#undergoes radical physical reconstruction
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text
Found: first actively forming galaxy as lightweight as young Milky Way
For the first time, the NASA/ESA/CSA James Webb Space Telescope has detected and ‘weighed’ a galaxy that not only existed around 600 million years after the Big Bang, but also has a mass that is similar to what our Milky Way galaxy’s mass might have been at the same stage of development. Other galaxies Webb has detected at this period in the history of the Universe are significantly more massive. Nicknamed the Firefly Sparkle, this galaxy is gleaming with star clusters — 10 in all — each of which researchers examined in great detail.
“I didn’t think it would be possible to resolve a galaxy that existed so early in the Universe into so many distinct components, let alone find that its mass is similar to our own galaxy’s when it was in the process of forming,” said Lamiya Mowla, co-lead author of the paper and an assistant professor at Wellesley College in Massachusetts. “There is so much going on inside this tiny galaxy, including so many different phases of star formation.”
Webb was able to image the galaxy in sufficient detail for two reasons. One is a benefit of the cosmos: a massive foreground galaxy cluster radically enhanced the distant galaxy’s appearance through a natural effect known as gravitational lensing. And when combined with the telescope’s specialisation in high-resolution imaging of infrared light, Webb delivered unprecedented new data about the galaxy’s contents.
“Without the benefit of this gravitational lens, we would not be able to resolve this galaxy,” said Kartheik Iyer, co-lead author and NASA Hubble Fellow at Columbia University in New York. “We knew to expect it based on current physics, but it’s surprising that we actually saw it.”
Mowla, who spotted the galaxy in Webb’s image, was drawn to its gleaming star clusters, because objects that sparkle typically indicate they are extremely clumpy and complicated. Since the galaxy looks like a ‘sparkle’ or swarm of fireflies on a warm summer night, they named it the Firefly Sparkle galaxy.
Reconstructing the galaxy’s appearance
The research team modelled what the galaxy might have looked like if its image weren’t stretched by gravitational lensing and discovered that it resembled an elongated raindrop. Suspended within it are two star clusters toward the top and eight toward the bottom. “Our reconstruction shows that clumps of actively forming stars are surrounded by diffuse light from other unresolved stars,” said Iyer. “This galaxy is literally in the process of assembling.”
Webb’s data show the Firefly Sparkle galaxy is on the smaller side, falling into the category of a low-mass galaxy. Billions of years will pass before it builds its full heft and a distinct shape. “Most of the other galaxies Webb has shown us aren’t magnified or stretched, and we are not able to see their ‘building blocks’ separately. With Firefly Sparkle, we are witnessing a galaxy being assembled brick by brick,” Mowla said.
Stretched out and shining, ready for close analysis
Since the image of the galaxy is warped into a long arc, the researchers easily picked out 10 distinct star clusters, which are emitting the bulk of the galaxy’s light. They are represented here in shades of pink, purple, and blue. Those colours in Webb’s images and its supporting spectra confirmed that star formation didn’t happen all at once in this galaxy, but was staggered in time.
“This galaxy has a diverse population of star clusters, and it is remarkable that we can see them separately at such an early age of the Universe,” said Chris Willott of the National Research Council Canada, a co-author and the observation programme’s principal investigator. “Each clump of stars is undergoing a different phase of formation or evolution.”
The galaxy’s projected shape shows that its stars haven’t settled into a central bulge or a thin, flattened disc, another piece of evidence that the galaxy is still forming.
‘Glowing’ companions
Researchers can’t predict how this disorganised galaxy will build up and take shape over billions of years, but there are two galaxies that the team confirmed are ‘hanging out’ within a tight perimeter and may influence how it builds mass over billions of years.
Firefly Sparkle is only 6500 light-years away from its first companion, and its second companion is separated by 42 000 light-years. For context, the fully formed Milky Way is about 100 000 light-years across — all three would fit inside it. Not only are its companions very close, the researchers also think that they are orbiting one another.
Each time one galaxy passes another, gas condenses and cools, allowing new stars to form in clumps, adding to the galaxies’ masses. “It has long been predicted that galaxies in the early Universe form through successive interactions and mergers with other tinier galaxies,” said Yoshihisa Asada, a co-author and doctoral student at Kyoto University in Japan. “We might be witnessing this process in action.”
“This is just the first of many such galaxies JWST will discover, as we are only starting to use these cosmic microscopes”, added team member Maruša Bradač of the University of Ljubljana in Slovenia. “Just like microscopes let us see pollen grains from plants, the incredible resolution of Webb and the magnifying power of gravitational lensing let us see the small pieces inside galaxies. Our team is now analysing all early galaxies, and the results are all pointing in the same direction: we have yet to learn much more about how those early galaxies formed.”
The team’s research relied on data from Webb’s CAnadian NIRISS Unbiased Cluster Survey, which include near-infrared images from NIRCam (Near-InfraRed Camera) and spectra from the microshutter array aboard NIRSpec (Near-Infrared Spectrograph). The CANUCS data intentionally covered a field that NASA’s Hubble Space Telescope imaged as part of its Cluster Lensing And Supernova survey with Hubble programme.
This work was published on 12 December 2024 in the journal Nature.
More information
Webb is the largest, most powerful telescope ever launched into space. Under an international collaboration agreement, ESA provided the telescope’s launch service, using the Ariane 5 launch vehicle. Working with partners, ESA was responsible for the development and qualification of Ariane 5 adaptations for the Webb mission and for the procurement of the launch service by Arianespace. ESA also provided the workhorse spectrograph NIRSpec and 50% of the mid-infrared instrument MIRI, which was designed and built by a consortium of nationally funded European Institutes (The MIRI European Consortium) in partnership with JPL and the University of Arizona.
Webb is an international partnership between NASA, ESA and the Canadian Space Agency (CSA).
Image Credit: NASA, ESA, CSA, STScI, C. Willott (NRC-Canada), L. Mowla (Wellesley College), K. Iyer (Columbia)
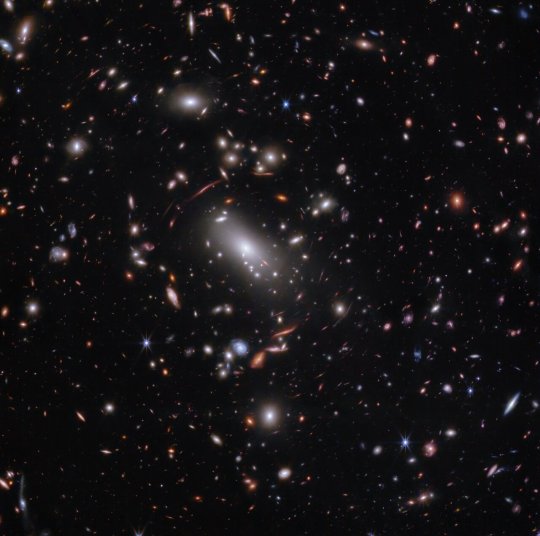
TOP IMAGE: Thousands of glimmering galaxies are bound together by their own gravity, making up a massive cluster formally classified as MACS J1423.
The largest bright white oval is a supergiant elliptical galaxy that is the dominant member of this galaxy cluster. The galaxy cluster acts like a lens, magnifying and distorting the light from objects that lie well behind it, an effect known as gravitational lensing that has big research benefits. Astronomers can study lensed galaxies in detail, like the Firefly Sparkle galaxy.
This 2023 image is from the James Webb Space Telescope’s NIRCam (Near-InfraRed Camera). Researchers used Webb to survey the same field that the Hubble Space Telescope imaged in 2010. Thanks to its specialisation in high-resolution near-infrared imagery, Webb was able to show researchers many more galaxies in far more detail.
[Image description: Thousands of overlapping objects at various distances are spread across this field, including galaxies in a massive galaxy cluster, and distorted background galaxies behind the galaxy cluster. The background of space is black.]Credit:
NASA, ESA, CSA, STScI, C. Willott (NRC-Canada), L. Mowla (Wellesley College), K. Iyer (Columbia)
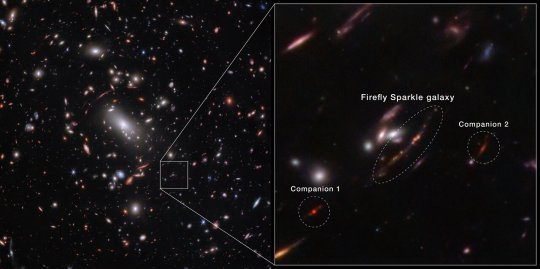
CENTRE IMAGE: For the first time, astronomers have identified a still-forming galaxy that weighs about the same as our Milky Way if we could wind back the clock to see our galaxy as it developed. The newly identified galaxy, the Firefly Sparkle, is in the process of assembling and forming stars, and existed about 600 million years after the Big Bang.
The image of the galaxy is stretched and warped by a natural effect known as gravitational lensing, which allowed researchers to glean far more information about its contents. (In some areas of Webb’s image, the galaxy is magnified over 40 times.)
While it took shape, the galaxy gleamed with star clusters in a range of infrared colours, which are scientifically meaningful. They indicate that the stars formed at different periods, not all at once.
Since the galaxy image is stretched into a long line in Webb’s observations, researchers were able to identify 10 distinct star clusters and study them individually, along with the cocoon of diffuse light from the additional, unresolved stars surrounding them. That’s not always possible for distant galaxies that aren’t lensed. Instead, in many cases researchers can only draw conclusions that apply to an entire galaxy. “Most of the other galaxies Webb has shown us aren’t magnified or stretched and we are not able to see the ‘building blocks’ separately. With Firefly Sparkle, we are witnessing a galaxy being assembled brick by brick,” explains astronomer Lamiya Mowla.
There are two companion galaxies ‘hovering’ close by, which may ultimately affect how this galaxy forms and builds mass over billions of years. Firefly Sparkle is only about 6500 light-years away from its first companion, and 42 000 light-years from its second companion. Let’s compare these figures to objects that are closer to home: the Sun is about 26 000 light-years from the centre of our Milky Way galaxy, and the Milky Way is about 100 000 light-years across. Not only are Firefly Sparkle’s companions very close, the researchers also suspect that they are orbiting one another.
[Image description: Horizontal split down the middle. At left, thousands of overlapping objects at various distances are spread across this galaxy cluster. A box at bottom right is enlarged on the right half. A central oval identifies the Firefly Sparkle galaxy, a line with 10 dots in various colours.]Credit:
NASA, ESA, CSA, STScI, C. Willott (NRC-Canada), L. Mowla (Wellesley College), K. Iyer (Columbia)
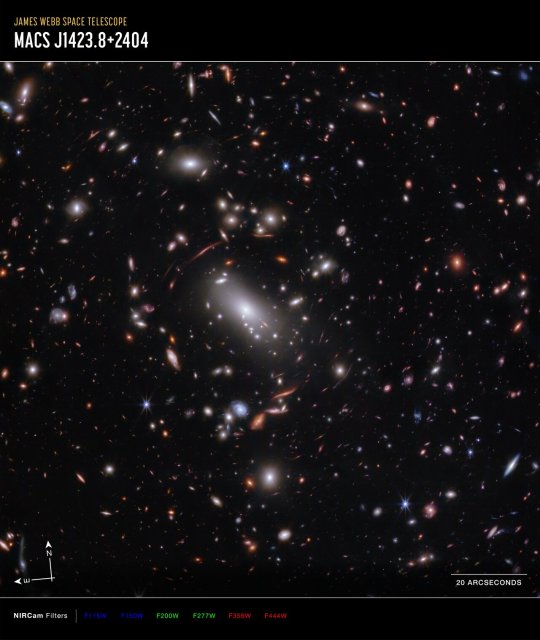
LOWER IMAGE: Thousands of glimmering galaxies are bound together by their own gravity, making up a massive cluster formally classified as MACS J1423.
The largest bright white oval is a supergiant elliptical galaxy that is the dominant member of this galaxy cluster. The galaxy cluster acts like a lens, magnifying and distorting the light from objects that lie well behind it, an effect known as gravitational lensing that has big research benefits. Astronomers can study lensed galaxies in detail, like the Firefly Sparkle galaxy.
This 2023 image is from the James Webb Space Telescope’s NIRCam (Near-Infrared Camera). Researchers used Webb to survey the same field the Hubble Space Telescope imaged in 2010. Thanks to its specialisation in high-resolution near-infrared imagery, Webb was able to show researchers many more galaxies in far more detail.
The north and east compass arrows show the orientation of the image on the sky.
The scale bar is labelled in arcseconds, which is a measure of angular distance on the sky. One arcsecond is equal to an angular measurement of 1/3600 of one degree. There are 60 arcminutes in a degree and 60 arcseconds in an arcminute. (The full Moon has an angular diameter of about 30 arcminutes.) The actual size of an object that covers one arcsecond on the sky depends on its distance from the telescope.
This image shows invisible near-infrared wavelengths of light that have been translated into visible-light colours. The colour key shows which NIRCam filters were used when collecting the light. The colour of each filter name is the visible light colour used to represent the infrared light that passes through that filter.
NIRCam filters from left to right: F115W and F150W are blue; F200W and F277W are green; F356W and F444W are red.
[Image description: A graphic labelled “James Webb Space Telescope; MACS J1423.8+2404.” A rectangular image shows thousands of galaxies of various shapes and colours on the black background of space.]Credit:
NASA, ESA, CSA, STScI, C. Willott (NRC-Canada), L. Mowla (Wellesley College), K. Iyer (Columbia)
youtube
9 notes
·
View notes
Text
Comprehensive Breast Cancer Surgery in Pune: A Guide to Treatment and Care
Breast cancer is a significant health concern affecting women worldwide, including those in Pune. However, with advancements in medical technology and specialized healthcare facilities, individuals diagnosed with breast cancer in Pune have access to comprehensive treatment options, including breast cancer surgery. This guide aims to provide valuable information about breast cancer surgery in Pune, covering key aspects such as surgical procedures, treatment approaches, and post-operative care.
Understanding Breast Cancer Surgery: Breast cancer surgery involves the surgical removal of cancerous tissue from the breast, with the primary goal of removing the tumor and reducing the risk of cancer spread or recurrence. The type of breast cancer surgery recommended depends on factors such as the stage of cancer, tumor size, location, and individual patient factors.
Types of Breast Cancer Surgery: In Pune, individuals diagnosed with breast cancer may undergo various types of surgical procedures, including:
Lumpectomy: Also known as breast-conserving surgery, lumpectomy involves the removal of the cancerous lump (tumor) along with a surrounding margin of healthy tissue. This procedure aims to preserve as much of the breast as possible while ensuring complete tumor removal.
Mastectomy: Mastectomy involves the surgical removal of the entire breast affected by cancer. Depending on the extent of cancer spread and individual preferences, mastectomy may be performed as a total mastectomy (removal of the entire breast), modified radical mastectomy (removal of the breast tissue along with lymph nodes), or radical mastectomy (removal of the breast tissue, lymph nodes, and chest muscles).
Sentinel Lymph Node Biopsy: During breast cancer surgery, sentinel lymph node biopsy may be performed to assess the spread of cancer to nearby lymph nodes. This procedure involves the removal and examination of one or a few sentinel lymph nodes to determine if cancer has spread beyond the breast.
Surgical Oncology Centers in Pune: Pune is home to several renowned surgical oncology centers and hospitals specializing in breast cancer treatment. These centers are equipped with state-of-the-art surgical facilities, experienced surgical oncologists, multidisciplinary teams, and support staff dedicated to providing comprehensive care to individuals diagnosed with breast cancer.
Multidisciplinary Approach to Treatment: Breast cancer treatment in Pune follows a multidisciplinary approach, involving collaboration between surgical oncologists, medical oncologists, radiation oncologists, pathologists, radiologists, nurses, and support staff. This collaborative approach ensures personalized treatment plans tailored to individual patient needs, preferences, and cancer characteristics.
Reconstruction Options: Following breast cancer surgery, individuals may choose to undergo breast reconstruction to restore the appearance of the breast and improve body image. Breast reconstruction options may include implant-based reconstruction, autologous tissue reconstruction (using tissue from other parts of the body), or a combination of both techniques.
Post-operative Care and Recovery: After breast cancer surgery, individuals require comprehensive post-operative care and support to promote healing, minimize complications, and facilitate recovery. This may include pain management, wound care, physical therapy, emotional support, and guidance on resuming daily activities and lifestyle modifications.
Support Services and Survivorship Programs: Dealing with a breast cancer diagnosis and undergoing surgery can be emotionally and psychologically challenging. Many healthcare facilities in Pune offer support services, survivorship programs, counseling, support groups, and educational resources to help individuals cope with their diagnosis, treatment, and recovery journey.
Conclusion: Breast cancer surgery in Pune offers individuals diagnosed with breast cancer access to advanced surgical techniques, specialized care, and comprehensive support services. By seeking timely medical attention, accessing specialized treatment options, and embracing a multidisciplinary approach to care, individuals can navigate their breast cancer journey with confidence and resilience, ultimately achieving optimal outcomes and quality of life.
0 notes
Text
Dr. R K Saggu: Your Oncoplastic Breast Surgeon in Delhi

