#but it's apparently not a high dose and Dr 2 says that's a sign of a low caffeine tolerance
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The average Tumblr user visits about 67 pages every month.
Text
A little advice
If you like me
have terrible neighbors
Who spent 3 hours shouting in the middle of the night
causing you to have to take a half day at work just so you'd sleep enough to be safe to drive
and also 36 miligrams of caffeine
in order to do things like cheerfully disassemble a cow to find out what kind of lung lesions it had
(Gross ones. The lesions were gross. And that's by our standards, see above about cow disassembly)
and additionally haven't regularly drank soda in 5+ years
and certainly not 20 oz of it at once
Maaaaaybe don't take your caffeine in soda form. My bones hurt. Why does carbonation make my bones hurt.
#also the coworkers were very helpful#in a vetmed type of way#things you don't know about vets probably is that they will self diagnose and self treat almost anything#leading to an ongoing joke that we're going to borrow various equipment to run bloodwork on ourselves#anyway 36 mg is probably too much caffeine#for me#but it's apparently not a high dose and Dr 2 says that's a sign of a low caffeine tolerance#I think it might have more to do with the cumulative 6 hours of sleep
7 notes
·
View notes
Text
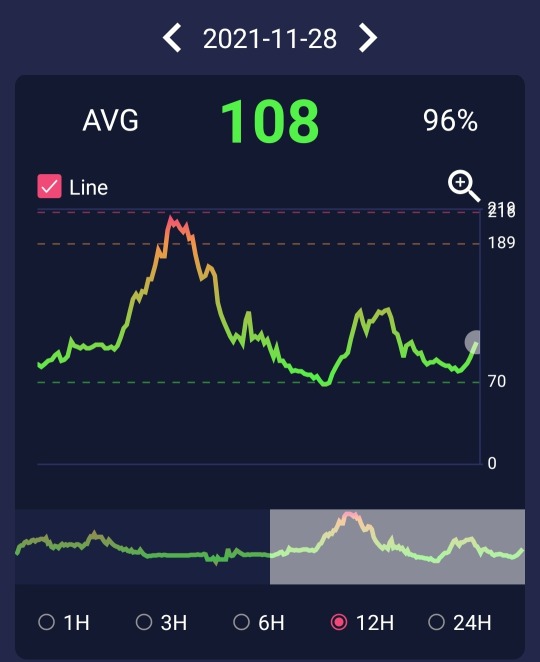
That extra info from the new Libre 2-plus-Diabox CGM setup is already coming in very handy indeed!
(Besides "just" enjoying being able to glance at a screen whenever I like, without a very minor blood sacrifice being required to satisfy my curiosity about glucose levels.)
From my first full day using it, starting from roughly when I got up as reflected by those teeny spikes at the beginning:


Hmm, that is really not looking right! That huge mountain started rising up before I even got anything in besides the usual cup of coffee--which really does not seem to affect my blood sugar otherwise. 🤔 And the pre-breakfast insulin should have at least been on the verge of kicking in when it started climbing? The extra correction dose barely seemed to touch it after it skyrocketed up to a concerning point?
Seriously, WTF body?! 😒
Okay, wait! I know I've heard about something like this before, from other diabetics.
But, I was up for at least an hour before my blood sugar started shooting up for no apparent reason? Idk, maybe that doesn't quite fit.
Still, it's worth cautiously trying a little insulin first thing tomorrow, just in case. If it drops too much, I have a good excuse to drink some of that fresh cider. ¯\_(ツ)_/¯

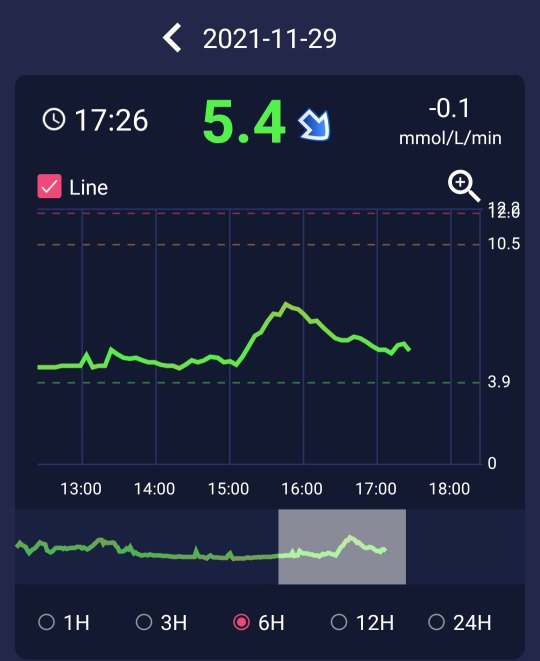
Erm, NOPE! Second verse...
INTERESTING to see that exactly the same thing happened again, if more than a little nerve wracking! Either one preemptive unit of insulin wasn't NEARLY enough, or that's not the right explanation or solution.
(Just barely avoided it dipping low after shooting an extra meal's worth of Novorapid then taking a short roll around the neighborhood, to try and bring that shit back down. Thanks again to keeping a close eye on the Diabox display, and grabbing a fast snack to keep ahead of it! 😃)
Anyway, at least the tentative little preemptive insulin dose didn't seem to make matters worse, or even bring my blood sugar down AT ALL like it normally would.
May well be worth trying to hit it much harder in advance next time, and see what happens? Again, worst case, I'll be guzzling something sugary or chomping down on candy for breakfast.
And there are still a few things to try if that still doesn't help.
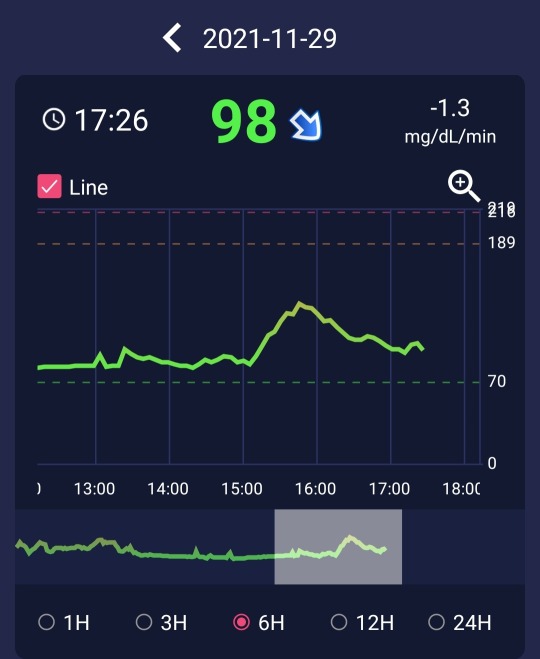
And, success! After taking a usual breakfast-sized dose of Novorapid as soon as I got up.
By the time I was ready to try some breakfast, the levels had not budged in any direction--which I took as an encouraging sign. So, I said fuck it and dosed more insulin as usual before getting in something lower in carbs, trying to play it safe.
(Normally I would say to change only one variable at a time, but jfc. I really DID NOT want a repeat of yesterday's stress!)
Result: Just about the sort of "normal" meal response I would expect? Definitely nothing alarming today. 🎉🥳🎊
And I felt way less like hot exhausted garbage, trying to get some shit done around here before Night Owl Lunch. (Suppertime just recently, for the folks on more socially acceptable schedules.)
Even without the added stress of watching the runaway roller coaster in near realtime, that shit COULD NOT possibly be good for your system. And this is with keeping watch and correction dosing to try and bring it back down. Who knows how high it might have been regularly spiking without that? 😰
I had no reason to think that anything weird might even be going on there, and had slacked on the after meal testing tbqh. Didn't really want to poke myself more than like 4-5 times a day on the regular, unless there was something more obviously unusual happening. So, I fell into a bit of a routine, and had generally called checking before I ate good enough. ¯\_(ツ)_/¯
And I really doubt that's unusual.
TL;DR: It's looking remarkably like I've been dealing with some sneaky version of the fairly common "Foot-on-the-Floor" phenomenon with my blood sugar, for Glod only knows how long. And I might not have known about it for a long time if ever, had I not FINALLY gotten set up with CGM technology to help me keep a better eye on what my busted diabetic metabolism is doing.
I had been finger-stick testing for breakfast not long after I got up, and this particular wacky endocrine stunt has apparently been working on just enough of a time delay for me to miss it. Then, by a couple-few hours later when I'm thinking about eating and test again? It's been back to high-"normal" at worst, the vast majority of the time.
This is yet another illustration of why at least all T1 diabetics--or anyone relying on insulin to stay alive and even vaguely healthy--should have ready, affordable access to continuous glucose monitoring technology! Plus any other tools that might make keeping on top of the situation easier, safer, and actually doable.
(Not to mention other folks who might benefit from that, and other currently available medical aids/assistance.)
Currently stuck in my head, however inappropriately! 😅
#personal#cgms#t1 diabetes#type 1 diabetes#diabetes#continuous glucose monitoring#look out honey cause i'm using technology#diabox#freestyle libre 2
13 notes
·
View notes
Text
The Same - Chapter 7 - 3/6
Meeting Elaine Brown slightly lifts his mood, but the conversation with his father is still weighing heavy on the back of his mind. Getting her signature is a bittersweet moment, as he forgot to bring a pen and made himself a fool in front of her.
Still, he's proud of himself for asking her to do such a thing during a case.
He observes the two of the doctor's as they speak about Alice Downey. Dr. Brown is lying. He can tell. There's something they're not telling them, something they're hiding.
Malcolm is disappointed. He had looked up to Elaine Brown, and it was eye opening to see her lie to their faces.
Pressures of doctoral pursuit, his ass. There was something wrong with this situation.
He just wasn't sure what it was.
---
By the time they get back to the debriefing room, Malcolm is exhausted. His entire body is tense, and if he doesn't stretch out his legs soon he'll go into a fit of charlie horses and muscle spasms.
Legs stretching underneath the table, Dani takes over for the moment. Pinning the picture of Alice Downey on the board.
She's a kind looking young woman. He wonders what drove her to suicide. Affair with Professor Holton? Drugs? Depression?
He wasn't sure. There was no true way to tell, as the man closest to her was found with no brain.
"What do you think, Bright?" Dani asks, and said man sighs. Putting his signed book on the table.
"I think that Dr. Brown is lying. Never meet your heroes." He gives a sardonic smile.
JT takes over. "I went over to the admin building. They're all as crazy about Elaine Brown as you are."
Malcolm rolls his eyes. Hard.
"But they did find this crazy anonymously submitted letter with theories about Alice Downey's suicide." He puts it on the table. "Look familiar?"
Malcolm's eyes widened, and he grabbed the paper, reading it over. The same scrawl, same off kilter lining of the words.. It was their guy.
"The killer was accusing the psych department of off-the-book experiments."
Dani's eyebrows raise. "How off the book?"
Bright continues reading, trying to make sense of the writing. It was much more coherent than the one left of the crime scene.
"Giving students LSD. Apparently, Alice was tripping on acid when she went over that building. Pretty serious accusations."
Malcolm sets the paper down again, examining the words and their placing closely.
"This is older than the other paper." He says after a long silence. "It's slightly inflammatory, but much more coherent. It shows our killer's slow descent into a full psychotic break."
Malcom runs his fingers through his hair (damp, slightly greasy from not showering the night before) inhaling through his nose. "There's some meaning in these words.. Something he has to be telling us. What is he saying? What does he want us to find?"
Bright's eyes are darting all around the evidence board, analyzing each piece and trying to put it together. Like a jigsaw puzzle.
An incredibly difficult puzzle.
While facing this dilemma, Dani gets a call and heads out of the room. He can't pay attention to her right now, he needs to crack the letters opens, find out the meaning, find the answers..
He's broken out of his thoughts when she comes back in, firmly telling them that Carl Mitchell had been drugged and they needed to head back to the research building.
Malcolm follows the other two with no hesitation, quickly yelling into Gil's office that they're Ieaving.
The man looks panicked for a second, but by the time he gets up to follow them, they're gone.
-----
For a long, gruelling moment, Malcolm thinks they are too late. Thankfully, going up the roof stairs and entering the space, he hears the muffled telltale, fearful babbling of someone taking too much LSD.
"He's still here!" Malcolm says, and JT goes off, searching for the killer. Dani stays for a moment, mouth open in shock.
They made it just in time. Carl Mitchell is laying on the ground, hands and mouth tied. Saws, knifes, and blades lay next to him. There is a line drawn on his head, a guide line.
Like a doctor would draw for plastic surgery, Malcolm thinks as he takes the tape off and cuts him free.
"You're safe now, Carl." Malcolm says, helping the man to his feet.
"Do you see? Do you see it? Do you see how high? I have to fight.. I have to fight it. Oh, please! Please!" Carl rambles, and Bright grabs him by the shoulders.
"Listen to me, Carl. You're high on LSD. In large doses, it can mimic a psychotic break." He tells the dosed man, trying to calm him down.
"Police!" Malcolm hears a far off shout.
"I need to fight, need to..!" Carl grabs him, turning him around and backing up.
"Carl, Carl, calm down. You don't need to fight, just breathe. Everything is alright." Malcolm tries his best to calm the man down, but it's not doing much. He feels cold metal against his neck and shit, he grabbed one of the blades. When had he done that?
Malcolm is scared. He's either going to get his throat slit or fall with Carl over the side of the building to their death. He knows not to struggle, but his heart is hammering so hard in his ears he can't help but want to squirm.
He looks up as Dani approaches, gun raised. "Don't shoot!" He tells her. "He's been dosed. He doesn't know what he's doing."
Dani slowly lowers her pistol. "What can you do?"
Malcolm's muscles tighten as Carl begins walking back again. "Not a whole hell of a lot." Except get away from the drugged man, which would either end with his throat cut open or the professor hurtled over the building.
Neither were good options.
"Oh, it's what they want!" The man holding the blade to his throat says, and if he can just get him to let go of it he can get out..
"We're so high up! Oh, we're so high up!" Closer and closer to the edge they go, and Malcolm can see the fear in Dani's eyes. His body is locking up, ready for impact.
They're going to fall.
Mere inches from falling, Malcolm relaxes and heads into action. He grabs the two protruding bones of Mitchell's wrist, squeezes, and feels him drop the knife. Gasping, Malcolm shoves his elbow into him and the man falls backwards, off of the building.
"Oh!" Dani yells, running forward as Malcolm barely catches himself from falling with him. He's disoriented for a moment.
"Bright." Detective Powell says, and he risks a peek over the ledge, preparing for a bloody splatter on the sidewalk 10 stories down.
In reality, 2 stories down, there was a miraculous balcony which Carl Mitchell had fell on. Malcolm feels his body relax with sheer relief. Thank God. He hadn't killed someone.
"Did you know that was there?" He hears his companion ask.
"..Sure." He says unconvincingly, wiping the sweat from his face. Sure.
-------
As they return to the NYPD building, Dani asks him a question that derails him.
"So, what should I put in the report?" She asks as they walk into the detective floor. All three of them had been miraculously silent on the ride back over, and on the elevator trip up.
Malcolm looks at her strangely. "Well, I don't know. When I did reports, I usually wrote what happened at the scene."
JT decides to join the conversation then. "Whacko consultant pushes vic off roof?" He suggests, and not for the first time Malcolm feels anger towards him.
JT hadn't even apprehended the suspect, and he was the one criticizing Malcolm's judgement? Malcolm knew what he was doing. He did his job well, damn well. Even if he had to put himself in danger for it.
Carl Mitchell wouldn't be alive if it wasn't for Dani receiving that call, if Malcolm hadn't brought him out of his trip by tipping him off that ledge.
