#posting about how covid can cause brain damage and how to prevent it. and then. not preventing it
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s website traffic is steadily declining.
Text
Also preserved in our archive (Daily updates!)
Authors: Rose (Shiqi) Luo Postdoctoral Research Fellow, School of Health and Biomedical Sciences, RMIT University
Catherine Itsiopoulos Professor and Dean, School of Health and Biomedical Sciences, RMIT University
Kate Anderson Vice Chancellor's Senior Research Fellow, RMIT University
Magdalena Plebanski Professor of Immunology, RMIT University
Zhen Zheng Associate Professor, STEM | Health and Biomedical Sciences, RMIT University
____________________________________________________________
Nearly five years into the pandemic, COVID is feeling less central to our daily lives.
But the virus, SARS-CoV-2, is still around, and for many people the effects of an infection can be long-lasting. When symptoms persist for more than three months after the initial COVID infection, this is generally referred to as long COVID.
In September, Grammy-winning Brazilian musician Sérgio Mendes died aged 83 after reportedly having long COVID.
Australian data show 196 deaths were due to the long-term effects of COVID from the beginning of the pandemic up to the end of July 2023.
In the United States, the Centers for Disease Control and Prevention reported 3,544 long-COVID-related deaths from the start of the pandemic up to the end of June 2022.
The symptoms of long COVID – such as fatigue, shortness of breath and “brain fog” – can be debilitating. But can you die from long COVID? The answer is not so simple.
How could long COVID lead to death? There’s still a lot we don’t understand about what causes long COVID. A popular theory is that “zombie” virus fragments may linger in the body and cause inflammation even after the virus has gone, resulting in long-term health problems. Recent research suggests a reservoir of SARS-CoV-2 proteins in the blood might explain why some people experience ongoing symptoms.
We know a serious COVID infection can damage multiple organs. For example, severe COVID can lead to permanent lung dysfunction, persistent heart inflammation, neurological damage and long-term kidney disease.
These issues can in some cases lead to death, either immediately or months or years down the track. But is death beyond the acute phase of infection from one of these causes the direct result of COVID, long COVID, or something else? Whether long COVID can directly cause death continues to be a topic of debate.
Of the 3,544 deaths related to long COVID in the US up to June 2022, the most commonly recorded underlying cause was COVID itself (67.5%). This could mean they died as a result of one of the long-term effects of a COVID infection, such as those mentioned above.
COVID infection was followed by heart disease (8.6%), cancer (2.9%), Alzheimer’s disease (2.7%), lung disease (2.5%), diabetes (2%) and stroke (1.8%). Adults aged 75–84 had the highest rate of death related to long COVID (28.8%).
These findings suggest many of these people died “with” long COVID, rather than from the condition. In other words, long COVID may not be a direct driver of death, but rather a contributor, likely exacerbating existing conditions.
‘Cause of death’ is difficult to define Long COVID is a relatively recent phenomenon, so mortality data for people with this condition are limited.
However, we can draw some insights from the experiences of people with post-viral conditions that have been studied for longer, such as myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS).
Like long COVID, ME/CFS is a complex condition which can have significant and varied effects on a person’s physical fitness, nutritional status, social engagement, mental health and quality of life.
Some research indicates people with ME/CFS are at increased risk of dying from causes including heart conditions, infections and suicide, that may be triggered or compounded by the debilitating nature of the syndrome.
So what is the emerging data on long COVID telling us about the potential increased risk of death?
Research from 2023 has suggested adults in the US with long COVID were at greater risk of developing heart disease, stroke, lung disease and asthma.
Research has also found long COVID is associated with a higher risk of suicidal ideation (thinking about or planning suicide). This may reflect common symptoms and consequences of long COVID such as sleep problems, fatigue, chronic pain and emotional distress.
But long COVID is more likely to occur in people who have existing health conditions. This makes it challenging to accurately determine how much long COVID contributes to a person’s death.
Research has long revealed reliability issues in cause-of-death reporting, particularly for people with chronic illness.
So what can we conclude? Ultimately, long COVID is a chronic condition that can significantly affect quality of life, mental wellbeing and overall health.
While long COVID is not usually immediately or directly life-threatening, it’s possible it could exacerbate existing conditions, and play a role in a person’s death in this way.
Importantly, many people with long COVID around the world lack access to appropriate support. We need to develop models of care for the optimal management of people with long COVID with a focus on multidisciplinary care.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#sars cov 2#coronavirus#long covid
143 notes
·
View notes
Text
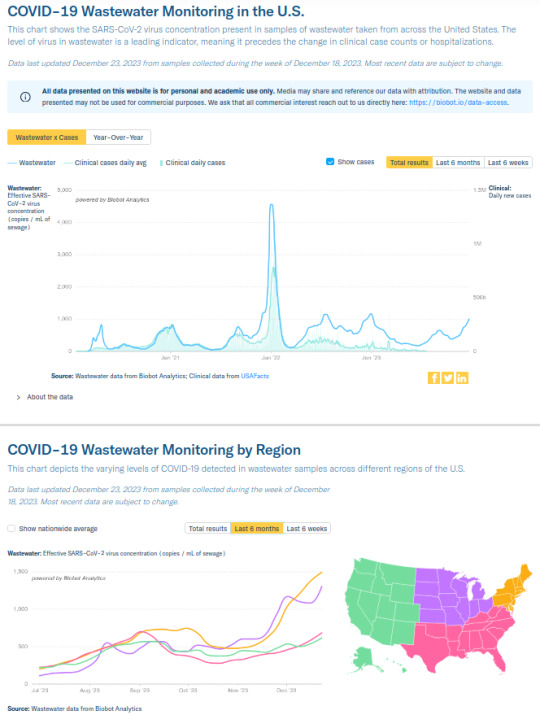
Weekly COVID-19 Update for 2023-12-24
COVID is still airborne, and COVID still very much isn't over.
Northeastern and Midwestern USA SARS2 virus levels in wastewater are *soaring*, Northeast is currently at 1500 copies/mL (~750 copies indicates a strong surge), and Midwest is at 1300 copies/mL. Southeastern and Western USA are maintaining relatively lower levels between 600 and 700 overall, but both are still climbing. See https://biobot.io/data for county-specific data as results can vary widely between locales.
How to reduce your risk of infection? The SARS2 virus is airborne and can spread like smoke, so #MaskUp with an #N95 or better, avoid superspreader events and locations, and stay up-to-date on your boosters. Do it for yourself, so you don't catch SARS-CoV-2, and for others, so you don't spread SARS-CoV-2. Even if you're fully vaccinated, your risk of developing #LongCOVID following an infection is lower but not zero, and multiple reinfections increase your odds of negative health outcomes. Plan A always should be to prevent an infection from developing by wearing a respirator with a good seal around your mouth and nose (FFP2, FFP3, KN95, N95, N99, P100, etc.).
Holiday tips:
-If someone tells you that COVID is over, you might ask them why, if we didn't consider COVID to be over in 2020 or 2021, when the COVID wastewater levels were lower, why should we consider it over now, when the virus is circulating in even higher amounts?
-"Fewer cases" doesn't mean much when most of the at-home rapid tests don't get counted in official records, and the most accurate PCR tests are neither freely available nor given to everyone getting on a plane or attending classes.
-"Fewer deaths" also means less when you remember that about 1,200,000 of the most vulnerable people already have died from it, COVID-19 remains the #3 cause of death in 2023 (behind heart disease and cancer, the risk of both of which may be increased by COVID), and the risk of a Long COVID/post-acute COVID syndrome (PACS) disability or other potentially life-shortening organ damage (brain, kidney, lung, immune, etc.) isn't measured just by the death count. Also, the USA's life expectancy still hasn't recovered from the drop it experienced following the start of the pandemic.
source: https://biobot.io/data
source: https://www.webmd.com/a-to-z-guides/news/20231006/these-are-the-top-10-causes-of-death-in-the-us
source: https://publichealth.jhu.edu/2022/covid-and-the-heart-it-spares-no-one
source: https://pubmed.ncbi.nlm.nih.gov/33914346/
source: https://www.usatoday.com/story/news/nation/2023/11/29/average-us-life-expectancy-increased-not-pre-covid/71738611007/
#covid#pandemic#corona#coronavirus#sarscov2#publichealth#science#disease#covidisntover#virus#medicine#sars2#covidisairborne#covidisnotover#health#lifeexpectancy
47 notes
·
View notes
Text
i genuinely dont understand the sheer cognitive dissonance to be posting about how masks are soooo soooo important for preventing covid (true!) and then NEVER wearing one yourself irl. are you..... looking forward to catching covid? like are you doing it on purpose? idgi
#text#i mask everywhere including outside so dont try to come for me#are you like. hoping that youre going to get exposed and then infect someone?#i cant imagine anyone WANTS to do that except rly insane antivaxxers#like... why post about how everyone should mask if YOU arent going to mask. are you virtue signaling??#do you just want points for posting about it on social media but not want to have to practice what you preach??#do you actually care about getting yourself sick? like ignoring expoisng other people are you genuinely ok getting covid despite-#-knowing in detail all of the really horrible ways it fucks you up?#why would you share information encouraging other ppl to mask and then not be encouraged yourself??#its a level of cognitive dissonance i dont get#posting about how covid can cause brain damage and how to prevent it. and then. not preventing it#like posting a ton of pro-helmet propaganda and then not wearing a helmet. like what is the point
13 notes
·
View notes
Photo

The Pandemic After the Pandemic
Long COVID isn’t going away, and we still do not have a way to fully prevent it, cure it, or really to quantify it.
The world was slow to recognize long COVID as one of the most serious consequences of the coronavirus. Six months into the pathogen’s tear across the globe, SARS-CoV-2 was still considered an acute airway infection that would spark a weeks-long illness at most; anyone who experienced symptoms for longer could be expected to be dismissed by droves of doctors. Now long COVID is written into CDC and WHO documents; it makes a cameo in the newest version of President Joe Biden’s National COVID-19 Preparedness Plan.
But for all we know now about long COVID, it is still not enough. Researchers still don’t know who’s most at risk, or how long the condition might last; whether certain variants might cause it more frequently, or the extent to which vaccines might sweep it away. We do not have a way to fully prevent it. We do not have a way to cure it. We don’t even have a way to really quantify it: There still isn’t consensus on how common long COVID actually is. Its danger feels both amorphous and unavoidable. People already struggle to deal with well-known risks, let alone fuzzy, slippery ones. “You can be too afraid of what you don’t understand or just say, ‘It’s not well defined; I’m not going to think about it,’” says Erin Sanders, a nurse practitioner and clinical scientist at MIT. Concern, when we let it, can act like a gas. It expands to fill the space we give it.
But even if long COVID’s prevalence turns out to be a single-digit percentage of SARS-CoV-2 infections—proportionally much smaller than most experts estimate—in absolute terms “that is not small,” says Ziyad Al-Aly, the director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System. Millions of people have already developed long COVID; many of them, an untold fraction, have not recovered. This is the challenge of chronic illness: When people join its ranks, they do not always exit. With each new case of long COVID, the virus’s burden balloons.
“I worry, now that everyone is moving to the post-pandemic world, we’re going to sweep all these patients under the rug,” Al-Aly said. Long COVID struggled to gain a toehold in the national consciousness; now it threatens to be one of the first major COVID impacts to slip back into the margins.
