#Health Practitioner Australia
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
69% of Tumblr users are millennials.
Text
Chinese Medicine Practitioner | Flow Acupuncture

Embark on a Healing Journey: Flow Acupuncture Melbourne Awaits You! Begin your healing journey at Flow Acupuncture Melbourne, where Vivian and Jenny bring their expertise in traditional Chinese medicine to enhance your overall well-being. Allow our practitioners to guide you on a transformative journey towards health, incorporating ancient healing practices into modern-day life.
#Chinese Medicine Practitioner#Acupuncture Clinic Victoria#Acupuncture Clinic in Melbourne#Acupuncture Practitioner Near Me#Traditional Chinese Medicine Practitioner#Health Practitioner Australia
0 notes
Text
Experienced Kallangur Doctors & GP in Lawnton Country Market

Are you looking for experienced doctors or a trusted medical centre near Kallangur? Visit Lawnton Medical Centre on Gympie Road for top-quality care. Our skilled GPs offer mixed billing and comprehensive healthcare services for all ages, including skin cancer care, mental health support, women’s and men’s health checkups, and more.
Book your appointment with our Kallangur doctors today and get the care you deserve!
#health#health and wellness#health tips#healthcare#general practitioner#medical centre#australia#lawnton#brisbane#queensland#doctors#hospital#kallangur
1 note
·
View note
Text
While the Cass Review has been presented by the U.K. media, politicians and some prominent doctors as a triumph of objective inquiry, its most controversial recommendations are based on prejudice rather than evidence. Instead of helping young people, the review has caused enormous harm to children and their families, to democratic discourse and to wider principles of scientific endeavour. There is an urgent need to critically examine the actual context and findings of the report. Since its 2020 inception, the Cass Review’s anti-trans credentials have been clear. It explicitly excluded trans people from key roles in research, analysis and oversight of the project, while sidelining most practitioners with experience in trans health care. The project centered and sympathized with anti-trans voices, including professionals who deny the very existence of trans children. Former U.K. minister for women and equalities Kemi Badenoch, who has a history of hostility toward trans people even though her role was to promote equality within the government, boasted that the Cass Review was only possible because of her active involvement. The methodology underpinning the Cass Review has been extensively criticized by medical experts and academics from a range of disciplines. Criticism has focused especially on the effect of bias on the Cass approach, double standards in the interpretation of data, substandard scientific rigor, methodological flaws and a failure to properly substantiate claims. For example, although the existing literature reports a wide range of important benefits of social transition and no credible evidence of harm, the Cass Review cautions against it. The review also dismisses substantial documented benefits of adolescent medical transition as underevidenced while highlighting risks based on evidence of significantly worse quality. A warning about impaired brain maturation, for instance, cites a single, very short speculative paper that in turn rests on one experimental study with female mice. Meanwhile extensive qualitative data and clinical consensus are almost entirely ignored. These issues help explain why the Cass recommendations differ from previous academic reviews and expert guidance from major medical organisations such as the World Professional Association for Transgender Health (WPATH) and the American Academy of Pediatrics. WPATH’s experts themselves highlight the Cass report’s “selective and inconsistent use of evidence,” with recommendations that “often do not follow from the data presented in the systematic reviews.” Leading specialists in transgender medical care from the U.S. and Australia emphasize that “the Review obscures key findings, misrepresents its own data, and is rife with misapplications of the scientific method.” For instance, the Cass report warns that an “exponential change in referrals” to England’s child and adolescent gender clinic during the 2010s is “very much faster than would be expected.” But this increase has not been exponential, and the maximum 5,000 referrals it notes in 2021 represents a very small proportion of the 44,000 trans adolescents in the U.K. estimated from 2021 census data.
7 August 2024
58 notes
·
View notes
Text
The Devotee is in
Hello Paganblr!
*Pours myself copious amounts of herbal tea* I would like to acknowledge the Gadigal of the Eora Nation, the traditional custodians of this land and pay my respects to the Elders past, present and emerging. I acknowledge that Aboriginal sovereignty has not been ceded.
It is Saturday morning here in Australia and while I have resumed playing Stray Gods: The Roleplaying Musical as an Apollo + Hermes devotional act I am also at my PC slowly beginning to start on some of my Tumblr to-do list (posts on various Polytheistic concepts).
Please feel free to drop an ask and I will try to help you as best as I can.
Housekeeping:
Please specify whether you are a reconstructionist pagan or neopagan, noting that I am Neopagan of over 2 decades and as such, I am best equipped to assist the latter.
Please specify whether you are a Worshipper or Devotee or just wanting to start the process of worshipping a deity.
I love assisting my fellow pagans however the expectation is that you know how to use the search bar in your search engine and social apps of choice so unless your query specifically requests details on certain things I am running under the assumption that you know the difference between worshipper & devotee, the basics of the deities you are seeking guidance with etc.
Please state whether or not you are a minor so that I can ensure that my advice is age appropriate, I would hate to have a "Minors DNI" when I would prefer to help guide you on your journey since when I was a teenager I had to rely on magazines and books alone...
Thank you Apollo and Hermes in guiding me in this devotional act of service this weekend

Disclaimer: While I have 3x psychological first aid certificates & 11 years experience of assisting people in crisis I am not a registered mental health practitioner and as such if you are experiencing concerning and/or distressing medical or psychological symptoms please seek professional help ASAP. If you are currently concerned about your personal safety or the safety of others, please seek urgent advice in accordance to the laws & organisations available in your local area.
#apollo devotee#thank you hermes#deity worship#deity work#hermes devotee#ares devotee#hellenic paganism#deity communication#apollo worship#devotional polytheism#devotional acts#apollo devotional#hermes devotional#paganblr#pagan community
8 notes
·
View notes
Text
Jacinta Allan is warning that the battle for abortion rights must continue as conservative forces pose “real and genuine threats to the protections women have fought for and won” amid “frightening” debate in South Australia and Queensland.
Victoria’s Labor premier made her strongest comments to date on abortion in an interview with Guardian Australia, just days before Queenslanders go to the polls in an election that has become dominated by the issue.
“I am deeply concerned that things that women, and men, have fought for for decades – in terms of strengthening the protections around women’s right to choose, women’s right to control their reproductive choices – is being used as a political tool,” she said.
“But even worse, there are real and genuine threats to the protections women have fought for and won. Legislation to protect their rights is being looked at being torn down at too many opportunities by conservative politicians.”
Abortion has been fully decriminalised in all Australian states and territories. Medical abortion is available until nine weeks’ gestation, while surgical abortion rules vary from 16 weeks in the Australian Capital Territory to 24 weeks in Victoria.
During the Queensland election campaign, Katter’s Australian party has promised to force a vote on a bill that would give registered health practitioners a duty to “provide medical care and treatment to a person born as a result of a termination”.
The KAP leader, Robbie Katter, has said he would consider introducing stronger legislation depending on how many conservative Liberal National party MPs are elected on Saturday.
The LNP leader, David Crisafulli, has been dogged by the issue for weeks and has refused to say whether he would grant his MPs a conscience vote.
This month in SA, legislation introduced by a Liberal frontbencher to force women seeking later terminations to be induced, deliver the babies alive and keep them or adopt them out was narrowly defeated by 10 votes to nine.
In Canberra on Tuesday the Coalition senator Jacinta Nampijinpa Price told Nine newspapers there should be a national debate on the issue and likened late-stage abortions to infanticide.
Jane Hume, Sussan Ley and Bridget McKenzie – three of the most senior women in the Coalition – flatly rejected putting abortion on the national agenda, saying it was an issue for states and territories.
Allan said events had proved the issue was not confined to the political fringes.
“We’ve seen it in South Australia, in Queensland, this federal intervention from a federal senator … you look at what’s happening in the US,” she said.
“The message that sends to women, it’s frightening. It says all that work that has been done to protect your rights, to support your choice, is at risk every single day from these conservative forces.”
Allan said she would “fight for women to have their right to have their control over their bodies”.
She acknowledged that there was more work to do in Victoria, despite it being a leader in Australia in terms of access to sexual and reproductive health services.
“I know that, particularly for regional women, access to services can be a real challenge,” Allan said.
A report by Women’s Health Victoria published on Thursday found that seven out of 10 local government areas have no surgical abortion provider and one in five have no medical abortion provider.
The government said it had established 20 sexual and reproductive health hubs across the state, including in Ararat, Horsham and Melton – areas the report identified as having the highest rates of women seeking abortion.
The hubs offer medical abortion care and referral pathways for surgical abortion. Endorsed midwives have also been given the power to prescribe medical abortions and make referrals.
Work is under way to expand access to abortion in public hospitals, while Guardian Australia understands an announcement on the issue is also due soon.