Gil approaches the rest of his team and tells them that Carl is stable, and the worst he had was a fractured rib.
The moment has already passed, but when Gil asks him if he's okay, Malcolm snaps.
"Whack job consultant's detailed understanding of the human psyche led him to anticipate, until diazepam could be administered, physical pain might be the only thing to bring the victim out of his psychedelic experience."
The team look at him in stunned silence for a moment, before Edrisa comes up to them, saying that Bright was right. Once again.
"50 times the standard dose.." Malcolm mutters to himself as the mortician goes on. "More than enough to induce fear and panic, leading to cardiac arrest."
"That could be his M.O." Gil suggests. Bright's eyes light up.
"To induce the fear that kills them." Finally, an answer.
"We're going to look for someone who was part of the experiments with Dr. Brown." They needed a list, and the only way they could get it was from Elaine herself.
"The taking of the brain is..it's like a metaphor. For the destruction of his own mind." It was easier to think about the case then his own situation. To fill the space with his own deductions instead of hearing his father's disappointed words on repeat.
"He wants to rid the world of those who wronged him. We need to keep tabs on Elaine Brown."
#my fic#my writing#the same#malcolm bright#malcolm whitly#martin whitly#malcolm/martin#dead dove do not eat#prxdigal sxn#dani powell#jt tarmel
3 notes
·
View notes
Text
COVID19 Updates: 08/06/2021
India: India's daily Covid-19 cases at one-week high of 44,643; deaths 464 LINK
World: Even with high vaccination rates it's not possible. Isle of Man has 71% of their population vaxxed and is experiencing a massive outbreak Gibraltar has vaxxed virtually every adult, plus all their cross-border workers, and has had massive outbreaks Vaccines alone aren't enough
World: Moderna says lab studies show a booster w half the dose of its #covid19 vaccine increases antibody levels against delta by 42-fold (of course they do)
World: Direct Evidence of Active SARS-CoV-2 Replication in the Intestine LINK
UK: JUST IN - New figures from Public Health England say nearly 35% hospitalized with #COVID19 had received two doses of a vaccine.
Virginia: Gov. Ralph Northam has announced that Virginia will require its state workers to show proof that they are fully vaccinated or be tested for COVID-19 every week. The policy will impact approximately 122,000 employees and will go into effect on September 1.
Texas: "In a sign that the delta variant is affecting more children on a daily basis, a baby in Texas has contracted COVID-19, and she had to be airlifted to a hospital 150 miles away because there were no ICU beds for her at the pediatric hospital in Houston." LINK
US: U.S. nurses' COVID-19 grief pours out online: 'I just don't want to watch anyone else die' LINK
California: San Diego County Reopens SDSU COVID-19 Testing Site, Plus 5 Others to Meet Demand LINK
UAE: UAE now vaccinating children age 3-17 with covid19 vaccine by Sinopharm at walkin clinics LINK
Japan: Japan reports 15,645 new coronavirus cases, the biggest one-day increase on record
RUMINT (Indiana): I got a call last night asking to transfer a patient from a small town in Arkansas to our hospital…in Indianapolis. 600+ miles away. Because every other hospital they tried to call any closer was on diversion status. Be patient with us America. We are tired. We are crowded.
World: Swedish Expert Claims People Could Require as Many as Five Covid Vaccine Shots LINK
World: New research has found a link between #COVID19 and lasting neurological cognitive deficits, including the acceleration of #Alzheimer’s disease. LINK
RUMINT (US): Nurse: It seems to me, Delta covid kills quick. Last year patients were in ICUs for weeks and even months. Now its days. Maybe hours. 4 crash carts are used in half of a 12 hr shift & another half still to go #GetVaccinated #WearAMask
Tennessee: 'All of them': Tennessee health chief says children's hospitals will fill up as the delta variant surges LINK
Texas: Texas won’t require schools to notify parents of COVID-19 cases LINK
Arkansas: “Dr. Rick Barr, at Arkansas Children’s Hospital, stated parents of hospitalized children are “shocked” because the “messaging out there has been that kids don’t really get sick with Covid, and we didn’t see serious illnesses, except for rare instances, with the previous variant.”
Senegal: Senegalese doctors, cemetery workers battle COVID-19 surge LINK
UK: COVID-19: Boris Johnson not expecting to isolate after member of his staff tests positive LINK
Kansas: Rep. Sharice Davids tests positive for COVID-19. She’s vaccinated. LINK
US: NEW: Number of Americans hospitalized with COVID-19 tops 62,000, highest since February
UK: NEW: The Government has drawn up plans for local and national lockdowns over winter, should the NHS be put under intense pressures
Texas: Texas GOP Official Mocked COVID Five Days Before He Died of Virus LINK
Poland: Poland> series of violent no-vaxx attacks on vaccination centers, including one arson in Zamosc. Investigators are treating these are terror acts from a group, trying to create instability - and by lower vaccination rates get to lockdowns and social unrest. There is apparently an international coordination of similar groups, being funded by domestic or foreign actors interested in creating worse covid waves, instability and social unrest.
Florida: Florida's weekly report shows 175 new coronavirus deaths. CNN and other media outlets are using this figure, but it's not correct. When you compare this week's death toll to last week, it reveals a much higher figure: 616
Australia: NSW recorded 319 new locally acquired cases of COVID-19 in the 24 hours to 8pm last night. Of these locally acquired cases, 125 are linked to a known case or cluster – 108 are household contacts and 17 are close contacts –
Texas: @texashealth announced its North ER Location in Rockwall will temporarily close. This will shift staff members to the main campus off Horizon Rd to provide #COVID19 care.
Australia: Melbourne’s numbers today make me want to cry. I think it is because to go from a donut day to 29 cases in 48 hours is just such a “f*ck you” from the virus and a reminder this is never going to end quickly or easily. Please, please, please get vaccinated. It is all we have.
Chile: Chile to give #COVID19 vaccine boosters for those inoculated with Sinovac LINK
Mexico: Mexico’s national Health Ministry raised Mexico City to its highest Covid-19 alert level, or “red stoplight,” due to rising infections, though city officials said it was remaining at the lower “orange level” LINK
US: U.S. COVID update: Biggest one-day increase in cases since January, deaths rising - New cases: 131,628 - Average: 105,677 (+4,193) - In hospital: 63,133 (+2,018) - In ICU: 15,404 (+397) - New deaths: 763
Florida: A child has died from the #DeltaVariant in Orange County Florida. This is the 9th pediatric death from COVID that I've posted in 3 days. Another child is on life support due to COVID. #SoulsLostToCovid
0 notes
Text
BACK FROM HIATUS
Even though I never declared one. my schedule was kept pretty full, so updating this blog wasn’t a priority. c’est la vie. but here I am.
2018 has had a weird start. but it’s an alright year so far, I guess.
Still living in Viet Nam. I drive a motorcycle now, a Hanamoto Nam, originally built in Laos. it’s helped me grow a new appreciation for mechanical systems, plus purchase price and self-maintenance is cheaper than renting a scooter. Recently, I’ve been pondering ways to bring advanced data science to corporations in this country as an industrial data analyst. it’s definitely possible, but, as a foreigner, there would be some significant hurdles to jump through. I also make money on the side by distilling natural insecticides (how I paid for my motorcycle!), and I’m really getting into vaporwave music.
My Vietnamese hasn’t really improved. I know some new words now and I can speak simple sentences, but it’s difficult to actually converse with Vietnamese individuals. even when I try my best to replicate proper tones and speech, they rarely recognize that I’m even trying to speak Vietnamese, and inevitably someone who speaks English comes over to help. literally every foreigner here that I have met who speaks fluent Vietnamese originally learned either by dating a Vietnamese person, or by taking classes. and since I don’t really have time to date or take classes... high regional diversity makes learning even more difficult. several times, I’ve learned words or phrases from one Vietnamese person and later been told by another Vietnamese person that “nobody would say it like that” or “people from [district\province\area] say that.” there’s some small phonetic\phonological differences between regiolects that can significantly impede acquisition.
Starting back in September, I wrote a new doctorate research project, and starting sending it to linguistics faculties in mid-November. the first version I sent out was not as good as it should have been, but subsequent revisions are much better. unfortunately, out of approximately 60 faculties (~40 linguistics faculties) that I contacted, none have shown interest. I haven’t sent an application in months, and I still receive a new rejection every 2-3 weeks. 5 soft categories of responses were noted: 1) This faculty does not focus on this research area, which is fine; 2) this is great and all but there’s nobody at this faculty who can supervise your project (which includes this faculty does not have the resources for a doctorate project like this), also fine, sure whatever; 3) This doesn't seem feasible\tractable\realistic\possible\logical\valid, which usually also included a hefty dose of you need to prove that this will work before we will even consider it, seems highly unfair, especially since the methods I’m advocating are already in use for 15 years and the citations for that are already in the proposal, plus how do I get the fucking data without an institution to back me up!? l; 4) This faculty is not interested in your project, fair enough, thats alright; 5) I can’t even understand what you’re proposing, like, come on, I know it’s complex and dense, but there’s a lot to say, and I did it with only 4 pages - did you try skimming any of the references or try using google or wikipedia? The worst response so far came from Dr. Mattis List, who literally just flat out responded with “this isn’t going to work”, and fallaciously attacked a very simplified example that I gave to him in order to help him understand the core concept of my proposal. Neither Dr. Heggarty nor Dr. Gray were particularly interested. Dr. Gerhard Jaeger had a fairly friendly response, but still questioned how feasible it actually is. My response to questions about tractability (which is a genuine concern, since a model must be economical in order to be feasible) has been: do you really think we can generate better resolutions for language typology, history, and ecology by retaining simple models and basic levels of information? Modelling a complex system requires a level of data that reflects the complexity of the source system. Groundbreaking results don’t just appear - innovations are required. after receiving rafts of negative, even some outright hostile, responses (mostly mocking my reductionist perspective on language), my opinion is that mainstream linguistics is ignoring this fact, and ignoring the additional fact that there are already methods for modelling complex systems, like human speech. and that these methods are already verified and in-use. so I’ve given up on rejoining the field of linguistics. y’alls be some orthodox mothafuckas, ya know that? Y’all like to pretend that you’ve moved past the formalist conceptions and theories of language but you really haven’t. There’s still a large and apparently high-level portion of the linguistics community that actively spurns the philosophy of computationalism and experimentation, who think that it’s a fad, and who also don’t even see the problems inherent to currently used methods (or don’t see them as problematic). I, on the other hand, think interdisciplinary linguistics is a better linguistics. or moreso, better to adopt methods from other disciplines than to have those disciplines steal chunks of research potential from linguistics. or better to be that person who steals chunks of research potential from linguistics for another field.
However, I might try new applications for 2018, but I’m really tired of dealing with academia. I turn 30 this year. I don’t have time to waste personalizing applications or writing 10 different variations on a research proposal to please every possible faculty that could be interested. at least if I present my ideas as a commercial venture to someone with dollar signs in their eyes, they’re going to see the potential dollar signs; that’s a hell of a lot better than an exhausted researcher who has exactly 2 days to review 80 reasonable doctorate candidates and their projects and choose which to actually consider. a close friend told me to not even bother with applying to linguistics faculties for next time, and I think he’s right. I might focus more on applying to mathematics and computer science faculties.
Here in Viet Nam, during the summer, air conditioning and mosquito spray\incense are your friends. Will exposing yourself to DEET and other synthetic insecticides possibly harm your body in currently-immeasurable\unknown ways? possibly, even probably; you know what will harm your body in currently-measurable\known ways? Getting dengue fever because you’re being bitten by at least 30 mosquitoes every night.
buying vegetables and fruits at the Cho (local open market) is so much cheaper and fun than the grocery store, but beware: unless the shopkeepers see that you’re a regular, a lot of them will try to rip you off. it can be annoying. but keep in mind: unless you can converse in Vietnamese with them, they’re almost always taking some extra time to help you obtain your products, so don’t be salty if you pay the foreigner-price; for a very large purchase at a cho, it’ll be maybe 35,000 VND extra.
guys, I can’t believe that there are only 2 episodes of Adventure Time left!
not much else to report on or to say at this time. if anyone in the tumblr science community is in a position to read and advance my proposal to a particular faculty, I’ll gladly email it to you, but I’m not making it publically available yet, and I would rather it not be shared or given to anyone without my consent first. I’ve already received some warnings - naming even specific faculties - about having my proposal unscrupulously stolen, and I have enough unfriendly acquaintances throughout linguistic academia that, yes, it is something I have to be worried about.
#life#research proposals#summer is alright though I really like the sun on our balcony#driving a motorcycle is more fun than I thought#I had to learn manual from the guy I bought it from#people literally pointed and laughed whenever I stalled. but just look at me now!
1 note
·
View note
Photo

Takhuk
August, 2020
Michele Moore Veldhoen
COWPOX, COVID, COMMERCE, AND COVAX An Unusual Glimpse Into the Vaccine World
When Covid-19 is eventually neutralized, will its’ backstory be engraved on the tablet of humankind’s greatest achievements, or will it be etched onto a cave wall, a hidden story of humankind’s failure to co-operate…….
An hour of online immersion into the history of how some of the most important vaccines were developed and distributed reveals at least these key factors: critical observations and personal sacrifice on the part of the scientists working on solutions to disease; public funding; international co-operation; general benevolence ; and, competitive, egotistical, scientists.
Vaccines as they are known to contemporary Canadians have been in use since the late 19th century, although the parent of all modern vaccines, the Smallpox vaccine, was actually invented in the late 18th century by the British doctor Edward Jenner. Jenner noticed that farmers who became infected with cowpox (a virus found in a cow’s udder) subsequently became immune to smallpox. This observation led to his invention of the smallpox vaccine. It can be said then, that we all owe a debt not only to Dr. Jenner, but also to cows. (Thus, the cow photo.)
Jenner’s private medical practice suffered as he dedicated himself to educating the world about vaccination. Without seeking or expecting financial reward, he shared his knowledge with medical practitioners around the world and sent his smallpox vaccine to other European countries and the United States. He also vaccinated the poor, in his own home, for free. Eventually, the British government recognized his sacrifices and the incredible contributions he had made to the health of the human population and provided him with some money.
About a century later, in the second half of the 19th century, the terribly competitive French chemist Louis Pasteur (think pasteurization), solved the mystery of both anthrax and rabies and made many other crucial contributions to medical science, especially in the area of germ theory. His work led to the creation of the internationally funded non-profit Pasteur Institute, where he continued to unravel the mysteries of germs and disease until he died.
Late 20th century revelations of Pasteur’s character suggest that, along with his zeal for studying and comprehending the way of germs, he was also interested in fame and glory, (he made his family swear never to reveal his notebooks, because, it is now known, in order to best his rivals, he wasn’t always honest about his processes). His deceptions and corresponding arrogance were the trade-offs for his invaluable work, as he has been memorialized around the world with statues and place names on streets, institutes, hospitals, and schools like Calgary’s Lycée Louis Pasteur School. The Pasteur Institute, which continues to be an internationally funded non-profit institute to this day, is likely populated with a few modern versions of Pasteur. Like many great achievers in any field, there is often a dark side to their story.
In Canada, at least one vaccine was developed and mass produced thanks to major contributions from scientists at Connaught Laboratories in Toronto. That vaccine was for polio, which hit Canada very hard throughout the first half of the 20th century. Connaught scientists worked feverishly on a solution and came up with a key aspect of the process that helped the American Dr. Salk produce the vaccine that ultimately saved lives around the world. But it was Connaught, and specifically, the chemist Dr. Leone N. Farrell, who invented a successful method to mass produce the vaccine. Her invention became known as The Toronto Method. The Toronto Method became the method for producing the vaccine which eventually eradicated polio.
