#cbt works for a reason. therapy works for a reason. they are teaching you skills that YOU utilize to improve your life
Text
sometimes i talk myself out of thinking i have adhd, but then i look at the diagnostic criteria again and i have adhd
#i hope the doctor i’m seeing isn’t dismissive like the last psychologist i saw was#that was genuinely kind of traumatic bc i felt like i was being gaslighted#like even if it’s not adhd i’m having PROBLEMS. help me in STRUGGLING and don’t know how to fix it#most validating moment of the year goes to when i mentioned testing to my PCP and he said ‘oh go to a third party our in house psychology#dept sucks’ (which is where the Bad Psychologist was from)#i mean i was in a really really bad place and he gave me a fucking book. about how to train my brain to be happier#i mean i’m all for taking charge of your mental health#cbt works for a reason. therapy works for a reason. they are teaching you skills that YOU utilize to improve your life#and a book can teach you those skills#but it should’ve been so fucking obvious that that was not what i needed at that time#fuck you dr. fish 🖕
6 notes
·
View notes
Text
the funniest thing about the batfamily is that they're so smart but they all have zero introspection skills.
the batfamily is smart. so smart. and they deal with the mentally ill population all the time. and most of the time they treat them good! they help them!
i find it absolutely impossible that bruce isn't educated on psychology. there's no way he isn't. no way he hasn't studied psychology, whether it was to understand the joker or any other villains, whether it was to learn how to instill fear, practice for going undercover, hostage negotiation, how to tell the difference between mental health issues and just violent criminals (because he wouldn't know which ones he could talk sense into without understanding why they were doing it), whether it was to learn better methods of interrogation, or even just an interest in how the brain works.
and i guarantee most of the other batkids are too. bruce had to have taught them that so they could learn how to go undercover or how to tell whenever violence is necessary or if you can just talk them down.
dick has a law degree, which means he had to do undergrad. i think it's insane to think that he wouldn't have taken a psychology class. he also was able to understand damian and how to handle him, and he wouldn't be able to do that if he wasn't aware of how his upbringing would've shaped his neural pathways.
tim has a genius level iq. no way he doesn't understand how the brain works. also, he was able to tell that bruce was in a terrible mental state just by observing him as batman, where bruce does everything in his power to hide his emotions. he's also, several times, shown to be one of the only if the not the only batfamily member to understand why jason acts the way he does.
damian likely isn't terribly empathetic to mental health issues. probably a little more now, but not very. but like. he might not be empathetic to it but there's no way he doesn't understand how it works. how the frontal lobe works. how the amygdala works. how to manipulate someone.
stephanie was in college, and just like i said with dick, i find it hard to believe she wouldn't have taken a psychology class.
cass is cass. enough said.
also!! they all have a pretty good relationship with leslia thompkins!! a psychologist!!
all this to say: how on God's green earth do none of them realize they need therapy.
and like i get why. bruce has suppressed his emotions so much that he genuinely think he's fine. dick is too focused on being a support for everyone to worry about himself. jason and stephanie push it all down. cass, and this is not a diss because i love her, would realistically be very emotionally stunted. damian wasn't raised to be empathetic to the mentally ill and even if he was, he's 15. his frontal lobe is so not developed. plus the trauma they've all endured? the training they've had from bruce, who probably wasn't that concerned about teaching them self care and most definitely taught them to put their emotions aside. so like i get it. but also.
they know all this stuff and??? don't for a single second (except for tim that one time) be like "hmmm i could benefit from CBT and EMDR"
except duke.
how is duke the only one who's like "yeah. you guys aren't okay." duke knows. he tries to reason with them and has several times been like "you guys are crazy. why are you chill with this."




which is all to say. i'm convinced that at some point duke is going to try to sit them all down and be like "you guys need therapy. please go to therapy. I'm begging you."
#i know that the whole “duke is the voice of reason” is kinda more fanon than anything bc he has to be crazy too to be a vigilante#but im convinced he's self aware of it#and is like wow#you guys are#so traumatized#batfamily#batfam#dick grayson#nightwing#damian wayne#robin#jason todd#red hood#tim drake#red robin
635 notes
·
View notes
Text

By: Jon Haidt
Published: Mar 9, 2023
In May 2014, Greg Lukianoff invited me to lunch to talk about something he was seeing on college campuses that disturbed him. Greg is the president of FIRE (the Foundation for Individual Rights and Expression), and he has worked tirelessly since 2001 to defend the free speech rights of college students. That almost always meant pushing back against administrators who didn’t want students to cause trouble, and who justified their suppression of speech with appeals to the emotional “safety” of students—appeals that the students themselves didn’t buy. But in late 2013, Greg began to encounter new cases in which students were pushing to ban speakers, punish people for ordinary speech, or implement policies that would chill free speech. These students arrived on campus in the fall of 2013 already accepting the idea that books, words, and ideas could hurt them. Why did so many students in 2013 believe this, when there was little sign of such beliefs in 2011?
Greg is prone to depression, and after hospitalization for a serious episode in 2007, Greg learned CBT (Cognitive Behavioral Therapy). In CBT you learn to recognize when your ruminations and automatic thinking patterns exemplify one or more of about a dozen “cognitive distortions,” such as catastrophizing, black-and-white thinking, fortune telling, or emotional reasoning. Thinking in these ways causes depression, as well as being a symptom of depression. Breaking out of these painful distortions is a cure for depression.
What Greg saw in 2013 were students justifying the suppression of speech and the punishment of dissent using the exact distortions that Greg had learned to free himself from. Students were saying that an unorthodox speaker on campus would cause severe harm to vulnerable students (catastrophizing); they were using their emotions as proof that a text should be removed from a syllabus (emotional reasoning). Greg hypothesized that if colleges supported the use of these cognitive distortions, rather than teaching students skills of critical thinking (which is basically what CBT is), then this could cause students to become depressed. Greg feared that colleges were performing reverse CBT.
I thought the idea was brilliant because I had just begun to see these new ways of thinking among some students at NYU. I volunteered to help Greg write it up, and in August 2015 our essay appeared in The Atlantic with the title: The Coddling of the American Mind. Greg did not like that title; his original suggestion was “Arguing Towards Misery: How Campuses Teach Cognitive Distortions.” He wanted to put the reverse CBT hypothesis in the title.
After our essay came out, things on campus got much worse. The fall of 2015 marked the beginning of a period of protests and high-profile conflicts on campus that led many or most universities to implement policies that embedded this new way of thinking into campus culture with administrative expansions such as “bias response teams” to investigate reports of “microaggressions.” Surveys began to show that most students and professors felt that they had to self-censor. The phrase “walking on eggshells” became common. Trust in higher ed plummeted, along with the joy of intellectual discovery and sense of goodwill that had marked university life throughout my career.
Greg and I decided to expand our original essay into a book in which we delved into the many causes of the sudden change in campus culture. Our book focused on three “great untruths” that seemed to be widely believed by the students who were trying to shut down speech and prosecute dissent:
1. What doesn’t kill you makes you weaker
2. Always trust your feelings
3. Life is a battle between good people and evil people.
Each of these untruths was the exact opposite of a chapter in my first book, The Happiness Hypothesis, which explored ten Great Truths passed down to us from ancient societies east and west. We published our book in 2018 with the title, once again, of The Coddling of the American Mind. Once again, Greg did not like the title. He wanted the book to be called “Disempowered,” to capture the way that students who embrace the three great untruths lose their sense of agency. He wanted to capture reverse CBT.
The Discovery of the Gender-by-Politics Interaction
In September 2020, Zach Goldberg, who was then a graduate student at Georgia State University, discovered something interesting in a dataset made public by Pew Research. Pew surveyed about 12,000 people in March 2020, during the first month of the Covid shutdowns. The survey included this item: “Has a doctor or other healthcare provider EVER told you that you have a mental health condition?” Goldberg graphed the percentage of respondents who said “yes” to that item as a function of their self-placement on the liberal-conservative 5-point scale and found that white liberals were much more likely to say yes than white moderates and conservatives. (His analyses for non-white groups generally found small or inconsistent relationships with politics.)
I wrote to Goldberg and asked him to redo it for men and women separately, and for young vs. old separately. He did, and he found that the relationship to politics was much stronger for young (white) women. You can see Goldberg’s graph here, but I find it hard to interpret a three-way interaction using bar charts, so I downloaded the Pew dataset and created line graphs, which make it easier to interpret.
Here’s the same data, showing three main effects: gender (women higher), age (youngest groups higher), and politics (liberals higher). The graphs also show three two-way interactions (young women higher, liberal women higher, young liberals higher). And there’s an important three-way interaction: it is the young liberal women who are highest. They are so high that a majority of them said yes, they had been told that they have a mental health condition.

Figure 1. Data from Pew Research, American Trends Panel Wave 64. The survey was fielded March 19-24, 2020. Graphed by Jon Haidt.
In recent weeks—since the publication of the CDC’s report on the high and rising rates of depression and anxiety among teens—there has been a lot of attention to a different study that shows the gender-by-politics interaction: Gimbrone, Bates, Prins, & Keyes (2022), titled: “The politics of depression: Diverging trends in internalizing symptoms among US adolescents by political beliefs.” Gimbrone et al. examined trends in the Monitoring the Future dataset, which is the only major US survey of adolescents that asks high school students (seniors) to self-identify as liberal or conservative (using a 5-point scale). The survey asks four items about mood/depression. Gimbrone et al. found that prior to 2012 there were no sex differences and only a small difference between liberals and conservatives. But beginning in 2012, the liberal girls began to rise, and they rose the most. The other three groups followed suit, although none rose as much, in absolute terms, as did the liberal girls (who rose .73 points since 2010, on a 5-point scale where the standard deviation is .89).

