#Best Medical Healthcare for Students
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
The “We are the 99%” Tumblr blog became the slogan for the Occupy Wall Street movement.
Text

Streamline Your Health with the Best Student Healthcare App
Experience seamless healthcare with the Best Student Healthcare App. Offering quick consultations, comprehensive health tracking, and discounts on tests, it’s designed to fit into any student’s hectic schedule, ensuring top-notch care with minimal hassle.
For Any Query : Call: +91-8929920932 WhatsApp: +91-8690006254 Download App: https://play.google.com/store/apps/details?id=io.Hgpp.app&hl=enBest Health App for students in India
#Student Health App#Students Healthcare App#Best Student Healthcare App#Teenage Healthcare Company#Students Healthcare Company#Students Healthcare Centre#Student Health Services#Online Student Health Services#Best Medical Healthcare for Students#Student Online Health Clinic#Best Health App for students in India#Book Appointment With Doctor#Doctor Appointment Booking App#Book Doctor Consultation Online#Online Medical Consultation#Online Doctor Consultation App#Best Online Doctor Consultation App#Schedule Doctor Appointment#Doctor Booking App#Best App for Online Doctor Consultation#doctor consultation app#online doctor consultation#Online Consultation with Doctor#Online Doctor Appointment#Best Doctor Near Me#Consult Doctor Online#Online Doctor Consultation India
0 notes
Text

