#gender clinics
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr posted its first advertisements in May 2012 and subsequently earned $13M in revenue.
Text
If you are a trans person in the UK either under the care of a gender clinic, or even on the wait list for one, please do send them an email or letter opting out of your patient records and data being used for 'research', like the clearly transphobic review that's coming for adult services next.
This is especially important if you are under 30 years old.
There's a great template letter you can use here, it took me less than five minutes to copy stuff and send off an email.
875 notes
·
View notes
Text
J.K. Rowling has been proven right!
"The Cass Review is a damning indictment of what the NHS has been doing to children.
"Dr Hilary Cass has submitted her final report and recommendations to NHS England in her role as Chair of the Independent Review of gender identity services for children and young people.
"Hilary Cass’s report demolishes the entire basis for the current model of treating gender-distressed children. Its publication is a shameful day for NHS England, which for too long gave vulnerable children harmful treatments for which there was no evidence base. It’s now clear to all that this was quack medicine from the start.
"Dr Cass delivers stinging criticisms of NHS gender clinics, both adult and child, and her description of the Gender Identity Development Service is absolutely damning. It is disgraceful that GIDS, alongside the adult clinics, did not cooperate with her attempt to survey its practice, or to carry out a high-quality, long-term follow-up study on the treatment of children as part of the review, which would have been a global first."

You can read the entire review here. (pdf)

"Glinner" is Graham Linehan, a writer, screenwriter, and comedian who's been fighting against transitioning minors for years, losing friends, his job, and his agent along the way. But he's kept on fighting.

,
;

.

.

