#cross-disciplinary studies
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text

The Observational Spectrum: From Empiricism to Embodiment in UAP Studies
The study of Unidentified Aerial Phenomena (UAP) stands at a critical juncture, confronting the complexities of merging diverse methodologies to comprehend a phenomenon that resists straightforward categorization. Recent scholarly discussions, notably Maya Owen's lecture and supplementary examinations of eyewitness testimony, scientific observation, and embodied experiences in UAP research, underscore the imperative of an interdisciplinary approach. This necessitates a nuanced exploration of the disciplinary divide, the pivotal role of embodied experiences, and the transformative potential of bridging methodologies to enhance our understanding of UAP.
The dichotomy between "nuts and bolts" (emphasizing physical evidence and material issues, grounded in hard sciences) and "embodied" (encompassing experiential, spiritual, and religious aspects, aligning with social sciences and humanities) approaches in UAP studies poses a significant challenge. While empirical validation is crucial, overlooking the profound personal and existential implications of UAP encounters can result in an incomplete understanding. Conversely, an "embodied" focus, without scientific rigor, risks lacking credibility. This dichotomy is not insurmountable; rather, it presents an opportunity for scholarly innovation.
Embodied experiences are indispensable in UAP research, offering first-hand accounts that can inform scientific investigation and highlighting the complex, often transformative, nature of UAP encounters. The integration of these experiences challenges traditional methodologies, necessitating an adaptation that accommodates subjective, yet potentially revelatory, aspects of human experience. Concepts like "Uncanny Science" and "Flip" provide a theoretical framework for reconciling the scientific with the experiential, suggesting that the intersection of science and spirituality can be a fertile ground for understanding UAP. This reconciliation is not about diminishing scientific rigor but about enhancing it with the depth and complexity of human experience.
A holistic approach to UAP studies, one that synergistically combines the empirical with the experiential, is the most promising path forward. This can be facilitated through the adoption of frameworks like Cyborg Anthropology, which recognizes the interplay between human experiencers, technology, and the sensory extensions afforded by instruments. Moreover, the development of standardized methodologies for collecting and analyzing experiential data can significantly enhance the credibility and utility of embodied accounts in scientific research. Encouraging cross-disciplinary dialogue and collaboration is equally crucial, fostering a more comprehensive understanding of UAP that addresses both its material and experiential dimensions.
The study of UAP is poised to redefine the boundaries of scientific inquiry and our understanding of human experience. By embracing an interdisciplinary approach that values empirical evidence, embodied experiences, and the transformative potential of their integration, UAP research can transcend current disciplinary limitations. This integration promises not only a deeper grasp of UAP phenomena but also contributes to a broader shift in understanding the interconnectedness of human experience, technology, and the unknown, thereby enriching the scholarly landscape.
Maya Cowan: Observatories and Experiencers (The Society For UAP Studies, Annual Summer Conference 2024, Varieties and Trajectories of Contemporary UAP Studies, August 2024)
youtube
Sunday, February 9, 2025
#uap research#interdisciplinary approaches#science and spirituality#embodied experiences#phenomenology#scientific methodology#academic discourse#cross-disciplinary studies#human experience and perception#lecture#ai assisted writing#machine art#Youtube
0 notes
Note
There's a lot of things that point to neurodivergency not being a bunch of discrete conditions, but rather a range of symptoms that are given names based on how they affect other people. (But since this post is about autism and ADHD, I'm going to focus on those two.)
-
1 in 5 ADHD people are also diagnosed with autism. 1 in 3-5 ADHD people are also diagnosed with learning disabilities. Similar numbers for ADHD and mental disabilities or Tourette's. Personality disorders, mood disorders, and sleep disorders are also much more likely to be diagnosed.
Similar numbers exist for autism co-occurring with other neurodivergencies.
Being autistic/ADHD increases BOTH your chance of having kids that are autistic, AND kids that are ADHD. Doesn't matter which one you've been diagnosed with.
And most of the experiences that are central to the the ADHD or autistic experience are actually considered separate conditions likely to co-occur (''co-morbid'). Hyper/hyposensitivity, sensory processing disorders, emotional regulation problems, etc. are co-morbid with BOTH conditions.
Even the diagnostic criteria (things that get you a label) are frequently just different presentations of the same thing.
We've known autistic special interests and ADHD hyperfixations are the same thing for at least 20 years, now. Not being expressive 'enough' is stereotypical of autism, being 'too' expressive is stereotypical of ADHD, and both come from the exact same root. Trouble focusing affects eye contact and attention. Difficulties with social skills lead to talking 'too much' or 'too little', interrupting, difficulties forming and maintaining relationships, etc. Both groups stim, though ADHD people are likely to have it attributed to hyperactivity. Both experience meltdowns and shutdowns.
And both groups tend to end up masking and suffering burnout.
Many of the ways to support ADHD and autism are the same. Explicitly teaching social skills. Allowing stim tools. Finding ways to control stimulation levels and support emotional regulation.
-
There are reasons for having different diagnoses. ADHD meds don't help most autistics very much, for example. Even if the two conditions were combined, it would definitely have subtypes with distinct management plans. (Probably a lot more subtypes than we currently have!)
But the overlap of autistic and ADHD symptoms is way higher than in anything else I've studied. And, as an ADHD person with 6 of the 8 people closest to me being autistic (and 2 of them being ADHD), the overlap is way higher even than the literature suggests. From the outside, we look different. But we really really don't seem to be from the inside.
Would you be open to elaborating more on your statement “#Admittedly I fundamentally don’t believe that many forms of ADHD and many of the tumblr-acceptable forms of autism are materially distinct”? I haven’t heard someone else voice this sentiment, but I think I have similar feelings to you around this topic and I am curious how others have come to this conclusion as well.
Sure.
When I was eight years old, I was diagnosed with ADD—Attention Deficit Disorder. This is considered a related but separate and distinct thing from ADHD.
When I was a teenager, a new DSM came out. ADD was no longer considered a distinct thing. My diagnosis changed to ADHD-I: Attention Deficit Hyperactivity Disorder, Inattentive Type.
My brain didn’t change, but the professional perception of what was up with it did.
Is ADD materially different from ADHD? Can you have ADHD without hyperactivity? That used to be no, now it’s yes; answer the first question, that used to be yes, now it’s no.
I see very similar things between ADHD and autism. Lots of people do. Traits like the ability to fixate on an interest to the physical inability to pay attention to anything else; infodumping past the point other people lose interest; penchant for physical clumsiness and poor coordination; emotional dysregulation; proclivity to sensory overload; anxiety over not emoting correctly… they’re ADHD things and autism things. Is bouncing my leg an autism stim or an expression of ADHD hyperactivity? Or is it just fidgeting like people do sometimes? I dunno. Are they in fact materially different things?
Similar to ADD, Asperger’s Syndrome is no longer a thing. It’s subsumed under Autism Spectrum Disorder now. Is “high functioning” autism the same material thing as “low functioning” autism? Is “high functioning” autism the same thing as “ADD”? Idk. In some people I think it is.
Especially in mental disorders and neurodivergences, diagnoses aren't physical, material things. They're names given to commonly occurring collections of traits or symptoms. There's no virus that causes ADHD, no bacteria that can be isolated that causes autism. COVID is caused by the virus SARS-CoV-2; strep throat is caused by Streptococcus bacteria. They have symptoms, but they are primarily defined by their root cause. ADHD, autism, and plenty of other Brain Things do have neurochemical correlates - that is, there is an aspect of physical reality to them, you brain is wired a certain way - but it's not like ADHD is caused by the ADHD Virus and Autism is caused by the Autism Germ. They're names given to observable sets of traits, in order to figure out ways of treating and managing them. And I think drawing a sharp distinction between them - THIS is ADHD, and THIS is autism, and they're NOT THE SAME! - is pointless.
I like to use the xkcd color survey as an analogy for... well, a lot of things about the human experience and the way we classify it.
If you weren't around in 2010, xkcd's Randall Munroe asked the internet to help crowdsource the true names and boundaries of colors. You could sit down at the screen, colors would appear before you by random hexcode, and you typed in the name you'd call it. You could do this as many times with as many colors as you wanted. This was the resultant chart he made:
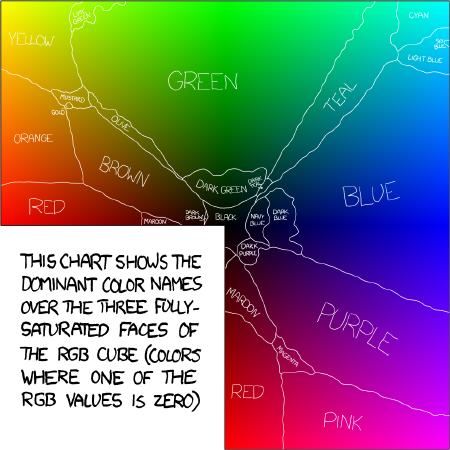
This shows the entirety of fully saturated RGB color space. Each pixel is a different hex code. Each pixel represents a different individual's brain.
I usually use this chart to talk about sexual orientation/queer identities. But it's also a great analogy for the categorizations being diagnoses.
If "Blue" is, say, ADHD, and "Purple" is Autism, you can image how one person's "purple" experience may be wildly different from another "purple" experience but very similar to a "blue" experience. But they're labelled differently, for various reasons. Maybe the doctor had recently seen a lot of blues, and this one seems more purple in comparison. Maybe the doctor has a really specific idea of what blue is, so this can't be blue, it must be purple. Which is not to say some blues aren't wildly different from some purples, that some purples match the platonic ideal image in your mind of what "purple" is more than others. There's still clearly a lot of overlap in blue and purple experiences.
That's kind of how I think about ADHD and autism.
And who knows, maybe I think this just because I am actually autistic. I've asked myself that, wondered that before. Am I? Or are these just ADHD symptoms that overlap? And honestly at this point the answer isn't super important to me. I know how my brain works and how to deal with it when it gets bad, and there's very little that pursuing a diagnosis would do for me at the point I'm at in my life.
But when I say that I suspect the two aren't as materially distinct as they're sometimes made out to be, this is what I mean.
#neurodivergence#autism#adhd#more cross-disciplinary studies of neurodivergence would help a LOT#many of my coping strategies for ADHD were developed while reading about bipolar and PTSD#but even just more studies that look at ADHD through an autistic framework and vice-versa#would help a lot
124 notes
·
View notes
Text
Reference saved in our archive (Daily updates!)
