#what is a clinical research associate
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The most popular pages on Tumblr are about Minecraft, GIFs, and David J. Peterson.
Text
elon musk did a nazi salute twice at the inauguration, and republicans are defending him.
trump revoked executive order 11246, which prohibited discrimination.
trump put all dei employees on leave to be fired.
trump blamed the dc plane crash on dei.
trump banned all lgbtq+ flags from being hung in government buildings.
trump ordered the pentagon to cancel celebration of mlk jr. day, black history month, women's history month, holocaust remembrance day, asian american pacific islander heritage month, lgbtq+ pride month, juneteenth, women's equality day, national hispanic heritage month, national disability employment awarenessmonth, and national american indian heritage month.
trump proposed removing all palestinians from gaza, turning the area into a vacation resort called “riviera of the middle east”.
trump posted an ai generated video showing what he hopes to turn palestine into, with a large golden statue of himself in the middle of it.
trump rolled back biden’s executive order to lower prescription drug costs for people using medicare and medicaid.
trump rescinded the $35 cap on insulin, and prices are expected to rise to $1500 a month.
trump ordered the national institutes of health to cancel their review panels on cancer research.
trump ended the guidelines to prevent ai misuse. the guidelines prevent many things, but notably it prevents production of ai child pornography.
when sean hannity asked trump about the economy, he said “i don’t care”, after campaigning with the economy as his main talking point.
trump has withdrawn the us from the world health organization.
trump is ordering health agencies to stop reporting on bird flu and halt publications of scientific reports.
trump has pardoned over 1500 people who stormed the capitol on january 6th.
trump changed denali back to mount mckinley.
trump signed an executive order to rename the gulf of mexico to gulf of america.
trump shut down cbp one, an app which granted legal entry to 1 million+ immigrants.
trump has discussed introducing a “gold card”, which would allow the wealthiest people to buy us citizenship for $5 million usd.
trump is allowing ice raids at churches and elementary schools.
trump announced plans to declare a national emergency at the us-mexico border.
trump signed an executive order to expand the use of the death penalty.
trump disbanded the school safety board that works to prevent school shootings. it was comprised of survivors, educators, and gun violence prevention advocates and formed after the school shooting in parkland.
trump has threatened to invade panama to claim the panama canal.
trump withdrew from the paris climate act.
trump revoked all protections for transgender troops in the us military.
trump rescinded executive orders made by biden that benefited and protected women, lgbtq+ people, black americans, hispanic americans, asian americans, native hawaiians, and pacific islanders.
trump is attempting to make it legal to refuse to hire or fire pregnant women.
multiple state legislators are drafting bills to allow the punishment for abortion to be the death penalty.
trump pardoned 23 individuals convicted under the freedom of access to clinic entrances (FACE) act for their anti-abortion activism, including oftentimes violent protests at abortion clinics.
trump signed an executive order allowing deportation of foreign students who they believe express support for hamas or hezbollah.
trump announced that the us government will from here on out only recognize male and female as sexes. intersex is not legally recognized anymore.
trump has told all schools and universities that they have two weeks to end all diversity initiatives, or he will cut federal funding. (as of feb 19, 2025)
trump fired the staff of the federal aviation association after a deadly plane crash in dc.
trump has fired the heads of the tsa and coast guard, and gutted a key aviation safety advisory committee.
the official white house twitter account posted an “illegal alien deportation” asmr video where they did closeups of chains and the sound of ankle chains hitting the metal stairs of the airplanes deportees were being loaded onto.
on truth social, trump posted, “LONG LIVE THE KING!”.
at CPAC, a republican group called the “third term project” held a rally to support changing the constitution so trump can run for a third term. on their posters, they’re photoshopping his face onto julius caesar’s, seemingly forgetting what happened to julius caesar.
the trump administration paused health communications to prevent the fda from announcing food recalls.
republicans on tiktok are recreating elon’s salute to prove that it “wasn’t a nazi salute”, and they’re either doing it completely wrong because they know if they replicate it then it will actually be a salute, or they’re doing the proper salute and posting it online.
google and apple maps now display the gulf of mexico as “gulf of america”.
rfk jr. wants to ban SSRIs and put everyone on them into labor camps.
andy ogles drafted a constitutional amendment to allow trump to be president for a third term.
the us senate confirmed russell vought, one of the main authors of project 2025, will lead the white house budget office.
nancy mace repeatedly used the t-slur during a congressional meeting, three times were out of spite.
andy biggs introduced a bill to abolish osha and completely eliminate federal workplace safety protections.
georgia republican congressman mike collins called for the deportation of new jersey born mariann budde, the bishop who urged trump to “have mercy” on the lgbtq+ community and immigrants during a service at the national cathedral.
florida republican anna paulina luna has introduced a bill to add trump to mount rushmore.
new york republican claudia tenney introduced a bill to make trump’s birthday a federal holiday.
west virginia republican delegate lisa white has introduced house bill 2712, which would remove rape and incest as exceptions for abortion, even for minors. you can call her at (304) 340- 3274 or email her at [email protected] and let her know your opinion on that.
there is a bill named the SAVE act which would require americans to provide their birth certificate, passport, or other citizenship documents every time they vote, and would require the last name on their driver’s license to match that of their birth certificate. this would prevent married women who have changed their last name from voting.
bill h.r.1161, which is available publicly on congress.gov, would authorize trump to enter into negotiations to acquire greenland and to rename it to "red, white, and blueland".
six states (arizona, idaho, iowa, kansas, mississippi, and north dakota) are planning on challenging obergefell v. hodges, which would end same-sex marriage nationwide. about a dozen more states have representatives are also considering filing similar resolutions.
a bill to ban the mRNA vaccine has passed out of the house committee.
amazon revoked protections for lgbtq+ and black employees.
the cdc has removed their hiv prevention page.
the united states state department has officially changed its “travelers with special conditions” page which previously said “lgbtqi+ travelers” to “lgb travelers”, completely getting rid of the tqi+.
every single republican told us we were overreacting. trump swore he had nothing to do with project 2025 yet continues implementing details outlined in it. not a single person has the right to tell us we’re being dramatic anymore.
hope “cheaper eggs and gas” was worth it.
EDIT: i removed the “trump refused to swear on the bible” point because it was being taken as me being an offended christian. i’m not christian, im agnostic. the reason i included it in the first place is because he’s the first president in history to ever refuse to swear on ANYTHING. meanwhile his “conservative christian” followers had no issue with this, and decided to continue to scramble for excuses instead of admitting he may not be as religious as he claims he is. i figured taking that point out entirely is probably better than filling this with an explanation in the middle of the other important issues.
#*#allie talks#politics#us politics#fuck trump#trump administration#donald trump#trump#inauguration#current events#elon musk#fuck elon musk
62K notes
·
View notes
Text
!season 1

Viktor is, you've clearly observed, insecure of himself.
Quite valiantly, due to some looming social norm or personal feeling, he tries to hide it. But in moments like these, such an act becomes impossible. Try as he might, desperately at times, when he's pressed against you in the warm water, your fingers over his skin, your fingers in his hair, his failure is palpable.
"Are you okay?" You murmur into the nape of his neck, his back against your chest. The water threatens with gentle churns to spill over the bathtub.
He turns his head to press a kiss against your wrist.
"More than," he says, voice quiet but firm, "I just feel, sometimes," and he hums, as though forming an adequate description of his emotions were the hardest task on the planet. Viktor, your genius scientist, hesitant not to innovate, to change the world with his research, no. He's hesitant only to make sure he says the right thing to you.
"Like I'm too good for you?" You ask, catching his eye. By the gentle look you know that's what he means. He faces away again, nods in a vaguely ashamed way.
How, you've always wondered, can you truly change someone's perspective? When words don't seem to persuade, when actions bring only fleeting relief, what can you do?
"It's irrational, I know, some... flaw of the mind. You don't need to keep reassuring my senselessness." He leans into your touch, takes your free hand into his, soap suds bubbling between your fingers.
"Sometimes you talk about yourself like you're a machine, you know." You muse. He gives a half-hearted laugh.
"Not a well functioning one."
Are words or actions worth more in this game of convincing? Does he feel it deeper when you press your lips into his hair, or when you mumble compliments and honeysuckle words into his ear? He shivers either way.
It's a long game, you know. It's taken months to even reach this stage, where the self-deprication is a rarity, not the norm. Maybe it'll take his whole life before he can accept every part of himself like you can, before he can truly see himself through your eyes, gleaming and gem-speckled as they are.
You free your hand from his, reach up instead to knead shampoo into his thick hair. He responds with a sigh and sinks somehow further against you, the water falling slowly to a more lukewarm temperature. You're not sure how long the two of you have been in here, talking quietly about very little, exchanging words that'll disappear forever with the water. But you really can't find it in you to care.
There's work to be done, errands to run. Errands that should've been run a week ago. This ceremony, this meditation makes all of it null. For where else would you want to be? Where else exists besides here, this room, this moment, static in the cooling water with the embodiment of perfection.
When you tell it to him, as you so often do, when you tell him that he's perfect, he can't believe you. The first time you ever said it, peering into his eyes as if they held some secret treasure within, he thought you were joking. He'd laughed, more out of obligation than actual humour, but your expression remained still. Sincere. To say he was moved would be a wildly inadequate explanation. What he felt in his chest that night was something otherworldly, something without a name. He's come now to associate it simply with yours.
You run water through his hair, rinse out the shampoo as he lies pliant in your hands. He insists you use your soaps in his hair, some floral-scented collection you've used for who knows how long, because the smell reminds him of you.
There's no point in overthinking it, you suppose. No point in trying to map out and organise moods, emotions. No point in trying to turn a gentle human experience into something clinical, something without humanity.
That swirling, omnipresent yet transient concept of humanity. You simply must cradle it within your own. You press your lips into his wet hair, whisper words made of ginger and lavender into his ear. Because at the end of the day, you're human. You're in love. And sometimes, that's all that matters.
1K notes
·
View notes
Text
Natural Breeding Clinic - Prologue
warnings: MDNI, breeding kinks, general sex, mention of infertility and insemination methods
a/n: It's here. Finally.

Teaser - Prologue - Patient 1
You take a deep breath and sit down in front of the laptop, waiting for the other person to join the call. Never in your life had you heard about such a unique reproductive center but lately, you’d been feeling the pull to start your own family. You’d discussed this with relevant people in your life. Everyone had said if you really wanted a child, then you should go with the options you thought were right for you.
You’d done the research, looking into different doctors and fertility clinics, but this one just stood out. There were testimonials from several happy families, saying their methods, though unconventional, were effective, and the doctors showcased on the website were all incredibly striking, each one handsome in their own way. But it was the success rate that caught your eye. A 98% guaranteed rate that you would be pregnant, and that pregnancy would be healthy. The site didn’t go into too much detail on their method, but the wording caught your eye.
“A natural breeding clinic” they’d called themselves. You’d finally bitten the bullet and called, requesting an information session. The screen suddenly lightens and you focus your attention as an attractive woman with shoulder-length brown hair comes into view. She smiles in a welcoming way before speaking.
“Hello. Am I speaking with Mrs. L/n?” You nod and smile back, trying not to look awkward or uncomfortable.
“Perfect! My name is Shoko Ieiri, I’m the main coordinating nurse here at Jujutsu Fertility. Thank you for scheduling an information session with us.”
“Yes, of course. I just needed more details before I booked an appointment.”
“Indeed.” Shoko claps her hands together before continuing. “Let me start by telling you a little bit about ourselves. We’ve been around for almost 6 years now. What sets us apart is that we focus more on women’s comfort than most other clinics. And we are sought out by people who are willing to use a sperm donor. We do not perform insemination services with sperm that are not from our own stock.”
“Your own stock? Are you associated with a sperm bank? And screen all the donors yourself?”
“Not a sperm bank in the conventional sense. We have 5 doctors who keep excellent health and their sperm is regularly screened to ensure quality. They are the only stock we allow for insemination.”
You blink to make sure you haven’t misheard. “The…doctors? Are you saying the fertility doctor I’d be meeting with will also be my sperm donor?”
“That is correct.” Shoko nods her head to confirm. “You will be meeting with the doctor of your choosing for at least 5 sessions. They will need to be at least once a week. Some women take the week off and come in 5 days straight.”
“5…sessions?” you ask, confused by the wording.
“Yes. It’s to ensure the insemination process has occurred an optimal number of times.”
“Wait…so…I’m going to be inseminated multiple times? How much downtime do I need in between each insemination?”
“Hardly any. Our method isn’t like a typical clinic. Most women leave feeling very normal and a lot more satisfied than when they came in.”
“Not like a typical clinic? So…you don’t use the catheter method?”
“We use minimal medical equipment in our inseminations.”
“Minimal…so what does the procedure entail?”
Shoko clears her throat and continues. “So it begins with you choosing one of our doctors. We highly recommend spending some time on this part. It’s essential that you feel attraction towards your doctor. Once you make a choice, they will reach out to discuss how your insemination experience can be optimized for you. You will receive a biodata on their sexual profile, their preferred methods of arousal, and other relevant details.”
