#the more I get into epidemiology and public health the more I get into political philosophy along ethos
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
anyways, wassup gamers, ya boy's seriously thinking about deriving into academia full time
the more I read about epistemology for my thesis, the more fascinating it seems, and the more I can find use for it, who'd've thunk
#like legit may end up picking up a philosophy course or degree later down life#the more I get into epidemiology and public health the more I get into political philosophy along ethos#and don't get me started on the sociological aspects of fucking dengue that's another can and a half#i may hate academia but it also has the best benefits in terms of working over where I live as of now#and I do enjoy teaching
8 notes
·
View notes
Text
anyway to Me the reason to wear a mask is not because it's a political symbol or because i am trying to Signal something it's because i want to reduce disease transmission. the mask is valuable to me insofar as it is a useful epidemiological tool. i don't think treating it like some kind of group identity symbol is helpful in encouraging other people to wear it (doing any sort of encouragement on an individual level is obviously only going to get us so far anyway) and in general public health communication that relies on guilt trips or involves demonstrating yr own moral superiority does not work, even in cases where you are legitimately doing something morally better. and the mask as a tool is limited, like any other technical intervention, and needs to be combined with other things like: ventilation, vaccines, actually avoiding prolonged unnecessary social contact (doing the exact same risky actions But Masked isn't magically protecting everyone actually. because they are still risky actions), reorganising society such that people are not forced to go to work to generate profit and transmit disease. we have been doing this for three years now i think we have got to get more ambitious than this just going round and round telling the other side off for not masking. again my point is that political problems cannot just be magicked away by singular technical interventions. it would be a lot easier that way!
124 notes
·
View notes
Note
You seriously have the best suggestions for books/documentaries/music/podcasts. I started listening to GastroPod on your recommendation and I love it! I'm in isolation for the next ten days and was wondering if you have anymore podcast suggestions or favourite books of 2021?
Thanks so much for the compliments! I love hearing that others enjoy my recs, makes me feel like I'm helping everyone find something interesting to read, watch, or listen to! For podcasts: Revisionist History - Malcolm Gladwell's podcast about rethinking certain historical events/moments/stories/etc. Some of my favorite episodes are: S1E6 The King of Tears, S2E1 Divide and Conquer, S2E2 Burden of Proof (this is the CTE episode for those who are wondering), S3E1 The Lady Vanishes (about glass ceilings), S3E4 Carlos Doesn't Remember, S3E5 Food Fight, S3E6 My Little Hundred Million, S3E8 Blame Game - clearly I love a bunch but I'll stop there! Heaving Bosoms - a hilarious romance novel recap podcast hosted by two amazing best friends! For those who already love romcoms/romance/romantic storylines: Start with episodes 30 & 31 The Hating Game! Then go watch the movie (which just came out). Then listen to episode 220 to hear them recap the movie!! For lesbians: episode 101 is Lady's Guide to Celestial Mechanics which was the first mainstream romance house historical romance. This podcast is absolutely one of my favorite things on the internet; they're so fun and funny and it makes me soooo happy every week to listen to them. Sometimes a little libfem cringe but not more than normal. Nolan Investigates: Stonewall - an investigative podcast series investigating how Stonewall has wiggled its way into UK politics, charities, businesses, and 'legal' advice. Bonus! A nonbinary male makes an absolute clown of himself, believes any normal person doesn't just get secondhand embarassment when he says he's attracted to someone based on alt appearances, most notable green hair. Outside/In - A great podcast on a variety of topics about the environment, but not in a stressful the environment is failing way. Some good episodes: Can an Animal be a Criminal, Scents and Sensibility, The Problem with America's National Parks, The Acorn: An Ohlone Love Story, 10x10: Pine Barren Dolly Parton's America - extraordinarily high quality podcast series from WNYC. Covers Dolly, Dolly's music, American culture, and how women are treated. A couple years old now but still really great and timely. Headlong: Running From COPS - podcast series about the tv show cops, how it fostered police faking evidence, falsely arresting individuals, exploited the people who were arrested on camera, and why the show continues to make many Americans believe stupidly in the police. Black Sheep - the stories of New Zealand's historical baddies. Covers a lot of racism, colonialism, treatment of women. RadioWest - this is out of Utah and covers the American West, especially the Mormons. If you're interested in how Mormons control state politics, command so much money, etc; are interested in stories about the American West; or are interested climate change, nonfiction author interviews for books you otherwise would never have heard of, and timely under-discussed political issues, then this is a great podcast to try. Not every episode is a winner, but I haven't found another podcast that covers anything like what RadioWest covers.
Books: The Premonition by Micheal Lewis - this book follows a few individuals who worked for years in public health, epidemiology, virology, and more. It covers their actions in the years and decades leading up to covid - how and why they ended up in the positions they did, how they tried to get the US to do something to combat covid deaths, and how they were silenced. Despite how I just made this book sound totally depressing (not that it isn't depressing) but it is also hopeful - there are people everywhere, in numerous fields, who have the knowledge and capabilities to help humanity - we just need to be better about listening to them, giving them resources, and supporting their work. So it makes me hopeful in a small way. Perks of Loving a Wallflower by Erica Ridley - an f/f historical romance! I haven't read this yet, but it's a top book of this year DESPITE being f/f (the genre far and away most ignored by romance readers)
Bill Bryson - if you listen to audiobooks, there are few audiobook narrations better than Bill Bryson's narration of his own works. He didn't narrate all of them (and literally the others aren't worth listening to) but he did narrate: A Walk in the Woods (his time on the Appalachian Trail), In a Sunburned Country (his travels in Australia), The Body: A Guide for Occupants (a journey into the human body), The Life and Times of the Thunderbolt Kid (his memories of growing up in Des Moines). The books are all easy to listen to, very funny, and make you want to actually spend time in Des Moines, getting blisters hiking, and spending all your money to visit Australia. The Liar's Dictionary by Eley Williams - fiction. I haven't read this but my mom was obsessed with it for like a month! So that's her recommendation Unwell Women: Misdiagnosis and Myth in a Man-Made World by Elinor Cleghorn. An easy to follow history of how medicine's domination by men has harmed women, from the theory of wandering wombs, to ovary removal, to modern medicine ignoring the sex based link of chronic diseases. After her intro saying women aren't real because trans blah blah blah she never goes back to it because she can't - everything is sex linked. New Native Kitchen: Celebrating Modern Recipes of the American Indian by Freddie Bitsoie - this is a cookbook that draws upon the foodways and food traditions of Native Americans, but still draws upon modern 'American' food. I love cookbooks as books to learn from. This book makes a great pairing with The Sioux Chef - together you'd get an interesting mix of 'modern' takes and traditional ingredients and methods. I highly recommend you get them from the library since cookbooks are very expensive in general.
60 notes
·
View notes
Text
Most reasonable people would agree that after years of what appeared to be remarkable success in containing the virus, China’s COVID-19 situation has turned to outright disaster.
Following the government’s sudden and unplanned dropping of strict quarantine and testing rules, hospitals in even the biggest and richest of the country’s cities, starting with Beijing, have been overrun. Patients struggling to breathe or showing other signs of distress are seeking urgent care.
Drugstore shelves throughout the country have been emptied of all medicines related to fever and cold symptoms. The few vetted, prescription antiviral COVID-19 treatments available in much of the rest of the world, such as Paxlovid, are almost impossible to find; when available, they cost an arm and a leg. Ambulance services are completely overstretched by the deluge of emergency calls. And crematoriums operating around the clock cannot keep up with the number of cadavers being delivered in body bags.
I imagine few will be prepared for the conclusion that follows. The COVID-19 crisis in China is not primarily a public health crisis. In fact, it could be argued that even on its present course, in public health terms, China will not come out of the current emergency phase as a global outlier in terms of the numbers of people killed by the pandemic and may even be counted as having done reasonably well. The real scene of the COVID-19 disaster in China is to its once confident and seemingly unshakable political system.
Three years ago, China’s early response to COVID-19, characterized by extraordinary lockdowns affecting big cities and even entire subregions, struck many people around the world (especially in affluent countries that place a priority on personal freedoms) as crude and even brutal. This first phase of what became known as country’s zero-COVID policy was followed, or more accurately supplemented, by the implementation of mass testing regimes that became more and more obsessive and even invasive in nature.
As I have written before, this was clearly not a way out of the pandemic. It was obvious all along to anyone with even a basic understanding of epidemiology or public health that once this regime was lifted, COVID-19 would spread in China just as it had in most other parts of the world. What the long experiment with lockdowns and endless mandated testing and tracking apps arguably accomplished was a postponement of the day of reckoning—until less deadly strains of the virus, as many believe Omicron and its sub-variants to be, had become prevalent.
I lived through the worst of the pandemic in an utterly devastated New York City, when the city’s infection rate was five times higher than the rest of the country (nearly 44,000 people have died in the city due to COVID-19 as of Dec. 27). In those days, depressingly, the incessant sound of ambulances, sometimes several at a time, drowned out everything else.
Had China taken something like the U.S. response at the outset of the pandemic, with few quarantine measures or other social controls, one imagines an even worse catastrophe, given that the country has ten cities roughly as large as New York (or much larger), and over 100 cities with more than a million residents. With no specific treatments for COVID-19 yet available, zero native immunity, and an early strain prone to murder, there is no telling how many people would have died.
