#urethral problem
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Celebrities use Tumblr as well.
Text
Everything You Need to Know About Urethral Stricture and Its Treatment
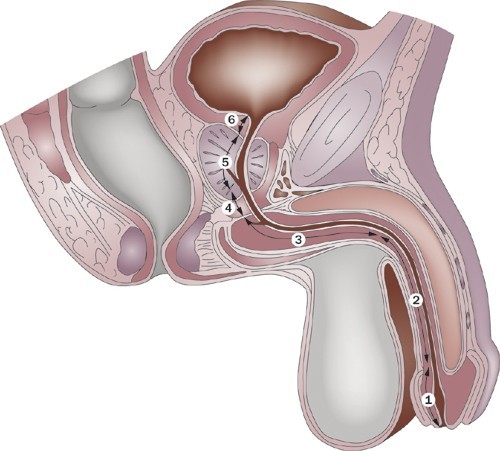
Urethral stricture is a urological condition that can severely impact a person's quality of life. It refers to the narrowing of the urethra—the tube that carries urine out of the body—due to injury, infection, or inflammation. If left untreated, it can lead to serious urinary problems and even kidney damage. Fortunately, effective and advanced urethral stricture treatment in Varanasi is available at Omkar Urology Hospital, under the expert care of Dr. Amit Kumar.
What is Urethral Stricture?
A urethral stricture occurs when scar tissue forms inside the urethra, restricting the normal flow of urine. This narrowing can be partial or complete and is more common in men than in women.
Common Causes:
Previous urinary tract infections
Injury or trauma to the pelvis or urethra
Catheter insertion or surgery
Sexually transmitted infections (STIs)
Inflammatory conditions
Symptoms of Urethral Stricture
Recognizing the symptoms early can help in timely diagnosis and treatment. Common symptoms include:
Decreased urine stream
Difficulty or pain during urination
Frequent urination
Incomplete bladder emptying
Urinary tract infections (UTIs)
Blood in urine (hematuria)
If you’re experiencing any of these signs, consult a urologist immediately for proper evaluation and treatment.
Diagnosis of Urethral Stricture
At Omkar Urology Hospital Varanasi, Dr. Amit Kumar follows a thorough diagnostic approach to accurately detect the presence and severity of a urethral stricture. This may include:
Physical Examination
Urine Flow Test (Uroflowmetry)
Ultrasound or MRI Imaging
Retrograde Urethrogram (RUG)
Cystoscopy – a direct visual examination using a scope
Urethral Stricture Treatment in Varanasi
Thanks to advancements in urology, several effective treatment options are available. The best treatment depends on the length, location, and severity of the stricture.
1. Urethral Dilation
A non-surgical procedure where the stricture is stretched using special dilators. It's often used for short, simple strictures.
2. Internal Urethrotomy (VIU)
A minimally invasive endoscopic procedure where the stricture is cut using a scope inserted through the urethra. It offers faster recovery but may require repeat procedures.
3. Urethroplasty
This is a surgical reconstruction of the urethra and offers a more permanent solution. Types include:
Excision and Primary Anastomosis (EPA): Best for short strictures.
Substitution Urethroplasty: Involves using grafts or flaps for longer or complex strictures.
4. Laser Treatment
At Omkar Urology Hospital, advanced laser technology is available for precise, less painful, and quicker recovery in suitable stricture cases.
Why Choose Omkar Urology Hospital for Urethral Stricture Treatment?
Expertise of Dr. Amit Kumar – Renowned urologist with years of experience in treating complex urethral conditions.
Advanced Diagnostic Tools – Ensures accurate assessment and personalized treatment.
Minimally Invasive Options – Faster recovery and less discomfort.
Patient-Centered Care – Compassionate approach and comprehensive post-treatment support.
Tips for Preventing Urethral Stricture
While not all cases can be prevented, you can lower your risk by:
Avoiding unnecessary catheterization
Treating infections promptly
Practicing safe sex
Avoiding trauma to the pelvic region
Conclusion
Urethral stricture is a manageable condition when diagnosed early and treated appropriately. If you're looking for expert urethral stricture treatment in Varanasi, trust Dr. Amit Kumar at Omkar Urology Hospital. With advanced facilities and patient-first care, we ensure you receive the best possible outcome.
Book Your Consultation Today
Visit [Omkar Urology Hospital Varanasi] or call now 09555042005 to schedule an appointment with Dr. Amit Kumar for a comprehensive urological evaluation.
#urethral stricture treatment Varanasi#best urologist in Varanasi#Dr. Amit Kumar urologist#Omkar Urology Hospital Varanasi#urethral stricture symptoms#laser treatment for urethral stricture#VIU procedure Varanasi#urethroplasty Varanasi#urinary problems treatment#male urology care Varanasi#advanced urology treatments
0 notes
Text
a story of one fake penis, 39 surgeries and counting.
This story I found through this post. don't click it unless you want to see frankendick. Frankly, the phalloplasty looks okay (only compared to most I've seen and I've seen too many. too... too many doing this work) besides the enormous scars and color mismatch. It's a low bar. But I was interested to see the user's progression.
That post, of surgery results the user admits took three years to achieve (""), is from two years ago. According to the user's more recent post history, it's been downhill from there.
