#how to increase testosterone levels
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text
I love seeing videos of trans joy on my social media feeds 🥰
#it makes me so so happy to see#the video that popped up in my feed was a video of someone sharing moments of euphoria in their transition#and he looked so happy and full of life#it just makes me so angry when I see all the anti trans rhetoric and legislation#because how is someone being their authentic self directly hurting/impacting you? it’s not#like no one bats an eye at all the ads targeted to cis het men about increasing their testosterone levels to perform better in the bedroom#but sure let’s go ahead and restrict life saving medical care and materials for people that want to be themselves#it just makes me so angry and all of the stupid sports stuff like shut up you’re a sore loser and that’s why you’re mad#and most of the times the person complaining wasn’t even the runner up so shut up!!!#also got a video in my feed of a tattoo artist doing free hp tattoo cover ups and donations going to a trans organization#they were based out of the uk so too#I wish all trans people a lovely day and life and transphobes to die mad in a ditch!
1 note
·
View note
Text
Boost Testosterone Levels With This Weird Trick Doctors Won’t Tell You
Let’s get real—something’s off. More men than ever before are feeling drained, distracted, emotionally flat, and physically “meh.” Sound familiar? If you’re in your 30s, 40s, or beyond, it’s easy to blame stress, work, or aging. But the truth may be deeper.Your testosterone levels might be tanking—and you wouldn’t even know it. The kicker? There’s a weird trick—yes, weird—that’s showing…

View On WordPress
#boost low testosterone#hormonal imbalance in men#how to increase testosterone naturally#increase male energy levels#natural testosterone boosters#primal biohacks#T levels and cortisol balance#testosterone boosting exercises#weird testosterone tricks#zinc testosterone connection
0 notes
Text
Feeling tired, moody, or not quite like yourself? It might be more than aging: It could be low testosterone. Discover what every man should know about testosterone, aging, and how to reclaim your vitality. #MensHealth #Testosterone #LowT #TRT #HealthyAging #HormoneHealth
#aging#benefits and risks of TRT#energy#exercise and testosterone levels#fitness#health tips#hormone therapy#how aging affects testosterone levels#how to boost testosterone naturally#libido#low T#male hormones#Men’s Health#men’s hormone health guide#mood#muscle loss#natural ways to increase testosterone#signs of low testosterone#strength#symptoms of low T in men#testosterone#testosterone and aging in men#testosterone and mental health#testosterone and sex drive in men#testosterone decline#testosterone decline after 30#testosterone FAQs for aging men#testosterone replacement therapy for men#TRT#what every man should know about testosterone
0 notes
Text
youtube
CAUSES OF LOW TESTOSTERONE IN MEN - SYMPTOMS, DIAGNOSIS AND TREATMENT
#low testosterone#testosterone#low testosterone symptoms#low testosterone treatment#signs of low testosterone#low testosterone in men#low testosterone causes#how to increase testosterone#low testosterone levels#testosterone booster#symptoms of low testosterone#boost testosterone naturally#testosterone replacement therapy#low testosterone symptoms in young males#low testosterone signs#boost testosterone#testosterone in women#testosterone and sleep#Youtube
0 notes
Text
youtube
#testosterone booster foods#how to increase testosterone#boost testosterone naturally#how to boost testosterone#foods that boost testosterone#how to boost testosterone naturally#best testosterone booster#best food that increase testosterone#best food that increases testosterone#how to increase testosterone in men#best food to increase testosterone#best way to raise testosterone naturally#foods that raise your testosterone#how to boost testosterone levels#Youtube
1 note
·
View note
Text
"Morning Flusters"

Pairing: Spencer Reid x f!reader
Genre: Fluff
Warnings: early seasons Spencer, early relationship awkwardness, Spencer being flustered, mentions of a boner (not sexual), morning wood
Words: 1k
Summary: Waking up tangled together for the first time was sweet—until you felt something unexpected.
The warmth you felt was comfortable.
It was the kind of cozy, sleep-heavy warmth that made you want to burrow deeper into the blankets and never move again. The kind of warmth that only came from waking up next to someone else—him.
Spencer.
The realization sent a flutter through your chest. It was the first time you had stayed over, and despite your nerves the night before, everything had gone… perfectly. He had been an absolute gentleman, offering you his comfiest pajamas, making sure you had an extra pillow, and even stammering through an offer to sleep on the couch if you weren’t comfortable sharing the bed.
Of course, you had wanted to sleep beside him.
And now, here you were, tangled up together in the soft morning light filtering through his apartment window.
You shifted slightly, stretching, only to realize just how tangled you were. Spencer’s arm was draped over your waist, his face buried in the crook of your neck. His breath was warm against your skin, slow and steady in sleep. One of your legs had somehow ended up between his, your bodies pressed together in the most natural, intimate way.