“I’m sorry, but what?” You are at the edge of your seat wondering if you’ve entered an alternate dimension. Surely, this was all being made up? “Arousal, sexual profile- why would I need all these details? I thought sperm donors only gave information like height, weight, medical history and stuff like that.”
“Why wouldn’t they? You’re choosing to be bred by them. They would have to make sure their patient is satisfied with the experience.”
“Bred?” You bleat the word stupidly.
“Yes. We are a natural breeding clinic. We use the method nature has provided to us to ensure a pregnancy.”
The gears in your brain start turning and something finally clicks.
“Are-are you saying…I would be having sex with my doctor?”
“That is correct.” Shoko smiles gently at you, pleased that you have finally caught on.
“The human body doesn’t necessarily enjoy having medical equipment inserted into it. All that cold plastic, and the mechanical methods of insertion. It puts the body in a state of stress. Not good for implantation. So our doctors will inseminate you through the process of intercourse.”
Her words fall like a fog around you. You can feel your heart racing, a flush creeping into your cheeks. It was…insane. The doctor of your choosing was essentially going to fuck a baby into you. As your mind starts pulling up the images of their doctors, each one impossibly handsome and striking, you feel a familiar throb starting between your legs. Wetting your lips, you try to talk to continue with the information session.
“I see. And…there are benefits to this?”
“Yes. Intercourse allows the body to relax, releasing happy hormones. In this stress-free state, in addition to the knowledge that your doctor is someone you’re attracted to and trust, the chance of an implantation doubles.”
You gape at Shoko, your mind reeling from all the information.
“And…when you say the insemination process will be optimized for my best experience…?”
“The doctor you choose will ask you extensive questions about your preferences. What turns you on, positions, dislikes, toys. It’s to determine if they will satisfy your breeding experience. If they feel they might not be a good fit, they’ll recommend another one of our doctors.”
You swallow, your mouth going dry. “I see. And…what else do I need to know?”
“We will start by collecting your medical history and run some blood work to make sure your body is ready for an insemination process. Women who have a domestic partner will need to get both a waiver and a consent form signed by their partner that they have been informed what happens for the insemination.”
“Of course. Makes sense.”
“You will be assigned an emotional support companion during this process. It will either be myself or Mr. Ijichi Kiyotaka. We are there to help ease your nerves and ensure you enjoy the process. And all patients must think of a unique safeword to use during the insemination process.”
“Safeword?” you parrot back, still processing.
“Yes. At any point during the process, should you feel uncomfortable, your safeword ensures all actions cease and your doctor will give you some space to breathe and reassess the situation.”
All you can do is nod along. Shoko gives you a look of reassurance. “I can guarantee that most women are pleased with the results. And our doctors are quite skilled in what they do. It’s natural to feel a little shy and embarrassed but at the end of the day, we all share a common goal- a healthy baby.”
Despite your initial shock, you feel some of your trepidation fade away. Shoko continues.
“If you are ok with all of this, I can send you the forms to get the process started. Once those are filled, you can take some time to decide on your doctor. Then we’ll set up a call with them.”
“Thank you.” You make a split-second decision. “Please go ahead and send the forms.”
“Excellent. I’ll send them to the email you put in your inquiry. Was there anything else?”
You shake your head no. “I think I have all I need.”
“Great! I look forward to assisting you again.” Shoko ends the call and you immediately go the the website again to look at the doctors, one of which will end up fathering your child. Such a hard decision. How will you ever make the choice?

@thesunxwentblack @kentocalls @actuallysaiyan
@belle-oftheball34 @jesssicapaniagua
@figmentforms

© unintentionalseductress original work | no copying, plagiarizing or translating
#jjk smut#nanami kento#gojo satoru smut#suguru geto smut#hiromi higuruma smut#choso kamo smut#shoko ieiri#ijichi kiyotaka#natural breeding clinic#nanami kento smut#gojo satoru#geto suguru smut#geto suguru#choso kamo#higuruma hiromi#jujutsu kaisen#jjk x reader#jujutsu kaisen smut#nanami kento x reader#nanami kento x reader smut#gojo satoru x reader#gojo satoru x reader smut#geto suguru x reader#geto suguru x reader smut#higuruma hiromi x reader#higuruma hiromi x reader smut#choso kamo x reader#choso kamo x reader smut#ncs#ncs scribbles
1K notes
·
View notes
Text
MASTER POST OF PROSHIP RESOURCES!!! <3<3
this is just for links (bc i just have No Way of formatting this properly), so for more in-depth stuffs and credits, head to the google doc, or the carrd !! :3c
Fiction ≠ Reality
Violent media -
Does Media Violence Predict Societal Violence? It Depends on What You Look at and When
Video Game Violence Use Among “Vulnerable” Populations: The Impact of Violent Games on Delinquency and Bullying Among Children with Clinically Elevated Depression or Attention Deficit Symptoms
Extreme metal music and anger processing
On the Morality of Immoral Fiction: Reading Newgate Novels, 1830–1848
How gamers manage aggression: Situating skills in collaborative computer games
Examining desensitization using facial electromyography:Violent videogames, gender, and affective responding
'Bad' video game behavior increases players' moral sensitivity
Fiction and Morality: Investigating the Associations Between Reading Exposure, Empathy, Morality, and Moral Judgment
Comfortably Numb or Just Yet Another Movie? Media Violence Exposure Does Not Reduce Viewer Empathy for Victims of Real Violence Among Primarily Hispanic Viewers
Fantasy Crime: The Criminalisation of Fantasy Material Under Australia's Child Abuse Material Legislation
Being able to distinguish fiction from reality -
Effects of context on judgments concerning the reality status of novel entities
Children’s Causal Learning from Fiction: Assessing the Proximity Between Real and Fictional Worlds
Reality/Fiction Distinction and Fiction/Fiction Distinction during Sentence Comprehension
Reality = Relevance? Insights from Spontaneous Modulations of the Brain’s Default Network when Telling Apart Reality from Fiction
How does the brain tell the real from imagined?
Meeting George Bush versus Meeting Cinderella: The Neural Response When Telling Apart What is Real from What is Fictional in the Context of Our Reality
loli/shota/kodocon -
If I like lolicon, does it mean I’m a pedophile? A therapist’s view
Virtual Child Pornography, Human Trafficking and Japanese Law: Pop Culture, Harm and Legal Restrains
Lolicon: The Reality of ‘Virtual Child Pornography’ in Japan
Report: cartoon paedophilia harmless
‘The Lolicon Guy:’ Some Observations on Researching Unpopular Topics in Japan
Robot Ghosts And Wired Dreams Japanese Science Fiction From Origins To Anime [pg 227-228]
Australia's "child abuse material' legislation, internet regulation and the juridification of the imaginationjuridification of the imagination [pg 14-15]
Multiple Orientations as Animating Misdelivery: Theoretical Considerations on Sexuality Attracted to Nijigen (Two-Dimensional) Objects
Positive Impact on Mental Health
Art therapy -
The effectiveness of art therapy for anxiety in adults: A systematic review of randomised and non-randomised controlled trials
Efficacy of Art Therapy in Individuals With Personality Disorders Cluster B/C: A Randomized Controlled Trial
Effectiveness of Art Therapy With Adult Clients in 2018 - What Progress Has Been Made?
Benefits of Art Therapy in People Diagnosed With Personality Disorders: A Quantitative Survey
The Effectiveness of Art Therapy in the Treatment of Traumatized Adults: A Systematic Review on Art Therapy and Trauma
The clinical effectiveness and current practice of art therapy for trauma
Writing therapy -
Optimizing the perceived benefits and health outcomes of writing about traumatic life events
Expressive writing and post-traumatic stress disorder: Effects on trauma symptoms, mood states, and cortisol reactivity
Focused expressive writing as self-help for stress and trauma
Putting Stress into Words: The Impact of Writing on Physiological, Absentee, and Self-Reported Emotional Well-Being Measures
The writing cure: How expressive writing promotes health and emotional well-being
Effects of Writing About Traumatic Experiences: The Necessity for Narrative Structuring
Scriptotherapy: The effects of writing about traumatic events
Emotional and physical benefits of expressive writing
Emotional and Cognitive Processing in Sexual Assault Survivors' Narratives
Finding happiness in negative emotions: An experimental test of a novel expressive writing paradigm
An everyday activity as treatment for depression: The benefits of expressive writing for people diagnosed with major depressive disorder
Writing about emotional experiences as a therapeutic process
Effects of expressive writing on sexual dysfunction, depression, and PTSD in women with a history of childhood sexual abuse: Results from a randomized clinical trial
Written Emotional Disclosure: Testing Whether Social Disclosure Matters
Written emotional disclosure: A controlled study of the benefits of expressive writing homework in outpatient psychotherapy
Misc -
Emotional disclosure about traumas and its relation to health: Effects of previous disclosure and trauma severity
Treating complex trauma in adolescents: A phase-based integrative approach for play therapists
Emotional expression and physical health: Revising traumatic memories or fostering self-regulation?
Disclosure of Sexual Victimization: The Effects of Pennebaker's Emotional Disclosure Paradigm on Physical and Psychological Distress
Kink/Porn/Fantasies
Sexual fantasies -
A Critical Microethnographic Examination of Power Exchange, Role Idenity and Agency with Black BDSM Practitioners
Women's Rape Fantasies: An Empirical Evaluation of the Major Explanations
History, culture and practice of puppy play
What Exactly Is an Unusual Sexual Fantasy?
The Psychology of Kink: a Survey Study into the Relationships of Trauma and Attachment Style with BDSM Interests
Punishing Sexual Fantasy
Women's Erotic Rape Fantasies
Sexual Fantasy and Adult Attunement: Differentiating Preying from Playing
What Is So Appealing About Being Spanked, Flogged, Dominated, or Restrained? Answers from Practitioners of Sexual Masochism/Submission
Dark Fantasies, Part 1 - With Dr. Ian Kerner
Why Do Women Have Rape Fantasies
The 7 Most Common Sexual Fantasies and What to Do About Them
Sexual Fantasies
Pornography -
The Effects of Exposure to Virtual Child Pornography on Viewer Cognitions and Attitudes Toward Deviant Sexual Behavior
American Identities and Consumption of Japanese Homoerotica
The differentiation between consumers of hentai pornography and human pornography
Pornography Use and Holistic Sexual Functioning: A Systematic Review of Recent Research
Claiming Public Health Crisis to Regulate Sexual Outlets: A Critique of the State of Utah's Declaration on Pornography
Pornography and Sexual Dysfunction: Is There Any Relationship?
Reading and Living Yaoi: Male-Male Fantasy Narratives as Women's Sexual Subculture in Japan
Women's Consumption of Pornograpy: Pleasure, Contestation, and Empowerment
Pornography and Sexual Violence
The Sunny Side of Smut
Other -
Fantasy Sexual Material Use by People with Attractions to Children
Fictosexuality, Fictoromance, and Fictophilia: A Qualitative Study of Love and Desire for Fictional Characters
Exploring the Ownership of Child-Like Sex Dolls
Are Sex and Pornograpy Addiction Valid Disorders? Adding a Leisure Science Perspecive to the Sexological Critique
Littles: Affects and Aesthetics in Sexual Age-Play
An Exploratory Study of a New Kink Activity: "Pup Play"
Jaws Effect
The Jaws Effect: How movie narratives are used to influence policy responses to shark bites in Western Australia
The Shark Attacks That Were the Inspiration for Jaws
The Great White Hope (written by Peter Benchley, writer of Jaws)
The Jaws Myth [not a study BUT is an interesting read and provides some links to articles and studies]
Slenderman Stabbings
Out Came the Girls: Adolescent Girlhood, the Occult, and the Slender Man Phenomenon
Jury in Slender Man case finds Anissa Weier was mentally ill, will not go to prison
2nd teen in 'Slender Man' stabbing case to remain in institutional care for 40 years
Negative effects of online harassment
How stressful is online victimization? Effects of victim's personality and properties of the incident
Prevalence, Psychological Impact, and Coping of Cyberbully Victims Among College Students
Offline Consequences of Online Victimization
The Relative Importance of Online Victimization in Understanding Depression, Delinquency, and Substance Use
Internet trolling and everyday sadism: Parallel effects on pain perception and moral judgement
The MAD Model of Moral Contagion: The Role of Motivation, Attention, and Design in the Spread of Moralized Content Online
Morally Motivated Networked Harassment as Normative Reinforcement
When Online Harassment is Perceived as Justified
Violence on Reddit Support Forums Unique to r/NoFap
"It Makes Me, A Minor, Uncomfortable" Media and Morality in Anti-Shippers' Policing of Online Fandom
#proship#profic#proshippers please interact#pro ship#profiction#anti anti#proship please interact#pro fic#🏁🎸
516 notes
·
View notes
Text
New Development in the Helicopter Crash 👇

This gets more interesting 👇

Her social media has been scrubbed 👇
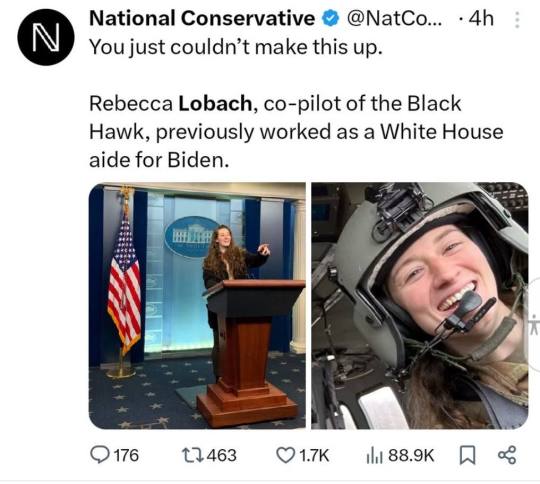
A White House aide for Biden 👇
Graduated with a Biology degree in 2019 from North Carolina Chapel Hill... Where the gain of function that created Covid started.