Nurse Croc charm, RN Jibbitz charm, cute Jibbitz Charm, cute Shoe Charm, RN shoe,Healthcare worker, Hero, DIY, Unique Gift, nursing students
#Nurse Croc charm#RN Jibbitz charm#Croc Charm#cute Jibbitz Charm#cute Shoe Charm#Nurse#RN#Healthcare worker#Hero#DIY#Unique Gift#student nurses gift#Shoe accessories#croc shoe accessories#best gift#nursing graduation gift#Medical croc charm#thank you#luxury croc charms#luxury gift#croc charm custom#croc charm Jibbitz#save a life#croc charm set#Jibbitz charm set#graduation gift
2 notes
·
View notes
Text
I went and found the original post in question, and I read all of the expectedly negative responses, so now I feel compelled to add this.
I’ve found almost universally that any nonmedical person talking about a failure of our medical system chooses to blame that failure on either the malice or the incompetence of individual doctors.
Earlier today I was on instagram and came across a reel mocking of the idea of hospitals having a physician week the way they have nurses week, and I think I finally realized why this happens.
Historically, physicians have been the owner/employer class. It is ingrained in our cultural consciousness that doctors are in charge. They own practices, they hire (and abuse and exploit and underpay and undervalue, etc etc) nurses, they make their own schedules, they choose whether they are willing to be there for you as a patient. Why would you hold an appreciation week for your CEO?
Except that’s very much not the case anymore. Doctors are employees now. They’re cogs in the machine. They’re told what to do and how to do it and spend mandatory meetings learning how to meet their metrics and get emails every month telling whether if they did it fast enough and cheap enough, from someone who couldn’t tell you the first thing about why.
As of 2023 a huge percentage of doctors - 77.6% - are employees of hospitals or corporations. I couldn’t find whether this number includes “independent contractors” like ER doctors, who are functionally employees. If it doesn’t, the number is even higher. And, because of how corporate medicine practices, I guarantee you these employee physicians account for an even higher percentage of patient encounters.
Since we’re almost 6 months into 2024, it has also almost certainly already gone up. This is not a casual shift. It’s an active corporate takeover. In 2018, that percentage was 47.4. Corporations and hospitals bought up 30% of private practice physicians in the past 6 years.
I’ve seen a lot of people mock the idea that working in medicine can be akin to a customer service job. But when such a majority of doctors are employees, it absolutely is. And much like blaming your waitress for being slow when the restaurant is understaffed, these corporations are counting on you blaming the doctor. If they demand your doctor perform an impossible amount of work caring for an impossible number of patients and you walk away thinking “my doctor just sucks” you’ve fallen for their grift.
I’m not saying this system doesn’t produce bad care, or that you shouldn’t be mad about receiving it. Quite the opposite. It provides horrible care! You should be mad!
But we have to be mad at the system which has deprived you of the quality care that your doctor wanted to give you. We can’t be so mad at the individual doctors. Even the ones who are so burnt out they aren’t trying anymore. Not because they should be allowed to be horrible, but because treating a symptom does not cure the disease.
I don’t know what the solution is here. I look at our healthcare system and I fear for our future. But I do know that blaming the corporations instead of the individuals and supporting doctors the way you would support any other exploited worker is a step in the right direction.
Got reblogged by Seanan McGuire again; can safely assume my notes will be a nightmare of people accusing me of being a lazy, incompetent, distracted, inhumane doctor, assuming they notice I’m a doctor. May take a week off.
People will simultaneously describe all the elements of the current US medical system that lead to burnout in service of making the very few shareholders very rich, and then pretend that doctors aren’t also profoundly negatively affected by it, and then decide the system is also actually our fault.
#obligatory I am a fat trans person who has faced medical discrimination for both of these things#and also received bad healthcare just because#the majority of doctors are well intentioned people doing their best#the majority of the ones who are not have been beaten down by the system#please if a doctor is complaining about the system don’t just assume they’re shitty people trying to excuse their own flaws#the system is so so so so so so so bad holy shit u don’t even know#we want and need more doctors to feel supported in speaking up about it#also if you can understand why someone would stay in an abusive relationship because they can’t afford to leave#you can understand why a physician will work for a corporation that continues to beat them down#the amount of debt medical students graduate with is astronomical#it does not allow for financial risk like starting your own practice to compete against corporations with seemingly endless resources#literally this is the anticapitalism website we all know all of the concepts that we need to understand the healthcare system#as long as we accept that doctors have become workers#and stop thinking of them as the elite
857 notes
·
View notes
Text
Also Preserved in our archive (Daily updates!)
What if the pandemic safety net cobbled together in 2020 had been a new beginning?
What if when Joe Biden came into office in 2021, the Covid-19 safety net he was handed had become a new floor?
What if that was his baseline—and the newly elected Democratic president, sold by his most ardent supporters as FDR 2.0, had used our Covid-19 response as the bare minimum of a new social contract with Americans?
What if the caring nature of the best aspects of the US Covid response became the map for international relations—leading not just to international cooperation on infectious disease, but on matters of war, climate and genocide?
What if, instead of dismantling the vaccine-delivery infrastructure—which, at its height, delivered some four million shots in a single day—the Biden administration built upon and made some version of it permanent, so that everyone could easily get annual Covid boosters, annual flu vaccines, or get specialty vaccinations during outbreaks of unusual viruses (such as for mpox during the 2022 summer outbreak among queer men) whenever they needed it?
What if the viral surveillance and communication mechanisms utilized for learning about SARS-CoV-2, treating it and telling the public about it were being used to address H5N1—a virus which has been moving from birds to farm mammals to humans with so little notice that dead cows were killed by the “avian flu” and left on the side of a road in California’s Central Valley, as “Thick swarms of black flies hummed and knocked against the windows of an idling car, while crows and vultures waited nearby—eyeballing the taut and bloated carcasses roasting in the October heat”?What if the leaders of the Democratic party had used Covid as a blueprint to make a national platform based on care?
What if all the ways Covid had made clear how farmers, industrial butchers, kitchen staff and other food workers are the most at risk people amongst us to viral infection led to meaningful, permanent protections, such that they were much less likely to contract not just SARS-CoV-2 but H1N1, H5N1, influenza, or any other existing or novel pathogens?
What if all the all the ways Covid exposed how unsafe industrial food production is (for the workers who make it and the people who eat it alike) had triggered safety reforms, instead of having these warnings ignored and leading towards record numbers of safety recalls for e-coli, Salmonella, and Listeria?
What if an airborne pandemic had led to indoor air being as filtered, treated and regulated as drinking water?
What if everyone with a child was still getting a $300 check from the US treasury, so that having a child was not a gambling-style risk, but a responsibility shared with all of society?
What if the paused-for-years student debts were forgiven, so that young people could actually begin their lives?
What if Biden built on Americans’ experience of just showing up somewhere to get the medical care they needed to create a universal healthcare system?
(What if Kamala Harris built upon Americans’ taste of not getting charged at the point of such service—and campaigned on Medicare for All?)
What if once the link between Covid and homelessness was established, the Democrats had pushed infectious disease as just one reason for an end to evictions and a robust, public-health-backed campaign to end homelessness and stop the United States from having more people living on the streets than any other country?
What if after the link between Covid and incarceration was established, the Democrats had pursued decarceration as a public health measure and—instead of throwing weed and cryptocurrency at us—had made reducing incarceration a centerpiece of the Harris campaign to earn the votes of Black men?
(What if after 100,000 Californians died of Covid and the links between Covid, homelessness and incarceration were clear, residents of the Golden State chose to allow rent control and to abolish legal slavery in prisons—instead of voting to ban rent control and to continue prison slavery?)
What if the leaders of the Democratic party had used Covid as a blueprint to make a national platform based on care?
Would we be in the lethal position we are now—with a genocide raging abroad, Covid deaths in the hundreds every week at home, a poisoned food supply, $17 trillion in household debt, oligarch goons ready to dismantle government regulations, and a sociopath heading back into the White House—if Covid had been the floor?
