#they have gills and they use their gills as their primary respiratory organ
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There are dozens of funny blogs to kill time on Tumblr.
Note
are sharks classed as fish? I am just very confused what classes as a fish and what doesn't. I think sharks go glub glub too so maybe fish but not sure.
Lucky for you friend, I am workshopping a big post which explains what (semi and fully) aquatic animals are and aren't fish! It's taking a while, because I'm editing together 14 different images for it and that can take a bit as a full-time student.. ^^''' As a little treat, I will give you two bits from my post which will give you your answer:
"-- we can gather many defining features for fish: a cranium*-having chordate, primarily aquatic, gill-bearing and uses gills as their main respiratory organ, lacking any limbs with digits, instead having their limbs be in paired and unpaired fins when present."
*cranium=skull
"-- I'll say it now: good news, sharks are indeed fish! So are their cousins, rays, skates, and chimaeras, also known as ghost sharks! All of these fish have a primarily cartilaginous skeleton, tooth-like dermal denticles and lack gill covers and a swim bladder."
#sharks are chordates and have a skull#they are primarily aquatic (some sharks can move on land but they must return to water!)#they have gills and they use their gills as their primary respiratory organ#and they have limbs that lack digits and that instead take the form of fins.#sharks are cartilaginous fish!#asks#anonymous#anon#anonymous asks
46 notes
·
View notes
Text
today's idea for a concept:

me trying to fix the inkling mouth breathing problem. With supplementary text:
Inkfish in particular have a multi-layered respiratory system with several adaptations to an active, terrestrial lifestyle. The paired gills have a large surface area in the chest area of the organ sac, and are the primary method of gas exchange. However, Inkfish also have a separate air sac in their chest for supplementary air capture. This air sac is a specialized chamber developed over time from a part of the stomach, and in modern Inkfish, it is used for breathing and vocalization. The gills and air sac function in tandem, although one can be momentarily disabled, and either function can be given priority. Breathing over the gills is typically a passive process of the body, whereas use of the air sac, or “lung”, ramps up in times of strenuous exercise, or in dry environments where it may be prioritized while the absorption efficiency of the gills is reduced. On top of these two methods, the thin skin of Inkfish also allows for somewhat efficient gas diffusion throughout the body’s surfaces.
It is thought that Cephalings and Inkfish specifically first adapted to breathing through their buccal cavities in their early land stage, during which their gills were fairly inefficient. Therefore, gulping air into the stomach and intestine became a method to absorb extra oxygen into the bloodstream, which helped the early Inklings thrive and keep up high levels of physical activity in spite of their early land gills and somewhat inefficient oxygen transportation. Over time, a part of the stomach modified into an air sac and separated from the stomach entirely into a large gas chamber. This also paved the way for complex vocal communication.
#squidthoughts#ive been posting these on my personal blog but ppl were following me there to see more of these. which is not the intended effect but#it tells me that people want to see these so HERE!!1#the reason i havent been posting these is because these are all extremely subject to change ive just been throwing stuff at the wall#archive
59 notes
·
View notes
Text
Art Studio 1 Research: Biology of Slime (IDEA 2) PART 1
Properties of slime
Most slimes in organisms are aqueous hydrogels. However, not all slimes are hydrogels and not all hydrogels are slimy.
Aqueous hydrogels = substances where water trapped in a 3D polymer network.
Therefore, it is important to know that the primary characteristic of slimes is:
Viscoelasticity: the quality of having both viscosity and elasticity, "uniting the properties of liquids and solids" and enabling it to change its properties (Wedlich, 2022).
This gives slime its many functions in living organisms: lubricants, adhesives, protection (e.g. acting as a 'semi-permeable membrane' to filter out particles, and catching pathogens), communication, self-defence (physical or chemical), dispersal of reproductive material, etc. The slimes in living organisms contain glycoproteins such as mucins.
Why is slime so important for life (including in humans)?
As alluded to previously, slime has a number of different purposes. These purposes include:
Adhesion (for movement or catching food)
Lubrication (for movement)
Protection and self-defence
Dispersal
Adhesion and lubrication:
Movement of gastropods (sea slugs, land/cone snails, etc.): Two purposes of gastropod mucus are adhesion for climbing up vertical surfaces and to prevent being blown away by powerful wind/water currents, and lubrication to move across surfaces with ease.
Mucus in the digestive tract (oesophagus and intestines): Facilitates movement of food through the gut.
Mucus in creatures such as pelagic snails ('slime nets') and sundew plants (mucilage): Helps to collect food (adhesion).
Protection and self-defence:
Mucus in the respiratory tract: Filters and collects pathogens and other debris, which is carried out the lungs.
Mucus in the stomach: Protects the inner lining from acid.
Parrotfish and hagfish: Both use mucus to protect themselves from predators - the parrotfish to 'hide' its scent from predators while it sleeps and the hagfish to clog the throat/gills of a predator so it can escape.
Mucus on certain nudibranchs: Protects their bodies from the stings of some of the anemone/jellyfish nematocysts they eat.
Mucus on various amphibious/aquatic creatures (frogs, cephalopods, etc.): Prevent their skin drying out, and in some species to facilitate additional gas exchange through the skin (frogs and squid).
Dispersal:
Mistletoe berries: Sticky, viscous flesh that carry the seeds, which are excreted by the birds that eat them (they are also toxic to humans and most other animals = additional function of self-defence).
Stinkhorn fungi: Gleba, a gelatinous, sticky substance covering the fruiting body of the fungus, carries the spores needed to reproduce - insects like flies eat the gleba and help distribute the spores now attached to their bodies.
It has also been found that not only are gelatinous/'slimy' organisms integral parts of the marine food web (siphonophores (predators) and jellyfish (predators/prey)), but there have been theories that the earliest organisms may have originated from a 'primordial slime'.
Why slime and disgust?
Throughout the history of literature and other media (particularly horror and/or science fiction), slime/mucus has been depicted as 'disgusting', 'alien' or 'monstrous' rather than a natural (and integral) part of biology. Examples of such portrayals include H.P Lovecraft's At the Mountain of Madness (1931) and the 1988 film The Blob.
As Susanne Wedlich details in the book Slime: A Natural History, this perception was grounded in many social and political biases/prejudices throughout history (as shown in historical writings):
The vilification of various marginalised groups: In this case, particularly women and LGBTQ+ people (however, works like The Blob were inspired by global tensions and political panic during the Cold War).
The fear of death, disease and decomposition: This stems from the fear of confronting our own mortality.
The perception of anything biological (particularly in women/AFAB people) as 'taboo': For example, sexuality as 'animalistic', childbirth as 'grotesque' and menopause/ageing as 'undesirable/ugly'.
Martha C. Nussbaum reinforces this notion in her 2018 opinion piece: "Human beings are probably hard-wired to find signs of their mortality and animality disgusting, and to shrink from contamination by bodily fluids and blood. But in every culture something worse kicks in: the projection of these feared and loathed characteristics... onto a vulnerable group or groups from whom the dominant group wishes to distance itself [from]."
Wedlich also presents instances where people (especially women) in history reclaimed 'slime' (and anything else in their biology that was seen as disgusting) as a form of empowerment. For example, American writer Patricia Highsmith loved observing and breeding/keeping snails, even going on several trips to smuggle them across the French border when she moved from London. Fiona Peters (Professor of crime fiction) argues that snails were present as themes within Highsmith's works: "transgressive feminine sexuality", identity ('the self and the other'), and sapphic*/lesbian relationships (Highsmith was a lesbian herself).
(*NOTE: 'Sapphic' refers to women/gender-diverse people who are attracted to women. While 'lesbian' (women/gender-diverse people primarily or exclusively attracted to women) does align with the umbrella definition of 'sapphic', so do other sexualities like 'bisexual' (attraction to two or more genders, with or without a preference) and 'pansexual' (attraction to people regardless of gender).)
There is also media that directly subvert the 'slime = disgust' trope. On one hand, some works may portray mucus as a beautiful, mysterious part of the landscape (the gelatinous 'alien ocean' in Stanisław Lem's Solaris (1961)). Others may use it as a basis for empathy towards historically-marginalised groups, and for criticising the discrimination/exploitation of these groups (the titular creatures in Karel Čapek's War with the Newts (1936)).
While many perceptions of historically-marginalised groups have changed since then, the association of slime with disgust still persists. In his article Corporeality, hyper-consciousness, and the Anthropocene ecoGothic: slime and ecophobia, Simon C. Estok discusses the following term in relation to slime and disgust:
Ecophobia: The fear, aversion or ethical dismissal/devaluing of the natural world, its importance, and the issues that impact it.
With this in mind, you could argue that disgust towards slime/mucus as a whole (even without the social biases) may be considered a form of biophobia.
Biophobia: The fear/aversion towards anything biological (living organisms, one's internal biology, etc.), typically stemming from a disconnect with nature.
Below is a TED Talk by David Pizarro. While the methodology of the study discussed (its accuracy and potential bias) is debated, it does further explain the connections between societal/political perceptions and the disgust response.
youtube
Interesting note: Dualities
In my research, multiple dualities have been observed here:
Beauty and disgust
Appreciation and repulsion
Familiar and 'alien'
Tangible and abstract
Understood and unexplained
Health and sickness
Open-minded and closed-minded
The comfortable and the 'abject'
Self and other
Us and them
Compassion and hostility
Life and death
Natural and 'unnatural'
Acceptable and taboo
Perhaps a few of those can be the basis of my work.
References
Bansil, Rama, and Bradley S. Turner. “The Biology of Mucus: Composition, synthesis and organisation.” Advanced Drug Delivery Reviews 124, no. 1 (January 2018): 3-15.
Brownworth, Victoria A. “Patricia Highsmith: A Lesbian Life in Diaries.” Philadelphia Gay News. Published December 9, 2021. https://epgn.com/2021/12/09/patricia-highsmith-a-lesbian-life-in-diaries/
Estok, Simon C. “Corporeality, hyper‐consciousness, and the Anthropocene ecoGothic: slime and ecophobia.” Neohelicon (Budapest) 47, no. 1 (June 2020): 27-36.
McShane, Abigail, Jade Bath, Ana M. Jaramillo, Caroline Ridley, Agnes A. Walsh, Christopher M. Evans, David J. Thornton, and Katharina Ribbeck. “Mucus.” Current Biology 31, no. 15 (August 2021): 1-7.
Greenwood, Paul G., Kyle Garry, April Hunter, and Miranda Jennings. “Adaptable Defense: A Nudibranch Mucus Inhibits Nematocyst Discharge and Changes With Prey Type.” The Biological Bulletin 206, no. 2 (April 2004): 113-120.