Far right defenses of 'freeze peach' keeping doctors from facing discipline for spreading medical misinformation.
Key Points Question How frequently do medical boards discipline physicians for spreading medical misinformation relative to discipline for other professional misconduct?
Findings In this cross-sectional study of 3128 medical board disciplinary proceedings involving physicians, spreading misinformation to the community was the least common reason for medical board discipline (<1% of all identified offenses). Patient-directed misinformation and inappropriate advertising or patient solicitation were tied as the third least common reasons (<1%); misinformation conduct was exponentially less common than other reasons for discipline, such as physician negligence (29%).
Meaning Extremely low rates of disciplinary activity for misinformation conduct were observed in this study despite increased salience and medical board warnings since the start of the COVID-19 pandemic about the dangers of physicians spreading falsehoods; these findings suggest a serious disconnect between regulatory guidance and enforcement and call into question the suitability of licensure regulation for combatting physician-spread misinformation.
Abstract Importance False medical information disseminated dangerously during the COVID-19 pandemic, with certain physicians playing a surprisingly prominent role. Medical boards engendered widespread criticism for not imposing forceful sanctions, but considerable uncertainty remains about how the professional licensure system regulates physician-spread misinformation.
Objective To compare the level of professional discipline of physicians for spreading medical misinformation relative to discipline for other offenses.
Design, Setting, and Participants This cross-sectional study analyzed and coded publicly reported medical board disciplinary actions in the 5 most populous US states. The analysis included data from January 1, 2020, through May 30, 2023, for California, Florida, New York, and Pennsylvania and from January 1, 2020, through March 30, 2022, for Texas.
Main Outcomes and Measures Medical board disciplinary proceedings that resulted in some form of sanction were analyzed. Codes were assigned for the different types of offenses relied on by medical boards for imposing physician discipline.
Results Among 3128 medical board disciplinary proceedings in the 5 most populous states, spreading misinformation to the community was the least common reason for medical board discipline of physicians (6 [0.1%] of all identified offenses). Two reasons tied for third least common: patient-directed misinformation (21 [0.3%]) and inappropriate advertising or patient solicitation (21 [0.3%]). The frequency of misinformation conduct was exponentially lower than more common reasons for discipline, such as physician negligence (1911 [28.7%]), problematic record-keeping (990 [14.9%]), and inappropriate prescribing (901 [13.5%]). Patient-directed misinformation provided a basis for discipline 3 times as often as spreading misinformation to the community. The frequency of disciplinary actions for any reasons related to COVID-19 care, even if not about misinformation, was also quite low (10 [0.2%]). Sanctions in misinformation actions tended to be relatively light.
Conclusions and Relevance The frequency of discipline for physician-spread misinformation observed in this cross-sectional study was quite low despite increased salience and medical board warnings since the start of the COVID-19 pandemic about the dangers of physicians spreading falsehoods. These findings suggest that there is a serious disconnect between regulatory guidance and enforcement and that medical boards relied on spreading misinformation to patients as a reason for discipline 3 times more frequently than disseminating falsehoods to the public. These results shed light on important policy concerns about professional licensure, including why, under current patient-centered frameworks, this form of regulation may be particularly ill-suited to address medical misinformation.
#mask up#pandemic#wear a mask#public health#covid#covid 19#wear a respirator#coronavirus#still coviding#sars cov 2
41 notes
·
View notes
Text
absolutely insane, out of pocket WIP that no one asked for that's not in my usual tense OR style, but I needed to exorcise it, under the cut
Ummm slight NSFW? Religious themes ? Dub-con? Age gap? Canon-divergence AU for the explicit purposes of (eventual if I continue this) smut ?? Under-age (female reader is a high-schooler of unspecified age, probably 17 ?? almost legal but not? idfk)
I've never written anything in the reader-insert or present tense ballpark. I have no business doing this. Anyway here's some of it! xoxo
Heels click the tile in brisk approach, luring his attentions to Mrs. Grady, an attendant of the main office, with you in toe. The rubber soles of your mary janes fall silent in your step, though your head is held high behind her, assured with the saunter of your hips. You're but a girl, though your walk is a womans. You carry yourself with the oversized confidence of a fatale. One who looks into his tired eyes and wary posture and sees herself staring back, wicked and red. A devil. His devil.
You come upon him like you know it all. Wiser than your years, lethal in your innocence feigned. You fix yourself to Mrs. Grady's shadow as if the position offers you to him meek, but your posture holds to a maturity that betrays you.
Father Brennan straightens with an amicable smile in greeting. Mrs. Grady returns it, though the quirk of her lips raises and falls so fast it's almost missed. Her skirts hem modestly swishes below the knee, three inches below to be exact. Three to four inches or so longer than yours had often been. Your waist band rolled twice to achieve the shortened length. An act of rebellion, a stab at the salacious you pretend yourself heedless of. Too pure to be deliberate.
The stunt with the skirt has landed you in the main office many times. Only until recently, when they turned to him for disciplinary action.
Their sole priest. One of but a few male staff members. They came to him at their wits end, and suddenly, you behaved. So mild and pious, suspicious with how quick you bent the knee. Confirmation he loathed.
Yet here you were, dragged before him once again. The same long walk to his domain, after school hours, when your studies wouldn't be interfered.
Not a walk of shame, but a strut.
︶⊹︶︶୨୧︶︶⊹︶
"What's been troubling you, my child?
He doesn't recall when my began to precede child, but he notes the way you're alight with covetous pride, and it beams up at him through the white of your smile, and glint in your eye. He basks in it with rueful conflict, one whose favor tips the scale in disappointment, both in himself, and you. Or at least he tries to tell himself that, shift part of the blame.
He sits on the edge of his desk before you, a bold maneuver, a vulnerability, but one he subjects himself to willingly. A deliberate ploy to show he can. To assert you have no hold over him, a display of his strength, his determination. Lofty and unaffected by your wiles.
Wiles you somehow seem unaware of even as you wield them; in your blushed cheeks and gaped lips, sighing his name minty fresh and bubblegum sweet, from the chewing gum you sneak, and the tinted lip balm that has sent you to his office more times than he can count.
A little silver crucifix collars your neck, dainty and simple, it signals your virtue, brands you as one of his own. He finds himself captured by it, dangling from your throat.
"What has you acting out so?"
He observes with the same raw anguish settling in his gut like a brick with how you sit before him. Your leg crossed, one over the other. Foot bobbing from a small ankle, restless and blurring. Your kilt slides back over your leg, hinting bare thigh above the thin green cotton of your knee-high.
The girls of St. Marys are supposed to sit straight back, hands clasped and ankles crossed. Demure, innocent, juvenile. You've been told not to sit the way you do, as if the correction itself scolds you for the impurity of which he fears you implicit. The way you are now. Alone in his office. Looking up at him.
He wonders if he shouldn't correct it again himself, but thinks better of it.
Weakness. He thinks. He chants. He affirms.
Baseless, primal, profane. He shouldn't pay any mind to how you sit. Like a woman.
You sigh, long-suffering, and troubled. Pouty lips and pleading eyes. Your lashes flutter, jet black and spindly with mascara applied so light it might go unnoticed. It doesn't.
Weakness.
Red flares within him, pointed, sleek. Igniting with a spark that fizzles and fades to gooey pink, soft and tender. And then golden again. Reverential. The sun setting on a dismissed mass. The aftermath of grace and due deference to his person leaving him hazy and contented. A school of faculty and students alike who adore him. Without them he's left to the sobering of an empty chapel, one whose light then shuns him. Daring him to continue to fester with the new, hungry monstrosity that swells and stiffens, ugly and blunt.
Heavy on his shoulders, digging at his back. A cross to bear, he drags it along his pilgrimage to the hill, where he will stake it in the ground, climb to its center, and crucify himself on the broad tines. And you're both the hammer and the nail. Sharp and unforgiving. A pierce of his flesh that damns his rotten soul. A giggle through his left hand, a sigh through his right, and kiss through both feet. He takes the pain and bleeds. He bleeds for you.
Weakness.
"I don't know, Father." You surrender, fingers picking the pleated hem of your skirt at your knee. A budding chest rising and falling beneath your buttoned blouse. His molars crack as he clenches his jaw firm. "I don't feel like I'm supposed to be here. I don't feel like I do any of this right."
His brows bow and his eye droops. Frosted brilliance chilled in pity. How wistful and lost his little lamb bleats.
"Do what right?" His voice is old and hoarse, and it catches in his throat. He hopes you think its breaks from disuse. From solidifying, stoic and cold in his lonely office, his clearing throat and crisp strokes of pen all that keeps him company there.
And not because of the way you take your bottom lip between your teeth.
"Belong." You reply, plain and real. So ahead of your years, and the vapid nuance that fill the heads of your classmates. Boys and lunches and status. He sighs, his smile so thin it disperses imperceptible in the deep lines that etch his face.
"We all belong, lass." He lilts around the pet names, feeling one weight lift in place of the new.
His vow of celibacy is a mutt gone rabid, and you're the child unawares, as you pull his ear and yank his tail, pushing at the warning ripple of jowl to get at his canines. Slick and yellowed by marrow, the memory of it's taste a perpetual haunt from the decades since it last soaked his tongue.
You're no Jezebel.
He almost sinks to his knees and sobs in relief. You're wayward. Wayward he knows. Wayward he can curve, he can herd, he can appease. And all without so much as a scuff to his shining piety. His stirred faith settles. Balls back up tidy, and tamed.
"You speak of nothing the Lord cannot quell." He eases himself into this routine, to the familiarity in advice he's since taken to using as a shield against your temptation. Or a muzzle to his own. "You need not but turn to him."
His suggestion is reasonable. One any good mentor, or spiritual counselor, should provide. You shake your head before his graveled words have the chance to settle.
"I try." Your insistence is earnest, as is your defeat. It strengthens his pity. "He doesn't listen to me. He never responds."
"My girl, of course he listens." You remain unconvinced. He sees it in your furrowed brow, and pout. "Come, I'll show you." He holds both of his palms out and open to you, thick and creased and stable. "We'll talk to him together."