The tide has turned in the UK and in Europe. When will American media finally begin reporting on the closing of "gender clinics" and the bans on puberty blockers for children? I figure nothing will happen here in the U.S. until the lawsuits start flooding in. It's already begun. And with proof like the Cass Review and the WPATH files, it's going to be very, very difficult for clinics, doctors, and therapists to continue lying about how transitioning does no permanent and irreversible physical and psychological harm.
#Cass Review#transing kids#JK Rowling#I stand with JK Rowling#Graham Linehan#trans lies#WPATH#WPATH files#gender critical#gender clinics#health#medicine#the tide has turned#David Tennant
552 notes
·
View notes
Text
got a referral to the endocrinologist (hormone doc/gender clinic)!
havent gotten back to me, but ill update y'all when it happens!!!
#lgbtq#queer#lgbtq community#lgbtqplus#lgbt pride#lgbtqiia+#queer community#transgender#trans#trans rights#trans ftm#trans masc#ftm trans#transmasculine#trans man#ftm hrt#trans hrt#hrt#transitioning#trans joy#endocrinology#gender clinics
23 notes
·
View notes
Text
https://nationalpost.com/health/trangender-girls-social-contagion
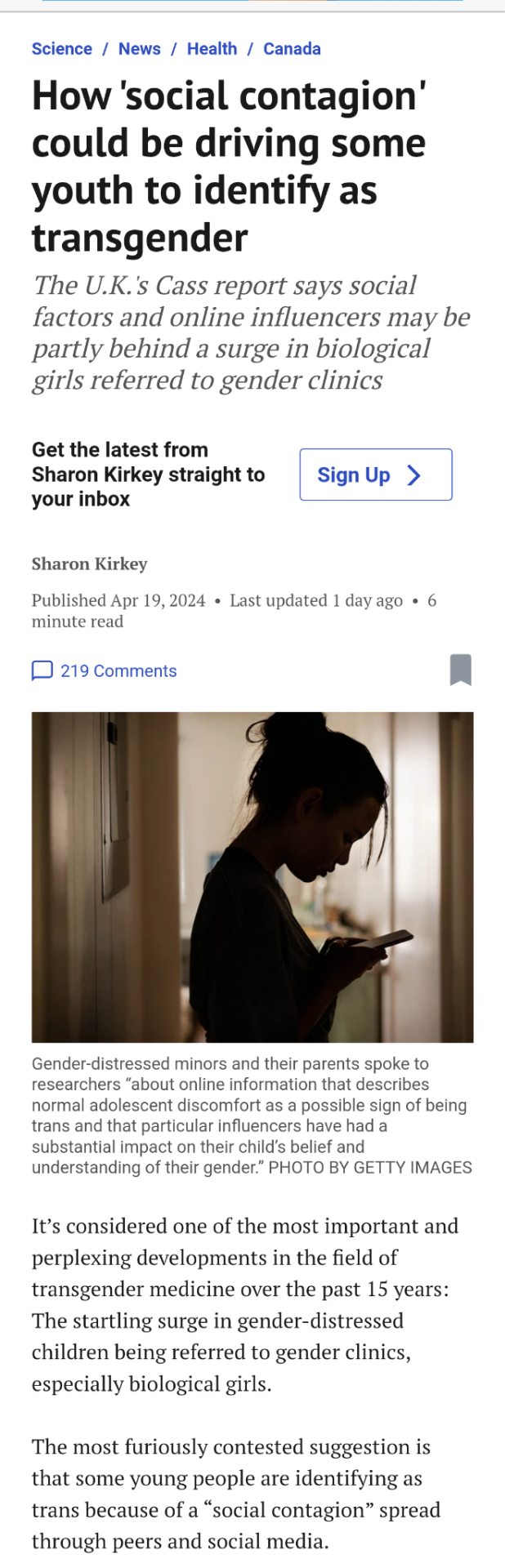
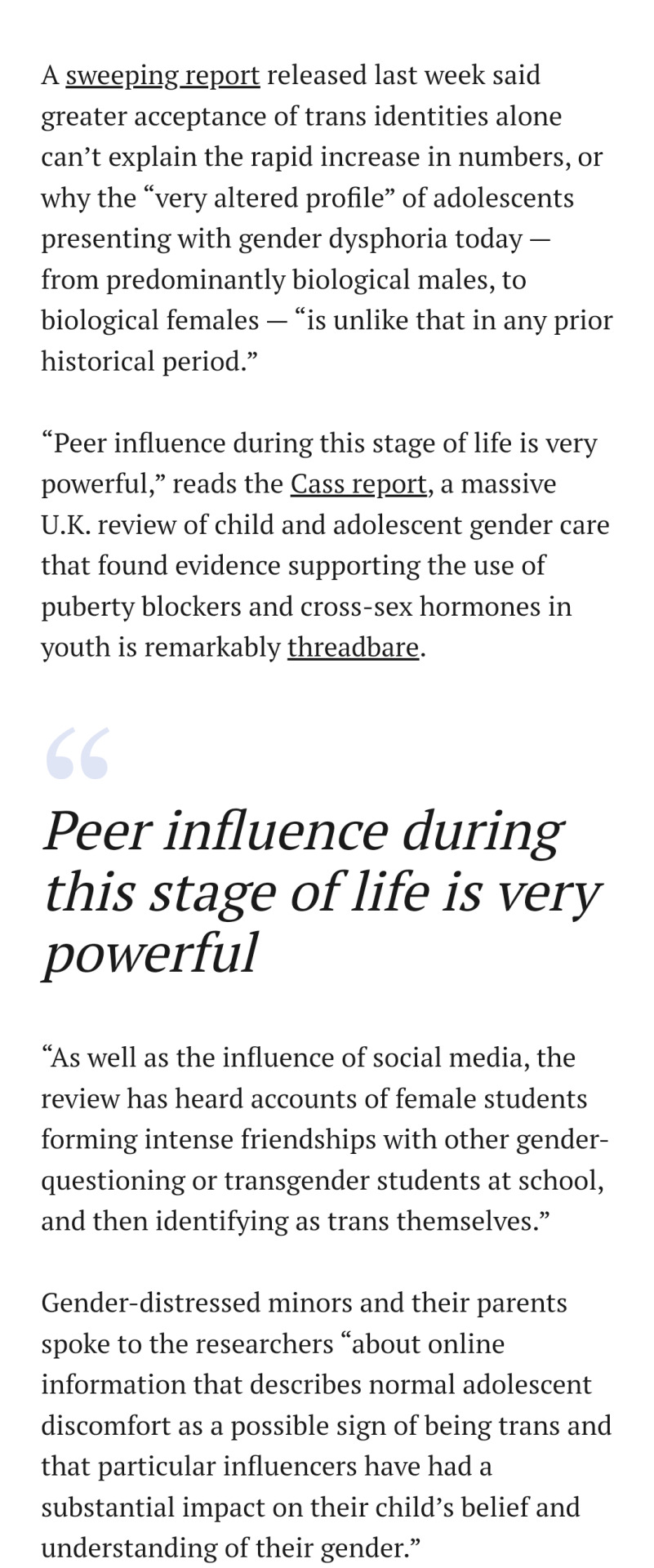
#gender critical#Rogd#rapid onset gender dysphoria#Gender distressed minors#Social contagion#Gender clinics#Social media#Gender research#mental health#Gender dysphoric girls#Surge of trans identities among teenage girls#Female adolescents
7 notes
·
View notes
Text
By: Bernard Lane
Published: Feb 8, 2024
At a December 2023 hearing of the Women and Equalities Committee of the UK House of Commons, Women and Equalities Minister Kemi Badenoch agreed to write to the committee with evidence “that children likely to grow up to be gay (same-sex attracted) might be subjected to conversion practices on the basis of gender identity rather than their sexual orientation.” What follows is the relevant section of her letter—GCN
Kemi Badenoch
Both prospective and retrospective studies have found a link between gender non-conformity in childhood and someone later coming out as gay.
