#suffering cmv
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text
one of my favorite things about the suffering cmv actually is the couple of people in the background- they bothered me at first cause I’d like it if there wasn’t any in the background, but if you look at them as the other SIRENS?? that shit goes hard.
they’re all only showing waist up far away in the water and that’s so tasty— like, they’re just out of sight so that odysseus’s attention is only on penelope but they’re still LURKING back there
anyways thanks random surfers in the background for worldbuilding my cmv


double anyways- GO WATCH THE CMV
youtube
#suffering cmv#epic the musical#epic the musical odysseus#epic the thunder saga#epic the musical suffering#etm#Youtube
211 notes
·
View notes
Text
HELLUVA BOSS - BLITZO | Family - Part 9 for Childhood Creativity Studios
#mep part#helluva boss#helluva boss edit#blitzo#blitzø#blitzø buckzo#tilla buckzo#cash buckzo#barbie wire#fizzarolli#vivziepop#amv#cmv#mep#badflower#family#angst#helluva boss angst#Blitzo is MY comfort character and I get to capitalize on his suffering however I please!
51 notes
·
View notes
Text
little thoughts about the brutus cmv
"that the people would see me too as a poet/and not just the muse" is really interesting coming from fable. because he kind of has a point. the aether is inherently derivative and dependent on the other three realms. if it's a work of great art, the other three major gods serve as muses
especially from fable's point of view; in more modern conceptions, the muse of an artist is often mistreated, exploited, and under-credited. (they're also usually like. women suffering under misogynist structures of art and finance, but fable has such a victim complex i can see him being fine with co-opting that /j)
similarly, "i'll never forget that you showed me how to make art" alerion made the other realms for his siblings, which then inspired the creation of mortals. the works of art that fable is driven to kill by losing to alerion also owe their existence to him, in a way
it is so weird seeing trees in full leaf knowing this cmv was filmed, what, two weeks ago? that is NOT how i'm used to trees looking in early may. why is it so green.
"frater meus" hits harder when you remember that vo'lete is largely based off latin. fable is calling alerion his brother in his own language while rationalising why he has to die
obviously the song choice is fucking incredible, you don't need me to tell you that. espicially when that fourth verse hits my god
also alerion desperately crawling backwards and fable shouting why and how this is for the best down at him. peak cinema
it seems like when fable is stewing on the bench there's actually blood on the tip of the sword? like it's mostly out of frame but i swear it's red in some places
in conclusion:

62 notes
·
View notes
Text
Also preserved in our archive
The cost is set to go far beyond human suffering, yet almost five years into the pandemic, not only are there still no treatments for long Covid, there aren’t even any diagnostic tools – and we don’t seem overly interested in finding them.
The jig is up. People are catching on that “mild” Covid-19 may not be so mild, and that the mysterious lingering symptoms they’ve experienced after catching the virus, such as fatigue and brain fog, may just be connected. For others, this will be the first time that they put two and two together. I hate to be the bearer of bad news, but strap in for what comes next.
Recently, RNZ ran a piece outlining the estimated $2bn per year economic cost of long Covid in New Zealand and signalling that further research would be needed to determine a more precise figure. The average reader would assume that this research is under way or has at least been planned and funded. Human suffering aside, such a hit to productivity would surely raise alarm bells across the political spectrum!
I say this solemnly: yeah… nah.
Almost five years into the pandemic, not only are there still no treatments for long Covid, there also aren’t even any diagnostic tools – and we don’t seem overly interested in finding them.
At present, a long Covid diagnosis relies on a patient finding a doctor with up-to-date knowledge, who will believe their symptoms, and who will spend time investigating further to rule out other possibilities. This mythical trifecta is out of reach for most people, particularly women, who are affected by immune conditions at far higher rates, but have their symptoms written off as hysteria; and Māori and Pasifika, who face barriers to healthcare, and have their symptoms written off as laziness. Obtaining accurate data on prevalence under these circumstances is simply impossible.
In this way, and several others, long Covid mirrors ME/CFS (myalgic encephalomyelitis), a brutally debilitating biophysical condition, though the oft misused term “chronic fatigue” doesn’t quite convey that. Around half of long Covid sufferers meet the criteria for ME/CFS, which by the World Health Organization’s scale has a worse disease burden than HIV/Aids, multiple sclerosis (MS), and many forms of cancer. But again, there are no treatments.
I suffer from ME/CFS myself. My illness predates Covid-19 and came on after an infection with cytomegalovirus (CMV). I went from a fit and active young man to debilitatingly sick and fatigued, with several unexplained symptoms.
Pre-pandemic there was estimated to be more than 25,000 people in New Zealand suffering from ME/CFS, and only one specialist in the country, working one day a week, who has since retired (well earned, bless her). For years I had been praying for any sort of diagnosis, even if it was bad, so that I could get on the path to recovery. I got the diagnosis – but for a disease with no path to recovery.
As the pandemic unfolded, patients and advocates in the ME/CFS community warned that a tsunami of disability was approaching. They were of course ignored, as they have been for decades, and are now joined by masses of long Covid sufferers facing the reality that the medical profession has no answers for them, except perhaps euthanasia.
Frustrated with my lack of options, I connected with cellular immunologist Dr Anna Brooks, who had become a leading expert on long Covid, so I assumed that her biomedical research would be well supported. Alas, she detailed the uphill grind that it’s been to gain traction compared to other countries, and that generous donations, usually from patients themselves, had been the driving force of funding.
Together we founded DysImmune Research Aotearoa, with the goal of developing diagnostic tools leading to treatment for post-viral illnesses like long Covid and ME/CFS. In layman’s terms, we collect blood samples, analyse differences in cells, and put together an immune profile. My priority is ensuring that Māori and Pasifika patients and researchers are at the table and taking action into our own hands.
We’ve made a small start, and we have some incredible collaborations lined up, with far-reaching implications for community health. We’re in the process of seeking partnerships to take things forward. The expertise exists, it’s here in New Zealand. Still, the barrier to progress across the research space is the urgency for resourcing. It is dire to say the least.
Without some long-term project certainty, it’s difficult to pull the necessary teams together. While study after study illuminates more horrifying long-term effects of Covid infections, and prevention has been completely abandoned, research and development for treatments for long Covid is tanking. The private sector is at the whim of the quarterly financial report, and with no guaranteed short-term profit in treating us, it has very little incentive to take the risk.
So, barring some philanthropic miracle, only government can fill this gap. Yet where Australia had set aside A$50m specifically for long Covid research, and the US Senate considers a billion-dollar long Covid “moonshot” bill, New Zealand has allocated nothing. We’re fast asleep at the wheel. No other country can determine how many of our people are impacted by post-viral illnesses. No other country can address our specific needs.
Since this government is focused on ambition, productivity and fast-tracking, I assume they’d want to be world leaders in research, warp-speed some projects, and get long Covid sufferers back into work, no? This is what we are calling for. Not surveys. Not “talk” therapy and positive thinking. Biomedical research.
Put the money down and commit to this. Seize this opportunity to right decades of neglect. There are tens of thousands of us fighting for our lives, and millions more around the world. You think it won’t be you, then after your next inevitable Covid-19 reinfection, it is, and you’re left to wonder why nobody stepped up.
Government, iwi and whānau ora groups, health organisations, philanthropists – reach out. Let’s work.
Rohan Botica (Te Ātihaunui-a-Pāpārangi, Ngāti Tūwharetoa) is a lived-experience researcher and co-founder of DysImmune Research Aotearoa.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#long covid#covidー19#covid conscious#covid is airborne#covid isn't over#covid pandemic#covid19#the pandemic isn't over
29 notes
·
View notes
Text
my thoughts after watching the Icarus Morningstar "Gold" cmv
I realized I never posted them anywhere so tumblr may have them. -the thought of quixis being a sherbert variant from another universe and them having no eyes. what if they had the power to change things to their will but couldn't controll it and on accident glitched out their own eyes and they were looking for a way to fix that giving the different sherbert variants across dimensions different eyes to see if one is stable and the can use it for themselve but no one is. it always bleeds… -also with the fingers being blackend. what if the more they change things the more it hurts them. we know the worldport is falling appart. and big changes like the wings cause more damage but they keep trying to communicate. trying to warn icarus. they once said at the pond that somebody was going to be in danger. and quixis changed the pond to brewing stands basically saying that icarus is in danger. -my running theory is: quixis is a sherbert whos home dimension was destroyed and who could safe themself into the world port. Now they are trying to warn other sherbert variants from suffering the same fate even if their powers get out of controll and they hurt themself while doing so. but i do like the idea of quixis being a rae variant i once saw too.
24 notes
·
View notes
Text
I normally post about how surrogacy exploits women but this is an example of how the business part of ivf exploits women. They took that couples money after promising careful screening of the soerm donors. Instead the mother was infected with an STI that would impact any future pregnancies, they lost one baby and the other will need life long care.
The state Supreme Court confronted philosophical questions about “wrongful birth” and the value of life Wednesday when the state asked the justices to reverse a $37 million verdict awarded to a family whose lives were upended by a tragically flawed artificial insemination procedure at UConn Health.
Jean-Marie Monroe-Lynch, her husband Aaron Lynch and their surviving son Joshua sued for malpractice after fertility specialists affiliated with the University of Connecticut’s medical center inseminated her with sperm from an anonymous donor infected with cytomegalovirus, or CMV, a common, sexually transmitted virus that has catastrophic effects on fetal development.
The procedure, a therapeutic donor insemination, succeeded in that the mother became pregnant with twins, a boy and girl. But she and the children were infected with CMV. One of the twins died and the other was born in January 2015 with a long list of devastating disabilities that will put him in need of constant, life-long care. The surviving twin, Joshua, cannot communicate or care for himself, has global developmental delays; suffers from cognitive, hearing and movement deficits; suffers from autism and seizures, and spends hours each day having nutrition pumped into his body through a tube.
In its appeal, the state is arguing, among other things, that the family’s suit was not based in the usual definition of malpractice but is rather what has become known as a wrongful life suit, a relatively new and controversial action against medical practitioners for failing to properly prevent the birth of children, such as Joshua, shown through prenatal examinations to have tragically debilitating conditions.
See rest of article
#usa#connecticut#Ivf#Wrongful birth#UConn Health#cytomegalovirus or CMV#Wrongful life suit#The fertility industry is just like another big business
9 notes
·
View notes
Text
Hokotae in Stalemate- Korlan Fails to Encircle Hēre in Fourth Month of Invasion
[Federal Kingdom of Vau’sena, Kuwhara, Rangat- 17 November 2053
Annalies Willems, Cosonan News Network]
The war in the Kuata Strait opened quickly- the robust Korlanic Navy wasted no time surrounding, besieging, and bombarding the islands of Hokoihoko and Hokotae off of the coast of Ramisola, Vau’sena’s largest island and home to over 74 million people in the constituencies of Kuwhara and Volios. After capturing Hokoihoko in only four days of conflict, Korlanic forces looked to make quick work of the Kuwharan province of Hokotae to complete its conquest of the Korlanic Isles before advancing into the heart of Kuwharan society on Ramisola.
Uniting the various ethnically Korlanic populations of Ailou has been a long-standing goal of Korlanic Rangatira Ikaroa Storinka, with Kuwhara’s status as a democratic and patriotic constituency of the Federal Kingdom of Vau’sena resting as a particular thorn in Storinka’s side. From its broad ethnic and linguistic diversity to its democratic leadership centered in the Ripieran constituency of Cosona, the very existence of the Vau’senaan state flies in the face of Storinka’s Ilfiatist ideology of control and uniformity. The ideological struggle simmering across the Kuata Strait came to a boil in late June, culminating in the ongoing battle on the Island of Hokotae.
The Battle of Hokotae, however, has proved to be far from the decisive victory that Korlan experienced on the island of Hokoihoko. Zones of control remain static as the battle drags into its 134th day, a fact held as a point of pride by Vau’senaan defenders initially caught encircled flat-footed by the sudden blockade. The beginning of the Korlanic attack employed brutal tactics to bring the island to its knees- a campaign of etymological warfare that employed swarms of locusts to destroy crops and block out targeting systems on the island, the deployment of chemical weapons into population centers, and the assassination of leading logistics directors which sent the island into famine and allowed Korlanic landing parties to make footholds on the south of the island.
The Korlanic blockade was first broken on the 21st day of the battle, however, through the use of new implosion-type precision ordinances by the Royal Vau’senaan Air Force. While the specifics of this new Vau’senaan weapon have remained highly classified, observers have described the missile’s implosive force as sufficient to rip a third of a battleship away in under 30 seconds, blasting away surrounding seawater and slowly falling into the air pocket left behind until losing power about 45 seconds after impact, leaving the battered ship to be crushed by the force of returning seawater. Each of the three times the new weapon has been deployed in significant numbers onto the battlefield it has seen crushing success, breaking blockades on the 21st, 77th, and 115th days of the battle, each time allowing between 6 and 18 days for Vau’senaan forces to bring in supplies, transport casualties and civilians to Ramisola, and even permitting the damaged aircraft carrier CMV Kiti Firine'a to be evacuated to Cosona for repairs. The Vau’senaan access to Hokotae, however punctuated by returning Korlanic ships, has proved crucial in repelling the Korlanic Army from the regional capital and largest city Hēre, which has come near to being encircled on numerous occasions.
The Battle of Hokotae has come at a heavy cost to attacking Korlanic forces. According to a statement given by the Dive’ira’Ministerie Vau’senaan (Vau’senaan Ministry of Defense), Defense Minister Liyet Ts’iyniyn estimates Korlanic casualties on the island to have reached 125,000 since the beginning of the invasion, putting Korlanic casualties suffered on the ground at a higher figure than those sustained in the 28 July nuclear strike which wiped out an estimated 100,000 embarked forces in deep water in the middle of the Kuata Strait. The Vau’senaan defense of Ponder has seen its own successes, succeeding in deterring an invasion at all from being launched from the Korlanic-occupied Hegiite province. However, the unfolding Korlanic invasion of Pylerick threatens to expose the Vau’senaan mainland to danger from Korlanic weaponry.
[In accordance with the Wartime Information Act of 2053, information published by any and all private persons and registered media outlets within the Federal Kingdom of Vau’sena may be subject to censorship with or without notice]
8 notes
·
View notes
Text
aight fam let's do this. pick out your favorite trio of war criminals and slap 'em into this baby. however i like the categories in the original post better so we're revoerting to them:
murderer
poor sleepless bastard
massive fuckup
now i will admit that i don't have an ot3, or otp, or otanything in 40k, i'm very much a multishipper kind of gal when it comes to this fandom. except for dantilux. THEY R IN LUUUUURVVVVVVV i guess that's my otp. ANGYWANYS everyone else is fair game for shipping for me, so i just picked out a threesome that i liked, which is Blondes in Crisis. Blondes in Crisis is the main reason i ever picked up an HH book outside of know no fear, love me sum oversized demigods YELLING!! at each other for fucking up everything, do you know how refreshing it was to watch gman lose his shit about lion at poor sangy in the middle of the rolling depression that is pharos?? AMAZING what an asshole. anyways they are clearly all fucking each other because if they didn't blow off steam that way they'd kill each other and possibly the whole of macragge in the process. so here's my breakdaown:
murderer - lion, because duh
poor sleepless bastard - sanguinius is the poor sleepless bastard for the whole damn series cmv, the man is the tragic wattpad self-insert we all wrote when we were 13 and we love him for it. and for what does a tragic wattpad slef-insert exist, if not to suffer? tragically? your honor i rest my case
massive fuckup - big bobby g earsn this for coming up with imperium sanctus in the first place. remember the bit in unremembered empire where he fucking talks himself into starting imperium 2.0?? my dude, just announce a regency while y;all figure the ruinstorm out, people will roll with it. gman himself agrees with this cateogorization later on in the timeline, he's soooo fucking ashamed of himself, dude got all melodramatic and closed the library of hera instead ovf burning a few books because he's so fucking embarassed
the only other trio i could think of was emps/malc/erda. this one's pretty straightforward:
murderer - empse, BECAUSE DUH
poor sleepless bastard - malcador, lord knows he cleans up all the messes. worst sugar baby job ever!!!
massive fuckup - erda. bitch yeeted her sons into the warp and called it a day, WHY WOULD YOU DO THAT, THAT DOES NOT FIX ANYTHING ANGRON WAS FUCKING LOBOTOMIZED YOU DUMBASS
ok i'm done it's your turns