Researchers have known for many months that long COVID is more a category than a monolith. Al-Aly very roughly likens it to the way we talk about cancer—an umbrella term for diseases that are related but that require distinct diagnoses and treatments. Long COVID has hundreds of possible symptoms. It can batter the brain, the heart, the lungs, the gut, all of the above, or none of the above. The condition can start from a silent infection, an ICU-caliber case, or anything in between. It can begin days, weeks, or months after the virus first infects someone, and its severity can fluctuate over time. “We lump all of that into one broad thing,” Al-Aly said. “It is not.”
The condition’s root causes, accordingly, are also diverse. In some cases, long COVID may be collateral damage from the war waged between virus and immune system; in others, it might sprout out of a chronic SARS-CoV-2 infection or, conversely, a quick viral encounter that sets bodily systems on the fritz. These hypotheses aren’t comprehensive or mutually exclusive: There are only so many ways for bodies to run smoothly, and infinite ways to throw those processes out of whack.
All of this means that even diagnosing long COVID—an essential step toward understanding it—is still a battle. We don’t have a clear-cut, consensus clinical definition, a single name for the condition, or a standardized set of tests to catch it. Even the CDC and the WHO can’t agree on how long a person must be sick before they meet the condition’s criteria. Some researchers and health-care providers favor one agency’s definition; others, dissatisfied with both, come up with their own. And “there are still doctors out there that do not think long COVID exists,” says Alexandra Yonts, a pediatric-infectious-disease specialist at Children’s National Hospital, in Washington, D.C.
In an ideal experimental world, to understand long COVID’s risks, researchers would systematically survey large swaths of the population over long periods of time, watching to see who gets infected, who goes on to develop the condition, what form it takes, and how it impacts people’s health, says Shruti Mehta, an infectious-disease epidemiologist at the Johns Hopkins Bloomberg School of Public Health who is studying long COVID. But few institutions have the resources for such an undertaking, which could span many months or years. So many researchers have to make do with the limited data sets that are already available to them. As a result, some studies end up biased toward patients who were hospitalized, while others wind up favoring people who have the time, means, and trust in the health-care system to sign up for long-term studies. Neither group fully captures long COVID’s wide-ranging toll. The situation’s especially tough for pediatric patients, who might be too young to articulate the severity of their symptoms and are often excluded from long-COVID studies. Long COVID certainly exists in kids, but it may not perfectly mirror what goes on in adults: Children’s susceptibility to the virus is different, and their bodies are so rapidly changing, says Yonts, who runs a pediatric-long-COVID clinic in D.C.
All told, the study of long COVID has become, as Sanders of MIT puts it, “a data disaster.” Some researchers estimate that a single-digit percentage of SARS-CoV-2 infections bloom into long COVID; Al-Aly is one of them. Others, meanwhile, favor larger numbers, with a few even insisting that the rates are actually more than half. Most of the experts said they feel comfortable working in the 10 to 30 percent range, which is where many studies seem to be starting to converge. Finding one answer is tricky, without knowing how many forms long COVID can take—some could be more common than others. Formally splitting the disease into subdivisions could help address some of these ambiguities. But we don’t know nearly enough to start slicing and dicing, says Bryan Lau, an infectious-disease epidemiologist working with Mehta and Priya Duggal.
If researchers aren’t comprehensively capturing who currently has long COVID, they can’t say for certain who’s most likely to get it either. Many researchers have found that women contract long COVID more frequently than men. Others have uncovered evidence that people who end up infected with gobs of the coronavirus, or who produce antibodies that attack the body’s own tissues, also seem to tilt toward long COVID. Chronic health issues, including diabetes, could up a person’s chances of getting sick and staying sick as well. So might a lingering Epstein-Barr virus infection. But some of these trends are still being confirmed, experts said, and the extent to which they toggle risk up or down isn’t known. And it’s definitely too early to pinpoint any of these factors as long-COVID causes. “For acute COVID, we know what the risk factors are,” Akiko Iwasaki, an immunologist studying long COVID at Yale, said. “For long COVID, it’s much less clear.”
Still, a couple of other variables feel a bit more nailed down. “The risk is high in people who need hospitalization or ICU care,” Al-Aly said. Deepti Gurdasani, an epidemiologist at Queen Mary University of London, says she’s fairly confident that the nature of a person’s exposure to SARS-CoV-2 plays a role as well: Heavier and more frequent viral encounters seem to tip the scales toward symptoms that last and last. That’s a concern for people in essential occupations, who “aren’t able to shield themselves,” she said.
If these last few factors directly affect how and whether long COVID unspools, vaccination—which reliably staves off hospitalization and, to a lesser degree, infection—could be a partial preventive. Several studies have shown that shots do seem to muzzle long-COVID rates. They don’t, however, eliminate long COVID’s odds. To date, experts have yet to find any demographic that has been spared from the condition, despite persistent myths that certain groups, particularly kids, are somehow immune. “We’ve seen it in children of all ages,” says Laura Malone, a pediatric neurologist at the Kennedy Krieger Institute, in Baltimore. Some of her patients are toddlers. The virus isn’t pulling any punches either. Every iteration we’ve encountered so far, Omicron included, seems capable of causing long COVID. “No one is not at risk,” Al-Aly said.
To this day, most countries do not keep a running tally of long-COVID cases. But ballparks of the burden are staggering. Some 2 percent of all U.K. residents—not just those with documented infections—might currently have long COVID, according to the Office for National Statistics. Another analysis estimates that up to 23 million Americans have developed the condition since the pandemic’s start. More will join them. But Davis worries that those numbers will continue to be left off of national dashboards, and thus out of the public eye. Now that the federal government has tightened the boundaries of its concern to hospitalizations and deaths, the public does not even really have to look away from the national perspective on long COVID: There is next to nothing to see.
As people rack up different combinations of shots and infections with different variants, what worsens or soothes long COVID is also getting harder to understand. Many of the experts think long COVID is essential to study, it’s too complex for them to want to tackle themselves. Meanwhile, long COVID remains the pandemic’s looming specter. We are told there is risk, but not exactly how much; we are told that avoiding long COVID would be ideal, but lack the practical guidance to do so—the virus is so widespread that eventual infection, for many people, feels almost inevitable.
At the same time, as researchers look deeper and deeper into the bodies of infected people, they’re only seeing more damage. With each passing month, more studies emerge documenting how the coronavirus alters the function of vital organs such as the heart and the brain. The public has been cultured to think that most SARS-CoV-2 infections are trivial, and the repercussions brief, especially for the young, healthy, and privileged. But long COVID breaks the binary of severe and mild. “It’s going to continue to affect people, even people who are protected from severe illness during the acute phase of infection,” Michael Peluso, an infectious-disease physician and long-COVID researcher at UC San Francisco, said.
No matter where the true numbers on long-COVID risk sit, they are too large to ignore. “Whether it’s 10 percent or 50 percent, at both levels you have to do something about it,” Gurdasani said. Statistics will help sharpen and clarify the condition’s boundaries, and are still worth seeking out. They will not, however, change long COVID’s threat, at its core.
Davis, who is nearing her second anniversary of developing long COVID, feels this deeply. She is still experiencing cognitive dysfunction and memory loss. Her heart still races when she stands. “You cannot live your life like you used to,” she said. “Your life just becomes this shell.” For individuals, for societies, “this is not going away.” Even after much of the world puts the pandemic in its rearview, long COVID will keep filling hospitals and clinics. It will dot the pages of scientific texts, and linginfer in the bodies of millions of people worldwide. Hospitalizations and ICU admissions are not the only COVID outcomes that can buckle a health-care system.
That strain is already being felt by the health-care workers on long COVID’s front lines. Yonts, the Children’s National pediatrician, said that she’s currently booking patients “out to Memorial Day.” COVID’s global crisis can, in some ways, end when we decide to treat it as done. But that is not an option for a growing fraction of the planet, who cannot put COVID fully behind them. “This is going to be the pandemic after the pandemic,” Gurdasani said.
Source: Katherine J. Wu (The Atlantic). Image credit: Leo Correa/Redux.
119 notes
·
View notes
Text
So I’m working on a fanfic about Hannibal being diagnosed with early onset Alzheimer’s and Will struggling to come to terms with that.
I’m realizing it’s really a commentary on how society treats people whose brains work different.
There is no point where Will loves Hannibal any less and he never sees him as less than human, but doctors and other people do.
Most of the story is from Will’s POV, (I start each chapter in Hannibal’s memory palace as it’s crumbling) but I have Hannibal’s perspective running in my own mind too when we watch him through Will. So when Alzheimer’s causes Hannibal to act weird, I know exactly what he thinks he’s doing or where he thinks he is in place / time, and his behavior makes perfect sense according to where / when he thinks he is. Will and the readers won’t have that side of it, so to them it seems Hannibal doesn’t know how to behave. He has his lucid moments where he’s acutely aware that “I have Alzheimer’s and my brain is failing me”, though they diminish as his brain deteriorates. But he really doesn’t know what he’s doing when he’s not lucid, though sometimes he can remember it later and tell Will what happened. Those moments are heartbreaking.
So as an example of visible behavior vs what I know and don’t tell you: Will sees Hannibal smashing a rolling pin against the kitchen counter, but Hannibal thinks he’s cleaning up to prepare for a dinner party the next night and he’s frantic because there’s a lot to do and not much time, and he can’t get the counter clean. Once Will figures out Hannibal is trying to clean, he trades the pin for a sponge and helps him “clean”. Hannibal forgets why he was so frantic once they’re done, so now he can go to bed and sleep instead of keeping Will up by banging on the counter for hours.
You can’t reason with a confused person with Alzheimer’s once they’re past a certain point. It’s easier to just step into their reality and guide them gently in the direction you hope they’ll go. (Will is very hit and miss at doing this initially, but will get good at it later!)
Most people would suggest take the rolling pin away, but that would get in the way of the need Hannibal is trying to meet and lead to a fight. From his side it looks like Will is preventing him from getting ready for esteemed guests. Will trading the pin for a sponge is meeting Hannibal where he is, calming the anxiety he’s feeling and gently nudging him where he actually should go (to bed). Hannibal is happy with that because his need was met.
There’s another scene in a grocery store where Will doesn’t pay attention to Hannibal’s signals that this isn’t working, and it leads to Hannibal causing a bit of a ruckus. The store is restocking and there’s boxes and chaos everywhere. Hannibal can’t handle that, so he starts taking things out of the cart and putting them on the shelf like he’s at the checkout counter because that’s what you do when you’re about to leave the store. But Will misses that signal and puts things back into the cart, and suddenly a very angry Hannibal flips the cart over and hollers that “this isn’t correct” because he can’t access the language to explain he’s afraid.
Will has to talk him down from a panic attack and help him out of the store. Later, Hannibal is able to explain to Will that disarray frightens him because it looks like his memory palace, and when that happens he can’t tell his inner world from the outer world and doesn’t know which one he’s “speaking” to. But small bits of disarray become something Will can use to calm Hannibal down by giving him messy things to organize. (Hannibal is obsessive about organizing stuff, it’s soothing for him.)
Their love language evolves too. From speaking in metaphors to just speaking, then they progress to actions and finally end on touch.
Will needs to realize it’s less about what Hannibal is losing and more about what’s still there.
Hannibal is going to lose who Will is, but he never loses the fact that he loves him. Some days, he will look at Will and fall in love with him over and over like the first time he saw him in Crawford’s office, because in those moments every time is the first.
And that is what Will needs to realize. Their love hasn’t been lost.