#mask up#covid#pandemic#public health#wear a mask#wear a respirator#still coviding#coronavirus#covid 19#sars cov 2#us politics#democratic party#ditch the dems
294 notes
·
View notes
Note
Do you have any tips for writing Obi Wan or any meta in mind with his characterizarion?
hmmm sure why not! i'll give a few tips on how i'd write obi-wan. mind you this is how i interpret the character, so ymmv.
i truly do not like it when fics have obi-wan voluntarily leaving the order. like it's so out-of-character for me in my head that the premise of the story + the writing would have to work triple-time to get me to stick around. now if he's been removed from it by an EXTERNAL SOURCE (not the order. i cannot stress this enough: the jedi kicking obi-wan out is so jarring to me i'll leave the fic in an instant) or somehow unable to return to the order for whatever reason, all is well.
not a prodigy, but a genius. obi-wan is an incredibly intelligent person with an absolutely staggering knowledge base in a wide variety of topics, but all that knowledge was earned through blood, sweat, tears, and time. he sat down with his game face on and put in the work. that's also why he makes an excellent teacher: he knows what most students will struggle with because he struggled too, and knows through experience how best to overcome them. i headcanon that it contributes to why he's such a good negotiator: he's really good at stripping down information to the essentials and communicating that information effectively and efficiently to others because of his intense study habits.
humble, but not ignorant of his skills. it's pretty impossible to fully divorce yourself from pride in your achievements, and i don't think it's healthy to not feel any pride at all, so i think obi-wan has a very clear understanding of his skillset and how best to use it. i don't think he'd be ignorant of how good he is at something, especially since the direct consequence of his aptitude led him to being a member of the jedi council. pretty hard to be blind to your strengths when you're being asked for your input on topics that directly draw from that knowledge.
averse to healthcare. listen i enjoy obi-wan whump just as much as the next obi-wan stan (the desire to put him in the cosmic salad spinner comes with the territory, i fear) but as a character who grew up in an environment that deeply cares for the well-being of all, and knowing that you cannot help others unless you yourself first have the ability to do so, i can't really see him ignoring injuries outside of combat scenarios. like on the battlefield he's got more pressing concerns than a pesky little shrapnel wound or five, but once the battle's over?? he might not be first in line to the medics but i can't see him avoiding them entirely. an army without a general is working at a sharp disadvantage and i don't think he'd risk his men by neglecting his physical health in that manner. note that i said 'physical'. make of that what you will :)
duty. obi-wan is the definition of a paladin. he takes an oath and by the force he's going to keep it. train the boy? absolutely, qui-gon. whether or not anakin chooses to respect that training is another matter, but he did definitively get knighted! refuse to kill anakin? listen he's handed vader his own ass to him twice post order 66 and each time he did it he did it nonlethally. that takes skill. that takes dedication. exile yourself to tatooine for 19 years and then decide fuck it, we ball, and die after Once Again Deciding Not To Kill Anakin Skywalker? step aside casper, there's a new friendly ghost in town. every time obi-wan commits to something the man COMMITS. you GOTTA respect that grind.
flirty but in the sense that he's going to match the energy someone brings to the table. like he's a negotiator. he knows how to read people and figure out the Vibes. if he thinks the other person will be 1) 100% receptive and 2) will respond with a delightful wit, why the hell not? obi-wan's highest stat is charisma and he's got expertise in persuasion. whether they're allies or not does not factor into this equation. he can have a little flirtation with morally dubious and potentially hostile characters. as a treat.
this has nothing to do with his character but i firmly believe that he and quinlan vos had at LEAST a fling when they were padawans. there is zero evidence to back this up aside from a few comics where they were being goofy teenagers together but i stand by this. it is an unshakeable aspect of obi-wan to me that has only gotten worse with the kenobi show.
no matter what, no matter how terrible or devastating or downright apocalyptic it gets, obi-wan kenobi will never fall to the dark side. never. it won't be easy, but that is a line he has never, and will never cross. i will not hear any "obi-wan touched the dark side during the theed generator fight" slander. if that was true tell me why the force theme was playing during his moment of triumph!!! Would John Williams Lie To Us Like That?? to our face?????
anyways i could go on forever about obi-wan because he is My Ultimate Blorbo but this post is getting super long so i'll leave it there. hope this helped even a little or at the very least was entertaining for you to read <3
681 notes
·
View notes
Text
I’ve been struggling lately with the feeling that my job is pointless. Intellectually I know it is not—nursing is one of those professions where you get to be real smug about knowing the value of your work. But it’s still felt very pointless. Like I’ll start a shift thinking, “what am I even doing here,” and end it thinking, “what have I actually even done.” It’s been a ROUGH couple months.
But I had a really good shift last time I worked, which was good for the soul and also a very useful data point. I got to do pain management advocacy and symptom management, met a bunch of cool patients, did education for new nurses, and had several long heart to hearts, which the kind of midnight heart to hearts that I think are the most important part of night shift, all of that while being well staffed with very pleasant and appreciative patients and coworkers, and I was still like. Pretty depressed. I had a sense of satisfaction and moments of joy and meaning, but it turns out that one good shift did not cure the depression that has been latched on to me for the last few months like some kind of fucked up mental health leech. As I realized I was still depressed and that it was still interfering with my life even when everything was going well, the sense of peace washed over me was the best I’d felt in a while. Because I was like, okay! None of my usual stuff as worked! I have no excuse not to try something new to get my brain out of the shit ditch it’s slipped into.
So I’m applying for short-term disability. I’m worried I won’t get it, and I’m not sure what the next step is if I get rejected, but I feel so much better having decided to pursue it. It’s so much fuckin paperwork for sure, to a degree that’s overwhelming except that that the form could be a checkbox that says, “you want money?” and I’d be like “THIS IS TOO MUCH.” I’m totally not writing this post instead of finishing an email to my manager. I’m definitely not writing this post to avoid dealing with coordinating all my various care providers. I’m certainly not at every moment worried that I’m secretly faking all this so I can get three to nine weeks of a cool summer vacation.
I was thinking about how I almost flunked nursing school in my final semester because I turned in assignments late for a class with a “no late homework” policy. The professor said that this was reflective of real life, where if you miss deadlines you’re just fucked. I ended up appealing my grade and passing, because frankly it was a weak reason for making me repeat a final semester when there was no issues with my actual work or knowledge. During my appeal, I was like “I also think this policy is ableist. Harsh penalties for late work hurt students with health problems, especially chronic health problems when you aren’t asking for one week off due to the flu but instead for a general and never ending flexibility. I’m not trying to make an excuse but explain why this policy is a bad one. Disabled healthcare workers are an asset to healthcare.” I’m trying to remember my own argument as I pursue help. My depression and ADHD and eating disorder do help me be a better nurse, not because like depression gives you superpowers, but because I manage my chronic illnesses every day, in ways that range from hardly noticeable to life or death. Being kind to patients means being kind to myself, and vice versa.
I’m rambling. I really do not want to do this paperwork or send these emails. And I’m not sure if I deserve the leave I’m trying to take. But I miss being love with my job. I miss enjoying it. I wouldn’t judge someone else for going on medical leave, and my job doesn’t want me to burn out or quit. It almost feels like I have to be skeptical of applying for leave because no one else is. Everyone I’ve spoken to has been very supportive, including my manager. And considering how many unpaid days off I’ve had to take lately, disability leave would be an improvement over some of my recent paychecks. All in all, short-term disability makes sense and seems like a reasonable response to circumstances. But FUCK. I wish it required like 90 percent less documentation.
317 notes
·
View notes
Text
The Best News of Last Week
1. ‘It was an accident’: the scientists who have turned humid air into renewable power
Greetings, readers! Welcome to our weekly dose of positivity and good vibes. In this edition, I've gathered a collection of uplifting stories that will surely bring a smile to your face. From scientific breakthroughs to environmental initiatives and heartwarming achievements, I've got it all covered.