This has probably DEFINITELY already been done before oof
Training Trio Training Trio Training Trio!!! ❤️💙💜
#warhammer 40k#lion el'jonson#sanguinius#roboute guilliman#the emperor 40k#malcador#erda#lion x guilliman x sanguinius#the emperor x erda x malcador#dantilux
860 notes
·
View notes
Text
Living Donor Kidney Transplant in India
Kidney diseases are on the rise. Lifestyles, dietary habits, and excessive alcohol and tobacco consumption are the major factors responsible for kidney diseases. In India, there are many Kidney transplant specialist surgeons at many better-equipped hospitals to provide successful live donor Kidney transplants. As the awareness and availability of organ donation post-death(deceased Donor) are still in a very nascent stage, Kidney from deceased donors are not readily available and patients suffering from an end-stage renal disease requiring a kidney transplant depend on donation from living family members for live donor kidney transplants. At CMCS Health We are associated with the best and most experienced Kidney transplant surgeons and the best kidney transplant hospitals in India.
Who can be a living donor for a Kidney transplant needing patient in India?
A healthy blood-related family member usually a son or daughter/parents, grandparents and grandchildren, and brothers and sisters are considered blood relations. The donor needs to be a major in the age group of 18-55 years preferably and healthy enough to donate one of his kidneys, without any risk to his quality of life post-donation. Prelim tests for the fitness and compatibility of donors are done for screening and choosing the correct donor for a successful kidney transplant. Any other relative is considered an unrelated donor and certain documents are needed to prove to the Government of India-appointed organ transplant committee that the donor is related to the patient requiring kidney transplant. And donor is willing to donate one of his kidneys to the patient out of love and family bonding and not under any pressure or monetary obligations.
What happens to a Living Donor after a successful Kidney Donation?
A healthy and fit donor lives a perfectly normal life post the donation of one of his kidneys. The doctors do advise him on certain do's and do not post-donation. Anything that is not good for the health of a person with both kidneys functioning normally is also considered bad for the live donor. Regular and periodic checkups are suggested for a live donor. As high blood pressure and diabetes are considered two major causes of kidney function going bad, the donor is advised to follow a healthy lifestyle to remain disease-free.
Does live donors have a health risk or compromised life post-kidney donation?
A healthy donor lives a perfectly normal life, post-donation. Donation of a kidney does not hurt overall life or quality of life for the donor. Selecting the right donor is important as it cuts down the cost of dialysis and the need for frequent admission of patients till the time we get approval from the government of India-appointed transplant committee for kidney transplants. Once the approval is given by the Committee, the patient is given a date and time for surgery. The following tests for donors are required to lessen the chances of flying in the wrong donor and save time and money for guests till we fly in the right donor.
1. Urine ( SPOT), Protein creatinine ratio, LFT (Liver function test), Urea, Creatinine, Sodium(Na), Potassium (K), Blood sugar( Fasting and Postprandial), HBA1C, Calcium (Ca), Phosphate (Po4), Uric Acid, PTH, Lipid profile, Vitamin D level, T3, T4, TSH and LDH.
2. Complete Hemogram, BT, CT, PT, PTTK, and urine routine.
3. Urine culture, CMV-IGG, EBV(CAPSId)_IGG, for MALE patient PSA (if above 50 years of age). for Female patient CA-125 and pap smear.
4. Blood group, HBSAG, Anti HCV antibody, HIV1 & 2, HCV RNA qualitative, Anti-HBS antibody.
5. ECG, Echo/stress echo, Cardiac clearance.
6. Chest X-ray, Ultrasound-whole abdomen, CT (Angio) for renal vessels, DTPA scan, etc.
CMCS Health is a leading medical tourism company in India. We offer medical tourism services such as finding the right doctor, the right hospital, and cost estimation for medical treatment in India for foreign patients. Some of the main countries are Bangladesh, South Africa, Egypt, Kenya, Saudi Arabia, Ethiopia, Nigeria, Uganda, Zambia, Sudan, Dubai, Namibia, Iraq, and so on. We provide free medical assistance aplastic anemia treatment cost, stomach cancer treatment, sickle cell treatment cost, the best hospital for heart valve replacement, heart valve surgery, arthroscopic surgery, bone marrow transplant cost, best liver transplant hospital, brain tumor surgery cost, cosmetic andplastic surgery, heart surgery, kidney transplant cost,spine tumor surgery,cancer treatment cost, lung transplant,liver transplant cost, top knee replacement surgeons, knee replacement surgery cost, top shoulder replacement surgeons, hip replacement surgery cost, best bone marrow hospital, etc. If you are searching for free medical and healthcare consulting to find the best hospitals and top doctors and surgeons in India for any treatment then contact us- Cmcshealth.com.
Source: https://cmcshealth1.blogspot.com/2024/11/living-donor-kidney-transplant-in-india.html
0 notes
Text
Cytomegalovirus Treatment Market Trends, Key Driven Factors, Region-wise Outlook, Segmentation And Forecast To 2022-2028
The global Cytomegalovirus Treatment market is experiencing significant growth, driven by a rising demand for effective treatment options and advancements in technology. Cytomegalovirus (CMV) is a common viral infection that can cause serious complications, particularly in individuals with weakened immune systems.
According to market research, the Cytomegalovirus Treatment market is predicted to increase at a steady CAGR of 6.1% from 2022 to 2028. The market growth can be attributed to various factors, including an increase in the prevalence of CMV infections, expanding geriatric population, and growing awareness regarding early diagnosis and treatment.
The cytomegalovirus treatment market is poised to grow at an impressive y-o-y of over 5.5% in 2019, as per the latest research study published by FMI. A cohort of macro factors, including rapid adoption of innovative treatment procedures and burgeoning investments in healthcare, are auguring well for the wide-spread adoption of cytomegalovirus treatment. These insights are per the latest FMI research study that conveys a healthy outlook for global cytomegalovirus market in 2019 and beyond.
Patient pool affected by cytomegalovirus is on a consistent rise, necessitating adoption of effective treatment methods and therapies. As per a revelation by the MedlinePlus, between 50 percent and 80 percent of adults in the US have suffered from cytomegalovirus by the age of 40. Statistics as such demonstrate augmented adoption of cytomegalovirus treatment products and procedures in the future, creating sustained opportunities for the manufacturers to reap sizeable revenues.
To remain ahead of your competitors, request for a sample – https://www.futuremarketinsights.com/reports/sample/rep-gb-8665
As per the FMI report, demand for valganciclovir drug continues to be buoyant on account of effective results if taken at evenly spaced intervals, with global sales likely to surpass US$ 55.5 Mn in 2019. In addition to this, valganciclovir is less time-consuming and affordable, which is further adding to its popularity in the cytomegalovirus treatment space.
“The drug development framework for treatment of cytomegalovirus continues to be progressive, offering ample scope for development of new products and procedures. There are multiple clinical trials being performed for cytomegalovirus treatment worldwide, led by prominent regions including Europe and North America. The late-stage pipeline comprises exceptional drugs which are envisioned to enter the market. This, in turn, is likely to create favorable scenario for cytomegalovirus treatment market over the forecast period”, says FMI report.
Hospital Pharmacies Remain Highly Lucrative Channel for Manufacturers with Notable ROI Benefits
As per the report, congenital CMV infection registers substantial demand for cytomegalovirus treatment, with global sales expected to surpass over US$ 65.5 Mn in 2019. Hospital pharmacies are likely to steer sales of cytomegalovirus treatment products and procedures, owing to reliable offerings at reasonable costs. The well-informed and modern patients seek a combination of efficiency with convenience, which is making e-commerce a rapidly growing distribution channel for manufacturers to commercialize their offerings.
As per the report, high cost of cytomegalovirus treatment procedures remains a key factor hampering adoption and deterring market’s growth potential. Along with high prices, associated side effects of cytomegalovirus treatment products and procedures are denting end-user confidence. Some of the prevalent side effects associated with cytomegalovirus treatment products and procedures include neutropenia, nausea, thrombocytopenia, hematological toxicity, renal dysfunction, and so on.
0 notes
Text

