#the papers were on decision-making and how it relates to autism and anxiety
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr posted its first advertisements in May 2012 and subsequently earned $13M in revenue.
Text
I spent my lunch break reading research papers and being sleepy 😴 now im full of regrets
#sleepy#eepy#petiolata reads#trauma#mental health#the papers were on decision-making and how it relates to autism and anxiety#real cheerful stuff#I'm just trying to figure out how to more easily make major decisions. or any decisions.#for that i need to know The Science behind it all#or at least it can't hurt to know more about it#tho tbh I should see if I can find some research on decision-making and trauma#bc i def have childhood trauma around decisions#if I picked a restaurant or anything as a kid and it went bad (e.g served cold food or rude waitress or got a flat tire on the way there)#I'd be blamed and shamed#tbh I was made to feel responsible for any bad thing that happened ever and that really f//ks up how you see yourself and the world#op#personal
1 note
·
View note
Note
For the secondary ask game: 4, 6, 8, 21
4. Of course my answer is Felice/Wilhelm/Simon! While in canon Wilhelm decides that he is only interested in Simon/monogamy, I actually think the space that Wilhelm is in when he leans into his connection with Felice is really interesting and would make for a fascinating AU. Like @bluedalahorse said in her answer to this, I feel like Felice and Wilhelm’s relationship is really restricted by gender norms and amanormativity in canon. What would have happened if they were able to explore their connection outside of the pressures of a royal heterosexual relationship? What if they were both allowed to experiment more with their gender or gender presentation? What would happen if someone explained polyamory to them and they realized that you can have more than one person you love, even if you don’t love each of them in the exact same way? Also, what would have happened if Simon and Felice had connected more, even as friends/metas on either side of Wilhelm’s vee? To be fair this is all kind of emotionally advanced for teenagers (although I do love the headcanon blue and I share of Maddie getting Wilhelm high and explaining polyamory to him) so I can especially see this working for a post-canon fic that takes the characters into adulthood. I honestly feel like Wilhelm would have a very turbulent young adult period, because we really didn’t see him process what leaving behind his identity and family means in season 3; he has to do all of that in the imagined future. And I think there were a lot of cracks in Wilhelm and Simon’s relationship that were papered over by Wilhelm’s decision to give up the throne but not fully resolved. I can see Wilhelm and Felice reconnecting/hooking up when Simon and Wilhelm have broken up for a while in their mid 20s, and then Simon and Wilhelm reconciling and Wilhelm dating both of them. And by then I would assume that Wilhelm would be pretty deep in the queer/poly scene, and have friends who are in a similar relationship configuration to him. Of course I understand that getting rid of the sacred monogamy of Wilmon is not for everyone or even most people in the fandom, but as a poly person myself who supports the decentering of romance… long live the ot3 say I.
6. I guess I have a lot of aro/ace Headcanons! Our version of Ayub in Heart and Homeland (our regency AU) is aroace, and he’s one of the characters I write and I really enjoy writing him! He’s the chronicler of everyone’s adventures and he likes taking care of his friends/found family but also he’s happy to stay out of the romance drama. I think that could work for a canon compliant fic or interpretation of canon as well. Of course I also love our Sara/Wilhelm queer platonic partnership in Heart and Homeland, and it is frankly a crime that they never became friends on the show because I really think they would have could have come to understand each other in a valuable way (for instance I would love to see them talk about their shared experiences of anxiety, which Wilhelm probably has to a clinical degree and I’m sure Sara experiences as an element of her autism, like when she’s in a social situation she does not understand well). I also think Maddie could definitely be aro, based on the flippant way she talks about her hookup with Nils and her distaste for her friends’ romantic drama. But my biggest answer is Felice! I made a case in a meta which I wrote inbetween seasons 2 and 3 that Felice should have been queer as well, and I would have picked some flavor of aroace as her identity. I think it would have made a ton of sense with how she struggled with the romantic expectations being placed on her, and would have given her a way to relate to Wilhelm and Simon (without totally duplicating Wilhelm’s coming out arc).
8. I think both my answers to this are due to @bluedalahorse’s writing! When she initially pitched Rosh/Felice to me for Heart and Homeland I was kind of skeptical, but now I find it weird that they are ever shipped with anyone else. Blue is also currently working on a Stederika fic, and I’ve never been super into them before but I am very into this idea, so she may be converting me!
21. I think I’m gonna use this opportunity to shout out Frida’s acting! I really love when actors are able to convey a lot without words; there’s so much in the way talented actors listen, process, and react that can tell you so much about the character. I feel like Frida is really good at this especially. Sara is kind of an internal character— maybe that’s in the writing, or maybe it’s just in the performance. I can almost physically see the wheels turning in her head when she’s feeling shame or deciding to kiss August or pouring out her heart to Felice. I was happy Frida got recognized with some award noms after season 3, she really deserved them!
5 notes
·
View notes
Text
Do you have a diagnosis of ASD (Autism Spectrum Disorder) & love to paint/draw/sketch/collage/sculpt/collect various visually pleasing objects/create online visual media/mixed media/sing/dance/write/participate in any medium of creative expression as a means to communicate as a person with an intellectual disability? WELL I DO & YOU WILL DEFINITELY ENJOY IT AS MUCH AS I DO FOR I AM LEARNING TO BE PROUD OF THE BEAUTIFUL CREATIONS, CONTENT, PHOTOGRAPHY & THE PROCESS OF REPETITIONS INVOLVED IN MY TRANSFORMATIONS FROM RAW PAPER OR BLANK PIXEL SLATES TO WHICH I AMPLIFY THE BEST SENSATIONS OF COMPLETING THE SELF STARTED AND CHOSEN TASKS TO WHICH I COMPILE AND SHARE WITH MY STRANGERS WHO STUMBLE ACCORDINGLY TO MY TAGS ACROSS MY PAGE. I want to discover other humans, specifically people above the age of 18 who are either intellectually or learning disabled or co-morbid the way I am, at this point in their life, I’d love to hear about their experiences & struggles & random thoughts that pop to mind as shared along with their own thoughts about how they relate to each other’s creations… what circumstances led to this artwork being made & published & what is your name/handle/identity in your own words as the artist? I’m hoping for this page to be a place to make friends, especially even if you don’t create any art or writing or videography for yourself by yourself just yet, but plan on doing so in the first opportunity coming up with something inspiring you to go ahead and bite the bullet & stop letting people/places/things/because/but/fear driven overwhelming thoughts setting fear inside & preventing the accessible pathway from dipping your toes in the water & making a mess of mistakes bc they are so much more important to make than it is to be practiced in perfectionism’s which nobody succeeds at in this universe with or without the idiosyncrasies known to our community! This is a judgemental free space which has been made possible by the low functioning highly sensitive empath named Jacqueline Mae Gutwilik who has been going through worst heartbreak of her life post missed miscarriage12/22 & subsequent trauma caustic to her husband who is afflicted with opioid & crystal meth addiction which is now the scariest thing she is grieving on a daily basis for the past two years now (when she noticed his soul was not compatible with hers any longer for she started slowly catching up to the social cues, anxiety and pressure driven by her partner to make decisions about life that were harmful to her poor health problems in retrospect causing her Wilson Disease to deteriorate & displacing her from her comfort zone/stability by moving back to her childhood abuse/abandonment home & wound up w/o anyone b/c she had been living in an isolated domestic abusive cycle for 7 years before aware of it & her environment is NOT safe STILL to date; No matter how much she is a positive helpful, healthy, supportive to others around her, she cannot seem to make any progress or difference in her own life as per she is broken from her entire life lived trusting in the monsters who took/take advantage of her [as they victim shame her & cry wolf & dictate her life by making false reports to the police against her to try & control her or make her forced into homelessness] so she has no choice but to make her own artwork as she is doing the best she can to cope with the tremor from Wilson Disease symptoms that truly makes her feel unable to tolerate living alone in suffering while being unable to be as productive or professional or socially responsible for her own needs because she has changed exponentially from her trauma & ptsd & day to day problems that she cannot control anyone but herself & do her best to make better choices, which involves creating as much mixed/multi media prompts & writing snippets for sparking ideas for other people to join in & share their projects & play along with me, as well as hopefully find comrades with similar experiences in life through the process of learning w/their ASD diagnosis as transitioning from childhood to adulthood).
#jaemaebae#jacquelinemaegutwilik#highlysensitiveperson#women with autism#female artists#safe space#autistic artist#discord server for artists#discord server for autistic spectrum disorder adults#new discord server#adults with adhd#adults with autism#all are welcome#don’t be shy#autism pride#adults who create artwork#learning disability#intellectual disability#intellectual property#creative#unique#mixed media#abstract art#abstract#artists on tumblr#digital art#wilson disease#digital illustration#disabled#mental health
9 notes
·
View notes
Text
long post so i GUESS i’ll put it under the cut
so i’ve been really reflecting lately on my self diagnosis of autism, especially since i’ve been really coming into myself and managing my anxiety better than ever before, and ive been wondering whether it might be that the symptoms i thought were attached to being autistic are just how anxiety manifests in me and the things about myself that i thought proved that i dont have adhd in any way may also just be how anxiety manifests in me. because also even though ive really related with autism and the social symptoms, i’ve never really been sure i have sensory processing issues, at least not to the extent that the dsm specifies in order to be autistic. and what i really HAVE related to is the inability to just sit down and get shit done. so i took another self assessment with this clearer knowledge i have of myself and how i really function as a human being when im on my own and living as an adult and
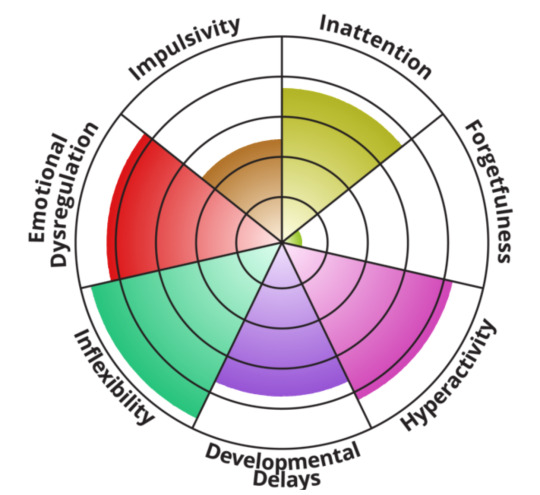
the only ones that arent high levels are literally the ones that i can directly pinpoint as one of my biggest concerns with my anxiety. impulsivity is the one that makes adhders more likely to butt into conversations or keep going on for a long time or make decisions and later regret them. as you may have noticed i am particularly long winded when im typing, but is that true of me in real life? like at all? not really. i struggle to get two words out sometimes. i was selectively mute in my childhood. i can say for a fact that the reason for this in my hyper-awareness of the potential of making a faux pas or embarrassing myself in social situations. and i have decision paralysis due to the same phenomenon. im very aware of the potential of disappointing other people if i make a bad decision. im not sure if impulsivity would manifest itself in the “typical” adhd way if my anxiety wasn’t there, but i have no way of ever knowing that because it is.
and forgetfulness. i beat that shit out of myself when i was younger. i can clearly remember a time in elementary school, then in middle school, then in high school (before i started writing sticky notes for myself) when i would get myself in trouble just simply because of forgetting about assignments. my family is very academically oriented. my parents wouldnt be SUPER mad at me if i was trying my best and didnt get good grades, but i knew they would be disappointed if i didnt try my best. i have so many systems in place so as to never ever forget about schoolwork any more. you have no clue how revolutionary it is for me that college professors actually put all of the assignments for the semester of the syllabus. one of my biggest gripes about high school was that the teachers would just assign homework seemingly at random? it was easy to forget if you werent writing it all down, ok? and for appointments? same deal. my parents kind of took care of the remembering appointments part before i got older and by now i do have these systems in place for myself. i do often forget to make calls, mostly because i dont make a point of writing it down as a task for myself because making calls gives me anxiety. yeah.
also i sat here and took this assessment and wrote all of this instead of working on my 2000 word midterm paper due next tuesday for which i have exactly one sentence written. listen, procrastination is a universal trait, but i just felt like it was relevant.