In May, a team at the University of Massachusetts Amherst published a paper declaring they had successfully generated a small but continuous electric current from humidity in the air. They’ve come a long way since then. The result is a thin grey disc measuring 4cm across.
One of these devices can generate a relatively modest 1.5 volts and 10 milliamps. However, 20,000 of them stacked, could generate 10 kilowatt hours of energy a day – roughly the consumption of an average UK household. Even more impressive: they plan to have a prototype ready for demonstration in 2024.
2. Empty Office Buildings Are Being Turned Into Vertical Farms

Empty office buildings are being repurposed into vertical farms, such as Area 2 Farms in Arlington, Virginia. With the decline in office usage due to the Covid-19 pandemic, municipalities are seeking ways to fill vacant spaces.
Vertical farming systems like Silo and AgriPlay's modular growth systems offer efficient and adaptable solutions for converting office buildings into agricultural spaces. These initiatives not only address food insecurity but also provide economic opportunities, green jobs, and fresh produce to local communities, transforming urban centers in the process.
3. Biden-Harris Administration to Provide 804,000 Borrowers with $39 Billion in Automatic Loan Forgiveness as a Result of Fixes to Income Driven Repayment Plans

The Department of Education in the United States has announced that over 804,000 borrowers will have $39 billion in Federal student loans automatically discharged. This is part of the Biden-Harris Administration's efforts to fix historical failures in the administration of the student loan program and ensure accurate counting of monthly payments towards loan forgiveness.
The Department aims to correct the system and provide borrowers with the forgiveness they deserve, leveling the playing field in higher education. This announcement adds to the Administration's efforts, which have already approved over $116.6 billion in student loan forgiveness for more than 3.4 million borrowers.
4. F.D.A. Approves First U.S. Over-the-Counter Birth Control Pill

The move could significantly expand access to contraception. The pill is expected to be available in early 2024.
The Food and Drug Administration on Thursday approved a birth control pill to be sold without a prescription for the first time in the United States, a milestone that could significantly expand access to contraception. The medication, called Opill, will become the most effective birth control method available over the counter
5. AIDS can be ended by 2030 with investments in prevention and treatment, UN says

It is possible to end AIDS by 2030 if countries demonstrate the political will to invest in prevention and treatment and adopt non-discriminatory laws, the United Nations said on Thursday.
In 2022, an estimated 39 million people around the world were living with HIV, according to UNAIDS, the United Nations AIDS program. HIV can progress to AIDS if left untreated.
6. Conjoined twins released from Texas Children’s Hospital after successfully separated in complex surgery

Conjoined twins are finally going home after the pair was safely separated during a complex surgery at Texas Children’s Hospital in June.
Ella Grace and Eliza Faith Fuller were in the neonatal intensive care unit (NICU) for over four months after their birth on March 1. A large team of healthcare workers took six hours to complete the surgery on June 14. Seven surgeons, four anesthesiologists, four surgical nurses and two surgical technicians assisted with the procedure.
7. From villains to valued: Canadians show overwhelming support for wolves

Despite their record in popular culture, according to a recent survey, seven in 10 Canadians say they have a “very positive” view of the iconic predators.
Here's a fascinating video about how wolves changed Yellowstone nat'l park:
youtube
----
That's it for this week :)
This newsletter will always be free. If you liked this post you can support me with a small kofi donation:
Support this newsletter ❤️
Also don’t forget to reblog.
1K notes
·
View notes
Text



