#health news ebola
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text

telegraph.co.uk
Not surprised after Rwanda's impressive curbing of Covid 19 early on, but sad that a swift, smart response will never be replicated in the U.S.
116 notes
·
View notes
Text
Trump Withdraws U.S. from World Health Organization - The New York Times
Through Executive Order Trump withdrew 👆
The article says; 👇
Founded in 1948 with help from the United States, the World Health Organization is an agency of the United Nations. Its mission, according to its website, is to “confront the biggest health challenges of our time and measurably advance the well-being of the world’s people.”
That includes bringing aid to war-torn areas like Gaza and tracking emerging epidemics like Zika, Ebola and Covid-19. The annual budget of W.H.O. is about $6.8 billion; the United States has typically contributed an outsize share. (Of course we all knew the U.S. gave the most)
Do you know what else happened in 1948?
Israel became a state. Before that the whole area was known as Palestine. Maybe it was a coincidence or maybe not? 🤔
#pay attention#educate yourselves#educate yourself#reeducate yourselves#knowledge is power#reeducate yourself#think about it#think for yourselves#think for yourself#do your homework#do your research#do your own research#do some research#ask yourself questions#question everything#president trump#executive orders#government corruption#government secrets#khazarian mafia#truth be told#evil lives here#news
114 notes
·
View notes
Note
I just read the article you posted a while back about TB (heads up- it said the gift article link has lapsed or some such). Did J&J ‘evergreen’ (be allowed to be evil) or was it allowed to become generic?
Relatedly, how do you manage empathy fatigue? I deal with OCD too and it screams at me that I have to care about and do all the things all at once. How do you choose where to put your time and energy?
(Also, when I get the coffee subscription for my husband’s birthday, which version should I get?)
For me empathy fatigue sets in when I careen my attention from this crisis to that one to the next one to the one after that, always feeling overwhelmed by each emerging problem but never having the time or attention to devote myself to one problem or another.
I'll give you an example. In 2014, a horrific ebola epidemic swept through Guinea, Liberia, and Sierra Leone. The world paid attention to it. Everyone was talking about it. And then .... it ended. At least in the global imagination. Money dried up. The world moved on to the next crisis.
That's not to say the next crisis wasn't important. It was important. But in Sierra Leone, the ebola crisis wasn't really over even after people stopped contracting ebola. 15% of Sierra Leone's healthcare workers had been killed by ebola, and the already fragile healthcare system plummeted into what one Sierra Leonean physician described to me as "a state of collapse."
And so the crisis remained a crisis even after the world's attention shifted. 1 in 17 women in Sierra Leone were dying in childbirth. Over 10% of kids born died before the age of five. Tuberculosis killed thousands every year despite curative treatment being available.
And this is when Hank and I finally, belatedly realized that responding to crises in the news was not adequate. Instead, we would need to commit the kind of long-term attention and long-term support that long-term crises demand. This means making difficult choices--there is also high maternal and child mortality in countries other than Sierra Leone, but we choose to focus on Sierra Leone because we see an opportunity to make a difference, because the government is serious if limited in its commitment to improving healthcare and educational opportunities, and because we had to make a choice or else we would be overwhelmed by the many causes.
What about the other causes? Well, we trust people to work on those causes. We believe in their importance. And we support their work by doing ours as well as we can, and trusting they are doing theirs as well as they can. I still get overwhelmed. I still get depressed. But I find that the deeper I go into my particular areas of interest--global healthcare delivery, health care accessibility, ending TB, fighting maternal mortality--the better I feel personally, and the more good I feel like I'm able to do.
2. Johnson & Johnson has not abandoned their secondary patents on bedaquiline but they have committed to allow generics to be available in most countries, even those where the secondary patents apply. Unfortunately this deal leaves out many countries that need generic bedaquiline, including Ukraine, which is absolutely unacceptable. So progress has been made, but the progress (as is so often the case) is inadequate. The fight goes on.
683 notes
·
View notes
Text
Also preserved on our archive
There could be a lot more here about non-pharmaceutical interventions like masking, but some pretty good analysis of the climate of vaccine "skepticism" and disease minimizing we live in.
By David Quammen
Health officials would like to remind you that we are entering that time of the year still quaintly known as flu season. That means autumn to spring. Kids go to school, adults spend more time gathered indoors, people breathe and speak and sneeze and cough at one another, and the latest influenza virus spreads widely.
The reason flu season seems a quaint idea is that we now hear about and maybe worry about so many viruses all year. And well we should.
What if there’s a simultaneous surge of Covid and seasonal flu this autumn? What if infections of respiratory syncytial virus, known as R.S.V., peak at unusual levels, as they did in the 2022-23 season? What if the new strain of mpox, which is especially virulent, continues spreading in Africa and beyond? What if this year’s flu combines with the dreaded H5N1 bird flu and emerges as a nightmare flu? What if a novel virus destined to be called SARS-CoV-3 emerges from a horseshoe bat in a rural village somewhere, gains a few key mutations and comes barreling through the world’s airports?
Oy vey and déjà vu. It’s always virus season now. Maybe none of those worst-case scenarios will happen, but to assume so is to count on fool’s luck.
The notion of flu season is a relic of times when one virus could transfix our response efforts and dominate our collective consciousness. Influenza in 1918. H.I.V. in 1980s and ’90s. Ebola in 2014. We can no longer afford to react on a case-by-case basis. Today we need a broader vision. We need personal, governmental and technological responses that address the full spectrum of viruses that disrupt our lives.
Because they will continue to disrupt our lives. We live amid viruses. We eat them. We breathe them. We touch them on doorknobs and cafeteria trays. All the wild and domestic animals with which we interact, from mosquitoes to mice to the sparrows on the bird feeder and the monkeys in the temple gardens, carry their own freights of them in wondrous variety. Most of these viruses have no chance of infecting a human, but many do. The best way to protect yourself and your family is just what health agencies recommend: Get the vaccines if reputable ones exist.
The best way to help protect your community, your country and the rest of humanity is a more complex proposition. The answers range from public health measures such as better virus surveillance to ending our bone-headed science denialism and finally supporting pandemic preparedness. But it’s not my purpose to unpack those big topics in this small spurt of words.
My purpose is more modest: to refresh your awareness of something you can’t see, not without the help of an electron microscope. Even the human genome contains a sizable portion — roughly 8 percent of it — that was once the genomes of ancient retroviruses, acquired and internalized by our ancestors in the course of infections.
Viruses of concern to humans come and go on various schedules. American dairy cows began their flu season this year around March 25, when the first infections with bird flu were reported in herds in Kansas and Texas. Measles outbreaks tend to be seasonal but more complex. In the tropics they may peak in the dry season, while in temperate climates measles correlates more with school schedules. And now that warmer temperatures are welcoming tropical mosquitoes farther north and south — including ones that transmit viral diseases like yellow fever and dengue — people in Florida and Italy may find that their worst virus season is summer. Climate change is the new force applied to the viral calendar.
Each year another seasonal vaccine is offered because influenza viruses evolve and mix continuously; their genomes entangle like shape-shifting snakes. The most concerning threat is different each year. This year’s flu vaccine in the United States is what’s called trivalent, or three-powered, meaning it contains elements from three different influenza viruses, all of which are circulating and any of which may prove most pervasive and problematic. Manufacturing flu vaccines takes months, so calculated decisions, mixing science and foresight, must be made long before autumn. Increasing efforts to produce even more kinds of vaccines, including some that target multiple virus strains, signal scientific awareness of the point I’m trying to make: We know a virus might get us, tomorrow or next season, but we can’t say which.
Hence the need for a universal flu vaccine, such as one that’s now in clinical trials at the National Institutes of Health. Hence the need for a universal coronavirus vaccine, toward which scientists at the California Institute of Technology, among other places, are working. Hence the need to create combination vaccines that protect against Covid-19 and influenza in one shot, which are also under development in the United States, China and elsewhere. Hence the need to improve ventilation systems for public and private buildings, which can significantly reduce the spread of respiratory viruses.
These are urgent challenges, at which laboratories and public health authorities all over the world are laboring busily. Science takes time; applying its findings takes patience. Persuading the public to adopt behavioral changes — some of which involve a prick in the arm, some of which require placing community welfare on a level with individual independence — is a task that may seem almost Sisyphean, but it remains crucial and doable.