When facing breast cancer surgery, the role of an oncoplastic surgeon becomes paramount for several reasons. The demand for an oncoplastic breast surgeon in Delhi has surged due to the need for a comprehensive approach that combines cancer treatment with cosmetic enhancements. Patients undergoing breast cancer surgery often experience emotional distress and concerns about body image post-surgery. An oncoplastic surgeon addresses these emotional aspects by not only focusing on cancer removal but also ensuring optimal cosmetic outcomes. This integrated approach not only aids in cancer treatment but also contributes significantly to the emotional well-being and quality of life of patients, making the expertise of an oncoplastic surgeon invaluable in the realm of breast cancer surgery. you looking for a skilled and compassionate oncological surgeon in Delhi to guide you through your breast cancer journey? Look no further than Dr. R K Saggu, a renowned Oncoplastic Breast Surgeon dedicated to providing personalized care and innovative surgical solutions. Let's delve into the world of breast cancer surgery and the expertise of Dr. R K Saggu.
Understanding Breast Cancer Surgery
When facing breast cancer, surgery plays a crucial role in removing the cancerous tissue. The choice of surgery depends on various factors such as the type and stage of cancer, overall health, and personal preferences.
Tailored Treatment Approach
Your treatment plan is customized based on:
Type of breast cancer
Stage of cancer
Overall health and medical conditions
Personal preferences
Types of Breast Cancer Surgery
Breast Conservation Surgery (BCS)
BCS, also known as Lumpectomy, involves removing the tumor while preserving the breast. This procedure is safe and effective for early-stage breast cancers. Factors like tumor size relative to breast size and ability to receive radiation treatments post-surgery determine candidacy for BCS.
Modified Radical Mastectomy (MRM)
MRM involves removing the entire breast in certain situations like multicentric tumors or patient preference. Dr. R K Saggu ensures a comprehensive approach with minimal downtime for patients undergoing MRM.
The Role of Oncoplastic Surgery
Oncoplastic surgery combines tumor removal with cosmetic techniques to enhance the appearance of the breast post-surgery. This approach aims to achieve better cosmesis and quality of life for patients undergoing breast conservation surgery.
Breast Reconstruction Options
For patients opting for reconstruction post-mastectomy, Dr. R K Saggu discusses various options such as implants or autologous tissues. Reconstruction is not only about physical restoration but also contributes to a patient's emotional well-being.
Hidden Scar Breast Surgery
Dr. R K Saggu specializes in Hidden Scar Surgery, a technique that minimizes visible scarring by strategically placing incisions. This advanced approach ensures minimal scarring while effectively removing cancerous tissue. Wire Localisation Excisional Biopsy
Very small cancers detected on mammograms may require precise localization for removal.
A guidewire is used to mark the area of concern in the breast.
The wire is placed under local anesthesia using ultrasound or mammogram guidance.
The marked area is surgically removed under general anesthesia.
X-ray confirmation and pathology analysis ensure complete cancer removal.
Mastectomy Options
Simple Mastectomy
Involves removal of the entire breast, most skin, and nipple-areolar complex.
Axillary lymph nodes are spared during this procedure.
Skin and Nipple Sparing Mastectomy
Entire breast removal with preservation of skin and nipple-areolar complex.
Often combined with reconstruction using implants or autologous tissue.
Suitable for high-risk individuals or early-stage breast cancer patients.
Lymphnode Surgery
Axillary Lymph Node Evaluation
Imaging (Ultrasound/MRI) and biopsy assess lymph node involvement.
Sentinel Lymph Node Biopsy (SLNB) or Axillary Lymph Node Dissection are surgical options.
Sentinel Lymph Node Biopsy (SLNB)
Identifies and examines the first draining lymph node for cancer cells.
Helps avoid extensive lymph node surgery and reduces complications like lymphedema.
Axillary Lymph Node Dissection
More extensive procedure for larger tumors, involving multiple lymph nodes.
Can lead to complications like lymphedema, seroma, numbness, and shoulder weakness.
Chemoport
What is a Chemoport?
Implanted device for administering IV chemotherapy safely and reliably.
Reduces risks to peripheral veins and tissues during treatment.
Allows frequent blood sampling without repeated needle sticks.
Benefits of Chemoport
Long-term IV access with minimal risk of vein damage.
Durable silicon material withstands numerous needle pricks.
Enhances quality of life during chemotherapy treatment.
For more information on Oncoplastic Breast Surgery in Delhi, visit Dr. Rajinder Kaur Saggu or Contact us on +91-9871056323.
#dr. rajinder kaur saggu#breast specialist doctor in delhi#breast specialist lady doctor in delhi#oncoplastic breast surgeon in delhi#breast surgeon in delhi#healthcare#breast lump doctor in delhi#breast cancer surgeon in delhi.#breast cancer surgeon in delhi#breast surgeon in delhi.
0 notes
Text
Web3 Wealth - MaVie Global and Personal Business Development in the Decentralized Economy
The landscape of the digital world is undergoing a monumental transformation, redefining the fundamental aspects of wealth and personal business development. At the helm of this remarkable transition is Web3, a decentralized online platform poised to redefine our approaches to creating, managing, and accumulating wealth in the digital age. With MaVie Global, the world's leading platform for WEB3 Affiliate Marketing, driving this shift, the promise of a robust, growth-centric ecosystem for business development is close at hand.
The Emergence of Web3
To understand Web3, it's essential to recognize its roots in the blockchain and cryptocurrency revolution that began with Bitcoin over a decade ago. Web3 represents the third generation of the internet. The first generation (Web1) brought static web pages, while the second generation (Web2) introduced dynamic, user-generated content and social media platforms like Facebook and Twitter.
Web3, on the other hand, is characterized by decentralization. It leverages blockchain technology, smart contracts, and decentralized applications (dApps) to create a more equitable and open digital landscape. Unlike Web2, where centralized intermediaries like Facebook and Google controlled user data and content, Web3 empowers individuals by giving them control over their data and digital assets.
Web3: A Paradigm Shift in Wealth Creation
Web3 presents a transformative potential to reconstruct the mechanisms of wealth creation and personal business development. A distinguishing feature of this revolutionary paradigm is its capability to tokenize assets, implying that practically anything of value can be digitally represented as a token on a blockchain. Assets, tangible or intangible, ranging from real estate and art, to stocks and intellectual property, can all be tokenized, offering a secure and transparent transaction process.
For entrepreneurs and creators, this opens up new avenues for monetization and wealth creation. Musicians can sell tokenized shares in their music, artists can tokenize their artwork, and startups can issue tokens as a means of crowdfunding. The possibilities are limited only by one's imagination.
Decentralized Finance (DeFi): A Financial Revolution
Decentralized Finance, commonly referred to as DeFi, is a critical component of the Web3 ecosystem. DeFi signifies a radical shift in the traditional financial paradigm, eliminating the need for conventional middlemen such as banks. Instead, DeFi utilizes the power of blockchain technology and smart contracts to orchestrate a multitude of financial activities including lending, borrowing, trading, and interest acquisition, all within a decentralized framework. This revolutionary financial model is inherently aligned with the principles of MaVie Global, further bolstering its commitment to personal business development within the sphere of Web3 Affiliate Marketing.
One of the most exciting aspects of DeFi is the opportunity for anyone with an internet connection to access financial services. This democratization of finance has the potential to empower billions of people worldwide who are currently excluded from the traditional banking system. With DeFi, individuals can earn interest on their crypto holdings, borrow assets, and trade without the need for a middleman.
NFTs: Unlocking the Value of Digital Assets
Non-Fungible Tokens (NFTs) have taken the digital world by storm. These unique, indivisible tokens represent ownership of digital or physical assets, and they are creating new opportunities for creators and collectors alike. Artists, musicians, and content creators can tokenize their work, ensuring they receive fair compensation and royalties every time their creations are bought or sold.
Furthermore, NFTs are expanding the definition of wealth beyond traditional assets. Digital real estate, virtual items in video games, and even tweets are being tokenized and traded. This opens up an entirely new realm of wealth creation in the digital age, where ownership of scarce digital assets can be as valuable as physical property.
Web3 and Personal Business Development
So, how can individuals leverage Web3 to develop their personal businesses and accumulate wealth? Here are some key strategies:
Tokenize Your Skills: If you have unique skills or knowledge, consider tokenizing them. Create an online course or informational product and sell it as an NFT. This allows you to receive direct compensation for your expertise and ensures you continue to benefit from it as demand grows.
Invest in Crypto and DeFi: Educate yourself about cryptocurrencies and DeFi platforms. By investing wisely and earning interest on your crypto holdings, you can grow your wealth over time. Be sure to research and understand the risks associated with crypto investments.
Create a Decentralized Business: Explore opportunities to start a decentralized business on blockchain platforms like Ethereum or Polkadot. These businesses can range from DeFi protocols to decentralized applications, and they often provide a share of their revenue to token holders.
Engage with NFTs: If you're a creator, consider minting your own NFTs to monetize your digital art, music, or content. Alternatively, you can invest in NFTs that align with your interests and hold them as assets that may appreciate in value.
Learn and Adapt: Web3 is a rapidly evolving space. Stay informed, learn from the community, and adapt your strategies as the technology and opportunities evolve. The more you understand the Web3 ecosystem, the better positioned you'll be to take advantage of its wealth-building potential.
Challenges and Considerations
While Web3 presents exhilarating prospects for business and wealth creation, it is crucial to navigate this domain with circumspection. The decentralized essence of Web3 underscores the importance of security. It's imperative to be vigilant of potential frauds and store your digital assets securely in a trustworthy wallet. Ensuring the safety of your digital resources not only safeguards your investments but also contributes to solidifying the foundation of yourpersonal businessin the Web3 sphere.
Additionally, regulatory frameworks around cryptocurrencies and NFTs are still evolving in many jurisdictions. It's crucial to stay compliant with local laws and tax regulations to avoid legal complications.
Web3 represents a paradigm shift in how we create, manage, and accumulate wealth in the digital age. By tokenizing assets, embracing DeFi, and engaging with NFTs, individuals can unlock new avenues for personal business development and financial growth. However, it's crucial to approach the Web3 space with knowledge, caution, and a long-term perspective to navigate the exciting yet volatile landscape of decentralized wealth creation.
0 notes
Text
So, I have no fucking clue why this is only just now occurring to me, but please consider: a fucking marvel au with Keigo Takami/Hawks as Steve Rogers/Captain America, and Touya Todoroki/Dabi as Bucky Barnes/The Winter Soldier.
This has to be a thing that someone's done already, right? Where is it? I need to see it. Fan art, headcanons, fics-- show me that good shit, I need to see it immediately.
#fucking HELL HOW did i not see this from the beginning???#(alleged) childhood friend/soulmate (alledgedly) dies#undergoes radical physical reconstruction#returns a villain with no recorded past#who may or may not have memory loss regarding his past/identity/relationship to said hero/soulmate/childhood friend#I'm fucking kicking myself for not seeing this sooner#i need this au in my life#dabihakws#stucky#bnha#don't mind me#text#mine
10 notes
·
View notes
Text
Feminism
Feminism can be described as a range of social or political movements, as well as ideologies which share a common goal. This goal is to achieve, define, establish, and define personal, professional, social and political equality for the sexes. Changes in dress and acceptable physical activity have often been part of feminist movements (Kaufman, 2012). Activism is widely defined as the action and policy of implementing intense campaigning to introduce social or political change.
Regardless of the different concerns that feminists have expressed in the reliance of experience in contemporary feminism, the term has been used severally as a political strategy. While the authors do not support the acceptance of the notion of a “prediscursive female experience” Oksala (2016) is of the opinion that feminist theory must “retrieve experience”. The author further asserts that this experience cannot be narrowed down to the theories that are created regarding social construction (Oksala, 2016). Dismissal of the value of experience means the rejection of a viable political tool that continues to state the case for the several oppressive social norms and practices today. Experience is also necessary in the emphasis of the need for experience to women who theorize sexual violence. This is in order to trigger their feminist side since it can only be achieved through emphasis on such terms as “date rape” and “sexual harassment” that are based on experience. The interpretation of the experiences that women undergo has been greatly aided by the feminist definition of the cases, thus playing a crucial role in disrupting the dominant discourses that currently exist. Experience allows females to have new constructions of the reality they face daily; hence, giving them a clear view of feminism. The rising wave of feminism in response to trauma associated with sexual violence has brought to life increased debates on the causes of sexual aggression, such as the ways in which it has been embedded into the normal forms of heterosexuality among men today. The definition of sexual violence and the ways and frequency of occurrence have been a challenging task as feminists and scholars try to justify the female experiences and validate their different ways in which women handle their experiences. The literature review further explored the increased state of trauma and the impacts it has on the victims. As more feminists and researchers forge the relationship between the two, there are also some concerns that the state of sexual violence continues to be depoliticized and medicalized in the context of trauma. Similarly, some feminist scholars have problematized the trauma of rape discourse that they see as dominating contemporary mainstream understandings of sexual violence. In contemporary feminism, there is an exploration of two concepts, which entail choice and experience and how these concepts of feminism are relevant to the issue of sexual violence. Therefore, the three concepts, that is, trauma, choice, and experience, complicate the discussions of feminism regarding the topic of assault, as people take the meanings in their individual ways. The correlation between sexual violence and feminist frameworks among victims can make it a difficult subject.
Feminist Activism among Men
Male participation in feminism can advance the cause, but, they refrain from getting involved following their first association with women (Holmgren and Heran, 2009; Preopio, 2015). According to Rentschler (2015), men can support feminism in numerous ways that include via media, endorsing and identifying with feminist beliefs, and taking part in feminist promotion initiatives. Although women subscribe to feminist views the most, few chose to self-label. Robnett, Anderson, and Hunter (2012) found this trend to highlight the subtle differences between beliefs, and identification. Preopio (2015) insists on the need to look past stigma and recognize shared understandings of the feminism before considering self-labeling or taking part in collective action to support the ideology.
Since the 18th century, men have played a key role in supporting the advancement of women and their quest to inclusion in society (Kaufman, 2012). In the 19th and 20th century, men were actively involved in the campaign for women's suffrage (John & Eustace, 1997). Despite the preference of women to advance their movement independently, men continued to support the women’s liberation movement whereby they set up their own sexist men groups (Messner, 1993). Roy et al., (2007) noted that people, especially men, were hesitant to identify with a particular group that others do not value. Over time, society has failed to endorse the views of feminists. Roy (2007) asserts that the adoption of feminist ideals by men results from the government and social change of perceptions towards women. Moreover, portraying women positively has added to the “commitment to social action” by men and consequently increasing the commitment by men (Roy et al., 2007).
Unfortunately, men supporting feminism have endured stigma and discouragement (Robnett et al., 2012). According to Elley and Wetherell (2001), feminists, both men, and women are branded as unattractive and foul. This form of stereotyping further complicates the attainment of feminist ideals in society as those advocating for feminism experience backlash. Women acknowledge that they are oppressed by patriarchy, and thus are better at advocating for their rights and can withstand the negative connotations from feminism (Yeung, Kay, and Peach, 2014). Men, in contrast, in appreciation of their gender privilege, are likely to be reluctant to participate in advocating for feminism. According to Jamili and Roshanzamir, (2017) the lack of one's self-identity results in both cultural trauma and PTSD. The authors assert that failure by feminists to encourage people to reconstruct their traumatized identities causes personal, painful, and traumatic experiences. However, ideal feminism according to Rudman, Mescher, and Moss, (2012) requires men to overcome the negative stereotypes, and change the structure of gender relations and act to eliminate all forms of patriarchy.
Mental Health
There has been considerable concern over the years over the feminist approach to counseling which is taken as an alternative to traditional variation of psychotherapy. The counseling sessions have been defined in a variety of ways. Nonetheless, the lack of a unified approach to feminism results in feminists ascribing to the differing philosophies. (Yoder, Tobias, & Snell, 2010). For this reason, Fischer et al., (2000) developed a Feminist Identity Composite (FIC) to expand the link between feminist identity and the variables: subjective well-being, and body image.
In 1971, Downing and Roush recommended that women move through phases of feminist identity from a position of accepting the gender status quo to equality activism (Cross, 1971). According to Cross, the five stages include passive acceptance, revelation, embeddedness, synthesis, and ongoing commitment. In applying this concept, Symanski (2004) discovered that the five phases had a positive correlation to the direction feminist ideologies took. The author found that embeddedness and revelation, for instance, were current commitments associated with positive attitudes towards feminism and the more significant endorsement of the ideologies of LGBT and other minority groups.
A comparison between three types of therapy, traditional, feminist, and explicit feminist reveals differences that include the level of confidence of the counselor’s helpfulness, willingness to attend sessions, and perceived similarity of the counselors (Simi and Mahalik, 1997). Simi and Mahilik found that subjects preferred feminist to traditionalists when attempting to resolve problems relating to a career. Overall, the authors found that patients were willing to see a traditionalist over a feminist counselor than an explicit feminist counselor. Similarly, Enns and Hacket (1990) examined the reaction by feminist and non-feminist women to counseling vignettes that depicted a non-sexist approach and using liberal and radical feminists. The authors found the liberal and radical feminists counselors to be more trustworthy than the non-sexist counselors are. Both feminist counselors were found to be helpful and willing to see the feminist for sexual assault and career concerns.
Domestic Abuse
In a broader context, domestic abuse encompasses hitting and physical abuse, but scholars argue the definition should not involve physical violence only (Stark, 2007; Rajan, 2018). Among feminists, domestic violence requires power imbalances between men and women in society and the family (Leung, 2011). The contest for dominance as illustrated by Leung is a global phenomenon particularly in the global south where men’s domination over women underpins the occurrence of domestic violence (Jewkes, Flood, and Lang, 2014). Studies by Akmatov et al. (2008) in Egypt and Tayyab et al. (2017) in Pakistan revealed wife beating was a common trend perpetuated by the commonly held norms and the role of women in society. For instance, in these countries, men were found to dominate women and assert their power over women and even correct the woman’s behavior. For this reason, feminists insist on the need to listen to women, accept their role in society, support them in their struggles rather than impose cultural norms (Rajan, 2018). However, the elimination of these norms would require the understanding of the influences of domestic violence, which according to Vung et al. (2008) includes: relationship, individual, societal and communal influences. The knowledge of how these variables contribute to domestic violence can aid in eliminating the vice and consequently prevent or reduce traumatic experiences that result from the abuse and the possible development of PTSD among the victims.
Activism
Citing de Lemus and Stroebe, Savas and Stewart (2019) assert that three factors contribute to collective action: belief in one’s ability to affect political outcomes, perceptions of being treated unjustly, and membership in a politicized group. The authors posit that there is only one way to learning about how individuals commit to social change, and that is by examining the narrative of those committed and comparing their experiences in the social-historical context during their upbringing. The authors further posit that marginalized members of society are likely to engage in collective action in an attempt to change the status quo of a particular group that they identify with; hence the Social Identity Theory. However, Savas and Stewart (2019) posit that traditionally, the theory failed to contrast negative and positive values attached to social groups in the context of power relations in society. Privileged groups were viewed positively even by marginalized groups while the latter was derogated by both.
Savas and Stewart (2019) recommended linking activism, group identification, and injustice. In doing so, the authors would achieve developing a relationship between injustices in the activists’ lives and their identity. The authors concluded that the events in the life of an activist precipitated their activism. The cohort in the study was found to vivid memories of moments in their lives marked their identities and their lives. However, most activists began well in their adulthood and were not full-time activists. For most of them, small and spontaneous political acts defined the experiences that led them into activism and helped them overcome the internalized oppression. These events also helped the people surveyed to see life differently and put them in a unique position to break the barriers created by internalized oppression and consequently participate in efforts for social change.
The Me Too movement (also known as #MeToo) is a new and upcoming movement that takes a stand against sexual assault and harassment. Actress Alyssa Milano jump started the movement by encouraging victims of these crimes to come forth via social media (twitter). Milano believed this topic needed to be brought into the light to expose how serious and frequent it has become. The movement originally began pre Milano in the year 2006, with Tarana Burke. Survivors would come forward using the phrase “me too” to raise awareness and prevention in what many deem rape culture. “Me Too” became a global phenomenon after the Harvey Weinstein abuse allegations. The mission of this movement has remained strong to support survivors of sexual violence to share their personal stories and get help to promote healing.
Feminism and Psychology
Eagly et al., (2012), posits that the 20th century had increased activities in feminist activism thus raising attention on the psychology and the study of women and gender. The authors conducted a survey aimed at demonstrating the overall growth of interest in the field. Using the PsycINFO database, they collected over 2500 journals covering over half a century. The authors discovered that there was significant growth of research on women and gender over the years. The results suggested that psychological research was no longer a preserve of men. Put into context, psychology, in consideration of one sex, is skewed toward women than men. According to Riger (1992), this skewness could result from studies on men psychology encompassing the study of humans in articles that do not explicitly state to be about men.
Feminists have criticized the discipline of psychology since the early 1960s because of its neglect of women and gender issues (Eagly and Riger, 2014). Citing Zammito, Eagly and Riger (2014) posit that the criticism by feminists follows the criticism of the larger field of science – virtually all fields of science. To find the changes in the field of psychology, the authors studied journals published in PsycINFO between 2003 and 2012 classified as postmodern. The authors found evidence of postmodernism, particularly on non-empirical journals. The authors posit that the changes in the field of psychology resulted from influences by society and intellectuals that encompass feminism. Moreover, women have risen to become professors, editors, and now head psychology departments despite critique by feminists.
1 note
·
View note
Text
HEALTHCARE INFORMATICS’ EVOLUTION AND REVOLUTION