-USMC MV-22 Ospreys on the deck of USS Bataan. | Photo: Staff Sgt. Wayne Campbell, USMC
Flightline: 62 - Bell/Boeing V-22 Osprey
After the disastrous failure at Desert One during the 1980 Iran hostage rescue mission, the US DOD recognized that there existed a requirement for a transport that could take off and land vertically, but also travel long distance at speed. The Joint-service Vertical take-off/landing Experimental (JVX) program was begun in 1981 to obtain and combine requirements from the Army, Navy, Marines and USAF. In late 1982 a request for proposals was released, attracting interest from Aérospatiale, Bell Helicopter, Boeing Vertol, Grumman, Lockheed, and Westland. Bell later teamed with Boeing Vertol, submitting a design based on the former’s XV-15 tiltrotor.
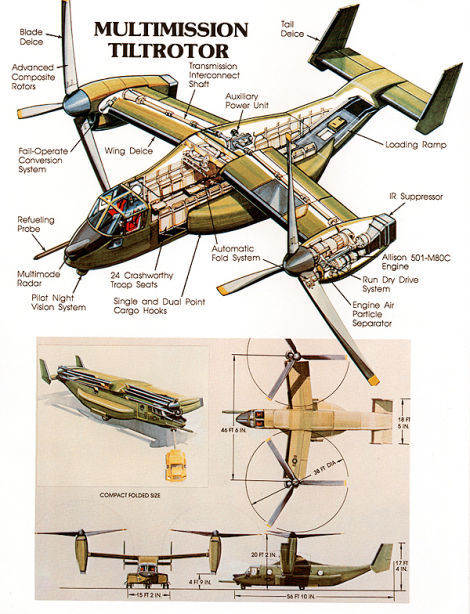
-Early concept image of V-22 Osprey, probably from mid to late-1980s. | Photo: US Navy
Bell/Boeing submitted the only design, and were awarded a preliminary design contract was awarded on 26 April 1983. In 1985 the Bell/Boeing JVX design was named the Osprey, and given the designation V-22, with USMC Osprey known as MV-22 and USAF CV-22, in part to avoid confusion with USN carrier designation (CV). By March of that year, the first half-dozen prototypes were under construction, with work split between Bell and Boeing. The first V-22 was rolled out in 1988, but the program also suffered major issues that year. Costs ballooned, from $2.5 billion in 1986 to a projected $30 billion in 1988. Citing a need to focus on other programs, the US Army dropped out of the program. The following year, the US Senate voted twice to cancel the Osprey, though the program survived. The DOD then ordered the Navy to not spend more money on the V-22, and SecDef Cheney tried several times from 1989 to 1992 to defund the program, though each time he was overruled by Congress.