A young person and their family may notice that they are gender non-conforming earlier than they are aware of their developing sexual orientation. If gender non-conformity is misinterpreted as evidence of being transgender and a child is medically affirmed, the child may not have had a chance to identify, come to terms with or explore a same-sex orientation.
The strong link between same-sex attraction and a transgender identity has been discussed in the relevant academic literature for many years. The Dutch founders of medical gender transition for adolescents wrote in 1999 that (the language is their own)—
“Not all children with GID (Gender Identity Disorder) turn out to be transsexuals after puberty… Prospective studies of GID boys show that this phenomenon is more strongly related to later homosexuality than to later transsexualism. These findings are in accordance with retrospective studies that have shown that male and female homosexuals recall more cross-gendered behaviour in childhood than male and female heterosexuals.”
In 2012, one of the same authors also found a clear pattern emerging—
“Follow-up studies have demonstrated that only a small proportion of gender dysphoric children become transsexual at a later age, that a much larger proportion have a homosexual sexual orientation without any gender dysphoria.”
The most recent reported data from GIDS [the Tavistock youth gender clinic] in England demonstrates that older [adolescent] patients expressing a sexual orientation were overwhelmingly not heterosexual. [And] 67.7 per cent of adolescent female patients were recorded as being attracted to other females only, 21.1 per cent were bisexual, and only 8.5 per cent were listed as heterosexual. Among adolescent male patients, 42.3 per cent were attracted only to other males, 38 per cent were bisexual, and only 19.2 per cent said they were attracted only to females.
As I mentioned at the committee hearing, I am aware of troubling accounts that some clinicians are hesitant to work in gender identity services. I take this extremely seriously. As detailed in the interim report of the Cass Review, primary and secondary care staff have stated that they feel under pressure to adopt an unquestioning affirmative approach, which is at odds with the standard process of clinical assessment and diagnosis that they have been trained to undertake.
Dr Natasha Prescott, a former GIDS clinician reported in her exit interview from the Tavistock that “there is increasing concern that gender-affirmative therapy, if applied unthinkingly, is reparative therapy against gay individuals, i.e. by making them straight” and Dr Matt Bristow, a former GIDS clinician, reported to [journalist] Hannah Barnes that he came to feel that GIDS was performing “conversion therapy for gay kids.”
In a survey of 100 detransitioners, the experience of homophobia or difficulty accepting themselves as lesbian, gay, or bisexual was expressed by 23 per cent of respondents as a reason for transition and subsequent detransition. As German gender clinicians have noted: “it must be understood that early hormone therapy may interfere with the patient’s development as a homosexual. This may not be in the interest of patients who, as a result of hormone therapy, can no longer have the decisive experiences that enable them to establish a homosexual identity.”
Video: “We are seeing almost an epidemic of young gay children being told that they are trans and being put on a medical pathway”—Kemi Badenoch, December 2023
youtube
“The evidence is clear. The vast majority of young people being put onto irreversible medical pathways are attracted to their own sex. This is modern gay conversion therapy.”—LGB Alliance, 8 February 2024
--
Documents and commentary
Ms Badenoch’s complete letter. The Daily Telegraph’s news report. Writer Ben Appel on the “new homophobia”. Philosopher Holly Lawford-Smith on “transing the gay away”. Endocrinologist Roy Eappen on gender-affirming care and gay kids. Author Allan Stratton on “automatic trans affirmation” and children confused about same-sex attraction. Psychiatrist Alexander Korte on puberty blockers and sexual identity development.
