#quadriplegia problems
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text
Honestly I'm pretty lucky¹ in that this doesn't happen to me too often but the next time some asshole asks why I still live with my family even though I'm an 'Adult' with a 'Job' or whatever I am going to staple the 100k USD² quote for my new wheelchair accessible vehicle³ to their forehead. Being disabled is so fucking expensive.
¹ for the value of lucky where you know, people only microaggress on you once in a while vs all the time
² no I'm not joking
³ no it's not a passenger van or like a bus. It's a modified Chevy Traverse. You know, those kind of cars that are like 35k USD⁴ off the lot brand new
⁴ for another fun trivia fact if insurance hadn't covered my wheelchair this is also the bill I would have got in the mail for that
#But the good news I'm finally in the process of getting a new car!#And insurance did end up totalling my last van after The Accident last month#So I won't be on the hook for all 100k. Thank god#disability#ableism#filing this under#quadriplegia problems#el problema es el capitalismo#why footnotes you may ask. because i think they're funny#i'm back on my bullshit
6 notes
·
View notes
Note
Hello ! I have gone through your archives lately and I'm pretty sure that this question has not been answered but in case you already did, I'm sorry. So I want to write a fic about the series Warrior Nun, in which the main character is originally quadriplegic, but because of a magic halo, she is not for the rest of the show. I want to keep her disability as part of her character but I was wondering if it would be a problem if I wrote her as paraplegic instead of quadriplegic ?
Hi!
I will say upfront that I'm not familiar with the series, so I might be missing some context, but I think it's great that you're undoing the magical cure that she got!
The question is, why do you want her to be paraplegic over quadriplegic? That's kind of the whole thing here. Why? Before you answer, make sure you understand how quadriplegia actually works (I… wouldn't trust the original book's portrayal, based on the cure thing?). The "100% paralyzed below the neck" can be a type of it, but the vast majority isn't like that; it depends on the level and completeness. Quadriplegia means that there is paralysis present in all four limbs, not that every single muscle is fully paralyzed.
If it's because you're worried that if she's quadriplegic she won't be able to do XYZ, make sure that it's a correct assumption. People with quadriplegia can learn to drive, play video games, compete in very high-impact sports, whatever. There's a ton of adaptive technology out here!
We don't have any quadriplegic mods, so it's hard for me to give you any specific advice other than "research" and "ask why". If you want to see how a quadriplegic person can do stuff, I recommend you check out Mason Ellis' YouTube channel, and/or watch the documentary Murderball - it's about quad rugby and a lot more :)
I hope this helps!
mod Sasza
41 notes
·
View notes
Text
All right, everyone! This is the fourth SCI awareness post of this month! So buckle up! Figuratively and literally!
You've probably read that beginning entry and probably thought oh God, she's going on about something that is really weird.. and you're absolutely right!
To give everyone a basic/general idea of a spinal cord injury I'll break it down like this a spinal cord injury is when your spinal cord gets injured/severed or completely damaged from a fall, motor vehicle accident, or a diving-related injury the most common injury's to get in car accidents are paraplegic and the most often injury to get in a diving related accident is a Quadriplegic injury!
You've probably read that and thought, “Uhh, I have no idea what you just said?” Well, I'll break it down a Paraplegic is someone who had an injury in the thoracic region of the spin or the lumbar even the sacral the spinal cord contains 33 vertebrae in itself and the thoracic region controls most of your core and your legs and a paraplegic is defined as someone who can move the arms and fingers but have no use of core or legs depending on the level or completeness of there injury! Every paraplegic is different and cannot be defined as just not walking. However, Quadriplegics also range from a different spectrum.
Quadriplegia or Tetraplegic can be defined as someone who has little use of their four limbs or complete paralysis of all four limbs. You can become a Quadriplegic from different types of disorders/conditions. It does not relate only to spinal cord injuries.
However, a Quadriplegic can also be very different from ANOTHER Quadriplegic! Not every Quadriplegic has no use of their arms, let me explain.
My wife and I are both Quadriplegics relating to different vertebrae in the neck, but I have some of the same injuries as my wife. I am a C3 incomplete & a C4-C5-T1-T10 Quadriplegic ♿ my wife, however, is a C4-C5-C6-T1 Incomplete Quadriplegic. She can move her arm and she can pick up things! Which Is something I can not do! This goes to show that everyone's spinal cord injury is different!
But One thing that is common in the SCI community is the inability to go to the bathroom! You might be thinking? Doc I thought being paralyzed means you can't walk!? That's what is typically shown in the media! Of course, I would be lying to you if I said that was the only issue we paralyzed people experience. In fact, I wish that was the only issue! Think of it like this. When you see an iceberg you would normally think that the tip is the worst we've got! But underwater there is a much deeper meaning and more problems than you realize. One of those issues is the inability to go to the bathroom. The reason for this is that when you get a spinal cord injury, it affects everything below, but it also affects your bladder and bowels, which is way worse than you think! Most of the time, you might think oh, y'all just get backed up, or y'all will eventually pee! But that's not the case! See we cannot choose when to go to the bathroom! And how we relieve ourselves might look different to most people. We use a catheter, which is a tube that makes its way up to the urethra and releases urine from our bladder! This is a lifesaving type of equipment for us! When we ignore this, we can get a UTI, which is not good for anyone! Another thing that involves more medical equipment is going number 2 or poop.
For me, in my case, I have no core! As you might think, my precious tush and a rickety surface are not a good combo! So I use a strap! And a backrest! To not make my rather T-Rex-shaped body fall and hit the ground as I slowly perish.. dark, ok. But it is essential that us disabled people have the vital medical equipment we need! To help us live fulfilling lives! This goes to show that living with a spinal cord injury can affect Many different people in many different ways!
But this concludes the Fourth SCI awareness post of this month! Thank you all for reading, and stay positive, my SCI friends 🙌❤️!
Img desc #1: doc is seen sitting on the toilet. Doc's body is seen getting held by a lifesaving blue strap, and the backrest. Around her head is a yellow pool floaty to help keep her head upright! Beside her is a white bathtub with a blue shower chair. Doc is wearing a black short-sleeved shirt and beige-colored sweatpants. Doc is giving a wide smile to the camera as her Atrophied arms rest in her lap.
Img Desc #2: doc's supportive chest strap is seen on the toilet. The white backrest is seen attached to the toilet with two white bars and a blue chest strap buckled up ready to use for her next bowel program!
Img desc #3: shows doc giving a wide expression with her mouth closed. She is seen with her hands in her lap wearing a grey short-sleeved shirt and blue jeans. There is text seen on the right side of her saying "13 A DAY" with the emphasis that's that a lot of catheters! It shows a blue wheelchair emoji under that text on the left side of the image, which shows a catheter with a bag on the end of that shadowed red. The image is enhanced with filters to give it a more dramatic look!



2 notes
·
View notes
Text
We often feel insecure about our semi-verbality because there are some scenarios in which we very much enjoy talking. The worry gets in our head and sticks there – if talking is hard for us, why do we enjoy doing it? Why do we seek it out? Why do we sit and chat with people if it's so difficult for us?
... But that's silly, isn't it? Plenty of people like doing things that their disability makes difficult!
There are people with joint problems that like to crochet. There are people with quadriplegia that like to paint. There are people with intellectual disabilities that like to learn. There are people with hearing impairments that like to listen to music, and there are people with visual impairments that like to watch movies. And so, so many more.