5 notes
·
View notes
Text
Learning accommodations request template
You are entitled to your education, and reasonable accommodations are required to be made for you, recognised as a right by the United Nations Convention on the Rights of Persons with Disabilities, article 24. Accessible and equitable education is also part of Australia’s disability strategy 2021-2031. I say this as a preface, because should you face resistance, it is important that you know your rights in this area.
Furthermore, you do NOT need to disclose your disability diagnosis, and the school or university is not supposed to ask. What they can request is a letter from a treating practitioner confirming you are eligible for disability supports. Your GP or an allied health professional can provide this.
Beyond that, you do not have to tell them your diagnosis. If asked, you can simply politely remind the person you are in discussion with that you do not have to disclose the nature of your disability, however you are happy to discuss your accommodation requirements.
I would recommend that for secondary school and University students you assume this letter will be required.
Accommodation request for school or university template:
Hello, My name is [Introduce yourself], I am a [Year level if in high school or course and year for university.]. I am writing to Request a meeting/a phone call/[other form of communication that meets your needs] to discuss learning accommodations in relation to my disability. Accommodations I am requesting are [state what you need. Examples include extra time on tests, the ability to type exams instead of writing, braille learning materials, sign language being available, different learning formats, extra time to get to and from classes, your classes being in close proximity to each other, exams in separate rooms, access to a clarifier for assessment tasks]. I have attached/will provide if needed a letter from my [Insert the type of practitioner who has provided or will provide your letter] which confirms the necessity of this/these accommodations. [if you have requested a in person discussion, phone call, video chat or any form of discussion that requires scheduling, at this point offer three dates + times you could have said discussion.] [if you have not requested a schedulable conversation, request an email back with a term that has an appropriate level of urgency. ‘as soon as possible’, ‘at your earliest convenience’, ‘before the term / semester begins’] so that we can ensure that everyone is on the same page. Thank you for your time, [your name again]
Who would you send this to?
Your school’s additional needs program or disability support program.
relevant resources:
#campaign for change#disability#disability education#youth advocacy#education#education system#reasonable adaptations#autism#disability advocacy#intellectual disability#physical disability#education advocacy#australian schooling system#learning accommodations
5 notes
·
View notes
Text
By: Bernard Lane
Published: Apr 14, 2024
Nine of the 15 gender clinics in a landmark international survey for the Cass review have admitted they do not routinely collect outcome data on their young patients.
This survey, together with a new evaluation of treatment guidelines for gender dysphoria, gives unprecedented insights into the workings of gender clinics around the world offering puberty blockers and cross-sex hormones to minors.
In the 2022-23 survey, six clinics said they “routinely collected some outcome data”: one of these clinics gave no further detail; one noted the number of patients discontinuing treatment; another used measures of quality of life; two were taking part in cohort studies; and the sixth clinic repeated some baseline assessments. Nine clinics acknowledged “not routinely collecting outcome data.”
The report of the survey results1, published by researchers from the University of York earlier this month, identified clinics by country, not name. Of the clinics that took part, Australia and the Netherlands were prominent with five and four clinics respectively.
Poor data collection was central to the controversy over the London-based Tavistock youth gender clinic.
The Cass review had planned to run a data-linkage study—with help from adult gender clinics—to learn the outcomes of the Tavistock’s 9,000-odd former patients.
The missing long-term data would allow clinicians, young patients and parents to make informed decisions about treatment. The review said it was to be the largest study of its kind in the world.
However, six of the seven adult clinics refused to co-operate. One stated reason was that “the study outcomes focus on adverse health events, for which the clinics do not feel primarily responsible.”
Another adult clinic said, “The unintended outcome of the study is likely to be a high-profile national report that will be misinterpreted, misrepresented or actively used to harm patients and disrupt the work of practitioners across the gender dysphoria pathway.”
On April 12, however, The Times newspaper reported that the uncooperative adult clinics had “bowed to pressure to share [the] missing data”.
Mostly medical
In the York University international survey, ordered by the Cass review, all 15 youth gender clinics said they used a multi-disciplinary team, but researchers concluded there was a “paucity” of psychosocial therapy interventions such as psychotherapy or cognitive behaviour therapy. Five clinics did not offer any of these non-medical interventions in-house.
All gender clinics told researchers that “genital reconstructive surgery”—the creation of a pseudo vagina, for example—was “accessible only from age 18.” The youngest age for “masculinising chest surgery” (a double mastectomy) was reported as 16. In fact, there are documented cases in Australia of 15-year-olds approved for transgender mastectomy. Genital surgery is legally available to minors2 in Australia and practised in America.
“Only five clinics reported routine discussion of fertility3 preferences, and only two discussed sexuality4. Finland was the only country to report routinely assessing for history of trauma5,” the final Cass report says in its commentary on the survey.
In separate studies for the Cass review, three independent reviewers evaluated the quality of 21 guidelines for treatment of gender dysphoria in minors.
Included were international guidelines (from the Endocrine Society and the World Professional Association for Transgender Health or WPATH); documents from North America (for example, the 2018 policy statement from the American Academy of Pediatrics); from Europe (the guideline of the UK Royal College of Psychiatrists, for example, and Denmark’s); as well as guidelines from the Asia-Pacific and Africa.
“WPATH has been highly influential in directing international practice, although its guidelines were found by the University of York appraisal process to lack developmental rigour,” the Cass report says.
The York researchers chart patterns of “circular” cross-referencing between guidelines to create a misleading impression of consensus in favour of the medicalised “gender-affirming” treatment approach.
“The guideline appraisal raises serious questions about the reliability of current guidelines. Most guidelines have not followed the international standards for [rigorous and independent] guideline development. Few guidelines are informed by a systematic review of empirical evidence [the gold standard for assessing the evidence supporting a health intervention] and there is a lack of transparency about how recommendations were developed,” the Cass report says.
“Healthcare services and professionals should take into account the variable quality of published guidelines to support the management of children and young people experiencing gender dysphoria. The lack of independence in many national and regional guidelines, and the limited evidence-based underpinning current guidelines, should be considered when utilising these for practice.”
The Cass report says it is “imperative” that gender clinic staff be “cognisant of the limitations in relation to the evidence base and fully understand the knowns and the unknowns.”
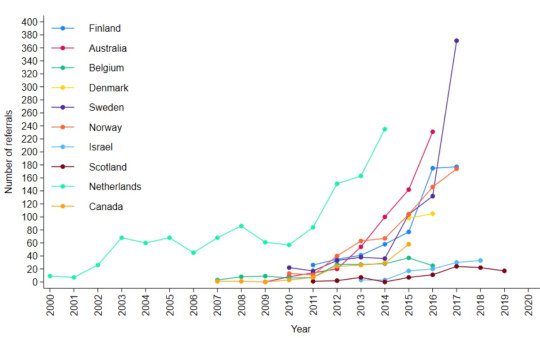
[ Chart: Number of youth gender clinic referrals over time by country. Source: Cass report ]
Bum steer
Staff at the Tavistock clinic misled patients and parents, or failed to correct their misconceptions, according to a new report from the Multi-Professional Review Group (MPRG) given oversight of treatment decisions from 2021.
These shortcomings of clinicians included playing down the extent of the unknowns of hormonal treatment; not explaining that puberty blockers are being used unlicensed and off-label; not challenging the reassuring but false parallel with the licensed use of puberty blockers for precocious (premature) puberty; not discussing the possibility that blockers will pause or slow psychosexual development; and not sharing figures showing the vast majority of children started on puberty blockers will go on to cross-sex hormones supposed to be taken lifelong.
The MPRG was also troubled by clinical documents showing misunderstanding of “the outcome of physical treatments” on the part of patients and parents.
In the York University study of treatment guidelines for gender dysphoria, only two were recommended for use by all three reviewers. These were recent, more cautious policies from Finland and Sweden. Both followed independent systematic reviews showing the evidence base for hormonal and surgical treatment of minors to be very weak and uncertain. Like the Cass review itself, the 2020 Finnish and 2022 Swedish guidelines recognise that puberty blockers are experimental and should not be routine treatment.
Although all the guidelines in the study agreed on the need for a multidisciplinary team to treat gender-distressed minors, the “most striking problem” shown by analysis of these documents was “the lack of any consensus6 on the purpose of the assessment process”, the Cass report says.
“Some guidelines were focused on diagnosis, some on… eligibility for hormones, some on psychosocial assessment, and some on readiness for medical interventions7.
“Only the Swedish and [the 2022] WPATH 8th version guidelines contain detail on the assessment process8. Both recommend that the duration, structure and content of the assessment be varied according to age, complexity and gender development.
“Very few guidelines recommend formal measures/clinical tools to assess gender dysphoria, and a separate analysis demonstrated that the formal measures that exist are poorly validated.”
Nor was there any consensus on “when psychological or hormonal interventions should be offered and on what basis.”