-Bell-Boeing’s first V-22 prototype transitions to forward flight. | Photo: Bell/Boeing
The first of six prototypes first flew on 19 March 1989 in the helicopter mode, and on 14 September 1989 in fixed-wing mode. Sea trials were completed on USS Wasp in December 1990, though the program was marred by crashes of the fourth and fifth prototypes in 1991 and 1992. The V-22 was grounded until June of 1993 to make needed changes. From October 1992 – April 1993, the V-22 was redesigned to reduce empty weight, simplify manufacture, and reduce build costs; resulting in the V-22B variant. The existing prototypes were upgraded to the new standard, and in 1997 flight testing of the first four full-scale development V-22s began at Pax River. Testing soon fell behind schedule, though a second round of sea trials on USS Saipan was accomplished in 1999.
On 8 April 2000, a night training exercise of four MV-22 in Arizona resulted in one aircraft crashing, killing the 19 Marines on board, and another suffered a hard landing, though no one aboard were killed. The V-22 was grounded again while the crash investigation was conducted, during which issues with the V-22's design, as well as with crew training, were determined to be the causes of the crash. As the V-22 descended to land it was dropping at 2,000 feet a minute, well above the prescribed 800 feet a minute. The speed caused the aircraft to enter an aerodynamic condition known as vortex ring state. In this condition, a vortex envelops the rotor, causing an aircraft to lose lift, in essence descending in its own downwash. Flight testing resumed after the board rendered its conclusions, but another MV-22 crashed in December 2000, killing four Marines. Despite the accidents, by June 2005 the V-22 had completed its final operational evaluation, including long-range deployments, high altitude, desert and shipboard operations. In September of 2005, the Pentagon approved full-rate production of the V-22, ordering 458 aircraft (360 for the USMC, 50 for the USAF, and 48 for the Navy). The USAF officially accepted the CV-22 in 2006, and the MV-22 reaching IOC the following year. Despite being in the 2005 contract, the Navy did not acquire any of the 48 HV-22 mentioned, for reasons unknown (though likely budgetary). Ospreys have since seen deployment to both Iraq and Afghanistan, as well as other hotspots around the world.

-Marines push boxes out the back of a V-22 Osprey aircraft in Zaranj, Afghanistan, on Dec. 14, 2009. | Photo: USMC

-V-22s are fitted with LEDs in the rotors, which create a glowing ring when spinning, allowing the crew, ground personnel and passengers a clear indication of the rotor disc. | Photo: USMC
In 2015, the Navy signed an MOU to buy 44 redesigned CMV-22B Osprey for COD (carrier on-board delivery) beginning in 2018, with initial delivery expected in 2020. The CMV-22 has larger sponsons, which carry additional fuel, as well as a high-frequency radio. The type will also include a hoist on the ramp, allowing it to deliver cargo to other Navy ships, replacing some helicopters.

-A CMV-22B landing at Pax River after being ferried from the Bell Assembly Center in Texas. | Photo: USN
In 2014, the Japanese Self-Defence Force decided to acquire 17 MV-22Bs, with the first delivery occurring in August of 2017. The JSDF Osprey are based at Kisarazu Air Field, with plans to station some on the Izumo-class helicopter destroyers (*cough*aircraftcarriers*cough*).
India, Indonesia, Israel, South Korea and the UAE have expressed varying degrees of interest in acquiring V-22 of their own, though as of 2020 none have formally acted.
In addition to the transport versions currently in service, other variants were studied during development:
An AEW&C version known as the EV-22, which would replace the E-2 in US Navy service as well as the Sea King ASaC.7 in Royal Navy service
SV-22 Anti-submarine warfare variant, to replace the S-3 and SH-2.
Neither was pursued, though Bell/Boeing continue to pursue variants.

-Rendering of an EV-22 AEW variant, showing the new triangular radar pylon. | Image: Jeff Head

-Model of the SV-22. The ASW variant would have been armed with four torpedoes and carried a dipping sonar. | Photo: Justin Gibb
-Model of the SV-22. The proposal didn’t include a MAD boom, but I added one. | Photo: Justin Gibb
In 2017, HMX-1, the Marine helicopter squadron responsible for transporting the President, Vice President and other senior leadership, recieved 12 MV-22B, replacing its fleet of CH-46 helicopters for support operations.

-HMX-1's first MV-22B, in the squadron’s traditional gloss olive drab paint scheme. | Photo: Sgt. Rebekka S. Heite
#aircraft#aviation#avgeek#cold war#airplanes#airplane#cold war history#usaf#coldwar#aviation history#usmc#us Navy#v22#v 22#v22 Osprey#v 22 osprey#bell v22#Bell Boeing v22#cv22#mv22#tilt rotors#tiltrotor#tiltrotors
111 notes
·
View notes
Text
It Started with a Piano