In the United States, impressively effective vaccines were rolled out in December 2020, representing an extraordinary triumph of sheer science that helped make up for the grave and persistent weaknesses of the U.S. public health system. I eagerly made an appointment and was grateful to receive my first shot of the new mRNA vaccines in early January 2021, and I kept getting boosters whenever I could (currently, up to five total shots).
As a matter of pride, or rather a deep-seated but foolish sense of nationalism that is incessantly drummed into the public by the country’s leaders, China failed to introduce foreign-made mRNA vaccines, instead pursuing a native vaccine breakthrough. This same mistake was made later, when antivirals effective against COVID-19, such as Paxlovid, were not widely imported, produced, or distributed in China because they were of Western origin; China’s rulers often rigidly insist on having native solutions even to problems that have been long solved by others.
Much has been written about how China squandered the time bought by its quarantine and surveillance efforts by neither pushing for a much higher vaccination rate in the country, especially among the vulnerable elderly, nor stockpiling antivirals or even ordinary fever medicines. But there were very real practical obstacles that stood in the way of near universal vaccinations.
China spent much of the past three years using the pandemic for crude propaganda purposes. Simply put, the rest of the world was getting sick, and China was not. The West, in particular, was afflicted with untold ravages from long COVID-19. The Chinese public was inundated with messaging, both direct and indirect, that concluded that the West’s troubles proved China’s overall system superior, and the Chinese Communist Party (CCP) the best possible guardian of people’s welfare. And in a land where actual COVID-19 cases were few and far between throughout most of this period, getting the public to line up for shots and then more shots, was a very hard sell. (Just think about how hard it has been to get elderly U.S. citizens, who live in a country where COVID-19 has never gone away, to get the latest boosters.)
Add to this indifference the fact that many Chinese people—nationalist state propaganda be damned—have had little faith in the country’s home-grown vaccines. Outside of China, too, much has been made about the country’s inferior vaccines—perhaps a bit too much. There is little doubt that Western vaccines, particularly those using mRNA technology, are more effective than China’s shots, which use older designs. But there are reasons to believe this difference in efficacy, much emphasized in Western coverage and perhaps even acknowledged by Chinese citizens who lack trust in their own system, is substantially overestimated, at least in practical terms. Although the Chinese vaccines are lower performing, staying up to date with repeated doses nonetheless appears to provide substantial protection against the worst effects of a COVID-19 infection—that is, hospitalization and death.
This brings us to the true nature of the ongoing catastrophe in China. The current situation is a self-dealt hand suffered by the CCP that both underpins and stands above the state, and the issue is trust. In the annals of self-ridicule, it would be hard to beat Beijing’s COVID-19 Dec. 21 death toll. In the face of overwhelming anecdotal evidence to the contrary, the government insisted that almost no one had died due to the forest fire-like spread of the disease.
But this is just the tip of the iceberg.
Up until the very moment of the policy turnaround, the Chinese public had been inundated with messages about why zero-COVID was necessary, why they needed to submit to ceaseless PCR tests and even invasions of their homes. The propaganda masters are failing, even now, to come up with a good explanation of the government’s reversal, much less a statement acknowledging that grave mistakes were made at the very top.
There was a time not so terribly long ago when suffocating censorship and national isolation made it possible for the propaganda system to brush aside inconvenient facts and incriminating narratives. In the aftermath of the 1989 Tiananmen Square killings, the CCP masked the facts of what happened through sheer fabulation. The cover story offered by former Communist party chairman Deng Xiaoping for the massacre of hundreds of people at that monumental square in the heart of Beijing was that “a few released prisoners who were not properly reformed, a few political hooligans, the residual dregs of the Gang of Four[,] and other social detritus” were responsible for the violent disturbance that swept China’s capital, and that it had all been instigated by “hostile foreign forces.” Someone deemed that the lily needed further gilding, though, so the propagandists stressed that the soldiers who had carried out the killings were the true victims and filled televisions for days with images of soldiers recovering in hospitals and wreckage of charred army vehicles.
But that era has passed. The present crisis signals the advent of an entirely new epoch, one that has been long in coming. No, this is not a prediction of the pending demise of a system of government that many had believed until only recently to be formidable. (I must add here a macabre thought: From the Chinese state’s point of view, the COVID-19-induced deaths of hundreds of thousands of people over the age of 65 might even have their benefits. That’s because the country is embarking on a globally unprecedented wave of aging that will drastically reduce the size of the workforce and make paying for so called entitlements, or long term health care for people with chronic diseases and retirement benefits, vastly more onerous. A large number of relatively quick deaths, eliminating the need for decades of dialysis or dementia care, for example, might be counted as a fiscal and actuarial blessing.)
Serious foundational cracks are now on display, reminders that even a state that relishes control is susceptible to losing it. In my more than 20 years combined of living in, traveling to, and working extensively on China, I have never seen the credibility of the state and of its propaganda messaging dip so low. What is different from the era of Tiananmen and of other previous crises is that Chinese society has become increasingly dominated by a big and growing middle class. It is much more educated than before. And despite Beijing’s unstinting efforts at information control, people now receive much more news from sources of all kinds, whether domestic or foreign, through formal or informal networks. Big questions loom about whether the country’s political system in its present configuration can endure without major reforms. Will the CCP be able to retain control only at the expense of an exodus of vast numbers of talented Chinese, and a slowing of middle-class economic growth?
The frontlines to watch are threefold. To what degree can the state abide the truth? Can it ever acknowledge its mistakes? And how much criticism can it allow from its own citizens, the overwhelming majority of whom are patriotic? What seems certain is that the state’s customary guise of all-knowing, never erring, and not accepting independent thinking has never fared worse.
2 notes
·
View notes
Text
Podcasting "Qualia"

This week on my podcast, I read “Qualia,” my May, 2021 Locus Magazine column about quantitative bias, epidemiology, antitrust and drug policy. It’s a timely piece, given the six historic antitrust laws that passed the House Judiciary Committee last week:
https://doctorow.medium.com/moral-hazard-and-monopoly-42e30eb159a8
The pandemic delivered some hard lessons about quantitative bias — that’s when you pay attention to the parts of a problem that you can do math on, not because they’re the most important, but because you know how to do math.
The most obvious lesson comes from the failure of exposure notification apps, which were supposed to take the place of “shoe-leather” contact tracing, wherein a public health workers establish personal rapport with infected people to help identify others who might be at risk.
Contact tracing is a human process, built on trust: trust enough to talk about the intimate details of your life, trust enough to take advice on how to get tested and whether you should self-isolate.
That’s not what apps do.
Exposure notification apps measure whether a Bluetooth device you registered was close to another Bluetooth device for a “clinically significant” period of time.
That’s it.
They don’t measure qualitative aspects, like whether you were close to an infected person because you were in the same traffic jam in adjacent, sealed automobiles — or whether you were both at the Ft Lauderdale eyeball-licking championship.
And they certainly don’t create the personal rapport that’s needed to understand each person’s idiosyncratic health circumstances and complications — whether they need child care, or are at risk of losing their under-the-table jobs if they self-isolate.
We didn’t want to commit the resources to do contact tracing at scale, we didn’t know how to automate it — but we did know how to automate exposure notification, so we incinerated the qualitative elements and declared the dubious quantitative residue to be sufficient.
It’s the quant’s version of searching for your car keys under the lamp-post because it’s too dark where you dropped them.
It’s not just foolish, it’s also deceptive — quantizing qualitative elements is a subjective exercise that produces numbers that seem objective.
This is where antitrust law comes in. Prior to the neoliberal revolution of the Reagan years, antitrust concerned itself with “harmful dominance,” with regulators asking whether mergers and commercial practices were bad for the world.
Obviously, “bad for the world” is hard to measure. Regulators evaluated claims from all corners: both political scientists worried about the outsized lobbying power of large companies and workers worried about monopolies’ outsized power over wages and conditions got a say.
So did environmentalists, urban planners, and yes, economists, too.
The Chicago School — hard-right conservative economists with cult-like status among Reagan and big business simps — insisted that all this qualitative stuff had to go.
They argued that consideration of qualitative elements left too much up to judges, so two similar companies engaged in similar conduct might get different verdicts out of the antitrust system. This, they said, make a mockery of the notion of “equal treatment before the law.”
Instead, the Chicago Boys — led by Robert Bork, a Nixonite criminal and a sort of court sorcerer to Reagan — demanded that qualitative measures be left behind in favor of a purely quantitative analysis of whether a monopoly hurt “consumer welfare.”
The way you’d measure “consumer welfare” was by checking to see whether a monopoly was making prices go up — if not, the monopoly was deemed “efficient” and thus socially beneficial. Prices are numbers, numbers can be measured.
But that’s not how it worked in practice. When two companies wanted to merge, they could hire a Chicago fixer to construct a mathematical model that “proved” that they resulting megafirm would not raise prices.
No one could argue with this, because Chicago School consultants had a monopoly over building and interpreting these models — the same way court magicians laid exclusive claim to the ability to slaughter an animal and read the future in its guts.
And if the prices did go up? Well, the same Chicago model-makers would be paid to produce a new model to prove that the price-rises were not the result of monopoly, but rather, rising energy costs or higher wages or the moon being in Venus.