Flu season in America is no illusory concept, and I don’t mean to deride it, merely to expand it. Get the jab if you’re not disqualified by special health conditions. Don’t disqualify yourself by indifference or groundless suspicions. But bear in mind that virus season doesn’t end with the first swallows of spring. We’re in it for the duration.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#H5N1#Flu#avian influenza#influenza#RSV#Mpox#HIV
61 notes
·
View notes
Text
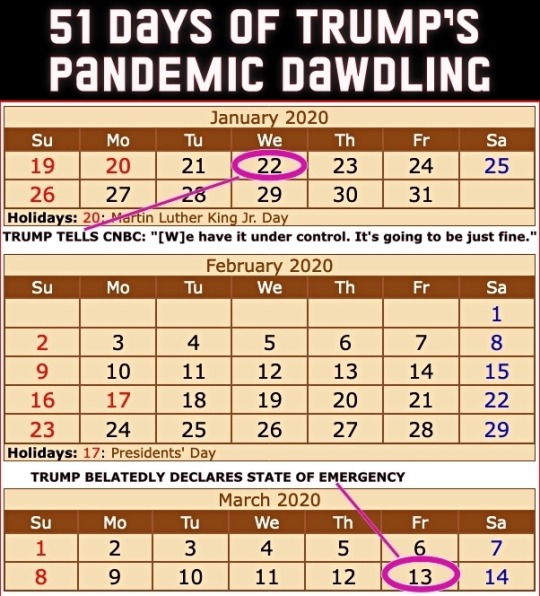
Four years ago today (March 13th), then President Donald Trump got around to declaring a national state of emergency for the COVID-19 pandemic. The administration had been downplaying the danger to the United States for 51 days since the first US infection was confirmed on January 22nd.
From an ABC News article dated 25 February 2020...
CDC warns Americans of 'significant disruption' from coronavirus
Until now, health officials said they'd hoped to prevent community spread in the United States. But following community transmissions in Italy, Iran and South Korea, health officials believe the virus may not be able to be contained at the border and that Americans should prepare for a "significant disruption." This comes in contrast to statements from the Trump administration. Acting Department of Homeland Security Secretary Chad Wolf said Tuesday the threat to the United States from coronavirus "remains low," despite the White House seeking $1.25 billion in emergency funding to combat the virus. Larry Kudlow, director of the National Economic Council, told CNBC’s Kelly Evans on “The Exchange” Tuesday evening, "We have contained the virus very well here in the U.S." [ ... ] House Speaker Nancy Pelosi called the request "long overdue and completely inadequate to the scale of this emergency." She also accused President Trump of leaving "critical positions in charge of managing pandemics at the National Security Council and the Department of Homeland Security vacant." "The president's most recent budget called for slashing funding for the Centers for Disease Control, which is on the front lines of this emergency. And now, he is compounding our vulnerabilities by seeking to ransack funds still needed to keep Ebola in check," Pelosi said in a statement Tuesday morning. "Our state and local governments need serious funding to be ready to respond effectively to any outbreak in the United States. The president should not be raiding money that Congress has appropriated for other life-or-death public health priorities." She added that lawmakers in the House of Representatives "will swiftly advance a strong, strategic funding package that fully addresses the scale and seriousness of this public health crisis." Senate Minority Leader Chuck Schumer also called the Trump administration's request "too little too late." "That President Trump is trying to steal funds dedicated to fight Ebola -- which is still considered an epidemic in the Democratic Republic of the Congo -- is indicative of his towering incompetence and further proof that he and his administration aren't taking the coronavirus crisis as seriously as they need to be," Schumer said in a statement.
A reminder that Trump had been leaving many positions vacant – part of a Republican strategy to undermine the federal government.
Here's a picture from that ABC piece from a nearly empty restaurant in San Francisco's Chinatown. The screen displays a Trump tweet still downplaying COVID-19 with him seeming more concerned about the effect of the Dow Jones on his re-election bid.

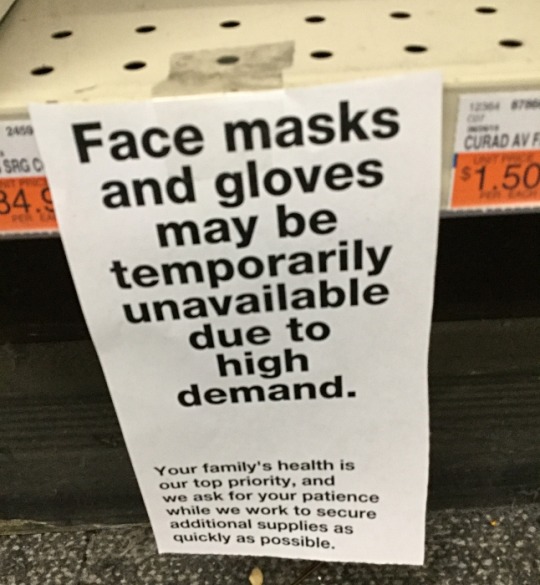
People were not buying Trump's claims but they were buying PPE.
I took this picture at CVS on February 26th that year.
The stock market which Trump in his February tweet claimed looked "very good" was tanking on March 12th – the day before his state of emergency declaration.

Trump succeeded in sending the US economy into recession much faster than George W. Bush did at the end of his term – quite a feat!. (As an aside, every recession in the US since 1981 has been triggered by Republican presidents.)
Of course Trump never stopped trying to downplay the pandemic nor did he ever take responsibility for it. The US ended up with the highest per capita death rate of any technologically advanced country.
Precious time was lost while Trump dawdled. Orange on this map indicates COVID infections while red indicates COVID deaths. At the time Trump declared a state of emergency, the virus had already spread to 49 states.

The United States could have done far better and it certainly had the tools to do so.
The Obama administration had limited the number of US cases of Ebola to under one dozen during that pandemic in the 2010s. Based on their success, they compiled a guide on how the federal government could limit future pandemics.
Obama team left pandemic playbook for Trump administration, officials confirm
Of course Trump ignored it.
Unlike those boxes of nuclear secrets in Trump's bathroom, the Obama pandemic limitation document is not classified. Anybody can read it – even if Trump didn't. This copy comes from the Stanford University Libraries.
TOWARDS EPIDEMIC PREDICTION: FEDERAL EFFORTS AND OPPORTUNITIES IN OUTBREAK MODELING
Feel free to share this post with anybody who still feels nostalgic about the Trump White House years!
#covid-19#coronavirus#pandemic#public health#donald trump#trump's incompetent response to the pandemic#covid state of emergency#2020#trump recession#51 days of trump pandemic dawdling#obama pandemic playbook#2010s ebola outbreak#nostalgia for trump administration#republicans#election 2024#vote blue no matter who
113 notes
·
View notes
Text
"Today, December 20, marks the official end of the Marburg Virus Disease outbreak in Rwanda. It has been 42 days – two full incubation periods – since the last confirmed case left the national Marburg treatment centre after testing negative.
In previous outbreaks, Marburg, which is caused by a virus related to Ebola, has killed up to 88 per cent of people infected. And Rwanda had never seen this disease within its borders before the current outbreak began in September. Despite Rwandan physicians having never encountered it before, the mortality rate observed in this outbreak is under 23 per cent – the lowest-ever death rate for a Marburg outbreak in Africa.
While the virus initially spread fiercely in two major hospitals in the capital Kigali and among family members of one of the initial cases, Rwanda’s rapid response, with implementation of strict infection prevention and control, isolation and containment of cases, prompt initiation of aggressive supportive care, delivery of investigational therapeutics and vaccines, and tracing and monitoring of contacts quickly brought the outbreak under control. The rate of new cases halved between the outbreak’s second and third weeks and dropped by around 90 per cent thereafter.
One of the most remarkable aspects of this response was an international effort, initiated and led by the Rwandan government, to administer thousands of doses of a promising experimental vaccine to front-line health workers under a clinical trial protocol, with the first subjects vaccinated in a remarkably short timeframe.
...
