#cadence: get a procedurally-generated room you two
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
After the announcement of the deal with Yahoo!, there were 170K signatures of unhappy Tumblr users petitioning to prevent the sale in 2013.
Text

The couple that slays together stays together✨
Masterpost
@zerorock41
#wisdomverse#wis echo#wis silent#wielders of wisdom#linked universe#suggestion fulfilled#wis cadence#echoes of wisdom#cadence of hyrule#lu wielders of wisdom#loz#zelda#lin responds#lin draws#wis aurora#cadence: get a procedurally-generated room you two
516 notes
·
View notes
Text
Fluffernutter Sandwich
Summary: Natasha is shot during a mission, and you are the surgeon that tends to her. Afterwards, upon seeing her in a distressed state despite the procedure going well, you also tend to Wanda.
Chapter 5
1587 words
Link to AO3 if you prefer that format:
https://archiveofourown.org/works/39221235/chapters/110067183
If you’d prefer to read it here:
In general, if one were in a great deal of discomfort, possibly because they had just been involved in a terroristic attack the previous day and were injured, they would do something to alleviate that pain. And under normal circumstances you would, except you couldn’t bring yourself to move when the two women who you really needed to discuss relationship labels with were lying right beside you, Wanda’s warm breath grazing over the skin of your neck, half of her body now covering yours while Natasha’s arms are holding you both protectively. The room’s still dark, and the compound is near silent other than some machinery that one would expect in a place as technically advanced as here. You let out a little sigh, trying to relax again when a shooting pain courses through your ankle, and although biting your lip stops the cry, you can’t hold back the grunt.
“Dorogaya?” Natasha is immediately awoken at the sound of your discomfort despite your attempt to quiet it, shifting so that she can look you in the eye. “What’s wrong?” You shake your head, trying to not get too distracted by the rasp in her voice due to sleep, and start to deny that anything was wrong when Wanda shifts off of you.
“It’s her ankle,” she murmurs, pushing back her tangled hair from her face as she glances down at the boot.
“It’s not fair that you can read thoughts.” She hums, her hand cupping your jaw as Natasha shifts on the mattress, pills rattling as she sits back with a medicine bottle and water bottle.
“I saw the imaging tests detka, I don’t need to read your mind to know you’re in pain.” She presses forward, leaving a soft kiss on your lips before pulling back, shifting to her knees and helping you sit up. As soon as your back hits the headboard, two pills are placed in your hand, Natasha’s fingertips lingering while her other hand holds the water in front of you. With a sigh you swallow the pills and down the water, not realizing how dry your throat was until only drops trickled from the bottle. As soon as you pull the bottle away Natasha’s lips are on yours, her sigh tickling your cheek. Your tongue swipes at her bottom lip in an attempt to deepen the kiss, but instead you whine when she pulls back with a small smirk.
“What are we?” You finally ask the question that has been probing at the back of your mind for ages, but to them the suddenness surprises them.
“What do you mean, detka?” Wanda tilts her head, and you suck in your lips as you build up your courage.
“Well, we’ve never discussed what exactly our relationship status is. You two are obviously a couple, but…” you shrug your shoulders, looking down at your lap, “…where do I fit in?” A hand cups your chin and you immediately melt into the gentle touch, Natasha’s thumb stroking along your jawline as she compels you to look at the two of them.
“Well, I think it’s fairly obvious what we’d like,” Natasha says, glancing over to see Wanda give an approving nod, the witch’s hand taking yours and squeezing. “But if you’d like a formal request,” you roll your eyes at the teasing cadence in her voice, “we’d like you to be our partner. If you’ll have us, of course.” You can’t help the smile the blooms across your face, nodding rapidly as you grab the two and pull them in for a tight embrace.
“Yes,” you whisper, giggling gleefully as your hold grows tighter, “yes, I’d like that. Love that, actually.”
“As happy as we are to hear that, I’d rather be kissing you than the headboard.” You let them go, growing warm when you realize that you’d forgotten how you’d been seated, but your two girlfriends just chuckled, Wanda’s hand reaching around the back of your neck and pulling you close while Natasha sat back, her hand resting on your knee. Soft lips press onto yours, teeth accidently clashing when neither of you can’t stop smiling, then suddenly you have to pull away to yawn.
“I think the pills are taking effect, dorogaya,” Natasha says as her hand moves to Wanda’s hip, and you pout at her. “Oh, don’t be like that. We’ll have plenty of time to continue once you wake up. And plenty more to do once that boot comes off.” They both laugh when you grow flustered at her words, both helping to lay you back down and pulling the covers over you. They take either side of you, and Wanda nuzzles back into you, Natasha gently kissing your shoulder before taking you both in her arms again. Their steady breathing only help to lull you to sleep further.
“Good night, our girl,” Natasha murmurs lowly, and as your eyelids drop your sleepy smile remains.
-
-
When you next wake up to only feel one body next to you, you blink away the sleep to see Natasha sitting up on the headboard with a phone in her hand. Her eyes dart across the screen quickly, annoyance evident on her features before she sighs and locks it, tossing it to her side.
“Everything okay?” She steels her features quickly before giving a tight smile, her fingers making their way to your hair. You furrow your brows at the odd shifts, but you hold back your questions as she leans down to kiss your forehead.
“Just an upcoming mission, they’re deciding who’ll be going.” Her hand starts massaging your scalp, and you relax under her touch. “It’s recon, so more likely than not me and Clint, but if they think that there’s a chance of engagement they’ll send others as well.”
“What do you think?” Before she gets the chance to respond, there’s a gentle knock on the door before Wanda looks in, a bright smile on her face.
“Hey, I just finished making pancakes if you two want some?” You barely get the chance to nod enthusiastically before you squeal in surprise as strong arms lift you up, Natasha laughing as she carries you out of the room. “So I’ll just go ahead and take that as a yes?”
“It’s a yes!” You shout back as you’re taken as quickly as possible to the kitchen without causing your leg any discomfort, the smell of not only pancakes but also eggs, bacon, hashbrowns and coffee filling the air.
“You really went all out, didn’t you?” Natasha teases as she sets you down at the counter, immediately reaching for a plate as Wanda’s arms wrap around your shoulders.
“Anything for my darlings,” she hums, her warm breath on your ear making you shiver. Her lips find your temple before she pulls away, asking what you want and plating it for you, the two sitting by you once you all have a hearty amount of food in front of you. “But hurry up and drink the coffee, Tony is going to be up here any minute.” Natasha curses, wincing when she tries to take a large sip of the still steaming drink.
“Why don’t you just hide it?” They both look at you incredulously and you shrug. “Rearrange some dishes, or put it in the pantry.” Wanda grins, waving her fingers and the coffee pot flies to sit behind several boxes of cereal before the door closes.
“I really hope you both know what you’ve just done,” Natasha whispers just before Steve walks through the doors, giving a small smile and nod to the three of you as he makes his way to the meeting room. “Especially if Cap calls for a-”
“All Avengers, please come to the meeting room,” F.R.I.D.A.Y.’s voice calls throughout the compound, and you smile sheepishly into your mug and Wanda fights back a laugh, Natasha’s head in her hands.
-
-
After Natasha carried you back to their room and Wanda cheekily told you that you could text them if you needed anything during the meeting, you relax onto their sofa with a sigh. The television was already turned to an episode of The Golden Girls, the best compromise Wanda and Natasha could come to when it came to shows. Halfway between a blurb between Dorothy and Sophia both Natasha and Wanda come rushing in, seeming equally stressed. You immediately sit up, watching both of them grab their typical clothes for missions.
“What happened to just recon?” Natasha’s brows furrow before she forces her expression to be neutral, but Wanda flinches before turning towards you.
“There was a change of plans. There were Hydra agents spotted at the base, and F.R.I.D.A.Y.’s facial recognition technology was able to identify some as those who attacked the compound. We need to move out now.”
“How long will the mission be?”
“Hopefully we’ll be back before morning,” Natasha says, zipping up the front of her suit before putting on the rest of her gear with an ease that shows her experience with them. Wanda pulls on her coat just as she finishes, it flapping behind her as she walks to you to kiss the top of your head.
“We’ll be back before you know it, detka.” They’re both out the door just as quickly as they came in, and despite knowing that they were well trained and well equipped for these missions, the image of the Black Widow on your operating table won’t stop flashing through your mind’s eye.
#wanda maximoff x natasha romanov x reader#wanda maximoff x natasha romanoff#wanda maximoff x reader#wanda maximoff#wandanat#natasha romanoff#natasha romanoff x reader#wandanat x reader#marvel#marvel mcu#marvel cinematic universe#fluffernutter saga
193 notes
·
View notes
Text
fond

➤idol!yeonjun x non!idol reader, pure fluffy goodness, yeonjun gets teased a lot lmao
↳yeonjun has always been a hard worker; reaching above and beyond the expectations of every person he’d even met and even himself. There was only one part of his life he knew was impossible to better--you. In Yeonjun’s eyes, you’d never been anything less than perfect from the day he met you. He never lets you forget it either, even if everyone else was beyond tired of hearing it.
Word Count: 1,501
Requested: yes!
Warnings: tooth rotting fluff, very small sprinkle of angst (self-doubt in reader)
A/N: I wrote this super fast so it may not be my best work but it felt really good to get something out and posted again! Love you all, hope you had a happy holiday!
•:•.•:•.•:•:•:•:•:•:•:•☾☼☽•:•.•:•.•:•:•:•:•:•:•:••:•.•
“Are you sure they want me to come?” You asked, shifting anxiously on the balls of your feet. “I mean, it seems like a thing reserved for just the five of you- celebrating the album- and none of the other guys have significant others to bring.” Yeonjun stopped in his tracks, leaving his shirt halfway buttoned up. Gently, he ran his warm hands up and down your arms. The sun had begun to set at some point while you were getting ready, and the light cascading in through the window opposite you washed Yeonjun in a golden ring of light.
You were so distracted by the sight that you almost missed the words coming out of his mouth.
“Baby, the guys love you. And they want you to be there. I promise. I wouldn’t ask you to come if it weren’t true. Hell, I wouldn’t even be going myself if it weren’t true. I’d much rather stay here with you and cuddle.” Your heart softened at his reassurance, anxiety bubbling away from your bloodstream in a few instants. Humming happily, you crushed Yeonjun into a hug that felt as if it could meld your bodies together.
Yeonjun lead you into the reserved restaurant with his fingers linked between yours with such fervor he might as well have glued your palms together. For that you were grateful though, because the party which you’d expected to be just the other boys and a few staff ended up being much more expansive. You spotted several important producers and a few other idols who had the time in their schedule to come and celebrate with their friends. The thrum of your heart kicked up tenfold as Yeonjun lead you through the crowds, eyes turning to him and his head of bright pink hair immediately. Damn him for always being the man of the hour. The two of you had almost made it to the safety of his table; so close in fact that you saw Soobin waving at you enthusiastically and pointing at a pair of empty seats saved by jackets and hats. Mere feet away, Yeonjun was stopped in his tracks by someone you only recognized vaguely, but knew instantly was of importance. The man was tall, handsome and well dressed, balancing a bottle of beer between his fingers with practiced ease.
As the two of them chatted about the album and general comeback procedures, you felt yourself becoming more and more out of place. For Yeonjun’s sake you plastered on a gentle smile, nodding along to whatever words were being exchanged between the two of them.
“...her name?” You caught the tail end of the sentence just in time to see that the man was gazing down at you. You glanced between him and Yeonjun, trying to collect any information as to why you were being addressed.
“I’m Y/N,” you offered carefully, not sure how they’d arrived at this topic. Yeonjun squeezed your hand reassuringly, running his thumb over the back of your hand.
“Well, I had no idea that Yeonjun had a girlfriend,” the man simpered. “What exactly do you do?” The implication of his words hit you like a MAC truck. What did you do? What did you do to deserve to be here, rubbing elbows with these famed people?
“She’s a student, actually! She’s always busy with school work or research.” Yeonjun cut in, voice rising protectively. “She pretends it isn’t a big deal, but she’s pretty high up in her department, got all the professors to love her. And she’s on track for a really cool internship- right baby?” He shot the conversation back to you, attempting to ease the tears crawling up your throat.
“Oh, it’s not that big of deal, I don’t know if I got it yet, so-”
“Shush, it’s amazing. And there’s no doubt in my mind that you’re the most qualified person for the position. You’re amazing,” Yeonjun beamed down at you warmly, a blush cropping up along your cheeks as you fought the urge to cover your face. Yeonjun quickly exchanged his goodbyes with the man and lead you finally to the table where you could take a deep breath. As soon as you settled into the chair next to Soobin, Yeonjun began to apologize in a hushed voice.
“I’m so sorry, I really didn’t think that he would say anything like that. You know that you’re amazing, though, right? I don’t want you to ever believe that I’m not proud of you, or you aren’t amazing because you aren’t an idol. I love how hard you work at school, I love that you aren’t busy with all the stupid idol things that I have to do. You’re such a positive light in my life, such an amazing person. I’m so happy that I know you. Seriously, I can’t imagine not knowing you. You know I love you, right? So much.” Your heart swelled, pumping so rapidly that it felt like it might fall out of your chest. All of the tension you’d felt during the conversation was completely gone, replaced by a pleasant buzz of happiness that only Yeonjun could provide you with. Despite the business within the restaurant, it felt as if you were in your own little bubble with Yeonjun alone, focused only on the gentle cadence of his voice and the steady heat radiating off of his body. His eyes were soft and round even under the concentrated eye makeup you’d helped him apply before leaving your apartment as he watched you carefully.
“I know, and I love you too,” a smile split your face before you could stop it, straining the muscles in your cheeks until they stung.
“Trust me, Y/N. We all know.” Taehyun laughed, causing the other three to nod in agreement.
“Seriously, he literally talks about how much he loves you all the time. Sometimes even in his sleep he’s asking where you are-”
“Hey! Stop it, you little-” Yeonjun growled, sending a menacing look toward Taehyun.
“No! Keep it coming, tell me more,” happy to encourage the teasing of your boyfriend, you leaned back in your chair and picked at the shared plate of fries that had appeared in the middle of the table at some moment.
“Oh, there was that one time we were in the studio and we couldn’t find him anywhere, like we even sent managers out to find him and everything and it turned out he got caught up talking with some random lady outside about you because he saw her carrying a bag you’d like.” Beomgyu offered, eyes sparkling at the chance to make fun of Yeonjun freely.
“Or the time when we were trying to film an episode of TO DO and he kept checking his phone because he was waiting for you to send a good morning text. The stylists were so mad that he refused to take his phone out of his pocket and they had to give him a top that would cover them.” Soobin jumped in this time, grinning just as wide as you were at the realization that Yeonjun was much more whipped for you than you’d ever estimated.
“And lets not forget literally any time we have extra time at the dorm and want to watch a movie or play a game. He literally always asks if he can invite you. At one point it was like nine days straight and when we said we’d rather not have a guest he pouted in his room instead of playing with us.” Your eyes grew wide with recognition at the story, as you remembered the exact time Soobin was referring to. You had, quite honestly, grown tired of visiting the dorm every single night after class but you did it anyway for the sake of spending time with Yeonjun.
“Did you guys know that he came to my apartment that night and complained that you were being mean to him?” Yeonjun whined loudly at your words, burying his flaming face into his own hands and letting out a defeated groan. He knew it was all true, and he was no stranger to admitting his attachment to you, but hearing it all at once made him shy.
“It’s okay, Junnie. You know I love how whipped you are for me,” you teased, rubbing the nape of his neck with delicate fingers in an attempt to get his head off of the table.
“I am not whipped!” He protests, sitting back up and trying his best to glare at you and his members. His face was still tinged with red, evidence of being caught in a lie.
‘If you’re not whipped, then what would you call it, hyung?” Hueningkai questioned, taking a poignant sip of his drink all while keeping his gaze locked onto Yeonjun. The entire table, sans Yeonjun, snickered together as he opened and closed his mouth in quick succession, trying to find the right words.
“I’m not whipped. I’m just...fond.”
#yeonjun#yeonjun fluff#yeonjun imagine#yeonjun imagines#yeonjun x reader#yeonjun fanfic#yeonjun fic#yeonjun reaction#yeonjun reactions#yeonjun drabble#yeonjun scenario#yeonjun scenarios#txt imagine#txt#choi yeonjun#txt imagines#txt fluff#txt reaction#txt reactions#txt x reader#txt fic#txt fanfic#tomorrow x together#tomorrow x together fluff#tomorrow x together fic#tomorrow x together imagine#tomorrow x together imagines#tomorrow x together reaction#tomorrow x together reactions#kpop fanfic
1K notes
·
View notes
Text
remember.
pairing: akaashi x reader
summary: akaashi’s lost his memories and you remember the events leading up to it.
genre: angst
word count: 2.4K
warnings: slight mention of blood, incident of car accident
author’s note: hi y’all! this is my contribution to the Haikyuu Headquarters server collab ✨ the prompt for this one is amnesia and I chose to write for Akaashi, but check out the other writers’ works here! I hope y’all enjoy!
part two.

The smell of the hospital is all too familiar to your senses now. There’s a low buzz of white noise around you as people come and go, walking around and minding their own business. What are they here for? Who are they here for?
You wait patiently for the elevator doors to slide open, your fingers wrung in front of you. You twiddle your thumbs three times before the light comes on above the silver doors accompanied by a ‘ding!’ and you step inside. Your finger immediately presses the button for the fourth floor, and you hold the door open for two more people as they enter the metal box. You ask which floor they need and press the corresponding buttons, watching as the doors close shut, and your steady ascent begins.
It’s quiet, save for the beeping of the elevator every time it reaches a new floor. When you arrive on the fourth floor, you wait a moment before the doors slide open before stepping out. You turn right and see the white sign above the familiar double doors that read ‘Intensive Care Unit’ and press the button for them to open automatically.
A few nurses give you small smiles upon seeing you and you do your best to reciprocate the gesture, though it never quite reaches your eyes. Nowadays, it never does.
Your hands are shaking as you reach for the door handle. The metal feels cold against your fingers and you inhale an unsteady breath before turning the bar. As the door opens, a gust of cold air hits you and the sound of multiple machines beeping fills your ears. You walk in and close the door behind you, setting your bag down on the countertop next to the entrance. Sighing to yourself, you pull the same chair you’ve been using for the past several days up to the edge of the bed and seat yourself in it. You sit in silence for a moment, unable to tear your eyes away from the main source of your joy—although, he was the current source of your heartache—Akaashi Keiji.