The AMA is it’s own deep dive. It’s nothing more than a PAC.
For those not in the know, they do not provide clinical guidelines, certifications, or anything that actually improves healthcare. They support legislation. That’s it. It’s a self licking ice cream cone that AT BEST has about 15% of all physicians as a member. But even that’s a misnomer as residents and medical students can be members. They are in fact the bulk members, largely lulled into the fancy title and sponsored dinners. Retired physicians and foreign grads licensed in the US can also join. Seasoned critical thinking physicians are not members. Use that as another metric to gauge the worthiness of your provider.
119 notes
·
View notes
Text
Love in the big city and HIV
So, I have recently watched one of the best dramas of the year, “Love in the big city”, in which HIV is a major theme.
The show portrays really well the stigmatized scenario around HIV: as a person living with the virus, Go Young feels exactly as if he's carrying some kind of curse. He can't accept it, but who can blame him for that, if "Kylie", as he calls the virus, is always around like an inconvenient person? In his sex life, while applying to a job, and even while hanging out with friends.
Society doesn't make it easy for a person living with HIV to accept the condition and that's essential when it comes to healthcare, which is what I want to address today.
First, let me introduce myself: my name is Nico and I'm a Medicine student in Brazil. Here, we have probably one of the biggest public health system in the world, the Unified Health System (a.k.a. SUS). In this essay, I intend to share some general information about HIV, its treatment and prevention, by using some parts of “Love in the big city” to discuss this theme, because although the show did an amazing job when it comes to talking about it, there are some points I found needed some better explanation.
HIV is a sexually transmitted infection (STI) that can also be transmitted by the contact with infected blood (e.g: incompatible blood transfusion; use of shared needles) or from the mother to a child inside the womb or during labor. The virus uses a specific type of immune cell to multiply. Explaining it in a very simple way, he gets inside the cell, uses its components to produce new viral copies and then ruptures the cell membrane to release these new copies in the blood, killing the cell by doing so. For this reason, untreated HIV is very dangerous, since it can cause immunodeficiency (failure of the immune system), making the person susceptible to acquire opportunistic infections, which are diseases that usually don’t occur in people with regular immune systems. When someone has immunodeficiency caused by HIV, this person is diagnosed with Acquired ImmunoDeficiency Syndrome (AIDS). That being said, AIDS and HIV are not the same. There are many people living with HIV that don’t have AIDS, thanks to appropriate treatment.
There are multiple ways a person can discover about having HIV: you can be notified because the person you have had relations with discovered the infection, or by taking blood tests for blood donation, or in the worst case scenario, when you are already suffering from an opportunistic infection. Go Young, for example, discovered it because of the blood tests results while he was in the army. One thing I found very outrageous was that the physician instantly inferred that Go Young was gay because of that, but this is impossible, since anyone can get the virus, regardless of their sexual orientation. This appointment was like a death sentence: the unempathetic doctor as a ruthless judge, blaming the patient and not offering a single word of comfort. (Quite the opposite: he even asked that very intimate question about sex positions. Seriously, I wanted to punch this doctor so hard.)


Nonetheless, even if it was made in a very inappropriate way, diagnosis is still very important, because that is the only way one can have access to treatment. Each patient must be evaluated separately, since treatment may vary due to the different genetic subtypes of the virus and the person’s own body response. Medication can also be adjusted until satisfactory results are accomplished. Overall, all patients are submitted to a lifetime antiretroviral therapy in order to stop the virus from multiplying and to keep immune cells at a higher level. In the series, we can see Go Young asking for any antiretroviral in a pharmacy, but in real life, he would be very specific about the drugs.

If done properly, treatment can provide quality of life and long life expectancy (very similar to people who don’t have HIV), prevent opportunistic infections and, most importantly, transmission! Yes, that is exactly what you read: treatment can result in really low levels of HIV in the blood, which is called “undetectable viral load” if it happens for at least six months. There is even a saying which goes “Undetectable = untransmittable”. In this scenario the patient can even have sex without a condom with their partner, which is what happened with Go Young and Gyu Ho in the series. However, it is important to mention that this only applies to HIV: one can still get other STIs while having unprotected sex.