What’s most interesting about Dr. Farrell’s story, is that, when asked if she would like to take out the patent for her method, she declined. Apparently, she made a direct request to Connaught that they not patent her method.
Little is known about Dr. Farrell, but it seems more than plausible she made this request because, like many of her predecessors and contemporaries in the world of disease prevention, she wanted her life saving technology to be available to as many people around the world, as possible.
This small collection of stories give an idea as to the range of humanity making profoundly valuable contributions to medical science. Whatever the motivation, we have benefited from their brilliance and often their benevolence.
Naturally, glory and dollars gleamed in the eyes of some of the players during those centuries of medical science enlightenment, however, vaccine production was very difficult and costly and therefore never a money making proposition. Therefore a mix of compassion and practical self-interest – contagious diseases do not necessarily exist only in the domain of the poor – drove the world-wide distribution of vaccines.
Until recently then, pharmaceutical companies gave little consideration to vaccine production. Vaccine manufacturing is heavily regulated and the customer base is small – primarily governments.
But the profit outlook began to change in the late 90’s when H1N1 appeared, threatening a pandemic. In response to this first hint of a possible flu pandemic, governments around the world conceived pandemic response plans and started stockpiling vaccines.
Vaccine stockpiling completely changed the profitability landscape, making big pharma a big player in the world of vaccines. This Globe and Mail article tells the story. https://www.theglobeandmail.com/life/health-and-fitness/health/conditions/how-vaccines-became-big-business/article572731/ .
With big pharma comes big dollars and with big dollars comes big moral dilemmas. Just as Dr. Jenner gave free vaccines to the English farmers and other disenfranchised of his era, today, those people without power and money or good government rely on the generosity of wealthier countries to provide vaccines and other medical resources. And of course, due to world trade and travel, wealthier countries also have a vested interest in the health of populations around the world.
This brings us to this year’s top news story.
Today with Covid-19, a lot of news commentators and analysts are reporting on the ‘race’ for a vaccine. Fears are being expressed about the possibility of greed (and the desire for glory) running rampant over our collective immune systems as pharmaceutical companies and leaders of some of the most powerful countries try to position themselves to be ‘first’ in the race and maximize profit from and access to the ‘winning’ formula. Already, some of the world’s richest countries have signed deals with pharmaceutical companies to hoard supply as it comes on stream. Russia has ‘certified’ an essentially untested vaccine, therefore allowing its’ leader to claim first place in that particular heat of the race.
Fortunately, there is hope for less financially powerful populations. A major international effort is underway, which Canada is supporting, to establish an equitable, and sensible, way to distribute the vaccine across the globe. COVAX, the COVID-19 Vaccines Global Access (COVAX) Facility, is the brainchild of several international organizations including the Bill and Melinda Gates Foundation and the World Health Organization. This initiative seeks to bring together developed and developing countries to invest in about 12 different vaccines and ensure early access when they become available. “The goal is to have 2 billion doses by the end of 2021,” says Seth Berkley, director of GAVI, the Vaccine Alliance, the third COVAX partner: 950 million for high- and upper middle-income countries, 950 million for low- and lower middle-income countries, and 100 million for “humanitarian situations and outbreaks that are out of control.” A first $750 million deal with AstraZeneca for 300 million doses was announced on 4 June.” (https://www.sciencemag.org/news/2020/07/vaccine-nationalism-threatens-global-plan-distribute-covid-19-shots-fairly)
So far, according to CBC, 75 developed countries have signed up, including Canada, and are partnering with 90 developing nations. Together these countries represent 60% of the world’s population. (https://www.cbc.ca/news/health/covid-19-vaccine-countries-world-1.5668835) The goal is to be able to provide each participating country with enough doses to vaccinate at least 20% of their populations, with medical related personnel being the first to receive the vaccine.
While some leaders see the acquisition of a vaccine as a winner take all proposition, the irony of such an approach is that, if there is not an equitable and sensible distribution of the vaccine across the world, any given wealthy country that hoards the lion’s share of the vaccine, (and of course, pharmaceutical companies would have to co-operate with such countries, which is where the question of health care provision driven strictly by profit and devoid of any ethical considerations begins to take on a sickly shade of green), the citizens of that country will be prisoners of their own perceived victory. With our supply chains for everything from energy to food to medical supplies to Nike shoes and cell phones being dependent on a healthy population in those countries that have been, thanks to those rich countries, unable to access a vaccine supply, the economy of those rich countries will continue to suffer until the world is collectively on the road to recovery. And, in a winner take all scenario, certainly, tourism will be dead and dried up in the petrie dish. Which means all the freshly vaccinated residents of wealthy countries would have to stay home anyway.
These notes are brought to you by someone soaking up the world’s free supply of Vitamin D while watermelon juice drips from her chin. May the rest of summer be so kind.
www.michelemooreveldhoen.com
0 notes
Text
Vitamin D and the Flu
One of the greatest triggers of influenza, the swine flu and deaths from pulmonary deficiency is vitamin D deficiency. One of the biggest reviews of the role of vitamin D in health found that people who took supplements of the vitamin for six years reduced their risk of dying from all causes. Studies have already suggested that vitamin D played a key role in protecting against cancer, heart disease and diabetes – conditions that account for 60 to 70 per cent of all deaths in the West.
Researchers from Winthrop University Hospital in Mineola, New York, found that giving supplements of vitamin D to a group of volunteers reduced episodes of infection with colds and flu by 70 per cent over three years. The researchers said that the vitamin stimulated “innate immunity” to viruses and bacteria. The decline in vitamin D levels between November and March is in reality the real “seasonal stimulus” that accounts for the peak in colds and flu in the winter. “Since there is an epidemic of vitamin D insufficiency in the US, the public health implications of this observation could be great,” the researchers wrote.[1]
The increasing use of sunscreens and the decreasing amount of time spent outdoors, especially by children, has contributed to what many scientists believe is an increasing problem of vitamin D deficiency. In the winter, the sun in Britain is barely strong enough to make the vitamin, and by spring, say scientists, 60 per cent of the population is deficient (defined as a blood level below 30ng per milliliter).
Exact dosages are difficult to determine because requirements vary by age, body weight, percent of body fat, latitude, skin coloration, season of the year, use of sun block, individual variation in sun exposure, and how sick someone is. If possible and you live in a warm climate, at least 15 minutes/day in noontime sun with exposure to as much skin as possible is the best way to get Vit. D. If you receive very little UVB exposure the Vit. D Council recommends the following dosing levels of D3:
Health children under the age of 2 – 1,000 IU per day* Healthy children over the age of 2 – 2,000 IU per day* Adults and adolescents – 5,000 IU per day.
10ug is equal to only 400 IU of Vit D3 so you need to take your dose up quite a bit or buy a supplement with greater Vit D content per capsule.
Dr. David Brownstein recommends: Ensure you are taking adequate amounts of vitamin D. I frequently have my patients take short-term, larger doses of vitamin D (10,000-50,000Units/day) for 2-5 days at the first sign of the flu.[2] The current dietary guideline for humans is to consume 50-200 IU of vitamin D a day. However the American Journal of Clinical Nutrition’s Dr Michael Hollick recommends levels as high as 50,000 IU.
It was back in 1981 that R. Edgar Hope Simpson proposed that a principal cause of seasonal influenza is linked with the deficiency of solar radiation which triggers the production of vitamin D in the skin. Vitamin D deficiency is common in the winter, and vitamin D is crucial in allowing your immune system to defend itself against invading organisms. In addition to vitamin D, studies have suggested that people who exercise moderately suffer fewer and less severe colds and flu infections.[3]
Exercise and the Flu
In a new study, researchers found that when they had a group of mice regularly run on a treadmill over 3.5 months, the animals developed less-severe symptoms when infected with the flu virus. Additionally, mice that exercised right before flu infection, but not regularly over the preceding months, also showed some protection against severe symptoms — which in mice means dampened appetite and weight loss. Those benefits, however, were only apparent in the couple days after infection, whereas regular long-term exercise reduced flu symptoms over the whole course of infection.
Dr. Mark Sircus AC., OMD, DM (P)
References (3)
https://www.independent.co.uk/life-style/health-and-families/health-news/the-virtues-of-vitamin-d-its-time-we-saw-the-light-402749.html
https://www.drbrownstein.com/category/dr-bs-parent-category/holistic-medicine-dr-bs-parent-category/natural-supplements/
https://www.independent.ie/lifestyle/health/vitamin-d-might-lessen-your-flu-risk-26576781.html
Related Posts
New Study Suggests Vitamin D is Better than Vaccines at Preventing Flu
Natural Allopathic Emergency Medicine for Flu
What’s the Best Time to Take Vitamins?
People are Dying from the Flu
from WordPress https://ift.tt/2UaR5he via IFTTT
0 notes
Text
I was doing you a favor by playing the long game...
I too was playing yet another long game by holding on to this for so long.
SO I had read earlier today the owner of a previous job of mine passed away. This was a place that tried to screw me pretty hard and I took some pro revenge on. It drug up some angry old feelings, so why not take an equal dose of catharsis?
WARNING: This is a doozy so strap in if you dare, no TL;DR it wouldn't do justice.
So this takes place almost a decade ago. I was working as a department manager for a fairly large privately owned pest control company. Their color scheme was black and yellow, much like the taxi's the owner's dad used to drive. Since the taxi industry would be around for ever(hello Uber/Lyft) so would this pest control company, (this is important later) or so the owner used to parrot constantly. My job was to over see the techs doing treatments and set their stops and generally manage assorted insect control services, inventory, payroll for that dept, etc etc. I had taken the job from the owners son who took it from the previous manager who they demoted and yet stayed in the dept...this is important later. The owners son was a late 30's early 40's man child. I mean if he had dialed it back a few degrees he would have been an awesome guy, but anytime booze was involved he was a mess. If it was weed, he turned into the stereo typical obnoxious stoner making nothing but bad Jamaican accented jokes. He also hit on anything younger than him that moved...while being married w a pregnant wife. But I digress, the owner was a piece of work too, old Jewish guy who was as racist as he was old, not with any kind of seething hatred. Just a "this is the way it is" type attitude. My fave line of his, "The sky is blue, Ch#@ks know math, N@&ers are lazy, Jews know gold. What else is new" Like it was the most clever thing of all time. Finally now on to the revenge and need for such.
I had been at said job for about two and a half years, while there I had gotten engaged about 6 month earlier. Due to the awesomeness of my staff I invited about 10 employees to my wedding(it was going to be big due to the wife's family and mine's tiny so..) including the owner his son and the previous manager. I should have felt the ripples in the water when I had planned the trip to propose. The day before I go the owner comes in to do something with a big job and I tell him of my vacation plans as he is looking at the schedule. After I tell him of the somewhat expensive accommodations (I was proposing to my then gf), he literally says, "that's a great idea I haven't been there in years, I think I'll go tomorrow too!" I think he is joking, but he immediately tells his son who was taking over my work that he needs to take over for him and be a presence at the job site. Then tries to demand I clear a day out of my booked vacation schedule for us to meet up with him so he can take us out to some expensive place or some crap. On that one day during the trip he ended up no call no show-ing after we invited him to meet and hang with our family. We spent about an hour trying to call/message/email the guy and he never responded the entire trip. I get back he starts cracking lame jokes about how I ditched him to get engaged...that really pissed me off.
It gets better. Over the course of the next few months strange shit starts happening. I am forced to let go of a few of my techs for BS reasons like the 3 strike rule of attendance randomly being enforced without writ-ups or even verbal warnings. One guy had a 3 month old kid with his GF and I had to let the guy go because of a 3rd lateness of over 5 min from almost 90 days earlier and the previous two being almost 2 years old with the notes of in-climate weather and no routes that day (they also denied him unemployment and tried to enforce a 90 day no compete clause that would have stopped him form getting a job w the competition). Then I get a high priority job of going through back logs of unpaid services and start trying to preform collections with me receiving a % of what I collect(that I was never paid). Over the next month or two I keep getting odd things thrown at me to make money which don't have much to do with my regular job. Till one week where the entire office gets the flu. The owners son, previous manager(now just an officer worker), my assistant and about half the techs call out over the course of the week. I still come in with a 102 fever and goddamn doctors note in case I need to bail, just to get everyone set up and do as much as I can before almost passing out 3 days in a row. I get the entire day's work done by 1pm and leave all with the boss's son's approval. He was thrilled things were still working while the plague rampaged on. But not the owner apparently. I got pulled into the office and yelled at about not taking initiative and calling out all these days...he sounds like he is about to fire me before he asks me if I have anything to say for my self. So I correct him and he looks really shaken and then tells me some BS about the EPA stepping in and making us reduce the number of services we are allowed to do from quarterly (4x a yr) to a trimester schedule (3x) all while paying the same price. Guess who got to call almost every paying customer and try to get them to swallow that? ::raises hand::. So I take care of that over another two weeks and once again get called in to the office. Saying we cannot have this anymore and the EPA is crashing down hard on us and I just keep giving out too many services because the EPA really said we are not allowed to treat more than 2x a year and they lied to me throwing me under the bus(turns out that was a lie too they were trying to get up to stop treatments all together). Knowing I never had the power to authorize a single extra service without consent from the owners. So they had to let me go...only 4 month before I was going to get married. It got a bit intense as emotions ran high, the asshole of a son tells, "My dad told me to fire you a while ago for attendance but I knew you were getting married and I didn't want to mess that up so I played the long game for you man...." In an office with no strict punch schedule for the office workers as we were salary and constantly did things like get food for the office or have to run errands for the business and get stock from another location. Along w/ the EPA bullshit he tells me he just couldn't have a dept with two other managers in it who made less than I do doing the same job. They also tried to block my unemployment with falsified paperwork, claiming unsatisfactory attendance. Tons of bullshit and I never got a strait answer as to why I was let go till I did some investigating. Turns out the old manager who was just an office hand was being put back in the spot she was fired form because she offered to take a 33% pay cut form her old salary and the son just didn't want the extra work.....So they tried to scapegoat me for EPA violations and tried to tell the rest of the office my fuckups were the reason people were let go and the department was going to close.
So now that you've read all that you may have a bit of a feel for why I took my revenge so far and for so long. Luckily I had snapped a few pics of the paperwork I signed upon leaving stating it was due to the EPA infractions. That gets printed out and sent to the department of labor with the rest of their awesome tactics(shorting over time and flat out not paying for paid vacations, time card edits). That lead to tens of thousands of dollars lost in pack pay and fines being levied. The guy w/ the 3 month kid I had to let go told me he eventually settled for almost 35k in back pay... My next stop was the EPA, who much to their surprise didn't even know the company had kept doing the treatments at all as it was supposed to be stopped altogether. Luckily they knew the deal and that it wasn't just me making treatments all willy nilly like. More fines, for each and every treatment performed by them from about 3 months before they fired me. That had to be in the 6 figure range as there was well over 1.5k treatments done in the time and the fine was supposed to be over 1k each. The problem with the treatments were they were too effective, and were wiping out the type of insect that has beneficial and necessary environmental roles. So the mfers were actually hurting the ecology of our goddamn state for their own profit. I created a few fake FB profiles to still be able to follow the owner and his son on FB and find out not 30 days after their EPA issues my department closed down.
Okay so that was 2006ish, two years pass and I keep seeing my POS old boss, speeding around the area (I lived near the place) in his old ass little red Mercedes. Guess who called the cops worrying about the safety of those on the road around this dangerous car? Guess who eventually got caught for DUI at 2pm in the afternoon?