A survey of staff at the Tavistock clinic, undertaken as part of the Cass review, found specialists divided on whether or not “assessment should seek to make a differential diagnosis, ruling out other potential [non-gender9] causes of the child or young person’s distress.”
Arguing for an ambitious research program well beyond a possible clinical trial of puberty blockers, the Cass report says the field of youth gender dysphoria is one of “remarkably weak evidence” where health professionals are “afraid to openly discuss their views” because of vilification and bullying.
“Although some think the clinical approach should be based on a social justice model, the NHS works in an evidence-based way,” the report says.
“The gaps in the evidence base regarding all aspects of gender care for children and young people have been highlighted, from epidemiology through to assessment, diagnosis10 and intervention. It is troubling that so little is known about this cohort and their outcomes.
“Based on a single Dutch study, which suggested that puberty blockers may improve psychological wellbeing for a narrowly defined group of children with gender incongruence [or dysphoria], the practice spread at pace to other countries.
“Some practitioners abandoned normal clinical approaches to holistic assessment, which has meant that this group of [gender-distressed] young people have been exceptionalised compared to other young people with similarly complex presentations.”
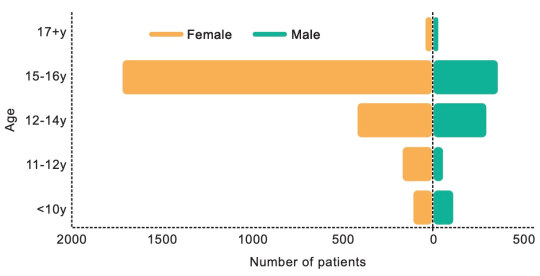
[ Chart: Age and sex on referral to the Tavistock clinic from 2018-2022. Source: Cass report ]
Who to trust?
The Cass report says the missing evidence “makes it difficult to provide adequate information on which a young person and their family can make an informed choice.”
“A trusted source of information is needed on all aspects of medical care, but in particular it is important to defuse/manage expectations that have been built up by claims about the efficacy of puberty blockers.
“The option to provide masculinising or feminising hormones from the age of 16 is available, but the [Cass] review would recommend an extremely cautious clinical approach and a strong clinical rationale for providing hormones before the age of 18. This would keep options open during this important developmental window, allowing time for management of any co-occurring [non-gender] conditions11, building of resilience, and fertility preservation, if required.”
The review stresses that “consent is more than just capacity and competence. It requires clinicians to ensure that the proposed intervention is clinically indicated as they have a duty to offer appropriate treatment. It also requires the patient to be provided with appropriate and sufficient information about the risks, benefits and expected outcomes of the treatment.”
“Assessing whether a hormone pathway is indicated is challenging. A formal diagnosis of gender dysphoria is frequently cited as a prerequisite for accessing hormone treatment. However, it is not reliably predictive of whether that young person will have long-standing gender incongruence in the future, or whether medical intervention will be the best option for them.”
Advocates for the gender-affirming approach assert that detransition and treatment regret are vanishingly rare, whereas suicide risk for those denied medical intervention is claimed to be very high.
The Cass report says: “It has been suggested that hormone treatment reduces the elevated risk of death by suicide in this population, but the evidence found did not support this conclusion.”
“The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The report cites three reasons why the true extent of detransition is unlikely to be clear for some time—patients who decide medicalisation was a mistake may not wish to return to their former clinic to announce this fact; there is a post-treatment honeymoon period and clinicians suggest it may take 5-10 years before a decision to detransition; and the surge in patient numbers only began within the last decade.
Faced with uncertainty and a lack of good evidence, those with responsibility—from health ministers and hospital managers down to gender clinicians—rely on treatment guidelines supposed to advise on clinical practice according to the “best-available” evidence and expert opinion.
In the York University guideline analysis, the 21 documents were rated on six domains, the key two being the rigour of their development and their editorial independence.
“[Rigour] includes systematically searching the evidence, being clear about the link between recommendations and supporting evidence, and ensuring that health benefits, side effects and risks have been considered in formulating the recommendations,” the Cass report says.
Only the Finnish and Swedish guidelines scored above 50 per cent for rigour. Only these two documents, the Cass report says, link “the lack of robust evidence about medical treatments to a recommendation that treatments should be provided under a research framework or within a research clinic. They are also the only guidelines that have been informed by an ethical review conducted as part of the guideline development.”
“Most of the guidelines described insufficient evidence about the risks and benefits of medical treatment in adolescents, particularly in relation to long-term outcomes. Despite this, many then went on to cite this same evidence to recommend medical treatments,” the report says.
“Alternatively, they referred to other guidelines that recommend medical treatments as their basis for making the same recommendations. Early versions of two international guidelines, the Endocrine Society 2009 and WPATH 7th version guidelines, influenced nearly all the other guidelines.
“These two guidelines are also closely interlinked, with WPATH adopting Endocrine Society recommendations, and acting as a co-sponsor and providing input to drafts of the Endocrine Society guideline. The WPATH 8th version cited many of the other national and regional guidelines to support some of its recommendations, despite these guidelines having been considerably influenced by the WPATH 7th version.
“The circularity of this approach may explain why there has been an apparent consensus on key areas of practice despite the evidence being poor.”
Sometimes these gender-affirming guidelines seek to buttress a strong evidence claim with a citation to a study that is weak or involves a different patient group.
The Cass report notes that, “The WPATH 8th version’s narrative on gender-affirming medical treatment for adolescents does not reference its own systematic review [of the evidence], but instead states: ‘Despite the slowly growing body of evidence supporting the effectiveness of early medical intervention, the number of studies is still low, and there are few outcome studies that follow youth into adulthood. Therefore, a systematic review regarding outcomes of treatment in adolescents is not possible’.”
Despite WPATH insisting such an evidence review is not possible, this is precisely what health authorities and experts have undertaken since 2019 in several jurisdictions—Finland, Sweden, the UK National Institute for Health and Care Excellence, Florida, Germany, and University of York research commissioned by the Cass review.
Yet in the 8th and current version of its guideline, WPATH makes the confident statement that, “There is strong evidence demonstrating the benefits in quality of life and well-being of gender-affirming treatments, including endocrine and surgical procedures… Gender-affirming interventions are based on decades of clinical experience and research; therefore, they are not considered experimental, cosmetic, or for the mere convenience of a patient. They are safe and effective at reducing gender incongruence and gender dysphoria”.
But WPATH “overstates the strength of the evidence” for its treatment recommendations, the Cass report says.
--
1 In the survey, there was one clinic each from Belgium, Denmark, Finland, Northern Ireland, Norway and Spain. The response rate was 38 per cent.
2 In Australia there is no good public data on trans surgery for minors.
3 Early puberty blockers followed by cross-sex hormones are expected to sterilise young people and may also impair future sexual function.
4 Some sizeable proportion of gender clinic patients might grow up in healthy bodies and accept their same-sex attraction were it not for trans medicalisation, according to testimony from detransitioners, clinicians’ reports and data.
5 Trauma from a history of sexual abuse, for example, or exposure to domestic violence is thought to be among the many possible underlying causes of what presents as gender dysphoria. The Multi-Professional Review Group (MPRG), given oversight of Tavistock treatment decisions from 2021-23, was troubled by the lack of curiosity by the clinic’s staff about the effect of a child’s “physical or mental illness within the family, abusive or addictive environments, bereavement, cultural or religious background, etc.”
6 Critics of the “gender-affirming” treatment approach say it is not mainstream medicine because the “trans child” in effect self-diagnoses while clinicians avoid differential diagnosis and attribute mental health disorders and other pre-existing issues to a “transphobic” society.
7 “In most cases [at the Tavistock clinic] children and parents were asking to progress on to puberty blockers from the very first appointment”, according to the MPRG.
8 In the MPRG’s opinion, the patient notes from the Tavistock “rarely provide a structured history or physical assessment, however the submissions to the MPRG suggest that the children have a wide range of childhood, familial and congenital conditions.”
9 Once referred to the Tavistock, patients typically were no longer seen by child and adolescent mental health services.
10 According to the MPRG, gender dysphoria in the diagnostic manual DSM-5 “has a low threshold based on overlapping criteria, and is likely to create false positives. Young people who do not go on to have an enduring cross-sex gender identity may have met the criteria in childhood. And early to mid-childhood social transition may be influential in maintaining adherence to the criteria. Sex role and gender expression stereotyping is present within the diagnostic criteria—preferred toys, clothes, etc—not reflecting that many toys, games and activities [today] are less exclusively gendered than in previous decades.”