11 months ago, the user's erectile implant began pushing through the skin, requiring surgery. Three months later, after the revision, the complication repeated. In this post from r/Everythingphallo 4 months ago, called "Is there anyone here who has had a phalloplasty reconstruction?"— the user states:
Initially, everything was perfect – it looked aesthetically pleasing, had great functionality, and the sensation was at 100%. However, over the past 3 years, I have had 15-20 surgeries due to complications and issues. The appearance is now completely deteriorated, and my functionality is greatly limited. The scars are contracting more and more, causing a loss of 4 cm in length, which wouldn't be so bad if it still looked good and functioned properly.
in the comments, the user clarifies a major reason for the many revision surgeries was problems with the constructed urethra. Multiple surgical revisions to the urethra caused stiffening, hardening, constricting scar tissue. A bacterial infection was additionally overlooked for "several years" which worsened the damage, and no doubt put the user at severe risk of bladder and kidney infection.
As indicated by the post's title, the user does not want to stop surgery, but instead wants to entirely reconstruct the phallus using the same technique, radial free flap phalloplasty, as performed the first time. This would mean she would have massive scars and limited mobility/strength in both of her arms and hands.
In this post from two months ago, things are somehow worse. (How..?!!)
user states:
Recently, I lost all sensation (previously 100%), can no longer experience orgasms, and suffered a 50% reduction in length due to a parasite that damaged the tissue. Furthermore, I am scheduled for an emergency surgery because my ED has once again resulted in the skin breaking, marking the 5th or 6th time in a year. In general this is my 39 surgery and I’m so tired.
Parasite?!? Which apparently doctors missed for OVER TWO YEARS?? Jesus Christ, if she was playing medical bingo she'd have won years ago. But of course, she's lost everything.
All that the first phalloplasty got her was 39 surgeries, urethral strictures, loss of all sexual sensation, bacterial infections, parasites, she still wants another one.
Don't you dare say this is life-saving surgery in any capacity. It is life-ending, mentally, physically, figuratively, literally.
451 notes
·
View notes
Text
Everything You Need to Know About Veggies and Fruits: Cranberries
Cranberry (Vaccinium Macrocarpon)
*Kitchen *Medical *Feminine

Folks Names: Bog fruit, Marshworts
Planet: Mars
Element: Water (juice), Fire (berry)
Deities: Astarte, Marjatta,
Abilities: Healing, Protection, Love, Lust, Positive Energy, Courage, Passion, Action
Characteristics: Native to Eastern North America and northern Asia. Small, slender, evergreen shrub growing to 1 ft with oval, dark green leaves, pink flowers and round/slightly pear-shaped red berries.
History: This jewel-toned gem of the bog is native to North America and a traditional food from Samhain through Yule. Its association with the American Thanksgiving meal is long rooted in tradition, but there is no historical evidence proving it was actually served at that first Thanksgiving celebrated by the Pilgrims. Despite this, cranberry something or other is commonly found on Thanksgiving and Christmas feast tables all across the United States, Canada, and the United Kingdom. Cranberry garlands made by stringing hundreds of the hard round red berries with a needle onto a long sturdy string is a traditional Christmas decoration. It is believed that cranberries got their name due to cranes always eating them and the blossoms of the berries look like the head of cranes. It is considered a sacred fruit in some indigenous circles such as Algonquian and Iroquois.
How to Grow:
Easy to Plant: Relatively
Rating: Moderate
Seeds accessible: Sometimes seasonal
How to Plant Cranberries
Video Guide
Where to Buy Seeds
Magical Properties
Can be used as a substitute for wine
Dried cranberries can be used in a charm to honor the wisdom of elders or as an offering to ancestors
It’s bright color signals energy, passion, courage, rejuvenation and rebirth
Can lend abundance, love and healing in kitchen spells
Since they are from the bog, it said to be feared by evil spirits and can offer protection
Placing a bowl of cranberries under one’s bed can restore depleted energy and cure an illness
Drinking the juice with your partner on a dark moon can keep your relationship free of trouble and continue to go strong
Can help link wisdom and guidance of ancestors
Can be utilized in energy cleansing rituals to remove negative energies from the aura
Is said to restore chakra alignment balance and create harmony
Burning bundles of cranberry stems can purify the energy of space and promote spiritual well-being during rituals and meditating
Medical Usage:
A classic remedy for urinary tract infections and can prevent and treat problems such as cystitis and urethritis
Can help to disinfect the urinary tubules and may be taken for problems associated with poor urinary flow such as enlarged prostate and blade infections
Can be used long term to prevent the development of urinary stones
Research in 1994 showed that cranberry juice helped really well with UTIs in women
Sources
#witch community#witchblr#witchcraft#paganblr#nature#witchcraft 101#plants and herbs#green witch#occulltism#cranberries#cranberry juice#cranberry sauce#kitchen witch#thanksgiving#fruits and vegetables#berries#baby witch
102 notes
·
View notes
Note
Hi Mrs Haitch! First let me say that I adore your stories and the way you write the men in your fics. Not only are they hot and enjoyable to read but also they feel real and adult. I don't want to bash on anyone by saying this, but sometimes it's difficult to enjoy fics written by younger people when you're pushing 30 because they portray a different reality. Please, never stop writing!
Before getting into the next part of the ask I'd like to say that this is in no way a demand and I it's not my intention to trauma dump on you. I just felt like talking a little about my experience could provide a bit of context.