In addition to condoms and proper treatment, there are other ways of preventing HIV infection. Susceptible people can use the pre-exposure prophylaxis (PREp) medication, which highly reduces the risk of getting HIV from intercourse (and also from blood contact in a less effective way). There is also the post-exposure prophylaxis (PEP), which can prevent infection if taken within 72 hours after possible exposure. Treating other STIs, not sharing needles, using lubricant (less chance of injury during intercourse) and avoiding sex while in use of alcohol or drugs are some other habits we can do ourselves to minimize the risk of acquiring HIV.
Nevertheless, individual actions can help only until a certain point, given that the best prevention is the “combination prevention”, which includes not only behavioral and biomedical approaches, but also structural interventions. Every country should have their own public policies to assist people living with HIV and to prevent transmission. I’m proud to say that, in Brazil, thanks to our public health system, everyone has access to condoms, lubricants, tests, treatment, PREp and PEP - all free of charge. The system also has policies of damage control, providing all of these strategies to the population of risk, such as sex workers and people with a substance use disorder, including kits with individual needles to prevent sharing and, consequently, blood transmission. No wonder we are an international reference for HIV/AIDS treatment and prevention.
To conclude, I also need to remind you that you can actively help in this cause by simply showing support. As we all watched in “Love in the big city”, a person living with HIV faces all kinds of prejudice in society. Go Young carried a heavy burden for years, not being able to share it with anyone until Gyu Ho embraced him. Sometimes, patients have these prejudices themselves and it can deeply hinder treatment. I have seen this myself: a patient that denied the diagnosis and returned to the hospital sometime later with a severe health condition.
You can be the person that will accept and embrace this other person, who is only living with a chronic condition, such as many people who live with hypertension or diabetes, for example. You can be the person that will call out on others for their preconceived opinions. You can be the person who will share high-quality information to your friends, family, fellow workers or students (There are links in the last paragraph with reliable information for those who want to do some further research).
Finally, I can’t stress enough how much I loved “Love in the big city” for addressing so many types of love and so many sensitive topics, including this one, in such a beautiful way. It has been a long time since I had felt so connected to a story, to a character so human like Go Young.
I hope this essay provided a little bit of information to you. I mostly used the knowledge I have learned in college and sites of well-recognized organizations, such as the UNAIDS, the World Health Organization (WHO) and, for the Portuguese speakers, the Brazilian Ministry of Health (Ministério da Saúde). Thank you for reading, and please, feel free to send me any questions you might have, I’ll do my best to answer them. Also, if you notice any English mistakes, please let me know so I can correct them.
#love in the big city#HIV#aids#health and wellness#healthcare#medicine#SUS#Unified health system#Sistema único de saúde#Viva o SUS#Proteja o SUS#go young#gyu ho
80 notes
·
View notes
Text
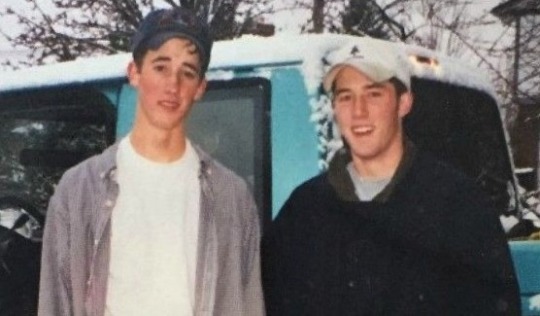
What is Pain? : How Austin Eubanks Dealt with Addiction and the Aftermath of Columbine.
Austin and Corey
Stephen Austin Eubanks was a junior and a star student in Columbine High School. Corey Tyler DePooter, his best friend, was also a particularly gifted student who prioritized his studies over anything else. Despite having a wide range of interests, the two kids particularly bonded over their shared passion for fishing.
At the age of 17, Corey had gotten a job doing maintenance at a golf club in order to earn money for a fishing boat that he planned to buy with a friend — likely Austin. The two often used to go fishing together and would talk about the struggles they had as teenagers.
Day of the Tragedy
On April 20th of 1999, the two were inside the library getting ready to get lunch with their friends, Jennifer Doyle and Peter Ball. That was until they had heard shots fired from the outside, not recognizing the sounds and believing that it was only the sounds of construction. Then they heard a bomb go off, a teacher rushing in to scream for the students to hide underneath the table because two students were armed with guns.
In a state of shock and fear, the four duck under the same table near the windows. With 10 minutes passing, the shooters had already entered the library and methodically fired under each table as recalled by him. His best friend, Corey, was one of those who were shot after being aimed with a semi-automatic rifle and shot at the neck, chest, and left arm by Dylan Klebold.
The bullet that hit Austin's hand first passed through his best friend, killing him instantly. With his best friend lying lifelessly beside him and being wounded on his hand and knee, Austin had no other choice than to try to play dead while laying in a pool of blood. When the shooting had stopped, Austin ran through the smoke and out of the backdoor of the library. He was only 17 when the shooting occured.
In Austin's TedTalk “What Columbine Shooting taught me about pain and addiction”, he recalls:
"I remember how I felt: I was confused, I was afraid, I felt sick and I was vulnerable. And just minutes later, I was playing dead underneath a table next to a pool of blood. I had just been shot and I witnessed my best friend murdered right in front of me as we were huddled together waiting for help to come."
Pain, Grief, and Narcotics
During the time he fled from the crime scene, Austin marked that as one of the most impacting and damaging experiences he has ever experienced in regards to the feeling of pain. His definition of pain was nothing similar to what he describes in his present days.
Pain, in a medical sense, is the variably unpleasant sensation of physiological systems mediated by specific nerve fibers of the brain that are conscious of receiving signals of awareness. According to Austin's TedTalk, the American Pain Society introduced the term "pain is the fifth vital sign" in 1996. This means that when you enter the room, your status is assessed using five different data points: blood pressure, pulse rate, temperature, respiration rate, and pain.
Due to a movement that was certain that we were undertreating pain, patient satisfaction surveys were implemented in order to monitor the campaign's success. To him, in order to uphold this new momentum and cause the patient's pain levels to cease completely, the ethical dilemma instantly arose:
“Do I issue this person with narcotics to make them happy or deny them and potentially hurt my compensation, the revenue of the hospital? Or at worse, open myself up for a grievance for undertreating pain that could potentially result in the loss of my job?”
Austin says that the healthcare system predominantly treats physiological systems and would rather not assess emotional pain into the equation. He akins the emotional pain of dealing with trauma being identical or if not more than when dealing with physical pain. With that, within months after the incident, Austin was prescribed opiate medication for his injuries.
In an exclusive interview with The Fix, he said that his injuries were not to the point of needing an opiate pain medication but was immediately given a 30-day supply and became addicted within three months. From then on, he said, “I used substances every day, day in and day out.”
After the shooting, his parents took him to a therapist who said Austin was too shut down to process his horrific trauma. But the reason no one could reach him was because he was overmedicated. He was addicted to painkillers, and used medication because of his unwillingness to engage in the stages of grief that he dreaded to face. He was haunted by the past. Struggling with survivor's guilt and the death of his best friend, he would rather ignore the intense burdening feelings he bore. According to him,
“Acute Physical Pain ends relatively quickly, complex emotional pain does not.”
The morphine Eubanks received at the hospital that day proved to be the opening dose of a costly addiction to prescription painkillers - one that revolved around commonly prescribed drug Oxycontin, he said.
“I learned to manipulate doctors … I could literally get whatever I wanted. Telling them I’d been shot at Columbine and lost my best friend was like [getting] an open prescription book from any doctor.”
He could not process the grief, moreso, he didn't want to. He didn't want to be haunted by the memories that scarred him. In his own words, he would describe the physical ailments he felt to be a 4 or 5, but the emotional turmoil was a 10.
Austin never set foot back to Columbine. His parents hired a tutor and he then went on to graduate in 2000. He attended the Columbine ceremonies but never went back inside the school. He then went into advertising and married in his early 20s. Around this time his substance abuse escalated, and his first attempt to get sober was in 2006. He went into a 30-day inpatient program but failed within hours of leaving, for relapsing using pain pills and Adderall.
Addiction and Sobriety
He failed both outpatient and rehab twice and it wasn't until 10 years later, in 2009 that he was able to overcome this addiction. Right before Columbine, young Austin had been misdiagnosed with ADD.
“I didn’t have ADD,” said Eubanks. “I just liked being outdoors and playing golf better than being in school. At that time, if anybody was truant at school they said, ‘Oh, they must be ADD. Let’s put them on a stimulant.’ That was why I got Adderall. I liked it because I could abuse opiate pain medication to the level that most people would be nodding out. With Adderall, I could function. Basically, I was doing oral speedballs. It was like using methamphetamine and heroin.”
His second try at being sober was in 2008. Gaining the motivation to change after recently separating from his wife, he went to treatment, stayed 90 days, and achieved eight months of sobriety. Then, he akinned addiction to a causal sequence, a domino effect. According to him, he achieved abstinence for a period of time, built up enough false confidence to where he thought he could drink, because alcohol was never a problem. From alcohol, he went to weed, then Xanax, then Oxycontin, and then back into the same routine.
In 2011, approaching the age of 30 and estranged from his wife and kids, he hit rock bottom: "My sobriety date is April 2, 2011. I woke up in a jail cell and had no clue how I got there." His downward spiral began with Oxycontin and alcohol abuse, leading to arrests for various offenses like car theft and fraud. Realizing that he needed a drastic change, he recounted that his lowest moment was waking up in withdrawal, hungover, and facing the ruins of his marriage and being estranged from his children. He knew he had to stop or he would die. After unsuccessful attempts at sobriety, he finally sought help, surrendered to treatment, and was now willing to follow any guidance to rebuild his life.
His journey to lasting sobriety didn't hinge on traditional 12-step programs, but rather on understanding behavioral triggers and brain function through a therapeutic community approach. He was five years sober and started working at The Foundry in Colorado, becoming the COO and handling approaches that combined neuroscience with 12-step principles, recognizing that each person's path to recovery is unique. Using comprehensive approaches aiming to rebuild the lives of those in recovery.
During this time, he would also indulge in old activities in remembrance of his bestfriend.
“It’s something I do to connect with Corey. It's always nice whenever I catch a fish that's above the normal or something special about it. I always tend to look up and give a nod to him. And I know he’s still looking out for me."
Sadly, despite his long battle against drug addiction, in 2019, Austin had passed away in his home in Colorado after an accidental heroin overdose. Just a month after the 20th anniversary of Columbine, Austin was 37 at the time.
What is Pain?
Pain, to Austin, encompassed many things: the confusion and vulnerability of not knowing what to do in such a time of terror, the physical wounds that the doctors tried to medicate to bring the pain meter to zero, and most importantly, the emotional hurt of knowing your best friend was gone, taken right in front of you. Knowing that very moment can never be undone.
His advice for survivors dealing with the same guilt is to feel it. Don't run away from it. Survivors often find other things that allow them to detach from the pain, but to him, that's the wrong choice.
“You can heal physical pain while you’re medicating it. You cannot heal emotional pain while you are medicating it, In order to heal emotional pain, you have to feel it ... You want to feel better immediately, [but] you have to have the courage to sit in and feel it, and if you can do that long enough, you will come out on the other side.”
Along with post-traumatic stress, there is also the potential for post-traumatic growth.
“That doesn’t imply you will ever be the same person again. After a trauma, you will be changed forever.”
136 notes
·
View notes
Text
✧ pre-med extracurriculars: for my future doctor angels ✧