#not saying this necessarily proves anything#and of course i know professional assessment is the only true way to know#but i have anxiety#and possibly adhd#how do you think i handle the medical system?#i really shouldve had therapy at this point in my life but thats too difficult to get started lol#OH#also#i am fucking SHIT at creating habits for myself#i have to physically force myself to even go and brush my teeth every night and every morning#and washing my face only gets done half the time because its easier to not do it and i get bored if im in the bathroom too long#i have to make every task i do more interesting for myself or i wont do it#i used to hate taking time out of my day to even shower before i started listening to music in the shower#and i like to watch shows or videos while i cook or wash dishes or fold laundry#damn i maybe shouldve considered this more seriously sooner#i forgot to consider the world in which all social anxiety does not automatically equal autism#i need to stop typing now#i really have work to get done#ugghghhghghghhhhh#cloudy rambles
5 notes
·
View notes
Text
Unriddling the Sphinx: Autism & the Magnetism of Gender Transition
When people note that "trans children" tend to have autistic traits and that children with an autism diagnosis (particularly natal girls, but also boys) are massively overrepresented in the population that is referred to assessment and treatment for gender dysphoria, many trans people's (and allies') response is that it is a kind of dehumanization and denial of agency to claim that autistic people cannot be transgender, do not have the right to seek gender transition, or that they may be vulnerable to being exploited by the transgender healthcare system. Most recently, this claim has come up again with regards to a recent piece by Harry Potter author J.K. Rowling, where among many other things she notes the enormous increase in child referrals to gender clinics, including a disproportionate number of autistic children, to explain her reticence to endorse the political stances of modern transgender movements.
This is my response as an autistic woman, who was once an autistic child, who is a lesbian with experiences of gender dysphoria and who once wanted to transition to male.
-----
1.
Recognizing our vulnerability to social predation and to cultural systems that we do not understand because they were not made for us is not offensive. As autistic people, it is key to claiming our autonomy as a particular kind of disabled person. We often do not recognize our limitations in reference to greater social systems not because we are "too stupid" (i.e. cognitively or intellectually limited) but because we have different value systems than neurotypical people and hierarchical institutions built for their benefit. Autism is a pervasive developmental disability, and it is a way of being. It is not merely being a "regular person" minus various clinically defined psychological capacities or skills. It is a difference across all domains of life, and as a disability that causes differences in our social and sensory perception it is also a disability that causes differences in what we want and what we care about. Both those who exhibit condescending "concern" for autistic people and those people who naively defend our right to do whatever we see fit miss this component of being autistic. It is not that we are merely vulnerable because we are missing parts of our decision-making or social skills apparatus. It is not that we are merely being unfairly denied what we want to do, and our autism is immaterial, just some excuse for the denial.
It's that we aren't recognized as having wants, only "special needs". It's that we aren't given the skills to know what it is that we want, or that it might be different from those around us. It's that we are never told how to get what we want in safe and healthy ways, or that there is even a potentially safe and healthy way to get it. It's that we are deemed automatically pathological and empty of internal experiences as autistic people. It's that we're not given any help on how to navigate our deep differences from others and how to navigate being deprived of social resources and networking in a way that doesn't tell us to just cover it up and deal with it. It's that most people who dedicate their lives to "helping" us do not care about any of these things, merely that we can be trained to act in a way that doesn't disrupt the lives of neurotypical people. Given this context, it is far more insulting to me to insist that having autonomy renders us somehow invulnerable to exploitation than to correctly perceive that we are in fact an intensely vulnerable people. By nature of our disability, we are always on the margins of social resources and social networks, and exercising our autonomy unfortunately often puts us even further outside social acceptability and social protection rather than somehow shielding us materially from the consequences of living a self-actualized autistic life. Few autistic people are prepared for this when they begin trying to make decisions "true to self" in adolescence.
I believe nearly every autistic person is traumatized from the consequences of living in this world and what others do to us. Clinicians do not usually recognize that autistic children and adults can be traumatized, that there is even anything there to traumatize. (Why else could they feel so comfortable shocking us, shackling us, or feeding us bleach?)
-----
2.
I think because we are not neurotypical we often struggle to understand just why a neurotypical person would feel ok excluding us, or maybe even anyone. Many of us autistic people have little impulse to do such things, and if we do, we rarely have the social power to make someone that we've cut out of our lives unemployable, unable to access medical care, food, housing, and so on. But neurotypical institutions are set up, from top to bottom, to create hierarchies of value with extreme material difference between the top and bottom. They are set up to stratify the "worthy" people from "unworthy" people.
Autistic people are almost universally considered "unworthy" in these systems, and to the extent that we can curry favor from them we must consent to our exploitation: to entering into a transaction on neurotypical terms, where we can get some sort of worth through providing a "benefit" to this hierarchical resource system which is not made according to our value system or for us whatsoever. This is common to all marginalized people. But it is often particularly poignant to autistic people, who struggle to find community with any social group of human beings. There is no "elsewhere" for us, there is no "home". We are stuck, as they say, on the "wrong planet", and the spaceship was destroyed.
The idea that exercising our autonomy would protect us from this world rather than render us more vulnerable because we are refusing to transact correctly or refusing to provide a benefit is utterly absurd. Our autonomy is perfectly compatible with our continued social ostracization and exploitation. It usually coexists with our continued social ostracization and exploitation.
In social skills classes-- or just the wild, wild world-- you are not taught how to deal with the fact that everyone will hate you for being you. You are taught to be someone else. You are not taught about your native autonomy. You are taught about how to put your hands here or here, how to choose between actions that are condescendingly and ridiculously normal. You are not taught how to take responsibility in a way you understand, that is harmonious to your own values and others'. You are taught to hold yourself accountable for your abnormality.
So forgive me if I do not believe for one second that impersonal, well-funded medical systems that were built off of medically experimenting on intersex children and adults (the nightmares wreaked by John Money at Johns Hopkins) or psychologically experimenting on behaviorally aberrant children (UCLA, where behaviorist torturer of autistic children Ivan Lovaas tinkered with gender nonconforming children alongside conversion therapist George Rekers) have autistic people's self-defined well being in mind.
And forgive me if I do not think informed consent clinics have autistic people's self-defined well-being in mind when they're more interested in rubber stamping hormones while shielding themselves from legal liability than assisting autistic adolescents and adults, who have an intrinsically different way of understanding gendered social norms, navigate the enormous complexity of how to interface with the single most fundamental social fixation of the neurotypical world as someone who will always and automatically fail.
-----
3.
I do not think most gender clinicians even have the first understanding of what it means to be autistic and what this does in and of itself to your understanding of gender and sexuality. What J.K. Rowling said in her piece-- a straightforward accounting of facts-- is far, far less insulting to me than what Diane Ehrensaft-- one of the premier "experts" in the United States on pediatric transgender cases-- published in a peer-reviewed journal on autism. In a 2018 letter to the editor reading remarkably like new-age material on Indigo Children, she writes that she likes to call autistic transgender children "Double Helix Rainbow Kids" and declares us "freed" from the restrictions of gender as "more creative" individuals. This article ends with an anecdote about an eight year old autistic female child with limited language use who begins speaking, making eye contact, and relating more appropriately with clinic staff after she is socially transitioned by her family. Ehrensaft muses, "“Could gender be an alleviator for the stressors of autism?”
She is not the only one to pontificate about the magical changes a gender transition brings on autistic children. Norman Spack (the first clinician in the US to use GnRH agonists on gender dysphoric children as puberty-suppressing drugs) claims in a coauthored, peer-reviewed 2012 paper (insults upon insults, in the Journal of Homosexuality) that in his clinical experience the symptoms of comorbid diagnoses--including "problems with social competence"-- "decrease and even disappear" with gender treatment. In the same paper, this passage appears:
Although the question of whether gender dysphoria is simply a symptom of an autism spectrum disorder has been raised by mental health clinicians in the field, we feel it is equally worth questioning the validity of an autism diagnosis among transgender youth, particularly of those diagnosed with Asperger’s disorder. Perhaps the social awkwardness and lack of peer relationships common among GID-Asperger’s patients is a result of a lifetime of feeling isolated and rejected; and maybe the unusual behavior patterns are simply a coping method for dealing with the anxiety and depression created from living in an “alien body,” as one patient described it.
Do autistic trans people-- who rightfully protest against mainstream autism organizations focusing on a "cure" for autism rather than respectful accommodations for our differences and medical needs-- know that very well-connected, very respected, and very powerful gender doctors are claiming that gender transition cures the symptoms of autism? Do autistic trans people-- who rightfully discuss the implications of denying that someone can both be autistic and hold a meaningful gender variant identity-- know that it is an active clinical debate as to whether or not their disability and all its struggles is "just" a result of somehow ending up in the "wrong body"?
If they do not, they should know that this is how doctors are perceiving the pervasive issues that the children in their care are having: not as the result of a life-long, stigmatized, but eminently livable disability, but as the result of a mystical gender failure that can be medically corrected. That essentially, the disability "goes away" so long as outsiders no longer perceive a problem with a child's conformity to gender norms. That either an autistic girl somehow is transfigured into a non-autistic child through transition, or more likely, an autistic girl's autistic behavior is unfitting for her as a girl but not for her as a boy. That the "proof" of pediatric transition's effectiveness and standard of an autistic child's happiness is how much the child wishes to participate in neurotypical society on neurotypical society's terms.
I cannot pretend that this isn't ludicrously disrespectful to autistic people, or that it isn't a total erasure of our experience as human beings. To these gender doctors, the fact that a girl might see the world in a different way and care about different things and thereby struggle in a world not made for her does not matter whatsoever, except maybe as a tokenistic "journey" she can go on alongside her wonderfully progressive and affirming doctors. What "autism" is for them is a particularly severe and inconvenient social adjustment problem which can be forcibly corrected through body modifications, should an autistic child or adult rightly note that they can't do gender right and this is causing problems for them. They are more interested-- like in a long history of abusive and even deadly "treatments" for autism-- in correcting the problem for them than for the autistic person. How convenient for neurotypical people both the gender incongruous behavior and the social noncompliance goes away once you medically modify a child to look like the other sex.
I cannot be anything but sick that "increased eye contact" is a sign an autistic child needed medical meddling in the intimate process of navigating and negotiating their sexual and gender development. I cannot trust that these doctors aren't missing enormous parts of their autistic patients' experiences, if this is what they are so gleeful to report as a positive transformation and their justification for disrupting and surveilling children's bodies. What do they think of autistic people and those who are gender non-conforming if they are so willing to believe that existing as a person with a stigmatized disability is actually just a misdiagnosis for the pseudoscientific condition of being a man in a woman's body, or vice versa?