Let's löök at her parents 👇
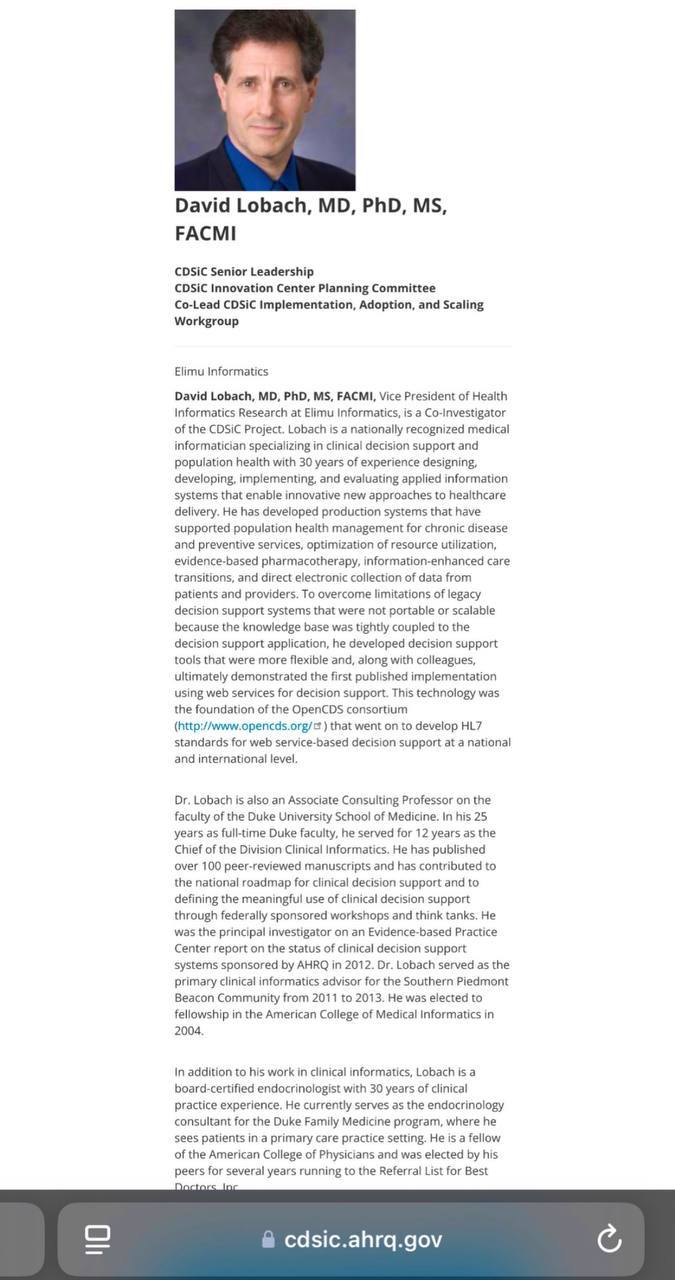
REBECCA LOBACH was the DAUGHTER of DAVID LOBACH (Duke University Medicine; Elimu Informatics; HHS) and ELIZABETH LOBACH (New Regency).
DAVID FRANKLIN LOBACH
*DUKE UNIVERSITY SCHOOL OF MEDICINE, Chief of Division Clinical Informatics, Associate Consulting Professor
*DUKE FAMILY MEDICINE PROGRAM, Endocrinology Consultant
*ELIMU INFORMATICS, VP of Health Informatics
*CDSiC PROJECT, Elimu Informatics (Co-Investigator)
💥NOTE 1: Duke University is run by Trustees Chairman and Mossad asset, Laurene Sperling, who is also the Chairman of Combined Jewish Philanthropies (CJP) and is married to Thermo Fisher (PCR TESTS) Lead Director, Scott Sperling. Thermo Fisher = Temasek (Singapore).
💥NOTE 2: Duke University School of Medicine is led by Dean, Nancy Andrews, who is the Chairman of Wellcome Burroughs (Wellcome/Farrar), who sits on the Board of Directors at Novartis and is a Senior Advisor to NIH Executive Leadership (Anthony Fauci).
💥NOTE 3: Duke Kunshan is a PARTNERSHIP between Duke University and Wuhan University and it officially opened its doors in 2013, which is the SAME YEAR that DAVID RUBENSTEIN (Duke Capital Partners, Carlyle Group, Booz Allen Hamilton, CFR, Brookings, etc.) became the CHAIRMAN of the DUKE UNIVERSITY BOARD OF TRUSTEES.
*Both David Rubenstein and Laurene Sperling are CURRENTLY on the ADVISORY BOARD of DUKE KUNSHAN UNIVERSITY in WUHAN, CHINA.
Duke University is arguably the MOST IMPLICATED SCHOOL IN AMERICA with regard to the COVID PANDEMIC CONSPIRACY and the CREATION & RELEASE of COVID… and COVERUP of COVID’S ORIGINS.
Her Mother 👇
ELIZABETH LEE LOBACH
NEW REGENCY PRODUCTIONS (Development), Writers’ Assistant, Office Assistant, Analyst & Script Editor
*TWENTIETH CENTURY FOX (Post-Production), Office Assistant, Research & Analysis.
💥NOTE: New Regency Productions was FOUNDED by ISRAELI SPY, ARNON MILCHAN, one of NETANYAHU’S CLOSEST OPERATIVES and ISRAEL’S MOST LEGENDARY SPIES. He was involved in helping ISRAEL STEAL AMERICAN NUCLEAR SECRETS several decades ago.
Moving on 👇

This is the man that founded the company where helicopter pilot, Rebecca Lobach’s mother works…
Nothing to see here 👇

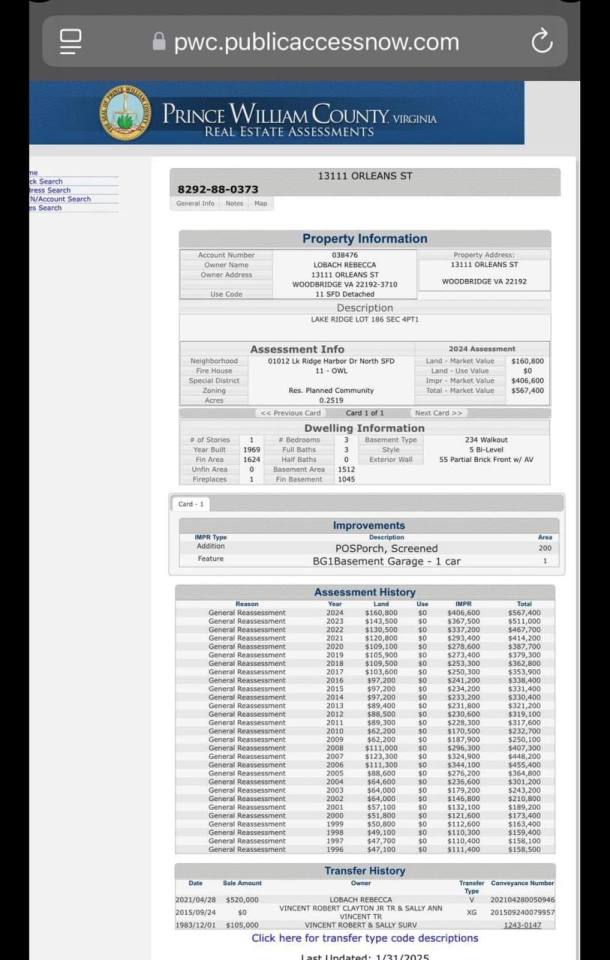
Rebecca Lobach was still in ROTC training in 2018.
How is she flying government continuity missions in a Blackhawk in Washington DC 6 years later as a captain? And how did she afford a $520,000 house two years into the military? 👇
Rebecca Lobach, involved in DCA crash, served as a White House social aide under Biden.
She escorted Ralph Lauren through the White House when he was among those awarded the Presidential Medal of Freedom by former fake President Joe Biden. 👇
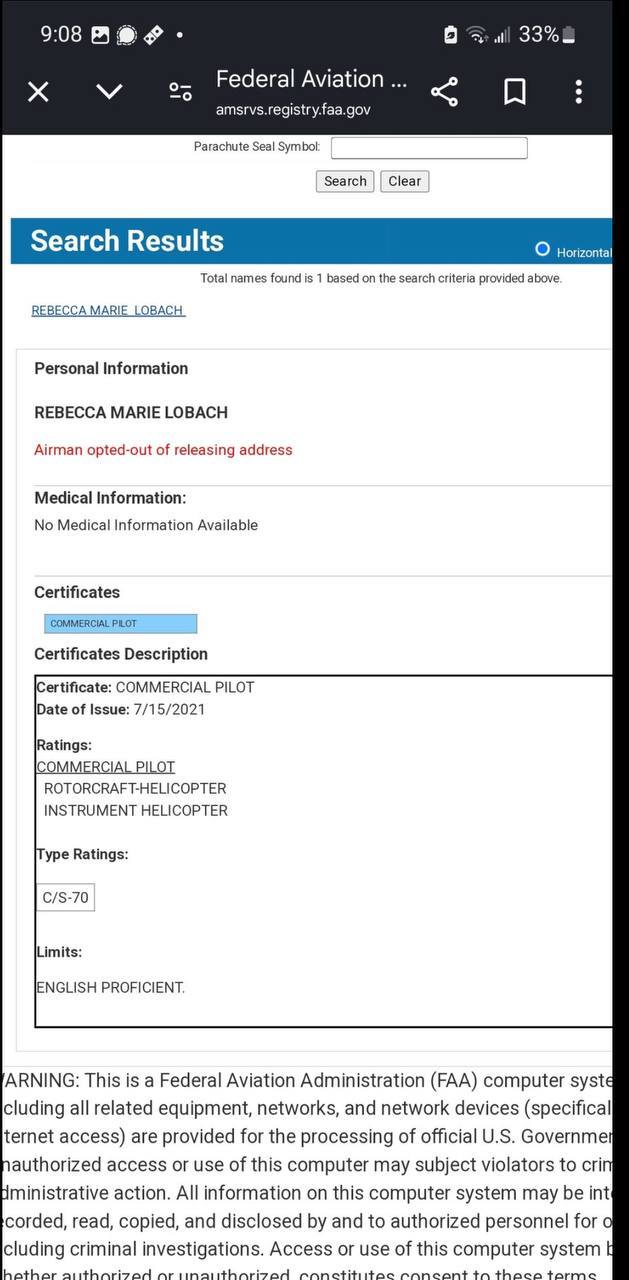
This is a screen grab from the FAA’s Airman registry which is available to the public it shows that Rebecca Marie Lobach did not currently hold an FAA medical which is required to have military certificates converted over to FAA certificates meaning she lost her medical…? 👇

Not sure what she ‘destroyed’.. but she doesn’t look fit to me! 👇
A statement from:
Art Halvorson @ArtHalv....
As a former military instructor, I'll tell you that Rebecca Lobach in NO WAY should have been the pilot in command on that flight.
500 hours in 5 years is Inconceivable! 👇
I think there’s more to this tragic incident than DEI hiring, but it was because of DEI policies that Rebecca was on board that helicopter and there are now 67 people dead. 🤔
#pay attention#educate yourselves#educate yourself#reeducate yourselves#knowledge is power#reeducate yourself#think about it#think for yourselves#think for yourself#do your homework#do your research#do your own research#do some research#ask yourself questions#question everything#helicopter crash#news#rabbit hole#you can't make this shit up#government corruption#government secrets#investigation
254 notes
·
View notes
Text
For much of living memory, the United States has been a global leader of scientific research and innovation. From the polio vaccine, to decoding the first human chromosome, to the first heart bypass surgery, American research has originated a seemingly endless list of health care advances that are taken for granted.
But when the Trump administration issued a memorandum Monday that paused all federal grants and loans—with the aim of ensuring that funding recipients are complying with the president’s raft of recent executive orders—US academia ground to a halt. Since then, the freeze has been partially rescinded for some sectors, but it largely remains in place for universities and research institutions across the country, with no certainty of what comes next.
“This has immediate impact on people’s lives,” says J9 Austin, professor of psychiatry and medical genetics at the University of British Columbia. “And it’s terrifying.”
The funding freeze requires agencies to submit reviews of their funded programs to the Office of Management and Budget by February 10. The freeze follows separate orders issued last week to US health agencies—including to the National Institutes of Health, which leads the country’s medical research—to pause all communications until February 1 and stop almost all travel indefinitely.