We still like to help out around the house even when our chronic pain means we can barely turn or bend over. Why shouldn't we like to talk even though our semi-verbality means it can be a struggle to do so?
Enjoyment of an activity that your disability makes difficult doesn't mean you don't have that disability. It just means you've weighed the difficulty of the activity and the side-effects performing it might cause you against the joy performing the activity would grant you, and you've decided that sometimes, you'd like to have some fun regardless of what it takes to get it. Considering how often abled people will do the same thing, undertaking something regardless of how difficult it is to achieve, I don't think it's all that unusual for the same to be said for disabled folks.
So, don't doubt yourself just because you like doing something your disability makes difficult, okay? Go out and have a great day
8 notes
·
View notes
Text
Most Valuable Technologies (Final Earth)
What might the most valuable technologies be in a hypothetical situation in which Remnant gets a portal to Earth?
Let’s take a look.
Power generation. Remnant has unlocked fusion and anti-matter reactors for power generation. Diana uses a closet-sized fusion reactor in her underground research bunker, for crying out loud. This technology would probably be the number one priority for Earth since it solves so many problems. Safe, cheap, plentiful energy is also a political excalibur. If you can deliver this to the electorate, you’re going to win a lot of elections.
Battery technology. The power cells that can be found in many forms of technology (e.g., cars, scrolls, etc.) are orders of magnitude better than anything Earth has. If you can get your hands on basically limitless energy (see the earlier point about power generation), better battery technology is the logical next step.
Gravity manipulation technology. This would revolutionise transport and logistics. Transportation of cargo immediately because vastly cheaper, as does travel for the general public. This also unlocks a whole host of options for space travel and air travel in general.
Medical technology. Nano-machine serums, reproductive science, and all sorts of other goodies are on offer here. Cancer? Cured. Viruses? Slaughtered by nano-machines. Paraplegia and quadriplegia? Gone. This is another excellent vote winner too.
Weapons technology. Yeah, people will be wanting this too. Remnant has been at war with the Grimm for basically forever. They’ve got forcefields, missile defence systems, mechs, the whole works. Heck, Ruby has an alternate weapon (Thunder Rose) that is a scythe that turns into a functional rail gun. People have built actual death rays.
If I was a politician, I’d focus on getting access to power generation technology. A fusion or anti-matter reactor would immediately reduce the cost of energy to a fraction of its present cost. Putting money back into people’s pockets is one of the best ways to get re-elected.
Furthermore, access to vast quantities of cheap electricity will have a huge impact on industry. Think of how much electricity is consumed by manufacturers across all industries. Now imagine how much more money they’d be able to make if their power bills were basically zero. Your domestic industries would be able to cut the cost of production and pass savings on to consumers while expanding their profit margins. International companies will relocate to take advantage of the cheaper energy costs.
More companies moving in means more employment, means more money, means more votes. There are a lot of other technologies you could use as well if power generation ceases to be an issue.
5 notes
·
View notes
Text
Choosing the Right Paralysis Treatment in Mumbai for Your Loved Ones
Introduction
Paralysis can be difficult for both the patient and their families. Finding the appropriate therapy in Mumbai, a city famed for its sophisticated medical facilities, can make a big difference in recovery and quality of life. This guide will walk you through the necessary procedures to select the finest paralysis therapy for your loved ones in Mumbai, ensuring they receive the best possible care.

Understanding Paralysis and Its Types
Paralysis is defined as the lack of muscular function in a specific region of the body. It may be partial or total, temporary or permanent. Understanding the sort of paralysis that your loved one has is critical. Standard forms are:
Paraplegia (paralysis of the lower half of the body).
Quadriplegia (paralysis of all four limbs).
Hemiplegia.
The first step in seeking suitable treatment is to obtain an accurate diagnosis and understand the problem's intricacies.
Exploring Treatment Options
Mumbai provides a wide range of paralysis treatment options, including traditional remedies and modern medical procedures. Physiotherapy is an essential component of paralysis treatment, helping patients regain strength and mobility. Occupational therapy helps to improve everyday living skills, whereas speech therapy helps people who have difficulty communicating. Advanced treatments such as stem cell therapy and robotic rehabilitation are also accessible in Mumbai, offering novel options to paralysis patients.
Factors to Consider When Choosing a Treatment Facility
Selecting the correct treatment facility is crucial for effective paralysis management. Consider the following factors:
Expertise and Experience: Ensure the facility has experienced neurologists, physiotherapists, and other specialists who are well-versed in paralysis treatment.
Reputation and Reviews: Research the facility's reputation. Read reviews and testimonials from other patients and their families to gauge the quality of care.
Comprehensive Care: Look for facilities that offer a multidisciplinary approach, including physiotherapy, occupational therapy, speech therapy, and advanced treatments.
Accessibility: Choose a facility that is easily accessible for regular visits and emergencies.
Evaluating the Care Team
The quality of the care team is critical in paralysis treatment. A trained and empathetic team can significantly improve the patient's recovery. Assess the qualifications and experience of the doctors, therapists, and support workers. It's also critical to ensure that the team communicates well and keeps you updated on your loved one's status and treatment plan.
Importance of Customized Treatment Plans
Each person living with paralysis is unique, and their treatment strategy should reflect this. Customized therapy regimens that address the individual's specific requirements and goals are more effective. Please discuss with the care team how they intend to adjust the treatment to the exact type and severity of paralysis. A personalized strategy boosts the patient's chances of a successful recovery while also improving their quality of life.
The Role of Advanced Technologies
Advanced technology plays an essential part in current paralysis treatment. In Mumbai, various facilities are outfitted with cutting-edge technology, such as robotic exoskeletons, virtual reality therapy, and modern neurorehabilitation equipment. These technologies can significantly improve the efficacy of existing medicines, resulting in better outcomes for patients. When selecting a treatment facility, enquire about the availability and utilization of sophisticated technologies.
Financial Considerations and Insurance
Paralysis therapy can be costly; therefore, it's necessary to examine its financial implications. Determine whether the treatment facility takes your health insurance and what fees are covered. Understanding the financial ramifications upfront might help you plan more effectively and avoid unforeseen expenses. In addition, certain facilities may provide payment plans or financial aid programs to families in need.
Emotional and Psychological Support
Paralysis affects both the body and the intellect. Emotional and psychological support are essential components of comprehensive paralysis treatment. Many clinics in Mumbai provide counseling and support groups for patients and their families. Providing enough emotional support to your loved one can improve their general well-being and help them recover.
Home Care and Rehabilitation
Post-treatment care is equally vital in the recovery process. Some patients may require home care and continuous therapy after leaving the treatment facility. Ensure that the facility has a solid post-treatment plan in place and offers home care support. This could involve regular follow-up visits, home physiotherapy sessions, and access to medical equipment required for healing at home.
Visiting and Evaluating Treatment Centers
Before making a decision, visit and analyze several treatment facilities in Mumbai. Observing the facilities, meeting the care team, and getting a personal feel for the setting will help you make an informed decision. Pay close attention to the cleanliness, infrastructure, and overall vibe of the center. A cheerful and supportive environment can have a substantial impact on the patient's rehabilitation process.