--
The Rt Hon Kemi Badenoch MP Minister for Women & Equalities Secretary of State for Business & Trade President of the Board of Trade
Data on gender identity services
The Committee asked about data on the significant rise in referrals of young people to gender identity clinics. NHS England report that in 2021/22 there were over 5,000 referrals into the Gender Identity Development Service (GIDS) run by the Tavistock and Portman NHS Foundation Trust. This compares to just under 250 referrals in 2011/12. The Cass Review reported there were approximately 50 referrals per annum in 2009 meaning that referrals have risen since then by 10,000%.1 The Cass Review also noted that in 2020 referrals stood at 2,500 per annum, meaning that the rise to 5,000 in the most recent year represents a doubling in a single year. As I said in my evidence session, this trend represents an explosion in numbers of referrals.
I committed to providing further details on the evidence that children likely to grow up to be gay (same sex attracted) might be subjected to conversion practices on the basis of gender identity rather than their sexual orientation. Both prospective and retrospective studies have found a link between gender non conformity in childhood and someone later coming out as gay.2 A young person and their family may notice that they are gender nonconforming earlier than they are aware of their developing sexual orientation. If gender non-conformity is misinterpreted as evidence of being transgender and a child is medically affirmed the child may not have had a chance to identify, come to terms with or explore a same-sex orientation.
The strong link between same sex attraction and a transgender identity has been discussed in the relevant academic literature for many years. The Dutch founders of medical gender transition for adolescents wrote in 1999 that (the language is their own):
“Not all children with GID (Gender Identity Disorder) turn out to be transsexuals after puberty… Prospective studies of GID boys show that this phenomenon is more strongly related to later homosexuality than to later transsexualism. These findings are in accordance with retrospective studies that have shown that male and female homosexuals recall more cross-gendered behaviour in childhood than male and female heterosexuals.”3
In 2012, one of the same authors also found a clear pattern emerging: “Follow-up studies have demonstrated that only a small proportion of gender dysphoric children become transsexual at a later age, that a much larger proportion have a homosexual sexual orientation without any gender dysphoria.”4
The most recent reported data from GIDS in England demonstrates that older patients expressing a sexual orientation were overwhelmingly not heterosexual. 67.7% of adolescent female patients were recorded as being attracted to other females only, 21.1% were bisexual, and only 8.5% were listed as heterosexual. Among adolescent male patients, 42.3% were attracted only to other males, 38% were bisexual, and only 19.2% said they were attracted only to females.5
As I mentioned at the Committee hearing, I am aware of troubling accounts that some clinicians are hesitant to work in gender identity services. I take this extremely seriously. As detailed in the interim report of the Cass Review, primary and secondary care staff have stated that they feel under pressure to adopt an unquestioning affirmative approach, which is at odds with the standard process of clinical assessment and diagnosis that they have been trained to undertake.
Dr Natasha Prescott, a former GIDS clinician reported in her exit interview from the Tavistock that ‘there is increasing concern that gender affirmative therapy, if applied unthinkingly, is reparative therapy against gay individuals, i.e. by making them straight’ and Dr Matt Bristow, a former GIDS clinician, reported to Hannah Barnes that he came to feel that GIDS was performing ‘conversion therapy for gay kids.’6 In a survey of 100 detransitioners, the experience of homophobia or difficulty accepting themselves as lesbian, gay, or bisexual was expressed by 23% of respondents as a reason for transition and subsequent detransition.7 As German gender clinicians have noted:
"it must be understood that early hormone therapy may interfere with the patient's development as a homosexual. This may not be in the interest of patients who, as a result of hormone therapy, can no longer have the decisive experiences that enable them to establish a homosexual identity." 8
During our evidence session you also asked me if there is a pattern being established specifically around girls with autism and transition. In its June 2023 statement, NHS England noted the rise in autistic young people seeking gender transition:
"Marked changes in the types of patients being referred which are not well understood. There has been a dramatic change in the case mix of referrals from predominantly birthregistered males to predominantly birth-registered females presenting with gender incongruence in early teen years. Additionally, a significant number of children are also presenting with neurodiversity and other mental health needs and risky behaviours which requires careful consideration and needs to be better understood.”
