#diagnosis via body language
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs



Fun Fact
70% of Tumblr users say the Dashboard is their favorite place to spend time online.
Text
when u look at nonverbal nonspeaking people diagnose with severe/profound intellectual disability you see roughly 2 group people:
1. people who it misdiagnosis because severe global apraxia motor issues make it impossible/near impossible mouth speak (at all or reliably). n difficulty control movement from that mean usual method of teach usual AAC not meet needs, make usual neuropsych etc assessment results unreliable because so much of it depend on reliable motor control, n unreliable movements often fit people assumption about what ID look like. but ultimately it not a intellectual/cognitive problem (many of them typical or high intelligence), it a global motor problem n it a speech problem (which for them is motor problem) not language problem.
2. people whose severe profound ID correct diagnosis & they nonverbal minimally verbal because language problem (n possibly speak motor problem but you need language first before think about mouth speak) because cognitive intellectual problem.
both group definitely exist. have seen people say group 1 not exist they all fake or faked by hopeful caregivers n clinicians, only group 2 exist. have also seen people say group 2 not exist, what you think of group 2 is all actually group 1 all of them. n both of them wrong
but base on how group 1 talk about how entire life they been assumed be group 2, both look similar enough under how developmental disabilities currently be understand n treated by professionals
2 group have some distinct n contradictory needs. group 1 want inclusion programs not segregated programs want same hardness education as nondisabled peers want be talked to n treated as same as cognitively able peers bc they cognitively abled, not 1+1 drills or “how cook” at school because assumed not able understand academics. they want communication methods that actually work with body with motor.
but if give same thing to group 2 it unhelpful at best n harmful/more frustrating n so cause more “challenging behaviors” - be taught things they will never understand because that what severe profound ID means, n be constantly surround by complicated thing dont understand n expect to do complicated thing dont understand is frustrating n they no way communicate that other than behaviorally. they often medically complex in way only have limited amount time n energy n brain slots to learn so it better teach them stuff that they may actually realistically use, like very basic daily life skills. communication support for them look like language development support n maybe communicate basic wants n needs via picture cards, n some them may never progress beyond answer basic question like what want eat with 1 maybe 2 picture cards, not to mention long phrases grammar sentences. some may not understand high tech AAC well enough to use. it not judgement it just realistic life for many.
n if give those to group 1 people, which many group 1 people got, my god it endlessly frustrating too
but. don’t know how tell apart group 1 from 2 beyond group 1 people say they group 1 (which, many group 1 people at parts of life not able do that bc motor). motor tests depend on cognitive intellectual understanding instructions, n cognitive intellectual testing depend on motor. “listen” n “presume competence” all true but idk how give what each group need without accident put them in other group n so give them “support” they not need. am not going be single person solve this but all scenario come up in head feel always there at least one reason fail. always fear that.
106 notes
·
View notes
Text
Watched ant’s werewolf video.
youtube
(And the transcript)
I applaud the history and mythology section but there’s never mention of the other werewolves!
And to that
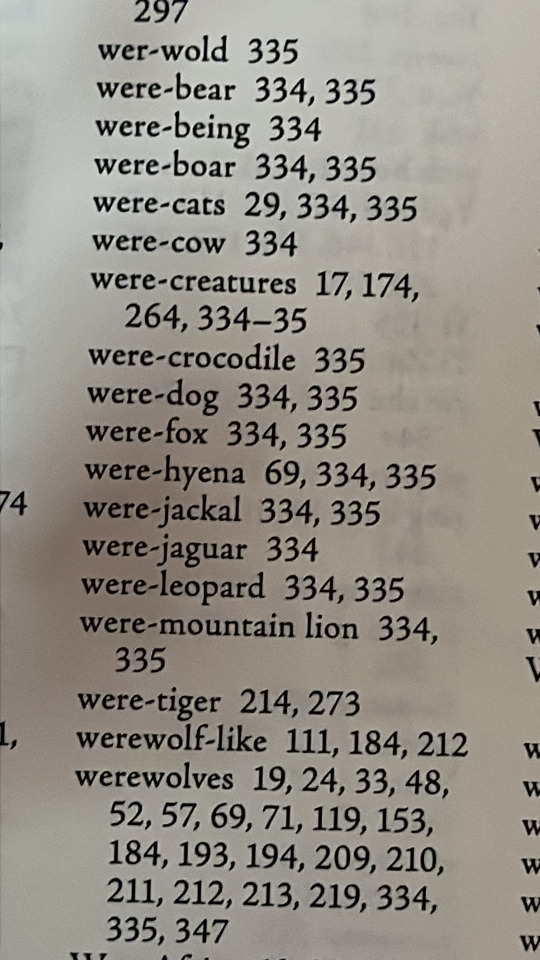
I have to grab the sources, More specifically this!
Welcome to my silly hyperfixation sperg!
I love me some mythology and history of these fantastical creatures. I do enjoy the movie approach and filmography of the werewolf history. (Even though you skipped shapeshifters from ❤️💀🤖) but I wanted to add to the cryptozoological side of it even if I’m a bit amateurish of the study.
Let’s dive in

Though early origins to the term of lycanthropy dating back to Ancient Rome and Ancient Greece via Latin language, humans that transform into dog like hybrids is a universal concept that can be found all over the world from Europe to South Asia!
As was our human way to explain what wasn’t yet known scientifically of modern times, for the civilizations who came before us, strangeness in people from neurological to physical abnormalities were thought to be otherworldly!
A rare mutation but oldest documented instance is when the hair on the body grow longer than what is “normal” leading to top to bottom fully covered in hair people: Hypertrichosis. Which is where the image of transformation came from or at least hypothesized to have been the origins of. Then there’s the actual clinically diagnosis of “clinical lycanthropy” which is when someone who has this believes they are in fact a werewolf.
So with the fun science out of the way! Allow me to list off every lycanthrope from around the world!
In alphabetical order of each name:
Airitech
Folklore of the Goidelic Celts.
Alp
Originating in Germany
Anjing Ajak
Indonesia
Azeman
Suriname folklore
Bal-bal
Philippines
Beast of Gevaudin
(Werehyena) France
Budas
Ancient Abyssinia
Buxenwolf
German folklore
Enkidu
Gilgamesh’s “best friend”
Headless mule
Iberian folklore - Portugal and Spain
Karkanxhol
Kolivilor
Albanian mythology
Kornwolf
Estonia, France, Germany, Hungary, Latvia, Poland and Russia
Lobis-Homem
Ancient Portuguese folklore
Lobishomen
(Female vampire witch werewolf) Brazil
Lobison
Argentina
Loup Garou
French origin and Caribbean island folklore
Luison
Paraguayan folklore
Lupo Mannaro
Italian and ancient Roman folklore
Marrock (Marrok the good knight)
Arthurian folklore
Zmag Ognjeni Vuk
Bosnian folklore (fire breathing werewolf)
I need a minute to catch my breath!