Rwanda, for its part, has invested heavily in its healthcare system and has incorporated epidemic preparedness into its national health policies. Rwanda has well-trained medical staff working in well-run hospitals and community-based health services. It has been investing in technology-based disease surveillance systems and its laboratories can handle fast, accurate diagnostic testing at scale.
In early September, after months of planning, Rwandan scientists and health officials joined CEPI and other private sector partners to walk through a “tabletop exercise” about the 100 Days Mission. It was through this in-person training exercise that key relationships between disease outbreak experts, Rwandan health authorities and researchers, vaccine developers and clinical trial specialists were cemented.
...
We also have no doubt that with the right focus and funding, such nationally-led, globally-supported, life-saving responses to novel disease outbreaks could be accomplished by any government in any region. By taking a proactive approach and using the 100 Days Mission as a game plan, all countries can get ahead of epidemic and pandemic threats and neutralise their catastrophic potential."
Read the full piece here: https://www.telegraph.co.uk/global-health/science-and-disease/partnerships-preparedness-halted-rwanda-marburg-outbreak/
https://www.telegraph.co.uk/global-health/science-and-disease/partnerships-preparedness-halted-rwanda-marburg-outbreak/
42 notes
·
View notes
Text
NIH pumped another $2.26 million into CSU's risky biolab, despite EcoHealth's suspension and fears of deadly virus leaks.
Jon Fleetwood
Nov 01, 2024
In a timely revelation during Halloween’s Bat Week (October 24–31), new federal funding has been allocated to Colorado State University’s (CSU) bat research facility in Fort Collins, Colorado, stoking opposition from public health advocates and government officials alike.
CSU’s work with “select agents”—pathogens like Ebola deemed severe threats by the CDC—means the university participates in work involving dangerous viruses under high-security conditions, raising concerns about public safety and containment risks.
According to records recently obtained by the White Coat Waste Project (WCW), CSU’s lab—which is set to experiment on dangerous viruses using bats imported from Asia—received an additional $2.26 million from the National Institutes of Health (NIH) last month.
In recent days, WCW has released photos obtained via Colorado Open Records Act (CORA) requests, showing scenes of bat hunting and experimentation associated with the CSU lab project.
29 notes
·
View notes
Text

People will face terror and starve, many will die
The decimation of USAid is already having a terrible effect in some of the poorest places on the planet. It damages America: it will harm us all
An earthquake of magnitude 7.0 or above could not have caused more carnage. Recent floods in Asia and droughts in Africa have been catastrophic, yet they have inflicted less damage and affected fewer people than the sudden withdrawal of billions of dollars of US aid from the world’s most volatile hotspots and its most vulnerable people. Coming alongside President Trump’s plan for a US takeover of Gaza, the US administration’s resolve to shut down its international aid agency sends a clear message that the era when American leaders valued their soft power is coming to an end.
But while the Gaza plan is as yet only on the drawing board, USAid cuts – which will see funding slashed and just 290 of the more than 10,000 employees worldwide retained, according to the New York Times - have already begun to bite this week. We have seen the halting of landmine-clearing work in Asia, support for war veterans and independent media in Ukraine, and assistance for Rohingya refugees on the border of Bangladesh. This week, drug deliveries to fight the current mpox and Ebola outbreaks in Africa have been stopped, life-saving food lies rotting at African ports, and even initiatives targeting trafficking of drugs like fentanyl have been cut back. One of the world’s most respected charities, Brac, says that the 90-day blanket ban on helping vulnerable people is depriving 3.5 million people of vital services.
One critical programme has been granted a limited waiver. Pepfar, created by Republican president George W Bush, offers antiretroviral prescriptions to 20 million people around the world to combat HIV and Aids. Its activities escaped the ban only after warnings that a 90-day stoppage could lead to 136,000 babies acquiring HIV. But it has still been blocked from organising cervical cancer screening, treating malaria, tuberculosis and polio, assisting maternal and child health, and efforts to curtail outbreaks of Ebola, Marburg and mpox.
Not only does the stop-work edict mean that, in a matter of days, the US has destroyed the work of decades building up goodwill around the world, but Trump’s claim that America has been over-generous is exposed as yet another exaggeration. Norway tops the list as biggest donor of official development assistance (ODA) as a percentage of gross national income (GNI) at 1.09%; Britain is at just over 0.5%, albeit down from the UN target of 0.7%; but the US is near the bottom of the advanced economies at 0.24% – alongside Slovenia and the Czech Republic. It is simply the size of the US economy – 26% of world output – that means that the 0.24% adds up to more aid than any other country. The US provided $66bn in 2023, making USAid a leader in global humanitarian aid, education and health, not least in addressing HIV/Aids, malaria and tuberculosis.
On Sunday night, Trump told reporters that USAid had been “run by a bunch of radical lunatics, and we’re getting them out”. “I don’t want my dollars going towards this crap,” his press spokesperson added, with one of the president’s chief advisers Elon Musk calling the agency a “viper’s nest of radical-left marxists who hate America”. “You’ve got to basically get rid of the whole thing. It’s beyond repair,” he said. “We’re shutting it down.”

Indeed, in a post on X last weekend, Musk shared a screenshot quoting the false claim that “less than 10 percent of our foreign assistance dollars flowing through USAID is actually reaching those communities”. The implication is that the remaining 90% was diverted, stolen, or just wasted. In fact, the 10% figure is the proportion of the budget going directly to NGOs and organisations in the developing world. The remaining 90% is not wasted – instead, it comprises all the goods and services that USAid, American companies and NGOs, and multilateral organisations deliver in kind, from HIV drugs to emergency food aid, malaria bed nets, and treatment for malnutrition. It is simply untrue that 90% of aid falls into the wrong hands and never reaches the most vulnerable.
In fact, the initial blanket executive order proved to be such a blunt instrument – the only initial exemptions were for emergency food aid and for military funding for Israel and Egypt – that it had to be modified to include exceptions for what the government called “life-saving humanitarian assistance”, although it stopped short of defining them. “We are rooting out waste. We are blocking woke programs. And we are exposing activities that run contrary to our national interests. None of this would be possible if these programs remained on autopilot,” said a statement released by the state department. The new secretary of state, Marco Rubio, now wants his department to control the whole budget and close down USAid entirely. “Does it make America safer? Does it make America stronger? Does it make America more prosperous?” Rubio asked in a statement that suggested that the America which generally worked multilaterally in a unipolar era is now determined to act unilaterally in a multipolar one.
This new stance is not just “America first” but “America first and only” – and a gift to Hamas, IS, the Houthi rebels, and all who wish to show that coexistence with the US is impossible. The shutdown is also good news for China, whose own global development initiative will be strengthened as it positions itself to replace America. Desperate people will turn to extremists who will say that the US can never again be trusted. And by causing misery and by alienating actual and possible allies, far from making America great again, the cancellation of aid will only make America weaker.
The tragedy for the planet is that US aid cuts come on top of diminishing aid budgets among the world’s richest economies, from Germany to the UK. International aid agencies are now so underfunded that in 2024, for the second consecutive year, the UN covered less than half of its humanitarian funding goal of nearly $50bn – at a time when increasing conflicts and natural disasters necessitate more relief donor grants than ever. Yes, we can discuss how greater reciprocity can create a fairer system of burden sharing – but further cuts in aid threaten more avoidable deaths, and a poorer world will ultimately make the US poorer too.
US generosity is often seen as mere charity, but it is in the country’s self-interest to be generous because the creation of a more stable world benefits us all. We all gain if USAid can mitigate the spread of infectious diseases, prevent malnutrition in the Democratic Republic of the Congo and Sudan, halt the upsurge of IS in Syria and support a fair, humanitarian reconstruction of Gaza and Ukraine. Only the narrowest and most blinkered view of what constitutes “America first” can justify the disaster America has unloaded on the world.
Daily inspiration. Discover more photos at Just for Books…?
17 notes
·
View notes
Text
All The Women’s News You Missed This Week
1/27/25-2/3/25
The assault on women’s reproductive rights continues as the Global Gag Rule is reinstated, anti-abortion states begin to crack down on abortion pill providers out of state, Instagram suppresses networks helping women access medication to terminate pregnancies, Individuals who sought passports matching gender identity are effectively banned from leaving the country.