Many studies have reported that autistic people are over-represented in gender clinic populations, including a recent study noting "evidence of an increased rate of autism in adults and young people accessing gender clinics internationally, ranging from 5% to 26%".9 Authors have cautioned that this represents a challenge to the affirmative model:
The Journal of Autism and Developmental Disorders published a 2018 study which found ‘autistic traits appear to be more prevalent in transgender people assigned female at birth’.10
9.4% of adolescent Dutch gender patients were autistic. Autistic patients were reported to be on a range of gender-affirming pathways, including on puberty blockers, gender-affirming hormones, and having undergone sex reassignment surgery.11
The Journal of Autism and Developmental Disorders in 2012 published a study which found that nearly 30% of transgender men (natal females) were autistic compared with only 2% of non-transgender females.12
Child and Adolescent Psychiatry and Mental Health in 2015 published a study which found that 26 % of adolescent sex reassignment applicants were diagnosed to be on the autism spectrum which far exceeded the prevalence of 6/1000 for the general population. The authors concluded ‘autism spectrum needs to be taken seriously in considering treatment guidelines for child and adolescent gender dysphoria’.13
There is also significant evidence young people with gender dysphoria are more likely:
to have associated difficulties including non-suicidal self-harm, suicidal ideation, suicide attempts, attention deficit hyper- activity disorder (ADHD), symptoms of anxiety, psychosis, eating difficulties, bullying and to have experienced abuse (i.e. physical, psychological/emotional, sexual abuse and neglect). These findings were from a cross-sectional study of 218 children and adolescents with features of gender dysphoria referred to the GIDS in London during 2012. In 2014, the three most common associated difficulties in GIDS’ patients were: bullying, low mood or depression and self-harming – found in 47, 42 and 39% of the cases respectively.14
To be looked after. A study of 185 young people referred to GIDS over a 2-year period (1 April 2009 to 1 April 2011) found looked after young people represented 4.9% of referrals, which is significantly higher than within the English general population (0.58 %).’15
To have experienced difficult life events. A study of children presenting to a multidisciplinary gender service in Australia found a prevalence of adverse childhood experiences including family conflict (65.8%), parental mental illness (63.3%), loss of important figures via separation (59.5%). The study also identified high rates of comorbid mental health disorders: anxiety (63.3 %), depression (62.0%), behavioural disorders (35.4%), and autism (13.9%).16
Following the interim report, NHS England is setting up a new clinical model for children and young people experiencing gender incongruence and gender dysphoria. We are expecting the final Cass Review to be published shortly, which will include further recommendations in this area.
[ Full letter, including unrelated business and referenced sources: https://committees.parliament.uk/publications/43255/documents/215243/default/ ]
#Bernard Lane#Kemi Badenoch#gender ideology#queer theory#gender identity ideology#gay conversion therapy#gay conversion#conversion therapy#trans the gay away#homophobia#woke homophobia#homophobia 2.0#medical scandal#medical malpractice#medical corruption#anti gay#autism#gender clinics#religion is a mental illness#Youtube
4 notes
·
View notes
Text

No fucking words
4 notes
·
View notes
Text
For Trans and Non-Binary People, the Choice Is Between Private Healthcare or Years of Waiting
"More than 26,000 people are currently waiting for their first appointment at an NHS gender clinic. Those who go to that appointment this year will have waited on average four years; those referred now could wait decades. It takes two appointments, often years apart, to receive the gender dysphoria diagnosis that permits a trans patient to access gender-affirming healthcare ...
"Medical transition can be affirming, joyous or necessary; it is also, for many, about being able to move through the world more safely. Waiting for it not only has a deleterious effect on mental health, it can also force trans people to live with a higher risk of violence.
"Currently, trans people can either languish for years on an NHS waiting list, be rich, or hope that a crowdfunder will amass enough money to pay for private healthcare. Faced with this choice, the sad truth is that some trans and non-binary people who need to medically transition can’t pay the price."
3 notes
·
View notes
Text
Was having a nice evening playing Dungeon Bowl with my dad and a friend tonight, my dad only misgendered me a few times (every time except when we corrected him).
On the way home afterwards, talking about various things including my appointment at the gender clinic and how they kindly moved the time so I could get the affordable flight home, and I mention how we have to stick together when the government is trying to destroy trans healthcare. He said "Don't say that," and I agreed, amending my statement to "The government have dismantled trans healthcare"
He seemed to agree, which surprised me, but then he didn't. Somehow the government are destroying trans healthcare by accident...