Fast forward a few years to 2011. Mr Whiz Kahlifa drops the song Black and yellow. Decent track. But remember how my old boss was a super racist fellow? Remember the business' color scheme? So I spent about a month sending him different youtube links to that song, from random email accounts. And finally one of a commercial for the company with Whiz's song over it vs the lame jingle they used. Not two weeks after I stop they change the goddamn color scheme of the place to a horrible red white and blue one. But not exactly red white and blue like the American flag more like the Blue white red of the French one. I wait about a month after the Black and Yellow attack and send him a vid of the French national anthem while a the flag is waving in the background. The next goddamn day the place is covered in that cheesy car dealer red white and blue American bunting and American flags everywhere.
Fast forward again to about 2014 and fuck me if I am not out for a walk, and see that company's sign in a lawn advertising that same old treatment on the same old signs from 06'...guess who got sent yet another email to the EPA w pictures? That one got them in major and local news as being "no friend to the environment".
Last time I went by their place they seemingly had half fleet of what are now used blue white and red covered mini trucks. Plus their call center building was emptied of furniture. Unfortunately they are still in business but are sitting at about a 3 star rating on Yelp and that was after they did the damage control to get it back from 1.5 stars.
Sorry(not sorry) guys, I was just playing the long game for you....
(source) (story by StendhalSyndrome)
1K notes
·
View notes
Text
The truth about asymptomatic COVID-19
Masks are still a crucial part of fighting COVID-19 (Anna Shvets/Pexels/)
Follow all of PopSci’s COVID-19 coverage here, including news on federal policies, the latest on immune-response research, and a state-by-state breakdown of confirmed cases.
The World Health Organization (WHO) seemed to claim earlier this week that asymptomatic carriers of COVID-19 weren’t major spreaders of the virus, before walking back their statements a day later. Many people were understandably confused and frustrated about the apparent flip-flopping, but the truth is, as ever, a bit more complicated.
“They were trying to quibble about a point,” says Monica Gandhi, an infectious disease researcher at the Division of HIV, Infectious Diseases, and Global Medicine at UCSF/ San Francisco General Hospital. “They were trying to make the point that we have no idea how much transmission occurs from asymptomatic versus presymptomatic people.”
Making that fairly semantic point at a major press conference—just days after the WHO changed its stance on mask wearing—caused all of this to be taken out of context and misunderstood, Gandhi notes. It’s understandable that it sparked such a controversy.
But the facts remain the same, says Gandhi: “It’s undisputed that spread occurs from those who don’t have symptoms.”
It’s true that, as the WHO stated, we don’t yet know to what degree asymptomatic or pre-symptomatic people are spreading COVID-19. Some early models suggested up to 55 percent of the disease’s spread could be due to these hidden carriers, which make up an unusually high number of the virus’s total cases. Gandhi notes that we still have a lot to learn about this kind of transmission: What we do know is that asymptomatic or pre-symptomatic people are definitely part of the equation. The virus has spread so fast in spite of social distancing and shutdown measures that it can’t only be symptomatic people who are propagating the virus.
What Dr. Van Kerkhove is really saying, I think, is that when WHO follows up with people who did contact tracing, they found that they could *not detect* a lot of asymptomatic spread of SARS-CoV-2. How do we square that with articles like this? https://t.co/40yQ6LRAJP Answer:
— Jeremy Faust MD MS (@jeremyfaust) June 8, 2020
That means you shouldn’t take the WHO’s statement as a sign that you should stop wearing a mask or stop social distancing. “What we did with social distancing and lockdown was necessary,” Gandhi says. “We can never say that wasn’t necessary.”
And in fact, Gandhi says, evidence suggests both of those measures are having a real impact on how COVID-19 spreads—though perhaps not in the way you might think.
The rate of asymptomatic infections seems to be getting higher and higher, and that may be because people are being exposed to lower viral loads due to social distancing and mask-wearing. Early rates of asymptomatic infection were low, based on populations where testing was widespread enough to catch all cases—6 percent in Singapore, and 18 percent on the Diamond Princess cruise ship, which was refused entry to Tokyo earlier this year and thus sat in the bay for 27 days until the passengers were allowed to leave. But later estimates put it much higher. A large testing mission in San Francisco found that around 50 percent of people with COVID-19 had no symptoms. Another cruise ship, this one sailing near South America, gave everyone on board masks and tested all passengers, and found that 81 percent of those with COVID-19 were asymptomatic.
There’s also a striking correlation between those countries that implemented mask-wearing early—mostly those previously hit by SARS, but also Czechia—and low death rates from coronavirus. “If you look at these countries there’s a near perfect correlation, no matter what else you do,” say Gandhi.
This from @WHO is getting a lot of attention and creating confusion. I want to quickly share what I understand about this. Bottom line question: Are infected people without symptoms an important cause of spread? My best guess: yes. A thread https://t.co/NnLpf7kTVh
— Ashish K. Jha (@ashishkjha) June 8, 2020
This phenomenon, where the dose of the virus a person is exposed to determines how sick they get, isn’t new. Influenza seems to work this way, as do GI diseases like norovirus and STDs like hepatitis C. The idea is that the more viral particles a person is exposed to, the sicker they’re likely to get. A huge influx of a virus into your body may be very hard for your immune system to fight off, while your cells could easily handle a smaller group of invaders. If this is true of SARS-CoV-2, this could actually be good news.
“That’s having your cake and eating it too, if you can not get sick and be immune,” says Gandhi. It’s not yet clear how much protection a recovered COVID-19 patient has thanks to their immune system’s antibodies, but they probably maintain some defenses against the disease for at least a few weeks or months, if not longer. If most COVID-19 cases carry no symptoms at all, people could develop protection—making them less likely to get a serious case or spread the virus to others in the future—without suffering ill effects. In the absence of a vaccine, which could take a year or more to actually develop, that could be crucial.
What we really care about, Gandhi notes, is the people who get seriously ill. If we can prevent people from getting really sick from COVID-19, even if those people still get the virus, that’s a good thing. And all the data we have suggests that wearing a mask and social distancing are still key to fighting this virus.
There’s still a lot we have to learn about SARS-CoV-2. We don’t know how much live virus asymptomatic people might spread, for instance. It’s also not clear how many people might be functionally asymptomatic—suffering nothing worse than a scratchy throat or headache they can easily ignore—while still spreading the virus as much as those with more obvious symptoms. But we’ve also learned a lot of helpful information in the past few months: Wearing masks may not protect you from getting the virus entirely, but it could keep you from getting seriously ill. That means you shouldn’t just wear a mask to protect others—you should do it for your own sake. Especially as states begin to reopen, it will be crucial to take whatever precautions we can.
View this post on Instagram
Confused by recent WHO statements? Here's the truth about asymptomatic #COVID19 transmission. #linkinbio for more coverage 👉 @popsci 📊: @sarachodoshviz
A post shared by Popular Science (@popsci) on Jun 9, 2020 at 12:59pm PDT
0 notes
Text
The truth about asymptomatic COVID-19
Masks are still a crucial part of fighting COVID-19 (Anna Shvets/Pexels/)
Follow all of PopSci’s COVID-19 coverage here, including news on federal policies, the latest on immune-response research, and a state-by-state breakdown of confirmed cases.
The World Health Organization seemed to claim earlier this week that asymptomatic COVID-19 patients weren’t major spreaders of the virus, before walking back their statements a day later. Many people were understandably confused and frustrated about the apparent flip-flopping, but the truth is, as ever, a bit more complicated.
“They were trying to quibble about a point,” says Monica Gandhi, an infectious disease researcher at the Division of HIV, Infectious Diseases, and Global Medicine at UCSF/ San Francisco General Hospital. “They were trying to make the point that we have no idea how much transmission occurs from asymptomatic vs presymptomatic people.”
Making that fairly semantic point at a major press conference—just days after the WHO changed its stance on mask-wearing—caused all of this to be taken out of context and misunderstood, Gandhi notes. It’s understandable that it sparked such a controversy.
But the facts remain the same, says Gandhi: “It’s undisputed that spread occurs from those who don’t have symptoms.”
It’s true that, as the WHO stated, we don’t yet know to what degree asymptomatic or presymptomatic people are spreading COVID-19. Some early models suggested up to 55 percent of the disease’s spread could be due to these hidden carriers, which make up an unusually high number of the virus’s total cases, but we don’t really know for sure. Gandhi notes that we still have a lot to learn about this kind of transmission. What we do know is that asymptomatic or presymptomatic people are definitely part of the equation. The virus has spread so fast, and in spite of social distancing and lockdown measures, that it can’t only be symptomatic people who are propagating the virus.
What Dr. Van Kerkhove is really saying, I think, is that when WHO follows up with people who did contact tracing, they found that they could *not detect* a lot of asymptomatic spread of SARS-CoV-2. How do we square that with articles like this? https://t.co/40yQ6LRAJP Answer:
— Jeremy Faust MD MS (@jeremyfaust) June 8, 2020
That means you shouldn’t take the WHO’s statement as a sign that you should stop wearing a mask or stop social distancing. “What we did with social distancing and lockdown was necessary,” Gandhi says. “We can never say that wasn’t necessary.”
And in fact, Gandhi says, evidence suggests both of those measures are having a real impact on how COVID-19 spreads—though perhaps not in the way you might think.
The rate of asymptomatic infections seems to be getting higher and higher, and that may be because people are being exposed to lower viral loads due to social distancing and mask-wearing. Early rates of asymptomatic infection were low, based on populations where testing was widespread enough to catch all cases—6 percent in Singapore, and 18 percent on the Diamond Princess cruise ship, which was refused entry to Tokyo earlier this year and thus sat in the bay for 27 days until the passengers were allowed to leave. But later estimates put it much higher. A large testing mission in San Francisco found that around 50 percent of people with COVID-19 had no symptoms. Another cruise ship, this one sailing near South America, gave everyone on board masks and tested all passengers, and found that 81 percent of those with COVID-19 were asymptomatic.
There’s also a striking correlation between those countries that implemented mask-wearing early—mostly those previously hit by SARS, but also Czechia—and low death rates from coronavirus. “If you look at these countries there’s a near perfect correlation, no matter what else you do,” say Gandhi.
This from @WHO is getting a lot of attention and creating confusion. I want to quickly share what I understand about this. Bottom line question: Are infected people without symptoms an important cause of spread? My best guess: yes. A thread https://t.co/NnLpf7kTVh
— Ashish K. Jha (@ashishkjha) June 8, 2020
This phenomenon, where the dose of the virus a person is exposed to determines how sick they get, is not new. Influenza seems to work this way, as do GI diseases like norovirus and STDs like hepatitis C. The idea is that the more viral particles a person is exposed to, the sicker they’re likely to get. A huge influx of a virus into your body may be very hard for your immune system to fight off, while your cells could easily handle a smaller group of invaders. If this is true of SARS-CoV-2, this could actually be good news.
“That’s having your cake and eating it too, if you can not get sick and be immune,” says Gandhi. It’s not yet clear how much protection a recovered COVID-19 patient has thanks to their immune system’s antibodies, but it’s likely they maintain some defenses against the disease for at least a few weeks or months, if not more. If most COVID-19 cases carry no symptoms at all, people could develop protection—making them less likely to get a serious case or spread the virus to others in the future—without suffering ill effects. In the absence of a vaccine, which could take a year or more to actually develop, that could be crucial.
What we really care about, Gandhi notes, is the people who get seriously ill. If we can prevent people from getting really sick from COVID-19, even if those people still get the virus, that’s a good thing. And all the data we have suggests that wearing a mask and social distancing are still key to fighting this virus.
There’s still a lot we have to learn about SARS-CoV-2. We don’t know how much live virus asymptomatic people might spread, for instance. It’s also not clear how many people might be functionally asymptomatic—suffering nothing worse than a scratchy throat or headache they can easily ignore—while still spreading the virus as much as those with more obvious symptoms. But we’ve also learned a lot of helpful information in the past few months: Mask-wearing may not protect you from getting the virus entirely, but it could keep you from getting seriously ill. That means you shouldn’t just wear a mask to protect others—you should do it for your own sake. Especially as states begin to reopen, it will be crucial to take whatever precautions we can.
0 notes
Text
Arizona Parents Falsely Accused of Child Abuse Lose Infant Son – Have 2-Day-Old Newborn Also Medically Kidnapped

Jordan Meissinger holds his newborn son. His joy was short-lived. When Baby Paxton was only 48 hours old, Arizona social workers took him away from his family. Photo provided by family.
by Health Impact News/MedicalKidnap.com Staff
Paxton Meissinger came into the world on Tuesday, October 16, 2018, weighing all of 7 pounds and 2 ounces. Like every newborn baby, he wanted and expected only one thing – the presence of his mommy.
To an infant, the most important thing in the world is be surrounded by the love and warmth of the person whose heartbeat he has heard for as long as he had the ability to hear.
In her arms, every need he has is met, from her milk and the nutrition and antibodies it provides to the reassurance of her warmth and love.
Brain growth, his immune system, and his respiration rate develop ideally as he rests against her skin-to-skin, releasing the perfect hormones needed for his system, and hers.
The foundation for basic trust is laid as he hears the voices of both father and mother, and they respond to his communication. The first few weeks and months of life have been likened to a “fourth trimester,” where baby humans are designed to remain still a unit with their mothers.
There is nothing in the world as important to a baby as his mother.
However, for Baby Paxton, these basic human needs are no longer being met, thanks to the Arizona Department of Children's Services (DCS).
When he was only 48 hours old, social workers took him away from his parents, Briana and Jordan Meissinger, claiming that this is “necessary to protect the child from suffering abuse or neglect.”
In the name of protecting him from potential possible harm, Child Protective Services is depriving him of the very things he needs the most.
Briana Meissinger told Health Impact News:
They took him! I was hoping they would leave us alone.

Newborn Baby Paxton Meissinger only had 48 hours with his parents before the state seized him away. Photo supplied by family
Social Worker – “We Are at Your House. Where Are You?”
The devastated parents got a call from DCS just 24 hours after Briana's c-section.
While she was recovering from surgery in her hospital room and bonding with her new baby, social workers were sitting in the driveway of the Meissingers' home demanding a meeting.
The workers refused to say what it was about other than that there were new allegations of “general neglect” that they needed to discuss. Obviously, Briana was not able to go home to meet with them since her baby had been born the day before and they were still at the hospital.
The social workers refused to divulge what the allegations were, but Briana and Jordan later learned that the social workers had reportedly received an anonymous call that the baby had been born 8 days prior and that they were home already neglecting the baby. The DCS workers had already obtained a warrant based on this and other incorrect information, but they didn't mention that to the Meissingers.
They showed up at the hospital the next day, Thursday, October 18, and seized Baby Paxton from his parents.
The incorrect birth date was another in a long line of wrong, false, or outright deceptive statements made by the department over the last year. In conjunction with Phoenix Children's Hospital and their Child Abuse Pediatrician, DCS had taken the Meissingers' son Keaton last September over allegations of Shaken Baby Syndrome.
From the very beginning of that case, some doctors suspected that he had an infection which was treated with several antibiotics. Other medical experts have stated the same, but DCS and the Child Abuse Pediatrician have stubbornly clung to their interpretation of Keaton's symptoms.
The long, drawn-out case to decide which diagnosis to believe is still in the Maricopa Juvenile Court. Dependency has yet to be determined by the courts.
After she learned that DCS intended to step in and take their newest baby, Briana said:
This warrant was one-sided. They didn't give our side, which is the fact that this is a highly contested case. We have experts and medical professionals that are saying that their allegations are bullshit.
THEIR experts are saying that they can't even for sure say that this is abuse, so they haven't proven anything. Nothing. And they're trying to take our newborn from us.