Change is everywhere. And whether you’re talking about your hometown or your day-to-day activities, adjustment and fine-tuning is inevitable. Within the context of the organizations in the Healthcare Industry, the challenge is learning to handle change effectively and to manage change with evolution and revolution as an end goal. From this perspective, there are basically two ways to understand change: Evolutionary or incremental change and Revolutionary or transformational change. Understanding the differences and learning how to make the most of these opportunities can be a challenge, but one that ensures the industry not only survives but also thrives.
Evolutionary and Revolutionary Change
Evolutionary change is incremental and takes place gradually, over time. Slow, gradual change often takes place to ensure the survival of the organization. It’s incremental in that it happens step by step, little by little. Organizations undergoing evolutionary change may have been prompted by outside pressure, in order to keep up with technology or addressing the needs of stakeholders more effectively.
By contrast, revolutionary change is profound. When we think revolutionary change, we envision complete overhaul, renovation, and reconstruction. Change is fundamental, dramatic and often irreversible.
From an organizational perspective, revolutionary change reshapes and realigns strategic goals and often leads to radical breakthroughs in beliefs or behaviours. When an organization decides to engage in revolutionary change, radical transformations to products or services often follow. In efforts to stay ahead of the curve and reach evolution, outstanding organizations often pursue revolutionary change.
The challenge in today’s healthcare industry is not in learning how to accept change, but in how to orchestrate the most efficient change leading to organizational evolution. Staying in touch with core values, maintaining a culture of innovation and learning to make the most of resources
What is Healthcare informatics?
Healthcare Informatics is a discipline that involves the use of information technology to organize and analyze health records to improve healthcare outcomes. Health Informatics deals with the resources, devices, and methods to utilize acquisition, storage, retrieval, and use of information in health and medicine. Other related areas include clinical research informatics, consumer health informatics, and public health informatics, biomedical informatics, imaging informatics, and nursing informatics.
In a nutshell, Health informatics is a specialization that links IT, communications and healthcare to improve patient care.
Why Health Informatics?
A few years ago, clinical care and documentation were all paper-based. Now, with the advent of clinical documentation that enables secure electronic sharing of patient data, healthcare providers can reduce wait times, improve inter-disciplinary collaboration, and minimize errors. Additionally, because we now have a database on every patient, we can analyze aggregated clinical data to help us to understand what is going on with larger groups of patients and identify trends in population health.
The fact that technology is rapidly transforming health care should come as no surprise to anyone. From robotic arms that perform surgery to nanorobots that deliver drugs through the bloodstream, the days of being tended to by the human country doctor seem to have fully given way to machines and software more in keeping with the tools of Dr Leonard H. "Bones" McCoy from “Star Trek.”
In a nutshell, It has come to stay!
Healthcare Industry vs. Technology Evolution and Revolution
First of all, health care isn’t just expensive; it’s wasteful. It’s estimated that half of all medical expenditures are squandered on account of repeat procedures, the expenses associated with more traditional methods of sharing information, delays in care, errors in care or delivery, and the like. With an electronic and connected system in place, much of that waste can be curbed. From lab results that reach their destination sooner improving better and more timely care delivery to reduced malpractice claims, health informatics reduces errors, increases communication, and drives efficiency where before there was costly incompetence and obstruction.
Apart from that, there’s a reason medicine is referred to as a “practice,” and it’s because health care providers are always learning more and honing their skills. Health informatics provides a way for knowledge about patients, diseases, therapies, medicines, and the like to be more easily distributed.
Also, when patients have electronic access to their own health history and recommendations, it empowers them to take their role in their own health care more seriously. Patients who have access to care portals are able to educate themselves more effectively about their diagnoses and prognoses, while also keeping better track of medications and symptoms. They are also able to interact with doctors and nurses more easily, which yields better outcomes, as well. Health informatics allows individuals to feel like they are a valuable part of their own health care team because they are.
More so, one criticism of approaching patient care through information and technology is that care is becoming less and less personal. Instead of a doctor getting to know a patient in real time and space in order to best offer care, the job of “knowing” is placed on data and algorithms.
Nevertheless, as data is gathered regarding a patient, algorithms can be used to sort it in order to determine what is wrong and what care should be offered. It remains to be seen what effects this data-driven approach will have over time, but regardless, since care is getting less personal, having a valid and accurate record that the patient and his care providers can access remains vital.
Moreover, Health care is getting more and more specialized, which means most patients receive care from as many as a dozen different people in one hospital stay. This increase in specialists requires an increase in coordination and it's health informatics that provides the way forward. Pharmaceutical concerns, blood levels, nutrition, physical therapy, X-rays, discharge instructions. It’s astonishing how many different conversations a single patient may have with a team of people regarding care, and unless those conversations and efforts are made in tandem with one another, problems will arise and care will suffer. Health informatics makes the necessary coordination possible.
Furthermore, the most important way in which informatics is changing health care is in improved outcomes. Electronic medical records result in higher quality care and safer care as coordinated teams provide better diagnoses and decrease the chance for errors. Doctors and nurses are able to increase efficiency, which frees up time to spend with patients, and previously manual jobs and tasks are automated, which saves time and money. Not just for hospitals, clinics, and providers, but for patients, insurance companies, local government, state and federal governments too.
Health care is undergoing a massive renovation thanks to technology, and health informatics is helping to ensure that part of the change results in greater efficiency, coordination, and improved care.

Artificial Intelligence (AI) and Healthcare Informatics
Artificial Intelligence (AI) is devoted to creating computer software and hardware that imitates the human mind. The primary goal of AI technology is to make computers smarter by creating software that will allow a computer to mimic some of the functions of the human brain in selected applications. Applications of AI technology include; general problem solving, expert systems, natural language processing, computer vision, robotics, and education. All of these applications employ knowledge base and inference techniques to solve problems or help make decisions in specific domains.
The global artificial intelligence market is expected to reach $19.47 billion by 2022, according to the research firm Allied Market Research. As AI is marking its presence, tech giants are working to capitalize on new opportunities. The healthcare sector is a natural fit, according to Sanjay Gupta, managing director, South Asia, and the Middle East for NICE.

Time and Life Saver
Among Google’s many AI ventures is an effort to develop new products targeting the health sector. The company is focusing on applications for life preservation, preventive care and improving health care services.
The company plans to launch a trial in India to test an AI system that scans a person’s eyes to look for signs of diabetic retinopathy. The company aims to license the technology to clinics. The system already has proven itself adept at detecting high blood pressure, or risk of heart disease or stroke, according to a study published in early 2018.
Accuracy and Scalability
AI advancements could be of great help to patients with an age of 65 years or older. According to the recent study published in the journal NPJ Digital Medicine, Researchers implemented AI to screen electronic health records along with notes taken by doctors for finding potential health risks. This included nearly 48 billion data points used in a deep learning model.
The AI analyzed the data and determined medical issues such as mortality rates, unplanned readmission, and long hospital stays with an accuracy of 90 per cent. In comparison to traditional predictive analysis models, the deep learning model provided 10 per cent more accuracy and scalability. The system did not only analyze electronic records but also took into account doctors’ notes and information on old charts stores as PDF files.

Blockchain and Healthcare Industry
A Blockchain approach offers several benefits over traditional location tracking products. The most obvious of which is the immutability and tamper-proof qualities of the Blockchain. This prevents a malicious user from changing the location history of a device or deleting it from the record. This is a particularly important factor considering that medical device theft and shrinkage has
There are several areas of healthcare and well-being that could be enhanced using Blockchain technologies.
These include device tracking, clinical trials, pharmaceutical tracking, and health insurance. Within device tracking, hospitals can trace their asset within a Blockchain infrastructure, including through the complete lifecycle of a device.
The information gathered can then be used to improve patient safety and provide after-market analysis to improve efficiency savings. This paper outlines recent work within the areas of pharmaceutical traceability, data sharing, clinical trials, and device tracking.

Social Media within Healthcare Industry
Social media including Web sites like Facebook Twitter Instagram and Linked-In have become part of the fabric of modern life online communities can hardly be avoided by anyone who lives even a modestly engaged life.
There are many advantages to social media both personal and professional. Businesses have become quite sophisticated in using social media to extend their message and to present their products and services to the public. But what about professionals or people like you who are involved in the healthcare industry.
What role does social media play in your work and what restrictions our health professionals are under when it comes to using social media?
First, it's important to keep in mind that most health care providers have policies and procedures for making public announcements. If you are not an official spokesperson vested with the authority to speak on behalf of your organization, please refrain from sharing news and occurrences on social media.
Unless you've been given specific permission to do so in your organization's official branded social media accounts so you can read tweets, like, share and comment on items posted there if you choose.
Secondly, you must not underestimate the valuable role that social media can play in the medical profession. For example, trauma teams in Maiduguri were able to prepare their ears quickly after learning of the Banki town bombing over social media networks.
In conclusion, change is the key to success.
About
Oladesanmi Arigbede is a Health IT expert, an entrepreneur, a technology enthusiast who likes cutting-edge technologies. In a career spanning one decade, he has been a business owner, technical architect, startup consultant, and CTO.
References
https://geneticliteracyproject.org/writer/pratik-kirve/
https://www.alliedmarketresearch.com/artificial-intelligence-market
https://ai.google/
https://hitconsultant.net/2016/03/02/health-informatics-transforming-health-care/
#HealthInformatics #Techonology #HealthcareIT #ArtificialIntelligence #Blockchain #SocialMedia #MedicalInformatics
1 note
·
View note
Text

Firefly Sparkle: Newly discovered galaxy mirrors Milky Way's early days
For the first time, the NASA/ESA/CSA James Webb Space Telescope has detected and "weighed" a galaxy that not only existed about 600 million years after the Big Bang, but also has a mass that is similar to what our Milky Way galaxy's mass might have been at the same stage of development.
Other galaxies Webb has detected at this period in the history of the universe are significantly more massive. Nicknamed the Firefly Sparkle, this galaxy is gleaming with star clusters—10 in all—each of which researchers examined in great detail. Their work is published in Nature.
"I didn't think it would be possible to resolve a galaxy that existed so early in the universe into so many distinct components, let alone find that its mass is similar to our own galaxy's when it was in the process of forming," said Lamiya Mowla, co-lead author of the paper and an assistant professor at Wellesley College in Massachusetts. "There is so much going on inside this tiny galaxy, including so many different phases of star formation."
Webb was able to image the galaxy in sufficient detail for two reasons. One is a benefit of the cosmos: A massive foreground galaxy cluster radically enhanced the distant galaxy's appearance through a natural effect known as gravitational lensing. And when combined with the telescope's specialization in high-resolution imaging of infrared light, Webb delivered unprecedented new data about the galaxy's contents.
"Without the benefit of this gravitational lens, we would not be able to resolve this galaxy," said Kartheik Iyer, co-lead author and NASA Hubble Fellow at Columbia University in New York. "We knew to expect it based on current physics, but it's surprising that we actually saw it."
Mowla, who spotted the galaxy in Webb's image, was drawn to its gleaming star clusters, because objects that sparkle typically indicate they are extremely clumpy and complicated. Since the galaxy looks like a "sparkle" or swarm of fireflies on a warm summer night, they named it the Firefly Sparkle galaxy.
Reconstructing the galaxy's appearance
The research team modeled what the galaxy might have looked like if its image weren't stretched by gravitational lensing and discovered that it resembled an elongated raindrop. Suspended within it are two star clusters toward the top and eight toward the bottom. "Our reconstruction shows that clumps of actively forming stars are surrounded by diffuse light from other unresolved stars," said Iyer. "This galaxy is literally in the process of assembling."
Webb's data show the Firefly Sparkle galaxy is on the smaller side, falling into the category of a low-mass galaxy. Billions of years will pass before it builds its full heft and a distinct shape. "Most of the other galaxies Webb has shown us aren't magnified or stretched, and we are not able to see their 'building blocks' separately. With Firefly Sparkle, we are witnessing a galaxy being assembled brick by brick," Mowla said.
Stretched out and shining, ready for close analysis
Since the image of the galaxy is warped into a long arc, the researchers easily picked out 10 distinct star clusters, which are emitting the bulk of the galaxy's light. They are represented here in shades of pink, purple, and blue. Those colors in Webb's images and its supporting spectra confirmed that star formation didn't happen all at once in this galaxy, but was staggered in time.
"This galaxy has a diverse population of star clusters, and it is remarkable that we can see them separately at such an early age of the universe," said Chris Willott of the National Research Council Canada, a co-author and the observation program's principal investigator. "Each clump of stars is undergoing a different phase of formation or evolution."
The galaxy's projected shape shows that its stars haven't settled into a central bulge or a thin, flattened disk, another piece of evidence that the galaxy is still forming.
TOP IMAGE: Horizontal split down the middle. At left, thousands of overlapping objects at various distances are spread across this galaxy cluster. A box at bottom right is enlarged on the right half. A central oval identifies the Firefly Sparkle galaxy, a line with 10 dots in various colors. Credit: NASA, ESA, CSA, STScI, C. Willott (NRC-Canada), L. Mowla (Wellesley College), K. Iyer (Columbia)
LOWER IMAGE: The Firefly Sparkle is a redshift zspec = 8.296 ± 0.001 gravitationally magnified arc lensed by the MACS J1423.8 + 2404 cluster. Credit: Nature (2024). DOI: 10.1038/s41586-024-08293-0

youtube
3 notes
·
View notes
Text
Paget’s Disease Of The Breast - Symptoms, Causes, And Diagnosis.
Paget's breast disease is a cancer type that can occur as or resemble eczema, with skin changes involving the nipple. The disease is a rare disease that represents 1% to 4.3% of all breast cancers and was first described by Sir James Paget in 1874. In This Article:
What does paget's disease of the breast look like?