I just read the ask about the soft spot and, although I'm not a virgin, I'm a serial victim of bad sex. I would love technical (even if explicit) descriptions on how to find the famed spot. I think is really cool when women in the medical field talk about sexual health, and it could be good having this kind of knowledge on a famous fic blog like yours, since I imagine a lot of fic readers are either virgins or had less than ideal sexual experiences, like me.
I don't want to seem like I'm pressuring you though! I totally understand if you prefer to keep this kind of thing out of your blog. It's just that a while ago I read on another blog from a healthcare professional a post about how sex shouldn't hurt even in the first time and I was blown away (this happened years after I started having sex and after having deemed myself "defective" and doomed to painful sex to the rest of my life)
Sorry for the long ask. Sending lots of hapiness your way <3
Well, if it helps even one person, it is absolutely my pleasure to do so.
I'm sorry for your bad sex. Nothing excuses it, frankly, and I'm a firm believer that most people are profoundly shit at giving vagina-owners orgasms.
(you calling my blog 'famous' does not go unnoticed and I could blush. Shhhh.)
I think age comes with so much beauty. I am a staunch believer in the unifying power of people, and when groups of women support the ducklings of the group, the ducklings are far less likely to be led down the garden path, on what is 'normal' or 'abnormal' or 'good' or 'bad' in sex.
This is why men and the media fear strongly-bonded groups of women so much-- it's almost like we'll talk and start to take note of the real problems. Cats amongst pigeons, right?
Anyway...
Cw and tw: medical discussion, discussion of self-examination
So again, while the location of the g-spot varies in exact location from vagina-owner to vagina-owner, on average it is located 2-3 inches into the vagina, on the anterior vaginal wall.
What I mean by anterior vaginal wall is, if standing and facing forwards, it's the wall of your vagina closest to the front of you, rather than your back.
Picture posted again, for reference!
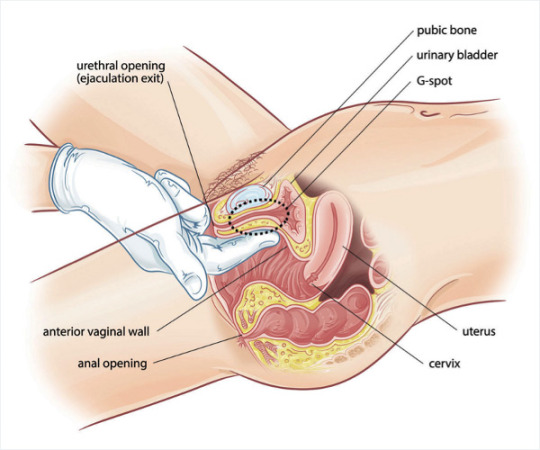
The g-spot is of variable size, usually the size of a large coin, and it may feel a bit rougher or ridged than other parts of your vagina, but becomes spongier or thicker and plusher when aroused or stimulated.
If you were to get two fingers on your dominant hand, reach inside the vagina up to the base of your fingers, and hook forwards, you should find it.
I suggest for the first time, finding it when you need to pee. This is because, the g-spot sits against the urethral canal (the tube you pee out of), and if you have a full bladder, you'll know you've found the g-spot because it will feel really sensitive and likely increase your urge to pee.
If you happen to orgasm with g-spot and clitoral stimulation while you have urine in your bladder, your chances of "squirting" (which, if you see my previous post, is almost certainly just pee) are much higher. It's a unique experience and you should try it. Put a towel down.
I find a good sized wand vibrator, inserted and positioned just-so, will give great continuous g-spot stimulation while you, or someone else, goes to town elsewhere.
Start combining all of the erogenous zones and it's party time.
As said previously, sensitivity is very variable. Exploring and knowing yourself is key to showing a partner how to pleasure you.
If you have sex with a partner who responds with anything other than "teach me" absolute enthusiasm, when you want to show them what works for you...if they 'try' for a short time, then give up? If they carry on doing their own thing anyway? If they're impatient?
Kick them to the curb. They can go fuck themselves.
Very much love as always,
-- Haitch xxx
39 notes
·
View notes
Note
Wow, hearing what you would do to a sub who ruined you makes me want to do that. Spend hours pleasuring you and then having you edge me and torture me in chastity for months. Sounds like a perfect plan
It does sound like a perfect plan. Problem is, there's no way I'd agree to it, because it's what you want.
Do you think you get to take something of mine and I'll just let you have your fun? No, we have to work out something far worse for you. Maybe include the cage but add a urethral rod to it. One that zaps or vibrates.
I think an excellent punishment for you in particular would be refusing to touch you at all and refusing to let you touch me. If you ruin me, you've proven that you're not trustworthy when it comes to my pleasure. So you don't get to grant me it anymore. I'll do it myself or get another, more well behaved pet to do it instead.
Tying you down while I bring myself to orgasm. Ignoring all your promises to do better until I decide your grovelling is enough for me. And that'll be a long time coming. I'm mean, after all.
It'd be interesting to see, if given the option, what you would would want more by the end of three months.
Permission to touch me again, or permission to touch yourself without the cage.