hi my lovely pre-med angels!! 🤍 it's mindy hereee!
today's post is extra special because so many of you have been asking about extracurriculars for medical school!! if you know, my ultimate dream is to become a doctor, i'd love to either be a psychiatrist or a cardiologist, so anything medical-related is my favorite cup of coffee!! i'm literally so excited to share this comprehensive guide that will help you shine on your future applications. this post is for you if you're in high school or college, this guide will be your bestie through the journey!!
~ ♡ for my precious high school sweethearts ♡ ~
hospital + healthcare volunteering (my absolute fave!!) • aim for 100-150 hours minimum • try different departments to explore • build relationships with nurses + staff • pro tip: volunteer during summer break for more hours • keep a reflection journal of your experiences • bonus: ask for recommendation letters if you connect well!!
research opportunities • reach out to local universities • email professors about summer programs • join science fairs with medical projects • create your own research project • tip: start with literature reviews if labs aren't available • document everything for future applications!!
leadership + school involvement • start a medical interest club • lead health awareness campaigns • organize blood drives • create mental health support groups • join science olympiad • participate in biology competitions • personal story: i started a "future doctors club" + it literally changed my life!!
~ ♡ for my darling college angels ♡ ~
clinical experience (super important!!) • medical scribing (literally the best!!) • certified nursing assistant (CNA) • emergency medical technician (EMT) • phlebotomy certification + gain a bunch of different certifications online • medical assistant • tip: aim for 200+ hours minimum • pro secret: try different specialties!!
research involvement • join multiple labs if possible • aim for publication opportunities • present at conferences • write abstracts + papers • network with graduate students • maintain good relationships with PIs • secret tip: join journal clubs!!
leadership positions • pre-med society officer • tutoring coordinator • mentorship program leader • research team leader • volunteer coordinator • tip: create new positions if none exist!!
~ ♡ extra special activities for everyone ♡ ~
medical mission trips (life-changing!!)
start a health education blog
create medical awareness social media
join medical podcasting
organize health fairs
volunteer at free/non-profit clinics
shadow different specialists
join pre-med summer programs
work as a pharmacy technician
volunteer at nursing homes
organize medical supply drives
create health education programs
~ ♡ my personal tips + secrets ♡ ~
quality over quantity always!!
maintain each activity for at least 6 months
document everything (literally everything!!)
take lots of pictures (for memories + portfolio)
get contact info from supervisors
keep detailed reflection journals
network with other pre-meds
create spreadsheets to track hours
always ask for recommendation letters
maintain professional relationships
~ ♡ time management secrets ♡ ~
use google calendar religiously
block schedule your activities
don't overcommit (seriously!!)
maintain 2-3 main activities
rotate seasonal activities
leave time for self-care
schedule study breaks
plan one year ahead
keep backup activities ready
remember my loves: medical schools want to see dedication + passion!! don't just collect activities like pokemon cards (even tho that would be cute). focus on meaningful experiences that truly speak to your heart!!
pro tip: start a bullet journal to track your journey!! include your thoughts, feelings, and learning experiences. future you will literally cry happy tears when writing your personal statement!!
also!! please please please remember that your mental health comes first!! it's okay to take breaks, it's okay to say no, and it's absolutely okay to prioritize self-care. you'll be a better doctor if you learn these habits now!!
sending you the biggest virtual hugs + all my love!! you're doing amazing sweetie, and your future patients will be so lucky to have you!!
feel free to send more asks if you need specific advice!! i'm always here to support my precious future doctors and followers i call my sweetheart community!!
xoxo, mindy 🤍
p.s. remember to hydrate, get enough sleep, and take your vitamins!! doctor's orders!! <3
p.p.s. i'll be sharing more detailed guides about each activity soon, so stay tuned my loves!!
btw, if you need personal study advice or anything, submit to glowettee hotline 💌: https://bit.ly/glowetteehotline

#premed#premedlife#medschool#futuredoctor#studyblr#studygram#medicalschool#studentlife#extracurriculars#medicalstudent#medschoolprep#premedmotivation#premedadvice#premedblog#medschooljourney#premedcommunity#futurephysician#medicaljourney#medschoolbound#studytips#medschoolguide#premedguide#medstudent#premedstudent#medschoollife#medicaladvice#collegelife#highschoollife#academicblogs#studyinspo
50 notes
·
View notes
Text
youtube
🏆 Proud Moment: Health Gennie Awarded Best Health App for Students
🎉 We are thrilled to announce that Health Gennie has been recognized as the Best Health App for students in India at the prestigious Global Skill Summit!🏆 This remarkable achievement is a testament to our dedication to improving student health and well-being. The award was proudly presented by the esteemed Member of Parliament, Shri Sanjay Deshmukh ji.
This accolade belongs to every team member who worked tirelessly to make Health Gennie a trusted companion for students across India. Let's continue to strive for excellence and make a positive impact on the health of our youth.🌟
#Best Health App for students in India#Student Health App#Students Healthcare App#Best Student Healthcare App#Teenage Healthcare Company#Students Healthcare Company#Students Healthcare Centre#Student Health Services#Online Student Health Services#Best Medical Healthcare for Students#Student Online Health Clinic#Youtube
0 notes
Text
just wanted to make my stance on here crystal clear . i am pro-choice, anti-deportation, i am pro-palestine, i support queer youth, the black lives matter movement and believe that children in schools lives are more valuable than the banning of an app that fosters lots of community and social interaction. i know my rights as a citizen of this country and i’m gonna exercise the fuck out of them.
if you think a convicted felon, and an accused sex offender has any right to be in office, especially after some of the events of yesterday’s inauguration speech, please feel free to block me! i don’t care that much <3. people i love are no longer safe and the only thing we can do is stay strong and fight the good fight.
birthright citizenship is being threatened, leaving people i care about vulnerable. basic healthcare is being denied, including life saving reproductive surgeries and medical transitions for queer/trans people. the 14th amendment of the constitution is under attack.
if you want to ask me questions i will more than happy answer them with sources to back up my claims! feel free to ask for resources for any knowledge you need and i will do the research for you (to the best of my abilities considering i am still a student).
KNOWLEDGE IS POWER AND YOU HAVE A SUPER COMPUTER IN YOUR HANDS RIGHT NOW!! GO LEARN SOMETHING!!
dont doomscroll too much these next few years and make sure to take care of yourself so we are ready to bounce back when we need it the most.
#i love you#you are loved#youre loved#you’re loved#inauguration#inauguration speech#2024 presidential election#democrats#democracy#republicans#the 14th amendment#undocumented immigrants#stay strong#politics#political#political posting#reproductive rights#reproductive health#reproductive freedom#trans healthcare#trans rights#transgender youth#trans youth#protect trans kids#black lives matter#black lives fucking matter#stop asian hate#stop asian violence#birthright citizenship#14th amendment
22 notes
·
View notes
Text
they could never make me hate you Shoko Ieiri


