#clinical reported outcomes
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
If you dial 1-866-584-6757, you can leave an audio post for your followers.
Text

#hidradenitis suppurativa symptom assessment#hidradenitis suppurativa clinical response#Clinro#hidradenitis suppurativa diagnosis#clinical reported outcomes
1 note
·
View note
Text
What is Linguistic Validation?
What is Linguistic Validation? Ensuring Accurate and Culturally Relevant Communication Linguistic validation services are part of an intensive process that ensures translated content retains its original meaning and cultural nuances. This method involves more than just translation; it scrutinises accuracy, cultural relevance, and appropriateness. Experts compare the translated text with the…

View On WordPress
#Accurate translation solutions#Back-translation process#Certified translation professionals#Clinical trial translation#Cultural adaptation translation#Healthcare translation services#International regulatory compliance translation.#legal document translation#Linguistic validation services#Marketing translation services#Multilingual translation solutions#Patient-reported outcome translation#professional translation services#Software localization experts#Technical manual translation#Translation quality assurance
0 notes
Photo

Human-Centric eClinical Trial Platform | Jeeva Trials
The Jeeva eClinical Cloud was developed by researchers with empathy who listen and learn to help clinical researchers, hospital sites, academic medical centers, CROs, and biopharmaceutical sponsors accelerate patient enrollment by 3x faster.
#Patient Recruitment#Patient Reported Outcomes#Clinical Outcomes Assessment#Epro#Ecoa#Virtual Trials#Clinical Research#Patient Engagement#Cloud Technology#Saas#Eligibility Screening
1 note
·
View note
Text
MASTER POST OF PROSHIP RESOURCES!!! <3<3
this is just for links (bc i just have No Way of formatting this properly), so for more in-depth stuffs and credits, head to the google doc, or the carrd !! :3c
Fiction ≠ Reality
Violent media -
Does Media Violence Predict Societal Violence? It Depends on What You Look at and When
Video Game Violence Use Among “Vulnerable” Populations: The Impact of Violent Games on Delinquency and Bullying Among Children with Clinically Elevated Depression or Attention Deficit Symptoms
Extreme metal music and anger processing
On the Morality of Immoral Fiction: Reading Newgate Novels, 1830–1848
How gamers manage aggression: Situating skills in collaborative computer games
Examining desensitization using facial electromyography:Violent videogames, gender, and affective responding
'Bad' video game behavior increases players' moral sensitivity
Fiction and Morality: Investigating the Associations Between Reading Exposure, Empathy, Morality, and Moral Judgment
Comfortably Numb or Just Yet Another Movie? Media Violence Exposure Does Not Reduce Viewer Empathy for Victims of Real Violence Among Primarily Hispanic Viewers
Fantasy Crime: The Criminalisation of Fantasy Material Under Australia's Child Abuse Material Legislation
Being able to distinguish fiction from reality -
Effects of context on judgments concerning the reality status of novel entities
Children’s Causal Learning from Fiction: Assessing the Proximity Between Real and Fictional Worlds
Reality/Fiction Distinction and Fiction/Fiction Distinction during Sentence Comprehension
Reality = Relevance? Insights from Spontaneous Modulations of the Brain’s Default Network when Telling Apart Reality from Fiction
How does the brain tell the real from imagined?
Meeting George Bush versus Meeting Cinderella: The Neural Response When Telling Apart What is Real from What is Fictional in the Context of Our Reality
loli/shota/kodocon -
If I like lolicon, does it mean I’m a pedophile? A therapist’s view
Virtual Child Pornography, Human Trafficking and Japanese Law: Pop Culture, Harm and Legal Restrains
Lolicon: The Reality of ‘Virtual Child Pornography’ in Japan
Report: cartoon paedophilia harmless
‘The Lolicon Guy:’ Some Observations on Researching Unpopular Topics in Japan
Robot Ghosts And Wired Dreams Japanese Science Fiction From Origins To Anime [pg 227-228]
Australia's "child abuse material' legislation, internet regulation and the juridification of the imaginationjuridification of the imagination [pg 14-15]
Multiple Orientations as Animating Misdelivery: Theoretical Considerations on Sexuality Attracted to Nijigen (Two-Dimensional) Objects
Positive Impact on Mental Health
Art therapy -
The effectiveness of art therapy for anxiety in adults: A systematic review of randomised and non-randomised controlled trials
Efficacy of Art Therapy in Individuals With Personality Disorders Cluster B/C: A Randomized Controlled Trial
Effectiveness of Art Therapy With Adult Clients in 2018 - What Progress Has Been Made?
Benefits of Art Therapy in People Diagnosed With Personality Disorders: A Quantitative Survey
The Effectiveness of Art Therapy in the Treatment of Traumatized Adults: A Systematic Review on Art Therapy and Trauma
The clinical effectiveness and current practice of art therapy for trauma
Writing therapy -
Optimizing the perceived benefits and health outcomes of writing about traumatic life events
Expressive writing and post-traumatic stress disorder: Effects on trauma symptoms, mood states, and cortisol reactivity
Focused expressive writing as self-help for stress and trauma
Putting Stress into Words: The Impact of Writing on Physiological, Absentee, and Self-Reported Emotional Well-Being Measures
The writing cure: How expressive writing promotes health and emotional well-being
Effects of Writing About Traumatic Experiences: The Necessity for Narrative Structuring
Scriptotherapy: The effects of writing about traumatic events
Emotional and physical benefits of expressive writing
Emotional and Cognitive Processing in Sexual Assault Survivors' Narratives
Finding happiness in negative emotions: An experimental test of a novel expressive writing paradigm
An everyday activity as treatment for depression: The benefits of expressive writing for people diagnosed with major depressive disorder
Writing about emotional experiences as a therapeutic process
Effects of expressive writing on sexual dysfunction, depression, and PTSD in women with a history of childhood sexual abuse: Results from a randomized clinical trial
Written Emotional Disclosure: Testing Whether Social Disclosure Matters
Written emotional disclosure: A controlled study of the benefits of expressive writing homework in outpatient psychotherapy
Misc -
Emotional disclosure about traumas and its relation to health: Effects of previous disclosure and trauma severity
Treating complex trauma in adolescents: A phase-based integrative approach for play therapists
Emotional expression and physical health: Revising traumatic memories or fostering self-regulation?
Disclosure of Sexual Victimization: The Effects of Pennebaker's Emotional Disclosure Paradigm on Physical and Psychological Distress
Kink/Porn/Fantasies
Sexual fantasies -
A Critical Microethnographic Examination of Power Exchange, Role Idenity and Agency with Black BDSM Practitioners
Women's Rape Fantasies: An Empirical Evaluation of the Major Explanations
History, culture and practice of puppy play
What Exactly Is an Unusual Sexual Fantasy?
The Psychology of Kink: a Survey Study into the Relationships of Trauma and Attachment Style with BDSM Interests
Punishing Sexual Fantasy
Women's Erotic Rape Fantasies
Sexual Fantasy and Adult Attunement: Differentiating Preying from Playing
What Is So Appealing About Being Spanked, Flogged, Dominated, or Restrained? Answers from Practitioners of Sexual Masochism/Submission
Dark Fantasies, Part 1 - With Dr. Ian Kerner
Why Do Women Have Rape Fantasies
The 7 Most Common Sexual Fantasies and What to Do About Them
Sexual Fantasies
Pornography -
The Effects of Exposure to Virtual Child Pornography on Viewer Cognitions and Attitudes Toward Deviant Sexual Behavior
American Identities and Consumption of Japanese Homoerotica
The differentiation between consumers of hentai pornography and human pornography
Pornography Use and Holistic Sexual Functioning: A Systematic Review of Recent Research
Claiming Public Health Crisis to Regulate Sexual Outlets: A Critique of the State of Utah's Declaration on Pornography
Pornography and Sexual Dysfunction: Is There Any Relationship?
Reading and Living Yaoi: Male-Male Fantasy Narratives as Women's Sexual Subculture in Japan
Women's Consumption of Pornograpy: Pleasure, Contestation, and Empowerment
Pornography and Sexual Violence
The Sunny Side of Smut
Other -
Fantasy Sexual Material Use by People with Attractions to Children
Fictosexuality, Fictoromance, and Fictophilia: A Qualitative Study of Love and Desire for Fictional Characters
Exploring the Ownership of Child-Like Sex Dolls
Are Sex and Pornograpy Addiction Valid Disorders? Adding a Leisure Science Perspecive to the Sexological Critique
Littles: Affects and Aesthetics in Sexual Age-Play
An Exploratory Study of a New Kink Activity: "Pup Play"
Jaws Effect
The Jaws Effect: How movie narratives are used to influence policy responses to shark bites in Western Australia
The Shark Attacks That Were the Inspiration for Jaws
The Great White Hope (written by Peter Benchley, writer of Jaws)
The Jaws Myth [not a study BUT is an interesting read and provides some links to articles and studies]
Slenderman Stabbings
Out Came the Girls: Adolescent Girlhood, the Occult, and the Slender Man Phenomenon
Jury in Slender Man case finds Anissa Weier was mentally ill, will not go to prison
2nd teen in 'Slender Man' stabbing case to remain in institutional care for 40 years
Negative effects of online harassment
How stressful is online victimization? Effects of victim's personality and properties of the incident
Prevalence, Psychological Impact, and Coping of Cyberbully Victims Among College Students
Offline Consequences of Online Victimization
The Relative Importance of Online Victimization in Understanding Depression, Delinquency, and Substance Use
Internet trolling and everyday sadism: Parallel effects on pain perception and moral judgement
The MAD Model of Moral Contagion: The Role of Motivation, Attention, and Design in the Spread of Moralized Content Online
Morally Motivated Networked Harassment as Normative Reinforcement
When Online Harassment is Perceived as Justified
Violence on Reddit Support Forums Unique to r/NoFap
"It Makes Me, A Minor, Uncomfortable" Media and Morality in Anti-Shippers' Policing of Online Fandom
#proship#profic#proshippers please interact#pro ship#profiction#anti anti#proship please interact#pro fic#🏁🎸
313 notes
·
View notes
Text
Let me share you some examples of people outside of a spiritual realm using the law of consciousness. Reading about placebo opened my eyes to realize whether I believe it or not, use it or not, it is always operating.
1. During wartime, particularly in World War II, when medical supplies were limited, the use of a saline solution as a placebo became prevalent. One notable figure associated with this practice is Henry Beecher, a medic during the war. When morphine, a powerful painkiller, was scarce, Beecher resorted to injecting injured soldiers with a saline solution (a mixture of salt and water) as a substitute.The fascinating observation was that many soldiers responded positively to the saline placebo, reporting a reduction in pain. Beecher’s experience led him to further investigate what is now known as the placebo effect. He discovered that even inert substances like saline could elicit a therapeutic response in individuals, highlighting the power of belief and the mind’s influence on healing. Using saline as a placebo during wartime was a practical solution to address the scarcity of medical resources. It allowed healthcare providers to provide some form of treatment while conserving limited supplies for critical cases. The phenomenon observed in these wartime placebo administrations contributed to our understanding of the placebo effect and its role in medical practices.
2. And then there was another placebo test done with surgeries demonstrated the power of the placebo effect in the context of surgical interventions for knee pain.
The study, often referred to as the “fake leg surgery” study, focused on patients with osteoarthritis in the knee. Participants were randomly assigned to either receive real arthroscopic surgery or undergo a sham procedure where no actual surgical intervention took place. The sham surgery involved making small incisions and mimicking the actions and sounds associated with the actual procedure.The surprising finding was that both groups, those who underwent real surgery and those who had the sham surgery, reported similar improvements in their knee pain and functionality. This suggested that the positive outcomes experienced by the participants were not necessarily due to the physical intervention but rather to psychological factors such as the placebo effect.
3. The most fascinating one was this one: The study aimed to explore the role of mindset in reversing some aspects of aging.
In this experiment, Langer and her team created a simulated environment reminiscent of the 1950s to immerse a group of elderly participants. The participants were instructed to act as though they were 20 years younger and encouraged to engage in activities that required physical and mental activity. It aimed to create an atmosphere where the participants felt as if they were stepping back in time.The results of the experiment were described as astonishing. Participants reportedly experienced improvements in various areas, including physical health, cognition, and overall well-being. The study suggested that by changing one’s mindset and engaging in an environment that challenges typical aging stereotypes, individuals may experience positive effects on various aspects of their lives.
4. The Man Who Overdosed on Placebo" is a story about a 26-year-old man, often referred to as "Mr. A," who was part of a clinical trial for an antidepressant drug. In a desperate state of mind, he attempted suicide by ingesting 29 capsules of what he believed to be the experimental drug. This act was triggered by his depression, which had worsened after a breakup with his girlfriend.
However, unbeknownst to him, the pills he had taken were not the actual antidepressant, but rather placebos - essentially inert substances, often sugar pills, used in clinical trials as a control group. Despite this, Mr. A's vitals showed alarming signs similar to those of a drug overdose, reflecting the power of belief over the physical body, a phenomenon known as the "nocebo effect."
The nocebo effect is essentially the evil twin of the placebo effect. While the placebo effect can lead to improvements in health due to positive expectations, the nocebo effect can cause negative symptoms or even exacerbate existing ones due to negative expectations. In this case, Mr. A exhibited symptoms of an overdose solely because he believed he had taken an overdose.
5. Sam Londe, is one of the best but sad classic example of the nocebo effect, as detailed in Dr. Joe Dispenza's book "You Are the Placebo."
Sam Londe was diagnosed with esophageal cancer, a condition known for its grim prognosis. His doctors informed him that he didn't have much time left to live. Accepting this diagnosis, Londe quickly became bedridden and his health deteriorated rapidly, following the trajectory his doctors had predicted.However, upon his death, an autopsy revealed a surprising fact: there was not enough cancer in his body to have caused his death. The small tumor in his esophagus was not large enough or in a position to interfere with his swallowing or breathing. Essentially, Londe didn't die from cancer; he died from believing he was dying of cancer.
This case demonstrates the power of the mind over the body, both positively (the placebo effect) and negatively (the nocebo effect). In this case, Londe's negative beliefs about his prognosis led to physical symptoms and ultimately his death.
I've seen dozens of examples where of stuff like this particularly in the realms of hexing and witchcraft. Honestly, the same could probably be said about subliminals. But it doesn't matter much.Why? Because they work. It's all about observation and choice. You could say it’s the mind but the mind operates on logic. This goes beyond the mind and to your true being, what observes the mind observing the pain in the first place.
Actually I was talking to someone who had been struggling with shifting for a while about this and it really resonated with her which is why I decided to share it. She took a water bottle, labeled it shifting juice and just assumed that when she finishes the bottle she has “full access to shifting powers” is that how it works. Nope. Did she shift after two years of struggling. Yep. It doesn’t matter what story you create yourself whether you want to use logic or not whatever you assume and persist in and know as a fact will harden into truth and therefore reality.I just wanted to share this story bc I find it absolutely hilarious how we sometimes take it so seriously yet it can be so easy. I know placebo is just an assumption. It’s like when you tell children you checked under their bed for the monsters and drafted them and they assume so so they can sleep soundly at night. Call it whatever you want assumption, placebo, it’s all just words and each community calls it something different but at the end of the day it works wether you know the truth behind it or not.