Even by their own lights, “consumer welfare” was a failure. Monopolies drive prices up. Amazon Prime is a tool to drive up prices in every store, not just Amazon:
https://pluralistic.net/2021/06/01/you-are-here/#prime-facie
Apple’s App Store monopoly drives up app prices:
https://www.engadget.com/2019-05-13-supreme-court-apple-app-store-price-fixing-lawsuit.html
Luxxotica bought every eyewear brand and every eyewear retailer and the world’s largest optical lens manufacturer and drove prices up 1000%:
https://www.latimes.com/business/lazarus/la-fi-lazarus-glasses-lenscrafters-luxottica-monopoly-20190305-story.html
The highly concentrated pharma industry raises prices every single year:
https://patientsforaffordabledrugs.org/2021/01/14/2021-price-hikes-pr/
What’s more, there’s a straight line from “consumer welfare” to price-fixing.
Think about publishing. A decade ago, the Big Six publishers were embroiled in a bid to force Amazon to raise ebook prices, which led to fines and settlements for harming “consumer welfare.”
Today, the Big Six publishers are the Big Four, because Random House, the largest publisher in the world, gobbled up Penguin and Simon & Schuster. When RH, S&S and Penguin were three companies, it was illegal for them to collude on pricing.
But after their mergers, the three former CEOs — now presidents of divisions within an unimaginably giant company — can meet in a board room and plan exactly the same price-fixing strategy, and that isn’t illegal under “consumer welfare” antitrust — it’s “efficient.”
The Chicago School’s “consumer welfare” was only ever a front for “shareholder welfare,” the ability of large firms to avoid “wasteful competition” and extract an ever-larger share of the take for shareholders at the expense of customers, workers and the public.
The entire business of “consumer welfare” is a fraud, starting with Robert Bork’s insistence that a close reading of the US’s four major antitrust laws will reveal that they were never intended to be used for any purpose *other* than consumer welfare protections.
This is manifestly untrue, a Qanon-grade conspiracy that is refuted by the plain language of the statutes, the statements of their sponsors, and the record of the Congressional debates leading to their passage.
Despite the wealth of evidence that US antitrust is not a “consumer welfare” project, neoliberals have insisted that their project was not “reforming” antitrust, but rather, “restoring” it to its original purpose.
It’s a Big Lie, and they know it. That’s why GOP Senators Mike Lee (UT) and Chuck Grassley (IA) introduced “The TEAM Act to Reform Antitrust Law” — a bill intended to neutralize the muscular new antitrust bills that just passed the House committee.
https://washingtonmonthly.com/2021/06/25/the-plan-to-water-down-antitrust-reform/
The bill does two things:
It takes antitrust authority away from the FTC, sidelining the incredible Lina Khan, a once-in-a-generation antitrust scholar who now runs the agency; and
It codifies “consumer welfare” as the basis for US antitrust law.
That second part is the tell: after 40 years of insisting that any rational reading of US antitrust proved that “consumer welfare” was obviously its sole purpose, they’re now introducing a law to *change* its purpose to “consumer welfare.”
Like the Stolen Election lie, they never truly believed this one. The pose of objectivity that quantizing antitrust allowed was never about creating a truly objective standard for competition policy — it was only ever about neutering competition policy.
The thing is, there is a way to integrate both the objective and subjective into policy-making — as was demonstrated by David Nutt’s 2008 leadership of the UK’s Advisory Council on the Misuse of Drugs, which established the policy framework for a wide range of drugs.
Nutt’s panel of experts rated drugs based on how harmful they were to their users, the users’ families, and wider society. This allowed him to sort drugs into three categories:
Drugs that were dangerous irrespective of your public health priorities;
Drugs that were safe irrespective of your public health priorities; and
Drugs whose safety changed based on whether you prioritized the safety of users, families or society.
Those priorities are a political choice, not an empirical finding. Nutt told Parliament that it was their job to establish those subjective priorities, and once they did, he could objectively tell them how to embody them in the rules for each drug.
This is a beautiful example of how the objective and subjective fit together in policy — and the tale of what happened next is a terrible example of how “consumer welfare” hurts us all.
You see, booze is one of the most concentrated industries in the world. The “consumer welfare” standard let booze companies buy one another until just a handful remain — globe-straddling collosii with ample resources to influence policy-makers.
Nutt, an empiricist, reported just as rigorously on the harms of booze — one of the most dangerous drugs in the world — as he did on other drugs. He was fired for refusing to retract his true statement that tobacco and alcohol were more dangerous than many banned drugs.
Thanks to “consumer welfare” antitrust, the alcohol industry is able to choose who its regulators are, and use their political influence — purchased with the excessive profits of a monopolist — to rid themselves of pesky officials who actually pursue objective policy.
You can read the column here:
https://locusmag.com/2021/05/cory-doctorow-qualia/
And here’s the podcast episode:
https://craphound.com/news/2021/06/28/qualia/
As well a direct link to the MP3 (hosting courtesy of the @InternetArchive; they’ll host your stuff for free, forever):
https://archive.org/download/Cory_Doctorow_Podcast_395/Cory_Doctorow_Podcast_395_-_Qualia.mp3
And here’s a link to my podcast feed:
http://feeds.feedburner.com/doctorow_podcast
Image: OpenStax Chemistry: https://commons.wikimedia.org/wiki/File:Figure_24_01_03.jpg
CC BY: https://creativecommons.org/licenses/by/4.0/deed.en
20 notes
·
View notes
Link
From the report by Beth Mole, posted 19 July 2021:
Fully vaccinated people are largely protected from delta; the current vaccines are still highly effective against developing COVID-19 from delta and other variants of concern. Though a small proportion of people can develop so-called “breakthrough infections,” those infections will mostly be asymptomatic or mild. But, unvaccinated people are completely vulnerable. Moreover, those who have received only one dose of a two-dose vaccine or have only recovered from COVID-19 are not much better off than those who are completely unvaccinated.
But according to new polling data from CBS News, a new wave of vaccinations seems unlikely. Among unvaccinated and partly vaccinated people, only 48% said they are concerned about delta. Among fully vaccinated people, 72% reported being concerned about the variant.
Despite the fact that the current COVID-19 vaccines have proven highly effective and safe, 53% of those who are unvaccinated or partly vaccinated said in the poll that they are concerned about side effects. 50% of the group cited a lack of trust in the government as a reason not to get vaccinated. And 45% said they don’t trust the science. All of these percentages are higher than they have been in earlier polls, indicating that these anti-vaccine sentiments are hardening among the unvaccinated.
Some unvaccinated people who may be more persuadable have said they are waiting for the vaccines to receive full approval from the Food and Drug Administration (currently, they are authorized by the FDA under an emergency use authorization). On Friday, Pfizer and BioNTech said that the FDA had granted them a Priority Review designation for their mRNA vaccine, but they didn’t expect a decision on full approval until January 2022. Currently, vaccine providers are administering only around 520,000 COVID-19 vaccine per day, down from a record of 4.6 million in a day in April.
With over 161 million people vaccinated, only 48.6% of the US population is fully vaccinated.
See also: How much COVID misinformation is on Facebook? Its execs don’t want to know
For years, misinformation has flourished on Facebook. Falsehoods, misrepresentations, and outright lies posted on the site have shaped the discourse on everything from national politics to public health. But despite their role in facilitating communications for billions of people, Facebook executives refused to commit resources to understand the extent to which COVID-19-related misinformation pervaded its platform, according to a report in The New York Times.
Early in the pandemic, a group of data scientists at Facebook met with executives to propose a project that would determine how many users saw misleading or false information about COVID. It wasn’t a small task—they estimated that the process could take up to a year or more to complete—but it would give the company a solid understanding of the extent to which misinformation spread on its platform.
The executives listened to the data scientists’ pitch and then reportedly ghosted them.
The data team’s proposal wasn’t approved, and they were never given an explanation for why it was silently dropped.
The revelations come as Facebook has drawn fire from the White House for its role in the spread of misinformation about COVID-19 and the vaccines that prevent it. “They’re killing people,” President Joe Biden said about the role of social networks in the spread of misinformation. “Look, the only pandemic we have is among the unvaccinated. They’re killing people.”
Biden later walked back his comments slightly, but they revealed the administration’s frustration with social media platforms—and with Facebook in particular—over their response to the pandemic.
For weeks, the White House pressed Facebook for details on how the company is combating COVID vaccine misinformation. The social network offered some details but gave unsatisfying answers to other requests.
Facebook’s unwillingness or inability to understand the scope of COVID misinformation on its platform was apparent in comments it gave to The New York Times, in which it blamed its nescience on the lack of a “standard definition” for pandemic-related misinformation. “The suggestion we haven’t put resources toward combating COVID misinformation and supporting the vaccine rollout is just not supported by the facts,” said Dani Lever, a Facebook spokeswoman.
“With no standard definition for vaccine misinformation, and with both false and even true content (often shared by mainstream media outlets) potentially discouraging vaccine acceptance, we focus on the outcomes—measuring whether people who use Facebook are accepting of COVID-19 vaccines.”
For researchers who study misinformation, that explanation isn’t sufficient. “They need to open up the black box that is their content ranking and content amplification architecture,“ Imran Ahmed, chief executive of the Center for Countering Digital Hate, told The New York Times. “Take that black box and open it up for audit by independent researchers and government. We don’t know how many Americans have been infected with misinformation.”
Me:
This situation is extremely bad!