In other words, Paget's disease of the breast refers to changes in the breasts that indicate cancer cells have formed in or around the nipples. Redness on or around the nipple shows changes are happening under the skin. Paget's disease usually occurs in other areas of the breast, with another type of cancer, usually ductal carcinoma in situ (CDIS) or invasive breast cancer. Paget's disease is very common in women, but it also can affect men. It usually occurs after 50 years. The average age at diagnosis is 62 for women and 69 for men, but it can really show anytime. 1% and 4% of breast cancer cases have Paget's disease. Symptoms of Paget's disease may resemble a skin condition, such as eczema or psoriasis. This sometimes delays diagnosis and increases the risk of life-threatening illness. The disease itself is harmless and superficially limited and is sometimes dismissed. Although it actually shows hidden breast cancer. Paget's disease of the nipple This could also mean Paget's disease of the breast. Paget's nipple disease is a very rare breast cancer form where cancer cells accumulate in or around the nipple. Cancer usually affects the nipple ducts (small milk-transport tubes) and then spreads to the nipple’s surface and the areola (dark skin around the nipple). Nipples and areolas are usually scaly, red, itchy and painful. A recent study by the National Cancer Institute shows that Paget's disease of the breast accounts for nothing less than 5% of all breast cancer cases in the USA is very important to be aware of the symptoms since it is known that more than 70% of people who have Paget’s disease also have cancer somewhere else in their breast, either DCIS or invasive carcinoma. Unusual occurrence and nipple or areola changes are often the early sign of breast cancer. Doctors aren’t fully sure how Paget's disease develops. It is possible that the cancer cells grow in the breast milk ducts and then reach the surface of the nipple. This seems to explain why many people with Paget's disease have a second area of cancer within the breast. A second theory is that breast cells become cancerous. This theory explains a small number of people who have Have Paget's disease only at the nipple or second breast cancer that seems to be completely independent of Paget's disease. Paget's nipple disease is prevalent in women, but just like other forms of breast cancer, it can also affect men. The disease often develops after the age of 50. The National Cancer Institute makes us understand that the average age of diagnosis is 62 for women and 69 for men. Paget’s disease symptoms Symptoms of Paget's disease depend on the stage of development. They usually occur only in one breast. The main symptoms are: Itching, tingling or burning in the area close to the nipple and areola. Redness or pigmentation. Peeling, thickening or scaling of the areola does not heal over time. Nipple discharge that may be yellow or contain blood. Flattened or inverted nipples A brittle lesion with irregular edges.in some cases, ulcers. These usually affect only one nipple. About half of all people with Paget's breast disease have a breast lump behind their nipple. 90% of these cases have invasive breast cancer. Paget's disease causes the nipple and surrounding skin to become red, painful, scaly or flaky. At first, these symptoms tend to come and go. Over time, the symptoms of breast Paget's disease often worsen and may include: Itching, tingling and/or burning sensation.Pain and tenderness or sensitivity.Scaling formation and skin thickening. Yellow or bloody discharge from the nipple Since Paget's nipple disease is rare, doctors often confuse it with eczema (severe skin rash and inflammation), infection or injury, or other skin conditions. For many people, it may take several months to get the correct diagnosis. If you are experiencing any or one of the symptoms mentioned above and it continues despite treatment, have it examined by a breast specialist. In most cases, Paget's breast disease affects one and not both breasts. Diagnosing Paget's disease usually involves the following steps: Physical examination of the breast With special attention to the areola or area around the nipple. The doctor may feel a lump or mass in the breast. A mammogram to check the breast area and look for signs of cancer in other areas of the breast. Ultrasound and/or MRI of the breast To take additional breast’s additional photos and search for other cancer areas. Nipple and areola biopsy A breast surgeon may perform minor surgery to get rid of a small piece of tissue from the areola and the nipple and study it under a microscope. If there are unusual discharges from the breast, the doctor may also take a sample for examination. Difference between Paget's disease and eczema Doctors often find it difficult to diagnose Paget's disease due to its similarity to dermatitis and eczema. Unlike Paget's disease, dermatitis and eczema usually affect the areola and then the nipple. A person should not consult a doctor, because they are confused with contact dermatitis or eczema. Anyone who notices a lump or skin irritation that does not heal within a month should seek advice from a specialist. A person may also have crisp, filtered, or hardened skin that looks like eczema in the nipple, areola, or both. Skin changes can fluctuate early and make the skin look healing. Burning can occur as the disease progresses. At this point, severe skin destruction often leads people to consult a doctor. Causes Doctors do not know the exact cause of Paget's breast disease. One theory states that a person already has breast cancer and some cancer cells migrate from the milk ducts to the surface of the nipple. Another possible explanation is that the nipple’s skin cell spontaneously turns into cancer cells. In some Paget's disease cases, there is no underlying breast cancer, or if tumors are present, it is not linked to disease in the nipple. Risk factors of Paget’s disease Risk factors are similar to other types of breast cancer. These include: Age because the risk increases over time The previous occurrence of breast cancer or breast abnormalities You have a relative with breast cancer having denser breast tissueOverweight or obesity Hormone replacement therapy (HRT) ]Excessive alcohol consumption The rate of spread of breast cancer depends solely on whether it is invasive or not. Learn more here Treatment for Paget's disease of the breast An examination of the unusual areas of the breast, especially the skin around the nipple, is carried out by a doctor, to for lumps or thickened areas. A doctor may recommend one of the following to confirm the diagnosis. a mammography an ultrasound scan or a magnetic resonance imaging (MRI) scan.biopsy Also, Unlike mastectomy, if you need breast-sparing surgery, you also need to undergo breast radiation therapy to treat Paget's disease. Studies have detected that postoperative radiation therapy reduces the risk of cancer coming back. If you have mastectomy and radiation therapy, you may also want to think about breast reconstruction. There are many opinions in the medical community during reconstruction for people receiving radiation therapy. Talk to your doctor if you are doing breast reconstruction before or after radiation. Treatment depends on the results. If there is breast cancer, the doctor will prescribe a treatment based on the characteristics and stage of the disease. Breast Paget’s Disease surgery If the changes affected a large area of the breast, surgery may be the only option needed for such a person. The type of surgery required for Paget's disease of the breast depends on how far the underlying breast cancer has progressed. In addition to removing the breast and areola, the surgeon will also need to remove any cancer within the breast. Surgery types Invasive cancer or ductal carcinoma in situ (DCIS) In these cases, a modified radical mastectomy can be recommended by a doctor. A surgeon removes the breast and crosses the pectoral muscles and some lymph nodes under the arm. Although mastectomy is the traditional treatment for breast Paget's disease, in some cases, it is a more limited surgical option. This surgery is sometimes called "breast-sparing surgery" and is designed to remove cancer while keeping the breast tissue healthy. The type of mastectomy depends on how far cancer has progressed: Total or simple mastectomy: breast removal without removing the axillary (underarm) lymph nodes. However, a sentinel node biopsy should be performed to examine nodules that are very close to the tumor for signs of cancer spread. Modified radical mastectomy: Surgery to remove the breast and some lymph nodes under the arm. Non-invasive breast cancer The doctor may determine to remove only the breast and some lining of the breast muscles if the underlying breast cancer is not invasive, by performing a simple mastectomy. Breast reconstruction can restore the appearance of the breast after the surgery. If there is cancer, but only affects the nipple and surrounding area, the doctor may recommend surgery and then radiation therapy to protect the breast or lumpectomy. This type of surgery removes the nipple, areola, and any part of the breast that contains cancer cells. For this reason, most people receive radiation therapy to prevent cancer from coming back. Breast-conserving surgery This usually means a lumpectomy to remove the breast and areola and also remove underlying cancer. The aim is to remove cancer and a small border of healthy tissue to ensure that cancer does not remain. Research suggests that anyone with Paget's disease should have a sentinel lymph node biopsy, although there is no cancer beyond the nipple. Some studies have shown that, although cancer appears to be limited to the areola and the nipple, it is possible to have cancer of the lymph nodes. It is imperative to know if your lymph nodes are carcinogenic to get proper treatment. Hormone therapy targeted therapy and chemotherapy. Depending on the cancer type, the doctor may recommend drug therapy with medication or with hormones that affect how a particular gene works. These treatments can reduce the risk of cancer spreading. Chemotherapy can help prevent the coming back of cancer, especially if: The tumor was large. The cells had spread to the lymph nodes. Cells are aggressive Once treatment is complete, it is important to attend all follow-up appointments and continue to look for changes. Read the full article
#differencebetweenpaget'sdiseaseandeczema#doespagetsdiseasecomeandgo#howispaget'sdiseaseofthebreastdiagnosed#pagetdiseasebreast#paget’sdisease#paget'sdiseasebreaststoriespaget'sdiseasebreastsymptoms#paget'sdiseaseofthebreast#pagetsdiseasebreastsymptoms#whatdoespaget'sdiseaseofthebreastlooklike#worriedaboutpaget'sdisease
0 notes
Text

Limb lengthening is a surgical treatment that improves the height ratio, balances the patient's gait and removes aesthetic concerns. The limb lengthening process requires time, patience and precision. The reconstructive surgeon performs a surgical osteotomy (fracture) with small incisions in the affected leg on the femur and/or tibia.
Most people want to be taller. Leg lengthening surgery (also called limb lengthening) is a really radical cosmetic procedure to increase height. An increasing number of people are undergoing such an operation in the US. Leg lengthening surgical treatment has gained popularity because it gives people a chance to gain a few extra inches. In 1951, Soviet Professor Gavrill Illizarov pioneered leg lengthening surgery in Russia to treat veterans of World War II with leg injuries. The Pentagon is currently funding a study investigating its use for leg trauma.
A magnetic lengthening rod and pins are placed in the bone which allows the leg to extend in a controlled manner over some time. The device has an external magnet that is applied to the nail which drives a gear and moves the telescopic rod. The magnet rotates the gears in the rod to increase the length of the limb. Using this advanced technology, surgeons can limit and/or eliminate the use of external fixation, the former device.
Once the magnetic rod and pins have been placed, patients are instructed how to adjust the bone to extend the bone over time, usually between three and 1 millimeters, each day, over the next three months (you can get one inch per month). As the bones slowly grow, the muscles, tendons, skin, and arteries also respond and grow. The true elongation phase is called distraction when the bones slowly grow over time. There is then a consolidation phase where the bones begin to heal and calcify, and finally, there is a recovery phase when rehabilitation begins and when more weight restriction is applied to the bones.
During surgery, doctors separate your bone in your short legs. The External Fixation System has bars attached to this part of the bone. These bars are connected to an external frame attached to the outside of your leg. The bars will help your bone growth, while the frame will support your limb. For several months, the limb can be extended 6 inches!
The time you need to wear the frame is determined by how much your limb should grow. For most patients, only six to nine months should be worn. During this time, you rotate the sticks several times a day to help the bone in your limbs grow. Most of the bone growth occurs within the first few months. After that, the frame is worn for stability as your bones heal.
After spending some time recovering from your surgery, you can return to school. You can participate in your favorite activities while wearing the chassis, including most sports. You can even go swimming as long as you swim in a salty or chlorinated pool. Your closet may need to be adjusted to include trousers, shorts or skirts that fit your frame. Since you will have to see a doctor every two weeks, you will be able to continue your routine.
ADVANTAGES AND DISADVANTAGES OF LON METHOD
The main advantage of the LON method is that the duration of the entire procedure is shortened more than the conventional methods and thus the patient's comfort is greatly increased. This has a more positive effect on patient psychology due to the early removal of the device. As with a motorized nail, you do not need a wheelchair in the first months. Patients usually start to walk using support from the second day.

When we look at the disadvantage of this method, the operation time is longer than the conventional operation. The experience of the physician who will undergo surgery will play a more important role. Prices are slightly higher than conventional methods due to the use of intramedullary nails.
COMPARISON OF LIMB LENGTHENING SURGERY PRICES
Leg lengthening surgery is often a very serious issue in many respects. When a patient decides that he wants to have cosmetic surgery - the need for detailed information becomes more important from the beginning; patients should fully understand the whole process. Specifically, how the surgical procedure will take place and what will happen during the preoperative stage and postoperative recovery. Limb Lengthening Surgery has become popular and has become much more common in the last few decades; Methodology and surgical techniques are constantly updated and revised to meet new innovative developments; provides better height increase and patient comfort.
In general, the cost of leg lengthening surgery depends on doctors, surgical methods and what they provide; Postoperative accommodation, physiotherapy, general service quality and so on. It may contain. All these factors must be analyzed by a potential patient who wishes to make a limb lengthening decision.
The prices of leg-lengthening surgeries have to take into consideration the doctors, methods used in this surgery and postoperative stay, physical therapy, quality of service and so on; thus varies accordingly. Analyzing all this by those who want to perform well is a very important decision to be healthy.
Normally, any surgical procedure is a very serious issue and all surgeries are at risk. In general, most patients undergo limb lengthening surgery without complications; Limb lengthening is generally considered a more risky procedure. Because external fixator systems are always at risk of infection and without proper hygiene and maintenance of the fixator, complications from infections can be a problem. Furthermore, it is highly recommended that this Limb Lengthening surgical procedure should always be performed by experienced doctors, hospitals, and proper postoperative care is always required. Most importantly, it is always advisable to choose the best country for leg lengthening and the best surgical teams, especially surgeons with extensive surgical experience. So, if you want to find the best limb lengthening surgeon, you should make research a lot about that.
When we look at US prices; Paley receives $ 97,500 for bilateral femoral lengthening and $ 109,000 for bilateral tibial lengthening using PRECICE Stryde. Jacob Rozbruch gets $ 120,000 using PRECICE. In Germany, prices are EUR 52,500 for double-sided femoral lengthening and EUR 55,500 for double-sided tibial lengthening. Prices for both females and tibia range from € 120,000 to € 160,000. Limb Lengthening in Turkey has cost-effective and hygienic as opposed to other countries, 13,500 € external fixator, 17.000 € LON method, 38,000 € intramedullary nail (PRECICE 2), 54.500 € Precor by the Stryer, € 12,000 lengthening acronym, € 9,000 limit inconsistency, € 7,500 Extremity Correction Surgery (Bow Legs), 12.000 € Limb Shortening Surgery.
However, in Russia, India, and Pakistan, many doctors have been very successful in performing the Leg lengthening surgical procedure, but unfortunately; they face significant negative criticisms, especially for the countries listed above. In general, complaints about the effectiveness of doctors or the hygiene of facilities and the overall quality of service in hospitals. Unfortunately, they are not the best country for leg lengthening surgery. In general, medical practitioners or doctors who tend to attract economic bargaining, or patients with the lowest price attractiveness; After the operation is completed and payments are made, they tend to neglect patients at the postoperative stage; A special time for any leg lengthening surgery. So it is inexpensive to make the surgical choice in this country because it is wrong.
However, it should be said that for those seriously considering such a limb lengthening procedure should provide a very balanced option. Facilities and doctors of similar quality to those of Western countries such as Germany, England, France, and the United States, which are said to be preceded by price and cost compared to Eastern Europe; It offers the best limb length surgeon in both worlds. In our commitment to our medical superiority and quality medical services, currently, the world's highest JCI specifies that it has to licensed medical institutions and hospitals for limb lengthening in Turkey is striking.