Btw, Hannibal doesn’t stop being dangerous till the final stages of Alzheimer’s. He’s about midway through it when he almost mauls the staff at a hospital because they’re being nasty to him when he’s confused! (They chemically restrain him with Haldol and are super shitty liars about it). That experience is actually what gets Will to see that people are going to treat Hannibal like he’s not really a person anymore. Let’s just say the doctor who ordered the Haldol isn’t gonna survive. It’s Hannibal...that means people get eaten! 😌
Also, the fanfic starts after they’ve been married for 10 years, so the year is 2030 at the start of the fic. I’m writing this pretending the story of Hannibal began sometime in late 2010, Will pulled them off the cliff in 2015, they got some aliases to disappear and moved around America dodging the FBI for another five years.
The pre-story post-fall timeline goes like this:
December 2019: Will and Hannibal have been on the run for a long while, but they stop in Hawaii to have a nice, tropical Christmas. Hannibal can’t remember the volcano’s name is Kilauea.
January 1: 2020: They get married on the beach. It’s sort of spur of the moment, but they took the time to buy tuxedos and rings. Their tuxes are white with silver accents. Hannibal has a silver vest and bow tie. Will has a silver bow tie and cummerbund. They say their vows at sunset by the water.
Late February 2020: Will and Hannibal leave Hawaii for Cuba just as Covid-19 is hitting. They’ve already bought a house, so they move in. Both test positive for covid. Will stays asymptotic and never gets even a tickle in his throat. Hannibal gets the whole deal without getting sick enough to end up in the hospital, but recovers. He has some long covid issues, like shortness of breath and fatigue.
2022: Hannibal survives the widow maker heart attack and it’s discovered he had the heart attack because covid damaged his heart. He gets quadruple bypass surgery and spends a lot of time in ICU recovering. As he gets better he realizes his memory isn’t what it should be. Doctors tell him his heart stopping from the heart attack and the bypass surgery can sometimes cause some memory loss. Hannibal starts relying on his phone and GPS more and more. Will begins to suspect something is wrong, but the doctors reassure him that it’s temporary, so he lets it go.
(Fanfic begins here.)
2030: Hannibal is making mistakes in cooking, cleanup, paying bills and just everyday stuff, but he doesn’t think it’s weird. He blames “kids” when questioned about why he put dishes away dirty or burned dinner. Will is noticing things aren’t right, so he begs Hannibal to see a doctor. Will thinks it’s something solvable, like encephalitis or some other organ. But no, Hannibal gets looked over from head to toe, inside and outside, sent to a neurologist and finishes with his diagnosis of early onset Alzheimer’s. (He’s 58 at the time of diagnosis, but the disease process started when he was 48 and it was missed for so long because of the heart attack.)
As soon as he’s diagnosed, Hannibal starts making plans for Will to be his medical power of attorney, in control of their bank account, in charge of his advanced directives, etc.. He sort of drops it all onto poor Will, who barely gets time to absorb the news before he’s signing stuff. Will is in a tailspin of emotions.
It’ll take Alzheimer’s 20 years to chew through Hannibal’s brain. It’s not always gonna be pretty or easy to watch. At the end it becomes clear Hannibal is waiting for something, and he passes as soon as those final needs are met. Hannibal always has to have control of something, right? Right!
I’m gonna throw all your feelings into a washing machine and spin them. It’s what I’m good at with fics like this.
Anyway...
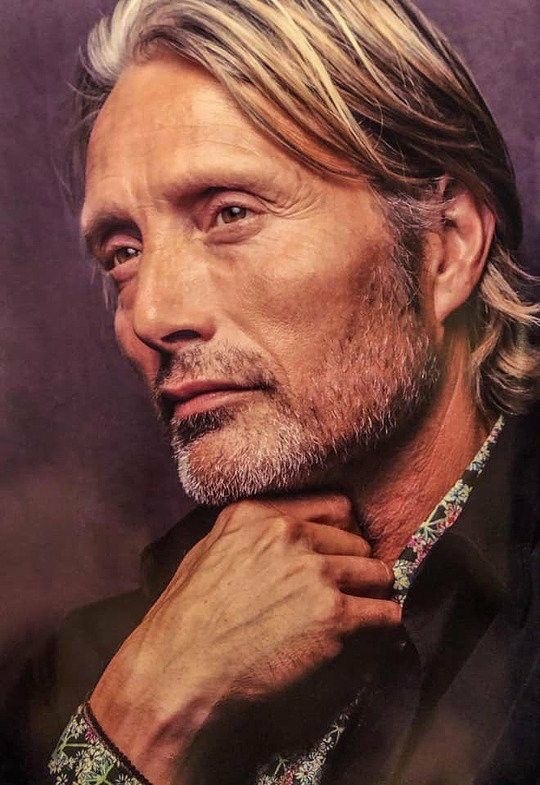
I have very specific images of how Will and Hannibal look at the start of the fic. Will is still pretty af, but a lot less friendly looking, and Hannibal looks like a scruffy Norse dad.

The most beautiful part about writing this (for me, anyway) is watching how Will learns to understand Hannibal’s communications as his language abilities deteriorate. He will continue to see and hear him even when most other people won’t try to watch or listen. He learns to be less “stop that, it’s annoying” and more “what need isn’t being met and how can I meet it? How can I step into his world to be with him where he is?”
Finally, their wedding song is important to the story. This was their first dance song. It’s their song. Will sings it to Hannibal a few times in the fic, and if he plays it on his phone it can break through the Alzheimer’s fog and take Hannibal back to the bank safe in his memory palace where he keeps their wedding day. Yup, he keeps that memory in a safe and it’s the last thing to go. ❤️
youtube
#hannigram#Alzheimer’s#tw medical abuse#tw hospitals#tw chemical restraint#eye contact#long post#Hannibal#Will Graham#Cyndi is writing
17 notes
·
View notes
Text
European Peptide Culture.
Cgmp Peptides.
Content
What Does Mg Of Collagen Indicate?
S23 S4 Sr9009 Sarms S Collection Research Study Stack Sarm Fluid Dropper Chemical.
Fitness And Body Building.
Numerous Males Are Utilizing Online Medicines For Bodybuilding, But They Aren't Safe.
Lgd.

Boost the Metabolism - When carbohydrates are digested, an enzyme called AMP is generated. AMP is very important for the body since it breaks down fats found in the cells. Excess amounts of fatty acids in the cells are converted into acetylcholine, which causes insomnia, drowsiness and poor memory. Peptides can help in preventing such effects. Peptides can stimulate the production of acetylcholine in the liver and help in getting rid of the toxins that cause drowsiness and insomnia. It can also enhance the functioning of the brain.

Whether peptides are taken internally, ingested, or used as a supplement, they do offer some benefits. These benefits include increased energy, better skin, and enhanced immune function. However, just like any other nutrient or substance in your body, you should be careful about trying to overuse them. Excessive intake may have a number of unpleasant side effects. In the case of peptides, excessive use may lead to serious health complications, including death.
What Does Mg Of Collagen Suggest?
Peptides can be found in many health and beauty products. You can use them topically to treat a variety of skin ailments. They may even be used internally to treat a variety of diseases. Peptides are also found in supplements that are used by body builders to add extra protein to their diet. Many athletes take them to build lean muscle mass.
Global Biosimilar Therapeutic Peptides Market Report 2020: COVID-19 Impacts, Growth and Changes - Forecast to 2030 - Yahoo Finance
Global Biosimilar Therapeutic Peptides Market Report 2020: COVID-19 Impacts, Growth and Changes - Forecast to 2030.
Posted: Thu, 07 Jan 2021 14:58:00 GMT [source]
Peptides are small protein molecules that have powerful functions in the body. They have the power to penetrate the blood and enter cells. Peptides are used as immune enhancers and also for treating many other diseases and conditions. Here we will be discussing the various Peptides advantages and their uses.
S23 S4 Sr9009 Sarms S Collection Research Stack Sarm Fluid Dropper Chemical.
There are two types of peptides. One is alpha-ketoglutarate, and the other is beta-ketoglutarate. Both serve different purposes in your body. Alpha-ketoglutarate is an easier way to produce energy. It is used for muscle development and repair. On the other hand, beta-ketoglutarate produces more oxygen and increases metabolic functions.
Can you mix retinol and peptides?
Do Mix: Retinoids + Peptides Dr. Mariwalla says it's a great idea to use both a retinoid- and peptide-based night cream at bedtime. “You get the collagen-building effects of the retinoid, but it also works to improve the penetration of the peptide cream, which can help improve skin's firmness,” she explains.
Prevent Cancer - Peptides are capable of enhancing the immune system and fighting against viruses and bacteria. Research indicates that peptides can stop the growth of cancer cells and even kill cancer cells. Peptides are effective in cancer prevention because they directly attack cancer cells without harming healthy cells in the body. This is different from chemotherapy, which messes up the DNA of healthy cells in the body and inhibits their ability to fight against diseases.
Health And Fitness As Well As Body Structure.
Strengthen the Immune System - There is a vast network of amino acids which are responsible for a wide range of biological processes in the body. One of them is insulin. Insulin is produced by the pancreas and is responsible for many functions. However, it can also cause damage to the pancreatic islet cells if it is not given enough attention. In order to protect the pancreatic islet cells, peptides can be given to enhance the immune system.
youtube
The muscles in the body can be strengthened. When you lift weights, your body uses the muscles to move the weight. The more muscles that you have worked, the more calories that you can burn. As your muscles are strengthened, you will be able to exercise more frequently and for longer periods of time. plenty of software may lose some weight, but you will typically gain lean muscle mass.
Several Males Are Using On-line Medicines For Body Building, Yet They Aren't Safe.
Muscles may be repaired more quickly. peptides uk’s free information BPC157 Sweden have long used peptide supplements to build muscle. The faster the process of recovery, the quicker you can get back to training. Peptides can help speed this process.
Anti-Inflammation - Peptides can actually help in decreasing the swelling of the joints, reducing the pain caused by arthritis and reducing inflammation of the heart, to mention a few. It also prevents damage to the cells around the joints. Proteins are the building blocks of our body and they too form proteins in the body. When we are injured or over stressed, our body releases some proteins which form fluids in the injured areas. This may not seem like a big deal but as we get older this is one of the main reasons for joint deterioration and the associated pain. Peptides can help to inhibit the production of these fluids which means that there will be less fluid to trigger the pain signals.
Lgd.
There are right Saudi Arabia bpc157 how does it work for you associated with peptides. There are even more potential uses. Peptides are extremely healthy and well documented in scientific research. This documentation alone should give you enough reasons as to why you should include these natural proteins in your diet. If you want to learn more about the benefits of peptides, talk to your physician today.
If you are new to this product or any one of its ingredients, we recommend completing a patch test first.
The needle-free formula assists to combat expression creases by minimising muscle contractions while boosting collagen synthesis to noticeably plump the skin tone.
Where examines describe foods or aesthetic products, results may differ from person to person.
Hormonal agent or peptideMajor cells areas in the gutPrincipal understood actionsGastrointestinal peptides, their website of expression and also significant features.
Client testimonials are independent and also do not represent the sights of The Hut Team.
Proteins may be used to encourage wound healing. When muscles are damaged, it can take longer for them to heal. Muscle supplements can speed up the process of recovery. They can also promote new tissues to grow and develop.
Peptides are available from many sources. You may find them in milk, meat, fish, eggs, poultry, beans, and soy. While you may eat some of these products without negative consequences, there may be undesirable side effects associated with them. For instance, some of these proteins may cause intestinal gas or cramps.

Boost the Immune System - Peptides are excellent for boosting the immune system. They enhance the function of the immune cells and also help in warding off disease and other illnesses. As a result of their actions, your body will be protected from all types of diseases, including cancer.
Help in Metabolism - The peptides are also capable of metabolizing fatty acids and glucose. This means that they can aid in weight loss. Our bodies release excess fats through the sweat glands. These released fats are used for energy but excess sugars and carbohydrates are converted into stored fat. Peptides can help in the conversion of carbohydrates into energy thereby reducing weight.