Conclusion
Choosing the best paralysis treatment in Mumbai for your loved ones requires careful consideration of several variables, including the care team's competence, the availability of innovative technologies, and the quality of emotional and psychological support. By thoroughly researching and assessing potential treatment facilities, you can guarantee that your loved one receives the best care available, tailored to their specific requirements. The right decision can make a significant impact on their recovery and overall quality of life.
The Banyan Tree International Geriatric Care Center, where compassion meets expertise in elderly care. Our center is a haven for seniors who are cherished and provided with top-tier care. Paralysis Care Services in Mumbai focuses on addressing senior citizens' unique social and personal needs who seek assistance with their daily activities and healthcare while preserving their dignity. Our comprehensive approach includes specialized physical, occupational, and speech therapy to accommodate paralysis and enhance functional abilities. We also offer a range of adaptive and assistive devices to improve overall quality of life.
0 notes
Text
Ayurvedic Treatment for Paralysis
https://starayurveda.com/ayurvedic-treatment-for-paralysis.php

Sudden weakness and numbness of half of the body,difficulty in speaking or hearing, nausea or vomiting, hazy or loss of vision in one eye,intolerable headache, imbalance and sudden fall, drowsiness, dizziness are the alarming symptoms to paralysis which may last for few hours to very few minutes and will disappear soon. Even if the symptoms fade off soon, seek medical help quickly, as it may lead to complete paralysis. Paralysis is the loss of muscle movements and coordination in some parts of the body or half of the body (right or left). Sudden reduction in blood circulation to a portion of brain tissue ends up in loss of brain function. Reduced blood supply may be due to either hemorrhage (rupture of the blood vessel) or due to clotting of blood in blood vessels. Accidents and people with high blood pressure and hypertension disorders can all cause paralysis. Blood vessel strokes are thought to be the most common cause of paralysis. So, in order to remove the Vata Dosha from the body, Star Ayurveda therapy Hospital offers a particular ayurveda treatment for paralysis in which everything from lifestyle to diet is handled by Ayurveda professionals. At any point in your life, paralysis can infect any part of your body. However, if you have it, you will most likely not feel any pain in the affected locations. Our treatment strategy and outlook for the illness will be determined by the underlying cause of paralysis as well as the patient's symptoms. Our ayurveda doctors for paralysis in Hyderabad will help you preserve your health and quality of life by using ayurvedic drugs for paralysis and therapeutic treatments. Ayurvedic term for paralysis is Pakshavata or ekanga vata. Any movement in the body including the nerve impulse is due to vata. Obstruction to such vata leads to this disease.
Depending on the affected body parts, its nomenclature differs−
Involvement of only one side − hemiplegia
Paralysis of the arms and legs − quadriplegia.
Paralysis of the lower half of the body including both legs− paraplegia.
Paralysis of facial muscle – bell’s palsy (ardhitha vata)
Spondylosis, hypertension, diabetes, smoking, alcohol intake, tumors in brain, trauma, heart disease is the most common causes and high risk factors to paralysis.
Complete symptoms are− weakness or unable to walk, loss of sensation of the affected body part, unable to hold any objects, loss of speech and difficulty in swallowing food or liquids due to paralysis of facial muscles, coordination problems.. Etc,.
Apart from all these symptoms, unused part of the body (viz., limbs) will end up in loss of strength, size and flexibility of the muscle which is called muscle wasting in medical terms. This condition is called atrophy. Hence, patients affected by this disease should always attempt to do some physical activity.
Patience and assurance is the first line of treatment, which plays a major role in speedy recovery. Early intervention of the ayurveda treatment gives maximum result. Apart from other treatment modalities, undoubtedly ayurveda stands first for the best possible recovery in paralytic condition. Fortunately, muscle and brain functions can be regenerated by panchakarma programs and rehabilitator measures.
Unique treatment like abhyangam and spastics shali panda swedham helps to bring back the strength and energy to the affected limb.
Special local regimens like shirodhara, shiro−vasti, nasyam will bring back the strength and neuro−muscular function. They even clear the channels by expelling the toxins and clear the blockage causing mood−swings and depression in patients. Mood changes are due to damage of the brain tissue, which cannot be controlled by the person.
As abnormal movement of vata is the main factor to this disease, basti is the best panchakarma treatment to bring back the movement of vata to normalcy. Internal medication like tablets, lehyams, kashayams are to be taken for several months for further improvement.
Along with the medication, at−most support from the family members and strong will power of the patient is of prime importance. Following the diet instructed by the ayurveda doctor and practicing yoga and meditation will further improve the state of the person.
0 notes
Note
I am a nondisabled who is trying to write a character with quadriplegia. I have seen people with quadriplegia calling themselves "quad". Is it okay if my characters call themself and their friends as such? Is it typical? How about them calling themself "disabled" and "quadriplegic" aka not person first language but it's only them who call themself as such (so no ablebodied character call them as such)? Thank you in advance.
Hey there!
This is a great question, actually, and makes me want to write a lil writing guide about terminology - thank you for that! It's been a while since I had a good idea for one of those.
Short answer: All of that sounds good to me!
Long answer: I see you're familiar with person-first language, but have you heard of identity-first language? That's where you use an identify feature to describe a person, like describing someone as a Christian man, a Black woman, or even a young person. Some disabled people prefer identity-first language. If that's what your character prefers, there's nothing offensive about them or others referring to the character as disabled person. (There is nothing offensive about the word disabled in any context, though some people do prefer "person with disabilities.")
As for quadriplegic and quad - the first is a medical diagnosis, so would not be considered offensive. Referring to someone as a quadriplegic rather than a quadriplegic person is, perhaps, pushing it a bit farther, but I have seen no indications online, or in the communities that I'm part of, that indicates this is offensive or wrong. If anyone has alternative experience, please jump in!
Finally, the word quad - I haven't heard of it being offensive (please correct me if I'm wrong), and actually have heard it in the context of The Rolling Quads, a disability rights group active at Berkley in the 60s. To sum up: I think you can absolutely use disabled, quadriplegic, and quad to describe your character, and honestly, I don't see a problem with nondisabled characters using this terminology either. As always, happy writing!
0 notes
Text
Spinal Cord Injury: What You Need to Know

Did you know that a spinal cord injury can have life-altering consequences? Whether caused by a traumatic accident or a medical condition, damage to the spinal cord can result in a range of physical and neurological impairments. This type of injury can affect people of all ages, from children to the elderly, and can have a significant impact on their daily lives.
In this article, we will explore the various aspects of spinal cord injuries, including the causes, symptoms, and treatment options available. We will also discuss the importance of early intervention and rehabilitation in improving outcomes for individuals with spinal cord injuries.
Understanding the intricacies of spinal cord injuries is vital not only for those directly affected but also for their families and caregivers. By providing comprehensive information on this topic, we aim to empower individuals to make informed decisions about their healthcare and offer support to those who may be facing the challenges associated with a spinal cord injury.
Join us as we delve into the world of spinal cord injuries and shed light on this complex and life-altering condition.
Understanding spinal cord injury
The spinal cord is a crucial component of the central nervous system, responsible for transmitting messages between the brain and the rest of the body. When the spinal cord is injured, these messages can be disrupted, leading to a range of impairments. Spinal cord injuries can be categorized as either complete or incomplete, depending on the extent of damage to the cord.