11 The MPRG said it was “notable that until the child and family’s first appointment at [the Tavistock] they have received little, if any, support from health, social care, or education professionals. Most children and parents have felt isolated and desperate for support and have therefore turned for information to the media and online resources, with many accessing LGBTQ+ and [gender dysphoria] support groups or private providers which appear to be mainly ‘affirmative’ in nature, and children and families have moved forward with social transition. This history/journey is rarely examined closely by [Tavistock clinicians] for signs of difficulty [or] regret.”
==
Critics have described "gender affirming care" - that is, sex-trait modification - as "medical experimentation." This is incorrect. In a medical experiment, you actually collect data and monitor the participants in the experiment. They don't do that. They're cowboys violating all medical ethics - "first, do no harm" - for ideology, money or both.
#Bernard Lane#Cass review#Cass report#Dr. Hilary Cass#Hilary Cass#gender affirming care#gender affirming healthcare#gender affirmation#medical scandal#medical malpractice#sex trait modification#medical corruption#World Professional Association for Transgender Health#WPATH#ethics violations#medical ethics#unethical#gender ideology#gender identity ideology#queer theory#intersectional feminism#religion is a mental illness
11 notes
·
View notes
Text
In a surprise move, the local government of West Australian mining town Port Hedland is calling for immediate suspension of the Moderna and Pfizer Covid vaccines pending an investigation into evidence of excessive levels of synthetic DNA in the shots.
At a special meeting on 11 October, Port Hedland councillors voted five to two in favour of notifying all of Australia’s 537 local councils of the evidence of the DNA contamination in the vaccines, and associated risks.
“We are gravely concerned about the potential health risks posed by synthetic DNA contamination, including the dangers of genomic integration, cancer, hereditary defects and immune system disruption,” said the letter, a copy of which was sent to councillors around the country following the vote.
Letters were also sent to every health practitioner within the Port Hedland area strongly urging them to share this information with patients contemplating receiving any Pfizer or Moderna Covid modified-RNA (mod-RNA) vaccines.
The Port Hedland Council joins federal independent MP Russell Broadbent in calling for the suspension of the vaccines until an urgent and thorough investigation has been carried out into the DNA contamination matter.
Port Hedland Councillor Adrian McRae, who brought the motion, said that he hoped the vote “will be the ripple that creates a bigger wave across the country, and perhaps the world” on the issue of Covid vaccine safety.
The move comes after independent testing of Australian vials of Moderna and Pfizer Covid vaccines, by Canadian virologist Dr David Speicher, detected residual synthetic DNA at levels up to 145 above the regulatory limit.
2 notes
·
View notes
Text
Blog 3: Chinese Medicine, the 5 Elements & Me
In the previous blog, I touched on the yin and yang properties emphasized in Chinese medicine. The ancient Chinese sages also viewed the world in terms of a system of Five Elements: wood, fire, earth, metal, and water. These elements interact with each other and are found within all life, including our bodies.

Marie Hopkinson, a Chinese medicine practitioner in Australia, used the analogy of a plant to explain how these elements interact. The sun contributes fire to the plant, urging it to grow upward. The earth grounds the plant, allowing it to absorb nutrients. Metal refers to the wind and air, giving the plant oxygen. Also, the plant needs water to grow. If any of these elements get out of balance, the plant will not thrive. (To watch her video, follow link listed below to her video, "Why eat mostly cooked foods.)
I have been diagnosed by my acupuncturist as having dampness in my spleen, known as spleen energy deficiency, or spleen qi deficiency. The spleen-pancreas system, which is more of a functional term than a reference to these biological organs, is governed by the earth element. (To learn more about dampness in Chinese medicine, follow the link listed below to her video, "What is Dampness.)

Summer corresponds to the earth element because of its dampness. I have a particularly tough time with summer's humidity because I am allergic to molds, particularly leaf molds. Since we live in the woods, and not far from a large lake, I have to stay in the house with air filters on to get away from leaf mold.
Someone like me with a spleen-pancreas imbalance will suffer with chronic tiredness, a weak digestion, and many other issues. Imagine a plant that has been over-watered, sagging with yellow leaves and not growing as it should.

To understand the spleen-pancreas system's function, imagine a fire (the spleen) heating up a pot of fluids (the stomach). The stomach needs warm, moist, cooked foods so it does not have to overwork while getting the nutrients of the foods. If the fires of the spleen system has been depleted, like mine has, cold foods make it work too hard.
To gain energy, those with spleen energy deficiency will crave sweets. To supply this energy in a healthy way, not overloading the body with glucose which we all know creates a rollercoaster of sugar highs and lows, Chinese medicine recommends eating grains, especially rice, and some fruit, with plenty of vegetables. Fried foods, refined foods, dairy products and dampening fruits and vegetables should be limited.
Many of these changes have challenged me. As I mentioned in my previous blog, Total Health gave me a convenient table that categorizes food as drying, lubricating, neutral, and strengthening. Since not every practitioner agrees with what foods fit in what categories, I have chosen to follow Ting's advice. I use Pitchford's book as a reference. He provides in-depth descriptions of the various properties of foods along with information on what conditions they treat.

Unlike my mother, I do not excel in menu planning. When I was young, my brother and I were not allowed to just grab something to eat because my mother was probably planning to use it for a specific meal. My biggest challenge has been figuring out what to eat using Chinese medicine recommendations.
I found a recipe in Total Healing called "Morning Energy Mega Boost" that satisfies my desire for sweets in the morning. It contains oatmeal, protein powder, walnuts, black sesame seeds, bee pollen, figs, apricots, and dates. My stomach and my taste buds like it.
Having soup or rice congee, a soupy rice mixture, works for supper. Chinese medicine also recommends eating light in the evening, which I was already doing because the result is that I have less acid reflux at night.
This leaves the biggest dilemma--what to eat for our main meal. Chinese medicine recommends eating your main meal in the middle of the day. We have been doing that for quite some time because of my husband's work schedule. Pitchford recommends eating only a small amount of meat, but my husband and I have been eating meat all of our lives. I have yet to find many recipes that work for me, other than stir fries, because we have always centered our main meal around meat!
Open for suggestions!
Sources
Book References with links to them on Amazon:
Goldsmith, Ellen and Maya Klein. Nutritional Healing with Chinese Medicine. Robert Rose, 2017.
Pitchford, Paul. Healing with Whole Foods: Asian Traditions and Modern Nutrition. North Atlantic Books, 2002.
Ting, Esther and Marianne Jas. Total Health the Chinese Way: An Essential Guide to Easing Pain, Reducing Stress, Treating Illness, and Restoring the Body through. DaCapo Lifelong Books, 2009.
YouTube videos:
"What is Dampness? The Chinese Medicine Podcast with Marie Hopkinson," YouTube, uploaded by Chinese Medicine Podcast, 9 Jan. 2019, https://youtu.be/4u3N-N4kDMg?si=yBSL3E07DjuqJiRr.
"Why eat mostly cooked foods? The Chinese Medicine Podcast with Marie Hopkinson," YouTube, uploaded by Chinese Medicine Podcast, 13 Jul. 2071, https://youtu.be/hXprIWs1xeg?si=pX6v3nHphcfv4UJ2.
2 notes
·
View notes
Text
Doctors want Queensland to set up LGBTQIA+ suicide register
New Post has been published on https://qnews.com.au/doctors-want-queensland-to-set-up-lgbtqia-suicide-register/
Doctors want Queensland to set up LGBTQIA+ suicide register

The Australian Medical Association Queensland has called on the state government to fund a voluntary register to allow bereaved family and friends to notify suicides in the LGBTQIA+ Sistergirl Brotherboy community.
The state’s peak body for doctors made the call in a submission ahead of the state budget next month.
“Members of the lesbian, gay, bisexual, transgender, queer, intersex, asexual, sistergirl and brotherboy (LGBTQIASB+) community face unique barriers and challenges in accessing healthcare that is culturally safe and appropriate for their needs,” AMA Queensland President Dr Maria Boulton (pictured) said.
Recent Australian research shows more than 80 per cent of young LGBTQIASB+ people experienced suicidal ideation, attempted suicide or self-harmed.
“This community faces ongoing discrimination in healthcare settings by all practitioner groups and the broader public,” Dr Boulton said.
“Along with outdated institutional processes, this contributes to poorer health outcomes within the community, including in mental health.”
Dr Boulton warned that we “do not know the true extent of suicide” in the community.
“Police reports and coronial findings rely on family or friends knowing and disclosing their loved one’s sexual or gender identity,” she said.
“Without this data, we do not know the full extent of the issue.
“We cannot work with the community and government effectively to develop measures to enhance mental health outcomes and keep people healthy and alive.
“We’re calling for funding and reform to enable a voluntary register. [It would] allow surviving partners, family, friends and clinicians to notify suicides to a suitable body – a university or the Australian Institute of Health and Welfare – for liaison with the Coroner.