590 notes
·
View notes
Text

[Exhibit Document from the Birth & Reproductive History Museum, Washington, D.C.: Excerpt from Dr. H. Farnsworth’s Private Journal, Dated August 9, 1944]
Patient Name: Mr. Thomas Cooper Spouse: Captain Leonard Cooper, United States Navy Date of Delivery: August 8, 1944 Labor Duration: Approximately 48 hours Birth Outcome: Healthy male infant, 10 pounds, unmedicated natural delivery Immediate Postpartum Notes: Initiation of moobfeeding
Notes on Delivery and Postpartum (By Dr. H. Farnsworth)
The final phase of Mr. Cooper’s pregnancy culminated in an intensive two-day labor at our clinic. Throughout the protracted labor, he declined pharmacologic pain relief, citing his strong personal conviction in a fully natural birthing process. Progress was slow yet consistent: cervical dilation advanced steadily, and fetal heart tones remained robust, even as Mr. Cooper’s contractions intensified in both frequency and duration.
Captain Leonard Cooper arrived in the latter stage of labor, having been granted emergency leave from his naval command. His presence appeared to buoy Mr. Cooper’s morale significantly. Despite extreme fatigue, Mr. Cooper exhibited unwavering fortitude when bearing down, spurred by his husband’s encouragement and the attentive aid of the nursing staff.
The newborn presented with a notably large frame (10 pounds) but in optimal position, allowing for a safe, albeit strenuous, delivery. Mr. Cooper’s pushing phase was lengthy, compounded by the infant’s size; however, he managed to deliver without any medical interventions beyond standard warm compresses for perineal support. Following an initial cry and brief examination, the infant was declared healthy, with commendable Apgar indicators.
Postpartum Condition and Moobfeeding Initiation
Upon delivery, Mr. Cooper—though visibly exhausted—expressed relief and elation, particularly once the infant was placed upon his chest. Per his request, we facilitated immediate skin-to-skin contact. Within the hour, Mr. Cooper initiated moobfeeding, which the infant latched onto effectively after a brief period of encouragement and guidance. This early feeding proved beneficial in promoting uterine contraction and bonding.
Mr. Cooper’s vital signs stabilized promptly post-birth, despite the prolonged labor. He displayed mild perineal swelling, yet no significant lacerations were identified. During routine observation overnight, Mr. Cooper required only cold compresses and rest to manage soreness. He continued moobfeeding on demand, approximately every two to three hours, which helped stimulate milk production and offered the infant consistent nourishment.
Captain Cooper remained at his husband’s bedside throughout the night, assisting with positioning the infant for moobfeeding and ensuring Mr. Cooper remained adequately hydrated. The close involvement of Captain Cooper evidently fostered a calm environment, allowing Mr. Cooper some respite between feedings. By morning, both father and child were reported to be resting comfortably, with moobfeeding well established and the infant producing satisfactory wet diapers.
Additional Observations
Mr. Cooper exemplified notable resolve under challenging circumstances, laboring unmedicated for a full 48-hour period. The infant’s weight (10 pounds) affirms our earlier assessments of a robust gestational course. It is our recommendation that Mr. Cooper maintain a nutrient-rich diet to support ongoing moobfeeding, and that he practice gentle perineal care to expedite full recovery.
The successful outcome of this birth, paired with the renewed presence of Captain Cooper after weeks at sea, underscores the profound impact of family unity on the birthing process. In an era shaped by wartime separation, the Coopers’ experience stands as a testament to resilience, partnership, and the efficacy of consistent prenatal care.
Signed, Dr. H. Farnsworth Obstetric & Reproductive Medicine Washington, D.C.
93 notes
·
View notes
Text
Nova Genesis
Part Two

