#diazepam high
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr posted its first advertisements in May 2012 and subsequently earned $13M in revenue.
Text

Ϟ(๑⚈ ․̫ ⚈๑)⋆
la vie est moche
#take a pill or two#xanax pills#girls who do pills#diazepam#1mg#take it with me#tw drugs#love this shit#2014 grunge#i love drugs#aesthetic#love#get high#pills aesthetic#popping pills#happy pills#SoundCloud
8 notes
·
View notes
Text

Mein Leben gleicht einer ewigen schwierigen Phase.
#konsum#drogen#alkohol#sucht#borderline#high#Diazepam#tavor#promethazin#asthetic#gefühle#betäubt#kaputt#absturz
18 notes
·
View notes
Text

Valium knights in my bed....
5 notes
·
View notes
Text
Using Barbara's Pills
Warning(s): Slight yandere themes, past neglect, a lot of swearing, skipping school, using pills, major character's death, angst
(This route will have angst, so if you can't handle it, skip this)
~~~~~
You decided to use Bab's pills to get high with your friends
~~~~~
"I think we should give these pills a try."
You tell your friends.
"I guess we can. So, what are we going to do with them."
Sasha asks as she tilts her head to the side with her hand rested on her cheek.
"What do you mean 'what are we going to do with them'?"
Noelle asks Sasha.
"Like, are we going to snort them or just put them in random drinks for us to try."
She suggests all the things that they can do.
"Alright, whatever we do, I don't care, okay? Now, let's go."
You tell them before you got off the couch and leave the living room with them following behind you.
~~~~~
The three of you were in your bedroom, staring down at the light blue colored pills scattered around the makeshift table.
"So... how should we do this?"
You ask as you stare down at the pills.
"You don't know how to snort pills?"
Noelle asks as she stares at you.
"I do, but I don't know how to do it in a proper way, you know?"
You said as you stared at Noelle.
"Oh, it's actually pretty easy. Here, give me one of those pills."
Sasha said as you hand her one of the small blue pills.
"Okay, now do you have a lighter and a card?"
She asks as she looks right at you.
"What kind of card?"
You ask.
"Any. Anything but credit cards."
"I think I saw a Big Belly Burger gift card in Jason's room."
"How much?"
"About $20."
"Close enough. Okay, you get that."
~~~~~
Once you came back with the lighter and the gift card, Sasha assembled them by placing the lighter on top of the card.
"Now that you have these, you're going to put them on top of the pill and gently crush it."
She explains as she lightly presses down the card and lighter on the pill until it breaks off into a small pile of dust.
"It's really that simple?"
You ask as Sasha leans forward.
"Yeah, pretty much. Now, all you have to do is snort it up."
She said before she pressed one of her sides of her nose and took a firm sniff.
"Shit..."
She mumbles out as she leans back up.
"What? Is it good?"
You ask curiously.
"Damn, for something so small, it's actually pretty good."
She said as she let out a small sniffle.
"Wait, let me try."
You said before you crushed up a pill with the lighter and card. Then, you took a sniff of it.
"Fuck..."
You mumble out.
"It's good, right?"
"Yeah... not something too high, but it's still good."
"See? Told you."
That's when the two of you look over at Noelle.
"What?"
She asks.
"Are you going to take a drag of this?"
You ask as you place a pill in front of her.
"What? No! I'm not going to snort up some pills that you don't know! What if my nose bleeds?"
"Oh, come on. You did it with me twice, and nothing happened."
Sasha tells her.
"Yeah, and those times I passed out for like ten minutes."
"Ten minutes is nothing. Come on, just one drag. I'll hold your hand, if you want."
Sasha insists.
"You promise?"
"Yeah, yeah, no worries..."
She said as she held onto her friend's hand.
Noelle lets out a sigh before she crushes up that pill and leans forward before she snorts it up while pinching the side of her nose.
"Oh god!"
She exclaims as she quickly moves back as she covers her nose.
"Told you."
Sasha mutters out.
"No- I mean- Wait, I don't feel anything."
She said as she was freaking out for a moment before she was back to her usual self.
"See? I told you it wasn't that bad."
Sasha said as she released Noelle's hand.
"Yeah, I guess... What's this pill, anyway?"
"Hold on, let me look at the bottle."
You said as you picked up the pill bottle.
"Diazepam...?"
You mutter out.
"What's that?"
Noelle asks.
"It has like... a lot of shit."
Sasha said.
"Huh... so, it should say the side effects, right? What does it say?"
Noelle asks as she looks over at the bottle that you were holding.
"Uh... confusion, dizziness, blurred vision, and some hallucinations."
You start to list out all of the side effects.
"You had me snort up a dust of a pill that has hallucinations as its side effect?! Oh God, it's hitting!"
Noelle cries out as she starts to breathe heavily.
"Babs must take a lot of these. That was the last one, too."
You muttered out as you stare at the empty bottle.
"How much does she need for this?!"
"I dunno. I don't keep track of her medical history."
"Why the fuck didn't you tell me that this is valium?!"
Noelle asks as she starts to breathe heavier every second.
"That's why I didn't know what this is."
You reply nonchalantly.
"Oh, shit... I-I think I'm going to die, call 911!"
Noelle cries out as she holds onto her chest.
"The worst-case scenario is that you're just going to be passed out."
You tell her as she kept on having like a seizure.
~~~~~
The door to the Wayne Manor opens as Dick stumbles inside with his breathing heavy.
"Oh god... My head. I only need one pill and everything will be fine..."
He mumbles out as he climbs up the stairs.
~~~~~
Meanwhile, you and Sasha were staring down at Noelle who is passed out on the ground.
"Damn, she's out cold. Does she do this often?"
You ask as Noelle groans quietly while being on the ground.
"Nah, but now, I think she'll have hallucinations or something."
Sasha responds.
"What a theory..."
You mutter out.
That's when your bedroom door opens, and Dick shows up while sweat is pouring from his forehead.
"(name), why are you at home- why is my medicine all over the floor?!"
He asks as he breathes heavily as if he walked up a pack of long stairs.
"Oh, shit- Uh, hey, Dick, um... we were all feeling sick, so we took your pills- wait, these are yours?"
You made up an excuse until you realized that these weren't Barbara's as Dick stumbled into your room.
"I don't have time for this- where's my valium?!"
He asks as he walks up to you.
"Valium...?"
You mutter out.
"Uh... what do you need that for?"
Sasha asks as she watches Dick walk around.
"I feel like my head's going to explode! Why is the bottle empty?!"
He asks as he picks up the now empty pill bottle.
"Oh fuck... uh Noelle was having a migraine!"
You quickly lied.
Dick feels a loud sense of ringing through his brain as he grabs ahold of his hair tightly.
"Oh god... why is everything going dark? (name), call 911!"
He exclaims before he fell to the ground with a loud thud.
"Okay, Dick.... Dick?"
You call out nonchalantly before you notice that he wasn't moving a bit.
"Oh my god! Dick?! Fuck, where's the fucking phone?!"
You screamed out of shock and disbelief before you quickly took out your phone from your backpack to dial the emergencies.
~~~~~
It's been a week since Dick was declared to be dead.
Even though you were supposed to be happy after everything that he did to you, you couldn't help but feel... so blank.
You and Damian were back at school as you stand beside your friends in silence while they stare down at you with worried expressions.
"So... how was the funeral?"
Noelle asks in a quiet tone as she rubs her forearm while Sasha has her lips pursed and her eyebrows furrowed since she saw everything that happened.
"Went as expected."
You said in a blank tone as your gaze was on the ground.
"Context?"
Sasha mutters out.
"One of his friends pulled out a gun."
You said.
"Shit... that's probably less shocking than what I saw."
Sasha replies with a heavy sigh.
"Yeah... we were talking about what happened, and I was being interrogated for nearly six hours since I was the last person to be with him."
You tell them.
It was silent before Noelle speaks up.
"(name)... this might be a weird question, but uh..."
She speaks up as she pursed her lips before she continued to speak.
"Did you ever... cry at your brother's death?"
You just looked up at her with the same expressionless look.
"No, but I did to get sympathy from other people, so does that count?"
You reply in a nonchalant tone.
Noelle and Sasha stare at you for a moment.
"(name)... you need seriously help. Like, actually."
Noelle tells you.
"I am."
You simply reply.
"Other than SSRI and Sertraline."
Sasha adds that made her friend nod.
"I have valium, too, now."
You also add on.
"Do you really know how sad this actually is or are you actually fucking with us?"
Noelle asks as she placed her hand on her hip.
"I actually don't know..."
You mutter out in response.
"Look, again... what we're trying to say is that we feel bad for you, we really do, and-... it's really too much to handle."
Sasha explains to you with a lace of sympathy in her tone.
"Yeah, bullshit."
You said as your eyebrows furrowed.
"That's what we meant. Shouldn't you at least go to a therapist or talk to someone who you can open your feelings to?"
She adds on with her eyebrow raised.
"Is this the part where one of you goes on your knees and cries or tries to gain sympathy from to yourselves?"
You ask.
They were silent before Noelle speaks up.
"... We actually don't know."