14 notes
·
View notes
Text
Mercy Upon Oneself
Relationship: The Last Knight/Ulpianus (Arknights)
Characters: The Last Knight (Arknights), Ulpianus (Arknights)
Tags:
#Masturbation #Seaborn Blood #Blood As Lube #unknown fluids #Tentacle Dick #Tentacle Sex #Rough Sex #Medically Unsafe Sex Even #throatfucking #Belly Bulge #Cock & Ball Torture #urethral insertion #Ear Canal Insertion #Biting #But not the way you'd expect! #Anal Sex #Choking #Bottom Ulpianus (Arknights) #I swear to Theresa and Rocinante that i do not remember what else is there worth tagging #Come Inside #Come Inflation #This isn't even a creampie its a milk bag #mentions of past Gladiia/Ulpianus as in she used to peg him
Words: 2,628
Summary:
Seaborn flesh is hard-coded to yearn for its own. So is human. The hybrids thereof have been aware of this problem since the beginning of the Abyssal Hunter program. Weeks into working with the Last Knight and five years since the last touch of a hunter, Ulpianus is losing his sanity to the point where the most outrageous methods start to sound enticing. He is not the only one. _____ Celebrate playable Ulpipi by reading of him getting tentacle railed.
May none of you be welcome but all of you bound by blood. And tentacles.
#arknights fanfic#ulpianus#the last knight#ulpianus arknights#the last knight arknights#ulpianus/the last knight#the last knight/ulpianus
16 notes
·
View notes
Text
Specific sex stuff that our Pascal blorbos are into
Previous: Pascal characters fave sex positions
Frankie - He wants to put a baby in you. So badly he's shaking. Just let him.
Joel - He will fuck you on an animal rug in front of a fireplace. He loves seeing the flames reflected on your naked skin, with fur underneath you. It awakens something feral in him.
Javi P - stockings. Rub him off with nylon-covered feet, and he will do absolutely anything and everything for/to you.
Pero - loves to put it in your ass.
Marcus P - wants to watch. Just you, or you with someone else. Will go crazy from seeing you pleasured, while he himself has to wait.
Dieter - craves urethral sounding. You don't only own his cock, he needs you to rule it and stick stuff into it.
Ezra - roleplay, especially you being a cute little fox or kitty with an ass plug tail.
Dave - dick cage during the day. Knowing the key is on a chain around your neck gets him hard, which is a problem. (This is why he kills people.)
Oberyn - he needs to eat off of you. Will serve himself, and eat, an entire meal on your body. Drizzling sweet sauces between your thighs, and licking it all up, is his favourite.
#frankie morales#joel miller#javier peña#pero tovar#dave york#marcus pike#dieter bravo#ezra#oberyn martell#my fic#headcanons#idk what this is
55 notes
·
View notes
Note
Hi! So I have a very lovely update!
Several [period of time because time isn't real] ago, I sent you a message asking about urethral pain (as a vulva-haver). And all these [time] later, I have *finally* discovered:
-being on testosterone can dehydrate you (and cause vaginal atrophy)
-eating gluten while having celiac disease can give you not only diarrhea but UTIs!
-trying to pee "after sex" (or any kind of penetration even if solo) WHEN YOU DON'T HAVE ENOUGH WATER IN YOUR BODY CAN HURT BECAUSE THERE'S NOTHING TO PEE OUT
So um, now that I'm not eating gluten and I'm drinking fluids at normal levels... I haven't had any issues with peeing afterwards. None. Nothing.
Urethral pain solved! If anyone else is having these problems (though I fully admit it might only be my dumb ass), make sure you're taking good care of yourself in *other* areas as well as your sexual health. Thank you, sex witch, for believing in me 💖🙏🏻
hey!!! this is so exciting! I love when people are not only able to find answers to their medical questions, but also come back and share! thank you so much for this, I hope it can be helpful to other people who might be experiencing something similar :)
also ps hey @ everyone: this is another one of the many reasons I advocate that people don't take "pee after sex" extremely literally! there's no need to sprint immediately to the toilet and force it, just go when the need naturally arises!
47 notes
·
View notes
Text
Dr. Smita Goel Homeopathy Clinic
www.thehomeopathyclinic.co.in
A urinary tract infection (UTI) is an infection in any part of the urinary system. Generally urinary system includes the kidneys, ureters, bladder and urethra. Most infections involve the lower urinary tract (bladder and urethra).
Comparison a man, a woman has at greater risk of developing a UTI. If an infection is limited to the bladder, it can be painful and annoying. But serious health problems can result if a UTI spreads to the kidneys.
Symptoms:
• A strong urge to urinate that doesn't go away
• A burning feeling when pee/ urinating
• Urinating often and passing small amounts of urine
• Urine that looks Cloudy, dark, bloody and strange-smelling pee
• Feeling tired or shaky
• Pelvic pain, in women — especially in the center of the pelvis and around the area of the pubic bone
• A frequent or intense urge to pee, even though little comes out when you do
• Pain in the penis or rectum (men)
• Mental confusion (mostly older people)
• Wetting the bed (children and older adults)
Types of urinary tract infections
Each type of UTI may result in more-specific symptoms. The symptoms depend on which part of the urinary tract is affected.
Kidney - Patient feel back or side pain, high fever, shaking & chills, nausea and vomiting;
Bladder - Pelvic pressure, Lower belly discomfort, Frequent, painful urination, Blood in Urine;
Urethra - Burning with urination, discharge.
Causes:
UTIs typically occur, due to bacterial infection in urinary system. It can spread to kidney. But the defenses sometimes fail. When that happens, bacteria may take hold and grow into a full-blown infection in the urinary tract.
Women tend to get them more often because their urethra is shorter and closer to the anus than in men. Because of this, women are more likely to get an infection after sexual activity or when using a diaphragm for birth control. Menopause also increases the risk for a UTI.