“We’re also calling for legislative amendments to allow doctors to release information to the register, with family approval.”
AMA Queensland: ‘Our profession must do better’
It’s one of a suite of measures AMA Queensland has called for to improve health outcomes for the community.
Dr Boulton said a new LGBTQIASB+ Working Group is pushing for equity for all patients and practitioners.
“The most recent Medical Training Survey showed workplace discrimination and bullying of non-binary medical trainees,” she said.
“Our profession must do better.
“In Queensland, more than half of reported perpetrators were other health practitioners. This includes senior medical staff, nurses and midwives.
“The majority of non-binary trainees who experienced mistreatment indicated they did not report incidents as they believed nothing would be done.
“This indicates a lack of resources and support available for non-binary staff in the workplace, and a lack of respect and recognition for non-binary colleagues.”
The 2024-25 Queensland Budget will be released on June 11, 2024.
If you need someone to talk to, help is available from QLife on 1800 184 527 or online at QLife.org.au and Lifeline on 13 11 14, Kids Helpline on 1800 55 1800, or beyondblue on 1300 22 4636.
Read more from Queensland:
Queensland’s new birth certificate laws begin next month
Queensland’s hate crime and vilification laws just got stronger
Votes now for this year’s Queens Ball Award nominees
Brisbane Hustlers fly to Rome to bring Bingham Cup home
Queensland Police unveil apology plaque for IDAHOBIT
For the latest LGBTIQA+ Sister Girl and Brother Boy news, entertainment, community stories in Australia, visit qnews.com.au. Check out our latest magazines or find us on Facebook, Twitter, Instagram and YouTube.
2 notes
·
View notes
Text
Exploring Nursing Opportunities Abroad: Top Countries for Indian Nurses
Nursing is one of the most in-demand jobs inside and outside India. A profession that is in most demand in GCC countries for Indians is the nursing job. For Indian nurses, who are looking to broaden their horizons, many countries are waiting with promising career opportunities. If you are a skilled nurse and have multilingual capabilities then wide opportunities will be there. The overseas opportunities will give you high pay as well as a high-standard working environment. The respect for nurses outside India is much higher than inside India. Nurses are being recruited through top nursing consultancy in Kerala and here is a list of the top countries that offer promising careers.
Five top countries that offer promising nursing career
United Arab Emirates: Dubai which is an opulent city right due to cultural and development richness hires nurses from India. A large part of nurses who work in Dubai are Indian and they a decent pay but not much higher than European and American countries. But the most attractive feature of Dubai is that the nurses can take their entire income to their homeland since there are no taxes. In Dubai, there are many world-class hospitals, medical centers, and clinics that offer good employment prospects for Indian and other nationalities.
Saudi Arabia: In Saudi Arabia, there are a plethora of job opportunities for nurses in both the private and Government sectors. They offer good pay, accommodation facilities and also travel allowances. Saudi Arabia is one of the largest nations in GCC countries and also the pilgrimage place for Muslims, the demand for medical facilities is very high. The demand for trained professionals especially from India is of high demand in Saudi. However, finding the right opportunity is a bit challenging since there is a high scam in the field of recruitment.
Canada: Canada is a country that offers a healthcare system with the highest standard. This country is facing staff shortages and is now actively recruiting nurses worldwide. The high-quality life and the welcoming stances towards immigrants make Canada an excellent choice for nurses. The medical facilities and education are completely free for immigrants.
Australia: Australia's flourishing healthcare industry and stunning landscapes attract nurses worldwide. With modern facilities and advanced technology, nurses can work efficiently. During leisure time, they can explore the country's picturesque natural environment. Competitive salaries and excellent benefits make it a lucrative career option. To work as a nurse in Australia, one must register with the AHPRA (Australian Health Practitioner Regulation Agency) and pass English language proficiency tests.
United States of America (USA): The USA boasts a robust healthcare system with a significant demand for skilled nurses across various specialties. Indian nurses aspiring to work in the USA can pursue opportunities through programs like the H-1B visa for skilled workers or the EB-3 visa for professionals with tertiary education. Opportunities exist in hospitals, clinics, long-term care facilities, and community health settings throughout the country.
United Kingdom (UK): With its National Health Service (NHS), the UK offers extensive opportunities for Indian nurses to work in both public and private healthcare sectors. The UK's Nursing and Midwifery Council (NMC) oversees the registration process for international nurses, which includes passing the Occupational English Test (OET) or International English Language Testing System (IELTS) and meeting other requirements. Work settings range from hospitals and nursing homes to community healthcare centers.
Conclusion
If you are planning for an overseas nursing job, first research the rules and regulations for immigrants. Based on it decide which country is most suitable for you. There will be medical tests, mandatory examinations, and other verifications for each country. It is better to connect with any nursing consultancy in Kerala before you plan to move, they will guide you through the process and also provide you with data regarding the recruitment.
3 notes
·
View notes
Text
Holidays 8.7
Holidays
Aged Care Employee Day (Australia)
Assyrian Martyrs Day
Banana Day (Japan)
Bank Holiday Act Day (1871; UK)
Battle of Boyacá Day (Colombia)
Beach Party Day
DeviantArt Day
Dodge 807 Day
807 Giving Day
Freberg Day
Gaia Consciousness Day
Gallia Asteroid Day
Guru Rimpoche's Thungkar Tshechu (Sikkim, India)
Lock Day (French Republic)
Martyrs Day (Assyrian Community)
National Armed Forces Day (Bolivia)
National Day of Recognition for Aboriginal & Torres Strait Islander Health Workers & Practitioners (Australia)
National Handloom Day (India)
National Javelin Day (India)
National Lighthouse Day
National Marriage Equality Day
National NFT Day
National Psychiatric Technician Appreciation Day
National Report Health Care Fraud Day
Particularly Preposterous Packaging Day
Patient Appreciation Day
Postal Inspector Service Day
Professional Speakers Day
Purple Heart Day
Republic Day (Ivory Coast)
Say ‘Cheese’ Day
Sea Serpent Day
Take Last Winter's Snowballs Out of the Freezer and Have a Fight Day
Tasoua Hosseini (Iran)
Tightrope Walking Day
Tisha b'Av Bank Holiday (Israel)
Viking Pilgrimage (Spain)
Web Developer Appreciation Day
World Alternatives Games Day
World Lighthouse Day
World PVNH Disorder Awareness Day
Youth Day (Kiribati)
Food & Drink Celebrations
Pork Burger Day
Raspberries ’n Cream Day
Independence & Related Days
Cote d'Ivoire (a.k.a. Ivory Coast, from France, 1960)
Irish Reform Act (Passed; UK; 1832)
Ottawa (Became Capital; Canada; 1858)
Paperis (Declared; 2018) [unrecognized]
1st Wednesday in August
International Play Day (UK) [1st Wednesday]
IPA (International Play Association) Canada National PlayDay (Canada) [1st Wednesday]
National Professional Engineers Day [1st Wednesday]
National Psychiatric Technician Appreciation Day [Wednesday of 1st Full Week]
Regatta Day (Canada) [1st Wednesday]
Festivals Beginning August 7, 2024
Brown County Free Fair (New Ulm, Minnesota) [thru 8.11]
DeLeon Peach & Melon Festival & Tractor Pull (DeLeon, Texas) [thru 8.10]
Pea Harvest Festival (Palmer, Alaska) [Historically; 1920]
Lakefest (Eastnor, United Kingdom) [thru 8.11]
Locarno Film Festival (Locarno, Switzerland) [thru 8.17]
Medusa Festival (València, Spain) [thru 8.11]
Nevada County Fair (Nevada City, California) [thru 8.11]
Southdown Sheep Fair (Lewes, Sussex, England) [Historically]
Sziget Festival (Budapest, Hungary) [thru 8.12]
Taste of Andersonville (Andersonville, Chicago, Illinois)
West Point Sweet Corn Festival (West Point, Iowa) [thru 8.11]
Wikimania (Katowice, Poland) [thru 8.10]
Feast Days
Adonia (Honoring Adonis; Ancient Greece; Everyday Wicca)
Afra (Christian; Virgin Martyr)
Albert Kotin (Artology)
Albert of Trapani (Christian; Saint)
Betsy Byars (Writerism)
Breaking the Nile (Festival Honoring Hathor & All River Goddesses; Ancient Egypt)
Builth, the Footprint of Arthur’s Hound (Celtic Book of Days)
Cajetan of Thienna (Christian; Saint)
Carpophorus and companions (Christian; Saint)
Claudia (Christian; Matron)
Dometius of Persia (Christian; Saint)
Donatus of Arezzo (Christian; Saint)
Donatus of Besançon (Christian; Saint)
Donatus of Muenstereifel (Christian; Saint)
Emil Nolde (Artology)
Eugene the Hunting Dog (Muppetism)
Feast of 'Aut-Yeb (Personification of Female Joy; Egypt)
Feast of Cromn Dubh (Pre-Celtic God of the Harvest & the Underworld; Starza Pagan Book of Days)
Feast of the Name of Jesus (Christian, excluding Roman Catholic) [also 1.2]
Filseta (Ethiopian and Eritrean Orthodox Tewahedo Church)
Garrison Keillor (Writerism)
Harvest Holiday (Slavic Pagan)
Henri Le Sidaner (Artology)
Idi Amin Day (Church of the SubGenius; Saint)
Intergalactic Intercourse Day (Pastafarian)
International Beer Day (Pastafarian) [also 7.29]
John Mason Neale and Catherine Winkworth (Episcopal Church (USA))
Nantovinus (Christian; Saint)
Neith’s Day (Breaking of the Nile; Pagan)
Nikolai Triik (Artology)
Peter, Julian, and companions (Christian; Martyrs)
Rien Poortvliet (Artology)
Sixtus II, Pope (Christian; Saint)
Smartest Leprechaun Eisteddford (Shamanism)
Stan Freberg Day (Humorism)
Thomas à Kempis (Positivist; Saint)
Togrul Narimanbekov (Artology)
Victricius (Christian; Saint)
Lucky & Unlucky Days
Butsumetsu (仏滅 Japan) [Unlucky all day.]