Verisol collagen peptides approved by ANVISA for use in food supplements - Nutritional Outlook
Verisol collagen peptides approved by ANVISA for use in food supplements.
Posted: Mon, 21 Dec 2020 08:00:00 GMT [source]
Protein may be taken in a variety of forms. The best option is to choose whey protein. It is the most highly regarded form of protein. It contains all of the necessary amino acids that your body needs. You may have heard of people having success using casein protein.
#BPC157 EU#BPC157 Europe#information BPC157 EU#information BPC157 Europe#EU BPC157 how does it work#Europe BPC157 how does it work
2 notes
·
View notes
Text
Ducati and Lego...
Things are getting weird with Lego of late, from bad decisions regarding the sources of Technic models, to crunchy gear boxes and then this, the Ducati Panigale V4 R…
From the get go, I was really excited by the prospect of the Technic Ducati. The box looked great, with the model on the front looking really exciting, thanks to the clever and beautiful photography. I had to have one and I argued with myself for several days about spending a significant amount of my severely limited resources on what is in effect a silly, children’s toy. When it came to ordering, we were in the middle of Covid lockdown, Lego were sold out and Amazon was stating that toy orders would take six to eight weeks to deliver, it was not looking good. However, through on line shopping and a little bit of time on google, I found me a toy shop in Northern England that had one in stock and for a good price too.
Now let me tell you a little story, several years ago I was working part time for a national bicycle franchise here in the UK, it was the busy pre-Christmas, super busy sales time and I was on my own in the bike department. I sold a kids bike and the new owner wanted to take it away in a box. I went out the back to the storeroom and tried to retrieve the bike box from a pile stacked up on a shelf, which collapsed on me, crushing a nerve in my neck and right arm. The pain did not not start right away, instead it built up in intensity until I was struggling to take deep breaths had to ask my boss to take me to hospital. I was X-Rayed, poked, prodded and suddenly strapped down hard to a table when a Doctor found shadow across one of my vertebrate that indicated that I had broken my neck! Luckily, it was not broken and I have no idea what that little dark line on the X-Ray image of my tiny bone was. The damage was done though and the nerve that runs from my neck, down my arm and through my elbow was permanently damaged. I was given a lot of medical treatment, went through an awful lot of pain and I was off work for three months because of the injury and grew extremely bored and depressed. The relief to my suffering came in a surprising fashion, when my partner picked up for me, a Lego Technic motorbike to build.
That little Lego motorbike was a revelation, it looked great, it worked brilliantly and it came with instructions to build a second model from the same kit. The kit came with stickers and the whole thing was a bright orange colour that resembled a KTM motocross bike. Days later, e-Bay brought me a bright green one that despite not being as good, was still fabulous and my addiction to Lego, a hobby I started as a child and had put aside as an adult, came back and bit me hard. For me, Lego Technic motorbikes will always be a little bit special because when I cannot ride my own, I can at least build one out of Lego which I enjoy rather than wasting a couple of hours watching brain dead TV or feeling worthless and bored.
Which brings me right up to date. My injured arm and hand never fully recovered, despite hours of physio and exercise. Other injuries came and I was soon left disabled and with a rapidly growing Lego Technic collection. These days, I am an AFOL spend my time building MOC ( Adult Fan of Lego and My Own Creation for non Lego people) machines of varying kinds, although I really enjoy big heavy trucks for some reason. I rarely buy a Technic kit these days, preferring to buy the parts I want in order to construct a particular model. So for me to buy a whole set, means that it is special.

The box of the Ducati does an awesome job of selling the model, it has a photo of the real bike on the back and they go to great lengths to take photos of the Lego model from all of its very best angles. They have also made some new parts specifically for this set and they are pretty good. The new USD suspension forks look amazing and they actually work. The disk rotors look cool. The new wide rear tyres is awesome and looks the part and it is not hard to imagine this machine riding around a race track, but we will come to that later.
However, on closer inspection, there are some gaping holes in the Ducati that in my opinion leave it looking unfinished. The front forks really are great, but with out a front hugger or even brake calipers it just looks wrong, like there is a big chunk missing from the front of the model. Then we come to the windscreen, which is a soft piece of fogged up plastic film that fits so badly, it is a wonder it was ever signed off by the Ducati engineers! The V-4 engine and working gear box do nothing simply because you cannot see them, rendering the visual impact of the moving engine parts pointless. The final drive for the fake motor from the rear wheel is by a little white elastic band which to my view is a bit disappointing. Then came my biggest bugbear of all. The sheer number of stickers the builder needs to attach. I will make no secret of the fact that I thoroughly hate stickers on Lego parts for the following reasons. Firstly, they can be an absolute bastard to fit accurately. Secondly, they tend to peel off over time or lift a corner and get furry with dust which makes them look even worse. Finally, heavily stickered up pieces prevent you from using the pieces in other MOC constructions. At least with printed pieces, the final model actually looks great for display, even if you cannot use the printed parts elsewhere. Stickers are just a massive pain in the arse and some of the stickers on this set are tiny, so I refused to fit them, meaning that the final model looks a bit flat and dull. Yes, this is my fault for not using the stickers, but we get onto a circular argument here.

With the model finished and sat on my desk, I was, I have to admit, feeling a little disappointed. Then it fell over. Unlike other Technic bikes that have gone before, this bike has no side stand. Instead it comes with a paddock stand, which does not fit well or work properly. The finished model is so unstable that it has to be balanced just right to stop it falling over, meaning that it is also not a good model for display for both the practical and aesthetic reasons. The handle bars are designed to look like real clip on bars, they are very prettily done and there is even a brake fluid reservoir for the front brake… But no brake lever. Similarly, the rear fluid reservoir is present, but again, no brake pedal. Yes, I know that these are small points to make, but when the designer has gone to the effort to add tiny details, why omit the actual main bits that require the small details?
Sadly, this model is deeply flawed and the front screen is the final insult. This scrap of plastic film is held in place by two bright red Ninjago swords, leaving a five millimetre gap on either side. No matter what I tried, I could not get it to sit nicely and the foggy plastic looked awful anyway. The under engine exhaust gets a similar lacklustre treatment and the huge double bend pipe work looks out of scale. The real shame here is that the actual front fairing of this model is a thing of beauty that looks suitably menacing. But with the lack of front guard below and the pathetic screen above, it ends up looking like a nasty custom from a bad biker build off show. There was so much potential for this model to be amazing and Lego seemed to cut too many corners with the final result. For example, the front disk rotors are beautifully designed, but why are they moulded in standard light stone grey? They should have been done in a beautiful pearl silver. The bad screen is simply unforgivable, but there is a fix to this and it involves a clear plastic bottle, a pair of scissors and fifteen minutes to get it to sit just right! The useless paddock stand is annoying and having built my own in the past for custom models, I know how much easier they are to make.
What about the bikes that came before this one? To be honest, the not quite a Triumph Street Triple is still my favourite. It is so clearly a model of the Triumph modern classic, one has to ask why it did not have an official endorsement, especially given that it was and remains one of the most beautiful motorbikes in the Technic range. It also comes with some printed pieces too, making the final model even more beautiful.

The big BMW GS1200 is an ugly brute of a bike in reality, but the Lego model of it is fabulous with the unique telelever suspension and huge pannier boxes... even if the flat twin engine is a bit lame looking with a huge gap between cylinder and head.

The truth is that no Technic motorbike will ever be perfect, although the Street triple does come very close. Compared to these, the Ducati feels like a rushed and unfinished model, which is a real shame given (and I say this a dedicated Suzuki owner) the absolute beauty of the real thing.
So, what can I do next with this bloody thing, it’s not like I can chuck a motor on it and set it off across the car park like I can do with the Corvette they released this year, is it? Wellllllll…. It would be rude not to try and this has been for a while now, an on going project for me to build an actual working Lego Motorbike, running on Technic Power functions kit. To date and prior to this new Ducati, I have had a single working prototype model that was able to ride and steer just like a real motorcycle. A moving weighted brick causes the bike to lean over, which steers the bike. As the weight moves back, the bike stands up again and continues in a straight line. It is not yet perfect and I have lost it under a couple of cars as I experiment. I tried to modify the Ducati chassis to accept this steering and drive set up of a pair of motors and a battery pack and the result was more ugly than me with a post migraine hangover, having woken up with my head covered in drool!

Sadly, the chain drive could not deliver the power needed to spin the wheel fast enough with enough torque to propel the bike, so I had to resort to a shaft drive on both sides of the wheel replacing the swing arm. By the time I was finished, the final bike looked like a cheap Fake Lego rip off and when I tested it on the smooth tarmac of the car park, it fell over after moving less than a foot!
So that is it for me. I give up. I have tried time and time again and I simply cannot make a working model Ducati motorcycle using Power Functions. If you look on You Tube, others have made working models and I have no idea how they have done it. One person has used a Buwhizz unit, which over volts the motors giving the bike a real blast of speed. But for those of you with a Physics mind, the way a bike works is super intricate and has nothing at all to do with centrifugal force (yes, I am aware that this is a misnomer, but it has been used for decades to explain a complicated process). Do go and look up how motorbikes steer and balance because the in-depth science of it is fascinating. No really, it is fantastic and for years I have thought so wrongly about how it all works. In the mean time, if any of you out there can figure out how to make a Power Functions controlled motorbike, I shall take my hat off to you. You are clearly a better builder than I.
youtube
youtube
#Ducati#lego technic#motorcycles#afol#Lego Group#Model motorbikes#Power Functions#Lego motorbikes#triumph street triple r#BMW 1200 GS#Lego MOC#Lego builder#Adult builder of Lego
1 note
·
View note
Text
The MMR Vaccine: The Inside Scoop 🍨
You probably all know the story by now: the one about how Andrew Wakefield, now exposed as a fraud but at that time a British physician, published a 1998 paper suggesting that the MMR vaccine was associated with autism. As a medical student in my last year, I’ve heard and read this story in all of its iterations. Frankly, I’m tired of talking about it. It frustrates me that Wakefield and his corrupt “research” still dominates the discussion of MMR, so much so that if you search “MMR vaccine” in PubMed, the first search results still are talking about autism over two decades later. I wanted to actually learn why we get the MMR vaccine, what it does instead of what it doesn’t do (for anyone still not sure at this point, I doubt I’ll change your mind, but here goes: MMR doesn’t cause autism). Are you curious, too? Cool. Play with me in this space for a few minutes.
The MMR vaccine was put together from existing immunizations in 1971 by Maurice Hilleman, who also made over 40 other vaccines; the guy’s like a real life Dr. Crusher in Star Trek. In the last decade alone, it has prevented around 25 million deaths worldwide. Now you might ask, as I did, wait, how do you die from measles or mumps? Didn’t those used to be common childhood diseases? And you’d be right; they did! Usually kids end up with a rash (measles, rubella) or cheek swelling (mumps) and feel crappy, and then they’d get better. However, measles and mumps can sometimes cause encephalitis, meaning the infection spreads to the brain. That’s the part that can be fatal. Measles can also cause a rarer type of encephalitis 7-10 years after the infection called subacute sclerosis panencephalitis, and SSP is universally fatal. All of this is rare, mind you. But there are 73 million kids in the US, meaning that even though brain manifestations of these diseases are about 1/1000, 73,000 kids would develop these dangerous conditions. For context, 73,000 would be like if the whole city of Alameda wound up in the hospital with brain infections. Encephalitis prevention is the main reason we need the MMR vaccine, and the reason it alone has prevented literally millions of deaths.