First off, the individuals that aren’t getting vaccinated just do not care to. They’ve bought hook line and sinker into all the disinfo and misinfo on facebook, instagram, youtube, tiktok, reddit, and/or whatever 8chan replacement one choosed. What they see and read reinforces their pre-conceived (and factually incorrect) views that “experts” “really don’t know shit about anything” and thusly are “blowing things way the fuck outta proportion,” etc. Their views are both informed by, and reinforced by:
what they read and see online
what they hear on FM/AM radio
what they watch on broadcast TV
what their friends and communities consume from media
what the prevailing societal and political attitudes in one’s community are
“rugged individualism” and the post-1980 erosion of the social contract
So, if your fb friends are covid truthers, if the on-air personalities you hear on the radio at work are covid truthers, if your neighbors and friends at werk are covid truthers, if the elected leaders are covid truthers, if the snippets of Fox News you get to see randomly are pushing covid truther disinfo, and if those in your inner circle at that 4th of July party you went to are covid truthers, then you yourself, at a minimum from peer pressure, will dismiss the recommendations of the American Academy of Pediatrics, the American Medical Association, scores of hospital operators, plus countless professionals in medicine and epidemiology in your decision not to get vaccinated, nor to mask up indoors in public even when “recommended”.
“I have rights. I know what’s really going on. I’ve got things figured out.” Or, at a minimum, “I don’t give a fuck either way.” “Fuck you.”
Facebook absolutely is responsible for the covid truther disinfo and misinfo being shared on their platform. I believe they are the largest vector of disinformation and misinformation to the public. So many people are chugging the “vaccines are a scam, masks don’t work and I have rights” kool-aid thanks to disinfo introduced and shared widely on facebook
Some other major vectors of disinfo: iHeartMedia - Premiere Networks - iHeartRadio, Entercom/Audacy, Westwood One, One America News, Fox News, Newsmax, Sinclair Broadcast Group, YouTube + Google, TikTok, and Reddit.
“I saw a video on YouTube where the military did a study…” or “I heard a guy on the radio saying mask mandates are part of a plot…” It's all bullshit!
At this point it cannot be anything but an active choice the leadership at these companies consciously make to pipe out total bullshit in a time of crisis. Content from all of the above easily makes its way to facebook, too, unrestricted!
The U.S continues to spiral into this post fact, post truth, anti-intellectual, anti-science neo-fascist hellscape where no lives matter and where mass death is AOK because “none of us get out of this world alive” or some asshat folksy quip that masks as wisdom. Empathy, reasoning, established facts and observable reality have all become political statements… People hear what they want to hear.

IMO this is truly a disastrous situation with no easy way out.
Many, many people will not wear masks again. Many, many people see the survival rate for coronavirus and they surmise wrongly that the risk for them of getting covid is worth it, that the risk for others isn’t remotely their concern, and that the entire situation is overblown. The social contract is in bad shape. Public confidence in the state is almost gone. Covid truthers are everywhere.
Getting a vaccine requires time off from work to travel to a mass vax site that’s still open, time off to recoup post-shot (if necessary), and overcoming fear that the anti-vax disinfo on social media was true after all. Plus overcoming peer pressure from unvaccinated friends and family.
Covid case numbers are likely undercounts. Test kits are still problematic. Persons with no health insurance have no PCP to call when they get sick. Underinsured persons may have to wait weeks for their approved PCP to get around to a telehealth call. Many people are getting sick and not getting tested and they’re not reporting anything to anyone. State officials, wanting to look good, may skew whatever data is reported to them.
COVID-19 is an airborne virus. Most people catch covid from contagious asymptomatic people. Coronavirus has always been a risk for children! Getting vaccinated is part of an overall good strategy to keep COVID-19 at bay. Masks work!!! If indoors, stay in a ventilated room if you’re with other people, and keep doors and windows open for air circulation. Coronavirus is producing extremely serious long-term cognitive and cardiovascular complications for many people who survive it. “Long covid” is real.
We don’t have to live with this! The political and business leadership in much of the United States today have collectively decided there’s nothing that can or should be done in regards to covid-19, no masking requirements, no easy supplies of N95 masks, and no mitigation efforts of any kind. They wrongly conclude that COVID-19, a new virus with so many unknowns, “isn’t that bad” and so the level of permanent damage or death resulting from covid is acceptable.
None of this is acceptable, the amount of permanent damage and death occurring from COVID-19 is far, far too high, and there’s no rational excuse whatsoever to allow this virus to spread across this country unchecked. There’s no reason to allow this virus to spread further. There’s no valid reason for me and anyone else to justify allowing covid to spread out of control.
#news#coronavirus#third wave#covid vaccine#facebook sucks#please get vaccinated#misinformation#disinformation#america 2021#rant#ars technica#vaccine hesitancy#anti vaxxer#things are going swimmingly#long post
4 notes
·
View notes
Text
Recent studies on what extreme heat does to our bodies
This is an excerpt from the weekly essay of Bill McKibben published in The New Yorker. This one is entitled, “It’s Not the Heat - It’s the Humanity.”
I happened to be talking with Dr. Rupa Basu, the chief of air-and-climate epidemiology at California’s Office of Environmental Health Hazard Assessment, on Friday, a day after Palm Springs had tied its all-time heat record with a reading of a hundred and twenty-three degrees Fahrenheit. That’s hot—hotter than the human body can really handle. The day before, with temperatures topping a hundred degrees before noon, a hiker in the San Bernardino National Forest had keeled over and died. “We talk a lot about biological adaptability, but as humans we’re not supposed to adapt to temps that high,” Basu said. “If your core body temp reaches a hundred and five, that means death can be imminent. As humans, we can only adapt so much. Once the air temperature is above a hundred and twenty, there’s only so much you can do, except rely on air-conditioning and other mitigation strategies. And that puts a lot of pressure on the power grid, and that could result in brownouts and blackouts. It’s not really a long-term, chronic solution. It’s just living for the moment and hoping it works.”
And often it doesn’t work. Last summer, Basu published a remarkable paper, a “systematic review” of research on pregnant women. The studies she looked at—which collectively examined more than thirty-two million births—found that higher temperatures in the weeks before delivery were linked to stillbirths and low birth weights. “It’s weeks thirty-five and thirty-six that seem to be the trigger,” she told me recently. “What we think is happening is that a lot of the mechanisms from heat-related illness start with dehydration. If there are symptoms of dehydration, those might be overlooked. If someone doesn’t connect it with heat, they might not get to a cooler environment. You see vomiting—and people might say, ‘That’s O.K. Bound to happen when you’re pregnant.’ But it’s because of the dehydration.” Further along in the pregnancy, she said, “your body releases oxytocin, which triggers contractions. And if it happens prematurely—well, heat raises the level of oxytocin faster. If you’re not able to thermoregulate, get the temp down, it can trigger low birth weight or, earlier on, miscarriage or stillbirth.” Past a certain point, the body diverts blood flow to the subcutaneous layer beneath the skin, where the body’s heat can radiate out into the air. That diverts the blood “away from vital organs,” Basu said. “And away from the fetus.”
The brain is an organ, too. For all its metaphysical magnificence, it’s a hunk of cells that comes with operating specs. Again, don’t let its temperature get too high: in 2018, Basu published a study showing the effect of seasonal temperatures on mental health. A ten-degree-Fahrenheit jump in temperature during the warm season was associated with an increase in emergency-room visits for “mental-health disorders, self-injury/suicide, and intentional injury/homicide” of 4.8, 5.8, and 7.9 per cent, respectively. Those are big numbers, and the search for mechanisms that explain them is fascinating. Among other things, certain medications impede the body’s ability to thermoregulate: beta-blockers, for instance, decrease the flow of blood to the skin, and antidepressants can increase sweating, Basu told me. “There’s also some evidence to show that heat affects neurotransmitters themselves—that everything is just a little bit slower.”
Both these effects show up more strongly in this country in Black and Hispanic patients—probably, as Basu explained, because those groups disproportionately live in low-income neighborhoods. “They’re often in areas where there are more fossil-fuel emissions, fewer green spaces, and more blacktop and cement, which really absorbs and retains the heat,” she said. “And also living closer to freeways. That exacerbates air pollution. And, with the heat, that’s a synergistic effect. It’s environmental racism that leads to these differences in exposure.” Some people, she added, bristle at hearing that: “Someone said to me, ‘Oh, so now we’re breathing different air?’ And I said, ‘Yes, that’s exactly right. We can track it down to the Zip Code level.’ ” Call it critical race epidemiology.
Which leads us, of course, back to politics. There’s only so much that doctors can do to help us deal with heat; ultimately, it’s up to the Joe Bidens and the Joe Manchins—and the Xi Jinpings—of the world. “We’re seeing these kinds of extreme temperatures in Palm Springs right now,” Basu said. “If we start to see those in more populated areas, imagine the public-health impact.” That’s obviously what’s coming. Last week, researchers at nasa and noaa found that, according to satellite data, “the earth is warming faster than expected” and that the planet’s energy imbalance—the difference between how much of the sun’s energy the planet absorbs and how much radiates back out to space—has doubled since 2005, an increase equivalent to “every person on Earth using 20 electric tea kettles at once.” And the National Weather Service is forecasting a heatwave this week for the Pacific Northwest that could smash regional records.
4 notes
·
View notes
Text
I really hate to say this, but it’s time for quarantine to end. Everyone...please... Let me break this apart for you. I know I will catch hell, but hear me out. Read to the end. Swallow what you want to say and hear what I need to say. There’s no politics in this. There’s no bias. I’m coming from science and simple balancing of difficult paradigms.