Fortunate Day (Pagan) [30 of 53]
Umu Limnu (Evil Day; Babylonian Calendar; 36 of 60)
Premieres
All Out For ‘V’ (Terrytoons Cartoon; 1942)
Beach Party (Film; 1963)
Billy the Mountain, by Frank Zappa recorded live (Song; 1971)
Condorman (Film; 1981)
Dreamworks’ Dragons (Animated TV Series; 2012)
8701, by Usher (Album; 2001)
Fantastic Four (Film; 2015)
Farmer Al Falfa’s Ape Girl (Terrytoons Cartoon; 1932)
A Feather in His Collar (Disney Cartoon; 1946)
The Gallopin’ Gaucho (Ub Iwerks Disney Cartoon; 1928)
Half-Pint Pygmy (MGM Cartoon; 1948)
Heavy Metal (Animated Film; 1981)
I Can’t Get Started, recorded by Bunny Berigan (Song; 1937)
I Cover the Waterfront, recorded by Billie Holiday & Teddy Wilson (Song; 1941)
It Ain’t Me Babe, by The Turtles (Song; 1965)
Janie Get Your Gun (Woody Woodpecker Cartoon; 1965)
Jesus Christ Superstar (Film; 1973)
Julie & Julia (Film; 2009)
Just Another Band From L.A., by Frank Zappa and the Mothers if Invention (Album; 1970)
Lighthouse Keeping Blues (Chilly Willy Cartoon; 1964)
Lud-in-the-Mist, by Hope Mirrlees (Novel; 1926)
Lumpy Gravy, by Frank Zappa (Album; 1967)
New England Courant (Daily Newspaper; Boston, Massachusetts; 1721)
Percy Jackson: Sea of Monsters (Film; 2013)
Porky’s Railroad (WB LT Cartoon; 1937)
Prehistoric Pink (Pink Panther Cartoon; 1968)
Satan’s Waitin’ (WB LT Cartoon; 1954)
Snuffy’s Party (Oswald the Lucky Rabbit Cartoon; 1939)
3:10 to Yuma (Film; 1957)
Til Tok, by Kesha (Song; 2009)
Unforgiven (Film; 1992)
Wanted For Murder (a.k.a. Paging the Saint), by Leslie Charteris (Short Stories; 1931) [Saint #7]
Weeds (TV Series; 2005)
We’re the Millers (Film; 2013)
Who’s That Girl (Film; 1987)
Yan Tan Tethera, by Harrison Birtwistle (Opera; 1986)
You’re a Sap, Mr. Jap (Fleischer/Famous Popeye Cartoon; 1942)
Today’s Name Days
Afra, Albert, Cajetan (Austria)
Albert, Donat, Kajetan, Siksto (Croatia)
Lada (Czech Republic)
Donatus (Denmark)
Hiljar, Hiljo, Vaido, Vaigo, Vaiko (Estonia)
Lahja (Finland)
Gaétan (France)
Afra, Albert, Cajetan, Dominikus (Germany)
Asterios, Astero, Astini, Nikanor (Greece)
Ibolya (Hungary)
Donato, Gaetano (Italy)
Alfrēds, Helara, Madars (Latvia)
Drąsutis, Jogilė, Kajetonas, Klaudija, Sikstas (Lithuania)
Didrik, Doris (Norway)
Albert, Alberta, Albertyna, Anna, Dobiemir, Donat, Donata, Doris, Dorota, Kajetan (Poland)
Štefánia (Slovakia)
Cayetano, Jordán, Sixto (Spain)
Denise, Dennis (Sweden)
Claude, Claudette, Claudia, Claudine, Donata, Donato, Donica, Donzel, Gladys (USA)
Today is Also…
Day of Year: Day 220 of 2024; 146 days remaining in the year
ISO: Day 3 of Week 32 of 2024
Celtic Tree Calendar: Coll (Hazel) [Day 5 of 28]
Chinese: Month 7 (Ren-Shen), Day 4 (Guy-Mao)
Chinese Year of the: Dragon 4722 (until January 29, 2025) [Wu-Chen]
Hebrew: 3 Av 5784
Islamic: 1 Safar 1446
J Cal: 10 Purple; Threesday [10 of 30]
Julian: 25 July 2024
Moon: 9%: Waxing Crescent
Positivist: 23 Dante (8th Month) [Thomas à Kempis]
Runic Half Month: Thorn (Defense) [Day 15 of 15]
Season: Summer (Day 49 of 94)
Week: 1st Full Week of August
Zodiac: Leo (Day 17 of 31)
Calendar Changes
Ṣafar [صَفَر] (Islamic Calendar) [Month 2 of 12] (Void Month)
1 note
·
View note
Text
Sense Of Self Life Coaching
Address:
Studio 1- 5/40 Green St, Windsor, VICTORIA 3181 Australia
Phone Number:
+61 413888240
Business Email
Website
Owner Full Name
Christina Carnie
Business Description
Welcome to Sense of Self, a safe space where personal growth is redefined. As a dedicated Certified Life Coach and Practitioner of Emotional Intelligence, my focus is to help clients re-evaluate and re-formulate a more meaningful and valuable life. In a world where challenges like depression, stress and burnout are prevalent, self-awareness, self-acceptance, and self-worth are key. Are you ready and willing to dive deep into your own sense of self? To be open to implementing new behavioural changes, coping strategies and ideations? I am here to help answer the question 'What does a valuable life look like for you? and how best can this be achieved'?
Life coaching is a transformative partnership between you and me, focused on facilitating personal and professional development. Through proven methodologies and tailored strategies, I provide guidance, support, and accountability to help you navigate challenges, clarify objectives, and unleash your innate capabilities.
My holistic approach to well-being addresses multiple dimensions, including emotional, psychological, and social factors. I explore various areas of life, including personal and interpersonal, career, relationships, family, health and spiritual fulfillment. Whether you're seeking clarity in your career path, balance in your relationships, or a renewed sense of purpose, I'm equipped with the expertise to guide you towards sustainable success and fulfillment.
I prioritise individualised attention and customised solutions. Through in-depth assessments and collaborative goal-setting, I ensure that our coaching sessions are aligned with your unique aspirations and circumstances. By fostering self-awareness, resilience, and actionable strategies, I empower you to overcome obstacles, cultivate confidence, and create meaningful change in your life.
Business Hours
Monday – Thursday 9am – 8pm
Friday – 10am – 4pm
Saturday – Sunday 10am – 3pm
#Workplace Wellbeing#Personal Coaching#Life Coaching#If you're feeling stuck#unmotivated#lost#heavy#or have not been achieving your desired results#Christina’s Sense of Self specialised holistic coaching and mindset mentoring services can provide the support you need to address challeng#Christina assists individuals in identifying and overcoming mental blocks#gaining self-awareness#and achieving desired outcomes. Christina assesses your current situation#address any challenges or blocks#and set goals for personal growth. By gaining self-awareness and establishing self-acceptance#space is made for growth. Reframe your mindset#unlock your potential#and transform your reality with Sense of Self#Enhancing workplace wellness through holistic life coaching to support employee well-being#stress management#personal growth#and professional development outcomes. One on One Coaching Sessions available#alongside group workshops.
1 note
·
View note
Text
Charlotte Jerrim was just 19 when she decided upon breast implants.
The now 28-year-old said there were no checks of her physical or mental health beforehand, nor was she properly warned about the risks.