You felt your heart swell at how relaxed he was. Spencer wasn’t always like this—so at ease, so unwound. You knew he had trouble sleeping sometimes, that his mind never quite let him rest. But right now, he looked peaceful.
And then—
Oh.
Oh.
You froze as you became aware of something else. Something firm pressing against your thigh.
Heat immediately rushed to your face.
It took a second for your sleepy brain to fully process it, but there was no mistaking what you were feeling. Spencer—soft, sleepy, completely unaware Spencer—had morning wood.
Your whole body went rigid.
This wasn’t bad or anything—totally normal, totally biological, totally not a big deal—but oh God, you were suddenly hyper-aware of everything.
You squeezed your eyes shut, willing yourself to stay calm. But of course, in your panic, your body betrayed you.
You shifted.
Just a tiny movement. But it was enough.
Spencer made a soft noise against your neck, his breath hitching slightly. His fingers flexed where they rested against your waist, and then—he stirred.
You felt it the moment he woke up.
His body stiffened, his breathing changed, and then—
“…Oh.”
Silence.
Complete, deafening silence.
Neither of you moved. Neither of you breathed.
You swore you could hear the gears in Spencer’s brain turning at a million miles per hour as he processed the situation.
And then—
“Oh my God.”
His voice was so horrified, so full of sheer mortification, that you couldn’t help it. Despite your own embarrassment, a nervous giggle bubbled up in your throat.
That seemed to snap him out of his stunned paralysis. He practically flung himself away from you, scrambling backward on the bed like he had just been electrocuted.
“I—I—this isn’t—” He ran a hand through his already-messy hair, eyes wide with panic. “It’s—it’s just biology! A completely involuntary physiological response—there’s an increase in testosterone levels during REM sleep which leads to—oh God, I’m explaining it, I need to stop explaining it—”
You bit your lip, watching him flail, his face rapidly turning as red as his pajama shirt. It was, objectively, the cutest thing you had ever seen.
“Spence.” You reached for his hand, but he was too busy burying his face in his palms, groaning in pure misery.
“I’m so sorry,” he mumbled through his fingers.
You couldn’t hold back your laughter anymore. It started as a giggle but quickly turned into full-blown laughter, your body shaking with it.
Spencer peeked at you from between his fingers, looking both betrayed and confused. “…You’re laughing?”
“I’m sorry, I’m sorry,” you gasped, trying to rein it in. “It’s just—oh my God, your face!”
He groaned again, flopping back onto the bed. “I’ll never recover from this. This is how I die.”
Still giggling, you scooted closer, resting your chin on his chest as you looked up at him. “Spence, it’s fine. I promise.”
He cracked one eye open, clearly skeptical. “…You’re not mortified?”
“Not even a little.” You grinned. "Why would I be? Watching you have a meltdown about it is kind of adorable.”
His face somehow turned even redder.
“I was not having a meltdown,” he muttered.
“You flung yourself across the bed like I was on fire.”
“…That’s a natural fight-or-flight response to extreme embarrassment.”
You laughed again, pressing a soft kiss to his jaw. “You’re ridiculous.”
Spencer let out a long breath, his body finally relaxing beneath you. After a moment, he tentatively wrapped an arm around your waist again, pulling you closer.
“…You really don’t think I’m a total disaster?” he asked quietly.
You smiled against his skin. “No, Spence. I think you’re perfect.”
His hand tightened on your waist, his breath a little uneven. “That makes one of us,” he mumbled.
You leaned up just enough to look into his warm, still-slightly-mortified eyes. “Hey. Just so you know—if we’re gonna keep sleeping in the same bed, this might happen again.”
Spencer groaned. “I was trying not to think about that.”
You giggled, pressing a kiss to his cheek. “I’m just saying—maybe next time, you don’t have to freak out so much.”
He hesitated, then, very slowly, buried his face against your shoulder with a small, resigned sigh. “…Noted.”
And with that, you both settled back into the warmth of the blankets, still tangled together, still flustered—but smiling.
#criminal minds#criminal minds fanfic#criminal minds fluff#criminal minds imagine#criminal minds one shot#criminal minds fic#criminal minds x you#criminal minds x reader#spencer reid#spencer reid imagine#spencer reid x reader#spencer reid fluff#spencer reid fanfiction#spencer reid one shot#spencer reid x you#matthew gray gubler imagine
1K notes
·
View notes
Note
Hi! Could make some writing notes regarding what happens to the human body when making out? Like the temperature increase and dopamine release, stuff like that? Or maybe just how the body reacts when you're nearby/interact to/with a loved one. I hope you're doing well! I love your posts!
Writing Notes: The Physiology of Love
Love can be distilled into 3 categories: lust, attraction, and attachment.