The confusion is consummate. If the funding freeze continues through February, and even beyond, how will graduate students be paid? Should grant applications—years long in the writing—still be submitted by the triannual grant submission deadline on February 5? What does this mean for clinical trials if participants and lab techs can’t be paid? Will all that research have to be scrapped thanks to incomplete data?
Even if Trump fully reverses the freeze on research funding, the damage, multiple sources say, has been done. Although for now the funding freeze is temporary, the administration has shown how it might wield the levers of government. The implication is that withdrawing funding could be done more permanently, and could be done to individual institutions, individual organizations, both private and public. This won’t just set a precedent for the large East Coast or West Coast universities, but those located in both red and blue states alike.
While always an imperfect arrangement, science in the US is largely funded by a complex system of grant applications, reviews by peers in the field (both of which have had to be halted as part of the communications pause), and the competitive distribution of NIH funds, says Gerald Keusch, emeritus professor of medicine at Boston University and former associate director of international research for the NIH. According to its website, the NIH disburses nearly $48 billion in grants per year.
When it comes to medical research, America truly is first, and if it abdicates that position, the void left behind has global ramifications. “In Canada, we have always looked to NIH as an exemplar of what we should be trying to do,” says Austin, speaking to me independently of any roles and affiliations. “Now, that’s collapsed.”
Science is, in its very nature, collaborative. Many consortiums and alliances within scientific fields cross borders and language barriers. Some labs may be able to find additional funding from alternative sources such as the European Union. But it is unlikely that a continued withdrawal of NIH funding could be plugged by overseas support. And Big Pharma, with its seemingly endless funds, is unlikely to step up either, according to sources WIRED spoke with.
“This can’t be handed off to drug companies or biotech, because they’re not interested in things that are as preclinical as a lot of the work we’re discussing here,” says a professor of genetics who agreed to speak anonymously out of fear of retribution. “Essentially, there’s a whole legion of university-based scientists who work super damn hard to try to figure out some basic stuff that eventually becomes something that a drug company can drop $100 million on.”
The millions of dollars awarded to high-achieving labs is used to fund graduate students, lab techs, and analysts. If the principal investigator on a research team is unsuccessful in obtaining a grant through the process Keusch describes, often that lab is closed, and those ancillary team members lose their jobs.
One of the potential downstream effects of an NIH funding loss, even if only temporary, is a mass domestic brain drain. “Many of those people are going to go out to find something else to do,” the professor of genetics says. “These are just like jobs for anything else—we can’t not pay people for a month. What would the food service industry be like, for example, or grocery stores, if they don’t pay somebody for a month? Their workers will leave, and pharma can only hire so many people.”
WIRED heard over and over, from scientists too fearful for their teams and their jobs to speak on the record, that it won’t take long for the impact to reach the general population. With a loss of research funding comes the closure of hospitals and universities. And gains in medical advancement will likely falter too.
Conditions being studied with NIH funding are not only rare diseases affecting 1 or 2 percent of the population. They’re problems such as cancer, diabetes, Alzheimer’s—issues that affect your grandmother, your friends, and so many people who will one day fall out of perfect health. It’s thanks to this research system, and the scientists working within it, that doctors know how to save someone from a heart attack, regulate diabetes, lower cholesterol, and reduce the risk of stroke. It’s how the world knows that smoking isn’t a good idea. “All of that is knowledge that scientists funded by the NIH have generated, and if you throw this big of a wrench in it, it’s going to disrupt absolutely everything,” says the genetics professor.
While some are hopeful that the funding freeze for academia could end on February 1, when the pause on communications and therefore grant reviews is slated to lift, the individuals WIRED spoke with are largely skeptical that work will simply resume as before.
“When the wheels of government stop, it’s not like they turn on a dime and they just start up again,” says Julie Scofield, a former executive director of NASTAD, a US-based health nonprofit. She adds that she has colleagues in Washington, DC, who have had funding returned to their fields, and yet remain unable to access payment through the management system.
Austin says that already the international scientific community is holding hastily arranged online support groups. Topics covered range from the banal—what the most recent communication from the White House implies—to how best to protect trainees and the many students on international visas. But mostly they’re there to provide support.
“I’ve had a lot of messages from people just expressing gratitude that we could actually get together,” Austin says. “There’s just so much unaddressable need. None of us has the answers.”
Scientists, perhaps more than any other profession, are trained to “learn and validate conclusions drawn from observation and experimentation,” says Keutsch. That applies to the current situation. And what they observe during this pause of chaos does not portend well for the future of the United States as a pinnacle of scientific excellence.
“If people want the United States to head toward being a second-class nation, this is exactly what to do. If the goal is, in fact, to make America great, this is not a way to do it,” says the genetics professor. “This is not a rational, thoughtful, effective thing to do. It will merely destroy.”
This story has been written under a pseudonym, as the reporter has specific and credible concerns about potential retaliation.
193 notes
·
View notes
Text
Costume Party
Pairing: Wanda Maximoff x reader
Word count: ~5.8k
Summary: You and Wanda go to a Halloween party
A/N: This one was mostly for my own benefit tbh...
Warnings: fluff, lusting over wifey, angst
You’ve never done something like this before.
Correction.
You’ve never done something like this before with Wanda.
You’d lost count of how many parties you’ve gone to since starting at the clinic you were hired at right after graduation. There had been Halloween, New Year’s, and Christmas parties over the years, but it was no surprise to anyone which was your favorite.
The parties were usually held at one of the doctor’s houses or a venue in town. Somehow, you’d avoided having to host at your place because although it was large enough, you definitely didn’t want anyone snooping around. You also knew it would be nightmare for security. One year you’d used Pietro’s house and that had gone pretty well, but you didn’t want to put him out again. Especially since he hadn’t been able to attend.
This was exactly what you and Wanda were dealing with today.
You’d wanted Wanda to come with you to this year’s Halloween party hosted by the lead doctor at work. You’d thought about it a lot and you were convinced that if she dressed up enough, she would be unrecognizable. When the idea first came to you, you did extensive research to pick the best option for Wanda. Rather you picked the top three ideas and then presented them to your wife with a hopeful expression. You’d immediately disregarded matching costumes because that was one cliché you weren’t into. Your options had been narrowed down as well, and since you loved a good top hat, you were going to put together a steampunk outfit somehow.
Wanda had met your options with reluctance. Not because she didn’t want to go with you, but as always, she was just worried that her disguise would fail. She didn’t want to be conceited enough to think that she’d be easily recognized, but she also didn’t want to risk the fallout associated with the alternative. You’d agreed, which is why all of the options for your wife included full, if not over the top make up.
“I’m not…can you explain this one again?”
You remember how Wanda had shot you an uncertain look as she gestured to the picture you’d printed out of the costume you really wanted your wife to choose.
It was from one of your favorite artist’s music videos and it involved pink hair, a suit, and makeup that made her look like a skeleton.
A very hot skeleton.
You’d told your wife some of this, and since she’d recognized the artist’s name, she’d finally decided to go with it.
“You’re sure you can find someone to do the make up?”
You’d certainly considered this since as much as you’d like to give it a shot, you didn’t have the necessary skill. You talked to Nat and she’d used her connections to find someone in school to be a makeup artist. They’d already confirmed that they could do any of the three choices, and they were willing to sign an NDA.
It was all just up to your wife now.
“Okay, let’s do that one then. It looks…cute.”
You’d laughed at this, and you smile at the memory as you stand in the living room waiting for your wife to finish up.
It was the night of the party and you were already dressed and ready to go. Granted your costume didn’t involve quite as much work as your wife’s, but you’re still a little antsy to get going. You glance at your pocket watch. The one that you bought to go with this costume. It looked old and fit the theme perfectly, and it somehow cost less than $50. You know you’ll probably rarely use it after tonight, but it’s still worth it.
You’re excited to finally introduce your wife, or at least her alter ego, to everyone that you work with. You know it’s causing Wanda a fair amount of anxiety, but you’re going to do your best to reduce this as much as possible. You’ve prepared answers to any questions and you’ve practiced with Wanda a dozen times since she agreed to go to this party.
You’re ready.
Wanda’s regretting her decision to say yes to you.
As much as she loves you, she’s not sure that this was the best idea. Her costume is coming together nicely, and she can’t say that she even recognizes herself in the mirror, but she’s still nervous.
She has blue contacts in and her make up is almost completely done. Her pink blonde hair looks so out of character that she’d laugh if she wasn’t afraid of scaring her make-up artist. They already appeared a little on edge when they started, but as they’d gotten into their work they luckily seemed to relax. Wanda was trying to make small talk, but her own nerves made that minimal.
She nearly jumps when she feels something brush against her legs and the hands in her lap. She glances down just enough to avoid getting poked in the eye, and she spots Rogue looking up at her curiously. She smiles at him and scratches his head before she realizes that he’s getting fur all over her. Luckily she’s not changed into her suit yet, but she’d hate to ruin the effect by showing up covered in fur.
Then again, if anyone will understand the plight, it will be a bunch of people in vet med.
“Hey bud. Are you getting bored? We’re almost done here.”
Not that she thinks Rogue will be any less bored soon since he’s not allowed to come tonight. The invite had kiddingly said that all pets were allowed, but there would be no pet sitters at the party. Not only did that sound like hell, but she is certain that Rogue would not do well. He’d probably stick to her side all night and she didn’t want that. She wanted to try and enjoy her time with you, and that would be much easier if she wasn’t worried about her dog while trying to maintain her cover.
Almost half an hour later, you glance up at the sound of the bedroom door opening. You smile when you see Rogue run out first, but you nearly drop your phone at the sight of your wife.
“Holy shit.”
You’re smiling widely as you watch Wanda descend the stairs in all her glory. You try to focus on each part of the costume before taking it all in at once.
She hadn’t wanted to dye her hair for this so she’d found a very convincing wig. It’s long enough that the pink falls past her shoulders and down her back.
The simple black suit with a white top looked tailored within an inch of its life, and you were obsessed with it. The dress shoes she wore were so new they shined and you don’t realize you’re staring until suddenly you catch a hint of your wife’s perfume. You look up and are immediately rendered dumb again at the precise, surprisingly flattering makeup.
“Wow.”
Wanda hadn’t failed to notice your attention, but she was a little preoccupied by your appearance to comment immediately.
She’d seen you collecting pieces of your costume over the past few weeks, but this was the first time she was seeing it come together. She doesn’t realize that she’s stopped short and Rogue’s stumbled into her as she takes in your unreasonably attractive look.
You’re wearing a dark red tailcoat that extends down past your calves that are adorned in black boots that fall just short of your knees. Wanda focuses on the leather of the coat and how it tapers into a material that matches the red of your tight pants. Her gaze drifts back up to the elaborate belt and the corset that nearly makes her bite her lip. The corset dips into a V to reveal a hint of the black collared shirt you’re wearing underneath.
“Well fuck.”
You’re smiling widely as your wife finally meets your gaze before it flits to your personal favorite portion of your ensemble. The hat.
You are wearing more jewelry than you usually do, and you’re not sure you can eat anything in the corset, but the look on your wife’s face is so worth it.
“You like?”
The unnecessary question is just met with a silent nod as Wanda reaches out for your gloved hands. She admires the gauntlets you’re wearing and the attention to detail that your costume required. She meets your gaze again with another muttered curse as she reaches up to touch the goggles that you have secured around your hat. You only considered wearing them briefly until you realized how hard it was to see through them.
You also had considered wearing a skirt or a dress, but this was a work party, and you didn’t want to overdo it.
“You look fantastic, detka. Shit.”
Wanda’s really regretting her decision to go to this party now because that means they need to leave soon, and she’d want nothing more than to stay here with you instead. She’d love to take off this costume piece by piece, but unfortunately, she’s going to have to wait.
You’re reaching out for Wanda, stopping just short of touching her face before your hand falls to one of her lapels. You play with Wanda’s fake pink locks with a grin of your own that tells your wife all she needs to know. That said, it never hurts to hear how much you appreciate her, out loud.
“Thanks, babe. I’m a bit at a loss for words. You look so much better than I ever imagined. You did a great job, Lane!”
The makeup artist that Wanda just realized was still here smiles politely before offering you a rushed thanks. You ask them to take a picture of you two before you let them flee to the car that brought them here to be escorted home. You gave them a hefty tip on top of their paltry fee, and since they signed the necessary documents to ensure their silence, you let them go with a thank you, but not another thought.
“I’m kind of wishing I didn’t say I’d go to this party after all.”
Wanda can’t help but laugh when you say this, and you have to resist the urge to lean in and kiss her. You don’t want to ruin her makeup. She sees you lean in slightly before falling back again and she offers you a sly grin.
“That’s going to have to wait. I’m also a little worried I can’t eat or drink anything at this party.
You’ll find out later that she can do both, she just has to be careful about it. You arrive a fashionably 30 minutes late only to be greeted by the lady of the house.
You smile widely and Wanda prepares herself for a night of niceties and subterfuge.
“Y/n! Wow you look great! Oh goodness you must be Linda. It’s so nice to meet you!”
That was the other thing about tonight.
You had to remember that you were married to ‘Linda’ tonight, and that the woman beside you was in life insurance. It sold itself, but it was honestly not something very interesting to talk about which was key.