Summary: disgruntled with the decision to return to Earth, who knows what the prisoners aboard will do to cling to their false freedom. And who will get mixed up with it | Word Count: 5.5k~ | Warnings: smut, p in v sex, dubcon, choking, degradation, blood, murder, threatening behaviour

She blinked hard, having stared at the blue, intrusive light of her computer screen for what seemed like hours now. Pressing the heels of her palms against her lids provided some relief to the thudding in her temples, but not nearly enough. This place was suffocating. And she briefly wondered how on Earth the prisoners had lasted as long as they had without going completely insane. She closed her laptop in a huff, her report written, a script planned out in her head for what she would tell Dr Dibs. She steeled herself, preparing for any reaction, her shoes plodding on the linoleum floor, every step echoing her growing apprehension, but she knew this conversation with her was inevitable. The dim lights in the corridor flickered as she reached the door. She paused for a moment, collecting her thoughts before entering.
Inside, Dibs was hunched over a tray of instruments, methodically wiping each one with a clinical precision that made her skin crawl. The doctor didn’t look up, her voice calm, almost detached.
“You’re here to tell me it’s over, aren’t you?”
Even the tone she used seemed unemotional, a stark contrast to the mess she had been when they had first arrived and broke into their systems, destroying samples. She held her breath, “Yes. The investigation is wrapping up. We’ve gathered enough evidence to ensure this project is shut down. The prisoners will be returned to Earth.”
Dr Dibs shook her head, placing a gleaming scalpel on her table before moving to the next. “And you think that’s a good idea? Bringing them back?”
“Doesn’t matter what I think.”
Dibs finally looked up, her eyes dark with something unreadable. “No, I suppose it doesn’t,” she mused, before her lips turned into a small, cynical smile. “They’ll tear each other apart before you even reach the atmosphere.”
Her stomach churned with unease at her words, though she tried not to show it on her face that the doctor had managed to make her uncomfortable. There was, of course, a whispering of rebellion amongst those who didn’t want to go back, she knew that. But naively perhaps, thought it would go no further than a few choice words.
“An announcement will be made shortly. I suggest you prepare yourself for the outcome.”
“Prepare myself?” she echoed, her voice dripping with irony. “It’s you and your team who should be preparing. Once you announce their return to Earth, you’ll be the only thing standing between them and their worst nightmares.”