Why you should choose the limb lengthening in Turkey? In Turkey, both healthy and fit your budget and you never attracted more difficulties in communication, in addition to them. Because there are services such as meeting and welcoming at the airports, transportation from the airport to hotels and hospitals, as well as an English-speaking carer who will help our patients 24/7. You can also socialize with our famous Turkish restaurants, such as historical and touristic visits, boat tours and free tours including meals. You don't have to worry about supporting devices to help you get around the hospital. Here you can easily get answers to your questions with our free consultation.
For more information regarding Limb Lengthening surgeries, please contact us at [email protected]
Or
For direct consultation, please contact our expert patient consultants via phone or WhatsApp: +90 531 988 3090Web site: https://bulmd.com/
Web site: limblengtheninginturkey.com
Facebook: Bulmd
Instagram: bulmdcom
Youtube: Bul MD
WhatsApp: +90 531 988 3090
0 notes
Text
How Orthopaedic Surgeries Help to Get Perfect Musculoskeletal System?
With increasing consciousness of being healthy among people, they are adopting different physical exercises in their lifestyle. Though it’s a good practice it has left them more prone to overuse and injuries of the bones, joints and muscles, especially in baby boomers. Some other conditions that require eventual treatment are caused by degenerative joint disease, osteoarthritis, and arthritis. All these problems are studied and treated by the medical speciality field of Orthopedics or Orthopaedics. Orthopaedics Surgery Treatments in India helps to treat a wide range of issues related to the Musculoskeletal System. This surgical procedure has become one of the most sought after medical treatment by the people willing to lead a healthy life.

What is Orthopaedics all about?
It is a branch of medical speciality that deals with the illness of the musculoskeletal system. Our musculoskeletal system involves bones of the skeleton, muscles, cartilage, tendons, ligaments, joints, and other connective tissue. All of the attributes to offer support to our body and binds tissues and organs together.
Why Orthopaedics Surgery?
Orthopaedics Surgeries include a number of surgical procedures like joint replacement surgery, hip replacement, knee replacement and more.
There are non-orthopaedic alternatives to a complete surgical procedure and if you can function with a little pain, you can avoid it if you desire. These include physical therapy, aids that will help you walk better, various medications that help relieve the pain, steroid injections into the joint itself, and supplements that help relieve the effects of arthritis. If done properly and you can live with it, any combination of these can help you avoid having more invasive procedures done.
If none of the above treatments works, you can take a more radical approach Orthopaedic surgery. Some common orthopaedic procedure includes the replacement of joints with the artificial ones. Then a socket is manufactured and inserted into the pelvis, but more bone is left behind than would be in replacement surgery. This is popular among younger people who suffer from arthritis.
The major areas of the body on which an orthopaedic surgery is performed are : Hand surgery
• Shoulder and elbow surgery • Total joint reconstruction (arthroplasty) • Pediatric orthopaedics • Foot and ankle surgery • Spine surgery • Musculoskeletal oncology • Surgical sports medicine • Orthopaedic trauma

Sports injuries, infections, tumours, degenerative diseases (a neurodegenerative disease affecting tissues or organs such as cancer, diabetes and Alzheimer's disease), congenital disorders (a condition that occurs before birth or within the first months of life such as Down syndrome) and musculoskeletal trauma all are treated by orthopaedists. It is the responsibility of orthopaedists to get their patients up and moving again, enjoying a pain-free activity and a higher quality of life.
The price of orthopaedic surgery varies from country to country. However, If you are willing to undergo this procedure in a developed nation it may cost you a fortune. Therefore, getting the surgery done in developing and newly industrialized countries like India can be the solution to this problem. Orthopaedic surgery price in India is only a fraction of the cost in your native country.
This idea is also supported by the fact that you would save a significant amount of money even after doing expenses in the cost of flights, holiday, accommodation, meals and local transportation while travelling to India. This is the reason why hordes from western countries rush for Medical Tourism in India.Source-http://indusmedtourism.over-blog.com/how-orthopaedic-surgeries-help-to-get-perfect-musculoskeletal-system.html
0 notes
Text
The Orthotropic Neobladder; How to Make It Easy?-JuniperPublishers
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php