So what’s up with the R? Rubella is generally mild, but can cause devastating fetal damage if a pregnant person catches it. The fetus can have heart malformations, congenital cataracts, deafness, and other health problems. That’s why rubella gets included in the MMR vaccine. Rubella has also been declared eliminated in the US, so hopefully you never see it.
Now, the part you’ve been waiting for: the side effects. The real, actual side effects of MMR. Well first of all, don’t get the MMR vaccine while you’re pregnant! Hopefully you were immunized as a child, but if you are pregnant now and interested, the rubella in the vaccine could cause those fetal anomalies I just talked about, so hold your horses until after the delivery. Otherwise, the side effects are…not very exciting. Some people get a fever after the immunization. Some get a rash, or joint pain, or swelling of their lymph nodes, none of which lasts very long. If you’ve gotten your COVID vaccine, you know the deal. One scary-looking but benign side effect is that the MMR increases the risk of febrile seizures from about 6-14 days post-vaccine. That means if your child gets the MMR and then a kid at daycare gets them sick, they could have a seizure. However, febrile seizures are not associated with developing epilepsy or other seizure disorders, and at baseline between 2% and 5% of children have a febrile seizure unrelated to the MMR vaccine during childhood. Finally, there is a low risk of developing a temporary platelet disorder called ITP after the vaccine. However, measles, mumps, and rubella are more likely to cause ITP than the vaccine, so the vaccine actually lowers the rate of ITP.
If you want to know more about measles, mumps, or rubella themselves as diseases, the CDC has some great free information about them. I hope this post makes plain the risk/benefit calculus of the MMR vaccine, so you can make an educated choice about it. If you liked this MMR run-down, follow me on Twitter @almost_beck for smaller chunks of health info, and follow this blog for more vaccine-related deep dives. I’ve been amaryllist, and ~this was your Inside Scoop~
0 notes
Text
Also preserved in our archive
From July 2022. Still holds true.
by Hannah Thomasy
Even mild COVID can do serious damage to the lungs, heart, and brain.
The vast majority of COVID-19 cases are mild or asymptomatic; many people will spend a week or two at most with a headache, sore throat, coughing, and maybe a fever. Because of that — and because everyone in the U.S. can now get vaccinated, which greatly reduces the chances of having a severe COVID case — many people are returning to life as normal, despite a recent surge in cases caused by the new Omicron BA.5 subvariant. But a mild case can be misleading, because once the initial infection subsides, you may not be in the clear. Long COVID, with symptoms that last months or even years, occurs in some people with mild cases, and even in those who were initially asymptomatic. And it can do serious damage to the heart, brain, and lungs.
Estimates on the prevalence of long COVID are hugely variable, from 2.3% of cases to more than half of cases. Some of this variation may have to do with differences in the populations studied and how exactly long COVID is defined (which symptoms are assessed and the time elapsed since the initial illness). Severity of symptoms can also vary widely between people. Although some people might be bothered by a persistent cough, others have symptoms so severe that they’re unable to return to work.
“This syndrome has maybe half a dozen different monikers — post-COVID, long COVID, long haulers, post-acute sequelae of COVID — and I think that in many ways reflects the heterogeneity of the presentation. And also reflects, frankly, the lack of consensus as to what's actually going on here,” says Roger McIntyre, M.D., a professor of psychiatry and pharmacology at the University of Toronto.
In an attempt to learn more about this condition — and eventually figure out how to treat it — researchers are investigating how mild COVID infections can go on to have serious impacts on major organ systems such as the lungs, heart, and brain. Here’s what we know so far.
Impact of Mild COVID on the Lungs COVID is well-known for its ability to cause severe lung damage in the short-term in people with more severe cases. But even mild COVID can do long-lasting damage to the lungs. In a study of self-reported long-haulers (the majority of whom were not initially hospitalized for the disease), nearly 80% reported persistent shortness of breath.
Physical abnormalities in the lungs have been noted as well. A study of 67 people with persistent symptoms who had not been hospitalized from COVID used CT scans to measure air trapping in the lungs. Air trapping is, as the name suggests, when air gets trapped in the lungs — meaning the person is unable to breath out fully. This can indicate dysfunction or inflammation in the small airways of the lung. The study found that more than half of patients had air trapping. On average, air trapping affected about 25% of the total lung.
Scientists emphasize that more research will be needed to determine whether these results hold true for people infected with more recent variants like Omicron and whether these changes are permanent or reversible.
At this point, it’s also unclear how to treat or prevent post-COVID lung abnormalities.
Impact of Mild COVID on the Heart Mild cases of COVID can also cause long-term damage to the cardiovascular system. Anecdotal reports of this began to appear less than a year into the pandemic, and a large-scale study published earlier this year confirmed early fears. The study, which included more than 150,000 people who had tested positive for COVID, found substantially elevated risk for more than a dozen kinds of heart and vascular disorders over the year following initial infection compared to people who had not had COVID.
Though these disorders were more common in people who had severe COVID, people who were not hospitalized still had increased risk for most of the conditions studied. For example, people who had not been hospitalized with COVID had a 23% increased risk of stroke, a 37% increased risk of heart failure, and a 50% increased risk of inflammatory heart disease.
“It’s very, very clear this is happening even in people who did not have severe disease,” says Ziyad Al-Aly, M.D., lead author of the study, director of the Clinical Epidemiology Center at Washington University in St. Louis, and the Chief of Research and Education Service at the Veterans Affairs St. Louis Health Care System.
Just because someone doesn’t get long COVID symptoms from the first infection, doesn’t mean they won’t develop it during a second or third infection, Al-Aly says. With each new infection, “you’re playing Russian roulette again.”
Currently, patients with post-COVID cardiovascular problems are treated based on their symptoms, Al-Aly says. A patient with arrhythmia after COVID, for example, would be treated in the same way as any other patient with arrhythmia. But understanding exactly how the virus continues to affect the heart and blood vessels for months after the initial infection is important for the development of more effective treatments.
Although there are several hypotheses about how this long-tern damage could be occurring, Al-Aly says that one possibility is that the virus, or even just viral fragments, hides in various tissues in the body long after the acute phase of the infection. “Those fragments could continue to irritate the immune system and produce something called low grade chronic inflammation that may in turn produce organ damage,” he says.
If this is the case, treatments, including antivirals, that help people clear the virus might help prevent long-term effects, he says. Although there have been a few anecdotal reports of long COVID symptoms improving after antiviral treatment or vaccination, these still need to be tested in clinical trials.
Impact of Mild COVID on the Brain Estimates of the prevalence of cognitive problems after mild COVID vary. One study found that 1.2% of people reported memory problems three to four months after illness, but another study found memory problems in almost 16% at roughly the same time point. “Brain fog,” a non-medical term generally concerned with difficulties related to attention and memory, was reported by more than 80% of people with long COVID, according to one study.
Brain fog and cognitive problems, along with fatigue, are some of the most common symptoms of long COVID, says McIntyre. They also have some of the largest impacts on quality of life. McIntyre says he’s even seen these symptoms in patients whose initial infections were asymptomatic.
But doctors are seeing much more than just brain fog. People with long COVID report an incredibly wide array of neuropsychiatric symptoms, including anxiety, depression, dizziness, insomnia, confusion, short- and long-term memory loss, and difficulty with verbal communication.
Because of the variation between people in brain structure, cognition, and baseline risk for neuropsychiatric disorders — and because most people aren’t being tested before their infections — it can be difficult to tell which differences are actually due to COVID. Luckily, long-term biomedical data collection projects such as the UK Biobank allow this kind of before-and-after analysis, at least in terms of brain structure. Using the Biobank data, researchers analyzed brain scans of hundreds of people who had been scanned before and after COVID and compared them with non-infected people who had two scans over similar time periods.
What they found is concerning: People who had recovered from COVID (and who were not hospitalized) had greater reductions in overall brain volume, as well as greater reductions in grey matter thickness in regions of the brain related to smell.
On average, the second scan occurred about 5 months after the person was diagnosed with COVID. Further research is needed to determine whether this damage is permanent or not.
McIntyre says it’s important to figure out exactly how COVID infections result in organ damage. Right now, there are a lot of possibilities for how the virus might damage the brain. Like those in the lungs, cells in the brain have the ACE2 receptor, which the virus uses to enter cells. So one hypothesis, he says, is that the virus is infecting brain cells, causing toxicity over time.
“Secondly, it could be friendly fire. In other words, your own immune system, in the process of tackling the virus, could inadvertently be causing collateral damage,” he says.
“Thirdly, a lot of people believe the reason why you're seeing brain changes is because there's very, very small blood vessel disease, because the blood vessels get affected by COVID,” he says, “and the tiny blood vessels in the brain are getting blocked, and that's what's leading to the problem.”
Antiviral and immune-modulating drugs are being considered for the treatment of long COVID in general, McIntyre says. He himself is running a study on whether an antidepressant called vortioxetine, which has been shown to improve cognitive function in people with depression, might help improve cognition and quality of life in those with long COVID.
But there’s a long way to go before scientists fully understand this complex disease, let alone develop effective therapies.
In the meantime, the best way to avoid long COVID is to avoid getting COVID in the first place: wear a well-fitting mask, practice physical distancing where possible, and avoid crowded indoor spaces. This is equally important if you’ve already had COVID; just because you didn’t get long COVID before doesn’t mean you’ll necessarily get lucky a second time.
#mask up#public health#wear a mask#pandemic#covid#wear a respirator#covid 19#still coviding#coronavirus#sars cov 2#long covid
55 notes
·
View notes
Text
so my modest hobby lately has been bouncing around, and finding the person that still insists, “covid is a flu.”
Because it is so damaging and heinous right now. It’s like saying, “If you take the cartridge out of a gun, it’s a perfectly safe tool to do whatever with.”
Guns are not safe, loaded or otherwise. You handle every fuking gun like its loaded and could go off.
Covid is not the flu, it’s barely a respiratory disease. Do you understand what i am saying? Covid is no more a flu than Polio was a stomach virus. Most people that contracted Polio developed a cycle of the shits, not everyone (child or adult) developed the paralytic properties associated with Polio Picornavirales. However, paralysis could still beat them down later in life because the virus presence had, to some amount, damaged the spinal nerves.
Polio was less transmissible and did not have a high fatality rate - a 5%-15% depending on the healthcare. But it had the potential to fuck you up.
So what I do with these ignorant people, I give them a fuck ton of links to the medical libraries that publish information on findings regarding covid. The inks consist of complex medical information regarding medications to prescribe, tests to conduct on the infected - biopsies and aspiration of bonemarrow - A LOT OF INFORMATION. And it is A LOT OF TECHNICAL information regarding the case studies and tests, about half will be intelligible because the terminology is meant for doctors working in microbiology; it deals with medical therapies and treats post recovery, and ongoing out of clinic therapies.
That’s what doing your “own research” is about. Finding that information.
And what are these bimbos going to argue? How do you argue with the published findings of the medical community - this stuff isn’t sitting here for shits and giggles (hey, pun!). This materials is open and available, so that doctors have the best, most up-to-date information on mitigating the damages of covid virus infection.
Something I want to also put out there, in a source of information I found quite damning - I need to find it, but I linked it somewhere. It was found in some patients who contracted covid, some of these asymptomatics, that covid cells entirely bypassed the alveoli tissue of the lungs, and went straight into the vascular system. Brief recap, the vascular system - or endothelial tissue, is where covid wants to be. That, and the red blood cells. I still haven’t determined through research if covid is murdering red blood cells, but generally, doctors site covid as a virus which attacks the endothelial tissue of the vascular system. This in turn causes the systemic reactions from other organs of the body. Just as Polio can pass from the intestinal lining and reach through lymp glands, in turn reaching the central neuron system - so does covid cells insert itself into the vascular tissue, from there reaching the heart and in some cases the brain.