Figure 2. Data from Monitoring the Future, graphed by Gimbrone et al. (2022). The scale runs from 1 (minimum) to 5 (maximum).
The authors of the study try to explain the fact that liberals rise first and most in terms of the terrible things that conservatives were doing during Obama’s second term, e.g.,
Liberal adolescents may have therefore experienced alienation within a growing conservative political climate such that their mental health suffered in comparison to that of their conservative peers whose hegemonic views were flourishing.
The progressive New York Times columnist Michelle Goldberg took up the question and wrote a superb essay making the argument that teen mental health is not and must not become a partisan issue. She dismissed Gimbrone et al.’s explanation as having a poor fit with their own data:
Barack Obama was re-elected in 2012. In 2013, the Supreme Court extended gay marriage rights. It was hard to draw a direct link between that period’s political events and teenage depression, which in 2012 started an increase that has continued, unabated, until today.
After examining the evidence, including the fact that the same trends happened at the same time in Britain, Canada, and Australia, Goldberg concluded that “Technology, not politics, was what changed in all these countries around 2012. That was the year that Facebook bought Instagram and the word “selfie” entered the popular lexicon.”
Journalist Matt Yglesias also took up the puzzle of why liberal girls became more depressed than others, and in a long and self-reflective Substack post, he described what he has learned about depression from his own struggles involving many kinds of treatment. Like Michelle Goldberg, he briefly considered the hypothesis that liberals are depressed because they’re the only ones who see that “we’re living in a late-stage capitalist hellscape during an ongoing deadly pandemic w record wealth inequality, 0 social safety net/job security, as climate change cooks the world,” to quote a tweet from the Washington Post tech columnist Taylor Lorenz. Yglesias agreed with Goldberg and other writers that the Lorenz explanation—reality makes Gen Z depressed—doesn’t fit the data, and, because of his knowledge of depression, he focused on the reverse path: depression makes reality look terrible. As he put it: “Mentally processing ambiguous events with a negative spin is just what depression is.”
Yglesias tells us what he has learned from years of therapy, which clearly involved CBT:
It’s important to reframe your emotional response as something that’s under your control:
• Stop saying “so-and-so made me angry by doing X.”
• Instead say “so-and-so did X, and I reacted by becoming angry.”
And the question you then ask yourself is whether becoming angry made things better? Did it solve the problem?
Yglesias wrote that “part of helping people get out of their trap is teaching them not to catastrophize.” He then described an essay by progressive journalist Jill Filipovic that argued, in Yglesias’s words, that “progressive institutional leaders have specifically taught young progressives that catastrophizing is a good way to get what they want.”
Yglesias quoted a passage from Filipovic that expressed exactly the concern that Greg had expressed to me back in 2014:
I am increasingly convinced that there are tremendously negative long-term consequences, especially to young people, coming from this reliance on the language of harm and accusations that things one finds offensive are “deeply problematic” or even violent. Just about everything researchers understand about resilience and mental well-being suggests that people who feel like they are the chief architects of their own life — to mix metaphors, that they captain their own ship, not that they are simply being tossed around by an uncontrollable ocean — are vastly better off than people whose default position is victimization, hurt, and a sense that life simply happens to them and they have no control over their response.
I have italicized Filipovic’s text about the benefits of feeling like you captain your own ship because it points to a psychological construct with a long history of research and measurement: Locus of control. As first laid out by Julian Rotter in the 1950s, this is a malleable personality trait referring to the fact that some people have an internal locus of control—they feel as if they have the power to choose a course of action and make it happen, while other people have an external locus of control—they have little sense of agency and they believe that strong forces or agents outside of themselves will determine what happens to them. Sixty years of research show that people with an internal locus of control are happier and achieve more. People with an external locus of control are more passive and more likely to become depressed.
How a Phone-Based Childhood Breeds Passivity
There are at least two ways to explain why liberal girls became depressed faster than other groups at the exact time (around 2012) when teens traded in their flip phones for smartphones and the girls joined Instagram en masse. The first and simplest explanation is that liberal girls simply used social media more than any other group. Jean Twenge’s forthcoming book, Generations, is full of amazing graphs and insightful explanations of generational differences. In her chapter on Gen Z, she shows that liberal teen girls are by far the most likely to report that they spend five or more hours a day on social media (31% in recent years, compared to 22% for conservative girls, 18% for liberal boys, and just 13% for conservative boys). Being an ultra-heavy user means that you have less time available for everything else, including time “in real life” with your friends. Twenge shows in another graph that from the 1970s through the early 2000s, liberal girls spent more time with friends than conservative girls. But after 2010 their time with friends drops so fast that by 2016 they are spending less time with friends than are conservative girls. So part of the story may be that social media took over the lives of liberal girls more than any other group, and it is now clear that heavy use of social media damages mental health, especially during early puberty.
But I think there’s more going on here than the quantity of time on social media. Like Filipovic, Yglesias, Goldberg, and Lukianoff, I think there’s something about the messages liberal girls consume that is more damaging to mental health than those consumed by other groups.
The Monitoring the Future dataset happens to have within it an 8-item Locus of Control scale. With Twenge’s permission, I reprint one such graph from Generations showing responses to one of the items: “Every time I try to get ahead, something or somebody stops me.” This item is a good proxy for Filipovic’s hypothesis about the disempowering effects of progressive institutions. If you agree with that item, you have a more external locus of control. As you can see in Figure 3, from the 1970s until the mid-2000s, boys were a bit more likely to agree with that item, but then girls rose to match boys, and then both sexes rose continuously throughout the 2010s—the era when teen social life became far more heavily phone-based.
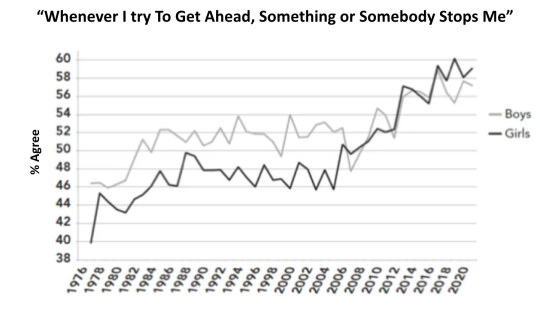
Figure 3. Percentage of boys and girls (high school seniors) who agree with (or are neutral about) the statement “Every time I try to get ahead, something or somebody stops me.” From Monitoring the Future, graphed by Jean Twenge in her forthcoming book Generations.
When the discussion of the gender-by-politics interaction broke out a few weeks ago, I thought back to Twenge’s graph and wondered what would happen if we broke up the sexes by politics. Would it give us the pattern in the Gimbrone et al. graphs, where the liberal girls rise first and most? Twenge sent me her data file (it’s a tricky one to assemble, across the many years), and Zach Rausch and I started looking for the interaction. We found some exciting hints, and I began writing this post on the assumption that we had a major discovery. For example, Figure 4 shows the item that Twenge analyzed. We see something like the Gimbrone et al. pattern in which it’s the liberal girls who depart from everyone else, in the unhealthy (external) direction, starting in the early 2000s.

Figure 4. Percentage of liberal and conservative high school senior boys (left panel) and girls (right panel) who agree with the statement “Every time I try to get ahead, something or somebody stops me.” From Monitoring the Future, graphed by Zach Rausch.
It sure looks like the liberal girls are getting more external while the conservative girls are, if anything, trending slightly more internal in the last decade, and the boys are just bouncing around randomly. But that was just for this one item. We also found a similar pattern for a second item, “People like me don’t have much of a chance at a successful life.” (You can see graphs of all 8 items here.)
We were excited to have found such clear evidence of the interaction, but when we plotted responses to the whole scale, we found only a hint of the predicted interaction, and only in the last few years, as you can see in Figure 5. After trying a few different graphing strategies, and after seeing if there was a good statistical justification for dropping any items, we reached the tentative conclusion that the big story about locus of control is not about liberal girls, it’s about Gen Z as a whole. Everyone—boys and girls, left and right—developed a more external locus of control gradually, beginning in the 1990s. I’ll come back to this finding in future posts as I explore the second strand of the After Babel Substack: the loss of “play-based childhood” which happened in the 1990s when American parents (and British, and Canadian) stopped letting their children out to play and explore, unsupervised. (See Frank Furedi’s important book Paranoid Parenting. I believe that the loss of free play and self-supervised risk-taking blocked the development of a healthy, normal, internal locus of control. That is the reason I teamed up with Lenore Skenazy, Peter Gray, and Daniel Shuchman to found LetGrow.org.)
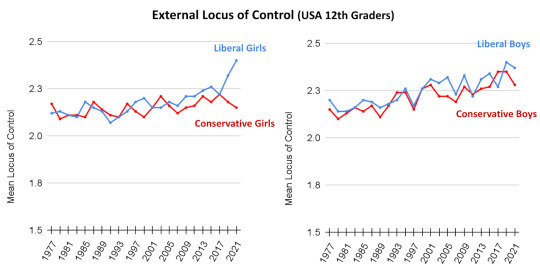
Figure 5. Locus of Control has shifted slightly but steadily toward external since the 1990s. Scores are on a 5-point scale from 1 = most internal to 5 = most external.
We kept looking in the Monitoring the Future dataset and the Gimbrone et al. paper for other items that would allow us to test Filipovic’s hypothesis. We found an ideal second set of variables: The Monitoring the Future dataset has a set of items on “self derogation” which is closely related to disempowerment, as you can see from the four statements that comprise the scale:
I feel I do not have much to be proud of.
Sometimes I think I am no good at all.
I feel that I can't do anything right.
I feel that my life is not very useful.
Gimbrone et al. had graphed the self-derogation scale, as you can see in their appendix (Figure A.4). But Zach and I re-graphed the original data so that we could show a larger range of years, from 1977 through 2021. As you can see in Figure 6, we find the gender-by-politics interaction. Once again, and as with nearly all of the mental health indicators I examined in a previous post, there’s no sign of trouble before 2010. But right around 2012 the line for liberal girls starts to rise. It rises first, and it rises most, with liberal boys not far behind (as in Gimbrone et al.).