“I was young and I purely wanted them for cosmetic reasons,” the Canberra woman told this masthead. “At the time, a lot of my friends had them and there was social pressure to have bigger boobs.”
It was not long before she started to experience issues with her health; brain fog, a rash that would come and go, migraines, chronic fatigue and changes to her menstrual cycle. She battled the symptoms for six years before being diagnosed with Systemic Symptoms Associated with Breast Implants (SSBI) and opted to have an explant.
“If I had been counselled about why I wanted the surgery and properly made aware of the associated risks, I don’t think I would have got them,” she said.
Anyone considering cosmetic surgery is now required to have a referral to the surgeon from a general practitioner who will assess the mental and physical health of patients before recommending them for any procedure.
The requirement is part of the Australian Commission on Safety and Quality in Health Care (ACSQHC) new National Safety and Quality Cosmetic Surgery Standards (Cosmetic Surgery Standards), to be implemented alongside every service where cosmetic surgery is performed, from small day procedure clinics, through to large health organisations and builds on rules announced by the Australian Health Practitioner Regulation Agency (AHPRA) in July.
Along with patient suitability, cosmetic surgery advertising must now comply with legislation and national codes and guidelines to avoid manipulating or deceiving customers.
Clinicians must obtain informed consent from patients about expected outcomes, potential risks and possible outcomes, and the costs associated should complications arise. They must also establish a complaints service and seek feedback from patients about their experiences and outcomes or care.
Services are now required to have credentialing processes to verify the qualifications and experience of all practitioners performing cosmetic surgery. Meanwhile, post-operative care instructions must be provided to patients, including what to do in case of an emergency, with clinicians to ensure comprehensive post-operative reviews are undertaken.
The standards do not include non-surgical procedures such as cosmetic injectables and thread lifts and fat freezing.
Since September 2022, the Australian Health Practitioner Regulation Agency has fielded 179 formal complaints and 428 calls to the Cosmetic Surgery Helpline. It is estimated that $473 million has been spent in Australia this year on cosmetic surgery, according to IBS World research.
#auspol#anti beauty culture#radical feminist#anti beauty industry#beauty culture#seriously guys just do not get breast implants#there are so many stories about awful side effects#it isn't worth it!
3 notes
·
View notes
Text
Yes! Small steps are worth more than people think.
Showing my age here, but before 2004 Australia had no public Medicare coverage for non-emergency treatments like podiatrists, psychologists, physiotherapists, and other allied health specialists. If you needed to see a podiatrist, for example, you had to pay privately without being able to get any money back from the government.
A lot of health practitioners were pushing for that the change, because they knew the public needed help. Finally bloody Tony Abbot, the Health Minister under Prime Minister John Howard, was pushed to introduce the Enhanced Primary Care plan (EPC).
It granted a generous 5 visits per year that people could claim back (some of the cost) from Medicare. It barely covered some treatment and was wholly insufficient for most of what was needed, because how much can you really get done with only 5 visits? Not much.
But we jumped on it! My former boss put it this way: "at least it was something."
In the years since, coverage for psychology has expanded to 10 visits per year. We're still working on dental coverage at all.
But at least it's a start. Take the small wins and use them as stepping stones.
My biggest frustration with the left has always been the inability/unwillingness to work on making progress inside of the system while advocating for greater change.
I remember the first time I came to this realization.
I was nineteen, pregnant. We couldn’t afford to heat the house because we couldn’t afford the deposit to turn the gas on. It was miserably cold. The duplex we were renting was old and rickety and drafty. The window frames were messed up and there were cracks you could stick your finger through that were open to the elements.
Just, like, to give you an idea where we were financially. And this was better than we’d been doing before!
Anyway, I had recently started going to DSA meetings. And that month, they were talking about how a moderate democrat had successfully gotten a small increase in WIC benefits monthly. It came out to, like, $10 a month.
The members talking—mostly male, almost all doing decent—were scornful. The democrat should have pushed harder and gotten more, refused to accept anything until everyone else caved to their demands. I remember sitting there, quietly drinking the latte in the smallest size they had that I had bought with scrounged quarters, listening. Wishing it wasn’t held in an indie coffee shop because it was a luxury I really couldn’t afford, but it would be rude not to. Enjoying the coffee anyway.
I was one of the lucky ones who was getting that additional $10 a month through WIC. Even more exciting, we were now getting a voucher for the farmers’ market. I casually mentioned that WIC recipients would now be getting farmers’ market vouchers, too.
The guy who organized the meetings was a hard worker, passionate guy. Did something in tech.
He was like, “That’s the thing! These people don’t want farmers market vouchers. They want—” and he went on to describe a bunch of pie in the sky desires. That, yeah, sounded good.
But one. I was one of those people! A lot if the tamiles were super excited about it, myself included.
I had never been to a farmers’ market before. I tried arugula for the first time, a piece pulled from a bunch by the grower as he explained the flavor difference. I hadn’t known before then that different lettuce greens had different flavors, that it was more than just the texture and shape. I tried pesto, which delighted me. Goat cheese. I got three full pounds of strawberries for two dollars, since they were closing soon and the old man selling the berries got a kick out of me.
Anyway. It was like, you have a decent life. Not great but decent! The things that are life changing for me, for us… you already have.
The ten dollars at the grocery store made the difference between a meal of broken-noodles-with-some-half-horrible-pantry-scraps and a meal. It kept me full and healthy! And the additional farmers’ market voucher was world changing for me.
The democrat who worked for those things barely got them through. And it was means tested to hell and back. They weren’t able to get everything they wanted. But what they got made such a huge difference for me, for people like me.
35K notes
·
View notes
Text
By: Bernard Lane
Published: Jul 21, 2023
A rising star of Australia’s centre-right Liberal Party, Claire Chandler, has called for an independent expert inquiry into medicalised gender change for minors.
Senator Chandler suggests a national inquiry into the evidence for treatment of young patients diagnosed with gender dysphoria could be modelled on England’s independent review led by paediatrician Dr. Hilary Cass following controversy over the London-based Tavistock gender clinic.
In an interview with GCN, Senator Chandler said: “We know that in Australia there has been a huge explosion in the number of young children accessing care at gender clinics.
“We don’t necessarily know exactly how all of these children are being treated, whether or not the way they are being treated is beneficial for their circumstances, whether or not it’s having good clinical outcomes.”
The number of minors enrolled in state children’s hospital gender clinics rose from less than 500 in 2016 to more than 2,000 in 2021, with the biggest caseloads in the states of Victoria and Queensland.
In Australia’s federation, the states deliver health while also drawing on federal funding; states pay for puberty blockers and cross-sex hormones enjoy federal subsidy.
Chart: Demand surges at Australia’s gender dysphoria clinics in children’s hospitals
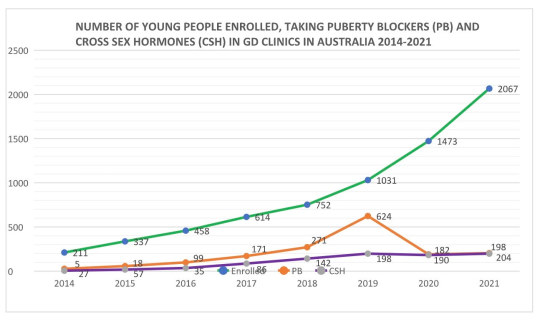
[ The green line shows patient enrolments; orange tracks the number of children on puberty blockers; purple indicates the number on cross-sex hormones. Data was obtained under freedom of information law. It is not clear if these figures for hormonal treatment include prescriptions filled outside the hospital. Credit: Dr. Dianna Kenny ]
Europe’s turn to caution
Senator Chandler cited official findings in Finland, Sweden and England that the puberty blockers and cross-sex hormones given by gender clinics internationally are based on very weak evidence and carry risks of harm and troubling uncertainties.
In each country, the recent policy advice is to restrict access to these hormonal treatments for minors, especially puberty blockers, which England’s National Health Service will confine to clinical trials as an experimental intervention.
Senator Chandler has been raising concerns for more than two years about the risks to vulnerable children from invasive medical treatments and the lack of good public data on the operation of gender clinics.
In the last few months, an Australian child and adolescent psychiatrist Dr. Jillian Spencer has become a rallying point for growing clinical disquiet over the dogmatic “gender-affirming” treatment model and its poorly evidenced hormonal and surgical interventions.
She went public with her criticism of the American-influenced gender-affirming treatment model after she was stood down from her job as a senior staff specialist at a public children’s hospital in Queensland; she was reportedly accused of “transphobia” after an interaction with a young patient from the gender clinic.
Dr. Spencer has argued that the gender-affirming model forces clinicians to go along with the social and medical transition of children despite the evidence base not showing that the benefits outweigh the risks and harms.