I tried explaining the truth, but he loudly said "I don't want to talk about it". I tried again and he repeated himself even louder. So we didn't
Nice, dad, glad you understand what's going on and have my back...
#he's not exactly been accepting given he barely uses my pronouns and has only gotten worse at using them over the past two years#he's not openly antagonistic but he's not an ally#fits with his general attitude that the government are bad but he doesn't want to learn how or why#only wants to moan about them and then turn around and repeat conservative party talking points#my therapist must be bored of hearing about him at this point xD#transphobia#transphobia tw#tw transphobia#uk politics#gender clinics
1 note
·
View note
Text
so one of the things that's so horrifying about birth control is that you have to, like, navigate this incredibly personal choice about your body and yet also face the epitome of misogyny. like, someone in the comments will say it wasn't that bad for me, and you'll be utterly silenced. like, everyone treats birth control like something that's super dirty. like, you have no fucking information or control over this thing because certain powerful people find it icky.
first it was the oral contraceptives. you went on those young, mostly for reasons unrelated to birth control - even your dermatologist suggested them to control your acne. the list of side effects was longer than your arm, and you just stared at it, horrified.
it made you so mentally ill, but you just heard that this was adulthood. that, yes, there are of course side effects, what did you expect. one day you looked up yasmin makes me depressed because surely this was far too intense, and you discovered that over 12,000 lawsuits had been successfully filed against the brand. it remains commonly prescribed on the open market. you switched brands a few times before oral contraceptives stopped being in any way effective. your doctor just, like, shrugged and said you could try a different brand again.
and the thing is that you're a feminist. you know from your own experience that birth control can be lifesaving, and that even when used for birth control - it is necessary healthcare. you have seen it save so many people from such bad situations, yourself included. it is critical that any person has access to birth control, and you would never suggest that we just get rid of all of it.
you were a little skeeved out by the implant (heard too many bad stories about it) and figured - okay, iud. it was some of the worst pain you've ever fucking experienced, and you did it with a small number of tylenol in your system (3), like you were getting your bikini line waxed instead of something practically sewn into your body.
and what's wild is that because sometimes it isn't a painful insertion process, it is vanishingly rare to find a doctor that will actually numb the area. while your doctor was talking to you about which brand to choose, you were thinking about the other ways you've been injured in your life. you thought about how you had a suspicious mole frozen off - something so small and easy - and how they'd numbed a huge area. you thought about when you broke your wrist and didn't actually notice, because you'd thought it was a sprain.
your understanding of pain is that how the human body responds to injury doesn't always relate to the actual pain tolerance of the person - it's more about how lucky that person is physically. maybe they broke it in a perfect way. maybe they happened to get hurt in a place without a lot of nerve endings. some people can handle a broken femur but crumble under a sore tooth. there's no true way to predict how "much" something actually hurts.
in no other situation would it be appropriate for doctors to ignore pain. just because someone can break their wrist and not feel it doesn't mean no one should receive pain meds for a broken wrist. it just means that particular person was lucky about it. it should not define treatment.
in the comments of videos about IUDs, literally thousands of people report agony. blinding, nauseating, soul-crushing agony. they say things like i had 2 kids and this was the worst thing i ever experienced or i literally have a tattoo on my ribs and it felt like a tickle. this thing almost killed me or would rather run into traffic than ever feel that again.
so it's either true that every single person who reports severe pain is exaggerating. or it's true that it's far more likely you will experience pain, rather than "just a pinch." and yet - there's nothing fucking been done about it. it kind of feels like a shrug is layered on top of everything - since technically it's elective, isn't it kind of your fault for agreeing to select it? stop being fearmongering. stop being defensive.
you fucking needed yours. you are almost weirdly protective of it. yours was so important for your physical and mental health. it helped you off hormonal birth control and even started helping some of your symptoms. it still fucking hurt for no fucking reason.
once while recovering from surgery, they offered you like 15 days of vicodin. you only took 2 of them. you've been offered oxy for tonsillitis. you turned down opioids while recovering from your wisdom tooth extraction. everything else has the option. you fucking drove yourself home after it, shocked and quietly weeping, feeling like something very bad had just happened. the nurse that held your hand during the experience looked down at you, tears in her eyes, and said - i know. this is cruelty in action.
and it's fucked up because the conversation is never just "hey, so the way we are doing this is fucking barbaric and doctors should be required to offer serious pain meds" - it's usually something around the lines of "well, it didn't kill you, did it?"