TED Ed. “The Strange Politics of Disgust - David Pizarro.” Published April 9, 2013. YouTube video, 14:02. https://www.youtube.com/watch?v=pqX9zMuKENc
Wedlich, Susanne. Slime: A Natural History. London: Granta Books, 2022.
Ze Frank. “True Facts: Stinkhorns.” Published November 21, 2019. YouTube video, 3:38. https://www.youtube.com/watch?v=ADrBo7u3tR4
0 notes
Text
Red Sea Body Plans
We’ve gone over the single-celled life from which everything else on Osmos V arose, so now it’s time to get into multicellular lifeforms. It’s here where things are going to get a little basic, purely because I don’t have the time, energy, or inclination to make up a dozen or so body plans per sea. Instead, we’re going to be building two or three base body plans each for both major forms of symmetry (radial and bilateral) for both haplicytes and lampicytes, and using them as the basis for life moving forward.
This is where the haplicytes are really going to split for us into specialized autotrophs and specialized heterotrophs. The autotrophs, which will become out Red Sea originating plants, will be dealt with at another time. Here we’ll be dealing with our heterotrophs, our animals.
We’ll call the autotrophs chlorocytes from here on out, and the heterotrophs phagocytes.
The things to keep in mind when designing any basic body plan are feeding, defense, respiration, and reproduction. We’ll be keeping all these in mind as we go forward.
Radial Symmetry
To start off with we’re going to focus on our radially symmetrical body plans. Radial symmetry is when creature can be split into multiple identical parts in a circle around a central point. These creatures are often slow moving, if not entirely sedentary, and we’re going to have to take that into account.
We’ll do two of these here, one sessile and one mobile, to start us off.
Sessile first. The first thing we know about this creature is that we’re going to have to work out a way for it to catch it’s food, as it can’t go hunting. The way most species in this predicament do it is through tentacles or fronds, with which they either catch passing animals or detritus floating along the currents. We’ll go with fronds to start with, say an even dozen, as it’ll make catching detritus easier and that’s probably where such a creature will start off. We can even give them external digestion, so they don’t yet have to worry about a stomach. As they don’t do much moving, respiration isn’t as much of a concern, so they can probably make due with using pores in their skins to diffuse oxygen in the water into their systems.
Reproduction will be more of an issue though. Nature tends towards sexual reproduction, which allows for greater genetic diversity and security for a species, but that’s difficult when you’re sessile. Can’t exactly hit up the club, ya know? Some sessile species handle it through pollination, others through spore distribution. In the water something like the latter is most common, referred to as ‘broadcast spawning’. We’ll be going with that, but to make it more interesting we’re going to make this a three sex species, all capable of making ’eggs’ and fertilizing them. We’ll make it a circular system, where Sex A+Sex B=Sex C, Sex C+Sex B=Sex A, and so on. They’ll broadcast their spawn, eggs will be fertilized, and the young will float around on the currents as zooplankton until they become large enough to settle in and attach to the sea floor. Their main defense at this stage will just be a pure numbers game.
As for the adults’ defense, toxicity is an option, but the scaly-footed snail has my interest recently and this Osmos V has a large amount of metals, so I think we’ll go with protective ‘shell’ around the base of our vaguely anemone-ish friend into which it can retract it’s fronds. We’ll make this shelter out of iron sulfide, just like the snail, which should give it oranges and blacks as coloration. To know when they have to retract, they’ll need some form of sensory input, so we’ll give them primitive eyes running along the fronds. That way they can see danger before it reaches them to retract to safety.
We’ll call these little guys siderpodes, or ‘iron foots’.
Which brings us to the mobile ones. These guys are gonna be able to track down dinner, rather than just having it come to them, but they’re still going to have to focus on slow moving or immobile food. Their mouths will most likely be located at their center, with a stomach attached, and with things like this are typically on the underside. We’ll make them omnivores, occasional scavengers, that feed on the chlorocytes, siderpodes, and other slow moving or immobile animals. They’re need to be able to track down their food, so we’ll give them rudimentary eyes as well, and thin tendrils they can use as early smell receptors. We’ll put these at the end of, say, seven thick arms, sort’ve like a starfish. They’ll breathe same as the siderpodes, and for defense will instead go with a chitin-like scale armor, to preserve mobility and maximize speed. (After all, if dinner moves at 0.0003 mph you don’t wanna be stuck moving at 0.00024)
For reproduction, we’ll still go with broadcast spawning for now, with the young joining those of the siderpodes as zooplankton. And actually, I think we’ll keep the three sex system, not just for these guys but as a Red Sea trait.
These guys will be the ozasters, meaning ‘smelling star’.
Bilateral Symmetry
Bilateral symmetry is the contrast to radial symmetry. We’re an example- species that can be divided into two symmetrical halves, generally with a notable front and back, with the front often but not always being where brains and sensory organs go. They’re the more motile of the two types of body plan, for the most part, and have higher respiratory needs. These guys will all have some form of circulatory system, generally a free-wheeling ‘blood everywhere’ system, and a form of respiratory system to go with it.
We’re gonna try to make two of these guys too, and they’re going to be the rulers of the open sea, at least the Red Sea.
The first thing we’re going to make is a segmented swimmer, because as near as I can tell they were quite literally everywhere in early evolution. Apparently you couldn’t put on a pair of socks without crushing something exhibiting distinct segmentation. We’ll give it a long, thin body, to minimize drag, with rudder-like fins along it’s sides, four to a segment. eight segments in total. It’ll primarily eat plankton, and to that end we’ll probably give it four little, almost feathery digits at the front to catch them in, then it can eat the plankton off them. This wouldn’t necessitate much sensory input, but I’ve got a plan for a predator for them so eyes will be handy. We’ll give it six, three along each side. These, along with the speed granted by it’s shape and fins, will serve as it’s primary defensive measure.
For respiration we’ll go with gills, placing them along the belly so water rushes over them as our little critter swims. Reproduction, meanwhile, will be more direct. With the ability to see comes the ability to see potential mates, and so these critters will be able to actually seek out members of their own kind for breeding purposes. This will probably lead to a degree of sexual dimorphism among them, possibly in coloration. They’ll lay their eggs in simple nests in crevices and on the sea floor.
They will be plumaretes, or ‘feather net’.
But our little plumaret buddies will need that predator I mentioned. We need at least one fishy line in this mess or I’ll riot, so let’s play around with that, hm? They’ll be larger than the plumaretes by a fair bit, large, long, and laterally flat. We’ll give them eyes as well, since everyone else has them- only four, forward-facing. They’ll have gills along their sides, along with eight fins, for mobility and respiration. Our first dedicated predators, willing and able to eat anything that’ll fit into their mouths.
They’ll also be our first foray into size as a defense. They’re big enough that the biggest threat to them at this point in development is other, larger, members of their group. This’ll come up more as the project progresses.
Reproductionwise, I think we can safely class them in the same spot as the plumaretes. Sexual reproducers, external fertilizers, that lay eggs in crevices and such. For both groups the young probably make up yet more zooplankton, because a body of water can never have enough of those.
These guys, we’ll call primavenes. ‘First hunters’.
And these four will be the base off which we build all future Red Sea originating species. Next time, we’ll dive into the Grey Sea and see what’s happening with those mad lads.
Trust me, it is definitely stuff.
4 notes
·
View notes
Photo

Anatomical Pathology Rotation
I had low expectations for this rotation, after a friend described it as, “anatomical pathology…more like anatomical crapology”. Despite the negative review, I was determined to keep an open mind and start the week with fresh enthusiasm for dead things!
Monday began with a bit of pathology revision and a few practice cases. It was really hard and I felt as though I may as well have been listening to another language (situation not helped by the strong French accent of our teacher). In the afternoon, we got out the aprons, boots and safety glasses, and worked in groups to perform a couple of necropsies (the word for post-mortem examination in non-human animals). I worked on a five month old mixed breed dog that had presented to the hospital in acute respiratory distress. We systematically worked our way through all the anatomical structures, recording our findings as we went. While my teammates worked on other parts of the body, I removed the “pluck” - a weird term for a group of structures that can be removed together by cutting out the tongue and dissecting away attachments along the trachea and oesophagus to the heart and lungs. It is every bit as gruesome as it sounds! Pneumonia was evident in the lungs and the lung tissue was so dense it sunk when placed in water. I cut down the length of the trachea and discovered, to my surprise, the cause of death! A chunk of cartilage was wedged into the right primary bronchus, and had cut full thickness through the trachea. For one very brief moment I considered a career as a pathologist. I then looked around at all the death and gore surrounding me and quickly came to my senses. My friend, who was working on the gastrointestinal tract, found a huge number of nematodes (parasitic roundworms) in the intestines, which made my skin crawl!
On Tuesday we began the day with some more theory, and then headed to the post-mortem room in the afternoon for some more dead animals. A horse, a dolphin and a cat needed to be necropsied (no, this is not the start of a bad joke), and somehow I managed to get landed with the cat. Boo! It was a pretty straightforward case of chronic kidney disease, which meant I had time to hang around the dolphin and have a bit of a nosy. The dolphin, who was known to have a young calf, had died as a result of fishing line entanglement. The line had cut into her dorsal fin and tail fluke, restricting her movements and leaving open wounds susceptible to infection. It was a sad case and a reminder of the damage caused by human waste.
On Wednesday morning we went to the Department of Primary Industries and Regional Development (aka the agricultural department). We were given a tour of the facility, had a couple of lectures on necropsy sampling and notifiable diseases, and participated in a quick parasitology workshop. We headed back to uni in the afternoon for a cow necropsy. Large animal necropsies are quite a task, and it’s easy to become so focussed on what you’re doing that you don’t notice the absurdity of squatting in the middle of a cow carcass, soaked in blood, surrounded by organs and wielding a huge knife!
Thursday began with some more practice cases. Our teacher broke the news to us that necrosis is in fact white, rather than black as we had all previously been led to believe. Mind blown! In the afternoon we went to the university fish health unit where we anaesthetised fish and practiced taking gill samples and skin scrapes. We then euthanised the fish with an anaesthesia overdose, followed by cutting the gill arches and severing the spinal cord, just to be sure. Once dead, we performed a necropsy and collected samples for a research project. The tiny heart continued to beat for many minutes after being removed from the body. Creepy-deepy!
The final day of the rotation involved assessed pathology rounds and an online case-based exam. For rounds we had to present a specimen collected during the week to our peers and a small audience of vets from the teaching hospital. I presented the trachea and lungs from the case on Monday. I was really nervous but it actually went much better than I expected. I even survived the brutal questioning from the pathologists and got complimented on my explanation of the pathophysiology of pneumonia! The exam, on the other hand, was straight out of hell. The questions were so random and specific - there was no way we could’ve known the answers! Luckily we we were all in the same boat. All in all, anatomical pathology is a great rotation for those who enjoy feeling like an idiot constantly. Although I do enjoy the odd necropsy, I think it’s fair to say a career in pathology is not for me!