The most common UTIs occur mainly in women and affect the bladder and urethra.
• Infection of the bladder. This type of UTI is usually caused by Escherichia coli (E. coli). E. coli is a type of bacteria commonly found in the gastrointestinal (GI) tract. But sometimes other bacteria are the cause.
Having sex also may lead to a bladder infection, but you don't have to be sexually active to develop one. All women are at risk of bladder infections because of their anatomy. In women, the urethra is close to the anus. And the urethral opening is close to the bladder. This makes it easier for bacteria around the anus to enter the urethra and to travel to the bladder.
• Infection of the urethra. This type of UTI can happen when GI bacteria spread from the anus to the urethra. An infection of the urethra can also be caused by sexually transmitted infections. They include herpes, gonorrhea, chlamydia and mycoplasma. This can happen because women's urethras are close to the vagina.
Risk factors:
UTIs are common in women. Many women experience more than one UTI during their lifetimes.
Risk factors for UTIs that are specific to women include:
• Female anatomy. Women have a shorter urethra than men do. As a result, there's less distance for bacteria to travel to reach the bladder.
• Sexual activity. Being sexually active tends to lead to more UTIs. Having a new sexual partner also increases risk.
• Certain types of birth control. Using diaphragms for birth control may increase the risk of UTIs. Using spermicidal agents also can increase risk.
• Menopause. After menopause, a decline in circulating estrogen causes changes in the urinary tract. The changes can increase the risk of UTIs.
Other risk factors for UTIs include:
• Urinary tract problems. Babies born with problems with their urinary tracts may have trouble urinating. Urine can back up in the urethra, which can cause UTIs.
• Blockages in the urinary tract. Kidney stones or an enlarged prostate can trap urine in the bladder. As a result, risk of UTIs is higher.
• A suppressed immune system. Diabetes and other diseases can impair the immune system — the body's defense against germs. This can increase the risk of UTIs.
• Catheter use. People who can't urinate on their own often must use a tube, called a catheter, to urinate. Using a catheter increases the risk of UTIs. Catheters may be used by people who are in the hospital. They may also be used by people who have neurological problems that make it difficult to control urination or who are paralyzed.
• A recent urinary procedure. Urinary surgery or an exam of your urinary tract that involves medical instruments can both increase the risk of developing a UTI.
Complications:
When treated promptly and properly, lower urinary tract infections rarely lead to complications. But left untreated, UTIs can cause serious health problems.
Complications of a UTI may include:
• Repeated infections, which means you have two or more UTIs within six months or three or more within a year. Women are especially prone to having repeated infections.
• Permanent kidney damage from a kidney infection due to an untreated UTI.
• Delivering a low birth weight or premature infant when a UTI occurs during pregnancy.
• A narrowed urethra in men from having repeated infections of the urethra.
• Sepsis, a potentially life-threatening complication of an infection. This is a risk especially if the infection travels up the urinary tract to the kidneys.
Prevention:
With help of following little steps, we can prevent from UTIs:
• Drink plenty of liquids, especially water;
• Try cranberry juice;
• Wipe from front to back;
• Empty your bladder soon after having sex;
• Avoid potentially irritating feminine products;
• Change your birth control method;
Homoeopathic point of view of the disease:
Considering Hahnemann’s classification of disease, UTI can be a miasmatic disease too. Miasms are psora and sycosis. Homoeopathic medicines are personalized for the person suffering with UTI based on the individual totality of symptoms few are listed below. Homoeopathic remedies which can be prescribed after detailed case study.
Some Homoeopathic medicines (Cantharis, Nux vomica, Sarsaparilla, Aconitum napellus, Apis mellifica, Belladonna, Berberis vulgaris, Borax, Chimaphila umbellate, Lycopodium, Sepia, Staphysagria etc.) are very effective in UTIs. But that should be as per symptoms and guidance of qualified homeopathy doctor.
Conclusion:
Hence, Homeopathy is efficient in treating UTI with holistic approach and considering the patient as a whole with individualisation. UTI is not merely a local disease. In Homoeopathy we treat an individual but not just the disease which is the result of deranged vital force. Therefore, it should be treated as a constitutional problem.

#health and wellness#greater noida#ghaziabad#health & fitness#indirapuram#homeopathy#chronic illness#homeopath#mental illness#new york#homeopatia#healthy food#healthy eating#health insurance#health#good health#health tips#health products#healthy diet#healthcare#healthy relationships#healthy weight loss#healthylifestyle#healthyhabits#healthyliving#mental health#healthyskin#public health#health ( height and weight ) scales#hazaribagh
3 notes
·
View notes
Note
Do you think in MHA medical/surgical stuff around trans ppl has improved since 1) takes place in the future and 2)a shitton of quirks that require more thought and diversity? What do you think would change?
yah for sure
hrt is probably a lot easier. instead of constant routine injections or tablets, it's probably not a stretch of the imagination to say they could just.. alter your endocrine system to naturally produce the hormone levels you need to achieve your transition goal
surgery is also probably a hell of a lot more advanced - im sure surgical scars are optional, and keeping sensation is a guarantee
like, for ftm top surgery, if you get free nipple grafts then you're pretty much gonna lose sensation there. mine are fuckin numb as shit. not a problem in the futuristic bnha world - if you wanted, you could get extra nipple sensation, why not!