#trying to mimic the beautiful insane unobtainable styles of my cooler older siblings jainydoe emmg and aldisobey tbh to be honest#i dont know okay I DONT#just gonna drop this and run#i dont even know how to tag this ???#ralph ineson x reader#the omen fanfic#the first omen#the first omen fanfic#father brennan#father brennan x reader#father brennan fanfic#x reader#reader insert#reader fic#reader smut
23 notes
·
View notes
Text
Xylella fastidiosa, the deadly disease-causing bacterium that has already wiped out millions of plants of emblematic Mediterranean crops, like grapevines, olive-trees and almond-trees, by clogging their ducts and plant tissues, will get a boost from climate change in relevant wine-producing regions where the risk is low at present. Researchers at the Institute of Cross-disciplinary Physics and Complex Systems (IFISC), a joint center of the Spanish National Research Council (CSIC) and the University of the Balearic Islands (UIB), have developed a new technique to characterize the risk of establishment of Pierce's Disease, and using state-of-the-art climatic data, have obtained predictions about the future expansion of the disease under different scenarios posed by global warming. Researchers from the Institute of Physics of Cantabria (IFCA), a joint center of the CSIC and the University of Cantabria, have collaborated in the work.
Continue Reading.
60 notes
·
View notes
Text
cross disciplinary training in gubat banwa

so, GUBAT BANWA is a big martial arts game of esoteric martial arts. of beatdown and bone breaking. bakbakan at suntukan, pangamot ug pagdaug. it focuses on martial arts and the culture that surrounds that. during ancient seasian times (the main foundation for this game), formal categorized schools didn't exist: participating in your culture was you learning its martial arts, or a random hermit in the sea cave could teach you a secret martial art, or your family could have its own secret martial art, etc. etc.

so martial arts classes (in gubat banwa they're called Disciplines) are expressions of culture and tradition. from a mechanical side, I knew I wanted to make Gubat Banwa a multiclassing-first game, a la Lancer, for multiple reasons
I like multiclassing, I almost always multiclass
You get access to more of the game and the game's lore (much of Gubat Banwa's lore is in the disciplines)
You get to write a plurality of classes that deal with a plurality of playstyles
It makes writing Disciplines easier--they become small packages of power instead of the long Narrative Playbooks that they are a la D&D 4e's classes. this also makes making Disciplines easier as you don't have to write one for a 12 Level long progression
it creates a more emergent character progression (a Mangangayaw learning Sword Saint techniques for example might be a raider who raided a Virbanwenyo settlement and got the resident martial artist to teach him a thing or two, or it could be that they started picking up how Virbanwenyo Penitents fought)
however, Disciplines were more than just classes, they're also martial arts in their own right. So as I deepened my understanding with the Martial Arts I also found further justifications for multiclassing [which we like to call crosstraining]). these are from my and GB's Art Director Dylan's experiences from Filipino Martial Arts:
to become a true grandmaster is to learn or observe a large variety of styles (see: Johnny Chiuten, Anciong Bacon, etc.)
most real grandmasters that began their own FMA schools are those that studied and learned techniques from a wide variety of martial arts (Anciong Bacon knew Boxing and Dumog, for example. Johnny Chiuten knew multiple Chinese Martial Arts and trained in Balintawak and Lapunti, GM Filemon Caburnay learned both the arts of blacksmithing and of multiple arnis styles as he traveled across Visayas and Mindanao, and learned Kung Fu from Johnny Chiuten, before going down the path of perfecting his own fighting style that became Lapunti Arnis de Abanico)
even my own master in Lapunti who started with Lapunti was exposed to other Arnis and Martial Art styles so he was able to build his own style around it, and was able to contribute his own moves into modern Lapunti. i can see a bit of Chinese Martial Art influence in his movements now, a bunch of balintawak progression
very often if you're a student of violence, you will be learning multiple combat arts both out of necessity and out of love for movement. a balintawak warrior might have their movements augmented with jiujitsu training, a lapunti could benefit from learning sikaran, etc. etc.
kadungganan are meant to be nascent grandmasters, especially those that reach legend 12, so this is the main justification for the multiclassing instead of just having 1 martial art that you perfect. in real life this doesn't really happen, especially if you want to perfect your own fighting style. the assemblage of multiple techniques from 12 Legends worth of progression is there to facilitate the fantasy of a Kadungganan perfecting their martial art style, like the grandmasters of old

i knew since the earliest stages of gubat banwa that i wasn't going to compromise the multiclassing aspect, i just find it very serendipitous that crosstraining fits so well into the martial arts fantasy. it makes me pretty satisfied and happy, and i'm glad i didn't bend to internal talking and thinking about making a "pure discipline" progression possible
132 notes
·
View notes
Text
An excerpt from Dunamantic Transmutation and Transmutative Dunamancy: A Cross-Disciplinary Chronicle (Iothe Bramblebrush, 955 PD), made available to affiliates of the Wynandir Society for Transmutative Studies as part of marketing materials for Coastal Academic Presses.
here we are, the most questionable use of my academic training to date, the wizard historiography fic! this is going to appeal to approximately two people and that's an optimistic estimate. it's a shameless indulgence of my own love for worldbuilding. it's also a gift to myself for submitting my final phd dissertation today.
shoutout to @essektheylyss for posting about "joan in the garden" that one time and absolutely jumpstarting my brain for this madness, the concept of which i've been sitting on since at least last august.
shoutout also to the incredible folks at @encyclopediacr for enabling me to do unnecessarily detailed research! you are legitimately more thorough than some of my real academic sources.
speaking of sources, i do have a half-completed bibliography for this "chapter," so let me know if i should finish and post that...
#critical role#mighty nein#cr2#caleb widogast#essek thelyss#shadowgast#i'm in my tolkien era. merely the translator for an in-universe author
45 notes
·
View notes
Text
Hahahaha, always funny to hear near start of semester.
No, the battle studies major includes almost no battling. It's a cross disciplinary history, social studies, and pre-veterinary degree. Did you seriously think you could get a degree in "battling good"?
15 notes
·
View notes
Text
The suspended Columbia University student that proclaimed “Zionists don’t deserve to live” stood by his incendiary remarks Tuesday after an anti-Israel campus group walked back an apology it offered over the shocking statement last school year.
Khymani James made clear he doesn’t regret spewing the hateful declaration before he was banished from the Ivy League school amid disruptive protests critical of Israel following the Oct. 7 Hamas terror attack.
“I will not allow anyone to shame me for my politics,” he tweeted on Tuesday. “Anything I said, I meant it.”
During a January disciplinary hearing with the university that he livestreamed and blasted on social media, James said that “Zionists don’t deserve to live comfortably, let alone Zionists don’t deserve to live.”
“Be grateful that I’m not just going out and murdering Zionists,” James added. “I’ve never hurt anyone in my life, and I hope to keep it that way.”
The videotaped remarks reemerged in April as anti-Israel protests intensified on campus. Columbia University Apartheid Divest, a student group of which James was a member, then posted a statement that read “Khymani’s words in January do not reflect his view, our values, nor the encampment’s community agreements,” the New York Times reported at the time.
But the anti-Israel organization apologized in an Instagram post Tuesday, stating the previous mea culpa “does not reflect Khymani or CUAD’s values or political lines.”
The group also said while the statement appeared to be on behalf of James, he had no involvement in it.
“We caused irrevocable harm to you by contributing to the ostracization you experienced from your fellow students, fellow organizers, the media, and the public,” the group posted online while stating James faced anti-blackness and queerphobia in the aftermath.
“By issuing a so-called ‘apology,’ CUAD exposed Khymani to even more hatred from white supremacist and queerphobic liberals and fascists, along with the neo-liberal media.”
In the same social media post where James stood by his repulsive remark, he thanked the group for setting “the record straight once and for all.”
The reversal from CUAD, which is made up of dozens of student organizations, incensed Jewish students that attend the university.
“They’re telling me very explicitly that I, as an Israeli, as a Zionist, and as a Jew have no right to live, much less study at the same institution as them,” PhD student Alon Levin told The Post.
“The justification of the desire to murder Zionists and the support for US designated foreign terrorist organizations by CUAD is entirely unsurprising because it’s nothing new,” said undergrad student Eden Yadega, who is part of Students Supporting Israel.
“The question is, why does Columbia still tolerate it? What line will these students have to cross before Columbia takes action?”
A Columbia spokesperson stressed it condemns any comments calling for violence.
“Statements advocating for violence or harm are antithetical to the core principles upon which this institution was founded,” the spokesperson said. “Calls for violence have no place at Columbia or any university.”
James filed a lawsuit against the school last month, arguing he was denied proper protocol when he was suspended in April.
James was actively involved in the anti-Israel encampment protest that took over Columbia starting in early April. ____________________________________
>James faced anti-blackness and queerphobia in the aftermath
poor thing can dish it out but can't take it then I guess,
#nunyas news#James faced anti-blackness and queerphobia in the aftermath#getting a serving of what you dished out back then#poor baby
10 notes
·
View notes
Text
Interesting study. And a great example of cross-disciplinary study.
8 notes
·
View notes
Text
Hirano to Kagiura light novel translation 4-1
Chapter 4: Fall.
Part 1
Prev || Next

It might be September by now, but the sun’s rays know no bounds.
Heat from the weather aside, the schoolhouse on the coattails of summer break is permeated with the fervor of the students.
Among all those in the athletic clubs who have undergone away games and training camps, there are many who have deepened both their tans and their virility. The sense of achievement characteristic of those who kept up with their exercise lives within their growth spurts.
Hirano’s roommate is, once again, one of them.
Kagiura, who’s gotten a bit taller, has gotten used to high school, completely devoid of the anxiety he’d seemed to have around the time he’d started school.
Since they’d met up over the summer, he’s become more and more relaxed, and Hirano can’t help but think of him as a beloved younger brother.
Wait, but younger brothers don’t do things like give you earrings, do they?
Hirano isn’t really in a position to judge, with no siblings of his own.
He’d found his original earrings while organizing his luggage after returning from Kagiura’s countryside home. They’d fallen into his school bag and hidden themselves beneath the stiff bottom plate.
What should I do about it? he’d wondered, but figured well, whatever, and didn’t bother switching out his new ones. He’ll keep them in the dorm just in case, but ultimately plans to keep using the ones Kagiura gave him.
As soon as the new term starts, preparations for the Cultural Festival are full speed ahead. Even the first years, who aren’t used to running events without the guidance of a faculty member, are gradually gaining opportunities to build character. The Executive Committee members have so many responsibilities that it has become difficult to carry out their studies without the cooperation of their classmates.