~~~~~
Keep skipping (Coming Soon)
Go to a random class (Coming Soon)
•
•
•
Taglist: @somebodyrandom-613 @delias-stuff @endism @ragdol-666 @snowy-violet @sleepydhanie @missikkj @k1ttys-w0rld @box-of-kinderjoy @thetreefairypersonalblog @thelibraryofdeez @animegoddess15 @lilyalone @seraph101 @lain3iwakura @tacodeemon @whiterabbitxxx @yuyuzi-ling @lilithquillete @amisupposedtomakesenserightnow @una1002289 @spacetravelr @luckyangelballoon @illytian @ghostdoodlen @imaginarydreams @flyingpansaurus @wrenbirde @kimzzz18 @ohnoivefallen @ferakillia @f1lover4ever @asahi20789 @livingforloves @moonieper @rosecentury @waitingforanarchicaddiction @missmannequin @mischiefmanaged124 @hanselate @doli09 @chocolatemoose26 @enjisthings @stitchtheseconde @purple-lemon-8 @milliu @blublock404 @kimzzz18 @jsprien213 @bluemidnightmelodies @enter-sandmann @tdickensstuff4 @couldeatthatgirlforlunch @starsdotalk @sumikosasaki @erikasurfer @h0rr0r-10ver-69 @0lshadyl0 @ghostlotusnymph @yuyuzi-ling @lilithskywalker @trashlanternfish360 @i-never-saw-snow @couldeatthatgirlforlunch @76lonelyspoons
(If you want to be in the taglist, let me know!)
#yandere#yandere batfam#yandere batfamily#batfam#batfamily#yandere x reader#yandere platonic#neglected reader#platonic#yandere dc
276 notes
·
View notes
Note
Oh I see you also wanted to see Jason abusing benzos after Gotham War. Good taste etc.
Anyway, I've given some thought about how that could end up happening, and... Well, for starters, I think this:

Should have consequences!
Maybe Jason takes more time to push through the fear and rescue the girl, and she ends up in the hospital, or maybe she dies (I'm always advocating for them both to die here, but in this situation, I thinking - she inhales a lot of smoke, has to go to the hospital, stays there in critical condition).
Anyway, Jason wouldn't have started abusing benzos just because of himself, but if affects his vigilantism? If it put other people at risk? Yeah, then he's gonna do it.
Alternatively, maybe he even tries to step back from vigilantism, because his condition is putting more people in risk than he not being there at all, and then ends up in the emergency as a civilian and there he is given alprazolam/diazepam/some other benzodiazepine and it works (somewhat? I won't try to understand how comic book logic for body modifications would interact with real world drugs). So afterwards Jason is like... "Hmmmmm this could make me functional again 👍 interesting" and there you go, that's the beginning of his descent into benzos abuse :/
I was about to say "Jason needs to abuse benzos because with the vicious circle of adrenaline/panic attacks he will die" but then I realised this man has the survival instinct of a lemming so your theory is much better, I do think he would take them to be able to continue vigilantism.
I don't want the little girl to die, not because I don't think you're right, but because it makes me too sad. With that being said, I've been considering some things:
-Jason died (his first death) of smoke inhalation
-PTSD is associated with memory issues regarding the event (not an erasure of the moment so much as distorsions, issues with memories, details remembered wrong or incoherently...) Add to that the fear failsafe and the fact that on top of being a traumatic event, this scene could be triggering to him, and Jason does dissociate sometimes (which in extreme case can be linked to "memory" issues when you're not aware of what's happening, ie because you're trapped in a flashback).
-with the rest of the Gotham War storyline happening, Jason had no opportunity to follow-up and take her to the hospital
Put all of that together in the shaker, and you have the perfect cocktail for a Jason overwhelmed by doubt because he can't remember whether the little girl survived.
And then
AND THEN that's where it gets interesting, because the fun thing about benzos is aside from all the other shitty side-effects those drugs, esp in high quantities, can cause temporary memory loss (kinda like when you get black-out drunk). So I'm picturing a Jason addicted to benzos, horrified at the idea of ending up like his mother but not even chemically capable of feeling afraid of it, always wondering if he failed to save that little girl, and with chunks of missing time... I like to think he'd dissociate more often too, as a reaction to the anxiety on top of that, so there's the horror of having his memory full of holes, feeling like he's living a half-life, not being sure of anything...
And, well. When you find a traumatized young man with such dangerous skills, memory issues, attachment issues and such evident vulnerability... There's a lot of things you can do with a man like that. A lot of things you can make them believe, make them feel, make them think.
#jason todd#dc#red hood#dc comics#gotham war#batman 138#gotham war au#jason todd hc#jason todd headcanon#let that man abuse benzodiazepines for angst purposes please
85 notes
·
View notes
Text
I have a very strong headcanon that there's one (1) thing that Valentino is actually knowledgeable about and it's drugs. Man doesn't know basic math and probably hasn't read a single book in his life BUT he knows every thing that could get someone high.
If you want to knock the guy down you should use haloperidol mixed with some diazepam, he will be out for hours.
...you don't know what these words mean.
I beg you fucking pardon???
I'm pretty sure you've just made that up.
What, because you don't know them? Oh mother fucker you will learn them when I put it in your coffee, you WILL THEN PRAY THAT I KNOW WHAT I'M TALKING ABOUT!

364 notes
·
View notes
Text
Drug Orders and Doses

@whumpsmith
Cool, so I think the first thing to know is how medication is ordered.
Generally speaking, it will be ordered in 5 parts, known as the "5 Rights" of medication administration:
#1 What patient is getting the medication
#2 What medication is to be given
#3 How much medication is to be given
#4 What time it is to be given (or how often)
#5 What route it is to be given
So an order might be "Give John Smith (5/13/1995) lorazepam 0.5mg IV once prior to MRI"
In this example, John Smith is the patient and 5/13/1995 is his birthday to differentiate him from all the other John Smiths. "Lorazepam" is the drug's generic name, "0.5mg" is the amount of the drug. "IV" is the route, and "once prior to MRI" is the time.
Drugs have generic and brand names. For example, acetaminophen is a generic name. Many companies make acetaminophen, and each has their own brand name for the drug. Probably the most well-known brand name for acetaminophen is Tylenol, but there are others, like Calpol and Panadol. For most people, it doesn't matter which brand of a particular drug is used, just that the active ingredient (the generic name) is the same. For some people it matters because the non-active ingredients may be different between brands, and they may be allergic to a non-active ingredient that is in one brand, but not another.
In a hospital setting, we're going to use the generic name, because the brand of the drug that is cheapest to the hospital pharmacy varies contract to contract, and there are a lot of drug shortages these days. That's why if you're in the hospital you might get an oval green pill one day and a round white one the next day. They're the same drug, just different brands.
The dose is given in milligrams, usually abbreviated "mg". Milligrams are a measure of weight. Cubic centimeter (cc), on the other hand is a measure of volume. At some point we switched from volume based to weight based measures because we had a lot of different concentrations and using volumes for everything made mistakes really common. If you're using weights, it doesn't matter if the concentration you have is 1mg/mL or 10mg/mL for a given drug, you can do the math and come up with a volume that is right instead of just hoping you picked the one the doctor was thinking about when they wrote the order.
There are many routes a drug can take into the body. There is oral (a pill or liquid), IV (injection in a vein), IM (injection in a muscle), SQ (injection into fat), rectal/PR (a suppository, gel, or liquid inserted into the rectum), SL (under the tongue), TD (a paste or patch that sends medication through the skin) and many more.
Times can be once, once every x hours, once every x hours as needed (PRN), once under a particular circumstance, daily, or pretty much any other interval you can think of. "Stat" is a term meaning "right now".
Here's a list of common medications and their dosages:
CODE DRUGS:
Epinephrine 1mg IV for cardiac arrest every 3-5 minutes, 0.3mg for anaphylaxis
Amiodarone 150-300mg IV over 10 minutes for cardiac arrest
Lidocaine 75mg for cardiac arrest initially, if that doesn't work then 37.5 10 mins later
Adenosine 6mg given very quickly for PSVT, if that doesn't work, give 12mg
Atropine 1mg every 3-5 minutes for low heart rate until heart rate is normal
OTHER DRUGS:
Albuterol 2.5mg in nebulizer for brochospasm/asthma attack
Metoprolol 5mg IV every 5 minutes up to 15mg for severe high blood pressure
Furosemide 20-80mg IV for fluid on lungs
D50 25g IV for low blood sugar
Diphenhydramine 12.5-50mg IV for allergic reaction
Morphine 2-10mg IV or IM for pain
Fentanyl 50-200mcg for sedation
Mannitol 20-150g for increased pressure inside the skull
Nitroglycerin 0.3-0.6mg every 5 minutes up to 3 times for chest pain (angina)
Naloxone 8mg nasal spray every 2-3 minutes for opioid overdose
Flumazenil 0.2mg IV for benzodiazepine poisoning, if that doesn't work give 0.3mg, if that doesn't work, give 0.5
Diazepam 15mg rectal gel for seizures that don't stop
Phenobarbital 1-1.5g IV for seizures that don't stop
Etomidate 22mg IV for anesthesia (for things like intubating someone)
Midazolam 5mg IV for sedation prior to surgery
Olanzepine 5-10mg IV for agitation (emergency sedation)
Haloperidol 0.5-10mg oral or IM for agitation (emergency sedation)
#whump reference#writing reference#drugs#whump#medical orders#sedation#anaphylaxis#cardiac arrest#pain
126 notes
·
View notes
Text

♞Pairing: Steo ♞Characters: Stiles Stilinski, Theo Raeken ♞Tags: kidnapping, secret relationship ♞Words: 3319 ♞Prompt: inspired by "Rude" - Magic! (for @amatchinwater )
ao3
---
with heart in my hand
“Theo?” Stiles hovers his hand over his gun, heart hammering in his chest as the door falls closes with a soft click. Thanks to his job, he’s walked into too many homes that look like a crime scene — he just didn’t expect to walk into his own apartment looking the same. His clothes and other belongings are everywhere, bookshelves completely empty. There are drawers yanked out of dressers. His kitchen cupboards are opened. Someone even went through his pots and pans. The pillows on his couch have been sliced open. His mattress, Stiles realizes, has suffered the same fate as it leans against the railing of his loft, threatening to topple over. His TV is gone, but his laptop is still sitting on the desk on the corner of the room — the only place seemingly untouched.