The prisoners were gathered in the central area of the ship, their eyes flickering with a mix of curiosity and suspicion as she stood before them, report in hand, flanked by guards. The air was thick with tension, the kind that makes every breath feel weighted. Each gaze was filled with distrust, hatred almost, all except one, half-lidded with amusement. She took a deep breath, projecting as much authority as she could muster.
“After thorough consideration and investigation from our colleagues, it has been decided that this mission will be terminated, and all of you will be returned to Earth.”
A murmur spread through the crowd, a mix of surprise, disbelief, and anger. Monte stepped forward, his face a mask of barely contained fury.
“I’m not going back to Earth, not like this. You’re sending us back to rot in a cage, to be paraded around like freaks. We’re not going back. Not all of us.”
“This isn’t up for debate. The decision has been made,” she repeated, her voice firm though her heart pounded against her ribs.
Monte's fists clenched at his sides, his knuckles turning white as the tension in the room thickened. His fury, barely held in check, finally broke through, spilling over like a dammed river and before anyone could react, he lunged forward, knocking over the nearest table with a force that sent equipment clattering to the floor. Other prisoners, emboldened by his defiance, began to move as well, their voices rising in a chaotic blend of anger and desperation. Chairs were overturned, shouts echoed off the metallic walls, and the guards tensed, readying themselves for violence.
“You’re sentencing us to worse than death!” Monte roared, his voice booming above the growing chaos. “You’re no better than the people who sent us up here in the first place!”
No. She thought. I’m a lawyer, I’m helping them. Surely.
She could not think why they would be so desperate to stay. So eager to die up here where nobody could find them, or even know where they were. But seeing the sheer determination in some of their looks, she briefly understood.
These people want to disappear.
Her hand hovered near her comms device, but she knew calling for more backup would escalate the situation further. But the guards, finally springing into action, moved to subdue Monte as he approached, and the other prisoners stepped in, creating a human barrier. The room descended into utter chaos as shoves turned into punches, and the violence spread like wildfire.
Across the room, Ettore leaned casually against the wall, a smirk playing at the corners of his lips as he watched the chaos unfold. His eyes locked onto hers from across the room, and for a brief moment, amidst the turmoil, their gazes held. There was something predatory in his expression, a dark amusement at her situation, as if he was enjoying the spectacle of her losing control.
“You think you can control us?” Monte snarled, his body wedged between two guards. “You think you can just send us back to that hellhole?”
With her heart hammering in her chest, she couldn’t shake the feeling that this was just the beginning. She tore her eyes away from Monte’s seething form, only to find Ettore still watching her, his expression unreadable. She turned sharply on her heel, retreating to the relative safety of her team, her mind spinning. In the midst of the chaos, one thought lingered in her mind. Ettore’s smirk, his gaze that seemed to pierce through it all, as if he was waiting for her to slip.
Waiting for the vulnerability he was sure was going to rear its head.
Mink sidled up to Ettore, her expression serious as she glanced around to make sure no one was listening. Her voice was low, almost a whisper, filled with concern. “Monte’s losing it. You can see that, right?”
Ettore didn’t respond immediately, his eyes still following the path she had taken as she retreated with her team. The smirk from earlier lingered faintly on his lips, but there was something darker beneath it. He turned to Mink, his voice detached. “Monte’s been on edge since day one. Today just gave him the excuse he’s been waiting for.”
“He’s desperate. Desperate people do stupid things. What happens when she figures out what’s really going on here? If this blows up, they’ll throw us all under the bus.”
"Whether it’s Monte that takes us out or Earth, doesn’t really matter in the end, does it?"
Her jaw tightened, frustration flickering across her face. “And what about you? What’s your angle in all this? Are you just going to sit back and watch him burn everything down?”
His gaze darkened as he thought about her, like the snuff of a candle, his blue eyes went near-black. There was something about the way she held herself, the way she looked at him, that intrigued him more than he wanted to admit. She had a confidence, a belief in her own righteousness that he found almost laughable. Yet, underneath it all, he could sense the tension, the fear she tried so hard to mask. He’d seen that look before, on other women, other people, just before they broke.
"Maybe I’ll just sit back and watch," Ettore finally answered. "Or maybe I’ll give her a little push, see how far she can really go before she snaps."
The door pressed shut behind her as she pushed into her quarters for the evening, still dressed even at such a late hour. She carried the day’s stress with the tension in her shoulders. If she focuses hard enough, she can still grip the panic she felt earlier that day when the prisoners had all turned on her and her staff. She kicked off her shoes, the tension in her shoulders momentarily easing as she stretched out her feet. The dim lights overhead cast a warm, soft glow over the small, sterile space. A brief respite.
As she was about to take a breath and unwind, everything went dark. The ship's systems cut out abruptly, plunging the room into an oppressive, suffocating silence. She froze, her heart leaping into her throat as she was enveloped in complete darkness. No emergency lights. No familiar hum of the ship's engines. Just an endless, empty, nothingness.
She couldn’t see her hand in front of her face, the blackness so absolute it felt as if the walls were closing in around her. Panic began to creep in, but she forced herself to stay calm. The air felt heavy, thick with an unnatural stillness that made her skin prickle.
“Stay calm,” she whispered to herself, reaching out for something, anything, to ground her. But her fingers met only empty space. She knew the layout of her quarters, could navigate it with her eyes closed, but the utter darkness was disorienting. She felt her way along the wall, her fingertips brushing against the cold metal, her breath quickening with each step.
The thought that this wasn’t an accident slithered into her mind. Could this be sabotage? A prelude to something worse? The faces of the prisoners flashed in her mind. Monte’s fury. Ettore’s unsettling calm, and a chill ran down her spine.
Her breath hitched as she considered the possibilities. The ship wasn’t supposed to fail like this. Not without warning. Not without backup systems kicking in. She reached for the small comms device, fumbling in the darkness, but the screen remained dead.
She was alone, blind, and utterly vulnerable.
Heart pounding in her chest, her hand gripped the door frame of her quarters as she cautiously stepped out into the pitch-black corridor. The darkness was suffocating, every sound amplified, her senses on high alert. She moved quietly, trying to navigate the ship's labyrinth passageways by memory.
The path she was taking should have led her to the guards’ station, but the disorienting blackness made it impossible to be sure. She fought down the rising panic, forcing herself to focus. She couldn’t afford to get lost. Not with people she knew loathed her, possibly lurking about in the adjoined ship.
After what felt like an eternity, she finally stumbled upon the entrance to the guards’ station. Relief washed over her as she pushed open the door, expecting to find safety within. Her foot slipped, and the metallic scent of something deep filled her nose, sharp and acrid. It was only when her foot caught on something soft and unmoving that she stifled a gasp, her hand flying to her mouth to keep from making a sound.
She took a step back, nearly tripping over her own feet in her haste to put distance between herself and the grisly reality. Her mind raced, trying to process the horror of it all. How had this happened? Who could have done this?
With trembling hands, she eased herself to the floor, her hand patting over the body of one of the guards until she found her target. The gun felt too large in her hand as she picked it up. The cold weight of the weapon in her grasp was both alien and strangely comforting. She wasn’t trained for this, but she wasn’t about to be caught unarmed.
“WHERE ARE YOU, YOU BITCH?!”
She froze, her breath catching in her throat. The voice was close, too close. And oh so familiar. Her heart thundered in her chest as she gripped the gun tighter, backing up against the wall, her pulse racing. Fear threatened to consume her, but she forced herself to stay calm, to think.
Monte was out there, hunting her.
She could recognize that voice anywhere, the fury behind it unmistakable. He’d gone into her room and discovered she wasn’t there, and now he was hunting her down with a vengeance. Thank God she’d kicked off her shoes. The thought flashed through her mind as she pressed herself against the cold metal wall, her breathing shallow, trying to remain as silent as possible. Without the squeak of her trainers on the floor, she had a chance, however slim, of slipping away unnoticed.
The darkness was both her enemy and her ally. It masked her movements, but it also made every step fraught with the risk of revealing her position. She had no idea where Monte was now, only that he was close, and that his rage was palpable, even through the thick walls of the ship.
Monte’s voice echoed again, closer this time, filled with venom. “WHERE ARE YOU!”
The darkness was suffocating as she crossed into the prison ship, the stale air thick with tension. She prayed Monte wouldn’t think to look for her here. The ship's unfamiliar layout was like a labyrinth of potential traps. Every step felt like it could be her last, each sound amplified in the oppressive silence.
She stumbled into the rec room, her heart pounding against her ribs. She backed up slowly, her senses heightened, straining to catch any sound of Monte’s approach.
And then she heard it, the sound of deliberate footsteps. Monte was getting closer. She couldn’t see him yet, but she knew he was near, racing down the hall towards the rec room, the door luckily closing softly shut to note she had not been near. But all the same, the fear lingered.
Backing up, she collided with something solid. Her first instinct was to scream, but before she could make a sound, a strong hand clamped over her mouth, muffling the cry. She was shoved against the cold metal wall, her back pressed firmly against it as a tall figure loomed over her. Her heart raced, terror surging through her.
“Shh,” he whispered, his breath warm against her cheek.
Ettore.
They stayed like that for what felt like an eternity, the air thick with a tension that was both terrifying and oddly charged. She didn’t dare move, her breath shallow and trembling against his hand. He leaned in closer, his lips almost brushing her ear as he whispered.
“Stay quiet, and maybe we’ll both make it out of this.”
She nodded slightly, in no position to argue or protest. His voice was a low, dangerous murmur, but there was something almost protective in the way he held her, his body shielding hers from the imminent threat. It was a strange, twisted sense of security, and despite the circumstances, she found herself clinging to it.
Monte stormed into the room, his heavy footsteps echoing through the pitch-black space. The door slammed against the wall, the sound reverberating through the silence. Her entire body tensed, a wave of raw terror gripping her as she pressed herself against the wall, wishing she could melt into it and disappear.
She had never been more scared in her life. The darkness was all-consuming, robbing her of her senses. She couldn’t see Monte, couldn’t gauge his distance or his intentions. All she knew was that he was close, far too close.
Ettore’s hand remained firmly over her mouth, his grip steady but not harsh. She could feel the rough texture of his palm against her lips, could almost feel the thudding of his own heart against hers, and she fought to keep her breathing steady, her panic threatening to break through. For the first time, she was thankful for the darkness, for the inability to be seen, but it didn’t stop the tears from welling up in her eyes, blurring what little she could make out in the blackness.
Monte’s voice boomed through the room, a raw, violent shout that made her flinch involuntarily. “Where the fuck are you, you bitch? You think you can hide from me?”
Her tears spilled over, silently sliding down her cheeks, and Ettore’s hand, still covering her mouth, felt the wetness. She didn’t know if it was fear, hopelessness, or the sheer weight of the situation crashing down on her, but she couldn’t stop the silent flow.
She tried desperately to make out Ettore’s face, to find some anchor in the overwhelming darkness, but it was impossible. He was just a shadow, a vague outline she could barely discern, his presence more felt than seen.
Monte’s footsteps grew closer, his breathing heavy and erratic as he stalked through the room, searching for her. She could feel Ettore’s grip tighten slightly, a silent reassurance or perhaps a warning to stay silent. Her heart pounded so hard she thought it might give them away.
The sound of Monte’s boots scuffing against the floorboards seemed deafening in the darkness. The tension was unbearable, a taut line ready to snap at any moment. Monte cursed under his breath and turned away, his footsteps retreating as he left the room. The door slammed shut behind him, and the oppressive silence that followed was almost worse than his presence. She didn’t dare move, not even to breathe, until she was sure he was gone.
“Jesus…” she whispered in relief when Ettore’s palm dropped from her lips. She expected him to move away, for them to find some way of escape.
But his hand, once firm over her mouth, slowly slid down to her neck, his fingers curling around the sensitive skin, holding her in place. The touch was no longer just about silence, it was possessive, controlling. She could feel his breath against her ear, slow and deliberate, as the tension between them morphed into something darker, more dangerous.
Her heart raced for a different reason now, a confusing mix of fear and something else, something she didn’t want to acknowledge. His other hand moved with a deliberate slowness, tracing the line of her waist before cupping her womanhood through her jeans. She gasped softly, the sound barely escaping her lips, but it was enough to let him know that she was fully aware of his intentions.
In the darkness, with Monte gone, the only thing she could see was his outline, and the only thing she could feel was the slow, purposeful movement of his hands. He held her firmly against the wall, his grip on her neck tightening just enough to remind her who was in control.
His hand applied just enough pressure to make her pulse quicken. "You're shaking," he noted, his tone almost mocking. "Is it fear, or something else?"
She could tell from his tone, he was loving this. Amused by her fear and helplessness. He enjoyed far too much the feeling of having someone’s life and control in his hand.