In complete spinal cord injuries, there is a total loss of motor and sensory function below the level of injury. This means that individuals with complete injuries may experience paralysis and loss of sensation in their limbs, trunk, and pelvic organs. In contrast, incomplete spinal cord injuries result in varying degrees of motor and sensory impairment, with some function remaining below the level of injury.
The severity and specific symptoms of a spinal cord injury depend on the location and extent of the damage. Injuries higher up in the spinal cord, such as those in the cervical region (neck), can result in quadriplegia, affecting both the arms and legs. Injuries lower down, such as those in the thoracic or lumbar regions (chest and lower back), may result in paraplegia, affecting only the legs.
It's important to note that spinal cord injuries can also lead to secondary complications, including respiratory problems, pressure sores, muscle spasms, and urinary and bowel dysfunction. These complications can significantly impact the overall well-being and quality of life of individuals with spinal cord injuries.
Causes and risk factors of spinal cord injury
Spinal cord injuries can occur as a result of various causes, including traumatic accidents and medical conditions. The leading cause of spinal cord injury is traumatic events, such as motor vehicle accidents, falls, and sports-related injuries. These accidents often involve sudden and forceful impacts that can damage the spinal cord.
Certain risk factors may increase the likelihood of sustaining a spinal cord injury. Men are more prone to spinal cord injuries than women, and young adults between the ages of 16 and 30 are at the highest risk. Engaging in high-risk activities, such as extreme sports or reckless behavior, can also increase the chances of a spinal cord injury.
Medical conditions, such as tumors, infections, and degenerative diseases, can also lead to spinal cord injuries. These non-traumatic spinal cord injuries may result from the compression or damage to the spinal cord caused by these underlying conditions.
Understanding the causes and risk factors of spinal cord injuries is crucial for raising awareness and promoting prevention strategies. By implementing safety measures and educating individuals about the potential risks, we can work towards reducing the incidence of spinal cord injuries.
Types and classifications of spinal cord injury
Spinal cord injuries can be classified based on their location and severity. The location of the injury refers to the specific section of the spinal cord affected, while the severity indicates the extent of damage and resulting impairments.
The spinal cord is divided into four regions: cervical, thoracic, lumbar, and sacral. Injuries to each region can result in different functional impairments. For example, injuries to the cervical region can affect the arms, legs, and pelvic organs, while injuries to the lumbar region primarily impact the legs.
In terms of severity, spinal cord injuries can be classified as complete or incomplete. Complete injuries involve a total loss of motor and sensory function below the level of injury. In contrast, incomplete injuries result in varying degrees of impairment, with some motor and sensory function remaining intact.
Within the classification of incomplete spinal cord injuries, there are further subcategories, including anterior cord syndrome, central cord syndrome, and Brown-Séquard syndrome. These classifications are based on the specific areas of the spinal cord that are affected and the resulting impairments.
Understanding the types and classifications of spinal cord injuries can help us and individuals affected by these injuries develop appropriate treatment plans and set realistic expectations for recovery.
Symptoms and signs of spinal cord injury
Spinal cord injuries can manifest through a variety of symptoms and signs, many of which are related to impaired motor and sensory function. The specific symptoms experienced by individuals with spinal cord injuries depend on the location and severity of the injury.
Common symptoms of spinal cord injury include paralysis or weakness in the limbs, loss of sensation, difficulty breathing or coughing, problems with balance and coordination, and changes in bowel and bladder function. Additionally, individuals may experience pain, numbness, or tingling sensations in the areas affected by the injury.
It's important to note that symptoms can vary significantly from person to person, and the full extent of the injury may not be immediately apparent. Some symptoms, such as difficulty breathing or loss of bladder control, may develop gradually following the initial injury.
Recognizing the symptoms and signs of spinal cord injury is crucial for early detection and intervention. Prompt medical attention can help prevent further damage and increase the chances of a successful recovery. If you suspect a spinal cord injury, it is essential to seek immediate medical assistance.
Diagnosing spinal cord injury
Diagnosing a spinal cord injury involves a thorough evaluation of the individual's medical history, physical examination, and diagnostic tests. The primary goal is to determine the location, severity, and extent of the injury to develop an appropriate treatment plan.
During the physical examination, healthcare professionals will assess the individual's neurological function, including motor strength, sensation, and reflexes. Imaging tests, such as X-rays, computed tomography (CT) scans, or magnetic resonance imaging (MRI), may be performed to visualize the spinal cord and identify any abnormalities or damage.
In some cases, additional tests, such as electromyography (EMG) or nerve conduction studies, may be conducted to evaluate nerve function and assess the extent of nerve damage.
Diagnosing a spinal cord injury requires the expertise of healthcare professionals, including neurologists, orthopedic surgeons, and radiologists. Their collective knowledge and diagnostic tools enable accurate assessment and the development of tailored treatment plans.
Treatment options for spinal cord injury
The treatment of spinal cord injuries aims to stabilize the injury, prevent further damage, and promote recovery. The specific treatment options depend on the location, severity, and extent of the injury, as well as the individual's overall health and preferences.
In cases of traumatic spinal cord injuries, immediate medical intervention is crucial. This may involve immobilizing the spine, stabilizing fractures or dislocations, and relieving pressure on the spinal cord through surgery. The primary goal of surgical intervention is to restore alignment and reduce compression of the spinal cord or nerves.
Following the initial stabilization, individuals with spinal cord injuries may require ongoing medical management and rehabilitation. This may involve a multidisciplinary approach, including physical therapy, occupational therapy, and psychological support.
Medications, such as corticosteroids, may be prescribed to reduce inflammation and swelling around the injured area. Additionally, individuals may benefit from assistive devices, such as wheelchairs, braces, or mobility aids, to enhance mobility and independence.
Experimental treatments, such as stem cell therapy or electrical stimulation, are also being explored as potential options for spinal cord injury treatment. These therapies aim to promote nerve regeneration and improve functional outcomes.
Ultimately, the treatment of spinal cord injuries requires a comprehensive and personalized approach to address the unique needs and challenges faced by individuals with these injuries.
Rehabilitation and recovery after spinal cord injury
Rehabilitation plays a crucial role in the recovery and management of individuals with spinal cord injuries. The goal of rehabilitation is to maximize independence, improve functional abilities, and enhance overall quality of life.
Rehabilitation programs for spinal cord injuries are typically tailored to the individual's specific needs and may involve various therapies, including physical therapy, occupational therapy, and speech therapy. These therapies focus on improving mobility, strength, coordination, and communication skills.
In addition to physical rehabilitation, individuals with spinal cord injuries may also benefit from psychological support and counseling. Coping with the challenges and changes associated with a spinal cord injury can be emotionally and mentally taxing, and having access to mental health professionals can provide much-needed support.
Recovery after a spinal cord injury is a long and often lifelong process. The extent of recovery varies from person to person, depending on factors such as the severity of the injury, the individual's overall health, and the level of support and resources available.
It's important to note that recovery is not limited to physical improvements. Rehabilitation also focuses on emotional well-being, social integration, and the development of adaptive strategies to navigate the challenges of daily life.
Assistive devices and technologies for spinal cord injury patients
Assistive devices and technologies play a vital role in enhancing the independence and quality of life of individuals with spinal cord injuries. These devices are designed to compensate for lost or impaired function and enable individuals to perform daily activities and participate in society.