#vetstudentdownunder#vetstudent#vetschool#vetmed#veterinary#veterinarian#vetlife#dvm#pathology#necropsy#postmortem#death#path#anatomy
19 notes
·
View notes
Text
Persistent Organic Pollutants and Heavy Metals and the Importance of Fish as a Bio-Indicator of Environmental Pollution| Lupine Publishers
Opinion
Nowadays water pollution is the burning issue all over the world. Aquatic ecosystems are frequently contaminated with different toxicants through anthropogenic activities, and some of them such as metals may be naturally present and essential in low concentration but toxic and harmful in higher concentrations. Having in mind that not all chemical forms of pollutants are equally bioavailable, and some pollutants can be accumulated in living organisms to a greater extent than others, there is a need to study the levels of pollutants in the organisms to be able to predict the environmental risk. Thus, chemical analyses of the tissues of aquatic organisms are used as a routine approach in studies of aquatic pollution, providing a temporal integration of the levels of pollutants with biological relevance at higher concentrations than those present in water or sediment, and facilitating their quantification [1]. Fish are among the group of aquatic organisms which represent the largest and most diverse group of vertebrates. A number of characteristics make them excellent experimental models for toxicological research, especially for the contaminants which are likely to exert their impact on aquatic systems [2]. Due to feeding and living in the aquatic environments fish are particularly vulnerable and heavily exposed to pollution because they cannot escape from the detrimental effects of pollutants. Fish, in comparison with invertebrates, are more sensitive to many toxicants and are a convenient test subject for indication of ecosystem health. Heavy metals are produced from a variety of natural and anthropogenic sources. In aquatic environments, heavy metal pollution results from direct atmospheric deposition, geologic weathering or through the discharge of agricultural, municipal, residential or industrial waste products. Heavy metals are able to disturb the integrity of the physiological and biochemical mechanisms in fish that are not only an important ecosystem component, but also used as a food source. Previous studies have shown that marine and farmed fish and shellfish are significant contributors to consumer intake of some contaminants due to their presence in the aquatic environment and their accumulation in the flesh of fish and shellfish. The objective of this article is to describe the effects of different persistent organic pollutants and heavy metals on the fish used as bioindicator of environmental pollution. Fish have been found to be good indicators of water contamination in aquatic systems because they occupy different trophic levels; they are of different sizes and ages and in comparison with invertebrates, are also more sensitive to many toxicants [3]. Last but not least, fish are the final chain of aquatic food web and an important food source for human. Therefore, some toxicants in aquatic environments can be transferred through food chain into humans.
Persistent Organic Pollutants and Their Effect on Fish Target Organs
Gills
The fish gills are multifunctional organs involved in ion transport, gas exchange, acid–base regulation and waste excretion. Given that the gills accounts for well over 50% of the surface area of a fish it is not surprising that one of the major target organs for waterborne toxicants is the gill. The gills are regarded as the important site for direct uptake from the water, whereas the body surface is generally assumed to play a minor role in xenobiotics uptake of fish. Thus, in teleost fish the gills are most frequently utilized in bioaccumulation studies and the pathological damage produced allows the toxicity of the environment to be defined, making fish highly suitable for evaluating the health of aquatic systems [4]. Fish metabolism, acting principally through the gills can be seriously damaged since toxicant incorporation occurs mainly through this respiratory organ. Furthermore, the fish gills are very sensitive to physical and chemical alterations of the aquatic medium such as: temperature, acidification of the water supply due to acid rain, salts and heavy metals, and to any change in the composition of the environment which is an important indicator of waterborne toxicants. fish gills are the main route of penetration of toxicants into the fish organism, thus they are the first organs which come in contact with environmental pollutants and are also sensitive subjects for identifying the effects of water toxicants on fish organisms. The fish gills can accumulate bioavailable pollutants, and their measurement on gills can reflect the speciation of pollutants, and in particular metals in water, therefore, they are a useful tool for assessing bioavailability of elements in water [5].
Liver and Kidney
Once the toxicants cross the biological barriers and enter the bloodstream, they will reach and accumulate in the internal organs of fish. Numerous studies have quantified contaminants in fish organs to evaluate environmental quality, seeking causal relationships with fish health, and, based on these, the liver is likely to be the best choice, followed by the kidney and gills. The liver is reported to be the primary organ for bioaccumulation and thus, has been extensively studied in regards to the toxic effects of xenobiotics. The liver is also a target organ due to its large blood supply which causes noticeable toxicant exposure. In addition, liver is a detoxification organ and it is essential for both, the metabolism and the excretion of toxic substances in the body. The vertebrate kidney is the main organ involved in the maintenance of body fluid homeostasis [6]. The morphology and function of the kidney have been modified through evolution to fulfill different physiological requirement and the widest range of kidney types is found in fishes. The kidney, together with the gills and intestine, are responsible for excretion and the maintenance of the homeostasis of the body fluids and, besides producing urine, act as an excretory route for the metabolites of a variety of xenobiotics to which the fish may be exposed. many studies showed that different toxicants accumulate mainly in metabolic organs such as the liver and kidney which can lead to many histological alterations. Levels of heavy metals such as lead, copper, cadmium, and zinc in marine fish have been extensively documented. These metals tend to distribute differentially between the liver and kidney and other organs, most likely because of metalbinding proteins such as metallothionein’s in the metabolic organs [7].
Fish Meat
The fish meat is a very important, valuable and recommended food in the human nutrition due to low content of fat and high content of proteins and mineral substances as well as optimal ratio of unsaturated fatty acids with cardioprotective effect [8]. On the other hand, fish muscle may be the depositary for different contaminants, which occur in the water ecosystem. Such environmental pollutants are dioxins and PCBs, heavy metals, and organochlorine pesticides are a global threat to food safety, thus fish meat could lose these properties due to environmental contamination. Hydrobionts can bioaccumulate many of these contaminants potentially making seafood of concern for chronic exposure to humans. The metal concentrations in the water are positively correlated with the concentrations in fish tissues, but some research has founded that the metal concentrations in the sediments are the most important factor for their levels in the aquatic biota [9]. Consumption of fish contaminated with heavy metals have deleterious effects on human health which was widely acknowledged after a series of events in the period from 1953 to 1960 when several thousand people died in Japan as a result of poisoning caused by the consumption of mercury contaminated fish. Therefore, concern regarding the presence of heavy metals and other contaminants in seafood has arisen during the last decades.
The Moust Important Heavy Metals for Fish as a Water Pollutants
The contamination of heavy metals and metalloids in water and sediment, when occurring in higher concentrations, is a serious threat because of their toxicity, long persistence, and bioaccumulation and bio magnification in the food chain. Fishes are considered to be most significant bio monitors in aquatic systems for the estimation of metal pollution level, they offer several specific advantages in describing the natural characteristics of aquatic systems and in assessing changes to habitats. In addition, fish are located at the end of the aquatic food chain and may accumulate metals and pass them to human beings through food causing chronic or acute diseases. Studies from the field and laboratory works showed that accumulation of heavy metals in a tissue is mainly dependent on water concentrations of metals and exposure period; although some other environmental factors such as water temperature, oxygen concentration, pH, hardness, salinity, alkalinity and dissolved organic carbon may affect and play significant roles in metal’s accumulation and toxicity to fish [10]. Heavy metals are known to induce oxidative stress and carcinogenesis by mediating free reactive oxygen species. In general, metals can be categorized as biologically essential and non-essential. The nonessential metals such as Al, Cd, Hg, Sn and Pb have no proven biological function, and their toxicity rises with increasing concentrations. Essential metals such as Cu, Zn, Cr, Ni, Co, Mo and Fe on the other hand, have a known important bilogical roles in toxicity. The deficiency of an essential metal can therefore cause an adverse health effect, whereas its high concentration can also result in negative impacts which are equivalent to or worse than those caused by non-essential metals [11]. The toxicity of metals to fish is significantly affected by the form in which they occur in water. The ionic forms of metals or simple inorganic compounds are more toxic than complex inorganic or organic compounds. The toxic action of metals is particularly pronounced in the early stages of fish development and adversely affects various metabolic processes in developing fish, resulting in developmental retardation, morphological and functional deformities, or death of the most sensitive individuals [10]. Heavy metals produce toxic effects at high concentrations, and thus could be considered as risk factors for several diseases [11]. Heavy metals are able to disturb the integrity of the physiological and biochemical mechanisms in fish that are not only an important ecosystem component, but also used as a food source [8]. Previous studies have shown that marine and farmed fish and shellfish are significant contributors to consumer intake of some contaminants due to their presence in the aquatic environment and their accumulation in the flesh of fish and shellfish.
Biomarkers can offer additional biologically and ecologically relevant information – a valuable tool for the establishment of guidelines for effective environmental management. So, it can be stated that fish biomarkers are necessary for monitoring environmentally induced alterations to assess the impact of xenobiotic compounds such as heavy metals on fish. Also, it is recommended that treatment of all kinds of wastewaters, sewage and agricultural wastes must be conducted before discharge into the aquatic systems. Also, enforcement of all articles of laws and legislations regarding the protection of aquatic environments must be taken into considerations.
To know more about our Veterinary Sciences click on https://lupinepublishers.com/dairy-veterinary-science-journal
For more Lupine publishers please click on below link https://lupinepublishers.com/
To know more about Lupine Publishers click on https://lupinepublishers.us/
#Dairy Journals#veterinary science journal#Lupine publishersLupine Publishers GroupDairy and Veterinary SciencesCDVS#Lupine Publishers Group
0 notes
Text
Presenting Complaint: Social Injustice

By ANISH KOKA, MD
Bobby
It took some doing, but I had finally made it to Bobby’s home.
It was a rowhome tucked into one of those little side streets in the city that non-city folks wouldn’t dream of driving down. As I step in, I’m met by the usual set up – wooden steps that hug the right side of the wall leading up to the second floor. Bobby certainly hasn’t made it up to the second floor in some time. At the moment she is sitting in her hospital bed in the living room. The bed is the focal point to a room stuffed to the gills with all manners of stuff. At least three quarters of the stuff seems to be food. Cinnamon buns, Doritos, donut holes, chocolate frosted Donuts, crackers, Twinkies. The junk food aisle at Wawa would be embarrassed by the riches on display here.