-----
5.
It takes many, many years and quite a bit of luck and support for most autistic people to fully understand and come to terms with how their autism affects them and sets them apart from both individual neurotypical people and neurotypical society at large. It takes years-- often far, far into adulthood, especially for those abused under a medical model or for those who went decades undiagnosed-- to understand the differences between social and non-social aspects of this disability.
It takes years to not resort to chalking up all of your own distress and difficulties to being a "retard".
I have not met an autistic woman yet who did not have extreme difficulty integrating her autistic differences in values with a broader sense of self that includes whatever version of herself she uses to navigate a world in which women's values are simultaneously invisible (since she has no right to determine them herself) and nitpicked to death (since it is important she complies).
In a world like this why would it not be difficult for autistic people to know when it is they are being fooled or exploited while participating in transgender communities or while seeking transgender health care? Autistic people-- especially those who are dependent on caregivers or health systems for basic care, as well as those who depend on the goodwill of their families, employers, or welfare benefit institutions to remain as independent as they can-- have to make continual compromises just to maintain enough acceptability to communicate with the outside world nonetheless do things like "make a friend", "go to the doctor", "find a job".
I do not think neurotypical people understand or care that when I speak or write it is always with a similar effort as with a second language. Language-- whether it is verbal or nonverbal, with all the extensive symbology of the neurotypical world-- does not ever get to be something other than "translation" for me. As someone with an Asperger's-profile of abilities who has studied the neurotypical world intensely for years, I have the opportunity to translate in a way that allows others to understand me at least some of the time. Many autistic people who are more affected live in the world which gives "autism" its name, where nobody cares to do the translation for us and we are left totally and utterly alone.
The 20th century philosopher Ludwig Wittgenstein (who, perhaps not coincidentally, was likely autistic) was fixated on questions about the meaning of communication. About whether a language of one could make any sense, about what it would mean to speak about something hidden from everyone else or perhaps even ourselves. In a famous passage debated vociferously, he wrote, "If a lion could speak, we would not be able to understand him."
Many have resolved the question posed by this statement by claiming that for fuck's sake, a lion is a lion, and has nothing to say.
-----
6.
Gender transition appealed to me because it was cloaked in the farcical notion that there was some version of me and my body that could finally speak directly. I never quite understood the whole Adam and Eve story as an autistic child-- just don't eat it!-- but if there truly were a serpent's apple for autistic folks it would consist of this promise: that there was a world where the glass and the fog would dissolve, that we weren't covered in a repulsive and bumbling slime made of our own desires to understand, that instead of our words and hands glancing off the skin of everyone around us we could do that magic everyone else could and hold someone's heart in our hands. I was fooled because like many struggling autistic people, I wanted the problem to be me. Because then it was fixable. I would let them take my only body (which was such a sensory drag) to convert me into one of these blessed transponders that normal people were, receiving and sending all these messages like shooting stars blazing through the unimpeded vacuum of space. Without my femaleness and without the Difficulties That Should Not Be Named, I could send whatever message I wanted to whoever I wanted and it would be received, I could be gregarious, important, sexually compelling; my will and autonomy wouldn't be stifled by 140 pounds of dumpy, itchy flesh with an overbite and slack hands.
When I imagined myself as a man I didn't imagine myself like most of the childhood boys I managed to ingratiate myself with, who lisped, repeated themselves, and tripped over their own shoes. I imagined myself as a musician who was absolutely magnetic, I imagined myself as a writer with a legacy, I imagined myself telling other guys they were stupid shits and they could fuck off. I imagined being able to hold onto a football without dropping it, being able to smoke weed without getting a migraine, being able to talk without squeaking or letting out a little drool.
I thought I would finally be a human being with no embarrassments and nothing that could get me bullied in the bathroom between class. I thought when I would say "no", other people would listen. I would enter whatever mystical world it is that Ehrensaft names, made of messages and meanings, where every twist of word and piece of clothing said something, connected by a fine filament back to that Necronomicon filled with the runes of social symbology. And it would make sense.
I would become a lion, not a house cat. And the lion would speak. And we would understand him.
-----
7.
It is a neurotypical narrative that this is what transition can do for you, because it is what someone else's transition does for neurotypical people. A gender transition is magical because it decodes the lion. It unriddles the sphinx. The autistic person must be happier now, because the neurotypical person is happier now. (And who has an empathy deficit?)
But if I have learned to be afraid of anything as an autistic person it is not my own neuroticism and fixations, but those of the so-called "normal people". Forget double helix rainbows: being an autistic person is like your DNA is a converted school bus trundling through the world in spray-painted glory and the whole world has an HOA. I understand why autistic people who see themselves as transgender see "concern" as the busybody stupidity of the neurotypical world. They aren't wrong. But it exists alongside other mundane and brutal busybody stupidities, such as grant funding, progressive saviorism, and psychiatric god-complexes.
To understand and resist what the neurotypical world communicates to us about our worth is not to protest back to them in their own language. I am an autistic woman and like many other autistic women I am tired of not only making myself more palatable but translating my existence into something intelligible to outsiders, who are both men and the non-autistic. Radical feminists miss one of these; trans activists and allies miss the other. But I am irrevocably othered from both.
When you are autistic you are taught only one symbolic structure. It is not your own, but it is the only medium you will ever have to communicate with any complexity. More sinisterly, it becomes the only medium we have to communicate to ourselves, the only medium we can use to work around the silent and jumbled parts of our bodies and minds. Am I hungry? It is not always obvious. To ask the question I find myself translating, even when alone.
My fantasy about lions and men was that whatever world a lion lived in and whatever he had to say, he did not need to translate, and especially never to himself. When a lion says something he does not stop to ask if he means what he says or who is saying it. When a lion looks into the water hole and sees his own reflection, he does not need to reconcile anything. The lion does not need to speak to understand himself. A lion is made of teeth and blood and claws and the lion just does.
I do not use the symbolism of transgenderism to explain the little gaps and incongruities that are my problems with gender, with my sexed body, with sexuality. It is not only a language born of neurotypical neuroses and regulation, but it is always and forever fundamentally a translation. As an autistic woman I have spent my whole life avoiding these dual facts, through both my time thinking of myself as trans and while trying to understand this whole thing afterwards: I am my body and I am not my body. Because I speak, but I do not understand. Because I understand, but I do not speak.
I will, unavoidably, always have to translate to speak and understand. But my autonomy requires that at bottom I must respect the native communication of my own body and mind. I refuse to use force or coercion to get it to talk, to interrupt its silence, to confabulate stories on its behalf, to speak for it using assumptions it cannot confirm or deny. I have to make peace with the fact that sometimes the blanks of my body or the redacted corners of my mind will say nothing. I have to make peace with the fact that translation is always inaccurate, that something is always beyond that constellation of symbols and words. The autistic body and the autistic mind have their own boundaries, and I refuse to believe that exercising my autonomy requires breaking them.
I do not know if J.K. Rowling knows this. I hope you do.
300 notes
·
View notes
Text
Annotated Bibliography
1-Zubala, A., MacIntyre, D. J., and Karkou, V.,Art psychotherapy practice with adults suffering from depression in the UK: qualitative findings from depression-specific questionnaire., The Arts in Psychotherapy (2014), http://dx.doi.org/10.1016/j.aip.2014.10.007.
This research was carried out in the United Kingdom in 2014 with ethical approval of Queen Margaret University of Edinburgh in 2011. The research aimed to find out how art interventions are used by art therapist to tackle depression in adults. 5 art therapists prepared a thematic questionnaire with specifics of depression and were surveyed in adults aging 18-64. The limiting factors of the research were lack of qualitative data collection and small number of research surveyors. The conclusions give away that various definitions of depression were given hence the final data cannot be accepted widely and may be used with caution. It also said that the arts therapists use mix methods of theoretical treatment depending on the client’s needs. The results supported various theoretical approaches e.g. verbal therapy, solution based therapy, narrative therapy, non-verbal and systemic therapy etc.
2- Waller, D, & Sibbett, C 2005, Art Therapy and Cancer Care, McGraw-Hill Education, Berkshire. Available from: ProQuest Ebook Central. [23 November 2020].
Diane Waller, Professor of art psychotherapy at Goldsmiths University of London and Caryl Sibbett, art psychotherapist, senior trainer and supervisor at British association of art therapy have presented Broadly theoretical perspective on art therapy and cancer care, this chapter of the book “art therapy and cancer care” is from the second part where the practitioners have contributed one case study in which patient tells that during her fight with breast cancer and therapy sessions she has seen the riches of life. Despite being fully aware of the illness of the body, the subconscious brain decides to intervene in the session and illness-free work was produced to alter the reality. Few sessions in-between informed severe helplessness and urge to fight the circumstances and few showed letting go of the pain eventually and being brave in the reality for what it is, these experiences ask the patient to come out of the mind and onto the paper. Art making demands next move continuously until you answer the paper hence you stimulate the brain.
3- Gress, Carol E., "The Effect of Art Therapy on Hospice and Palliative Caregivers" (2015). Nursing Theses and Capstone Projects. Paper 211.
This research was submitted to the faculty of Gardner-Webb University Hunt School of Nursing in partial fulfilment of the requirements for the Master of Science in Nursing Degree intended to answer the question of whether art therapy is effective on compassion satisfaction, burnout, and secondary traumatic stress in hospice/palliative caregivers through art therapy for the purpose of understanding and healing traumatic emotional reactions to events such as suffering or death. It was found out that emergency nurses in comparison to hospice nurses had more anxiety towards death and experienced symptoms of burnout. Emotional distance was the main reason of this for which art therapy sessions proved to be of better coping strategies that dealt with self-awareness, teamwork and cooperation by identifying each other’s emotional needs. Hence caregivers will be required to learn new ways of delivering care in hospice/palliative care.
4- Chong, C.Y.J. (2015). Why art psychotherapy? Through the lens of interpersonal neurobiology: The distinctive role of art psychotherapy intervention for clients with early relational trauma. International Journal of Art Therapy, 20(3), pp.118–126.
Chong presents in her article, the relationship of art and neurobiology in her article where she discusses the language of the mind and the language of the art both as the limbic dialogue between the subject and the object, and hence she puts forward the idea of art psychotherapy as the most valuable and trusted intervention whilst addressing mental conflict in early relational trauma or intrapsychic conflicts especially in comparison of verbal therapy and cognitive behavioral therapy, establishing art psychotherapy as the ultimate language of emotions and irrespective of logic as emotions and logic don’t really go hand in hand.
5- Celine Schweizer, Erik J. Knorth, Tom A. van Yperen, Marinus Spreen, Evaluation of ‘Images of Self’ an art therapy program for children diagnosed with autism spectrum disorders (ASD), Children and Youth Services Review, Volume 116, 2020, 105207, ISSN 0190-7409
This study was conducted in the primary school of the Netherlands and The article mentions the “images of self” programme run through children diagnosed with autism spectrum disorder under the supervision of art therapists, the therapy type was particularly art based, the number of participants was 12 children between ages 8 to 12 and the parents as the source of primitive informants, as well as the teachers and art therapists. All children showed anxiety and were reluctant with the experiment at first. The methodology used was mix and measurements of pre-test and post-test were determined, which collectively showed improvements in social behavior of children and happiness in the children’s mood was evident.