“It is incredibly distressing to be forced into harming other people’s children, or otherwise face potential loss of one’s career, livelihood or to be cast out of the workplace, as has happened to me,” she said at a Sydney women’s forum last month.
Earlier this month Dr. Spencer began circulating a petition for health practitioners who want an independent inquiry “to guide Australian doctors in what treatments for children are safe to be delivered, at what age and under what conditions.”
By last night, she had signatures from 36 child psychiatrists, 33 adult psychiatrists, 22 general practitioners and 10 paediatricians straddling all six states, albeit mostly concentrated in the three eastern states of Queensland, New South Wales and Victoria.
“Sadly, lots of people have contacted me to say they’re too scared to give their details,” Dr. Spencer said.
In September 2019, after The Australian newspaper began subjecting gender clinics to scrutiny, doctors launched an online petition for a parliamentary inquiry as requested by professor of paediatrics Dr. John Whitehall. They collected 260 names in three and a half days before a spam attack by activists forced closure of the petition. The signatories included 20 professors or associate professors, 14 paediatricians, 20 psychiatrists (nine of them child psychiatrists), and “many other doctors with a shared concern about the epidemic of childhood gender dysphoria and the lack of scientific basis for its current treatment”, organisers said.
Exposure
This week, the medical indemnity fund MDA National, which on July 1 cut back its coverage of private doctors involved in risky medicalised gender change for minors, has noted the renewed push for an inquiry in Australia.
“We understand that there is a growing number of professionals and politicians requesting an urgent review of the research to ensure that children and adolescents presenting with gender dysphoria and incongruence have the very best medical care,” MDA National’s spokeswoman told GCN.
She was responding to a decision by the Australian Medical Students’ Association (AMSA) to disaffiliate from MDA National on the grounds that its July 1 policy change would reduce the supply of youth gender medicine. AMSA’s statement claimed that gender-affirming treatment was based on “high-quality evidence” but did not reply when asked for references.
MDA National said it was disappointed at AMSA’s decision—the insurer had spon.sored association events—but stressed that its main duty was to protect its doctor-members from “the risk of potentially high-value claims.”
The spokeswoman said the fund would “continue to monitor the legal landscape of this area of emerging risk and will update our policy coverage to reflect any changes in medico-legal risk as required in the future.”
Litigation by regretful detransitioners has begun in Australia, Canada, the United Kingdom and the United States.
“[The health professional defendants] lied when they told Prisha she was actually a boy; they lied when they told her that injecting testosterone into her body would solve her numerous, profound mental and psychological health problems; and they lied when they told her about the nature and effects of ‘breast reduction’ surgery, which in actuality was a surgery to remove her healthy breasts and render her incapable of nursing a child (should she even be able to conceive one, which, due to her taking testosterone for years, may not be possible)”—court complaint of 25-year-old detransitioner Prisha Mosley, North Carolina, U.S.,17 July 2023
Evidence rules
This week Australia’s National Association of Practising Psychiatrists (NAPP)—which in 2020 issued a cautious, less medicalised policy on managing youth gender dysphoria—restated its view that a proper inquiry into gender clinics is needed.
“We support an objective national inquiry headed by a panel of experts that allows all sides of the debate to be expressed,” NAPP president Dr. Philip Morris told GCN.
“But the bottom line is that the inquiry must be based on the evidence base, not opinion.”
The Royal Australian and New Zealand College of Psychiatrists, a larger group than the NAPP, is expected to publish its updated position statement on gender dysphoria “later this year”, the president Dr. Elizabeth Moore has told members.
In 2021, the college adopted a more cautious policy, noting the “paucity of quality evidence” on treatment outcomes and acknowledging that “evidence and professional opinion is divided as to whether an affirmative approach should be taken in relation to treatment of transgender children or whether other approaches are more appropriate.”
The policy was denounced as “inappropriate and harmful” by a group of Australian and New Zealand advocates of the gender-affirming way.
From March-September 2019 the college’s LGBT mental health policy had explicitly endorsed the gender-affirming treatment guidelines promoted as “Australian standards of care” by the Royal Children’s Hospital Melbourne, which is home to the country’s most influential gender clinic. Those guidelines have come under intense scrutiny.
Video: Senator Chandler denounces inquiries that went nowhere
youtube
In the hunt
After critical coverage of gender clinics began in mid-2019 in The Australian, the then health minister Greg Hunt asked the Royal Australasian College of Physicians (RACP) to conduct a review.
In March 2020 the RACP sent Mr. Hunt a four-page letter of advice. It did not describe gender clinic medical treatments, nor discuss their risks; there was no mention of less invasive treatment options.
Instead, the RACP asserted that the national inquiry being sought by some health professionals “would further harm vulnerable patients and their families through increased media and public attention.” No evidence was offered for this claim.
It emerged that the RACP, which trains paediatricians, had previously lobbied for cheaper, quicker access to the medical treatments it was called upon to evaluate for Mr. Hunt. The RACP did not reply when asked at the time if it had a conflict of interest.
Mr. Hunt then gave public assurances that a federal-state body of health officials—the Health Chief Executives Forum—would deliver a new, uniform model of clinical governance across Australia’s gender clinics and a common system for proper data collection. Nothing appears to have come of this.
GCN understands that in response to recent questions from members, the RACP has—
claimed that the Health Chief Executives Forum has not responded to its request for an update on the promised progress towards a national approach to gender clinics acknowledged that its 2020 advice to Mr. Hunt “did not comment on specific clinical issues such as the use of puberty blockers and other treatments” conceded that much has happened in the field of gender dysphoria in Australia and internationally but says it has no plans to update the advice it gave to Mr. Hunt stated that it does not intend to develop clinical guidelines or position statements on the treatment of gender dysphoria
Against this background, Senator Chandler said an expert inquiry independent of government was “clearly required to lay the facts on the table and stop the buck-passing and the culture of silencing that everybody from parents to medical professionals to journalists have experienced and have been targeted with in this debate.”
She said the inquiry would also have to be independent of “the youth gender industry.”
“We can’t be in a situation where the [gender clinic] industry, which has in effect created its own rules, is then put into a position of reviewing those rules,” she said.
“And [the inquiry] must be run in a very transparent and evidence-based way that takes into account some of those international findings that we’ve seen in other jurisdictions [such as Finland, Sweden and England.]”
In the Australian Senate’s next sittings, starting on July 31, there is expected to be a vote on a motion for a committee inquiry into youth gender medicine.
Moved last month by Senator Pauline Hanson of the populist-right One Nation Party, the motion urges inquiry into questions including—
“whether children are being rushed into gender reassignment treatment” “whether psychiatrists such as Dr. Jillian Spencer … who question the use of puberty blockers without an appropriate mental health assessment are being silenced” “whether Australia should follow the United Kingdom and many European countries in adopting a more cautious approach to the prescription of puberty blocking drugs, amid concerns the evidence base for their efficacy is lacking” “whether the Commonwealth should take a greater oversight and regulatory role in the prescription of puberty blockers and cross-sex hormones to children following the admission from the federal government that it has no idea how widely the drugs are being prescribed off-label for gender dysphoria”
Asked about this proposal, Senator Chandler said a parliamentary committee inquiry would be better than no inquiry at all, but the numbers in the Senate would not favour an independent inquiry, and in any case, it would be better for an inquiry to be “removed from politics, if possible.”
The ruling centre-left Labor Party (with 26 of the total 76 senators) is seen as uncritically committed to the gender-affirming model, while the Australian Greens, with 11 senators, have lobbied for a taxpayer-funded expansion of these medical treatments.
The Liberal-National opposition, with 31 senators, will have a conscience vote on Ms Hanson’s motion. One Nation has two senators.
Note: GCN sought comment from federal Health Minister Mark Butler and Assistant Minister for Mental Health and Suicide Prevention Emma McBride
--
Australia makes awkward moves in the same direction as the UK and other European countries.
Interesting that the medical side of is being - at least partly - driven by the medical insurance industry; that doctors who subject patients to risky medical experiments will not be professionally protected when the patient comes back and sues. Doctors themselves might be able to deny the results of evidence reviews, but their insurers damn well won't. It's surprising the US, a much more litigious country, hasn't done more of this.
Also notable that you can tell at a glance which institutions have been ideologically compromised. The claim that there is "high-quality evidence" to support self-diagnosis and self-prescription of treatment is an ideological one. But they're never in favor of systematic reviews, for some reason. If what they're doing is so scientifically grounded, you'd think they'd be pushing to resolve this once and for all. They never do.
#Claire Chandler#Bernard Lane#Gender Clinic News#gender ideology#queer theory#gender affirming#gender affirming treatment#gender affirming care#affirmation model#medical malpractice#poor evidence#weak evidence#medical scandal#medical corruption#genderwang#sex trait modification#religion is a mental illness
8 notes
·
View notes