Bobby weighs in at four hundred pounds, 5 foot 5 inches. She has a tracheostomy from multiple prior episodes of respiratory failure that have required ventilatory support. I’m here at the request of a devoted primary care physician that still makes home calls. I’ve looked through the last number of hospital stays. The last few discharge summaries are carbon copies of each other. Hypoxemic respiratory failure related to pulmonary edema complicated further by morbid obesity. Time on the vent. Antibiotics. Diuretics. Home. Return to the hospital 2 weeks later. The last echocardiogram done was 3 admissions ago. A poor study. Not much could be seen due to ‘body habitus’.
I sit on the side of the bed trying to acquire my own images of her heart. I talk to her as I struggle. Bobby is 58, the youngest of three sisters, and the only surviving member of the family. Her elder sisters died of respiratory complications as well. They both died with tracheostomies. The conversation is circular. The problem according to Bobby is the tracheostomy. Everything was fine before that. I explain that a prolonged period of time on the ventilator on a prior admission prompted the tracheostomy, and that the multiple recent admissions to the hospital that required a ventilator seemed to validate that decision. She doesn’t waver. Both her sisters died shortly after they got tracheostomies. Bobby thinks the physicians taking care of her sisters had a hand in their demise. “They didn’t care”. “We told them they were sick.”
Perhaps.
The picture on the nightstand suggests Bobby was the smallest of the three sisters.
It doesn’t take much to get Bobby talking. Her favorite holiday is July 4th because she makes the family favorite tuna casserole, and her favorite niece, April, helps her with the casserole every year.
Meanwhile, the echocardiogram shows a large right side of the heart. Her pulmonary pressures are elevated, and she seems to be fluid overloaded. Review of her bloodwork from the hospital also strongly suggests her weight may be hampering her ability to expel carbon dioxide. She really needs to be on a ventilator nightly. In other more normal contexts there are additional diagnostic steps to take, but trust won’t be built in a day. She’s heard variations of these recommendations before. She is adamantly opposed to any other invasive tests.
But a small victory. She agrees on the higher diuretic dose.
Bobby is black. I’m brown. We hail from very different zipcodes. She clearly harbors a deep mistrust of the medical system. But I’m hopeful to make some inroads. It doesn’t seem to matter to Bobby that I’m brown, or that I was born in Delhi, or that I reside in a much different zipcode than her. At the moment, I’m just another caregiver in her living room.
I sense a thaw. As I pack up, she asks me when I’ll see her again.
Hopefully soon, Bobby.
Mr. Chalhoubi
Hussain Chalhoubi is in the office with one of his three devoted daughters. It’s a different daughter every week and I can never keep their names straight. I met him after he had suffered a stroke that leaves him frustratingly aphasic. He enjoys food and drink, and like clockwork would appear in my office in the early years frequently with swollen hands and feet days after a dietary indiscretion. He always had a sheepish look on his face as his exasperated daughters would tattle on him.
At some point I learned there was little point to piling on. Scolding only gets you so far. Instead, I asked him about Syria. Boy do those eyes light up. His family had fled shortly after Syria had been plunged into civil war.
I’m curious who he blames for the mess. Assad, the dictator who the US has held responsible? He vigorously shakes his head. His daughter chimes in.
“We are Christians.”
Not much more needs to be said. Assad may be the boogie-man to many, but he is an Alawite, a minority sect of Islam in a sea of Sunni Muslims that makes up the Levant in the Middle East. The rebellion against the Alawite Assad is of the behead-first-ask-questions-later extremist Sunni kind that scares the Syrian Christian minority much more than the ruling dictator accused of his own share of atrocities.
As the conversation comes back to the medical, he forwards through his daughter that he has been trying to flush out his kidneys by drinking copious amounts of water. I try to explain to him that his kidneys and his heart don’t function normally, so they can get overwhelmed.
No flushing.
Over time, he’s started to listen more. He doesn’t skip his medications, avoids drinking too much. He used to be in the office monthly, but now every 3-4 months for routine visits.
Serving patients, or populations ?
It is now a rather quaint idea that outcomes for patients are best improved one doctor-patient relationship at a time. I understand the sentiment. For most patients the outcome is decided well before their encounter with me. Your zipcode seems to be a lot more important to your outcome than your doctor, and unsurprisingly a movement to address matters that have traditionally lived outside of the health care system has gained steam
In an earlier era the doctor’s mission was to recognize and manage diseases. Medical students were taught to hear the severe aortic regurgitation that was causing the progressive shortness of breath. The advances in the management of disease over the last half century have been nothing short of magical. Crack open a chest, arrest the heart, replace an aortic valve, bring the heart back to life. The power of medicine realized was to change the natural history of disease for the ill patient that arrived in distress seeking help.
And here the very reasonable human desire to address systemic inequities in society found synergy with a darker current of thought within medicine that felt the resources expended to care for the very ill are resources poorly spent. The focus, the theory goes, should be on preventing illness in the much larger healthy population. The scope of keeping the healthy well, of course, extends well beyond the medical, and puts everything in play. Sanitation, transportation, air quality, climate change, access to the means to pay for healthcare are just the start of a long list of priorities for those in charge. These programs need scarce budgetary dollars, and so it was only a matter of time after the government started paying for healthcare that politicians and the public health gurus they empowered to manage the health of the population began to voice their disdain for the care of those deemed “too ill”.
The tension here is that medicine’s greatest strides in the last half century have come in those with afflictions that brought them to death’s door. The inroads in this group of unfortunates have come by way of super-specialists far removed from the concerns of the worried well. Richard Lamm, the former governor of Colorado famously derided the work of Thomas Starzl, the father of organ transplantation, questioning the great surgeons use of public health resources to attempt to save individual patients at death’s door. These were the early days of transplantation, when successes were a far cry from the results enjoyed today. As the passage of time made transplantation success rates north of 90% and the public watched children destined for death skipping down hallways, Lamm’s cold calculus came to easily be rejected.
Yet in 2000, writing for Health Affairs, Lamm doubled down.
“Colorado’s doctors were constantly reminding me that in medicine, ‘cost was never a consideration.’ But health care was the fastest-growing segment of my budget, demanding increasing amounts of public funds for the medical school, for new equipment at the hospital, and for Medicaid. Daily, if not hourly, hospitals in my state would effectively appropriate state funds for a high-risk, low-benefit procedure, while I knew that those funds could easily save more lives elsewhere in the health care system or outside of it, say, by buying three new teachers, fixing a broken sewer main, or adding two police officers to a high-crime area for a year. How could cost not be a consideration in making a public budget?”
“How can patient advocates feel so good about the system they work in when I, as public advocate, feel so guilty for having so many people without even basic health care?”
It never strikes Lamm that the citizens he is so desperate to ‘cover’ with health insurance may want to choose not to die and opt to receive an organ transplant. What good is a health insurance plan that doesn’t pay for life saving therapy when you actually need it? This would be akin to paying for a fire suppressing sprinkler system, but not paying to have firefighters come to battle a structure threatening blaze.
The kinder, gentler, smarter society the ideology Lamm represents is a society that turns its back on the tangible, acute needs of the sick for hypothetical needs of the well. In a perfect world, perhaps one could do both. Unfortunately, when it comes to interventions for the worried well, controversy abounds for how exactly one accomplishes this. Does one advocate for zoning and tax policy to allow fresh produce and groceries to be sold in poor zip codes to address ‘food deserts’ so Bobby has more healthy options? Should we advocate for sin taxes on alcohol, tobacco and sugar containing products that by their very nature are meant to be regressive taxes that affect the behavior of patients like Bobby? Does caring for Mr. Chahloubi mean taking a position on US foreign policy interventions in that country, or perhaps advocacy for immigration for asylum seekers?
In an age not so long ago, it was easily recognized that the answers to these questions were to be wrestled with well outside the purview of the medical field. That a growing number in the medical community think medical training gives us special expertise to solve these problems speaks to a self-important medical echo chamber that believes society’s values should mirror its values.
We would be wise to heed the words of C.S. Lewis – “Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies… those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.. This very kindness stings with intolerable insult. To be “cured” against one’s will and cured of states which we may not regard a disease is to be put on a level of those who have not yet reached the age of reason or those who never will; to be classed with infants, imbeciles, and domestic animals.”
Bobby and Mr. Chalhoubi aren’t particularly interested in my views on sugar taxes or my feelings about Bashar al-Assad. They want someone invested in them, not in some abstract population. Advocacy by physicians has its place. Its just not in the exam room.
Anish Koka is a physician in private practice in Philadelphia.
The post Presenting Complaint: Social Injustice appeared first on The Health Care Blog.
Presenting Complaint: Social Injustice published first on https://venabeahan.tumblr.com
0 notes
Text
Presenting Complaint: Social Injustice

By ANISH KOKA, MD
Bobby
It took some doing, but I had finally made it to Bobby’s home.
It was a rowhome tucked into one of those little side streets in the city that non-city folks wouldn’t dream of driving down. As I step in, I’m met by the usual set up – wooden steps that hug the right side of the wall leading up to the second floor. Bobby certainly hasn’t made it up to the second floor in some time. At the moment she is sitting in her hospital bed in the living room. The bed is the focal point to a room stuffed to the gills with all manners of stuff. At least three quarters of the stuff seems to be food. Cinnamon buns, Doritos, donut holes, chocolate frosted Donuts, crackers, Twinkies. The junk food aisle at Wawa would be embarrassed by the riches on display here.
Bobby weighs in at four hundred pounds, 5 foot 5 inches. She has a tracheostomy from multiple prior episodes of respiratory failure that have required ventilatory support. I’m here at the request of a devoted primary care physician that still makes home calls. I’ve looked through the last number of hospital stays. The last few discharge summaries are carbon copies of each other. Hypoxemic respiratory failure related to pulmonary edema complicated further by morbid obesity. Time on the vent. Antibiotics. Diuretics. Home. Return to the hospital 2 weeks later. The last echocardiogram done was 3 admissions ago. A poor study. Not much could be seen due to ‘body habitus’.
I sit on the side of the bed trying to acquire my own images of her heart. I talk to her as I struggle. Bobby is 58, the youngest of three sisters, and the only surviving member of the family. Her elder sisters died of respiratory complications as well. They both died with tracheostomies. The conversation is circular. The problem according to Bobby is the tracheostomy. Everything was fine before that. I explain that a prolonged period of time on the ventilator on a prior admission prompted the tracheostomy, and that the multiple recent admissions to the hospital that required a ventilator seemed to validate that decision. She doesn’t waver. Both her sisters died shortly after they got tracheostomies. Bobby thinks the physicians taking care of her sisters had a hand in their demise. “They didn’t care”. “We told them they were sick.”
Perhaps.
The picture on the nightstand suggests Bobby was the smallest of the three sisters.
It doesn’t take much to get Bobby talking. Her favorite holiday is July 4th because she makes the family favorite tuna casserole, and her favorite niece, April, helps her with the casserole every year.