The simple fact is that ALL communicable diseases run this course. Look up the numbers. Go on, I’ll wait. Every year, thousands die of malaria, flu, cholera and on and on. Most of them die in places you don’t care about, but they die in the USA too. In higher numbers. And it’s always the old and the weak. It always those people you are now weeping over losing. Always. Illness is happening all the time. It’s not the illness that’s important here. I’m glad that suddenly you all care, in this modern climate when no one seems to care...I’m ecstatic that suddenly you are all worried about each other. Good. Thank you. But it should have been this way all along. Humans should have ALWAYS worn masks in public and learned how to wash their hands. Outbreaks always happen. Always! Every year! All ages die from diseases it’s easy to avoid if you observe proper etiquette and hygiene! Now all of a sudden it’s Vogue to be safe. Good. But keep an eye on the proportions.
Depending on how you record the deaths and look at the statistics, somewhere between 30 and 60k die from flu or flu complications EVERY YEAR. That’s a lot. Many people. No one cared. Now all of a sudden it’s 80k from corona AND 50k of that normal flu, with some overlap. That’s a lot of people. What I’m trying to say is, you could have cared all this time, but no one did. What Immsaying is, everyone is so busy picking a side, no one stopped to say “We all are terrible and have been all along”
There is an irrational panic happening right now. Truly. Yes this disease exists, and it is more contagious than flu, but it’s going to be here for as long as it takes for it to be asymptomatic within your genome. Flu has been at its evolution within your species for hundreds of years. Now Corona will be too. It’s excatly the same type of concern. So if you care about this virus? Good. Care about all of them. Create a culture that cares about all of them. Don’t say “I want it to go back to normal” because the norm clearly wasn’t right. Instead say “I want to resume life with the right culture in place, the right safeguards in place, the right action plans in place to prevent this from ever being a concern again.” Say “I want there to be a real sense of responsibility toward all fellows from all humanity”.
This system is and has been broken. Now you’ve noticed. So demand more and vote for more. Wear masks in public now. Forever. Always. Wash your hands. Demand your transport and businesses have hand sanitizing stations. You have toyed with ignoring numbers long enough at the cost of lives. Stop doing that! Change the culture.
That said, let’s chat about the economy. I’m not going to even bother with the GOP talking point “the cure can’t be worse than the disease” because as I’ve made clear above, I think the system is broken and they’re idiots. What should anger you, what should outrage and infuriate you, is that with the numbers we have always known exist, with regards to communicable disease...NO BUSINESSES OR GOVERNMENT OFFICES WERE PREPARED. Your health benefits are linked to your work? What? You can’t get care? What? Your government knows how many people die from flu every year and gamble with your lives over corona? What. Don’t let this happen. Demand a change that ensures health care FOR ALL regardless of job status! That stockpiles resources, that manages epidemics ! A system that mandates that the epidemiological posts and heathcare posts be the first positions appointed and that they go to QUALIFIED PROFESSIONALS IN THE FIRLD AND NOT CRONIES!. Organize for organization and basic rights. If you want to protest that the quarantine has gone on this long? Protest instead that universal health care at the behest of the government didn’t exist, and by existing create significant motivation for the government to bark about communicable disease.
Don’t you get it? Capitalism is about markets. If a capitalist society embraces socialist medical care, then the government has to save money by preaching about self care and being wise about the science of communicable disease. Whoever has to pay the bills has to invest in the heath of the nation. You want a country that’s prepared? Give it the incentive to care.! These illnesses are and always have been a problem, but the people in charge got out of addressing them by hiding the numbers. This virus was a memetic and sociological shitstorm they couldn’t avoid! That means you can use it to change things! So do.
The quarantine has to end. Sensibly. So make it happen. The new normal is free hand-sanitizer and face masks. The normal as it always should have been, is an awareness of the risk to others. That’s what it needed to be all along. Freedom isn’t just about you. It’s about raising your awareness and sticking to your observations so that everyone gets as much as they choose to reach toward. So fucking do it. Write your representatives. Protest. Get angry. Do something!
Oh and Bezos needs to divest himself of 3/4 of his wealth or the world economy will collapse.
I’m finished.
TL;DR if you care now. Good. But you should always have cared. Make things change, or shut up.
133 notes
·
View notes
Text
Coronavirus: Information & Guidelines
What you can do now, and what to prepare for
There seems to be a lack of what-to-do suggestions on tumblr beyond handwashing, so I thought I’d put something together. I’ve never actually encouraged people to reblog something of mine before, but this might be the time. To be clear: I am not personally a public health expert of any kind. Both my parents are (epidemiology/global health degrees, worked for CDC) and I’ve run this by them. My information is coming from disease researchers on twitter and official public health guidelines online. Sources at the end of the post. This is mostly directed at people in countries where COVID-19 has been reported (I’m in the U.S.), but is not *yet* widespread in the community. Written Mar. 1st 2020, last updated 3/9 (shorter, helpful twitter thread here, helpful NPR article here)
General Info
Firstly, a lot of politicians are *still* trying to sugarcoat things, but it should be clear by now that the new coronavirus is spreading widely and will continue to do so. Because of the incubation period, and in the U.S. at least the delay in testing, the number of cases is almost certainly going to increase rapidly in the near future no matter what we do now. Official government sources are helpful, but its also good to look at what experts on viral epidemics who aren’t directly government-affiliated are saying. Their agenda is purely informing the public in the most constructive way possible, without politics getting in the way.
Two key points- COVID-19 can have a long incubation period (the time from when you catch the virus to when you start showing symptoms) and most people don’t get severe symptoms. Some are entirely asymptomatic, but most people get typical flu-like symptoms. Specifically, the early symptoms to watch out for are a fever and dry cough (meaning, a stuffy nose is probably just a regular cold). Its possible but unlikely to transmit the virus while asymptomatic, most transmission happens when you have heavier symptoms.
The most vulnerable people are the elderly (~ over 60) and those with preexisting health conditions (i.e. cardiovascular disease, respiratory condition, diabetes), or a simultaneous infection with something else (NOT kids in particular!) So far the mortality rate has been about 1-2% (compared to 0.1% for the general winter flu - yes, this really is worse). However, that might be an overestimate, both because people with mild cases aren’t getting tested (the denominator should be bigger), and because the early situation in Wuhan, where a lot of our numbers come from, was especially bad in regards to availability of healthcare.
This is an emotional, difficult situation. Don’t panic. The world didn’t end in 1918, and its not going to end now. But it is very serious, and we need to be thinking about it rationally, not pretending everything is just going to be okay, or uselessly pointing blame. Take care of your mental health, and check in with each other. Epidemics test our generosity and selflessness. Those qualities are needed right now, but don’t neglect yourself either.
What You Can Do Now
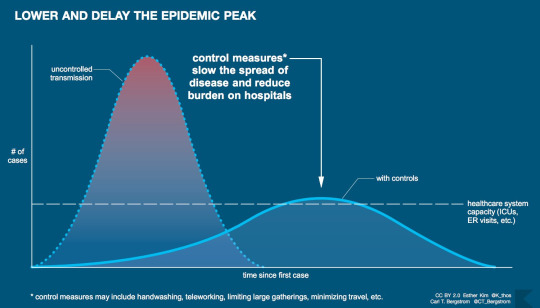
There is stuff everyone can do both to prevent yourself from getting infected, and to prepare if you do. ***The big picture to keep in mind is that the biggest risk of epidemics is that they overwhelm our system, especially our healthcare system. What I mean by this is that our society is built to deal with a certain volume of things happening at once- people buying groceries, getting sick, etc. If we suddenly all rush to do something, we overburden these systems and they won’t be there for the people who need them most. Therefore our goal is to slow down the spread of disease, buying time and lowering the overall burden on these systems. This is called “flattening the curve”. It looks like this, and I cannot stress how important this is.***
A very helpful thread on preparedness
Staying Healthy
Like similar viruses (think colds and flu), COVID-19 is mostly transmitted from person to person, usually by close contact but sometimes from an infected surface. More here.
Wash your hands. Everyone has heard this one- 20 seconds, soap all over your hands, wash the soap off. If you can’t wash your hands use an alcohol-based hand sanitizer (at least 60% alcohol). But handwashing is absolutely better. Also- cough into your elbow/shoulder, not your hand, and avoid shaking hands- try elbow bumps or maybe a polite nod instead! If you’re handwashing so much that you’re hands are threatening to crack and bleed though, consider washing more strategically or using hand sanitizer instead.
In combination with hand-washing- stop touching your face, especially while out! This takes practice, everyone does it all the time without thinking. A good practice is to avoid touching your face while out, then wash your hands thoroughly as soon as you get home.
Similarly, avoid touching surfaces as much as possible! Particularly bad are door handles, elevator buttons, that kind of thing. The virus can probably (based on studies of related viruses) last a while on these. Regular gloves can help a bit. Use a tissue then throw it away, use your elbow, etc.
Do Not buy face masks! There’s mixed evidence on whether they’re at all helpful when used by the general public to prevent catching a virus, but actual medical professionals who need them are facing shortages (that’s probably part of why so many healthcare workers got sick in Wuhan), so our buying them up is really bad. The only times you should be wearing them is if you yourself are sick (they do help then!) or if you’re looking after a sick person. Seek instruction in that case in how to use them properly. (Thread on why buying those fancy masks is not good).
If COVID-19 is in your community, try to stay 6 feet from people, which basically means going places as little as possible. See below.