🎶 Hello! Honestly, this may be my most anticipated fic ever. Not because it’s been requested of me a lot, but because I have wanted to write a fic with this song probably since I saw a marauders CMV with it.
Until today, I had no clue how to write this and never thought too hard on it, then suddenly I’m listening to the song and it clicks. Talk about Inspiration. So anyway, enjoy this piece of wolfstar fluff from their Hogwarts years!
If you want to listen along, here’s the link to the song that inspired me to write this. Or you could listen to the piano cover.
The song technically doesn’t start until Remus begins playing the piano but do with that as you will.
Anyways, I hope you enjoy! 🎶
.
When life leaves you high and dry, I'll be at your door tonight. If you need help, if you need help.
I'll shut down the city lights, I'll lie, cheat, I'll beg and bribe. To make you well, to make you well.
Remus opened the doors of the fifth-floor classroom, grateful to find it empty, not that he hadn’t asked Professor Flitwick for permission beforehand. He didn’t know how he would've explained this - given that he wasn’t taking music as an extracurricular.
Avoiding his fellow marauders was easier than he had anticipated, though to be fair, he had already told James and Sirius the plan for their next prank. He had some spare time as they brewed the necessary potion.
Walking towards the piano in the back center of the room, he gently lifted the lid and propped it open before taking a seat at the bench. Running a soft hand over the ivory keys, he thought about the cords that he had put together late last night in the dorms.
Listening to the song over and over until it was ringing in his ears. Humming softly under his breath, he pulled a notebook out of his pack and flipped through the pages.
Taking a breath, Remus began to play the first notes of the instrumental beginning, relaxing as the familiar tune began to fill the air and his strong focus lessened as it neared the first verse.
“When life leaves you high and dry, I'll be at your door tonight, if you need help, if you need help.” He sang aloud, content at this moment to be on his own.
When enemies are at your door, I'll carry you away from war. If you need help, if you need help.
Your hope dangling by a string, I'll share in your suffering. To make you well, to make you well.
Sirius had a song stuck in his head, it echoed throughout the day ever since late last night. He knew it was because of Remus, though he had no idea what that song meant. Remus had him listen to countless muggle songs on his tape player that were his favorites or songs that they had discovered together.
It was fascinating to hear the variety of music that could be created with instruments and recorded, to the point that it became a habit for them within their dorms.
Something seemed strange though, he couldn’t help but muse as James stirred the fluxweed and knotgrass together for their Polyjuice Potion. Why is it that Remus took off after class? The moon wasn’t for another few weeks so he wouldn’t be headed to the hospital wing.
He found himself unconsciously humming the tune again. What was Remus’ reasoning for the song? Wait, he was writing while he was listening. Was that song the reason why he avoided the preparation for today?
His eyes widened slightly at that. Wordlessly, he got up from his chair, grabbing his pack, and headed out the door- ignoring the protesting and curious voices of Prongs and Wormtail that followed.
Give me reasons to believe, that you would do the same for me.
There was no sign of Remus in his usual locations. Not in the library, or the courtyard fountain, by the fire in the Gryffindor common room, or the tree by the Great Lake- actively all the spots where he could be alone and have the Marauders come and find him.
Sirius found himself walking up the grand staircase to the fifth floor, lost in thought about Moony when a soft piano piece seemed to flow through the air from the closed corridor doors. Once again, he thanked the fact that his animagus was a dog. There was no way he’d be able to hear it clearly otherwise.
As he walked down the halls of the corridor, nearing the classroom, the piece grew louder. He recognized it. The song. But, this was different than just hearing the words of the original singer or the instrumental melody.
Remus was singing? Not the quiet hums he was used to hearing, but strong and carefree. His voice was hypnotizing, melodious, and the song seemed effortless to sing. He couldn’t help but smile, Moony always seemed to surprise him.
And I would do it for you, for you. Baby, I'm not moving on, I'll love you long after you're gone.
For you, for you. You will never sleep alone, I'll love you long after you're gone.
And long after you're gone, gone, gone.
“Give me reasons to believe, that you would do the same for me.” Remus sang to himself, faintly hearing the approaching footsteps of someone but it was already too late to stop.
“And I would do it for you, for you. Baby, I'm not moving on, I'll love you long after you're gone.” Another voice joined his own, one that was familiar. That brought a smile to his face, but right now made him only feel embarrassed.
Pausing with a gasp and widened eyes, he quickly turned behind him. Sirius stood at the entrance of the classroom, leaning against the doorframe with a smile upon his face. Most likely filled with zero regrets, meanwhile, Remus could feel his cheeks beginning to flush at the fact that Sirius absolutely heard him.
“Why’d you stop? You just reached the chorus.” Sirius said teasingly.
“Pads what… why are you here?” Remus replied with caution, pulling his hands away from the keys. The ebony-haired boy didn’t respond to him exactly, just pushed off of the doorframe and began making his way over to Remus’ side until he was at the bench and Remus had to look up to meet his eyes.
“Well Moons, I wanted to find you. That, and you’ve gotten that song stuck in my head with your long hours of playing it last night.” He said with a chuckle as Remus’ eyes widened even further if it were possible. “Scoot over.”
Without waiting, Sirius placed his pack down on the floor beside the leather satchel that was already by the bench, then sat down to join his friend. Giving Remus a smile, he looks to the makeshift music sheet within the notebook, putting the melody together.
Remus stared at Sirius for a few seconds, stunned that he wanted to stay. Glancing down to their hands which were quite close together, he could feel the warmth radiating off of the other boy.
He looks up to the notebook, then back to Sirius, watching as his grey-blue eyes scoured over the pages. “... Can you play?” He asked in curiosity.
Sirius looked at the tawny-haired boy beside him and nodded, “Mother dearest had a private teacher give Regulus and I lessons since I was five.”
At the look upon Remus’ face, which frequented whenever he spoke of his previous home life, he shakes his head. “I don’t play too often anymore, but I’ll make an exception for you.” He continued with a wink.
Remus chuckled exasperatedly, with a shake of his head, worry seeming to bypass for the moment. He stared silently at Sirius, watching as pale hands rested upon the ivory keys and began following the scale, then began playing the melody of the chorus.
“You will never sleep alone. I'll love you long after you're gone, and long after you're gone, gone, gone.” Sirius sang softly, and it was Remus’ turn to be surprised. How much of the lyrics has he memorized? Enough he supposes, given that he had apparently forgotten to cast the silencing charm on his bed.
When you fall like a statue, I'm gon' be there to catch you. Put you on your feet, you on your feet.
And if your well is empty, not a thing will prevent me. Tell me what you need, what do you need? “I surrender honestly, you've always done the same for me.” He continued, increasing the tempo of the piece as the chorus nears once again as he looks back to Remus with a smile and encouraging nod. Sing with me. His look said, and honestly, when has he ever said no? Or wanted to?
“So I would do it for you, for you. Baby, I'm not moving on, I'll love you long after you're gone.” They sang in unison, voices melding together in a harmony that seemed rather perfect. Remus carried the melody as a guide as Sirius continued the rhythm.
For you, for you. “You will never sleep alone. I'll love you long after you're gone, and long after you're gone, gone, gone.”
It was as if they were being pulled by a string, Remus found himself ever closer to the warmth that Sirius always provided. With a short pause, Sirius pulled his hands away and pulled Remus ever closer, shifting himself in the process.
You’re my backbone you're my cornerstone. You're my crutch when my legs stop moving.
You're my head start, you're my rugged heart. You're the pulse that I've always needed.
Like a drum, baby, don't stop beating. Like a drum, baby, don't stop beating.
With Sirius now flush behind him, Remus couldn’t help but blush, yet he did not pull away. It was warm and comfortable within his friend’s arms, and he found himself never wanting to leave Sirius’ embrace. He could hear his heart beating in his ears, and felt the fast pace of Sirius’ own heart.
Remus hesitantly reached down, and took hold of Sirius’ hands, intertwining their fingers. Just to see how he’d react. When he didn’t pull away, he sighed in relief and lifted their hands so that they rested together upon the keys.
Turning to look behind him, he saw the soft smile upon Sirius’ face. And he knew. That smile, it was only for him. He found himself mirroring it unconsciously, “Sirius…”
“I know Re,” He said softly, almost in a whisper. “Come on, we’re almost there. Want to sing this?” Remus nodded in reply, and turned back to the keys as he began to play again, Sirius’ hands never leaving his own.
As the song began nearing its end, Remus began to relax leaning back slightly into the warm weight behind him, causing Sirius to chuckle fondly. What the tawny-haired boy didn’t know, was that he had been watching him as he sang with a smile.
Teasing from James be damned, he knew he was in love with Remus. And from the way Remus’ head leaned against his own, intertwined fingers tightening as the tempo began to slow, after placing a kiss upon his flush cheeks, he didn’t doubt that Remus felt the same.
Like a drum, baby, don't stop beating. Like a drum my heart never stops beating for you.
And long after you're gone, gone, gone. I'll love you long after you're gone, gone, gone.
.
Tag List:
@epithymiahua
@whataboutmyfries
@fleetingpieces
@wonder-womans-ex
@heyitssmiller
@spookypotato
#remus lupin#sirius black#remus x sirius#wolfstar#marauders era#lyric fic#song fic#piano#hogwarts#pre first war#sixth year#wolfstar fluff#pining#get together#it started with a piano
70 notes
·
View notes
Text
Penile Enhancement Surgery – The Ultimate Way to Be Confident with Your Sexual Life
What anybody desires in bed is ultimate satisfaction, and that’s achievable through only one thing, confidence. Confidence in bed comes from one’s penile size. Now some may argue that size doesn’t matter, but ultimately it does in giving a man the confidence he needs to please his partner. So many people today suffer a case of low esteem just on account of their small penile size. Thankfully, cosmetic surgery is changing that for good.
Although pills, pumps and exercises have been floated out from time to time in the past as solutions to that, it is penial enhancement surgery Sydney that first brought promises of visible results.
How Does Penile Enhancement Surgery Works?
Now the interesting part, how does such a surgery work? That question has puzzled people since the launch of this procedure. It’s really quite simple. The size of penis is enhanced through implantation of a silicon piece. This medical-grade silicon adds a few cmv fvs to the original size of the penis making it longer and fuller than it normally is. An incision is made through which this piece is introduced and when the cut heals, it becomes a part of the organ. Indistinguishable from the penis, it appears as a part of the same.
Who Need Penile Enhancement Surgeries?
The normal size of a penis is between 5 and 6 inches when erect. Flaccid that shrinks to 4 to 5 inches. So, technically, anybody who is below that mark is a candidate for a penile enhancement surgery. But size is not the only concern in determining the need for this surgery. A lot of other things, mostly psychological comes into play.
Ideally, people suffering from the condition medically referred to as micro penis where the size of the organ is below 3 inches need to consider getting an enhancement surgery done. Thankfully this condition is pretty rare today. One is either born with it, or had a developmental slack due to hormonal irregularities.
The second candidate for a penile enlargement surgery Sydney is someone who is going through a lot of psychological distress on account of their small penis size. So if you lack confidence or find yourself questioning your worth owing to your penis size, then its best corrected before it’s too late. People often go into depression and distance themselves socially due to inferiority complex born out this particular situation. So, if someone is going through a rough phase in life because of this, a penile enlargement surgery can most definitely be a solution.
Is the Result of Such a Surgery Customizable?
The results of a
penile enhancement surgery Sydney
is very much customizable. A surgeon can make your penis exactly as big or small as you’d like. Normally the silicon implant used for the surgery is available in three sizes, namely large, XL and XXL. Every piece adds an inch or two to the organ. So, depending on how much you want to enhance your organ and its current size, the doctor chooses a size that would work best.
1 note
·
View note
Photo

