became significant; there are rather a lot of straight people!
The CDC also has us covered for a more current picture, as of 2017-2021 in the US:

This does vary greatly by country. Notably, as of 2022 in England, 49% of new diagnoses were among heterosexuals, compared to 45% among gay/bi men. (Do keep in mind that there are far more straight people, so still, a far higher fraction of gay/bi men were diagnosed.)
I personally find that I get the best understanding when I'm able to combine some direct evidence/data with an understanding of the history and social forces; hopefully this piece helps at least one person out in that way!
[Finally, as a footnote: trans women also exist (hi I'm one) and have historically been at high risk. I am unsure to what extent trans women are omitted versus misgendered in the above data. I wanted to focus on historical estimates over time here, and unfortunately wasn't able to find that for trans women, but this review article links to and summarizes some data from two meta-analyses.]
124 notes
·
View notes
Text
Pretty sure it’s COVID. So let’s talk science, history, statistics, politics and facts. It’s got me a little rattled. I’ve had COVID at least once before. I slept 48 hours, dealt with flavorless food for a week and it was gone. The incubation period was a little over a week. This time, I presumably got it from Mrs. Doc who came down with it first. Within 12 hours both I and our youngest got it. We may all have been exposed at the same time, given her weakened immune state. Hard to say. But 12 hours is lightning fast. I then gave it to an employee. I try to never breathe on people, as I have a thing about being breathed upon. Still, standing shoulder to shoulder with him, within 48 hours he got it.
Viral infections have no cure. No vaccine. A vaccine is made up of dead, crushed cell parts of the bacterium, injected into the host (you and me), it allows the bodies soldiers a snapshot of what to look for so when it sees it or any mart of it, it can isolate and destroy it. mRNA doesn’t do that at all. It modifies YOUR genetic markers, changing you, hopefully to be resistant to the virus. That in my not so expert opinion is a wildly dangerous theory that should NEVER have been tested on the population.
So, 12-48 hours incubation. Where else have we seen this? 1918 with the Spanish Flu. That too was a Corona/SARS virus. It was a naturally occurring hybrid of swine and avian flu. The incubation period was an estimated 12 hours. Diagnosed, the patient was dead within 12 hours. It attacked the young, vibrant and healthy. Starting with cold like symptoms, observers witnessed a plaque build up of White Blood Cells presenting as mucous on the back of the throat that quickly spread to the bronchioles rendering them worthless. The patients would turn a deep purple to black color and then, just prior to death, all of that mucous/WBC plaque would simply vanish. They literally suffocated. In 1918, the average daily death toll in Philadelphia was 426. That’s per day. Let that sink in.
From 1918-1926 the newly established Department of Public Health, along with the US Army and the insurance company Mutual of New York conducted a study. What they found was the wearing of (cloth) surgical masks did nothing to slow or abate the spread. Also, the imposition of quarantine was a death sentence for those not infected, living in the same residence.
The US government has had in its labs since 1967, COVID-19. It was by direction of Dr. Fauci, approved by President Obama that the bio weapons lab at Ft. Detrick be shut down and those agents/experiments be outsourced to among other places, Wuhan, China. That is China, a communist country/enemy of the US.
Dr. Fauci and Dr. Collins funded the Gain of Function research of COVID-19. There are two very similar definitions for the term Gain of Function. The civilian definition is that it is the ability to understand what makes a given virus/bacterium tick so that we can then either kill it or render it ineffective. Sounds good. The military definition is the same but the goal is to enhance its virulence all the while we can control/target it to a given enemy. Think mustard gas and gas masks in WW I.
Now, think back to 2020 when this thing sprang out of nowhere. No one stopped to ask how Dr. Fauci knew immediately what it was. Nor did anyone bother to question his constant reversals on whether or not wearing a mask was necessary. He just knew because he is smarter than the rest of us. At least, that is what we were told.