Shoko is such a tragic character (and to me, the most relatable character in jjk (lolol the numbly depressed med student is jumping out))
she gets a lot of shit for her apathy but to be honest, there’s not much else she can do to protect herself
Shoko has been patching people up and doing autopsies since she was in school. Out of the entire cast of characters, she is probably the one who has the clearest view of how many of her fellow sorcerers die and/or are seriously injured in battle… it is a decently well documented phenomenon that working in healthcare lowers your active empathy levels, as a defense mechanism to distance yourself from all of the pain and loss you are confronted with on a daily basis… it is another fact that in most if not all countries, there are strict laws in place to prevent doctors and other medical professionals from treating their close friends and relatives
Shoko never had that protection… Jujutsu society is small and everyone knows everyone, she is in a position where she is constantly having to stay calm and level headed while her friends and comrades and injured and dying …
in addition to that Shoko, as their best healer, has always been taught to take a passive role in the action (she wasn’t sent out on dangerous missions, she had to stay back during Shibuya etc)
getting emotional over any of this wasn’t going to help her, or anyone else for that matter
Shoko grew up between Gojo and Geto, two once in a generation (once in a century in Gojo’s case) powerhouses who were both highly emotional in their own ways (cue the clip of her leaving the gym when the two were bickering in the hidden inventory arc)
She isn’t like them, and she CANT be like them, cause it would be detrimental to her role in the team
she does not GET to be emotional, so she trained herself out of it till it became second nature
when Geto defected, she did not rage at him or fight him cause there wouldn’t have been a point… she is not a fighter, she knows him well enough to know she is not in direct danger as long as she doesn’t attack first and arguing with him would not have done either of them any good… so she has a last casual conversation with him and calls Satoru, who is the only person who could actually do anything about the situation (either in an argument or in a physical fight)
when he left, all she could do was stay there with Gojo (and she is silently hurt that he never leans on her but she also can’t make him open up against his will)
it’s lonely at the top, but it’s lonely in the morgue too
then, years later, Geto initiated the Night parade of a hundred Demons, forcing Gojo to execute him… we don’t know if Shoko ever saw his body after his death (if Gojo took it to her and didn’t let her cremate him or if he didn’t take Geto’s body to her at all), either way, it can’t have been easy
less than a year later, Gojo is sealed and we see Shoko’s thoughts, about how Gojo felt alone despite the fact that she was there too and that (in my interpretation) they are all monsters on some level (Gojo doesn’t have to be the only monster) waiting for him to come back to them
and when he does come back, (according to Shoko’s own prediction) possibly questionable mental state) he immediately throws himself back into a fight with their two strongest enemies
and for the first time… everyone has to consider the possibility of Satoru Gojo losing… and the students even say, it’s hard to react appropriately cause the possibility of him losing is such a foreign concept
and now to their back up plan for when he does…(the thing my girl gets the most shit for)
Shoko not protesting is rooted in multiple things:
1) They are up against Sukuna and this is the only plan they have in the event of Gojo’s death… if they don’t use every trump card in their deck they WILL die (hence why Yuuta is upset… he is not upset by Gojo’s body being weaponised, he is upset by others hesitating to sacrifice their own humanity)
2) yes she could protest but it wouldn’t help anyone, the last thing you need in a crisis is your doctor getting emotional, if both of the people involved are alright with the procedure, Shoko’s feelings don’t matter and she knows it too, the last thing they need is for her not to be able to do her job
#shoko ieiri#my girl my girl my girl#should have used a read more huh#jjk meta#shoko defense squad#jjk spoilers#jujutsu kaisen#shoko & gojo#platonic sashisu angst#character analysis#character deep dive
62 notes
·
View notes
Note
Hello!
This isn’t exactly a question about your game, so hopefully it’s okay to ask you here - feel free to delete this if you’d like! I saw in your bio that you work in vascular surgery at only 23 - first of all, that’s incredible! I didn’t even realize it was possible to enter the medical/surgical field in any way that young. My question kind of relates to this: as someone who wants to get into medicine and healthcare, I’m wondering how you’ve started so young and/or if you have any advice on how to succeed in school/get a job in the industry early on? Thank you so much for your time and have a lovely day :)
You’re good, it’s totally okay! I enjoy my work and talking about it. I’ll put my answer under a cut so people who are just here for game stuff can easily skip it
There are a lot of options in the medical field!! Advice really depends on what you want to do. I’ve only experienced one side of it, so I’m not sure if anything I say would be relevant to what you’re wanting to do. I hope this is at least a little helpful though, and I’m wishing you the best of luck with it!! 🍀🍀✨✨
I’m a vascular interventional radiologic technologist. Every hospital is different, and people with that job title often work in a cardiac cath lab or interventional radiology. I’ve talked about the types of operations I help perform here!
Here it requires 4 years of university with a lot of clinical hours and 2 registry exams at the end to get certified / have proper credentials.
As a student I spent a lot of my clinical hours in the vascular surgery department. I was always told to treat your clinical shifts like an interview! I knew I wanted to work here, so I talked to the manager over the department and actually got hired a few months before I graduated (with the condition of me successfully graduating + passing my exams to get credentials). Most medical programs should have some type of clinical hour requirements, so my biggest advice is to try to spend that time in the department you’re passionate about + try to show that you’re someone worth hiring while you’re a student! A couple of my classmates got hired for cath lab & IR before graduating too.
There are also so many different types of jobs in the medical field!! A lot of people outside of the field have never heard of my position, or they’re only aware of it in interventional radiology. My other suggestion is to make sure you know what you want to do & look at all options! There are many cool positions that would allow you to start working earlier in life :)
I hope this was helpful in some way, and again I’m wishing you the best!!
45 notes
·
View notes
Text
In the last few weeks, I've received many asks from Palestinians asking for support in their GoFundMe campaigns. I don't have much to spare, but I've managed to donate make a total donation of 15 dollars to them. Can you match my donation?
Here's a list of the people who have contacted me and some words from their campaigns' pages. Please take the time to read their stories and, if you can, please share and donate, even if it's a dollar!
Heba Al-Anqar (@heba-baker) - €4,503 - €60,000
Hello, I am Heba Al-Anqar, 21 years old, a university student. My university was suspended due to the war. I am writing about my family: my father Bakr (54 years old), my mother Alaa (46 years old), and my sisters Aya (18 years old), Amal (15 years old), Muhammad (13 years old), and Maryam (8 years old). We have faced many challenges in this war, from the destruction of our home to the famine we continue to suffer in northern Gaza.
Ahmed Altaban (@ahmed4palestine) - $18 309 USD/ $20 000
There are seven members of the family: Heba (the mother), Amjad (the father), their sons Ahmed, Khaled, Soliman, and Abdallah, their young daughter Lamar, and Ahmed (the grandfather). The siblings were all pursuing engineering, design, or completing grade school. Lamar in particular aspires to be a doctor some day.
Eman Zaqout (@rakan2010) - $25 669 CAD- $40 000
My name is Eman Zaqout, from Occupied Gaza, Palestine. I am contacting you at a really desperate and urgent moment. I am seeking your assistance to raise funds for saving our lives, facing the starvation in Gaza and help me achieve my doctoral degree dream after awarding prestigious PhD Fellowship. I'm a wife and mother of two little kids. My husband Mahmoud Zaqout 39 years old, my son Rakan 12 years old and my doughter Seba 10 years old. I am also an employee working in a medical field and at the same time a scientific researcher conducting different research inside and outside Gaza as well.
Mohi (@mohiy-gaza2) - $30,000 USD- $31,000
I am 23 years old. I live under the bombardment and constant aggression against Gaza. Here we struggle with a life of constant death and loss. I lost a large part of my family. We also lost our house in which we used to live. We were displaced more than 10 times from one place to another, searching for safety. In fact, there is no safe place. We had many ambitions and hopes. I graduated from university and intended to travel, work, and many other things. But the war came and destroyed all that. We also had a source of livelihood and clothing shops. The occupation completely destroyed and burned them all, and we no longer have any source of livelihood. (...) Therefore, I hope you can help, even if just a little, as this will help us get out of death."
Islam Al-Najjar (@islamgazaaccount3) - €2,150/ €30,000
My name is Islam Al-Najjar, a 27-year-old Palestinian from Gaza. My life was turned upside down when our home was destroyed, and I lost many loved ones and friends. Now, I find myself homeless, jobless, and struggling to survive. We lack basic needs such as food, water, and healthcare. Despite these hardships, we still hold onto hope, believing that your generous support can help us overcome these adversities. My grandfather is 85 years old. He lost his left hand due to a previous Israeli bombing and suffers greatly from this serious injury. We also suffer a lot in taking care of him due to the scarcity of basic resources like water and food, and their complete absence.
Ahmed (@ahmadresh) - $13,241 USD/ $31,000
Hello, my name is Ahmed, 19 years old from Gaza. I finished high school with a high average and a very good grade, and because of the genocide war on Gaza, I was deprived of enrolling in university. I had dreams and ambitions to study photographic design, but I was deprived of all of that because of the genocide war on Gaza. I was living the best days of my youth. But with the beginning of this war, I became unable to live my normal life. At least our warm house sheltered me and my family until it was bombed for the first time, that damned night. Our house has become like a ghost town. We continued to seek refuge from death there until we were besieged and displaced from our safety under fire to a tent (shelter) in the bitter cold of winter, with the lack of basic necessities of life (water pollution, high cost of living, disease, insect infestation, malnutrition, Difficulty of movement, overcrowding), and many other daily difficulties, especially with the significant increase in prices.
Haya (@hayanahed) - €86,967/ €100,000 target
I'm Haya from Gaza , from a family of 8 people: my parents, two sons, and four daughters (two of them suffer from allergies). I've witnessed the evidence of the tragedy that has struck our lives in Gaza, where my family and I have survived amidst numerous previous wars. But today, we face the most dangerous and fierce battle in the current war. The urgent need intensifies for us, as we have nothing left and are unable to secure our basic needs such as food, water, and safe shelter.
Sara (@sara-97a) - €1,297/ €50,000 target
Before the war, 7 -year-old Sewar dreamed of becoming a doctor to treat people and alleviate their pain. Sewar is a kind, active, intelligent and diligent girl in her studies. Every day, Sewar and her two brothers, Abdul Aziz and Omar, begin a bitter journey to get water and food, collect firewood for cooking and help their father and mother secure the necessities of life. The lives of the three children, Sewar, Abdul Aziz and Omar, have been turned upside down. They were kind and innocent children who went to school every morning with enthusiasm. Please help us arrange the costs of food, water and medicine for the children and their sick grandmother.
Nisreen Suhail/Hazem Shawish (@nisreensuhail - vetted by association) - €7,869/ €50,000
I’m Hazem Shawish, trying to save my family from the war. We’re a family of 8 members, me, my mother, and I have 4 brothers and two sisters. And their kids. Islam (30) years old, Hashem (31), Samer (29), Mohammad (35), Nisreen (37), Noor (36), Amal (12), Kenzy (17), Zoheer (19) In the shadow of conflict, our family has faced unimaginable hardships. The passing of my father, a victim to the cruel grasp of hunger and inadequate healthcare, left a void in our lives, underscoring the fragility of our existence here. My brother, Samer, battles bipolar disorder, a condition exacerbated by the ongoing war and the severe shortage of essential medications. Without access to the necessary treatment, his life is at risk, and we live in constant fear for his well-being amidst the chaos that surrounds us. These personal tragedies have deepened the urgency of our situation.
Dr. Husam Farhat (shamfarhat1) - $8,590USD/ $29,500
Amidst the relentless bombardment, Dr. Farhat faced an unthinkable tragedy: the martyrdom of his beloved sisters, Inas and Amal, along with their husbands and children, and his brother Mustafa. This devastating loss shattered not only their dreams but also their hopes for a peaceful future. (...) Now, after all this devastation, my family and I are living as displaced people, homeless and jobless, with no clear future for ourselves or our children. Every day is a struggle to find food for my children, who have been robbed of every chance at a normal life by this war. Once, we lived in Shuja'iyya, in North Gaza, where we had a home, a life, and dreams. But now, after being displaced over nine times, we find ourselves in the refugee camps of Nuseirat, the war has stripped us of everything—our home, our security, and our future.
Dr. Mohammed Aldeeb (@mohammedaldeeb) - €41,065/ €55,000 target
I am Dr. Mohammed Aldeeb, a dedicated medical professional specializing in emergency care, hailing from the Gaza Strip, We are a family of 4 members. (...) In the chaos and carnage of conflict, I sustained injuries, and the sanctuary of my home was obliterated, leaving my family and me destitute and displaced. Yet, amid the ruins, a flicker of hope persists. At Al-Aqsa Hospital, I continue to extend a helping hand to those in need, drawing strength from the resilience instilled in me through years of education and service. Today, we find ourselves sheltering in a humble tent, stripped of our possessions and livelihoods. The loss of my job, my home, and the comforting presence of my loved ones weighs heavily on my heart. Nevertheless, I refuse to surrender to despair, clinging to the belief that brighter days lie ahead.
If it serves as an incentive, anyone who sends me proove over at my inbox that they've matched my donation of $15 USD can request a drawing of their choice to me, on my quick commission style, as seen bellow



22 notes
·
View notes