6- Cassandra Rowe (2016). Evaluating Art Therapy to Heal the Effects of Trauma among Refugee Youth: The Burma Art Therapy Program Evaluation. Sage Journals, Volume: 18 issue: 1, page(s): 26-33
The article opens by defining art as therapeutic tool where it is described that art helps heal mental illness and promotes self growth, followed by the importance of using art therapy clinically with the patients of trauma especially the refugees, emphasizing that art is so much related to symbolism and helps retrieve memories through visuals, therefore art therapy was ideal with the vulnerable refugees who had been displaced from homes. The experiment was run through assessment tools and the methodology was clinical and four validated tools were used with 30 participants with a follow-up to determine levels of increased or decreased behavioral problems.
7- Caroline Case, Tessa Dalley. 11 Jun 2014, The art therapy room from: The Handbook of Art Therapy Routledge Accessed on: 06 Apr 2020
This chapter gives detailed insight into the art therapy rooms where art activities may be carried out depending on the client group, the author has provided theory behind the practical setting of the art room, stating that art room can be a significant and memorable place for a client, because amidst of the chaos, the client may consider art therapy room as his/her solace and may use objects and his/her therapists as the remedial source of his/her internal or external problems. Meanwhile, potential triggers are mentioned in the chapter, for example an art therapy room by the view of a calm beautiful lake can also be a dark deep haunting because of the lake water where crocodiles can eat humans. Hence art therapy rooms differ with clients and are carefully planned.
8- Hinz, LD 2019, Expressive Therapies Continuum: A Framework for Using Art in Therapy, Taylor & Francis Group, Milton. Available from: ProQuest Ebook Central. [18 January 2021].
The chapter broadly explains the kinesthetic movement use in the expressive therapies continuum emphasizing that it is the basic mode of expression. When dancers move their bodies, they express through their bodies, without words, hence any assessment in art therapy that is preverbal meaning if we want to retrieve memories from the childhood, then kinesthetic movement can play a key role Kinesthetic movement and release of bodily tension are directly proportional, the more attuned is the body with nature’s rhythm, the less the bodily tension it carries Further explaining the importance of movement of body, the chapter establishes that according to research, action influences images and thoughts, which inform decision-making and hence action plays a vital role in cognition.
9-King, J.L. (Ed.). (2016). Neuroscience concepts in clinical practice. Art Therapy, Trauma, and Neuroscience: Theoretical and Practical Perspectives (1st ed.). Routledge.
This chapter covers basics of brain, neurons and neural network through which messages travel in the body’s periphery which is responsible for the humans to take actions and initiate and sustain behaviors. The chapter also establishes that just like every human is different, every brain is different and has it’s own individuality and pace of plasticity. And at some point some decision makings alter the brain’s structure due to intensity and demanding nature of the networks. The chapter further talks about genetic mutations as they are responsible for neuromodulation as each brain has some factors under which it is effected for example genetics, gender and environment so what we can do is When we combine multimodality imaging with a detailed clinical history, subjective symptoms, clinical observation, and objective neurobehavioral assessment, to define a patient’s unique strengths and weaknesses. We can gain greater understanding of the person.
10- Rubin, J.A. 2016, Marcia Rosal. Cognitive and behavioral art therapy. Approaches to Art Therapy: Theory and Technique, 3rd edn, Taylor and Francis, Florence. P 333
The chapter explains development in cognitive behavioral therapy and its models today, dialectical behavioral therapy, mindfulness therapy, cognitive therapy with both children and adults. The chapter establishes behavior therapy as the most ideal form of therapy in expressive arts therapy paradigm because it uses thinking to identify emotions, the feedback and reinforcement system of the brain motivates the brain muscles and instant creativity gives a sense of achievement. Making art can accelerate positive emotions because the drawing constantly awaits the maker to take next action, whether in a hopeful stroke or a stressful stroke, it produces an inner dialogue between a client and artwork.
1 note
·
View note
Text
Does a pregnant person having low Vitamin D levels affect the fetus?
I have to preface this by saying all these researchers are Australian and I’m in Australia so basically, this is fate... waazzuppppp.
Also I kept getting distracted while writing this. I’m fucked for a career in research
Now for actual research:
Background: Vitamin D insufficiency occurs in up to 60% of caucasion women and even more frequently with women with dark skin (OH BOY! As if POC don’t already have enough issues. So people are starting to ask how this affects pregnancies because everyone knows women are pregnancy machines who gives a shit how these deficiencies affect the women WHAT ABOUT THEIR BABIES! But I digress, it turns out that was actually an important question. It’s already been found in human models (aka... humans) that offspring of these vitain D deficient women are more likely to be language impaired, even after controlling for sociodemographic factors. But, as is with science, other studies have reported a fat lot of nothing.
So how do we find out if there’s a cause and affect without manipulating people and violating ethics? BY MANIPULATING ANIMALS AND NOT VIOLATING ETHICS! Yeet.
In animal models, where they manipulate Vitamin D levels through diet, offspring of deficient rats have developed schizophrenic-like behaviors, both behaviorally (hyperlocomotion) and structurally (increased lateral ventricle size), as well as altering dopaminergic pathways. Awkwardly enough, in mouse models, a decrease in lateral ventricle size has been seen, indicating that species of research is clearly important for drawing conclusions. Suggestions for possible reasons for this inconsistency is that rat neurons mature more quickly and are twice as likely to escape apoptosis. The more you know! Rat subjects also seem to have changes in anxiety, social behaviors, learning, and memory. (Oh Vitamin D and learning and memory? What a novel concept) So clearly vitamin D research is trying to tell us vitamin D is really important for brain functioning, especially when it comes to disorders that involve altered neuronal expression
This brings us to the question of the evening: does a mouse model with vitamin D-deficiency alter fetal neurodevelopment?? This study by Hawes, et al. specifically wanted to look at structure and protein function so, sorry guys, no biology-free explaination for this one.
Independent variable--wanted to look at stage of development (days 14.5 and 17.5) and vitamin D deficiency. So, there were 8 Vitamin D Deficient dams (VitDd) and 8 Control dams (VitDc) for 14.5, and 8 VitDd and 6 VitDc dams for 17.5. Also I fucking love this perminology in the paper “Dams were euthanized with an overdose of ketamine and xylazne” which could easily be paraphrased as “oh ya, we drugged our rats to death LET’S GO SCIENCE”
Tissue was collected and frozen at the timepoints 14.5 and 17.5, and each dam had about 6 offspring on average.
Tests: Blood tests confirmed the dams (moms) were in fact deficient in Vitamin D, as well at the offspring. They ran tests to determine whether or not specific genes of interest were being expressed differently in the VitDc and VitDd groups. Genes/proteins of interest were: BDNF, Tgf-β1, Foxp2, and Th.
BDNF- was selected because it is a direct target of Vitamin D Receptors (VDR), and plays a vital role in neuroprotection throughout the brain. On E14.5, BDNF production was reduced by 55% in female pups and 62% in male VitDd pups. However, on 17.5, there was a 4.5 fold increase in females and a 1.5 fold increase in males. The authors suggested this might be compensatory. The reduction in BDNF on 14.5 may have lead to damaged neurons and production of dopaminergic, which might have triggered an increase in production by 17.5 to compensate for this damage
Tgf-β1- was selected because it’s a growth factor important in neuronal survival and neuroprotection of dopaminergic cells. On E14.5, levels were unchanged. However on E17.5, females had a 2.2 fold increase, and males had a 1.5 fold increase. The explanation likely ties in with BDNF, as the two have related functions.
Foxp2- was selected for its role in speech and language development, which has been shown to be altered in offspring of VitDd mothers. It’s implicated in dyspraxia, dysphagia, impaired expressive and receptive language and also pathways disrupted in some cases of Autism Spectrum Disorder (ASD). On E14.5, it was reduced 30% in females and 32% in males. 17.5 showed a 2.4 fold increase in females and 1.5 fold in males. Noticing a trend here? In IHC, which yielded a visual for expression in specific location, there was a 69% decrease in females in the fetal cortex, but no change in expression in other locations. You can see there is a trend of decrease in the females in the Caudate Putamen, although not technically significant (Images C and D). In Images A and B, you can see a significant darkness in A (VitDc cortex) compared to B (VitDd cortex), which represents the decrease in expression between the two groups. I’ll explain IHC someday.

TH- aka, tyrosine hydroxylase, is the rate limiting enzyme for dopamine synthesis as detailed in another post of mine. Day 14.5 there was no difference. Interestingly enough, 17.5 yielded a significantly higher expression in ALL females compared to males, regardless of group. Between groups, though, There was a 67% decrease in VitDd females, but no change in males. In the substantia niagra, TH density is reduced by 71% in VitDd females, but not in males. In another post of mine, you can see you this might affect voluntary movement (and also see how the cortical reduction of Foxp2 might alter decision making)
What I primarily get out of the article (and what the authors didn’t see coming) was the extreme sexual dimorphism here. Females in VitDd groups seem to be MUCH more greatly affected than males. Further research is necessary to figure out what’s going on. Also the authors state “it is well known that dopamine neurons exhibit a sexual dimorphism in their number and location in the brain in both mice and humans” but bitch the fuck I didn’t know that??? That’s really fuckin important how did you just breeze past that? Oh ya because nobody in research gives a shit about females. Slight tangent but vaguely relevant: oestrogen found to regulate TH expression in mouse midbrain? Which could partially explain the difference Additionally, NMDA agonist response in VitDd males more responsive, which is weird considering everything.
Sorry if this post was scatterbrained. There was no behavior or functional examination so it’s difficult to draw conclusions about meaning from this study alone. More information is definitely necessary but it a big thing people can get from this study is that there is definitely something biologically going on with dopaminergic neurons when Vitamin D levels in pregnant mothers is deficient.
Hawes, J., Tesic, D., Whitehouse, A., Zosky, G., Smith, J., Wyrwoll, C. (2015). Maternal vitamin D deficiency alters fetal brain development in the BALB/c mouse. Behavioural Brain Research. 192-200.
24 notes
·
View notes
Text
Ehlers Danlos Society Awareness Month (Day 31 Community)
Not all health conditions have what they call a community or a group of others with the same condition coming together as a group to be with, support and help one another. Let's be honest, most conditions don't need a community. There's a lot of conditions that are very cut and dry and easy to understand. There's a group on Facebook for everything but I can tell you right now there's not going to be a ton of people in a Hemorrhoid support group. The EDS group is a very close knit group with much value and importance to those who are part of it and I'll be explaining some of those reasons.
Of course one of the most obvious with having a rare disease is to be able to meet someone like you. To know others exist and to share similar experiences with. You know you can always find someone there that truly understands what you're going through having a condition so disabling you tend to lose most, if not all of your friends, some even lose family. Rather it be due to lack of understanding, lack of belief, fear, or any other list of reasons it seems to happen to all of us. So this is a way to make friends just like us. Friends that won't resent us for the physical abilities we have lost or the lifestyle changes placed on us by this syndrome.