Had it not been for the various tubes connected to him and the reason behind this situation, he almost looked peaceful. You lift a hand and brush some hair away from his closed eyes, allowing your fingers to linger a little longer as you float them along the frame of his face. You bite your lip and hold back the tears beginning to line your eyes as your hand retracts back towards yourself.
You hum along to the song playing on the radio and keep your eyes fixed on the moving buildings and cars around you. You feel Akaashi’s thumb rubbing soothing circles around your own, squeezing your intertwined fingers every so often. As the current song comes to an end, you reach over with your empty hand and grab his phone from its spot in the console and unlock it to queue up the next couple of songs. As you do so, his phone buzzes and an unfamiliar name appears accompanied by a message.
What are you doing right now? :)
You frown slightly but choose to disregard it and continue to queue up three more songs. You look over at him and see that he continues to keep his eyes fixed on the road, completely unaware of what’s going on. You put the phone back down and debate on whether or not you should address it or not.
“Hey, you got a message,” you finally say after a few moments.
Akaashi’s eyes flicker over to you for a brief moment.
“I’ll just read it later.”
You hum in acknowledgement and decide to ignore the bubbling curiosity settling within your stomach.
Your eyes flit over to the heart monitor beeping behind the bed and you trace the cadence of each steady beat. You lower your gaze back down and sigh again. You lift your hand and grasp Akaashi’s, giving it a soft squeeze.
The breeze feels good against your skin and you inhale the fresh air with a smile on your face. The two of you finally arrived at your favorite lookout point and the city below still bustles with activity. You turn around and feel the corner of your lips falter when you see Akaashi on his phone, his thumbs tapping quickly along the screen. You turn back around and remind yourself that it’s nothing, probably just someone from work or something.
“Hey, I have to make a call really quick,” he says. You turn your head and nod.
“Okay, I’ll set everything up.”
He smiles apologetically as he takes a few steps away from the car. You choose not to dwell on it and make your way to the car to set up the little picnic the two of you had planned together.
Just as you finish setting everything up, Akaashi makes his way over and presses a kiss against your forehead.
“Sorry, I’m here now. Thanks for setting up.”
You tell him it’s no problem, simply happy with the fact that he’s here now as the two of you sit down. You hear his phone buzz and try to ignore him as he pulls the device out, typing again.
Tears continue to line your eyes as your fingers trace over his knuckles, feeling how prominent they’ve become under his skin. You lift his hand to your lips and press a small kiss against it, gently setting it back down at his side.
He’s so still. Had you not known any better, he reminded you of a living photograph.
For a split second, you could’ve sworn you saw his finger move ever so slightly but figure you’d just imagined it. You miss hearing his voice, feeling his arms around you, just him in general.
“I’m so full,” you sigh in content as you begin to clean up around yourself.
The sun has already begun setting and it’s starting to get dark. As the two of you continue to collect your things, you hear his phone buzz again with yet another text notification. At this point, you’ve lost count of how many times he’d stopped to respond. You want to ask, but you can’t help but feel as if you’re just being paranoid for no reason. However, he’s been on his phone more than he’s even looked you in the eyes tonight.
When you’re both done, you head back to the car and get inside, sitting patiently for him to start up the engine. He sits in the driver’s seat, eyes still fixed on his phone with the slightest trace of a smile on his lips. You can’t help but feel a little irked and albeit a bit jealous, so you finally decide to ask, deciding that you’ve waited enough.
“Who is it?”
“Hm?” Akaashi finally looks up from his phone and blinks innocently at you.
“You’ve been on your phone all night long,” you can’t resist the small pout on your lips.
“Sorry, love,” he says as he puts his phone down. “One of my coworkers just had a question about an upcoming project.”
“Do they know that tonight was supposed to be our date night?” You ask, trying your best to maintain an indifferent demeanor, though the question comes out more aggressively than you’d intended.
Akaashi doesn’t seem to mind, offering another apologetic smile. You do your best to stand your ground, though his smile alone makes you feel like you’re crumbling.
“It was just time sensitive,” he says. “I’ll be sure we aren’t interrupted for our next date night, okay?”
He reaches for your hand and brings it to his lips, pressing a kiss to your knuckles. He starts the engine and you feel at ease, mentally scolding yourself for getting worked up over nothing.
You grasp onto Akaashi’s hand again, missing its warmth. Right now, all you want is for him to squeeze back reassuringly, remind you that everything’s going to be okay.
The doctors had explained to you that he would be able to recover quickly so long as he followed the proper procedures once he was conscious. Even in this state, he was already improving greatly. He just needs to wake up. You need him to wake up.
The drive home is dark. You watch the road ahead of you as Akaashi rests his right hand on your thigh. You continue to reprimand yourself internally for overthinking things, even having the audacity to suspect your otherwise perfect boyfriend.
He treats you so well, taking care of you, and putting up with the different mood swings you’d have from time to time.
“You’re being quiet,” Akaashi breaks the silence first.
“Hm?” You look over at him.
“You seem to be deep in thought,” he says, giving your thigh a slight squeeze before removing his hand altogether. You shake your head—whether it’s to shake yourself back into focus or to rid yourself of other thoughts, you’re not sure.
“I’m just thinking about you,” you reply. It’s not a lie.
Akaashi’s ears and cheeks tint a soft pink at your forwardness.
“Care to elaborate?”
You shake your head again, though this time it’s more playful.
“My thoughts will stay within my head,” you say, grinning to yourself.
As the two of you continue to converse, you both fail to notice a car nearing the intersection at full speed.
You could’ve sworn you just felt Akaashi’s fingers move in your hands. The first time might’ve been a hallucination, but this time, you definitely felt it. You let go of his hand and quickly make your way towards the door, reaching for the handle and pulling the door open. You quickly get the attention of the closest nurse nearby and explain what had happened. He nods and follows you back to the room.
You stop dead in your tracks, feeling your heart flutter with emotion as gunmetal blue eyes stare back at you. Just as you’re about to run over and throw your arms around him, Akaashi opens his mouth to speak.
“Who are you?”
His voice is hoarse, not having been used in days, but you heard him loud and clear.
“I’m one of the nurses here—”
Akaashi shakes his head, keeping his eyes locked on yours.
“Who are you?”
In three simple words, it feels like your world is falling apart faster than you can pick up the pieces. He doesn’t have the same soft smile you’re used to, the same warmth and love in his eyes. Instead, he’s guarded, and confusion is written all over his face.
“I need to go get a doctor. I’ll be right back,” the nurse says, quickly rushing out of the room. You’re left alone once again.
“Do you not know who I am?” You frown, approaching him slowly.
“Should I?” Akaashi shakes his head with furrowed eyebrows. This can’t be happening.
“We’ve been dating for over a year,” you respond, feeling tears prickling your eyes once again. “Come on, Keiji, it’s me.”
Your voice comes out weaker than you’d anticipated and the look of indifference you’re receiving in return hurts.
“I’m sorry, I don’t know who you are,” he says politely. You open your mouth to say something else, but the door swings open and a doctor accompanied by a couple nurses walks in.
You’re unsure of what happened. One moment, you’re having a good time with your boyfriend, but the next, you feel your body jerking in multiple directions as the car spins out of control. The sound of glass shattering accompanied by a soft sting of pieces cutting across your skin is sharp in the night.
There isn’t much noise—though, you’re unsure if it’s because the ringing in your ears is too loud to notice—and your eyes feel out of focus. You look over and see Akaashi slumped over, a thick and dark red liquid seeping from the side of his head and beginning to stain his shirt.
Your heart is pounding in your chest as you call out for Akaashi, but he doesn’t respond. You continue to scream and cry for him to wake up, preparing for the worst until your throat feels raw. You ignore the pain and stiffness in your neck, gripping onto his bleeding arm and shake him. You’re unsure of how much time passes, but soon you hear sirens and suddenly, your world is black.
“He’s showing signs of amnesia,” the doctor sighs heavily as she looks through the chart on her clipboard. “He’s retained his basic motor skills, but he doesn’t seem to remember much of anything in the past couple of years. This is probably a result from a really intense concussion. When we scanned him for brain damage, we didn’t see anything intense, so it could be possible that this is short-term memory loss.”
“How can he get his memories back?” You bite your lip nervously, trying to hold back the tears so that you can hear out the doctor’s orders appropriately.
“Unfortunately, there’s no promise that he’ll get his memories back at all,” the doctor sighs. “You can try to jog his memory, but there’s a potential risk in doing so; you’d be writing new memories in and forcing him to believe that as reality. It’s quite easy to take advantage of.”
You nod, though you’re still trying to wrap your head around everything.
“The best thing you can do is give him time,” she says. “I understand this is hard for you, but I will also suggest consider making new memories with him.”
You nod again, this time more understandingly.
“When can he be discharged?”
“I’d like to keep an eye on him for a few more days, but after that, he’s home free. Also, I don’t know if this will help you feel better, but some patients can end up getting their memories with a single trigger and everything is fine.”
“Thank you,” you say to the doctor, sighing softly to yourself.
“We have to run some more tests on the patient, but please keep an open mind,” she says. “He’ll be back home before you know it.”
You ride the train back to your shared apartment, feeling numb all over. You’re happy he’s finally awake, but he doesn’t remember you. He doesn’t remember the memories you’ve made together and the idea that he never will twists your stomach into a knot, bringing tears to your eyes.
You want him to remember and you’ll do whatever it takes for him to do so.
#akaashi x reader#akaashi x you#akaashi haikyuu#akaashi angst#haikyuu!!#haikyuu#haikyuu x reader#haikyuu angst#haikyuu headquarters#akaashi keiji#akaashi keiji x reader
347 notes
·
View notes
Text
Humans are weird “Hypnosis”
Hope you guys are already having a great weak :)
BOOK UPDATE: You guys have been asking when my next update on wattpad is going to be within the next week, so don’t worry. My beta readers have chapter three, and I am feverishly working on the chapter after that.
The fairgrounds were alive ad teaming with color. The once deserted terrestrial moon had since been turned into the largest ever recorded outdoor market that had ever existed. The introduction of humans into the GA had brought the universe new and unconsidered ways of selling, buying, and tourism. On all sides humans and aliens alike were demonstrating their artistic craft. There were metal workers, carpenters, sculptures, artists, leather workers, and artists. A few industrious groups had even crossed inter-species borders to collaborate on projects. They had a real tough time pulling Sunny away from a Drev/human blacksmith partnership that created Drev armor in the style of medieval humans and human armor in the style of the Drev, but now after she had purchased herself a helmet, which Commander Vir, Adam, openly admitted looked ‘friggin awesome’, but then again, that was coming from someone who had purchased himself a cape, and insisted upon wearing it because it “made him look fancy.”
Krill tried not to be distracted by the frivolous, but turned out to have a great weakness for a specific vendors art works which depicted surrealist landscapes. Of course, when captain vir pointed out that they travel the universe and often see things just as strange, the doctor pointed out that, this way, he could look at how pretty it was and not worry about how dangerous it was.
They cut a strange group in the crowd, a human, a Drevv, and a Vrul, one wearing a steel- horned helmet, the other a cape, and the third holding a large roll that was almost taller than him.
Technically they were supposed to be here providing security, but out of all the jobs they had been given, recently, this one was surprisingly easy. They met up with another “Patrol” walking down the main thoroughfare and found hat Cannon, sunny’s brother had also purchased himself some new armor.
They walked with each other for a few minutes before a voice caught their attention over the roaring of the crowd.
“COME ON IN, SIT DOWN, AND ENJOY IT BECAUSE I’M ONLY GOING TO BE HERE ANOTHER DAY…. YES YOU THREE.”
Adam lept easily onto sunny’s back peering over the crowd trying to see what it was all about.
Sunny craned her head back to look at him, “What is it.”
He squinted, “Hold on, I can’t- wait a HYPNOTIST hell yeah! I love those guys. Come on lets go before all the seats are taken.”
“What is a hypnotist?” Sunny wondered, but received only a pat on the muzzle.
“You shall see.”
She blinked shaking her beak in mild confusion. Krill inflated his helium pouch and allowed Sunny to drag him through the crowd. A few of the other humans followed along curiously as did Cannon.
Together they made their way to a row of benches and took their seats. Sunny looked on stage to find a well dressed man in a suit, standing in front of a line of chairs. He didn’t look particularly special, but who was she to judge. He glanced around at the crowd for a few more minutes hollering for people to come in. Once the crowd was filled up, an assistant pressed a button at the back of the stage, and a sudden flash of blue light surrounded them before fading away to a dim shimmer.
The sound field left the interior quite silent, and the man cleared his throat taking a sip of water, “That can’t be good for my voice.” before smiling and clapping his hands together, “let's get started, how many of you know what a hypnotist is?”
Most of the humans raised their hands.
He glanced around the crowd, “Well that was to be expected, for those of you inhuman visitors, a hypnotist is someone who is trained to bring other people to a state of, what should be best explained as, deep state of concentration and suggestibility. We have used hypnotism for thousands of years in psychological treatment, relaxation techniques, and certain types of medical procedures. However, I’ll have you know now that it is STILL one of the most controversial techniques in both the psychological and physiological medical fields, however, I’m not a doctor, I am an entertainer, so we shouldn’t have any issues here today.”
He looked around the crowd, “Let me get rid of a few common misconceptions about hypnotism. First of all, if you don’t want to be hypnotized you CANNOT be. There has never, ever been a case of someone who was hypnotized against their will. This as to be something you are willing to participate in because most of the work is done by the subject, and not me. You CHOOSE to allow me to do my work, the second misconceptions is that, once you are hypnotized, you will not be persuaded to do anything against your moral code, like murder, or injuring someone, unless you are that kind of person anyway, and in that case it isn’t my fault that you’re a terrible person.”
The crowd chuckled.
“So no one will be dropping any deep dark secrets on us that they wouldn’t already tell us anyway. Last of all, if you are a human you have 100%, for sure, been in a state similar to hypnosis before. Daydreaming, meditation, driving home and then realizing when you got home that you cannot remember driving home, all those states are, in essence a form of self hypnosis, so what I am going to do here, is, I am going to give you a bit of a test, and then pick those of you who seem good subjects to be part of my demonstration. If you do not want to be hypnotized than don’t do the test, simple as that. I invite our inhuman friends to try too because I would find it very interesting to see what the results are.”
He motioned towards his assistant, who fiddled for a moment with a speaker before the soft eerie sci-fi music began, “Don’t look at me like that, we are on a moon circling a gas giant, so I can choose whatever weird music I want….. Alright, now those of you who want to try this, can I have you stand up,there we go, some aliens too, that’s good.”
Sunny glanced to her left and right. On her left Adam had taken to his feet, but that wasn’t surprising. On her other side, rill was looking on skeptically. Her brother Cannon had chosen to stand. Sunny herself was content to simply watch and see what would happen.
“Alright, everyone ready? Good…. Now those of you who want to participate I will ask to close your eyes, and when you close your eyes, I want you to hold your hands out in front of you, your right palm facing down and your left palm facing up. Now on your right hand, I want you to imagine that you have a string tied around your wrist, and on that string is a balloon, those things in the fair that are really colorful and filled with helium for those of you who don’t know. Now as you hold your hand there, the balloon gets bigger and bigger, and as it gets bigger and bigger, its filled with more helium, and as it is filled with more and more helium, it pulls you hnd higher towards the sky. Your hand grows lighter and lighter. Your arm is being pulled towards the sky higher and higher making your arm feel lighter and lighter.”
Sunny watched in general amusement as the participants right hands began to raise slowly towards the sky. Over to her right, Krill would have rolled his eyes if he could. The man continued to speak his voice retaining a distinct cadence repeating and then continuing to repeat the same instructions, and as he did hands raised towards the air. A couple of people peaked towards their counterparts sitting down once they realized it wasn’t going to work on them.
“Now in your right hand I want you to imagine you are holding a weight, and every second I keep talking the weight grows heavier and heavier dragging your hand towards the ground. Heavier and heavier the weight gets while lighter and lighter the balloon gets.” The man continued to speak as he stepped down into the crowd glancing around at the subjects. He made a few people sit back down , examined another and then came around their side of the room stopping at Adam, who, to sunny’s amusement, probably wouldn't have raised his arm any higher or dropped his arm any lower.
He looked pretty dumb.
The man paused at his side, placed a hand on his shoulder, and began to whisper something in his ear. Sunny and Krill couldn’t hear it from where they were sitting, but then the man reached up and tapped Adam on the forehead.
“Sleep.”
The crowd gasped.
The humans laughed.
He collapsed like a wet bag of sand s if his spine had suddenly vanished, knees buckling and sagging forward face first. Sunny lunged to catch him, but the hypnotist had already caught him grunting slightly under Adam’s dead weight.
Krill leaped to his feet in shocked horror stepping forward to help, but the man held up a hand, “It’s alright.” he grunted under the dead weight, “here, do you mind?” Before she could say anything, the man had turfed Adam’s corpse? Onto her lap. He sagged towards the floor, and she caught him, holding him in place with all four of her arms as his arm dangled towards the floor.
Krill reached over and felt for his pulse.
“What the hell.” He muttered
“What/” Sunny whispered to him
The Vrul held up an appendage for a second counting internally, “His pulse….. 45 bpm.”
“Isn’t that….. A sleeping heart rate?” She wondered unsure.”
Krill nodded. Off to their left another human slumped into her seat. This went on until about 12 people had been incapacitated. Adam was still not moving.
The hypnotist took a stand back on stage, “Alright now I am going to count back from three, and once I count back from three, those who are asleep are going to wake up, and then I’m going to ask them to come up on stage. When I count back from three and say wake up they are going to wake up and then come up on stage…. three …. two ... one …. Wake up.”
Adam stirred, lifting his head groggily from Sunny’s lap blinking owlishly around looking almost confused.
“Please welcome our volunteers to the stage everyone. Sunny nuged Adam to his feet, and, almost drunkenly he plodded up the isle and onto the stairs. By the time he had taken a seat in one of the chairs he APPEARED to be awake bright eyed and looking around at his neighbors as they introduced themselves.