Meanwhile, the echocardiogram shows a large right side of the heart. Her pulmonary pressures are elevated, and she seems to be fluid overloaded. Review of her bloodwork from the hospital also strongly suggests her weight may be hampering her ability to expel carbon dioxide. She really needs to be on a ventilator nightly. In other more normal contexts there are additional diagnostic steps to take, but trust won’t be built in a day. She’s heard variations of these recommendations before. She is adamantly opposed to any other invasive tests.
But a small victory. She agrees on the higher diuretic dose.
Bobby is black. I’m brown. We hail from very different zipcodes. She clearly harbors a deep mistrust of the medical system. But I’m hopeful to make some inroads. It doesn’t seem to matter to Bobby that I’m brown, or that I was born in Delhi, or that I reside in a much different zipcode than her. At the moment, I’m just another caregiver in her living room.
I sense a thaw. As I pack up, she asks me when I’ll see her again.
Hopefully soon, Bobby.
Mr. Chalhoubi
Hussain Chalhoubi is in the office with one of his three devoted daughters. It’s a different daughter every week and I can never keep their names straight. I met him after he had suffered a stroke that leaves him frustratingly aphasic. He enjoys food and drink, and like clockwork would appear in my office in the early years frequently with swollen hands and feet days after a dietary indiscretion. He always had a sheepish look on his face as his exasperated daughters would tattle on him.
At some point I learned there was little point to piling on. Scolding only gets you so far. Instead, I asked him about Syria. Boy do those eyes light up. His family had fled shortly after Syria had been plunged into civil war.
I’m curious who he blames for the mess. Assad, the dictator who the US has held responsible? He vigorously shakes his head. His daughter chimes in.
“We are Christians.”
Not much more needs to be said. Assad may be the boogie-man to many, but he is an Alawite, a minority sect of Islam in a sea of Sunni Muslims that makes up the Levant in the Middle East. The rebellion against the Alawite Assad is of the behead-first-ask-questions-later extremist Sunni kind that scares the Syrian Christian minority much more than the ruling dictator accused of his own share of atrocities.
As the conversation comes back to the medical, he forwards through his daughter that he has been trying to flush out his kidneys by drinking copious amounts of water. I try to explain to him that his kidneys and his heart don’t function normally, so they can get overwhelmed.
No flushing.
Over time, he’s started to listen more. He doesn’t skip his medications, avoids drinking too much. He used to be in the office monthly, but now every 3-4 months for routine visits.
Serving patients, or populations ?
It is now a rather quaint idea that outcomes for patients are best improved one doctor-patient relationship at a time. I understand the sentiment. For most patients the outcome is decided well before their encounter with me. Your zipcode seems to be a lot more important to your outcome than your doctor, and unsurprisingly a movement to address matters that have traditionally lived outside of the health care system has gained steam
In an earlier era the doctor’s mission was to recognize and manage diseases. Medical students were taught to hear the severe aortic regurgitation that was causing the progressive shortness of breath. The advances in the management of disease over the last half century have been nothing short of magical. Crack open a chest, arrest the heart, replace an aortic valve, bring the heart back to life. The power of medicine realized was to change the natural history of disease for the ill patient that arrived in distress seeking help.
And here the very reasonable human desire to address systemic inequities in society found synergy with a darker current of thought within medicine that felt the resources expended to care for the very ill are resources poorly spent. The focus, the theory goes, should be on preventing illness in the much larger healthy population. The scope of keeping the healthy well, of course, extends well beyond the medical, and puts everything in play. Sanitation, transportation, air quality, climate change, access to the means to pay for healthcare are just the start of a long list of priorities for those in charge. These programs need scarce budgetary dollars, and so it was only a matter of time after the government started paying for healthcare that politicians and the public health gurus they empowered to manage the health of the population began to voice their disdain for the care of those deemed “too ill”.
The tension here is that medicine’s greatest strides in the last half century have come in those with afflictions that brought them to death’s door. The inroads in this group of unfortunates have come by way of super-specialists far removed from the concerns of the worried well. Richard Lamm, the former governor of Colorado famously derided the work of Thomas Starzl, the father of organ transplantation, questioning the great surgeons use of public health resources to attempt to save individual patients at death’s door. These were the early days of transplantation, when successes were a far cry from the results enjoyed today. As the passage of time made transplantation success rates north of 90% and the public watched children destined for death skipping down hallways, Lamm’s cold calculus came to easily be rejected.
Yet in 2000, writing for Health Affairs, Lamm doubled down.
“Colorado’s doctors were constantly reminding me that in medicine, ‘cost was never a consideration.’ But health care was the fastest-growing segment of my budget, demanding increasing amounts of public funds for the medical school, for new equipment at the hospital, and for Medicaid. Daily, if not hourly, hospitals in my state would effectively appropriate state funds for a high-risk, low-benefit procedure, while I knew that those funds could easily save more lives elsewhere in the health care system or outside of it, say, by buying three new teachers, fixing a broken sewer main, or adding two police officers to a high-crime area for a year. How could cost not be a consideration in making a public budget?”
“How can patient advocates feel so good about the system they work in when I, as public advocate, feel so guilty for having so many people without even basic health care?”
It never strikes Lamm that the citizens he is so desperate to ‘cover’ with health insurance may want to choose not to die and opt to receive an organ transplant. What good is a health insurance plan that doesn’t pay for life saving therapy when you actually need it? This would be akin to paying for a fire suppressing sprinkler system, but not paying to have firefighters come to battle a structure threatening blaze.
The kinder, gentler, smarter society the ideology Lamm represents is a society that turns its back on the tangible, acute needs of the sick for hypothetical needs of the well. In a perfect world, perhaps one could do both. Unfortunately, when it comes to interventions for the worried well, controversy abounds for how exactly one accomplishes this. Does one advocate for zoning and tax policy to allow fresh produce and groceries to be sold in poor zip codes to address ‘food deserts’ so Bobby has more healthy options? Should we advocate for sin taxes on alcohol, tobacco and sugar containing products that by their very nature are meant to be regressive taxes that affect the behavior of patients like Bobby? Does caring for Mr. Chahloubi mean taking a position on US foreign policy interventions in that country, or perhaps advocacy for immigration for asylum seekers?
In an age not so long ago, it was easily recognized that the answers to these questions were to be wrestled with well outside the purview of the medical field. That a growing number in the medical community think medical training gives us special expertise to solve these problems speaks to a self-important medical echo chamber that believes society’s values should mirror its values.
We would be wise to heed the words of C.S. Lewis – “Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies… those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.. This very kindness stings with intolerable insult. To be “cured” against one’s will and cured of states which we may not regard a disease is to be put on a level of those who have not yet reached the age of reason or those who never will; to be classed with infants, imbeciles, and domestic animals.”
Bobby and Mr. Chalhoubi aren’t particularly interested in my views on sugar taxes or my feelings about Bashar al-Assad. They want someone invested in them, not in some abstract population. Advocacy by physicians has its place. Its just not in the exam room.
Anish Koka is a physician in private practice in Philadelphia.
The post Presenting Complaint: Social Injustice appeared first on The Health Care Blog.
Presenting Complaint: Social Injustice published first on https://wittooth.tumblr.com/
0 notes
Text
CPR: A neglected but important part of fighting the opioid crisis
Opioid overdose is a frightening and potentially life-threatening event. Rescue drugs like naloxone are lifesaving, but the value of CPR doesn’t get as much attention. And it should.
How does opioid overdose lead to death?
Opioids (like oxycodone, heroin, and fentanyl) bind to special receptors in the brain called mu receptors. These receptors are responsible for a variety of functions, most importantly breathing. When the mu receptor is stimulated by an opioid, it releases chemicals that work downstream on parts of the brain that tell the body to slow down breathing, or even stop it altogether. This respiratory depression or apnea, when breathing stops, is the primary cause of death in opioid overdose.
Reversing the effects of opioid overdose
Thankfully, there is an antidote that can help to reverse the effects of opioids and save lives. As highlighted by Dr. Scott Weiner in his post in May 2018, naloxone can be used to reverse the effects of opioids and help to restore breathing. As we learned, it does this by displacing the opioid from the mu receptor, which reestablishes the signal to breathe. Naloxone can be given by a variety of routes, including by nasal spray or by an injection. It is easy to use, works quickly, and has saved a lot of lives after an opioid overdose.
But it can take several minutes for naloxone to work. On average, when delivered nasally it takes around two to five minutes for naloxone to take effect. In someone who isn’t breathing, those minutes are critical. Providing rescue breathing or CPR can help to save a life, and is the most important first step in treating an opioid overdose.
So, as important as naloxone is, anyone trained to use this medication should also be trained in another equally important intervention: cardiopulmonary resuscitation (CPR). The first thing, in fact, that a rescuer — be it a family member, friend, or good Samaritan — should do in the setting of an opioid overdose is to provide rescue breaths, or if needed, rescue breaths and chest compressions.
The value of knowing CPR
While traditionally thought of as something reserved for people who have had a heart attack, knowing CPR is growing ever more important in the opioid epidemic. Providing CPR while waiting for naloxone to arrive or waiting for it to work can be of significant benefit and a lifesaving measure. CPR is easy to learn, and training is often offered free or at a nominal cost. Anyone can learn it and anyone can do it.
Knowing CPR is important for other reasons. There are more than 350,000 out-of-hospital cardiac arrests in the United States each year. When bystanders act by providing CPR, the number of lives saved is dramatic. Nearly 45% of individuals who get it survive. Bystander CPR also helps to reduce the negative outcomes, such as injury to the brain or other organs.
Knowing the signs and symptoms of opioid overdose is important. These include: a depressed level of consciousness, small (constricted) pupils, and shallow or absent breathing. Carrying and knowing how to provide naloxone is important too, and so is knowing how to do CPR. If you know someone with an addiction to opioids, it may be one of the most important things that you do.