Wheelchairs are perhaps the most well-known assistive device for individuals with spinal cord injuries. There are various types of wheelchairs available, ranging from manually operated to power-driven. These devices provide mobility and enable individuals to navigate their environment with greater ease.
In addition to wheelchairs, individuals may benefit from other assistive devices, such as orthoses or braces, which provide support and stability to weakened or paralyzed limbs. These devices can help improve mobility and prevent further complications, such as joint contractures or deformities.
Advancements in technology have also led to the development of innovative assistive devices for individuals with spinal cord injuries. Exoskeletons, for example, are wearable robotic devices that enable individuals to stand and walk. These devices utilize sensors and motors to mimic natural human movement.
Other technologies, such as functional electrical stimulation (FES), use electrical currents to stimulate paralyzed muscles and restore movement. FES can be used in combination with assistive devices or as a stand-alone therapy, depending on the individual's specific needs and goals.
Assistive devices and technologies continue to evolve, offering new possibilities for individuals with spinal cord injuries to regain independence and participate in activities they may have thought impossible.
Coping with life after spinal cord injury
Adjusting to life after a spinal cord injury can be challenging, both for individuals directly affected and their families and caregivers. The physical, emotional, and social changes associated with these injuries require ongoing support and adaptation.
Coping strategies and resources can play a significant role in helping individuals with spinal cord injuries navigate the challenges they face. Peer support groups, counseling services, and educational programs can provide valuable information, encouragement, and a sense of community.
Maintaining a positive mindset and focusing on achievable goals can also contribute to emotional well-being and overall satisfaction with life. Setting realistic expectations and celebrating small victories can help individuals stay motivated and maintain a sense of purpose.
Additionally, it's important for individuals with spinal cord injuries to prioritize self-care and maintain a healthy lifestyle. This includes proper nutrition, regular exercise within the constraints of their abilities, and adequate rest and relaxation.
Family and caregiver support is crucial in the recovery and adaptation process. Providing emotional support, assisting with daily activities, and advocating for the individual's needs can make a significant difference in their well-being and quality of life.
Prevention and safety measures for spinal cord injury
Preventing spinal cord injuries is a crucial aspect of promoting overall health and well-being. While it may not be possible to prevent all spinal cord injuries, there are various safety measures that individuals can take to minimize the risk.
Wearing seat belts while driving or riding in a vehicle, using appropriate safety gear during sports or recreational activities, and practicing safe behaviors, such as not diving into shallow water, can significantly reduce the risk of sustaining a spinal cord injury.
Educating individuals about the potential risks and providing guidelines for safe practices is essential. This includes teaching children about playground safety, promoting safe driving habits, and raising awareness about the risks associated with alcohol and drug use.
Creating an environment that is accessible and safe for individuals with spinal cord injuries is also crucial. This may involve modifying homes, workplaces, and public spaces to accommodate individuals with mobility impairments and implementing safety features, such as grab bars and non-slip surfaces.
By prioritizing prevention and safety measures, we can work towards reducing the incidence of spinal cord injuries and creating a safer and more inclusive society for all individuals.
In conclusion, spinal cord injuries can have life-altering consequences, affecting individuals of all ages and impacting their physical and neurological function. Understanding the causes, symptoms, and treatment options for spinal cord injuries is crucial for individuals directly affected, as well as their families and caregivers.
Through early intervention, rehabilitation, and the use of assistive devices and technologies, individuals with spinal cord injuries can regain independence and improve their overall quality of life. Coping strategies, peer support, and access to resources also play a significant role in helping individuals adjust to life after a spinal cord injury.
By prioritizing prevention and safety measures, we can work towards reducing the incidence of spinal cord injuries and creating a society that is inclusive and supportive of individuals with these complex and life-altering conditions.
Other Related Links:
Best Neurologist in Jaipur
Neurologist in Jaipur
Top Neurologist in Jaipur
Neurologist Doctor in Jaipur
Epileptic Seizures Treatment in Jaipur
#best neurologist doctor#epileptic seizures#health#neurologist in jaipur#top neurologist in jaipur#best migraine treatment in jaipur#best neurologist in jaipur#back pain#best doctor#hospital
0 notes
Text
What Are the Home Physiotherapy Services Covered by Ndis?
You may be wondering if your NDIS plan covers home physiotherapy service in Sydney. Well, in short, it does. Your NDIS plan covers physiotherapy care under both “Improved Living” and “Capacity Building” sections. If you opt for NDIS registered Physio in Sydney, who will come to your home to cater to your specific physiotherapy needs, the plan will cover those expenses as well. But what specific services can you expect? Scroll on!

Under the Capacity Building section, you can expect the following services:
Preventive awareness for falls
Group exercises
Dry needling therapies
One-to-one consultations
Personal hygiene and complex care
Who needs home physiotherapy?
Participants with certain conditions have more mobility issues than others. They require daily physiotherapy sessions to even perform day-to-day activities. For example, autistic people and others with similar intellectual and mental issues face problems moving. Then there are people who have suffered strokes or heart attacks recently and are almost bedridden. Sufferers of Parkinson’s disease, Alzheimer’s and Dementia may also require definitive and regular physiotherapies to live independently.
Coming to physical disabilities, participants suffering from Down ’s syndrome, Quadriplegia, Paraplegia and Hemiplegia need more exercises than most to even walk or ride their wheelchairs to the bathroom. With NDIS covering the expenses of their basic exercising needs, you can breathe a sigh of relief.
The advantages of opting for NDIS services providers
Caring for such people lifelong not only takes a mental toll on the primary carers but also burns a hole in their pockets. A reliable NDIS services provider offering home physiotherapy service in Sydney can be of huge help in such cases. They will not only cover the expenses but also provide you with the best nurses and therapists for your loved ones. What are you thinking then? Get in touch with a reliable provider and do the needful. Your loved ones deserve to be taken care of in the right way without worrying about money.
#home physiotherapy services in Bankstown#Home physiotherapy service Sutherland#Home Physiotherapy Services#Mobile Physio Sydney#NDIS Registered Physio Sydney#Home care mobile physiotherapy Sydney
0 notes
Text
(941) wireframe
my head is a wireframe ratcheting up the wires i’m living among the metal stretches not even stable - rust spreading from every angle random weaknesses where i put my weight, i’m tangled up by uncaring edges razor-sharp tearing through my limbs iron stings matching red rust, it’s all guilt that i’m ignoring which leaves thin strips frizzing fraying off filed edges-points like steel wool my head’s buzzing, buzzing empty
i keep telling myself pour myself back into a gutful clay cup of sunshine live in now, no problems here though they loom, weave them into a tapestry to stare at but i’m navigating an abandoned jungle gym with learned helplessness i might have analysis quadriplegia because low mellow sunshine can���t melt cacophonies of steel grinding pig iron rust flaking away with every rustle --last month i could let it all fall open away like a rabbit hutch gnawed open with no rabbit inside but back here, baking in the hot summer, boiling in the humidity face stinging at the gray sheet of sleeting spit the rust expands and it’s so hard to climb out
1 note
·
View note
Text
Things are looking up. Over the last three days Hubby has come back to reality. He’s still lethargic from the antipsychotics they’re giving him but he’s back to a functioning human.
We squabbled even. I said something about moving to Omaha this summer and how I’d gotten some applications for accessible apartments for him and it would be a good idea to get on the waiting lists now. He said he didn’t want to move but doesn’t want to be that far away from The Girl.