Sunny wasn’t entirely sure what to make of it.
The hypnotist walked down the line pausing near the woman who sat Next to Adam, “What is your name Ms?”
“Jessie.”
“Ok Jessie, tell me, do you think you are hypnotized?”
She nervously shuffled her feet, “Um, no, I don’t think so?”
“Well don’t ask me, I don't know.” He turned to Adam, “Can you raise your arm for me, Sir, yes right there.” He then reached out a hand to the woman, “Well it was nice to meet you Jessie.” With a sharp tug he pulled on her arm, “Sleep!” She collapsed head first onto Adam, who looked a little more than surprised. The hypnotist moved his arm to keep hold of her, “Hold his for me will ya.”
Adam looked horribly uncomfortable as the man went down the line asking others their names and then causing them to collapse onto each other “Asleep.”
He eventually made his way back to Adam, “Comfortable there?”
Adam shrugged, “Um…. not sure.”
“Not sure, well why don’t you tell me your name.” He had reached out to take Adam’s hand.
“Adam.”
“Alright, Adam, are you hypnotized?”
“Er…. I don’t know>”
“If you had to guess?”
“Um…. Yes?” he looked pretty confused, and sort of nervous despite the fact he was smiling.
“And what do you do for a living.” The handshake was getting really long and awkward.
“I captain a spaceship.”
“Wow, thas a new one. Well Adam, do me a favor, and why don’t you look in the crowd, and focus right there on your blue friend, yeah the shiny top of her head right there, and Sleep.” He jerked his hand forward, and Adam collapsed over the top of the first human one arm dangling towards the ground. The crowd giggled.
Krill still looked quite skeptical.
The man spent the next few minutes repeating his instructions to relax repeating, “And as you go deeper and deeper into this state of relaxation, you will feel your muscles relax, the muscles in your face, the muscles in your arms, the muscles in your back, all deep and relaxed and limp, relaxed and limp, loose relaxed and limp.”
The crowd burst into a fit of giggling as Adam and his neighbor slipped onto the floor. Adam’s mouth was wide open lying flat on his back crumbled in a heap.
The hypnotist paused behind them and chuckled, “This always happens, can never keep them in their chairs, now, I know some of you out there are probably skeptical.” He looked pointedly at Krill, “Im looking at you spider legs, I can spot a skeptic a mile off. Now I know what you must be thinking, if he CAN”T hypnotize people against their will than it isn’t real, they are just pretending, but no; what you don’t understand is, I am not doing this, they are doing it to themselves, and they are using me as an excuse to do it. Think about it, wouldn’t you want to be this relaxed. What I have done is convinced THEM that they can make themselves relax.” He reached down picked up Adam’s arm and dropped it, and like a wet noodle it flopped back onto the floor, “You can’t just fake relaxation like that. These people really have convinced themselves, through my suggestion that they can do this, and that they should do it. They have DECIDED to follow my instructions.”
There was a murmuring from the crowd, and Sunny turned to find that, her brother, Cannon had fallen to the floor supposedly unconscious. The hypnotist raised his head, “Do we have another one….. Oh look at that, he’s not human.” More muttering as he stepped off stage, walked over and woke Cannon up, “Do you want to come on stage with us.”
Cannon paused and then drunkenly nodded his big head. Sunny found it greatly amusing as the tiny human led her 9 foot brother onto the stage, “Here, just sit down right her big guy till I figure out what to do with you…..” He glanced at the crowd, “happens to me every time. Someone in the crowd always gets it,” He tapped Cannon on the head, “Sleep.” he hit the stage with a loud echoing thud, but otherwise looked rather peaceful.
The man did a few more demonstrations with rigidity as opposed to relaxation, explaining the entire time what he was doing so the crowd could follow along with his intentions, “Oh now when I count back from three you are all going to wake up, and you are going to feel relaxed and fresh, and great, but when you wake up you are going to see the most beautiful person you have ever seen, guys girls, girls guys doesn't matter, he or she is the perfect specimen, drop dead gorgeous, you would do anything to impress this person. Three two one… awake.”
Sunny couldn’t help being amused at the sight of ten humans doing their best to impress an imaginary hot person. One guy stood up and began posing like a model, the women twirl their hair around their fingers, one woman even adjusted her chest. The crowd giggled. Her brother Cannon didn’t seem interested, and probably wouldn’t, not after the death of his made, so he just looked on quietly approving following some unknown Drev back and forth across the stage.
Adam on the other and, went red, shuffled his feet, and promptly crawled over e back of his chair to hide.
The crowd howled with laughter.
“Hey, hey Adam, where are you going.” Adam did not show his head. The hypnotist went back behind the chairs, “What are you doing back here.”
“Pretty girl.” Came the muttered answer.
“Well don’t you want to impress her.”
“No…. yes…..no.”
“Well why not. Come on you fly a spaceship, how could she not be impressed.”
A loud whisper this time, “What if she sees me.”
The hypnotist had to stifle a giggle, “Well that’s alright if you want to stay here that's alright, I’ll Come get you when the coast is clear.” He stepped out from behind the chairs. Sunny wasn’t entirely sure if she should laugh hysterically or feel bad for him. The other members of the crew were giggling madly from the side.
Krill had at least accepted he was stuck here at this point, and so looked on at the antics with mild amusement.
“Ok ok, the hot person is gone now, you can all return to your seats.” Adam moved a bit shamefaced from behind his chair and took a seat. “Alright, here is an easy one, the hot person is gone but all of a sudden you are going to realize that I am suddenly very very naked, and not only am I horribly naked, but I am also about 100 years old.”
The expressions of disgust, embarrassment and avoidant eye contact was greatly amusing.
“Um…. sir, sir.”
The hypnotist turned to Adam, who had stood from his seat.
“yes , Adam.”
“Um…. you’re not…. Wearing anything.” With one hand he offered up the cape he had bought earlier, “You should put this on.”
The crowd laughed, the hypnotist turned to look at them, “Such a kind your man.”
“Sleep.”
The entire group collapsed back into their seats, and in some cases, onto their seats and then onto the floor.
Sunny found herself chirping madly with glee and amusement. Whether it was real or not was beside the point, the humans were doing goofy things He had one human convinced he was fighting ninjas, another that she had forgotten her name, a third that she was the world's premier prima ballerina.
He walked up to Adam’s sleeping form, “The person whose shoulder I am touching and only the person whose shoulder I am touching, when you wake up you are going to realize that you do not speak English at all, hear that you do not speak English at all, three two one wake.”
Adam lifted his head.
“What’s your name.”
The human made a strange hissing and humming noise at him.
The crowd murdered in surprise. They hadn’t exactly expected him to start speaking fluent Vrul either. The hypnotist looked on in surprise and reached up to switch on his translator, “Oh I see, you don’t speak English…. Ha ... isn't that interesting. What would happen if you couldn't speak Vrul either.”
He tried, and when Adam began speaking again, Sunny was stunned. The noises he was making were deep and guttural originating from inside his belly and chest. It used a lot of grunting gurgling, clicking and hissing far deeper than the human’s usual voice…..
He hadn’t told her he was learning how to speak Drev…
-
“Alright when you all wake up, you realize that I have something you really want, and in order to get something that you really want, you are going to have to bring me a gift, the best gift you can think up.”
What followed was probably the funniest thing Sunny had ever seen. It was pretty tame at first, a few of the humans simply pulled out money, some gave him the things they had purchased at the fair. Cannon walked into the crowd, grabbed one of the crew members and brought him up confused and laughing to sand on stage.
“What is this?”
“Gift.” Cannon grunted
Howling laughter.
“What am I going to do with this?” The hypnotist wondered trying to hold back a laugh.
“Good mechanic.” Cannon grunted patting the human on the head, who was nearly doubled over laughing.
Another human came up on stage holding his baby.
Sunny was pretty sure some of the humans were crying now, “What the hell is this!”
“My firstborn son.”
“What do I have that you would trade your firstborn son for?” the hypnotist choked.
The human stood confused holding the baby for a moment, “Um…. second born son.”
Sunny lost it.
Trying to keep a straight face, the man turned to Adam, only to find he was proffering his own leg, the prosthetic one obviously. “Can I have my friends back now?” He wondered
The man looked down confused, “Aright Mr. Unexpectedly wholesome, back to your seats everyone.”
-
By the end, Sunny’s sides hurt, even krill looked like he was having a good time. The man had convinced them they were all naked which was amusing to watch. Many hid themselves, a few made themselves comfortable, Adam looked resigned, Cannon was unaffected.
He did a few more things before time was up before convincing the humans they were awake and no longer susceptible to his hypnosis. Adam stumbled down from the stage looking a little confused. Sunny motioned him over.
“So, when were you going to tell me you could speak Drev?”
He groaned, “Shit, that was supposed to be a surprise.”
She just grinned, “It was pretty good.”
“Really?”
“Really…..” She smiled, “You should have seen yourself.”
He blushed, “Was it bad?”
“I almost peed myself. I’ll have to tell you about all the stupid things you did later.” She wrapped one arm around him, and he tried to escape but found the attempt useless.
Krill walked past, “Yes…. I should have to write a paper about this….. Still don’t entirely believe it, but a good paper.”
Adam sighed, “Oh great, now the entire galaxy is going to know about me being an idiot.”
Krill didn’t look up, “Don’t worry, they already know.”
“Thanks for that.”
#humans are insane#humans are space orcs#humans are space australians#humans are space oddities#humans are weird#earth is a deathworld#Earth is space Ausralia
782 notes
·
View notes
Text
Towel Down
For the #PB100 drabble challenge. This week’s prompt: towel.
Maybe next time I’ll even try not to overshoot the wordcount by a factor of ten! (...sure, Jan)
Rating: Gen Wordcount: 1,062 Domestic fluff, Castiel/Dean (in theory) On AO3.
The goddamn dish towel is what finally does it.
Cas has been driving him crazy all week, ricocheting around the bunker like a fucking pinball in search of an outlane. And now Cas is in the kitchen, and he is drying the dishes with the wrong fucking towel.
So Dean dings him on the back of his head and snaps – “Hey, Typhoid Mary. We use that one to wipe down the counters.”
Cas looks at him in silent bafflement.
Dean yanks the damp towel from his hands. “How many did you dry with this thing?”
Cas’s gaze flicks over to the towering stack of dishes on the far side of the sink and, yep, Dean’s definitely gonna have to rewash them all.
“I don’t understand,” Cas says, in that tone that he probably thinks is apologetic but in actuality comes off as so nakedly petulant that Dean could strangle him right here and now and no jury would convict.
“Clean towel, for things we touch with our mouths,” Dean says, gesturing broadly the drying towel which is right under the dish cabinet. “Dirty, dirty towel, for things we rub raw chicken all over,” he says, holding up the towel, and then lets it drop to the floor. It hits Cas’s shoe, but he doesn’t look down.
“Dean, the human body hosts as many bacterial cells as it does its own. I can assure you that the health implications in this case are negligible.”
Dean snorts. “Yah. Says the guy who doesn’t need to eat.”
Cas stiffens. “No, I don’t,” he replies, and now it’s pure piss and vinegar. He shoves his sleeves back down. “Nor do I have any reason to contribute to this particular domestic activity –”
“Dude –”
“– or, for that matter, even to occupy this room. I apologize for the disruption. I’ll remove myself before I cause irrevocable harm.” Then he bombs out of the kitchen like he’s running late for a murder on the other side of town.
A moment later, Sam’s head and shoulders dip into the doorway, his face set to what the fuck was that about?.
Dean rolls his eyes. “Just bein’ a goddamn diva,” he sighs.
Sam ticks over to a facetious frown. “You, or him?”
Dean flips him the bird and starts in on the dishes.
Thirty minutes and two solid feet of dishes later, Dean is inevitably feeling a little internal blowback from snapping at the guy. Dean is still, let us not pretend, completely and absolutely correct about Towel Procedure because exactly one person in this bunker has successfully faked possession of a food-handling license in six different states without yet sending anybody (…human) to the hospital, and it is very much him – but, Jesus. They’re all on top of each others’ chicken-fried nerves right now, waiting for a case to break, for the snow to melt, for an absent God to relieve the suffering of his orphaned Creation, for Doctor Sexy MD to come off mid-season hiatus.
He finishes the last of the dishes – and maybe he should really just find them a drying rack, because air-drying really is the most sanitary solution even if counter space is kind of at a premium down here – and heads to the garage to scour some road salt out of the Impala’s intimate zones. His apologies are typically less half-assed if he workshops them under two tons of metal.
He gets there just in time to find Cas climbing out of the hot, ticking, slush-crusted Continental. Cas is looking about the same, and his expression doesn’t change when he finally spots Dean, standing frozen in the doorway. He shuts the car door behind him with a frankly adorable degree of care given how pissed he looks – the dude will smash a demon’s head into cement like a rotten pumpkin but apparently the Continental is one of God’s children. Then he stalks straight up to Dean and thrusts a plastic bag at him like he’s serving a subpoena.
“Uh,” Dean says.
Cas actually grabs Dean’s hand from where it’s hanging by his side and shoves the bag into it. “They’re anti-microbial,” Cas says, with the same gravelly cadence he normally deploys for Powerful Incantations.
Dean cautiously peels back the plastic, finds another couple layers of cellophane inside encasing two sets of: motherfucking dish towels. One set white, one set blue. There are possibly some screenprinted ducks.
“White for dishes. Blue for countertops. I find the claim scientifically dubious at best,” Cas grumbles, before rushing out: “but I recognize that sanitation standards are not…at the heart of the disagreement.”
“Okay, but seriously, Cas, you don’t fuck around with salmonella,” Dean says, which is just the dumbest shit he could possibly say, but at least it comes out kind of sorry-sounding.
Cas continues, undeterred in his apparently sworn mission to unload a formal diplomatic apology. “I recognize that you are able to exert control over a very select few areas of your general environment – ”
“Yeah, I could also probably stand not to be such a dick about it.”
That stumps him. Dean clears his throat. “Sorry, didn’t mean to mess up your speech, or whatever.”
“I’m apologizing,” Cas monotones.
“I got it. Accepted. Right back at you. We’re good.”
Castiel looks almost disappointed. “Are we?”
Dean rubs his free hand along the back of his neck – there’s a mean-ass little knot forming up in there from glaring down at all those dishes. “Look, Cas…it’s been a fuckin’ week, okay? But you…don’t need to…do stuff like this.” He waves the dishtowels half-heartedly, plastic crinkling as they flop back and forth over his knuckles. “I want you hanging out in the damn kitchen, messing things up.”
“I’d prefer to contribute positively, Dean.”
“You do, okay? Look, man, we’re family. Means when you screw up you don’t have to…say it with flowers,” He thwaps the bag against Cas’s collarbone, “or whatever.”
Cas sighs, lets his shoulders down, closes his eyes. Stays still for a long, fragile moment, which shaves a few hours off the back end of Dean’s life. Then he opens his eyes again, nails Dean with the high-beams. Guides Dean’s hand back against Dean’s own chest.
“It’s a gift,” Cas says.
Then he smiles a little, lets his hand trail away as he steps past Dean and back into the bunker. “You keep those.”
59 notes
·
View notes
Text
8 Tips from Pro Cyclists to Improve Your Next Ride
Whether you’ve been riding for decades or you’re just starting to pedal around the neighborhood, there’s always room for improvement in your cycling. Even members of the Rally CyclingSM team who have been racing for nearly two decades are still learning new tips and tricks. Here’s some great road riding advice from members of the men’s and women’s teams, sharing tips that they wish someone had clued them in on years ago.

1. Corner Like a Boss
Corners can be the trickiest piece of riding for new cyclists. Pretty much every cyclist manages some fear when heading into a turn, yet on the off chance that you pursue this guidance, you'll be cornering all the more easily in the blink of an eye. To begin, center around the passage to the corner.
"Cornering and braking go connected at the hip," says Erica Allar, who's been dashing for a long time. "You need to back off before you're quite the turn: You would prefer not to brake while turning." She's completely right. Braking in a corner can be perilous, as you'll lose footing and risk slamming.
She additionally reminds riders to concentrate on where they need to go, not where they would prefer not to go! "In a tight turn, on the off chance that you take a gander at the trees to the side, you'll likely finish up in the trees," she says. Ensure your tires have a strong association with the ground, and remain unfaltering by driving your outside foot down on the pedal. Long-term Rally colleague and previous National Criterium Champion Brad Huff says this will offer you the most footing and steadiness.
2. Discover Your Tribe
Indeed, even stars just wanna have a fabulous time. Nigel Ellsay's top tip is to concentrate on making riding fun, not a pound, by riding with other individuals who realize what they're doing, and who influence you to appreciate the time spent accelerating. His sister and colleague Gillian concurs, saying, "Be OK with the general population you're riding with: Don't ride with 30-year-old first class men in case no doubt about it!" You may need to attempt a couple of nearby gathering rides before you discover a team that feels like a solid match, so don't fear trying out a bundle of various gatherings.
3. Get Comfortable Riding in the Drops
Keeping your hands on the hoods of your handlebars for the simplest moving and braking access — and agreeable upstanding stance — might appear the best thought, yet you really lose a portion of your control. Riding in the drops (the lower some portion of bended handlebars) offers the best soundness, particularly at high speeds and going down slopes, says long-term professional Ryan Anderson.
"It's something you can chip away at on a straight street to become acclimated to it first. Riding in the drops isn't the most agreeable position at first, so do what needs to be done for a couple of minutes on end," he says. Center work off the bicycle can help make this vibe progressively agreeable, says Anderson.
4. Turn It to Win It
"Foresee the trip… and afterward turn to win!" says climber Gillian Ellsay. While the rider by you on your gathering ride may assault a slope in the enormous ring and blend, accelerating very moderate in a hard rigging, that is not the best technique — and you'll never observe a master do it. The quickest path to the highest point of a long trip is really pre-changing to a simpler gear before the ascension begins, and turning your way up it — that is Gillian's sibling Nigel's best guidance. You spare vitality, and by the top, the person in his huge ring will probably be granulating gears attempting to move down while you easily pedal past.