Planning Ahead
Its also a good idea to prepare in case you need to self-quarantine. Self-quarantine is necessary if you’ve potentially been exposed to COVID-19, or if you’re sick but not enough to need to go to the hospital. Follow local guidelines- if there’s lots of transmission in your area, nonessential workers will probably be advised to stay home as much as possible.
If you’re able, get medication now. Don’t go crazy and buy out the drug store, just a reasonable amount. Try to get at least a month’s worth of any prescription medications. This can be hard at least in the U.S. - your doctor may well be able to prescribe more, but insurance companies and drug stores can be terrible. I’ve found trying a different drugstore can sometimes help. Try your best. They may also be reluctant to prescribe more to avoid causing shortages. Idk what the right answer is here.
Don’t go crazy and buy out the store, but start getting a little extra shelf-stable or frozen food. Even some root vegetables that will last a few weeks. You want enough for 2 weeks in case of self-quarantine, but you do NOT want to empty out stores. Panic buying is definitely a stress on the system. Just add a few extra things each time you shop. Don’t forget about pets. You can always eat the food and replenish it over time.
Make a plan with your family/community. If someone gets sick or needs to self-quarantine, is there a corner of the house they can stay in? Who can take care of them? etc. I haven’t focused on plans for schools/religious communities/workplaces etc but those are very important too! This is one place where keeping an eye on local and national news is important. In the U.S., for example, school systems are planning ways to make food available to kids if they’re not going to school.
If COVID-19 is starting to spread in your community, think about how else you can be a good community member. Cancelling nonessential doctor’s appointments, surgeries etc may be very important, for example. If schools are closed, can you help out neighbors with childcare? Do you have a cleaner who may need to be payed in advance if there’s a quarantine?
If You Might Be Sick/Need to Quarantine
See likely symptoms above. Remember, normal colds still exist, and if you go to the doctor for every one of those you will overwhelm the system.
Don’t just go to a hospital! Call ahead to your doctor/clinic/hospital and get instructions on what to do. Getting healthcare workers sick is something we really want to avoid. That said, DO get tested as soon as possible, and act as if you are contagious. The health coverage situation is the U.S. is not yet clear (and ofc its not something the current admin is eager to clarify). Hopefully testing will be covered financially by the government, but I can’t promise that at this time.
In the meantime, stay home and quarantined if you show any symptoms of illness if you possibly, possibly can. This is especially difficult in the U.S. if you don’t have sick leave/childcare, but please. Do your utmost.
Look after yourself. Skype/google hangouts/etc is great for keeping connected. Have some chocolate/chicken broth/other sick foods ready.
The Big Picture
Coronavirus/COVID-19 has not been declared a pandemic yet, but it probably will be before long. This is almost certainly going to get worse before it gets better. We don’t yet know if warmer weather will slow its spread, and a vaccine will probably take about 1-1.5 years to be developed and tested. As I mentioned before, the best thing we can do to keep the world working, minimize mortality, etc is to slow the spread as much as we can, and minimize the strain on the system. Hospitals are going to be overwhelmed. There aren’t infinite unoccupied beds or ventilators, or people to operate them, and supply chains could get disrupted. Thinking about these things is scary, and it will take time to adjust to what’s happening. Start that process now, and help everyone you know reach the point where they’re able to act, not panic. Another reassuring thing- if we slow the spread of COVID-19, in addition to fewer total people getting sick, you will soon have people who are recovered and almost certainly immune. These people will be invaluable as helpers in their communities.
Now that the practical stuff is out of the way, I want to say from a U.S. perspective that yes, our lack of social welfare other countries take for granted is going to hurt us. Lack of access to childcare, no guaranteed paid sick leave, and of course expensive healthcare are massive problems that will make it much harder to limit disease transmission. Help each other in any way you can, and vote for candidates that support implementing these policies! And of course, watch out for propaganda of all kinds, whether its using the virus as an excuse for racism, calls to delay elections, etc. So far my biggest concern is a lack of willingness to admit how serious this is, but we can do this. Lets put extra pressure on politicians to be honest and change policies to actually help people. But, yes, lets also stay united. We need each other now (just, you know, 6 feet apart).
A few sources
In general, the Guardian is a great, free, reliable source of news. In the U.S., NPR (website as well as radio) is another great source. The Washington Post and Seattle Times have made their coronavirus-related coverage open access, not sure about other national newspapers.
twitter thread from World Health Organization (WHO)
U.S. Center for Disease Control and Prevention (CDC) COVID-19 homepage (not being updated in some ways it should be, like total # of tests)
A reality check from some non-Governmental experts (basically, what governments don’t want to say yet, which is that this virus is going to spread, and the goal now is to infect as few people as possible, as slowly as possible. Read this.)
Why you should act now, not when things get bad in your area (we’re always operating on outdated information)
If you want the latest technical info, The Lancet (major medical journal group) has all of their content compiled here, open access.
I can do my best to answer questions (i.e. ask my dad) but those or other reliable, readily find-able sources should have you pretty well covered. Do let me know if anything on here is wrong or needs to be updated! Stay safe, stay positive, we can do this.
150 notes
·
View notes
Text
COVID-19 lockdown isn't easy, but these small Newfoundland towns are pulling it off
On Sunday night, before the tiny town of Harbour Breton on Newfoundland's south coast asked businesses to temporarily close following two confirmed cases of COVID-19, Mayor Georgina Ollerhead got a call from the mayor of Deer Lake, about 430 kilometres away.
Deer Lake Mayor Dean Ball was calling to offer support and a few pro tips. He'd had to shut down his town a few weeks earlier as a cluster of cases emerged, and he knew it wasn't easy to ask businesses to close and people to stay calm in the face of a pandemic.
"It was actually quite an honour to have the conversation," Ball said in an interview Wednesday.
Shortly after Ball phoned, the town of Harbour Breton posted its public notice @urging residents to stay home as much as possible and calling on non-essential businesses to close.
"Mayor Ball certainly put us on the right steps to proceed forward," Ollerhead said. "We're small communities. We need to nip these things in the bud."
Taking on the arrival of a global pandemic is a massive job for the province's towns, said Sheila Fitzgerald, president of Municipalities Newfoundland and Labrador. She's also the mayor of Roddickton-Bide Arm, a town of just under 1,000 people on the Northern Peninsula.
Newfoundland and Labrador has about 520,0000 people and more than 270 municipalities. Almost all are small towns, and many have just a few dozen residents, Fitzgerald said. Like Ollerhead, their mayors and councils are all volunteers.
"In some of these small communities, they get a turkey at Christmas," she said. "Yet they sign on to be leaders in their communities and they don't look back."
In the past month or so, COVID-19 clusters have bloomed in Grand Bank, a town of about 2,000 on the Burin Peninsula, and in Deer Lake, a western Newfoundland town with about 5,000 people. Harbour Breton has about 1,600 people and two cases. As of Wednesday, the number of cases in the area had held steady at two, with no new infections announced since the weekend.
"If there was ever a time where things would break down and there would be chaos, it would be at a time like this, but that's not what we see in this province," Fitzgerald said, adding: "Nobody has said, `I'm done with this, this is not what I signed up for.' "
Ball said the two weeks he kept Deer Lake on partial lockdown were the most stressful time of his 31 years in municipal politics.
Ollerhead has been in municipal politics for eight years, and mayor for four of those. She's also the Lion's Club president, chairperson of the local Children's Wish Foundation and treasurer of the local darts league. She's seen her town through a shutdown at its fish plant, and now COVID-19.
Every new day without a case in the community is a good day, she said, but she's cautious. "Tomorrow we might get 10," she said. "But guess what, we'll have to deal with that, too."
Harbour Breton is at the end of a two-lane highway that turns off the Trans-Canada Highway and cuts down across the vast, empty centre of Newfoundland to the end of the Connaigre Peninsula. At this time of year, there's nothing but trees, water and caribou for most of the drive.
"No one thought that COVID was going to get here," Ollerhead said.
The two positive cases were workers at the town's health centre, which includes a long-term care facility. Residents and staff had to be tested, and the regional health authority moved in to set up a mobile testing unit. Rapid-testing kits were due to arrive this week, Ollerhead said.
During Wednesday's public health briefing, chief medical officer of health Dr. Janice Fitzgerald said the source of one of the area's cases is untraceable and is now considered non-epidemiologically linked. That means someone was sick and didn't know it, or that they perhaps left the province, she said. It also means Harbour Breton needs to stay in partial lockdown until the risk of transmission abates, Fitzgerald said.
Ollerhead said she's ready for it. The people in Harbour Breton are doing well, they're co-operating, and they're taking care of each other, she said. And they're being kind and supportive to the two people who are sick.
"Right now being the mayor of Harbour Breton, I'm so proud," she said. "Everybody's being a leader right now, and that's what we need."