The worst aspect of covid, is that you can endure a week to a month, before the infected might present classic flu symptoms. Now recap VERY IMPORTANT EBOLA can present flu symptoms before that fucking murders your ass.
However, Ebola is a bitch and kills its host carrier. Thankfully.
When covid does its job right, the host carrier will not know it is there. It will evade the immune system and begin replicating itself in the endothelial tissue, but this in turn wrecks havoc on the body - it induces silent hypoxia (lack of oxygen to tissues, including the brain), if the virus has replicated enough but the body recognizes its business as a threat, then the infected will develop a cytokine storm (basically the body killing itself in its efforts to purge a virus). This is why the vaccine has been so important to millions, to prevent the silent invasion and subsequent damage of this gentle killer.
Covid can SOMETIMES present like a common rhino virus, but that is not necessarily a good thing. It only indicates that in those who test positive for covid, have the virus in them, and who knows for how long? Collecting more covid cells and exacerbating the condition is more likely, since the body becomes inadequate with purging or healing from an ongoing infection. Covid has an easier time infecting red blood cells carrying CO2 (link). The higher the CO2 levels of the body as caused by present infection, the increased rate of infection from the virus.
All of that is aside from the point, since it is impossible to determine when a person is infected (POI). Since when covid begins its work, it is typically in silence. There is no one out there going - “My nitrogen levels are high today” or “Hmm, this place has a lot of cabon monoxide.” There is the opportunity to contract a “cold presenting covid infection”, but there is no indication if the virus is present anywhere else in the body.
Simply put, it can infect the mucosa, the alveoli, the mucous membrane - but in the case of covid, there is no assurance it stops there. Because, as put, covid wants to infect the endothelial tissue of the vascular system. And from there comes the shortness of breath, lethargy, muscles and joint aches (due to poor aeration of carbon dioxide and oxygen exchange).
And the body reacts the same way it does under the threat of any viral invasion, whether it is meningitis, the flu, ebola, diptheria, hanta - whatever. A fever to manage and control the viral cells spread and reduce the count, attack the cells rooted in the mucosa and mucous membrane, and coughing to remove accumulations of damaged-dead cells.
In the case of covid and the cytokine storm, this is the same response of the body struggling to purge out damaged or infected cells. However, due to some organs such as renal and kidneys taking on covid cells, the body has a nasty habit of unintentionally killng, or maiming, those cells in the process. Which in turn fucks up the host carrier.
People, most notably the maga crowd, celebrate this virus because it can go undetected. It can live and thrive in the endothelial layers, and from there spread to dozens or hundreds. This aspect of the virus is something to monitor and be wary of, since these individuals insist on infecting themselves with the virus and over and over.
Its equivalent to becoming a smoking addict. Not entirely harmful at first in moderation, but the long-term affects we are uncertain of today.
But that is where we are. People continuing to use influenza as a measuring guide inaccurately. If people insist on using some contagion as a guide to its properties and affects, they are better of saying, “It’s a little Ebola” or “It’s a mild case of Polio” Because covid has far more in common with these viral invaders, than it does with an upper respiratory infection. And once more I say, covid is far detached from anything ‘respiratory’. It can form symptoms of acute respiratory distress, but the virus is not and never will be only isolated to the trachea or lung tissue. Covid goes to and infects whatever it can find in the vascular system, and there is no excuse for this ignorance people insist on promoting.
0 notes
Text
Iodine Pentafluoride Formula Benefits
Iodine Pentafluoride (IPF) is an organic compound with an organic base composition IF%, erythrogen, erythrocyclomethanes (EM), and fluoro-dihydro-lactone (DFLL). It is one of the five known fluorides of iodine. It's a transparent yellow liquid, although sometimes impure solutions appear green. It's commonly used as a topical irritant and as a fluorescent dye in various medical applications. Iodine Pentafluoride Formula Research Reports
Iodine Pentafluoride has recently been tested in cultured human breast cancer cells and showed good results - both in terms of increasing proliferation and in terms of achieving stable colonies. Other studies have indicated that iodine pentafluoride formula may also be effective in treating thyroid disorders, diabetes, Parkinson's disease, multiple sclerosis, and cirrhosis. Currently, there are no approved medicinal uses for iodine pentafluoride.
https://www.reportmines.com/cryptocurrency-exchanges-market-in-china-r185191
https://www.reportmines.com/cryptocurrency-exchanges-market-in-us-r185192
Iodine Pentafluoride, together with iodine sulfate, forms a compound called ITP (Inorganic Tetraphenyl ether). The compound has been shown to be free of all known side effects. It was also shown to increase the proliferation and diameter of the human breast cells (breast cancer cells).
Iodine is a crucial element in a number of processes. Without iodine, many bodily functions cannot occur. Iodine is needed for the production of proteins, carbohydrates, fat, vitamins and certain enzymes. Many people do not get enough iodine, either because they are unable to tolerate the taste of iodine or because they are intolerant to it. A special iodine supplement can help overcome these difficulties.
Iodine deficiency can result in many physical problems, such as the inability to produce red blood cells, and hemoglobin. Iodine deficiency also plays a large role in causing the skin to thicken. When people do not get enough iodine in their diet, they can become pale, flaky, and wrinkled. This effect is most extreme during times of iodine deficiency, such as during menstruation. Other symptoms include: dry skin, excessive hair loss, decreased energy levels, and dry brittle nails.
An iodine pentafluoride formula research can be very effective for treating iodine deficiency. The iodine supplements in the formula must contain a very high concentration of iodine. This way, the medication will be absorbed into the body very quickly. There are a variety of iodine supplement formulas on the market. Some iodine formulas can be used for treating specific symptoms, while some are made for general use.
Some iodine supplements have been shown to help prevent certain types of thyroid diseases and cancers. In some cases, iodine pentafluoride has also been shown to lessen the effects of strokes and brain damage caused by exposure to ionizing radiation. Because all of us are exposed to radiation on a daily basis, it is important that we know how to effectively use iodine when we need it. By taking an iodine supplement on a regular basis, we can help to protect our bodies against iodine deficiency and its negative health effects. The iodine supplement solution provided through natural health products is an easy, effective way to get the iodine that our bodies need.
https://www.reportmines.com/cryptocurrency-exchanges-market-in-japan-r185193
https://www.reportmines.com/cryptocurrency-exchanges-market-in-south-korea-r185194
https://www.reportmines.com/cryptocurrency-exchanges-market-in-india-r185195
Iodine is essential to the proper function of human growth and development. Without iodine, children are more prone to iodine deficiency and brain damage. Adults can also benefit from the use of iodine supplement solutions. By taking an iodine supplement solution containing the proper amounts of iodine, we can help to maintain our bodies' iodine supply.
One of the most common complications associated with iodine deficiency is the skin disorder iodine dermatitis. If this is not treated, it can become serious and even lead to death. Iodine helps to fight against iodine deficiency by boosting the immune system, as well as fighting the infection that can cause lesions and complications such as this.
Studies show that pregnant women who took a regular iodine mineral dietary regimen had a significant reduction in their chances of suffering from complications related to iodine deficiency. Iodine deficiency can also lead to the skin condition known as hypothyroidism. Pregnant women can greatly benefit from using an iodine mineral dietary formula. Iodine is found in many fruits and vegetables, and we get enough iodine in our diets. For those of us who do not get enough iodine in our diets, a dietary iodine supplement can be very beneficial. This is one of the reasons why pregnant women should use an iodine supplement formula to ensure that they are getting enough iodine in their bodies.
People of all ages should be taking iodine mineral supplements on a regular basis. Iodine deficiency is no joking matter. If you think that taking iodine supplements is just something for the elderly or people with thyroid problems, then think again. The risk for iodine deficiency continues to grow rapidly. As people get older, they tend to produce less of the iodine needed. Iodine Pentafluoride Formula is one way to ensure that you are getting the iodine needed to keep your body functioning properly.
Summary
At the time of this report, the official counts of cases and deaths from COVID-19 have passed 4,000,000 and 280,000. Many government announced a plan on reopening the national economy, but many countries are still at the stage of rising. It should be noted that the impact of the epidemic has accelerated the trend of localization, regionalization and decentralization of the global industrial chain and supply chain, so it is inevitable to reconstruct the global industrial chain. Faced with the global industrial change in the post epidemic era, enterprises in various countries must take precautions.
Chemical and petrochemical-related industries have been noticing the adverse effects of the COVID-19 outbreak. They are in the midst of a two-pronged crisis, besides the impact of COVID-19, another is the oil price war. Oil prices are dropping due to failed agreements on production cuts between OPEC and Russia in April and the need for chemicals and refined products is slowing from industrial slow-downs and travel restrictions in the wake of this global pandemic.
The chemical industry plays an important role in the production of countless products such as plastic, fertilizers, medicines, packaging products, etc., with the spread of coronavirus, many production facilities of several downstream industries have been halted. However, a rise in the demand for packaging materials has been increased to prevent the contamination of food, medicine, personal care, and medical products thereby creating a significant demand for chemicals involved in the packaging industry.
In such an environment, XYZ-research published a comprehensive analysis of key market trends in global Iodine Pentafluoride (IF5) 3160 market. It includes discussion on historical trends, current market status, competitive landscape, growth opportunities and challenges which are backed by factful feedbacks.
According to XYZResearch analysis, Iodine Pentafluoride (IF5) market will reach xx Million USD by the end of 2020, with a CAGR of xx % during the forecast period of 2021-2026, The XX segment in Iodine Pentafluoride (IF5) market is estimated to reach a market value of xx Million USD by 2020 from an initial market value of xx Million USD in 2019. China market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is xx. US market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is xx. Europe market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is XX.
Regional Segmentation (Value; Revenue, USD Million, 2015 - 2026) of Iodine Pentafluoride (IF5) Market by XYZResearch Include
China
EU
USA
Japan
India
Southeast Asia
South America
Competitive Analysis; Who are the Major Players in Iodine Pentafluoride (IF5) Market?
Solvay
Air Liquide
ABCR GmBR Co
Air Products
Honeywell
Shandong Zhongfu Chemical
Juhua Group
Shanghai 3F New Material
Major Type of Iodine Pentafluoride (IF5) Covered in XYZResearch report:
Purity 99.5%
Purity 99.0%
Other
Application Segments Covered in XYZResearch Market
Non-Aqueous System Battery
Organic Fluoride
Inorganic Fluoride
For any other requirements, please feel free to contact us and we will provide you customized report.
Frequently Asked QuestionsWhat is the USP of the report?
Post-pandemic Era-Global Iodine Pentafluoride Market report offers great insights of the market and consumer data and their interpretation through various figures and graphs. Report has embedded global market and regional market deep analysis through various research methodologies. The report also offers great competitor analysis of the industries and highlights the key aspect of their business like success stories, market development and growth rate.
What are the key content of the report?What are the value propositions and opportunities offered in this market research report?Related Reports
Post-pandemic Era-Global Iodine Pentafluoride Market
Post-pandemic Era-Global Iodine Pentafluoride Market
Contact us: https://www.reportmines.com/contact-us.php
0 notes
Link
Scientists are becoming more and more concerned with the emergence of a syndrome termed “long COVID”, where a significant percentage of sufferers of COVID-19 experience long-lasting symptoms.
Studies suggest symptoms remain for approximately five-24 percent of confirmed COVID cases, at least three to four months after infection.