and with bottom surgery, fuck i bet they have it good - you wouldn't even need a full thickness skin graft for phalloplasty, they would just create that shit for you without you having to live life with huge scars like that - i bet it's no big deal to just graft a quirk-grown penis onto someone without all the potential complications that urethral connection and nerve grafting have currently
fuck it! if a trans woman wanted to have a womb and ovaries and the capability to have a baby, that's fully on the table! trans men with working testes and sperm and the ability to have bio kids without the debilitating dysphoria of pregnancy - please god i wish that was real
if someone out that had a chromosome swapping quirk they'd make a fuckin living helping trans people
also like some people in that world are animals so i really can't comprehend transphobia existing in bnha
25 notes
·
View notes
Text
Top Clinics for Pediatric Urology in Rajasthan: What Parents Need to Know

The health of children, especially the urinary and reproductive systems, requires special skill. Pediatric urology handles everything from urinary tract infections, bladder control, congenital conditions, and disorders of the genitalia in babies, children, and adolescents. Pediatric urology in Rajasthan has improved due to increased awareness and improved medical infrastructure providing high-quality, child-friendly care in some of the elite clinics across the nation.
Top clinics in pediatric Urology...
The health of newborn and children...
Pediatric Urology handles everything from Urinary tract infection, congenital anomalies (since birth) like Hypospadias, Posterior Urethral Valves, Hydronephrosis (swelling in kidney and urinary tract) VESICO-URETERIC REFLUX,
Incontinence of urine, Bladder Dysfunction, undescended Testis, Deformity of Penis/ Genitals, etc.
Compared to general Urology, Pediatric Urology Sub-speciality deals with New born babies to Adolescent boys and girls suffering from Kidneys and urinary tract problems.
They have exclusive and advanced training in Pediatric centres having Pediatric Urology armamentarium and ICU backed by Pediatric post operative care experts.
Dr. Aadil Farooq is among the early pioneers in Pediatric Urology in Rajasthan and North India.
He has perfect background of Pediatric Urology training from renowned institutes and mentors from India and abroad.
Understanding Pediatric Urology
Pediatric urology differs from general urology in that it focuses entirely on younger patients. It is a different process that requires medical skill, but also compassion, patience, and an understanding of child psychology. From a diagnosis of kidney abnormalities to repairing congenital problems such as hypospadias or undescended testis, pediatric urologists have an essential role in child health and well-being.
Why Choose Specialised Clinics in Rajasthan?
Rajasthan is becoming a preferred location for pediatric care, particularly in cities like Jaipur, Udaipur and Jodhpur. The increase in super-speciality hospitals and devoted children’s clinics has simplified the process for parents needing expert treatment. Many of these facilities have advanced diagnostics, minimally invasive surgical options, and experienced pediatric urologists who are trained to execute procedures involving delicate organs in young humans.
Leading clinics providing pediatric urology in Rajasthan not only provide the most up-to-date medical treatment but also family-oriented support systems. Thus, the child in care, as well as all guardians, are informed as to the process and feel comfortable and emotionally supported. Read more
#pediatric urology in Rajasthan#Pediatric Urology clinic in jaipur#endourology Surgeon in Jaipur#dynamic pediatric surgeon in jaipur#hypospadias diagnosed#puj obstruction treatment#Posterior Urethral Valves (PUV)#Dr. Aadil Farooq
2 notes
·
View notes
Text
Phallojourney Part 3
Hi everyone! I had my consult with the plastic surgeon, my urologist, and a licensed social worker yesterday. We went over some of the next steps, they took some measurements of my forearm, and talked about what I need to do to prepare.
One of the unfortunate things is that they’re going to have to use my left arm for the skin graft, which means I’ll be losing the tattoos on that arm. They’ll be internal so the phallus won’t be tattooed. They want me to do electrolysis and check back in 3 months to see if the skin is ready. I’ve heard that it’s not comfortable, but about on par with pinching or getting a tattoo.
Another step for me is losing weight. I don’t appear to be very overweight, but because I’m short my BMI is more heavily affected. I’m currently 214 lbs and will be aiming for around 190 lbs before the surgery. I don’t want to take weight loss drugs, so I’m going to be increasing my normal activity and working on eating out less. Depending on your BMI, this may be a requirement for surgery if you go through the same process. People with a higher BMI are more at risk for complications or problems healing, so someone surgeons have restrictions in place.
Another thing I’ll need to do is getting my letters for insurance. I’m currently seeing a psychiatrist, so I’ll be asking her for a letter. The social worker at my appointment will also set up an appointment with me and will write me a second letter. Some insurance companies are more strict about how many letters are needed, so definitely talk with your insurance to see what is required. The surgeon is also asking that I get established with a new therapist since I’m currently not seeing one.
They also gave me some information about what I can expect from the surgery and recovery. The actual procedure will take all day and then I’ll spend around 5-7 days in the hospital. I’m also being advised to take around a month off work, even though I work from home at a computer. If you’re in a more active job, you’ll likely need to take longer. I’ll have 2 catheters alongside drains, so they recommend having someone at home to help you with taking care of it.
Last for this update, we also discussed the additional features of the surgery. I decided that I did not want to do the scrotoplasty and I want the vaginectomy. This means that they will remove any vaginal tissue and sew it closed. They will not be creating a scrotum. I also made the decision that, in terms of appearance, I would prefer a circumcised look. I am also not pursuing an erectile implant, but I will be doing urethral lengthening to be able to urinate through the new phallus. All of these are options that you can choose to customize your new phallus, but are not required. Any additional surgery, such as creating the circumcised appearance, will take place a few months after the creation of the phallus after it has healed enough.