There's nothing we can do!
She explained that, until they can go before a judge, they cannot even fight this to keep their baby.
The Maricopa County social workers went to a different judge than the one in Keaton's case in order to get the warrant to seize Baby Paxton. The Meissingers believe that, had they gone to the judge who is currently presiding over their case, they would not have been able to get a warrant. The judge who signed it was “misled,” says Briana.
Their judge has heard some of the Meissingers' side of the story as well as a little bit from medical experts who adamantly disagree with the diagnosis of abuse by the Child Abuse doctor at Phoenix Children's Hospital.
There are still at least a couple more days left of the trial. The next one is at the end of October, followed by another day or two possibly to be held in December before the dependency case wraps up.
According to several doctors and medical experts whose presuppositions have not blinded them to see other medical conditions that can cause similar symptoms, Keaton's medical history and records do not show any signs of trauma or abuse. Rather, they are, in the words of one of their experts, “100% consistent with [a] brain infection.”
Baby Keaton's Story – Force Vaccinated in Spite of Medical Problems
Baby Paxton's big brother was born on June 6, 2017. Briana's labor was induced, and she was given high doses of pitocin (labor-inducing drug).
After 2 days of hard labor, the baby was not handling the contractions well. His chart showed “decels” in his heart rate, and Briana began having convulsions. They were rushed into surgery for an emergency c-section.
Keaton required resuscitation to help him to breathe when he was born, and he was given oxygen. His APGAR score was just 5 at both one minute and 5 minutes, which indicates that he was in trouble.
He spent his first few hours in the NICU, but he recovered. He was given a Vitamin K shot and Hepatitis B vaccine.
Briana says that “he was extremely fussy for a newborn baby.” After a few weeks, he improved, until his 2 month shots:
At his 2 month doctor appointment he was diagnosed with Acid Reflux and was prescribed renititidine. I had done quite a bit of research on vaccines, but not nearly enough I know now. At his 2 month appointment on 8/10/2017, I asked his Pediatrician at the time, Dr. Mary Lavalley, to do a delayed and spaced out schedule for his vaccinations.
He was very croupy frequently as he breathed, which was another concern we brought up at the appointment. Because of this, Dr. Lavalley got upset and snappy with me stating that we HAD to get ALL of his vaccines THAT day, BECAUSE he was sick- that not doing this would mean we were knowingly neglecting his safety. She bullied us into it, so I sat there and cried while he received all of his shots aside from the pneumococcal vaccine. [It was a total of 6 vaccines.] That's when things began, and steadily went downhill.
For the first almost 4 days he screamed a shrill painful scream as he tensed up his whole body, pulling his legs to his chest. He would scream so hard that he would have a ” silent scream ” where he would hold his breath, which really worried us and broke our hearts. knew he was in pain, but at the time I had no idea that this was due to encephalitis.
He ran a fever on and off for the next week. His typical hour or two naps became 20 minutes, and he “would wake up from his sleep tensed up screaming before he'd even open his eyes.”
The second week is when the vomiting started. Keaton began seeming dazed, and the happy baby we knew started to fade away. He wasn't focusing or tracking as much. He was rarely smiling. All of this, the pediatrician informed us was “normal,” and that some babies' symptoms last a little longer than others.
As a Mother, I knew, I FELT that these things weren't normal. I felt it with every inch of my being that something was wrong with my baby.

It was apparent to Briana and Jordan Meissinger that Keaton was not the same after his 2 month shots. Photo provided by family.
On August 24, 2017, Keaton woke up from a nap, crying. Briana was out running an errand, and Jordan changed his son's diaper. When he went into the kitchen to prepare a bottle, the baby suddenly stopped crying.
Alarmed, his father went to check on him. He looked like he was sleeping, but when Jordan picked him up, he was “completely limp” and wouldn't wake up.
He called Briana who was just 5 minutes away from home by that time. When she got home, Keaton was “awake, but not alert.”
While she stripped him down to check for any sign of insect or spider bites or a rash or some other explanation, he seemed dazed. She says his eyes were as wide as saucers and his pupils were “huge.”
The terrified couple knew immediately that they needed to rush him to the hospital.
At nearby Banner Del Webb Hospital, a nurse recommended that they try to feed him. Keaton promptly projectile vomited “everywhere.”
Doctors began running tests. One doctor came in and said that the x-ray showed that he had “junked up lungs,” and told them that this could be septic pneumonia or meningitis.
His white blood cell count was high, at 22,000. The normal range is 5,000 to 10,000. (Source). Elevated levels usually indicate infection.
With babies that young, the doctor explained, infections can be very serious. They cannot afford to wait for the results of a culture to determine what organism is causing the infection. They begin treatment immediately. Doctors started Keaton on 3 strong antibiotics.
The baby began improving dramatically in less than an hour. He stopped crying, and began cooing and making eye contact. Briana and Jordan were greatly relieved.
The Doctor then said that he needed a Lumbar Puncture, and that he also needed to be transferred to a Childrens Specialty Hospital – that we could either choose Banner Thunderbird, or Phoenix Children's, and that we could either have him get the LP there, or once he's transferred.
This is where we made our biggest mistake, we chose Phoenix Children's Hospital, and opted to have them do the LP, because they specialize in Children, and we felt we could trust them more with doing an LP.
They were wrong.
Phoenix Children's Hospital has a long history of medically kidnapping children, as we have reported many times.
The Meissingers didn't know that information. Nor were they aware that, like many Children's Hospitals, Phoenix has Child Abuse Pediatricians on staff.
The pattern of these doctors is to “find” abuse where none exists, often ignoring signs of real medical conditions or neglecting to do needed testing in order to do differential diagnoses.
At Phoenix Children's Hospital, the lumbar puncture showed that Keaton's cerebral spinal fluid was positive for enterovirus, a virus that can cause various illnesses including encephalitis (brain inflammation) and meningitis.
Other tests were run, including repeat x-rays, an MRI, a CT scan of Keaton's head, and an ophthalmology test.
Not surprisingly, given Keaton's traumatic birth history, he was found to have subdural hematomas and retinal hemorrhaging. These symptoms can even occur in the most normal of childbirths, and they are extremely common with difficult births, pitocin induction, and rescuscitation with oxygen, all of which factors were present when Keaton was born.
See:
Common Childbirth Practice Could Lead to Later False Diagnosis of Shaken Baby Syndrome
Combined with the brain swelling likely caused by the enterovirus, that meant that “the triad” was present.
When this trio of symptoms are present, some doctors, including most Child Abuse Pediatricians, view that as diagnostic of Shaken Baby Syndrome, even if there are genuine medical conditions, such as a viral illness, that could cause the same symptoms.
Neuropathologist Doctor: I Believed in Shaken Baby Syndrome until Science Showed I was Wrong
By the time labs were run for Keaton at Phoenix Children's Hospital, his white blood cell was much closer to normal, at 11,000. He tested negative for any bacterial infection at that time, but he had been on 3 strong antibiotics for several hours. According to several medical expert reports, this was normal.
However, the Child Abuse Pediatrician at Phoenix Children's, Dr. Cynthia Nelson, didn't see it that way. From her medical reports, it appears that once she saw the “triad” of symptoms associated with Shaken Baby Syndrome, she threw out the possibility of infection or anything else besides abuse being the the cause of Baby Keaton's symptoms.
DCS was called, and the Meissingers were accused of abusing Keaton by shaking him, and he was seized from them.
The family has been fighting to get him back ever since.
A juvenile court trial to determine dependency was set for early April, but in typical fashion, DCS has requested delay after delay. There were a couple of court dates in September, but the hearings are not complete. Most of the defense testimony has not yet been heard. The next court date is set for October 31.

A case worker argued that Keaton was developmentally delayed. The Guardian ad Litem promptly went to see him at his day care, and found that nothing the social worker said about his development was true. Photo provided by family.
Meanwhile, Briana Meissinger gave birth to a new baby this week. The parents had hoped that everything would be resolved by the time Baby Paxton would be born, and that DCS and the court would see that they didn't hurt Keaton, that instead he was sick.
The first hospital that saw Keaton saw no reason to suspect abuse. They believed that there was evidence of an infectious process, and they began treatment in line with that evidence. Other medical experts have looked at their case and come to a very difference conclusion than the doctors at Phoenix Children's and DCS.
In fact, in contrast with the Child Abuse Pediatricians, these experts take into account the entire symptom picture, not throwing out symptoms such as 3 days of fever, shrill, high-pitched crying, frequent leg tremors, and other symptoms such as the high white blood cell count.
The Child Abuse Pediatrician wrote in the records that the baby tested positive for enterovirus but that it was not the cause of Keaton's problems. Because he had the triad, it was “suspicious for abuse,” and other symptoms were thrown out the window as irrelevant. Because she suspected abuse, she rejected the possibility of infection, though meningitis was never truly ruled out.
Everything was seen from that point through the lens of abuse.
This is circular reasoning at its most insidious. The parents are deemed guilty because the doctor has interpreted the data as evidence of guilt. DCS and the family court system often makes no room for another interpretation of the facts.
During the course of the DCS case against the Meissingers, they and their attorneys thought at one point that they had all of the medical records. They were supposed to have them, and DCS told them that they had all the records. A representative of Phoenix Children's Hospital signed an affidavit that all of the records had been released to the family's attorneys.
However, some evidence, specifically some of the scans that DCS and Phoenix Children's Hospital said were evidence of abuse, were not included in the records they released. DCS said they do not consider medical imaging and scans to be part of the medical record, thus their practice is never to disclose them. This deprives the defense of being able to have them independently evaluated.
Circular Reasoning and Arrogance by Child Abuse Pediatricians
Attorneys for the couple filed an objection with sobering words about the arrogance that the decision represents:
DCS's position also presumes that the scans are subject to only one interpretation and PCH's report on the scan is conclusive to 100% accuracy.
That decision is not theirs to make.
If that is DCS's position, it is disingenuous at best and a misrepresentation to the Court at worst.
It is indicative of a factor common to almost every medical kidnapping case that we have covered involving Child Abuse Specialists: These doctors apparently expect that their verdict is the only possible conclusion.
As they work hand in hand with Child Protective Services, their testimony is elevated above any other evidence and is not to be challenged.
Dissenters are ridiculed and discredited. All other interpretations, even if they are more solidly aligned with scientific evidence, are rejected.
Social workers, attorneys, and judges are all expected to fall into line in giving one particular class of people – Child Abuse Pediatricians – the omnipotent ability to be judge and jury, boding no challenge or alternate interpretation of the evidence.
They are accountable to no one for their decisions, even if it leads to the destruction of an innocent family or the incarceration of an innocent parent.

A doctor with an agenda and a conflict of interest is allowed to unilaterally make decisions that rob children and parents of each other. Photo provided by family.
In countless cases across America, medical professionals who challenge the decisions of Child Abuse Pediatricians are ridiculed and discredited.
Judges have been known to ignore a dozen reports by various experts in favor of one report by a Child Abuse Pediatrician.
Yet these doctors are not qualified or trained as experts in the fields who are better suited to identify medical conditions that are not the result of abuse. They are not experts in radiology, infectious diseases, genetics, or neurology.
See:
Pediatric Child Abuse “Experts” are NOT Experts in Anything
Child Abuse Pediatricians Have Financial Motive to Kidnap Children
Attorneys for the Meissingers have discovered that taxpayers, through the Arizona Department of Children and Families, are paying financial incentives to Child Abuse Pediatricians to turn in parents for abuse. The hospitals get kickbacks of more than $800 per child.
Here is a price sheet for the Kids for Cash agreement between DCS and Phoenix Children's Hospital – the hospital that has been involved in more Medical Kidnap stories than any other hospital in the entire country:
Source: Phoenix Children's Hospital
There is ample evidence that the Meissinger's son Keaton suffered from a viral infection following vaccines. While the trial is not yet finished and all the testimony has not yet been heard, DCS social workers have proceeded as though Briana and Jordan Meissinger are guilty. There is no presumption of innocence until proven guilty with the agency.
Social workers presented a petition to a judge asserting their guilt as established fact though it is far from such.
The warrant says:
Due to the parents' continued denials about the cause of the injuries to Keaton, their home is an unsuitable environment for Baby Boy Meissinger.
Because they refuse to admit guilt, the social workers reasoned, the parents are guilty.
The warrant also states:
The parents have claimed the injuries to Keaton were the result of vaccines and/or viral infections but medical professionals have indicated Keaton's injuries could not have been sustained from vaccines or viral infections as suggested by the parents.
The social workers represent that the opinion of the Child Abuse Pediatrician at Phoenix Children's Hospital is the only valid one, while ignoring the fact that numerous doctors and medical experts assert that Keaton's injuries were, indeed, the result of a viral infection.
Thus, based on wrong information, Baby Paxton has been ordered by a judge to be taken from his parents.
In the course of “protecting” him, DCS is subjecting him to risks that began from the moment they tried to put him in a social worker's car at the hospital.
Paxton's father noticed that the car seat in her vehicle did not have the insert to protect a newborn's head. In order to protect his baby, he had to inform the worker that it was needed, and then he was the one who provided the insert for the social worker's car.
How You Can Help
A Facebook page was established by supporters when the family first began trying to get Keaton back called Bring Keaton Home. Now, as Briana and Jordan Meissinger work to get Paxton home as well, supporters want to continue to utilize Keaton's page for people to learn how they can help with getting both babies restored to their parents.

Governor Doug Ducey can be reached at 602-542-4331 or contacted here.
Greg McKay is the Director of DCS/CPS in Arizona. His office may be reached at 602-255-2500.
The Senator for the Meissingers' district is Senator Rick Gray. He is on the Health and Human Services Committee and may be reached at 602-926-5413 or contacted here.
The House Representative for their district is Representative David L. Cook. He may be reached at 602-926-5162 or contacted here.
Many Arizona parents are fed up with Phoenix Children's Hospital and DCS medically kidnapping children, and some of them are gathering together to rally in front of the hospital next Saturday, October 27, 2018. See the event page, Peace Rally – Against Medical Kidnapping on Facebook for more details.
Comment on this article at MedicalKidnap.com.
Medical Kidnapping: A Threat to Every Family in America T-Shirt

100% Pre-shrunk Cotton! Order here!
Medical Kidnapping is REAL!
See: Medical Kidnapping: A Threat to Every Family in America Today
Help spread the awareness of Medical Kidnapping by wearing the Medical Kidnapping t-shirt!
Support the cause of MedicalKidnap.com, which is part of the Health Impact News network.
Order here!
<!--//<![CDATA[ var m3_u = (location.protocol=='https:'?'https://network.sophiamedia.com/openx/www/delivery/ajs.php':'http://network.sophiamedia.com/openx/www/delivery/ajs.php'); var m3_r = Math.floor(Math.random()*99999999999); if (!document.MAX_used) document.MAX_used = ','; document.write ("<scr"+"ipt type='text/javascript' src='"+m3_u); document.write ("?zoneid=3&target=_blank"); document.write ('&cb=' + m3_r); if (document.MAX_used != ',') document.write ("&exclude=" + document.MAX_used); document.write (document.charset ? '&charset='+document.charset : (document.characterSet ? '&charset='+document.characterSet : '')); document.write ("&loc=" + escape(window.location)); if (document.referrer) document.write ("&referer=" + escape(document.referrer)); if (document.context) document.write ("&context=" + escape(document.context)); if (document.mmm_fo) document.write ("&mmm_fo=1"); document.write ("'><\/scr"+"ipt>"); //]]>-->

Support the cause against Medical Kidnapping by purchasing our new book!