Immediately, the US Army deployed a Surgical Field Hospital to NYC. Dozens of refrigerator semi trailers were brought in as holding containers or the onslaught of dead that they were sure were coming. A month went by and due to great expense, having seen only 100 patients, none of who had COVID-19, the Army packed it in and went home. The CDC brought in Dr. Birx who changed the way we count Cause of Death. People who objected quit and were immediately silenced. No longer interested exclusively in COVID-19 as the Primary COD, we now actually paid hospital groups to test the dead for COVID-19. Literally, you could die in a horrific car crash, and post mortem be tested for, pop positive and then have that secondary, tertiary or ancillary finding become the Primary COD. Philadelphia 1918, 426 per day. Philadelphia 2020, you weed through and filter out the extraneous bull shit diagnoses and what you end up with is a probable 23 per month. A monumental intentional inflation of numbers. Now pay attention because here where federal law and policy matter.
In 2012 President Obama signed into law the new Smith-Mundt Modernization Act. That allows the government to pay “news” sources - like ABC, CBS, NBC, CNN, MSNBC, etc., to report propaganda pieces that can be patent lies. Now think fear mongering, suspension of inalienable rights, and the liberty to exercise those rights.
Federal law requires that there be no other known cure available, in a time of “national emergency” to suspend and waive requisite testing of new drugs or vaccines. There were again doctors: immunologists, who spoke out against mRNA and pointed to other drugs that could prove effective. Just like those at the CDC who opposed Dr. Birx, these experts were shut down, silenced and in several cases imprisoned.
Sound like “conspiracy theory”? Think twice. Look up nuclear testing on US military from 1946-1962. Having signed a record of non disclosure many went to their graves carrying that secret. That non disclosure was finally lifted in 1996. MK Ultra, The Tuskegee Experiments, etc.. Would the Democrats diabolically unleash this upon the world to rid themselves of Trump? Both Charles Schwab and Bill Gates insist this is exactly what happened - and they are both in favor of it. I’m not saying the Democrats did this, I’m only looking at history, their party history. Figure the odds. And so many want to turn healthcare over to these monsters?
15 notes
·
View notes
Text
Rabies facts
• neurons can try getting rid of infections, but they can’t interact with nervous system.
• Neurons are needed for feel, sensing, thinking, and movement, alongside other basic things in life
• they can’t replenish themselves after cell death
• immune cells like neutrophils often do jobs with some level of collateral damage
• neurons are a protected class of cells and evolved to tone down their immune response so we can not accidentally hurt them.
• so how nervous tissues protected if the immune system can’t get in to fight germs that make it there? by intercepting threats before they make it to neurons, they can continue to do their jobs safely.
• however, with rabies, the strategy fails
• rabies happens via animal bite, something that can penetrate many layers of tissue and circulation that are supposed to stop viruses from getting to neurons.
• in the earlier stages, treatment is somewhat more likely to be successful as it isn’t in the brain yet. if stopped before it gets there, you may survive.
• neurons are the longest cell type in the body. the distance for the rabies virus to travel to ur brain would be from florida to sweden. even so, time is scarce.
• rabies evolved a dastardly technique that hijacks the cellular transport system by binding into the protein dyenin
• dyenin usually transports useful cell cargo from the periphery of the cell towards its body; rabies evolved to stick to dyenin and hitch a ride up the neurons towards the brain.
• dyenin isn’t a slouch; it is small but can move at 800 nanometers per second. thus it can take rabies 14 days to move up a meter long neuron.
• if humansized, it would be 212 miles per hour or 342 kilometers per hour, as fast as a bullet train or arrow or eight usain bolts. and the closer a rabid animal bites you, the less distance it has to travel before your dead.
• this can explain the variation in the incubation period of rabies (20-90 days) where those infected have no symptoms.
• rabies races among neuronal tracks, setting up areas of concentrated viral centers called negri bodies
• negri bodies act as viral factories and pump out more copies of the rabies virus within neurons.
• the viral setup happens without our knowledge or interference
• neurons minimize distress signaling for the good of the body even if in bad shape. not only are they quiet signalers but the rabies virus inhibits interferon (an immune signal that normally alerts us to the site of infection) action
• the double whammy of immune interference means the infected neurons are nearly silent
• Apoptosis or programmed cell death is one more tool neurons have for infection. via apoptosis a cell undergoes a demolition of itself, disintegrating into smaller bubbles, denying the virus further access to its virus making machinery
• the smaller bubbles can then be safely scooped up by immune system cells
• however, rabies possibly evolved in a way to take even this cellular nuclear option away from the neuron. rabies strains causing less apoptosis have been found to be more infectious in mice, implying that rabies could have evolved to stop apoptosis in its tracks
• if rabies blew up neurons too early or frequently it might never make it to the brain without being cleared up by the immune system .