Follow me on Twitter @stephenpaulwoo4
The post CPR: A neglected but important part of fighting the opioid crisis appeared first on Harvard Health Blog.
from HealthIsWealth via Anna Gill on Inoreader https://ift.tt/2mKDUU1
0 notes
Text
Shark Fishing Charters
All of us have experienced fish. They are very elegant in their colouration and many people love to have them as pets. A fish might be identified as an aquatic vertebrate animal whose body may or may not be covered by scales and bears two sets of paired fins and lots of unpaired fins. fish are cold blooded or ectothermic animals which mean that their body's temperature keeps on changing because of the temperature of water. fish are distributed in most aquatic habitats which range from the mountain streams to the deepest oceans. About 32,500 types of fish are known and additionally they together form the biggest diversity associated with organisms when compared with other classes of vertebrates. fish will also be caught because of the fish keepers and are also kept in aquaria as a source of decoration. Also they are associated with movies, cultures and religions. The word fish relates to an animal which suggests any non-tetrapod craniate that bears gills throughout its life and contains fins as opposed to limbs. Like other vertebrates fish are of various types and are usually classified relating to their characters. The primary kinds of fish found in the modern world will be the hagfish, sharks, rays, lampreys, ray-finned fish, coelacanths and lungfish. A fish possesses streamlined body to swim rapidly into the aquatic environment, has gills or accessory respiratory organs to get oxygen and also have paired along with unpaired fins. The paired fins range from the pectoral therefore the pelvic fins. The unpaired fins are the dorsal, anal while the caudal fins. Usually the body regarding the fish is covered with scales but there are some fish also which lack scales and so are scale less. The jaws have become well toned when you look at the fish. They are oviparous. Generally fish are cold blooded vertebrates but exceptions always exist. Tuna, swordfish plus some types of sharks have adaptations to the warm blooded category. The streamlining and the swimming efficiency regarding the fish also varies for instance tuna, salmon and jacks can swim 10-20 body lengths per second although the eels and sharks cannot move more than 0.5 body lengths per second. Some species of fish are capable of extracting oxygen directly from the air in addition to through other substances as they bear some specialized structures for this purpose for instance lungfish have paired lungs, gouramis have labyrinth and catfish extract oxygen through the intestine or perhaps the stomach. The shape associated with body as well as the arrangement associated with fins is also variable. The scales are of different types just like the placoid, cosmoid, ganoid, cycloid and ctenoid. There are particular fish also which live on land like the mudskippers which go on the mudflats and on being disturbed hide themselves in their underground burrows.

The human body size of the fish varies from as small as the stout infant fish which will be only 8mm long to as huge as the white shark that will be 16meter long. Many animals are often confused with fish because the term fish is associated with them such as the starfish, jellyfish, cuttlefish, shellfish. Strictly speaking they are not fish. There are at present 28,000 extant fish of which 27,000 will be the bony fish, 970 are the sharks, rays and chimeras and 108 will be the hagfish. About 64 categories of fish are monotypic because they contain just one species. The entire total associated with the fish comes to about 32,500 at present. fish respire through gills present on either region of the pharynx. The gills are made up of thread-like structure known as filaments. Each filament is furnished by the capillary network which boosts the surface area for the easy exchange of oxygen and carbon dioxide. fish draw the oxygen rich water through their mouth and pump it on the gills. In a few fish the capillary blood flows in opposite direction through counter current system. The gills pass the water poor in oxygen into the gill openings present in the sides associated with the pharynx. Sharks and lampreys have multiple gill openings while many fish have single gill opening. The gill openings are included in a protective covering called as operculum. The breathing mechanism can be variable in fish. The skin of anguillid eels has the capacity to absorb oxygen. The buccal cavity associated with electric eel gets the potential to soak up oxygen. Some fish such as the perches, cichlids will be able to breathe air directly but greater part of the fish are dependent on the oxygen dissolved in water. Some air breathing fish also hide themselves underneath the moist burrows and show a temporary hibernation mechanism so when loads of water is present they show aestivation by returning to water. fish may be obligate or facultative air breathers. The African lungfish comes underneath the group of obligate air breathers because it comes towards the surface of water for gulping out air otherwise it's going to die because of suffocation. Facultative air breathers comprise the heavy area of the fish as most of the fish breathe oxygen dissolved in water because they conserve energy by not arriving at the area of water to best time to fish in costa rica gulp air. The catfish in absence of dissolved oxygen can depend on oxygen dissolved in gills. The circulatory system of the fish is in the form of a closed loop. The heart pumps blood through this single loop into the entire body. The fish heart is made of four parts including two chambers, one entrance and another exit opening. The very first the main heart may be the sinus venosus which will be a thin walled sac and collects blood through the veins of this body before passing it towards the second part which is atrium. Atrium is a big muscular chamber which sends blood to the third part which will be the ventricle. The ventricle is thick walled and it also passes blood towards the fourth part the bulbous arteriosus. From here the blood is passed to your aorta and then to your gills for oxygenation. Jaws in fish are extremely well toned and enable them to eat a wide variety of food materials whether it is a plant or an animal. Ingestion of food occurs through the mouth which is broken on to the oesophagus. The digestion of food occurs in the stomach plus in some fish characteristic finger like projection are present which secrete the digestive enzymes. These projections are called as pyloric caeca. Pancreas and liver also secrete enzymes and help when you look at the easy digestion for the food material. Your whole process of digestion and absorption leads to the intestine. The waste material of fish is high in ammonia this means these are typically ammonotelic. The waste materials leaves your body either through the gills or through the kidneys. Saltwater fish lose water through osmosis and reverse happens in case of freshwater fish. The kidneys excrete dilute amount of urine. The scales in fish originate from your skin.
0 notes
Text
Biology of Inkfish - Body Plan
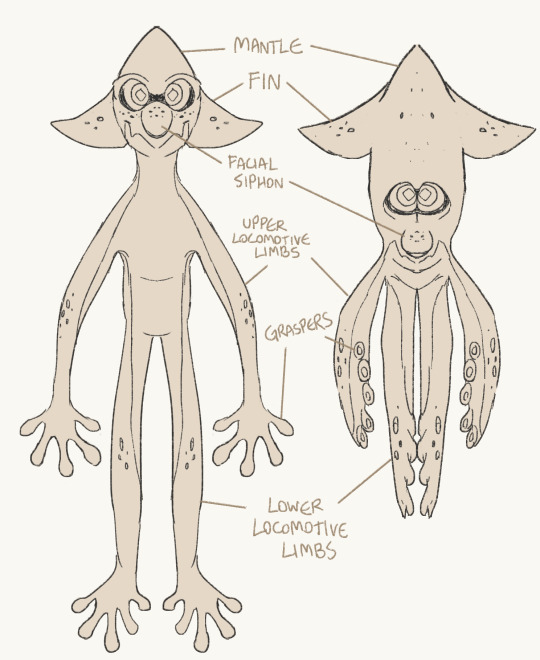
[The general body plan of one of the most common Neocephalopods, the Squid Inkling showing variance between forms (with tentacle crown omitted).]
General Body Plan
Neocephalopods are usually clearly split into two loose “segments” - the head and the body. In many species of inkfish, the head and body can squeeze together to fade the distinction between body segments and become a singular mantle. Neocephalopods are shell-less with the exception of the Neonautiloids, which have a large shell which their head protrudes out of, and which their body is fused into. The body contains most of their organs suspended within an organ sac. All neocephalopods are notable for the presence of tentacle-like limbs, with eight to ten limbs being present.
The head of a neocephalopod contains the brain, two large eyes, a parrot-like beak and some, or all, of the limbs - depending on species. Limbs attached to the head are typically referred to as the tentacles, with the distinction of hunting tentacles and crown tentacles to differentiate between “true” and “false” tentacles*. In some species, a hyponome or siphon is present on the face or head - in others it is absent or present in another part of the body. All neocephalopods with the exception of neonautiloids have a pair of fins on the head - even octolings, in which these fins evolved independently.
(*True and false tentacles from the viewpoint of human-originated cephalopod limb classification.)
All neocephalopods have a minimum of four crown tentacles attached to their head. In cephalings, these are vestigial limbs that are repurposed into mostly decorative body parts. The crown tentacles have few suction cups - used mostly for capturing olfactory information from the air around them and holding their eggs when applicable. In octolings specifically, these suction cups have a lot of surface area and can be notably large. In neonautiloids, the ten tentacles that attach to the base of their neck are not vestigial and are actively used for hunting and locomotion and they lack suction cups or specialized graspers, instead being muscular sheaths for more prehensile cirri hidden within.
Mouthparts
The beaks of Neocephalopods are made of chitin, and their primary purpose is to pierce, cut or crush their prey and inject venom if needed. The beaks come in varying shapes based on species and may come in black or white*. The color of one’s beak varies by genetics. Within the mouth and the beak, there is a radula covered with teeth. The radula, sometimes called the rasping tongue, is used to carve out food. Food travels down through the narrow esophagus into the digestive system.
(*The beaks of real cephalopods are black, but fade to white towards the base that is connected to the muscle. The beaks of Inklings are likely white to make them appear more humanoid. When in doubt, just include them both. White parts of the beak are also softer, so you could choose to portray that their beaks simply got softer over time, potentially due to diet changes or an increase in size.)
Respiration
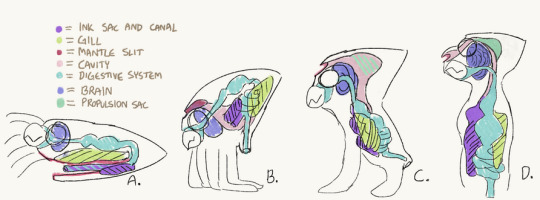
[A widely accepted anatomical diagram of the development of the facial siphon throughout inkling evolution.]
Neocephalopods, like most other terrestrial invertebrates new to the Mollusc Era, sport a pair of modified gills within their bodies. These gills are perpetually kept moist by internal mucus processes to allow them to capture oxygen from incoming air, which is then pumped out through the facial siphon. In inkfish, the gills connect to the facial siphon through a long cavity which also connects to the ink sac - while this passage is normally closed, it opens when ink is ejected and sprayed through the siphon.
Inkfish in particular have a multi-layered respiratory system with several adaptations to an active, terrestrial lifestyle. The paired gills have a large surface area in the chest area of the organ sac, and are the primary method of gas exchange. However, inkfish also have a separate air sac in their chest for supplementary air capture. This air sac is a specialized chamber developed over time from a part of the stomach, which in modern inkfish is used for breathing and vocalization. The gills and air sac function in tandem, although one can be momentarily disabled, and either function can be given priority. Breathing over the gills is typically a passive process of the body, whereas use of the air sac, or “lung”, ramps up in times of strenuous exercise, or in dry environments where it may be prioritized while the absorption efficiency of the gills is reduced. On top of these two methods, the thin skin of inkfish also allows for somewhat efficient gas diffusion throughout the body’s surfaces.
It is thought that cephalings and inkfish specifically first adapted to breathing through their buccal cavities in their early land stage, during which their gills were fairly inefficient. Therefore, gulping air into the stomach and intestine became a method to absorb extra oxygen into the bloodstream, which helped the early inklings thrive and keep up high levels of physical activity in spite of their early land gills and somewhat inefficient oxygen transportation. Over time, a part of the stomach modified into an air sac and separated from the stomach entirely into a large gas chamber. This also paved the way for complex vocal communication.