I felt like an evil witch when I said that the choice is his but I’m moving. Of course, The Girl will have to live with me.
It has been my plan to move out of Mayberry once Boy #2 graduates for more than 2 years. I’ve made no secret of that. We’ve talked multiple times about him moving too.
I’d be upset over arguing with him if I wasn’t so glad that he’s participating in his own life. The man hasn’t had an opinion in years. Maybe he has the capacity to be an adult after all?
I’m sure there are families out there with more fucked up dynamics than ours, but I don’t know any.
#fucking mayberry#coparenting problems are exponentially compounded by quadriplegia#my kingdom for a divorce#literally#I’d let him have everything#but it wouldn’t be enough to not have to take care of him
14 notes
·
View notes
Text

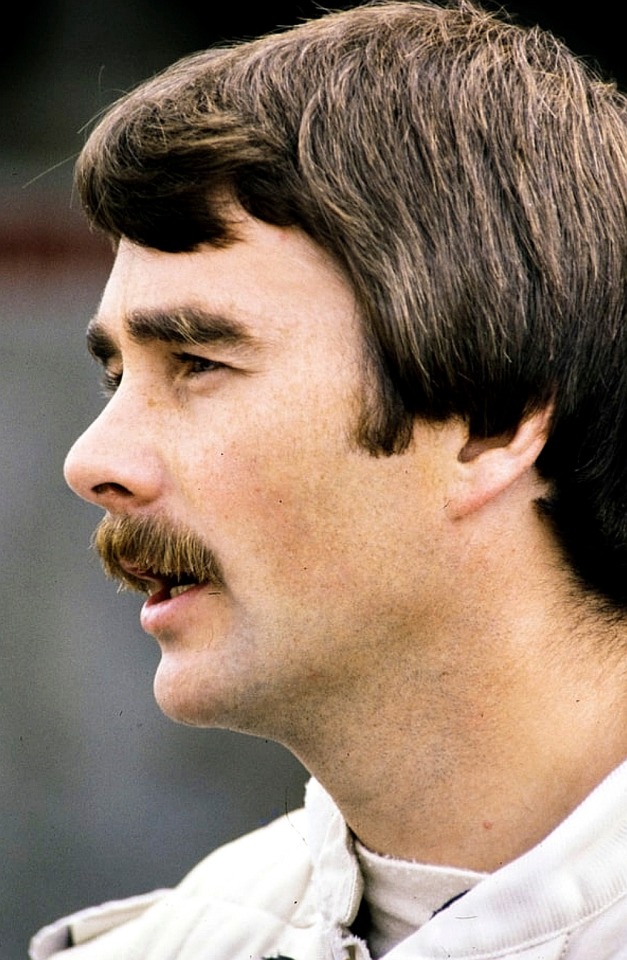
Happy birthday NIGEL MANSELL!!!!!!!!!!!!! (08/08/1953) 🦁⚡
“I think life is full of challenges and problems. I don't believe that anyone is perfect. We all make mistakes. It's not a bed of roses, and you have to work real hard at it.”
Nigel Ernest James Mansell was born in Baughton near Upton-upon-Severn, but grew up in Hall Green, Birmingham. He was the third of four children: Michael, Gail and Sandra. His first approach to driving came early when, at the age of 7, he drove an Austin in a field nearby; but something that fed Nigel's need for speed and curiosity towards motorsport was definetely witnessing Lotus driver, Jim Clark, win at the 1962 British Grand Prix. Subsequently Nigel started driving karts, where wheel-to-wheel battles were the ordinary, young Nigel started crafting and developing his driving skills.
After gaining a good amount of succsess, he then moved to race in the Formula Ford series, which turned out to be very challenging: his father disapproved his son's choice to race, he had to sold a lot of his personal belongings to be able to finance his career, he resigned from his job as aerospace engineer and suffered a broken neck in a accident during a qualyfing session. After being hospitalized, the doctors told him that he had come perilously close to quadriplegia (condition that after an injury can cause the loss of use of the four limbs) and that he would be confined for six months and would never drive again, but Nigel had other plans: he sneaked out of the hospital by telling the nurses he was going to the bathroom, and later returned to racing; despite the injuries and financial issues, he became the 1977 Formula Ford champion. From 1978 to 1980, Nigel raced in Formula Three, but in 1979 he had a seriuos accident that left him with broken vertebrae. But that did't prevent him to attend some tryouts with the Lotus team, hiding the extent of his injury with painkillers.
Being so impressed with Nigel's skills, Colin Chapman decided to give him a trio of F1 starts. Nigel made his official F1 debut at the 1980 Austrian GP, but a fuel leak in the cockpit that developed shortly before the start of the race, left him with painful first and second degree burns on his buttocks. Despite being unlucky on his other two races too, Colin Chapman suprisingly signed the young British driver, after Mario Andretti announced he would move to Alfa Romeo, making Nigel an official Lotus driver, joining the Italian driver Elio De Angelis in the team. After Colin Chapman's sudden passing in 1982, Peter Warr took over in the team, but he and Nigel never really got on, so this lead Nigel to sign with Williams for the '85 season. In the first year with the British team, he would go and score his first win at the '85 European GP. Through difficulties Nigel scored many other wins with the team, but when in 1988 Williams had a terribly unreliable car, an opportunity arose when Ferrari offered him a seat for the '89 season. Nigel became the last driver to be personally chosen by Enzo Ferrari before his passing. There were a lot of mechanichal changes in the sport that year, so Nigel was hopeful to have a competitive car by 1990, but unfortunately it revealed to be the opposite: the car was extremely unreliable and furthermore, his relationship with his french teammate Alain Prost, got worse and led to the Bristish driver to leave the Scuderia, only to return to Williams for two whole seasons. 1992 would be a very special year for Nigel since he would go a win the much coveted World Championship title. The following year, after a public disagreement with Williams, Nigel retired from F1 and moved to the US to race in the CART series, but would later make a come back, driving once again for Williams in 1994 and the following year he moved to McLaren, only to retire definitely from F1 after a series of disagreements with the team.
Despite leaving Formula 1, Nigel competed in many other motorsports; still to this day he makes appereaces at various motorsport events, like it happened recently at Goodwood.
For eleven years Nigel was a Special Constable on the Isle of Man, and later in Devon after retiring from Formula 1.
Nigel was a keen golfer and reveald a desire to compete in the British Open. In 1988, he briefly took part in the Australian Open.
His innocent-looking appearence, calm voice and nice sounding accent are all in pure contrast with his fierce, daring and aggressive driving style and determined nature. Inspired by these characteristics, the Italian Tifosi nicknamed him as "Il leone" ("the lion"), underlining even more Nigel's fearless driving style.
60 notes
·
View notes
Text
WIP day, newest day of the week
Tagged by @doodlevich @flamingbluepanda @energievie and @sisitrip to share bits of what I'm working on.
BUT
I at the moment don't have any chapter drafts, so I'll just share all the WIPS and little blurbs about them.
Stranger Things
Chrissy Wake Up
Chrissy has nightmares and looks to Eddie for help. She also begins to lose the chains that her mother and Jason tie her down with thanks to Eddie's help and acceptance.
The New Girl At Hawkins High
Eddie Munson x Plus size reader where the reader is new to Hawkins and Eddie is drawn to her. Inviting her to join Hellfire for the night.