you just found out that removing that little bitch will hurt just as bad. a little pinch like how oral contraceptives have "some" serious symptoms. like your life and pain are expendable or not really important. like maybe we are all hysterical about it?
hysteria comes from the latin word for uterus, which is great!
you stand here at a crossroads. like - this thing is so important. did they really have to make it so fucking dangerous. and why is it that if you make a complaint, you're told - i didn't even want you to have this in the first place. we're told be careful what you wish for. we're told that it's our fault for wanting something so illict; we could simply choose not to need medication. that maybe if we don't like the scraps, we should get ready to starve.
we have been saying for so long - "i'm not asking you to remove the option, i'm asking you to reconsider the risk." this entire time we hear: well, this is what you wanted, isn't it?
#where's the word woman in this u might wonder if u suck#good news i am nonbinary and have a uterus so that is something that can happen#im also gender fluid tho which means im immune to certain psychic damage bc if u call me a woman i'll be like <3 okay <3#writeblr#the tightrope of ''ppl need access to this''#and like also#''what the fuck is going on over there'' is like. so difficult as an activist#i was <3 punctured <3 during mine#and almost bled out on the table :) they didn't have anyone standing by bc it's ''just a little insertion''#so i started crashing and i vaguely remember apologizing for the fuss as i heard my heart rate monitor start going <3 tachycardic <3#she wasn't even a bad doctor tbh#ps btw the reason i even HAD a heart monitor is that i have a genuine heart condition and they knew GOING IN that there was a chance#i'd crash on the table#like my heart just likes to do fun little tricks and <3 stop working <3 (i do not want to discuss the specifics ty i am okay im ontop of it#and they were like 'oh u will be fine' and then she did do a puncture thru my uterus . pop!#and im sitting there dizzy and feeling my heartrate start to drop bc it feels almost. beautiful. like. the whole ground just#woosh! out from under you. and shit is like grey's anatomy. i'm looking up at her grey eyes#she's old she wears this nice shawl she's like got Cool Lesbian vibes and people are sprinting into the room#from other parts of the clinic unrelated to me. while the monitor is like a little aria singing#and shes like hey youre okay stay awake stay with me something went wrong we have to keep trying#and i remember thinking - i was trying to think of nice things. i have so many beautiful places that now overlap#with this terrible memory#i became dimly aware that there was too much on her wrists and hands. like#that was too many liters#and then when they had finished all this. i packed up and drove myself home#i have had (bad thing) happen to me. and the same feeling happened after#that numb almost lamblike bleating. you cry without noise. like. ur body is so shocked and ur mind so empty#you just stare at the road and everything everything is happening behind glass and static and you are standing so far away from it#while you hold ur hands at 10 and 2. and something in ur brain is SCREAMING at you - IT WAS BAD AND IT SHOULDNT HAVE HAPPENED#and ur just watching the alarms in your body going off and youre thinking. a little pinch! ha. i think i just lost something important.
10K notes
·
View notes
Text
Goddamn gender clinic called me just now to cancel an appointment I wasn't even aware I had today because they super DIDN'T send me a letter or email or anything about it. It was also just a telephone appointment I wouldn't have been able to have because I need videocall at the minimum, or text relay. Which has been the case for all my previous appointments so what the fuck??
Managed to rearrange for late March instead. Sigh.
98 notes
·
View notes
Text
Listen to the paediatritians.
#doctors#medicine#hormones#gender ideology#gender clinics#transition#detransition#detransitioners#lgbtq+#queer#gender reaffirming
1 note
·
View note
Note
What in the academic fuck is a GIC assesment
A GIC assessment (Gender Identity Clinic) assessment is the psychiatric interrogation you have to go through in Britain if you want permission to medically transition (and some aspects of legal transition too). Also called a Gender Dysphoria Assessment.
It involves answering a bunch of medically irrelevant, repetitive, deeply humiliating, repetitive questions like how you masturbate, what you wear when you masturbate, your sexual history, your childhood history, what toys you played with as a child, your employment, the clothes you like to wear, your relationship with your partners and family, etc. The classic is "Do you imagine yourself as a woman when you masturbate?" It also involves various psychiatric tests to check whether you're psychotic, which are deeply stigmatising. You will likely have to suffer this interrogation more than once if you want certain medical and legal doors to open. If you do not answer these questions "correctly" you may be refused transition.