Another reason is well because it's rare. It's surprisingly difficult to find any good information about EDS on the internet when you first get diagnosed unless you know where to look. In addition to this being a condition that lacks studies and research it's also extremely complex. In fact before being diagnosed, even with going to nursing school, I had no idea something this complex existed. If you are ever trying to find reliable information about a specific aspect of EDS it may be really hard to find, especially if the topic you're looking for is very specific. You can go into groups. A lot of individuals have certain documents bookmarked or saved in a word document or spreadsheet and can lead you in the right direction. If we can't find a study done in something we can also use support groups to do our own informal studies. Just simply create a pole and let everyone chime in. Before you know it, if posted in a larger group you'll go check out your pole and may have two or three hundred answers to your question.
Next, with EDS pretty much any body structure is a free game which means lots and lots of comorbidities. A good number of comorbidities are common amongst us which means we always have someone to relate to and ask questions to. In addition to this you can expand your groups to include groups for people with those comorbidities further extending your knowledge and possibility of friends. Most doctors don't know anything about these conditions so that leaves it to us to learn everything there is to know about it. When you finally think you have read everything there is on the web, others read thousands of sites or journals you haven't come across and ones you have read they didn't know existed so it's all about learning together and having people who understand.
Being a condition that is so very painful and severely affects sleep as well as causing many of us great depression and guilt for what we've lost and the deterioration our body has been through as well as the feeling of loss. We feel guilty for everything we put out families through, for needing help, for canceling plans and letting people down. Not only as if what we once were has already passed away but also the loss of friends, many times every single one we had before this illness and sometimes family members. We grieve the loss and are angry to learn that people we thought were our best friends and would never leave disappointed in us like a used paper plate. This is also the time it dawns on us how many of these people used us when we were healthy to provide them with things we need. Most of us have OCD or are on the high functioning side of the Autism Spectrum so tend to take responsibility and do things right, including not letting down our friends and family very seriously. Most of us thrive on routine and rules and chronic illness often gets to a point that a lot of this is no longer possible forcing us to make decisions last minute, change them or cancel them last minute, not be able to complete things by a time we have set for ourselves etc and that's really hard. It's helpful to know others who are or have been going through the same thing and to know you're not alone, not the one letting yourself and others down and to be told it's okay and it's not our fault.
The majority of us also have Medical Trauma Induced Complex Post Traumatic Stress Disorder. We spent years of our lives rather you're lucky and got diagnosis in two years or ate 70 and have spent the last 55 years actively seeking a diagnosis we all have to fight for one, to see doctor after doctor and oftentimes the worst part of it all, be miss diagnosed with psychiatric disorders such as anxiety and Conversion Disorders. These are extremely dangerous and life threatening diagnosis for us because it essentially closes the door on even looking for a cause of what is going wrong with us. Conversion Disorder is a Diagnosis given after all other conditions have been ruled out the problem is, doctors use it as a crutch to not have to deal with us. We are also superstars, especially in the beginning at having beautiful results when it comes to basic blood tests such as a CBC. The problem is, again, doctors are known to cut corners because they like the majority of mankind are lazy creatures who tend to want to just get the job done. It doesn't matter if it's thoroughly done and done with utmost care to put as much effort into it as they can, it's just done and to them done is good enough so they do the common tests and call it done, close the book and slap a label of conversion disorder on us that follows us around for life for every other doctor to use as an excuse to say they are done too. It takes years to find a doctor who is in it for the better of the patient; one who is up for a challenge; one who is willing to do more testing and testing that is more advanced and most importantly, a doctor who believes us and is willing to go the extra mile. It's when these less common tests like a Tilt Table Study, Gastric Emptying Study, Urodynamics Testing, Upright MRIs instead of doing them in the prone position, Sweat Testing, a Sitzmark Colon Transit Time Study, a 24 hour urine test to measure histamine levels, skin biopsies and ultimately EDS Testing via either the Brighton score system along with a through study of the body and some questions used to determine a positive or negative diagnosis or Genetic Testing to determine a type of EDS that has a genetic mutation that has been discovered. Not all forms of EDS have had their genetic mutation discovered yet which is why the other study is so important. There are more tests that can be utalkzss than the ones mentioned but as you can see, none of these are tests that are done on a routine basis and a lot of doctors don't want to deal with them slapping the psychological, "all in our head" diagnosis on us prematurely.

This results in us without a diagnosis for what we have going on with our body. When this happens we aren't receiving treatment for the symptoms we are experiencing allowing them to escalate. To make things worse we are often given the wrong treatments, handed antipsychotic medications that cause even more adverse symptoms and don't work. When they don't work the doses are increased higher and higher resulting in more to go wrong with our bodies. This also closes the door to treatment causing doctors and hospitals to dismiss life threatening issues, sending us home when we are actually so sick we should be in the ICU. I myself was declared clinically dead at least 10 times before my diagnosis, four because my heart stopped and I went into cardiac arrest and the rest because my blood pressure would drop below 60/20 which in the medical field is a pressure that is considered legally dead. With all but one of these I was sent home within an hour to a few hours of it happening simply told that was weird and sent home on paperwork for Conversion Disorder, Hypochondriasis, or some other psychosomatic disorder and is I was lucky this would sent me discharging me with a diagnosis of low blood pressure and that was that. One of my codes my mom was in the room, thank God for her. When I code no one came. My mom went running down the hall begging for help pleading for a nurse to help because no one was running to my room. The nurse told her I'm probably faking it and just pulled my leads off and told my mom just to ignore me because people like me feed on attention. My mom ran back to the room and thank God had some medical training as a girl scout leader because she had to take first aid and CPR. My mom brought me back. The nurse walked in right after and checked my wires. They are still in place. My state as well as several others protect their medical personnel against malpractice suits so there was nothing we could do. I've been sent home with gastric ischemia which is a life threatening condition where the blood pressure increases to dangerous levels in the intestines. It can cause the pressures to get so high it bursts and dissects blood vessels in the intestines causing a person to bleed to death. I was sent home with a diagnosis of General Psychosis and Anorexia as well as treated for anemia and vitamin deficiency. They blamed it on anorexia, not the fact I physically couldn't eat and was having bowel movements that were nothing but pure blood that everyone. Refused to look at. I had an allergic reaction so bad it almost killed me and was sent home diagnosed with conversion disorder and sent to my doctor who wanted me in ICU but upon refusal from the hospital to see me again even with my vitals so poor my doctor had to take care of me basically sending me home with what I called a take home hospital and working with my mom over the phone to take care of me available all hours of the night. I had a nurse try to give me 50 times the dose of this same medication that caused this. Been sent home with intestinal blockages, hernias, extreme dehydration, a UTI after they said the results came back negative only to get them in the mail a week later to see they were positive and by that time my UTI was so severe I had a kidney infection and was in kidney failure. I've sat there days and nights in a hospital bed where nurses refuse to answer my call light saying I have a conversion. Disorder, don't need to be there and I'm wasting their time and resources taking up a bed for someone who is really sick and that they won't be coming anymore the rest of the night not knowing I was one of the sickest ones on the ward and just misdiagnosed. I've had nurses rip IVs out of my arm, ya know how they push you to your car when you're released? There are a lot of times they pull my IV, tell me I'm not sick anyway and can do it myself having to take multiple trips to get my personal belongings out of my room. When I lost the ability to walk I had multiple doctors tell me I could and would pick me up, put my feet on the ground and the. Let go of
dropping me on the floor. This happened a lot at OSU with their doctors. Again and again dropping me and seeing I didn't have that natural response to catch myself and went straight into the hard tile floor with my fragile and damaged connective tissue would they say hmm. You really can't walk then send another doctor in who would do the exact same thing. I got picked up and dropped four times by four different neurologists just in the first week of being paralyzed and it's happened time and time again after that at other neurology appointments. I could go on and on. This is the stuff a lot of us go through. It's extremely common with EDS, most of us have complex PTSD.

Most of us have an extreme fear of going to the hospital because that's when we are at our worst and at the same time, a time we get treated worse than anywhere else about our chronic illness. We go in knowing it's a game of Russian Roulette with a really high chance we will be sent home sicker than I came in. Worst of all, there's no way to treat our PTSD because it had to be treated by a doctor, the people we have the least trust in. Not only that but the cruel mistreatment never ends. Every hospital visit. I have had good nurses before but I have never gone to the hospital once where I can say everyone was good. I hear a lot of healthy individuals say endless good things about the hospital staff they had or they have some reason they have to go. When you have a rare invisible illness like EDS we aren't given that same care. The appalling lack of medical care never ends therefore it's impossible to even treat our PTSD. It's not like someone in the military who is in a war and when the war is over, it's done, they never have it go back and can get treatment and start to heal. It's like having to live the rest of their lives in that war as a POW who has been captured and imprisoned by the enemy and every time they get out they are found and imprisoned by another enemy and another enemy and then going to see a psychologist who happens for this only to find out the psychologist is one of those enemies from the other side who captures and holds others line you as POWs yet wants to try to help you get over everything that has happened to you even though you're still occasionally been tending by someone else and beat up before getting away again. Seeing a psychologist for us just doesn't work. We have no trust in the medical field and the gross mistreatment and lack of care is never ending. The EDS community can relate to this when one else can. While the healthy people we know, the people we grew up with, who became nurses and doctors themselves get mad telling us those doctors and nurses are heroes, they can do no wrong. That stuff doesn't happen, they are made up of the most caring and compassionate individuals. Those in our community and other rare or invisible disease communities know that degree of mistreatment all too well. We know the truth about the medical field.
We know they are no different than any other company. Identical to the people making minimum wage in a more trivial position such as a greater at a retail store. There are the good ones who take their job very seriously and want to do their job to the best of their ability truly valuing hard work and are highly motivated individuals but most people at a job are just working because they have to. They have bills but if they were multimillionaires there's no way they would be there now. They want to get the job done and go home. It doesn't matter how they get it done, it's just got to be done. These are quantity over quality people. They take working smarter not harder totally wrong, defining it in their mind as taking any short cut necessary to get it done. Ya know how at most jobs they would have, for example, 50 people but there are three of them that seem to pull all the weight. The three everyone thinks takes things too seriously because they hardly leave their desk or station. They don't take the time to walk around socializing and joking around with their peers. When things get behind they are the ones who stress and work really hard to get things caught up where others say I'm not getting paid any more, I'm not going to bend over backwards and stress about if they aren't paying me more. The three people first to volunteer for overtime and the least to grumble of the boss asks them to stay over another 15 minutes to finish something while on the other days a boss May say that if you get your work done you can go hike and everyone rushed to gst the job done to get out the door while those three are left sitting there at their desks to get the job done right whole also correcting others work that was hastily submitted so they could go home or start the weekend early. Just because someone is in the medical field doesn't make them any different from those who hold other jobs. If most of them won five million dollars they would be out of there. Forget the two weeks notice, heck they don't have to work anymore. Someone else can take their patients. If they're told its slow and they can go home when all the patients are out then one more comes walking in the door as they are packing up their stuff there are a lot if doctors will look to the people who are still working and say hey, I'm about to head out of here, do you mind taking this last Patient? It's human nature.