Kagiura also has the situation of being part of the ‘Sports Recommendation Squad’, and his grades are not up to snuff. It would be good if they don’t take a hit from his extracurricular responsibilities, but that will come down to his own efforts.
It’s not just the Executive Committee members who are swamped. The students in the culture clubs are also at their busiest, and with the autumn tournament right around the corner, there’s no way the athletics clubs can cut back on practices.
The sweltering nights have yet to abate; yet despite these conditions which could even be called cruel, most of the students are eagerly awaiting the Cultural Festival. You might even get away with saying all of them.
Because, after all, girls come to visit the cultural festival.
And even without that element, a festival is still a festival.
This is a time when the whole student body is restless, so the Disciplinary Committee will be on top of keeping everyone in line—or such is their public stance, but they won’t be too strict about moderating uniforms and hair styles.
In any case, a high proportion of the students will be in costumes on the day of the festival.
There's also at least one class cross-dressing every year.
This year, that’s right, it's the class that Hirano is unfortunately a part of. More specifically, it's been decided that Hirano will be one of the ones in drag.
Oiwa-san—a famous spirit who makes an appearance in the Yotsuya Kaidan.¹
There are many variations of the famous ghost story, in which Oiwa, the deceased wife, holding a grudge over the betrayal of her husband, Iemon, slaughters every last person involved. Apparently, they will be basing the makeup off of Tōkaidō Yotsuya Kaidan², which is popular among Hirano’s classmates.
He’d been shown reference images of the ghost, her face half disfigured and inflamed by poison, but the picture was nightmare fuel when viewed in the dark.
Supposedly it’s a style of Halloween makeup that’s been popular in recent years, but the trial makeup that had been applied to his arm after school in order to match the shade to his face had been truly grotesque.
This information is to be kept top secret until the last possible minute on the day of, in the interests of building hype.
While Hirano is putting away his homework, the door opens with a click.
His roommate is home.
It’s still bright outside, but the dining hall is just about to open for dinner.
“Hirano-san, I’m home!”
“Welcome home, Kagi-kun.”
These days, Kagiura usually gets a bit bashful in reply to Hirano’s greeting, seemingly tickled. So naive and innocent he must be, making such an expression with no fear of being misunderstood.
There were days they’d spent together, but summer vacation had been long.
There’s an air of a different kind of newness from the one there’d been in the period before they’d gotten used to sharing a dorm—Kagiura probably feels it too. At least, Hirano thinks so.
He feels closer to Kagiura compared to before. After all, he’s met his immediate and extended family, so of course they’d feel more intimate. It’s as if the part of himself that had been on guard while thinking about how to act as a senpai in his second year in the dorms has been absolved.
After Hirano had filled out his print-outs as if in competition with Kagiura, who’d spread out his homework in a frenzy, they’d headed to the dining hall a little later than usual.
It always takes him about 3 or 4 days to get back into the swing of dorm life.
Speaking of which, he thinks.
Before Kagiura moved into the dorms, Hirano had been quite nervous.
He’d talked to Hanzawa about it one time when the Disciplinary Committee had a meeting, and they’d brainstormed strategies to avoid scaring Kagiura off.
He’d also felt it would be a waste of his efforts if he was only friendly at the beginning of their time spent living together; thus, they’d come to the conclusion that it wouldn’t be too far out of Hirano’s depths to give him a nickname and use “-kun”.
Oh yeah, that’s right. At the beginning I called him Kagiura-kun.
He’s been calling his name every day, enough that he’d ended up shortening it, thinking it’s too long and clunky.
Kagiura has morning practice tomorrow, too, so there's no way he can let him oversleep.
Hirano got that, but there was something on his mind that just wouldn’t go away, so he asked before shutting off the lights.
".....Hey, um. I know you're working hard, so I don't wanna rain on your parade, but are your studies going all right? I haven't heard how your proficiency test went yet."
As the words leave his mouth, he thinks, what am I, a private tutor? and laughs drily to himself.
For the results of the test held right after summer break, a list ranking every student in their grade and the standard score were passed out to each person, the same as for the periodic exams.
For first years, they can be used as nothing more than a reference, but due to the breadth of the material covered, in some cases they might be used to determine which schools to apply to when compared to results from previous cram schools.
“...I just barely passed.”
“What’s the damage?”
“The teacher said, ‘You didn’t do badly enough that I need to pull you aside, but keep working hard’...”
“I see.”
Which is bad in and of itself, really.
Kagiura hangs his head dejectedly, and Hirano’s tempted to comfort him all the more for having seen the extent of his efforts, but his lack of preparation is unmistakable.
“Kagi-kun, after the cultural festival is over, you gotta step it up. If you miss some of the notes, get someone to show you theirs before the next day. Don’t let them build up. If you end up with a backlog of notes to take, you’re not gonna be able to understand them.”
Hirano knows deep down he’s probably worrying too much, but he keeps the expression on his face stern. The beginning is the key to everything. Among his classmates in the ‘Sports Recommendation Squad’ who, like Kagiura, are bad students, there are many whose grades plummeted after going on to their second year.
Who knew he’d become this much of a worrywort after becoming someone’s senpai?
“Yeah…Hirano-san, will you teach me again?”
“Sure. But you better bring back good grades.”
“I will! …By the way, can I ask you something?”
He ducks his head as he asks the question, a gesture with all the charm one would expect from someone as cute as him.
“What’s up?”
“When you were a first year, did the senpai you roomed with teach you how to study, too?”
“Nah, no way.”
“Hm…did you not get along?”
“It’s not that we didn’t get along, we just weren’t really that close. I wasn’t nearly as friendly a kouhai as you are.”
This is usually the case for dorm students. Hanzawa, contemptuous of homosexual relations, has a reputation in certain circles for having a finely-tuned gaydar and showing up to cockblock any time he senses anyone getting a little too close.³
His distaste isn’t unwarranted; apparently it has to do with his family, so even Hirano feels bad for him.
“...Does that make me special, then?”
“Why are you so happy about that?”
At Hirano’s jests of what are you, a dog? Kagiura breaks into a grin.
“Yeah. You know, I’m glad I’m your roommate, Hirano-san.”
Hirano smiles wryly; Kagiura’s got him wrapped around his little finger without a hint of insincerity.
With Kagiura cozying up to him like this, he doesn’t stand a chance.
*****
T/N: (1) Not sure I need to add more info on this to the story, but it's pretty interesting, so you can read more about it here.
(2) A movie based on the story made in 1959.
(3) Yall....idek what to say about this. I tried to keep the tone lighthearted but the original text literally says 'gay-hating Hanzawa' and describes his feelings as disgust. Idk why the writer put this but our boy is NOT like that 😭 I actually broke my vow of not looking at the official TL just to see how they handled this bit and they completely watered it down lmao. and tbh, yall know my dedication to accuracy but I WAS TEMPTED. While going back and forth about what I should do, I told my sister about it, and she suggested that Hanzawa doesn't actually hate gays, he just hates gay sex and will stand for none of it in his dorm so...we're going with that interpretation 💀🙃💀🙃
Prev || Next
Special shoutout to @jeizet, @jujupanic, @massyworld, @umbreonwolfy, and @acidsuzanne-blog for sponsoring these updates 🙌
#you guys can reblog these posts btw <3#remember likes are great but they don't do anything to spread the posts around!#friendly reminder that tumblr is not ig/tt and we love her for it <3#re 3rd footnote: im still trying to cope#im really hoping that the 'homophobic' and 'disgust' etc are referring to his reputation rather than his real feelings#tho i'm not sure that's much better 💀#also im sorry but wtf is up with the whole 'its to do with his family so hirano feels bad for him thing'#like??? oh poor you your sibling is gay that must be such a struggle#guess you have the right to hate gay people. ??????#this makes it sound like there was some TRAUMA involved#but it was literally just his brother (and other sibling) saying btw im gay and then they all moved on with their lives??#shoutout to my sister for this slightly inaccurate but much better take#i told her about it and she was like 'nah this mf just repressed as hell 💀'#she does not read ssmy/kghr btw#hirano to kagiura#hirano and kagiura#kagihira#hirano to kagiura light novel#hirano to kagiura translation#harusono shou
136 notes
·
View notes
Text
BBMCT: Embark on Medical Research at AIIMS Hospital
Clinical research plays a pivotal role in advancing medical science, improving patient care, and bringing innovative therapies to market. British Biomedicine Clinical Trials (BBMCT) at AIIMS Hospital offers an invaluable opportunity to be part of groundbreaking research in the healthcare field. Known for its prestigious reputation, robust facilities, and ethical approach, BBMCT is a trusted partner for clinical trials. In this blog, we will explore how BBMCT at AIIMS Hospital is revolutionizing medical research with its world-class resources, experienced researchers, and ethical commitment.
## Prestigious Institution for Clinical Research
AIIMS Hospital, India’s premier medical institution, has long been recognized as a leader in clinical research. Established in 1956, AIIMS has become synonymous with high-quality healthcare and research excellence. BBMCT leverages this prestigious legacy, offering researchers and patients access to a facility that is both globally recognized and locally impactful.
The institution is renowned for its research in diverse medical fields, ranging from oncology to neurology, pediatrics to cardiology. Its affiliation with the government ensures significant funding and support for clinical research, making it an ideal setting for conducting advanced trials. Whether for early-phase studies or large-scale trials, BBMCT provides a dependable platform for research excellence.
## Access to a Varied Patient Demographic
One of the key advantages of conducting clinical trials at AIIMS Hospital is the institution’s access to a wide and varied patient demographic. Located in the heart of India’s capital, AIIMS draws patients from across the country and beyond. This diverse population provides invaluable insights into how treatments and therapies work across different genetic backgrounds, socioeconomic statuses, and health conditions.
BBMCT at AIIMS can effectively conduct research across a wide range of diseases, ensuring that clinical trial data is comprehensive, robust, and reflective of global health trends. Researchers can rely on this broad patient base for better generalizability of trial outcomes, making their findings highly applicable to diverse patient populations.
## Cutting-Edge Research Facilities at Your Disposal
AIIMS Hospital is equipped with state-of-the-art research facilities that are at the forefront of medical innovation. From advanced diagnostic laboratories to high-tech imaging centers, BBMCT at AIIMS ensures that clinical trials are conducted under the best possible conditions. The hospital’s cutting-edge infrastructure includes sophisticated equipment for monitoring patient responses, analyzing data, and providing precise outcomes.