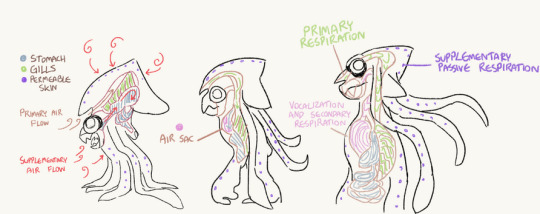
(A chart hypothesizing the evolution of the cephaling air sac and highlighting the functions of the complex respiratory system.)
Torso and Limbs
The torso of neocephalopods is, in very simple terms, a “muscular bag”, just like their mantle (in species where applicable). The torso holds most of the internal organs, including the systemic heart*, the stomach and the digestive tract, and the ink sac - these organs are mostly within a protective bag called the organ sac. In inkfish, a particularly sturdy yet flexible organ sac allows the organs to safely shift position around the body during compression into swim form. In swim form, specialized pulling muscles across the mantle, torso and neck area contract to effectively withdraw the contents of the torso within the mantle cavity and reduce the torso itself to an almost nonexistent size. Most non-inkfish neocephalopods do not have this ability.
(*Cephalopods have three hearts, but the systemic heart is the one that is closest to our heart as it pumps blood around the body. The two branchial hearts pump blood through the gills, so that is likely still their primary function.)
The limbs of neocephalopods are unsegmented and muscular. In cephalings, the four limbs include two upper locomotive limbs (arms) and two lower locomotive limbs (legs). Although used for different functions, they are mostly identical in terms of anatomy and function and can be used interchangeably with practice. The hind legs are often curved to better accommodate the weight of a cephaling and keep balance, which in turn makes the arms appear proportionally longer. In neonautiloids, six limbs typically have carrying capacity and these “tanglers” are even tangled together to create sturdier “legs”, whereas the four remaining limbs are secondary and used for further object manipulation and communication. In cirrates, which tend to have cartilaginous skeletons, the limbs sometimes appear unusually long and straight.

[From left to right; two cirrates of different species (a type of inkless cephaling), a squid inkfish (a type of inkling or ink-having cephaling), and a nautilus (a type of neonautilus) demonstrating physical differences and similarities.]
Aside from neonautiloids, most neocephalopods have limbs with modified tips for grasping onto and manipulating objects. The limbs of Cephalings have modified suckers called graspers (or fingers) on the ends of the limb. These graspers typically split off from a central point, are in sets of four or five, and have a suction pad at the tips; depending on species, they may or may not also have hooks or teeth for defense and capturing prey. In Cirrates, instead of suction cups developing into graspers, a similar function is typically served by a set of particularly large and muscular cirri. The tips of the arm still typically have some suction cups for added gripping power. In Neonautiloids, the function of grasping onto things and manipulating objects is also handled by cirri that are normally sheathed within the tentacles, but these are not particularly specialized.
Neocephalopods, like all cephalopods, are boneless and move largely due to strong musculature. In inkfish, a clever system is implemented in which their muscles utilize a system where much of their structure and shape is supported by the presence of ink as padding. This makes their shape, weight and musculature quite flexible at a moment's notice, but makes them very vulnerable to loss of ink in the body in return. Inkless cephalings, such as cirrate octopodes, lack this system and instead sport a very modest cartilaginous skeletal system. Neonautiloids sport a shell, and crawl around on their several muscular tentacles or weave them together to better support their weight.
28 notes
·
View notes
Text
Craniosacral Bodywork: A Balloon Filled With Hot Air Or Totally Effective Modality?
There are many topics I'm enamored of that I would like to search additionally. However, before I really do, I get that I have to know about the subject. If we go back to the times of a slower, easier life, this perfectly clearly meant going to "the stacks" of the local university library, along with libraries a little bit an excessive distance from your area. It involved using the Internet to dial up to website library IBM VM systems, and it conveyed that one was looking at the local Public Library for books, mags, and articles in newspapers concerning the subject of interest. Quite simply, a super dependence on libraries, in true to life and both virtual. Nowadays, I commence my goal with WikiPedia. I understand that the information presented is moderated, and is commonly appropriate, although on leading problems, some content articles could be skewed at times. It isn't the literal Word, routed from the Lord's Abode. Nevertheless, I've mainly been satisfied with the quality of job they do, & most content articles happen to be thoroughly sourced and they are a superb starting place for more weeks of learning. Below, I wrote an interesting article that is usually typically excerpted from WikiPedia articles and reviews. Even though I've rewritten it, I must even give credit and recognition where it is necessary. I'd be plagiarizing if I failed to, because a basic substitution of words isn't a new work, in line with the regulations. Thankfully, the Creative Commons license enables me to employ these interesting articles for my own intentions. Having said that, please delight in this quick jump into this issue. Craniosacral therapy (CST) is a kind of bodywork or some other therapy using peaceful touch to manipulate the synarthrodial joints of the cranium. A specialist of cranial-sacral remedy could also apply light details to a patient's backbone and pelvis. Practitioners think that this manipulation regulates the flow of cerebrospinal fluid and supports inches primary respiration". Craniosacral remedy originated by John Upledger, D. U. in the 1970s, because an offshoot osteopathy in the cranial subject, or cranial osteopathy, which was developed in the 1930s simply by William Produce Sutherland. In accordance with the American Cancer Culture, although CST might relieve the symptoms of stress and anxiety or strain, "available scientific facts will not support promises that craniosacral therapy helps in eliminating malignancy or any type of additional disease". CST provides been characterized as pseudoscience and its own practice has been termed quackery. Cranial osteopathy has received a similar assessment, with one 1990 paper getting there was zero scientific basis for any from the professionals ' promises the paper reviewed. The term craniosacral or cranial-sacral are based on the keywords cranium and sacrum, a bone fragments of the pelvis which links the cheapest lumbar vertebra to both hip bone fragments and the tailbone. Cranial osteopathy, a forerunner of CST, is originated simply by osteopath William Sutherland (1873-1954) in 1898-1900. While researching at a disarticulated skull, Sutherland was struck simply by the theory which the cranial sutures of the temporal bones where they meet the parietal bone fragments were "beveled, like the gills associated with a seafood, indicating articular mobility to get a respiratory mechanism. " John Upledger created Craniosacral therapy. Evaluating it to cranial osteopathy he had written: "Dr. Sutherland's finding regarding the overall flexibility of skull sutures led to the early research at the rear of CranioSacral Therapy - and both strategies impact the cranium, sacrum and coccyx - the similarities closing there. " However , present day cranial osteopaths mainly consider the two methods to be the comparable, but that cranial osteopathy provides "been educated to non-osteopaths beneath the name CranialSacro therapy. inch From 1975 to 1983, Upledger and neurophysiologist and histologist Ernest W. Retzlaff performed at Michigan State University while clinical experts and teachers. They set up a research team to research the purported pulse and additional study Sutherland's theory of cranial bone motion. Upledger and Retzlaff went on to create their particular results, which they interpreted since support pertaining to both the idea of cranial bone activity, and the idea of a cranial rhythm. Later testimonials of these studies have figured their analysis didn't meet up with enduring values to offer definitive substantiation meant for the effectiveness of craniosacral therapy and the living of cranial bone tissue movements. Professionals of both cranial osteopathy and craniosacral remedy assert that we now have little, rhythmic movements of the cranial bone fragments related to cerebrospinal liquid pressure or arterial force. The premise of CST is definitely that palpation of the cranium can be used to find this rhythmic movement from the cranial bone fragments and selective pressures may be used to change the cranial bones to accomplish a therapeutic end result. However , the amount of mobility and compliance of the cranial bones is known as controversial and can be a critically important concept in craniosacral therapy. Key respiratory system mechanism THE PRINCIPAL Respiratory Instrument (PRM), the device originally suggested by Sutherland, comes with been summarized in five ideas: The postulated intracranial fluid fluctuation can be defined by practitioners as an connections between four main components: arterial blood, capillary blood vessels (brain volume ), venous blood vessels and cerebrospinal fluid (CSF). Fluctuation from the cerebrospinal liquid There's analysis which demonstrates examiners are unable to measure craniosacral action dependably, as indicated by too little inter-rater contract among examiners. The writers of the analysis conclude this "measurement error may be sufficiently large to render many clinical options potentially erroneous". Alternate medication practitioners possess interpreted this consequence since a product of entrainment among individual and specialist, a theory which lacks technological assist. Whether craniosacral action can be dependably palpated continues to be a subject of question with studies making mixed outcomes. Mobility from the intracranial and intraspinal dural membranes In 1970, Upledger detected throughout a medical procedure around the neck what he referred to as a poor pulsating motion within the vertebral meninges. He attempted to hold the membrane still and discovered that he cannot due to potency of the action behind the mobility. Mobility of the cranial bones The extent that cranial bones can move is known as questionable and research of the lifestyle and amount of cranial motions have produced mixed results. Cranial sutures will be the areas where the eight cranial bone fragments are joined up with. During infancy, the cranial bone fragments are not rigidly fused to one another, yet are instead bound jointly by way of a membrane layer referred to as a fontanelle where two sutures join. Between your first and second 12 months of existence, the cranial bone fragments begin to go alongside one another and fuse as a normal part of development. Research examining age the closure of the cranial sutures feature reported blended findings. Closure provides been reported to occur during adolescence whilst other studies indicate better specific variability in the timing of this closure with fusion of the lambdoid stitch, sagittal stitch, and coronal sutures taking place in the 4th decade of lifestyle, but finish fusion of all sutures not occurring until advanced time (the eighth 10 years of life continues to be reported ); some studies have discovered that the sutures by no means rigidly fuse. According to Gray's Anatomy, "hen such sutures happen to be linked by sutural ligament and periosteum, nearly complete immobility benefits inches. Treatment The therapist gently palpates the patient's physique, and centers intently to the communicated movements. A practitioner's being of being in tune with an individual is described as entrainment. Sufferers often article feelings of deep rest after and during the therapy program, and may feel light-headed. While sometimes regarded as brought on by a rise in endorphins, study shows the consequences could possibly become brought about by the endocannabinoid program. You will discover couple of reports of adverse situations from CST treatment. In one analysis of craniosacral manipulation in patients with traumatic human brain syndrome, the incidence of undesireable effects from treatment was 5%. Reception According to the American Malignancy Contemporary society, although CST might ease the symptoms of anxiety or strain, "available scientific facts does not support cases that craniosacral remedy helps in curing cancer tumor or any type of various disease". Cranial osteopathy comes with received an identical evaluation, with 1 1990 newspaper finding there is no technological basis for just about any of the practitioners ' promises the paper analyzed. In Oct 2012 Edzard Ernst conducted a organized overview of randomized clinical trials of craniosacral therapy. He concluded that " the idea that CST is associated with more than non-specific effects isn't based on information from rigorous randomised clinical trials. inch Commenting especially on this bottom line Ernst commented on his blogging site that he previously picked the wording as "a courteous and technological way of expressing my thanks that CST is just phony. " Ernst also left a comment that the grade of five from the six studies he had analyzed was "deplorably poor, inches a emotion which echoed an Aug 2012 review that mentioned the "moderate methodological quality of the included studies. inch Ernst criticized a 2011 systematic critique performed simply by Jakel and von Hauenschild for addition of observational research and including research with healthy and balanced volunteers. This review figured the evidence platform surrounding craniosacral therapy as well as its efficiency was sparse and composed of research with heterogeneous designing. The authors of the review explained that currently available evidence was insufficient to draw final thoughts. The evidence bottom for CST is definitely sparse and lacks a proven biologically credible mechanism. From the absence of demanding, well-designed randomized managed studies, it's been characterized as pseudoscience, and its practice called quackery. Thank you to WikiPedia concerning the impressive information that's distributed to Internet users by dedicated staff of unpaid editors and team members. This information was gleaned from WikiPedia.org. Please sincerely reflect on DONATING BY TAPPING ON THIS LINK.