• rabies also evolved in a way to protect neurons during incubation.
• T-cells are small but extremely strong ; infected cells display pieces of the viral protein on their surface. when killer t cells recognize and bind that protein it releases a potent cocktail of enzymes that trigger cell death.
• rabies would inhibit neurons ability to fight it but the t cell would send it over the edge… however rabies has a cheat code.
• it stops apoptosis in neurons, but encourages it in t cells. its still unknown how it happens. the t cell would attempt to stop the virus only to be forced to self destruct
• Also, the rabies virus only has five genes.
• There is still hope: rabies is minmaxed for stealth, and if detected by the immune system before it goes to the brain, the risk of death from rabies is none. the vaccine also trains the immune system to better recognize the virus. however, if one waits too long, it’s over, and the vaccine is also expensive
Source: https://youtu.be/uDF83PEUQRs?si=s_5iFH0AnMSWkLxV
Thumbnail ID: A cartoon-style illustration features a virus with a purple, oval shape, surrounded by small spikes. The virus is highlighted by a red arrow pointing to it. Bold, dramatic text below the virus reads '99.9% Lethal Virus,' suggesting the virus's high lethality rate. The background is a textured off-white color, lending a scientific and educational tone. A blue, fluffy shape below the text may represent another biological entity or cells.
youtube
10 notes
·
View notes
Text
After being repeatedly reminded in recent days that many people, even those who are close to me and intelligent, have entirely missed the point on why, beyond just what it can do to you, COVID is such a terrifying illness, I feel I now have to reiterate some important points that have conveniently drifted away from common knowledge.
First: You cannot know that you've contracted COVID for upwards of several days from the point of contact. Can not.
Your diligence, your knowledge of self, your assertions of certainty, your record of good personal upkeep and health and hygiene and diet, are all useless for this.
Second: If you have COVID, there is an incubation period of up to several days. During that incubation period, there is a window prior to symptoms appearing when you begin to be infectious; this time period places you in the category of asymptomatic carrier -- so, regardless of if you never develop symptoms or develop them later, when you get COVID you will at some point be in this category.
This period of time generally occurs before rapid tests can reliably detect it. Thus, for this time period, once again, YOU CANNOT KNOW that you are sick or infectious.
Third: The severity of a case of COVID you are exposed to says nothing about the severity of the case you will get from that exposure.
Fourth: The COVID rapid tests they tell you to take to make sure you can come into work were not implemented by the CDC for the safety of workers. This practice was enacted as a form of medical theater, to convince you that things are being done to assure your safety at work, so that you can go back to work. It is literally a capitalist ploy.
Fifth: Masks actually work remarkably well -- to protect others from catching the virus from you if you happen to have it, which, I repeat, you cannot know if you are spreading. They do help protect you against catching it, but are not nearly as effective at this as they are at stopping you from spreading it.
This messaging has been consistent throughout the pandemic from medical experts; time, as well as repeated insinuation by right-wing shitheads, has obfuscated this messaging. Masks are not chiefly to protect you from catching it. They are for stopping you from spreading it. Because, again, for a very crucial period of time during the infection, YOU CAN'T KNOW IF YOU'RE INFECTED.
13 notes
·
View notes
Note
So, ive recently gotten back into Protocreed and a what if..? idea i had was:
After Abstergo recovers Desmonds body, they experiment with his DNA and Blacklight. Resulting in him being revived after an outbreak and breaking free.
It could even be the assassins fault that the outbreak happened!
.
In the midst of the chaos, no one noticed the body dissapearing. It's only after the outbreak was contained and culled that Subject 17 was noted as missing. With all the footage being destroyed it is impossible to tell what happened to it, but the general consensis is that one of the infected ate it. It is a crushing blow to their research, but thankfully they have plenty of samples stored in a different facility, so all hope is not lost. No one thought of the possibilty that a repeat of Alex Mercer's revival could happen. Subject 17 has been dead for months, the body is simply too old. So no one thought too look in the shadows of the city, where something lay lurking. Tracking. Hunting.
Hungering
So I have a ProtoCreed idea similar to this that I posted here.