5. Accelerate Your Descents
Going downhill sounds straightforward, however most cyclists can review when they felt speculative on a winding plummet. Furthermore, that is totally fine, as indicated by Anderson. "You need to incorporate with it. Do what makes you feel great," he says. You need to feel in charge consistently, and if that implies crawling down a slope at first, that is totally fine. To work on including some speed, Anderson prescribes finding a drop that you do routinely, timing it, and afterward, "endeavoring to do it only a little quicker unfailingly." As far as where your eyes ought to be, Anderson alerts that taking a gander at the ground straightforwardly before you isn't the most secure: Always look in front of you to perceive what's coming!
6. Get in the Draft
Being in the draft — riding straightforwardly behind somebody in a gathering so as to make a "slipstream" impact — is an awesome inclination. It makes riding much simpler and significantly increasingly fun, however it tends to be an extreme expertise to ace. Long-term racer Danny Pate prescribes beginning little in case you're new to the idea: Get a companion to ride with you and practice with one individual. At that point, steadily, increment to a couple of companions or a little gathering ride, and get settled there before handling extensive rides or races.
"Give the individual before you a little space — you don't need to be an inch from his wheel like the folks hustling on TV!" says Anderson. "Focus on the breeze, as well. On the off chance that the breeze is originating from your right, endeavor to remain a bit to one side of the bicycle that is before you. It's somewhat more secure and it'll be significantly simpler."
At last, Anderson exhorts against gazing in the driver's seat before you. Rather, you ought to be always checking out the individual in front of you, so you can perceive what's coming up.
7. Find out About Cadence
Is it true that you are an apparatus masher who will not drop out of your huge ring? Assuming this is the case, you're missing out on important speed and power. On the off chance that you have a cycling PC that tracks your rhythm, investigate it while in-ride so you can perceive what rate you're turning. In the event that you don't have one, you can utilize a clock for one moment and endeavor to tally the pivots every moment (rpm) that you're accelerating. It won't be as exact, yet you'll get a thought regarding whether you're route down at 50 rpm or turning like insane at 120 rpm.
will feel and turn into."
8. Look for Expert Advice
"There's dependably somebody who has more involvement than you," says Danny Pate. Indeed, even following 18 years hustling as a master, he says that despite everything he adapts new tips each year — thus can you.
"On the off chance that you can look for other individuals' info and help, you'll get incredible guidance," he says. "That is the reason it's smarter to ride with individuals who are somewhat superior to you — you'll find out additional."
To discover incredible individuals to enable you to improve your riding, Pate suggests using neighborhood procedures like club groups and bicycle shops to discover rides. Be that as it may, there's one proviso: "Be honest with yourself about your capacity level when picking — you need to be with individuals somewhat quicker, not getting dropped each ride." If you are looking for more information about 8 Tips from Pro Cyclists to Improve Your Next Ride Click Here https://xpertchoose.com right away.
8 Tips from Pro Cyclists to Improve Your Next Ride Watch the Video
youtube
1 note
·
View note
Text
Managing Surgical Wait Times in the Intra-COVID-19 World
Finding the Right Prioritization Model
By JUSTIN SPECTOR
Restrictions on elective surgical volume in hospitals across the United States are causing a dilemma heretofore unseen in the American healthcare system. Surgeons across services have large and growing backlogs of elective surgeries in an environment where operating room (OR) capacity is restricted due to availability of inpatient beds, personal protective equipment (PPE), staffing, and many other constraints. Fortunately, the U.S. is not the first country to experience and deal with this situation; for many countries, this is the normal state of medicine.
By combining the accumulated experience of health systems around the world with cutting-edge technologies, it is possible to make this crisis manageable for perioperative leadership and, potentially, to improve upon the preexisting models for managing OR time.
The first step in creating an equitable system that can garner widespread buy-in is to agree upon a method for categorizing cases into priority levels. Choosing a system with strong academic backing will help to reduce the influence of intra-hospital politics from derailing the process before it can begin.
Why Cases Should Be Prioritized
If your hospital has a mix of surgeons who perform highly time-sensitive cases — cases where patient quality of life is substantially impacted — as well as cases with minor health or quality of life outcomes, it is important to make sure there will be enough capacity to get the higher urgency cases done within a reasonable amount of time. This allows cases in the backlog to be balanced against new cases that are yet to be scheduled and will help to optimize the flow of patients through the OR.
Case Prioritization Best Practices
The most important feature of a prioritization model is for it to be something your hospital, surgeons and schedulers will be able to understand and be willing to use. For this reason, we have excluded systems that are difficult to implement, such as that used by the Department of Veterans Affairs. The models included, with one exception, have long track records of success, and any hospital should be able to implement them.
Another important consideration in prioritization is what factors you want to consider. These can be broken into three major categories: clinical urgency, risk to the patient, and risk to the hospital. Risk to the patient would include factors such as ASA score, age and any complicating conditions that would make the patient especially at risk if infected with SARS-CoV-2. Clinical urgency — the rate at which the patient’s condition is worsening and the patient’s ability to wait for surgery — is the most straightforward. Finally, risk to the hospital takes into account many factors such as the risk of the patient spreading infection to hospital staff and other patients, their likelihood of needing an ICU bed and blood, and the amount of PPE needed for the case. Each hospital will need to place a different amount of emphasis on each category.
Four Prominent Case Prioritization Models
Descriptive – Surgical Waiting List Info System (SWALIS): SWALIS is a system based on the Italian government’s case prioritization guidelines that solely take into account clinical urgency to assign a case one of five levels, and each priority level is associated with a maximum time before treatment (MTBT). This model is easy to understand and requires minimal administrative oversight, but it does not take into account other factors such as equipment needs and risk to the patient and hospital. Because of the ease of implementation and clarity of the segmentation, this is a favored model.
A model to prioritize access to elective surgery on the basis of clinical urgency and waiting time
Prescriptive – British Columbia Ministry of Health Surgical Patient Registry (SPR): The model used in British Columbia, Canada, is similar to the Italian model in that it divides cases into groups by clinical urgency. However, instead of the surgeon subjectively determining the priority level, this model prescribes a level based on the procedure. This system is especially effective if it will be difficult to instruct your clinics on the prioritization methodology but requires a lot of decisions to be made centrally to determine the priority for each procedure and any modifiers that need to be considered.
Patient Prioritization Codes: Overview
Surgical Wait Time Strategy
Surgical Wait Times – Procedures A-Z
Dental Surgery ‐ Adult – BC List of Patient Condition and Diagnosis Descriptions
Qualitative Patient Need – General Surgery Prioritization Tool (GSPT): New Zealand was one of the first countries to implement clinical priority assessment criteria (CPAC) nationwide. One CPAC tool being used is the GSPT. It uses a 0-100 scale for each case based on aspects of the impact on the patient’s quality of life and health to determine a relative priority. (See Appendix)
General Surgery Prioritization Tool: a pilot study
Qualitative Multifactor – Medically Necessary, Time-Sensitive (MeNTS): Published in the Journal of the American College of Surgeons, this system uses a mix of subjective and objective scores in different categories to create a cumulative score between 21 and 105. Higher scores equate to a greater risk to reward for the procedure. The process of scoring each case requires 21 factors to be rated on a scale of 1 to 5, making this best suited to systems with strong admin staff who can complete these evaluations for each case.
Medically Necessary, Time-Sensitive Procedures: Scoring System to Ethically and Efficiently Manage Resource Scarcity and Provider Risk During the COVID-19 Pandemic
Choosing the Right Model
The two most important factors when designing a prioritization model for your hospital or system are consistency and compliance. It is important that across surgeons and service lines there is an understanding of what priority level is appropriate and that those are in line with leadership’s intent. It is also important to consider the ease of use as models that require too much work per individual case may be ignored or half-heartedly complied with.
As there has been little national or state-level guidance on this subject, each hospital organization has a great deal of leeway to choose a method that fits their unique needs.
Other Considerations
If your hospital is constrained on beds, PPE, blood or any other surgical input, consider adding these as factors in your prioritization system. For example, if PPE is a constraint, it’s important to balance case lengths as shorter cases result in more PPE use throughout a surgery day. Similarly, if inpatient beds are limited, you may want to set a threshold on the total number of cases that require greater than six hours of in-bed recovery time. This is an area where web-based tools excel due to their ability to leverage sophisticated packing algorithms.
Translating Priority Scores Into Surgery Dates
In the American healthcare system, surgical schedules are built around block allocation. This means that each case’s score is not enough to determine when it should be performed since the surgeons will not be coming in to do just one case. Each surgeon or department’s entire backlog should be considered to determine how surgical time should be distributed.
The challenge is to balance priority against wait time and overall backlog volume. While certain service lines may only have low- to medium-priority cases, if their caseload is sufficient, then they should be given time even within the first few weeks of opening up elective booking. Using a scoring system for each case that takes into account wait time, along with determining the MTBT for each priority category, it is possible to formulate how much time each surgeon or service should receive each week. Because surgeons’ waitlists are constantly changing, it is useful to repeat this exercise at a weekly or biweekly cadence to ensure optimal distribution.
Further Reading
Below are academic papers that discuss the importance and process of prioritization that may also be useful. The author would like to thank Dr. James Caldwell, director of surgical services, Parkview Medical Center, for his assistance in compiling this information.
Edwards RT. Points for pain: waiting list priority scoring systems. BMJ. 1999;318(7181):412–414; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1114887/
Curtis AJ, Russell COH, Stoelwinder JU, McNeil JJ (2010). Waiting Lists and Elective Surgery: Ordering the Queue. Medical Journal of Australia. 192: 217-220. doi:10.5694/j.1326-5377.2010.tb03482.x; https://www.ncbi.nlm.nih.gov/pubmed/20170460
COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures (Online March 17, 2020); https://www.facs.org/covid-19/clinical-guidance/triage
Mullen P M (2003). Prioritising waiting lists: how and why? European Journal of Operational Research, 150(1), 32–45. doi: 10.1016/S0377-2217(02)00779-8; https://www.sciencedirect.com/science/article/abs/pii/S0377221702007798?via%3Dihub
Davis B, Johnson SR. Real-time priority scoring system must be used for prioritisation on waiting lists. BMJ. 1999;318(7199):1699. doi:10.1136/bmj.318.7199.1699; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1116039/
Testi A, Tanfani E, Valente R, Ansaldo GL, Torre GC. Prioritizing Surgical Waiting Lists. Journal of Evaluation in Clinical Practice. 2006; ISSN 1356-1294; https://pubmed.ncbi.nlm.nih.gov/18211645/
Appendix
Scoring system for NZ, GSPT
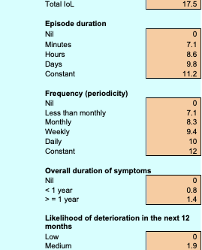
Justin Spector is a product manager at LeanTaaS where he is continuously enhancing ways to help hospitals ease access to OR time and optimize OR utilization.
Managing Surgical Wait Times in the Intra-COVID-19 World published first on https://venabeahan.tumblr.com
0 notes
Text
Managing Surgical Wait Times in the Intra-COVID-19 World
Finding the Right Prioritization Model
By JUSTIN SPECTOR
Restrictions on elective surgical volume in hospitals across the United States are causing a dilemma heretofore unseen in the American healthcare system. Surgeons across services have large and growing backlogs of elective surgeries in an environment where operating room (OR) capacity is restricted due to availability of inpatient beds, personal protective equipment (PPE), staffing, and many other constraints. Fortunately, the U.S. is not the first country to experience and deal with this situation; for many countries, this is the normal state of medicine.
By combining the accumulated experience of health systems around the world with cutting-edge technologies, it is possible to make this crisis manageable for perioperative leadership and, potentially, to improve upon the preexisting models for managing OR time.
The first step in creating an equitable system that can garner widespread buy-in is to agree upon a method for categorizing cases into priority levels. Choosing a system with strong academic backing will help to reduce the influence of intra-hospital politics from derailing the process before it can begin.
Why Cases Should Be Prioritized
If your hospital has a mix of surgeons who perform highly time-sensitive cases — cases where patient quality of life is substantially impacted — as well as cases with minor health or quality of life outcomes, it is important to make sure there will be enough capacity to get the higher urgency cases done within a reasonable amount of time. This allows cases in the backlog to be balanced against new cases that are yet to be scheduled and will help to optimize the flow of patients through the OR.
Case Prioritization Best Practices
The most important feature of a prioritization model is for it to be something your hospital, surgeons and schedulers will be able to understand and be willing to use. For this reason, we have excluded systems that are difficult to implement, such as that used by the Department of Veterans Affairs. The models included, with one exception, have long track records of success, and any hospital should be able to implement them.
Another important consideration in prioritization is what factors you want to consider. These can be broken into three major categories: clinical urgency, risk to the patient, and risk to the hospital. Risk to the patient would include factors such as ASA score, age and any complicating conditions that would make the patient especially at risk if infected with SARS-CoV-2. Clinical urgency — the rate at which the patient’s condition is worsening and the patient’s ability to wait for surgery — is the most straightforward. Finally, risk to the hospital takes into account many factors such as the risk of the patient spreading infection to hospital staff and other patients, their likelihood of needing an ICU bed and blood, and the amount of PPE needed for the case. Each hospital will need to place a different amount of emphasis on each category.
Four Prominent Case Prioritization Models
Descriptive – Surgical Waiting List Info System (SWALIS): SWALIS is a system based on the Italian government’s case prioritization guidelines that solely take into account clinical urgency to assign a case one of five levels, and each priority level is associated with a maximum time before treatment (MTBT). This model is easy to understand and requires minimal administrative oversight, but it does not take into account other factors such as equipment needs and risk to the patient and hospital. Because of the ease of implementation and clarity of the segmentation, this is a favored model.
A model to prioritize access to elective surgery on the basis of clinical urgency and waiting time
Prescriptive – British Columbia Ministry of Health Surgical Patient Registry (SPR): The model used in British Columbia, Canada, is similar to the Italian model in that it divides cases into groups by clinical urgency. However, instead of the surgeon subjectively determining the priority level, this model prescribes a level based on the procedure. This system is especially effective if it will be difficult to instruct your clinics on the prioritization methodology but requires a lot of decisions to be made centrally to determine the priority for each procedure and any modifiers that need to be considered.
Patient Prioritization Codes: Overview
Surgical Wait Time Strategy
Surgical Wait Times – Procedures A-Z
Dental Surgery ‐ Adult – BC List of Patient Condition and Diagnosis Descriptions
Qualitative Patient Need – General Surgery Prioritization Tool (GSPT): New Zealand was one of the first countries to implement clinical priority assessment criteria (CPAC) nationwide. One CPAC tool being used is the GSPT. It uses a 0-100 scale for each case based on aspects of the impact on the patient’s quality of life and health to determine a relative priority. (See Appendix)
General Surgery Prioritization Tool: a pilot study
Qualitative Multifactor – Medically Necessary, Time-Sensitive (MeNTS): Published in the Journal of the American College of Surgeons, this system uses a mix of subjective and objective scores in different categories to create a cumulative score between 21 and 105. Higher scores equate to a greater risk to reward for the procedure. The process of scoring each case requires 21 factors to be rated on a scale of 1 to 5, making this best suited to systems with strong admin staff who can complete these evaluations for each case.
Medically Necessary, Time-Sensitive Procedures: Scoring System to Ethically and Efficiently Manage Resource Scarcity and Provider Risk During the COVID-19 Pandemic
Choosing the Right Model
The two most important factors when designing a prioritization model for your hospital or system are consistency and compliance. It is important that across surgeons and service lines there is an understanding of what priority level is appropriate and that those are in line with leadership’s intent. It is also important to consider the ease of use as models that require too much work per individual case may be ignored or half-heartedly complied with.
As there has been little national or state-level guidance on this subject, each hospital organization has a great deal of leeway to choose a method that fits their unique needs.
Other Considerations
If your hospital is constrained on beds, PPE, blood or any other surgical input, consider adding these as factors in your prioritization system. For example, if PPE is a constraint, it’s important to balance case lengths as shorter cases result in more PPE use throughout a surgery day. Similarly, if inpatient beds are limited, you may want to set a threshold on the total number of cases that require greater than six hours of in-bed recovery time. This is an area where web-based tools excel due to their ability to leverage sophisticated packing algorithms.
Translating Priority Scores Into Surgery Dates
In the American healthcare system, surgical schedules are built around block allocation. This means that each case’s score is not enough to determine when it should be performed since the surgeons will not be coming in to do just one case. Each surgeon or department’s entire backlog should be considered to determine how surgical time should be distributed.
The challenge is to balance priority against wait time and overall backlog volume. While certain service lines may only have low- to medium-priority cases, if their caseload is sufficient, then they should be given time even within the first few weeks of opening up elective booking. Using a scoring system for each case that takes into account wait time, along with determining the MTBT for each priority category, it is possible to formulate how much time each surgeon or service should receive each week. Because surgeons’ waitlists are constantly changing, it is useful to repeat this exercise at a weekly or biweekly cadence to ensure optimal distribution.
Further Reading
Below are academic papers that discuss the importance and process of prioritization that may also be useful. The author would like to thank Dr. James Caldwell, director of surgical services, Parkview Medical Center, for his assistance in compiling this information.
Edwards RT. Points for pain: waiting list priority scoring systems. BMJ. 1999;318(7181):412–414; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1114887/
Curtis AJ, Russell COH, Stoelwinder JU, McNeil JJ (2010). Waiting Lists and Elective Surgery: Ordering the Queue. Medical Journal of Australia. 192: 217-220. doi:10.5694/j.1326-5377.2010.tb03482.x; https://www.ncbi.nlm.nih.gov/pubmed/20170460
COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures (Online March 17, 2020); https://www.facs.org/covid-19/clinical-guidance/triage
Mullen P M (2003). Prioritising waiting lists: how and why? European Journal of Operational Research, 150(1), 32–45. doi: 10.1016/S0377-2217(02)00779-8; https://www.sciencedirect.com/science/article/abs/pii/S0377221702007798?via%3Dihub
Davis B, Johnson SR. Real-time priority scoring system must be used for prioritisation on waiting lists. BMJ. 1999;318(7199):1699. doi:10.1136/bmj.318.7199.1699; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1116039/
Testi A, Tanfani E, Valente R, Ansaldo GL, Torre GC. Prioritizing Surgical Waiting Lists. Journal of Evaluation in Clinical Practice. 2006; ISSN 1356-1294; https://pubmed.ncbi.nlm.nih.gov/18211645/
Appendix
Scoring system for NZ, GSPT

Justin Spector is a product manager at LeanTaaS where he is continuously enhancing ways to help hospitals ease access to OR time and optimize OR utilization.