Natural Pharmers CBD Oil Dutchman Anton van Leeuwenhoek (1632-1723) demonstrated the value of these basic research tools by utilizing them to analyze blood cells, spermatozoa and microbes. A build up of live Orgone energy in the human physique lead to optimistic mental and spiritual health and maintained a very good physical body. In abstract, sufferers may expertise some, all or not one of the following symptoms: shortness of breath, chest pain, lightheadedness, irregular heartbeat, sudden loss of consciousness. These embrace the small, on a regular basis decisions that profit our mental and bodily health: going to bed on time to get sufficient sleep, taking our medication, eating nicely, getting fresh air and a little bit of exercise, showering often, seeing other individuals, spending time with animals, and making time for hobbies. Reich contended that Orgone Vitality deficits or constrictions within the human physique were the root of all illnesses and this lead to his now infamous invention known as the Orgone Accumulator. He, his lovely spouse, and their son live the healthy life-style he encourages amongst his patients, friends and family. Recently individuals have claimed that there is empirical proof for the afterlife. USA About Website The main supply for reliable and timely health and medical news and knowledge. After treatment, you have to to see your health care provider frequently to be sure that the pituitary gland is working usually. Pink blood cells are someday simply called red cells. Tinospora cordifolia (300 mg three times daily) - In one research, individuals with allergic rhinitis who took a selected formulation of tinospora (Tinofend) for 8 weeks had many fewer symptoms than those who took placebo. Individuals who have autoimmune illness reminiscent of rheumatoid arthritis or Crohn's disease mustn't take astragalus without asking their physician. Which translation is true, I do not know, however both point out that when bread was to be eaten it ought to be thought-about, at the least symbolically, to be the body of Jesus Christ - similarly with wine and his blood. Name for an appointment with your health care provider when you've got symptoms of acute CMV infection. Human physique is made of enormous number of cells. All doable elements - private, economic, social, political, or environmental - that can probably influence human capabilities which dictate the real properly-being of people, come relevant. MHealth may help bridge gaps in care by permitting sufferers to communicate with their doctor or care staff and vice versa with out meeting head to head. https://www.nutrawins.com/natural-pharmers-cbd-oil/
https://medium.com/@howardoelich/https-www-nutrawins-com-natural-pharmers-cbd-oil-a90a4a83f9fa
https://howardoelich-89.webself.net/
http://www.imfaceplate.com/howardoelich/the-natural-pharmers-cbd-oil
https://twitter.com/howardoelich
http://howardoelich.simplesite.com/
http://howardoelich.bravesites.com/
1 note
·
View note
Photo