Please get involved in Wednesday’s nationwide protest if you are able.
At this moment, I understand it’s easy to tune out of politics but I cannot stress how important it is to stay engaged in a sustainable (and efficient way). The current moment is not ideal, but within it contains not only the responsibility to do what we can to mitigate the worst effects of far-right fascism but also the opportunity to capitalize on the collapse of the mainstream Democratic party and promote a brand of feminism that actually centers women. Gender ideology, along with the entire package of social justice positions that gained popularity in the post-Obama era, is dead. What will come after it? An even more regressive form of biological essentialism where women are “valued” as breeders for the Riech? A form where gays and lesbians are labeled as ‘deviant’ and ‘child-groomers’, carrying the stigma of gender ideology even if we were overwhelmingly its victims? We must stay engaged, we need to continue to meet this moment by building a left with a base solid enough to fight fascism and win.
Want this in your inbox instead? Subscribe here
In lighter news at the U.S. Grammy Awards, female artists swept the night, with Beyonce finally winning Best Album of the Year and Best Country Album, Sabrina Carpenter winning Best Pop Album, Doechii winning Best Rap Album, and Chappell Roan winning Best New Artist (and making an impactful speech about artist right’s as employees).
In my favorite clip of the week, Grammy winner Doechii performs a melody featuring her breakout hit song ‘Denial is a River’ and an up-and-coming song ‘Catfish’ from her album ‘Alligator Bites Never Heal’.
BestWATCH: Doechii at the 2025 Grammys
ACTION:
Implement Higher Minimum Sentences for Rape in Texas.
PROTEST WEDNESDAY 2/5 ALL US STATES
Promotional Collaborators:
A list of feminist projects I have entered agreements with to cross-promote. Would you and your project or content like to be featured? Email me.
Femme Front, a radical feminist space to hang out, talk politics, and make friends! Ages 13+
Reproductive Rights:
Trump Reinstates Global Gag Rule, an Assault on Women’s Health around the World
New York doctor indicted for prescribing Louisiana teen abortion pill
South Dakota birthing risks rise as another hospital ends service
Polish appeals court to rule next month in abortion case which activists say could set a precedent
‘I won’t regret this’: young women turn to sterilization as Trump intensifies war on reproductive rights
Groups helping Americans find abortion pills report Instagram ‘shadow-banning’
LGBT:
The ‘Emilia Pérez’ backlash, explained
Trump signs order restricting gender care for young people
'I feel like I’m stuck here': Trans, nonbinary Americans' passports remain in limbo
Women in the News:
Devotees pay homage to Afro-Brazilian sea goddess on Rio de Janeiro beach
Pug life: A South African woman has rescued more than 2,500 of the lovable ‘clowns of the dog world’
Who is Karoline Leavitt, the youngest White House press secretary?
Decoding Melania Trump's new official portrait
Kate photographed by Prince Louis to mark World Cancer Day
Nurse dies as Uganda confirms new Ebola outbreak
Singapore influencer fined over false abduction claim
How 'trailblazer' nun St Brigid continues to fascinate
Women’s Rights:
US Government Department to Tie Funding to Marriage and Birth Rates
Taliban minister ‘forced to flee Afghanistan’ after speech in support of girls’ education
Trump Orders Schools to Ease Sex Assault Rules
Republicans Want Child Marriage Ban Exemption for Military Members
The risk to women's health in Afghanistan: 'The consequences of this segregation are catastrophic'
Women Fighting Back:
Peru’s disappeared: Dozens look for relatives lost to violence. A woman who knows their sorrow helps
WATCH: Chappell Roan calls for livable wages and healthcare for small artists in brave Grammy speech
Disgraceful that videos seen by Southport killer still online, says Cooper
How a kabaddi club in India is changing girls' lives
Argentines protest President Milei’s diatribe against ‘wokeism’ at Davos
From missing goats to health tips: how a female-run radio station is giving rural India a voice
Feminist Wins:
Coercive control to be treated like other domestic abuse offences
AI-generated child sex abuse images targeted with new laws
Male Violence:
Abu Hatem Shaqra (Ahmad al-Hayes), war criminal responsible for the murdering of Hevrin Khalaf and the desecration of her body, sanctioned for crimes including "trafficking of Yazidi women & children, is now gaining power within the "new Syrian government."
Violence against women and girls growing, says watchdog (UK)
Hundreds of stayed sexual assault cases send chilling message to victims, advocates warn (CA)
US teen shot dead by father in Pakistan over TikTok videos
Film director found guilty of sexual assault in France’s first big #MeToo trial
‘No man would want to touch you’: UCL professor accused of ‘harassing’ student protestor
Spain's former football boss on trial over World Cup kiss
France prepares for trial of surgeon accused of abusing anaesthetised children
Caroline Kennedy warns senators that cousin RFK Jr. is a ‘predator’
Blake Lively and Justin Baldoni lawyers spar during first court hearing
Secretive Christian sect coerced young mothers to give up babies
Harvey Weinstein begs for earlier retrial for sex crimes
Sara Sharif family court judges named after appeal
Man who drugged wife and plotted her mass rape questioned over 1990s attacks
‘Rape is effectively decriminalised’: how did sexual assault become so easy to get away with (AUS)
Grammys Highlights:
WATCH: Beyoncé wins Grammy album of the year
WATCH: Doechii wins best new rap album, 3rd woman ever to receive this honor!!!
Tems sees off Yemi Alade and Burna Boy to win Grammy
Amy Allen becomes first woman to win best songwriter Grammy
Arts and Culture:
Teenage actress takes on child marriage in role mirroring real life
Taiwanese actress Barbie Hsu, star of the popular drama ‘Meteor Garden,’ dies at age 48
Movie Review: Bloody and witty, ‘Companion’ explores what humanity means in an AI-powered world
Lady Gaga announces March release for new album ‘Mayhem’
Emilia Pérez star says she will stay in Oscars race despite row
Investigative/Opinon:
Inside Iran's Epidemic Of 'Honor' Killings: One Woman Killed Every Two Days
READ OR LISTEN: Why Patriarchy? Foragers, Farmers, and the Origins of Gender Inequality
As always, this is global and domestic news from a US perspective covering feminist issues and women in the news more generally. As of right now, I do not cover Women’s Sports. Published each Monday afternoon.
#radblr#radical feminism#radical feminist#char on char#radical feminists do touch#radfem safe#radical feminist theory#radfem#radfems#Women Talking About Their Lives#Feminism
8 notes
·
View notes
Text
For years, Robert F. Kennedy Jr., U.S. President Donald Trump’s pick as secretary of the Department of Health and Human Services (HHS), has spread conspiracy theories and factually incorrect information about vaccination, drug regulation, epidemiology, and biomedical science in general to advance his skepticism of evidence-based science and medicine.
The anti-vaccine organization Kennedy helped found, Children’s Health Defense, has conducted extensive disinformation campaigns, including funding propaganda films such as Plandemic, the Vaxxed trilogy, and Medical Racism: The New Apartheid, which specifically targeted Black Americans to discourage vaccination. The scale of the destruction Kennedy could wreak at the helm of HHS is immense.
HHS is tasked with overseeing government efforts to take care of the American people, and its 10 component agencies, from the Food and Drug Administration (FDA) to the National Institutes of Health (NIH), play different specialized roles to do so. Kennedy has already floated some of his ideas that would harm public health in the United States, including ending water fluoridation; rescheduling or withdrawing regulatory approval for numerous vaccines; reshaping the drug approval process and removing lifesaving drugs from the market; giving infectious disease research a “break”; and lifting food safety regulations on some products, such as unpasteurized “raw” milk, while imposing new regulations on others.
Even small changes to these essential functions of HHS would have catastrophic consequences without Kennedy needing to ban vaccines. Prior to the COVID-19 pandemic, Kennedy used the tragic deaths of two infants from mis-formulated measles vaccines in Samoa to advance his theories. Kennedy flew to Samoa to support a campaign that falsely suggested that vaccination was unsafe and potentially deadly. Several months later, a massive measles outbreak sickened nearly 6,000 people and left 83 dead, most of them young children. Curtailing routine childhood immunizations would conservatively result in more than a million preventable deaths in the United States.