Mini Review
The Orthotropic Neobladder; How to Make It Easy?
Ahmed M Moeen* and Diaa A Hameed
Assiut urology and nephrology Hospital, Assiut University, Egypt
Submission: February 14, 2017; Published: March 03, 2017
*Corresponding author: Ahmed M Moeen, Assiut urology and nephrology Hospital, Assiut University, Egypt, Email: [email protected]
How to cite this article: Ahmed M M, Diaa A H. The Orthotropic Neobladder; How to Make It Easy?. JOJ uro & nephron. 2017; 2(1): 555580.10.19080/JOJUN.2017.2.555580
Go to
Abstract
Radical cystectomy and urinary diversion is the standard treatment for patients with muscle invasive bladder cancer. Urinary diversion after radical cystectomy requires skill and expertise. Multiple techniques of urinary diversion are present. However, the orthotropic neobladder (OBS) may be better in terms of quality of life. For the sake of simplicity, neobladder reconstruction is better divided into the following stages;
Stage I: Patient selection and preparation
Stage II: Radical cystectomy and lymphadenectomy
Stage III: Neobladder reconstruction
Stage IV: Uretero- and Urethro-enteric anastomosis
Stage V : Postoperative management
Stage VI: Management of complications
Keywords: Orthotopic neobladder; Reconstruction; Stages; Complications
Abbreviations: RCX: Radical Cystectomy; OBS: Orthotopic Neobladder; ERAS: Enhanced Recovery after Surgery; LND: Lymphadenectomy
Go to
Introduction
Radical cystectomy (RCX) and urinary diversion is the standard treatment for patients with muscle invasive bladder cancer and some patients with non-muscle invasive disease who failed the intra-vesical treatment [1]. Multiple techniques of urinary diversion are present. However, the orthotopic neobladder (OBS) may be better in terms of quality of life, as it is the closest to the normal bladder in location and function. However, it is measured as one of the most difficult urologic procedure [2]. In this short review, we try to simplify the basic principles of neobladder reconstruction for the beginners to make their practice easier. For the sake of simplicity, neobladder reconstruction is better divided into stages; the higher stages need higher experience. We divide it into the following stages;
Stage I: Patient selection and preparation
Stage II: Radical cystectomy and lymphadenectomy
Stage III: Neobladder reconstruction
Stage IV: Uretero- and Urethro-enteric anastomosis
Stage V: Postoperative management
Stage VI: Management of complications
Stage I: Patient selection and preparation
To start with, successful neobladder reconstruction starts with appropriate patient selection and preparation. The main pillars of this stage that should be well recognized are; the indications, contraindications, how to counsel the patients and the peri-operative preparations.
In general, two important criteria must be maintained in patients indicated for RCX to be eligible for OBS: an intact rhabdosphincter to preserve the urinary continence and the radicality of surgery should not be compromised by the retained membranous urethra to which the neobladder will be anastomosed.
On the contrary, the contraindications are multiple and diverse. This implies that the selection criteria are strict and the patient should be an "A1" patient medically and mentally. It includes, patients indicated for urethrectomy as those with bladder neck tumors and extensive infiltrations of the prostate, urethral sphincteric or stricture diseases, those with permanently compromised renal function or severely impaired liver functions, increased risk of metabolic complications as those with previous bowel resection or sever diverticulosis mental or physical Impairments that precludes the ability to self-catheterize when this is necessary, incompliant patients for postoperative regular follow-up, impossibility of nerve- sparing surgery at least on one side, high dose of peri operative radiotherapy and Age > 80 years [3]. The age is not an absolute contraindications and the differentiation between the biological and chronological age is the most important. However, the age of 80 may be the stimulus not to do OBS, as it may be associated with a higher incidence of postoperative morbidity but without increased mortality even in high volume centers [4].
Counseling is very critical. The patient should know all the risks and benefits of this surgery. He/she should know that the possibility of conversion to other diversion forms is an option due to any intra-operative oncological, anatomic or anesthetic reasons [3]. Also, the expectation should be realistic, he/she should know that his neobladder is not a new bladder and there is no urinary diversion technique that could replace all the functions of the natural bladder.
RCX needs an extensive preoperative preparation, careful intra-operative and postoperative manipulations to optimize the functional outcomes. In 2014, published in the European urology a 22 items designed for enhanced recovery after Surgery (ERAS). These include; preoperative medical optimization, bowel preparations can be safely omitted, avoidance of long-term sedative, thrombosis prophylaxis, antimicrobial prophylaxis 1 hr before skin incision, skin preparation with Chlorhexidine- alcohol to decrease surgical site infection, epidural analgesia should continue for 72 hrs to relieve pain without opioids, careful peri-operative fluid management and avoidance of intraoperative hypothermia, early removal or no nasogastric tube use, prevention of postoperative ileus and nausea and vomiting, early mobilization and early oral diet. They concluded that these ERAS items improve the patient care, decrease the postoperative morbidity and the length of hospital stay [5].
Stage II: Radical cystectomy and lymphadenectomy
When discussing the stage of RCX, we will not discuss the surgery on details, but we will stress on three important issues; timing of surgery, how quality of RCX and lymphadenectomy will affect the outcome and lastly certain surgical steps should be done carefully and others should be avoided.
First, timing is very critical as it was shown that there is window of opportunity of about 3 months, after which delaying cystectomy may be associated with increase in the risk of progression and cancer specific mortality [6].
Second, how quality of surgery affecting the outcome is evident from the following; positive surgical margin occurs in 4% with high volume urologists and 14% in low volume ones. Local recurrence will develop in 6% of margin negative patients if compared to 68% of margin positive counterparts. The Mortality rate is about 0.7% in high volume hospitals and 3.1% in low volume ones [7,8].
Certain surgical steps during RCX will affect the reconstructive functional outcome greatly. Ureteric dissection should be done carefully to preserve its vascularity and preserve the lower most part of the ureters which is very important factor in reflux prevention. The pressure in the lower part of the ureter is about 20-30 cm of water and the bladder end filling pressure is 20cm for an optimal cystometric capacity of 450 cm. So, this pressure difference is a safety margin [9].
Multiple techniques of dorsal vein ligation are present; it should be done carefully to avoid bleeding. If done so, it will help so much in preparation of the urethral stump in a traumatic way with preservation of a well-functioning urethral length and performing nerve sparing RCX in a visually clear field which not only improve the sexual function but also affect continence status [10,11].
On the contrary, prostatic capsule and seminal sparing RCX should be avoided. It may improve the postoperative erectile function but does not really improve the continence status. In the meantime, 10-15% higher oncologic failure rate makes it preferably should be avoided [12,13].
Regarding lymphadenectomy (PLND), extended PLND should be considered the standard in patients undergoing RCX as it will clear up to 90% of the lymph nodes if compared to 50% nodal yield when a limited PLND is only performed [14]. When an extended PLND was compared to limited one in patients with ≤pT3P N0.2 disease, the 5 years recurrence-free survival was significantly better (49 vs. 19%, respectively) [15]. Surprisingly, with expanding the template to the inferior mesenteric artery, similar survival and recurrence rates in pT2-3cN0 cM0 patients were found as extended PLND [16]. This may be due to the lymph node metastases higher than the common iliac bifurcation is a characteristic of systematic disease which cannot be controlled by extensive surgery [17].
Stage III: Neobladder reconstruction
Certain goals should be achieved to obtain a good reservoir which are; large capacity, low intra-luminal pressure, no reflux, continence preservation and minimal absorption of urinary solutes.
All intestinal segments were extensively studied for reservoir reconstruction. However, the intestinal segment which stood the test of time is the ileum due to the following reasons; it is more distensible if compared to other segments [18], has favorable urodynamic parameters in the form of large capacity, better compliance and lower filling pressure [19], better continence rates if compared with colonic neobladder [20], its mucosal atrophy with less reabsorption of urinary solutes is more reliable than the large bowel [21] and finally the ease with which the small bowel can be surgically manipulated.
Originally, neobladders were reconstructed from larger intestinal segments as the original Studer (56-60cm) and Hautmann (70cm) ileal neobladders to Improve the nighttime Incontinence [22,23]. However, for more than two decades, 40-45cm of the ileum, 25cm apart from the ileo-cecal valve proved to be quit sufficient [24 ,25 ]. The functional capacity will increase within weeks or months from 150 to 500 ml. This will decrease the incidence of chronic retention with low intra-luminal pressure [26].The postoperative electrolyte disturbance or metabolic acidosis will be minimized [27]. Also, preservation of the terminal part of the ileum and the ileo-cecal valve will decrease the postoperative diarrhea and vitamin B12 deficiency [28]. The risk of spontaneous rupture will decrease as the tension on the large reservoir when filled with urine is significantly higher than in small reservoir with the same intraluminal pressure [27].
Configuration of the reservoir will affects the functional outcome to a great extent. Detubularization and cross folding will minimize the development of high pressure peaks. A spherical reservoir has multiple advantages, the maximum radius according to Laplace's law will be obtained, so the maximum volume to surface area ratio with lower end filling pressure will results. Also, higher wall tension (tension=pressure × radius) in response to the urethral closure pressure will make the sensation of fullness is more likely [3]. Also, there is metabolic advantage as the length of the bowel resection and the area available for reabsorption from the reservoir are minimized [29].
Stage IV: Uretero- and Urethro-enteric anastomosis
The uretero-enteric and urethro-enteric anastomosis are two risky steps during neobladder reconstruction. Improper reconstruction will endanger the upper urinary tract or the whole urinary tract respectively. Good anastomosis should be tension free, water tight, mucosa to mucosa and stunted. Regarding ureteric reimplantation, to do or not to do anti- refluxing technique is a matter of debate [30]. However, the stricture rate is generally higher with anti-refluxing techniques. Regarding the urethro-enteric anastomosis, there are 2 types of neourethra; hole and non-hole techniques. In order to perform safe urethro-enteric anastomosis, we should preserve well- functioning urethral length and prepare the urethral Stump carefully, the neourethra should be wide button hole, most dependent, mucosa to mucosa, tension free with no leakage or tube anastomosis. If the urethro-enteric anastomosis is under tension, certain sequential steps should be performed; careful selection of bowel loops, opening of the peritoneum covering the mesentery, releasing the mesenteric fat, removing the sigmoid colon out of the pelvis, reducing the steep of trendelnburg positioning angle, perineal pressure and freeing the right colonic junction and moving the ileum and the right colon downwards.
Stage V: Post-operative management
Meticulous postoperative care and life-long follow up are very critical for good long-term results [23]. In the immediate postoperative setting, thrombosis prophylaxis by subcutaneous heparin should be administered preferably in the arm instead of the thigh to prevent lymphocyte. The neobladder should be irrigated gently and frequently to avoid mucous accumulation. Bowel stimulation with para sympathomimetics should be instituted from day 2 or 3. Serial body weight and blood gas analysis should be measured [3].
Regarding the catheters and stents, the time of their removal is debated. Originally, the ureteric catheters, supra-pubic tube and the urethral catheters were removed at about 10, 12 and 21 days respectively. However, in updated experience of some experts, they stated that they could be removed at days 5-7, 8-10 (after cystogram) and at 10-12 respectively [3].
Following catheter removal, patients are carefully instructed how to void. Initially, in a sitting position every 2 h during the day by slight increase the intra-abdominal pressure. Thereafter every 3 h; later every 4 h until approaching a capacity of 400-500 ml. use of alarm clock at night to avoid nocturnal enuresis.
Serial check of the residual urine, urine analysis, venous blood gas analysis and supplement of bicarbonate (2-6g) and salt whenever indicated should be performed. Long-term follow- up is very important to early detect and manage the following events; metabolic complications (vitamin B12, electrolytes, base excess), voiding complains (incontinence, difficulty and increased mucous production due to infection), occurrence of delayed complications (neobladder outlet obstruction or uretero-enteric strictures) and oncological failure [3].
Stage VI: Management of complications
RCX is the most difficult urologic procedure with a wide range of peri-operative complications even with most experienced surgeons with a post operative complications rate of 25-57%. However, the rate of severe and lethal complications is acceptably low with in-hospital mortality of 3% and re-operative rates of 2.3-17%. The complications should be classified by the five- grade modification of the original Clavien system [3].
Management of neobladder complications requires patience and expertise. It could be managed either by endoscopic, laparoscopic or open surgery routes. But, the minimally invasive endoscopic management should be tried first, whenever possible. As it saves a lot of hazards that may occur with laparoscopic or open surgery due to marked intra-abdominal adhesions and allows the patient to return faster to normal daily activity. Uretero-enteric stricture, pouch stones, recurrent neobladder tumors, urethral recurrence and urethro-enteric stenosis all could be managed endoscopically [28].
Go to
Conclusion
In conclusion, RCX and OBS is an advanced multi-steps urologic procedure. To make it easy, certain precautions should be followed. We should carefully select our patients. Standard RCX and extended PLND should be performed. Dorsal vein ligation and urethral stump preparation should be done cautiously as they are risky key steps. Familiarity with other urinary diversion techniques is important for the urologistas intra-operative findings may change the plane. Regular life-long follow up for delayed complications is important. For best results, a regular skilled operative team and a high volume well- equipped hospital with high case load are mandatory.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#Juniper Publishers#JuniperPublishers#Juniper Publishers LLC#Juniper Publishers Review#juniper publishers group#urology#Open access journal of Urology#Nephrology#open access Journal of Nepharology#open access journals
0 notes
Text
How to Prevent Wrinkles – Expert Advice
The skin is an organ that constantly renews itself. The rate of renewal of skin cells slows down with time. In this article, Dr. J. Shetty providing you the expert advise about how to prevent wrinkles and delay the skin ageing through using natural ingredients and healthy lifestyle. Aging is linked to impaired cell repair mechanisms. Internal factors such as hormones play an important role in skin aging. Receptors of skin cells (keratinocytes, fibroblasts) lose, over time their ability to process the hormonal inputs necessary for their development. The decrease in hormonal activity further accentuates skin aging.
External factors related to the environment and hygiene of life are strongly involved in the acceleration of skin aging. Sun and tobacco can weaken skin cells: they become more fragile multiplies less easily.
While anti-aging medicine delays the body and skin effects of aging, the speed of appearance of these signs is therefore strongly linked to sun exposure since childhood and tobacco consumption.
THE EFFECTS OF THE SUN ON SKIN AGING
The sun is useful to health for its anti-rickets action related to UVB (UVB stimulates the synthesis of vitamin D in the skin). The sun is the first enemy of the youth of the skin.
The danger of ultraviolet rays from the sun is known. Under the effect of ultra-violets, skin cells become fragile and can no longer make a quality “fabric”. Under the effect of UV the skin is stiffer, thinner, less resistant. The body accumulates the effects of UV over the years. Skin aging will depend on the total dose of photons received and natural resistance of each.
EFFECTS OF TOBACCO ON SKIN AGING
Tobacco significantly accelerates the aging of the skin. Clinical studies have shown that tobacco is an independent factor of skin aging. Studies show the importance of the dose of tobacco. Women would be more affected. These effects are dissociated from solar exposure and are enhanced by UV.
The Effects of Smoking are Multiple:
Alteration of the basic structures of the dermis (hyaluronic acid) cause poor elastin production,
Decreased water in the stratum corneum,
Decrease in collagen synthesis by assignment of connective tissue fibers,
Acceleration of destruction of elastic fibers.
HOW TO PREVENT WRINKLES
Generally used to combat the adverse effects of time, anti-aging medicine is a preventive medicine. Anti-aging medicine is comprehensive and proposes to act on internal factors: nutrition, micro-nutrition, hormonal system. Aesthetic Medicine provides external aids to prevent and repair skin aging. It allows to delay the heavy interventions of medicine or cosmetic surgery (prevention) and to rejuvenate facial features and skin (repair).
WHEN SHOULD ANTI-AGING MEDICINE BE USED?
It is better to act from an early age, before the appearance of signs of aging in order to stimulate the tissues and keep its health and youth capital. Aging of the skin is natural and begins at the exit from childhood. Anti-aging medicine is often solicited by from the age of 40, when the signs of aging begin to be visible and impair well-being.
Aging is an inevitable phenomenon, aesthetic medicine complements the physiological and individual approach by providing support to cells and tissues to prevent skin aging and delay the appearance of wrinkles.
AESTHETIC MEDICINE AND SURGERY
The self-image can be altered by the signs of the weather visible on the parts of the skin that are daily exposed to the eyes. Social and mental well-being can be degraded and lead to dysfunctions in daily life and relationships, thereby limiting activities or projects.
The use of medical techniques to combat aging or skin rejuvenation is a complementary solution to life hygiene.
ANTI-AGING TECHNIQUES
Anti–aging medical techniques make it possible to prevent, delay and correct the signs of weather on the skin. These techniques, whether chemical (peeling) or physical (energy sources such as the LASER) can act on the effects due to time (loosening of the skin) and on the effects due to the sun (stains on the skin).
Peeling or dermabrasion can indirectly stimulate cell renewal by accelerating the cleansing of dead skin. Skin cells can be destroyed to the dermis. These techniques can be very aggressive, they bring random results and have adverse effects.
Triggered laser photorejuvenation (Q-Switch) is a preventive intervention, indicated for people of all ages allowing the skin to make new collagen. Collagen is the main protein of connective tissue (supporting tissue). It brings strength and flexibility to fabrics. Triggered laser photorejuvenation (Q-Switch) creates a “neocollagenesis” by specific heating of the vessels of the dermis. The production of new collagen by the skin will allow it to keep its tone and delay the installation of facial wrinkles.
Non-ablative fractional photo thermolysis (NFP) is a method that diffuses energy (photons) on the skin through small microscopic treatment Zones. The laser is passed on the skin, deep heating of the very small areas only. Affected tissues can be repaired without significant side effect. Skin not affected by light is not altered, this which contributes to the rapid healing of the treated surface. It allows to treat wrinkles and fine lines, pigment and vascular disorders. It also acts on the texture of the skin.
The principle of action of fractional photothermolysis is the rise in temperature of the target area, it is a thermal effect. Thermal effect: mechanism of action most exploited in laser treatments, it is a complex process that can be broken down into three stages: conversion of light into heat, heat transfer and tissue reaction related to temperature and warm-up time.
The wavelengths used for nFP are close to infra-red and are absorbed by water. NFP techniques offer great flexibility in the choice of energy doses deployed. Treatment can easily be adapted to each person according to the desired results. The individualization of the protocols also allows to control the treatment sequences. Non-ablative fractional photo thermolysis (NFP) is a safe technique that benefits from 10 years of practice and recoil.
Combined Techniques: Several laser and light techniques can be combined for this indication. The triggered laser photo rejuvenation (Q-Switch) is completed episodically by a non-ablative fractional LASER treatment. In addition to the benefit of “neocollagenesis” induced by the 2 lasers, the non-ablative fractional LASER allows an improvement of existing wrinkles.
amzn_assoc_placement = "adunit0"; amzn_assoc_tracking_id = "acnevulgaris2-20"; amzn_assoc_ad_mode = "manual"; amzn_assoc_ad_type = "smart"; amzn_assoc_marketplace = "amazon"; amzn_assoc_region = "US"; amzn_assoc_linkid = "fe6343a8aeddaa14b3c9d89bb6e1cc88"; amzn_assoc_design = "in_content"; amzn_assoc_title = "Anti Ageing Products"; amzn_assoc_asins = "B00OQQLNG4,B07TPLZ7F3,B07QXBS32K,B002E1116K";
How to Prevent Wrinkles Using Natural Supplements
Here we share with you the best supplements and most effective natural remedies to prevent wrinkles. In order to age in beauty and avoid vitamin and mineral deficiencies, here are natural supplements and remedies that are recommended by specialists to strengthen your skin health and to prevent wrinkles.
Vitamins C and E
Vitamins C and E are antioxidants that fight the effects of free radicals. Vitamin C and flavonoids act within the cells themselves, while vitamin E protects the fat membrane around them; it strengthens the immune system of older people, thus keeping away the risk of age-related conditions, such as cardiovascular disease, certain forms of cancer and, perhaps, Alzheimer’s disease. Other antioxidants are probably even more effective: green tea (long touted for its effects on longevity), selenium (40 µg 2 times a day) and Grape Seed Extract (100 mg 2 times a day), which contains many antioxidant flavonoids.
Folic Acid
Folic acid, a Vitamin of Group B, maintains the level of red blood cells in the blood, protects the heart and contributes to the proper functioning of the nervous system. Its action is promoted by vitamin B12, which contributes to the proper functioning of the brain. Elderly people have an interest in taking this vitamin as a supplement, since many of them no longer assimilate vitamins brought from food. However, a deficiency of vitamin B12 may cause nervous disorders, accompanied by depression. It is probably better to take B vitamins in the form of polyvitamins and minerals that strengthen immune defenses and keep away the risk of infection in the elderly.
Beer