Thank you for joining me on this journey and I’ll see you all with the next update!
11 notes
·
View notes
Text
Neoplasms of Soft Tissue
Alright, you can break these down by what's fucked up. We'll look at all kinds of them, but we'll get to that in a bit. First, we gotta talk about CELLS and TUMORS in general. Malignant soft tissue tumors are only about 1% of soft tissue tumors. The rest are benign. They are mostly sporadic, but some are linked with gene mutations, radiation, burns, toxins, etc. Basically, cells start dividing abnormally. Cells get fucked up all the time. It's only when our body doesn't kill these cells that they become a problem. Okay, that's enough of that, onto the fun stuff.
Adipocytic
You got lipomas and liposarcomas. Lipomas are benign fat tumors, and are the most common soft tissue tumor in adults. They are well-encapsulated, mature adipocytes that are typically found under the skin of the limbs. On rare occasions, they can be intramuscular and poorly-circumscribed. However, most a soft, mobile, and painless, and can just be cut out by a PCP. Lipomatosis is a condition in which there are a whole lot of lipomas on a limb.
A liposarcoma is malignant. They are the most common sarcomas in adults and are found in the deep soft tissue of the extremities, as well as the retroperitoneum. They most commonly occur in old people. Symptoms include pain, swelling, fatigue, and decreased range of motion. There are three subtypes based on karyotype: well-differentiated, myxoid, and pleomorphic. Pleomorphic ones are aggressive and frequently metastasize.
Fibroblastic
You got nodular fasciitis, fibromatosis (superficial and deep), and fibrosarcoma. Nodular fasciitis is a self-limited proliferation of fibroblasts and myofibroblasts that is seen in young adults. It's mostly going to be found on the forearms, chest, or back. These nodules feel firm, fixed, and may be tender. They usually regress by themselves.
Superficial fibromatoses is a benign growth that is found on the palms, bottom of the feet, or penis. It is a firm, painless thickening made of plump spindle cells and dense collagen. If it is on the penis, it can cause urethral blockage. Recurrence is common, even if you cut these off.
Deep fibromatoses (Desmoid tumors) are large (like about 10 cm in diameter) and infiltrative. They don't metastasize, but they are prone to recurring. They can be painful. They're going to be rubbery and fixed.
Fibrosarcoma are rare, malignant tumors of fibroblasts. They are typically found in the deep soft tissue of the legs and trunk, and are painful, fixed, and soft. A common first sign is unexplained weight loss. On histology, they have a characteristic herringbone pattern and variable collagen. The 5 year survival is ~41%.
Skeletal Muscle
We're talking about rhabdomyosarcoma. These are rare, malignant tumors of mesenchymal origin that differentiate to skeletal muscle. Typically seen in childhood, and present as a quickly growing, painful mass, as well as unexplained weight loss. A pleomorphic subtype is seen in adults. Rhabdomyosarcomas are aggressive, and require excision plus chemotherapy, and maybe radiation therapy. The fatality is based on the subtype, with alveolar types having a 4-year survival of 65% and pleomorphic being fatal.
Unknown
We're only gonna discuss synovial sarcoma and undifferentiated pleomorphic sarcoma. Synovial sarcoma is typically found in the deep soft tissues next to large joints (like the fucking knee). Sometimes, it throws us for a loop and says fuck it lets grow where there's no synovium. Fuck that. Be what you're told to be. Anyway, these mostly they appear in 20-40 year olds, and present with deep-seated pain, numbness, limited motion, and swelling. They are firm and fixed. The swelling and inflammation can be present for several years :D They can metastasize, typically to the lung and lymph nodes.
Undifferentiated pleomorphic sarcoma is a malignant, high-grade tumor of mesenchymal origin. The cells cannot be classified into a category. They typically appear in the deep soft tissues of the extremities of middle-aged adults. If they get big, they can cause numbness or pain. They can grow up to 20 cm, are gray-white fleshy masses, and commonly hemorrhage. Prognosis is poor.
3 notes
·
View notes
Note
For the OC ask game, I wanted to use 6, 12, and 17 to ask about Damian! :D
6. do they see themself as experienced?
i think so! he looks like the type of person to have a phase in early adulthood where sex is his solution to most problems in his life lawl. now he does it like its a competitive sport /j
12. favourite sexual acts (giving and receiving)
giving: he likes fucking someone! a lot!
receiving: hmhmhm receiving blowjobs maybe? he has a terrible gag reflex so (but is not opposed to it if someone hot forces him to suck them off instead)
17. sex toy preferences?
vibrating cock ring or just normal cock ring. also sex toys involving urethral sounding
4 notes
·
View notes
Text
What is Urethral Stricture? Causes, Symptoms, Treatment & Prevention Explained
What is Urethral Stricture? Urethral stricture is a disease characterized by the narrowing of the urethra — the tube that carries urine from the bladder to the outside of the body. This narrowing is usually caused by scarring due to inflammation, infection, injury, or previous surgical methods.