AIIMS also hosts specialized centers of excellence in areas like cancer research, cardiology, and neurosciences, ensuring that BBMCT has access to the latest research tools and methodologies. This focus on high-quality facilities provides a solid foundation for successful clinical trials, enabling researchers to make well-informed, evidence-based conclusions.
## Knowledgeable Researchers Deliver Reliable Outcomes
At the heart of every successful clinical trial is a team of knowledgeable and skilled researchers. BBMCT at AIIMS benefits from a team of experienced professionals who are experts in their respective fields. The institution attracts top-tier medical practitioners, scientists, and researchers who are committed to pushing the boundaries of medical knowledge.
AIIMS Hospital fosters a collaborative environment, encouraging cross-disciplinary research that ensures comprehensive, reliable outcomes. Researchers are well-versed in both the scientific and regulatory aspects of clinical trials, allowing them to design and execute studies that meet international standards while producing valid, reproducible results. This expertise significantly enhances the credibility of trials conducted under BBMCT.
## Firm Commitment to Ethical Research Standards
BBMCT at AIIMS Hospital places a strong emphasis on ethical standards in clinical research. The institution is committed to ensuring that patient rights, safety, and well-being are prioritized at all times. Strict adherence to ethical guidelines is ensured through institutional review boards (IRBs), regular audits, and continuous monitoring throughout the trial process.
The institution follows established ethical guidelines such as the Declaration of Helsinki and Good Clinical Practice (GCP), ensuring that trials meet international standards. By upholding these ethical standards, BBMCT builds trust with patients, researchers, and regulatory bodies, contributing to the reliability and legitimacy of the research conducted.
## Strong Support for Regulatory Compliance
Navigating the complex landscape of regulatory compliance is one of the critical components of conducting clinical research. BBMCT at AIIMS Hospital offers robust support in ensuring that all clinical trials comply with both Indian and international regulatory requirements. The research team is well-versed in guidelines set by regulatory bodies like the Drugs Controller General of India (DCGI) and the World Health Organization (WHO).
AIIMS Hospital’s research department has a dedicated team to assist in preparing, submitting, and reviewing clinical trial protocols to meet regulatory standards. This strong focus on compliance ensures that trials proceed smoothly without legal or procedural obstacles, fostering a trustworthy environment for all stakeholders involved.
## Efficient Management of Trial Execution
The execution of clinical trials requires careful planning, organization, and real-time management. BBMCT at AIIMS excels in the efficient management of trial execution, from recruitment to monitoring and reporting. The institution’s infrastructure, experienced staff, and technological tools help streamline trial processes, ensuring timelines are met and patient safety is maintained throughout.
BBMCT utilizes advanced project management software and patient monitoring tools to ensure trials are executed with precision. This attention to detail and structured management approach increases the likelihood of successful trial outcomes, providing timely and accurate data that can influence future medical practices and treatments.
## Established Success Record in Trials
BBMCT has built a solid track record of success in clinical trials over the years. With numerous trials completed successfully, the institution has gained recognition for its commitment to research excellence and its ability to deliver dependable results. This history of success has attracted global pharmaceutical companies, biotech firms, and research organizations to collaborate with BBMCT at AIIMS Hospital.
The success of BBMCT can be attributed to the institution’s rigorous trial methodologies, advanced technologies, and highly skilled teams. These factors combined have resulted in impactful clinical research, often leading to the development of new drugs, therapies, and medical procedures that improve patient outcomes globally.
/media/88de57a97f470a96a9071d7d2f030cba
## FAQs About BBMCT at AIIMS Hospital
**1. What makes BBMCT at AIIMS a trusted partner for clinical trials?**
BBMCT at AIIMS Hospital is trusted due to its prestigious standing, cutting-edge research facilities, and experienced team of researchers. The institution adheres to the highest ethical and regulatory standards, ensuring that trials are conducted safely and effectively. Its ability to recruit a diverse patient population further enhances the reliability and applicability of trial outcomes, making it a trusted partner for advanced clinical research.
**2. How does AIIMS Hospital support patient safety during clinical trials?**
AIIMS Hospital prioritizes patient safety through rigorous monitoring, ethical protocols, and regular audits by Institutional Review Boards (IRBs). Strict adherence to Good Clinical Practice (GCP) guidelines ensures that patient welfare is safeguarded throughout the trial process. Additionally, patients are fully informed about the potential risks and benefits before consenting to participate, ensuring that their rights are upheld.
**3. What regulatory bodies oversee clinical trials at BBMCT?**
Clinical trials conducted at BBMCT at AIIMS are overseen by several regulatory bodies, including the Drugs Controller General of India (DCGI) and the World Health Organization (WHO). These organizations set the framework for regulatory compliance and ensure that clinical trials meet international safety and ethical standards.
**4. What types of clinical trials are conducted at BBMCT?**
BBMCT at AIIMS conducts a wide range of clinical trials, including Phase I-IV studies in fields such as oncology, cardiology, neurology, and infectious diseases. The trials may involve testing new drugs, therapies, diagnostic methods, or medical devices, and can be designed to explore safety, efficacy, or the optimal dosage of treatments.
**5. Can international companies partner with BBMCT for clinical research?**
Yes, BBMCT at AIIMS welcomes partnerships with international pharmaceutical companies, biotech firms, and research organizations. The institution’s reputation for high-quality research, access to a diverse patient base, and advanced facilities make it an attractive partner for global clinical trials.
## Conclusion
British Biomedicine Clinical Trials (BBMCT) at AIIMS Hospital provides a unique and prestigious platform for conducting advanced clinical research. With its world-class research facilities, experienced teams, diverse patient base, and unwavering commitment to ethical practices, BBMCT is paving the way for the future of medical science. The institution’s strong regulatory compliance, efficient trial management, and successful track record make it a leading choice for both national and international clinical research partnerships. For those seeking to embark on medical research, BBMCT at AIIMS Hospital is undoubtedly the trusted partner for innovation and success in the healthcare industry.
Subscribe to BBMCLINICALTRIALS YouTube channel for Research Insights
Be sure to subscribe to the **BBMCLINICALTRIALS YouTube channel** for exclusive access to the latest updates and in-depth insights into British Biomedicine Clinical Trials (BBMCT). Stay informed on cutting-edge research, clinical trial advancements, patient safety protocols, and breakthrough therapies being tested at AIIMS Hospital. Our channel provides expert discussions, industry trends, and detailed videos on the clinical trial process across various therapeutic areas. Whether you’re a healthcare professional, researcher, or simply interested in biomedical innovation, subscribing will keep you at the forefront of clinical research developments. Don’t miss out — join our community today!
#artists on tumblr#anya mouthwashing#agatha harkness#batman#cats of tumblr#dan and phil#bucktommy#agatha all along#911 abc
4 notes
·
View notes
Text
Masks and respirators for prevention of respiratory infections: a state of the science review - Published May 22, 2024
SUMMARY
This narrative review and meta-analysis summarizes a broad evidence base on the benefits—and also the practicalities, disbenefits, harms and personal, sociocultural and environmental impacts—of masks and masking. Our synthesis of evidence from over 100 published reviews and selected primary studies, including re-analyzing contested meta-analyses of key clinical trials, produced seven key findings. First, there is strong and consistent evidence for airborne transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and other respiratory pathogens. Second, masks are, if correctly and consistently worn, effective in reducing transmission of respiratory diseases and show a dose-response effect. Third, respirators are significantly more effective than medical or cloth masks. Fourth, mask mandates are, overall, effective in reducing community transmission of respiratory pathogens. Fifth, masks are important sociocultural symbols; non-adherence to masking is sometimes linked to political and ideological beliefs and to widely circulated mis- or disinformation. Sixth, while there is much evidence that masks are not generally harmful to the general population, masking may be relatively contraindicated in individuals with certain medical conditions, who may require exemption. Furthermore, certain groups (notably D/deaf people) are disadvantaged when others are masked. Finally, there are risks to the environment from single-use masks and respirators. We propose an agenda for future research, including improved characterization of the situations in which masking should be recommended or mandated; attention to comfort and acceptability; generalized and disability-focused communication support in settings where masks are worn; and development and testing of novel materials and designs for improved filtration, breathability, and environmental impact.
SUMMARY AND CONCLUSION
This review was commissioned partly because of controversy around a Cochrane review which was interpreted by some people as providing definitive evidence that masks don’t work (9). Our extensive review of multiple streams of evidence from different disciplines and study designs builds on previous cross-disciplinary narrative reviews (233, 412) and aligns with the recent call from philosophers of science to shift from a “measurement framework” (which draws solely or mainly on RCTs) to an “argument framework” (which systematically synthesizes evidence from multiple designs including mechanistic and real-world evidence) (19). Using this approach, we have demonstrated a more nuanced set of conclusions, summarized below, and have revealed why certain inaccurate assumptions and defective reasoning about the science of masks and masking seem to have become widely accepted among certain groups.
We began by reviewing basic science evidence on the transmission of SARS-CoV-2 and other respiratory pathogens and showed that there is strong and consistent evidence that they spread predominantly by the airborne route. We also showed that masks are effective, and well-fitting respirators are highly effective, in reducing transmission of respiratory pathogens, and that these devices demonstrate a dose-response effect (the level of protection increases as adherence to masking increases).
We then provided a methodological critique of clinical trials of masks in the control of respiratory disease epidemics and outbreaks, including listing common design flaws. We summarized evidence from RCTs, including repeating methodologically flawed meta-analyses, and showed that respirators are significantly more effective than medical or cloth masks, especially (and to the extent that) they are actually worn in all potentially hazardous circumstances.
We also reviewed an extensive body of observational and modeling evidence which showed that, overall, masking and mask mandates are effective in reducing community transmission of respiratory diseases during periods of high community transmission. The observational findings are particularly striking since various inherent limitations of such designs are likely to bias findings toward the null.
Our review of adverse effects and harms of masks found strong evidence to refute claims by anti-mask groups that masks are dangerous to the general population. We also found that masking may be relatively contraindicated in individuals with certain medical conditions and that certain groups (notably D/deaf people) are disadvantaged when others are masked.