Though there are overlaps and subtleties to each, each type is characterized by its own set of hormones:
Testosterone and estrogen - drive lust
Dopamine, norepinephrine, and serotonin - create attraction
Oxytocin and vasopressin - mediate attachment
When we are falling in love, chemicals associated with the reward circuit flood our brain, produce a variety of physical and emotional responses:
Racing hearts
Sweaty palms
Flushed cheeks
Feelings of passion
Anxiety
Two decades of research shows that when it comes to early-stage intense romantic love—the kind we often think of when we talk about being lovestruck—a very primitive part of the brain’s reward system, located in the midbrain, is activated first.
Some Physiological Reactions to a Kiss
Pulse and blood pressure increase
Pupils dilate
Breathing deepens
Rational thought retreats, as desire suppresses both prudence and self-consciousness
Lust
Driven by the desire for sexual gratification.
The evolutionary basis for this stems from our need to reproduce, a need shared among all living things.
The hypothalamus of the brain plays a big role in this, stimulating the production of the sex hormones testosterone and estrogen from the testes and ovaries. While these chemicals are often stereotyped as being “male” and “female,” respectively, both play a role in men and women.
As it turns out, testosterone increases libido in just about everyone. The effects are less pronounced with estrogen, but some women report being more sexually motivated around the time they ovulate, when estrogen levels are highest.
Lust and attraction shut off the prefrontal cortex (includes rational behavior).
Attraction
Dopamine
Produced by the hypothalamus, is a particularly well-publicized player in the brain’s reward pathway – it’s released when we do things that feel good to us:
E.g., Spending time with loved ones and having sex.
High levels of dopamine and a related hormone, norepinephrine, are released during attraction. These chemicals make us:
giddy,
energetic, and
euphoric, even leading to decreased appetite and insomnia – which means you actually can be so “in love” that you can’t eat and can’t sleep.
Norepinephrine, also known as noradrenalin, may sound familiar because it plays a large role in the fight or flight response, which kicks into high gear when we’re stressed and keeps us alert:
Released more often at the beginning of a couple's relationship when many unknowns are present, putting the brain in a ‘proceed with caution’ mode.
Early in a relationship, there is heightened adrenalin, which causes feelings like butterflies in the stomach and a faster heart rate. There is also reduced activity in the parts of the brain that help us to make judgements, which is why you may be 'blinded' to another person’s faults in early love or infatuation,
Brain scans of people in love have actually shown that the primary “reward” centers of the brain, including the ventral tegmental area and the caudate nucleus, fire like crazy when people are shown a photo of someone they are intensely attracted to, compared to when they are shown someone they feel neutral towards (like an old high school acquaintance).
Attraction seems to lead to a reduction in serotonin:
It is a hormone that’s known to be involved in appetite and mood.
Interestingly, people who suffer from obsessive-compulsive disorder also have low levels of serotonin, leading scientists to speculate that this is what underlies the overpowering infatuation that characterizes the beginning stages of love.
This explains why people in the early stages of love can become obsessed with small details, spending hours debating about a text to or from their beloved.
Attachment
The predominant factor in long-term relationships.
While lust and attraction are pretty much exclusive to romantic entanglements, attachment mediates friendships, parent-infant bonding, social cordiality, and many other intimacies as well.
The two primary hormones here appear to be oxytocin and vasopressin.
Oxytocin
Often nicknamed “cuddle hormone” or “hormone of love”.
Produced by the hypothalamus.
Released in large quantities during sex, breastfeeding, and childbirth.
This may seem like a very strange assortment of activities – not all of which are necessarily enjoyable – but the common factor here is that all of these events are precursors to bonding.
It also makes it pretty clear why having separate areas for attachment, lust, and attraction is important: we are attached to our immediate family, but those other emotions have no business there (and let’s just say people who have muddled this up don’t have the best track record).
The Brain During a Kiss
The brain goes into overdrive during the all-important kiss.
It dedicates a disproportionate amount of space to the sensation of the lips in comparison to much larger body parts.
During a kiss, this lip sensitivity causes our brain to create a chemical cocktail that can give us a natural high.
This cocktail is made up of three chemicals, all designed to make us feel good and crave more: dopamine, oxytocin, and serotonin.
Like any cocktail, this one has an array of side-effects.
The combination of these three chemicals work by lighting up the 'pleasure centres' in our brain.
The dopamine released during a kiss can stimulate the same area of the brain activated by heroin and cocaine. As a result, we experience feelings of euphoria and addictive behaviour.
Oxytocin fosters feelings of affection and attachment. This is the same hormone that is released during childbirth and breastfeeding.
Finally, the levels of serotonin present in the brain whilst kissing look a lot like those of someone with Obsessive Compulsive Disorder.
No wonder the memory of a good kiss can stay with us for years.

Love happens less in the heart and more in the brain, where hormonal releases and brain chemicals are triggered.