Figure 6. Self-derogation scale, averaging four items from the Monitoring the Future study. Graphed by Zach Rausch. The scale runs from 1 (strongly disagree with each statement) to 5 (strongly agree).
In other words, we have support for Filipovic’s “captain their own ship” concern, and for Lukianoff’s disempowerment concern: Gen Z has become more external in its locus of control, and Gen Z liberals (of both sexes) have become more self-derogating. They are more likely to agree that they “can’t do anything right.” Furthermore, most of the young people in the progressive institutions that Filipovic mentioned are women, and that has become even more true since 2014 when, according to Gallup data, young women began to move to the left while young men did not move either way. As Gen Z women became more progressive and more involved in political activism in the 2010s, it seems to have changed them psychologically. It wasn’t just that their locus of control shifted toward external—that happened to all subsets of Gen Z. Rather, young liberals (including young men) seem to have taken into themselves the specific depressive cognitions and distorted ways of thinking that CBT is designed to expunge.
But where did they learn to think this way? And why did it start so suddenly around 2012 or 2013, as Greg observed, and as Figures 2 and 6 confirm?
Tumblr Was the Petri Dish for Disempowering Beliefs
I recently listened to a brilliant podcast series, The Witch Trials of J. K. Rowling, hosted by Megan Phelps-Roper, created within Bari Weiss’s Free Press. Phelps-Roper interviews Rowling about her difficult years developing the Harry Potter stories in the early 1990s, before the internet; her rollout of the books in the late 90s and early 2000s, during the early years of the internet; and her observations about the Harry Potter superfan communities that the internet fostered. These groups had streaks of cruelty and exclusion in them from the beginning, along with a great deal of love, joy, and community. But in the stunning third episode, Phelps-Roper and Rowling take us through the dizzying events of the early 2010s as the social media site Tumblr exploded in popularity (reaching its peak in early 2014), and also in viciousness. Tumblr was different from Facebook and other sites because it was not based on anyone’s social network; it brought together people from anywhere in the world who shared an interest, and often an obsession.
Phelps-Roper interviewed several experts who all pointed to Tumblr as the main petri dish in which nascent ideas of identity, fragility, language, harm, and victimhood evolved and intermixed. Angela Nagle (author of Kill All Normies) described the culture that emerged among young activists on Tumblr, especially around gender identity, in this way:
There was a culture that was encouraged on Tumblr, which was to be able to describe your unique non-normative self… And that’s to some extent a feature of modern society anyway. But it was taken to such an extreme that people began to describe this as the snowflake [referring to the idea that each snowflake is unique], the person who constructs a totally kind of boutique identity for themselves, and then guards that identity in a very, very sensitive way and reacts in an enraged way when anyone does not respect the uniqueness of their identity.
Nagle described how on the other side of the political spectrum, there was “the most insensitive culture imaginable, which was the culture of 4chan.” The communities involved in gender activism on Tumblr were mostly young progressive women while 4Chan was mostly used by right-leaning young men, so there was an increasingly gendered nature to the online conflict. The two communities supercharged each other with their mutual hatred, as often happens in a culture war. The young identity activists on Tumblr embraced their new notions of identity, fragility, and trauma all the more tightly, increasingly saying that words are a form of violence, while the young men on 4chan moved in the opposite direction: they brandished a rough and rude masculinity in which status was gained by using words more insensitively than the next guy. It was out of this reciprocal dynamic, the experts on the podcast suggest, that today’s cancel culture was born in the early 2010s. Then, in 2013, it escaped from Tumblr into the much larger Twitterverse. Once on Twitter, it went national and even global (at least within the English-speaking countries), producing the mess we all live with today.
I don’t want to tell that entire story here; please listen to the Witch Trials podcast for yourself. It is among the most enlightening things I’ve read or heard in all my years studying the American culture war (along with Jon Ronson’s podcast Things Fell Apart). I just want to note that this story fits perfectly with both the timing and the psychology of Greg’s reverse CBT hypothesis.
Implications and Policy Changes
In conclusion, I believe that Greg Lukianoff was exactly right in the diagnosis he shared with me in 2014. Many young people had suddenly—around 2013—embraced three great untruths:
They came to believe that they were fragile and would be harmed by books, speakers, and words, which they learned were forms of violence (Great Untruth #1).
They came to believe that their emotions—especially their anxieties—were reliable guides to reality (Great Untruth #2).
They came to see society as comprised of victims and oppressors—good people and bad people (Great Untruth #3).
Liberals embraced these beliefs more than conservatives. Young liberal women adopted them more than any other group due to their heavier use of social media and their participation in online communities that developed new disempowering ideas. These cognitive distortions then caused them to become more anxious and depressed than other groups. Just as Greg had feared, many universities and progressive institutions embraced these three untruths and implemented programs that performed reverse CBT on young people, in violation of their duty to care for them and educate them.
I welcome challenges to this conclusion from scholars, journalists, and subscribers, and I will address such challenges in future posts. I must also repeat that I don’t blame everything on smartphones and social media; the other strand of my story is the loss of play-based childhood, with its free play and self-governed risk-taking. But if this conclusion stands (along with my conclusions in previous posts), then I think there are two big policy changes that should be implemented as soon as possible:
1) Universities and other schools should stop performing reverse CBT on their students
As Greg and I showed in The Coddling of the American Mind, most of the programs put in place after the campus protests of 2015 are based on one or more of the three Great Untruths, and these programs have been imported into many K-12 schools. From mandatory diversity training to bias response teams and trigger warnings, there is little evidence that these programs do what they say they do, and there are some findings that they backfire. In any case, there are reasons, as I have shown, to worry that they teach children and adolescents to embrace harmful, depressogenic cognitive distortions.
One initiative that has become popular in the last few years is particularly suspect: efforts to tell college students to avoid common English words and phrases that are said to be “harmful.” Brandeis University took the lead in 2021 with its “oppressive language list.” Brandeis urged its students to stop saying that they would “take a stab at” something because it was unnecessarily violent. For the same reason, they urged that nobody ask for a “trigger warning” because, well, guns. Students should ask for “content warnings” instead, to keep themselves safe from violent words like “stab.” Many universities have followed suit, including Colorado State University, The University of British Columbia, The University of Washington, and Stanford, which eventually withdrew its “harmful language list” because of the adverse publicity. Stanford had urged students to avoid words like “American,” “Immigrant,” and “submit,” as in “submit your homework.” Why? because the word “submit” can “imply allowing others to have power over you.” The irony here is that it may be these very programs that are causing liberal students to feel disempowered, as if they are floating in a sea of harmful words and people when, in reality, they are living in some of the most welcoming and safe environments ever created.
2) The US Congress should raise the age of “internet adulthood” from 13 to 16 or 18
What do you think should be the minimum age at which children can sign a legally binding contract to give away their data and their rights, and expose themselves to harmful content, without the consent or knowledge of their parents? I asked that question as a Twitter poll, and you can see the results here:

Image: See my original tweet.
Of course, this poll of my own Twitter followers is far from a valid survey, and I phrased my question in a leading way, but my phrasing was an accurate statement of today’s status quo. I think that most people now understand that the age of 13, which was set back in 1998 when we didn’t know what the internet would become, is just too low, and it is not even enforced. When my kids started 6th grade in NYC public schools, they each told me that “everyone” was on Instagram.
We are now 11 years into the largest epidemic of adolescent mental illness ever recorded. I know so many families that have been thrown into fear and turmoil by a child’s suicide attempt. You probably do too, given that the recent CDC report tells us that one in ten adolescents now say they have made an attempt to kill themselves. It is hitting all political and demographic groups. The evidence is abundant that social media is a major cause of the epidemic, and perhaps the major cause. It's time we started treating social media and other apps designed for “engagement” (i.e., addiction) like alcohol, tobacco, and gambling, or, because they can harm society as well as their users, perhaps like automobiles and firearms. Adults should have wide latitude to make their own choices, but legislators and governors who care about mental health, women’s health, or children’s health need to step up.
It’s not enough to find more money for mental health services, although that is sorely needed. In addition, we must shut down the conveyer belt so that today’s toddlers will not suffer the same fate in twelve years. Congress should set a reasonable minimum age for minors to sign contracts and open accounts without explicit parental consent, and the age needs to be after teens have progressed most of the way through puberty. (The harm caused by social media seems to be greatest during puberty.) If Congress won’t do it then state legislatures should act. There are many ways to rapidly verify people’s ages online, and I’ll discuss age verification processes in a future post.
In conclusion: All of Gen Z got more anxious and depressed after 2012. But Lukianoff’s reverse CBT hypothesis is the best explanation I have found for Why the mental health of liberal girls sank first and fastest.
#Jonathan Haidt#Greg Lukianoff#Reverse CBT#reverse cognitive behavioral therapy#cognitive behavioral therapy#emotional fragility#fragility#emotional reasoning#external locus#internal locus#victimhood#victimhood culture#Generation Z#Gen Z#anxiety#depression#mental health#mental health issues#trauma#personal identity#hellsite#Tumblr culture#religion is a mental illness
327 notes
·
View notes
Text
@bdkdkens , I happened to see your reply to a comic from @autball asking about what ABA is, and it doesn’t look like you have had an answer yet.
I studied ABA as part of my Community Psychology degree, and am happy to give you a rundown.
ABA = Applied Behavioral Analysis
It is a specific school of psychology with an emphasis on changing the behaviors of people - “Applied” means the focus on change (and not just accumulation of data), Behavior is obvious, and “Analysis” is an indication of the intention to be “scientific.”
On it’s own, everything in ABA is neutral to good: understanding the situations in which people do behaviors, and the forces that can either cause them to do behaviors more (reinforce) or less (punish in a very scientific sense of ‘make less desirable’).
The issue is two fold:
ABA focuses only on the observable, as part of their “scientific” obsession. I phrase it that way because the choice of “observable” means that internal thoughts, memories, etc….. If the Analysis themselves can’t prove they exist? They are literally ignored as irrelevant. If they happen to interfere with the Analyst’s work? They are actively suppressed - punished out until they stop being a “problem.” Instead of, you know, addressed as part of the individual.
This is because the most important person in the equation of ABA is the Analyst. Not the client, and not even the patient - which may be two different people, in the case of working with children. The Analyst is the be all, end all expert, and everyone else needs to acknowledge that or, well, be punished for interfering with the Analyst’s work.
Point 1 is baked into ABA; if you want to include beliefs, memories of past experiences, and even intrusive thoughts as things that influence behavior and are important, you’re going to go into Cognitive Behavioral Therapy. I, myself, align strongly with CBT as a therapy philosophy.
Point 2 is technically avoidable, but having studied under old-school supporters of ABA it’s almost impossible to avoid in practice.
One of my courses in college was taught by an adjunct - that is, someone who works in the field and teacher part time as a service for people entering into the field.
He was humane, reasonable, and respectful of the clients (adults with moderate to severe mental or intellectual disabilities) and teaching them life skills.
He convinced me behavioral principles worked, even in situations where explaining necessary things to people was not possible.
My other classes????
The most recent textbook actively told the students to prevent Autistic patients from stimming because it would interfere with teaching them.
The core issue with using ABA to “correct” Autistic children is the culture of ABA is that you have to force the child to act Neurotypical/Allistic, no matter the cost to the child.
(I use both NT and Allistic because an ABA will use the same principles on trauma symptoms, depression symptoms, etc.)
The goal is to either make the child act NT - explicitly to conform to the societal majority - or else at least not act Autistic and therefore bother the Allistics.
Because conforming to society - as defined by the Analyst - is the end goal of the majority of ABA
Not learning life skills - life skills are a means towards conformity - not mental health - because remember the internal mind doesn’t matter - and definitely not what the patient wants.
The patient is a problem to be fixed. To be cured, or hidden.
And that is why ABA needs to be stopped, burned to ashes, and a new field of applied behavior technicians put in its place for situations where straight CBT is not able to be applied (because I admit there are levels of mental and intellectual disability that prevent CBT from being as effective as pure Behavioralism).
Unfortunately…..
Guess what’s easiest for parents for parents of Autistic children to find, and get insurance to cover????
😣 😣 😣
#tw applied behavior analysis#aba#actually autistic#i can never exaggerate about aba#shocks have been used as punishments#electric#shocks#and it gets government funding#i am rage#an i was never a patient#i can only weep for those that were#my whole hearted sympathy
6 notes
·
View notes
Text
What are some of the applications of cognitive psychology?
Cognitive psychology, a field of psychology that studies mental processes such as perception, memory, reasoning, and problem-solving, has numerous practical applications in various areas. Some of these applications include:
Education: Cognitive psychology principles are used to develop effective teaching methods and curricula to enhance learning and memory retention in students.
Clinical Psychology: Cognitive-behavioral therapy (CBT) is a widely used treatment for various mental health disorders, helping individuals change their thought patterns and behaviors.
Human-Computer Interaction: Cognitive psychology is applied to design user-friendly interfaces and improve the user experience in software and technology.
Marketing: Understanding consumer decision-making and memory processes is crucial for designing effective advertising and marketing strategies.
Forensics: Cognitive psychology aids in eyewitness testimony analysis and understanding memory reliability in legal cases.
Workplace Productivity: Cognitive psychology is used to optimize workplace processes, such as task management, problem-solving, and decision-making.
Cognitive psychology plays a vital role in enhancing our understanding of how the human mind works and how we can use this knowledge to improve various aspects of life. If you're interested in exploring your cognitive abilities and skills, you can assess them on our online platform, iScalePro.
#ai tools for assessment#interview skills#mock test for interview#skill assessment platform for students#skill assessment platform for job seekers#skill assessment#mock test for interviews#online skill assessment platform#skill assessment platform for employers#interview skill assessment
0 notes
Text
What Is Addiction Treatment?