We summarized evidence from multiple countries and cultures which shows that masks are important sociocultural symbols about which people care deeply (positively or negatively). We also showed that adherence (and non-adherence) to masking is sometimes linked to political and ideological beliefs and to widely circulated mis- or disinformation, and hence hard to change.
In a section on mask policy, we described how governments and organizations need explicit policies on using masks for prevention and control of respiratory infections, covering personal protection of at-risk groups; protection in specific settings, including workplaces and healthcare facilities; seasonal respiratory infections; and pandemics. These policies need to be based on sound risk assessment, risk management, and implementation principles.
Finally, we reviewed environmental impacts from single-use masks and respirators and highlighted novel materials and designs with improved performance and less environmental risk.
We believe this evidence supports several important conclusions and implications for further research.
First, the claim that masks don’t work is demonstrably incorrect, and appears to be based on a combination of flawed assumptions, flawed meta-analysis methods, errors of reasoning, failure to understand (or refusal to acknowledge) mechanistic evidence, and limitations in critical appraisal and evidence synthesis. Masks and respirators work if and to the extent that they are well-designed (e.g., made of high-filtration materials), well-fitting and actually worn. The heterogeneity of available mask RCTs does not appear to have been fully understood by some researchers who have conducted high-profile meta-analyses of the same. It is time for the research community to move on from addressing the binary question “do masks work?” through unidisciplinary and epistemologically exclusionary study designs and pursue more nuanced and multi-faceted questions via interdisciplinary designs.
A fruitful avenue for future research, for example, would be the combination of experimental, observational and modeling data to refine our understanding of when universal masking should be introduced during respiratory epidemics and how best to promote and support masking policies in different situations and settings, and especially for groups at increased risk, during such outbreaks. Research on ventilation, filtration and other measures to improve indoor air quality was beyond the scope of this review [it has been covered elsewhere (330, 395)], but there is scope for cross-disciplinary modeling to bring the science of indoor air into more direct dialogue with that of infectious disease transmission and masking to address the question of when and in what circumstances indoor masking can be deemed unnecessary (or, alternatively, advised or mandated) based on air quality. As noted in Modeling Masking, some research groups have begun to contribute to this interdisciplinary knowledge base.
Second, given that masking is an effective (though not perfect) intervention for controlling the spread of respiratory infections, and that it may be particularly important in the early stages of pandemics (when the pathogen may be unknown and drugs and vaccines are not yet available), improving understanding among scientists, clinicians, policymakers and the public about the effectiveness of masks and respirators is an urgent priority. The continuing recalcitrance of many (though not all) in the infection prevention and control community on this issue could prove a major threat to public health in future pandemics, particularly since such individuals often hold influential positions on global and national public health decision-making bodies.
Third, mask policies should better reflect the actual risks and harms of masks rather than being overly influenced by speculative risks (such as retention of carbon dioxide) that have no empirical foundation, or by adverse effects affecting certain defined groups (e.g., some people with autism) which could be covered by exemptions. Rather, the focus should be on supporting effective mask use by addressing well-described and widely experienced adverse effects of masking such as communication difficulties, physical discomfort, and skin reactions. Communication is a vital human need, so communication resources and best practice guidelines should be integral to mask policy and operational in every setting where masking is required or advised. Physical adverse effects of masks should be addressed by better mask design, which should be a priority for research.
Fourth, there is scope for research centered on helping people find masks that they find comfortable, aesthetically appealing, and which fit them well. If masking is to be normalized in certain risk situations, there needs to be a range of masks and respirators available in different sizes, shapes, colors, and designs to take account of the many physical and sociocultural factors affecting uptake, fit, and use. This stream of research is especially important for people who are clinically vulnerable (e.g., immunosuppressed), who may need to mask much or all of the time and, in some cases, lifelong.
Fifth, research should continue into novel materials which could lead to masks with improved comfort, lower breathing resistance, and good quality reusable products which will greatly reduce waste and environmental pollution. Plastic-backed medical masks that are ill-fitting, uncomfortable, and made of non-biodegradable materials should be phased out and replaced with masks and respirators that meet a higher standard for filtration efficacy, breathability, fit, and environmental sustainability. Research should also be directed at maximizing options for recycling mask waste.
Finally, as the COVID-19 pandemic continues into a fifth (and, quite possibly, subsequent) year, the grave danger posed by ideologically driven anti-mask narratives to public and global health should be acknowledged and systematically addressed. Anti-mask sentiment is increasing, along with anti-vaccine sentiment (413), and this bodes ill for both the current and any future pandemics. While there are no simple solutions to the problem of widespread disinformation, clear and consistent messaging from public health bodies on masks and other mission-critical topics would help considerably.
#covid#covid 19#mask up#pandemic#coronavirus#public health#sars cov 2#wear a mask#still coviding#wear a respirator#masks work#masking#covid masks#covidー19#covid news#covid conscious#covid is airborne#covid isn't over#covid pandemic
15 notes
·
View notes
Text
By: Bernard Lane
Published: Apr 14, 2024
Nine of the 15 gender clinics in a landmark international survey for the Cass review have admitted they do not routinely collect outcome data on their young patients.
This survey, together with a new evaluation of treatment guidelines for gender dysphoria, gives unprecedented insights into the workings of gender clinics around the world offering puberty blockers and cross-sex hormones to minors.
In the 2022-23 survey, six clinics said they “routinely collected some outcome data”: one of these clinics gave no further detail; one noted the number of patients discontinuing treatment; another used measures of quality of life; two were taking part in cohort studies; and the sixth clinic repeated some baseline assessments. Nine clinics acknowledged “not routinely collecting outcome data.”
The report of the survey results1, published by researchers from the University of York earlier this month, identified clinics by country, not name. Of the clinics that took part, Australia and the Netherlands were prominent with five and four clinics respectively.
Poor data collection was central to the controversy over the London-based Tavistock youth gender clinic.
The Cass review had planned to run a data-linkage study—with help from adult gender clinics—to learn the outcomes of the Tavistock’s 9,000-odd former patients.
The missing long-term data would allow clinicians, young patients and parents to make informed decisions about treatment. The review said it was to be the largest study of its kind in the world.
However, six of the seven adult clinics refused to co-operate. One stated reason was that “the study outcomes focus on adverse health events, for which the clinics do not feel primarily responsible.”
Another adult clinic said, “The unintended outcome of the study is likely to be a high-profile national report that will be misinterpreted, misrepresented or actively used to harm patients and disrupt the work of practitioners across the gender dysphoria pathway.”
On April 12, however, The Times newspaper reported that the uncooperative adult clinics had “bowed to pressure to share [the] missing data”.
Mostly medical
In the York University international survey, ordered by the Cass review, all 15 youth gender clinics said they used a multi-disciplinary team, but researchers concluded there was a “paucity” of psychosocial therapy interventions such as psychotherapy or cognitive behaviour therapy. Five clinics did not offer any of these non-medical interventions in-house.
All gender clinics told researchers that “genital reconstructive surgery”—the creation of a pseudo vagina, for example—was “accessible only from age 18.” The youngest age for “masculinising chest surgery” (a double mastectomy) was reported as 16. In fact, there are documented cases in Australia of 15-year-olds approved for transgender mastectomy. Genital surgery is legally available to minors2 in Australia and practised in America.
“Only five clinics reported routine discussion of fertility3 preferences, and only two discussed sexuality4. Finland was the only country to report routinely assessing for history of trauma5,” the final Cass report says in its commentary on the survey.
In separate studies for the Cass review, three independent reviewers evaluated the quality of 21 guidelines for treatment of gender dysphoria in minors.
Included were international guidelines (from the Endocrine Society and the World Professional Association for Transgender Health or WPATH); documents from North America (for example, the 2018 policy statement from the American Academy of Pediatrics); from Europe (the guideline of the UK Royal College of Psychiatrists, for example, and Denmark’s); as well as guidelines from the Asia-Pacific and Africa.
“WPATH has been highly influential in directing international practice, although its guidelines were found by the University of York appraisal process to lack developmental rigour,” the Cass report says.
The York researchers chart patterns of “circular” cross-referencing between guidelines to create a misleading impression of consensus in favour of the medicalised “gender-affirming” treatment approach.
“The guideline appraisal raises serious questions about the reliability of current guidelines. Most guidelines have not followed the international standards for [rigorous and independent] guideline development. Few guidelines are informed by a systematic review of empirical evidence [the gold standard for assessing the evidence supporting a health intervention] and there is a lack of transparency about how recommendations were developed,” the Cass report says.
“Healthcare services and professionals should take into account the variable quality of published guidelines to support the management of children and young people experiencing gender dysphoria. The lack of independence in many national and regional guidelines, and the limited evidence-based underpinning current guidelines, should be considered when utilising these for practice.”
The Cass report says it is “imperative” that gender clinic staff be “cognisant of the limitations in relation to the evidence base and fully understand the knowns and the unknowns.”
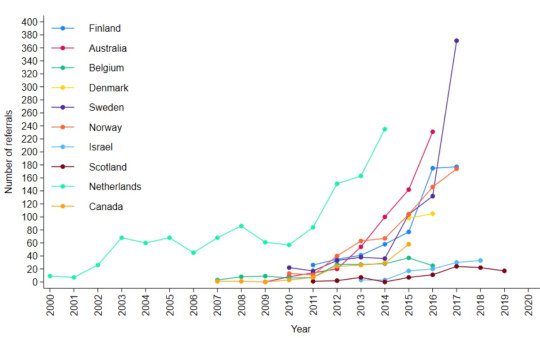
[ Chart: Number of youth gender clinic referrals over time by country. Source: Cass report ]
Bum steer
Staff at the Tavistock clinic misled patients and parents, or failed to correct their misconceptions, according to a new report from the Multi-Professional Review Group (MPRG) given oversight of treatment decisions from 2021.
These shortcomings of clinicians included playing down the extent of the unknowns of hormonal treatment; not explaining that puberty blockers are being used unlicensed and off-label; not challenging the reassuring but false parallel with the licensed use of puberty blockers for precocious (premature) puberty; not discussing the possibility that blockers will pause or slow psychosexual development; and not sharing figures showing the vast majority of children started on puberty blockers will go on to cross-sex hormones supposed to be taken lifelong.
The MPRG was also troubled by clinical documents showing misunderstanding of “the outcome of physical treatments” on the part of patients and parents.