Ok!
As you can tell there’s quite a lot but I feel the need to also mention a morally good lycanthrope
Hailing from the Shetland isles of Scotland: the Wulver
They’d watch over flocks and tend to chores and leave behind fish on the windowsills of homes once they’re done helping. It’s said they’d only act in violence if provoked but other than that they were mostly seen as good!
So that’s my lil sperging about werewolf mythology! Good video Anthony!
I’m shook that no one mentioned the werewolves from the Halloween anthology film “Trick or Treat” or “the wolf among us” which was about the big bad wolf being a detective in a modern setting with fairytales and murder! Or the other red riding hood movie! “Red Riding Hood” (2011); with really good color story of mostly black and white scenery and striking red from our leading lady!
Ohmygod I nearly forgot that Pokémon even has a werewolf pokemon!

But ye I don’t have any better way to end this… other than a silly animation >:3c
40 notes
·
View notes
Text
Autistic Josh Headcanon Meta/Analysis - Introduction Episode
So I'm rewatching the show and decided I wanted to go ahead and type up some meta about why this headcanon is so vivid to me to the point that it's literally my url. Gonna do a post every time I hit an episode that is significant/relevant! And this is not going to be like based on clinical definitions or anything, just comparing what we see in the show to lived experiences of myself an other autistic people in a casual manner.
Starting with his introduction to the show!
An abrasive first impression. I love the way he's introduced to us, because they start off not exactly putting him in the best light. He's extremely direct and really leaves zero time for Maddie to get a word in edgewise, literally throws her book of notes in the trash, etc. And while this immediately gets contrasted with his demeanor once the shit hits the fan, and we see how his behavior is motivated by competency and passion for the job, that initial first impression of, "Wow, this guy seems like kind of a jerk" is one that many of us autistics have had to contend with.
An impatience for teaching. Something I've noticed among autistic people is that, unless teaching is their Thing that they have a passion for, explaining things to people is... well... not our strong suit. I'd much rather just do the task myself than try to teach someone else how to do it! And we see that in how much he just does NOT want to be training Maddie at that point, and the reliance on throwing her directly into the task and demonstrating it himself feels very autistic coded to me.
Quoting a famously autistic coded character. This one's more minor but like... not only is trying to connect with people via quotes and references already an autistic thing to do, the fact that one of his first lines is quoting Dr. Gregory House is sooo... I'm like okay I see you. Do you find this character relatable to you. Asking for your diagnosis.
Missing the joke. There is a moment after Maddie makes a joke by pretending not to have heard him that he just... it doesn't click. It takes a second. And man is that relatable. The amount of times I have started to genuinely repeat myself because I missed that the other person was doing a bit and was only pretending to have not heard me! And having to quickly recover like oh! haha! funny joke, I definitely understood it and I too am in on the joke! Very autistic exchange to me.
Being a dispatcher. I'll probably elaborate on this more in the episode where we learn how he ended up in this profession, but really the job of being a 911 dispatcher is evidence in itself. A job where you quite literally can't be asked to interpret facial expressions or body language? Where you don't have to worry about what your own face is doing because you never have to interact with these people in person and can just stay behind a computer screen? A job that requires you to stay calm and unemotional in the face of dangerous situations and other people's heightened emotions? Autistic. It's just an autistic coded job.
That's all for now, stay tuned for the next one. No idea which ep is next going to be relevant actually so I guess we'll find out when we get there <3
10 notes
·
View notes
Text
via internetkatze: #i recently read a book about speech impediments and ppl with developmental conditions#and one of the points it made was that a neurotypical able-bodied baby will babble things like this#and parents will respond with the correct cues even though the baby's speech is inaccurate#giving them the 'benefit of the doubt' and teaching them through conversation#but babies with disabilities are treated as stupid and their babbling is considered nonsensical#if the baby in this story could not point to the light fixture#and the parent had no high expectations due to a disability diagnosis#would they have responded with understanding and infant-directed speech?#in other words language development depends a lot on being willing to understand someone's difficulty expressing themself to you.#I KNOW THAT WAS A LONG TAG RANT i just wanted to talk about it bc it really made a good point and this was a great example
(me, my parents, my sister, and the baby are sitting at the kitchen table eating lunch)
baby, pointing at the light fixture over the table and signing "on": o.*
my sister: we actually can't turn that light on right now, because the lightbulb inside is burnt out! it needs a new one.
baby: ighbu.
sister: yes, lightbulb! granddaddy said after we eat he's going to climb up there on a ladder and change it, and then the light will come on!
baby: gadada! adda, uuu! ighbu o!
sister: exactly!
baby, signing "on" and pointing at the light and then my dad, with increasing urgency: GADADA ADDA UUUU. O.
my sister: we're going to finish eating first though, ok?
baby: nonono. O. gadada adda uuu.
[a split second goes by]
baby, pointing to himself: ba. adda uuu. ighbu.
me: you're going to climb the ladder and change the lightbulb yourself?
baby: dzyeah. *pointing to the buckle where he is buckled into the high chair* ububu.
me: unbuckle you? so you can change the lightbulb?
baby, highly businesslike: dzyeah.
*pronounced like "on" without the n
171K notes
·
View notes
Text

@heartmourne asked: the trouble with utilizing a submarine as their seafaring vessel, was that if something went wrong… well, the consequences were often a bit more dire than for those who sailed the seas on a ship, especially for a man like Law, who wielded a devil fruit and would sink faster than any anchor they could decide to drop. It was why he ran such a tight ship, choosing less to name a first mate and more to keep his fingers in every single pot of the Polar Tang’s day to day… from each engine check to his crew’s daily nutrition intake via meals. Some might call him micro-managey. Shachi and Penguin would declare him to have control issues. They were both right. Law was a smart man. He knew how to perform complex heart procedures by the tender age of thirteen. But that didn’t mean he knew everything - the ins and outs of his own ship’s submarine structure included. That was where Ikkaku came in, and not for the first time - the sleepless captain approached her in the wee hours of the morning, looking more like a ghoul than a man. “Ikkaku,” somber and serious as always, captain clutches Kikoku like a comfort, as if any social exertion demanded his cursed swords energy to muddle through ( he was far from a morning person ). “The stairwell next to the Captain’s quarters is making that horrible banging noise again.” It’s said as monotone as possible - not an order, certainly not a plea. Maybe closer to a question. It would explain why he looked extra exhausted though. “I checked, and I believe the hinge on the one metal doo-hickey is loose on that one thing.” At least he tried. Unprompted (Always Accepting!)