Dopamine, serotonin and oxytocin are some of the key neurotransmitters that help you feel pleasure and satisfaction.
So, your body often approaches love as a cycle.
It feels good to be with that person, so your brain says, "Do that again."
Sources: 1 2 3 4 5 6 7 8 ⚜ Notes & References ⚜ Love ⚜ Kinds of Love
Thanks so much for your kind words. Hope you're doing well yourself! Would love to read your writing if these notes inspire you.
#anonymous#writing notes#love#writeblr#dark academia#spilled ink#writing reference#literature#writers on tumblr#writing prompt#poets on tumblr#poetry#creative writing#fiction#novel#light academia#writing ideas#writing inspiration
565 notes
·
View notes
Text
my conspiracy theory is that part of the reason the natural girlygirl influencers suddenly started being so anti birth control and fearmongering about hormonal contraception is based in transphobia and meant to stir up health paranoia and fear around HRT. you tell afab people that their hormones are so extremely delicate that just taking an estrogen/progestin pill to prevent pregnancy will so severely fuck up your endocrine system that it will wholly ruin your life.
there's a subtle implication: "if hormonal birth control ravages the female body in this way, good god, imagine what testosterone will do to it!!" ive even heard some girls talk about the "chaos" their body was put through when they had a natural rise in testosterone after coming off the pill. it was just their testosterone levels returning to natural after the influx of estrogen stopped from the pill, but some of these girls talk like they suddenly became hulking beasts just from a slight increase in natural t. theres already so much fearmongering around testosterone specifically, it makes me wonder how many trans men chose not to go on HRT because they had been led to believe that any altering of your body's hormones is poison...
167 notes
·
View notes
Note
idk if this is a sex ed question, or if you're the right person to ask, sorry, but do you have any reputable sources about what testosterone *actually* does?
i see people saying it limits your emotions, that it gives you breast cancer, that it makes you malnourished, its a second more dangerous puberty, etc, and I'd like to think im good at picking out lies, but there's a lot of stuff that sounds like bullshit coming from blogs i thought were trustworthy.
if not, all good, thank you in advance!
hi anon,
I'm really glad you sent this ask, because this kind of scaremongering misinformation is deeply upsetting and I'm so happy to provide a better information.
there are tons of reputable sources as to what testosterone does; some that I'll be pulling from in this answer include Cleveland Clinic, Harvard Medical School, University of California San Francisco, Mayo Clinic, the Society for Endocrinology, and Planned Parenthood.
so, what's up testosterone?
testosterone is a hormone produced in everyone's bodies, either in the testes or the ovaries depending on which set of equipment you're working with. all bodies produce both estrogen and testosterone, usually in different levels. regardless of the genitalia you were born with, how you understand your gender, or what levels of testosterone you have in your body, testosterone affects things like your sex drive, your hair growth, muscle and bone density, and the production of red blood cells.
in people born with testes, puberty usually comes with an increase in testosterone that kicks off changes such as growth of the penis and testicles, the production of sperm, an increase in hair growth all over the body, deepening of the voice, greater production of oil on the skin, and an increase in height, weight, and muscle mass.
either an overabundance or a deficit of testosterone can have health complications, just as having more or less of any hormone that a body needs can cause complications.
people who choose to transition by taking testosterone will experience many similar effects as cisgender men going through puberty, including the increase in body hair, skin oils, and muscle mass, as well as a deepening voice. while people on testosterone are unlikely to experience significant growth in terms of height unless they start hormone replacement therapy (HRT) at a fairly young age, testosterone does frequently cause a redistribution of fat on their bodies to be more similar to that of cisgender men. bottom growth, the increased size and sensitivity of the clitoris to more closely resemble a penis, is also common; the clitoris and the penis are homologous structures (they're made out of the same goo when embryos start developing genitalia), hence why they react similarly to testosterone.
to address your specific concerns:
testosterone does not limit the range of a person's emotions. while it may impact a person's mood and the severity of their feelings, the same is true of any hormone - for instance, people also report mood changes when they take antidepressants or birth control. the sometimes drastic mood fluctuations experienced during puberty are not tied to a specific hormone; this is a turbulent time regardless of what hormones your body is producing the most. testosterone is stereotyped as making people angry and violent, but all people are people regardless of their biology and are shaped by much more than the hormones in their body.
while cisgender men and trans people on testosterone can both get breast cancer, testosterone does not pose any particular risk. several of the sources linked about don't find any significant link between taking testosterone HRT and an increased risk of breast cancer, reporting that transgender individuals who take testosterone are not at any particularly higher risk of developing breast cancer than cisgender women. for more detailed information about potential health problems affiliated with taking testosterone, I recommend the "Risks" section of the linked UCSF document. yes, there are health risks affiliated with taking testosterone; this is true of literally any medication and, more importantly, is also true of just being a person with any kind of hormones in your body. cis men and women also have health conditions affiliated with being cis men and cis women, this is the price of admission for having a human body. nobody gets out unscathed.