The comments/replies have more details on how it would go but, in a nutshell, Blacklight is a failed/abandoned Isu project headed by Tinia (so we can have a little hehe moment with Alex being called ‘Zeus’) and Dr Mercer is not a Templar but he’s still a piece of work.
And Desmond’s Isu to human genes ratio + his Bleeding Effect screwed up the virus that he still has the superhuman feats that Alex has but he can’t morph his body to have weapons or anything like that.
Instead…
It’s like he can spawn three specific humanoid figures made of the black and red writhing flesh which only has one specific goal: keep Desmond safe.
There’s more details in the link above but the main point is that Desmond’s virus makes him be able to ‘summon’ his ancestors who holds a piece of Alex’s OG abilities and it’s unclear if they are mindless or if their connection with Desmond keeps them docile because when Abstergo try to cut their connection (which are tendrils of red and black connecting the creatures to Desmond’s shadow), the creature goes berserk and attacks and devours everything around until Desmond reconnects with it.
So we have:
Altaïr = Blade
Ezio = Hammerfist
Ratonhnhaké:ton = Whipfist
Ezio gets Hammerfist because the sword of Altaïr is iconic so Altaïr gets the Blade and Ratonhnhaké:ton had the ropedart so he gets the Whipfist. XD
Although, in my original idea, Desmond keeps his memories (thanks to the Bleeding Effect) but if you want to go down the route of Desmond being ‘incubated’ by the virus during the story of Prototype and waking up afterwards, we can easily do that and the incubation period is actually what corrupted Desmond’s mind.
So in this situation, Desmond would be more like ‘Eve’ from Parasite Eve, the new origin of an outbreak (and everyone believes it’s Alex’s fault which will lead us to a modified setup for Prototype 2 and Alex and Desmond having an antagonistic start).
But the outbreak is strange because it seemed… targeted.
The ones to be hit first were Abstergo facilities or facilities under Abstergo’s shell companies.
And the spread only began when these facilities had fallen and the barricades have been breached, like… it wasn’t truly intentional but more of a ‘side effect’.
So now we have Alex trying to figure out what this new outbreak is because the ‘children’ for this one are faster and more cunning, using their surrounding to hide and wait. And these children seemed to be taking orders from three creatures made of darkness and blood.
(Or, if you want to preserve the Assassin white and red color scheme, it’s gonna be grosser with them being filled with pus and blood instead. The pus could be a sign that the virus is being combated by Desmond’s Isu genes though and that could be a clue for Alex)
And any time Alex tries to eat any of them, he only gains snippets of the memories of the same person: a man named Desmond Miles.
The three commander creatures also seemed to travel via shadows, being able to melt into the shadows before Alex could ever destroy them completely.
Later, he would realize that the whole city (whichever city we’re planning to set this on) are filled with what looked like lines all over (maybe one would say that maybe it’s the ley lines or something and Alex would say that it looks more like… veins…) and these veins are actually how the commanders travel all over the city.
At the center of the veins is a cocoon…
#maybe calling desmond “eve” might not be correct in this one?#but it’s the first comparison i thought of#so the outbreak happens because desmond needs to ‘eat’#to heal up#and the creatures are all acting#with that directive in mind#alex is an anomaly that they attack on sight#but he’s also an anomaly that is dangerous#so they don’t try to “eat” him#I’m thinking dana is the one to get in contact with the assassins#via erudito or something#and shaun and rebecca support alex via drones#all named the same as the ac syndicate drones#protocreed#ask and answer#assassin's creed#desmond miles#teecup writes/has a plot#fic idea: assassin's creed#prototype#alex mercer
92 notes
·
View notes
Note
Wait so Lilia is dead in the Blot infection Au? :,d
Also you take more inspiration in the last of us or like Walking dead when it comes to the blot infection?
GOOD QUESTION.
yes Lilia is dead BUT only according to silver (it's hard to imagine what must have happened for silver to think he was dead)
AND SECOND.
It's really about everything at once and nothing at all.
When it comes to infection, I guess virus, any secretions from the second stage onwards is contagious.
In the first stage, there is a conditional incubation period when the disease becomes established in the organism and in the second stage it reaches the spinal cord and glands, causing the organism to mutate and spread spots.
It is important that the object that has been infected is alive. but after the third stage of infection, it doesn't matter if the organism is alive or dead, as long as the cerebellum and spinal cord are intact.