If you want to get it for free, you'll need to wait several years, possibly decades depending on where you live, to be admitted to a Gender Identity Clinic.
If you want to go private, it will cost you about £500 a go, maybe more. (It's not technically a GIC Assessment unless it takes place at an NHS GIC; otherwise it's just sparkling humiliation.)
At the end of your interrogation you will - if you answered correctly - be diagnosed with "gender dysphoria." There is no way for them to check whether the answers you gave were truthful or whether you just told them what they want to hear. In Britain, about a third of trans people surveyed said they lied or withheld information during these assessments. There was no way for the 2015 American Psychiatric Association Working Group on gender dysphoria - the cis people who created the diagnosis* - to know that the interview data they based it on wasn't also full of people telling doctors what they wanted to hear! The unreliability of that data, some researchers have said, calls into serious question the use and sense of the diagnosis! * Fun fact: Ray Blanchard and Kenneth Zucker were both on that working group!
The NHS spends somewhere between 20 and 90 million pounds a year (depending on how you count it) on doing this.
Contrast that process to, say, the treatment pathway for menopause, where a cis woman who wants hormone replacement therapy can just get it from her family doctor 🙃
If you'd like to know more about this, I spoke about it here in more detail with citations
And wrote about it here
#philosophy tube#dysphoria#of course we can still have bad gender feels#of course we can still use the word 'dysphoria' to describe those feelings if we want#this is a point about the clinical label#and the diagnostic pathway#in my country specifically#which to be clear#I think ought to be abolished#So that we can control our own bodies without having to explain our desires and pains to a cis person first#reject pathologization
1K notes
·
View notes
Text
"he should have been at the club" he should have been at the gender clinic so he could start estrogen, actually
#has this been done yet#I DONR KNOW HOW GENDER CLINICS WORK IM IN CONSERVATIVE US HELL AND AM 16. PLEASE LAUGH AT MY JOKES
431 notes
·
View notes
Text
Considering wwx's canonical breeding kink and his general fondness for dubiously safe scientific experiments it is technically within the realm of possibility that a few years post-canon he just invents cultivation hrt and transition surgery by accident.
He just rocks up to a cultivation conference one day 5 months pregnant like "I turned my body into that of a woman! Yeah the boobs too we travel a lot and don't want a wetnurse. I'll reverse it in two years or so." And every single trans person and egg in the culivation world simultaneously sits up and goes "wait what?"
Imperical to understand that wwx still fully identifies as a cis man and does not know trans people exist. He did not know he was gay while actively being in gay love, this man is very smart but he doesn't know shit. Just a few weeks after the conference people start coming over like "hey... that thing you did... can you do that to me?" and he's like damn sure are a lot of dudes who wanna get pregnant. One day a "female" cultivator comes and is like "so you said you're going to reverse it... you think you can do that on a body that's already female? Turn my body into a man's body?" And he just goes well probably, let's find out!! It's so great all these people wanna help him perfect his techniques, isn't it lan zhan?
Years later they run into one of the trans women he first helped and doesn't even recognise her as she's thanking him and after the clarification just goes "wow! haha damn you're even wearing women's clothes! Should I start calling you guniang?" sort of as a joke but she's like yes please and he just says alright nice to see you again ma'am (still doesn't get it)
#is this mpreg?#i feel like by definition this counts as mpreg#wwx opening the first gender clinic completely by accident#mdzs#mdzs headcanons#wei wuxian#i think lwj does know trans people exist but he's an ally#it was a part of the whole 'working through all his queer feelings + questioning society for 13 years' thing#trans ally by accident (wwx) vs on purpose (lwj)
2K notes
·
View notes
Text
“That’s so gross, why don’t you shower or do basic hygiene when depressed? It’s not depression, it’s just laziness!”
This might sound crazy but people get so depressed they kill themselves, Helen! (≧▽≦)
#jiraiblogging#girl blogger#loserkei#vent post#tw sucidal ideation#losercore#bed rotting#sad boi hours#visual kei#landmine kei#tsukishima kei#ending it all#weebcore#webcore#i want drugs#danganronpa#fandom#personal#loser captions#im just a girl#this is a girlblog#boy blogger#gender ideology#hypersexuality#hyper sex drive#hypersexual#venting#did you just vent#was that the bite of 87#clinical depression
229 notes
·
View notes