Managing Surgical Wait Times in the Intra-COVID-19 World published first on https://wittooth.tumblr.com/
0 notes
Text
The Captain’s Secret - p.12
“Affairs of the Heartless”
Full Chapter List << 11 - The Cure for What Ails 13 - Callbacks >>
"Testing one, two, three. Huh. Well, that's creepy."
"I don't know, I think it's an improvement."
Lorca fixed Benford with a look. They were in the ready room running a final test of the fake Peter Bhandary: a live-rendered image of Bhandary mapped on top of Lorca's expressions and movements, with fake kelbonite interference to mask any imperfections. Benford grinned back at Lorca. "You haven't looked that good in, well, ever!"
Lorca pointed at the display and the image in the display pointed right back. "You really think this asshole looks better than I do? And remember, I am your captain."
"Well, when you put it that way, he looks ten times as good as you."
"Jack!" said Lorca, exasperated but laughing.
Benford laughed, too. "If you didn't know how good-looking you were, the universe would be a much better place."
It was a blatant lie. It had to be, because Benford had used Lorca's good looks to his own advantage in various bars over the years before he'd gotten married. "I didn't know you found me attractive," Lorca shot back.
Benford raised an eyebrow. "Ah, I didn't say that. I think what I said was you find yourself attractive? And that is a dangerous thing."
Lorca snorted. There was nothing to be gained by arguing the point. "All right, let's turn on the audio filter." He cleared his throat.
"Ready when you are."
"Jack Benford is the worst." As Lorca spoke these words aloud, the computer rendered the speech into a tone and pitch matching Bhandary's voiceprint just a smidge of a second behind real-time, so it sounded like two people saying the exact same thing at the same rate in near-unison. It was, for Lorca at least, markedly disconcerting hearing another voice at virtually the same time as his own. He specifically chose a few unusual test sentences to push the limits of the speech algorithm. "Rubber baby buggy bumpers. This fortune cookie intentionally left blank. Not for all the horses in Andalusia."
"Now that's creepy," declared Benford, muting the audio. "But it's working. You want to go over any more lines?" They'd spent much of the past ninety minutes running through various conversational scenarios in preparation for the main event.
"Nope. Let's get Lalana up here and go." Benford sent the summons and double-checked everything one more time.
While he waited for Lalana's arrival, Lorca ran his hand through his hair and was annoyed to see Bhandary's image do the same. Luckily he wouldn't be looking at the image during the actual transmission, because Bhandary's smug face still irked him. He scrunched up his own face and tried to make it look like Bhandary was crying.
An incoming commlink interrupted this diversion. It was Ek'Ez. "Yes, doctor?"
"Captain, I have discovered the most amazing thing about lului!"
"Is it an emergency?"
"I—no, captain. Not an emergency."
Lalana arrived with her security escort. Lorca motioned for her to wait and the escort stepped outside. "Is it anything that will change in the next ten minutes? Or that I need to know right now?"
Ek'Ez paused. "No. It is nothing of the sort."
"Then I'll talk to you again in ten minutes." He terminated the comm link.
“Captain!” said Lalana cheerfully. "I am so happy to be able to help you."
"Yep," said Lorca, slipping in the earpieces that would let them pass him any pertinent information in a manner that wouldn't distract him from the task at hand. Lalana wasn't, strictly speaking, necessary to this part of the plan, but on the off chance something came up, it was better she be present to provide her insight into the Dartarans on demand, and if nothing else, Lorca knew she'd be an appreciative audience.
Benford went over the procedure for the transmission one more time with Lalana. Lorca stared into the monitor and smiled. Here went nothing, do or die. "Initiate transmission."
The answer wasn't immediate, but it came. T'rond'n's face appeared onscreen. Because they were copying Bhandary's previous transmission codes from the Dartarans' archives, T'rond'n expected exactly what he saw: Peter Bhandary, albeit with significant visual interference.
Lorca affected a tone he thought fit the conceited persona of a smarmy socialite like Bhandary. It came out like a bad cross between a California valley girl and a mimicry of foppish, old school British aristocracy, with a smattering of sycophantic insincerity thrown in on top for good measure. Of course, the computer made it sound like Bhandary, but the emotion and cadence of the performance came through to add that extra layer of scumbag. "T'rond'n! You're alive! I'm so glad to see you! When I heard what happened... "
"Peter," said T'rond'n, apparently all the greeting Lorca was going to get. "This is unexpected."
"I heard Starfleet destroyed your ship!" The words had been carefully chosen to convince the Dartarans of the impetus for Bhandary's contact, and having the facts of the matter appear diluted through a small game of interstellar telephone gave it the ring of truth. It wouldn't do to have Bhandary seem too well-informed and make the conversation smell like the setup it actually was. "Is Margeh...?"
"Margeh is here. We were not on the ship that was destroyed."
"Thank goodness. Who was on it?"
T'rond'n shifted but did not immediately answer. Margeh came into view. "A thief," she said, appraising the interference on the transmission. "Where are you?"
Lorca wouldn't have minded trying the whole conversation on T'rond'n, but luck wasn't with him. From everything he knew about the couple, Margeh was the savvier of the two, and he would have to tread carefully to get this conversation where he needed it to go. Of course, that was why he'd insisted on doing it himself. "Sorry about the picture quality. I'm at a kelbonite mine. In fact, if you're in the market for any..."
"No, thank you, Peter," said T'rond'n, gruffly but not angrily.
Lorca switched right back to the chase. "So the thief stole your ship?"
Margeh hissed angrily. "Our lului was stolen. The ship was... circumstantial."
Lorca was pleasantly surprised to have Margeh come out and say it. He'd had four other lines prepped to convince her to reveal the fact, and now that he didn't have to use them, he could jump right into the next part. "The lului? Really? Did you get it back at least?"
"No," said T'rond'n, in something like a sigh. "She was on the ship that was destroyed."
"No! Oh, that's a shame." Lorca's voice practically oozed concern. It was maybe a tad overwrought, but Dartarans were notoriously stoic and tended to think of humans as emotional, and Lorca knew Bhandary was an emotional enough person to stay up late crying, so may as well play up to their expectations. "It was such a charming creature. The way it changed colors on command... Really impressive." Lorca imagined Lalana was probably having a good laugh right now. Of course, Margeh was not so kindly disposed towards her former pet at this point, since the thief and the stolen goods were one and the same. "Will you get another one?"
"Unlikely."
Minor setback, but expected. Margeh had to be led to the idea in such a way that it felt like her own. She was almost a harder nut to crack than Billingsley. (Lorca wondered if Margeh might be susceptible to the same sort of icebreaker he'd applied in the chief engineer's case. Probably not.) "That's right, I remember, you said they were almost impossible to catch. Such a shame. You probably won't get that lucky again."
Margeh jerked her head in affront. There it was. "Luck had nothing to do with it," she said. "Hunting is about skill, preparation, patience, and knowledge of your prey. Luck is for amateurs."
"Of course, you're right, my apologies. I'm sure no one knows more about lului than you at this point." Ha. "You could probably catch as many as you wanted. At the end of the day, you don't need any proof. You know you had a lului, and that's all that matters. No one can take that accomplishment away from you. And if anyone ever doubts it, you can call me, and I'll set the record straight." He smiled.
Most people could have found comfort in that sentiment, but from everything Lorca had heard and read about Margeh, she was not most people.
As a general rule, Dartaran society split certain roles down gender lines, as many human societies once had in the past. The difference was that the Dartaran split persisted into the present day. Some sociologists theorized that it did so because while the two genders were seen as fundamentally different, they were both equally important and present in Dartar's overall political, societal, and historic landscape. Co-dominance, Starfleet's file called it. A subtle but distinct difference from true egality.
The split was this: male Dartarans mostly handled logistics, production, and trade, while females governed sciences, culture, and spirituality. They were called the Hand and the Head in Dartaran philosophy respectively. Starfleet's sociological profile included a foundational Dartaran axiom, "Without the Hand, the Head cannot act, and without the Head, the Hand has nothing to do." (It was additionally worth noting that Dartaran culture was slightly more monolithic than most, as Dartar featured but a single supercontinent that had unified under the Head and Hand banner around the time that Caesar walked the Earth.)
It wasn't a hard rule, and there were plenty of figures in Dartaran history who defied these gender norms, but that didn't mean there wasn't pushback when someone did break the mold, simply because it was seen as abnormal.
As a successful merchant, Margeh had broken that mold and had the chip on her shoulder to match. Her entire life, she had been motivated by the need to prove herself to everyone around her, and this still held true today. To doubly undercut something she had accomplished by suggesting she needed a human male to back her up on it as proof...
"Anyway, I've taken up enough of your time. I'm just so glad you're both safe. Let me know if you're in the market for a new ship. I've got a line on some Vulcan shuttles. They're not cheap, but they're very fast." Nice little dig at the slow speed of Margeh and T'rond'n's transports, just in case they still weren't feeling inadequate enough to motivate Margeh to compensate.
"Yes," said Margeh softly, her mind clearly elsewhere.
"Thank you, Peter," said T'rond'n, almost mechanically, and the transmission terminated.
Lorca removed the earpieces and turned around. Benford had his padd under his arm and was clapping slowly. "I don't know that they took the bait, but..."
"It really looked like you were Peter Bhandary!" said Lalana excitedly, hands rotating.
"Don't say that," groaned Lorca. If he never had to see Bhandary's face again, it would be a day too soon.
Her hands paused. "Why? Was that not the point?"
"Yes, but..."
Benford snorted and explained, "He thinks his face is much better looking than Bhandary's is." The reveal was his little way of getting back at Lorca .
"Oh, without doubt!" agreed Lalana, earnestly and without hesitation. "Your face is the best."
Lorca's disgruntled glare at Benford was replaced by a look of surprise and delight. "Look at that, even Lalana agrees."
"How do you mean?" asked Benford suspiciously, wondering how a lului could possibly gauge human attractiveness when the two species were so incredibly different.
"I have noticed that humans do not express with movements very much, because you don't have tails and fur, so instead you put the things that you feel on your faces. And you have the most things of any human on your face."
The sentence was so ridiculous, Lorca's shoulders shook with silent laughter and he covered his face with his hand. He had the most things on his face? What did that even... Perceiving her comment had made Lorca happy, Lalana resumed rotating her hands.
"I think you've got that backwards," Benford said, thinking lului probably expressed so many emotions with their hands and tails because their faces were largely incapable of expression. They were basically two eyes and a mouth that switched between an upside-down V shape when closed and a diamond when open. They could not smile, squint, or even blink. "But more importantly, captain, what about Margeh and T'rond'n?
"What about them?" His tone was jovial, even nonchalant.
"Their response was a little... lackluster, maybe?"
Lorca snorted with amusement. "Tell me, Jack. You in a gambling mood?"
Benford had learned a long time ago: never, ever bet against Gabriel Lorca. "I guess you saw something I didn't!"
Probably several things, thought Lorca, but said diplomatically, "If they haven't made their overture by the end of the day, we'll call it a bust. But they will. Now, if you'll give me the room... and sorry I didn't end up needing you, Lalana, but you can never be too prepared for a curveball."
"Oh, that is no trouble, captain, it was my pleasure. But what is a 'curveball' and how do we 'give you' the..." Lalana began saying, but Benford ushered her out.
Lorca glanced past his reflection in the window and drummed his fingers, expression blank. He also needed to check in with Dr. Ek'Ez. He may as well do that first, in case it was something worth reporting to Starfleet. He took a moment to crack a cookie as a quick snack, then opened a visual comm line to sickbay. "Dr. Ek'Ez, you had something to report?"
"Captain!" Though it had been several minutes now, Ek'Ez's excitement and enthusiasm had not waned one bit. "In my most recent battery of tests, I have discovered the most amazing thing!"
Lorca hadn't given Ek'Ez permission to run any tests. He hadn't forbidden it, but he hadn't approved it, either. "I thought you were just running decon."
"Well, yes, captain, but Lalana kept insisting it was not necessary, and once I determined the reason she thought this, it merited scientific exploration."
"Well don't leave me in suspense, doctor," said Lorca. Trying to get succinct answers out of Ek'Ez verbally was every bit as hard as trying to parse his rambly, meandering written reports.
"Captain, Lalana is, and I apologize for the inadequacies of language in communicating this, but she is a many-celled organism."
Lorca blinked slowly and took a breath. Almost all forms of life were cellular in origin, with the higher forms being comprised of trillions and trillions of cells. "Anything else?"
"Ah, I am not explaining it right. She is many cells unified into a single, coherent organism." This cleared absolutely nothing up. "She is cells!" Lorca began to wonder if this was some sort of mental breakdown. Ek'Ez turned his head. "Sam! Will you please come and explain this?"
Li's face came into view, her dark eyes staring with disturbing lifelessness at Lorca. "She is the cells, captain," said Li. It was a subtle difference of a single word, but it was enough of a difference that Lorca realized what Ek'Ez was trying to say. Li further clarified, "Individually and collectively."
"Are you saying she's a trillion self-aware cells?" he attempted.
"Not quite! Yes, in that she is aware of herself on a cellular level, and that all her cells are part of a neural network, and no, in that there is what could be described as a central neural structure which is the core of her consciousness... Allow me to back up a moment." Ek'Ez blinked his eyes repeatedly, something he did when he was clearing his mind. Lorca winced, expecting this would get worse before it got better.
"In most species, cells are differentiated into tissue types, and form unique biological structures, which we call organs."
Lorca wanted to smack Ek'Ez. "They do teach biology at the Academy," he deadpanned. "Even to meatheads."
"Yes, of course, I apologize. I simply want to make sure the distinction here is clear. While Lalana possesses several differentiated tissue structures — her eyes, for example, and bone structure, and her central neural structure — the majority of her tissues are not differentiated. She does not have blood, or a heart, or a liver, or even what you and I would call a stomach. Rather, her body is made up of a mass of multipurpose, unspecialized — or perhaps more accurately, multi-specialized — cells which perform all the basic biological functions at once, configured as an interlocking lattice of cells and operating as a diffuse network transmitting nutrients and information through connections of the cellular membrane!"
There was an accompanying graphic showing a lului cell and the pipelike structures on the cell's outer membrane which connected to other, identical cells with the same features.
Lorca knew Lalana had no heartbeat from their conversation on the Tederek moon, and had seen firsthand the lack of blood in the wound on her leg, but hadn't put those two facts together until now. She was literally heartless.
"It's like she's made up of stem cells," offered Dr. Li from off-screen. (Lorca wished she would just decide if she wanted to be in this conversation or not, and behave accordingly.)
"Yes, they do have a progenitive nature. The medical implications, captain!"
The medical implications were what, exactly? This was interesting and all, and Lorca hardly wanted the doctors to condescend to him with infantile explanations, but... They already knew Lalana was strange. She was an alien. It was sort of the point, to seek out strange, new life.
Ek'Ez continued, oblivious to Lorca's disinterest in the unnamed implications. "If only her cells were more robust. My research was completely confounded while you were gone with her."
"If it's a question of keeping the cells alive," said Li, trailing off mysteriously.
"Would you like to join this conversation, Dr. Li?" Lorca said finally, and was rewarded by Li moving into view just behind Ek'Ez. (In so much as Li's dead-eyed face could be considered a reward of any kind.)
"The problem is," Ek'Ez began to explain, as if Lorca had asked him for an explanation (he had not), "the tremendous cellular decay rate. When lului cells are disconnected from the central matrix, they quickly begin to die. The samples survive for mere minutes, captain." He closed his eyes in disappointment.
"We can easily solve this by studying the cells without removing them," said Li, more to Ek'Ez than Lorca.
Ek'Ez was reluctant. "That is true, but..."
Lorca understood perfectly what Li was suggesting. They'd just rescued Lalana from captivity, and Li wanted to subject her to live experimentation. Sometimes Lorca wondered if Li had become a doctor because she was interested in curing infectious diseases or causing them. Technically-speaking, Li had a heart, but the word "heartless" suited her even more than it did Lalana. "Have you spoken to Lalana about this?"
Li nodded. "Yes, she was amenable."
Of course she was amenable, it was Lalana. "I really wish you hadn't," said Lorca. "You understand she's our guest? We're taking her back to her planet?"
"I wish to mount a medical research mission on that planet when we do!" said Ek'Ez.
Lorca suspected that was why Ek'Ez had contacted him, really: not to share the news of his discovery, but to ask Lorca to petition Starfleet on his behalf to lead a research mission before someone else of more importance learned about lului and tried to do the same.
One big problem with that. Two, actually. "Doctor. Has Lalana told you the history of Luluan?"
"History, captain?" Ek'Ez's inquiries had been entirely centered around medical and biological subjects, not history. Problem one: lului historically did not welcome aliens who used technology, and Ek'Ez had clearly missed the memo on the type of greeting such visitors tended to get.
That wasn't all. "You understand her people aren't warp-capable?" Understatement of the day, there.
"Well, yes, but as they have already been interfered with... by other parties..." Ek'Ez realized what he was saying and trailed off. "I see." Problem two: General Order 1. While it wasn't fully intact in this case, that didn't mean it didn't merit applying after the fact, especially if it was what the lului wanted for themselves.
"I'll do what I can, doctor, but no promises. Whether or not you get any sort of research expedition out of all this, I can't say. Best make use of the time you have now."
"The facilities on this ship, captain... they are..." The Triton wasn't a research ship. It wasn't even an exploration ship. Its medical and science facilities were, compared to most ships in the fleet at this point, rudimentary at best.
"It may be the only chance you get. Anything else?"
"Mm, no. Thank you for your time, captain."
Two down, one to go. Lorca double-checked San Francisco local time out of habit and requested a channel.
To his surprise, Cornwell appeared on the other end of the line. "Hello, Gabriel."
Her greeting indicated this wouldn't be an entirely formal conversation and he responded in kind. "Katrina. Wasn't expecting you."
"Are you ever?"
Lorca thought a moment. "No. You are a singularly surprising woman any man would be a fool to try and wrap his head around."