As far as Ikkaku was concerned, submarines were superior vessels when compared to most ships. Sure, they had their dangers and problems, but they circumvented many issues plaguing traditional ships. If there was a storm, the Polar Tang could sink beneath the waves into the calmer waters of the depths. They could hide from enemy ships and attack from below, keeping themselves safe and catching their opponents unawares.
Still, a submarine did have its dangers if not looked after carefully, which was why as the head engineer, Ikkaku took her job seriously. If anyone mentioned an odd sound or something not working as it should, she was on it instantly, checking thoroughly and making sure everything was working perfectly. Her crew wouldn't be harmed on her watch.
So while she was still a bit groggy herself, morning coffee having not quite hit her brain yet when Law approached, she immediately snapped to attention when her captain brought up his concerns. No, his language was far from technical, but she didn't expect him to know the name of every type of gear and piston any more than he'd expect her to name every bone in the body. And despite that, his description was helpful. Especially pointing out that it was a hinge that was loose. That narrowed things down significantly, so her diagnosis of the problem would go more quickly.
"Banging in the stairwell again, Captain? That can't be helping your sleep much," she said sympathetically. Rubbing her chin in thought, she considered what the issue could be. "Good news is that generally a loose hinge isn't something critical, so I don't think we'll need to surface. Still, I'll have a better idea once I've taken a look." Downing the rest of her coffee like a shot, she nodded. "Take me to the patient, Boss. I'll get that fixed up right away!"
#heartmourne#The Engine is the Heart of the Ship (canon)#Oh Captain My Captain (Law)#Join the Hearts: We Have Uniforms#(Ikkaku can't judge Law for using “doo-hickey” when she uses “thingamabob” to describe organs she can't identify)
1 note
·
View note
Text
AI Holobox Technology 2025: Transforming Human Interaction with 3D Intelligence

Introduction
AI Holobox Technology 2025 is revolutionizing the way we communicate, learn, and engage with digital environments. As the boundaries between the virtual and physical world continue to blur, AI-powered Holoboxes are emerging as a game-changing tool across industries such as entertainment, education, marketing, and customer engagement. In this article, we explore the top applications, innovations, and future of AI Holobox technology in 2025—and how it's reshaping the digital landscape.
What is AI Holobox Technology?
AI Holobox is a cutting-edge 3D holographic projection system enhanced by artificial intelligence. It allows lifelike holograms of people, objects, and environments to be displayed in real-time, offering immersive experiences that go beyond screens. Integrated AI enables these holograms to interact, respond, and learn, creating an intelligent virtual presence.
Top Applications of AI Holobox in 2025
1. Virtual Meetings & Remote Collaboration
With remote work now a standard in many industries, AI Holobox enables employees to appear as life-size holograms, adding human touch and body language to digital meetings.
2. Education and Training
AI Holoboxes bring virtual teachers, 3D models, and interactive simulations into classrooms, making complex topics easier to understand.
3. Retail & Customer Engagement
Brands are deploying Holoboxes to create virtual shopping assistants or display products in 3D, enhancing customer experience and reducing the need for physical inventory.
4. Healthcare Consultations
AI Holoboxes allow for remote medical consultations with 3D visualizations, enhancing diagnosis and doctor-patient interactions.
5. Entertainment and Live Events
Musicians, actors, and speakers can appear globally via hologram, powered by AI that adapts to audience engagement in real-time.
AI-Driven Personalization
AI Holoboxes in 2025 are equipped with emotion recognition, natural language processing, and real-time adaptation. This allows them to offer personalized responses, making digital interactions more human-like. For example, a virtual teacher can change tone based on student behavior or a sales hologram can recommend products based on past behavior.
How AI Holobox is Disrupting Marketing
Forward-thinking brands are using AI Holobox to:
Launch products with interactive 3D demos
Create immersive storytelling experiences
Run 24/7 virtual showrooms
Personalize content dynamically for users based on AI analytics
Companies that are early adopters of Holobox tech in 2025 are seeing improved conversion rates and engagement.
Challenges and Future Scope
While promising, AI Holobox faces challenges including high costs, content creation limitations, and privacy concerns. However, ongoing R&D and increased accessibility of AR/VR and AI tools are expected to reduce these barriers in the next 2–3 years.
In the near future, we might see:
Portable Holobox units for home use
Integration with blockchain for secure identity representation
Real-time translation for multilingual holographic communication
Conclusion
AI Holobox Technology 2025 represents a new frontier in human-machine interaction. Its ability to create immersive, intelligent, and real-time holographic experiences is opening doors across every industry—from education and healthcare to marketing and entertainment. As hardware becomes more accessible and AI continues to advance, Holoboxes will likely become a core part of our daily digital lives.
Brands, educators, and innovators who embrace this shift early will lead the next generation of communication. As AI Holobox technology evolves, the potential for impact is vast—reshaping not just how we communicate, but how we connect, learn, and grow in a digitally enhanced world.