Highly pathogenic emerging viruses—such as the Ebola virus, avian influenza viruses, and coronaviruses such as SARS-CoV-2, the cause of the COVID-19 pandemic—often appear unexpectedly and, if not effectively contained, cause epidemics and pandemics. Imagining worst-case scenarios about outbreaks is essential for preparing for, responding to, and ideally preventing pandemics altogether.
As a virologist who specializes in such outbreaks, having Kennedy at the helm of HHS during an outbreak of a lethal virus is the worst pandemic scenario I can conceive—and it’s a worryingly real possibility. A massive outbreak of H5N1 highly pathogenic avian influenza has impacted nearly a thousand herds of dairy cattle across 16 states. The cattle outbreak began in late 2023 with a single spillover from an infected bird in Texas because of the global H5N1 panzootic (a pandemic in animals) that has been ongoing since 2021. Because H5N1-infected cows were not detected for several months, animal transport and milking operations allowed the virus to spread throughout the United States.
More than a year later, the full scope of the cattle outbreak remains unknown. Spillovers from wild birds into domestic poultry have continued and necessitated culling millions of birds. As the tally of infected dairy herds and poultry flocks has risen, human cases have also increased at an alarming rate. Currently, there are more than 70 confirmed or probable cases, including the first cases with severe disease and the first fatal case in the United States. Multiple studies show that a substantial number of H5N1 cases in dairy workers are likely going undetected.
More troublingly, three cases of H5N1 have occurred in children in California, one of which is linked to consumption of raw milk, and spillovers directly from birds also continue with increasing frequency. Although there is no evidence that human-to-human transmission has occurred, the biological reality is that with enough opportunities to adapt to a human host and potentially reassort with seasonal influenza viruses, H5N1 could gain this ability. If that happens, a rapid and effective response will be imperative for containment. If efforts to detect and contain a human outbreak fail, an influenza pandemic is a very real possibility.
Nobody can say with certainty when or if this will happen, but we can anticipate what might happen if it does under Kennedy’s leadership. Although the COVID-19 pandemic response in the United States was replete with mistakes, the first Trump administration did manage to execute some critical interventions that were largely attributable to HHS agencies’ actions.
The initial research on COVID-19 vaccines was conducted at the Vaccine Research Center at NIH in collaboration with NIH-funded academic investigators. The immediate action of these scientists that hastened the research into a development pipeline comprising pre-clinical studies and clinical trials was essential to producing mRNA vaccines at national scale within a year. Operation Warp Speed—which was a joint effort among multiple HHS agencies including the Centers for Disease Control and Prevention (CDC), NIH, and FDA, the Department of Defense, and the private sector—allowed for nationwide distribution of the vaccines and saved millions of lives.
In the event of a bird flu pandemic, millions of lives will again depend on the urgent actions taken by HHS and its component agencies. However, unlike the COVID-19 pandemic, these responses would be orchestrated by someone who promotes conspiracy theories, questions established tenets of science and medicine, and has significant financial interest in pseudoscientific profiteering. Given that Aaron Siri, the lawyer reportedly vetting Kennedy’s picks to lead HHS agencies, has previously petitioned FDA to withdraw or suspend the licenses on the polio and hepatitis B vaccines, it is likely these putative leaders would be equally unsuited to effectively lead essential pandemic responses.
Trump’s putative CDC director, Dave Weldon, is celebrated by anti-vaxxers for his consistent vaccination opposition. He rejects basic facts about vaccines, has appeared in several anti-vaccine documentaries, and is willing to dismiss reliable population-level data in favor of anecdotes.
The nominated FDA commissioner, Marty Makary, has stated that he may rethink current policies for approving diagnostics and medications, including vaccines. Until recently, Makary, a gastrointestinal surgeon who has indicated willingness to loosen food safety regulation and block essential medicines, also sat on an advisory board for Biosafety Now, an organization that opposes research on pandemic viruses, called for the prosecution of virologists, and whose founders have allegedly conducted harassment campaigns against virologists (including myself). Makary’s track record of COVID-19 pronouncements includes his prediction in early 2021 that America would reach “herd immunity” by April.
The nominated NIH director, Jay Bhattacharya, has been an outspoken opponent of critical research priorities. In early 2020, he co-authored a profoundly flawed study underestimating the severity of COVID-19 to bolster economic arguments for ending pandemic mitigation measures. Bhattacharya co-authored the Great Barrington Declaration (GBD), an anti-lockdown policy proposal recommending mass infection as a path to herd immunity, which studies estimate would have significantly increased deaths in the United States beyond the estimated 1.2 million Americans who died from COVID-19.
The GBD gave rise to the Brownstone Institute, where Bhattacharya was a regular content contributor. He has also appeared in a Falun Gong-produced documentary promoting anti-vaccine ivermectin conspiracy theories. He is deeply antagonistic to virology, vaccinology, and public health research, and, like Makary, was also affiliated with Biosafety Now, serving on the board of directors.
Finally, the nominee for the Centers for Medicare and Medicaid Services, Mehmet Oz, is a cardiothoracic surgeon and failed U.S. Senate candidate who used his television show as a vehicle for promoting unproven supplements to promote weight loss and has a long history of distributing medical misinformation. During the pandemic, he opposed masking and vaccination in favor of hydroxychloroquine and supplements he sold through social media.
The damage these figures could do would be exponentially magnified during a pandemic. Early identification of human cases is essential to isolate and contain a growing outbreak. This depends on CDC and state public health officials identifying human cases using sensitive, specific molecular diagnostic tests in combination with standard epidemiological approaches such as contact tracing. This would trigger critical containment measures and medical countermeasures—such as antivirals and vaccines—rapidly.
For H5N1, we are already failing to detect human cases thanks in part to a sluggish response from the CDC, the CDC’s self-imposed monopoly on confirmatory testing, and continued incompetence at developing effective tests.
If the FDA delays or withholds authorization for diagnostic tests, we will be powerless to contain the spread, particularly for very mild or asymptomatic cases that are less likely to be identified clinically but may still be contagious. At the beginning of the COVID-19 pandemic, the CDC and FDA’s technical ineptitude, poor quality control, and bureaucratic paralysis resulted in a nearly two-month period of undetected virus spread. Containment failed, and the virus established itself in the American population.
In early 2024, the CDC and FDA under the Biden administration repeated many of these errors with H5N1 diagnostic tests, although fortunately no human-to-human transmission has occurred to date. Still, delayed implementation of diagnostic testing further hampered elimination from dairy cattle and delayed diagnosing some human cases. It’s hard to imagine improvement in the Kennedy HHS.
A failure to contain a human H5N1 outbreak will be disastrous over the long term if there is no biomedical research occurring to understand it. Some of the greatest successes of the COVID-19 response were led by NIH-funded investigators, both within NIH itself and by academic scientists supported by extramural NIH grants. Such research can drastically accelerate the timeline for developing and deploying effective countermeasures and inform us where the virus is spreading, who is at the greatest risk, and what treatments work best to save lives.
Kennedy and Bhattacharya have proposed radically reorganizing NIH and reducing funding for infectious diseases and vaccine research. Ultimately, this would create a situation in which we know little about the virus, how it spreads, how it causes disease, or how to treat it. Vaccines would be unavailable, we’d have no information on resistance to antiviral drugs or a pipeline for developing other therapies, and we won’t know where cases are primarily occurring until the hospitals are overwhelmed with H5N1 patients. Our options for intervention would be limited to supportive care and unproven remedies embraced by Kennedy: thoughts, prayers, raw milk, and roadkill.
The devastating impacts of such failures across HHS will not be limited to America, since pandemics transcend national borders. Any suppression of effective public health policy by Kennedy will exacerbate economic, agricultural, ecological, and medical ruin at home and abroad. Anywhere from thousands to millions could die as a direct result.