She looked immensely satisfied by the compliment. "Coming from the great Gabriel Lorca..." They'd had plenty of conversations in the past about Lorca's tendency for self-aggrandizement and Cornwell was well within her rights to make light of it. "Admiral Wainwright's at a conference on Rigel IV. He appointed me full admiral pro tem in his absence."
"Moving on up in the world, aren't we?"
She gave a short laugh. "I like to think so! At any rate, tell me how it went."
His childhood love of exploratory fiction served him well as he outlined the events of the Tederek mission. He knew exactly which parts to mention, which parts to gloss over, and how to phrase it all in a way that made Cornwell's eyes go wide with awe. He made sure to include Billingsley's fall from the ladder for the comedy and heroics, the gruesome joke that was the leskos for the drama and adventure ("galaxy's most murderous herbivore," he called it), and the encounter with the mind-eaters for a dash of horror and a second helping of heroism. He did not mention the near-miss with T'rond'n in the bathroom, or the giant gaping hole in Lalana's leg. Neither mishap had affected the mission's outcome, and he already knew they did not appear in Morita's writeup
She laughed and shook her head at the end of the tale, trying to picture Lorca impersonating an interstellar socialite. "So what's why you needed those files!"
"What did you think I was going to do with them?"
"Honestly?" she said, fixing him with a look. "I thought you might try to track him down and kidnap him, or detain him and have him do the outreach to the Dartarans."
"That was Plan C at best," he offered, and she laughed, despite the fact she suspected the joke wasn't far from the truth.
Something occurred to Lorca. "Say, you wouldn't happen to be the reason Admiral Over-My-Dead-Body signed off my little project, would you?"
Cornwell snorted, amused but disapproving. "Maybe we don't call him that in his office, even if he's not here."
It wasn't an answer. Lorca lifted an eyebrow.
Cornwell relented. "I only said he might give you a little leeway and see what you'd do with it. And that you wouldn't disappoint if he did."
"And have I disappointed?"
"Not yet," she smiled, "but you still don't have a direct line to the merchants."
"It's coming."
"So you say." Her tone was more lighthearted than worried. If Lorca said it was forthcoming, she believed him. But she did have another concern. Her expression darkened as she leaned forward and asked, "Be honest with me now, if Admiral Wainwright had said no to this whole mission, would you have accepted it?"
"He didn't say no."
"If he had."
"Focus on the road you're on, not the road you didn't travel," said Lorca. Cornwell recognized a fortune cookie when she heard one and frowned in response. Lorca knew he had to give her more than that. "If I'd thought I wasn't going to get the go-ahead, I wouldn't have checked in with command in the first place, I'd've exercised my discretion as captain. But I knew you'd have my back."
Cornwell mentally kicked herself for inadvertently enabling the whole charade. "So the whole point of you informing Starfleet in the first place was just to show off."
Lorca scoffed with feigned offense and smiled. "You got me." A moment later he was serious again. "I would have accepted Starfleet's orders, but I knew you wouldn't let Wainwright or anyone else stop me from doing the right thing." The right thing, in this context, meaning whatever he wanted to do. "A whole planet, Katrina, and they need our help."
"Your help, you mean."
Lorca shrugged as if it made no difference. "Right place, right time. That's all."
"Seems to happen a lot with you," she observed. "Careful now. Karma might balance the scales one day."
It was an entirely different aspect to karma than the one he'd talked about with Lalana, and while Lorca didn't fully ascribe to the idea as Cornwell was presenting it, there was a fortune cookie that read, All jokes have a kernel of truth. "That's why I'm on a starship. Karma will never catch up." She rolled her eyes at him. Lorca felt the tiniest pang. "You know, you're missed out here on the far reaches of civilization."
Cornwell smiled and shook her head. "Someone has to maintain the inner reaches, or else what's the point? Anyway, it was good to see you, Gabriel."
"Oh, I'm sure it was. Apparently, I have the most things of any human on my face."
Momentary confusion colored Cornwell's face. "What?"
"Nothing," said Lorca, smiling to himself. "Something our alien guest said."
Part 13
1 note
·
View note
Text
Lemonade Stands And The Cadence Of Two Easy Steps
"So Beatrice, exactly what are you going to make today?"
“Lemonade.”
"As well as what's the first active ingredient? "
“Lemons.”
“And what’s second?”
“Sugar.”
“And then what?”
“Um…ice.”
"Yes, ice, however also water, right? "
“Yes, and water!”
And that's how it went on my oldest little girl Beatrice's final PRESCHOOL share and leader day recently-- 3 simple actions-- much like Unique Representative Oso from Disney Junior educates toddlers to do. Really, 4 easy actions in this case, just because when Bea makes lemonade, it's always as well warmer for her as well as so she intends to add ice to cool it down, together with including the water.
Three (to four) very easy steps to discovering something brand-new. In a fun means. A method you'll always keep in mind which assists the learning stick, without much inhibition as well as a full-throttle curiosity of how things function that can be pressing. To understand is to do, once more and once again and also again.
And the kids, well, that's where they have us defeat. United States being the adults in the space. According to a current Freakonomics podcast titled Think Like a Youngster, Alison Gopnik, a lecturer of psychology as well as philosophy at the College of California-Berkeley as well as the writer of The Philosophical Child: Just what Kid's Minds Tell Us About Fact, Love, and the Definition of Life, has done some remarkable research on youngsters's cognitive processes and also development. In this podcast, Gopnik defines how contemporary research study shows that children are much more than just underdeveloped grownups:
“Think of the youngsters as being the study and development division of the human species. As well as we're-- adults-- we're production as well as marketing. From the manufacturing and also advertising viewpoint, it might look like the R&D people are truly not doing anything that looks really sensible or valuable. They relax throughout the day in their beanbag chairs playing Pong and having blue-sky suggestions. And we bad production as well as marketing individuals, who are actually making the earnings, have to support these individuals! But obviously, one of the many things that we know is that type of blue-sky, merely pure, study in fact settles over time."
Those are my ladies for sure. Initially, there's a goal. There's constantly a goal.
"Beatrice, do you intend to find out how you can make lemonade?"
“Yes, I do. It’s yummy.”
There you go. The objective. Making lemonade. Grace, all we obtained ta do following is put a lemonade stand together out front and we obtained ourselves a lil' business. It is nearly summertime, you know.
The major goal. The 3 easy steps to reach that main goal, as well as the objectives around finishing the 3 very easy steps. A baby-steps business design. A cadence that includes getting to said goals, establishing brand-new ones, and also discovering something brand-new each and every time that results in growth and success.
To know is to do, time and again as well as once again.
Unfortunately, this ain't the instance for several business. Heartache as well as employee turnover are still all as well usual difficulties for companies of all sizes and shapes as well as sectors. It's an overgrown as well as thorny path that leaders and also HR groups walk bare foot daily, without compass to lead them, no "where the wild points are" inquisitiveness driving the cadence of learning as well as growing (directly, professionally as well as monetarily).
This unmanageable, wild west "talent pattern" could produce bad environments and societies where your individuals are compelled to rush and also hire reactively each time a worker makes a step toward the door.
Listening to Andre Lavoie, Chief Executive Officer and co-founder of ClearCompany, talk concerning just how business and company leaders have to develop worths and main objectives (or restore them), aligning cascading objectives and creating as well as taking care of a cadence to get all business at hand done efficiently and also constantly, absolutely motivated me to share the lemons-to-lemonade backstory.
Us adults in the room have eliminated the childhood R&D, as well as in the very same last gasping breath, ability management methods of the previous not job. Today people function in a different way, are inspired in different ways and are involved differently, and desire their performance measured in a different way. Millennials could have pressed all the employer flexibility buttons, today every generation is requiring more.
For instance, staff members desire continuous growth opportunities, workplace adaptability, tools as well as systems that motivate cooperation, and dedication to a reciprocatory environment of assistance and also support, every one of which lead to paybacks in worker retention, contentment, and total business performance. Organizations could no more manage to just "handle people," due to the fact that individuals require even more-- they want aligned company goals that they belong to and that are attainable as well as evolve collaboratively over time.
We want lemonade stands as well as the tempo of two very easy steps:
Recognize. Organizations need to offer attractive company and staff member cultures that acknowledges the specific, while ensuring innovation, learning, collaboration and connections. They require a visionary talent engagement experience that is orchestrated around people as well as individuals goals, not procedures. The secret now is to drive a greater level of payment, deeper engagement via a much better "people management" experience.
Experience. These qualities-- the lined up objectives, the learning, the growth, the sound company design, the full-throttle curiosity of just how points work-- all culminate in supplying an amplifier effect on skill contribution and also success. Organizations that offer an even more appealing experience could better acquire adoption of the skill efforts throughout the business, and line up individual purposes to business goals to improve performance, retention, and also productivity.
This "amplifier result" of people's payments upon lined up, completed goals has a quick as well as long lasting effect with time. Favorable company results become the norm.
Just add sugar and ice? It's delicious indeed.
0 notes
Text
Managing Surgical Wait Times in the Intra-COVID-19 World
Finding the Right Prioritization Model
By JUSTIN SPECTOR
Restrictions on elective surgical volume in hospitals across the United States are causing a dilemma heretofore unseen in the American healthcare system. Surgeons across services have large and growing backlogs of elective surgeries in an environment where operating room (OR) capacity is restricted due to availability of inpatient beds, personal protective equipment (PPE), staffing, and many other constraints. Fortunately, the U.S. is not the first country to experience and deal with this situation; for many countries, this is the normal state of medicine.
By combining the accumulated experience of health systems around the world with cutting-edge technologies, it is possible to make this crisis manageable for perioperative leadership and, potentially, to improve upon the preexisting models for managing OR time.
The first step in creating an equitable system that can garner widespread buy-in is to agree upon a method for categorizing cases into priority levels. Choosing a system with strong academic backing will help to reduce the influence of intra-hospital politics from derailing the process before it can begin.
Why Cases Should Be Prioritized
If your hospital has a mix of surgeons who perform highly time-sensitive cases — cases where patient quality of life is substantially impacted — as well as cases with minor health or quality of life outcomes, it is important to make sure there will be enough capacity to get the higher urgency cases done within a reasonable amount of time. This allows cases in the backlog to be balanced against new cases that are yet to be scheduled and will help to optimize the flow of patients through the OR.
Case Prioritization Best Practices
The most important feature of a prioritization model is for it to be something your hospital, surgeons and schedulers will be able to understand and be willing to use. For this reason, we have excluded systems that are difficult to implement, such as that used by the Department of Veterans Affairs. The models included, with one exception, have long track records of success, and any hospital should be able to implement them.
Another important consideration in prioritization is what factors you want to consider. These can be broken into three major categories: clinical urgency, risk to the patient, and risk to the hospital. Risk to the patient would include factors such as ASA score, age and any complicating conditions that would make the patient especially at risk if infected with SARS-CoV-2. Clinical urgency — the rate at which the patient’s condition is worsening and the patient’s ability to wait for surgery — is the most straightforward. Finally, risk to the hospital takes into account many factors such as the risk of the patient spreading infection to hospital staff and other patients, their likelihood of needing an ICU bed and blood, and the amount of PPE needed for the case. Each hospital will need to place a different amount of emphasis on each category.
Four Prominent Case Prioritization Models
Descriptive – Surgical Waiting List Info System (SWALIS): SWALIS is a system based on the Italian government’s case prioritization guidelines that solely take into account clinical urgency to assign a case one of five levels, and each priority level is associated with a maximum time before treatment (MTBT). This model is easy to understand and requires minimal administrative oversight, but it does not take into account other factors such as equipment needs and risk to the patient and hospital. Because of the ease of implementation and clarity of the segmentation, this is a favored model.
A model to prioritize access to elective surgery on the basis of clinical urgency and waiting time
Prescriptive – British Columbia Ministry of Health Surgical Patient Registry (SPR): The model used in British Columbia, Canada, is similar to the Italian model in that it divides cases into groups by clinical urgency. However, instead of the surgeon subjectively determining the priority level, this model prescribes a level based on the procedure. This system is especially effective if it will be difficult to instruct your clinics on the prioritization methodology but requires a lot of decisions to be made centrally to determine the priority for each procedure and any modifiers that need to be considered.
Patient Prioritization Codes: Overview
Surgical Wait Time Strategy
Surgical Wait Times – Procedures A-Z
Dental Surgery ‐ Adult – BC List of Patient Condition and Diagnosis Descriptions
Qualitative Patient Need – General Surgery Prioritization Tool (GSPT): New Zealand was one of the first countries to implement clinical priority assessment criteria (CPAC) nationwide. One CPAC tool being used is the GSPT. It uses a 0-100 scale for each case based on aspects of the impact on the patient’s quality of life and health to determine a relative priority. (See Appendix)
General Surgery Prioritization Tool: a pilot study
Qualitative Multifactor – Medically Necessary, Time-Sensitive (MeNTS): Published in the Journal of the American College of Surgeons, this system uses a mix of subjective and objective scores in different categories to create a cumulative score between 21 and 105. Higher scores equate to a greater risk to reward for the procedure. The process of scoring each case requires 21 factors to be rated on a scale of 1 to 5, making this best suited to systems with strong admin staff who can complete these evaluations for each case.
Medically Necessary, Time-Sensitive Procedures: Scoring System to Ethically and Efficiently Manage Resource Scarcity and Provider Risk During the COVID-19 Pandemic
Choosing the Right Model
The two most important factors when designing a prioritization model for your hospital or system are consistency and compliance. It is important that across surgeons and service lines there is an understanding of what priority level is appropriate and that those are in line with leadership’s intent. It is also important to consider the ease of use as models that require too much work per individual case may be ignored or half-heartedly complied with.
As there has been little national or state-level guidance on this subject, each hospital organization has a great deal of leeway to choose a method that fits their unique needs.
Other Considerations
If your hospital is constrained on beds, PPE, blood or any other surgical input, consider adding these as factors in your prioritization system. For example, if PPE is a constraint, it’s important to balance case lengths as shorter cases result in more PPE use throughout a surgery day. Similarly, if inpatient beds are limited, you may want to set a threshold on the total number of cases that require greater than six hours of in-bed recovery time. This is an area where web-based tools excel due to their ability to leverage sophisticated packing algorithms.
Translating Priority Scores Into Surgery Dates
In the American healthcare system, surgical schedules are built around block allocation. This means that each case’s score is not enough to determine when it should be performed since the surgeons will not be coming in to do just one case. Each surgeon or department’s entire backlog should be considered to determine how surgical time should be distributed.
The challenge is to balance priority against wait time and overall backlog volume. While certain service lines may only have low- to medium-priority cases, if their caseload is sufficient, then they should be given time even within the first few weeks of opening up elective booking. Using a scoring system for each case that takes into account wait time, along with determining the MTBT for each priority category, it is possible to formulate how much time each surgeon or service should receive each week. Because surgeons’ waitlists are constantly changing, it is useful to repeat this exercise at a weekly or biweekly cadence to ensure optimal distribution.
Further Reading
Below are academic papers that discuss the importance and process of prioritization that may also be useful. The author would like to thank Dr. James Caldwell, director of surgical services, Parkview Medical Center, for his assistance in compiling this information.
Edwards RT. Points for pain: waiting list priority scoring systems. BMJ. 1999;318(7181):412–414; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1114887/
Curtis AJ, Russell COH, Stoelwinder JU, McNeil JJ (2010). Waiting Lists and Elective Surgery: Ordering the Queue. Medical Journal of Australia. 192: 217-220. doi:10.5694/j.1326-5377.2010.tb03482.x; https://www.ncbi.nlm.nih.gov/pubmed/20170460
COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures (Online March 17, 2020); https://www.facs.org/covid-19/clinical-guidance/triage
Mullen P M (2003). Prioritising waiting lists: how and why? European Journal of Operational Research, 150(1), 32–45. doi: 10.1016/S0377-2217(02)00779-8; https://www.sciencedirect.com/science/article/abs/pii/S0377221702007798?via%3Dihub
Davis B, Johnson SR. Real-time priority scoring system must be used for prioritisation on waiting lists. BMJ. 1999;318(7199):1699. doi:10.1136/bmj.318.7199.1699; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1116039/
Testi A, Tanfani E, Valente R, Ansaldo GL, Torre GC. Prioritizing Surgical Waiting Lists. Journal of Evaluation in Clinical Practice. 2006; ISSN 1356-1294; https://pubmed.ncbi.nlm.nih.gov/18211645/
Appendix
Scoring system for NZ, GSPT

Justin Spector is a product manager at LeanTaaS where he is continuously enhancing ways to help hospitals ease access to OR time and optimize OR utilization.
Managing Surgical Wait Times in the Intra-COVID-19 World published first on https://wittooth.tumblr.com/
0 notes
Text
The EBM Wars: Manufacturing Equipoise (Part 1)
By ANISH KOKA
The phone rings. It’s not supposed to be ringing. It’s 2 am. The voice on the other line is from an apologetic surgery resident.
Resident: There is this patient..
Me: Yes, go ahead. Please.
Resident: He’s tachycardic.
Me: How fast?
Resident: 160 ?
Me: What’s the blood pressure?
Resident: 130/90
Me: Rhythm?
Resident: An SVT I think.. I gave adenosine. Nothing happened
Me: Audibly groaning. I’ll be in..
Forty five minutes later I’m at the bedside of a decidedly ill appearing man.
I want to be triumphant that his heart rate is only 145, and a quick glance at the telemetry monitor above his bed uncovers juicy p waves in a cadence that suggests this is no primary electrical arrhythmia.
Something is very wrong somewhere – the heart in this case is an innocent bystander being whipped into a frenzy to compensate for something.
At the moment the whip is a norepinephrine infusion being used to keep his blood pressure up.
I ask the nurse if the amount of norepinephrine infusing has been stable. She replies that his dose has been slowly escalating.
Eureka! I think – the heart rate response in this case is being driven by the norepinephrine – a powerful adrenaline that acts on beta receptors and alpha receptors within the body that increase heart rate and constrict the blood vessels to raise blood pressure. Fix the cause of the low blood pressure, come down on the norepinephrine, and perhaps the heart rate would be better.
But it turns out this particular post surgical patient doesn’t have a medical cause of low blood pressure I can find. I cycle through cardiac ultrasounds, blood gases, steroid and volume challenges, and try inching down on the norepinephrine.