#tagbin#writers on tumblr#artificial intelligence#technology#tagbin ai solutions#ai trends 2025#AI Holobox technology 2025#holographic AI communication#Holobox in marketing#3D hologram AI applications#futuristic education tools#AI in retail 2025#AI Holobox in healthcare#tumblr
0 notes
Text
Vital Role of Professional Nursing Organizations in Canada and British Columbia According to the society of Registered Nurses Association of British Columbia (RNABC), which will be renamed College of Registered Nurses of British Columbia (CRNBC), effective after May 2005, (Seale, 2005) the primary purpose of having professional nursing regulatory bodies and nursing associations for nurse practitioners in Canada and British Columbia are to ensure that all nurses have the basic competencies required of nurse practitioners expected by the public. Although nursing as a profession is regulated in virtually all Western, industrialized nations in some shape or form, in Canada and British Columbia, registrant participation through chapters has long been a particular cornerstone of the governance processes of the profession of nursing and expanded the profession's ability to evolve and serve the changing physical and mental needs of the public. (Nursing BC, 2004) Nursing Organizations -- Establishing Professional Standards, Contributing to Professional Enrichment Professional nursing organizations provide vital aid to Canadian nurses. These organizations not only ensure that nurses are certified as competent in the public's eyes, but provide important information to nursing professionals regarding their own health insurance, keep a careful regulatory eye on the need to fulfill nurse's personal health and safety requirements on the part hospitals and employers, and provide a source of comradeship and continuing education for nurses over the course of their careers. Professional organizations such as the CRNBC ensure that all nurses meet certain core competencies over the course of the initial phases of a nurse's professional orientation and education. These competencies are usually achieved through graduate nursing education and substantial registered nursing practice experience. These organizations ensure that nurses' educations will provide nurses with the ability to show, via their membership and certification that they have satisfied the basic standards to become registered nurses and have achieved the competencies required for registration as a nurse practitioner with their organization. Recently, the Canadian Nurse Practitioner Initiative (CNPI), led by the Canadian Nurses Association, has sought to expand the education and role of nursing practioners by "developing a pan-Canadian framework for the sustained integration of nurse practitioners in primary health care, often the first point of access to health-care services for patients in Canada." (CNPI, 2005) Nurse practitioner competencies by organizations are used "to establish the eligibility of registered nurses for registration as nurse practitioners." (RNABC, 2003, p.2) Professional organizations strive to define exactly what nurse practitioners are in their defined functioning in the health care system. They are health care providers who provide health care services from "a holistic nursing perspective, combined with a focus on the diagnosis and treatment of acute and chronic illnesses, including prescribing medications. Nurse practitioners work as integral members of the health care team to provide and coordinate initial, continuing and comprehensive advanced nursing services. The changing face of Canada has brought new resolve to nurse practitioners who strive to "serve the ethnically and culturally diverse population" of the nation. The Canadian Nurse Practitioner Institute website is multilingual, both French and English, as well as including links to other language sites with information on health care in observance of this reality of today's Canada. (CNPI Website, 2005) Also, the aging population and increased lifespan of many Canadians means that nurses must serve patients, "across the continuum of health throughout the life span. The health services provided by nurse practitioners include health promotion and maintenance of wellness," and "illness and injury prevention; and health care management of acute and chronic illnesses, including ordering diagnostic investigations and prescribing treatment (including medications). Nurse practitioners collaborate with other members of the health care team to improve client health outcomes by increasing accessibility to health care services, expanding clients' health care options and filling gaps in health care delivery." (RNABC, 2003, p.4) The Canadian Nurses' Association has lobbied for future legislation to enable nurses to perform some of the traditional functions of doctors, to fill some of the provider gaps within the Canadian healthcare system. (C.N.A., 2005) Today, all nurse practioners strive to fulfill this vision or mission statement of their profession will attempt to expand upon the nursing profession's essential functions. The national advanced nursing practice has established core competencies for all nurses to fulfill the current requirements of their profession, as well as to serve the changing faces and bodies of Canadian patients. For instance, one of the nurse practitioner core competencies is that a nurse performs an advanced, comprehensive and holistic health assessment, including a health history and complete physical examination. "The assessment considers the psychosocial, emotional, ethnic, cultural and spiritual dimensions of health," as well as the purely physical and involves achieving an understanding with clients the meaning of their health/illness experiences and how their daily living is affected." (RNABC, 2003, p.6) The thus, the nurse must strives to teach and treat the whole patient, not merely assess the relative sickness of the patient. But how does this mission and statement of core competencies affect ordinary nurses in the field, one might ask? According to the journal British Columbia Nursing, one nurse, under the supervision and training of her local nursing organization, "has also taken a leadership role in the community as a casual registered nurse for the after-hours Urgent Response Program for community mental health/addictions, in an effort to treat the mental as well as the physical complications of addiction she saw in her patients while she was completing her baccalaureate degree, and obtained Canadian Nurses Association (CNA) certification in psychiatric/mental health nursing. The organization encouraged her to completed a diploma in advanced psychiatric nursing, and now she sits "on a variety of committees and worked with other Royal Inland workplace representatives and with the British Columbia Nurses Union (BCNU) Io promote a quality practice environment." (Priest, 2004) This is an example of the mentoring, certification, and mission statement process in action, coalesing in the successful professional involvement an dcommunity activism of one motivated individual. Some concerns of nurses are, of course, slightly less idealistic. But nursing organizations also provide vital information regarding, for example, nursing insurance. For instance, as an independent contractor a nurse is considered to be self-employed. One nurse recently queired her local nursing organization regarding her self-employed status regarding her own health insurance, and was advised: "To be considered as a practicing self-employed registered nurse in British Columbia, you must hold current practicing registration with RNABC. This then provides you with liability coverage through the RNABC Captive Insurance Corporation (a wholly owned subsidiary of RNABC that is managed outside of RNABC). Depending on the circumstances of your work as a self-employed registered nurse, you may need to purchase additional insurance to adequately protect yourself (contact RNABC Practice