If you know people who are skeptical and cannot believe that medical kidnapping happens in the U.S. today, this is the book for them! Backed with solid references and real life examples, they will not be able to deny the plain evidence before them, and will become better educated on this topic that is destroying the American family.

1 Book – 228 pages Retail: $24.99 FREE Shipping Available! Now: $14.99 Order here!
2 Books Retail: $49.98 (for 2 books) FREE Shipping Available! Now: $19.99 (for 2 books) Order here!
Also available as eBook:

eBook – Download Immediately! $9.99
<!--//<![CDATA[ var m3_u = (location.protocol=='https:'?'https://network.sophiamedia.com/openx/www/delivery/ajs.php':'http://network.sophiamedia.com/openx/www/delivery/ajs.php'); var m3_r = Math.floor(Math.random()*99999999999); if (!document.MAX_used) document.MAX_used = ','; document.write ("<scr"+"ipt type='text/javascript' src='"+m3_u); document.write ("?zoneid=3&target=_blank"); document.write ('&cb=' + m3_r); if (document.MAX_used != ',') document.write ("&exclude=" + document.MAX_used); document.write (document.charset ? '&charset='+document.charset : (document.characterSet ? '&charset='+document.characterSet : '')); document.write ("&loc=" + escape(window.location)); if (document.referrer) document.write ("&referer=" + escape(document.referrer)); if (document.context) document.write ("&context=" + escape(document.context)); if (document.mmm_fo) document.write ("&mmm_fo=1"); document.write ("'><\/scr"+"ipt>"); //]]>-->
0 notes
Text
Lawsuit: Company spread pills around Colorado
DENVER (AP) — The sales rep for one of America's most prominent opioid manufacturers walked out of a Wheat Ridge pain clinic in May 2010 and couldn't help but notice something odd.
"(M)ost patients were young and particularly healthy looking," he wrote in a note on the visit.
Reps from Purdue Pharma were hardly unfamiliar with Dr. Kevin Clemmer's clinic. They had been there 94 times before in the previous four years — a rate of nearly twice a month — mostly to sell their blockbuster opioid painkiller, OxyContin, The Colorado Sun reported Thursday.
In the early years, Clemmer had been hesitant, saying he had concerns "about doing this because of abuse and diversion," according to a Purdue rep's note quoted in a newly unsealed court document. But, after Purdue representatives paid him roughly 60 visits, Clemmer warmed up to OxyContin, telling a representative that he liked prescribing the drug because Purdue coupons made it inexpensive, according to the court document.
When a Purdue representative visited Clemmer's clinic in April 2010 to ask about an apparently forged prescription from Clemmer, the representative made sure to leave behind more OxyContin coupons. A month later came the May 2010 visit, where a Purdue representative was again looking into a pharmacy's concern that the opioid prescriptions coming out of Clemmer's clinic were not legitimate.
Clemmer, who had faced previous discipline for his narcotics prescription practices, told the rep that he was following the rules. The rep, despite his observation about Clemmer's patients, gave Clemmer a resource guide "on how to protect his practice," according to the rep's note.
That day was the 95th and final visit Purdue reps paid to Clemmer.
Three months later, one of Clemmer's patients overdosed and died. A year-and-a-half later, Clemmer's medical license was revoked. Three years later, Clemmer pleaded guilty in federal court to illegally distributing OxyContin — with at least three deaths linked to his clinic and Colorado's opioid epidemic now raging.
Federal law requires drug companies to inform the DEA when they notice suspicious orders or prescribing patterns. But, all along, Purdue representatives said nothing, a lawsuit brought against the company by the Colorado Attorney General's Office alleges.
"Purdue never reported any of these red flags about Dr. (Clemmer's) practice to state or federal law enforcement in Colorado," the lawsuit's complaint states.
Five-hundred-sixty people died last year in Colorado from opioid overdoses.
Even after massive efforts by doctors and hospitals to change their prescribing patterns and by state officials to make opioid treatment and overdose reversal drugs more available, opioids still accounted for most of the 1,012 drug overdose deaths in 2017. That is the largest number of people killed by overdoses in a single year in Colorado history.
The attorney general's lawsuit provides a never-before-seen account of how part of the epidemic began, told through the notes of Purdue sales representatives who methodically pursued, encouraged and manipulated Colorado doctors to set aside their concerns about addiction and to prescribe higher and higher doses of potentially deadly drugs, according to the lawsuit's complaint.
"Purdue unleashed a surge of prescription opioids on Coloradans while hiding the facts about their drugs' addictive properties," Colorado Attorney General Cynthia Coffman said in a statement when the lawsuit was filed last month. "Their corporate focus on making money took precedence over patients' long-term health, and Colorado has been paying the price in loss of life and devastation of its communities as they struggle to address the ongoing opioid crisis."
Colorado is at least the 28th state to sue Purdue Pharma over the opioid crisis. The lawsuit's 96-page complaint was originally filed under seal but was recently made public.
Reached for comment on the lawsuit, a Purdue spokesman sent this statement to The Colorado Sun:
"We vigorously deny the state's allegations. The state claims Purdue acted improperly by communicating with prescribers about scientific and medical information that FDA has expressly considered and continues to approve. We believe it is inappropriate for the state to substitute its judgment for the judgment of the regulatory, scientific and medical experts at FDA. We look forward to the opportunity to present our substantial defenses."
The spokesman also provided a chart from the federal Food and Drug Administration showing that OxyContin accounts for only about 2 percent of the roughly 200 million opioid prescriptions dispensed per year in America.
"We share the state's concern about the opioid crisis," the Purdue statement said. "While Purdue Pharma's opioid medicines account for less than 2 percent of total prescriptions, we will continue to work collaboratively with the state toward bringing meaningful solutions to address this public health challenge."
The attorney general's lawsuit paints a picture of a company that cared little about its drugs' consequences.
Beginning in 2000, Purdue representatives or surrogates gave presentations extolling the benefits of OxyContin in Colorado, according to the lawsuit. They worked to ingratiate themselves into local medical professional associations, which the lawsuit alleges did not disclose connections to Purdue when testifying on opioid regulation.
The lawsuit cites numerous notes from sales calls made by Purdue reps and obtained by the attorney general's office.
By 2006, according to notes cited in the lawsuit, Purdue sales reps were encouraging doctors to prescribe higher and higher doses of OxyContin to compensate for doctors' observations that standard doses of OxyContin did not last the 12 hours Purdue claimed they would. Doctors who had begun with relatively small doses — 10 or 15 milligrams, twice a day — soon were prescribing 80-milligram doses, after visits from Purdue reps.
During one sales call in Colorado, a Purdue rep wrote in a note, referring to the prescriber, "get her over fear of dosing too high."
And Purdue was aware of the financial incentive to push higher doses, the lawsuit alleges. The complaint cites a Purdue marketing presentation warning that a shift of 15,000 prescriptions from 20- or 15-milligram doses to 10-milligram doses represented a loss of $2 million.
"OxyContin is promotionally sensitive, specifically with the higher doses, and recent research findings reinforce the value of sales calls," Purdue's business plan stated, according to the lawsuit.
Meanwhile, the lawsuit alleges that Purdue reps downplayed the risk of addiction. During one call in August 2006, a Purdue rep discussed with a Colorado doctor, "addiction in clinical issues to show how rare(ly) it occurs in pain (patients) to alleviate concerns."
Purdue invented the concept of "pseudoaddiction," according to the lawsuit — a condition that supposedly looked like addiction but that Purdue claimed was actually a sign of patients being undertreated and needing higher doses of opioids. During a May 2006 call, a Purdue rep noted discussing pseudoaddiction with a Colorado prescriber.
"He admitted he has a hard time identifying these patients," the rep noted, according to the lawsuit.
In 2010 — a year in which more than 200 Coloradans died from prescription opioid overdoses — a Purdue rep noted a visit with a Colorado doctor in which the doctor said, "many (patients) have (a) fear of getting addicted if they go on (OxyContin)."
"I told him," the rep noted, according to the lawsuit, "that if (patients) are fearful of addiction they will probably be good when taking (OxyContin) and convince them you would not prescribe any product that would lead to major problems."
Purdue's marketing push began paying off handsomely for the company as early as 2006. More than 2.9 million opioid prescriptions were written in Colorado that year — including 15,000 for OxyContin. That year, 1.3 million tablets of OxyContin flowed into the state.
But it only increased from there. By 2012, at the peak of opioid prescriptions in Colorado, doctors wrote nearly 3.9 million opioid scripts — enough for nearly three-quarters of the state's residents to get one. About 123,000 of those were for OxyContin; 8.3 million tablets of OxyContin landed in Colorado hands that year.
The lawsuit portrays Purdue's marketing force as relentless in its pursuit of OxyContin sales. Doctors were visited dozens of times a year. Sales reps focused on specialty pain-management physicians but also family-practice doctors who were less experienced in treating pain.
In one visit with a Purdue rep in 2013, a Colorado medical provider said she was going to stop treating chronic pain patients. The Purdue representative responded by saying she was not telling the provider she should specialize in pain, "it's just that pain is one of (the) main reasons patients come to (the doctor)," according to the sales rep's notes quoted in the lawsuit.
When the provider insisted that she wasn't going to treat any new chronic pain patients, the sales rep said, "What are you going to do when (a) current patient develops (a) pain condition? . Let me show you what some of your peers are doing," according to the lawsuit.
And, at least for some doctors, these tactics had an impact on their prescribing practices.
The lawsuit cites an instance from 2006 when a provider who rarely wrote high-dose prescriptions for OxyContin said she was "freaked out" by a patient who had been referred to her and who was on a 480-milligram dose of OxyContin every 12 hours. The Purdue rep responded by saying there was no "ceiling dose and end organ damage with OxyContin," according to the rep's notes quoted in the lawsuit.
In the five years prior to that interaction, according to the lawsuit, the provider had written only 17 prescriptions for more than 60 milligrams of OxyContin. But that visit kicked off a sharp increase in the provider's dosing. The next year alone, in 2007, the provider wrote another 17 high-dose prescriptions. In 2010, the provider wrote 102 high-dose prescriptions.
What changed? During the four-year stretch between 2006 and 2010, Purdue reps visited the provider 108 times, or more than twice a month, according to the lawsuit.
To some patients, the doctor was known as "Candy Man."
By the time the doctor was arrested and sentenced in 2017 to eight years in federal prison for illegal narcotics distribution, Purdue sales reps had visited his clinic dozens of times — and apparently never alerted authorities to any suspicions about the doctor's prescribing patterns.
"Upon information and belief, Purdue rarely, if ever, reports suspicious opioid prescribers to federal or state authorities in Colorado," the lawsuit alleges.
This may be the lawsuit's most explosive claim. Even in cases where doctors were breaking the law or violating medical ethics, such as with Clemmer or "Candy Man," the lawsuit alleges that Purdue didn't step in to stop them.
In the case of "Candy Man," the lawsuit refers to the doctor only by the initials D.H. But the details included in the complaint make clear the doctor was Douglas Hammond, who is now serving a sentence at a federal prison in southern Colorado.
Hammond, according to his plea agreement in the federal criminal case, admitted to "routinely" writing prescriptions to patients for more than 300 oxycodone tablets a month. Many of those pills were later diverted into illegal sales, according to state and federal court documents.
One patient of Hammond's stood out in particular, though.
When Eddie Brantner first visited Hammond's clinic in December 2010, according to the lawsuit and plea agreement, he received 60 80-milligram OxyContin tablets and 180 15-milligram oxycodone tablets without even having to produce medical records — just a story about a hiking accident some years prior. At Brantner's next visit, a month later, Hammond upped the dose. Two weeks later, Hammond prescribed even more opioids.
By April 2011, Hammond had Brantner on 180 40-milligram OxyContin tablets and 600 30-milligram oxycodone tablets. And the next month, Hammond and his physician assistant upped the dose again, to 900 30-milligram oxycodone tablets for just one month, according to the plea agreement.
Brantner was only taking some of the pills and was giving the rest to an illegal pill-distribution ring, the plea agreement states. But his prescriptions didn't occur in a vacuum, either.
According to the attorney general's lawsuit, Purdue reps had visited Hammond 69 times in the two years prior to Brantner's first prescription. At Purdue's last visit to Hammond, a sales rep talked to the doctor about potent opioid patches for high-dose patients, and the rep assured Hammond that "there is no ceiling dose as long as the patient can tolerate the side effects," according to the lawsuit
That was on June 13, 2011.
The next day, according to court records, Brantner overdosed and died at the age of 34.
from Local News https://www.thedenverchannel.com/news/local-news/lawsuit-opioid-company-spread-pain-pills-around-colorado
0 notes
Text
Billionaire Opioid Executive Stands to Make Millions More on Patent for Addiction Treatment
youtube
By Dr. Mercola
An estimated 202,600 Americans died from opioid overdoses between 2002 and 2015,1 and drug overdoses are now the leading cause of death among Americans under the age of 50.2
Chronic opioid use also accounted for 20 percent of the increase in male unemployment between 1999 and 20153 and, remarkably, 74 percent of farmers report being addicted to opioids, or know someone who is.4
Aside from the staggering death toll, addiction to narcotic pain relievers also places an enormous economic burden on society, costing the U.S. an estimated $504 billion each year (2.8 percent of gross domestic product), according to a November 2017 White House report.5,6
Opioid Epidemic Is No Random Fluke
Adding insult to injury, evidence suggests opioid makers are directly responsible. They knew exactly what they were doing when they claimed opioids — which are chemically very similar to heroin — have an exceptionally low addiction rate when taken for pain.
In fact, the massive increase in opioid sales and subsequent addiction rates have been traced back to an orchestrated marketing plan aimed at misinforming doctors about the drug's addictive potential, and it is this false advertising campaign that seeded the current opioid epidemic — an epidemic so great it has even lowered the national life expectancy.
Purdue Pharma, owned by the Sackler family, was one of the most successful in this regard, driving sales of OxyContin up from $48 million in 1996 to $1.5 billion in 2002.7
Studies now show addiction affects about 26 percent of those using opioids for chronic non-cancer pain, and 1 in 550 patients on opioid therapy dies from opioid-related causes within 2.5 years of their first prescription.8
Meanwhile, Purdue's sales representatives were extensively coached on how to downplay the drug's addictive potential, claiming addiction was occurring in less than 1 percent of patients being treated for pain.
Evidence also shows Sackler family members were intimately involved with the marketing machinations behind OxyContin.9,10 In fact, attorney Mike Moore — who represents Ohio, Louisiana and Mississippi in lawsuits against Purdue Pharma — claims to have evidence connecting the Sackler family "directly, and personally, to corporate misdeeds" committed in the 1990s and 2000s.11
In 2007, Purdue Pharma did plead guilty to charges of misbranding "with intent to defraud and mislead the public," and paid $634 million in fines.12 Alas, a decade later, it's quite clear the company has not changed its ways to any significant degree. It, and the Sackler family, is still in the business of profiting from addiction.
OxyContin Maker Patents Opioid Addiction Treatment
As reported by STAT News earlier this month, Dr. Richard Sackler — who, according to Esquire journalist Christopher Glazek,13 was deeply involved in the marketing of OxyContin as head of the company's research and development, sales and marketing divisions — was recently awarded a patent for a new, faster-dissolving form of buprenorphine, a mild opioid drug used in the treatment of opioid addiction. As noted by STAT News:14
"… Sackler is listed as one of six inventors on the patent, which was issued in January [2018] … Critics told the [Financial Times] that they were disturbed that the patent could enable Sackler to benefit financially from the addiction crisis that his family's company is accused of fueling."