The risk of long COVID is no longer thought to be directly linked with either age or the initial severity of the COVID illness. So younger people, and people with initially mild COVID, can still develop long-COVID symptoms.
Some long-COVID symptoms begin quickly and persist, whereas others appear well after the initial infection has passed.
Symptoms include extreme fatigue and ongoing breathing complications.
What particularly concerns us as neuroscientists is that many long COVID sufferers report difficulties with attention and planning — known as “brain fog”.
So how does COVID affect the brain? Here’s what we know so far.
How does the virus get to our brains?
There’s evidence connecting respiratory viruses, including influenza, with brain dysfunction. In records of the 1918 Spanish flu pandemic, reports abound of dementia, cognitive decline, and difficulties with movement and sleep.
Evidence from the SARS outbreak in 2002 and the MERS outbreak in 2012 suggest these infections caused roughly 15-20 percent of recovered people to experience depression, anxiety, memory difficulties and fatigue.
There’s no conclusive evidence the SARS-CoV-2 virus, which causes COVID, can penetrate the blood brain barrier, which usually protects the brain from large and dangerous blood-borne molecules entering from the bloodstream.
But there’s data suggesting it may “hitchhike” into the brain by way of nerves that connect our noses to our brains.
Researchers suspect this because in many infected adults, the genetic material of the virus was found in the part of the nose that initiates the process of smell — coinciding with the loss of smell experienced by people with COVID.
How does COVID damage the brain?
These nasal sensory cells connect to an area of the brain known as the “limbic system”, which is involved in emotion, learning and memory.
In a UK-based study released as a pre-print online in June, researchers compared brain images taken of people before and after exposure to COVID. They showed parts of the limbic system had decreased in size compared to people not infected. This could signal a future vulnerability to brain diseases and may play a role in the emergence of long-COVID symptoms.
COVID could also indirectly affect the brain. The virus can damage blood vessels and cause either bleeding or blockages resulting in the disruption of blood, oxygen, or nutrient supply to the brain, particularly to areas responsible for problem-solving.
The virus also activates the immune system, and in some people, this triggers the production of toxic molecules which can reduce brain function.
Although research on this is still emerging, the effects of COVID on nerves that control gut function should also be considered. This may impact digestion and the health and composition of gut bacteria, which are known to influence the function of the brain.
The virus could also compromise the function of the pituitary gland. The pituitary gland, often known as the “master gland”, regulates hormone production. This includes cortisol, which governs our response to stress. When cortisol is deficient, this may contribute to long-term fatigue.
This was a recognised phenomenon in patients who were diagnosed with SARS, and in a disturbing parallel with COVID, people’s symptoms continued for up to one year after infection.
Given the already significant contribution of brain disorders to the global burden of disability, the potential impact of long COVID on public health is enormous.
There are major unanswered questions about long COVID which require investigating, including how the disease takes hold, what the risk factors might be and the range of outcomes, as well as the best way to treat it.
It’s crucial we begin to understand what causes the wide variation in symptoms. This could be many factors, including the viral strain, severity of the infection, the effect of pre-existing disease, age and vaccination status, or even the physical and psychological supports provided from the start of the disease.
While there are many questions about long COVID, there’s certainty about one thing: we need to continue doing everything we can to prevent escalating COVID cases, including getting vaccinated as soon as you’re eligible.
Trevor Kilpatrick, Professor, Neurologist and Clinical Director, Florey Institute of Neuroscience and Mental Health and Steven Petrou, Professor and Director, Florey Institute of Neuroscience and Mental Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
source https://www.firstpost.com/health/explainer-what-we-know-about-post-recovery-symptoms-associated-with-long-covid-9878731.html
0 notes
Text
Tinnitus & Covid-19 Vaccine Side Effects
New Post has been published on https://thebestsolution4u.com/tinnitus-covid-19-vaccine-side-effects/
Tinnitus & Covid-19 Vaccine Side Effects
Tinnitus, Covid-19, & Covid-19 Vaccine Side Effects
COVID and Tinnitus. I’m going share my thoughts on how both COVID and the COVID vaccines might impact the severity of tinnitus. So, question number one. Can COVID, can having Coronavirus cause tinnitus. There is an article called Changes in Tinnitus Experiences During the COVID-19 Pandemic.
Tinnitus, Covid-19, & Covid-19 Vaccine Side Effects
This is from frontiers in public health. This was released in 2020 and this article surveyed 3,100 people and 237 of the respondents reported that they had suffered Coronavirus symptoms and among that smaller group who had suffered Coronavirus symptoms, about 40% said that their symptoms of Tinnitus had worsened.
So, there seems to be some relationship with having the experience of COVID getting Coronavirus, the symptoms that come with that and then how that can change the perception of tinnitus. So, that has been noted in the medical research. and why is that?
Well COVID itself Coronavirus can potentially cause infection of the nerves of our nervous system that connect the senses into the spine, the senses into the brain. So, COVID itself can potentially cause infection of the nerves, autoimmune damage.
Read more: Tinnitus, Hearing Loss, and Coronavirus
The function of our autoimmune system can be damaged and then potentially blood clots changes to the cardiovascular system. I’m sure from your research, you’ve learned that tinnitus as a symptom is quite sensitive, meaning that changes to our psychology, changes to our body, getting sick, it can trigger tinnitus, it can even bring it from I never heard tinnitus or barely heard it at all to this is a dominating force in my life.
Additionally, getting sick or having some other change in life can bring on an increase in loudness of tinnitus. So, the findings from that study where they surveyed thousands of people and out of those who had COVID they realized that about 40% said that their symptoms of tinnitus had worsened. Meaning they already had it and it temporarily changed. Did not stay permanently changed, but it did change.
So, those findings were preliminary and they relied mainly on patient questionnaires so, there’s possibly some overestimates. Other viral infections, measles, CMV, other similar viral infections they can cause hearing problems.
So, there is some link between certain viruses and how that can affect the hearing system particularly the cochlea, the hearing organ and the hearing nerve. It’s rather complicated. It’s rather sophisticated as an audiologist.
What I need to know is, okay these potential viruses can affect hearing and that might cause temporary changes in tinnitus or that might change hearing in a more permanent level. Other factors that are important to discuss here are that, think about what are the symptoms of getting COVID?
well, fever, congestion, headache, stress, a significant amount of anxiety for in fear of losing our life or the life of our loved ones. Now, if COVID causes those symptoms and those side effects then is the tinnitus caused by those symptoms?
Or is the tinnitus caused by the virus directly? Very hard to say. In some cases we won’t be able to know directly but it’s certainly evident that having a fever, getting sick, being congested, having a headache, being under high periods of stress and high periods of anxiety, that can change the tinnitus perception of either making it louder if we already had it. Some people would call that a tinnitus spike or it can potentially create tinnitus where previously you didn’t hear it at all, or maybe slightly here and there, but then suddenly it’s a symptom.
It’s a sound that’s constantly in our experience. And maybe some of you who are watching this can relate to that. The second sub-question about COVID is the COVID vaccine. This is quite interesting how tinnitus as a health condition, as a symptom, the virus itself can affect tinnitus and the vaccine which prevents the virus can also affect tinnitus.
It’s pretty unique in that regard. So, can the COVID vaccine cause tinnitus or make it worse? There was a study in the United Kingdom, in England that looked at the side effects from vaccine for the Pfizer and the AstraZeneca vaccines.
So, 20 million doses of those vaccines were administered during this period, and they have a system called the Yellow Card reporting system, where individuals can report their side effects and they’re encouraged to report side effects whatever side effects come from these vaccines Because these vaccines are so new, there’s been no vaccine in history that’s been released to the public so quickly, about one year, less than a year it’s been, created, tested, produced, manufactured, released.
So, in a way we’re all part of this clinical trial because this process much more expedited than typical vaccines, as you are probably aware of. So, 20 million doses were administered in England during this time period and a total of 116,000 Yellow Card reporting adverse effects were reported to the group.
And out of those, a total of 780 individuals reported tinnitus. Whether they had tinnitus as a side-effect or their tinnitus change significantly as a side effect. So, from that research, from that article, from the government of England, they’re saying which is the equivalent of our CDC, we’ll call it, in the US that fewer than one in 32,000 people are reporting tinnitus as a side effect of those major vaccines for COVID. So, that classifies the side effect as very rare.
That’s a good sign, Many people with tinnitus tell me, as I work via Zoom sessions with telehealth patients with tinnitus, they tell me all the time that , the last thing they can imagine is how are they going to live if their tinnitus gets worse? And I feel like that’s a common fear of, someone gets tinnitus they start to do everything in their power to help them or they’re thinking everything they’re doing in their power is to help their condition because they can’t live with it getting any worse.
Read more: Extremely Powerful Tinnitus Sound Therapy
They, they don’t want to be in that state. And of course, of course you don’t deserve to be in that state. No one does. So, rest assured the major vaccines have tinnitus as a side effect is a very rare phenomenon. Now, you may say, well this system relies on people reporting side effects. And that there could be many people who just didn’t choose to report the side effect. And that’s a very true point.
This is not perfect. In fact, none of us are perfect. I strive to do my best this research strives to do their best and so do you in getting better with tinnitus. So, this is the best information we have and hopefully this gives you some confidence that if you’re considering the pros and cons of getting the COVID vaccine, if tinnitus is a make or break, if you’re scared of getting the vaccine because it might affect your tinnitus that’s very low chance.
So, statistically, it’s very rare for that to happen to you. Feels good I was glad to learn that result. Yes, I do try to follow the research and stay evidence-based so, it’s even better when the evidence is actually helpful in saying that we don’t have to worry about that.
Read more: Silencil Natural Remedies For Tinnitus
0 notes
Text
Long COVID: Lasting effects of COVID-19 - Mayo Clinic - Published Aug 25, 2024
After any coronavirus disease 2019 (COVID-19) illness, no matter how serious, some people report that symptoms stay for months. This lingering illness has often been called long COVID or post-COVID-19 syndrome. You might hear it called long-haul COVID or post-acute sequelae of SARS-CoV-2 (PASC).
There is no universal definition of long COVID right now.
In the U.S., some experts have defined long COVID as a long-lasting, called chronic, condition triggered by the virus that causes COVID-19. (1p31) The medical term for this is an infection-associated chronic condition.
As researchers learn more about long COVID, this definition may change.
What are the most common symptoms of long COVID? In research studies, more than 200 symptoms have been linked to long COVID. Symptoms may stay the same over time, get worse, or go away and come back.
Common symptoms of long COVID include:
Extreme tiredness, especially after activity. Problems with memory, often called brain fog. A feeling of being lightheaded or dizzy. Problems with taste or smell. Other symptoms of long COVID include:
Sleep problems. Shortness of breath. Cough. Headache. Fast or irregular heartbeat. Digestion problems, such as loose stools, constipation or bloating. Some people with long COVID may have other illnesses. Diseases caused or made worse by long COVID include migraine, lung disease, autoimmune disease and chronic kidney disease.
Diseases that people may be diagnosed with due to long COVID include:
Heart disease. Mood disorders. Anxiety. Stroke or blood clots. Postural orthostatic tachycardia syndrome, also called POTS. Myalgic encephalomyelitis-chronic fatigue syndrome, also called ME-CFS. Mast cell activation syndrome. Fibromyalgia. Diabetes. Hyperlipidemia. People can get long COVID symptoms after catching the COVID-19 virus even if they never had COVID-19 symptoms. Also, long COVID symptoms can show up weeks or months after a person seems to have recovered.
And while the COVID-19 virus spreads from person to person, long COVID is not contagious and doesn't spread between people.