Brewer’s yeast, which brings all the vitamins of Group B, is also an excellent supplement to compensate for the metabolic deficiencies of aging.
Caution: if you are undergoing medical treatment, consult your doctor before taking any supplements.
Natural Remedies
1. Green Tea
Dose: one infusion (3 to 5 min) per day, one sachet in a large cup of boiling water.
2. Vitamin C / Flavonoids
Dose: 50 mg of vitamin C and 100 mg of flavonoids 2 times a day.
Note: Also eat 5 servings of fruits or vegetables a day.
3. Vitamins E
Dose: 20 mg per day.
Attention: It is better to take vitamin E in natural form (wheat germ, oil fruits…).
4. Folic Acid / Vitamin B12
Dose: 400 µg of folic acid and 5 µg of vitamin B12 vitamin B12 1 time per day.
Note: Vitamin B12 is always presented as a polyvitamin complex.
5. Calcium / Magnesium
Dose: 50 mg of calcium and 250 mg of magnesium Magnesium 1 or 2 times a day.
Note: These supplements strengthen bones; vitamin D can be added to it at a rate of 10-15 µg per day; refrain from magnesium in case of kidney disease.
6. Fish Cartilage and Collagen
Dose: 250 to 500 mg per day in tablet form.
Note: Exist in pure form or mixed with fish products that contribute to the reconstruction of cartilage.
7. Brewer’s Yeast
Dose: 2 to 4 capsules per day.
Vitamin E could prolong human life. A study conducted by the American Institute of Gerontology showed that the risks of dying from cardiovascular disease were half lower in people taking vitamin E supplements. According to another study, this vitamin strengthens the immune system of individuals over 65 years of age. Also, A study conducted on a group of elderly people demonstrated the existence of a link between the presence in the blood of high doses of antioxidants (beta-carotene and vitamin C) and better memorization ability.
Did You Know?
Although appetite decreases with age, the need for vitamins, minerals and other nutrients increases with age. In addition, physical exercise, including walking at a rate of 4-5 km per day, is one of the best ways to combat aging. Before taking supplements and natural remedies, consult your doctor or pharmacist.
Conclusion
This article about How to Prevent Wrinkles is written with the support of Dr. J. Shetty, Skin Specialist. If you like this article please share it and subscribe our beauty magazine for latest beauty trends and tips by experts.
Most Popular
Tips
How to Prevent Wrinkles – Expert Advice
June 6, 2020
Home Remedies
Nutritional Supplements – 15 Most Effective Nutritional Supplements
June 6, 2020
Home Remedies
Natural Skin Care Secrets for Radiant Glowing Skin
June 6, 2020
Treatment, Types of Acne
Fungal Acne – The Fastest Way to Treat Fungal Acne
June 5, 2020
Treatment
How to Get Rid of Acne Fast?
June 5, 2020
Acne, Home Remedies
Acne on Face – The Fastest Way to Cure It
June 3, 2020
DIY
ACNE SPOT TREATMENT DIY BY EXPERTS
June 3, 2020
Types of Acne
What Are the Different Types of Acne?
May 31, 2020
Acne
Acne Vulgaris ICD 10 – 10th Revision L70.0
May 30, 2020
Treatment
Acne Vulgaris Treatment – Get Rid of Acne Vulgaris Fast
May 30, 2020
Types of Acne
Acne Vulgaris – An Overview
May 30, 2020
Acne
Acne – An Overview, Causes Treatment and Prevention
May 29, 2020
Acne
Adult Acne: An Adult Dilemma as Well
May 29, 2020
Acne
Acne – An Overview and Few Facts You May Not Know
May 28, 2020
Treatment
Acne Cure for Sure, Get Glowing Skin After Acne
May 28, 2020
The post How to Prevent Wrinkles – Expert Advice appeared first on Acne Vulgaris.
from WordPress https://ift.tt/3f1ipHL via IFTTT
0 notes
Text
Our Scalp Block Results in Craniotomy Cases-Juniper Publishers
Abstract
Aim: The aim of this study is to investigate the effect of scalp block performed with 0,5% of bupivacaine in craniotomy cases in preventing hemodynamic response due to the incision and its effect on postoperative analgesia and the need of analgesics.
Materials and method: The study was planned as a randomized, placebo controlled, double-blind study. 40 patients between the ages of 40-85 with ASA II-III classification were included in the study for elective craniotomy after the approval of the ethics committee and informed consents of the patients were received and they were separated into two groups (Group S: 20ml 0,9% normal saline, n=20), (Group B: 20ml0, 5% Bupivakain, n=20). Scalp block was performed 15 minutes before craniotomy. The mean arterial pressure (MAP) and heart rate (HR) of the patients wererecorded. Postoperative complications observed in the recovery room (bradycardia, hypotension, drug allergy, nausea, vomiting) were recorded. Pain was evaluated in postoperative conscious patients in the 2, 4, 8, 12, 16 and 24th hours with a 10cm visual analogue scale; and it was planned to administer 75mg of intramuscular meperidine if the VAS score was 5 and above in the postoperative period.
Result: During the craniotomy the MAP and HR values of the patients in Group S were significantly higher than Group B (p<0.05 respectively p=0.002, p=0.029). The VAS scores were also significantly higher in Group S compared to Group B in the postoperative 1, 2, 4, 6 and 12th hours (p<0.05 respectively p=0.022, p=0.031). Use of additional medication in Group S due to perioperative hypertension and tachycardia was significantly higher in comparison with Group B (p<0.001). Similarly, in terms of postoperative analgesic need, Group B had significantly less need for analgesics. Regarding the complications, however, no significant difference was found between the two groups.
Conclusion: In conclusion, scalp block ensures the stabilization of hemodynamic responses by reducing the sympathetic response in the intraoperative period in craniotomy cases and helps reduce the pain in the early postoperative period. We think that bupivacaine can be effectively used in scalp block procedures.
Keywords: Scalp block; Craniotomy; Bupivacaine
Introduction
The aim of neuroanesthesia is to prevent the increase of intracranial pressure without distorting the cerebral autoregulation and to ensure convenient surgical conditions and a safe anesthesia for the patient by maintaining a sufficient level of cerebral perfusion pressure (CPP). Anesthetic agents have obvious effects on cerebral metabolism, cerebral blood flow, cerebrospinal fluid (CSF) dynamics, intracranial volume and pressure [1]. As the intracranial pressure is directly related to the blood pressure, it is crucial to prevent the elevation of blood pressure due to any reason whatsoever in craniotomy patients. Radical elevations in systemic arterial pressure may temporarily distort cerebral autoregulation and, if not prevented, may cause cerebral edema by increasing the pressure in cerebral capillaries. Particularly, in interventions related to lesions involving intracranial areas, the detrimental effects of acute hypertension are more obvious as intracranial compliance is already decreased. Especially if the autoregulation capacity of cerebral vessels is already compromised, this increase will lead to an increased intracranial pressure [2]. Since increased intracranial pressure may cause a decrease in cerebral perfusion pressure or a shift effect in the brain, it should absolutely be prevented before durotomy [3].
Painful stimulants and sudden increases in blood pressure and heart rate cause herniation, cerebral aneurism and arteriovenous malformation rupture by increasing the intracranial pressure, and lead to ischemia in subarachnoid hemorrhage patients, who develop vasospasms, and an increase in the potential morbidity risk. Furthermore, hemodynamic instability will lead to adverse effects in those with atherosclerotic heart disease in the preoperative period [4,5]. Cranial surgical procedures involve continuous change in the intensity of painful stimulants, therefore they require a very close monitoring of the level of anesthesia [3,6].
The aim of scalp block is to block the nerves innervating the scalp at their exit points from the scalp before they form branches with the use of local anesthetic agents. Minor and major occipital nerves innervating the scalp, supraorbital and supratrochlear nerves, zygomaticotemporal nerve, auriculotemporal and major auricular nerve are blocked. As a result, the transmission in the fibers located in the nerve trunk in the area where the drug is delivered is blocked. Scalp block was first defined by Pinosky and bupivacaine was used as the local anesthetic agent. The most frequently used agent has also been bupivacaine in further studies, however there are also some studies performed with lidocaine, ropivacaine and levobupivacaine [5,7,8].
Mainly bupivacaine, ropivacaine and lidocaine have been used for scalp block in the studies [8-10]. Scalp block is a difficult technique requiring the use of local anesthetics in high volumes, which in turn increases the risk of local anesthetic toxicity in patients [9,11]. In awake craniotomies, an average of 150-175mg of levobupivacaine is used for the scalp block and maximum concentration measured in the plasma is 0.98-2.51µg/ml and the time needed to reach this level of concentration is 5-15 minutes and no central nervous system or cardiovascular system toxicity is observed at this level of concentration. It is reported that post-craniotomy pain is less than the pain experienced after operations such as lumbar laminectomy or fascial reconstruction ]12[. However, in contradiction to the general opinion, moderate or severe pain after craniotomy is reported to be quite common and it is observed that this pain is very intense particularly in the first 2 hours after craniotomy [13]. For the treatment of this pain, either local anesthetics are injected to the scar area or systemic nonsteroidal anti-inflammatory agents, drugs such as ketamine, opioids, or tramadol are given. In the meantime, there is still an ongoing search for an ideal analgesic agent and or approach in craniotomy cases complaining of severe pain. If the patient is conscious and have a perception of pain, postoperative analgesia should absolutely be used [14-16]. Bupivacaine is an amide type local anesthetic and was developed by Ekenstom et al. in 1963, it is available as hydrochloride salt in the market. It provides analgesia without motor block in low densities. Since it is highly fat-soluble, its systemic absorption is slow. It is metabolized in the liver except for a small portion excreted through the kidneys. It becomes effective within 5-10 minutes. This duration may reach up to 20 minutes in caudal and peridural injections. Motor and sensorial blockade may last up to 3 hours. It reaches maximum plasma concentration after 30-45 minutes. Its half-life is 9 hours in adults. It is one of the longest acting local anesthetics (5-16 hours). Scalp block is a method used to relieve pain in the early postoperative period and to help ensure hemodynamic stabilization in the intraoperative period [17]. In this study we aimed to investigate the effect of scalp block performed with bupivacaine in elective craniotomy cases in preventing hemodynamic response due to incision, and its effect on postoperative analgesia and the need for analgesics.
Materials and Method
The ethics committee approval was received from the Clinical Studies Ethics Committee of Samsun Ondokuz Mayis University, Faculty of Medicine (Approval number B.30.2.ODM.0.20.08/1192). The study was planned between June/1/2015-December/31/2015. The study was started after receiving the consents of the patients planned to be included in the study. 40 patients, who were accepted at the Neurosurgery clinics of Ordu University Training and Research Hospital and Ordu State Hospital for elective craniotomy due to intracranial mass, were included in the study. Our study was a multicenter, randomized, placebo controlled, double-blind study. 40 patients to undergo elective craniotomy in the study were between the ages. of 40-85, in ASA II-III groups according to the risk classification of the American Society of Anesthesiologists (ASA) defining the physical condition of the patients. All the patients were informed about the study beforehand, and written consents were received from the volunteers who accepted to participate in the study. Those who had a systemic disease under ASA IV risk class, who had allergy against bupivacaine, advanced stage organ failure, alcohol and substance addiction and who were below the age of 40 and over the age of 85 were excluded from the study In our study, patients were not excluded from the study and all data were analyzed. Attached consort diagram drawn for our scientific work (Figure 1).
The patients were randomized with the sealed envelope method before the induction into 2 groups each comprising 20 patients; 20ml of 0.5% bupivacaine (Group B) and 20ml of 0.9% normal saline as the control group (Group S). Preoperative routine monitoring of the patients was done with Datex-Ohmeda Cardiocap™/5 (GE, Finland) device, followed by electrocardiogram (ECG), peripheral oxygen saturation (SpO2) and noninvasive blood pressure monitoring. Before the induction of anesthesia all the patients were premedicated with 0.05mg/kg of intravenous midazolam. After the induction of anesthesia with 2-3mg/kg of intravenous propofol, 2µg/kg of intravenous fentanyl and 0.6mg/kg of intravenous rocuronium, invasive arterial monitoring was performed by inserting a 20G intra-arterial cannula into the radial artery. Anesthesia was maintained with 6mg/kg/h of propofol infusion, 0.15mg/kg of intravenous rocuronium and 0.25µg/kg/min of continuous intravenous infusion of remifentanil. The patients were exposed to mechanical ventilation to reach an EtCO2 level of 30-35 mmHg with an air mixture of 50% O2. Once the baseline hemodynamic values were recorded before and after the induction, scalp block was performed. Skull-pin head holder was placed 5 minutes after the block was done. The medication to be used for the scalp block was prepared in a 20ml syringe by an anesthesiologist, who would not attend the surgery. 20ml of normal saline was put in the syringe for Group S. After being numbered according to the results of randomization, the responsible anesthesiologist made the injections with a 23G needle on the outer layer of the skull by inserting the needle into the skin with a 45° angle. Supraorbital and supratrochlear nerves were blocked by the injection of a 2ml solution on the bilateral supraorbital notch above the eyebrows. Bilateral auriculotemporal nerves were blocked by injecting a 2ml solution at 1.5cm anterior to the ear at tragus level. Bilateral postauricular nerves were blocked by injecting a 3ml solution at 1.5cm posterior to the ear at tragus level. Finally; the major, the minor and the third occipital nerves were blocked by injecting a 3ml solution at the intersection point of the midsection of the line between protuberentia occipitalis and mastoid process, and the upper nuchal line. Skull-pin head holder was placed by the neurosurgeon 5 minutes after the block.
Regarding the systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MAP), heart rate (HR), peripheral oxygen saturation (SpO2) and end- tidal carbon dioxide (ETCO2) of the patients; the time when the patient was taken into the operating room before the scalp block was accepted as 0 min (= control value). After the scalp block was done, in the 1st, 5th and 10th minutes and then in the 20th, 30th, 40th, 50th, 60th, and 70th minutes, all the parameters were recorded until the end of the operation with 10-minute intervals.
Postoperative pain was evaluated in patients, who were conscious after the operation, in the 2nd, 4th, 8‘h, 12th, 16th and 24th hours with a 10cm visual analogue scale (0 is no pain, 10 is the worst possible pain). It was planned to give 75mg of intravenous diclofenac sodium to patients with a VAS score above 2 and 75mg of intramuscular meperidine to patients with a VAS score above 5. Postoperative analgesic needs and the amount of analgesics used were recorded.
Decrease of SpO2 below 94% for 45 seconds was accepted as hypoxia and elevation of ETCO above 45mmHg was assessed as hypercapnia. Hypertension was accepted as an increase of SBP by 20% above the control value and tachycardia was defined as a heart rate of at least 20% above the control value, and it was planned to administer 2µg/kg of intravenous fentanyl and to increase the propofol infusion dose to 9mg/kg/h. It was planned to administer 0.01mg/kg of bolus intravenous nitroglycerin if SBP and HR were still 20% above the control values.
Hypotension was accepted as an SBP value of 20% of the control value and less and 5-10mg of intravenous ephedrine was planned to be administered. Bradycardia was assessed as 20% below the control value or a value less than 40beats/ minute, and 0.5mg of intravenous atropine was planned. 10mg of intravenous metpamid was planned for the treatment of postoperative nausea and vomiting, and in the case of blurred vision or tinnitus the plan was to keep the patient in the recovery room for a longer period of time and observe.
SPSS for Windows 21.0 package program was used for the statistical analysis of this study. For measurable parameters (age, weight, amount of remifentanil, duration of anesthesia, duration of operation) the Kolmogorov-Smirnov test was used in order to identify whether the distribution was normal or abnormal. For those with normal distribution, Student t test was employed in independent groups to see whether there were differences between the groups. Data, such as gender and ASA, were analyzed with the Chi-square test. Heart rate and MAP data were assessed with repeated measures analysis of variance. In cases of differences, the comparison between the groups was done with the intergroup Posthoc-Scheffe test. Intragroup control values of HR and MAP, for which it was determined that the time factor was crucial according to the repeated measures analysis of variance, were compared by using the Post hoc Bonferroni test. Mann-Whitney U test was employed for the comparison of postoperative VAS scores between the two groups. For statistical analyses p<0.05 was accepted as significant.
Results
None of the 40 patients in the study was excluded from the study. The age, body weight, height, gender, ASA classification of the patients, duration of anesthesia and operation, the total amount of remifentanil used during the operation were found to be similar. All the patients were referred to the surgical intensive care units of Ordu University Training and Research Hospital and Ordu State Hospital postoperatively (Table 1). Demographic characteristics of the groups did not indicate any statistically significant difference.
The average values of the heart rate (HR) according to the time of measurement are given in Table 2. While there was no difference between the groups in the control measurements in terms of average heart rates, the HR value after intubation was found to be significantly lower in Group B as compared to Group S (p<0,05). When the intragroup HR values measured at different times were compared according to the control value, it was observed that the average HR values were not statistically different from the control HR average values in both groups. The average values of the mean arterial pressure (MAP) according to the measurement times are given in Table 3. While there was no significant difference between the groups in terms of mean arterial pressure values in the control measurements, the MAP values acquired in the intraoperative 20th and 30th minutes after the scalp block were found to be significantly lower in Group B compared to the control group (normal saline group) (p<0,05). When the intragroup differences were investigated, on the other hand, intraoperative MAP values measured in the 10th, 20th, 30th, 40th, 50th, 60th, and 70th minutes after the scalp block in Group B were observed as significantly lower than the control values (p<0.05).
*p<0.05: in comparison with Group S.
*p<0.05: in comparison with Group S, µ: p<0,05: in comparison with the control measurement values.
**p<0.01: in comparison with Group S
Postoperative pain assessment results of the conscious patients according to the visual analogue scale are given in Table 4 and Figure 2. The VAS scores acquired in the postoperative 30th min, 60th min, 2nd, 4th, 6th and 12th hours were found quite significantly lower in Group B as compared to Group S. The values in the recovery room and postoperative 24th hour were close to the statistical significance level in Group B (p=0.05 and p=0.06 respectively). No serious complications such as nausea, vomiting, bradycardia, and hypotension was observed in any of the patients in the postoperative period. In Group B, except for the patient, who needed 75mg of diclofenac sodium, no patients required meperidine. In Group S, on the other hand, 12 patients (60%) required meperidine in addition to diclofenac sodium particularly in the postoperative 12th and 24th hours.
Discussion
There is a common belief that those undergo neurosurgery suffer from minimum postoperative pain and need analgesics. While it is obvious that this group of patients experience relatively less pain when compared to those underwent orthopedic surgery or thoracic surgery, more than 60% of these patients feel moderate to severe postoperative pain. In a study conducted by Benedittis et al.90% of the patients suffered from post-craniotomy pain in the first 12 hours, which sometimes extended to 48 hours [18]. Our results overlap with those reported in the study of Benedittis et al. Likewise, in our study, there were many patients with a VAS score of 5 and above in the control group (normal saline group, Group S) particularly in the 12th and 24th hours. In a retrospective study conducted by Quient et al. postoperative pain in elective craniotomy patients was assessed in the first 24 hours. In the first 2 postoperative hours, 18% of the patients complained about severely distressing pain; 37% of the patients had severe, 29% had medium and 4% had mild pain. Only 12% of the patients did not describe a post-craniotomy pain in the first 24 hours [19]. Persistent post-craniotomy headache has also been identified and its incidence increases with postoperative unsuccessful analgesia [20,21]. In a study by Kaur et al. [21] 22 out of 126 supratentorial surgery patients developed persistent headache. 7 of these cases (5.6%) had headache for a period of longer than 2 months but shorter than 1 year; 15 cases (11.9%) had headaches for more than a year in the postoperative period.
In neurosurgery cases, laryngoscopy, skull-pin applications, interventions to the periosteum and dura cause painful stimulants. Even in cases with sufficient anesthetic depth, skullpin application and skin incision lead to acute hypertensive response [2,22]. Following the skull-pin placement, efferent pain sensation generated from the periosteum results in severe acute hypertensive response due to sympathetic system activation and eventually, intracranial pressure increases . This technique, which was defined for the first time by Pinosky et al. [10] and had not been implemented in practice before, was compared in a prospective, randomized, double-blind study in terms of the effect of scalp block performed by using 0.5% bupivacaine and normal saline on hemodynamic response to skull-pin placement and on the anesthesia need; and they were able to show that scalp block was successful in controlling the hemodynamic response to skull-pin placement. In our study, we followed the exact description of Pinosky et al. [10] while performing the scalp block. Lee et al. investigated the effect of scalp block performed with 0.25% bupivacaine under general anesthesia on hemodynamics and plasma catecholamine metabolites. 16 elective craniotomy patients were included in this prospective, randomized, double-blind study. One group underwent scalp block procedure with normal saline under general anesthesia induced with isoflurane and 50% N20-02, while the other group underwent the same procedure with a total of 20ml of 0.25% bupivacaine. Looking at the heart rate and mean arterial pressure measurements, it was revealed that scalp block led to more stable hemodynamics and decreased the need of intravenous or volatile anesthetics [23]. We used 0.5% bupivacaine and obtained more stable perioperative hemodynamics just as Lee et al. did in their study.
Gazoni et al. [8] compared perioperative results of the scalp block performed with ropivacaine in patients, who had supratentorial brain tumor, with remifentanil. In the prospective, randomized, double-blind study, while one group received 0.5% ropivacaine during the scalp block procedure, theother group received remifentanil infusion. Although, it was reported that scalp block did not bring along significant advantages in terms of postoperative pain and narcotic analgesics need when compared to remifentanil infusion, it was observed that hemodynamic parameters (MAP, HR) were more stable with the scalp block procedure.