Addiction treatment involves a team of medical professionals and licensed therapists who treat the physical, emotional and social aspects of addiction. It can be a long, complicated process and frequently requires multiple episodes of treatment to restore abstinence. Read more great facts on Meridian HealthCare, click here.
The first step in treating addiction is to acknowledge that you or a loved one has an issue with addiction and seek help for it. This may be the hardest step to take, but it's often the most important.
This is where therapy and counseling become an invaluable resource. It provides a safe space for individuals to open up and talk about the reasons why they have an addiction, what has caused them to abuse drugs or alcohol, and how they can begin working towards sobriety.
Counseling is a critical component of addiction treatment, as it addresses the psychological and behavioral components of the disease, teaches patients new coping skills, and facilitates interpersonal relationships. It helps patients overcome the compulsion to use and replace their drug use with constructive and rewarding activities.
It also facilitates relapse prevention and helps people learn how to live without drugs or alcohol in their lives. It can be used alone or with other therapies, such as cognitive behavioral therapy (CBT), which involves changing negative thought patterns and learning new ones that support sobriety.
Once an individual has acknowledged they have a problem and are willing to get help, the next step is finding a quality addiction treatment center. There are a number of factors to consider when choosing the right rehab facility for you or your loved one, including location, price and experience.
Look for programs that are in-network with your insurance company and meet quality standards set by the company. This is important because you will likely have a limited amount of money to spend on a recovery program, so being able to receive assistance with the cost of treatment can be a big relief.
There are several different types of addiction treatment programs available, so you'll want to find one that best suits your needs and lifestyle. These include inpatient or residential rehab, outpatient rehab, online rehab and video rehab.
Inpatient/Residential Rehab: These programs offer patients a more structured and supportive environment, which can make the treatment process easier. These programs are often accompanied by medication management and other treatments that can help clients avoid relapse.
These types of programs are typically offered in a clinical setting and include medical evaluations, psychiatric evaluations, and treatment plans that address the physical, emotional, and social aspects of an individual's drug abuse. These services can also include family and/or adolescent support, case management and referrals to other treatment services.
The cost of addiction treatment can be high, but it is often worth the expense to achieve long-term sobriety. There are many rehab facilities and treatment centers across the United States, so it's important to do research into your options before making a decision.
Once you have identified a quality drug rehab facility, it's time to schedule an assessment. This will allow caregivers to determine the level of care you need and recommend the most appropriate treatment program for you. It can be a stressful and difficult process, but it is vital to your success in recovery. Please view this site https://www.addictioncenter.com/rehab-questions/how-long-does-treatment-take/ for further details.
0 notes
Note
Can therapy be helpful if there isn't anything specifically wrong or glaring in my life right now? What does it do exactly?
Honestly, I think therapy can be helpful for pretty much anyone.
You don’t need to have a diagnosable mental health condition to see a therapist, and you don’t need to be dealing with a specific crisis or particularly difficult period in your life. You can see a therapist simply because you need someone to talk to, or because you’re trying to understand patterns in your relationships, or because you aren’t sure what you’re doing with your life, or because you simply don’t think your mental health and coping skills aren’t as good as you’d like them to be. There are all sorts of reasons to see one. Ideally you should have some sort of goal or something you’d like to get out of therapy - the therapist needs something you can work towards or structure your sessions around - but that goal can be as vague as “be more confident” or “feel better about my life”.
The main thing that therapy does is that it teaches you the tools you need to cope with difficult circumstances; it helps you to recognize, stop and challenge your own unhealthy thought patterns and replace them with new, healthier ones. Your therapist can’t “fix” your problems for you, and they can’t tell you what to do with your life (at least, they shouldn’t be telling you that), but they can help you examine your current thought processes, identify thoughts that aren’t serving you well, and help you develop new strategies and tools to approach situations in a healthier way in the future.
If you go into therapy to work on your low self-esteem and your fear of rejection, for instance, a CBT therapist might start by helping you break that down. What is it, exactly, that makes you afraid of rejection? What thoughts do you have around it? Are you afraid that people who reject you will think that you’re stupid? Do you have evidence that that’s true? Even if it was true, would it be the end of the world? How do those thoughts create the fear that you experience? What other thoughts might serve you better? Your therapist would likely assign you some homework after each session - this could be facing a fear, reflecting on something from the session, or going out into the world and practicing a skill you learned. You can see an example of what a CBT-style therapy session looks like here. As you can see, it’s not a quick fix or an instant solution - it’s a process that teaches you how to help yourself over time.
Hope this answers your question!
MM
40 notes
·
View notes
Text
Us Vs. Them
Abstract
In this essay, I will be assessing my personal feelings and attitudes toward different and defined groups. During this analysis, I will be breaking up the population into four groups: Us, Them, Allies, and Enemies. These groups have been formulated by and based on the workings and fields of psychology, psychiatry, individuals with mental illnesses (including me) and how societal norms fit into issues raised in this paper. I hope you find this to be worthwhile and I hope this sparks the fire of your intellectual flame.
-‐----------------------------------------
The American population, in the terms of mental illness, psychology, and sociology, fall into one of four categories which are detailed below:
US
This group of people are those who suffer from profound mental illness. The affliction must be (Your illness doesn't have to be all of these things, but it must be most of them):
Chronic; recurring; cause suffering; affect your relationships with others; make it so you cannot keep a job; make it so you cannot function in society; possibly get government compensation for your illness; *been hospitalized in the psych ward; been arrested when your symptoms were active; reckless and/or impulsive behaviors; suicide attempt(s); and became violent when your symptoms were active.
Them
These people are the majority of the population. They blindly follow pop culture and buy into what the masses are doing, believing, and saying. They do not have severe mental illness although they may be diagnosed with the garden-variety depression and anxiety. They have never been to inpatient for mental disorders, except maybe once, a long time ago. They will try to relate to you when it comes to mental health but they are just regurgitating what the trendy treatments and hardships are (the commonplace “social anxiety” is on the rage right now). In the inpatient hospital, the Them are the hospital staff. Especially the ones who give you the shot and put you in isolation. They are the ones who pink slip you and call the police. They think drugs are bad. You can’t truly trust Them. They don’t understand you and they probably never will. Most of Them are not hateful or mean. They are just ignorant, inexperienced, and constantly lecturing you or preaching to you. Most of Them view you as less-than, whether it is intended or not.
Allies
Imagine a straight line down the middle of a square. This divides the “Us” and “Them” that we already went over. But directly on that line, not leaning to one side or the other, sits the “Allies.” The Us’s allies have most likely not gone to the mental hospital except maybe once, long ago. But they have a mental illness that brings them suffering. They may be in mental health treatment. They struggle almost every day and their behaviors reflect that. They are a part of society and will never and have never been deemed unfit to be a working part of society. They get along with others although they feel like no one completely understands them. They do not blindly follow all of pop culture’s rules and trends. They support the Us. We can trust them somewhat. They are our allies.
Enemies
The Enemies only exist within the “Them” group. They are the ones we must watch the most carefully and never trust. Most of “Us'' do not have many Enemies on the outside but we have plenty of Enemies on the inside (inpatient). The Enemies at the hospital are those who give you the shot after they have to hold you down when you’re screaming and thrashing around because you’re so fucking freaked out. They are the ones who put you in four point restraints and let you “tire yourself out.” On the outside, the police are the Enemy for apprehending you while they get a pink slip. They are anyone who pink slips you. The Enemy tells you that you’re crazy when you know you are doing well. They threaten the hospital and hang it over your head. The Enemy treats you unfairly because something that you cannot control or help is wrong with you. The reason why Them can never be fully trusted is because any one of Them could become the Enemy at any time.
-------------------------------------------------------
I first felt the “Us Vs. Them” divide when I started frequenting mental hospitals. And when I started showing signs of severe symptoms of mental illness. In the hospital, you are a “rat in a cage” (Smashing Pumpkins song) with the staff holding the only key to get out. A drastic power imbalance exists between the staff and the patient: we are the prisoners and they are the guards. All we want to do is get out. All we want to do is go home. And if not home, then at least to a different, free place.
When I had my major mental breakdown/manic episode of winter 2019, I had been taking my medications- they were just the wrong ones. In the cage, you must take your medications, whether you want to or not. Whether you trust Them or not. If you refuse medication, They take you to court and get a court order forcing you to take your medication while you are inpatient.
There are some key ways that the “Us” and the “Them” are different in the mental hospital dynamic. They own your body: you are forced to take medications, you are locked in a box (hopefully not isolation). You can’t hurt yourself and if you do, you will stay longer (same goes for violence against others). They control your behaviors: They deem what is “appropriate” and “inappropriate” behaviors. If you break the rules surrounding these behaviors, you will get the shot, isolation, moved to a worse ward (for the more violent and disruptive patients), restraint holds, staying longer, or any combination of these events. The worst one I can think of is moving wards up a number. They try to brain-wash you: They say: “There is only one way to live life and we know the correct way to live it.” “The correct way to live is only what we arbitrarily and subjectively call “healthy coping mechanisms” and you must abandon all “unhealthy” ones in order to live life correctly and avoid being society’s pariah.” “Your only hope to be a functioning person is to abide by the teachings of CBT and DBT. All other methods will not work.” They have the opinion that their methods of recovery always work and if you are not having positive effects from their treatments, you must be doing it wrong- they deny that their treatments do not work for everybody and fail to recognize that the “bad” coping mechanisms are the only way that certain people can get by.
When you are mandated as an inpatient in the hospital, you have no rights. They take away your rights as a person. They tell you where to go, what to eat, and they control how long you are in there, what medication you take, and worst of all- when you get put down like a dog with a shot or when you switch to a more severe level. You are treated like an animal in a cage, and there is nothing that you can do about it. Losing control of your own body to this degree leads to something inside of you breaking and you turning into a feral animal (hospital song). After that happens (especially if it happens multiple times), you are never the same.
There are laws to keep other people from harming you or your property. I believe that it is a good thing that these laws are in place and that they should be upheld. But there are also laws that are made to prevent you from harming yourself and I don’t think such laws should exist. Once again, I question what the authorities, our working society (Them) and the masses (Them) deem “harmful” and ultimately illegal.
Most people in society simply follow popular culture. They just look to what the majority of others do and follow suit. But they have blinders on: they don’t see that they come up with justifications and sorry attempts at reasons to back-up their choice to blindly follow the majority.
The authorities and society says:
Drugs = Bad→ Laws against it.
Self-harm = Bad→ No laws against it but there is intense societal disapproval and shaming connected to it.
*It is the least harmful on this list because it does not alter your mood or drastically change your brain chemistry for prolonged periods of time. But, apparently, it is the most shocking and the most taboo.
Medication = Good→ Sometimes there are laws enforcing it.
I believe all of these things can be good or bad depending on the specific person that it affects. Everyone is different and if you simply follow what pop culture’s opinion is on these issues without looking into them further, it shows ignorance, a lack of curiosity and exploration, rigidity, and a propensity towards the judgement of others. It often signifies that the “Them” in question is too weak to think for themselves and to withstand society’s brainwashing.
I will never think of cutting or drugs as “bad coping skills.” “Good coping skills” consist of talking about your issues and crying according to the “Them.” And according to the hospitals, CBT, and DBT, good coping skills include activities like aroma therapy and drawing. But what do these things do? Nothing. You need a release or a change in the state of mind. Talking about what upsets you is just reliving it all over again. Plus, what if you do not trust anyone enough to tell them what's on your mind? Crying is bullshit. I feel that it is pathetic for me to cry. That’s just how I feel. I have trained myself not to. So why should I do something detrimental to myself when I am already in distress? “Good” coping skills don’t really work and only the simple-minded buy into them. “Bad” coping skills shouldn’t be judged as bad or taboo just because others have all-or-none thinking about them when it's the only thing that helps some people.
Medication: Taking medication should be the mentally ill’s choice. Medication is not right for everybody; it is not always the best thing to do. Not everyone likes themselves on medication. Who are we to judge if a person is the “correct” version of themselves or not? Forcing someone to take psychiatric medications is rooted in a power and control structure that overshadows others. I believe that we should leave others alone when it comes to this and let them live how they want to live. Just because we’re mentally ill, doesn't mean we have to do what you want with our bodies anymore.
In conclusion, I believe individuals and society as a whole should look beyond the systems of the law, procedures in mental health facilities, standard practices of therapies, pop culture trends/rules , and societal norms to find each of our unique spots in this society. We need to rethink what is considered “unhealthy” and what is “healthy” and why we put actions into those categories. We need to be more open and steer clear of letting others dictate what we believe. I’m tired of being lectured and shamed. Let's move on together.
#mental hospital#mental illness#mental health#mental disorder#essay#prose#prose essay#sociology#abnormal psychology#psych#psychology#psychology student
27 notes
·
View notes
Text
How can Depression Debilitate a Person

Depression and its Impacts
Depression is a mood disorder that can affect everything you do in your daily life. It causes a persistent feeling of sadness and loss of interest. Also called major depressive disorder or clinical depression, it affects how you feel, think and behave and can lead to a variety of emotional and physical problems. You may have trouble doing normal day-to-day activities, and sometimes you may feel as if life isn't worth living. It is not a normal part of growing older, and it should never be taken lightly. Unfortunately, depression often goes undiagnosed and untreated in older adults, and they may feel reluctant to seek help. Symptoms of depression may be different or less obvious in older adults.
For many people with depression, symptoms usually are severe enough to cause noticeable problems in day-to-day activities, such as work, school, social activities or relationships with others. Some people may feel generally miserable or unhappy without really knowing why.
-Yhessen Roselim Ecuacion
Its Causes

The Causes of Depression has numerous effects which affect not only the person but the people around them. Depression doesn’t have a specific cause; in most cases it’s different for everyone. It is a common, treatable mental illness that can be experienced at any time in life. It is often described with feeling sad, unhappy, miserable, or “down in the dumps”. Most people have these feelings on occasion. True clinical depression interferes with mood disorder in everyday life for weeks, months, or even years. Family and friends become worried about this person. They don’t understand why this person may be depressed or know how to help. So in turn both the person and their loved ones feel helpless. People that have strong social support and loved ones to lean on tend to recover faster than people that isolate themselves or have no one. Most people choose to take antidepressants rather than actually getting help with their problem. They shouldn’t rely on the medication alone; if they do it can bring unwanted side effects. Depression can be genetic, triggered by stressful events, or both. Here are some reasons that can trigger or cause depression:
Abuse. Past physical, sexual, or emotional abuse can cause depression later in life.
Certain medications. For example, some drugs used to treat high blood pressure, such as beta-blockers or reserpine, can increase your risk of depression.
Conflict. Depression may result from personal conflicts or disputes with family members or friends.
Death or a loss. Sadness or grief from the death or loss of a loved one, though natural, can also increase the risk of depression.
Genetics. A family history of depression may increase the risk. It's thought that depression is passed genetically from one generation to the next. The exact way this happens, though, is not known.
Major events. Even good events such as starting a new job, graduating, or getting married can lead to depression. So can moving, losing a job or income, getting divorced, or retiring.
Other personal problems. Problems such as social isolation due to other mental illnesses or being cast out of a family or social group can lead to depression.
Serious illnesses. Sometimes depression co-exists with a major illness or is a reaction to the illness.
Substance abuse. Nearly 30% of people with substance abuse problems also have major or clinical depression.
- Jannah Jane B. Apas
Ministration