Natural Pharmers CBD Oil Dutchman Anton van Leeuwenhoek (1632-1723) demonstrated the value of these elementary research tools through the use of them to analyze blood cells, spermatozoa and microbes. A construct up of reside Orgone energy within the human body lead to constructive mental and religious well being and maintained an excellent bodily physique. In summary, sufferers might expertise some, all or none of the following signs: shortness of breath, chest pain, lightheadedness, irregular heartbeat, sudden lack of consciousness. These embrace the small, on a regular basis choices that profit our psychological and physical well being: going to mattress on time to get sufficient sleep, taking our treatment, consuming nicely, getting contemporary air and a little bit of exercise, showering usually, seeing other people, spending time with animals, and making time for hobbies. Reich contended that Orgone Power deficits or constrictions in the human physique have been the foundation of all diseases and this result in his now notorious invention referred to as the Orgone Accumulator. He, his lovely spouse, and their son reside the healthy life-style he encourages amongst his patients, friends and family. Just lately individuals have claimed that there's empirical proof for the afterlife. USA About Web site The leading supply for trustworthy and timely health and medical information and data. After therapy, you will need to see your health care provider commonly to guantee that the pituitary gland is working usually. Purple blood cells are someday merely called pink cells. Tinospora cordifolia (300 mg 3 times each day) - In a single research, folks with allergic rhinitis who took a particular formulation of tinospora (Tinofend) for eight weeks had many fewer signs than those that took placebo. People who have autoimmune illness reminiscent of rheumatoid arthritis or Crohn's disease shouldn't take astragalus without asking their physician. Which translation is true, I don't know, however both indicate that when bread was to be eaten it must be thought of, at least symbolically, to be the body of Jesus Christ - similarly with wine and his blood. Call for an appointment with your well being care supplier in case you have symptoms of acute CMV infection. Human body is made of large number of cells. All possible elements - personal, economic, social, political, or environmental - that may probably influence human capabilities which dictate the real well-being of individuals, come related. MHealth may also help bridge gaps in care by allowing patients to speak with their doctor or care crew and vice versa without assembly head to head. https://www.nutrawins.com/natural-pharmers-cbd-oil/
1 note
·
View note
Text
Our IUI Journey Begins

Well, that title may be a little misleading. Technically it began back in January when my partner and I visited the fertility clinic. So, I guess I should start there.
January
Our first visit to the fertility clinic was nerve-racking to begin with. Technically, my partner and I do not suffer from infertility. We are just an average lesbian couple that want to conceive. SO anyways, the first visit. I’m not a huge fan of needles, so majority of my anxiety came from the fact that I knew that I would be getting stuck and boy did my anxiety live up to its expectations. I had to get some routine labs drawn as far as hormones , a1c, TSH etc. I also agreed for genetic testing as well. I’m a pretty hard person to get blood from. 1: I have tiny veins that roll, so usually a butterfly needle is used. 2: No matter how much I pump my hand and drink tons of water, my veins are not easy to find. 3: I go to pass out....which is exactly what happened this time.
Once we got pass the excitement of me going to pass out, I then had to get a transvaginal ultrasound. It’s basically to see how everything is looking inside. This is the scan that showed me that I could potentially have PCOS. On one of my ovaries, it looked like a string of pearls. Which is usually an abnormal accumulation of immature follicles. Of course, fancy ovaries.
We met with the Dr and he explained everything. I don’t typically fall into the PCOS category because I have regular periods.nI do not have unwanted hair growth. I do however have fancy pearls on my ovaries, have sugar resistance (high A1c) and a weight problem which no matter how much I stay active, it does not seem to matter. The Dr said he did not see this as a problem, but suggested a low carb diet , some more blood work and also said I would probably be put on Clomid when we decided to begin the whole process. We then left we our check list of things to do before we could begin.
February
One of the things on the checklist was to meet with a counselor to make sure we were ready to go on this journey together and to also give us some helpful information. The 2nd was to get some more blood work which included STD testing, blood type, RH and CMV. This was definitely not a good time, but that's only because of my fear of needles. My want of having a baby was much stronger, so I sucked it up and got it done.



I did get put on Metformin 500mg extended release three times a day. My A1c has been at a 6.2 for the past few years now, so they felt that this was necessary. I also had my Vit D dosage increased and was put on Synthroid because my TSH was a 5.5 which is high.
My STD testing came back fine. I already knew my blood type. I had thought that I was CMV positive because majority of the adult population have been exposed to that, but I was one of the few that has not. I have CMV negative which means that I do not have the antibodies and resistance to the virus. It not a big deal if you have a healthy immune system and you get the “Cytomegalovirus” but when you are trying to get pregnant and are going to use a sperm donor, it is pretty important. When you are CMV negative, it is important to also find a donor who is CMV negative. This helps to reduce the risk of infection to the unborn child. This also meant that we had to pick a new donor. My partner and I had already picked out two potential donors on an online sperm bank site, but they were CMV positive. Of course, since majority of the adult population has been exposed to CMV, the results for CMV negative donors is a much shorter list, especially when you add in different filters (height, eye color, hair color etc). We did find one that we really liked and decided to go with him.
Along with the labs I had done, it showed that I was not immune to MMR. which is crazy because I have had all of my immunizations done when I was a child, I even have all the old paperwork to show. So I was required to get the shot again and then we would have to wait 30 days to even begin trying IUI.
March
We had all of our stuff completed on our checklist, my MMR 30 days was set to be clear the 2nd week of March. We were feeling really on top of everything and excited. Then COVID happened and everything had to be put on hold. Along with all other non essential businesses, the fertility clinic had to close. It was deemed a want not an essential.
April
.........................................
May
Fertility clinic is open
And so it begins................
1 note
·
View note