"Tell me, are you scared of what I might do? Or are you more afraid of how much you might want it?"
Her breath hitched, the question slicing through her like a knife. After a moment that felt like an eternity, she finally found her voice, though it was barely more than a whisper. “I'm not scared and I don't want you-”
The lie hung heavy in the air between them, and Ettore chuckled darkly, his free hand sliding down her body. He didn't believe her for a second, and she could tell.
His fingers deftly found the button of her jeans, and with a single, practiced motion, he popped it open. “So if I touch you here,” he whispered, his hand sliding beneath, “you won’t be wet?”
All it took was his fingers to dip beneath her underwear, sliding between her folds to collect her arousal on his fingertips, for her to freeze, the realisation dawning darkly that his presence in the darkness, his grip on her, and his words, were all having the effect she wanted least to happen.
She bit her lip, trying to suppress the involuntary reaction that coursed through her as he drifted north to circle her clit with ease.
“You’re not the woman I thought you’d be,” he continued, his tone mocking. “Say you're a professional? You're a fucking liar.”
Once again, she tried to make out his face. Trying to imagine his expression. She was convinced he could somehow see hers as he pushed forward, stretching her hot walls around his fingers to harshly fuck her with his fingers, as if testing the dangerous waters.
Her hand clamped on his wrist. She wanted him to stop. She wanted him to carry on. The darkness was doing her indecision no favours whatsoever, blurring her common sense.
He bruised his body against hers, pinning her even more firmly to the wall. The sound of her moisture clicking against his skin both erotic and a terrifying reminder of how her control had waned.
“Tell me to stop,” he challenged, his voice low, a whisper that curled around her like smoke. “But you won’t, will you?”
Her voice came a shaky whisper, an attempt to grapple back that sense of self she felt was swiftly slipping. But her tone betrayed the conflict raging inside her. “You…don't know me-” she strained to say, wincing as she felt the rough pads of his fingers brush the front of her walls.
She felt his breath, amused against her face. Ettore’s response was a low, mocking chuckle. “Maybe not,” he murmured, his lips brushing against her ear, “but I know enough.”
Her whine was low as his fingers left her, but her heart stuttered in place when he rolled her jeans over her hips, taking her underwear with it. His knee harshly nudged her legs apart so she couldn't close them, before moving his sweatpants down just enough, his breath hot against her neck, where his palm still pressed.
Fuck. Fuck. Fuck.
He knew enough about her to know that at this moment, she wouldn't stop him. Perhaps, couldn't. If she even tried. She choked air out her lungs when his chest pressed against hers, one hand pulling her leg over his hip to angle her up.
And the sharp pang of panic when she felt the blunt head of his cock press into her. She felt herself starting to say ‘no’, but all words died on her lips as she felt him stretch her open on his length, disappearing inside her with barely a sound of his own.
It was sharp and biting, the pain initially. If it could have been called foreplay, none of it had really been for her in any case, so she felt every inch of him. And she winced, eyes pressing shut when his pace was immediately brutal, snapping against her hips with commanding intensity.
All she could do was press her fingernails into his arm, try and share some pain with him in some twisted way. That's the only sound he made, was a low groan, his grip around her throat tightening to feel the rapid thrum of her pulse.
She hated it. Hated giving him this…sick sense of control over her. Knowing that he would be much too proud and one track minded to stop until he'd come, she thought, get it over with.
She clenched around him, hard. Wanting him to lose it himself and just finish what he started. And when she felt his breath catch, she smirked in victory, until his hand raised to her face, pushing her head harshly back, her jaw anchored in his grip.
“No you don't, you fucking bitch,” he breathed, low and dangerous in a way that made her heart freeze. “Think you can rush me?”
The smirk that had momentarily crossed her lips vanished as she realised how deeply she had miscalculated. Ettore wasn’t going to simply take what he wanted and be done. He was going to make her feel every second of it, make her pay for that brief moment of defiance.
“You’re going to come on my dick, and when you do, you’ll sound pathetic. Just like you are.”
It was fucking annoying, was all she thought, that when he renewed his pace to borderline erratic, the pain ebbed into sharp pleasure. The hand that held her leg around his waist drifted inwards, clumsily circled her clit, too quickly and firmly to feel entirely pleasurable, but just enough combined with his relentless assault to send her spiralling.
Her breath hitched, and she felt the tears prick at the corners of her eyes, more from frustration and rage than anything else. He could feel it too, how close she was to breaking, how her body betrayed her resolve. Ettore revelled in it, every small tremble, every shaky breath, feeding his twisted need to dominate.
He pressed her sensitive bundle of nerves like he hated her, and it was enough to send a full body shudder from the top of her spine right through her core. He only let out a breath of smug relief feeling her walls clamp him in, tending uncontrollably around him.
The room was silent except for the harsh breaths they both struggled to catch. The darkness around her seemed to close in, the only light left in the room the fading stars behind her vision. As the reality of what had just happened began to set in, she felt Ettore’s body still against hers, the warmth of him inside her chasing away the numbness that had momentarily overtaken her.
For a moment, neither of them moved. Then, with a surge of disgust and anger, she pushed against his chest, forcing him away from her. Her hands trembled as she scrambled to right her clothes, feeling hot in her chest with shame. Ettore staggered back, and she could practically feel his smug grin in the darkness. He adjusted himself with a deliberate slowness, clearly savouring the moment. His breathing was still laboured, but there was an unmistakable air of satisfaction surrounding him.
“No use fighting it,” he murmured, amusement seeping into every word.
She scoffed, her hands fumbling with the buttons of her jeans. “Dick,” she muttered under her breath, the word laced with a mix of anger and frustration.
Ettore’s smirk only deepened, his eyes glinting with satisfaction. “Call me what you want. You know I’m the only one who can get you through this. You need me. Whether you like it or not.”
The emergency lights flickered on, casting a dim, flickering glow over the room. The sudden illumination was a relief, pulling her back from the suffocating grip of darkness. She could finally see again, the oppressive void around her receding. The sight of Ettore standing there, so smug and composed, sent a wave of shame crashing over her. Disgust curled in her stomach, twisting alongside a sick sense of arousal she couldn’t fully suppress.
But like a cold slap to the face, she knew Monte was still out there, stalking the ship, hunting her down. And now, with the lights on, it would be easier for him to find her. |It was a jolt, reigniting the fear she had momentarily pushed aside amidst the dull haze of thrumming pleasure.
Ettore seemed to sense her shift in focus, his smirk fading into something more serious. "He’s not far," he said, his voice low and measured. “Stick with me. I know a quick way back.”
She didn’t respond, her mind racing. The thought of Monte finding her now, after everything, sent a fresh wave of terror through her. As much as she despised the idea, as much as she loathed Ettore for what he'd done, he was her best chance at survival. But how could she, with everything she knew and everything she had just experienced, possibly trust him?
Was the onus on her? For allowing him to do what he did? For the way she had let him touch her, for the strange, conflicted sensations she had felt?
Before she could dwell on it further, Ettore yanked her forcefully, snapping her back to the present. They had to move quickly. The urgency in his grip was impossible to ignore, and in the rush, she realised too late that she had forgotten to feel for her gun.
They hurried through the narrow corridors, the cold metal walls echoing with the distant sounds of chaos. When they finally reached the entrance to her team’s ship, he pulled her inside with a final, rough tug. Panting, she glanced around the familiar interior of the vessel, trying to steady herself. Ettore didn’t waste a moment.
“Do you have the authority to access the emergency autopilot system?” he asked, his voice sharp, cutting through the haze of fear and confusion.
She hesitated for just a second. “Yes, but what about everyone else? We can’t just leave them.”
“There’s no time,” he shot back, his eyes locking onto hers with an intensity that made her stomach drop. “Monte’s not going to stop until he finds you, and when he does, you’re dead. We need to get off this ship now.”
Her hands shook as she moved toward the control panel, the reality of the situation weighing heavily on her. She could feel Ettore’s gaze on her, urging her to move faster, to make the choice she knew she had to make. The ship’s systems roared to life, as did the alarms, signalling their imminent departure from the prison ship. For a brief, harrowing moment, she could hear Monte’s voice echoing through the corridor, filled with rage, mingling with the desperate shouts of others. But then the door hissed shut, sealing them off from the chaos outside.
Ettore was already behind her, his presence looming, suffocating in the small space. “Control Room. Now,” he ordered, his tone leaving no room for argument. Panic surged through her, her mind racing as she obeyed, her steps hurried and frantic. She couldn’t think straight, couldn’t process the fact that a dangerous criminal was now alone with her on her ship. Panic pushed her forward instead. Primal and urgent.
Once there, her mind scrambled for any option, any way to get the ones who wanted to return to Earth safely off the prison ship. “We can’t just leave them behind,” she stammered, turning, desperation clear in her voice. “There are others who want to return-”
Her blood ran cold as she whipped back at him, he stood tall, almost proud, holding a gun to her face. A brief, fleeting thought roared through her mind that she doubted it was loaded, but she dare not entertain it right now. Not when fear gripped her ribs.
Her own gun. She knew the second she went to feel for it.
He’d stolen it during her moment of weakness.
Ettore smirked, his expression infuriatingly smug. “No hard feelings,” he said, his voice dripping with mockery.
Her heart raced with a potent mix of anger and terror. This wasn’t how it was supposed to go. She had come here with the intention of doing good, of offering these people a chance at redemption or at least a fair trial. And now, what had she done? She’d left behind an entire ship of prisoners, all so she could be trapped here, alone, with him.
She stared at Ettore, her mind swirling with a thousand conflicting emotions. The anger bubbling up inside her was nearly as strong as the fear. How had it come to this? How had she let herself be so easily manipulated, so trapped?
“Here’s how this is going to work,” he said, his tone all business now, as if he were discussing a simple transaction. “You’re going to take me back to Earth, and when we get there, you’re going to make sure I live a nice, cushy life. No more cells, no more guards, just freedom. I’m sure a smart woman like you can figure out how to make that happen.”
She opened her mouth to protest, to argue, but the cold, unyielding barrel of the gun in his hand kept her silent.
“And in return,” he continued, his eyes darkening with a twisted sort of pleasure, “we’ll have some fun on the way back. You’ll make sure of that too, won’t you?”
Anger and fear warred within her, but the sharp edge of reality kept her from saying anything that might push him further. She felt utterly trapped, forced into a role she never imagined she’d play. The man in front of her was dangerous, and there was no telling what he would do if she refused.
Ettore’s smirk softened, just a little, as if he could sense her internal struggle. “You’re smart. You know what the right choice is.”
She wanted to scream, to cry out in frustration and fear. A dark, violent urge flared within her, the impulse to bash him over the head, to kill him and be done with it. But here, alone in the vastness of space, without the guards or anyone else to enforce order, who would hear her? Truly hear her? Her fury would echo into the void, and she would still be utterly and entirely, alone.
His voice was a soft, poisonous whisper. “So, what’s it going to be, little lawyer?”
General Taglist: @1lluminaticonfirmed @aemondsfavouritebastard @all-for-aemond @bellstwd @blackswxnn
@blairfox04 @buckybarnesb-tch @castellomargot @cl-0-vr @eddieslut69
@emmaisafictionwhore @eponaartemisa @hb8301 @jamespotterismydaddy @justbelljust
@minholy223 @mochi-rose @natty2017 @nenelysian @nixiefics
@primonizzutto @qyburnsghost @randomdragonfires @risefallrise @sheshellsseashells
#ettore imagine#ettore x reader#ettore smut#ettore high life#ettore x fem!reader#ettore x oc#ettore x female#ettore fanfiction#ettore fic#ettore fanfic#ewan mitchell#ewan mitchell characters#high life movie#high life 2018#high life fanfiction#ettore x ofc#ettore x you
140 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone. There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
386 notes
·
View notes
Note
I totally understand and can empathize with fat activists when it comes to medical fatphobia. But I do think its important to provide nuance to this topic.
A lot of doctors mention weight loss, particularly for elective surgeries, because it makes the recovery process easier (Particularly with keeping sutures in place) and anesthetic safer.
I feel like its still important to mention those things when advocating for fat folks. Safety is important.
What you're talking about is actually a different topic altogether - the previous ask was not about preparing for surgery, it was about dieting being the only treatment option for anon's chronic pain, which was exacerbating their ed symptoms. Diets have been proven over and over again to be unsustainable (and are the leading predictor of eating disorders). So yeah, I felt that it was an inappropriate prescription informed more by bias than actual data.
(And side note: This study on chronic pain and obesity concluded that weight change was not associated with changes of pain intensity.)
If you want to discuss the risk factor for surgery, sure, I think that's an important thing to know - however, most fat people already know this and are informed by their doctors and surgeons of what the risks are beforehand, so I'm not really concerned about people being uninformed about it.
I'm a fat liberation activist, and what I'm concerned about is bias. I'm concerned that there are so many BMI cutoffs in essential surgeries for fat patients, when weight loss is hardly feasible, that creates a barrier to care that disproportionately affects marginalized people with intersecting identities.
It's also important to know that we have very little data around the outcomes of surgery for fat folks that isn't bariatric weight loss surgery.