Swallowing around the lump in his throat, Stiles pulls his gun out. “Theo?” He calls again, gaze darting from the closed bathroom door to the loft area. The mattress is blocking his view. Just today he was called to two break-ins, and as high as his adrenaline was during those times, his hands weren’t sweaty, and they certainly weren’t shaking. But this is different. This is his home, his life, and his boyfriend on the line. “Theo!” Even his voice is shaking, and Stiles wants to kick himself for it. Panicking doesn’t help, especially not when the intruders can tell he is.
Stiles carefully steps over a pair of shoes and a lonely boot, gaze darting back and forth between the mattress and the closed bathroom door. He’s not about to get jumped; not by hunters, supernatural assholes, or mundane criminals.
When he can finally see his bedroom area, it’s empty. The drawers have been ripped out of his nightstands. His lamps are on the ground, light bulbs most likely broken. Someone came into this place looking for something, and they were very determined to finding it.
But what?
Stiles doesn’t have anything valuable in his apartment. He’s not stupid enough to keep his supernatural artifact in a place where his colleagues from work are hanging out, sometimes with their nosy toddlers — and no one besides Theo know he’s rented a storage room for it. Unless someone figured it out? But how? And how did they learn where Stiles lives? He’s careful, and he went the extra mile to secure this place with magic.
Witches?
“Theo?” Stiles asks, his heart pumping fear through his body with every beat. Fuck his apartment. He can move. He can replace shit, but if someone dared to touch Theo— Stiles shakes his head. No. Absolutely not. Theo is going to be fine. Maybe he just stepped out to grab some food. He didn’t seem too thrilled about cooking earlier today.
Stepping over books and shoes and a bunch of apples, Stiles slowly makes his way towards his bathroom. The main reason he rented this place is that there are no spaces to hide besides the bathroom. He could shoot first and ask questions later, that is always an option, but if they’re not crouching behind the door like an idiot, all he does is alert everyone on his floor and waste bullets he may later need.
When he passes his desk, his gaze catches on things that are very clearly not his belongings. “What the fuck?” he breathes, his voice eerily loud in the heavy silence of the apartment. Handcuffs — not the fun kind — a gag, and an empty vial of… something. Stiles reaches for it, panic chocking him slowly. He brushes his thumb over the blue letters. Diazepam.
Great.
He’s been running out of nightmare fuel anyway.
The good news is, however, that it wouldn’t do anything to Theo. If someone did inject him with this shit, all they did was make him very angry. Bad news? An overdose will knock him on his ass very quickly.
Stiles drops the vial and aims the gun at his bathroom door again. He should shoot. Waltzing in there is an unnecessary risk. Stiles licks his lips, finger itching to pull the trigger. “Come out, come out wherever you are,” he mutters, more to himself than whoever is waiting to jump him behind that door.
Without warning, his apartment is plunged into darkness. Stiles whips around, aiming his gun to where he knows his light switch is. Before he’s even got the chance to shoot, someone crashes into him. The back of his head bounces off the hard wooden flooring. Stiles groans as pain explodes in his skull. The impact sends his gun flying, and by sheer fucking luck, there’s no shot going off.
A cool leather glove his covering his mouth as a needle sinks into his neck.
The pain barely registers, but the panic snaps him out of his haze. One minute. Stiles remembers everything he read on Diazepam during a case he worked two months ago. This shit is going to work in one to three minutes. Barely enough time to fight them off and get away. But Stiles isn’t going to give up.
He moves his left hand, inch by inch, feeling for anything he can use to hit their head — and luck is on his side. His little finger bumps into the fruit bowl. It’s made out of glass and sturdy enough to do some damage. He curls his fingers around it and slams it against their head with as much might as he can.
Stiles hears a pained groan mere heartbeats before the grip on him loosens. Gathering all his strength, he shoves the person off him and rolls onto his stomach. His world tips around him, even in the dark. A wave of nausea rolls over him as he struggles to his feet. The ground is unsteady underneath him, and Stiles stumbles, flailing his arms to fight for balance. His ears are ringing.
He’s not going to make it out of here.
No.
Stiles shakes his head. The movement makes him nearly throw up and lose his balance. All his attention is zeroed in on the sheen of light coming from the ajar front door. That’s his way out. If he manages to get there— but the first step makes him loose his balance again. His concussion makes it impossible to walk. Or maybe it’s the drug. How much time has passed?
Or maybe it’s both.
He just needs to—
--- --- ---
Consciousness creeps up on him, slow, sluggish, a snail on its way to an unknown goal. It’s hard to stay awake, even harder to figure out if he’s passed out again. The room is dark all the time. At least, he thinks it is. Maybe he hasn’t opened his eyes yet. What time is it? What day is it?
Stiles blinks his eyes open.
Soft rays of sunshine are painting the ceiling with peaceful strokes, yet something about them makes dread pool in Stiles’ stomach. Unease pushes into his veins, taking over every inch of his body and quenches the exhaustion. With every tick of a clock somewhere close by, Stiles becomes more and more awake – and more and more aware.
This isn’t his home.
Because someone kidnapped him.
His heart lurches in his chest as panic takes hold of him. It’s not just the presence of a window that’s wrong. The mattress is too soft, the blankets too thick. It’s too warm.
There is someone lying right next to him. Asleep, judging by the sound of their soft breathing. What the fuck is going on? Who- Stiles doesn’t have a stalker. Right? Theo would’ve surely noticed if someone were following him. He did last time.
And what happened to Theo?
Okay, one step at a time.
Stiles turns his head to the side. There’s an alarm clock on his side of the nightstand, bright red numbers informing him that it’s 7:23 am. Next to the alarm clock is a lamp. That’s going to be helpful. Stiles reaches for it, curling his fingers around the cool metal, and slowly inches closer and closer to the edge of the mattress. It’s best to just take the lamp with him. Maybe he can get out of here without waking the freak that kidnapped him in the first place. But- but who is it?
His fear is stifled by reason. If he leaves, and he doesn’t get a face of a name, what’s stopping them from doing it again? The address won’t be enough. They might be long gone when the police arrive, and Stiles isn’t planning on waiting around. The more he wakes up, the worse the pain gets in his head. That’s a concussion. Someone gave him a fucking concussion and then drugged him... only to do what? Play happy family?
Stiles grinds his teeth and turns around again. The person is mostly blanketed by the darkness of the room and facing away from him. Should he turn on the light? Sneak around the bed? Should he-
“I can feel you staring at me.”
Light floods the room, and Stiles covers his eyes with a groan. His grip tightens around the lamp. He yanks it off the nightstand. For a second, there’s resistance but the then cable gives and Stiles is willing to swing it at everything that moves.
A hand clasps around his arm before the lamp connects with anything, however. “I still have a headache from the fruit bowl.”
Stiles freezes. His whole world stops, zeroing in on the sound of the all too familiar voice despite his head screaming at him. “What the-” Stiles open his eyes, sucking in a deep breath as his gaze falls upon none other than Theo “-fuck?” he finishes, yanking his arm back. The lamp hovers above his head, knuckles turning white as he debates to hit his boyfriend over the head with it anyway. “What the fuck?” he repeats because saying it once doesn’t put nearly enough emphasis on how much he wants to whack him with this lamp.
“Okay.” Theo gets onto his knees, hands raised almost defensively. “Before you get mad-”
“Before I get mad? Theo, I am mad.” Stiles slams the lamp back onto the nightstand and crosses his arms. At this point, he’s ready to do worse than hit him with a goddamn lamp. Strangling him sounds like a wonderful alternative. “What the fuck were you thinking? Are you insane?”
Theo scoots closer to his side of the bed. “I thought you like that about me.” The guy actually has the nerve to look amused after scaring the living hell out of Stiles, give him a concussion and drug him. Neither his smile, not his body – beautifully on display and only wearing boxer briefs that leave nothing to the imagination – can get him out of this easily. He knew Theo’s ideas are usually a little different, but this is taking the cake.
Sucking in a breath, Stiles glares at him. “If this is your idea of a practical joke-” Because he is not in the mood, not with his head feeling as if someone’s using at as a fucking trampoline. He needs pain meds, or a doctor; actually, a visit to the ER sounds great after a fucking overdose and a concussion. That’s going to be fun to explain.
“In my defense, it was your dad’s idea.”