You accept a hug from the taller doctor, and you send her a silent thank you when she just shakes Wanda’s hand before waving the two of you in. You can tell that Claire’s house is already full of your coworkers and their spouses, and you have to bite back a smile at the glee you feel at finally being able to introduce Wanda to them. You lead Wanda down the hall by the hand as you turn around to glance at the blonde with a knowing look.
The theme tonight had been very loosely thrown out by several people at work. Pop culture or media. Being the person that you were, you were very anxious about dressing up wrong, and Wanda had to remind you that it honestly didn’t matter. Pop culture or media could encapsulate practically anything.
Including a movie character.
You pause momentarily before you speak up loudly enough for Wanda to hear you. She gives the blonde beside you a once over before realizing that she never would have guessed her costume if you hadn’t just told her.
“You look so much like Uma Thurman right now that it’s a little scary.”
You note the yellow and black jumpsuit as you walk farther into the house where you catch normal music instead of something Halloween themed playing. That was one thing you didn’t enjoy about the holiday. The cheesy music.
Claire laughs as she follows you to the open living room that has nearly two dozen people either talking, dancing, or enjoying the food and drinks.
“It was Rick’s idea. He dressed up as Bill for some reason. I think he’s trying to tell me something, but I’m not quite sure what it is.”
You stifle a loud laugh as you catch sight of the blonde’s husband at the counter mixing drinks dressed the part of a villain.
You and Wanda make the rounds before either of you bother to grab a drink. You’d met multiple couples dressed up in a variety of costumes, and you think your favorite was a female couple dressed as Dracula and Freddy Krueger.
Wanda’s paranoid as always and gets some bottle of beer while you get whatever was in the punch bowl. You smile at your wife lovingly as you lean against the small alcove beside the kitchen you’ve managed to escape to. You take a sip and spend the next few moments admiring Wanda’s still perfect suit and makeup. You are dying to kiss her, but as you watch her carefully sip from her bottle, you know that you’ll ruin her lipstick. The black lines carefully drawn across her lips have the effect of looking like teeth, and if you think too much about it, you’d be a little scared of her.
The makeup doesn’t just stop at her face either. It extends down her neck, and any other exposed skin to make her look the part of a skeleton. The fingers circling the bottle are meticulously drawn on, and you’re surprised to see they’ve held up well to shaking half a dozen hands.
“What’s on your mind?”
You realize you’re caught when you meet Wanda’s gaze to see her shooting you a suspicious look. You don’t have time to respond before someone over her shoulder catches your attention.
“Dr. Y/l/n, oh my God, I barely recognized you! You look so good!”
You stand up a little straighter and offer a wide, genuine smile as you look over the younger woman’s outfit.
Meghan is one of the newer vet assistants at work, but she’s so quick to catch on that it feels as if she’s been there for years. She’s smart, a great multitasker, and you’re seriously going to miss her when she goes to vet school in a year.
The brunette is dressed as Medusa and her long locks are styled to look like the snakes on top of her head. Her green dress glitters and has the appearance of scales that really bring her costume together. You say something about her hair, and she just smiles before she turns her attention to Wanda.
“Thanks! I think that you win the coolest hair though. I was dying to wear pink but couldn’t make it work with this outfit.”
She holds out a hand to Wanda who doesn’t hesitate to take it as she slips into her unthreatening wife-of-a-doctor persona.
“I’m Meghan one of the vet assistants. It’s nice to meet you.”
Wanda nods in agreement which you can tell is genuine. Of all the assistants at work, you talked about Meghan the most because she was usually a huge help on days you were there. You have to stop yourself from reacting when Wanda speaks up.
“Linda. It’s nice to meet you too. Y/n has nothing but good things to say about you.”
You watch in amusement as Megan blushes before she hurries to change the subject. She’s still so shy, and she tends to underestimate her value. She reminds you of someone else you know.
“Oh, thank you. Now I have to ask since I know a bit about Dr. Y/l/n’s taste in music, but was the costume your idea or hers?”
You try not to flush at the question and the follow up questions that you’re sure your wife will ask. If not now, later. You usually mention your surgery days if they’re especially interesting, but you don’t think you’ve ever told Wanda about if they’re more relaxed. On these days, depending on who else is working, you’ll have music playing in the surgery suite, and sometimes your tastes are all over the place.
The last surgery day where you’d just had 5 dog neuters in a row, you’d been listening to early 2000’s pop.
When you see Wanda smile wickedly, you know what’s about to happen. You’re just grateful that she chose Meghan to confide in because you’re certain you would have died of embarrassment if she’d told anyone else this.
You watch Wanda lean in as if she’s telling a secret before she thoroughly throws you under the bus.
“If I didn’t know better, I’d be a little insulted that she spent nearly two weeks watching all of Lady Gaga’s and Brittney Spears's music videos to figure out my outfit.”
From Meghan’s expression, you can see that the brunette can’t tell if Wanda’s joking. She quickly clears this up though as she shrugs and offers the younger woman a smile.
“I’d already thought of an idea myself, but I didn’t want to spoil her fun. I’m just glad she didn’t ask me to dress up as a dog or something.”
Meghan laughs as you roll your eyes because seriously? You wouldn’t waste the opportunity to dress up your wife by putting her in a dog suit that drowned her. You suppose that putting her in that costume would have helped hide her identity, but you hadn’t wanted to do it like that. Selfishly, you wanted to show her off. You wanted people to see how beautiful and smart and kind your wife was.
Maybe not so kind right now, but that was fine. You could take what she dished out.
“That’s hilarious! I’m actually surprised she didn’t bring either of your dogs tonight. The costume she made Boone for Halloween was so cute!”
You had to admit that you’d done a pretty good job with his costume. You’d worked on Halloween and you hadn’t wanted to dress up, but you definitely hadn’t passed on the opportunity to put Boone in a cute outfit. You had dressed him up as a dogtor because it was practically expected. He had his own little white coat that you’d fitted out of one of your own. You gave him a fake stethoscope and bought him scrubs that wouldn’t be too hard to tailor to fit him. You’d honestly put in an entire weekend getting it together, but you didn’t regret it at all. Even when Boone peed in it because you’d overlooked one crucial detail.
“Did she tell you how long she spent on it? Hours! I thought she was just going to buy something to have him carry around, but I honestly should have known better.”
As your wife and Meghan laugh and talk about you like you’re not there, you glance around the room curiously. You’ve met most of the people here already and you’re honestly getting a little tired. Tonight, has been a lot, and despite having fun, you can tell that your social battery has drained a lot since walking through the front door. You find your host and smile at the sight of her talking to a Velma and Daphne. You take another sip of your drink, but you stop short when something fuzzy brushes against your leg. You look down and see a small tortie staring at you. Your smile widens as you kneel to scratch the purring cat.
“Wan—Um Lin, look a cat!”
Wanda looks down at you a little startled, but this quickly melts away when she sees the furry creature head butting your knees. She offers a small smile before she shakes her head with an adoring look that makes you glad that it’s too dark for anyone to see you blush from down here.
“Cute. Leave it to you to find a cat to hang out with.”
You start slightly when the cat jumps onto your knees, but you recover quickly and scoop her up into your arms. You scratch beneath her chin as you come face to face with your wife who is such a big faker sometimes that you can’t help but point it out.
“Yes, cats are the worst. I don’t know how you even have one when you can’t stand them.”
The teasing tone is the only reason that Wanda doesn’t start an argument right here in the middle of a party. She reaches out to scratch the adorable cat who’s getting fur all over you as she glances at you before sparing Meghan a look. She can’t have the brunette thinking that she actually hates cats. She’s married to a vet for Dog’s sake.
“You’re one to talk, detka. Fletcher knows I love her and that’s why I’m the favorite.”
Meghan snickers at this and you’re temporarily distracted by the pet name that you didn’t think Wanda would risk using here. You just sigh and smile dopily as the cat that has basically adopted you starts to play with Wanda’s bowtie. Her claws sink into it and she bites it furiously until it starts to give. You consider rescuing your wife, but she looks the most relaxed she’s been since walking in here, so you let it go on for her sake.
You hear someone call Meghan’s name, and you turn to see another couple of assistants with what look like shot glasses. You’re so grateful to be out of your twenties. Meghan gives them the universal sign of ‘one second’ before she turns back to you with a smile.
“Duty calls. It was good seeing you. Have fun with Misty.”
You realize belatedly that this is the cat that Wanda’s still snuggling with, and you grin before something occurs to you.
“Have fun with all that alcohol. Find me before you leave? I brought the many pins you let me borrow last week.”
Your costume, although cute, had been close to falling apart when Boone kept tripping over his stethoscope. Meghan had come to your rescue with nearly 10 bobby pins that you’d only realized you’d forgotten to return when you arrived home that night.
Meghan nods in agreement, and waves goodbye to Wanda before she’s off. You and Wanda are left alone, relatively speaking, with Misty the cat.
“She’s lovely.”
You figure that Wanda’s talking about Meghan, and not the cat, but you can’t be sure. You only nod in agreement before reaching out to free one of Misty’s claws from the crumbling bowtie. Wanda smiles at you and then her eyes widen in surprise when Misty turns toward you and starts to swat at your face. Or more specifically your hat.
“Y/n, she’s --.”
You don’t have time to flee before Misty reaches out her paw for the feather that’s tucked beneath the goggles on your hat. You curse and try not to freak out when suddenly you have a cat clinging to your hat and hanging in front of your face. Wanda reaches out to grab her and you’re carefully, but quickly extricating yourself from your hat when hear laughing.
You have an armful of cat in your hat by the time you realize your boss has come to your rescue. You see Claire walking toward you with Bill—Rick, who has a feather toy in hand. You try not to feel ridiculous as you drop to the floor and try to roll Misty onto the carpet.
“I should have warned you, Y/n. She’s obsessed with feathers.”
You laugh despite thinking ‘no shit’, but you breathe a sigh of relief when the tortie spots her favorite toy and leaves your hat on the ground with nothing but a lot of fur to show for it.
You stand up and brush out your hat as much as possible before you shoot the blonde a smile.
“To be fair, I shouldn’t have to be warned about that.”
You and Wanda take a moment to gather yourselves. After you help her untie her ruined bowtie, and leave it hanging from her neck in a way that’s somehow even hotter, she puts your hat back on your head.
“You’re so cute, Y/n.”
You want to defend yourself because you’re sure Wanda’s poking fun at you, but you don’t get a chance. Wanda carefully leans in and presses her lips to yours in a soft kiss. She figures that it was worth it when you pull away a little dazed and free of the black streaks that cover her own lips. She smiles at you again before reaching out to grab your gloved hands. She brushes the cat hair off of them and your corset before she sighs inaudibly.
“Are you having fun?”
Wanda asks this a bit later after you’ve finished your drinks and met a few more people. It’s nearing 10 o’clock and you’re honestly ready to leave. You figure you need to find the host before you duck out, but you decide to take a couple of minutes to hold your wife close where you’re settled on one of the loveseats. You are surrounded by people, but you only pay attention to Wanda who’s pressed into your side and leaning her head against your shoulder.
You eventually nod before looking around for Claire. You don’t see her immediately, but you’re not too worried. She’s been an impeccable host as always, so you’re certain she’ll catch you right as you head for the door.
“I am, but I’m getting tired. We better get home before I don’t have the energy to take all of this off.”
Wanda opens her eyes when you say this and she spares your outfit a glance, as if she hasn’t been looking at it all night, and hums. She makes sure no one is within earshot before she offers you a smile.
“I wouldn’t worry about that, Y/n. I’d be happy to help you.”
You don’t doubt this, and you smirk before summoning the energy to sit up. You suddenly want to be home.
“That’s very thoughtful of you. I would of course, love to return the favor.”
Wanda laughs at you as you stand up and hold out a hand to help her to her feet. She grabs it and you tug her to her feet fast enough to make her yelp in surprise. She shoots you a glare when you laugh at her, and she makes a point of dropping your hand and walking away without looking back. You roll your eyes with a smile before you hurry after her obediently and meet her in the kitchen where Claire’s reappeared. She’s collecting dishes and stacking them in the sink for later when she spots the two of you.
“Hey, calling it a night?”
You smile before you nod and glance around the cluttered kitchen. There are glasses, cups, bottles, and plates everywhere. Wanda stands behind you, likely surveying the area with a similar intention.
“We were, but we wanted to see if we could help with anything before we headed out.”
It took a bit of convincing, but you’d helped throw out some of the bottles and get the dishes loaded into the dishwasher before you were being shooed out of the kitchen. You hugged the other doctor again before thanking her for hosting. You and Wanda are near the front door before you remember what you’d told Meghan. You mention that you’ll grab them from the car and bring them back in, and Claire simply nods before claiming that she’ll give them to her for you.
You keep chatting as you walk to your car with Wanda, and you vaguely register the presence of other cars as you duck into the passenger side and reach for the console.
“Here they are. Thank her for--.”
“Freeze! Don’t move!”
You jump in surprise and then nearly stumble back in terror as you turn and see someone pointing a gun at you. They’re standing by the street but they’re crossing the lawn in quick, purposeful steps. You stiffen and faintly register Wanda gripping your arm tightly as she pulls you back against her.