All of it is to no avail. I’m growing more and more convinced this problem is surgical in nature. Perhaps an infarcted piece of bowel? All I know is that the man acts like he has no peripheral vascular tone.
An interesting thing happens shortly after. The norepinephrine drip runs out.
As one nurse runs to get another bag from the pharmacy – a quick cascade of events unfolds.
The brisk upstroke from the arterial line that marks the pressure wave generated with every beat of the heart starts to dampen. The color seems to visibly drain from the patients face, and he begins to complain that his vision is getting blurry. His systolic blood pressure is 70 – an almost forty point drop within a minute of the norepinephrine running out.
I call for help.
I try to keep a level tone. Project control, not panic.
“Open the code cart, I need a half a milligram of epinephrine”
“You’re going to be ok, sir. Hang with me.” I squeeze his hand.
He closes his eyes
The code cart – a fully stocked cabinet on wheels with almost everything you need for resuscitation efforts – is wheeled into the room. The epinephrine vial is handed to the nurse, and hurriedly pushed.
Within seconds, I can see the blood pressure and heart rate rise. The patient’s grip on my hand relaxes. Or maybe its my grip on his hand. I forget which. His vision returns to normal as his blood pressure ‘normalizes’.
Of course nothing has been fixed. Why his blood pressure remains low continues to be a mystery. The bag of norepinephrine soon isn’t enough even at its maximal dose. The same scenario (hypotension -> pallor -> vision loss ) recurs 30 minutes later, and another bolus of epinephrine aborts a rapid spiral towards pulselessness.
This case is an anecdote, the weakest possible form of evidence apparently. Yet there are powerful lessons learned that night. Blood flows in pulsatile fashion with a certain pressure head. Below some threshold of pressure, the end organs of the body stop functioning. Agents that are active on peripheral vasoconstrictor receptors (norepinephrine, epinephrine) raise blood pressure. Epinephrine was keeping this patient alive while a team worked to understand why his blood pressure was so low. My suspicion was that he was in something called distributive shock – a catastrophic life threatening syndrome that requires a furious hunt for cause to save the patient. Overwhelming infection and an even more aggressive immune response renders normally relatively impervious vasculature to be a sieve. At the present time the therapy is directed towards replacing the fluid lost in the intravascular space and using medications that act on peripheral vascular receptors that increase peripheral tone.
There is, of course, much that isn’t known about this process. Hopefully it will come to pass that we will arrive at a better understanding of what specifically creates this mileu so our therapies may be more directed. But for the time being, our solutions are limited by our current, always imperfect understanding of the world.
The culprit in this case was a leak of intestinal contents into the peritoneal space from two pieces of bowel that should have been exactly apposed. The body had attempted to tell us this very thing with that high heart rate post-operatively. It took us, the clinicians, some time to translate.
The uninformed prior: Unlearning what has been learned.
For many, medicine has for too long been an imperfect science. The history of medicine is replete with physicians acting with certainty in a manner that – in hindsight – was ineffective, or even worse – harmful. Blood letting to allow the release of bad humors is believed to have hastened the demise of the greatest American – George Washington. The disconcerting part of this is that the physician players were not motivated by anything but the best intentions. They relied on their experience, intuition and judgement to deliver exactly the wrong prescription. Intuition fails. No matter how many patients died soon after blood letting, operating biases didn’t let physicians link the two events. After all, the patients may have died even sooner if blood letting hadn’t been done.
The idea that medicine had progressed – by the 1980’s – to the point that doctors were not engaged in the equivalent of blood letting came under heavy fire when it was demonstrated a number of standard practices of the time could indeed be ineffective. Extra beats (also known as ectopic heart beats) after heart attacks were noted in cardiac units to portend a higher risk of dying suddenly. The obvious approach to this was to use medications that effectively suppressed ectopic heart beats. Testing this in a double blind randomized control trial did not just demonstrate ineffectiveness, but harm. More people randomized to suppression of ectopic beats actually died. It turns out the anti-arrhythmic drugs being used were actually proarrhythmic as well. The attack on ‘expertise’ that relied on intuition and experience was on, and it was a rout.
Glue ear – a condition that developed in the middle ears of little kids after ear infections was treated with insertion of a tube to drain that space. The trial to determine efficacy using a randomized trial to blindly allocate patients to surgery or no treatment?
Negative.
Many of the children turned out to do just fine if you left them alone. Given the fact that all procedures have a certain complication rate, the lack of efficacy here was no small matter.
And so it went – the populace had to be on guard not just against the afflictions of disease, but against the intuitions of its doctors.
Uncertainty reigned, and in search of certainty, the field fled to the warm embrace of ever greater empiricism. In the early ’80s from the McMaster University in Canada, David Sackett gave voice to a new sheriff – Evidence Based Medicine (EBM).
“EBM de-emphasizes intuition, unsystematic clinical expertise, and pathophysiologic rationale . . . and stresses the examination of evidence from clinical research. In 1960, the randomized trial was an oddity. It is now accepted that virtually no drug can enter clinical practice without a demonstration of its efficacy in clinical trials. Moreover the same randomized trial method is increasingly being applied to surgical therapies and diagnostic tests.” (Sackett et. al, Evidence Based Medicine)
The premise as outlined is simple – don’t believe anything that hasn’t been tested in a randomized control trial. The only real evidence is that found within RCTs or in reviews that amalgamated RCTs.
The usual response from EBM experts can be found below in the response to the statement that real evidence may come from outside an RCT.
It is quite possible Professor Francis is right on here about the specific subject being discussed, but the point is that there is an established hierarchy of evidence on display. The RCT is king, everything else is no better than the court jester.
While an RCT may certainly be better than anything cobbled together at a pub, the conventional parallel group RCT certainly isn’t always King of the Hill. As nicely expounded on by the prolific statistician Stephen Senn, there are plenty of potential errors the conventional RCT finds itself humbled by.
The clinician may thus feel somewhat mollified about conclusions drawn about the effect of epinephrine in the earlier anecdote.
The idea that real evidence may live outside the confines of RCTs was also countered by none other than the godfather of EBM, David Sackett:
“Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions. To find out about the accuracy of a diagnostic test, we need to find proper cross sectional studies of patients clinically suspected of harboring the relevant disorder, not a randomized trial. For a question about prognosis, we need proper follow up studies of patients assembled at a uniform, early point in the clinical course of their disease. And sometimes the evidence we need will come from the basic sciences such as genetics or immunology. It is when asking questions about therapy that we should try to avoid the non-experimental approaches, since these routinely lead to false positive conclusions about efficacy. Because the randomized trial, and especially the systematic review of several randomized trials, is so much more likely to inform us and so much less likely to mislead us, it has become the “gold standard” for judging whether a treatment does more good than harm. However,some questions about therapy do not require randomized trials (successful interventions for otherwise fatal conditions) or cannot wait for the trials to be conducted. And if no randomized trial has been carried out for our patient’s predicament, we must follow the trail to the next best external evidence and work from there. (Sacket et al, Evidence based medicine: what it is.. )”
Sackett also noted that there were therapies whose ” ‘face validity’ is so great that randomized trials were unanimously judged by the team to be both unnecessary, and, if a placebo would have been involved, unethical”.
In effect, there was always an escape clause to let common sense prevail over EBM. But as frequently happens in movements, the second generation of followers moves in directions unintended by the founders. If the safeguards in place involve only areas where equipoise exists, but equipoise is itself determined by fallible judgement, the range of unacceptable experiments becomes very narrow. This especially applies to new therapies where members of the community not involved in design and development have skeptical prior beliefs. This is, of course, not a bad thing – it is entirely possible that the usually overoptimistic prior of the developers of a new therapy are farther from the truth than the skeptics. But it is a major problem if we ask doctors to discard their prior beliefs that are not based in RCTs. In doing so, we are manufacturing equipoise. This means travel in dangerous ethical waters for physicians and their patients that is at best unwise, and at worst willfully foolish.
The EBM Wars: Manufacturing Equipoise (Part 1) published first on https://wittooth.tumblr.com/
0 notes
Text
The EBM Wars: Manufacturing Equipoise (Part 1)
By ANISH KOKA
The phone rings. It’s not supposed to be ringing. It’s 2 am. The voice on the other line is from an apologetic surgery resident.
Resident: There is this patient..
Me: Yes, go ahead. Please.
Resident: He’s tachycardic.
Me: How fast?
Resident: 160 ?
Me: What’s the blood pressure?
Resident: 130/90
Me: Rhythm?
Resident: An SVT I think.. I gave adenosine. Nothing happened
Me: Audibly groaning. I’ll be in..
Forty five minutes later I’m at the bedside of a decidedly ill appearing man.
I want to be triumphant that his heart rate is only 145, and a quick glance at the telemetry monitor above his bed uncovers juicy p waves in a cadence that suggests this is no primary electrical arrhythmia.
Something is very wrong somewhere – the heart in this case is an innocent bystander being whipped into a frenzy to compensate for something.
At the moment the whip is a norepinephrine infusion being used to keep his blood pressure up.
I ask the nurse if the amount of norepinephrine infusing has been stable. She replies that his dose has been slowly escalating.
Eureka! I think – the heart rate response in this case is being driven by the norepinephrine – a powerful adrenaline that acts on beta receptors and alpha receptors within the body that increase heart rate and constrict the blood vessels to raise blood pressure. Fix the cause of the low blood pressure, come down on the norepinephrine, and perhaps the heart rate would be better.
But it turns out this particular post surgical patient doesn’t have a medical cause of low blood pressure I can find. I cycle through cardiac ultrasounds, blood gases, steroid and volume challenges, and try inching down on the norepinephrine.
All of it is to no avail. I’m growing more and more convinced this problem is surgical in nature. Perhaps an infarcted piece of bowel? All I know is that the man acts like he has no peripheral vascular tone.
An interesting thing happens shortly after. The norepinephrine drip runs out.
As one nurse runs to get another bag from the pharmacy – a quick cascade of events unfolds.
The brisk upstroke from the arterial line that marks the pressure wave generated with every beat of the heart starts to dampen. The color seems to visibly drain from the patients face, and he begins to complain that his vision is getting blurry. His systolic blood pressure is 70 – an almost forty point drop within a minute of the norepinephrine running out.
I call for help.
I try to keep a level tone. Project control, not panic.
“Open the code cart, I need a half a milligram of epinephrine”
“You’re going to be ok, sir. Hang with me.” I squeeze his hand.
He closes his eyes
The code cart – a fully stocked cabinet on wheels with almost everything you need for resuscitation efforts – is wheeled into the room. The epinephrine vial is handed to the nurse, and hurriedly pushed.
Within seconds, I can see the blood pressure and heart rate rise. The patient’s grip on my hand relaxes. Or maybe its my grip on his hand. I forget which. His vision returns to normal as his blood pressure ‘normalizes’.
Of course nothing has been fixed. Why his blood pressure remains low continues to be a mystery. The bag of norepinephrine soon isn’t enough even at its maximal dose. The same scenario (hypotension -> pallor -> vision loss ) recurs 30 minutes later, and another bolus of epinephrine aborts a rapid spiral towards pulselessness.
This case is an anecdote, the weakest possible form of evidence apparently. Yet there are powerful lessons learned that night. Blood flows in pulsatile fashion with a certain pressure head. Below some threshold of pressure, the end organs of the body stop functioning. Agents that are active on peripheral vasoconstrictor receptors (norepinephrine, epinephrine) raise blood pressure. Epinephrine was keeping this patient alive while a team worked to understand why his blood pressure was so low. My suspicion was that he was in something called distributive shock – a catastrophic life threatening syndrome that requires a furious hunt for cause to save the patient. Overwhelming infection and an even more aggressive immune response renders normally relatively impervious vasculature to be a sieve. At the present time the therapy is directed towards replacing the fluid lost in the intravascular space and using medications that act on peripheral vascular receptors that increase peripheral tone.
There is, of course, much that isn’t known about this process. Hopefully it will come to pass that we will arrive at a better understanding of what specifically creates this mileu so our therapies may be more directed. But for the time being, our solutions are limited by our current, always imperfect understanding of the world.
The culprit in this case was a leak of intestinal contents into the peritoneal space from two pieces of bowel that should have been exactly apposed. The body had attempted to tell us this very thing with that high heart rate post-operatively. It took us, the clinicians, some time to translate.
The uninformed prior: Unlearning what has been learned.
For many, medicine has for too long been an imperfect science. The history of medicine is replete with physicians acting with certainty in a manner that – in hindsight – was ineffective, or even worse – harmful. Blood letting to allow the release of bad humors is believed to have hastened the demise of the greatest American – George Washington. The disconcerting part of this is that the physician players were not motivated by anything but the best intentions. They relied on their experience, intuition and judgement to deliver exactly the wrong prescription. Intuition fails. No matter how many patients died soon after blood letting, operating biases didn’t let physicians link the two events. After all, the patients may have died even sooner if blood letting hadn’t been done.
The idea that medicine had progressed – by the 1980’s – to the point that doctors were not engaged in the equivalent of blood letting came under heavy fire when it was demonstrated a number of standard practices of the time could indeed be ineffective. Extra beats (also known as ectopic heart beats) after heart attacks were noted in cardiac units to portend a higher risk of dying suddenly. The obvious approach to this was to use medications that effectively suppressed ectopic heart beats. Testing this in a double blind randomized control trial did not just demonstrate ineffectiveness, but harm. More people randomized to suppression of ectopic beats actually died. It turns out the anti-arrhythmic drugs being used were actually proarrhythmic as well. The attack on ‘expertise’ that relied on intuition and experience was on, and it was a rout.
Glue ear – a condition that developed in the middle ears of little kids after ear infections was treated with insertion of a tube to drain that space. The trial to determine efficacy using a randomized trial to blindly allocate patients to surgery or no treatment?
Negative.
Many of the children turned out to do just fine if you left them alone. Given the fact that all procedures have a certain complication rate, the lack of efficacy here was no small matter.
And so it went – the populace had to be on guard not just against the afflictions of disease, but against the intuitions of its doctors.
Uncertainty reigned, and in search of certainty, the field fled to the warm embrace of ever greater empiricism. In the early ’80s from the McMaster University in Canada, David Sackett gave voice to a new sheriff – Evidence Based Medicine (EBM).
“EBM de-emphasizes intuition, unsystematic clinical expertise, and pathophysiologic rationale . . . and stresses the examination of evidence from clinical research. In 1960, the randomized trial was an oddity. It is now accepted that virtually no drug can enter clinical practice without a demonstration of its efficacy in clinical trials. Moreover the same randomized trial method is increasingly being applied to surgical therapies and diagnostic tests.” (Sackett et. al, Evidence Based Medicine)
The premise as outlined is simple – don’t believe anything that hasn’t been tested in a randomized control trial. The only real evidence is that found within RCTs or in reviews that amalgamated RCTs.
The usual response from EBM experts can be found below in the response to the statement that real evidence may come from outside an RCT.
It is quite possible Professor Francis is right on here about the specific subject being discussed, but the point is that there is an established hierarchy of evidence on display. The RCT is king, everything else is no better than the court jester.
While an RCT may certainly be better than anything cobbled together at a pub, the conventional parallel group RCT certainly isn’t always King of the Hill. As nicely expounded on by the prolific statistician Stephen Senn, there are plenty of potential errors the conventional RCT finds itself humbled by.
The clinician may thus feel somewhat mollified about conclusions drawn about the effect of epinephrine in the earlier anecdote.
The idea that real evidence may live outside the confines of RCTs was also countered by none other than the godfather of EBM, David Sackett:
“Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions. To find out about the accuracy of a diagnostic test, we need to find proper cross sectional studies of patients clinically suspected of harboring the relevant disorder, not a randomized trial. For a question about prognosis, we need proper follow up studies of patients assembled at a uniform, early point in the clinical course of their disease. And sometimes the evidence we need will come from the basic sciences such as genetics or immunology. It is when asking questions about therapy that we should try to avoid the non-experimental approaches, since these routinely lead to false positive conclusions about efficacy. Because the randomized trial, and especially the systematic review of several randomized trials, is so much more likely to inform us and so much less likely to mislead us, it has become the “gold standard” for judging whether a treatment does more good than harm. However,some questions about therapy do not require randomized trials (successful interventions for otherwise fatal conditions) or cannot wait for the trials to be conducted. And if no randomized trial has been carried out for our patient’s predicament, we must follow the trail to the next best external evidence and work from there. (Sacket et al, Evidence based medicine: what it is.. )”
Sackett also noted that there were therapies whose ” ‘face validity’ is so great that randomized trials were unanimously judged by the team to be both unnecessary, and, if a placebo would have been involved, unethical”.
In effect, there was always an escape clause to let common sense prevail over EBM. But as frequently happens in movements, the second generation of followers moves in directions unintended by the founders. If the safeguards in place involve only areas where equipoise exists, but equipoise is itself determined by fallible judgement, the range of unacceptable experiments becomes very narrow. This especially applies to new therapies where members of the community not involved in design and development have skeptical prior beliefs. This is, of course, not a bad thing – it is entirely possible that the usually overoptimistic prior of the developers of a new therapy are farther from the truth than the skeptics. But it is a major problem if we ask doctors to discard their prior beliefs that are not based in RCTs. In doing so, we are manufacturing equipoise. This means travel in dangerous ethical waters for physicians and their patients that is at best unwise, and at worst willfully foolish.
The EBM Wars: Manufacturing Equipoise (Part 1) published first on https://wittooth.tumblr.com/
0 notes
Text
The EBM Wars: Manufacturing Equipoise (Part 1)
By ANISH KOKA
The phone rings. It’s not supposed to be ringing. It’s 2 am. The voice on the other line is from an apologetic surgery resident.
Resident: There is this patient..
Me: Yes, go ahead. Please.
Resident: He’s tachycardic.
Me: How fast?
Resident: 160 ?
Me: What’s the blood pressure?
Resident: 130/90
Me: Rhythm?
Resident: An SVT I think.. I gave adenosine. Nothing happened
Me: Audibly groaning. I’ll be in..
Forty five minutes later I’m at the bedside of a decidedly ill appearing man.
I want to be triumphant that his heart rate is only 145, and a quick glance at the telemetry monitor above his bed uncovers juicy p waves in a cadence that suggests this is no primary electrical arrhythmia.