Common Causes of Urethral Stricture: Several factors can lead to the development of a urethral stricture:
Trauma or Injury: Accidents causing injury to the pelvic area or perineum can result in scar tissue formation. Medical Procedures: Insertion of instruments into the urethra during surgeries or catheterization can cause damage leading to strictures. Infections: Sexually transmitted infections (STIs) like gonorrhea or chlamydia can cause inflammation and scarring. Radiation Therapy: Treatment for prostate cancer can lead to tissue damage and subsequent stricture formation. Congenital Conditions: Some people are born with abnormalities that predispose them to strictures. Symptoms of Urethral Stricture: Decreased urine flow or a weak stream Difficulty starting urination Frequent urge to urinate Pain or burning sensation during urination Dribbling of urine after urination Blood in urine (hematuria) Recurrent urinary tract infections (UTIs) Incomplete bladder emptying If you’re experiencing these symptoms, early consultation and diagnosis are essential. Left untreated, urethral stricture can lead to bladder damage, kidney problems, and serious infections.
When to Consult a Doctor? It’s important to seek medical attention if you experience:
Persistent Urinary Difficulties: Persistent problems with urination should not be ignored. Recurrent UTIs: Multiple infections may indicate an underlying stricture. Inability to Urinate: A complete blockage needs prompt medical intervention. Earlier diagnosis and treatment can prevent complications such as kidney damage or bladder infections.
Diagnosis of Urethral Stricture at Leela Superspeciality Hospital, Wakad: At Leela Superspeciality Hospital, patients benefit from state-of-the-art diagnostic technologies that help accurately detect the location, length, and severity of the stricture. Dr. Akhil S Mane follows a thorough diagnostic method, which includes:
Physical Examination: A complete urological examination is conducted to evaluate symptoms and rule out other conditions. Urine Flow Test (Uroflowmetry): This non-invasive test measures the strength and rate of urine flow. A decreased flow may indicate a stricture. Post-Void Residual Volume: This test determines how much urine remains in the bladder after urination using ultrasound. Retrograde Urethrogram (RUG): An imaging study where a contrast dye is injected into the urethra and X-rays are taken to identify the stricture’s exact location and length. Cystoscopy: A thin tube with a camera is inserted into the urethra to visually examine the affected area. With these diagnostic tools, Dr. Mane accurately assesses the stricture and customizes a treatment plan suited to each patient’s condition.
Urethral Stricture Treatment Options by Dr. Akhil S Mane: Treatment for urethral stricture depends on the location, severity, and length of the stricture, as well as the patient’s overall health and medical history. Dr. Akhil S Mane provides the most advanced, minimally invasive, and effective options for urethral stricture treatment in Pune.
Urethral Dilation: A simple technique where the narrowed segment is gradually widened using dilators. Suitable for short and mild strictures. May require being repeated if stricture recurs. Internal Urethrotomy (VIU – Visual Internal Urethrotomy): A minimally invasive endoscopic technique. The stricture is incised using a special endoscopic knife or laser under direct vision. Short recovery time with minimal discomfort. Ideal for short strictures (less than 1.5-2 cm). Urethroplasty (Open Surgical Repair): A highly effective permanent solution for longer or recurrent strictures. Types include anastomotic urethroplasty and substitution urethroplasty using grafts (e.g., buccal mucosa from the cheek). Offers excellent long-term success with low recurrence rates. Requires expertise and surgical precision, which Dr. Akhil S Mane is highly skilled at. Catheterization and Suprapubic Catheter Placement: In cases of complete blockage or emergency urinary retention, temporary catheterization may be needed. Mane ensures the safest catheter placement to prevent complications. Laser Treatment for Urethral Stricture: An advanced, bloodless, and precise treatment option. Involves laser incision of the stricture with minimal tissue injury. Faster healing and fewer complications. Benefits of Advanced Urethral Stricture Treatment: Relieves urinary symptoms and improves urine flow. Minimally invasive options for faster recovery. Lowers risk of recurrent infections and complications. Permanent solutions are available for long-term relief. Improves quality of life by reducing discomfort and urinary problems. Get the best urethral stricture treatment in Wakad, PCMC, Pune with expert care at Leela Superspeciality Hospital.
How to Prevent Urethral Stricture? While not all strictures can be prevented, certain measures can lower the risk:
Safe Sexual Practices: Using protection to prevent STIs. Prompt Treatment of Infections: Managing urinary infections early to prevent complications. Cautious Use of Catheters: Ensuring proper technique and hygiene during catheterization. Avoiding Urethral Trauma: Being cautious during activities that may cause pelvic injuries. Regular medical check-ups can also help in the early detection and management of potential problems.
Why Choose Leela Superspeciality Hospital for Urethral Stricture Treatment in PCMC, Pune? Leela Superspeciality Hospital stands out for several reasons:
The expertise of Dr. Akhil S Mane: With over 12 years of experience, Dr. Mane is recognized as one of the best urologists in Pune. Advanced Technology: The hospital is equipped with state-of-the-art facilities for diagnosis and treatment. Patient-Centric Approach: Emphasis on ethical practices and personalized care. Comprehensive Services: From diagnosis to post-operative care, all services are available under one roof. Patients can expect high-quality care and successful results at Leela Superspeciality Hospital.
1 note
·
View note
Note
The ask that said they saw a post where someone tagged some images as "he's so urethral" made me curious as to what it was. I searched on tumblr and there's more than one. Is it a meme? Are they serious? Some seem to be serious like they think it's the actual word to use. I'm so confused...
--
I'm sure it's a common autocorrect problem, among other things.
13 notes
·
View notes