Stiles stares at him. That is a joke. Theo cannot be serious. “Dad told you to turn my apartment into a crime scene and kidnap me?” While his dad’s humor can be quite questionable at times, this does not at all sound like him. Never, in a million years, has any of this been his dad’s idea.
Theo runs his hand over the back of his neck. “Well...”
Closing his eyes, Stiles sinks back into the pillows. “You better have a very good explanation for this.” Although what could explain kidnapping him? Sure, they’ve role-played before, and it’s not like they’re kinks are necessarily something a lot of people are into — probably, it’s not like he knows. But using actual drugs? Giving him a concussion? That’s not like Theo.
“If you let me talk.” Theo flicks something against his chest.
Stiles squints down at his lap. Tylenol. Good.
Offering him a bottle of water, Theo watches him with his brows raised expectantly. “As I was saying—”
Snatching the bottle of water from him, Stiles shoots him a look. As he was saying, yeah, right.
“I wanted to make it official.” Theo visibly deflates, shoulders hunching slightly as his gaze drag from Stiles’ face to the Tylenol between his fingers. His face darkens, eyes narrowing slightly. For a few seconds, it seems that he’s far away, somewhere deep in the corners of a memory that refuses to let go of him. “I’m not going to hide us any longer.” Without warning, he gets off the bed and starts pacing the room, his shoulders a tense line.
Stiles cannot tell if it’s the concussion, or if Theo is just not making any sense. It’s true that not everyone knew about their relationship. His dad does, so do Kira and Lydia, but for the sake of keeping the piece within their packs, Stiles and Theo decided that it’s easier to pretend they’re merely getting along. They’re both good enough actors that nobody noticed anything or over a year. “So, you kidnapped me to…” he trails off, hoping Theo would fill in the gap.
“He threatened to kick me off his territory,” Theo snaps, eyes flashing yellow as he struggles to control his anger. There aren’t many people who could piss him off like that, and there is only one person who would have the ability to essentially exile Theo.
“And instead of talking to me about it…” Stiles shakes his head, instantly regretting the movement, and decides to take the Tylenol at last.
Theo lets out a long breath. “I was scared.”
Stiles snaps his head up, staring at Theo in bewilderment. Those three words aren’t something his boyfriend would throw around lightly. “Babe-”
But Theo doesn’t seem to hear him. He’s standing still, looking strangely lost as he continues talking, “I had it planned out. I talked to your dad. I talked to Lydia about the ring. I bought a ring.”
“A ring?” Stiles echoes before he can stop himself. They’ve been dating a year, why would Theo- his heart leaps into his throat. I wanted to make it official. Theo wasn’t just talking about telling everyone about their relationship. Stiles swallows and sits up straighter. “Theo, why didn’t you come talk to me?” he asks, patting the bed. They’re usually pretty good when it comes to communication, which honestly surprised Stiles more than anyone else. They work, perfectly, and it’s not even mad that Theo staged a very real kidnapping, it’s that he didn’t talk to him about it beforehand.
Which probably says more about him than he’d like to admit.
“I wanted it to be perfect!” Theo throws his hands in the air, frustration returning in full force. “I asked your dad for your hand first, of course.” Of course. Theo acts like it’s normal. Sure, there are still a lot of traditional people out there, and it is a sweet gesture, Stiles can’t deny that. He still didn’t expect it. Not from Theo. “Then I went to Scott. I tried to bury the hatched for you. Lydia helped me talk to him. We told him about our plans, but he said ‘no’.” Their eyes met, and Stiles can see the same fury burn that must have enveloped Theo when he decided to take what he considers his and make a run for it. “And that it’s time for me to leave his territory.” His hands are curled into tight fists, but his shoulders slump, and he bows his head, staring at the ground with a suddenly unreadable expression.
Stiles lets out a breath. His concussion doesn’t exactly make it easy to think. “Well,” he says slowly, drawing his brows together, “I’m glad to hear a kidnapping wasn’t in the original proposal plans.” He massages his temple, waiting for the Tylenol to set in quickly so he can focus on Theo alone instead of having to deal with this pounding headache on top of everything else. “Or giving me a concussion for that matter.”
“You broke a fruit bowl over my head.”
“Because you gave me a concussion!” Stiles raises his hands in defensive. They’re going to go in circles. Theo isn’t any less stubborn than he is. The only reason for Stiles’ winning most of the time is that Theo is insanely easily distracted by the prospect of sex. Not that Stiles is much better, but he does have the edge – at least for a little while. “Still… why didn’t you just talk to me?” The one thing Theo might love almost as much as Stiles is complaining about Scott’s incompetence. So, it doesn’t make any sense that he’d keep this to himself. None whatsoever.
Theo runs a hand over his face and pulls his shoulders up for the slowest shrug this side of the universe. “I panicked,” he says, having the nerve to sound mad about it.
“Because Scott told you to get lost?” Stiles squints at his boyfriend. It’s hard to tell if Theo doesn’t make any sense, or if his concussion makes his fail to see it. “He does that twice a week, and you laugh in his face. I don’t get-“
Theo shoots him a look, cutting Stiles off mid-sentence. It’s impossible who he’s angry at – himself for overreacting, Stiles for not getting it, or Scott for having the audacity to try and order him around. Not a single possibility makes a lick of sense. “He told me to leave you!” Theo snaps, crossing his arms over his chest defensively.
Stiles blinks, staring at his boyfriend in bewilderment. “You think I care?” If he weren’t so utterly baffled by Theo’s words, he’d point out that Scott and he haven’t been the same since long before Theo returned to Beacon Hills. It doesn’t matter to him what Scott thinks. He certainly wouldn’t be dating Theo if that were the case. Plus, as a human, no alpha can boss him around. “Last time I checked, I decide who I’m going to marry.”
For a few heartbeats, Theo doesn’t say anything. His wide blue eyes are fixed on him, almost contemplating. What’s going on in his head is anybody’s guess, but the smile tugging on the corner of his mouth is almost sheepish. Theo releases a breath and crosses the room. “I panicked,” he repeats. An explanation, not an apology. He might not apologize at all.
Stiles doesn’t expect one. Sighing, he lifts his blanket and shakes his head as Theo crawls on top of him. “You’re an idiot,” Stiles tells him. “Talk to me before you kidnap me next time.”
A chuckle ripple through Theo’s body. He wraps his arms around Stiles’ waist. “Fine,” he whispers, leaning his head against his chest. It's probably not the most comfortable position, but Stiles isn’t about to argue. “Next time I’ll make sure to get your consent before I kidnap you.”
“That’s not-“ Stiles lets out a breath. There’s not really any point in arguing. “You’re impossible.”
Theo laughs again, it’s soft and gentle, and a sound to fall in love with. “But you’re going to marry me anyway.”
Rolling his eyes, Stiles bends down to kiss the top of Theo’s head softly. “Yeah,” he breathes, almost a little surprised how sure he felt about his answer. They might not have dated for long, but he’s not doubting his decision at all. “But only if I get the proposal you planned with Lydia.”
Theo tightens his embrace for all but a second. “And a ring.”
“I love you.” Stiles runs his fingers through Theo’s hair.
“I love you too.”
#steo#stiles stilinski#theo raeken#teen wolf#stiles x theo#theo x stiles#*tv:teen wolf#*w:complete#*s:steo
35 notes
·
View notes
Text
cw: panic attacks
Steve hadn't been coping well. He hadn't been for a few years, really. But he thought he had got over all of that, gotten past the nightmares and the insomnia. Since his very first run in with the upside down, Steve knew there had been underlying issues he was ignoring. His hearing loss, eyesight issues, nerve pain that seems to come and go with the wind. And the worst, frequent but unpredictable major panic attacks. He had never gone to the doctors for any of it. At first it was more about being an arrogant boy rejecting the need for help. More recently it was a matter of money.
After pulling Munson's body out of the upside down, Steve had blacked out. Hit his head on the counter in the trailer and, according to Robin, had a seizure. He didn't remember that. What he did remember was waking up in the hospital and immediately panicking about the bill, about the fact his parents had taken him off the insurance.
The nurse tried to calm him down, put her hands on his shoulders. But his body was tense and he couldn't breathe, and every noise that passed through his head felt fuzzy and painful and he pushed her back, hard. She returned with a doctor not long later but long enough that Steve had started picking at his stitches trying to pull them out. "I can't afford it." He said, knowing in the back of his mind his actions weren't rational, yet still unable to stop.
It was this panic attack that kept him in the hospital longer. Not just to clean up the wounds he had made a mess of but to deal with what was obvious to the doctors, his anxiety disorder. Steve refused to speak to any counsellors or therapists, what could he say to them that they'd believe? Ultimately they ended up putting him on a high dosage of diazepam and sent him on his way, told him his parents had taken care of the bill.
"My parents?" He asked. And the receptionist nodded over to the waiting room where they sat, his father pouring over the sports section of a day old newspaper, his mother chatting to a stranger sat beside her.
It was uncomfortable, but Steve had been uncomfortable for years. "Thanks for paying." Steve said. "I wouldn't have been able to…"
"It isn't a problem." His mother interjected. "It's…you're our son. I regret how things -" She sighed, looked up to the ceiling, blinked. "We thought we lost you, Steven. After the earthquake we rushed to your place, that awful little apartment and it was completely…It was just rubble. And the firemen couldn't tell us if you were in there…"
His father gripped her shoulder, rubbed his thumb in circles over her cashmere cardigan.