Indeed, the company is currently fighting more than 1,000 lawsuits brought by tribes, cities, counties and states across the U.S., which claim Purdue Pharma helped orchestrate the opioid addiction epidemic and should therefore help pay for the societal costs.
President Trump has also stated he would like to see a federal lawsuit be brought against opioid makers.15
Apparently, Sackler decided to pursue avenues to cash in on the epidemic instead. Salon magazine16 reported on the patent saying, "Sackler made billions off of sales of a drug that caused a massive public health crisis — and now he stands to make more billions by selling the public a solution." But that's not all. The Sacklers have actually been profiting from addiction in more ways than one for over a decade.
Purdue Pharma Secretly Owned Generic Oxycontin Too
As reported by Financial Times17 and the New York Post,18 the Sackler family also secretly owns Rhodes Pharma, "one of the biggest producers of generic opioids, which had never before been linked to the family."
What's more, this company was launched just four months after Purdue Pharma's guilty plea back in 2007. When combined, Purdue Pharma and Rhodes Pharma account for about 6 percent of the total opioid market in the U.S.
So, "not only did the Sacklers fail to scale back its marketing of OxyContin after the plea, they further cashed in on the pill crisis — by launching the second firm and selling more of the drug under a different name," the New York Post writes, adding:
"Rhodes [Pharma] was set up as a 'landing pad' in case the under-fire drug maker needed a clean start amid the 2007 criminal charges, a former senior manager at Purdue told the paper.
Together, both firms accounted for 14.4 million opioid prescriptions in 2016. Rhodes Pharma also makes other highly addictive opiates such as morphine, oxycodone and hydromorphone, according to the FDA."
Purdue Pharma to Offer Free Opioid Addiction Therapy
Sackler's new buprenorphine patent is actually held by Rhodes Pharma and, according to Bloomberg, Purdue has offered to donate an undisclosed number of treatment doses of this drug as part of any settlement that might come out of the 1,000 lawsuits currently pending. University of Kentucky law professor Richard Ausness told Bloomberg:
"I'd have to say this is a pretty clever move. Over the last 20 years, Purdue hasn't shown any real contrition or remorse, so I see this offer of free step-down drugs as a savvy negotiating tactic to limit what they have to pay in any settlement."
Opioids Still Being Widely Overprescribed
In related news, recent research19 published in the Annals of Internal Medicine shows nearly one-third of opioid prescriptions given in an outpatient setting are not backed by a documented medical reason for the prescription,20 suggesting the drugs are still being widely overprescribed and misused.
According to the authors, their findings "show the need for stricter rules on patients' needs for the highly addictive drugs."
Of the opioid prescriptions handed out during 809 million doctor's visits across the U.S. between 2006 and 2015, only 5 percent were prescribed for cancer-related pain; more than 66 percent were given for non-cancer pain — the most common being back pain, diabetes-related pain and arthritis — while just over 28 percent were prescribed in cases where no pain-related condition could be ascertained in the patient's medical record.
Curiously, the most common nonpain conditions for which an opioid was prescribed were high blood pressure and high cholesterol.
Dr. Harshal Kirane, director of addiction services at Staten Island University Hospital in New York City, who was not part of the study, told HealthDay News,21 "Despite numerous policy changes, recent analyses suggest national opioid prescribing rates have not meaningfully decreased … Lax prescribing practices remain widespread."
Seeing how doctors are largely failing to significantly cut down on opioid prescriptions, might cutting insurance coverage do the trick? Both Cigna and Blue Cross Blue Shield of Florida have stopped paying for OxyContin, and as of January 2019, Blue Cross Blue Shield of Tennessee will no longer pay for it either.22
They all still pay for other brands of opioids, though, which may water down the impact of the decision. According to Blue Cross Blue Shield of Tennessee, the decision to drop OxyContin was primarily based on the fact that it still has a higher street value and is easier to crush, snort or inject than other opioids.
Struggling With Opioid Addiction? Seek Help!
Regardless of the brand, it's vitally important to realize that opioids are extremely addictive drugs that are not meant for long-term use for nonfatal conditions. Chemically, opioids are very similar to heroin, and if you wouldn't consider shooting up heroin for that toothache or backache, you really should reconsider taking an opioid to relieve the pain as well.
The misconception that opioids are harmless pain relievers has at this point killed hundreds of thousands of people, and destroyed the lives of countless more, including the families and friends of those who have died. Don't be so quick to be the next in line.
Some marketing materials for opioids still claim the drug will not cause addiction "except in very rare cases," describing the adverse effects patients experience when quitting the drug as a "benign state" and not a sign of addiction. This simply isn't true.
Panic is one psychological side effect commonly experienced when quitting these drugs, and this can easily fuel a psychological as well as physical dependence on the drug.
It's important to recognize the signs of addiction, and to seek help. If you've been on an opioid for more than two months, or if you find yourself taking higher dosages, or taking the drug more often, you're likely already addicted and are advised to seek help from someone other than your prescribing doctor. Resources where you can find help include:
Your workplace Employee Assistance Program
The Substance Abuse Mental Health Service Administration23 can be contacted 24 hours a day at 1-800-622-HELP
Treating Your Pain Without Drugs
With all the health risks associated with opioid painkillers, I strongly urge you to exhaust other options before resorting to these drugs. The good news is there are many natural alternatives to treating pain. Following is information about nondrug remedies, dietary changes and bodywork interventions that can help you safely manage your pain.
Medical cannabis — Medical marijuana has a long history as a natural analgesic and is now legal in 31 states. You can learn more about the laws in your state on medicalmarijuana.procon.org.24
Kratom — Kratom (Mitragyna speciose) is a plant remedy that has become a popular opioid substitute.25 In August 2016, the DEA issued a notice saying it was planning to ban kratom, listing it as Schedule 1 controlled substance. However, following massive outrage from kratom users who say opioids are their only alternative, the agency reversed its decision.26
Kratom is safer than an opioid for someone in serious and chronic pain. However, it's important to recognize that it is a psychoactive substance and should be used with great care. There's very little research showing how to use it safely and effectively, and it may have a very different effect from one person to the next. The other issue to address is that there are a number of different strains available with different effects.
Also, while it may be useful for weaning people off opioids, kratom is in itself addictive. So, while it appears to be a far safer alternative to opioids, it's still a powerful and potentially addictive substance. So please, do your own research before trying it.
Low-Dose Naltrexone (LDN) — Naltrexone is an opiate antagonist, originally developed in the early 1960s for the treatment of opioid addiction. When taken at very low doses (LDN, available only by prescription), it triggers endorphin production, which can boost your immune function and ease pain.
Curcumin — A primary therapeutic compound identified in the spice turmeric, curcumin has been shown in more than 50 clinical studies to have potent anti-inflammatory activity. Curcumin is hard to absorb, so best results are achieved with preparations designed to improve absorption. It is very safe and you can take two to three every hour if you need to.
Astaxanthin — One of the most effective oil-soluble antioxidants known, astaxanthin has very potent anti-inflammatory properties. Higher doses are typically required for pain relief, and you may need 8 milligrams or more per day to achieve results.
Boswellia — Also known as boswellin or "Indian frankincense," this herb contains powerful anti-inflammatory properties, which have been prized for thousands of years. This is one of my personal favorites, as it worked well for many of my former rheumatoid arthritis patients.
Bromelain — This protein-digesting enzyme, found in pineapples, is a natural anti-inflammatory. It can be taken in supplement form, but eating fresh pineapple may also be helpful. Keep in mind most of the bromelain is found within the core of the pineapple, so consider eating some of the pulpy core when you consume the fruit.
Cayenne cream — Also called capsaicin cream, this spice comes from dried hot peppers. It alleviates pain by depleting your body's supply of substance P, a chemical component of nerve cells that transmit pain signals to your brain.
Cetyl myristoleate (CMO) — This oil, found in dairy butter and fish, acts as a joint lubricant and anti-inflammatory. I have used a topical preparation of CMO to relieve ganglion cysts and a mild case of carpal tunnel syndrome.
Evening primrose, black currant and borage oils — These oils contain the fatty acid gamma-linolenic acid, which is useful for treating arthritic pain.
Ginger — This herb is anti-inflammatory and offers pain relief and stomach-settling properties. Fresh ginger works well steeped in boiling water as a tea, or incorporated into fresh vegetable juice.
Dietary Changes to Fight Inflammation and Manage Your Pain
Unfortunately, physicians often fall short when attempting to effectively treat chronic pain, resorting to the only treatment they know: prescription drugs. While these drugs may bring some temporary relief, they will do nothing to resolve the underlying causes of your pain. If you suffer from chronic pain, making the following changes to your diet may bring you some relief.
Consume more animal-based omega-3 fats — Similar to the effects of anti-inflammatory pharmaceutical drugs, omega-3 fats from fish and fish oils work to directly or indirectly modulate a number of cellular activities associated with inflammation. While drugs have a powerful ability to inhibit your body's pain signals, omega-3s cause a gentle shift in cell signaling to bring about a lessened reactivity to pain.
Eating healthy seafood like anchovies or sardines, which are low in environmental toxins, or taking a high-quality supplement such as krill oil are your best options for obtaining omega-3s. DHA and EPA, the omega-3 oils contained in krill oil, have been found in many animal and clinical studies to have anti-inflammatory properties, which are beneficial for pain relief.
Radically reduce your intake of processed foods — Processed foods not only contain chemical additives and excessive amounts of sugar, but also are loaded with damaging omega-6 fats. By eating these foods, especially fried foods, you upset your body's ratio of omega-3 to omega-6 fatty-acids, which triggers inflammation. Inflammation is a key factor in most pain.
Eliminate or radically reduce your consumption of grains and sugars — Avoiding grains and sugars, especially fructose, will lower your insulin and leptin levels. Elevated insulin and leptin levels are one of the most profound stimulators of inflammatory prostaglandin production, which contributes to pain.
While healthy individuals are advised to keep their daily fructose consumption below 25 grams from all sources, you'll want to limit your intake to 15 grams per day until your pain is reduced. Eating sugar increases your uric acid levels, which leads to chronic, low-level inflammation.
Optimize your production of vitamin D — As much as possible, regulate your vitamin D levels by regularly exposing large amounts of your skin to sunshine. If you cannot get sufficient sun exposure, taking an oral vitamin D3 supplement, along with vitamin K2 and magnesium, is highly advisable. Get your blood level tested to be sure you're within the therapeutic range of 60 to 80 ng/mL year-round.
Bodywork Methods That Reduce Pain
The following bodywork methods have also demonstrated effectiveness for pain relief and pain management.
• Acupuncture — An estimated 3 million American adults receive acupuncture annually,27 most often for the treatment of chronic pain. A study28 published in the Archives of Internal Medicine concluded acupuncture has a definite effect in reducing back and neck pain, chronic headache, osteoarthritis and shoulder pain, more so than standard pain treatment.
• Chiropractic adjustments — While previously used most often to treat back pain, chiropractic treatment addresses many other problems, including asthma, carpal tunnel syndrome, fibromyalgia, headaches, migraines, musculoskeletal pain, neck pain and whiplash.
According to a study29 published in the Annals of Internal Medicine, patients with neck pain who used a chiropractor and/or exercise were more than twice as likely to be pain-free in 12 weeks compared to those who took medication.
• Massage therapy — Massage releases endorphins, which help induce relaxation, relieve pain and reduce levels of stress chemicals such as cortisol and noradrenaline. A systematic review and meta-analysis30 published in the journal Pain Medicine, included 60 high-quality and seven low-quality studies that looked into the use of massage for various types of pain, including bone and muscle, fibromyalgia, headache and spinal-cord pain.
The study revealed massage therapy relieves pain better than getting no treatment at all. When compared to other pain treatments like acupuncture and physical therapy, massage therapy still proved beneficial and had few side effects. In addition to relieving pain, massage therapy also improved anxiety and health-related quality of life.
• Emotional Freedom Techniques (EFT) — EFT continues to be one of the easiest and most effective ways to deal with acute and chronic pain. The technique is simple and can be applied in mere minutes. A study31 published in Energy Psychology examined the levels of pain in a group of 50 people attending a three-day EFT workshop, and found their pain dropped by 43 percent during the workshop.
Six weeks later, their pain levels were reported to be 42 percent lower than before the workshop. As a result of applying EFT, participants felt they had an improved sense of control and ability to cope with their chronic pain. In the video below, EFT expert Julie Schiffman, teaches you how to use EFT to address chronic pain.
youtube
from HealthyLife via Jake Glover on Inoreader http://articles.mercola.com/sites/articles/archive/2018/09/26/purdue-pharma-owns-generic-opioids.aspx
0 notes
Text
3 Forms of Cancer that High Dose IV Vitamin C Can Help Beat
The use of IV vitamin C for cancer is nothing new. This treatment has been utilized since the 1970s all over the world. In fact, there are ongoing studies and clinical evidence that shows significant improvement in cancer patients’ quality of life, physically, mentally and emotionally.
This article aims to show you how a high dose IV vitamin C therapy can help fight three types of cancer. Read on to find out more.
1. Metastatic Liver Cancer
Freeofdisease.com published an article stating that IV vitamin C for cancer can help with fighting metastatic liver cancer. It says:
“IV Vitamin C Puts Metastatic Liver Cancer into Remission: In this remarkable new case study from Korea, intravenous vitamin C at a dose of 70 grams per infusion (given two times weekly) has apparently cured an elderly woman of her liver cancer. The 74-year-old woman had primary liver cancer (HCC) which had metastasized to her lungs and lymph nodes and was not being helped with conventional treatments. But after 10 months of treatment with IV vitamin C, the metastases had disappeared and the primary liver tumor had shrunk down in size. After another year of vitamin C therapy, and three more rounds of conventional treatment (transarterial chemoembolization—called “TACE”), PET-CT scans showed the liver tumor had completely disappeared.”
This finding is indeed remarkable considering the survival rate of patients who have metastatic liver cancer is slim to none.
Source: Freeofdisease.com
2. Colorectal cancer
In an article published by Yogesh Sharma last October 12, 2017, he wrote that recently researchers from Stem Cells and Regenerative Medicine Centre at the Yenepoya University, Karnataka, India, have discovered how high doses of water-soluble Vitamin C and niacin or Vitamin B3 can kill cancer stem cells.
According to the article:
“Research team lead by Dr Bipasha Bose and Dr Sudheer Shenoy investigated the effects of high doses and low doses of the two vitamins and found that low doses (dose range 5-25 micromolar) of Vitamin C and B3 lead to high proliferation and aggressiveness of colon cancer stem cells thereby indicating a need to be cautious while prescribing low doses of these vitamins to colon cancer patients.
However, high doses of the two vitamins (dose range 100 to 1000 micromolar) were successful in killing cancer stem cells. Such high doses of vitamins can only be achieved through intravenous injections in colon cancer patients…
This work is of significance, and researchers hope to establish a therapeutic dose of Vitamin C and B3 for colon cancer stem cell therapy. “If the therapeutic dose gets well validated under in vivo animal models, clinical trials can be a possibility in the long run,” added Dr. Bose.”
Source: TheHinduBusinessLine.com
Lots of colorectal cancer patients will significantly benefit from this treatment should the clinical trial show positive results.
3. Breast Cancer
The National Cancer Institute, one of eleven agencies that are part of the U.S. Department of Health and Human Services, and is the leading agency for cancer research and training, found this about IV vitamin C for cancer patients:
“Intravenous (IV) vitamin C was studied in patients with breast cancer who were treated with adjuvant chemotherapy and radiation therapy. The study found that patients who received IV vitamin C had a better quality of life and fewer side effects than those who did not.”