Support if you need more information)." (Willson, 2005) Nursing associations thus provide vital sources of practical as well as mission-statement oriented data for practioners. Conclusion Despite these contributions, the structure and function of professional chapters has been of concern to the Board of Directors for many years. For instance, a recent review of registrants' involvement in RBABC chapters indicated that there is no longer a broad base of support or involvement with chapters as they currently exist. "Of the 4,817 responses received to an e-mail survey of 14,180 RNABC registrants, 93% of the respondents described themselves as 'not active at all' or 'not very active' with their RNABC chapters. Forty-eight per cent said they have never attended a chapter meeting. Only 20% said they had attended a chapter meeting in the previous 12-month period. Yet, the continued striving of professional organizations such as the Canadian Nurses Association, CPNI, and the RNABC to expand the role of the nurse practioner as "workplace representatives who take on leadership roles are central to progressive change and to guiding others toward a common goal or desired end," ensures that such organizations must forge ahead to remain vital sources of professional connection in the changing world of Canadian health care. ("RNABC Reviews Chapters Under the Health Professions Act," Nursing BC, 2004) Works Cited C.N.A. (2004) Official Website. Retrieved 24 May 2005 at http://www.cna-nurses.ca/CNA/practice/advanced/initiative/default_e.aspx CNPI. (15 Apr 2005) "Nurse Practitioner Role to Strengthen Canada's Primary Health-Care System" Retrieved 24 May 2005 at http://www.cnpi.ca/documents/pdf/CNPI_news_conference_April_15_e.pdf CNPI. (2005) Official Website of Canadian Nursing Practioners. Retrieved 24 May 2005 at http://www.alden-bugden.ca/cnp/modules/news/ Registered Nurses Association of British Columbia (2003) "Competencies required for Nurse Practitioners." Retrieved 24 May 2005 at http://www.rnabc.bc.ca/pdf/416.pdf 'RNABC Reviews Chapters Under the Health Professions Act" (Dec 2004) Nursing BC. Retrieved 24 May 2005 at http://www.findarticles.com/p/articles/mi_qa3916/is_200412/ai_n9471965 Searle, Howard. (Feb 2005) "Continuing to Support Provision of Safe Care." Nursing BC. Retrieved 24 May 2005 at http://www.findarticles.com/p/articles/mi_qa3916/is_200502/ai_n11826269 Priest, Alicia. (Feb 2005) "Born Leaders." Nursing BC. Retrieved 24 May 2005 at http://www.findarticles.com/p/articles/mi_qa3916/is_200502/ai_n11826271 Willson, Barbara (Feb 2005) "Liability Insurance Coverage When Working in a Private Medical Clinic." Retrieved 24 May 2005 athttp://www.findarticles.com/p/articles/mi_qa3916/is_200502/ai_n11826270 Read the full article
0 notes
Text
The Secret
by Coors2 On a cold night in Colorado, Johnny Lawrence enjoyed the warmth of the moment beside Daniel, until the sound of a phone interrupted the calm. Driven by curiosity, Johnny read the message on the screen: Ali was asking about Daniel, expecting him to come back early. A chill ran down his spine as he assumed the worst—Daniel was with her, and everything had been a lie. Heartbroken and furious, Johnny hurriedly got dressed and left the room without looking back. Back in Los Angeles, he tried to resume his routine, but the memory of that night haunted him. He threw himself into work and drinking, trying to forget what could never be. However, something in his body began to change. Nausea, fatigue, and dizziness made him suspect something was wrong. At first, he blamed stress and hangovers, but when the symptoms persisted, he decided to see a doctor. The diagnosis was a shocking revelation—he was pregnant. Words: 1302, Chapters: 1/1, Language: English Fandoms: Cobra Kai (TV), Karate Kid (Movies) Rating: General Audiences Warnings: Creator Chose Not To Use Archive Warnings Categories: F/M, M/M Characters: Samantha LaRusso, Anthony LaRusso, Amanda LaRusso, Johnny Lawrence, Daniel LaRusso, Bobby Brown (Karate Kid) Relationships: Daniel LaRusso/Johnny Lawrence Additional Tags: pregnat male via https://ift.tt/fLMvxgz
0 notes
Text
Survivalism
Survivalism https://ift.tt/pjBy8Kh by bleuzombie Genetic engineers Castiel Novak and Dean Winchester are on the verge of a breakthrough in cancer treatment and possibly even a cure, using genetic manipulation and incredibly, shark DNA. Following a devastating diagnosis of brain cancer, and amid growing pressure from his boss, Dick Roman, for results, Castiel is pushed to an act of desperation. He tests the cure on himself with disastrous and violent results. He has never been so hungry. Words: 14067, Chapters: 4/4, Language: English Fandoms: Supernatural (TV 2005) Rating: Explicit Warnings: Graphic Depictions Of Violence, Major Character Death Categories: M/M Characters: Castiel (Supernatural), Dean Winchester, Charlie Bradbury, Mick Davies, Dick Roman (Supernatural), Edgar (Supernatural), Royce (Supernatural), Chet (Supernatural) Relationships: Castiel/Dean Winchester Additional Tags: Scientist Castiel (Supernatural), Scientist Dean Winchester, Genetic Engineering, genetic manipulation, Bad Scientist Castiel, Cannibalism, Animal Autopsy, Animal Death, like a lot of animal death, Blood, Violence, Blood and Violence, Blood and Gore, Body Horror, Bad Scientific Practices, Human Experimentation, physical assault, Minor Character Death, Barely Anyone Makes it Out Alive, Killing a Fan Favorite, Eating Live Animals, eating rats, Popping Baby Rats Like Jellybeans, Dead Dove: Do Not Eat via AO3 works tagged 'Castiel/Dean Winchester' https://ift.tt/5Gj1MnS October 12, 2024 at 02:26PM
#IFTTT#AO3 works tagged 'Castiel/Dean Winchester'#Destiel#ao3feed#ao3feed Destiel#Destiel fanfic#Dean Winchester/Castiel#Castiel/Dean Winchester#Dean x Castiel#Castiel x Dean
0 notes
Text
[𝐓𝐇𝐈𝐒 𝐈𝐒 𝐀𝐍 𝐔𝐏𝐃𝐀𝐓𝐄𝐃 𝐁𝐈𝐎
𝐓𝐖: 𝐅𝐎𝐑 𝐕𝐀𝐑𝐈𝐎𝐔𝐒 𝐒𝐄𝐍𝐒𝐈𝐓𝐈𝐕𝐄 𝐓𝐎𝐏𝐈𝐂𝐒]
𝐆𝐄𝐍𝐄𝐑𝐀𝐋
❧Full Name: Sofia Jazmine Hartfield
Maiden name: Leonetti
Goes by: Jasmine
❧Age: 29
❧Sex: Female
❧Birthday: April 13
❧Occupation: Owner of two hotels based in NYC that she inherited from her late husband. When the money gets tight she makes her money through less conventional means, via streaming lewd content.
❧Sexual Orientation: Bisexual
❧Relationship Status: Single
❧Languages: Fluent in French and English, knows some Italian
𝐀𝐏𝐏𝐄𝐀𝐑𝐀𝐍𝐂𝐄
❧Height: 5’3
❧Body Build: Thinner than usual due to complications, medications she is on, and hospitalizations.
❧Skin color: On the lighter side but if desired she could tan into more of an olive color thanks to her Italian in her.
❧Hair style: Medium length with curtain bangs usually worn down with soft ironed curls. For special occasions she’ll wear it up.
❧Hair color: Dark brown
❧Eye color: Medium brown
❧Distinguishing Features: Wide smile with pouty lips usually sporting red lipstick, on the rare occasion she gives you a smile it’s full of warmth, and her nose, a rather unique shape.
❧Preferred Clothing: Anything fancy or “classic”. Fond of more vintage styles like the 40’s and so on. Sometimes this plays a light role in the things she buys or wears. Willing to spend ridiculous amounts on clothing, jewelry, or shoes. Usually found in a skirt or a dress paired with some heels if she’s out and about.
❧Accessories: Has jewelry for every occasion and outfit. Regularly wears a ring gifted from her spouse on her right hand.
❧Tattoos: She has a rose done by a former friend on her side under her boob which has a significant meaning to her, a moth between her breasts, and “Parker” written in cursive between her fingers.
❧Scars: Her thighs are littered with past self inflicted scars, and one fading on the inside going down her forearm.
𝐇𝐄𝐀𝐋𝐓𝐇
❧General health: Drastically has improved within the last three months. However is currently slipping back into past habits.
❧Posture: Very proper, however if she’s comfortable around you she can be found lounging about more often than not. Often like a cat would make themselves comfortable just about anywhere.