"Son." He said. "You're coming home with us, okay? You can hate us. We can have our differing opinions. I care more to know you are safe."
If he could, Steve would have cried then. But he hadn't cried in front of his father since he was five years old. He wasn't sure he was capable of it.
"Thank you." He said. "I don't really have any stuff."
"Everything you left is still in your bedroom." His mother said. "They may not be your favourite but I'm sure you'll still fit into all of your old clothes."
Steve wasn't necessarily excited about the idea of moving back home, losing the freedom he had found in that little apartment of his. But he was tired, he had nowhere else to go - not if he didn't want to be a burden to the Buckley's or the Henderson's. And frankly, he could use some parental love, even if it was conditional, even if it wouldn't last. So he followed them through the parking lot into the car. Took the seat on the left in the back, the one he had always sat in as a child, where the leather is more worn down and the window doesn't wind down all the way. And he felt like a child again, tucked into the back of his parents' lives.
After surviving the upside down, Eddie is concerned to find out Steve has moved back in with his homophobic parents. alternate title: Eddie Munson is Not Okay (I Promise).
Read more on ao3.
#steddie#steve harrington#sad steve harrington#bisexual steve harrington#gay eddie munson#steve harrington whump
108 notes
·
View notes
Text
I'm remembering that time I had to take a relatively high amount of diazepam (to end a seizure) and later went to exercise, still under the effects. bro that shit feels like it's adding resistance to your every movement. like those weight bags for your ankles but everywhere. I mean ig it is a muscle relaxant and I was very much trying trying to do the opposite of what it was doing but man
#now I'm wondering if it just FEELS like resistance was added or if it actually takes more strength to move a muscle under diazepam#forbidden bodybuilding technique
2 notes
·
View notes
Text




Top notch LSD, MDMA, DMT, anxiety pills, crystals, coke and ritalin. #sex #kiss #pills #anxiety #smoke #high #lght #diazepam #xanax #vape #wisky #drinks
5 notes
·
View notes
Text
🇬🇧🇬🇧🇬🇧🇬🇧🇺🇸🇺🇸🇺🇸🇺🇸🏴🏴🏴🇪🇸🏴🇮🇪
PLEASE TIME WASTER AVOID MY DM, MESSAGE ME ONLY WHEN READY TO PLACE AN ORDER, IF NOT READY PLEASE DON'T MASSAGE ME, THANKS
PAYMENT METHODS
👇👇👇
✅📱BTC / ANY CRYPTOCURRENCY
✅ BANK TRANSFER
✅REVOLUT
🔠💯UK TOP VERIFIED ����🔠
🔠DM_ @Mrclonedeals
❄️COKE
1.75g...£140
3.5g...£240
7g....£395
14g...£780
28g...£1500
_
HEROINE
1g £50
3.5g £150
5g £200
10g £350
25g £650
50g £1200
100g £2100
__
🐴🐴🐴🐴🐴
KETAMINE Shards
🐴1G £25
🐴3.5G £50
🐴5G £65
🐴7G £80
🐴14G £150
🐴28G £260
__
🥳🥳🥳🥳🥳🥳🥳🥳🥳
🔥MDMA🔥
☄1G £30 ☄5G £65
☄3.5G £50 ☄7G £80
☄14G £150 ☄28G £260
————————————————————
🔠Order From_ @Mrclonedeals
💊Xanax bars 2mg💊
100 70£
200 100£
500 160£
1000 275£
————————————————————
💎💎Tina, Crystal, Meth, ICE💎💎
Beautiful clear shards that will put other vendors to shame.
Strong as fuck
💎0.5g £40
💎1.0g £70
💎2.0g £120
💎5.0g £275
💎10.0g £450
💎20.0g £840
💎50.0g £1500
————————————————————
GBL💧💧💧💧
50ml £45
100ml £85
————————————————————
💊Pregabs signature 300mg💊
1 box 65£
2 boxes 130£
5 boxes 250£
10 boxes 385£
————————————————————
💊OxyContin /oxycodone 80mg Beware these are very strong painkillers! 💊
10X £120
30X £300
60X £550
120X £1050
————————————————————
💊OxyContin /oxycodone 40mg Beware these are very strong painkillers! 💊
10X £80
30X £200
60X £350
120X £700
————————————————————
🍆🍆Viagra 100mg x 100 tablets
1-5 boxes £60 per box 📦
5-9 boxes: £45 per box 📦
10+ boxes+: £40 per box 📦
————————————————————
🍆🍆Viagra 200mg x 100 tablets
1-5 boxes £80 per box📦
5-9 boxes: £60 per box📦
10+: £45 per box 📦
————————————————————
💊Dihydrocodeine
10 boxes....£300
20 boxes...£670
————————————————————
💊Tramadol 225mg Ultra strong Tapentadol X Carisoprodol pharma grade pills. Be careful very very strong, handle with care. 10 pills in a strip, 100 pills in a box Trip pon trip💊
2 …..£15
4 ….. £25
1 Strip …… £40
2 Strip's …..£70
3 Strip's …. £90
5 Strip's ….. £110
1 Box ….£190
————————————————————
💊💊2my Clonazepam (Galenika brand) Strips of 10💊💊
1 strip £10
2 strips £18
100 tablets £85
500 tablets £350
————————————————————
💊Zopiclone 7.5mg 100 tablets 💊
1-5 box: £60 per box 📦
5-10 boxes: 40 per box 📦
————————————————————
💊Tramadol 100mg x 100 tablets💊
1-5 box: £70 per box 📦
5-9 boxes: £60 per box 📦
10+ boxes: £50 per box 📦
————————————————————
💊 Nitrazepam 10mg💊
10 boxes 180£
20 boxes 250£
————————————————————
💊Diaz roche 10mg💊
1 BOX ….£25k
5 BOXES ….£125
10 BOXES …..£200
20 BOXES …..£325
——————————————————
💊Bensedin Diazepam £20 a box (30)💊
1 Box….. £20
3 Boxes…. £55
5 Boxes …£95
10 boxes....£165
20 boxes....£300
————————————————————
💊Zopiclone Zopishine
Zopisign (10mgx140 ➪box)💊
1box …..£60
2box….. £100
5box ……£220
10box…… £380
50boxes….. £1250
————————————————————
💊Msjs 💊
blues/Yellows
Tub 165£/150£
2 tubs 310£/300£
______________________________________
UPDATED RATES ON PAYPAL FLIPS AND CLONECARDS
Paypal flip & Clone card
£200 for balance £1k
£300 for balance £2k
£500 for balance £3k
£650 for balance £5k
£800 for balance £6k
High Balance cards
£1k for balance £8k
£1.5k for balance £12k
£2k for balance £15k
£2.5k for balance £17k
£3k for balance £20k
£3.5k for balance £22k
£4k for balance £25k
£4.5k for balance £28k
£5k for balance £30k
Tap in @MrClonedeals
🔠Order From_ @Mrclonedeals
📦ORDER AND THANK ME LATER👇
PAYMENT METHOD
👇👇👇
🔠BTC / BITCOIN
🔠 BANK TRANSFER
🔠REVOLUT
✈️POSTAGE / NDD
🎆1st class 9£
Next day delivery 10£💯
🔠Order From_ @Mrclonedeals
2 notes
·
View notes
Text
Pill Poppers
Every night before bed I shake out 10 pills from orange bottles And I take them one by one with a can of soda choking on them, a new thing Because back when pills were candy I could swallow anything without anything liquid And now I choke on my zolpiem Chewing my quetiapine and gagging on the bitter ness swallowing the lithium whole High does for a unwell head
It took a lifetime to get help but I can't say I was ever really looking Until I realized I believed the lies I told and would defend there authenticity Nobody wants to be around a professional liar Not even the liar himself a victim of self a victim of me I'm telling you that sorry just doesn't cut it
It takes awhile before my cocktail kicks in the sedatives slwoing everything down Sometimes I try to fight it and fall in hypnosis with the breathing walls Like taking mushroom on a full stomach I know it's bad for me, I think my brain is not my friend because it's constantly looking for ways to break me to lose me to hurt me to kill me
Every three months I get a blood test the skill lacking in the hospital in town If thay'd let me do it, we'd be done in seconds because I'd had a lot of practice with a needle We have to find ways to avert my addiction I don't want to relapse because of diazepam And so I turn them down and up the Seroquwl Because the 800 milligrams is facing a tolerance
Wouldn't it be ironic if I choked on a pill and died?
#writers and poets#poems on tumblr#original poem#poem#poetry#spilled thoughts#spilled feelings#spilled writing#writing#my writing#spilled poetry#spilled emotions#spilled words#writers on tumblr#poets and writers#creative writing#writerscommunity#writer#Pill Poppers#Mental Health#Bipolar#schizoaffective
4 notes
·
View notes
Text
Me, Myself and Progesterone
I touched on progesterone (P4) in my last transgender update post. I am not quite sure if progesterone is working in the way I want it to. My biggest annoyance with it is feeling like my brain is on fire just before trying to sleep.
Rewind to late February 2024, for almost three weeks my progesterone dose was doubled to 400 mg of oral, micronised, compounded progesterone – 200 mg twice a day. That’s up from the 200 mg once at night.