there is no evidence that testosterone causes someone to become malnourished. people undergoing a testosterone-based puberty, whether they're cis or trans, are likely to experience a great deal of growth and bodily changes that will use a great deal of calories, which means they may be hungry and need more food than they did previously. this is a normal effect of puberty on a body, and is only a risk for malnourishment if a person isn't able to eat in sufficient amounts to keep their body properly nourished.
there is nothing about a testosterone-based puberty that is "more dangerous" than an estrogen-based puberty, which is what I assume is the point of comparison. puberty is a completely natural process that does not pose any significant dangers unless you want to be a real dipshit about it and pull some shit like "puberty is dangerous because you grow breast tissue and then you're at risk for breast cancer," in which case sure, great job, Sherlock. you solved it, puberty is cancelled forever. I cannot emphasize enough how stupid this is, conceptually; roughly half the human population goes through this kind of puberty every day and they're fucking fine. puberty by itself is not a risk factor of anything.
I don't know what particular interest the blogs you've been following have in making testosterone-based puberty sound like it's going to turn you into an emotionally stunted skeleton with breast cancer, although I fear it's transphobia hidden unsubtly behind concern trolling and disdain for cisgender men.
if you're interested in taking testosterone and are concerned about the changes you might see in your body please, for the love of god, consult with reputable health resources and a doctor rather than whatever nematode is posting about testosterone ruining your life.
682 notes
·
View notes
Note
47 bucktommy for the prompts 🙏
47. A kiss... out of spite.
Content Warning for Homophobic Language
•
Tommy’s been around the block. He’s heard pretty much every homophobic slur in modern day use, and had most of them thrown his way at some point. Not to say that he’s used to it, not by any means. It still irritates him, still pisses him off, but he’s got a thicker skin now than he did when he was younger. He’s grown into himself, is more confident and comfortable than he’s ever been.
Evan is… To say he’s unconfident isn’t correct. And to say he’s uncomfortable with their relationship isn’t right either. But it’s new to him. This is new to him. Being with another man, maneuvering around the mire of bigotry that still courses through people. Los Angeles is a liberal place, but it’s far from perfect.
They’re at the beach. Tommy doesn’t go often enough, considering how close it is. The water’s too cold for Tommy’s taste right now, winter weather still clinging stubbornly to the beginnings of spring. But it’s bright and clear, just like the sky, just like Evan’s eyes. They’re walking along the surf; Evan’s hand is firmly in his. Evan keeps stopping them to duck down and grab shells out of the sand, holding it up and talking excitedly about bivalves and snails.
“Is it true that oysters are an aphrodisiac?” Tommy asks, pitching his voice just low enough that Evan’s grin turns sly and excited, “Because I’m thinking seafood for dinner.”
“Not necessarily,” Evan says, nudging their shoulders together and squeezing Tommy’s fingers, “But they’ve got high levels of zinc, which can slightly increase testosterone.”
Evan wiggles his eyebrows suggestively, and pokes his tongue out from between his teeth, pink and wet. Tommy opens his mouth to say something dumb about how he’s very familiar with his own testosterone levels, when someone next to them says loudly and clearly–
“Faggots.”
Evan jerks like he’s been slapped, face immediately going bright red. There’s a collection of snickers, and they turn to see a group of six young men. They look college age, in varying stages of sunburnt and tan, loitering together around a collection of folding beach chairs. There’s a veritable mound of empty hard seltzer cans around them.
“Excuse me?” Evan snaps, already turning on his heel to take a step in their direction.
Tommy tightens his grip on Evan’s hand.
“Nothing,” One of the men smirks. He’s wearing a pair of sunglasses, mirrored and tinted to an obnoxious shade of orange, “Didn’t say anything.”
“Really?” Evan snaps, “Sounded like something to me.”
“Sounds like you’re hearing shit,” Another guy says, goading and slurred. He’s got a snapback tipped sideways on his head.
All six of them start laughing to themselves again. Tommy watches as Evan’s free hand clenches into a fist.
“Baby,” Tommy says firmly, reaching out to snag Evan’s other arm, “They’re just a group of drunk dumbasses, let’s go.”
“Yeah, baby,” Orange sunglasses call out meanly, “Listen to your boyfriend.”
Tommy snorts derisively, and twists to press a dirty little kiss to Evan’s scowling mouth. The kiss is just long enough for Tommy to nip at Evan’s lower lip, to taste the surprised noise he makes in response. The laughter wobbles, turns confused. Tommy pulls back.
“Cackle all you want,” Tommy says, flipping them off, “Baby here’s guaranteed to get his dick wet tonight, and it looks like you six are just guaranteed to feel like shit tomorrow.”