❧Any physical illnesses?: N/A
❧Any mental illnesses?:
—Borderline personality disorder with psychotic features: Being very open with her BPD it’s hard not to tell she has this personality disorder, causing her to be irrational, impulsive, and harmful to herself. Jasmine’s moods often change at the drop of a hat, ranging from depressive episodes to irrational anger. She can be difficult to understand at times. The part she isn’t so open with is her psychotic symptoms and episodes she has.
—Anorexia Nervosa: She is not open about this diagnosis with anyone not even her partner or people closest. Its a struggle that shes dealt with since her early teens fed on by her mother. Causes her to be overly obsessive and get anxious over food. However she writes it off as being particular to most people.
—CPTSD: This is more private and rare she will open up about some of the things she went through, she’d much rather pretend it didn’t happen.
❧Take prescription drugs?: Attempts to take her prescriptions daily, however the meds she has moved onto make her feel like a shell of a human so no longer takes them. It’s always
❧Indulge in drugs?: Not anymore, going on 2 months clean.
❧Drink?: Tends to steer away from alcohol because she gets carried away with anything and everything and overly self indulges to the point it’s unhealthy.
❧Smoke?: Yes, regular smokes cigarettes.
𝐌𝐄𝐍𝐓𝐀𝐋/𝐄𝐌𝐎𝐓𝐈𝐎𝐍𝐀𝐋 𝐒𝐓𝐀𝐓𝐄
❧Mental age: Somewhere near hers, not as grown in some ways as she should be.
❧Act before thinking/Think before acting?: Acts before thinking. Tries to break out of the habit but often is driven by impulse and emotions.
❧Likes:
-Art in all kinds of forms like literature and painting
-Moths/Butterflies
-Flowers hold great significance to her so she has her own garden she often tends to
-Clean and tidy appearances on her and in homes or work spaces
This would be a long list if I went on and on, she has all kinds of interests.
❧Dislikes:
-Being unsure of others emotions or how they feel
-Passive aggressive behavior
-Foods she deems gross or unhealthy
-People bringing up her past/childhood or trying to get more on it from her. Much rather it be forgotten.
❧Fears:
-Abandonment, which she feeds so it plays an unhealthy role throughout her life.
-Being undesirable or not being useful to the ones she loves or cares for.
❧Dreams/Goals:
-She hopes to achieve some time of stability with her mental health and declining financial status.
-Would love to be somewhere warm and have a complete and real family.
-Ultimately wants to feel how she used to, less reliant on others and a sense of self. Which is often shifting and changing due to her BPD, she adapts and mirrors certain aspects.
𝐅𝐚𝐯𝐨𝐮𝐫𝐢𝐭𝐞𝐬
❧Foods:
-Fruits (just about all them)
-Dubliner cheese
-Vegetables
-Sushi
-A good mushroom burger if she’s not being overly thoughtful about food.
❧Colour: Red
❧Animals: Cats, bunnies— really all kinds of animals. Pretends to be grossed out but really enjoys them.
❧Holiday: When she used to party often she looked forward to the holidays but now she isn’t particularly into them.
❧Season: Spring, when it comes to life and everything get warmer
❧Time of day: Evening, when everything winds down and feels peaceful
❧Type of art: Old oils on canvas/panels
❧Genre of music: All different types, loves attending the opera or seeing more classical things
❧Genre of literature: All kinds, loves to read whenever she can, her nose is often stuck in a book.
❧Genre of shows: Not big on shows unless it’s a short series, only a couple episodes
❧Genre of movies: Psychological thrillers, slowly loving romance more and more
-𝐁𝐀𝐂𝐊𝐆𝐑𝐎𝐔𝐍𝐃 𝐀𝐍𝐃 𝐌𝐎𝐑𝐄 𝐈𝐍𝐅𝐎 𝐓𝐎 𝐂𝐎𝐌𝐄-

#original character#oc#bio#biography#basic info#roleplay#role play#jasmine Hartfield#character info#template#open to write#AUs#alternate au#alternate universe#multi para rp#novella#novella rp#para#para rp#banter
40 notes
·
View notes
Text
psychology + mental health deep dive !

general mental health related trigger warnings apply. feel free to include more or exclude those facts / test results that take too much time or don’t apply, you can check out this list for more personality-related quizzes to include!
QUICK FACTS ,
diagnoses: none at present , probably some type of trauma related disorder depending on the verse / time. triggers: unexpected biting / roughness, mentions of former abuse / people calling her out on how she should react to damon’s abuse positive coping skills: organization, talking to people, likely breathing techniques or mantras negative coping skills: hyperfocusing on tasks, poor sleep management, avoidance, over-dependency / co-dependency, minimizing symptoms / history attachment style: anxious love language: words of affirmation + physical touch myers briggs / mbti: enfj
HISTORY EXPLORATION ,
are their diagnoses formal ( via a doctor, therapist, etc. ) or informal ( self diagnosis, a hunch, unrealized, etc. ) she’s never had any formal diagnosis but she probably would have fit criteria for like panic disorder or ptsd
have they ever been treated / medicated? she probably saw a therapist like one time at her dad’s request after the divorce, but she probably refused to go back. no medication history.
have they ever been hospitalized or treated on an inpatient basis? no
how old were they when they first started experiencing / realizing symptoms? mid-teens, she definitely started having a lot more anxiety-related issues when her dad left due to fears of not being “perfect” enough, and then it all came to a head after damon, when she would have panic attacks semi-frequently
do they have a family history of mental illness? none that she’s aware of
how was mental health handled / discussed in the family / community? it wasn’t! bill very likely discussed it in terms of being able to be treated / trained / conditioned out, so her view is that a lot of it can probably be “fixed” through some level of intervention, and therefore she probably grew up thinking that a lot of mental health aspects meant you were broken
what are their thoughts on mental health / their diagnosis? she refuses to think about it or acknowledge it because she doesn’t know how to properly explain it and she’ll minimize it to no end
in what ways has their diagnosis shaped their life or experiences? she’s never processed a lot of things because she’s never known how to, and therefore she just kinda keeps it all internalized and therefore if it’s brought up unexpectedly or she’s confronted with it, she doesn’t have the tools to manage the reaction
SYMPTOMS: note that all of the below are, on their own, normative and typical aspects of human functioning. they become “symptoms” when they last longer than “normal” or when they pose a significant impact on someone’s life / functioning.