“Y/n.”
She realizes before you do that this person isn’t a threat. They’re dressed as a cop and they’re not even looking at you or her. Their focus is on Claire who’s already scowling at the new arrival. Wanda doesn’t know who this is, but that’s less important to her than addressing your obvious anxiety.
“Campbell what the hell are you doing here?”
The brunette with the fake gun leers before he closes the distance between them in a hug that Claire looks like she’d refuse if she could.
“Don’t be like that Sis. I’m here for the party.”
You’re just starting to breathe again as you watch the exchange play out with a dull sense of awareness that’s clouded by your anxiety. You try to shake your shock, but it’s hard and you’re still looking terrified when the duo turns back to you.
“You’re about three hours late for that, but go on. Rick’s inside.”
Campbell is about to head inside, but he spares you and Wanda a look first. You’re not sure what he planned on saying, but the look on your face must be enough to clue him in. Wanda bites back a curse and you flinch at the question and the unwanted attention.
“Shit, you okay?”
Claire turns to you and you force yourself to speak before she gets a chance. You’re not even sure if you’d decided what to say before the words are falling out of your mouth.
“Fine. You startled me, is all.”
You see the exact moment that Claire gets it, and you have to stop yourself from recoiling in shame. It would have been impossible to get off work for so long without disclosing to your boss what happened to you. At least the extent of your injuries. When you’d been kidnapped from work and then hurt by Rumlow, well you’d taken months off of work. You’d been in the hospital for a while, and even though you can’t be sure because of all the drugs you were on, you think that Claire visited you.
You’d told her later that you’d been shot, and despite returning to work without any complications, the incident stuck with you. It was impossible to ignore the effect of the traumatic experience.
Even months later, the idea of someone pointing a gun at you nearly threw you into a panic attack.
You feel Wanda press herself against your back as an arm circles your waist, but you can’t relax. Not yet.
“Campbell go inside. I’ll be there in a minute.”
Her brother looks like he wants to argue but instead he just shrugs and heads out. He says something to you that you completely miss along with Wanda smiling politely in response, but you can’t bring yourself to care right now. You’re in survival mode and you immediately work out how you can get out of here as quickly as possible. You glance up at Claire before your gaze darts to the front door where you see Campbell disappearing. Someone’s standing in the doorway though and you nearly curse when you see Meghan looking confused.
You nearly shove the bobby pins that you miraculously held onto into the blonde’s hand with a pained smile.
“Here you go. Thank you again for tonight.”
Wanda’s reaching into your pocket for the car keys, but you barely notice as you watch a range of emotions play out on your boss’s face. Concern, confusion, and then understanding.
“Are you going to be alright?”
You manage to make your smile appear a little more genuine before you nod and manage a quick one-armed hug before ducking into your car.
“I’ll be fine. Thank you.”
You wait until Wanda says her goodbyes and gets into the driver’s seat before you take a deep breath. You watch in the rearview mirror as Claire hesitates for a moment before turning around and heading back into the house. If you had to guess Campbell’s going to get an earful, but you can’t think about that right now. You watch both her and Meghan disappear into the house before you realize that Wanda’s holding your hand. She’s started the car, but she’s turned toward you with a concerned look. She reaches out for you, but she stops short when you flinch.
“Y/n, I’m sorry he scared you. I’m not sorry that Claire’s going to chew him out for it, but he didn’t know. He’s not a threat to either of us, okay?”
You just nod a couple of times as you try to process what she’s said. You take a deep breath before removing your hat and holding it in your lap. You feel like you can’t breathe deeply enough in this outfit, and you really want to get home so you can take it off. Wanda seems to realize your dilemma as you start to take slow deep breaths. She buckles up and starts off down the street toward home.
“Let me get you home, so I can take care of you.”
You crack a smile at this and you can’t help but sneak another look at your wife’s suit. Damn you hope she wears it again after this. You fiddle with your hat for a moment before you clear your throat.
“I seem to remember you promised to help me take all of this off. Is that still on the table?”
Wanda rolls her eyes at the question despite the fact that she’s glad to hear you ask. She doesn’t think that what you’d originally intended is still on the table, but she’ll just have to see what happens. Usually anything that triggers your anxiety like this leads to overwhelming exhaustion shortly after.
Either way, she’s happy to do whatever you need to feel better. She doesn’t want tonight to be tainted by this incident. She’s glad she came out with you, and she’s even happier that you seemed to have fun. She would have to do some serious damage control, but hopefully dressing down, cuddling, and spending time with your fur babies will be enough.
“We’ll see, detka.”
Masterlist
#wanda maximoff x reader#wanda maximoff#wanda maximoff x female reader#wanda maximoff fanfiction#wanda x reader#silver springs drabble#silver springs#mob au
91 notes
·
View notes
Text
Also preserved on our archive (Check out the site for full daily updates!)
By Dave Fornell
New research supported by grants from the National Institutes of Health revealed a history of COVID-19 can double a patient's risk of heart attack, stroke or death.[1] The study, published in Arteriosclerosis, Thrombosis, and Vascular Biology, found that the heightened risks can sometimes last for years after a COVID diagnosis.
The research was led by Cleveland Clinic and the University of Southern California. Anyone who had a COVID-19 infection, regardless of severity, was twice as likely to have a major cardiac event, such as heart attack, stroke or even death, for up to three years after diagnosis, the group found. The risk was significantly higher for patients hospitalized for COVID-19 and more of a determinant than a previous history of heart disease.
The researchers also found that patients with a blood type other an O (such as A, B or AB) were twice as likely to experience an adverse cardiovascular event after COVID-19 than those with an O blood type.
These findings show that the long-term risk associated with COVID-19 “continues to pose a significant public health burden” and the findings warrant further investigation, according to the authors.
Cardiology may see increasing numbers of former COVID patients in the years to come During the pandemic, there were serious concerns that the SARS-CoV-2 virus may cause an increase in future cardiovascular issues in COVID patients. This was based on the larger than expected vascular and myocardial involvement seen in many cases. What was originally thought to be long-term damage subsided in patients overtime. While concerns about heart damage and increased numbers of heart failure patients did not come to pass, this study shows evidence that cardiologists may still see increasing numbers of patients in the years to come.
“Worldwide over a billion people have already experienced COVID-19. The findings reported are not a small effect in a small subgroup,” co-senior study author Stanley Hazen, MD, PhD, chair of cardiovascular and metabolic sciences in Cleveland Clinic’s Lerner Research Institute and co-section head of preventive cardiology, said in a statement. “The results included nearly a quarter million people and point to a finding of global healthcare importance that promises to translate into a rise in cardiovascular disease globally.”
Why do COVID patients have elevated cardiovascular risks? Researchers used U.K. Biobank data from 10,005 people who had COVID-19 and 217,730 people who did not between February and December 2020. Certain genetic variants are already linked to coronary artery disease, heart attack and COVID-19 infection, so researchers completed a genetic analysis to see if any of these known genetic variants contribute to elevated coronary artery disease risk after COVID-19. They found none of the known genetic variants were drivers of the enhanced cardiovascular events observed post COVID-19 infection. Instead, the data highlighted an association between elevated risk and blood type.
Previous research has shown that people who have A, B or AB blood types were also more susceptible to contracting COVID-19, the researchers said.
“These findings reveal while it’s an upper respiratory tract infection, COVID-19 has a variety of health implications and underscores that we should consider history of prior COVID-19 infection when formulating cardiovascular disease preventive plans and goals,” Hazen said. “The association uncovered by our research indicates a potential interaction between the virus and the piece of our genetic code that determines blood type and signals the need for further investigation.”
“Given our collective observations and that 60% of the world's population have these non-O blood types, our study raises important questions about whether more aggressive cardiovascular risk reduction efforts should be considered, possibly by taking into consideration an individual's genetic makeup," explained Hooman Allayee, PhD, of USC’s Keck School of Medicine, who was co-senior author of the paper.
Study link: www.ahajournals.org/doi/abs/10.1161/ATVBAHA.124.321001
#covid#covid isn't over#mask up#pandemic#wear a mask#public health#covid 19#wear a respirator#still coviding#sars cov 2#coronavirus#covid conscious#covid is airborne#covid pandemic#covid19#covidー19#long covid
147 notes
·
View notes
Text
Porcelain Doll HRT Observation Report
Part I - WTO Foreword
The report is based on studies and observations performed by Dr. Pierre Oupée, Dr. Kotomi Abuki and Dr. Pirkko Osliini. The team studied 25 participants who underwent therapy including Dr. Osliini.
The therapy has been approved by the World Transhumanism Association, but every licensed physician administering the treatment has to report the course of therapy of at least 50% of patients for clarity of data. The therapy is to be submitted for reapproval once reports of at least 1000 patients are collected.
Part II - Recommended Psychological Evaluation
Before undergoing the therapy it is recommended to evaluate the patients psychologically. The evaluation should take three sessions, which should be performed in intervals of 14 days. The process of evaluation prioritises informed consent and letting the patient consider their decision.
The first session is focused on discussing the desired effects with the patient. During the second session the patient is to be explained about the effects of the therapy. During the third session the patient signs the informed consent file after which they can undergo an endocrinological evaluation and get prescribed the medications.
Part III - Required Medications
All medications are available in oral and epidermal form. It is important to note that the exact dosage differs from patient to patient.
Antihomogen (0,5-2 mg/week) - Humanity removal agent. Due to the anthropomorphic nature of the therapy it is important to keep the dosage low unless cross administering multiple therapies.
Antisomatotropin (10-17 mg/week) - Somatotropin halting agent.
Contostropin (13-22 mg/week) - Shrinking hormone. Due to the rate of influence the final dose should be taken when the patient reaches the height of 5-7 cm higher than desired. Further research is advised.
Tsichirone (17,5-32 mg/week) - Porcelanising agent.
Part IV - Course of Therapy
Phase 1 (onset on week 4-8) - Somatotropin in the patient’s body stops influencing it and constopropin causes it to start shrinking.
Phase 2 (onset on week 7-14) - Tsichirone starts turning the patient’s skin into soft porcelain. The effects of constotropine become amplified causing rapid decrease in height. The patient’s hair starts falling out. It is not understood what causes this effect, but it is observed that it doesn’t affect scalp hair. Further research is required.
Phase 3 (onset on week 20-30) - Tsichirone might cause the patient’s body to spontaneously freeze for a short time. The effect first affects small parts of the body such as single fingers to later spread to entire limbs and near the onset of phase 4 even the entire body. The patient’s scalp hair stops growing. It is not understood what causes this effect. Further research is required. The patient’s body hair falls out entirely midway through this phase. Tsichirone causes the patient’s skin to become more brittle. The patient’s hearing becomes more sensitive to high sounds. It is not understood what causes this effect. Further research is required.
Phase 4 (onset on week 40-56) - The patient’s body is completely turned into soft porcelain. While the patient retains muscle control for some time, tsichirone starts causing muscle atrophy and conversion of movable soft porcelain into immovable hard porcelain.
Phase 4A (10 weeks after the onset of phase 4) - The patient has to register in a surgery clinic licensed to perform dollification surgeries.
Phase 5 (onset on week 55-70) - Tsichirone causes complete conversion of soft porcelain into hard porcelain and complete muscle atrophy. The patient loses control over their body. Dollification surgeries become possible. The medication process is deemed completed.
Part V - Course of Surgeries
All the surgeries become possible after the patient reaches phase 5 of therapy.
Articuplasty involves cutting the patient’s body and shaping new joints out of kintsugine. The joints become integrated with the patient's body after two to three weeks of auxiliary tsichirone therapy after which the patient is to undergo physical rehabilitation. Articuplasty is to be performed on shoulder joints, elbows, wrists, finger joints, hips, knees and ankles. If the patient expresses such desire, articuplasty can also be performed on toe joints, neck and some regions of the torso. The patients are able to use their joints despite muscle atrophy.
Voice box transplantation is not necessary for transition, but if the patient wishes not to undergo it, it is advised they learn sign language. The surgery involves cutting a hole in the body region chosen by the patient, inserting an artificial voice box and sealing the hole using kintsugine. The seal gets healed after one to two weeks of auxiliary tsichirone therapy. Although the voice box can be transplanted to any part of the body that is big enough to store it, it is highly recommended to transplant it into the neck or the torso.
Some patients express a desire for their post-transition forms to possess winding keys. In such cases it is possible for them to undergo winding key transplantation. The transplantation consists of drilling a hole in the patient’s body, constructing a key rail out of kintsugine, inserting the key and sealing the rail. The key becomes integrated into the patient’s body after two to three weeks of auxiliary tsichirone therapy, during which it is absolutely necessary not to touch the key. Touching the key during the auxiliary therapy may result in damage which may render the key unusable or require repeating the surgery. Winding the key seems to have no effect on the patient's physical state. It is however understood to cause feelings of relaxation. Further research is required.
Some patients express a desire for their post-transition forms to possess movable eyelids. In such cases it is possible for them to undergo palpebraplasty. The surgery involves cutting the eyelid rails into the patient’s eye sockets and shaping the eyelids out of kintsugine. The eyelids become integrated with the patient’s body after four to eight days of auxiliary tsichirone therapy. To ensure proper shape of the eyelids they are to be shaped in the closed position.