This report by The Canadian Press was first published Dec. 10, 2020.
from CTV News - Atlantic https://ift.tt/3nbWjqA
2 notes
·
View notes
Note
ive noticed you’re one of the few people who still mentions covid and participates in analyzing ppl’s behavior around it like other social issues and ongoings, outside of a few disability/illness-focused blogs. my friends still mask but I get blank stares from them too when I mention covid. most people are uninformed that covid is still a threat but a fair number of people know covid is still around but still avoid talking about it. i thought maybe this is just how people deal with crisis, by ignoring it/making it a social taboo to mention it, but I’m in the US and when trump was in office everyone talked about trump and the threats (and perceived threats) under trump all the time. they still talk about the trump years. now I have …thoughts on how people talk about trump but not other presidents, but i just mean it as an example of people acknowledging something and not immediately forgetting about it. people do routinely ignore ongoings that don’t immediately effect them, like some groups of people ignoring police brutality for example, but covid does affect them or at the very least affected their life in 2020, no matter how briefly. and of course, many people are talking about current events/historical events or analyzing social phenomena all the time but never mention covid. do you know why that might be? because I feel like im in the twilight zone
i disagree that it never comes up at all; i think what you're picking up on is more that it has become, in many people's minds, so ordinary as to be mostly invisible in the same way as, like, the flu. generally people accept that these illnesses exist but they're seen to be inevitable and minor and thus mostly not worth talking about, save for a few bits of eg health journalism that emphasise individual actions (never political solutions) and maybe a convo about immunisations at a doctor's office for those who can access a doctor. now obviously i don't agree that covid and the flu belong in the same category of seriousness, epidemiologically, but narrativising infectious diseases has always been sociologically much more complex than just accumulating Correct Facts based on Observing The Illness. people will give you even blanker looks if you mention that hiv/aids is ongoing, yet here it is still. our perceptions of public health events (of any events really) are formed in complex ways and it's not a new issue to see that the consensus narrative (esp in an imperialist country pumping out back-to-work propaganda about chronic illness in general and covid complications specifically) doesn't match up with what data we can collect. im sorry if that sounds bleak but i do think 'public opinion' in this case and in general is more an effect of capitalist policymaking than an independent entity formed by each rational individual entity like, carefully evaluting the evidence and coming to an independent conclusion or whatever
74 notes
·
View notes
Text
What's the difference between pandemic, epidemic and outbreak?
by Rebecca S.B. Fischer

It’s a matter of scale. (Edward A. "Doc" Rogers/Library of Congress via AP
The coronavirus is on everyone’s minds. As an epidemiologist, I find it interesting to hear people using technical terms – like quarantine or super spreader or reproductive number – that my colleagues and I use in our work every day.
But I’m also hearing newscasters and neighbors alike mixing up three important words: outbreak, epidemic and pandemic.
Simply put, the difference between these three scenarios of disease spread is a matter of scale.
Outbreak
Small, but unusual.
By tracking diseases over time and geography, epidemiologists learn to predict how many cases of an illness should normally happen within a defined period of time, place and population. An outbreak is a noticeable, often small, increase over the expected number of cases.
Imagine an unusual spike in the number of children with diarrhea at a daycare. One or two sick kids might be normal in a typical week, but if 15 children in a daycare come down with diarrhea all at once, that is an outbreak.
When a new disease emerges, outbreaks are more noticeable since the anticipated number of illnesses caused by that disease was zero. An example is the cluster of pneumonia cases that sprung up unexpectedly among market-goers in Wuhan, China. Public health officials now know the spike in pneumonia cases there constituted an outbreak of a new type of coronavirus, now named SARS-CoV-2.
As soon as local health authorities detect an outbreak, they start an investigation to determine exactly who is affected and how many have the disease. They use that information to figure out how best to contain the outbreak and prevent additional illness.
Epidemic
Bigger and spreading.
An epidemic is an outbreak over a larger geographic area. When people in places outside of Wuhan began testing positive for infection with SARS-CoV-2 (which causes the disease known as COVID-19), epidemiologists knew the outbreak was spreading, a likely sign that containment efforts were insufficient or came too late. This was not unexpected, given that no treatment or vaccine is yet available. But widespread cases of COVID-19 across China meant that the Wuhan outbreak had grown to an epidemic.

COVID-19 was first noticed in Wuhan, China, in late 2019 but quickly spread across the globe. This map shows all countries with confirmed cases on March 5, 2020. CDC
Pandemic
International and out of control.
In the most classical sense, once an epidemic spreads to multiple countries or regions of the world, it is considered a pandemic. However, some epidemiologists classify a situation as a pandemic only once the disease is sustained in some of the newly affected regions through local transmission.
To illustrate, a sick traveler with COVID-19 who returns to the U.S. from China doesn’t make a pandemic, but once they infect a few family members or friends, there’s some debate. If new local outbreaks ensue, epidemiologists will agree that efforts to control global spread have failed and refer to the emerging situation as a pandemic.
Terms are political, not just medical
Epidemiologists are principally concerned with preventing disease, which may be fundamentally different than the broader concerns of governments or international health organizations.
As of this writing, the World Health Organization classifies the risk of global COVID-19 spread as “very high,” the highest level in their risk classification scheme and one step below an official pandemic declaration. This means that the WHO remains hopeful that, by taking aggressive steps now, containment of localized outbreaks may still be possible.
But I and other scientists and public health officials are already calling this a pandemic. The official numbers count an excess of 100,000 cases in almost 100 countries, and community spread has been documented in the U.S. and elsewhere. By the classical definition, it’s a pandemic.
A formal declaration of COVID-19 or any other infectious disease as pandemic tells governments, agencies and aid organizations worldwide to shift efforts from containment to mitigation. It has economic, political and societal impacts on a global scale.
Formal declaration needn’t incite fear or cause you to stockpile surgical masks. It doesn’t mean the virus has become more infectious or more deadly, nor that your personal risk of getting the disease is greater. But it will be a historical event.

About The Author:
Rebecca S.B. Fischer is an Assistant Professor of Epidemiology at Texas A&M University
This article is republished from our content partners over at The Conversation under a Creative Commons license.
#computer science#science news#public health#epidemiology#disease#covid-19#coronavirus#epidemic#pandemic#sars-cov-2#featured
30 notes
·
View notes
Quote
As a reporter, in general I’m not supposed to say something like this, but: The president’s statements to the press were terrifying. That press availability was a repudiation of good science and good crisis management from inside one of the world’s most respected scientific institutions. It was full of Dear Leader-ish compliments, non-sequitorial defenses of unrelated matters, attacks on an American governor, and—most importantly—misinformation about the virus and the US response. That’s particularly painful coming from inside the CDC, a longtime powerhouse in global public health now reduced to being a backdrop for grubby politics. During a public health crisis, clear and true information from leaders is the only way to avoid dangerous panic. Yet here we are. Most of the deaths from Covid-19 in the US so far have been in Washington state, concentrated in a care facility for the elderly in Seattle. At the CDC, the president said of Washington’s governor Jay Inslee (who has declared a State of Emergency), “That governor is a snake … Let me just tell you, we have a lot of problems with the governor and the governor of Washington. That’s where you have many of your problems, OK?” That animosity doesn’t seem to be related to Inslee’s handling of the outbreak. The president may have been reacting to criticism from Inslee on Twitter about the way the outbreak has been handled, and until last summer Inslee was a candidate for the Democratic nomination to run against Trump in the November presidential election. Azar started talking about the tests health care workers use to determine if someone is infected with the new coronavirus. The lack of those kits has meant a dangerous lack of epidemiological information about the spread and severity of the disease in the US, exacerbated by opacity on the part of the government. Azar tried to say that more tests were on the way, pending quality control. Then Trump cut Azar off. “But I think, importantly, anybody, right now and yesterday, that needs a test gets a test. They’re there, they have the tests, and the tests are beautiful. Anybody that needs a test gets a test,” Trump said. This is untrue. Vice President Pence told reporters Thursday that the US didn’t have enough test kits to meet demand.
Trump’s Coronavirus Press Event Was Even Worse Than It Looked | WIRED
27 notes
·
View notes
Text
“Is it just me, or is it getting crazier out there?”
“Is it just me, or is it getting crazier out there?”
Arthur Fleck-Joker (Phillips, 2019)
This phrase makes much sense lately. Maybe it is just me getting mature and realizing what is going around us. For sure poverty, crime, political corruption etc. are not new to many countries around the World. But with Covid-19 pandemic, so called developing countries such as mine, has gone crazier than before.
What shocked me is that people became much and much ignorant, the more they witnessed deficiancy of their government. They bound to their baseless excuses and prejudices as if their life depends on it.
I do not meant to underestimate the danger of a pandemic, yet here we are imprisoned by our own faults and governmental choices. While mortality rate should be of 3-4% (WHO, 2019), we are standing over a mass grave MORE THAN 900 000 death toll (WHO,2020). Besides, this is only the reported body count.
On my behalf, I can say that, expecting everything to magically heal and our wounds to be patched is childish. For roots of our problems goes way dipper than what is seen outside. Education system is infected with inflated majors and graduate enflation. While public schools are moderately cheap, they are overpopulated and cannot offer pupils a bright future. Private schools and colleges are legal pirates with blinding promises.
Corruption and discrimination are the routines of a Daily work. If you refuse to take bribe or be a just citizen, you are blamed to be naive and childish.
Sometimes I wonder whether we are living in DC movie or not. The problem is even the villains in such movies are much more logical than our enemies in real World. When I look at our President, I wonder how can our people chose someone. His rage, ambition and weakness are dropping from his face. I guess we must be thankful for not having movie kind of villain in our lives for sure, but I cannot stop thinking “how come we, as human kind, make so little of ourselves” .
All the nations on the World brag about their power, history and heroism. Yet, we still cannot overcome basic problems. Still people die of hunger, powerty controls humans’ fate. Crusadors and pilgrims talk about religion and cihad without understanding a Word from any of the holly books. Though we are capable of doing great things, we are still bound to our egos, which makes us look like poorly written Comic Book characters.