BOLD all that are present, ITALICIZE those that are resolved or in the history.
depression. anxiety. panic attacks. dissociation. derealization. depersonalization. suicidal ideation. self harm. homicidal ideation. psychosis. auditory hallucinations. visual hallucinations. delusions. mania. hypomania. racing thoughts. hyperactivity. attention difficulty. flashbacks. nightmares. hyperarousal. hypoarousal. hypersexuality. hyposexuality. psychopathy. risky behavior. catatonia. somatic / bodily concerns. mutism. phobia. agoraphobia. hoarding. obsessions. compulsions. body dysmorphia. hair picking. skin picking. amnesia. illness anxiety / hypochondria. sensory loss. speech difficulty. comprehension difficulty. communication difficulty. tics. defiant behavior. irritable mood. vindictiveness. aggression. pyromania. kleptomania. paranoia. attention seeking. narcissism. avoidance. dependency. pica. rumination. food restriction. food binging. purging. soiling the bed. insomnia. fatigue. sexual dysfunction. delirium. developmental delays.
explanations / elaborations on any of the above symptoms:
she never self harmed in the typical sense, but she would definitely do things that qualify as inadvertent self harm --- like neglecting proper sleep scheduling to work on a project or not really taking care of herself. the dissociation and hypoarousal are both things that she experienced a lot after damon, as well as the panic attacks ( which can still pop up time to time )
tagged by: no one i made it :) tagging: @shesdaylight , @sithdestined , @desafia , @klarsynt , @sororanimarum , @negotiaetor , @webheadedhero , @littlebennettbitch , @lowsurvival , @fatedtragedy , @awalkoflife , @heirceleste , @eiiidetic + and everyone else bc im curious .
19 notes
·
View notes
Text
psychology + mental health deep dive
general mental health related trigger warnings apply. feel free to include more or exclude those facts / test results that take too much time or don’t apply, you can check out this list for more personality-related quizzes to include!

quick facts
diagnoses: ptsd, unspecified anxiety disorder/s (needs further evaluation) triggers: undefined, usually resistant to triggering situations to a degree. positive coping skills: maintaining a routine, eating and sleeping regularly, maintaining her own hygiene as well as the hygiene of her surroundings and her dog negative coping skills: social isolation + withdraw, (sometimes) under-eating or sleep deprivation, self-sabotaging and suicidal plans attachment style: disorganized / fearful-avoidant love language: physical touch (receiving), quality time (mutual), acts of service (giving) myers briggs / mbti: ISTJ
history exploration
are their diagnoses formal ( via a doctor, therapist, etc. ) or informal ( self diagnosis, a hunch, unrealized, etc. )
semi formal. a proper psychological evaluation was done when riza formalised her military career after the war.
have they ever been treated / medicated?
no, she was deemed "functional" and has not had any follow up treatment.
have they ever been hospitalized or treated on an inpatient basis?
no, only hospitalised for physical injuries after the promised day events.
how old were they when they first started experiencing / realizing symptoms?
some steem from childhood, some from war.
do they have a family history of mental illness?
yes, her father berthold hawkeye was severely mentally ill though undiagnosed.
how was mental health handled / discussed in the family?
it wasn't.
what are their thoughts on mental health / their diagnosis?
she sees it the same as other physical injuries. the brain is just another organ.
in what ways has their diagnosis shaped their life or experiences?
it hasn't. much like other physical illness and injuries, if it's something she can live and deal with and go without medical assistance she'll take that route. unfortunately, mental health does fall under this.
symptoms
bold all that are present, italicize those that are resolved or in the history.
depression. anxiety. panic attacks. dissociation. derealization. depersonalization. suicidal ideation. self harm. homicidal ideation. psychosis. auditory hallucinations. visual hallucinations. delusions. mania. hypomania. racing thoughts. hyperactivity. attention difficulty. flashbacks. nightmares. hyperarousal. hypoarousal. hypersexuality. hyposexuality. psychopathy. risky behavior. catatonia. somatic / bodily concerns. mutism. phobia. agoraphobia. hoarding. obsessions. compulsions. body dysmorphia. hair picking. skin picking. amnesia. illness anxiety / hypochondria. sensory loss. speech difficulty. comprehension difficulty. communication difficulty. tics. defiant behavior. irritable mood. vindictiveness. aggression. pyromania. kleptomania. paranoia. attention seeking. narcissism. avoidance. dependency. pica. rumination. food restriction. food binging. purging. soiling the bed. insomnia. fatigue. sexual dysfunction. delirium. developmental delays.
note that all of the below are, on their own, normative and typical aspects of human functioning. they become “symptoms” when they last longer than “normal” or when they pose a significant impact on someone’s life / functioning.
explanations / elaborations on any of the above symptoms
riza is generally very self aware and has a strong grip on herself, most "symptoms" are either circumstantial (i.e high stress, life or death situations, fighting homunculi and all that jazz) and laying dormant until a specific event triggers a reaction, or are underlying subconsciously in her thoughts hardly ever being expressed outwardly instead appearing always calm, collected and even cold or emotionless.
tagged by: i stole this from @seesgood ! tagging: @kingsleyer, @hongdiwang, @fullmtal, @stovthearted, @bidotheuncanny, @blanchette + anyone else who wants to do it
6 notes
·
View notes
Text
psychology + mental health deep dive !
general mental health related trigger warnings apply. feel free to include more or exclude those facts / test results that take too much time or don’t apply, you can check out this list for more personality-related quizzes to include!
QUICK FACTS ,
diagnoses: triggers: positive coping skills: negative coping skills: attachment style: love language: myers briggs / mbti:
HISTORY EXPLORATION ,
are their diagnoses formal ( via a doctor, therapist, etc. ) or informal ( self diagnosis, a hunch, unrealized, etc. ) depressive disorder. it’s largely undiagnosed, though I wouldn’t be surprised if Dr. Kafka had diagnosed him.
have they ever been treated / medicated? He’s had a few informal therapy sessions with Kafka, but largely no.
have they ever been hospitalized or treated on an inpatient basis? he’s been hospitalized for physical injuries, but mental ones? no.
how old were they when they first started experiencing / realizing symptoms? I would say around five. since that’s not long after his parents were killed. Only fo rthings to get worse when he was fifteen and his uncle was murdered.
do they have a family history of mental illness? hmmm, there’s not much mention of it but I would say, no.
how was mental health handled / discussed in the family? for the most part, it isn’t. peter is pretty closed off, and since he didn’t let his aunt in on his secret until he was an adult. he was a bit more open about things that were bothering him, but even then he didn’t really open himself up entirely.
what are their thoughts on mental health / their diagnosis? in general, he thinks mental health is an important thing to keep up with. he’s compassionate to a fault, and is almost always willing to try and rehabilitate or help someone through whatever they’re going through. as for his diagnosis, he’s vaguely aware of it but he doesn’t have many thoughts about it.
in what ways has their diagnosis shaped their life or experiences? it had an impact in the way he views himself. I made a post about it (thanks in large part to lia cause she’s the best) but. short version is, for the longest time he was isolated because he chose to be. he thought it was best if people weren’t associated with him, because death seemed to surround him. he had difficulty forming friendships and relationships with others. he didn’t view himself as a good person for the longest time, and in many ways still doesn’t. he has a tremendous amount of guilt on his conscience. I could go on and on, and have in another post for now, this will do.