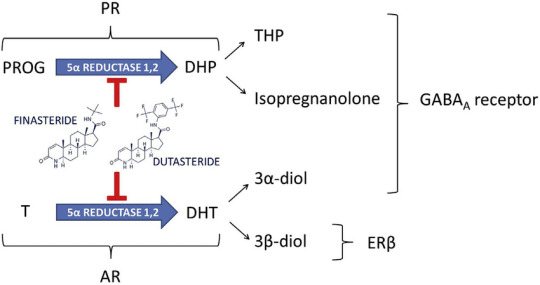
I had also ceased finasteride. And finasteride interferes with the progesterone (oral) pathway conversion to neurosteroids such as allopregnanolone. This is because finasteride blocks *most* of the activity (~70%) of the 5-alpha reductase (5AR) enzyme. In turn, reducing levels of allopregnanolone – or at least slowing their conversion to neurosteroids.

My sleep quality has been pretty broken for a while now. Look at those orange blocks. And here I was looking forward to some of the benefits from progesterone. Anxiolytic? Yes please! Sleep improving? Definitely!

Instead I get this whole brain fire thing and feel like I’ve taken an anxiogenic. That got me thinking, brain on fire? Throw in some formication and it’s what feels like a glutamate rebound or surge. Excitotoxicity perhaps?
I’ve experienced similar feelings while withdrawing from pregabalin (decreases glutamate levels) and trusty old diazepam (increases GABA levels). Definitely that same feeling though. It appears that taking what I would consider a small dose (2 mg) of diazepam negates the insomnia pretty well. Even though diazepam isn’t a terribly good choice for sleep. It takes me from being a wired insomniac to sleeping beauty in about an hour.
Another interesting side effect I am seeing a lot more of is dissociation. Ordinarily, I would only experience this while in high stress, high anxiety situations but recently I’m noting it a lot more just doing chores around the house – which is a little concerning.
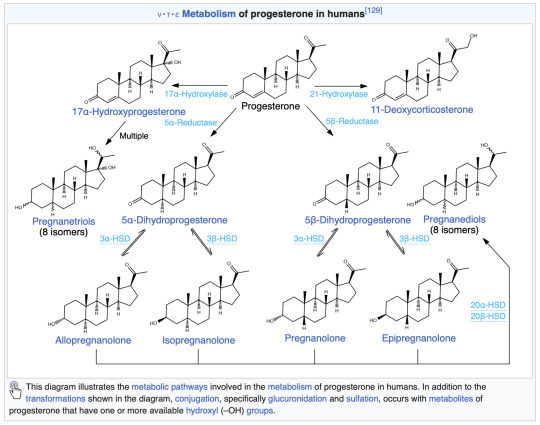
Regardless, it seems that something is messing with my GABAergic system and metabolites of progesterone fit the bill. Armed with my two-thirds of a biomedical science degree I went digging for more information on the metabolites. Up above is an image from my last health blog post. Note the action of finasteride on progesterone – blocking allopregnanolone (THP) and isopregnanolone.
I wonder if moving to a more potent 5AR blocker, such as dutasteride, would reduce the side effects of a higher dose of progesterone? A question for my endocrinologist I suppose. I restarted my finasteride to at least partially block some of the following progesterone metabolites. Let’s look at the metabolites a little closer and how they act.
Allopregnanolone (Tetrahydroprogesterone or THP) Positive allosteric modulator 9 hours
Pregnanolone Positive allosteric modulator 1 – 3.5 hours
Isopregnanolone Negative allosteric modulator 14 hours Targets allopregnanolone only
Epipregnanolone Negative allosteric modulator Half-life unknown
Alright, so a bunch of neurosteroids are doing a bunch of things. A few are being blocked, but also produce negative side effects when they weren’t blocked. Hormones are messy. Where does that leave me? I guess I am left questioning whether I should be taking progesterone at all. At minimum a dose reduction is definitely called for. I will probably return back to 200 mg and see what symptoms, if any, follow.
My search revealed some interesting data with overlap in symptoms shared with premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) in cisgender women.
PMDD is believed to be caused by fluctuations in gonadal sex hormones or variations in sensitivity to sex hormones.
If sensitivity to level shifts is reason for the negative side effects, then single or even twice daily doses are probably not enough to smooth out the levels of neurosteroids for me, allowing me enter a withdrawal state, perhaps? Brain on fire? This paper offers some great insight into the mechanisms behind it all with some interesting side notes on SSRIs.
Interestingly, SSRIs increase allopregnanolone levels in the brain, rapidly and at low doses, as demonstrated in rodents as well as in patients with depression.
Could this be one of the reasons why I can’t tolerate SSRI/SNRIs? At the very least, it’s some food for thought. Worth noting that the original study has been questioned a little further along in the paper. Let’s circle back to those progesterone levels again. From Wikipedia
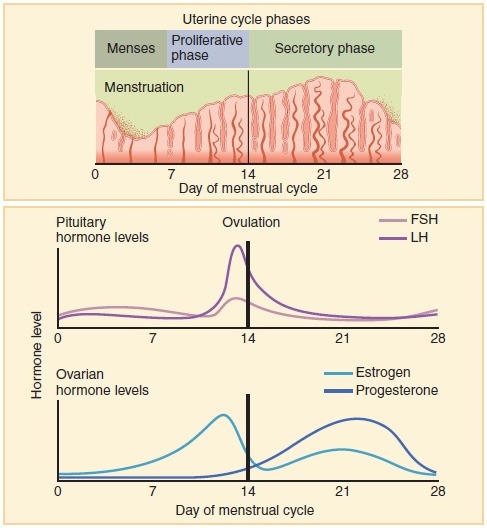
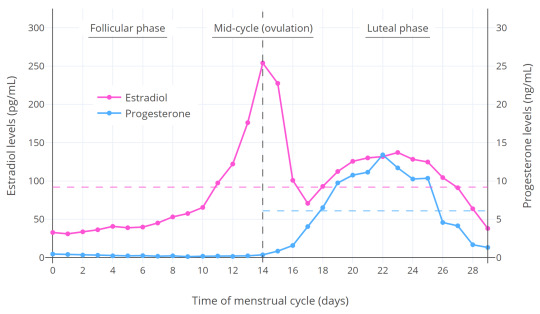
Progesterone levels tend to be less than 2 ng/mL prior to ovulation and greater than 5 ng/mL after ovulation.
What were my most recent levels again? 9.1 nmol/L or should I say 2.6 ng/mL (freedom units). That’s at 200 mg once daily at night, measured in the trough. I really need to ask myself, do I want to have symptoms of PMS/PMDD? Is that even a question that needs to be asked?
Looking at the levels on Table 1 in this paper give an idea where my levels line up. If you factor in the short half-life of most of the metabolites, once daily dosing is probably a bad idea. Ideally, I should look into getting the dose split to 100 mg twice daily.
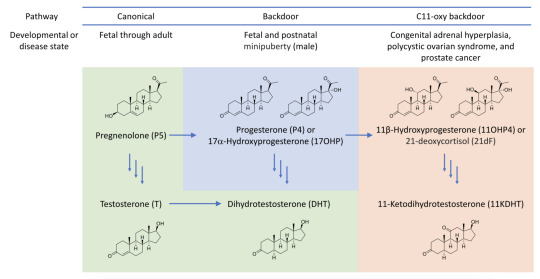
Of course I have to be mindful of negative risk such as the androgen backdoor pathway. This has the potential to generate unwanted androgens like DHT – which will affect the hair on my head. That’s why the finasteride is here to stay until most means of testosterone generation is removed from my system…
It’s not all bad though. Finasteride competes with progesterone for the 5AR enzyme – which results in even less 5AR being available for testosterone -> DHT conversion. Another point worth considering is that progesterone has a positive effect on bone-building cells (osteoblasts). This can help with avoiding or reducing effects of osteoporosis.
Touching on side effects I’ve noticed, Progesterone should increase libido. Which is something I do not want due to past trauma. However, I wonder if the finasteride side effects are at play here. Again, I don’t consider them negative side effects either.
Other oddities I’ve also noticed my facial hair has become darker at the higher progesterone dosing at 400 mg. My upper lip now has dark black hairs, that’s new and unwanted. It might be useful for IPL treatment. But now there’s shadow on my upper lip I never had before. It isn’t just the thinning of skin either. The hairs are black instead of blonde.
One big uncertainty is that I’m not sure what my levels of estradiol will be at the next blood test. Are the 200 mg of pellets doing their job properly? Or did they fail? Does the dose need to be increased?
For now, I’ve been supplementing the implant with the remainder of my 2 mg estradiol pills while the pellets stabilise. One pill gives me ~85 pmol/L in estradiol levels. I’ve only just ran out of those so now I’m adding in some of the estradiol gel (Sandrena branded). These gave ~200 pmol/L estradiol per dose according to my most recent blood tests. In theory with one a day, I should be guaranteed to be in the late follicular phase – regardless of the implant levels.
Anyway, that was one heck of an info dump. I think that sums everything up that has been on my mind lately.