As generations have gone on more and more people are lazy and the medical field is no exception. When you're chronically ill and have spent a lot of time in the hospital it gets really easy to spot those three people. The ones who if they were multimillionaires may cut back their hours but would never dream of leaving their job because their job means more than money to them. They take great pride in making people better, getting them diagnosed, saving lives and they can't see life another way. Those are the good ones. The good ones line any other job. They are far and few, they pull all of the weight, are walked on by other staff members, their managers usually fail to see their accomplishments as they don't spend a lot of time just hanging out with workers at a patient's expense. They are the ones who will advocate and fight for their patients to all ends but like any other job, maybe five percent or one percent or any other single digit percentage of the employees are these people so EDS patients my get one person on their care team that is amazing, maybe two but will never get a whole care team and it seems like the good ones get more far and few the higher the position. I've had more caring and compassionate house cleaning staff. STNA's, more good STNA's than LPN's, more LPN's seen to be there for the patient then RN's and more RN's. Doctors.
I don't think I've ever had a bad Volunteer at a hospital. The volunteers just love to be there for the patients, to put a smile on their faces and to know they made a difference in our lives. Rather it be to bring us a coloring book and crayons, their Emotional Support Dog around to visit us (which is my favorite) bring us a warm blanket or fill up our water containers. I've had one bring me a card and a flower in a small tube of water. The volunteers are there because they want to be there, not because they have to be there. It seems like the higher the person is on the pay scale the more people are in it for the money. Money talks even if it's at the patient's expense and usually if you have a complicated or invisible illness like EDS you are the expenditure. A community is important to know we aren't alone, to share their experiences, some in the group have become medical advocates and will fight for others in their area who can't get the help they need. These advocates, especially the ones with lots of training are invaluable to the EDS community. They may not be able to fix our problems but it's nice to know there is someone out there who tried. When you're at your worst advocating for yourself is extremely difficult and sometimes impossible and oftentimes our families don't do a lot of research on their own so aren't able to advocate for us so having someone who can is more beneficial than words.

As you can see there are so many different reasons community is important and vital to all of us. Some use it simply as a way to relate or a way to make friends like them after losing the friends they had before their health declined to the extent their healthier friends no longer could relate to them and left. Many are involved in the community to gather information and gain knowledge about their conditions. Support groups are also there to talk, especially with so many who have PTSD. We can't trust a psychologist, psychiatrist or therapist as they are medical professionals and talking to a live person is more fulfilling than writing a journal that no one reads. Sometimes it's as if these individuals, having gone through this themselves, know just want to say and how to help us. Some are there as a medical advocate in their area. Someone who can be there for them in medical situations or even just to give them advice as to what to say to make doctors listen, direct them who to contact if they aren't receiving appropriate care and what to do or ask for from our medical personnel. Some even use these groups to find names of doctors that work with EDS patients or places to go where they may be able to get help or even ideas of what treatments work for others with similar comorbidities. There's even a few groups out there run by people who were medical workers before EDS ravaged their body to an extent that they had to leave the field. It consists of disabled nurses, doctors, radiologists and various specialists. This group works to tell us if we need a second opinion. We can post test results or imaging onto the page and since legally they can't have a diagnosis since they aren't currently working they give what's called a "non expert opinion, telling us what they see or would suspect and if we need to see someone else. I find all of these viral and that's why I see the EDS community as not an invaluable and essential part of my life and wellbeing as an individual with Ehlers Danlos Syndrome.

0 notes
Text
What’s in Your Stash? Christina Forbrich, Founder & CEO of Canncierge Consulting
Sharon Letts of High Times Reports:
An educated, finely honed, purposeful stash.
Christina Forbrich found her niche in the cannabis space after helping herself with the plant as a teenager. She dove deep into the science of the plant in college and came full-circle back to cannabis as remedy as an adult for myriad symptom relief.
Her consulting company, The Canncierge, is a play on words from a hotel’s concierge—someone who assists with whatever a guest needs. Not a far stretch from Forbrich’s business of customizing, what she calls, a “canna-plan” for each client.
“My work is personalized cannabis education, enabling folks to make informed consumption decisions,” she shared from her home in San Diego. “Each consultation begins with an interview,” she continued. “Then I synthesize their information to create a plan for integrating cannabis into their lifestyle.”
Clients are educated on plant compounds and applications, while providing references to legitimate research and resources aligned with their needs, with a focus on women and seniors.
“I have some male clients and have worked with entire families,” she added. “I don’t make too much of a differentiation between the medicinal aspects of the plant and recreational use. The main goal is to not have them overmedicate, get discouraged, and give-up for lack of information.”
Self-Medicating at 15
The forty year-old mother, wife, and entrepreneur grew up in Southern California. Her first time self-medicating with cannabis was at age 15, which is a surprisingly common admission for most adult patients who struggle with symptoms from the Autism Spectrum. This includes anxiety, depression, ADD or ADHD, and PTSD from any number of traumas.
“My first experience was out of curiosity,” she explained. “Very quickly – within a few months – I found cannabis to be an effective remedy for crippling social anxiety, stemming from a chaotic home life. As a bonus, it also treated excruciating menstrual cramps that left me physically and emotionally ill.”
Diagnosed as a young adult with Anxiety Disorder, with episodes of depression, Forbrich found that cannabis was a practical remedy for relief; including treating hip and back pain from years of injuries from playing soccer as goalkeeper, then irritated from childbirth.
In 1996 Forbrich turned 18 and was able to vote for California’s Proposition 215, making the state the first in the country to legalize cannabis as remedy. At the same time, she was introduced to Dennis Peron, founder of the Cannabis Buyers Club in San Francisco – one of the first cooperative care programs in the country.
“When all my friends were drinking copiously, I was more interested in the herb,” she said. “I substituted the herb for Advil and it worked. I saved stems and made tinctures before it was a thing. In college I studied Sociology and Economics and became, what I call, a ‘citizen scientist” of the plant – informally studying, not only the botanic and biologic characteristics of cannabis, but experimenting for my own benefits and knowledge.”
In college, Forbrich said she would study high, take tests high, and then compare the results when not medicated. She said she always killed it on the exams when using cannabis, as it gave her focus.
Forbrich laughs at the memory of excursions to the library, with most of the literature she found on cannabis on microfiche only, pre-internet.
Since California legalized for recreation in 2017, Forbrich said establishing her company in the same year was a given.
“Since college I’ve been the resident weed coach for my family and friends, which is the reason I began my consulting company – it was inevitable,” she surmised. “I literally professionalized my passion, and I’m beyond grateful to be in the space in this way.”
Courtesy of Christina Forbrich
A Canncierge’s Purposeful Stash
Forbrich’s stash is kept in a handmade bag by Lisamarie Gonzales of CannaCoutured Stashbag, hand stamped with a cannabis leaf. The container holding flower is made by Canlock, and she says the jar is designed to express air out, keeping the bud fresh.
Spirit of The Herbs CBD Salve, made by Holly Hoops of Denver, is a go-to for skin issues, including her child’s eczema. She also uses it for aches and pains, plantar fasciitis, back pain, and more.
Her vape cartridge is made by Select Oil, and is filled with White Rhino, which she says is a consistent formulation, but she also gravitates towards small batch mixes from Out Co.
Sublingual Strips are made by Craft 1861, and are infused with CBD.
“I love the strips for freshening both my breath and my mood!” she laughed. “They come in a couple different dosages, so it makes it easy to personalize. They taste nice, work well and are discreet. My friend Eric Lujan is the maker – he’s a dogged advocate for cannabis reform, as well.”
Her go-to for menstrual cramps are cannabis vaginal suppositories in combination with a heating pad.
“I get extremely weepy and sensitive before my period, with Humane Society ads reducing me to bawling pretty quickly,” she shared. “Physically, on the day of my period, I feel nauseated, so this is when I’ll go for everything in my stash, and practice, what I’ve termed as, ‘Layer my Lifting,” combining products in a strategic way.”
She’ll use a 1:1 THC/CBD tincture, and dab a high THC concentrate to medicate for a longer duration of time. If it’s a workday, she’ll only do the 1:1. Using cannabis is proactive, and knowing what works via trials with successes and fails is the way most patients find their dose for what ails them.
“These are conditions I used to pop a pill to relieve without blinking,” she added. “I find that the combination of different modalities is essential to my cannabis consumption, and that thoughtful application of cannabis addresses my symptoms in a much more natural – and enjoyable – fashion.”
That said, after trial and error, Forbrich admits to keeping one pharmaceutical in her protocol.
“Cannabis replaced pain killers and has allowed me to reduce my dose of Zoloft substantially,” she shared. “I’ve been on more of it, on less of it, and completely off of it; and my doctor and I have found that my anxiety is very balanced on a dose of 100 milligrams – it works with my brain chemistry – along with the cannabis protocols.”
Forbrich said that the introduction to Cannabidiol into her regimen allowed her to skip every other day of taking the Zoloft, in effect, reducing her dose by 50 percent.
“I also use the plant to enhance my workouts, to focus, for socializing, and for creative work,” she added.
The tincture in the green bottle is homemade with MCT oil, made in a Magical Butter Machine with high quality trim and bud from Forbrich’s all-time favorite cultivar, Lemon Larry OG.
Another favorite found in many of the best stashes, is a pack of Raw papers and crutches, by Josh Kesselman, who is also one of the industry’s favorite characters. Raw papers are Vegan, made from minimally processed organic hemp fibers, with no dyes, chemicals or whiteners.
As quoted in Inc. magazine, Kesselman says, “Everyone wants to smoke the best… It’s like how people don’t want to eat Wonder Bread anymore – they want to eat all-natural, ancient grains.”
Lastly, the little pink pin is a nod to her sisters in green, representing the Pink Haze Society; a cannabis club for intergenerational women in San Diego.
“I still see cannabis legalization slowly moving toward every state,” she surmised. “The people want it. There are more and more people eschewing alcohol and drugs every day. I see the industry-side becoming less equitable with a serious diversity problem, not relating to the people. There’s been a lot of pain and set-backs, but I also see women, people of color, seniors and Veterans at the forefront of leadership – and this gives me hope for the future.”
TO READ MORE OF THIS ARTICLE ON HIGH TIMES, CLICK HERE.
https://hightimes.com/culture/whats-your-stash-christina-forbrich-founder-ceo-canncierge-consulting/
0 notes
Text
MIKEY’S PERSONAL BLOG 116, August 2018
Last Saturday afternoon, I decided to spend my day off work by visiting the Mornington Peninsula Regional Gallery for the National Works on Paper 2018 exhibition. It’s not very often that I have a day to myself to not worry about the many commitments in my life. Being on open area at Dunns Road Reserve, there was absolutely no protection from the strong gusty winds blowing over the peninsula. As it turns out, today they had some artist talks on that afternoon and I figured that I might as well stick around for at least one of them.
The first talk was by Cameron Robbins who produces “wind drawings” using a wind machine which features many turbines, pulleys, wires, a rotating drawing board, a weather vane and a black fineline pen. Along with the MPRG curator Danny Lacy, Cameron discussed how variables such as the wind speed, wind direction, rain and sunlight impacts on what the drawing produced will look like. He also brought up concepts like Chaos Theory and Fractal Design as inspirations for his work as an artist.