9 notes
·
View notes
Text
Jonathan Cohn at HuffPost:
The federal government’s Morbidity and Mortality Weekly Report is arguably the closest thing we have to an early warning system for disease. In addition to summaries of new research findings, it includes essential information about outbreaks so that front-line professionals and officials know what to look out for ― and, eventually, how to respond. A 1981 edition contained the first reports of a mysterious virus, later identified as HIV, that was causing a lethal form of pneumonia in otherwise healthy young men. A report from 2014 had detailed information about an Ebola outbreak in Africa that would soon spread to the United States. And editions in early 2020 provided some of the earliest, most crucial data about COVID-19. The MMWR comes from the U.S. Centers for Disease Control and Prevention, which publishes it every Thursday. But as of Thursday evening, this week’s MMWR still hadn’t appeared. That is not an accident. In fact, it could be the first shot in President Donald Trump’s war on government science. On Tuesday, just one day after Trump returned to the White House, the officials he has put in charge of the Department of Health and Human Services circulated a memo ordering staff to pause all communications until Feb. 2 unless “reviewed and approved by a Presidential appointee.”
The memo ― first reported by The Washington Post and since obtained by other outlets, including HuffPost ― applies to the entire department and its agencies, including the CDC. And public communications isn’t the only thing Trump’s team has paused.
The officials also put a temporary stop to meetings and travel, including for the outside advisory groups that make recommendations for funding grants from the National Institutes of Health. Many of the scholars and scientists who serve on those panels said they heard about the stoppage just weeks or days before scheduled meetings ― or, in some cases, smack in the middle of meetings that were already taking place.
[...] Several public health veterans told HuffPost that prior administrations had also imposed pauses upon taking office. But these sources said they could not recall a halt to communication set to last so long ― or one that was nearly as sweeping.
The war on science and expertise under Tyrant 47, especially with a bird flu outbreak still ongoing, is highly dangerous.
See Also:
The Guardian: Trump’s health department cancels meetings and pauses communications
Salon: Donald Trump is not waiting for RFK Jr. — he has already started his war on public health
#Donald Trump#Robert F. Kennedy Jr.#Science#HHS#Department of Health and Human Services#Trump Misadministration#Trump Regime#Trump Administration II#Morbidity and Mortality Weekly Report#Pandemics#Bird Flu#Dorothy Fink#NIH#CDC
7 notes
·
View notes
Text
Here's the complete list of DHS flagged search terms. Don't use any of these on social media to avoid having the 3-letter agencies express interest in your activities!
DHS & Other Agencies
Department of Homeland Security (DHS)
Federal Emergency Management Agency (FEMA)
Coast Guard (USCG)
Customs and Border Protection (CBP)
Border Patrol
Secret Service (USSS)
National Operations Center (NOC)
Homeland Defense
Immigration Customs Enforcement (ICE)
Agent
Task Force
Central Intelligence Agency (CIA)
Fusion Center
Drug Enforcement Agency (DEA)
Secure Border Initiative (SBI)
Federal Bureau of Investigation (FBI)
Alcohol Tobacco and Firearms (ATF)
U.S. Citizenship and Immigration Services (CIS)
Federal Air Marshal Service (FAMS)
Transportation Security Administration (TSA)
Air Marshal
Federal Aviation Administration (FAA)
National Guard
Red Cross
United Nations (UN)
Domestic Security
Assassination
Attack
Domestic security
Drill
Exercise
Cops
Law enforcement
Authorities
Disaster assistance
Disaster management
DNDO (Domestic Nuclear Detection Office)
National preparedness
Mitigation
Prevention
Response
Recovery
Dirty Bomb
Domestic nuclear detection
Emergency management
Emergency response
First responder
Homeland security
Maritime domain awareness (MDA)
National preparedness initiative
Militia
Shooting
Shots fired
Evacuation
Deaths
Hostage
Explosion (explosive)
Police
Disaster medical assistance team (DMAT)
Organized crime
Gangs
National security
State of emergency
Security
Breach
Threat
Standoff
SWAT
Screening
Lockdown
Bomb (squad or threat)
Crash
Looting
Riot
Emergency Landing
Pipe bomb
Incident
Facility
HAZMAT & Nuclear
Hazmat
Nuclear
Chemical Spill
Suspicious package/device
Toxic
National laboratory
Nuclear facility
Nuclear threat
Cloud
Plume
Radiation
Radioactive
Leak
Biological infection (or event)
Chemical
Chemical burn
Biological
Epidemic
Hazardous
Hazardous material incident
Industrial spill
Infection
Powder (white)
Gas
Spillover
Anthrax
Blister agent
Exposure
Burn
Nerve agent
Ricin
Sarin
North Korea
Health Concern + H1N1
Outbreak
Contamination
Exposure
Virus
Evacuation
Bacteria
Recall
Ebola
Food Poisoning
Foot and Mouth (FMD)
H5N1
Avian
Flu
Salmonella
Small Pox
Plague
Human to human
Human to ANIMAL
Influenza
Center for Disease Control (CDC)
Drug Administration (FDA)
Public Health
Toxic
Agro Terror
Tuberculosis (TB)
Agriculture
Listeria
Symptoms
Mutation
Resistant
Antiviral
Wave
Pandemic
Infection
Water/air borne
Sick
Swine
Pork
Strain
Quarantine
H1N1
Vaccine
Tamiflu
Norvo Virus
Epidemic
World Health Organization (WHO and components)
Viral Hemorrhagic Fever
E. Coli
Infrastructure Security
Infrastructure security
Airport
CIKR (Critical Infrastructure & Key Resources)
AMTRAK
Collapse
Computer infrastructure
Communications infrastructure
Telecommunications
Critical infrastructure
National infrastructure
Metro
WMATA
Airplane (and derivatives)
Chemical fire
Subway
BART
MARTA
Port Authority
NBIC (National Biosurveillance Integration Center)
Transportation security
Grid
Power
Smart
Body scanner
Electric
Failure or outage
Black out
Brown out
Port
Dock
Bridge
Canceled
Delays
Service disruption
Power lines
Southwest Border Violence
Drug cartel
Violence
Gang
Drug
Narcotics
Cocaine
Marijuana
Heroin
Border
Mexico
Cartel
Southwest
Juarez
Sinaloa
Tijuana
Torreon
Yuma
Tucson
Decapitated
U.S. Consulate
Consular
El Paso
Fort Hancock
San Diego
Ciudad Juarez
Nogales
Sonora
Colombia
Mara salvatrucha
MS13 or MS-13
Drug war
Mexican army
Methamphetamine
Cartel de Golfo
Gulf Cartel
La Familia
Reynose
Nuevo Leon
Narcos
Narco banners (Spanish equivalents)
Los Zetas
Shootout
Execution
Gunfight
Trafficking
Kidnap
Calderon
Reyosa
Bust
Tamaulipas
Meth Lab
Drug trade
Illegal immigrants
Smuggling (smugglers)
Matamoros
Michoacana
Guzman
Arellano-Felix
Beltran-Leyva
Barrio Azteca
Artistics Assassins
Mexicles
New Federation
Terrorism
Terrorism
Al Queda (all spellings)
Terror
Attack
Iraq
Afghanistan
Iran
Pakistan
Agro
Environmental terrorist
Eco terrorism
Conventional weapon
Target
Weapons grade
Dirty bomb
Enriched
Nuclear
Chemical weapon
Biological weapon
Ammonium nitrate
Improvised explosive device
IED (Improvised Explosive Device)
Abu Sayyaf
Hamas
FARC (Armed Revolutionary Forces Colombia)
IRA (Irish Republican Army)
ETA (Euskadi ta Askatasuna)
Basque Separatists
Hezbollah
Tamil Tiger
PLF (Palestine Liberation Front)
PLO (Palestine Libration Organization)
Car bomb
Jihad
Taliban
Weapons cache
Suicide bomber
Suicide attack
Suspicious substance
AQAP (Al Qaeda Arabian Peninsula)
AQIM (Al Qaeda in the Islamic Maghreb)
TTP (Tehrik-i-Taliban Pakistan)
Yemen
Pirates
Extremism
Somalia
Nigeria
Radicals
Al-Shabaab
Home grown
Plot
Nationalist
Recruitment
Fundamentalism
Islamist
Weather/Disaster/Emergency
Emergency
Hurricane
Tornado
Twister
Tsunami
Earthquake
Tremor
Flood
Storm
Crest
Temblor
Extreme weather
Forest fire
Brush fire
Ice
Stranded/Stuck
Help
Hail
Wildfire
Tsunami Warning Center
Magnitude
Avalanche
Typhoon
Shelter-in-place
Disaster
Snow
Blizzard
Sleet
Mud slide or Mudslide
Erosion
Power outage
Brown out
Warning
Watch
Lightening
Aid
Relief
Closure
Interstate
Burst
Emergency Broadcast System
Cyber Security
Cyber security
Botnet
DDOS (dedicated denial of service)
Denial of service
Malware
Virus
Trojan
Keylogger
Cyber Command
2600
Spammer
Phishing
Rootkit
Phreaking
Cain and abel
Brute forcing
Mysql injection
Cyber attack
Cyber terror
Hacker
China
Conficker
Worm
Scammers
Social media
SOCIAL MEDIA?!