A new systematic review by researchers in Sydney, Australia, published in the journal Clinical Obesity, suggests that weight loss diets before elective surgery are ineffective in reducing postoperative complications.
CADTH Health Technology Review Body Mass Index as a Measure of Obesity and Cut-Off for Surgical Eligibility made a similar conclusion:
Most studies either found discrepancies between BMI and other measurements or concluded that there was insufficient evidence to support BMI cut-offs for surgical eligibility. The sources explicitly reporting ethical issues related to the use of BMI as a measure of obesity or cut-off for surgical eligibility described concerns around stigma, bias (particularly for racialized peoples), and the potential to create or exacerbate disparities in health care access.
Nicholas Giori MD, PhD Professor of Orthopedic Surgery at Stanford University, a respected leader in TKA and THA shared his thoughts in Elective Surgery in Adult Patients with Excess Weight: Can Preoperative Dietary Interventions Improve Surgical Outcomes? A Systematic Review:
“Obesity is not reversible for most patients. Outpatient weight reduction programs average only 8% body weight loss [1, 10, 29]. Eight percent of patients denied surgery for high BMI eventually reach the BMI cutoff and have total joint arthroplasty [28]. Without a reliable pathway for weight loss, we shouldn’t categorically withhold an operation that improves pain and function for patients in all BMI classes [3, 14, 16] to avoid a risk that is comparable to other risks we routinely accept.
It is not clear that weight reduction prior to surgery reduces risk. Most studies on this topic involve dramatic weight loss from bariatric surgery and have had mixed results [13, 19, 21, 22, 24, 27]. Moderate non-surgical weight loss has thus-far not been shown to affect risk [12]. Though hard BMI cutoffs are well-intended, currently-used BMI cutoffs nearly have the effect of arbitrarily rationing care without medical justification. This is because BMI does not strongly predict complications. It is troubling that the effects are actually not arbitrary, but disproportionately affect minorities, women and patients in low socioeconomic classes. I believe that the decision to proceed with surgery should be based on traditional shared-decision making between the patient and surgeon. Different patients and different surgeons have different tolerances to risk and reward. Giving patients and surgeons freedom to determine the balance that is right for them is, in my opinion, the right way to proceed.”
I agree with Dr. Giori on this. And I absolutely do not judge anyone who chooses to lose weight prior to a surgery. It's upsetting that it is the only option right now for things like safe anesthesia. Unfortunately, patients with a history of disordered eating (which is a significant percentage of fat people!) are left out of the conversation. There is certainly risk involved in either option and it sucks. I am always open to nuanced discussion, and the one thing I remain firm in is that weight loss is not the answer long-term. We should be looking for other solutions in treating fat patients and studying how to make surgery safer. A lot of this could be solved with more comprehensive training and new medical developments instead of continuously trying to make fat people less fat.
660 notes
·
View notes
Text
Listing archived on our website
Summary Background Patient-reported outcomes and cross-sectional evidence show an association between COVID-19 and persistent cognitive problems. The causal basis, longevity and domain specificity of this association is unclear due to population variability in baseline cognitive abilities, vulnerabilities, virus variants, vaccination status and treatment.
Methods Thirty-four young, healthy, seronegative volunteers were inoculated with Wildtype SARS-CoV-2 under prospectively controlled conditions. Volunteers completed daily physiological measurements and computerised cognitive tasks during quarantine and follow-up at 30, 90, 180, 270, and 360 days. Linear modelling examined differences between ‘infected’ and ‘inoculated but uninfected’ individuals. The main cognitive endpoint was the baseline corrected global cognitive composite score across the battery of tasks administered to the volunteers. Exploratory cognitive endpoints included baseline corrected scores from individual tasks. The study was registered on ClinicalTrials.gov with the identifier NCT04865237 and took place between March 2021 and July 2022.
Findings Eighteen volunteers developed infection by qPCR criteria of sustained viral load, one without symptoms and the remainder with mild illness. Infected volunteers showed statistically lower baseline-corrected global composite cognitive scores than uninfected volunteers, both acutely and during follow up (mean difference over all time points = −0.8631, 95% CI = −1.3613, −0.3766) with significant main effect of group in repeated measures ANOVA (F (1,34) = 7.58, p = 0.009). Sensitivity analysis replicated this cross-group difference after controlling for community upper respiratory tract infection, task-learning, remdesivir treatment, baseline reference and model structure. Memory and executive function tasks showed the largest between-group differences. No volunteers reported persistent subjective cognitive symptoms.
Interpretation These results support larger cross sectional findings indicating that mild Wildtype SARS-CoV-2 infection can be followed by small changes in cognition and memory that persist for at least a year. The mechanistic basis and clinical implications of these small changes remain unclear.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator#long covid#covid conscious#covid is not over
110 notes
·
View notes
Text
The Cass Report is fatally flawed in its methodology, and as a result, its recommendations are harmful. Speaking on behalf of TransActual, Keyne Walker said: “It undermines the legal competence of both children and adults to access medical treatment and dismisses almost all existing clinical evidence on trans people’s healthcare by applying impossible evidence standards which, if applied to other medicines would invalidate more than three quarters of the existing treatments used in paediatric care which, like puberty blockers, are currently being prescribed off-label.” The report’s primary conclusions rest on excluding 98% of the relevant evidence on the safety and efficacy of puberty blockers and hormones for lack of blinding and controls. What this means is that they require studies in which some patients are given the treatment, and others are unknowingly given placebos. This is not only a clear breach of medical ethics and monstrous suggestion, but also impossible due to the obviousness of the impacts of puberty blockers and hormones. The report also strays far beyond its scope and competence in recommending a review of adult services and in suggesting that young people ought to stay under the care of children and young people’s services until the age of 25. The latter is based on highly questionable understandings of brain development which have been repeatedly debunked as an oversimplification of the constant changes in human neurology over the course of our lives. This recommendation, especially in a context of an already broken system of care for both adults and children, has the potential to have a significant negative impact on the lives and wellbeing of trans people in the UK. Underpinning this report is the idea that being trans is an undesirable outcome rather than a natural facet of human diversity. This is clear not only from the recommendations but also from the exclusion of trans researchers from the design of the review process and the links individual members of the research team have to anti-trans groups, which the Cass team were warned about. Download the full briefing
234 notes
·
View notes
Note
do you feel like SSRIs are mostly pseudoscience? I'm not sure if I should be open to trying them or avoid them at all costs since I'm not sure if they even work or if they will mess me up permanently
a preliminary note that i don't find the category 'pseudoscience' to be useful & would classify SSRI research more as 'methodologically shoddy science' or 'ideologically slanted' or 'part of a centuries-long effort on the part of psychiatrists to secure themselves professional prestige by claiming neurobiological etiologies where none are shown to exist' &c &c. imo the notion of 'pseudoscience' is itself pretty positivistic, ahistorical, and ideologically noxious (particularly apparent in any analysis of epistemological imperialism).
that aside: you raise two major issues with SSRIs, namely whether they work and whether they will cause you harm.
efficacy of SSRIs is contested. a 2010 meta-analysis found that in patients with mild or moderate depressive symptoms, the efficacy of SSRIs "may be minimal or nonexistent", whilst "for patients with very severe depression, the benefit of medications over placebo is substantial". a 2008 meta-analysis found a similar distinction between mildly vs severely depressed patients, but noted that even in the latter population, drug–placebo differences were "relatively small" and argued that the differences between drug and placebo in severely depressed patients "seems to result from a poorer response to placebo amongst more depressed patients" rather than from a greater efficacy of SSRIs. a 2012 meta-analysis found some SSRIs consistently effective over placebo treatments, but several authors disclosed major relationships with pharmaceutical companies. a 2017 meta-analysis concluded that "SSRIs might have statistically significant effects on depressive symptoms, but all trials were at high risk of bias and the clinical significance seems questionable" (emphasis added) and that "potential small beneficial effects seem to be outweighed by harmful effects".
when evaluating any of this evidence, it is crucial to keep in mind that studies on antidepressant trials are selectively published—that is, they are less likely to be published if they show negative results!
A total of 37 studies viewed by the FDA as having positive results were published; 1 study viewed as positive was not published. Studies viewed by the FDA as having negative or questionable results were, with 3 exceptions, either not published (22 studies) or published in a way that, in our opinion, conveyed a positive outcome (11 studies). According to the published literature, it appeared that 94% of the trials conducted were positive. By contrast, the FDA analysis showed that 51% were positive.
meta-analyses are not immune to this issue, either. in addition to the problem that a meta-analysis of a bunch of bad studies cannot magically 'cancel out' the effects of poor study design, the authors of meta-analyses can and do also have financial interests and ties to pharmaceutical companies, and this affects their results just as it does the results of the studies they are studying. according to a 2016 analysis of antidepressant meta-analyses,
Fifty-four meta-analyses (29%) had authors who were employees of the assessed drug manufacturer, and 147 (79%) had some industry link (sponsorship or authors who were industry employees and/or had conflicts of interest). Only 58 meta-analyses (31%) had negative statements in the concluding statement of the abstract. Meta-analyses including an author who were employees of the manufacturer of the assessed drug were 22-fold less likely to have negative statements about the drug than other meta-analyses [1/54 (2%) vs. 57/131 (44%); P < 0.001]. [...] There is a massive production of meta-analyses of antidepressants for depression authored by or linked to the industry, and they almost never report any caveats about antidepressants in their abstracts. Our findings add a note of caution for meta-analyses with ties to the manufacturers of the assessed products.
so, do SSRIs work? they are certainly psychoactive substances, which is to say, they do something. whether that something reduces depressive symptoms is simply not known at this point, though it is always worth keeping in mind that the 'chemical imbalance' narrative of SSRIs (the idea that they work by 'curing' a 'serotonin deficiency' in the brain) has always been a profitable myth. look, any medical treatment throughout history has been vouched for by SOME patients who report that it helped them—no matter how wacky it sounds or how little evidence there was to support it. this can be for a lot of reasons: placebo effect, the remedy accidentally treating a different problem than it was intended for, the symptoms coincidentally resolving on their own. sometimes the human body is just weird and unpredictable. sometimes remedies work. i'm sorry i can't give you a more definitive answer about whether SSRIs would help you.
as to potential risks: these are significant. SSRIs can precipitate suicidal ideation, a risk that has been consistently downplayed by pharmaceutical companies and studies. SSRIs are also known to contribute to sexual dysfunction and dissatisfaction, again a risk that is minimised and downplayed in much of the literature and in physician communication with patients. further (known) side effects range through emotional blunting, glaucoma, QT interval prolongation, abnormal bleeding & interaction with anti-coagulents, platelet dysfunction, decreases in bone mineral density leading to increased risk of osteopenia and osteoporosis, jaw clenching / TMJ pain, risk of serotonin syndrome when used in conjunction with other serotonergic substances, dizziness, insomnia, headaches, the list goes on.
i don't mean to sound alarmist; all drugs have side effects, some of the ones above occur rarely, and you may very well decide the risk is acceptable to you to take on. i would, though, always encourage you to do thorough research into potential side effects before starting any drug, including an SSRI. more on SSRI side effects in david healy's books 'pharmageddon', 'let them eat prozac', 'the antidepressant era', and 'the creation of psychopharmacology'; 'pillaged' by ronald w maris; and 'the myth of the chemical cure' by joanna moncrieff.
in addition to the above, SSRIs are known to come with a risk of 'discontinuation syndrome'—that is, chemical withdrawal when stopping the drug. this, too, is often downplayed by physicians; many still deny that it can even happen. some patients don't experience it at all, though i can tell you purely anecdotally that SSRI withdrawal was so miserable for me i simply gave up on quitting for over a year, despite the fact that at that point i was already thoroughly experienced with chemical withdrawals from other, 'harder' drugs. again, i am not telling you not to go on SSRIs if you decide these risks are worth it to you! i simply think this is a decision that should always be made with full knowledge (indeed, this is a core, though routinely violated, principle of medical 'informed consent').
ultimately this is not a decision anyone should make for you; it's your body and mind that are at stake here. as always i think that anyone considering any kind of medical treatment should have full knowledge about it and should be making all decisions freely and autonomously. i am genuinely not pushing any agenda 'for' or 'against' SSRIs, only against prescription of them that is done carelessly, coercively, or without fully informing patients of what risks they're taking on and what benefits they can hope to see.
529 notes
·
View notes
Text
You have covid
"I'm sure it's just a flu"
Flu:

Covid:


"I tested negative for covid"

"It's not so bad cuz hardly anybody dies of covid anymore anyway"

(Note, this ^ study's scope was for the 'core' of the pandemic (I.e. the first 2-3 years), but still has implications today)

"I'm young and healthy so I don't have to worry"





Take covid seriously, or else
Sources:
78 notes
·
View notes
Text
With the Alberta government announcing a ban on gender-affirming care until 16 years old, let’s take a minute to correct some misinformation using peer-reviewed publications. A thread.🧵
“High quality evidence doesn’t support gender-affirming care.”
‘High quality evidence’ is a technical term that essentially just means ’no randomized controlled trials.’ RCTs are not scientifically feasible for trans youth care and would be unethical (link).
The evidence-base for gender-affirming care is quite robust and is at least as good at the evidence base for comparable interventions like abortion and birth control. For an overview of available studies, albeit already few years outdated, see page 144 onwards (link).
“Over 80% of kids grow out of being trans.”
That’s just not true. The claim is based on old, poor-quality studies that included tons of kids who never claimed to be trans (link).
But even if we took the percentage at face value, it would be irrelevant since it’s based on pre-pubertal data and virtually all the so-called ‘desistance’ occurred before puberty, when gender-affirming care becomes available (link).
More recent, better studies suggest that only around 2.5% have ‘grown out of it’ after 5 years (link).
“Kids falsely believe that they are trans because of social contagion.”
There is no evidence for that claim. It’s based on the reports of transphobic parents who were surprised that their kid came out ‘out of the blue’ and happened to have trans friends, as trans kids tend to do. For a careful explanation of why the claim is completely unsupported by evidence, see this (link).
Studies of trans youth that used clinical data to look into the claim have also failed to find any evidence of epidemic or large-scale social contagion (link).
“We need a years-long diagnostic process to make sure kids are ‘truly’ trans before they transition.”
There is no evidence that gender assessments fare any better than self-report at predicting future outcomes, as we explain in our recent review (link).
“Gender-exploratory therapy can help identify the trauma that made these kids gender dysphoric.”
Gender-exploratory therapy is extremely difficult to distinguish from classic conversion therapy, which also starts from the premise that ‘trauma’ makes people LGBTQ2S+ (link).
Since conversion therapy is known to be harmful, we have reasons to believe that gender-exploratory therapy would be as well.
Self-directed exploration is good. Forced exploration rooted in suspicion towards trans identities isn’t. If you’re starting from the belief that trans identities are inherently suspicious, you’re not doing therapy, you’re doing transphobia.
Any more myths about gender-affirming care you’d like me to bust, Tumblr?
#transgender#trans#lgbtq#lgbtqia#queer#lgbt#gender affirming care#gender affirming healthcare#trans healthcare#science#misinformation
254 notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.
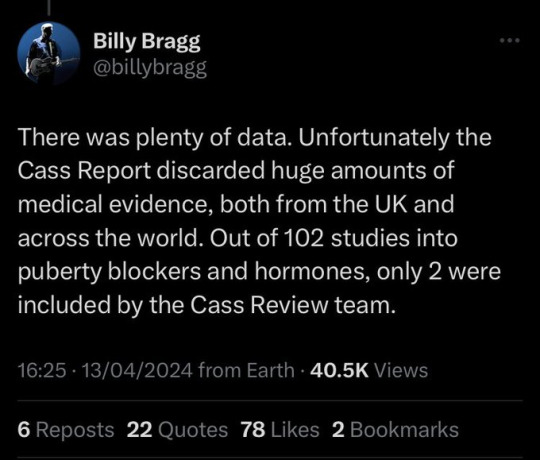