They all blink stupidly at him, temporarily unsure of how to respond. Tommy takes advantage of it to tug Evan close, and uses the momentum of that to turn the two of them around towards the parking lot.
“Assholes,” Evan grumbles, glaring at them over his shoulder, before turning his attention back to Tommy, “What the fuck?”
“Yeah,” Tommy hums in agreement, turning his own head to press a softer, sweeter kiss to Evan’s birthmark, “C’mon, let's go get a shitton of oysters. You can tell me all about their mucus while we suck on those, and then when we get home I’ll suck on you.”
Evan huffs out a reluctant laugh.
“Sweet talker,” Evan says, “It’s called liquor, and it’s basically seawater and oyster juice.”
“Exactly,” Tommy nods seriously, “Mucus.”
Evan twines their fingers together. Tommy rubs his thumb across Evan’s knuckles. Behind them, the drunks have apparently gotten their words back, and shout something incoherent that would probably get censored on prime time tv.
They ignore it.
163 notes
·
View notes
Text
A brief guide to Testosterone HRT
If you’d like the one for Estrogen HRT, ask in the comments and you shall receive.
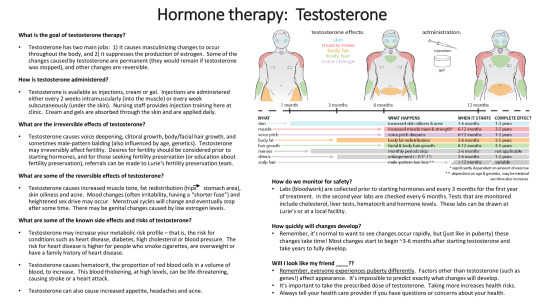
Image from the Transpeak Discord - unsure of actual source (a clinic?) (if anyone knows, please tell!)
Alternate text under the cut
Alt:
What is the goal of testosterone therapy?
Testosterone has two main jobs: It causes masculinizing changes to occur throughout the body, and it suppresses the production of estrogen. Some of the changes caused by testosterone are permanent (they would remain if testosterone was stopped), and other changes are reversible.
How is testosterone administered?
Testosterone is available as injections, cream, or gel. Injections are administered either every two weeks intramuscularly (into the muscle) or every week subcutaneously (under the skin). Nursing staff provides injection training here at clinic. Creams and gels are absorbed through the skin and applied daily.
What are the irreversible effects of testosterone?
Testosterone causes voice deepening, clitoral growth, body/facial hair growth, and sometimes male-pattern balding (also influenced by age and genetics). Testosterone may irreversibly affect fertility. Desires for fertility should be considered prior to starting hormones, and for those seeking fertility preservation (or education about fertility preservation), referrals can be made to Lurie’s fertility preservation team.
What are some of the reversible effects of testosterone?
Testosterone causes increased muscle tone, fat redistribution (hips to stomach area), skin oiliness and acne. Mood changes (often irritability, having a “shorter fuse”) and heightened sex drive may occur. Menstrual cycles will change and eventually stop after some time. There may be genital changes caused by low estrogen levels.
What are some of the known side effects and risks of testosterone?
Testosterone may increase your metabolic risk profile — that is, the risk for conditions such as heart disease, diabetes, high cholesterol or blood pressure. The risk for heart disease is higher for people who smoke cigarettes, are overweight or have a family history of heart disease.
Testosterone causes hematocrit, the proportion of red blood cells in a volume of blood, to increase. This blood thickening, at high levels, can be life-threatening, causing stroke or a heart attack.
Testosterone can also cause increased appetite, headaches, and acne.
A low-detail diagram of the upper half of three bodies is displayed. From left to right, the bodies represent having been on testosterone for little to no time (a month or less), a medium amount of time (six to eight months) and a greater amount of time (a year or more).
The diagram is a visual representation of testosterone effects on the body. Hip mass shifts to the stomach area, The adam’s apple grows. Muscle mass grows and shoulders become broader. Facial and body hair grows on the arms, face, and assumably the legs not displayed in the image. The skin gets oily and acne appears on the face.
Testosterone affects: skin, muscle mass, body fat, body hair, voice change.
Increased skin oiliness and acne starts within 1-6 months of testosterone. Its complete effect can be within 1-2 years.
Increased muscle mass and strength starts within 6-12 months of testosterone. Its complete effect can be within 2-5 years. This effect is highly dependent on the amount of exercise one does.
Voice pitch deepening starts within 6-12 months of testosterone. Its complete effect can be within 1-2 years.
Body fat redistribution starts within 3-6 months of testosterone. Its complete effect can be within 2-5 years.
Facial and body hair growth starts within 6-12 months of testosterone. Its complete effect can be within 3-5 years.
Monthly periods stop within 2-6 months of testosterone.