Something is very wrong somewhere – the heart in this case is an innocent bystander being whipped into a frenzy to compensate for something.
At the moment the whip is a norepinephrine infusion being used to keep his blood pressure up.
I ask the nurse if the amount of norepinephrine infusing has been stable. She replies that his dose has been slowly escalating.
Eureka! I think – the heart rate response in this case is being driven by the norepinephrine – a powerful adrenaline that acts on beta receptors and alpha receptors within the body that increase heart rate and constrict the blood vessels to raise blood pressure. Fix the cause of the low blood pressure, come down on the norepinephrine, and perhaps the heart rate would be better.
But it turns out this particular post surgical patient doesn’t have a medical cause of low blood pressure I can find. I cycle through cardiac ultrasounds, blood gases, steroid and volume challenges, and try inching down on the norepinephrine.
All of it is to no avail. I’m growing more and more convinced this problem is surgical in nature. Perhaps an infarcted piece of bowel? All I know is that the man acts like he has no peripheral vascular tone.
An interesting thing happens shortly after. The norepinephrine drip runs out.
As one nurse runs to get another bag from the pharmacy – a quick cascade of events unfolds.
The brisk upstroke from the arterial line that marks the pressure wave generated with every beat of the heart starts to dampen. The color seems to visibly drain from the patients face, and he begins to complain that his vision is getting blurry. His systolic blood pressure is 70 – an almost forty point drop within a minute of the norepinephrine running out.
I call for help.
I try to keep a level tone. Project control, not panic.
“Open the code cart, I need a half a milligram of epinephrine”
“You’re going to be ok, sir. Hang with me.” I squeeze his hand.
He closes his eyes
The code cart – a fully stocked cabinet on wheels with almost everything you need for resuscitation efforts – is wheeled into the room. The epinephrine vial is handed to the nurse, and hurriedly pushed.
Within seconds, I can see the blood pressure and heart rate rise. The patient’s grip on my hand relaxes. Or maybe its my grip on his hand. I forget which. His vision returns to normal as his blood pressure ‘normalizes’.
Of course nothing has been fixed. Why his blood pressure remains low continues to be a mystery. The bag of norepinephrine soon isn’t enough even at its maximal dose. The same scenario (hypotension -> pallor -> vision loss ) recurs 30 minutes later, and another bolus of epinephrine aborts a rapid spiral towards pulselessness.
This case is an anecdote, the weakest possible form of evidence apparently. Yet there are powerful lessons learned that night. Blood flows in pulsatile fashion with a certain pressure head. Below some threshold of pressure, the end organs of the body stop functioning. Agents that are active on peripheral vasoconstrictor receptors (norepinephrine, epinephrine) raise blood pressure. Epinephrine was keeping this patient alive while a team worked to understand why his blood pressure was so low. My suspicion was that he was in something called distributive shock – a catastrophic life threatening syndrome that requires a furious hunt for cause to save the patient. Overwhelming infection and an even more aggressive immune response renders normally relatively impervious vasculature to be a sieve. At the present time the therapy is directed towards replacing the fluid lost in the intravascular space and using medications that act on peripheral vascular receptors that increase peripheral tone.
There is, of course, much that isn’t known about this process. Hopefully it will come to pass that we will arrive at a better understanding of what specifically creates this mileu so our therapies may be more directed. But for the time being, our solutions are limited by our current, always imperfect understanding of the world.
The culprit in this case was a leak of intestinal contents into the peritoneal space from two pieces of bowel that should have been exactly apposed. The body had attempted to tell us this very thing with that high heart rate post-operatively. It took us, the clinicians, some time to translate.
The uninformed prior: Unlearning what has been learned.
For many, medicine has for too long been an imperfect science. The history of medicine is replete with physicians acting with certainty in a manner that – in hindsight – was ineffective, or even worse – harmful. Blood letting to allow the release of bad humors is believed to have hastened the demise of the greatest American – George Washington. The disconcerting part of this is that the physician players were not motivated by anything but the best intentions. They relied on their experience, intuition and judgement to deliver exactly the wrong prescription. Intuition fails. No matter how many patients died soon after blood letting, operating biases didn’t let physicians link the two events. After all, the patients may have died even sooner if blood letting hadn’t been done.
The idea that medicine had progressed – by the 1980’s – to the point that doctors were not engaged in the equivalent of blood letting came under heavy fire when it was demonstrated a number of standard practices of the time could indeed be ineffective. Extra beats (also known as ectopic heart beats) after heart attacks were noted in cardiac units to portend a higher risk of dying suddenly. The obvious approach to this was to use medications that effectively suppressed ectopic heart beats. Testing this in a double blind randomized control trial did not just demonstrate ineffectiveness, but harm. More people randomized to suppression of ectopic beats actually died. It turns out the anti-arrhythmic drugs being used were actually proarrhythmic as well. The attack on ‘expertise’ that relied on intuition and experience was on, and it was a rout.
Glue ear – a condition that developed in the middle ears of little kids after ear infections was treated with insertion of a tube to drain that space. The trial to determine efficacy using a randomized trial to blindly allocate patients to surgery or no treatment?
Negative.
Many of the children turned out to do just fine if you left them alone. Given the fact that all procedures have a certain complication rate, the lack of efficacy here was no small matter.
And so it went – the populace had to be on guard not just against the afflictions of disease, but against the intuitions of its doctors.
Uncertainty reigned, and in search of certainty, the field fled to the warm embrace of ever greater empiricism. In the early ’80s from the McMaster University in Canada, David Sackett gave voice to a new sheriff – Evidence Based Medicine (EBM).
“EBM de-emphasizes intuition, unsystematic clinical expertise, and pathophysiologic rationale . . . and stresses the examination of evidence from clinical research. In 1960, the randomized trial was an oddity. It is now accepted that virtually no drug can enter clinical practice without a demonstration of its efficacy in clinical trials. Moreover the same randomized trial method is increasingly being applied to surgical therapies and diagnostic tests.” (Sackett et. al, Evidence Based Medicine)
The premise as outlined is simple – don’t believe anything that hasn’t been tested in a randomized control trial. The only real evidence is that found within RCTs or in reviews that amalgamated RCTs.
The usual response from EBM experts can be found below in the response to the statement that real evidence may come from outside an RCT.
It is quite possible Professor Francis is right on here about the specific subject being discussed, but the point is that there is an established hierarchy of evidence on display. The RCT is king, everything else is no better than the court jester.
While an RCT may certainly be better than anything cobbled together at a pub, the conventional parallel group RCT certainly isn’t always King of the Hill. As nicely expounded on by the prolific statistician Stephen Senn, there are plenty of potential errors the conventional RCT finds itself humbled by.
The clinician may thus feel somewhat mollified about conclusions drawn about the effect of epinephrine in the earlier anecdote.
The idea that real evidence may live outside the confines of RCTs was also countered by none other than the godfather of EBM, David Sackett:
“Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions. To find out about the accuracy of a diagnostic test, we need to find proper cross sectional studies of patients clinically suspected of harboring the relevant disorder, not a randomized trial. For a question about prognosis, we need proper follow up studies of patients assembled at a uniform, early point in the clinical course of their disease. And sometimes the evidence we need will come from the basic sciences such as genetics or immunology. It is when asking questions about therapy that we should try to avoid the non-experimental approaches, since these routinely lead to false positive conclusions about efficacy. Because the randomized trial, and especially the systematic review of several randomized trials, is so much more likely to inform us and so much less likely to mislead us, it has become the “gold standard” for judging whether a treatment does more good than harm. However,some questions about therapy do not require randomized trials (successful interventions for otherwise fatal conditions) or cannot wait for the trials to be conducted. And if no randomized trial has been carried out for our patient’s predicament, we must follow the trail to the next best external evidence and work from there. (Sacket et al, Evidence based medicine: what it is.. )”
Sackett also noted that there were therapies whose ” ‘face validity’ is so great that randomized trials were unanimously judged by the team to be both unnecessary, and, if a placebo would have been involved, unethical”.
In effect, there was always an escape clause to let common sense prevail over EBM. But as frequently happens in movements, the second generation of followers moves in directions unintended by the founders. If the safeguards in place involve only areas where equipoise exists, but equipoise is itself determined by fallible judgement, the range of unacceptable experiments becomes very narrow. This especially applies to new therapies where members of the community not involved in design and development have skeptical prior beliefs. This is, of course, not a bad thing – it is entirely possible that the usually overoptimistic prior of the developers of a new therapy are farther from the truth than the skeptics. But it is a major problem if we ask doctors to discard their prior beliefs that are not based in RCTs. In doing so, we are manufacturing equipoise. This means travel in dangerous ethical waters for physicians and their patients that is at best unwise, and at worst willfully foolish.
The EBM Wars: Manufacturing Equipoise (Part 1) published first on https://wittooth.tumblr.com/
0 notes
Text
The EBM Wars: Manufacturing Equipoise (Part 1)
By ANISH KOKA
The phone rings. It’s not supposed to be ringing. It’s 2 am. The voice on the other line is from an apologetic surgery resident.
Resident: There is this patient..
Me: Yes, go ahead. Please.
Resident: He’s tachycardic.
Me: How fast?
Resident: 160 ?
Me: What’s the blood pressure?
Resident: 130/90
Me: Rhythm?
Resident: An SVT I think.. I gave adenosine. Nothing happened
Me: Audibly groaning. I’ll be in..
Forty five minutes later I’m at the bedside of a decidedly ill appearing man.
I want to be triumphant that his heart rate is only 145, and a quick glance at the telemetry monitor above his bed uncovers juicy p waves in a cadence that suggests this is no primary electrical arrhythmia.
Something is very wrong somewhere – the heart in this case is an innocent bystander being whipped into a frenzy to compensate for something.
At the moment the whip is a norepinephrine infusion being used to keep his blood pressure up.
I ask the nurse if the amount of norepinephrine infusing has been stable. She replies that his dose has been slowly escalating.
Eureka! I think – the heart rate response in this case is being driven by the norepinephrine – a powerful adrenaline that acts on beta receptors and alpha receptors within the body that increase heart rate and constrict the blood vessels to raise blood pressure. Fix the cause of the low blood pressure, come down on the norepinephrine, and perhaps the heart rate would be better.
But it turns out this particular post surgical patient doesn’t have a medical cause of low blood pressure I can find. I cycle through cardiac ultrasounds, blood gases, steroid and volume challenges, and try inching down on the norepinephrine.
All of it is to no avail. I’m growing more and more convinced this problem is surgical in nature. Perhaps an infarcted piece of bowel? All I know is that the man acts like he has no peripheral vascular tone.
An interesting thing happens shortly after. The norepinephrine drip runs out.
As one nurse runs to get another bag from the pharmacy – a quick cascade of events unfolds.
The brisk upstroke from the arterial line that marks the pressure wave generated with every beat of the heart starts to dampen. The color seems to visibly drain from the patients face, and he begins to complain that his vision is getting blurry. His systolic blood pressure is 70 – an almost forty point drop within a minute of the norepinephrine running out.
I call for help.
I try to keep a level tone. Project control, not panic.
“Open the code cart, I need a half a milligram of epinephrine”
“You’re going to be ok, sir. Hang with me.” I squeeze his hand.
He closes his eyes
The code cart – a fully stocked cabinet on wheels with almost everything you need for resuscitation efforts – is wheeled into the room. The epinephrine vial is handed to the nurse, and hurriedly pushed.
Within seconds, I can see the blood pressure and heart rate rise. The patient’s grip on my hand relaxes. Or maybe its my grip on his hand. I forget which. His vision returns to normal as his blood pressure ‘normalizes’.
Of course nothing has been fixed. Why his blood pressure remains low continues to be a mystery. The bag of norepinephrine soon isn’t enough even at its maximal dose. The same scenario (hypotension -> pallor -> vision loss ) recurs 30 minutes later, and another bolus of epinephrine aborts a rapid spiral towards pulselessness.
This case is an anecdote, the weakest possible form of evidence apparently. Yet there are powerful lessons learned that night. Blood flows in pulsatile fashion with a certain pressure head. Below some threshold of pressure, the end organs of the body stop functioning. Agents that are active on peripheral vasoconstrictor receptors (norepinephrine, epinephrine) raise blood pressure. Epinephrine was keeping this patient alive while a team worked to understand why his blood pressure was so low. My suspicion was that he was in something called distributive shock – a catastrophic life threatening syndrome that requires a furious hunt for cause to save the patient. Overwhelming infection and an even more aggressive immune response renders normally relatively impervious vasculature to be a sieve. At the present time the therapy is directed towards replacing the fluid lost in the intravascular space and using medications that act on peripheral vascular receptors that increase peripheral tone.
There is, of course, much that isn’t known about this process. Hopefully it will come to pass that we will arrive at a better understanding of what specifically creates this mileu so our therapies may be more directed. But for the time being, our solutions are limited by our current, always imperfect understanding of the world.
The culprit in this case was a leak of intestinal contents into the peritoneal space from two pieces of bowel that should have been exactly apposed. The body had attempted to tell us this very thing with that high heart rate post-operatively. It took us, the clinicians, some time to translate.
The uninformed prior: Unlearning what has been learned.
For many, medicine has for too long been an imperfect science. The history of medicine is replete with physicians acting with certainty in a manner that – in hindsight – was ineffective, or even worse – harmful. Blood letting to allow the release of bad humors is believed to have hastened the demise of the greatest American – George Washington. The disconcerting part of this is that the physician players were not motivated by anything but the best intentions. They relied on their experience, intuition and judgement to deliver exactly the wrong prescription. Intuition fails. No matter how many patients died soon after blood letting, operating biases didn’t let physicians link the two events. After all, the patients may have died even sooner if blood letting hadn’t been done.
The idea that medicine had progressed – by the 1980’s – to the point that doctors were not engaged in the equivalent of blood letting came under heavy fire when it was demonstrated a number of standard practices of the time could indeed be ineffective. Extra beats (also known as ectopic heart beats) after heart attacks were noted in cardiac units to portend a higher risk of dying suddenly. The obvious approach to this was to use medications that effectively suppressed ectopic heart beats. Testing this in a double blind randomized control trial did not just demonstrate ineffectiveness, but harm. More people randomized to suppression of ectopic beats actually died. It turns out the anti-arrhythmic drugs being used were actually proarrhythmic as well. The attack on ‘expertise’ that relied on intuition and experience was on, and it was a rout.
Glue ear – a condition that developed in the middle ears of little kids after ear infections was treated with insertion of a tube to drain that space. The trial to determine efficacy using a randomized trial to blindly allocate patients to surgery or no treatment?
Negative.
Many of the children turned out to do just fine if you left them alone. Given the fact that all procedures have a certain complication rate, the lack of efficacy here was no small matter.
And so it went – the populace had to be on guard not just against the afflictions of disease, but against the intuitions of its doctors.
Uncertainty reigned, and in search of certainty, the field fled to the warm embrace of ever greater empiricism. In the early ’80s from the McMaster University in Canada, David Sackett gave voice to a new sheriff – Evidence Based Medicine (EBM).
“EBM de-emphasizes intuition, unsystematic clinical expertise, and pathophysiologic rationale . . . and stresses the examination of evidence from clinical research. In 1960, the randomized trial was an oddity. It is now accepted that virtually no drug can enter clinical practice without a demonstration of its efficacy in clinical trials. Moreover the same randomized trial method is increasingly being applied to surgical therapies and diagnostic tests.” (Sackett et. al, Evidence Based Medicine)
The premise as outlined is simple – don’t believe anything that hasn’t been tested in a randomized control trial. The only real evidence is that found within RCTs or in reviews that amalgamated RCTs.
The usual response from EBM experts can be found below in the response to the statement that real evidence may come from outside an RCT.
It is quite possible Professor Francis is right on here about the specific subject being discussed, but the point is that there is an established hierarchy of evidence on display. The RCT is king, everything else is no better than the court jester.
While an RCT may certainly be better than anything cobbled together at a pub, the conventional parallel group RCT certainly isn’t always King of the Hill. As nicely expounded on by the prolific statistician Stephen Senn, there are plenty of potential errors the conventional RCT finds itself humbled by.
The clinician may thus feel somewhat mollified about conclusions drawn about the effect of epinephrine in the earlier anecdote.
The idea that real evidence may live outside the confines of RCTs was also countered by none other than the godfather of EBM, David Sackett:
“Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions. To find out about the accuracy of a diagnostic test, we need to find proper cross sectional studies of patients clinically suspected of harboring the relevant disorder, not a randomized trial. For a question about prognosis, we need proper follow up studies of patients assembled at a uniform, early point in the clinical course of their disease. And sometimes the evidence we need will come from the basic sciences such as genetics or immunology. It is when asking questions about therapy that we should try to avoid the non-experimental approaches, since these routinely lead to false positive conclusions about efficacy. Because the randomized trial, and especially the systematic review of several randomized trials, is so much more likely to inform us and so much less likely to mislead us, it has become the “gold standard” for judging whether a treatment does more good than harm. However,some questions about therapy do not require randomized trials (successful interventions for otherwise fatal conditions) or cannot wait for the trials to be conducted. And if no randomized trial has been carried out for our patient’s predicament, we must follow the trail to the next best external evidence and work from there. (Sacket et al, Evidence based medicine: what it is.. )”
Sackett also noted that there were therapies whose ” ‘face validity’ is so great that randomized trials were unanimously judged by the team to be both unnecessary, and, if a placebo would have been involved, unethical”.
In effect, there was always an escape clause to let common sense prevail over EBM. But as frequently happens in movements, the second generation of followers moves in directions unintended by the founders. If the safeguards in place involve only areas where equipoise exists, but equipoise is itself determined by fallible judgement, the range of unacceptable experiments becomes very narrow. This especially applies to new therapies where members of the community not involved in design and development have skeptical prior beliefs. This is, of course, not a bad thing – it is entirely possible that the usually overoptimistic prior of the developers of a new therapy are farther from the truth than the skeptics. But it is a major problem if we ask doctors to discard their prior beliefs that are not based in RCTs. In doing so, we are manufacturing equipoise. This means travel in dangerous ethical waters for physicians and their patients that is at best unwise, and at worst willfully foolish.
The EBM Wars: Manufacturing Equipoise (Part 1) published first on https://wittooth.tumblr.com/
0 notes