Phillips, T. (Director). (2019). Joker [Film]. Warner Bros. Prictures, DC Films, Joint Effort Bron Creative, Village Roadshow Pictures.
World Health Organization (2019, 17 September). Q&A: Influenza and COVID-19 - similarities and differences.
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-similarities-and-differences-covid-19-and-influenza#:~:text=Mortality%20for%20COVID%2D19,quality%20of%20health%20care. Accessed on 22th of Septemper 2020.
World Health Organization (2020, 6 September). Coronavirus disease (COVID-19): Weekly Epidemiological Update.
https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200907-weekly-epi-update-4.pdf?sfvrsn=f5f607ee_2 Accessed on 22th of September 2020.
1 note
·
View note
Text
Mayor of Las Vegas says the "free market" will decide what's safe

Reality - especially epidemiology - has a distinct leftist bias, which almost makes you feel sorry for right-wing ideologues like Las Vegas Mayor Carolyn Goodman, who says that every business in town will get to make up its own rules after she unilaterally lifts quarantine.
She told CNN, "I am not a private owner. That's the competition in this country. The free enterprise and to be able to make sure that what you offer the public meets the needs of the public."
https://edition.cnn.com/2020/04/22/politics/las-vegas-mayor-social-distancing-cnntv/index.html
You can see where she's coming from. Her entire worldview is shaped by the Thatcherite dogma that "there is no such thing as society." The Reaganite cant that "The nine most terrifying words in the English language are: I'm from the government, and I'm here to help."
This only makes sense if you don't believe that humans have shared destiny - that your neighbor's problems are not your problems. Even in the best of times, this is obviously untrue (your neighbor's decision to play loud music at 2AM or to store plutonium in his backyard).
Humans OBVIOUSLY have a shared destiny, including/especially a shared microbial destiny. There's a great Lenny Bruce sketch about this, positing that the basis of society is agreement about where we crap and where we eat.
https://scrapsfromtheloft.com/2017/08/25/lenny-bruce-berkeley-concert-1965-full-transcript/

Mayor Goodman's position comes down to this: "We're all in the same swimming pool. This end is the no-pissing-in-the-pool end. That end is the pissing-in-the-pool end. This will all be fine."
The small business that reopens with inadequate measures will not harm only itself and its customer. It will harm everyone who comes into contact with those people.
There's lots more wrong with Goodman's idea: like the fact that, workers rely on governments for protection from employers. There's a buyer's market for labor, so employers can treat workers as disposable, murdering them through inadequate protection and then replacing them.
Or the fact that neither business owners nor customers are qualified to assess the sufficiency of a given plan to re-open. That's like saying, "OK, everyone who wants to fly in an airplane should just inspect it themselves and decide whether it's safe."
The complex technical questions of the modern world cannot be navigated through individual research: you can't individually assess the safety of planes, or building codes, or food prep. You can't know if a slot-machine is fair or gimmicked.
We need impartial expert agencies that conduct truth-seeking exercises to determine the best practices, and then conduct inspections and enforcement on our behalf. Not the "personal responsibility" of becoming an expert in every technical subject we live and die by.
These agencies need to show their work, recuse themselves over conflicts of interest, and hear and act on new information as it becomes available.
They need to use a universally legible PROCESS that comes to technically legible CONCLUSIONS.
That is, they need to govern, as part of a legitimate, responsive state.
The problem of electing people who believe in dismantling government is that they dismantle government.
That works great, but fails badly - I neither want to have to determine whether a barber is safe to visit, nor trust the barber to make that determination. I want a public health expert to make it, and I want that person to be overseen by a democratic institution.
What's more, if YOU are willing to trust the barber (or yourself) and you get it wrong, you could infect ME. This is not a matter of personal choice and personal responsibility. It is a matter of stubbornly irreducible shared destiny.
I get that this is inconvenient for people who believe that shared destiny is a Communist plot. But, as our friends on the right are fond of reminding us, "reality doesn't care about your feelings."
Image: Las Vegas Guy, modified
https://commons.wikimedia.org/wiki/File:Las_Vegas_Sign_Nightly.jpg
CC BY-SA https://creativecommons.org/licenses/by-sa/4.0/deed.en
56 notes
·
View notes
Text
Ideal questions and responses about COVID for Biden in an interview situation
I know there's no chance of this actually happening but I really wish 1. someone would throw these hardballs and 2. we had a snowball's shot in hell of getting these kinds of answers for them. It's really a shame that our media is both designed to cater to the lowest common denominator and are the only ones who get to have both remit AND access to provide oversight on the government, because #1 often leads to them completely missing the point on #2 in pursuit of a rating
1Q. Many critics have pointed to errors in the White House response to the early days of the coronavirus pandemic, before it had reached community spread status in the US, as a lost opportunity to take drastic action to control the situation. What do you think was the most critical error made during this period, and how would you have approached it differently?
1A. The number one error here was that the responsibility for handling this was left in the hands of political actors, automatically turning it into a political situation. Public health is not a spectrum for political debate or posturing; it is a matter for science and evidence-based problem solving, and the primary decision-making should have been placed in the hands of qualified doctors and epidemiology experts as early as possible. In a situation like this, the President should serve in more of a co-ordinating role, ensuring that the states and various federal departments which must work together to solve such a problem are all on the same page and mediating any conflicting interests or needs. The current administration failed abysmally in this role and there are in fact fairly substantial rumors that the White House chose to play parties against each other which should have been working together, in hopes of exacting a political gain out of the situation. That is an extremely inappropriate abuse of power in any case, but particularly when the lives and livelihoods of so many are on the line.
2Q. For well over a decade before the COVID-19 virus was first identified, public health experts had been saying that the US' preparedness for a pandemic response was a major weak point in our homeland security, with events such as SARS, MERS and H1N1 serving as something of a canary in the coal mine showing where major deficiencies in the system lay. What lessons would you take about emergency preparedness into your own administration, and how will you implement them?
2A. From a very young age I've been taught that a failure to plan is a plan for failure. When millions of lives are on the line, you can't just wing it. The current administration's decision to disband the already-neglected pandemic response team in 2018 was a critical point of failure, and the unqualified, partial and partisan leadership which it has appointed to various other departments has also stripped many critical structures and steering committees in those departments. We are still unprepared for another national pandemic, particularly one of significantly greater virulence or mortality, and there are many other crisis situations our nation could face for which we are equally unprepared. One of the missions of my first 100 days in office would be the appointment of new, nonpartisan, disinterested and highly qualified leadership to as many cabinet positions and executive departments as possible, and tasking these new leaders with the development of actionable contingency plans for the various emergencies for which we are currently underprepared. Having these plans in place would then allow nationally coordinated "war games" type training exercises to occur on a regular basis, making key figures' responses as rehearsed and coordinated as possible should the worst come to pass. In a situation like that, we do not need to be scrambling for our first steps; everyone should know their role and what immediate actions they should take to control the severity of the situation and mitigate it as much as possible.
3Q. What might an effective plan for pandemic response look like?
3A. Obviously I am not the best person to ask and this would be better directed to public health experts, but based on the notable areas of deficiency this situation has thrown into relief, I would say:
1. Begin by having a better social safety net in place which helps reduce the number of people in exceptionally vulnerable situations such as homelessness or being without access to affordable healthcare
2. As soon as possible upon the identification of the threat, get tests developed to diagnose it. If another country has developed an effective test and is willing to share with us, work with them and try to return the favor somehow (eg. supplying equipment).
3. Use the Defense Powers Act to ramp up manufacture of these tests, PPE, equipment and medicines needed to treat the disease, etc. ASAP. Better to be in a position where we can provide extra supplies to other nations with limited resources than stuck without any ourselves.
4. Advise US travelers in foreign countries to return home immediately if they lack resources to remain abroad indefinitely; require airlines to allow these travelers to change to earlier flights home for no fee in order to receive subsidy during the likely coming drought of flights. Initiate quarantine measures or, preferably, testing for the disease at all entry points to the US, possibly by deploying the National Guard if extra hands are needed, in hopes of containing the disease at the border. Care for affected individuals in secure locations isolated from the public, with medical professionals taking every biosecurity precaution available when entering and exiting the facility.
5. In preparation for the possibility of community spread, issue an advisory to businesses, educational institutions, etc. to prepare for the potential of a stay-home environment and perhaps begin preemptively transitioning those who are capable to a work-from-home environment. In the case of colleges issue guidance for an ideal management plan that allows students to move out of campus housing with all their belongings and doesn't strand out-of-state and international students who can't afford or arrange an immediate flight home.
6. Work with Congressional leadership to prepare succinct, bipartisan legislation protecting the American people and their livelihood for immediate action should the need arise, including stimulus checks, welfare for those out of work as a result of the disaster, hazard pay and minimum protective standards for essential workers, and rescue funding for small businesses forced to shutter during the crisis.
7. Work with state and local governments on preparing initiatives to limit community spread and protect citizens which operate better at this scale, such as stay-at-home orders and rent freezes
8. Remain in close contact with leading experts at HHS, DHS, CDC, FDA and other relevant organizations to stay abreast of further developments and draft a course of action to address them
9. Remember that in a situation like this the most valuable resource by far is TIME and early, preventative action saves a lot of heartache down the line.
#I am so tired of this country being run by the keystone kops#personal#politics#I play the bassoon better than Donald Trump plays the role of president
5 notes
·
View notes