Clitoral enlargement of 0.5 inches to 1 inch begins within 3-6 months of testosterone. Its complete effect can be within 1-2 years.
Male pattern hair loss starts when you have been on testosterone for over a year. Its complete effect date is variable. It depends on age and genetics, and can be minimal.
Sex drive also increases.
How do we monitor for safety?
Labs (bloodwork) are collected prior to starting hormones and every three months for the first year of treatment. In the second year, labs are checked every six months. Tests that are monitored include cholesterol, liver tests, hematocrit, and hormone levels. These labs can be drawn at Lurie’s or a local facility.
How quickly will changes develop?
Remember, it’s normal to want to see changes occur rapidly, but (just like in puberty) these changes take time! Most changes start to begin around 3-6 months after starting testosterone and take years to fully develop.
Will I look like my friend _____?
Remember, everyone experiences puberty differently. Factors other than testosterone (such as genes!) affect appearance. It’s impossible to predict exactly what changes will develop.
It’s important to take the prescribed dose of testosterone. Taking more increases health risks.
Always tell your health care provider if you have questions or concerns about your health.
#mod cole#trans#transmasc#transgender#trans man#ftm#transmasculine#trans guy#testosterone gel#testosterone#testosterone hrt#ftm hrt#trans hrt#hrt#hormone replacement therapy#testosterone replacement therapy#trans boy#transsexual#trans ftm#trans men#trans male#trans pride#transblr#transsexuality#trans masc#ftm trans#trans resources#trans resource#resources#has this already been posted on this blog? we’re about to find out
354 notes
·
View notes
Text
The Vital Role of Testosterone in Your Body
Testosterone is often misunderstood as just the “male hormone,” but its influence stretches far beyond that. From muscle mass to mood regulation, testosterone plays a pivotal role in your physical, emotional, and sexual health—regardless of gender. Whether you’re looking to boost performance, manage aging, or simply understand your body better, knowing the role of testosterone is essential. What…

View On WordPress
#causes of low testosterone#functions of testosterone#how to increase testosterone#increase testosterone#low testosterone#low testosterone causes#low testosterone in men#low testosterone signs#low testosterone symptoms#low testosterone therapy#low testosterone treatment#signs of low testosterone#signs of low testosterone in men#symptoms of low testosterone#Testosterone#testosterone booster#testosterone hormone#testosterone levels#testosterone supplements
0 notes
Text
I really dgaf about sports and the Olympics, but I just saw the tweets JKR posted. I can’t really stay silent on her nonsense, especially since her words hit me hard as a woman with PCOS.
JKR claims to be this "great feminist” standing for women against “transgender ideology" then goes and attacks a cis woman of color because she has a genetic disorder.
It is so stupid to claim that being born with different hormones means that you're automatically of the opposite gender.
I'm also a woman who produces excessive amounts of testosterone and did look ‘manly’ for a certain period of my life. I remember going through something similar to male puberty. Instead of menstruating, I got thick, dense facial and body hair, my jaw got wider and my acne worsened.
That's when the vicious rumors about me being a "fake girl". It pressured me to start taking hormones at an early age (13). Kids lacked basic decency because of their immaturity, but to have a grown ass woman bullying an athlete is just horrific. I seriously can’t put how I felt when I saw that stupid terf call a cis woman ‘a man’ into words.
It's also racist and sexist to assume woman = dainty and frail. It's mostly WOC who have increased levels of testosterone and maintaining that sexist stereotype affects us the most.
And please don’t get me started on how that Italian boxer is a racist cop with links to the FAR RIGHT. Would I be taking it too far to say that she quit on purpose so she could sabotage the reputation of Imane 🤔 I don’t think so…
In summary, fuck JKR. I stand with Imane Khelif.
#olympics#fuck jkr#imane khelif#jk rowling#trans rights are human rights#transgender#sexism#tw transmysoginy#pcos#intersex
413 notes
·
View notes
Text
hello to trans, intersex, gender non conforming & all folks starting testosterone HRT, just wanted to let you know that while your body adjusts to the hormone, you will be very tired and often have to sleep in a lot or take extra naps because of how much is changing. you deserve to have adequate time for rest as your body changes fat and muscle distribution, begins and intensifies certain hair growth, and so on.
one of the first effects most folks see is bottom growth, along with an increase in libido. this can be very intense for several months until it reaches its peak and levels out. some folks continue to have a high libido whereas others return to their base level. your hair and skin will become oilier during this time, and your body odor changing will also be around this time. a lot of these effects can make your body very tired, as it is changing how it maintains itself, and you may find you need to completely change your grooming rituals and products or accessories.
be kind to yourself during this time, it's easy to feel awkward because you are very much entering puberty once again, so rest when you can, eat plenty when you're hungry, stay hydrated, and keep your chin up, you'll see the effects you're looking for not long after you see these. take care of yourself
#transgender#trans#lgbtqia#queer#transmasculine#transneutral#transsexual#nonbinary#enby#genderqueer#gnc#butch#butch lesbian#bear#intersex#ftm#transmasc#trans guy#trans boy#trans dude#trans men#trans man#our writing
2K notes
·
View notes
Text
Hair Regrowth for Detrans Women
As someone who experienced a lot of hair loss during my transition, I wanted to share things that have helped me with regrowing it. Hopefully this can help other women with their hair too!