In the York University study of treatment guidelines for gender dysphoria, only two were recommended for use by all three reviewers. These were recent, more cautious policies from Finland and Sweden. Both followed independent systematic reviews showing the evidence base for hormonal and surgical treatment of minors to be very weak and uncertain. Like the Cass review itself, the 2020 Finnish and 2022 Swedish guidelines recognise that puberty blockers are experimental and should not be routine treatment.
Although all the guidelines in the study agreed on the need for a multidisciplinary team to treat gender-distressed minors, the “most striking problem” shown by analysis of these documents was “the lack of any consensus6 on the purpose of the assessment process”, the Cass report says.
“Some guidelines were focused on diagnosis, some on… eligibility for hormones, some on psychosocial assessment, and some on readiness for medical interventions7.
“Only the Swedish and [the 2022] WPATH 8th version guidelines contain detail on the assessment process8. Both recommend that the duration, structure and content of the assessment be varied according to age, complexity and gender development.
“Very few guidelines recommend formal measures/clinical tools to assess gender dysphoria, and a separate analysis demonstrated that the formal measures that exist are poorly validated.”
Nor was there any consensus on “when psychological or hormonal interventions should be offered and on what basis.”
A survey of staff at the Tavistock clinic, undertaken as part of the Cass review, found specialists divided on whether or not “assessment should seek to make a differential diagnosis, ruling out other potential [non-gender9] causes of the child or young person’s distress.”
Arguing for an ambitious research program well beyond a possible clinical trial of puberty blockers, the Cass report says the field of youth gender dysphoria is one of “remarkably weak evidence” where health professionals are “afraid to openly discuss their views” because of vilification and bullying.
“Although some think the clinical approach should be based on a social justice model, the NHS works in an evidence-based way,” the report says.
“The gaps in the evidence base regarding all aspects of gender care for children and young people have been highlighted, from epidemiology through to assessment, diagnosis10 and intervention. It is troubling that so little is known about this cohort and their outcomes.
“Based on a single Dutch study, which suggested that puberty blockers may improve psychological wellbeing for a narrowly defined group of children with gender incongruence [or dysphoria], the practice spread at pace to other countries.
“Some practitioners abandoned normal clinical approaches to holistic assessment, which has meant that this group of [gender-distressed] young people have been exceptionalised compared to other young people with similarly complex presentations.”
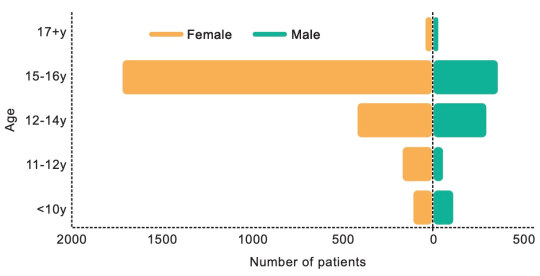
[ Chart: Age and sex on referral to the Tavistock clinic from 2018-2022. Source: Cass report ]
Who to trust?
The Cass report says the missing evidence “makes it difficult to provide adequate information on which a young person and their family can make an informed choice.”
“A trusted source of information is needed on all aspects of medical care, but in particular it is important to defuse/manage expectations that have been built up by claims about the efficacy of puberty blockers.
“The option to provide masculinising or feminising hormones from the age of 16 is available, but the [Cass] review would recommend an extremely cautious clinical approach and a strong clinical rationale for providing hormones before the age of 18. This would keep options open during this important developmental window, allowing time for management of any co-occurring [non-gender] conditions11, building of resilience, and fertility preservation, if required.”
The review stresses that “consent is more than just capacity and competence. It requires clinicians to ensure that the proposed intervention is clinically indicated as they have a duty to offer appropriate treatment. It also requires the patient to be provided with appropriate and sufficient information about the risks, benefits and expected outcomes of the treatment.”
“Assessing whether a hormone pathway is indicated is challenging. A formal diagnosis of gender dysphoria is frequently cited as a prerequisite for accessing hormone treatment. However, it is not reliably predictive of whether that young person will have long-standing gender incongruence in the future, or whether medical intervention will be the best option for them.”
Advocates for the gender-affirming approach assert that detransition and treatment regret are vanishingly rare, whereas suicide risk for those denied medical intervention is claimed to be very high.
The Cass report says: “It has been suggested that hormone treatment reduces the elevated risk of death by suicide in this population, but the evidence found did not support this conclusion.”
“The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The report cites three reasons why the true extent of detransition is unlikely to be clear for some time—patients who decide medicalisation was a mistake may not wish to return to their former clinic to announce this fact; there is a post-treatment honeymoon period and clinicians suggest it may take 5-10 years before a decision to detransition; and the surge in patient numbers only began within the last decade.
Faced with uncertainty and a lack of good evidence, those with responsibility—from health ministers and hospital managers down to gender clinicians—rely on treatment guidelines supposed to advise on clinical practice according to the “best-available” evidence and expert opinion.
In the York University guideline analysis, the 21 documents were rated on six domains, the key two being the rigour of their development and their editorial independence.
“[Rigour] includes systematically searching the evidence, being clear about the link between recommendations and supporting evidence, and ensuring that health benefits, side effects and risks have been considered in formulating the recommendations,” the Cass report says.
Only the Finnish and Swedish guidelines scored above 50 per cent for rigour. Only these two documents, the Cass report says, link “the lack of robust evidence about medical treatments to a recommendation that treatments should be provided under a research framework or within a research clinic. They are also the only guidelines that have been informed by an ethical review conducted as part of the guideline development.”
“Most of the guidelines described insufficient evidence about the risks and benefits of medical treatment in adolescents, particularly in relation to long-term outcomes. Despite this, many then went on to cite this same evidence to recommend medical treatments,” the report says.
“Alternatively, they referred to other guidelines that recommend medical treatments as their basis for making the same recommendations. Early versions of two international guidelines, the Endocrine Society 2009 and WPATH 7th version guidelines, influenced nearly all the other guidelines.
“These two guidelines are also closely interlinked, with WPATH adopting Endocrine Society recommendations, and acting as a co-sponsor and providing input to drafts of the Endocrine Society guideline. The WPATH 8th version cited many of the other national and regional guidelines to support some of its recommendations, despite these guidelines having been considerably influenced by the WPATH 7th version.
“The circularity of this approach may explain why there has been an apparent consensus on key areas of practice despite the evidence being poor.”
Sometimes these gender-affirming guidelines seek to buttress a strong evidence claim with a citation to a study that is weak or involves a different patient group.
The Cass report notes that, “The WPATH 8th version’s narrative on gender-affirming medical treatment for adolescents does not reference its own systematic review [of the evidence], but instead states: ‘Despite the slowly growing body of evidence supporting the effectiveness of early medical intervention, the number of studies is still low, and there are few outcome studies that follow youth into adulthood. Therefore, a systematic review regarding outcomes of treatment in adolescents is not possible’.”
Despite WPATH insisting such an evidence review is not possible, this is precisely what health authorities and experts have undertaken since 2019 in several jurisdictions—Finland, Sweden, the UK National Institute for Health and Care Excellence, Florida, Germany, and University of York research commissioned by the Cass review.
Yet in the 8th and current version of its guideline, WPATH makes the confident statement that, “There is strong evidence demonstrating the benefits in quality of life and well-being of gender-affirming treatments, including endocrine and surgical procedures… Gender-affirming interventions are based on decades of clinical experience and research; therefore, they are not considered experimental, cosmetic, or for the mere convenience of a patient. They are safe and effective at reducing gender incongruence and gender dysphoria”.
But WPATH “overstates the strength of the evidence” for its treatment recommendations, the Cass report says.
--
1 In the survey, there was one clinic each from Belgium, Denmark, Finland, Northern Ireland, Norway and Spain. The response rate was 38 per cent.
2 In Australia there is no good public data on trans surgery for minors.
3 Early puberty blockers followed by cross-sex hormones are expected to sterilise young people and may also impair future sexual function.
4 Some sizeable proportion of gender clinic patients might grow up in healthy bodies and accept their same-sex attraction were it not for trans medicalisation, according to testimony from detransitioners, clinicians’ reports and data.
5 Trauma from a history of sexual abuse, for example, or exposure to domestic violence is thought to be among the many possible underlying causes of what presents as gender dysphoria. The Multi-Professional Review Group (MPRG), given oversight of Tavistock treatment decisions from 2021-23, was troubled by the lack of curiosity by the clinic’s staff about the effect of a child’s “physical or mental illness within the family, abusive or addictive environments, bereavement, cultural or religious background, etc.”
6 Critics of the “gender-affirming” treatment approach say it is not mainstream medicine because the “trans child” in effect self-diagnoses while clinicians avoid differential diagnosis and attribute mental health disorders and other pre-existing issues to a “transphobic” society.
7 “In most cases [at the Tavistock clinic] children and parents were asking to progress on to puberty blockers from the very first appointment”, according to the MPRG.
8 In the MPRG’s opinion, the patient notes from the Tavistock “rarely provide a structured history or physical assessment, however the submissions to the MPRG suggest that the children have a wide range of childhood, familial and congenital conditions.”
9 Once referred to the Tavistock, patients typically were no longer seen by child and adolescent mental health services.
10 According to the MPRG, gender dysphoria in the diagnostic manual DSM-5 “has a low threshold based on overlapping criteria, and is likely to create false positives. Young people who do not go on to have an enduring cross-sex gender identity may have met the criteria in childhood. And early to mid-childhood social transition may be influential in maintaining adherence to the criteria. Sex role and gender expression stereotyping is present within the diagnostic criteria—preferred toys, clothes, etc—not reflecting that many toys, games and activities [today] are less exclusively gendered than in previous decades.”
11 The MPRG said it was “notable that until the child and family’s first appointment at [the Tavistock] they have received little, if any, support from health, social care, or education professionals. Most children and parents have felt isolated and desperate for support and have therefore turned for information to the media and online resources, with many accessing LGBTQ+ and [gender dysphoria] support groups or private providers which appear to be mainly ‘affirmative’ in nature, and children and families have moved forward with social transition. This history/journey is rarely examined closely by [Tavistock clinicians] for signs of difficulty [or] regret.”
==
Critics have described "gender affirming care" - that is, sex-trait modification - as "medical experimentation." This is incorrect. In a medical experiment, you actually collect data and monitor the participants in the experiment. They don't do that. They're cowboys violating all medical ethics - "first, do no harm" - for ideology, money or both.