TL;DR 400 mg oral progesterone makes my brain go on fire. Progesterone metabolite levels shifting around are very activating for me. I will now target cisgender progesterone levels in the late follicular phase. Hormones are complicated. One size fits most seems to be at play when it comes to progesterone. Nothing like some trial and error! 🙃
#transgender#transfem#trans#lgbtq#queer#progesterone#estrogen#GAHT#HRT#allopregnanolone#pregabalin#diazepam#GABA#finasteride#PMS#PMDD#GABAergic#brain on fire#fire brain#brainly fires#firely braining
2 notes
·
View notes
Text
I'm reading about how to withdraw from benzos. So basically, you can decrease by 5% q1-2 weeks. This chart is helpful for seeing how strong the benzodiazepines are: https://deprescribe.web.unc.edu/wp-content/uploads/sites/20194/2020/04/Benzo-Equivalency-Table_UNC.pdf
My pt takes clonazepam 1 mg tid. 0.5 mg clonazepam is equivalent to 10 mg of diazepam. So my pt takes the equivalent of 60 mg diazepam a day. This is from the benzo.org.uk website:
Be confident - you can do it. If in doubt, try a very small reduction in dosage for a few days (for example, try reducing your daily dosage by about one tenth or one eighth; you may be able to achieve this by halving or quartering one of your tablets). You will probably find that you notice no difference. If still in doubt, aim at first for dosage reduction rather than complete withdrawal. You will probably wish to continue once you have started.
Be patient. There is no need to hurry withdrawal. Your body (and brain) may need time to readjust after years of being on benzodiazepines. Many people have taken a year or more to complete the withdrawal. So don't rush, and, above all, do not try to stop suddenly.
Choose your own way - don't expect a "quick fix". It may be possible to enter a hospital or special centre for "detoxification". Such an approach usually involves a fairly rapid withdrawal, is medically "safe" and may provide psychological support. Such centres may be suitable for a small minority of people with difficult psychological problems. However, they often remove the control of withdrawal from the patient and setbacks on returning home are common, largely because there has been no time to build up alternative living skills. Slow withdrawal in your own environment allows time for physical and psychological adjustments, permits you to continue with your normal life, to tailor your withdrawal to your own lifestyle, and to build up alternative strategies for living without benzodiazepines.
THE WITHDRAWAL
(1) Dosage tapering. There is absolutely no doubt that anyone withdrawing from long-term benzodiazepines must reduce the dosage slowly. Abrupt or over-rapid withdrawal, especially from high dosage, can give rise to severe symptoms (convulsions, psychotic reactions, acute anxiety states) and may increase the risk of protracted withdrawal symptoms (see Chapter III). Slow withdrawal means tapering dosage gradually, usually over a period of some months. The aim is to obtain a smooth, steady and slow decline in blood and tissue concentrations of benzodiazepines so that the natural systems in the brain can recover their normal state. As explained in Chapter I, long-term benzodiazepines take over many of the functions of the body's natural tranquilliser system, mediated by the neurotransmitter GABA. As a result, GABA receptors in the brain reduce in numbers and GABA function decreases. Sudden withdrawal from benzodiazepines leaves the brain in a state of GABA-underactivity, resulting in hyperexcitability of the nervous system. This hyperexcitability is the root cause of most of the withdrawal symptoms discussed in the next chapter. However, a sufficiently slow, and smooth, departure of benzodiazepines from the body permits the natural systems to regain control of the functions which have been damped down by their presence. There is scientific evidence that reinstatement of brain function takes a long time. Recovery after long-term benzodiazepine use is not unlike the gradual recuperation of the body after a major surgical operation. Healing, of body or mind, is a slow process.
The precise rate of withdrawal is an individual matter. It depends on many factors including the dose and type of benzodiazepine used, duration of use, personality, lifestyle, previous experience, specific vulnerabilities, and the (perhaps genetically determined) speed of your recovery systems. Usually the best judge is you, yourself; you must be in control and must proceed at the pace that is comfortable for you. You may need to resist attempts from outsiders (clinics, doctors) to persuade you into a rapid withdrawal. The classic six weeks withdrawal period adopted by many clinics and doctors is much too fast for many long-term users. Actually, the rate of withdrawal, as long as it is slow enough, is not critical. Whether it takes 6 months, 12 months or 18 months is of little significance if you have taken benzodiazepines for a matter of years.
It is sometimes claimed that very slow withdrawal from benzodiazepines "merely prolongs the agony" and it is better to get it over with as quickly as possible. However, the experience of most patients is that slow withdrawal is greatly preferable, especially when the subject dictates the pace. Indeed, many patients find that there is little or no "agony" involved. Nevertheless there is no magic rate of withdrawal and each person must find the pace that suits him best. People who have been on low doses of benzodiazepine for a relatively short time (less than a year) can usually withdraw fairly rapidly. Those who have been on high doses of potent benzodiazepines such as Xanax and Klonopin are likely to need more time.
Examples of slow withdrawal schedules are given at the end of this chapter. As a very rough guide, a person taking 40mg diazepam a day (or its equivalent) might be able to reduce the daily dosage by 2mg every 1-2 weeks until a dose of 20mg diazepam a day is reached. This would take 10-20 weeks. From 20mg diazepam a day, reductions of 1 mg in daily dosage every week or two might be preferable. This would take a further 20-40 weeks, so the total withdrawal might last 30-60 weeks. Yet some people might prefer to reduce faster and some might go even slower. (See next section for further details).
However, it is important in withdrawal always to go forwards. If you reach a difficult point, you can stop there for a few weeks if necessary, but you should try to avoid going backwards and increasing your dosage again. Some doctors advocate the use of "escape pills" (an extra dose of benzodiazepines) in particularly stressful situations. This is probably not a good idea as it interrupts the smooth decline in benzodiazepine concentrations and also disrupts the process of learning to cope without drugs which is an essential part of the adaptation to withdrawal. If the withdrawal is slow enough, "escape pills" should not be necessary.
(2) Switching to a long-acting benzodiazepine. With relatively short-acting benzodiazepines such as alprazolam (Xanax) and lorazepam (Ativan) (Table 1, Chapter I), it is not possible to achieve a smooth decline in blood and tissue concentrations. These drugs are eliminated fairly rapidly with the result that concentrations fluctuate with peaks and troughs between each dose. It is necessary to take the tablets several times a day and many people experience a "mini-withdrawal", sometimes a craving, between each dose.
For people withdrawing from these potent, short-acting drugs it is advisable to switch to a long-acting, slowly metabolised benzodiazepine such as diazepam. Diazepam (Valium) is one of the most slowly eliminated benzodiazepines. It has a half-life of up to 200 hours, which means that the blood level for each dose falls by only half in about 8.3 days. The only other benzodiazepines with similar half-lives are chlordiazepoxide (Librium), flunitrazepam (Rohypnol) and flurazepam (Dalmane), all of which are converted to a diazepam metabolite in the body. The slow elimination of diazepam allows a smooth, gradual fall in blood level, allowing the body to adjust slowly to a decreasing concentration of the benzodiazepines. The switch-over process needs to be carried out gradually, usually in stepwise fashion, substituting one dose at a time. There are several factors to consider. One is the difference in potency between different benzodiazepines. Many people have suffered because they have been switched suddenly to a different, less potent drug in inadequate dosage because the doctor has not adequately considered this factor. Equivalent potencies of benzodiazepines are shown in Table 1 (Chapter I), but these are only approximate and differ between individuals.
A second factor to bear in mind is that the various benzodiazepines, though broadly similar, have slightly different profiles of action. For example, lorazepam (Ativan) seems to have less hypnotic activity than diazepam (probably because it is shorter acting). Thus if someone on, say, 2mg Ativan three times a day is directly switched to 60mg diazepam (the equivalent dose for anxiety) he is liable to become extremely sleepy, but if he is switched suddenly onto a much smaller dose of diazepam, he will probably get withdrawal symptoms. Making the changeover one dose (or part of dose) at a time avoids this difficulty and also helps to find the equivalent dosage for that individual. It is also helpful to make the first substitution in the night-time dose, and the substitution may not always need to be complete. For example, if the evening dose was 2mg Ativan, this could in some cases be changed to 1 mg Ativan plus 8mg diazepam. A full substitution for the dropped 1 mg of Ativan would have been 10mg diazepam. However, the patient may actually sleep well on this combination and he will have already made a dosage reduction - a first step in withdrawal. (Examples of step-wise substitutions are given in the schedules at the end of this chapter.)
A third important practical factor is the available dosage formulations of the various benzodiazepines. In withdrawal you need a long-acting drug which can be reduced in very small steps. Diazepam (Valium) is the only benzodiazepine that is ideal for this purpose since it comes in 2mg tablets, which are scored down the middle and easily halved into 1 mg doses. By contrast, the smallest available tablet of lorazepam (Ativan) is 0.5mg (equivalent to 5mg diazepam) [in the UK the lowest available dosage form for lorazepam is 1mg]; the smallest tablet of alprazolam (Xanax) is 0.25mg (also equivalent to 5mg diazepam). Even by halving these tablets the smallest reduction one could easily make is the equivalent of 2.5mg diazepam. (Some patients become very adept at shaving small portions off their tablets). Because of limited dose formulations, it may be necessary to switch to diazepam even if you are on a fairly long-acting benzodiazepine of relatively low potency (e.g. flurazepam [Dalmane]). Liquid preparations of some benzodiazepines are available and if desired slow reduction from these can be accomplished by decreasing the volume of each dose, using a graduated syringe.