How Is Depression Treated? The first step to getting the best treatment for depression is to meet with a mental health professional such as a psychologist, social worker, or other licensed therapist. At the same time, schedule a physical exam with your doctor. Certain medications, as well as some medical conditions such as viral infection, can cause the same symptoms as depression, and should be evaluated by a physician. The exam should include lab tests and an interview that tests for mental status to determine if speech, memory, or thought patterns have been affected. Although a physician may prescribe antidepressant medication, medication alone is not the most effective treatment for depression. Concurrent guidance of a mental health professional is strongly recommended. The therapist or counselor will listen to your concerns, screen you for symptoms of depression, and assist you in developing ways to address your stress and build new coping patterns. Treatment Options Upon review of a physical and mental health evaluation, a course of treatment may be recommended. Here is an overview of some of the therapies for depression :
Cognitive Behavioral Therapy (CBT). Cognitive behavioral therapy is the gold standard therapy for treating people with depression. Central to the treatment is teaching people that their thoughts, feelings and behaviors are all interconnected, so changing one of these points can change all three. For example, one technique called “behavioral activation” encourages people to participate in activities and then observe the effect it has on their mood. Dialectical behavior therapy (DBT) For people with more severe depression, dialectical behavior therapy can be helpful. DBT is a form of CBT that was adapted for people who have trouble managing very painful emotions, and may engage in risky behavior, self-harm like cutting, and suicidal thoughts or attempts. Interpersonal psychotherapy (IPT) Social relationships can sometimes influence and even maintain depression. When a person is depressed her relationships can also suffer.
Interpersonal Therapy. This works by addressing a person's relationships to make them more healthy and supportive. In this therapy the person learn skills for better communicating their feelings and expectations, they build problem-solving skills for handling conflicts, and they learn to observe when their relationships might be impacting their mood.
Mindfulness-based Cognitive Therapy (MBCT). While its efficacy is still being measured in adolescents, mindfulness-based cognitive therapy is another treatment that has been shown to work for young adults and adults with depression. MBCT works by combining cognitive behavioral therapy (CBT) methods with mindfulness. Mindfulness teaches people to be fully present in the moment and observe their thoughts and feelings without judgment. This can help them interrupt undesirable thought patterns that can maintain or lead to a depressive episode, like being self-critical or fixating on negative things in ways that are not constructive. MBCT was originally developed to help people with recurring episodes of depression, but it can also be used for treating a first episode of depression.gnitive behavioral therapy (CBT) Cognitive behavioral therapy is the gold standard therapy for treating people with depression. Central to the treatment is teaching people that their thoughts, feelings and behaviors are all interconnected, so changing one of these points can change all three.
Dialectical Behavior Therapy (DBT). For people with more severe depression, dialectical behavior therapy can be helpful. DBT is a form of CBT that was adapted for people who have trouble managing very painful emotions, and may engage in risky behavior, self-harm like cutting, and suicidal thoughts or attempts.
Interpersonal Psychotherapy (IPT). Social relationships can sometimes influence and even maintain depression. When a person is depressed her relationships can also suffer. Interpersonal therapy works by addressing a person's relationships to make them more healthy and supportive. In this therapy the person learn skills for better communicating their feelings and expectations, they build problem-solving skills for handling conflicts, and they learn to observe when their relationships might be impacting their mood. Mindfulness-based cognitive therapy (MBCT) While its efficacy is still being measured in adolescents, mindfulness-based cognitive therapy is another treatment that has been shown to work for young adults and adults with depression. Mindfulness teaches people to be fully present in the moment and observe their thoughts and feelings without judgment. This can help them interrupt undesirable thought patterns that can maintain or lead to a depressive episode, like being self-critical or fixating on negative things in ways that are not constructive.
- Shieloh Angelene Cariaga & Assumpta F. Arot
WATCH OUR VLOG!
youtube
2 notes
·
View notes
Text
Research Paper Final Draft
Remi Headman
Fish Burton
English 2010
30 November 2019
Rape is the leading cause of Post-Traumatic Stress Disorder (PTSD) in women (Tiihonen 1-9). On top of that, it is estimated that one in every four women have raped or sexually abuse at one point in their lives, and about one third of rape survivors will develop PTSD after their assault (Littleton 1). The high rates of PTSD call for a high demand in therapists and treatment options. One popular form of PTSD treatment is Cognitive Behavioral Therapy (CBT). Donald G. Beal explains CBT by stating that our cognition can change our behavior, our cognitive processes can change over time, and there is a positive correlation between cognitive change and behavior change (5). Cognitive Behavioral Therapy isn’t just one type of therapy, but “loosely organized therapeutic approaches” (Beal 5). Despite the many forms CBT can take on, for the sake of this paper, we will be using Beal’s propositions as a loose definition for CBT. In relation to PTSD, CBT can either start by making changes in thinking patterns or behavior patterns. After a change is made, there will be natural change that happens in whatever aspect wasn’t intentionally changed at first.
Another way to conceptualize CBT is explained by the People in Pain Network. The narrator demonstrates the basics of CBT on a “Mental Health Wheel” (PIPN Time stamp?). The wheel is split up into four different sections: actions, thoughts, emotions, and health. The idea is that each section of the wheel affects the other parts. The clip proceeds to break down how CBT works, and different strategies to implement into daily life that will help minimize symptoms of PTSD and depression. Basically, if you are depressed because of one of the sections on your mental health wheel is lacking, you will target the other three sections to improve your overall health (PIPN Time Stamp?). Cognitive Behavioral Therapy isn’t just popular for no reason. Studies have proven its effectiveness for rape related PTSD. CBT has long lasting effects on minimizing PTSD symptoms (Resick 201-210).
In order to fully understand CBT and how it works for rape and sexual abuse survivors, PTSD must be looked at more in depth. One generalized characterization of PTSD I found is “the persistent re-experiencing of the traumatic event, persistent avoidance of stimuli associated with this event, numbing of general responsiveness, and symptoms of increased arousal” (Tiihonen 1-9). However, PTSD in rape survivors is a little more specific. Some of the signs of rape related PTSD include feelings of isolation and/or depression, shame, self-blaming, distancing self from loved ones, and resisting physical touch. (AAETS 2014).
Cognitive Behavioral Therapy for rape survivors struggling with PTSD is obviously very effective and popular amongst those who have been treated with it. Especially since it is a treatment that reaps long lasting results for minimizing symptoms of PTSD. However, how can rape survivors receive treatment that not only minimizes their PTSD symptoms, but also improves their over-all recovery process and wellbeing? Implementing practices of CBT can, and will have a positive impact on lives that are affected by PTSD and depression. (Resick 201-210). However, it seems that CBT focuses specifically on symptoms, and doesn’t take the whole recovery process into consideration.
Every recovery process is going to look different, because every assault situation is different. As far as targeting PTSD and depression goes, CBT is the way to go. But I believe there is a way to do more for survivors and for their recovery process. Instead of therapists focusing on changing the way they are thinking/behaving, what if they started teaching clients life skills that will be beneficial in other areas of their life other than their PTSD symptoms? This question leads me to my proposition: Stewardship therapy. Oxford Dictionary defines stewardship as “The job of supervising or taking care of something, such as an organization or property.” However, for the purposes of this paper, I am going to open that definition up to taking care or managing your own wellbeing, and those around you. Some key words that come to mind when thinking about stewardship are empowerment and gratitude. There are many other aspects of stewardship that could play in, but both topics have research to back them as well. Survivors could potentially re-orient their entire lives if they had the proper encouragement and mind set alongside the standard therapy. Being empowered is key in achieving mental health (Grealish 314-335). For her study, A. Grealish defines empowerment as “enabling a person to take charge of their life and make informed choices and decisions about their life” (Grealish 314-335). If more clients were exposed to empowerment during the early stages of their treatment, they could potentially take control over their lives again. I see this being very beneficial to rape survivors in the way that they are learning to regain control over themselves after they had that control stripped away from them in their assault.
2 notes
·
View notes
Text
41/100 - Curiosity saves lives
Some days, I don’t know what to write about. Other days, I keep thinking about the same thing all day long and it becomes super easy to know what I am going to write about. Or at least, where I would start. Even if sometimes the start becomes the middle, or even the end. I find this artistic process incredibly fascinating.
Curiosity is the primary act of self-love. Adriene Mishler
Here’s the phrase which has resonated in my head all day long. I often used it in my therapies and it can left some patients’ minds really boggled. I talk a lot about curiosity, especially with people suffering from depression, anxiety and addictions.
It can seem so superficial to talk about curiosity when we are facing mental illness and human suffering, almost lacking of empathy. But I have found it to be the exact opposite.
My main goal with most patients of mine is to help them get more curious about themselves and their feelings. Cultivate the idea that they are deserving of their own interest. How are we supposed to love ourselves if we believe we are unworthy of attention, interest and care?
More of what I’m talking about :