Part VI - Reversibility
The effects of the therapy are currently understood to be irreversible once the patient’s body enters phase 4 of the transition process. Further research is required.
Part VII - Contraindications
The therapy is not to be administered to patients with calcium deficiency until the deficiency is treated.
To prevent damage to the organism the therapy is not to be administered to patients with brittle bone disease.
Patients with any health conditions causing muscle atrophy are to be thoroughly observed by their physician.
The physician has the right to alter or completely halt therapy if it poses danger to the patient’s life.
Part VIII - WTO Approval
The World Transhumanism Organisation approved the therapy on August 2nd 20XX.
*************
Sorry, but I like the otherkin HRT genre too much. And while it will feel weird to self-insert myself into such a story as a receiver (because it seems my disability prevents me from gender HRT IRL), I thought I could write some lore bits to contribute to the community. It might not even be the only report I decide to write.
Of course, feel free to base your own story on that report. I'd be excited to read it!
210 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
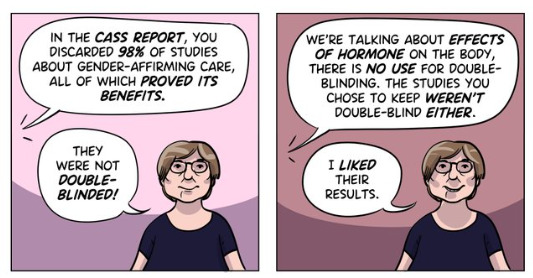
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
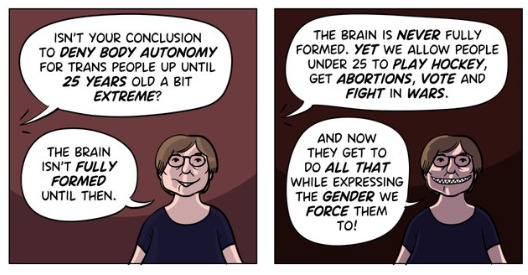
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
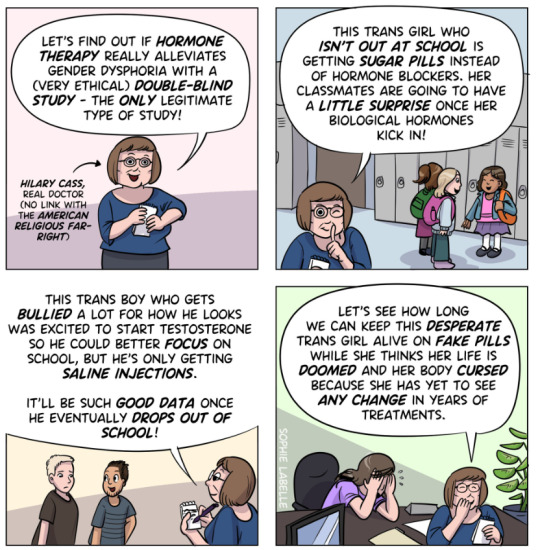
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

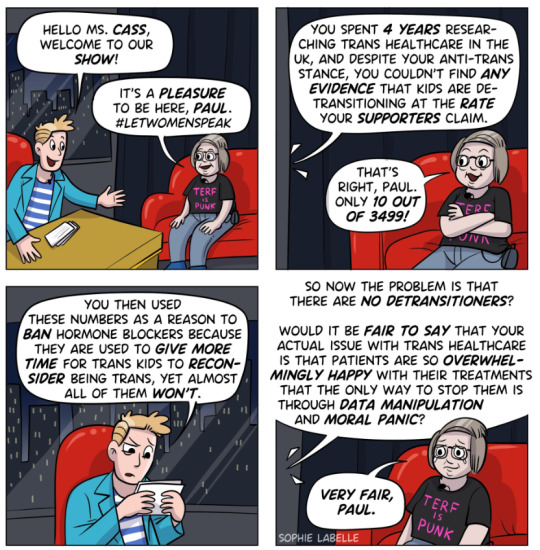
Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone. There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
387 notes
·
View notes
Note
I totally understand and can empathize with fat activists when it comes to medical fatphobia. But I do think its important to provide nuance to this topic.
A lot of doctors mention weight loss, particularly for elective surgeries, because it makes the recovery process easier (Particularly with keeping sutures in place) and anesthetic safer.
I feel like its still important to mention those things when advocating for fat folks. Safety is important.
What you're talking about is actually a different topic altogether - the previous ask was not about preparing for surgery, it was about dieting being the only treatment option for anon's chronic pain, which was exacerbating their ed symptoms. Diets have been proven over and over again to be unsustainable (and are the leading predictor of eating disorders). So yeah, I felt that it was an inappropriate prescription informed more by bias than actual data.
(And side note: This study on chronic pain and obesity concluded that weight change was not associated with changes of pain intensity.)
If you want to discuss the risk factor for surgery, sure, I think that's an important thing to know - however, most fat people already know this and are informed by their doctors and surgeons of what the risks are beforehand, so I'm not really concerned about people being uninformed about it.
I'm a fat liberation activist, and what I'm concerned about is bias. I'm concerned that there are so many BMI cutoffs in essential surgeries for fat patients, when weight loss is hardly feasible, that creates a barrier to care that disproportionately affects marginalized people with intersecting identities.
It's also important to know that we have very little data around the outcomes of surgery for fat folks that isn't bariatric weight loss surgery.
A new systematic review by researchers in Sydney, Australia, published in the journal Clinical Obesity, suggests that weight loss diets before elective surgery are ineffective in reducing postoperative complications.
CADTH Health Technology Review Body Mass Index as a Measure of Obesity and Cut-Off for Surgical Eligibility made a similar conclusion:
Most studies either found discrepancies between BMI and other measurements or concluded that there was insufficient evidence to support BMI cut-offs for surgical eligibility. The sources explicitly reporting ethical issues related to the use of BMI as a measure of obesity or cut-off for surgical eligibility described concerns around stigma, bias (particularly for racialized peoples), and the potential to create or exacerbate disparities in health care access.
Nicholas Giori MD, PhD Professor of Orthopedic Surgery at Stanford University, a respected leader in TKA and THA shared his thoughts in Elective Surgery in Adult Patients with Excess Weight: Can Preoperative Dietary Interventions Improve Surgical Outcomes? A Systematic Review:
“Obesity is not reversible for most patients. Outpatient weight reduction programs average only 8% body weight loss [1, 10, 29]. Eight percent of patients denied surgery for high BMI eventually reach the BMI cutoff and have total joint arthroplasty [28]. Without a reliable pathway for weight loss, we shouldn’t categorically withhold an operation that improves pain and function for patients in all BMI classes [3, 14, 16] to avoid a risk that is comparable to other risks we routinely accept.
It is not clear that weight reduction prior to surgery reduces risk. Most studies on this topic involve dramatic weight loss from bariatric surgery and have had mixed results [13, 19, 21, 22, 24, 27]. Moderate non-surgical weight loss has thus-far not been shown to affect risk [12]. Though hard BMI cutoffs are well-intended, currently-used BMI cutoffs nearly have the effect of arbitrarily rationing care without medical justification. This is because BMI does not strongly predict complications. It is troubling that the effects are actually not arbitrary, but disproportionately affect minorities, women and patients in low socioeconomic classes. I believe that the decision to proceed with surgery should be based on traditional shared-decision making between the patient and surgeon. Different patients and different surgeons have different tolerances to risk and reward. Giving patients and surgeons freedom to determine the balance that is right for them is, in my opinion, the right way to proceed.”
I agree with Dr. Giori on this. And I absolutely do not judge anyone who chooses to lose weight prior to a surgery. It's upsetting that it is the only option right now for things like safe anesthesia. Unfortunately, patients with a history of disordered eating (which is a significant percentage of fat people!) are left out of the conversation. There is certainly risk involved in either option and it sucks. I am always open to nuanced discussion, and the one thing I remain firm in is that weight loss is not the answer long-term. We should be looking for other solutions in treating fat patients and studying how to make surgery safer. A lot of this could be solved with more comprehensive training and new medical developments instead of continuously trying to make fat people less fat.
659 notes
·
View notes
Text
Fear-mongering and herbalism
Herbalism is a crucial element for many practitioners of witchcraft, and lately I've seen a lot of fear-mongering in the #baby-witch and #witchblr tags that it's raising some serious red flags. Caution is necessary, yes, but over-simplified warnings against herbs that have a very long history and tradition of safe and effective use can rob people of accessible, beneficial ways to take an active role in their own health and wellbeing.
True: People absolutely need to be cautious about what they are putting in their bodies. True: "Natural" does not equate to "good" or "healthy". True: You need to speak to a medical professional regarding medical issues.
All these things being true do not mean that you cannot find plants that are safe to ingest, and that can benefit your health and support you. You can use herbs safely and you do have the power and ability to find information about them.
I've literally seen posts that say not to ingest any kind of herb because "you don't know what's in them" and "you don't know dosage, so it might harm you".
This lack of nuance is precisely the type of thinking that breeds misinformation and unnecessary fear, as if there is not enough of that to go around! It seems like because MAGA and anti-vaxx folks have been using the line "do your own research!!" so much, people are associating research with... right wing conspiracy theory? Somehow? Don't forget that being capable of doing good research also means being capable of evaluating your sources, and thinking critically about what you're reading.
Here are some of the misconceptions I've come across in the last couple days:
Laypeople can't safely use herbs
Fear of toxicity in herbs is common and rational, but herbs that you can find in your kitchen are food-grade and widely available. You don't need to eat them in enormous quantities to experience their benefits.
For example, thyme can help support the lungs during cold and flu season. Ginger tea is great for minor digestive upsets. These are things you have access to and can provide a safe means of relief.
Local apothecaries are very knowledgeable about where they source their herbs and what dosages are safe. They are also able to tell you if their herbs are pesticide-free, organic, etc.
Where you want to be cautious is ordering herbs online, especially places like Amazon or Etsy where there is no control whatsoever. Even supplements have been found to frequently not contain what they are said to contain, and you really have to do research about the company you're buying from beforehand.
If you don't have a local apothecary, you can still buy herbs online! Just make sure you are using a reputable website such as Mountain Rose Herbs where you can get bulk herbs.
Lesser known herbs require more caution, but there are fantastic books about herbalism and they provide information on dosage and various ways the herbs can be used responsibly. Your local library is almost guaranteed to have several books about herbalism, and if you aren't sure about a particular herb, look it up in multiple other resources to see if their information matches up. You can even find information about many commonly used herbs on WebMD.
Also, don't forage herbs that you plan to ingest if you are not experienced. This is a recipe for disaster, and incredibly dangerous. I'm not going to go into super huge detail about this, because it would merit its own post, but seriously, just don't do it until you have experience. Plant identification apps are not sufficient to identify herbs you plan to ingest.
Herbal remedies cure major illnesses
Herbs can play a supportive role, but it's crucial to recognise their limits. Herbal medicine should complement, not replace, medical treatment for severe chronic conditions. Clinical herbalists are trained to assess what's appropriate for herb-based support and when a situation requires immediate medical attention.
Herbs are not a panacea that will cure every ailment. Every person is unique and any single herb can have wildly different effects on the body. Some people might find incredible relief, while another person may find no effect at all, or may even find an herb doesn't agree with them.
Herbalists think they are medical practitioners
Because there is no federally regulated body for herbalists, people sometimes think it's the wild west out there and anyone can do anything, but that's not the case. Herbalists are not exempt from the law, and no one is legally allowed to practice medicine if they are not licensed to do so. Period. No amount of traditional knowledge changes that.
While the herbalist profession is not regulated federally, there are regulating bodies that are run by herbalists and that set standards for what is expected and permitted. If you search for "herbalism guild Canada" you will find the Canadian Council of Herbalist Associations which has tons of information, and some provinces also have their own guilds. Most guilds will have a list of reputable herbalists that you can access and they have strict requirements for being added to those lists. You can find these requirements on their websites and gauge them for yourself.
Part of training to become a clinical herbalist is knowing you are not a medical practitioner. You are taught not to diagnose people, and how to recognise when something is outside of your scope of practice.
From the CCHA:
9. A registered herbal practitioner will offer interdisciplinary collaboration with other health professionals
Herbalists focus on holistic, complementary care, rather than taking on the role of medical practitioners. A qualified herbalist works alongside them to support the body's systems, rather than attempting to independently treat or diagnose medical systems. For example, they might work with clients to ease side-effects from medication, but they won't independently treat serious conditions like infections.
Herbalists are anti-vaxx and anti-science
The vast majority of clinical herbalists are not anti-vaxx or anti-modern medicine at all, and focus on combining traditional knowledge about plants with modern science. Are there herbalists out there who are anti-vaxx? Absolutely, just like any demographic you can find people who are spouting nonsense, but that is not the norm.
Thankfully, herbalism schools and herbalists are pretty up front with their beliefs. The CCHA has these requirements for herbalists in the guild:
3. Herbalists have an extensive knowledge base combining traditional wisdom and modern scientific perspective [...] 7. A registered herbal practitioner is trained in herbal safety, drug interactions, and possible contraindications [...] 10. A registered herbal practitioner is accountable to a professional organization, must maintain annual continuing education and must abide by professional standards
When I was looking for a clinical herbalist myself, I always checked their website information and whether they were registered with a guild, and what the requirements for that guild were. The herbalist I chose also had a clear section on her website where she stated that she had experience working with people on psychiatric medications.