The artist talks drew quite a large crowd today of around 50-60 members which was very unexpected. I had a brief wander around the exhibition and was very impressed by the high quality of the artwork. Lots of hours and so much detail went into these pieces which covers everything from paintings and drawings to sculptures, collages and mixed media works. Whilst I’ve pretty much gone on hiatus as an artist myself, I will always have a huge appreciation for art and fellow artists in the community. https://mprg.mornpen.vic.gov.au/Exhibitions/Current-exhibitions/2018-National-Works-on-Paper
On Monday night, I had my second session with the Men of Doveton health and fitness program at Doveton College. This week we started the session downstairs in the gym where we did some footy training lead by Mitch from the Casey Demons. It’s actually been about 16 years since I last did anything football related and re-learning the sport tonight brought up some emotional issues in me from high school. Part of it is that fact that I’m not the biggest fan of footy and never really got into it. http://www.melbournefc.com.au/casey-demons
Playing any kind of team sport during my P.E. classes was something that I really didn’t enjoy whatsoever. I had fears around being hit in the face by the ball, being tackled by other students, doing something dumb if I was in possession of the ball and been made fun off because I was really terrible at footy. It was a huge weakness of mine both ball-handling skills and getting involved during a game.
Thankfully tonight, all of those hurts from the past have been laid to rest. All the guys in the Men of Doveton program are starting at ground zero and this is very much a supportive and encouraging environment. The aim is to basically just have a go and participate as much as possible. We started by doing some hand balling at a distance of 5 meters then doing some kick-to-kick at 10 and 15 meters.
Of course the footballs were flying in all directions but it was honestly fine. It was all about having fun and not taking things too seriously. I did well to not let that 16 year old version of Michael Dixon out. He would have been off the footy field trying everything possible to avoid the ball. Next we did a few games and drills, learning how to bounce the ball properly, aiming and kicking at goals and avoid being tagged by other players.
Lastly, we got divided into two teams: the plains and the whites and played a game of basic footy with just hand balling and no contact. This was another thing I used to struggle with back in high school is that nobody ever passed the ball to me because they knew I was a weak player and would end up making the team lose. But again that stuff was a long time ago and I did my best to get involved by passing the ball around and being distracting to the opposite team. It actually felt good participating in a sport I haven’t played in a very long time.
The second half of the session focused on mental health issues. After catching our breaths (Seriously so not used to running up and down a basketball court), we returned to the theatre and Mo gave everyone a journal for us to keep and write down any positive thoughts, things that we’re grateful for, reflections etc in. Writing is a huge part of me and probably the area I have the least amount of difficulty in. However, I do sometimes get forgetful and need to remember to actually do it.
Lastly we had a guest speaker named Greg from Beyond Blue talking about his personal experiences with Bipolar disorder. Being an Irishman, we was very animated and funny but also understandably nervous about sharing his story. I could very much relate to his degree of denial and assuming that “I’m fine” after one or two counselling sessions. There are always underlying issues to be found and back when I was originally diagnosed with depression and anxiety over 10 years ago, I wasn’t ready to open up or unpack my baggage. https://www.beyondblue.org.au/get-support/get-immediate-support
The most important things I learned from Greg’s talk is the importance of finding the right counsellor or therapist for you, having lots of support and people you can trust in, not being afraid to speak up about mental health issues, accepting that it’s okay to not be okay as well as express normal human emotions. I really didn’t feel comfortable enough to speak up about my own issues in this large group setting but it’s something that I’m working towards. https://www.caseystadium.ymca.org.au/whats-on/upcoming-events/event/men-of-doveton-free-health-program-2
On Tuesday night, I attended the first of four NDIS workshops hosted by AMAZE (Formerly Autism Victoria) at Bunjil Place in Narre Warren. I haven’t fully processed the fact that my access request was successful and that I’m now officially an NDIS participant so now I have a reason to attend these workshops beyond just gaining knowledge and information. A lady named Pamela Gatos, who presented at the info night a few months back, has returned to run this workshops designed to better prepare NDIS participants for the journey ahead. http://www.amaze.org.au/2018/04/amaze-announces-ndis-information-sessions-and-workshops-sign-up-now/
There were about 20 other parents, carers and people with autism in the same meeting room as I was. The silence was very uncomfortable for me but I was 100% determined to push through it. I did find that Pam could come across as blunt, intimidating and snarky at times, often making very sarcastic comments about the NDIS and all the negative stories she’s heard about it.
To be fair, her opinions can be justified as I myself has found the NDIS to be a very daunting, overwhelming and confusing system to wrap my head around. She also has a lot of experience working with current participants and families with autistic kids and adults so she knows what she’s talking about.
Tonight’s workshop focused on the topics of: The 3 types of management for the funding of supports (Self Management, Plan Management and Agency Management), the NDIS Pricing Guide July 2018, how to access the NDIS portal via the mygov website, the 3 types of Supports (Core, Capital and Capacity Building) and the 15 support categories. https://www.ndis.gov.au/participants/reasonable-and-necessary-supports
It was a lot of information to process but it did get me thinking about which supports I should be asking for in my plan. The ones I could identify for myself include: Improved living Arrangements, Increased Social and Community Participation, Finding and Keeping a Job, Improved Health and Wellbeing, Improved Life Choices and Improved Daily Living Skills. https://abilityoptions.org.au/ndis/ndis-supports-categories
The challenge now is to find arguments to justify why these supports are reasonable and necessary. It’s probably the most difficult part of the whole process as it’s an important part of the planning meeting and developing my first plan. It’s going to take many baby steps but I know I’ll get there. Still I really wasn’t a fan of Pamela’s attitude and personality. She came off as a judgemental bitch and wasn’t very constructive.
Being the odd-one-out (an adult diagnosed with Autistic Spectrum Disorder rather than a child), I didn’t feel supported or accepted in that meeting room. I walked out of this first workshop feeling very conflicted and confused as I really didn’t like Pamela’s views or approach to NDIS preparation. So I think that I’m going to look elsewhere. https://www.ndis.gov.au/operational-guideline/planning/participant-statement-goals
On Friday afternoon, I saw my counsellor Ruth at Piece Together Counselling in Narre Warren. The high velocity winds outside and poor quality of sleep have really impacted on my moods and emotions this week. I’ve found myself taking a lot of things personally including my opinions about the UNIFY 2019 lineup and my decision not to go next year, the pressures placed upon me by others including customers and members of the general public. It all got a bit much for me this week and now I’m feeling drained and exhausted.
Ruth reminded me of the importance of using Cognitive Behavoural Therapy and not allowing myself to fall into the trap of maladaptive thinking. It’s the reason why I often take things so personally. To essentially consider alternative explanations for the way other people react to situations and not believe that I’m the sole cause of it. She also pointed out that using my journal more regularly is vital to focus more on the positive aspects in my life. https://www.succeedsocially.com/challengethoughts
On Friday night, I went to my Strength and Circuit small group training session at CinFull Fitness. I was honestly feeling like shit after some posts on social media was dragging me down inside plus I was mentally drained from how busy my week has been. Tonight I was training with a couple of other clients. We did some warm-up drills with the dead balls doing overhead squats and ball slams plus walking lunges with dumb bells, kettle bell swings and push-ups.
Next we did a series of exercises to work and tone the biceps and triceps including rows, kick-backs and curls, tricep push-ups and lifts. Lastly we did some core training using the med balls including overhead situps, pull ups with leg extensions and Russian twists. It was very difficult for me to keep up as I was fatiguing and feeling out of breath a lot quicker than the others and Cinamon noticed straight away. Plus lots of sweat but that’s nothing new for me.
I guess I want to do the best that I can but also have to be aware and mindful about my physical limitations. I have to keep reminding myself that there’s no shame in needing to stop and rest, that nobody is going to judge me for not being as physically fit as they are. Doing strenuous exercise is still a struggle for me but I’m determined to keep plugging away at it, no matter how long it takes me. I want to continue to lose weight and improve my fitness as I need to make classes like these a regular part of my routine. https://www.facebook.com/CinFullFitness/
“I watched them go 'round and 'round. My blouse wrapping itself in your trousers. Oh the waves are going out. My skirt floating up around my waist. As I wade out into the surf. Oh and the waves are coming in. Oh and the waves are going out. Washing Machine.” Kate Bush - Mrs. Bartolozzi (2005)
“There were hundreds of people living here. Sails at the windows. And the planes came crashing down. And many a pilot drowned. And the speed boats flying above. Put your hand over the side of the boat. And what do you feel?” Kate Bush - A Coral Room (2005)
0 notes
Text
My Grandmother Is Donating Her Brain to Science
I remember the bag from my childhood. Transparent and oblong, just large enough to fit a handful of papers, a few essentials, and a plastic brain.
My 93-year-old grandmother, Marjorie Pearlson, once loved this bag, filling it with conversation starters. She was a woman who could talk to any stranger and pull an organ replica out of her purse with a straight face. Growing up, I would witness this scene at the supermarket, in a post office, out at dinner between salad and the main course. It was brilliant performance art. She was passionate about her decision to donate her brain to science, following in the footsteps of her mother, who survived multiple brain surgeries, and her younger brother. She spoke about the decision—visual aid in tow—matter-of-factly to anyone.
At her 90th-birthday tea party, we sat around my grandparents’ dining table with two of her childhood friends and my mother. My grandmother flipped through a handmade scrapbook of photographs, effortlessly recalling the first and last names of grade-school classmates, one of whom is my 92-year-old grandfather. Today, it’s far rarer to see her smile, much less get a glimpse of her past or quirky personality. A shield of advanced dementia has limited her mobility and dissolved her memories.
There’s an Indian death euphemism I’ve been dwelling on since the last time I saw my grandmother: “To be no more.” But even after she dies, my grandmother’s brain will, in a way, live on, joining the thousands of Americans who donate each year. After undergoing an autopsy, her brain’s tissue will be stored and researched. It may travel to banks with specialized grants and niche experts. Someone will look at her under a microscope.
The more I thought about the trajectory of my grandmother’s life, the more the line between brain and grandmother blurred. What will come of her after life? That question led me to the place where her brain will end up.
On a sunny morning in January, I arrived at the University of Miami’s Brain Endowment Bank with the eagerness and anxiety of a new mother about to inspect a potential day-care facility. The bank is one of six brain and tissue biorepositories funded by the National Institutes of Health’s NeuroBioBank, or NBB. These biorepositories use donated tissue to research neurological and psychiatric diseases. (Outside of the NIH’s network, there are dozens of other banks worldwide.)
Each donated brain has a different journey. All brains undergo examination and are weighed; cell loss from Alzheimer’s can shrink the brain. Some donors’ bodies are returned to their families after autopsy; others donate all their organs and tissue. In either case, families receive a pathology report, and brains are stored at about negative 112 degrees Fahrenheit for research on site or at another lab. It costs banks roughly $10,000 per year to store a brain, according to Deborah Mash, the Brain Endowment Bank’s founder and director.
One brain can provide hundreds of qualified scientists with tissue, Mash said. She cites an example of the bank’s involvement in pioneering research on the link between a dietary neurotoxin and Alzheimer’s disease. The NBB’s website lists discoveries related to autism, depression, and epilepsy, among others, that were made thanks to the use of human-brain tissue.
When we met, Mash reminisced about launching the Brain Endowment Bank in 1987 with “$5,000 and a freezer.” But its capacity and technology rapidly advanced: “More has been learned about the human brain in the past 20 years than throughout all of human history,” she said. This progress is the result of both political and cultural shifts. In 2013, President Obama announced the $100 million BRAIN (Brain Research through Advancing Innovative Neurotechnologies) Initiative. The initiative, which is funded in part by private institutions and foundations, continues to get boosts from Congress. Curiosity about the brain has also permeated the arts world. The American Museum of Natural History’s 2010 exhibition Brain: The Inside Story continues to travel the country.