Geze et al. compared the effects of scalp block and local infiltration on hemodynamics and stress response in craniotomy cases with skull-pin placement. In this prospective, randomized, placebo-controlled study, one group had scalp block with 0.5% bupivacaine and another group had local anesthetic infiltration with 0.5% bupivacaine; in the control group, on the hand, in order to prevent excessive hemodynamic responses, after an IV bolus of 0.5µg/kg remifentanil or a loading dose of 500µg/kg/ min esmolol, an IV infusion of esmolol 50µg/kg/min for 4 min was administered. In the study, it is reported that in the scalp block group, increase in blood pressure and heart rate due to skull-pin placement was prevented; there was no need for an additional anesthetic and antihypertensive agent, and blood pressure and heart rate were more stable when compared to the local infiltration and the controlgroups. When the groups are compared in terms of their metabolic and endocrine responses to surgery, stress response was significantly lowered after skull-pin placement in the scalp block group in comparison with the control group. In our study, we also used 0.5% bupivacaine and obtained well-matched results with that of Geze et al. We also observed perioperative hypertension and tachycardia in patients included in the normal saline group. 86% of the patients have pain with somatic features indicating that the source of pain is pericranial muscles and soft tissue. It is also known that local anesthetics administered before the skin incision on scalp have preemptive analgesic effect [24]. Therefore, scalp block is a technique that can be preferred to be used as a stand-alone analgesic method or to decreasethe dose of analgesics [25]. Taking all these remarks into account, we interviewed our conscious patients in the postoperative 30thmin, 1st, 2nd, 4th, 6th, and 24th hours on VAS and the use of additional analgesics. Our VAS scores were significantly lower in the bupivacaine group compared to the normal saline group.
Ayoub et al. [26] investigated the efficacy of scalp block in a group of 50 patients following remifentanil-based anesthesia. In this double-blind study, anesthesia was induced with 1-3mg/ kg of propofol and 1.0µg/kg of IV bolus remifentanil; followed by 0.1µg/kg/min of intravenous remifentanil infusion. The patients were randomized into two groups; one group having scalp block with bupivacaine or lidocaine and the other group having 0.1mg/kg intravenous morphine during dural closure at the end of the surgery. As an additional analgesic agent, codeine was administered subcutaneously in both groups. Both groups had similar pain scores. There was no significant difference between the two groups in terms of the total dose of codeine administered and the first codeine dose. While there was no difference between the groups in terms of confusion, nausea and vomiting was higher in the morphine group. The authors indicated that scalp block offered the same analgesic quality with a postoperative hemodynamic profile similar to morphine. Scalp block is an adjuvant method that can be used in order to avoid nausea and vomiting experienced with opioids [26]. Similarly, Bala et al. performed scalp block in 40 supratentorial craniotomy patients with bupivacaine or placebo following skin closure and they used intramuscular diclofenac or intravenous tramadol as analgesic. Patients without a scalp block had moderate to severe pain and had more frequent needs of additional analgesics. In this study too, it was revealed that the pain scores recorded after 6 hours were equal [27]. In our study, on the other hand, we obtained pain-free postoperative periods of over 12 hours, even extending to 24 hours. Scalp is a highly vascularized area, there are some studies analyzing the rate of transmission of local anesthetics applied to this area to the systemic circulation [7,28]. In our study, bupivacaine was administered very slowly in order to avoid drug toxicity, as it was required in high volumes in scalp block procedures and prior to the administration of bupivacaine, needle aspiration was performed in order to avoid accidental intra-arterial injection. After making sure that there was no blood, local anesthetic agent was injected. Although the patients were not monitored for QT intervals, there was no arrhythmia or asystole observed in routine ECG monitoring. In the postoperative period, no findings such as blurry vision, tinnitus or convulsion indicating systemic toxicity were reported.
Conclusion
In conclusion, in craniotomy cases, scalp block provides stabilization of hemodynamic responses by decreasing sympathetic response intraoperatively and helps reduce the early postoperative pain. Therefore, we believe that scalp block should play a more important role in anesthesiology practices and should be performed in all craniotomy patients.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
Omnisubjectivism and Predestination
Christian theologians generally believe that God is not altered in relation to the World. (That is to say, whenever there is an encounter between God and creation, the change is always on the side of creation). This of course includes the act of creation, since to say otherwise implies God was incomplete without creation. (and that has implications for the essential goodness of creation; if creation is necessary for God’s own completion, creation itself might be worthless, only serving to perfect God. However, if creation is unnecessary and created by a good God, then it must be good in itself; for it can serve no other end).
However, Christian theologians also generally believe that God, in some sense, could choose which world to create; he did not need to create this world, or even a world that particularly resembles this world. (at the very least, Christian theologians tend to believe God could have created a world that only contains spiritual entities or only contains physical objects, which would be quite different from our own. Moreover, as some more rigorous science-fiction or fantasy alludes to, it seems quite possible that the world could be very different even through modifying certain fundamental constants or through introducing new kinds of fundamental forces).
Christian theologians also generally believe that human beings have some level of free will. Free will here does not necessarily mean “absolutely undetermined wills” but rather that human choice is a real causal element in the universe. At the minimum, this commits the standard Christian theologian to something like an emergantist account of the will; the will at the very least as to be among the things you would include in a final account of the world, and the failure to include it would make your description of the world wrong.
However, this creates the following oddity: God chooses a particular world to create, and that results in various new facts being true, among them the existence of time itself. For God to choose rationally, he must know the implications of what he is choosing, otherwise he is simply creating “the big bang” and letting the dice fall where they may (and while such a concept is appropriate to a demiurge, such a being would not be the fundamental source of all being, unless all being is just quarks and everything else is epiphenomena. But the Christian cannot believe that). But knowledge of this type would appear to require perfect, atemporal and unchanged knowledge of future free actions, and all future free actions. (Since God is unchanging).
How can such a thing be true without falling into radical determinism? God’s foreknowledge is necessary for all goods to participate in him and to truly be good gifts (and also, since temporality at least in the mode that we know is essentially tied with matter and energy in complex ways, the only way to preserve an immaterial God is for God to be eternal; either God is free from time and space and matter, or he is confined to all three). But it seems like future free actions should be unpredictable to some degree if persons are truly free.
I think the best solution here is Zagebski’s idea of God having, along with the other omni-attributes, something she calls omni-subjectivism. On Zagebski’s account, insofar as my experiential knowledge of myself (what-it-is-like to be me) is a good and a kind of knowledge, then it must find its ultimate completion in God; since there is no knowledge that does not originate in him. (We tend to collapse this distinction, and think that only Being originates from God, with the Goodness, Truth, and Beauty of individual beings being epiphenomenal from the gift of Being. However, while there might be some conceptual structure between the transcendentals, in God they are identical, and there is no ontological priority between them [as God is simple], and in the truth of each being [its self-disclosure to investigating minds and intellects] and in their goodness [its appeal to those who desire it in various ways] come as directly from God as their being. Self-knowledge is a particular modality of that, but an important modality. In a certain sense, knowing beings are both determined by their actual existence and their beliefs, habits, experience, and concepts about their existence (among other things, of course). [to use a rather common trope on this site; the idea of “coming out to oneself” would be unintelligible without something like this as a background belief.]. However, this means knowing objective facts about a person is not necessarily enough to know “them”, knowledge of them requires knowing how those facts impact their own self-knowledge and knowledge of the world; how it shapes their mode of being-in-the-world (to mangle Heidegger).
So purely objective knowledge is not enough to be a complete knower; and insofar as God by stipulation is a complete knower, he must know what it is like to be me. [indeed, God must know what it is like to be me better than I do; insofar as my self-knowledge and awareness flickers in and out with tedium, drink, exhaustion and collective euphoria. God lacks my tunnel vision about myself, he knows what it is like for me to be myself in toto eternally].
However, presumably I act based on my own knowledge, insofar as my actions are free, then if God knows what it is like to me be, he also knows what *I* would choose given any particular level of self-knowledge. But this is simply because he knows the very fact that is my exercise of freedom as intimately as I do, not because he knows some other facts, independent of that exercise, which enable perfect prediction. So there is no contradiction in fact, God’s knowledge of my *future* actions is because in a certain sense, my subjective being pre-exists in God before it is produced as created being. (However, insofar as God is completely simple, there is no “part” of God which is identical to “God’s eternal knowing of what-it-is-like to be me”, so there is no individual being other than me of which it is right to say, “you are me”.)
Objection: Doesn’t this mean that God knows what it is like to commit various sins?
Response: No, God knows what it is like to desire various goods, and strive for them under different levels of virtue or knowledge. Many aspects of our self-experience are not actually self-knowledge, and thus God does not need to eternally participate in them. This includes actual participation in sin, as well as the contemplation of sin. However, the core of every sin is a good thing (albeit, in some cases under such a incredibly strained or distorted vision that it is not worthwhile for humans to attempt a reconstruction of that core, as it will only distort our own vision of the good by requiring us to ‘emulate’ a deeply disordered way of viewing the world. What is metaphysically true does not require us to ethically rework in particular cases, the demonstration of the ultimately parasitic nature of evil is not some kind of empirical or inductive demonstration from cases, but rather is an argument from first principles). More broadly, for us good and evil, self-knowledge and various kinds of impositions our surroundings tend to be intimately intertwined. We cannot, and thus are not, expected to divide things up so finely; God tells us to follow general injunctions which handle the vast majority of normal cases, and instructs us to love each other and Him in all cases; because this intertwining cannot be sorted out short of the eschaton. [and indeed, God’s modes of revelation in history can be understood as accommodation to that intertwining].
Incidentally, God-in-Christ did experience temptation, but in his human nature and not in his divine nature. So God knows (humanly) what it is like to be actually tempted, even though that is not something that the divine nature could undergo in itself.
0 notes
Text
How Could Routine Nasal Surgery Increase Risk for Anxiety and Suicide?
Imagine feeling like you're suffocating every minute of the day. No matter how big a breath you take, you still feel like you can't get enough air. This is the reality for people suffering from empty nose syndrome (ENS), a complication of nose or sinus surgery.
Despite the condition being a horrifying reality for an untold number of people, it remains controversial, with some otolaryngologists (ear, nose and throat physicians) brushing it off as purely psychological.
However, ENS is becoming an increasingly recognized complication of sinus surgery, one that may occur in up to 20 percent of cases following a procedure known as turbinate resection.1 With no known cure, and the condition so severe that sufferers cannot even gain respite while they sleep, some describe it as a "life worse than death"2 — and many have committed suicide as a result.
What Type of Sinus Surgery May Lead to Empty Nose Syndrome?
People with a deviated (or bent) septum may suffer from nasal congestion and chronic sinus infections, leading their physician to recommend septoplasty and turbinate reductions to aid in opening the nasal passage. A septoplasty aims to straighten a bent or deviated nasal septum, which is the divider separating the two sides of the nose.
A turbinate reduction, or turbinectomy, (which is also sometimes recommended for sleep apnea) seeks to reduce or remove the curved structures sticking out from the side of the nose. These can be enlarged for various reasons, such as allergies or sinus inflammation. It is this loss of tissue that may cause some people to feel as though they can't breathe, despite having clear nasal passages.
Each side of your nose contains three sets of turbiantes (a low, middle and high). The low, or inferior, turbinate is most often the one that's reduced or removed, and physicians may use a variety of procedures, ranging from cauterization to radio frequency, to do so. The amount of turbinate that's removed also varies by case and physician, with some removing the bottom third and other removing a bit off the top.
It's a common procedure. In the U.S., an estimated 600,000 people undergo sinonasal procedures every year, which includes septoplasty, turbinate surgery and others.3 By some measures, turbinate reduction is said to be "the most common procedure in rhinology."4 In many cases, the procedure works, leaving patients to breathe easier. But in some people ENS is the agonizing result.
9 Symptoms of Empty Nose Syndrome You Should Be Aware Of
The primary symptom is a feeling of nasal obstruction, or the sensation of suffocating, difficulty breathing or breathlessness. Some people feel they have an "empty nose" while others may report the following, which may develop immediately after surgery or not until months or years later:5
Sensation of excessive airflow
Lack of sensation of nasal airflow
Hypersensitivity to cold air
Hyperventilation
Headache
Nasal pain
Nasal dryness
Difficulty falling asleep
Fatigue
The physical symptoms give way to a debilitating condition that often makes daily living difficult, and carries with it significant psychological symptoms as well. Anxiety is common, as is depression, with one study finding ENS sufferers experienced a 62 percent reduction in productivity at work and a 65 percent reduction in productivity in all other activities.6
Writing in the Huffington Post, Barbara Schmidt, who developed ENS in her 20s after a routine sinus procedure for chronic sinusitis, lives in a constant state of anxiety and described the condition this way:7
"Immediately after my procedure, I experienced a lack of air resistance when breathing and speaking, making these activities that ordinarily came naturally and effortlessly entirely exhausting. I needed to exert great effort simply to project my voice, and for decades I had to catch my breath after speaking just five or six words.
… Although I was in fact breathing and getting oxygen, my brain was no longer made aware of it, so it communicated to my body that it was suffocating, triggering an unremitting fight/flight response … my brain, perceiving suffocation, woke me up every night by generating nightmares when I drifted off.
… The suffering didn't end there: dehydration, dry eyes, ear and facial pain, and the jarring sensation of cold air piercing my lungs whenever I was in an unheated area were miserable, yet mere nuisances compared to the agony of never being allowed to enter into the deeper, restorative levels of sleep ― a torment that's been used as a torture tactic in war."
Still, there was more: Restlessness and simultaneously feeling exhausted yet wired. Unable to focus or articulate. Not sensing air all day, hyperventilating. The brain shocking the body day and night in a desperate attempt to escape the misperception of suffocation. The continuous coursing of stress hormones catabolizing the body, breaking down precious tissues. Constant, agonizing fear."
What Causes ENS?
Turbinates are involved in a number of processes that regulate your breathing. This includes making cold air feel warmer when it's inhaled, swelling and shrinking in size to regulate airflow through your nose, and controlling the amount of heat or liquid lost when exhaling.8
"Physiopathology remains unclear," researchers wrote in the European Annals of Otorhinolaryngology, Head and Neck Diseases, "but probably involves disorder caused by excessive nasal permeability affecting neurosensitive receptors and inhaled air humidification and conditioning functions. Neuropsychological involvement is suspected."9
Likewise, in the journal Current Allergy and Asthma Reports, it's explained, "Little is known about the pathogenesis of ENS, though it is speculated that anatomical changes leading to alterations in local environment, disruption of mucosal cooling, and disruption of neurosensory mechanisms are strongly implicated."10
It's a paradox of sorts, because while expanding the nasal pathways by reducing turbinates would theoretically seem to make breathing easier, one study that compared nasal aerodynamics before and after nasal surgery revealed a 53 percent reduction in flow resistance along with "radical redistribution of nasal airflow, as well as dryer and colder nasal microclimate for the postoperative case."11
As for why ENS develops in some patients but not others, only hypotheses exist. One suggests climate may be a factor, with turbinectomy in warmer, humid clients not resulting in as many reported instances of ENS. Other hypotheses suggest ENS may be the result of sensory nerves in the surgical area not regenerating properly or perhaps due to surgical methods that damage nerves more so than others.12
It's also likely that the way air flows through an individual's nose also plays a role, so much so that researchers at Ohio State University's Wexner Medical Center are using 3D technology to design models to test surgery outcomes prior to the procedure. Using a computer model, they can simulate the removal of tissue to determine how it affects air flow, which could help surgeons be better prepared prior to surgery.
"Because the sinuses are surrounded by the brain and the eyes, you have be very precise, within millimeters," otolaryngologist Dr. Alex Farag said in a news release.13 In addition to ENS, other risks of sinus surgery include losing sense of smell or taste, for instance.
Are There Treatments for ENS?
Prevention is by far the most important strategy for avoiding ENS, which is why, if you're considering nasal surgery you should carefully weigh the benefits versus the risks before making a decision. At the very least, if you do undergo surgery, be sure the most conservative surgical techniques are used.14
"Ultimately, prevention of this feared complication through turbinate-sparing techniques is essential," the Current Allergy and Asthma Reports researchers wrote.15 That being said, if you or someone you love has had nasal surgery and is struggling with ENS, there may be some helpful treatments, including "mucosal humidification, irrigations and emollients" as well as surgery to reconstruct the turbinates using implants.
At least one study found that surgical treatment of ENS improved depression and anxiety,16 along with other symptoms. However, there's still much to be learned about which types of implants and placements work best.
"Recent studies have revealed that surgery may result in clinical improvement in patients with ENS but that it does not guarantee improvement in all patients, and insufficient evidence is available to favor any particular implant material," according to a study published in the Journal of International Medical Research.17
In some cases, people with ENS may also benefit from treatment to address individual symptoms, such as hyperventilation, which may be improved via respiratory rehabilitation.18 In Schmidt's case, she sought holistic treatment using Ayurveda, dietary changes, yoga, meditation and conscious breathing, as well as stress mitigation and careful attention to temperature and humidity in her environment.
In addition, she received injections of platelet-rich plasma and stem cells through Dr. Subinoy Das, CEO and medical director for the U.S. Institute for Advanced Sinus Care and Research, which is intended to stimulate new nerve and blood vessel growth and tissue remodeling of the turbinates. According to the U.S. Institute for Advanced Sinus Care and Research, they've had a greater than 75 percent improvement rate with these therapies.19
Alternatives to Surgery for Sinusitis and Sleep Apnea
ENS is iatrogenic, i.e., caused by a medical treatment, diagnostic procedure or physician. This means it's entirely preventable by avoiding nasal surgery. If you're struggling with the symptoms of a deviated septum, including chronic sinusitis, the following natural remedies may help:20
Drink hot liquids — Sipping on hot tea, bone broth or soup may help relieve congested nasal passages.
Breathe in steam — Inhaling steam helps reduce the inflammation of your nasal tissues, allowing your breathing to return to normal.
Stay hydrated — Drinking plenty of water may help reduce the pressure in your sinuses, which decreases the inflammation in your nose.
Use a warm compress — The warmth from a hot compress may help relieve the pain and inflammation in your nasal passages.
If you're considering turbinate surgery due to sleep apnea, there are also nonsurgical options to consider including continuous positive airway pressure (CPAP), a special type of sleeping mask that mechanically restores your breathing by using air pressure to open your airway. Other potential treatment options include:
Buteyko Breathing Method — Named after the Russian doctor who developed it, the Buteyko technique can be used to reverse health problems caused by improper breathing, including sleep apnea.
Orofacial Myofunctional Therapy — Myofunctional therapy involves the neuromuscular re-education or repatterning of your oral and facial muscles. It includes facial and tongue exercises and behavior modification techniques to promote proper tongue position, improved breathing, chewing and swallowing. Proper head and neck postures are also addressed.
Oral appliance — If your mild to moderate sleep apnea is related to jaw or tongue issues, specially trained dentists can design a custom oral appliance, similar to a mouth guard, that you can wear while sleeping to facilitate proper breathing.
from http://articles.mercola.com/sites/articles/archive/2018/12/20/empty-nose-syndrome.aspx
source http://niapurenaturecom.weebly.com/blog/how-could-routine-nasal-surgery-increase-risk-for-anxiety-and-suicide
0 notes