Gallavich/Shameless
Can We Skip To The Good Stuff
Mandy drags Mickey to a concert where they have a VIP pass to play dodgeball with the band and the crew, Mickey clocks the redhead in the face, gets taken back by security and talks with the redhead, hitting it off. Only when he sees Ian on stage does he realize he's the main singer.
The Upside
After Ian is injured after a bipolar manic episode that leaves him with c7 quadriplegia and in a wheelchair his older sister and brother decide he needs a caretaker.
Mickey is needing a job to appease his parole officer when he accidentally applies as Ian's life auxiliary. Which means up close and personal time with the redheaded boss.
Spare Parts
After a run with Terry goes bad and Mickey is shot, he has to undergo surgery to get his right arm and his right leg. His world is turned upside down as he tries to rehabilitate and cope with the sudden changes he is going through.
Ian is a physical therapist dealing with inner mental health problems and is working at Mountain Heights Physical Therapy when a tough looking brunette woman comes in to make an appointment for her brother.
Knight in a Shining Youber
Mickey is an uber driver, one night picking up a couple from the Fairy Tale he realizes the ginger is drugged out of his mind and the geriatric fuck he's with is taking advantage of him. Mickey takes Ian somewhere safe until he can sober up and tell him where he can take him.
Ian doesn't have anywhere to go, he's in dept to a drug dealer and he's recently been abused in several ways and his mind is all fucked up. When he wakes up to an unfamiliar surroundings with a blue eyed man making breakfast he doesn't know what to think, where to go. But Mickey is there to help.
Once Upon a Food Truck
Mickey and Ian are rival food truck operators in Chicago and when they begin fighting over a parking spot it starts to get personal with views being racked up on social media, the rivals decide a little fake dating for the fans will get them both plenty of customers. But the fake dating starts getting a little more realer than the two planned.
Valorous Vigilantes
Ian is an EMT when he gets a call to go to the Alibi where there's a fight happening. He's surprised to see Mickey Milkovich getting beat close to death by his father, even more surprised to find out that Terry was beating him because Mickey came out as "a big ol mo." Ian picks Mickey up and takes him to the hospital.
Once admitted Ian visits him and finds out more about Mickey than he had planned.
Big Top Beloveds
(This one doesn't get regularly updated, I just needed to get this bit out of my head.)
Mickey Milkovich is the new Circus Ringmaster/owner of the Gallagher Circus, Terry won it from Frank as a form of payment and is throwing the responsibility to Mickey, thinking it's a shit job. Mickey, completely out of his element, starts changing things around much to the irritation and anger of some members there, the tall redhead being one of them. Ian Gallagher is one of the acrobats and aerial performers of his father's circus, when a new ringmaster joins them and starts to change shit around Ian is pissed, until he realizes that the new ringmaster is the man with the stunning blue eyes from before.
#Jesus I have so many WIPS#don't know why I can't just work on one at a time#think I'll try that next time#stranger things#stranger things eddie munson#Eddie Munson#Eddie Munson x plus size reader#Eddie Munson x Chrissy Cunningham#Chrissy Cunningham#chrissy wake up#hellcheer#otp: mean and scary#mean and scary#shameless#gallavich#Ian Gallagher#Mickey Milkovich#The New Girl at Hawkins High#Chrissy Wake Up#hellfire club#eddissy#Valorous Vigilantes#can we skip to the good part#once upon a food truck#big top beloveds#the upside#spare parts#knight in a shining youber#ian gallagher loves mickey milkoich#mickey milkovich loves ian gallagher
44 notes
·
View notes
Text
Spain's assisted suicide law is in the spotlight after doctors allowed the death of a former security guard who faced trial for having allegedly stormed his former workplace a year ago, shooting and wounding three people and later a police officer.
Eugen Sabau, known in Spain as "the Tarragona gunman," applied for euthanasia in June, six months after he was left with quadriplegia when police subdued him in a shootout following the attack on Dec. 14 in the northeastern city.
Victims had argued that Sabau should not be helped to die before his trial, but two Spanish courts ruled that the accused's right to seek assisted suicide prevailed. The man died Tuesday in a prison in northeastern Spain. Sabau was 46 at the time of his death, according to AFP.
In March 2021, Spain became the fourth country in Europe to allow physician-assisted suicide for patients with incurable diseases and for people with unbearable permanent conditions.
A Tarragona court ruled that Sabau suffered unbearable pain with no possibility of relief and agreed with the medical commission that delaying his death until after the trial violated the accused's dignity and rights.
"I am paraplegic," Sabau previously told the judge, according to AFP. "I have 45 stitches in my hand. I can't move my left arm. I have screws (in my body) and I can no longer feel my chest."
José Antonio Bitos, a lawyer for the injured police officer, said Wednesday that Spain's assisted suicide law had been rushed in and should be reformed to prevent similar cases in the future. He said the case set a precedent and could potentially be used by defendants who find themselves in similar circumstances and face lengthy sentences if convicted.
Ramón Riu, an expert in constitutional law, told Spanish National Television that the case "is a precedent and courts will certainly take it into account in the future but they will not be obliged to follow the same criteria."
Bitos took the case to the European Human Rights Court but was unsuccessful in getting a stay. He said he hopes the court will study the case and urge Spain to make changes.
Sabau, a Romanian with Spanish residency, had problems with the private security firm he worked for and had warned several colleagues that he would take revenge. Bitos said he never apologized for what he had done.
The lawyer said it was now unclear how the four victims, who sustained serious injuries, may claim compensation, given that there will be no trial.
6 notes
·
View notes
Text
Lupine Publishers|Ciprofloxacin-Induced Cervical Spinal Stenosis and Upper Limb Paresis Post-Typhoid Fever: A Case Report

Abstract
Rationale: Typhoid (enteric) fever is one of the most serious infections worldwide. Drug-induced diseases is a vital issue in toxicology and clinical medicine. Ciprofloxacin is a fluoroquinolone antibiotic can cause a serious or irreversible disabling side including tendon, bone, muscles, joints, nerves, and central nervous system problems. Patient concerns: A middle-aged married male patient presented to the physician outpatient clinic with a typhoid fever progress to severe neck pain and weakness of both upper extremities.
Diagnosis: Ciprofloxacin-induced bilateral upper limb paresis and cervical spinal stenosis. Interventions: Magnetic resonance imaging Electrocardiography, Widal test, and decompressive surgical neck repair.
Outcomes: The deterioration after decompressive surgical neck repair had happened. Quadriplegia was a major complication.
Lessons: This is the first case that reports these adverse drug reactions with oral ciprofloxacin. Oral ciprofloxacin can induce bilateral upper limb paresis and cervical spinal stenosis. The identification of drug-induced disease is a pivotal step in the diagnosis decision making of any medical problems.