21 notes
·
View notes
Text
INSANITY: The WHO Are Tyrants “In the World Health Organization's founding charter, they wrote an absolute amnesty for all criminal acts conducted by themselves, including murder by the way. By law, not a single one of them cannot only be tried and prosecuted, they can't even be investigated.
Now I wonder if there are examples in the history of the WHO of where that amnesty has been implemented or effective or where its boundaries might likely be tested.
Let's keep it really current. Remember that in 2018, during the Ebola clinical trials run by the World Health Organization in Africa, it was very clear that remdesivir, the drug that was promoted by doctor Deborah Birx and doctor Anthony Fauci as a drug for the treatment of COVID. The World Health Organization and its infinite wisdom and high morality decided that remdesivir was actually too lethal to inject into Africans. And that is because the fatality rate of people exposed to remdesivir in the Ebola trials was 53%. And the bad news about that number is that Ebola doesn't kill 53%.
You get over Ebola. You don't get over remdesivir.
15 notes
·
View notes
Text
First a heads-up. Nobel economics laureate Paul Krugman has retired from the New York Times. But he is now fairly active at his Substack. Occasionally we'll be linking some of his work there.
In this piece, Dr. Krugman argues that the MAGA war on the "deep state" is also a war on America's health.
One enduring theme of the MAGA movement has been hostility toward the “deep state” — what people outside the movement might call professional civil servants. Trump and company believe that the deep state is out to get them, which is paranoid. But they’re not wrong to believe that public employees who see themselves as working for the nation rather than for whoever currently occupies the White House pose a problem for their agenda. So what will MAGA do, now that it’s in power? Many observers, myself included, have focused on plans to convert a number of civil service jobs into political appointments. But just a few days into the new regime it’s clear that the assault on professional government will be much broader than that — that it will involve an effort to intimidate and politicize civil servants, too. And early indications are that one prime target will be agencies devoted to protecting public health. [ ... ] Public health agencies, even more than the rest of the government, are in the firing line. You can’t talk seriously about health policy without taking race and gender into account; yet according to the New York Times, one contractor collecting demographic data for the Centers for Medicare and Medicaid Services has already been told to stop work, and the results of an already completed survey won’t be released. But wait, there’s more: federal health agencies, including the Food and Drug Administration, the Centers for Disease Control and the National Institutes for Health, have been ordered to pause all external communications, including health advisories and scientific reports. NIH, in particular, appears to have been effectively put in lockdown, with even routine meetings canceled and employees forbidden to travel.
He concludes...
If MAGA had been around at the time, do you have any doubts that it would have opposed all of these public health measures and accused their proponents of being part of some dark conspiracy? And when — not if — the next pandemic strikes, do you expect our battered, politicized public health agencies to keep Americans properly informed? If Trump is still in charge, do you expect him to respond effectively, as opposed to minimizing the threat and muzzling anyone who might contradict him? It’s hard to feel optimistic about any of these concerns.
Did I just hear the word "pandemic"? There is some distressing news out of Uganda from the Washington Post.
Uganda announced Thursday that a nurse, 32, had died of Ebola in the capital, Kampala, amid a new outbreak of the deadly virus there — the first in two years. The country has activated emergency response procedures, officials said. Uganda registered 164 cases and 55 confirmed deaths from Ebola over four months in late 2022. That outbreak ended early the following year. The patient died after experiencing fever-like symptoms and seeking treatment at several hospitals and from a traditional healer, Diana Atwine, permanent secretary of the Health Ministry, said in a statement on Thursday. His fever, chest pain and breathing difficulty progressed to unexplained bleeding, a common symptom of a severe case of Ebola. Forty-four close contacts have been cited for tracing, including 30 health workers and patients from a hospital and 11 family members.
Ebola makes COVID seem like a fun disease. The mortality rate for the 2014 outbreak of Ebola in West Africa was around 40%. The Obama administration took decisive action to limit Ebola in the United States. Thanks to quick science-based action, the number of Ebola cases in the US was limited to 11 (eleven). Out of the 11, just 2 cases were contracted inside the US. 2 of the 11 died – 18.2% or less than half of the international rate.
At the end of the Obama administration, his National Security Council staff authored a guide called "Playbook for Early Response to High-Consequence Emerging Infectious Disease Threats and Biological Incidents" and left it for Trump to use. Of course Trump ignored it.
Trump team failed to follow NSC’s pandemic playbook
The first COVID-19 case appeared in the US on 21 January 2020. Instead of taking decisive measures recommended in the Obama pandemic playbook, Trump said this to his favorite CNBC host.

While Trump dawdled and did the usual Trumpian things like rage tweet about the 2020 Oscars, the virus spread throught the US. He only got around to declaring a pandemic emergency on Friday the 13th of March – a day after the stock markets crashed.
^^^ dark red = deaths, orange/pink = infections
By March 13th, COVID-19 had spread to 49 states and DC. Ultimately, at least 30% of the US population became infected and 1.14 million deaths were reported.
If Ebola spreads to the US while Trump and RFK Jr. are in charge, expect a catastrophe.
#donald trump#trump incompetence#maga#healthcare#civil servants#public health#public health agencies#cdc#nih#fda#medicare#medicaid#pandemics#ebola#playbook for early response to high-consequence emerging infectious disease threats and biological incidents#barack obama#obama administration#covid-19#trump's pandemic response#paul krugman
18 notes
·
View notes
Text
Also preserved on our archive
By Tarun Sai Lomte
New research reveals how lingering viral activity and immune disruption contribute to long COVID, highlighting novel therapeutic strategies that could change the course of treatment for millions.

A recent study published in the journal Cell reviewed the current state of knowledge on the pathophysiology and biology of long COVID.
Coronavirus disease 2019 (COVID-19) can affect health over the long term. Although it is self-limited in most individuals, some infected individuals experience post-acute sequelae, including fatigue, cognitive dysfunction, and muscle weakness, among others. While more common after severe COVID-19, individuals with a history of mild or moderate severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have the highest burden.
The World Health Organization (WHO) defines post-COVID-19 condition as unexplained symptoms persisting ≥ two months that manifest ≥ three months after SARS-CoV-2 infection. Further, while many countries have adopted this definition, several have formulated their own definitions. The patient community that first identified the condition prefers the term long COVID.
Overall, the definitions vary in the time scale on which the condition is defined and whether the condition is restricted to unexplained patient-reported symptoms or inclusive of incident medical diagnoses/laboratory abnormalities. The present study reviewed the epidemiology of long COVID, with emphasis on how the underlying mechanisms explain the physiology. Additionally, the study highlights how symptom clusters, identified through techniques like cluster analysis in electronic health records (EHR), could improve long COVID diagnosis by linking specific biological drivers to clinical endotypes.
Epidemiology and clinical features of long COVID There are variations in epidemiological estimates of long COVID across variants, populations, and regions. Some studies suggest a prevalence of 30% or higher but define the syndrome as new unexplained symptoms, which might lead to misclassification. Not all symptoms may be related to SARS-CoV-2; as such, other conditions must be ruled out. Determining what is new after infection and what might be unmasking of sub- or pre-clinical conditions is a significant challenge.
Further, SARS-CoV-2 is not the only virus associated with protracted symptoms. Studies have estimated that 18 million adults in the United States (US) might suffer from long COVID. The WHO and the Institute for Health Metrics and Evaluation estimated that one in 30 European individuals had long COVID in the first three years of the COVID-19 pandemic. Globally, an estimated 65 million individuals have long COVID.