#Bernard Lane#Cass review#Cass report#Dr. Hilary Cass#Hilary Cass#gender affirming care#gender affirming healthcare#gender affirmation#medical scandal#medical malpractice#sex trait modification#medical corruption#World Professional Association for Transgender Health#WPATH#ethics violations#medical ethics#unethical#gender ideology#gender identity ideology#queer theory#intersectional feminism#religion is a mental illness
13 notes
·
View notes
Text
Developpe Ch. 3
1.2k words | Getting fluffy over here
Taglist: @luna2034 @mylittlemermaid221 @notagreekgal28

When you came into class on Friday, you found Jonah setting up by himself again.
"Oh," you muttered when you walked in the doorway of the studio. You thought it was to yourself, but he heard you, and turned your direction right as you were about to walk back out the door.
"(Y/N)? Everything okay?"
You stopped in your tracks and turned back to face him.
"Yes, sorry. I didn't realize I'd be the first to class again today." You looked down at your hands, fidgeting with them.
You heard a strange noise that resembled a chuckle. Your eyes shot up and goosebumps erupted on your skin at the pleasant sound.
"Don't be silly," Jonah smiled, "come in and stretch."
Not used to this friendly nature of his, your cheeks warmed as you shrugged off your coat, and put it on the hook.
"Thanks," you mumbled, passing him to go to your normal spot.
The two of you worked in peaceful silence until other students began pouring in.
"How peculiar," you thought to yourself.
The class went on without a hitch. You were learning a particular dance sequence for Don Quixote most of the period.
"Alright," Jonah addressed everyone at the end of class. "Keep an eye out on Monday for the casting of our Don Quixote performance. I will post it in here for easy access for everyone. Your assigned parts will dictate what you learn going forward. Everyone have a great weekend!" he clapped his hands together.
You told Sebastian goodbye, and raced to the back of the room with a small smile on your face. You loved the excitement of casting. Grabbing your jacket off the hook, you swung it over your shoulders on the way out the door. The sound of something falling to the floor made you pause. Bending down just outside the doorway, you picked up a small piece of paper, and studied it as you began the walk back to your room. It was a folded yellow post-it. Had someone slipped a note in your pocket? You opened it as you exited the building, crossing the campus courtyard.
Scribbled in slanted, but neat, cursive writing was a question.
Keep this between us.
Would you prefer to be cast as Kitri or Dulcinea?
You stopped walking to stare at the note. You re-read it three times. This note was from Jonah? It had to be. Why would he care what you preferred? You started your trek again while your brain ran in circles.
It must be because you helped him. A favor for a favor, maybe? This could be considered favoritism. He could get in trouble for this, if anyone found out. Perhaps that's why he wrote you a note. You had told him about software that could locate deleted pictures and messages from phones. You supposed that he thought, this way, no one would find a trace. You slipped the note back into your pocket, and held it there, pondering your options. As you ascended the stairs inside your housing, one thought stuck out in your mind. You couldn't let anyone find out about this. Jonah would be at risk of disciplinary action, or even losing his job. You couldn't let that happen.

Jonah's stomach dropped when he saw the note fall out of your pocket. If anyone else were to find it, he'd be in some serious shit. Luckily, you're very observant, and you picked up the note before walking away with it. Jonah felt relief flood his system. He was taking a big risk. He didn't particularly know why he'd written you the note. He'd suddenly had the idea, and quickly scrawled it before class, ripping the sticky note off to take with him. During the group routine of your rehearsal, he'd slipped it into your coat pocket. He didn't know what your answer would be, or if you would be okay with this kind of communication: outside of class, personally, between the two of you. The thought made him nervous. For some reason, you'd caught his eye over the course of the past two weeks. He couldn't put his finger on why.

You had a choice to make. Were you willing to embark down this path of secrecy with Jonah? You didn't know where it would lead. There was the high probability that it would lead nowhere. If you weren't willing, however, you could simply ignore it. You could act like you hadn't seen the note. You were sure Jonah hadn't seen you pick it up. No one would find out. No harm, no foul.
You took another hot shower to process your thoughts. You ultimately decided that you wanted to go to Jonah's office during office hours to ask him about it. You had so many questions. Why you? Why now? The list went on and on. Securing your hair in a high ponytail that you were sure would give you a headache, you made your way across campus. Stepping up to the familiar door, you anxiously knocked.
"Come in," you heard Jonah call in his normal, harsh tone.
When you opened the door, he smiled at you, and adopted a friendlier demeanor.
"Oh, hello (Y/N). How can I help you?"
You bit your lip and quietly shut the door behind you.
"Hi," you mustered as you sat down in his office. "I came to ask you about the note," you studied Jonah's expression. It stayed relatively relaxed.
"Yes. I'm sorry, I know it was unexpected. What did you do with it?" he peered at you over his glasses.
"I burned it. Lit a match and put it in the sink. I didn't want anyone to find it," you chewed the skin of your bottom lip nervously.
Jonah nodded.
"Thank you, I appreciate that. I could get myself into trouble," he grimaced.
"Yes, you could," you said matter-of-factly. "Is that why you wrote a note? Because I told you about the data recovery software?"
Jonah clicked his tongue.
"Yes. Again, I apologize. I didn't mean to be so informal," he looked at you curiously.
You shook your head.
"No, that doesn't bother me. I just don't want you to get in trouble," you confessed. "Do you really think I have what it takes to be cast as Kitri?"
Jonah watched your cheeks flush. So you didn't mind the informal communication. You were just questioning your ability. Jonah steepled his fingers in front of his mouth.
"Yes, I do, (Y/N). But, if you're not ready for such a big role, you can be cast as Dulcinea. The choice is yours."
You sat quietly for a moment, looking down at your hands in your lap.
"Okay. I want to do it. If you think I'm ready, I want to be cast as Kitri. I'll give it my all," you looked up at Jonah with determination.
He smiled at you, and you noticed his eyes linger on your lips for a second. The sight sent chills down your spine.
"I have faith in you, (Y/N)."
You smiled, letting your gaze drop down to his adorable dimples. Suddenly feeling warm, you cleared your throat, and stood to leave.
"Thank you, Mr.- er, Jonah, I mean," you curtseyed. "I appreciate your support. I'll see you next week," you waved, already opening the door.
"Have a lovely weekend," Jonah smiled one last time.
You had to look away. That smile made butterflies erupt in your stomach. Crossing campus again, you wondered why the hell you'd curtseyed, and exactly what kind of arrangement you'd just consented to.
#jonah hauer king#jonah hauer king x reader#jonah hauer king x y/n#jonah hauer king imagine#my stuff#the little mermaid 2023#jonah hauer king x fem reader#jonah hauer king x you
19 notes
·
View notes
Text

This is Ross Ulbricht. 10 years ago today, Ross was arrested for creating a website.
If the government gets their way, he'll die in prison.
Ross is serving a double life sentence plus 40 years for, again, creating a website.
If that sounds ridiculous and infuriating to you, keep reading. It gets worse.
Ross created a website called Silk Road, which he designed to be a free market, secure, anonymous marketplace. It used Bicoin for payment, and utilized a system called Tor which allowed buyers and sellers to access it anonymously and without any trace.
An avid libertarian, Ross prohibited anything being sold on Silk Road that violated the Non-Aggression Principle.
This included stolen items, counterfeit/fraudulent items, child p**n, assassinations, etc.
A devout believer in nonviolence, Ross also prohibited the sale of weapons.
Many items that were sold on Silk Road were legal, and a third-party study of the site inventory by Carnegie-Mellon University concluded that the drugs most commonly sold were small amounts of cannabis.
Most importantly, Ross was not convicted for selling, buying, or being in proximity to any of the items that were sold on Silk Road, legal or illegal.
He was convicted for what others did on the site.
Imagine if Elon, or Zuck, or any of the other owners of web platforms were charged for what other people did on them.
On October of 2013, Ross was arrested by the FBI and charged with money laundering conspiracy, computer hacking conspiracy, fake ID trafficking conspiracy and narcotics trafficking. (Ross did not actually launder money, hack computers or sell illegal items himself. These charges were based on what users listed on the site.)
After his arrest, the prosecution fraudulently alleged that Ross attempted to have several people killed, but never charged him for this at trial, and his supposed "victim", Curtis Green, publicly stated that those allegations were false. He is a fervent supporter of Ross.
Despite the fact that these false, unproven allegations were never prosecuted, the federal government used them in the media to paint Ross as some kind of violent criminal kingpin, despite the fact that he was nonviolent and lived a very meager life, living with 3 other roommates in an apartment.
The FBI also seized over 144,000 Bitcoin that they found in a shared wallet on Ross's computer, which today is worth over $3.8 billion.
During Ross's trial:
Evidence and testimony showing that multiple people ran the website was banned from being discussed at trial.
Ross's defense team was not allowed to cross-examine the prosecution's witnesses or present their own witnesses
Key exonerating evidence was blocked by the judge
The prosecution was permitted to allege to the jury that Ross had hired hits on people despite never charging him with this or allowing him the opportunity to defend himself against the allegation
The jury found Ross guilty on all charges, and the judge sentenced this first-time, nonviolent person to double life plus 40 years without parole.
After Ross's trial, two of the key investigating federal agents were convicted on corruption charges related to Ross's case. Their existence was hidden from the jury during trial.
Despite all of this, Ross’s conviction was lost on appeal, and the Supreme Court refused to hear his case.
There is no other way to say it: Ross was railroaded by a corrupt federal government that wanted to make an example of him and steal his Bitcoin.
During his 10 years in prison, Ross has continued to be a model citizen, teaching classes and tutoring his fellow inmates and helping them to earn their GEDs. He has also completed several educational programs himself and has never received a single disciplinary sanction.
Ross Ulbricht is a peaceful, nonviolent man who has never harmed anyone and whose only "crime" was to create a website that other people used to sell drugs that shouldn't be illegal in the first place.
And for this, he's already spent a decade in prison.
If he is not pardoned, or his sentence commuted, he will die there.
That is unacceptable, and it is long past time for Ross to be set free.
Obama could have set Ross free with the stroke of a pen, but he wouldn't.
Neither would Trump.
Neither has Biden.
Let's replace them with someone who will.
Ross, I am sorry for what you're going through, and I will not stop fighting for your freedom until you're back home where you belong.
Free Ross Ulbricht.
Spike Cohen on Twitter/X
26 notes
·
View notes