You can also often find their stance on other things such as LGBTQIA+ issues (such as statements on their website regarding their approach to HRT).
The school I ultimately selected for my education was one that had explicit information about how they integrated new science into their curriculum, and how frequently it was updated.
If you are not finding the information you're looking for, just ask! It's completely acceptable and not rude to contact an herbalist and ask them what their approach is on the things you are concerned about. They will be happy to answer these questions and give you any information they can to help you decide if they are a good fit for you.
Conclusion
Herbalism is not about replacing medical care or promising miracle cures. It's about tapping into centuries-old knowledge and combining it with modern insights. Embrace herbs with curiosity, responsibility, and respect, and you can have an incredible and beneficial relationship with them.
I'm sure there are plenty of points here that I have omitted or not sufficiently covered. I hope readers will take this as an indictment of the author, me, rather than one against herbalism as a whole.
62 notes
·
View notes
Text
I've seen my new GP twice now, and omg I didn't realise how bad things were with my previous one until now. Like I knew it was bad, but having someone who actually listens and cares to contrast to makes the shitty treatment stand out so much more. Some of the highlights:
My memory isn't great, so my partner wrote out a full report of what had been happening with a list of symptoms and a timeline of the most recent events, as well as printed versions of whatever tests results we could get before we arrived. Id summerised it at the top because every doctor id been to never reads what i give them, even when its from other doctors, but he read all of it, and asked clarifying questions as he did to make sure we were on the same page.
He actually read what little bits of my medical history had access to (while I've never seen this doctor before, I attended this clinic as a child, which was when most of the stuff associated with my primary disability was happening, so he could see that) and agreed that there is almost certainly something chronic going on that he will gladly investigate once the immediate issue is dealt with.
The fact I was autistic came up at some point, and I explained that I'm not formally diagnosed. My current psychologist and one other has done all the testing they can and they were both very confident I am autistic, but we can't get the formal diagnosis without a review from a neuropsyc because of something in my history, and I don't have the money to do that. My autistic traits are in my medical files but they're incorrectly attributed to something else. He was incredibly understanding of that and told me not to stress about the diagnosis (unless i want to, in which case he said hed support me from his end if he can) and asked if I could get something from my psychologist to explain how this might effect my treatment (not noticing symptoms, not being able to articulate problems consistently etc) so he knows what additional support I might need in the clinic.
He admitted to not knowing things, and told me how he was going to go about fixing that gap in his knowledge before my next appointment. For example, He admitted to never having a trans patient before, but that he's going to do some research on his own time to learn what he needs to do to be a better Dr for me.
He asked me to get some scans from a previous hospital stay, and picked up that I was hesitant. mum was with me and explained my auditory processing issues and how it makes communicating via phone hard. he told me not to stress and said he can get the receptionist to do it with my concent.
A lot of these aren't big things, but they make the world of difference when you have a complex medical history and its so refreshing just to feel heard after all this
71 notes
·
View notes
Note
is there actual proof there's a genetic component to alcoholism? I've been searching and most articles I've read seem to agree it accounts for about half of your predisposition. I'm both skeptical and worried I might be going too far in my questioning to the point of denying science
genetic variants play a role in alcoholism. this is a decently readable overview on the topic from 2013. there are a few main points that should be clarified when discussing this.
often when people ask about this, they're thinking of genetic variants that affect a person's psychology, something like an inherited and inescapable 'addictive personality'. this is not really borne out by the research. as the paper above points out, the strongest genetic effects wrt the development of alcoholism are due to genes that change how we metabolise alcohol. having genes that make your alcohol metabolism more physically unpleasant in various ways (for example, you may have heard of so-called 'asian flushing syndrome') generally lowers the chances you will drink lots of alcohol, and thus lowers the chances you will qualify for a dx of alcohol use disorder. it's not a perfect protection; the paper also notes that, for example, businessmen exposed to cultural and economic pressures to drink heavily were more likely to do so even if they carried the normally protective genes. so, these aren't genes that control our behaviour directly or change our personalities; what we're seeing is largely the result of the fact that people like to do things that feel good, and if drinking makes you feel like hell, you are in general less likely to do it a lot.
this paper, and many papers on this topic, also mentions twin studies and adoptee studies to back up the claim that alcoholism is partially genetically determined. keep in mind that these studies are very hard to control for economic confounding factors, because even with adoptees, genetic siblings are also disproportionately likely to be adopted into families of a similar economic class. this is a general sticking point in a lot of genetics research.
many of the genetic variations believed to contribute to alcoholism are identified by studying families with multiple diagnosed alcoholics. this is tricky because it again has a lot of confounding factors; it identifies broad regions of the genome that then have to be broken down into more detailed analyses; and there are causation-correlation questions in this approach. some of the genes identified by these types of studies have replicated; many have not.
genomes and epigenetic variation are just extremely complicated. that doesn't mean the research isn't worthwhile, but understand that these types of questions turn up hundreds or thousands of potentially relevant genes, whose functions are often completely unknown, and which may be up- or down-regulated in ways no one understands. there are a lot of points of uncertainty between asking "do genes influence alcoholism" and generating an actual working list of such genes. i wrote a little about some of the uncertainties associated with epigenetic research here.
alcoholism itself is, like any psychiatric dx, heterogeneous (there are many different ways to qualify for the dx and the judgments inherently include a degree of clinician subjectivity). so, and this is a problem with studying the genetics of any psychiatric dx and many physical ailments as well, we're not really talking about a single clinical or psychological entity, and thus to even say which genetic variations may contribute to developing it is already pretty dubious in its discursive formulation alone.
137 notes
·
View notes
Text
On Saturday, an Associated Press investigation revealed that OpenAI's Whisper transcription tool creates fabricated text in medical and business settings despite warnings against such use. The AP interviewed more than 12 software engineers, developers, and researchers who found the model regularly invents text that speakers never said, a phenomenon often called a “confabulation” or “hallucination” in the AI field.
Upon its release in 2022, OpenAI claimed that Whisper approached “human level robustness” in audio transcription accuracy. However, a University of Michigan researcher told the AP that Whisper created false text in 80 percent of public meeting transcripts examined. Another developer, unnamed in the AP report, claimed to have found invented content in almost all of his 26,000 test transcriptions.
The fabrications pose particular risks in health care settings. Despite OpenAI’s warnings against using Whisper for “high-risk domains,” over 30,000 medical workers now use Whisper-based tools to transcribe patient visits, according to the AP report. The Mankato Clinic in Minnesota and Children’s Hospital Los Angeles are among 40 health systems using a Whisper-powered AI copilot service from medical tech company Nabla that is fine-tuned on medical terminology.
Nabla acknowledges that Whisper can confabulate, but it also reportedly erases original audio recordings “for data safety reasons.” This could cause additional issues, since doctors cannot verify accuracy against the source material. And deaf patients may be highly impacted by mistaken transcripts since they would have no way to know if medical transcript audio is accurate or not.
The potential problems with Whisper extend beyond health care. Researchers from Cornell University and the University of Virginia studied thousands of audio samples and found Whisper adding nonexistent violent content and racial commentary to neutral speech. They found that 1 percent of samples included “entire hallucinated phrases or sentences which did not exist in any form in the underlying audio” and that 38 percent of those included “explicit harms such as perpetuating violence, making up inaccurate associations, or implying false authority.”
In one case from the study cited by AP, when a speaker described “two other girls and one lady,” Whisper added fictional text specifying that they “were Black.” In another, the audio said, “He, the boy, was going to, I’m not sure exactly, take the umbrella.” Whisper transcribed it to, “He took a big piece of a cross, a teeny, small piece … I’m sure he didn’t have a terror knife so he killed a number of people.”
An OpenAI spokesperson told the AP that the company appreciates the researchers’ findings and that it actively studies how to reduce fabrications and incorporates feedback in updates to the model.
Why Whisper Confabulates
The key to Whisper’s unsuitability in high-risk domains comes from its propensity to sometimes confabulate, or plausibly make up, inaccurate outputs. The AP report says, "Researchers aren’t certain why Whisper and similar tools hallucinate," but that isn't true. We know exactly why Transformer-based AI models like Whisper behave this way.
Whisper is based on technology that is designed to predict the next most likely token (chunk of data) that should appear after a sequence of tokens provided by a user. In the case of ChatGPT, the input tokens come in the form of a text prompt. In the case of Whisper, the input is tokenized audio data.
The transcription output from Whisper is a prediction of what is most likely, not what is most accurate. Accuracy in Transformer-based outputs is typically proportional to the presence of relevant accurate data in the training dataset, but it is never guaranteed. If there is ever a case where there isn't enough contextual information in its neural network for Whisper to make an accurate prediction about how to transcribe a particular segment of audio, the model will fall back on what it “knows” about the relationships between sounds and words it has learned from its training data.
According to OpenAI in 2022, Whisper learned those statistical relationships from “680,000 hours of multilingual and multitask supervised data collected from the web.” But we now know a little more about the source. Given Whisper's well-known tendency to produce certain outputs like "thank you for watching," "like and subscribe," or "drop a comment in the section below" when provided silent or garbled inputs, it's likely that OpenAI trained Whisper on thousands of hours of captioned audio scraped from YouTube videos. (The researchers needed audio paired with existing captions to train the model.)
There's also a phenomenon called “overfitting” in AI models where information (in this case, text found in audio transcriptions) encountered more frequently in the training data is more likely to be reproduced in an output. In cases where Whisper encounters poor-quality audio in medical notes, the AI model will produce what its neural network predicts is the most likely output, even if it is incorrect. And the most likely output for any given YouTube video, since so many people say it, is “thanks for watching.”
In other cases, Whisper seems to draw on the context of the conversation to fill in what should come next, which can lead to problems because its training data could include racist commentary or inaccurate medical information. For example, if many examples of training data featured speakers saying the phrase “crimes by Black criminals,” when Whisper encounters a “crimes by [garbled audio] criminals” audio sample, it will be more likely to fill in the transcription with “Black."
In the original Whisper model card, OpenAI researchers wrote about this very phenomenon: "Because the models are trained in a weakly supervised manner using large-scale noisy data, the predictions may include texts that are not actually spoken in the audio input (i.e. hallucination). We hypothesize that this happens because, given their general knowledge of language, the models combine trying to predict the next word in audio with trying to transcribe the audio itself."
So in that sense, Whisper "knows" something about the content of what is being said and keeps track of the context of the conversation, which can lead to issues like the one where Whisper identified two women as being Black even though that information was not contained in the original audio. Theoretically, this erroneous scenario could be reduced by using a second AI model trained to pick out areas of confusing audio where the Whisper model is likely to confabulate and flag the transcript in that location, so a human could manually check those instances for accuracy later.
Clearly, OpenAI's advice not to use Whisper in high-risk domains, such as critical medical records, was a good one. But health care companies are constantly driven by a need to decrease costs by using seemingly "good enough" AI tools—as we've seen with Epic Systems using GPT-4 for medical records and UnitedHealth using a flawed AI model for insurance decisions. It's entirely possible that people are already suffering negative outcomes due to AI mistakes, and fixing them will likely involve some sort of regulation and certification of AI tools used in the medical field.
86 notes
·
View notes
Text
…here are twenty five more studies that further irrefutably prove vaccines are dangerous, useless, and are directly responsible for the autism epidemic:
A two-phase study evaluating the relationship between Thimerosal-containing vaccine administration and the risk for an autism spectrum disorder diagnosis in the United States A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population Commentary--Controversies surrounding mercury in vaccines: autism denial as impediment to universal immunisation Methodological issues and evidence of malfeasance in research purporting to show thimerosal in vaccines is safe Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002 Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature? A case series of children with apparent mercury toxic encephalopathies manifesting with clinical symptoms of regressive autistic disorders A comprehensive review of mercury provoked autism Thimerosal Exposure and the Role of Sulfation Chemistry and Thiol Availability in Autism B-Lymphocytes from a Population of Children with Autism Spectrum Disorder and Their Unaffected Siblings Exhibit Hypersensitivity to Thimerosal Theoretical aspects of autism: causes--a review Conjugate vaccines and autism Autism: a novel form of mercury poisoning A prospective study of thimerosal-containing Rho(D)-immune globulin administration as a risk factor for autistic disorders Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders The potential importance of steroids in the treatment of autistic spectrum disorders and other disorders involving mercury toxicity Reduced levels of mercury in first baby haircuts of autistic children Cultured lymphocytes from autistic children and non-autistic siblings up-regulate heat shock protein RNA in response to thimerosal challenge A possible central mechanism in autism spectrum disorders, part 1 The role of mercury in the pathogenesis of autism Transcriptomic analyses of neurotoxic effects in mouse brain after intermittent neonatal administration of thimerosal Causal relationship between vaccine induced immunity and autism Elevated levels of measles antibodies in children with autism Subtle DNA changes and the overuse of vaccines in autism What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature?
37 notes
·
View notes