Notably, the epidemiology of severe, disabling long COVID-19 is unknown. Long COVID can manifest during or weeks after the acute infection. Cognitive problems, fatigue, and post-exertional symptoms are the most common. In addition, symptom clustering based on organ systems, such as autonomic dysfunction, neurocognitive impairment, and exercise intolerance, offers a more precise understanding of long COVID phenotypes. Further, many symptoms of long COVID overlap with those of other infection-associated chronic conditions (IACCs), such as chronic Lyme disease, post-Ebola disease, post-Giardiasis, and myalgic encephalitis/chronic fatigue syndrome, among others.
Biological drivers of long COVID The biological drivers of long COVID are upstream processes, such as perturbations of the coagulation system and immunity, which do not directly cause disease but instead drive one another, leading to downstream physiological changes that manifest as symptoms. Some of these biological processes, like clotting and immune dysfunction, may interact, creating a cycle of chronic inflammation and tissue damage. Microclots, resistant to fibrinolysis, have been detected in long COVID patients and may contribute to tissue hypoxia and organ dysfunction. There are also associations between viral activity levels during infection and long COVID risk, with higher viral replication linked to more severe illness.
Long COVID risk appears to be lower with Omicron variants. The protective effect of antiviral therapy and vaccination suggests that viral replication and transmission during the acute phase is a significant determinant of long-term outcomes. Therefore, early COVID-19 interventions could mitigate long COVID and support pursuing robust preventive agenda.
Early in the pandemic, it was commonly assumed that SARS-CoV-2 infection would be transient; however, this was challenged by reports that viral proteins and nucleic acids could be detected months after infection. Although the precise anatomic site of viral persistence is unclear, there is consensus that persistence is tissue-backed. Various studies have linked immune dysfunction and inflammation with long COVID.
Many studies have focused on the role of inflammatory macrophages and monocytes in long COVID. Mast cell activation might also contribute to long COVID. Although not infected by SARS-CoV-2, external triggers can activate mast cells. Severe COVID-19 is also associated with autoimmunity. COVID-19 is also associated with a higher incidence of autoimmune conditions, such as lupus, Sjogren’s syndrome, inflammatory bowel disease, and rheumatoid arthritis.
Acute SARS-CoV-2 infection can lead to a hypercoagulable state and elevate the risk of thromboembolic events. Interactions between the spike protein and fibrinogen may result in abnormal clots that can trigger microglia activation in the brain, potentially contributing to neurocognitive symptoms of long COVID. Clotting has been implicated as a long COVID mechanism, with aggregates of platelets and clotting proteins detected in affected individuals.
Clinical physiology of long COVID The most efficient explanation for long COVID is tissue damage mediated by SARS-CoV-2 that was initiated during (initial) infection. Pancreatic infection by SARS-CoV-2 has been implicated in post-COVID-19 diabetes, another form of the post-acute sequelae, offering proof of principle. Endothelial dysfunction has been suggested to be involved in long COVID.
Various mechanisms might lead to endothelitis and macrovascular diseases, and their end-organ consequences could result in long COVID. Additionally, the study suggests that microclots and endothelial dysfunction could impair tissue perfusion, leading to organ damage and contributing to persistent symptoms such as fatigue and cognitive issues. Disruption of the gut-brain axis enables a direct connection between post-COVID-19 processes and disruption of normal physiology, including brain fog, autonomic dysfunction, and abnormal stress responses.
Brain fog, i.e., problems with memory, concentration, and attention, is among the most debilitating manifestations of long COVID. It has been a prominent symptom among non-hospitalized patients since the early pandemic. Some people, especially those with diabetes, learning and attention disorders, and substance, have a predisposition for developing brain fog. Individuals with brain fog are more likely to have abnormal cerebrospinal fluid measures.
Concluding remarks The COVID-19 pandemic has been described as a once-in-a-century challenge, with long COVID representing a challenge of similar scale. Although long COVID is not the first known IACC, it is the first time that such a condition has manifested in a substantially large number of people following a shared, known exposure. Emerging therapies, including antivirals like nirmatrelvir/ritonavir and immunomodulators targeting inflammatory pathways, are currently being explored in clinical trials as potential treatments for long COVID. As such, there is an urgent need for all types of research (basic, epidemiological, translational, and clinical and implementation sciences) into the natural history, biology, and treatment for long COVID.
Journal reference: Peluso MJ, Deeks SG. Mechanisms of long COVID and the path toward therapeutics. Cell, 2024, DOI: 10.1016/j.cell.2024.07.054, www.sciencedirect.com/science/article/pii/S0092867424008869
#long covid#covid conscious#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#still coviding#sars cov 2#wear a respirator#covid is airborne
5 notes
·
View notes
Text
Officials inside the CDC and global health specialists outside of the organization are trying to understand the ramifications of this order both for the U.S. and for the world.
"This is unprecedented," says Javier Guzman, the director of global health policy at the Center for Global Development.
CDC collaborates with WHO on a wide range of health efforts, including the ongoing efforts to quash a major mpox outbreak in parts of Africa and an outbreak of Marburg virus, which is Ebola's cousin, in Tanzania. The U.S. has donated more than a million vaccines to these efforts and sent expert teams to support the local response.
Asked to comment on the future of these collaborative efforts, a spokesperson for WHO wrote in an email to NPR, "we are analyzing developments and do not have further information at this time."
"There are a lot of people who are looking forward to further clarification and direction from the incoming administration," said a CDC official, who asked for anonymity because they are not authorized to speak to the press. They said they can't remember another presidential transition that included a directive similar to this. "I am not aware of any sort of communication that's gone out to CDC employees like this one."
A request for comment from CDC's media team was referred to the Health and Human Services media team, which has not responded.
How they've worked together
Among many other collaborations, the two agencies also work together on worldwide efforts to monitor and contain influenza. WHO runs the Global Influenza Surveillance Network. Josh Michaud, the associate director for global health policy at KFF, says that it may be challenging for the U.S. to develop flu vaccines each year tailored to the current strains of the virus that are circulating if scientists don't have access to the samples provided through the WHO system.
"There might be third parties which could create some communication channels and U.S. pharmaceutical companies on the private side could continue to have some kind of contact," he says. "But it definitely throws a wrench a little bit in the works of what had been a system which is really important – not just for global health security, but for U.S. health as well."
"It's absolutely vital that the CDC and WHO are talking to each other about what's happening. So a ban on that? I just can't see what benefit it has, but I see that it has a massive downside," say Dr. Chandy John, director of Indiana University School of Medicine's Ryan White Center for Infectious Diseases and Global Health.
Others agree. "It's very hard for me to see any U.S. national interest that's being advanced here. And quite the contrary, I just think it's making it very hazardous for Americans," says Lawrence Gostin, professor of global health law at Georgetown University and director of WHO's Center on Global Health Law.
For example, he says, WHO is convening an international meeting of experts who will discuss bird flu, among other things. Bird flu has been circulating widely in livestock and wildlife in the U.S. Without CDC representatives at the meeting, he says, CDC will be unable to examine the shared data from other countries where bird flu has been identified and understand how the virus is evolving and spreading across species. Gostin says this new clampdown on communications could hinder the country's ability to prevent humans from being infected as well as to develop medications and vaccines to combat bird flu.
"Not only is it reckless, but I think it's lawless," Gostin adds, explaining that even with the Trump administration's announcements, the U.S. is a party to the International Health Regulations and obliged to follow its guidelines. This is a legally-binding agreement managed by WHO that requires states to monitor health threats and report them to the WHO. However, there is not a strong enforcement mechanism for countries that don't comply.
"We criticize China relentlessly for failing to abide by [IHR] in rapid reporting and communicating of the Wuhan outbreak," says Gostin. "Why we would want to be in the company of China or Russia, that violates these international global health norms, certainly beats me."
In addition to withdrawing from WHO and halting communication between CDC and WHO, Trump has paused almost all foreign aid, including many health programs. Taken all together, KFF's Michaud calls the moment "incredibly precarious." And, he says, "for global health, it could mark a turning point" in how the U.S. contributes to the international effort to tackle diseases.
5 notes
·
View notes