0 notes
Text
Presenting Complaint: Social Injustice

By ANISH KOKA, MD
Bobby
It took some doing, but I had finally made it to Bobby’s home.
It was a rowhome tucked into one of those little side streets in the city that non-city folks wouldn’t dream of driving down. As I step in, I’m met by the usual set up – wooden steps that hug the right side of the wall leading up to the second floor. Bobby certainly hasn’t made it up to the second floor in some time. At the moment she is sitting in her hospital bed in the living room. The bed is the focal point to a room stuffed to the gills with all manners of stuff. At least three quarters of the stuff seems to be food. Cinnamon buns, Doritos, donut holes, chocolate frosted Donuts, crackers, Twinkies. The junk food aisle at Wawa would be embarrassed by the riches on display here.
Bobby weighs in at four hundred pounds, 5 foot 5 inches. She has a tracheostomy from multiple prior episodes of respiratory failure that have required ventilatory support. I’m here at the request of a devoted primary care physician that still makes home calls. I’ve looked through the last number of hospital stays. The last few discharge summaries are carbon copies of each other. Hypoxemic respiratory failure related to pulmonary edema complicated further by morbid obesity. Time on the vent. Antibiotics. Diuretics. Home. Return to the hospital 2 weeks later. The last echocardiogram done was 3 admissions ago. A poor study. Not much could be seen due to ‘body habitus’.
I sit on the side of the bed trying to acquire my own images of her heart. I talk to her as I struggle. Bobby is 58, the youngest of three sisters, and the only surviving member of the family. Her elder sisters died of respiratory complications as well. They both died with tracheostomies. The conversation is circular. The problem according to Bobby is the tracheostomy. Everything was fine before that. I explain that a prolonged period of time on the ventilator on a prior admission prompted the tracheostomy, and that the multiple recent admissions to the hospital that required a ventilator seemed to validate that decision. She doesn’t waver. Both her sisters died shortly after they got tracheostomies. Bobby thinks the physicians taking care of her sisters had a hand in their demise. “They didn’t care”. “We told them they were sick.”
Perhaps.
The picture on the nightstand suggests Bobby was the smallest of the three sisters.
It doesn’t take much to get Bobby talking. Her favorite holiday is July 4th because she makes the family favorite tuna casserole, and her favorite niece, April, helps her with the casserole every year.
Meanwhile, the echocardiogram shows a large right side of the heart. Her pulmonary pressures are elevated, and she seems to be fluid overloaded. Review of her bloodwork from the hospital also strongly suggests her weight may be hampering her ability to expel carbon dioxide. She really needs to be on a ventilator nightly. In other more normal contexts there are additional diagnostic steps to take, but trust won’t be built in a day. She’s heard variations of these recommendations before. She is adamantly opposed to any other invasive tests.
But a small victory. She agrees on the higher diuretic dose.
Bobby is black. I’m brown. We hail from very different zipcodes. She clearly harbors a deep mistrust of the medical system. But I’m hopeful to make some inroads. It doesn’t seem to matter to Bobby that I’m brown, or that I was born in Delhi, or that I reside in a much different zipcode than her. At the moment, I’m just another caregiver in her living room.
I sense a thaw. As I pack up, she asks me when I’ll see her again.
Hopefully soon, Bobby.
Mr. Chalhoubi
Hussain Chalhoubi is in the office with one of his three devoted daughters. It’s a different daughter every week and I can never keep their names straight. I met him after he had suffered a stroke that leaves him frustratingly aphasic. He enjoys food and drink, and like clockwork would appear in my office in the early years frequently with swollen hands and feet days after a dietary indiscretion. He always had a sheepish look on his face as his exasperated daughters would tattle on him.
At some point I learned there was little point to piling on. Scolding only gets you so far. Instead, I asked him about Syria. Boy do those eyes light up. His family had fled shortly after Syria had been plunged into civil war.
I’m curious who he blames for the mess. Assad, the dictator who the US has held responsible? He vigorously shakes his head. His daughter chimes in.
“We are Christians.”
Not much more needs to be said. Assad may be the boogie-man to many, but he is an Alawite, a minority sect of Islam in a sea of Sunni Muslims that makes up the Levant in the Middle East. The rebellion against the Alawite Assad is of the behead-first-ask-questions-later extremist Sunni kind that scares the Syrian Christian minority much more than the ruling dictator accused of his own share of atrocities.
As the conversation comes back to the medical, he forwards through his daughter that he has been trying to flush out his kidneys by drinking copious amounts of water. I try to explain to him that his kidneys and his heart don’t function normally, so they can get overwhelmed.
No flushing.
Over time, he’s started to listen more. He doesn’t skip his medications, avoids drinking too much. He used to be in the office monthly, but now every 3-4 months for routine visits.
Serving patients, or populations ?
It is now a rather quaint idea that outcomes for patients are best improved one doctor-patient relationship at a time. I understand the sentiment. For most patients the outcome is decided well before their encounter with me. Your zipcode seems to be a lot more important to your outcome than your doctor, and unsurprisingly a movement to address matters that have traditionally lived outside of the health care system has gained steam
In an earlier era the doctor’s mission was to recognize and manage diseases. Medical students were taught to hear the severe aortic regurgitation that was causing the progressive shortness of breath. The advances in the management of disease over the last half century have been nothing short of magical. Crack open a chest, arrest the heart, replace an aortic valve, bring the heart back to life. The power of medicine realized was to change the natural history of disease for the ill patient that arrived in distress seeking help.
And here the very reasonable human desire to address systemic inequities in society found synergy with a darker current of thought within medicine that felt the resources expended to care for the very ill are resources poorly spent. The focus, the theory goes, should be on preventing illness in the much larger healthy population. The scope of keeping the healthy well, of course, extends well beyond the medical, and puts everything in play. Sanitation, transportation, air quality, climate change, access to the means to pay for healthcare are just the start of a long list of priorities for those in charge. These programs need scarce budgetary dollars, and so it was only a matter of time after the government started paying for healthcare that politicians and the public health gurus they empowered to manage the health of the population began to voice their disdain for the care of those deemed “too ill”.
The tension here is that medicine’s greatest strides in the last half century have come in those with afflictions that brought them to death’s door. The inroads in this group of unfortunates have come by way of super-specialists far removed from the concerns of the worried well. Richard Lamm, the former governor of Colorado famously derided the work of Thomas Starzl, the father of organ transplantation, questioning the great surgeons use of public health resources to attempt to save individual patients at death’s door. These were the early days of transplantation, when successes were a far cry from the results enjoyed today. As the passage of time made transplantation success rates north of 90% and the public watched children destined for death skipping down hallways, Lamm’s cold calculus came to easily be rejected.
Yet in 2000, writing for Health Affairs, Lamm doubled down.
“Colorado’s doctors were constantly reminding me that in medicine, ‘cost was never a consideration.’ But health care was the fastest-growing segment of my budget, demanding increasing amounts of public funds for the medical school, for new equipment at the hospital, and for Medicaid. Daily, if not hourly, hospitals in my state would effectively appropriate state funds for a high-risk, low-benefit procedure, while I knew that those funds could easily save more lives elsewhere in the health care system or outside of it, say, by buying three new teachers, fixing a broken sewer main, or adding two police officers to a high-crime area for a year. How could cost not be a consideration in making a public budget?”
“How can patient advocates feel so good about the system they work in when I, as public advocate, feel so guilty for having so many people without even basic health care?”
It never strikes Lamm that the citizens he is so desperate to ‘cover’ with health insurance may want to choose not to die and opt to receive an organ transplant. What good is a health insurance plan that doesn’t pay for life saving therapy when you actually need it? This would be akin to paying for a fire suppressing sprinkler system, but not paying to have firefighters come to battle a structure threatening blaze.
The kinder, gentler, smarter society the ideology Lamm represents is a society that turns its back on the tangible, acute needs of the sick for hypothetical needs of the well. In a perfect world, perhaps one could do both. Unfortunately, when it comes to interventions for the worried well, controversy abounds for how exactly one accomplishes this. Does one advocate for zoning and tax policy to allow fresh produce and groceries to be sold in poor zip codes to address ‘food deserts’ so Bobby has more healthy options? Should we advocate for sin taxes on alcohol, tobacco and sugar containing products that by their very nature are meant to be regressive taxes that affect the behavior of patients like Bobby? Does caring for Mr. Chahloubi mean taking a position on US foreign policy interventions in that country, or perhaps advocacy for immigration for asylum seekers?
In an age not so long ago, it was easily recognized that the answers to these questions were to be wrestled with well outside the purview of the medical field. That a growing number in the medical community think medical training gives us special expertise to solve these problems speaks to a self-important medical echo chamber that believes society’s values should mirror its values.
We would be wise to heed the words of C.S. Lewis – “Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies… those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.. This very kindness stings with intolerable insult. To be “cured” against one’s will and cured of states which we may not regard a disease is to be put on a level of those who have not yet reached the age of reason or those who never will; to be classed with infants, imbeciles, and domestic animals.”
Bobby and Mr. Chalhoubi aren’t particularly interested in my views on sugar taxes or my feelings about Bashar al-Assad. They want someone invested in them, not in some abstract population. Advocacy by physicians has its place. Its just not in the exam room.
Anish Koka is a physician in private practice in Philadelphia.
The post Presenting Complaint: Social Injustice appeared first on The Health Care Blog.
Presenting Complaint: Social Injustice published first on https://wittooth.tumblr.com/
0 notes