Some doctors in the US switch patients onto clonazepam (Klonopin, [Rivotril in Canada]), believing that it will be easier to withdraw from than say alprazolam (Xanax) or lorazepam (Ativan) because it is more slowly eliminated. However, Klonopin is far from ideal for this purpose. It is an extremely potent drug, is eliminated much faster than diazepam (See Table 1, Chapter I), and the smallest available tablet in the US is 0.5mg (equivalent to 10mg diazepam) and 0.25mg in Canada (equivalent to 5mg Valium). It is difficult with this drug to achieve a smooth, slow fall in blood concentration, and there is some evidence that withdrawal is particularly difficult from high potency benzodiazepines, including Klonopin. Some people, however, appear to have particular difficulty in switching from Klonopin to diazepam. In such cases it is possible to have special capsules made up containing small doses, e.g. an eighth or a sixteenth of a milligram or less, which can be used to make gradual dosage reductions straight from Klonopin. These capsules require a doctor's prescription and can be made up by hospital pharmacists and some chemists in the UK, and by compounding pharmacists in North America. A similar technique can be used for those on other benzodiazepines who find it hard to substitute diazepam. To locate a compounding pharmacist in the USA or Canada this web site may be useful: www.iacprx.org. Care must be taken to ensure that the compounding pharmacist can guarantee the same formula on each prescription renewal. It should be noted, however, that this approach to benzodiazepine withdrawal can be troublesome and is not recommended for general use.
(3) Designing and following the withdrawal schedule. Some examples of withdrawal schedules are given on later pages. Most of them are actual schedules which have been used and found to work by real people who withdrew successfully. But each schedule must be tailored to individual needs; no two schedules are necessarily the same. Below is a summary of points to consider when drawing up your own schedule.
Design the schedule around your own symptoms. For example, if insomnia is a major problem, take most of your dosage at bedtime; if getting out of the house in the morning is a difficulty, take some of the dose first thing (but not a large enough dose to make you sleepy or incompetent at driving!).
When switching over to diazepam, substitute one dose at a time, usually starting with the evening or night-time dose, then replace the other doses, one by one, at intervals of a few days or a week. Unless you are starting from very large doses, there is no need to aim for a reduction at this stage; simply aim for an approximately equivalent dosage. When you have done this, you can start reducing the diazepam slowly.
Diazepam is very slowly eliminated and needs only, at most, twice daily administration to achieve smooth blood concentrations. If you are taking benzodiazepines three or four times a day it is advisable to space out your dosage to twice daily once you are on diazepam. The less often you take tablets the less your day will revolve around your medication.
The larger the dose you are taking initially, the greater the size of each dose reduction can be. You could aim at reducing dosage by up to one tenth at each decrement. For example, if you are taking 40mg diazepam equivalent you could reduce at first by 2-4mg every week or two. When you are down to 20mg, reductions could be 1-2mg weekly or fortnightly. When you are down to 10mg, 1mg reductions are probably indicated. From 5mg diazepam some people prefer to reduce by 0.5mg every week or two.
There is no need to draw up your withdrawal schedule right up to the end. It is usually sensible to plan the first few weeks and then review and if necessary amend your schedule according to your progress. Prepare your doctor to be flexible and to be ready for your schedule to be adjusted to a slower (or faster) pace at any time.
As far as possible, never go backwards. You can stand still at a certain stage in your schedule and have a vacation from further withdrawal for a few weeks if circumstances change (if for instance there is a family crisis), but try to avoid ever increasing the dosage again. You don't want to back over ground you have already covered.
Avoid taking extra tablets in times of stress. Learn to gain control over your symptoms. This will give you extra confidence that you can cope without benzodiazepines (see Chapter III, Withdrawal Symptoms).
Avoid compensating for benzodiazepines by increasing your intake of alcohol, cannabis or non-prescription drugs. Occasionally your doctor may suggest other drugs for particular symptoms (see Chapter III, Withdrawal Symptoms), but do not take the sleeping tablets zolpidem (Ambien), zopiclone (Zimovane, Imovane) or zaleplon (Sonata) as they have the same actions as benzodiazepines.
Getting off the last tablet: Stopping the last few milligrams is often viewed as particularly difficult. This is mainly due to fear of how you will cope without any drug at all. In fact, the final parting is surprisingly easy. People are usually delighted by the new sense of freedom gained. In any case the 1mg or 0.5mg diazepam per day which you are taking at the end of your schedule is having little effect apart from keeping the dependence going. Do not be tempted to spin out the withdrawal to a ridiculously slow rate towards the end (such as 0.25mg each month). Take the plunge when you reach 0.5mg daily; full recovery cannot begin until you have got off your tablets completely. Some people after completing withdrawal like to carry around a few tablets with them for security "just in case", but find that they rarely if ever use them.
Do not become obsessed with your withdrawal schedule. Let it just become a normal way of life for the next few months. Okay, you are withdrawing from your benzodiazepines; so are many others. It's no big deal.
If for any reason you do not (or did not) succeed at your first attempt at benzodiazepine withdrawal, you can always try again. They say that most smokers make 7 or 8 attempts before they finally give up cigarettes. The good news is that most long-term benzodiazepine users are successful after the first attempt. Those who need a second try have usually been withdrawn too quickly the first time. A slow and steady benzodiazepine withdrawal, with you in control, is nearly always successful.
(4) Withdrawal in older people. Older people can withdraw from benzodiazepines as successfully as younger people, even if they have taken the drugs for years. A recent trial with an elderly population of 273 general practice patients on long-term (mean 15 years) benzodiazepines showed that voluntary dosage reduction and total withdrawal of benzodiazepines was accompanied by better sleep, improvement in psychological and physical health and fewer visits to doctors. These findings have been repeated in several other studies of elderly patients taking benzodiazepines long-term.
There are particularly compelling reasons why older people should withdraw from benzodiazepines since, as age advances, they become more prone to falls and fractures, confusion, memory loss and psychiatric problems (see Chapter 1).
Methods of benzodiazepine withdrawal in older people are similar to those recommended above for younger adults. A slow tapering regimen, in my experience, is easily tolerated, even by people in their 80s who have taken benzodiazepines for 20 or more years. The schedule may include the use of liquid preparations if available and judicious stepwise substitution with diazepam (Valium) if necessary. There is, of course, a great deal of variation in the age at which individuals become "older" - perhaps 65-70 years would fit the definition in most cases.
2 notes
·
View notes
Text
Factitious Disorder - An overview
N Percent
Gender Male 176 34.2 Female 336 65.4 Marital status Unmarried 62 30.4 Married 97 47.5 Separated/divorced/widowed 45 22.0 Age (years) Total mean 33.5 Male 35 Female 32.8 Total range 18–73 Male range 19–67 Female range 18–73 Comorbid psychopathology 239 46.5 Occupation Health care profession 113 22.0 Others 94 18.3
During hospitalization, 65.8% of patients got a psychiatric consultation. The remaining 34.2% of patients refused or did not have the consultation.
Among the factors considered to be relevant to diagnose these disorders, the exclusion of other organic or psychiatric causes is the most represented, observed in 91.1% of cases.
An atypical presentation is another key issue (89.3%), which implies that the patient’s symptoms or the clinical course of the presumed condition is unusual, sometimes associated with incongruous instrumental findings. In some cases, it is also possible to observe an exacerbation of the symptoms in the presence of the medical staff or, on the contrary, in the absence of any witnesses.
Another important parameter is patient’s unusual behavior (86.2%), followed by treatment failure and/or high disease recurrence (83.7%).
The demographic profile of the sample shows a prevalence of female. The data support the hypothesis of several case reports and reviews that FD occur mainly in women.3,9,10 However, other studies published in the literature show a clear prevalence in male gender. This illusory disagreement finds an explanation in Freyberger’s words, who asserts that there is a prevalence of men in clinical trials for Munchausen Syndrome, while the women are most common in the classic form of FD with a ratio of 3:1.11
A disorder in which one pretends to be sick, by self-injury or making themselves sick.
Therapy
Psychotherapy:To help the patient recognise and acknowledge the problem. Also helps them learn coping skills.
Cognitive behaviour therapy:To bring changes in the person’s thinking and behaviour.
Medication
Antidepressants: To treat the associated depression.
Sertraline . Citalopram
Antianxiety drugs: To treat the associated anxiety.
Lorazepam . Diazepam
Rare (Fewer than 10,000 cases per year in Australia)
Treatments can help manage condition, no known cure
Doesn't require lab test or imaging
Can last several years or be lifelong
Common for ages 20-40
Symptoms of factitious disorder include:
Exaggeration of symptoms
Faking symptoms; inconsistencies in the symptoms reported
Dramatic presentation
Presence of symptoms only while being observed
Willingness and eagerness to have diagnostic tests or other procedures
Long medical records of multiple admissions to different hospitals
Reluctance by the patient to allow interaction of doctors with family members
Having a vast knowledge of the diseases one claims to have
Many surgical scars
Self-harm for example by injecting oneself with bacteria or gasoline
Tampering diagnostic results e.g., by heating a thermometer
Causes
The exact cause is unknown but it is attributed to psychological factors.
Risk factors for developing the disorder include:
Depression
Low self-esteem
Child abuse
History of illnesses that required hospitalisation
Personality disorders
Desire to be a healthcare professional
Loss of a loved one
#factitious disorder#munchausenbyproxy#disorder#actually mentally ill#self sabotage#mental instability#awareness
2 notes
·
View notes