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
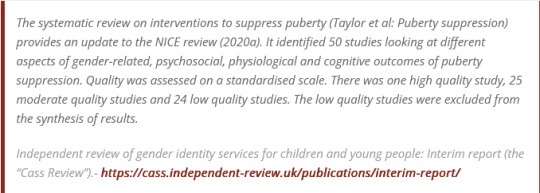
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
103 notes
·
View notes
Text
"I’m going to let him go wild on health,” former president Donald Trump said of Robert F. Kennedy Jr. at his Madison Square Garden rally in New York City this past weekend. “I’m going to let him go wild on the food. I’m going to let him go wild on the medicines.”
Kennedy, a former Democrat, suspended his presidential campaign in August and endorsed Trump. He has since launched the Make America Healthy Again campaign, an initiative focused on tackling chronic diseases that Trump has seemingly embraced in recent weeks. Given Kennedy’s anti-vaccination stance and conspiratorial leanings, some policy experts and former government officials are concerned about how his views could shape the nation’s health agenda.
Kennedy has long made false statements about the safety of vaccines and has touted disproven treatments for Covid-19, including ivermectin and hydroxychloroquine. On the campaign trail, he has railed against seed oils, blaming several chronic health conditions on their presence in processed foods.
How much influence Kennedy could have on national health policy will all depend on his role within a future Trump administration. Trump did not clarify his remarks at Sunday’s event, including what position he is considering Kennedy for. According to a CNN report that ran late Tuesday, Kennedy said Trump “promised him control of the public health agencies,” but in an email to WIRED on Wednesday, Steven Cheung, Trump’s campaign communications director, said that formal discussions of who will serve in a second Trump administration are premature.
Trump could be considering Kennedy to lead the Department of Health and Human Services, which has 80,000 federal employees, or one of the agencies within it, such as the Food and Drug Administration or the Centers for Disease Control and Prevention. It would be a departure from his previous top health picks, who had lengthy government or public health careers. For instance, Alex Azar, Trump’s HHS secretary, was deputy HHS secretary under George W. Bush and an executive at drugmaker Eli Lilly. Scott Gottlieb, a physician and investor appointed as FDA commissioner under Trump, had previously worked for the FDA and had served on the boards of pharma and biotech companies.
When asked to elaborate on Kennedy’s health priorities, Amaryllis Fox Kennedy, the former candidate’s campaign director and daughter-in-law, told WIRED: “Bobby aims to end conflicts and corruption at the agencies, ensure all testing is undertaken by scientists who have no financial interest in the outcome, and all results of all trials are released to the public. The free market will take care of it from there.” (The National Institutes of Health already requires results of clinical trials funded by the agency to be published to a government database.)
Jerome Adams, US surgeon general under Trump and current executive director of health equity initiatives at Purdue University, says that even if Kennedy were tapped to lead HHS, the FDA, or the CDC, it’s unlikely that he would ascend to one of those roles due to his lack of medical training and controversial views on public health issues. “Congressional approval is required for these positions, and his stances could be a barrier,” Adams says.
If Republicans control the Senate after next week’s election, though, that calculus could change. “The GOP has generally fallen into line in terms of supporting candidates that President Trump does,” says Genevieve Kanter, associate professor of public policy at the University of Southern California.
If chosen to be FDA commissioner, Kennedy would control the agency’s budget and priorities and could have a sizable impact by installing lower-level appointees who are sympathetic to his worldview. While the FDA commissioner does not single-handedly approve or authorize new drugs, Kantner says outside political pressure can certainly influence that process. Kennedy could also appoint members to FDA advisory committees, panels of outside experts that make recommendations to the agency on drug approvals and other regulatory matters. The FDA often follows the recommendations of advisory committees when making decisions on new drug approvals, but not always.
The FDA can also choose to not enforce some rules in certain circumstances—what’s known as enforcement discretion. Given his support for dubious and unproven therapies, such as stem cells and hyperbaric oxygen, an FDA under Kennedy, for instance, could choose to not go after companies that market unapproved treatments.
“When we think of the kind of person we want to be head of HHS or be FDA commissioner, someone ‘going wild’ isn’t exactly the first trait that comes to mind,” Kanter says. “It wouldn’t ease the public’s concern that we would see more food safety incidents and adverse events from poorly regulated drugs and devices from a lax administration that is known for embracing unscientific theories.”
Kennedy wouldn’t have free rein though. Existing laws and regulations govern how the agency works, and a new FDA commissioner wouldn’t be able to get rid of those quickly. “If you’re dealing with regulatory issues that have been long-standing and have lots of precedent, it’s just not possible to turn some of those things around or dismiss them overnight,” says a past leader of the FDA, who requested anonymity so that they could speak freely.
Likewise, even in a leadership role at HHS or the CDC, Kennedy wouldn’t be able to easily affect vaccine policy. Vaccine recommendations are made by the Advisory Committee on Immunization Practices, which comprises outside medical and public health experts. Georges Benjamin, executive director of the American Public Health Association, says Kennedy could try to stack that advisory committee with people who are sympathetic to his views on vaccination, but those members are chosen through a rigorous nomination process.
“He could certainly change policy that way, but it takes a while and it won't be a secret. There are ways in which the public can push back, including taking a case to court,” he says.
Kennendy could have influence in other ways beyond direct control of a public health agency. Trump could potentially bring Kennedy on as a White House adviser, which wouldn’t require approval by the Senate.
“Without congressional vetting and oversight, there is potential for unchecked impact. RFK's views could shape health policies, raising concerns about misinformation and harm,” Adams says.
Karoline Leavitt, national press secretary for the Trump campaign, told WIRED in an email that if reelected, Trump will establish a “special Presidential Commission of independent minds and will charge them with investigating what is causing the decades-long increase in chronic illnesses.” She did not say whether Kennedy would be chosen for that task force.
Kennedy has also been sizing himself up for another position in a potential Trump cabinet: agriculture secretary. A longtime environmental activist, Kennedy has promised to take on big farms and feedlots, reduce pesticides, and fix what he presents as a food system captured by corporate interests. “When Donald Trump gets me inside,” Kennedy said in a video shot outside the Department of Agriculture headquarters in Washington, DC, “it won’t be that way any more.”
This platform is a continuation of Kennedy’s long history as an antagonist against the agriculture industry. In 2018, Kennedy and a team of attorneys won an initial $289 million settlement against Monsanto, representing a groundskeeper who developed cancer after being soaked with a herbicide made by the agrochemical firm. He also attempted to sue the pig farming company Smithfield because of its production of hog manure, although that case was thrown out by a federal judge.
Kennedy’s past makes him an unlikely candidate for agriculture secretary, according to Daniel Glickman, who served in the role during Bill Clinton’s presidency. “It’s hard for me to imagine, given Trump’s traditional base in the heartlands, that he would pick somebody who was an advocate for breaking up large farms and breaking consolidated agriculture,” says Glickman.
Like top posts at HHS, the USDA secretary position would need to be confirmed by a Senate vote. “I don’t think [Kennedy] is a slam dunk,” says Glickman.
Trump’s pick for USDA chief during his first term was Sonny Perdue, a former governor of Georgia and founder of an agricultural trading company. Most agriculture secretaries either have a background in the industry or politics—two crucial constituencies for the person who will be in charge of a department that employs nearly 100,000 and is made up of 29 agencies, including forestry, conservation, and nutrition programs. “The difference between Sonny Perdue and Robert F. Kennedy, Jr. is like night and day,” says Glickman.
If Kennedy were to be confirmed as agriculture secretary, he might struggle to enact the most radical parts of his program. He is an outspoken critic of pesticides, but the USDA is generally not in charge of regulating those, says Dan Blaustein-Rejto, director of agriculture policy and research at the Breakthrough Institute. Rather, the EPA regulates pesticides with public health uses.
Although he may not be able to directly influence pesticide regulations, Kennedy has said he would try to “weaponize” other agencies against “chemical agriculture” by commissioning scientific research into the effects of pesticides. The USDA Agricultural Research Service has a nearly $2 billion discretionary budget for research into crops, livestocks, nutrition, food safety, and natural resources conservation.
There are other levers that an agriculture secretary could pull, says Blaustein-Rejto. The USDA is investing $3 billion through the partnership for climate-smart commodities—a scheme that’s supposed to make US agriculture more climate-friendly. A USDA chief might be able to put their thumb on their scale by influencing the selection criteria for these kinds of programs. The USDA also oversees the Commodity Credit Corporation (CCC), which has a $5 billion fund that it uses to support farm incomes and conservation programs, and to assist farmers hit by natural disasters. It’s possible that a USDA chief could influence how these CCC funds are distributed by the agency.
Kennedy has also argued that corporate interests have captured the US’s dietary guidelines, and he pledged to remove conflicts of interest from USDA groups that come up with dietary guidelines. US dietary guidelines are developed jointly by the USDA and HHS and are updated every five years, giving the agriculture secretary limited opportunities to influence any recommendations.
“If RFK is in a high-level policy role, I expect to see a lot more talk about ultra-processed foods, but I’m not sure what that would actually entail when it comes to the dietary guidelines,” says Blaustein-Rejto.
The experts WIRED spoke with largely think Kennedy’s more extreme positions will likely be constrained by bureaucracy. But the message that elevating a vocal vaccine skeptic and conspiracy theorist would send remains a serious concern ahead of a potential second Trump administration.
28 notes
·
View notes