Keywords: Ciprofloxacin; drug-induced; typhoid fever; bilateral upper limb paresis; cervical spinal stenosis
Abbreviations: ECG: Electrocardiogram; MRI: Magnetic resonance imaging; VR: Ventricular rate
Introduction
Typhoid and paratyphoid (enteric) fever is a potentially serious infective disease mostly, in developing countries1 Poor sanitation and bad food hygiene are major risk factors [1,2]. It is caused by Salmonella Typhi, Paratyphi A, Paratyphi B, and Paratyphi C2. The usual incubation period is 7-14 days with a range of 3-60 days. The infection is usually manifested with fever which increases with disease progression, frontal headache, fatigue, muscular pain, anorexia, and cough. Constipation, less frequent diarrhea, abdominal pain, bradycardia, splenomegaly, and rose spots ‘rash are other possible presentations1. The diagnosis of typhoid cannot be confirmed based on symptoms and signs of the infection alone. There is a wide variation in the symptoms of typhoid fever rather than the broad differential diagnosis [3]. Serological markers and bacterial culture with antigen discovery; and DNA intensification are suggested tests [2]. Unfortunately, all of these are unacceptable [2]. The Widal test measured the agglutinating antibodies against LPS (O) and flagellar (H) antigens of Salmonella serovar Typhi in the sera of in suspected cases of typhoid fever. It is an essential and economic to perform is still widely used test [4,5]. Fluoroquinolones (e.g., ciprofloxacin) and third generation cephalosporins (e.g., ceftriaxone) is used the initial antibiotics of choice1. Australian guidelines recommend ciprofloxacin 500 mg orally, 12 hourly for 7-10 days [6]. Typhoid fever may be complicated with intestinal bleeding, intestinal perforation, encephalopathy pancreatitis, heart failure endocarditis, myocarditis, liver failure, hepatitis or pyelonephritis, glomerulonephritis, renal failure, pneumonia from and respiratory failure, orchitis, arthritis and disseminated intravascular coagulation [1,3]. The overall mortality rate is 10% but it is less than 1% with adequate antibiotic therapy [1]. Ciprofloxacin is a fluoroquinolone broad-spectrum antibiotic that is commonly used to treat different types of bacterial infections, e.g., dermatitis, osteomyelitis and arthritis, sinusitis, pneumonia, urinary tract infections, and infective diarrhea [7]. Ciprofloxacin was patented in 1980 and introduced in 1987 [8]. It is on the World Health Organization’s List of Essential Medicines [9]. It is active against some Gram-positive and many Gram-negative bacteria [10]. It acts by inhibiting the type II topoisomerase (DNA gyrase) and topoisomerase IV that are essential for bacterial DNA separation and inhibiting the cell division [11]. Fluoroquinolone antibiotics can cause serious or irreversible disabling side effects e.g., tendon rupture and nerve problems7. So, ciprofloxacin adverse effects are frequently including tendon, bone, muscles, joints, nerves, and central nervous system problems [7,12]. Fluoroquinolone treatment should be immediately ceased if a patient reports neuropsychiatric side effects, tendons, muscles, joints adverse effects. The physician should be switch to a non-fluoroquinolone antibiotic [7,9,13]. All patients who receive a systemic fluoroquinolone should be made aware of the potential for changes in memory, attention span, and other psychiatric functions, and should report signs of alarming CNS effects to a healthcare professional [13]. Aim of this study: In this manuscript, I reported the development of cervical spinal stenosis and bilateral upper limb paresis within 7 days after using ciprofloxacin in a middle-aged male patient.
Case Presentation
A 58-year-old married, farmer, Egyptian male patient presented to the physician outpatient clinic with palpitations, fever, and headache. The patient gave a history of constipation and abdominal pain. The patient denied a history of cardiac, thyroid, neurological, and musculoskeletal complain or other relevant diseases. Upon examination, the patient appeared sweaty, rigor, fatigued, and coated tongue. His vital signs were as follows: blood pressure of 100/70 mmHg, the pulse rate of 66/bpm; and regular, the respiratory rate of 32/min, the temperature of 39.8°C, and the pulse oximeter of oxygen (O2) saturation of 99%. No more relevant clinical data were noted during the clinical examination. The electrocardiogram (ECG) was done within 7 days of treatment which showed normal sinus rhythm at 76 beats/min (Figure 1). The direct agglutination test for Widal was positive for; Typhi (O); 1/160, Typhi (H); 1/640, Paratyphi (A); 1/160, Paratyphi (B); 1/320. Ciprofloxacin (oral tablet) 750 mg twice daily was prescribed. The patient started to complain of acute neck pain, shoulders pain, tingling, numbness, and weakness in both upper limbs. Symptoms was elicited after bending and twisting the patient neck (Spurling’s maneuver). Ciprofloxacin was immediately ceased. The patient referred to neurosurgeon for consultation. MRI film of the cervical spine was requested. It is showing marked cervical canal stenosis at C 3-4 level and mild cervical canal stenosis at C 4-5 level and at level C 5-6 level (Figure 2A). The neurosurgeon decided to make decompressive neck surgery. But, unfortunately, quadriplegia was the end result. The patient was managed conservatively. The investigations done were the troponin test, electrolyte level, thyroid studies, and random blood sugar with no detectable abnormal results. Complete blood count showed leucopenia. Within 15 days of decompressive neck surgery, Plain X-Ray film of the cervical spine on both extension and flexion view was done. It is showing evidence of cervical spine internal fixation at C 3-4 level (Figure 2B). Complete clinical characteristic of the patient on presentation and after treatment was summarized (Table 1).
Discussion
a) Overview: The current case is a middle-aged married male patient presented to the physician outpatient clinic with bilateral upper limb weakness within 7 days after using oral ciprofloxacin in typhoid fever. b) The primary objective for the current case study was the presence of cervical spinal stenosis and bilateral upper limb paresis within 7 days after using oral ciprofloxacin. c) The secondary objective for the case study was How would you manage cervical spinal stenosis and bilateral upper limb paresis? d) The main differential diagnosis for the study case is cervical myelopathy.
e) After the exclusion of other possible triggers in the current case, the Naranjo probability scale was used to evaluates the association between oral ciprofloxacin and development of both cervical spinal stenosis and bilateral upper limb paresis. Naranjo probability scale in the current case study was 9. It is meaning that there was a definite relationship between these adverse drug reactions and the causing drug; oral ciprofloxacin (Table 2). f) Finally, I reported the development of cervical spinal stenosis and bilateral upper limb paresis within 7 days after using oral ciprofloxacin in a 58-year-old male. g) Indeed, the mechanism of oral ciprofloxacin inducing cervical spinal stenosis and bilateral upper limb paresis is unknown. The author thinks that the age may be a trigger factor. The cartilaginous damage and spinal osteoarthritis may interpret this complication. h) This is the first case that reports these adverse drug reactions with oral ciprofloxacin. So, I can’t compare this case with another case because there was no similar publicized case report. i) Despite the drug-drug interactions (DDIs) or even drugfood interactions have a strong impact in inducing various serious drug adverse effects, but it was unviable in my case report. Absent of using drug combinations in the patient history may exclude the theory of drug-drug interactions. j) Drug-induced diseases is a pivotal step in the diagnosis decision making of any medical problems. k) Drug side effects are a sometimes-strong way for the diagnostic challenge in clinical medicine.
Limitations of the study: There are no known limitations in the study.
Conclusions
a) Ciprofloxacin can induce bilateral upper limb paresis and cervical spinal stenosis. b) So, attention must be taken on using ciprofloxacin. to reduce the risk of the development of these adverse drug reactions.
#For more information#https://lupinepublishers.com/medical-science-journal/#Please click here#https://lupinepublishers.com/medical-science-journal/archive.php#lupine Publishers lojms#drug-induced#LOJMS
4 notes
·
View notes