While there's nothing wrong with hair loss and it's not something we should be ashamed of – It's a medical problem, plain and simple! – Hair is important to people and it's a big part of our appearance and self-esteem, so I don't think there's anything wrong with doing things that can help.
Women tend to hide it (with wigs, hair toppers, etc) because there is shame associated with hair loss, and because of that we don't always know that there are women around us who have dealt with this problem too. Since experiencing this myself, I've noticed plenty of women with hair loss and recession. It may not be super common, but it's nothing to be ashamed of!
First things first - If you've stopped taking testosterone and your T levels are within a normal-ish female range, you shouldn't need any kind of DHT blockers. So you should avoid all of that stuff unless you know there's a medical reason that it could be beneficial.
You're not a man - your hair loss is the type that women get when their testosterone levels are too high. Many women with conditions like PCOS develop pattern hair loss, and plenty of other conditions can cause hair loss for women too. It's far from something that only affects men.
Minoxidil - I had success with this, but quickly lost hair every time I would stop using it, even for a week or so. I was also uncomfortable with the idea of potential negative health effects and didn't want to risk that over the long run. So I switched to rosemary oil.
Rosemary Oil - I used this recipe to make a rosemary oil spray. I expected to lose hair when I stopped the minoxidil and started using this, but not only did I not lose hair, I've also seen new growth come in. I use this once a day, spraying enough to cover the areas of thinning and then rubbing it thoroughly into my scalp.
I recommend starting with rosemary oil instead of minoxidil. If it doesn't work, at least you tried the safer option first.
Microneedling - This is what I think has done the most for my hair! (Disclaimer: This is not medical advice. If you want to try microneedling, either go to a professional or be very careful that you're being safe and disinfecting before and after.)
I looked up a lot of tutorials and information and this is the protocol I landed on:
I use a high quality dermastamp set to 1.25mm length once every 10 days. First I soak the stamper in rubbing alcohol for at least 2 minutes, then wash my hair with shampoo. After drying it, I rub alcohol on the areas I'll be treating just to be safe. Then I stamp it over the areas until the skin turns pink. There shouldn't be any bleeding, but it is a little painful. (Much less painful than a tattoo!) Once the areas are pink, stop using the stamper. You're done. After that I rub more alcohol on my scalp and then wash my hair again.
The whole thing only takes about 10 minutes. It is important to wait 10 days in between treatments, because your skin needs time to heal again.
The theory behind how microneedling works for hair growth is that it damages the skin and hair follicles just enough that it triggers your cells to repair, which can cause follicles to grow thicker hair again, and even to grow hair where you thought the follicles were dead. It also increases blood flow to the scalp the same way that minox and rosemary oil do.
For anyone who wonders if any of this is really worth it – It might not be for you, but it definitely was for me. Before I detransitioned and started treating my hair, my only option was to buzz it because it was so thin on the top and the recession was really far back. It's not back to how it used to be (and it might never be) but I managed to reverse multiple years worth of hair loss and I feel much more confident.
I have no way of knowing how much of my hair regrowth is due to this treatment, and how much is just from being off testosterone. But considering a lot of women have little or no improvement in their hair after stopping T, I think it's probably a little of both.
I've only been at this for about a year, so I'd love anyone who has more experience in treating their hair for regrowth, or anyone who has had other treatments or procedures to comment or reblog with their experiences too!
89 notes
·
View notes
Text
Just got some good news from the doctor.
Weaning off the medication is working. My testosterone levels are shooting back up. My free testosterone isn't quite in range yet, but it is close. And my total testosterone is in range now, but could be higher. To give an idea of how much I have improved, my free T increased 5x and my total T increased 3x.
The good...
I've been having much less intense hot flashes. My libido has improved. I'm sleeping more. I have been able to cook a bit more and I have been able to write more on my blog.
The bad...
I am still very fatigued (more than my baseline). I am still extremely sedentary. I can't clean. I can't do basic chores. I can't stand for more than a few minutes at a time without major consequences. I can't do photography or complex photo editing.
And when I drop my dosage again that will all probably get worse until I adjust.
I can't describe how much misery it took just to get to this point. And I am still not out of the woods by any means. I'm guessing a few more months at minimum. But these test results prove that if I see this through, I will probably feel better on the other side.
Cautious optimism.
116 notes
·
View notes