Michelle Freund, the director of the NIH NeuroBioBank, says she has witnessed significant progress in postmortem brain research in the four years since the organization was established, such as the potential for groundbreaking studies with a relatively new technology known as CLARITY (Clear Lipid-exchanged Anatomically Rigid Imaging/immunostaining-compatible Tissue Hydrogel). CLARITY enables researchers to view neurons three-dimensionally, and could be instrumental in identifying neuronal circuits and specific cell types involved in a number of brain disorders.
Mash insisted that insights like this can’t come fast enough. Despite growing public awareness of brain research and sophisticated research tools, there’s still the matter of securing brain donations. Donation advocates have made some progress on this front, especially among athletes: Recently, several sports figures, including three female Olympians in February, pledged to donate their brains to the Concussion Legacy Foundation; the former professional footballer Nick Buoniconti also committed to donating after being diagnosed with dementia last year. But the need for viable specimens is still substantial, Mash said. Across all banks in the country, she estimated that there may be “only about 5,000 donors per year.” My grandmother was the only brain donor I knew; other people I spoke to who are organ donors assumed they were brain donors, too.
In fact, the challenge of recruiting donors comes in part from the fact that organ donors are not automatically brain donors. “Donors need to specifically designate their brain for donation,” explains Howard Rosen, a professor of neurology at the University of California at San Francisco, whose work focuses on the early diagnosis of dementia. In the early 1990s, Mash went to the Florida legislature in an attempt to add brain donation to driver’s licenses alongside other organs and tissues, but failed. The separation between donations remains intact throughout the country.
Nina Silverberg, the director of the Alzheimer’s Disease Centers program at the NIH’s National Institute on Aging, says that a donation “is of much more value if we know about the person when they’re living”—that is, if the person has participated in a longitudinal study of brain function. Silverberg explains that the Alzheimer’s Disease Centers conducts annual tracking assessments that include cognitive, neurological, behavioral, and linguistic tests for observing the changes in brain function as people age.
Another major challenge, Silverberg says, is obtaining tissue from donors of varied backgrounds. “There’s a stigma in some cultures around even talking about donating organs, or even death at all, but it’s tremendously important that we get diverse populations to donate their brains,” so that resulting treatments are broadly applicable, she says. She highlighted the efforts of the African American Network Against Alzheimer’s.
Rosen adds that there is lingering skepticism toward medical research due to historic injustices such as the Henrietta Lacks case and Tuskegee experiments.
Walking the halls of Miami’s Brain Endowment Bank, I was introduced to researchers and peered into a microscope at Alzheimer’s tissue. I wondered what people and which spaces would encounter my grandmother’s brain. I struggled—still—to reduce her to tissue on a slide. I wanted to ask the researchers if they can call tissue inanimate with conviction.
At one point, the bank’s office manager plopped a thick folder on a desk in front of me. This was my grandmother’s file—a collection of medical records as well as letters, photographs, and invitations that my grandmother shared with the bank to keep them informed about her life over the years. The office manager called the file impressive, wagging another thin manila folder, the norm for most donors.
As I walked through the halls, I was introduced as “Marge Pearlson’s granddaughter” and most people shook my hand with what I sensed was recognition and gratitude. Mash called my grandmother a “living legacy” for understanding the importance of this research. I longed for the opportunity to share this knowledge with her. I knew just how she would smile. This is my process of accepting the absence of a loved one who is physically present.
Because of her dementia, I’ll never have the opportunity to talk more with my grandmother about her decision to be a donor. So I can only glean her motivation from conversations with those who know her best, my mother and grandfather. But at a recent book talk related to neuroscience, I met someone who—upon hearing about my research—introduced me to a 61-year-old donor, George Henry Keen. In a lively discussion, Keen explained that he decided to donate to ensure he could make positive contributions during and after life, a sentiment that captured what I believe guided my grandmother’s existence.
from Health News And Updates https://www.theatlantic.com/science/archive/2018/04/grandmother-brain-donation/557510/?utm_source=feed
0 notes
Text
My Grandmother Is Donating Her Brain to Science
I remember the bag from my childhood. Transparent and oblong, just large enough to fit a handful of papers, a few essentials, and a plastic brain.
My 93-year-old grandmother, Marjorie Pearlson, once loved this bag, filling it with conversation starters. She was a woman who could talk to any stranger and pull an organ replica out of her purse with a straight face. Growing up, I would witness this scene at the supermarket, in a post office, out at dinner between salad and the main course. It was brilliant performance art. She was passionate about her decision to donate her brain to science, following in the footsteps of her mother, who survived multiple brain surgeries, and her younger brother. She spoke about the decision—visual aid in tow—matter-of-factly to anyone.
At her 90th-birthday tea party, we sat around my grandparents’ dining table with two of her childhood friends and my mother. My grandmother flipped through a handmade scrapbook of photographs, effortlessly recalling the first and last names of grade-school classmates, one of whom is my 92-year-old grandfather. Today, it’s far rarer to see her smile, much less get a glimpse of her past or quirky personality. A shield of advanced dementia has limited her mobility and dissolved her memories.
There’s an Indian death euphemism I’ve been dwelling on since the last time I saw my grandmother: “To be no more.” But even after she dies, my grandmother’s brain will, in a way, live on, joining the thousands of Americans who donate each year. After undergoing an autopsy, her brain’s tissue will be stored and researched. It may travel to banks with specialized grants and niche experts. Someone will look at her under a microscope.
The more I thought about the trajectory of my grandmother’s life, the more the line between brain and grandmother blurred. What will come of her after life? That question led me to the place where her brain will end up.
On a sunny morning in January, I arrived at the University of Miami’s Brain Endowment Bank with the eagerness and anxiety of a new mother about to inspect a potential day-care facility. The bank is one of six brain and tissue biorepositories funded by the National Institutes of Health’s NeuroBioBank, or NBB. These biorepositories use donated tissue to research neurological and psychiatric diseases. (Outside of the NIH’s network, there are dozens of other banks worldwide.)
Each donated brain has a different journey. All brains undergo examination and are weighed; cell loss from Alzheimer’s can shrink the brain. Some donors’ bodies are returned to their families after autopsy; others donate all their organs and tissue. In either case, families receive a pathology report, and brains are stored at about negative 112 degrees Fahrenheit for research on site or at another lab. It costs banks roughly $10,000 per year to store a brain, according to Deborah Mash, the Brain Endowment Bank’s founder and director.
One brain can provide hundreds of qualified scientists with tissue, Mash said. She cites an example of the bank’s involvement in pioneering research on the link between a dietary neurotoxin and Alzheimer’s disease. The NBB’s website lists discoveries related to autism, depression, and epilepsy, among others, that were made thanks to the use of human-brain tissue.
When we met, Mash reminisced about launching the Brain Endowment Bank in 1987 with “$5,000 and a freezer.” But its capacity and technology rapidly advanced: “More has been learned about the human brain in the past 20 years than throughout all of human history,” she said. This progress is the result of both political and cultural shifts. In 2013, President Obama announced the $100 million BRAIN (Brain Research through Advancing Innovative Neurotechnologies) Initiative. The initiative, which is funded in part by private institutions and foundations, continues to get boosts from Congress. Curiosity about the brain has also permeated the arts world. The American Museum of Natural History’s 2010 exhibition Brain: The Inside Story continues to travel the country.
Michelle Freund, the director of the NIH NeuroBioBank, says she has witnessed significant progress in postmortem brain research in the four years since the organization was established, such as the potential for groundbreaking studies with a relatively new technology known as CLARITY (Clear Lipid-exchanged Anatomically Rigid Imaging/immunostaining-compatible Tissue Hydrogel). CLARITY enables researchers to view neurons three-dimensionally, and could be instrumental in identifying neuronal circuits and specific cell types involved in a number of brain disorders.
Mash insisted that insights like this can’t come fast enough. Despite growing public awareness of brain research and sophisticated research tools, there’s still the matter of securing brain donations. Donation advocates have made some progress on this front, especially among athletes: Recently, several sports figures, including three female Olympians in February, pledged to donate their brains to the Concussion Legacy Foundation; the former professional footballer Nick Buoniconti also committed to donating after being diagnosed with dementia last year. But the need for viable specimens is still substantial, Mash said. Across all banks in the country, she estimated that there may be “only about 5,000 donors per year.” My grandmother was the only brain donor I knew; other people I spoke to who are organ donors assumed they were brain donors, too.
In fact, the challenge of recruiting donors comes in part from the fact that organ donors are not automatically brain donors. “Donors need to specifically designate their brain for donation,” explains Howard Rosen, a professor of neurology at the University of California at San Francisco, whose work focuses on the early diagnosis of dementia. In the early 1990s, Mash went to the Florida legislature in an attempt to add brain donation to driver’s licenses alongside other organs and tissues, but failed. The separation between donations remains intact throughout the country.
Nina Silverberg, the director of the Alzheimer’s Disease Centers program at the NIH’s National Institute on Aging, says that a donation “is of much more value if we know about the person when they’re living”—that is, if the person has participated in a longitudinal study of brain function. Silverberg explains that the Alzheimer’s Disease Centers conducts annual tracking assessments that include cognitive, neurological, behavioral, and linguistic tests for observing the changes in brain function as people age.
Another major challenge, Silverberg says, is obtaining tissue from donors of varied backgrounds. “There’s a stigma in some cultures around even talking about donating organs, or even death at all, but it’s tremendously important that we get diverse populations to donate their brains,” so that resulting treatments are broadly applicable, she says. She highlighted the efforts of the African American Network Against Alzheimer’s.
Rosen adds that there is lingering skepticism toward medical research due to historic injustices such as the Henrietta Lacks case and Tuskegee experiments.
Walking the halls of Miami’s Brain Endowment Bank, I was introduced to researchers and peered into a microscope at Alzheimer’s tissue. I wondered what people and which spaces would encounter my grandmother’s brain. I struggled—still—to reduce her to tissue on a slide. I wanted to ask the researchers if they can call tissue inanimate with conviction.
At one point, the bank’s office manager plopped a thick folder on a desk in front of me. This was my grandmother’s file—a collection of medical records as well as letters, photographs, and invitations that my grandmother shared with the bank to keep them informed about her life over the years. The office manager called the file impressive, wagging another thin manila folder, the norm for most donors.
As I walked through the halls, I was introduced as “Marge Pearlson’s granddaughter” and most people shook my hand with what I sensed was recognition and gratitude. Mash called my grandmother a “living legacy” for understanding the importance of this research. I longed for the opportunity to share this knowledge with her. I knew just how she would smile. This is my process of accepting the absence of a loved one who is physically present.
Because of her dementia, I’ll never have the opportunity to talk more with my grandmother about her decision to be a donor. So I can only glean her motivation from conversations with those who know her best, my mother and grandfather. But at a recent book talk related to neuroscience, I met someone who—upon hearing about my research—introduced me to a 61-year-old donor, George Henry Keen. In a lively discussion, Keen explained that he decided to donate to ensure he could make positive contributions during and after life, a sentiment that captured what I believe guided my grandmother’s existence.
Article source here:The Atlantic
0 notes