SYMPTOMS: note that all of the below are, on their own, normative and typical aspects of human functioning. they become “symptoms” when they last longer than “normal” or when they pose a significant impact on someone’s life / functioning.
BOLD all that are present, ITALICIZE those that are resolved or in the history.
depression. anxiety. panic attacks. dissociation. derealization. depersonalization. suicidal ideation. self harm. homicidal ideation. psychosis. auditory hallucinations. visual hallucinations. delusions. mania. hypomania. racing thoughts. hyperactivity. attention difficulty. flashbacks. nightmares. hyperarousal. hypoarousal. hypersexuality. hyposexuality. psychopathy. risky behavior. catatonia. somatic / bodily concerns. mutism. phobia. agoraphobia. hoarding. obsessions. compulsions. body dysmorphia. hair picking. skin picking. amnesia. illness anxiety / hypochondria. sensory loss. speech difficulty. comprehension difficulty. communication difficulty. tics. defiant behavior. irritable mood. vindictiveness. aggression. pyromania. kleptomania. paranoia. attention seeking. narcissism. avoidance. dependency. pica. rumination. food restriction. food binging. purging. soiling the bed. insomnia. fatigue. sexual dysfunction. delirium. developmental delays.
explanations / elaborations on any of the above symptoms:
with the hallucinations it’s tough. cause he’s had moments where he’s heard people who have died speak to him, or appear. though it’s tough to say if it was a true hallucination or more of a writer’s technique, or just pure guilt ridden brain. maybe a bit of both? I didn’t know whether to italicize it, but. I left it blank fjaksldjfklds.
tagged by: @seesgood and @desafia
tagging:YOU
6 notes
·
View notes
Text
The Secret
by Coors2 On a cold night in Colorado, Johnny Lawrence enjoyed the warmth of the moment beside Daniel, until the sound of a phone interrupted the calm. Driven by curiosity, Johnny read the message on the screen: Ali was asking about Daniel, expecting him to come back early. A chill ran down his spine as he assumed the worst—Daniel was with her, and everything had been a lie. Heartbroken and furious, Johnny hurriedly got dressed and left the room without looking back. Back in Los Angeles, he tried to resume his routine, but the memory of that night haunted him. He threw himself into work and drinking, trying to forget what could never be. However, something in his body began to change. Nausea, fatigue, and dizziness made him suspect something was wrong. At first, he blamed stress and hangovers, but when the symptoms persisted, he decided to see a doctor. The diagnosis was a shocking revelation—he was pregnant. Words: 1302, Chapters: 1/1, Language: English Fandoms: Cobra Kai (TV), Karate Kid (Movies) Rating: General Audiences Warnings: Creator Chose Not To Use Archive Warnings Categories: F/M, M/M Characters: Samantha LaRusso, Anthony LaRusso, Amanda LaRusso, Johnny Lawrence, Daniel LaRusso, Bobby Brown (Karate Kid) Relationships: Daniel LaRusso/Johnny Lawrence Additional Tags: pregnat male via https://ift.tt/5eEnjST
0 notes
Text
Sensory Processing Disorder
Their unique brain structure and function enables high IQ individuals to receive and process greater amounts of sensory input at once. Gifted people can detect and respond to sensory stimuli more quickly. They can think more complex and abstract thoughts, scan visual images quicker, detect visual and cognitive patterns, and make connections between seemingly unrelated bits of information. They can read micro facial expressions and body language, perceive what others are thinking, and accurately predict their responses. These abilities make high IQ individuals good at researching, detecting, code breaking, and intelligence gathering. Their quick reflexes and superior hand-eye coordination allow them to control a speeding vehicle and reverse a trailer with high accuracy. Their superb memories and auditory processing capacity allow them to function as human tape-recorders and to rapidly acquire foreign languages. In a military setting, their high visual-spatial processing IQ scores flag them as potential elite sniper squad recruits. Combine superior reaction time, hand-eye coordination, physical strength, agility, sniper skills, physical fitness, and a whole lot of ability enhancement via brainwashing – and you have a potential super soldier. This might explain why the CIA targeted high IQ visual-spatial learners.
Unfortunately, that which enables gifted individuals to perform impressive cognitive tasks is the same thing that makes them hypersensitive to sensory stimuli. The higher the IQ, the greater the sensitivity to light, noise, touch, smell, taste, and emotional stimuli. Such sensitivity has been labelled a developmental condition, Sensory Processing Disorder. SPD contributes to why gifted people often turn to drugs and alcohol, to subdue the constant overwhelming barrage of sensory input.
Note that people on the autism spectrum are also prone to SPD. While they share hypersensitivity and certain cognitive abilities, autism must not be confused with giftedness. Remember McGilchrist’s observation that these developmental disorders feature profound right hemispheric abnormality. In stark contrast, gifted individuals demonstrate exceptional right hemispheric functioning. Yet ignorant and jealous health professionals routinely misdiagnose intellectual giftedness as high-functioning autism.
Extreme visual-spatial processing ability renders gifted individuals susceptible to PTSD, and this can confound diagnosis. The high IQ victim is so sensitive that merely hearing a traumatic story second-hand affects them as though they witnessed the event first-hand. They turn the verbal rendition of the event into an internal movie so that the traumatic scene is permanently stored in memory and may be replayed. Their right hemisphere repeatedly plays an internal movie of a trauma incident.
This hypersensitivity makes the trauma-based nature of mind control programming especially painful for high IQ victims. Fundamental brainwashing techniques involve overwhelming the victim’s nervous system with sensory stimuli. Sensory overload is achieved via the parallel infliction of loud screeching sounds, foul smells, electrocution, and forcing the eyelids open to view horrific images.
Gifted individuals have a greater capacity for empathy, to picture themselves in others’ shoes, and anticipate how others might feel, think, and respond in a situation. This tendency to over-empathise also contributes to the gifted individual’s sensory overload. Their capacity for empathy makes the sight of tortured animals and children extra painful. Their empathic nature places victims at risk of revolting
#sensory processing disorder#high iq#intellectually gifted#autism#asc#high functioning autism#misdiagnosis#spd#pz
8 notes
·
View notes