If you remove the spinal cord, it'll stop producing the substance and the organism won't be able to sustain itself.but if the cerebellum remains, it will live for a while.
Cutting off a limb as a defence will work, but only if done as quickly as possible. Also, the stains won't do any harm if they just get on the skin.
updated:
I also forgot to add that over time the infected will not decompose but will continue to mutate.
5 notes
·
View notes
Note
Can rabies spread in the incubation period BEFORE any symptoms show in the host?
So this is one I don't know. I know the general rule of thumb is "if symptomatic, considered contagious", but the incubation period is when any post-exposure therapies would be effective, which makes me think no. Except maybe like... idk in lactating mothers nursing their young?
More or less during the incubation period, the virus is way more concerned with hitchhiking its way up to your brain to start chewing on your brain stem than it is trying to spread itself. Once it reaches its goal, it populates and then spreads itself to the saliva via the bloodstream in order to infect as many other animals as possible. So by my guess, outside of situation like breastfeeding and pregnancy where mother and child are significantly impacted by any change in the mother's body, I'd say no.
38 notes
·
View notes
Text
The influx of the MLP Infection trend has gotten me thinking about the concept I had for an EAH reboot (TL;DR: it would eventually be revealed that the original EAH universe still exists, but the characters there would be suffering from a sort of zombie apocalypse situation due to the Narrators abandoning them). I decided that I want to fine-tune this idea!
You know how I initially said the condition of the characters becoming those papier-mâché creatures wasn't contagious? Retconning that!
The narrators abandoning the original universe created a sort of... disease, known as The Bookworm Virus.
The first victim was bitten by an infected insect. (When the infection got into its later stages, the virus within the infected individuals began to warp the land, too.)
There are four stages to this virus:
Stage 0: Victim is infected via bite from other infected individual or insect. This stage comes with an incubation period. Victim's mental/psychological symptoms begin with brain fog, while physical symptoms begin with headaches and slight pain at the area of the bite, as well as skin discoloration, with the area of the bite turning more of a white-ish color, almost like paper. (note: amputation is unfortunately not a viable treatment.)
Stage 1: The time it takes to reach this stage varies from person to person. The mental/psychologist symptoms become more prominent after the incubation timeframe, however, as the victim begins suffering from confusion, memory loss, disorientation, and behavioral/personality changes. The physical changes, too, become more severe- pain is no longer present, but the area of the bite skin further discolors into a sickly, wrinkly yellow... it should be noted that the wrinkles almost look like writing.
Stage 2: Spread of skin discoloration and change in texture; the victim becomes far more unrecognizable, due to the further spread of the physical symptoms, and delirious, as brain activity is thought to be further deteriorating by this point, at this stage. The victim also begins becoming aggressive towards others. (note: the victim is now contagious.)
Stage 3: Victim has been completely taken over, having the appearance similar to a Papier-mâché or origami creature. It is unknown if there any brain activity/consciousness other than the basic instincts. The victim is also extremely aggressive in this stage.
By the time the Narrators are made aware of the situation, the world of Ever After has fallen into ruin. They are fortunately able to get into contact with a group of the immune: the Brothers Grimm and Maddie.
(Also: just because there's a group of an immune doesn't mean that there are those who are conditionally immune or are partially infected 🙂😉)
Maddie tries to convince the Narrators to come back, to fix this mess- but they refuse. This story has been over for a long time now, at least in their minds, and even if they did, they probably wouldn't be able to do anything about it. And, to rub salt in the wound, Milton wants out. He asks the Narrators, much to the horror of Giles and Maddie, if the Narrators can remove him from this story and take him to the next. Despite the pleas of the two survivors, the Narrators agree, and in the blink of an eye, Milton is gone.
The Narrators whisk Milton away to a new realm, one where he works with them to remake Ever After. This rebooted realm goes smoothly- well, as smoothly as it can- until, through some way or another, the rebooted versions of Kitty, Maddie, Blondie, and Alistair find out the truth, and decide to work with Brooke, go to the original EAH universe, and fix it.
...And that's about it! As I did with the concept, I may add more on later. Feel free to ask questions and/or add your own ideas!
#ever after high#eah#ever after high au#eah au#the bookworm virus au#bookworm virus au#the bookworm virus#bookworm virus
21 notes
·
View notes