I love this so much. You wouldn’t believe how many of our problems are due to the fact that we want to feel differently than we do. I am writing about it everywhere in this corner of the Internet if you are interested.
How many times did I hear (or thought!) “I should feel happier/more hopeful/stronger/more loving”?...
When we have actually very little control over what we feel, and mental illness just makes it even worse.
Not only can’t we control feelings, but worse : the more we try to change them, the more sure we can actually be to feel exactly how we don’t want to feel.
AND then we add on top of our pain some extra suffering about feeling worthless for not being able to control those unpleasant emotions, “like everybody else”. So we try harder, and reinforce the toxic cycle.
A lot of people suffering from depression, addiction and anxiety know exactly (and painfully) what I am talking about here.
And that’s where I start a lot of my therapies : by instilling reasonable doubt. Because let’s face it : it’s not a very helpful to function that way, if it were, they wouldn’t be seeking therapy and most people would be way happier.
Obviously, the second we start to talk about how it’s ‘not working’, most of us want to know ‘how it is working then?’.
I try to not answer that directly, as much as I can : part of me loves my job so much I want to tell it all right away. I just learned the hard way that it is mostly a waste of both of our energy and time.
Instead, now, I focus on teaching how to be curious. I explain less, and ask more questions. One of them is “Would you be willing to try something new, even if it may feel counter-intuitive at first?”.
Most say yes out of despair and will to feel better (if they don’t, we can explore why and what that means for them), and then we can start to unpack our mental rigidity, our very own trapping device.
I use a lot of CBT and ACT techniques. So my starting point is always observation.
“For a week, I am going to ask you to not try to change how you feel, especially the really big ones, and instead, take a moment, breathe, and take notes about what happened to you right before the feeling, what kind of emotions rose, what you end up doing about it, and how it felt afterwards.”
I often add “This is how you start to really know yourself. Without self-awareness, our whole work will be useless. It’s going to be hard and frustrating at times, note that too.
No matter what the feelings are about, they’re yours and will help you learn more about what’s happening inside of you. It also doesn’t matter at all what you do in the end, for now, we’re getting back to basics.
Real deep change needs to be prepared and planned.”
Curiosity dismantles the stories invading our heads, without trapping ourselves into useless debate.
Instead of “Is that true?”, that can always be turned and turned over until it is a bit true...
Pause, and ask yourself :
“Is this helpful to me? Is it allowing me to be my truest and best self?”
“Ok, if is that was to happen, what would it mean about you and what could you do about it?”
“Is acting/responding this way helping you cultivate the values that really matter to you? If not, what could help if being changed?”
“What, in my life story, taught me to react and feel that way?”
“What if it all turned out okay?”
Finally, curiosity helps us heal and grow. That’s what makes it the primary act self-love.
Many patients suffering from depression (myself included) can only start to heals once we drop the “Everything is awful, nothing matters and it won’t ever change” once in a while, in exchange for a bit of gentle curiosity about the world and others.
My favourite prescription for depression is Internet browsing (no need to go out first if we really dread it) about new things to learn, no matter the subject, as long as it’s something we like, or at least think could be interesting or fun.
Learning is like brain play, and school, ironically, often strips out every bit of fun out of it by design (so much more to say on that... but not today).
But we can totally get it back by choosing our own learning, I see it as creating a life curriculum : what topics do you want to study? What skills do you want to learn?
Platforms like EdEx or Skillshare or even just Youtube are full of courses and tutorials about everything.
All we have to do it is start anywhere that sparks the tiniest bit of interest, wether it’s something new or more of something we already have in our life, and start to train and flex our curiosity muscles.
The world feels very differently once we look for all it has to offer more than we lament about what it is lacking.
See you tomorrow,
Love,
L.
#curiosity#mental health#depression#addiction#anxiety#counselling#therapist#psychologist#writer#100 days project#100 days of writing#the happy mess project
3 notes
·
View notes
Note
How did depression not sap your ability to reason? I find I can’t rationalize with myself because without being able to feel good about anything, my reasoning just goes in pessimistic directions immediately. And honestly the fact that I *know* my own reason is so easily twisted makes me skeptical of your entire argument.
Depression DID sap that ability as well, but when you know that your reason is twisted and skewed toward pessimism because you have a disorder that does that, you have the facts with which to rationally fight against that tendency. You can pause and consider “I know that I suffer from depression and that depression makes me think things which are pessimistic distortions of reality. What evidence is there for this assumption other than my own thoughts about it? Does that external evidence support the assumption, or call it into question?”Another, related answer: A lot of effort and practice including when NOT in the depths of depression lows, and dedication to Doing Logic Anyway even when it’s hard.Depression’s a real bitch all around, it makes everything harder than it “should” be, but if I relied primarily (or worse, exclusively) on my feelings rather than subjecting them to logical questioning… well, I’d be long dead to suicide, frankly. A capacity for, and willingness to do the work of, metacognition – that is, thinking about and analyzing my own thought processes, observing and recognizing when my own thinking is distorted (CBT apparently teaches this, but I did it for myself, I guess I just got lucky to have good metacognition skills already developed when depression hit me like a brick shithouse. DBT is related but more specific to using reason for emotional regulation rather than general metacognition to cognitive distortions, at least that’s my impression of the difference, I am not a therapist or any kind of professional with experience at anything in this field except hacking *my own* brain) – is probably at least 80% of the reason I lived long enough to get a treatment that’s helped. And logic also got me to figuring out what that treatment was; I’ve never had a lot of financial resources to expend on trying a bunch of therapies and medications, so instead of burning money I didn’t have enough of to waste trial-and-erroring my way to an answer, I used my time researching about the neurochemistry of depression and identifying factors specific to my own situation, and treatments aimed specifically at those factors. Then sought my first medication specifically based upon that personal research, armed with a long list of reasons to expect it to help and why more usual go-to’s would probably not be ideal. And that first medication WORKED. (note that none of this is meant to shame people who do trial-and-error their process of finding a medication that helps them, this is a personal anecdote and should not be taken to imply any judgment upon people who go about solving their mental health problems in different ways than I have. The conventional path was not a viable option for me, so I found a different path to the same answer. I also put myself through exposure therapy for arachnophobia with success after researching about the concept, and I know not everyone’s capable of being their own therapist and there is no shame in that, but from multiple experiences it is possible to do a lot for oneself at least for some people. I couldn’t access a real therapist, it wasn’t an option, I had to make do with what I had, and what I had was my own screwed-up but still reason-capable brain and an internet connection).
1 note
·
View note
Text
Goals, Treatment Plan, and More
New Post has been published on https://depression-md.com/goals-treatment-plan-and-more/
Goals, Treatment Plan, and More

CPP helps enhance the caregiver-child relationship and teaches parents strategies for decreasing problems within the relationship.
It’s a commonly held belief that attachment between parents and their children just happens naturally. Society likes to pretend that humans are born with an innate desire to love and rely upon their parents, and that parents instinctively know how to love, protect, and bond with their children.
The truth is much more complicated than that. Attachment can be disrupted or impaired for a variety of reasons, and parents and children alike can both struggle to form healthy bonds.
This is unfortunate because research has found that healthy attachment between a child and their caregivers is a crucial part of a child’s healthy development. Without it, behaviors may be impacted, and psychological disorders may result.
The good news is, child-parent psychotherapy (CPP) can help.
Liora Hoffman, PhD, is an assistant clinical professor of medical psychology and program clinical director at New York-Presbyterian Hospital and Columbia University Medical Center. She describes CPP as an evidenced-based treatment plan best suited for children ages 0 to 5 years and their caregivers.
“Typically, families seek out CPP treatment following the experience of a traumatic event or due to concerns regarding their child’s mental health, behavior, or attachment relationships,” Hoffman explains.
There is ample research on the benefits of CPP in improving attachment between a child and their caregivers.
“CPP is a dyadic therapy, so it typically involves a therapist meeting with a child and caregiver together,” Hoffman said. “CPP clinicians like to say that the caregiver-child relationship is the ‘client’ as opposed to the child or caregiver alone.”
Working together with the parent and child, a CPP clinician strives to enhance the caregiver-child relationship and to teach parents strategies for decreasing any problems that may exist within the relationship.
“This is done through the use of play, developmental guidance, emotional support, and case management,” Hoffman says.
Child-parent psychotherapy is a well-known treatment plan in foster and adoptive parent circles. This is because it’s often used to treat early disruptions in a caregiver-child bond.
Jennifer Weber, PsyD, is the director of behavioral health for PM Pediatrics Behavioral Health. She says CPP is most often recommended following childhood trauma.
“Although it can be applicable for a range of other childhood mental health-related reasons including behavior problems and high family conflict,” she explains, “At the core of CPP is the idea of a child’s attachment to [their] primary caregiver, usually the mother.”
Webber says the goals of CPP typically include:
strengthening the attachment between the child and parent
improving the overall mental health of the child and parent
providing both the child and parent with coping skills
increasing the sense of safety and security in the child-parent relationship
“Most of the literature around CPP pertains to exposure to abuse and violence, such as in domestic violence situations,” Weber explained.
A CPP treatment plan can vary widely depending on the reasons for treatment and the age of the child.
“For babies and toddlers, CPP will provide help in engaging in developmentally appropriate play and help to understand the child’s development,” Hoffman says. “CPP will also explore the caregiver’s own history as it impacts their parenting of the child.”
For children this young, treatment may also be referred to as infant-parent psychotherapy (IPP).
When treatment involves children over the age of 2 years, she explains that CPP usually consists of a lot of play between the child, caregiver, and therapist.
“Children tend to express themselves through play at a young age, and play will be used to understand the internal experience of the child,” Hoffman says. “CPP will help the caregiver understand how their and their child’s experience may affect the child’s functioning and development.”
An average CPP session lasts 45 to 60 minutes and involves both the parent and child, as well as other members of the family on occasion. Hoffman says sessions usually happen weekly and can last for about a year, although there is no set time limit, and therapy generally continues until improvements in the parent-child attachment are made.
Weber explains how CPP differs from other therapy approaches.
“Treatment may be in a therapist’s office or in the family’s home,” she says. “Unlike cognitive behavioral therapy (CBT), which promotes skills-building and emphasizes the identification and challenging of maladaptive or distorted thought patterns, CPP is an integrated approach based in psychodynamic psychotherapy and attachment theory that pulls in elements of CBT and social learning and is trauma-informed.”
The main focus, she says, is often on the relationship between the child and mother.
“The therapist will focus on how parent and child interact, making observations and encouraging changes to improve trust and foster adaptive coping skills,” she explained.
According to Weber, there are several ways the attachment between a child and their caregiver may be disrupted or impaired, including:
domestic violence
parental mental health-related issues (e.g., maternal depression)
other traumatic events
“The optimal attachment style is referred to as a ‘secure’ attachment, meaning a child of this age (up to 5 years) feels safe and secure in leaving the primary caregiver for short periods of time, has practice returning to the caregiver as a ‘secure base,’ as [they know] where [their] caregiver is, and is assured that the caregiver will react in a warm and welcoming way when they do return.”
In an ideal environment, CPP should help that level of attachment to develop.
“This is a process of learning,” Weber says. Throughout that learning process, she explains, the child should come to see their caregiver as reliable, predictable, and warm.
“[This] not only reassures the child and prevents an acute anxiety response or a disorganized way of interacting with the caregiver, but also acts as a model for future relationships for the child,” she explains.
Of course, achieving these goals, and improvement in the child-parent relationship, requires the full commitment and involvement of the child’s caregiver. Without that, CPP will not be successful.
CPP is only suited for families in which the parents are open to full participation, Weber says.
“Even though treatment may be started due to the child’s behavioral or other mental-health-related issues, this is psychotherapy based in the parent-child dyad, and both participants must be fully and equally involved,” she explains.
Some families may find this difficult, especially in cases where childhood trauma on behalf of the parent is unearthed and worked through.
“It can be difficult for caregivers to acknowledge their own role in unhealthy interaction patterns or to have to relive their own experience of a particular trauma,” Weber says.
But therapists are trained in helping caregivers work through this process, and the result can be healing for both the parent and child when a caregiver is fully committed.
“Rest assured providers who are well-trained in CPP will be supportive and validating along the way,” Weber says.
Parents should know that early CPP sessions will typically occur between them and the provider alone, so that the therapist may learn more about the parent-child relationship as well as the overall family history.
“The therapist will speak with the caregiver about their reasons for seeking out CPP, so it may be helpful to write down what is bringing you and your child to therapy,” Hoffman says. “Then, the therapist can work with the caregiver to make collaborative treatment goals.”
She explains that the CPP therapist will also provide the parent with tips and ideas for talking to the child about CPP sessions and preparing them for what to expect.
“Typically, the first session with the child may include some observation of the child and caregiver playing together,” Hoffman says. “Children typically enjoy CPP sessions as it is an opportunity for special time with their caregiver.”
If you’re a caregiver of a child who has dealt with childhood trauma, or if you’re simply a parent who feels the attachment between yourself and your child has been disrupted in some way, child-parent psychotherapy may be a good solution for you and your family.
You can usually start by discussing your concerns with your child’s pediatrician or with your own therapist. Either of these professionals should be able to make recommendations and referrals to a CPP practitioner in your area.
ChildParentPyschotherapy.com is also a great resource for learning more about what CPP involves and how it can help. They even have a tool to help you find a CPP provider.
The most important thing to know is that by seeking ways to improve the attachment between yourself and your child, you’re already taking the first steps and proving your desire to have a healthy relationship with your little one. Reaching out for help can be scary, but it’s an indication of your commitment as a parent — and that’s a great thing!
Both you and your child deserve to have a healthy attachment style, and your entire family will benefit because of your dedication to that goal.
Source link
0 notes
Text
What is Mindfulness Cognitive Therapy and How Does it Help
Mindfulness-Based Cognitive Therapy or MBCT was developed by three therapists, Zindel Segal, Mark Williams, and John Teasdale. They were looking at upgrading cognitive therapy and combined it with a program called mindfulness-based stress reduction.
What followed was a relatively new but promisingly successful therapy on not only treating disorders like depression and anxiety but also preventing relapse. MBCT seems to be especially useful with the latter by teaching patients how to understand and manage their thoughts that would normally cause distress.
How Mindfulness Cognitive Therapy Works