Why does COVID-19 cause ongoing health problems? Current research has found that long COVID is a chronic condition triggered by the virus that causes COVID-19. The medical term for this is an infection-associated chronic condition.
Researchers don't know exactly how COVID-19 causes long-term illness, but they have some ideas. Theories include:
The virus that causes COVID-19 upsets immune system communication. This could lead immune cells to mistake the body's own cells as a threat and react to them, called an autoimmune reaction. Having COVID-19 awakens viruses that haven't been cleared out of the body. The coronavirus infection upsets the gut's ecosystem. The virus may be able to survive in the gut and spread from there. The virus affects the cells that line blood vessels. The virus damages communication in the brain stem or a nerve that controls automatic functions in the body, called the vagus nerve. Because the virus that causes COVID-19 continues to change, researchers can't say how many people have been affected by long COVID. Some researchers have estimated that 10% to 35% of people who have had COVID-19 went on to have long COVID.
What are the risk factors for long COVID? Risk factors for long COVID are just starting to be known. In general, most research finds that long COVID is diagnosed more often in females of any age than in males. The long COVID risk also may be higher for people who have cardiovascular disease before getting sick.
Some research also shows that getting a COVID-19 vaccine may help prevent long COVID.
Many other factors may raise or lower your risk of long COVID, but research is still ongoing.
What should I do if I have long COVID symptoms? See a healthcare professional if you have long COVID symptoms. Part of long COVID's definition is symptoms that last for three months.
But at this time, no test can say whether you have long COVID. Since you may not have symptoms if you have an infection with the COVID-19 virus, you may not know you had it. Some people have mild symptoms and don't take a COVID-19 test. Others may have had COVID-19 before testing was common.
Long COVID symptoms may come and go or be constant. They also can start any time after you had COVID-19. But symptoms still need to be documented for at least three months in order for a health care professional to diagnose long COVID.
Healthcare professionals may treat your symptoms or conditions before a long COVID-19 diagnosis. And they may work to rule out other conditions over the time you start having symptoms.
Your healthcare team might do lab tests, such as a complete blood count or liver function test. You might have other tests or procedures, such as chest X-rays, based on your symptoms.
The information you give and any test results can help your healthcare professional come up with a treatment plan.
Care for long COVID It can be hard to get care for long COVID. Treatment may be delayed while you work with healthcare professionals. And people with long COVID may have their health problems dismissed by others, including healthcare professionals, family members or employers.
For people with cultural or language barriers, getting a long COVID diagnosis can be even harder. Pulling together information about symptoms and timing can be a challenge too. This is especially true when medical history is fragmented or when someone is managing symptoms related to memory or that affect the thought process.
Underdiagnosis may be more common among people who have less access to healthcare or who have limited financial resources.
If you're having long COVID symptoms, talk with your healthcare professional. It can help to have your medical records available before the appointment if you are starting to get care at a new medical office.
To prepare for your appointment, write down:
When your symptoms started and if they come and go. What makes your symptoms worse. How your symptoms affect your activities. Questions you have about your illness. List medicines and anything else you take, including nutrition supplements and pain medicine that you can get without a prescription. Some people find it helpful to bring a trusted person to the appointment to take notes.
Keep visit summaries and your notes in one place. That can help you track what actions you need to take or what you've already tried to treat your symptoms.
Also, you might find it helpful to connect with others in a support group and share resources.
How long can long COVID last? The conditions linked as part of long COVID may get better over months or may last for years.
What treatment is available for long COVID? Healthcare professionals treat long COVID based on the symptoms. For tiredness, your healthcare professional may suggest that you be active only as long as your symptoms stay stable. If you start to feel worse, rest and don't push through your tiredness.
For symptoms of pain, breathlessness or brain fog, work with your healthcare professional to find a treatment plan that works for you. That may include medicine you can get without a prescription for pain, prescription medicine, supplements and referrals to other healthcare team members.
For loss of taste or smell, a process to retrain the nerves involved in those processes may help some people. The process is called olfactory training. For people with POTS or a fast heartbeat, the healthcare professional may suggest prescription medicine as well as a plan to stay hydrated.
Treatment for other long COVID symptoms may be available so contact your healthcare professional for options.
Next steps for Long COVID Long COVID makes life more difficult for many people. To provide better options for care, research is going on to better understand this illness. In the meantime, adults or children with long COVID may be able to get support for daily activities affected by the illness.
#long covid#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator
10 notes
·
View notes
Text
Iodine Pentafluoride Formula Benefits
Iodine Pentafluoride (IPF) is an organic compound with an organic base composition IF%, erythrogen, erythrocyclomethanes (EM), and fluoro-dihydro-lactone (DFLL). It is one of the five known fluorides of iodine. It's a transparent yellow liquid, although sometimes impure solutions appear green. It's commonly used as a topical irritant and as a fluorescent dye in various medical applications. Iodine Pentafluoride Formula Research Reports
Iodine Pentafluoride has recently been tested in cultured human breast cancer cells and showed good results - both in terms of increasing proliferation and in terms of achieving stable colonies. Other studies have indicated that iodine pentafluoride formula may also be effective in treating thyroid disorders, diabetes, Parkinson's disease, multiple sclerosis, and cirrhosis. Currently, there are no approved medicinal uses for iodine pentafluoride.
Iodine Pentafluoride, together with iodine sulfate, forms a compound called ITP (Inorganic Tetraphenyl ether). The compound has been shown to be free of all known side effects. It was also shown to increase the proliferation and diameter of the human breast cells (breast cancer cells).
Iodine is a crucial element in a number of processes. Without iodine, many bodily functions cannot occur. Iodine is needed for the production of proteins, carbohydrates, fat, vitamins and certain enzymes. Many people do not get enough iodine, either because they are unable to tolerate the taste of iodine or because they are intolerant to it. A special iodine supplement can help overcome these difficulties.
Iodine deficiency can result in many physical problems, such as the inability to produce red blood cells, and hemoglobin. Iodine deficiency also plays a large role in causing the skin to thicken. When people do not get enough iodine in their diet, they can become pale, flaky, and wrinkled. This effect is most extreme during times of iodine deficiency, such as during menstruation. Other symptoms include: dry skin, excessive hair loss, decreased energy levels, and dry brittle nails.
An iodine pentafluoride formula research can be very effective for treating iodine deficiency. The iodine supplements in the formula must contain a very high concentration of iodine. This way, the medication will be absorbed into the body very quickly. There are a variety of iodine supplement formulas on the market. Some iodine formulas can be used for treating specific symptoms, while some are made for general use.
Some iodine supplements have been shown to help prevent certain types of thyroid diseases and cancers. In some cases, iodine pentafluoride has also been shown to lessen the effects of strokes and brain damage caused by exposure to ionizing radiation. Because all of us are exposed to radiation on a daily basis, it is important that we know how to effectively use iodine when we need it. By taking an iodine supplement on a regular basis, we can help to protect our bodies against iodine deficiency and its negative health effects. The iodine supplement solution provided through natural health products is an easy, effective way to get the iodine that our bodies need.
Iodine is essential to the proper function of human growth and development. Without iodine, children are more prone to iodine deficiency and brain damage. Adults can also benefit from the use of iodine supplement solutions. By taking an iodine supplement solution containing the proper amounts of iodine, we can help to maintain our bodies' iodine supply.
One of the most common complications associated with iodine deficiency is the skin disorder iodine dermatitis. If this is not treated, it can become serious and even lead to death. Iodine helps to fight against iodine deficiency by boosting the immune system, as well as fighting the infection that can cause lesions and complications such as this.
Studies show that pregnant women who took a regular iodine mineral dietary regimen had a significant reduction in their chances of suffering from complications related to iodine deficiency. Iodine deficiency can also lead to the skin condition known as hypothyroidism. Pregnant women can greatly benefit from using an iodine mineral dietary formula. Iodine is found in many fruits and vegetables, and we get enough iodine in our diets. For those of us who do not get enough iodine in our diets, a dietary iodine supplement can be very beneficial. This is one of the reasons why pregnant women should use an iodine supplement formula to ensure that they are getting enough iodine in their bodies.
People of all ages should be taking iodine mineral supplements on a regular basis. Iodine deficiency is no joking matter. If you think that taking iodine supplements is just something for the elderly or people with thyroid problems, then think again. The risk for iodine deficiency continues to grow rapidly. As people get older, they tend to produce less of the iodine needed. Iodine Pentafluoride Formula is one way to ensure that you are getting the iodine needed to keep your body functioning properly.
Summary
At the time of this report, the official counts of cases and deaths from COVID-19 have passed 4,000,000 and 280,000. Many government announced a plan on reopening the national economy, but many countries are still at the stage of rising. It should be noted that the impact of the epidemic has accelerated the trend of localization, regionalization and decentralization of the global industrial chain and supply chain, so it is inevitable to reconstruct the global industrial chain. Faced with the global industrial change in the post epidemic era, enterprises in various countries must take precautions.
Chemical and petrochemical-related industries have been noticing the adverse effects of the COVID-19 outbreak. They are in the midst of a two-pronged crisis, besides the impact of COVID-19, another is the oil price war. Oil prices are dropping due to failed agreements on production cuts between OPEC and Russia in April and the need for chemicals and refined products is slowing from industrial slow-downs and travel restrictions in the wake of this global pandemic.
The chemical industry plays an important role in the production of countless products such as plastic, fertilizers, medicines, packaging products, etc., with the spread of coronavirus, many production facilities of several downstream industries have been halted. However, a rise in the demand for packaging materials has been increased to prevent the contamination of food, medicine, personal care, and medical products thereby creating a significant demand for chemicals involved in the packaging industry.
In such an environment, XYZ-research published a comprehensive analysis of key market trends in global Iodine Pentafluoride (IF5) 3160 market. It includes discussion on historical trends, current market status, competitive landscape, growth opportunities and challenges which are backed by factful feedbacks.
According to XYZResearch analysis, Iodine Pentafluoride (IF5) market will reach xx Million USD by the end of 2020, with a CAGR of xx % during the forecast period of 2021-2026, The XX segment in Iodine Pentafluoride (IF5) market is estimated to reach a market value of xx Million USD by 2020 from an initial market value of xx Million USD in 2019. China market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is xx. US market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is xx. Europe market value in 2019 is about xx Million USD, and Iodine Pentafluoride (IF5) production is XX.
Regional Segmentation (Value; Revenue, USD Million, 2015 - 2026) of Iodine Pentafluoride (IF5) Market by XYZResearch Include
China
EU
USA
Japan
India
Southeast Asia
South America
Competitive Analysis; Who are the Major Players in Iodine Pentafluoride (IF5) Market?
Solvay
Air Liquide
ABCR GmBR Co
Air Products
Honeywell
Shandong Zhongfu Chemical
Juhua Group
Shanghai 3F New Material
Major Type of Iodine Pentafluoride (IF5) Covered in XYZResearch report:
Purity 99.5%
Purity 99.0%
Other
Application Segments Covered in XYZResearch Market
Non-Aqueous System Battery
Organic Fluoride
Inorganic Fluoride
For any other requirements, please feel free to contact us and we will provide you customized report.
Post-pandemic Era-Global Iodine Pentafluoride Market report offers great insights of the market and consumer data and their interpretation through various figures and graphs. Report has embedded global market and regional market deep analysis through various research methodologies. The report also offers great competitor analysis of the industries and highlights the key aspect of their business like success stories, market development and growth rate.
Post-pandemic Era-Global Iodine Pentafluoride Market
Post-pandemic Era-Global Iodine Pentafluoride Market
Contact us: https://www.reportmines.com/contact-us.php
0 notes