If you are suffering from depression or anxiety, you are probably often experiencing timeframes with low mood, negative thoughts, unpleasant memories, etc. Mindfulness cognitive therapy can teach you cognitive techniques and mindfulness meditations that help interrupt these timeframes.
With these techniques, you are first learning to recognise the negative thoughts and feelings, especially since they often result in physical reactions like weariness or sluggishness. You will learn that you can separate your inner self from your negative experiences.
Once you can do that and you start seeing the reasons behind your negative thoughts and emotions, you can interrupt them with positivity. Essentially, MBCT teaches you how to anticipate and replace negative thoughts and low moods with positivity.
Techniques You Can Learn in MBCT
To effectively address your thoughts you have to become deeply aware of them. This is why MBCT sessions often include talking about your feelings and experiences in a non-judgmental manner.
Through meditation, breathing techniques, and even yoga, you will also learn to become more mindful in general. Techniques like body scan exercises where you lay down and become aware of each part of your body, and the three-minute breathing exercise can help you calm your mind and negativity and realize there is no reason to feel as negative as you do.
Preventing Depression Relapse With Mindfulness Cognitive Therapy
Patients with severe depression and anxiety often go through difficult and life-changing therapies to heal themselves with the help of their therapists. The reason MBCT seems so effective at preventing relapse of those illnesses is that it equips the patients with the skills they need to go through the day.
When you learn the negative patterns and the reasons behind them, you will easily foresee a downward spiral. If you can see it coming, you can react to it and prevent it from happening, or at least, prevent it from having such a devastating effect.
Are You Looking for Cognitive Therapy?
I am not using MBCT in my therapy sessions but cognitive behavioural therapy in combination with reality therapy. While there are many effective methods for treating many illnesses, I found these to suit my patients and their needs the best.
If you are looking for a CBT therapist because you are suffering from an issue like depression, anger management, or low self-esteem, or you are not sure and you need advice, you can always reach me here or call me on 086 3835910.
0 notes
Text
Basics of family therapy San Diego
What is it that helps us survive this complex life? Oh. Systems. As humans, we thrive as part of assistance, inclusion, and collaborative effort network. And the ultimate system is family, which makes family therapy an invaluable addition to any program. Huh?
Yet, when our therapists talk about working in therapy with families, our collective anxieties increase. We don't walk, as much as we speak the talk. The truth is, in therapy, families are not seen very often. We even bring’s entire family into the room less often.
We believe that we've shied away from this style of the job for a variety of reasons. It's not that we think less endemically, or look less at the value of families.
The modern world feels far busier, stretched, and weighed down than ever before; something in therapy we are increasingly adapted to accommodate. It was more feasible to have the whole family participate in treatment when members of the family were not operating in silos. However, the argument can be made that it is involved and get the whole family to engage and take part in family therapy, as it takes considerable work to bring the family together in the misery of life. We had clients represent the sense of dedication that is shown when members of the family take the time to attend meetings. A lot of disappointment and economic decline stems from the lack of a family member in the treatment.
The theory of psychoanalytic philosophy is based on the basics of Psychodynamic therapy San Diego. Through key empirical schools, including drive, hubris, object relations and developmental psychology, personality, and contemporary relational theory, it has a rich historical tradition and evolution.
The most commonly used treatment for anxiety disorders is cognitive behavioral therapy in san Diego. CBT's theory is that your emotions affect how you behave and then respond, not your present position.
Our marriage therapist in san Diego are considered best because of their parenting services and marriage counseling that we alter over time. They help families realize the fact that families are focused on 'parenting perfection' and 'raising' successful children.' The focus on making things right, both for parents and kids, challenges the work of a family therapist who is tasked with improving relationships and parenting practices rather than promoting perfection. At times, by teaching the art of weakness, it feels like an impossible balance to manage this pressure for perfection. The joining of the bubble wrapping, the snow shoveling, and the avoidance of sitting in the messiness of it all is all too easy. So we do what we can control; we shy away from family work and try to assist the individual through it.
Our trauma therapy of san Diegoisa particular therapy approach that acknowledges and emphasizes the understanding of how the traumatic experience affects the mental, behavioral, emotional, physical, and spiritual well-being of a child. The aim of sandigotherpy’strauma-focused therapy is to provide skills and strategies to help your child better understand, cope with, and process feelings and memories linked to traumatic experiences.
0 notes
Text
Basics of family therapy San Diego
What is it that helps us survive this complex life? Oh. Systems. As humans, we thrive as part of assistance, inclusion, and collaborative effort network. And the ultimate system is family, which makes family therapy an invaluable addition to any program. Huh?
Yet, when our therapists talk about working in therapy with families, our collective anxieties increase. We don't walk, as much as we speak the talk. The truth is, in therapy, families are not seen very often. We even bring ’s entire family into the room less often.
We believe that we've shied away from this style of the job for a variety of reasons. It's not that we think less endemically, or look less at the value of families.
The modern world feels far busier, stretched, and weighed down than ever before; something in therapy we are increasingly adapted to accommodate. It was more feasible to have the whole family participate in treatment when members of the family were not operating in silos. However, the argument can be made that it is involved and get the whole family to engage and take part in family therapy, as it takes considerable work to bring the family together in the misery of life. We had clients represent the sense of dedication that is shown when members of the family take the time to attend meetings. A lot of disappointment and economic decline stems from the lack of a family member in the treatment.
The theory of psychoanalytic philosophy is based on the basics of Psychodynamic therapy San Diego. Through key empirical schools, including drive, hubris, object relations and developmental psychology, personality, and contemporary relational theory, it has a rich historical tradition and evolution.
The most commonly used treatment for anxiety disorders is cognitive behavioral therapy in san Diego. CBT's theory is that your emotions affect how you behave and then respond, not your present position.
Our marriage therapist in san Diegoare considered best because of their parenting services and marriage counseling that we alter over time. They help families realize the fact that families are focused on 'parenting perfection' and 'raising' successful children.' The focus on making things right, both for parents and kids, challenges the work of a family therapist who is tasked with improving relationships and parenting practices rather than promoting perfection. At times, by teaching the art of weakness, it feels like an impossible balance to manage this pressure for perfection. The joining of the bubble wrapping, the snow shoveling, and the avoidance of sitting in the messiness of it all is all too easy. So we do what we can control; we shy away from family work and try to assist the individual through it.
Our trauma therapy of san Diego is a particular therapy approach that acknowledges and emphasizes the understanding of how the traumatic experience affects the mental, behavioral, emotional, physical, and spiritual well-being of a child. The aim of sandigotherpy’strauma-focused therapy is to provide skills and strategies to help your child better understand, cope with, and process feelings and memories linked to traumatic experiences.
0 notes
Last Seen Blogs

mamamalike
LIVE FAST DIE YOUNG

jennie-blossom-blog
Untitled

trexjapan-blog
TrexJapan

cosmicevila
I fight for the Users.

fantasydoctor
i wondr wuts 4 DINNER