Source: Cancer.gov
With these pieces of evidence set in place, there is no reason why Oncologists would not include high doses of IV vitamin C for cancer as part of their standard clinical practice. Cancer patients now have a higher chance of beating this disease and live a far more healthier and longer life.
If you think this article is insightful, share this now! Who knows, the next life saved could be yours, your family, or your friends.
Want more information on IV vitamin C for cancer? Contact Dr. Amauri Caversan at his IV therapy Toronto lounge – (416) 922-4114. Free 15-minute consultation available!
You May Also Like: 4 Signs You May Need An IV Vitamin Therapy
The post 3 Forms of Cancer that High Dose IV Vitamin C Can Help Beat appeared first on Dr. Amauri Caversan.
0 notes
Link
Psychological Aftermath of Natural Disasters Dr. Mercola By Dr. Mercola With Texas, Florida and the Caribbean still reeling in the aftermath of hurricanes Harvey, Irma and Maria, the physical destruction is readily apparent. Less easily quantified is the effect of natural disasters like hurricanes on the human psyche. Not surprisingly, a study on the impact of Hurricane Sandy, which hit the East Coast of the U.S. in October 2012, revealed that experiencing personal and property damage during the storm increased the risk of long-term post-traumatic stress disorder (PTSD) symptoms.1 However, as the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) points out, natural disasters affect mental health not just during the event but before and after as well. "The toll and trauma that stems from disasters can contribute to stress and anxiety, acute stress reaction and ability to self-regulate — and for some, posttraumatic stress disorder," they note.2 If it seems like natural disasters are becoming more frequent, it's not in your head. The number of events increased threefold from 1980-1989 to 2000-2009.3 This makes it more important than ever to be aware of the psychological toll that natural disasters exert, as well as ways to help circumvent it and heal from the trauma. Anyone Can Be Mentally Harmed by Natural Disaster, But Children May Be Most at Risk People may have a wide range of reactions to experiencing a natural disaster, from stress and fear to depression and feelings of insecurity. Among those with preexisting mental health problems, natural disaster is likely to make them worse. Meanwhile, some people who had no preexisting problems may develop mental issues after the storm. Baylor College of Medicine professor and executive vice chair for community psychiatry told MedicalXpress, however, that children in particular should be closely monitored following a natural disaster. "The way kids react in these situations is very different from adults," he said. "Families need to watch out for the warning signs that kids may not be coping well with the events they've experienced."4 Warning signs may include isolating themselves or hiding in rooms, changes in eating habits or having fewer social interactions. A child may also have trouble getting over the loss of a favorite item like a blanket or toy. Among school-age kids, meanwhile, the ramifications can extend into their ability to succeed in school, due to both practical considerations and psychological consequences. In 2008, for instance, research found exposure to Hurricane Katrina increased aggressive behavior in high school students via PTSD and poorly regulated emotion.5 The extent of PTSD and other mental health symptoms in youth exposed to traumatic events vary widely, however, with PTSD increasing in those exposed to both a hurricane and community violence and decreasing in those with more social support from their peers.6 Speaking with The Atlantic, Joy Osofsky, a professor of pediatrics and psychiatry at Louisiana State University, also noted that the severity of a natural disaster's impact on children is associated with the stability of their broader environment.7 In particular, lack of stability and family chaos may harm the child's academic performance,8 whereas getting back to a routine can be therapeutic. "For instance, children who may have had a close relative relocate following the storm, or whose families experienced outsized economic strain," The Atlantic reported, "were likely to show greater signs of stress than those who had more stability. In the midst of such upheaval, Osofsky said, schools had the opportunity to be a source of stability." Natural Disaster Coping Strategies One of the best ways to alleviate anxiety if a natural disaster is approaching is to be prepared. The Anxiety and Depression Association of America (ADAA) recommends creating a plan ahead of time,9 including knowing where you'll go if you need to evacuate and compiling a preparedness kit with basic supplies, such as nonperishable food, water, a flashlight, a battery-operated radio and extra batteries. In addition, stay informed on the latest weather updates and warnings to help you feel you have some control over the situation. At the same time, accept that you cannot control the path of the storm and can only take the best steps to be prepared and take precautionary measures based on the latest information. The American Psychological Association (APA) further recommends emotionally preparing for a hurricane by:10 Having a plan and implementing it Getting the facts to determine your risk so you can take reasonable actions Making connections with family members and friends as an additional source of support Staying healthy via proper diet, exercise and rest, as a healthy mind and body will help you to make the best decisions and better deal with any oncoming threat Maintaining a hopeful outlook to help you through the storm and its aftermath After a natural disaster strikes, many find that doing something constructive and positive helps them to cope. You may consider donating blood, volunteering or cleaning up brush in your area to give you a sense of purpose and hope. Many experts also recommend getting back to your normal routine as soon as possible, and avoiding exposure to news stories if they contribute to your stress and anxiety. Meanwhile, take care of your body — eat well, sleep and exercise — to keep up your physical and mental stamina.11 Use Relaxation Strategies to Keep Calm If you're riding out a storm or trying to calm yourself as a hurricane approaches, relaxation techniques can be invaluable, and simple strategies, like breath work, can actually increase your resilience to stress. In the Annals of the New York Academy of Sciences, researchers reviewed data showing controlled breathing, or pranayama as it's known in the practice of yoga, may be beneficial in the treatment of depression, anxiety, post-traumatic stress disorder and for victims of mass disasters. "By inducing stress resilience, breath work enables us to rapidly and compassionately relieve many forms of suffering," the researchers concluded.12 One of the most effective breathing exercises to reduce stress and anxiety comes from the Buteyko Breathing Method, which involves making a conscious effort to breathe through your nose instead of your mouth. As such, it focuses on small breaths taken through your nose, as follows: Take a small breath into your nose, followed by a small breath out Then hold your nose for five seconds in order to hold your breath, and then release your nose to resume breathing Breathe normally for 10 seconds Repeat the sequence Other methods to help you invoke your body's relaxation response and counter the effects of stress include meditation, guided imagery and the Emotional Freedom Techniques (EFT). Research has shown that EFT significantly increases positive emotions, such as hope and enjoyment, and decreases negative emotional states, including anxiety.13 EFT is particularly effective for treating stress and anxiety because it specifically targets your amygdala and hippocampus, which are the parts of your brain that help you decide whether or not something is a threat. You can watch a demonstration of how to use EFT in the video below. Manage Your Stress Before, During and After the Storm Stress due to a natural disaster can be long-lasting, but your resiliency to the stress can make all the difference in how well you're able to cope and how quickly you're able to bounce back. For starters, choose healthy foods known to support a positive mood. Among them: Green leafy vegetables Organic, free-range turkey Fermented foods Wild-caught Alaskan salmon, sardines and anchovies Blueberries Dark chocolate, in moderation Avocado A daily dose of sunshine may also help to stabilize your mood. Serotonin, the brain hormone associated with mood elevation, rises with exposure to bright light and falls with decreased sun exposure. In 2006, scientists evaluated the effects of vitamin D on the mental health of 80 elderly patients and found those with the lowest levels of vitamin D were 11 times more prone to be depressed than those who received healthy doses.14 Low vitamin D levels are also associated with an increased risk of panic disorders.15 If you find your mind is running wild with what-ifs and worst-case scenarios, try to switch it around for the better. Teri Harbour, a stress management instructor at Frederick Community College near Washington, D.C., told news outlet WTOP, "We so often use our imagination to worry and to fear. Let's flip that around to use it to envision the best and to seek out the positive. We're going to feel better if we're doing that. We're going to have less stress; we're going to be fortified against the stress that's coming at us."16 She also recommends not only detaching from the situation if you find you're overly focused on the stressor, but also detaching from screens. "With the digital age, we are living a very fast-paced life," she says, "and I think stress affects everyone more today than ever before because things are so instant with technology. It can be very overwhelming and we sometimes don't even realize how stressful it is."17 Sources of Stress in America Are Changing Stress in America is nothing new, and the top stressors have long been money, work and the economy. In APA's 2017 Stress in America report, however, an increasing number of Americans cited stress not only related to the political climate but also to their personal safety.18 Thirty-four percent of Americans said their personal safety was a very or somewhat significant source of stress — the highest percentage since 2008. Fifty-nine percent regard acts of terrorism as a significant source of stress, as well. A survey of Americans' top fears conducted by Chapman University in 2016 also revealed that nearly one-quarter of Americans are very afraid of devastating natural disasters like hurricanes, earthquakes and floods.19 If you need immediate counseling to help you deal with the psychological effects of a hurricane (or any disaster situation) call the Disaster Distress Helpline 1-800-985-5990, which is run by SAMHSA and operates 24/7, 365 days a year. You can also text TalkWithUs to 66746 to connect with a crisis counselor. For more long-term help if you're having trouble moving past your anxiety and fear, or if you think you may have PTSD, professional counseling may be appropriate. Virtually everyone, however, can benefit from SAMHSA's tips for coping with a natural disaster, which include, as mentioned, taking care of yourself with a healthy diet, proper sleep and exercise, and avoiding the use of drugs and alcohol. In addition, put off making any major life decisions until after you've had time to recover from the disaster. They, too, recommend limiting your exposure to news and maintaining your regular routine, but do be gentle with yourself and allow time for recovery. "It is important that people try to accept whatever reactions they have related to the disaster," SAMHSA notes. "Take every day one at a time and focus on taking care of your own disaster-related needs and those of your family."20
0 notes
Link
This feature on statins and their adverse reactions was published in Dutch on January the 10th 2004, in AD Magazine, the weekend magazine of the newspaper Algemeen Dagblad. The article led to furious attacks on the author. In a primetime television show doctors and peer journalists accused him for deliberately spreading false, biased and potentially deadly information. He finally ended up in the Dutch Press Council, accused by a pharma-sponsored patient organization. The Council concluded: ‘Although the article is coloured, the author presented enough journalistic evidence to write such a piece’. The accusation was called unfounded. Despite this judgement and although the article elicited hundreds of reactions from readers (among them doctors) who reported severe side effects, the item has never been followed up.
Statins - Miracle drug or tragedy?
by Melchior Meijer
Statins, drugs that lower our ’bad’ cholesterol, are being prescribed like if it were aspirin. Not only in ‘crazy’ America, also in the Netherlands. This year we swallow for about 320 million Euro and the trend points up, not in the least place thanks to our rapidly aging population. The golden milk cow of the pharmaceutical industry is saving lifes. Claims the industry. Say also most doctors. But a growing group of concerned scientists starts sending out SOS signals. “Statins prevent a few heart attacks, but they also cause chronic heart failure,” says a cardiologist. A colleague: “I think people taking those drugs should be really, really alert.”
Are you on Lipitor? Congratulations! By taking Lipitor (…) you are on the right track to healthy cholesterol levels. On Pfizers Dutch website, those who just got a prescription for the popular cholesterol drug Lipitor are welcomed like the Long Lost Son. The message is cristal clear: do exactely as Pfizer says – which usually means taking the drug for the rest of your life – and the feared black limousine will pass your front door for decades to come. On the background fit and active babyboomers ride there bicycles and have a good time. Together we will beat the bloody cholesterol. Join the club!
Lipitor (atorvastatin) is just one of the excellent selling members of the family of HMG-CoA reductase inhibitors, most often called ‘statins’. In 1987, pharmaceutical giant Merck was first to launch this drug under the name Mevacor (lovastatine). Mevacor was nothing short of a revolution. Finally it was possible to normalize even very high levels of cholesterol. Popping just one pill a day did the trick. Gone were the days of the weird, inhumane diets, limiting the patients cuisine to cardboard bread and carrots. No more bitter powders, making you feel terribly sick. And what was even better: statines didn’t affect the ‘good’ HDL cholesterol.
Now, seventeen years later, all the big pharmaceutical companies market their own statin. Some are a bit more potent than others, but they all basically do the same thing. Millions of people all over the world are obediantly taking their daily Zocor, Lipitor, Lescol, Crestor, Pravachol and several no name clones. ”Statins are the new aspirin,” researcher Rory Collins recently proclaimed in the medical journal The Lancet, referring to the ‘terrific’ outcome of his Heart Protection Study.
This seven-year lasting trial among 20.000 Britons, partially paid by Merck, showed that statins offer everybody a slight protection from getting a heart attack. The eldery, the young, men, women, people with very high cholesterol levels and people with normal or even low levels. Our own expert on atherogenesis Prof. Dr. Anton Stalenhoef from Nijmegen University expressed himself a little subtler, but nevertheless welcomed the results as ‘tremendously positive’. He rather calls statins ‘the new penicillin’. It must be quite nice to be employed by companies like Merck, Astra-Zeneca, Novartis and Pfizer these days. It looks like their cholesterol lowering treatments à 1000 Euro per person and year will get unmatched sales within the coming years.
There are, however, physicians and scientists who watch the crusade of this lucrative miracle pill with Argus eyes. In prominent medical journals they warn against negative side effects of long time use. Their doubts are not exactly benign. Using statins could over time promote cancer, chronic heart failure and memory problems, they say; side effects that we don’t find in the information receipt.
A heart medicine causing heart failure? Early 2002, a group of Australian cardiologists appealed in The American Journal of Cardiology for an independent study into this supposed, paradoxical ‘side effect’. Chronic heart failure, a disabling disease in which the heart muscle slowly but steadily loses its ability to pump, is becoming more and more common in the western world. So common, that it can not be explained by the increasing age of the population and the growing number of people surviving an acute heart problem, according to the authors of the article. They add that ‘observant doctors all over the world suspect a role for the generously prescribed statins’.
This suspicion is of course not falling out of the bright blue sky. “Statins make victims – a lot of victims – and by now it’s pretty clear how they do it,” is the bold comment of cardiologist Dr. Peter Langsjoen from Tyler, Texas, USA. Langsjoen gave up an attractive career in a university hospital to dedicate his competence to what he calls ‘statin induced congestive heart failure’. Langsjoen: “Statins block the enzyme HMG CoA-reductase.
This enzyme is responsible for the production of a substance called ‘mevalonate’. Mevalonate on its turn is the precursor of both cholesterol and co-enzyme Q10. This Q10 – also called ubiquinone because it is involved in myriads of physiological processes – is essential for the function of the mitochondria, the energy plants in our cells. Someone using statins, not only deprives the body from cholesterol, but also from a great deal of the Q10 normally being produced. The higher the statin dose, the less of both essential factors will be available to the body. The cells most depending on Q10 are those from the nerve system, the skeletal muscles, but particularly those from the heart muscle. Heart muscle cells literally stuff themselves with Q10. If they don´t get enough, they’ll say goodnight sooner or later. That’s the moment the patient presents with symptoms of heart failure. Older statin users will develop dangerously low levels within 6 to 12 months. For younger people it might take several years before problems manifest.”
What are those symptoms? Mainly extreme tiredness and muscle and joint pain, according to Langsjoen. Later on, shortness of breath may follow. “I see 2 to 3 new cases of statin induced heart failure per week in my practice. The first things I do are to measure their Q10 levels and improve them with a supplement. By the way, in Japan supplementing Q10 is a routine intervention in patients with congestive heart failure. The treatment is well documented.”
Last year Langsjoen published own research in which he observed that two thirds of elder statin users show signs of ‘diastolic dysfunction’, one of the first signs of heart failure, after only six months of therapy. ”Physicians are prescribing these drugs with reckless abandon. We’re talking about extremely tricky stuff.”
In the summer of 2001 a striking amount of people ‘suddenly’ died of rhabdomyolysis, a ‘rare but very serious side effect of statin use’. All these people were on Baycol/Lipobay (cerivastatin), a statin that Bayer introduced three years earlier. When an aggressive strategy of denial didn’t work, the company saw no other way out than to take the pill that was meant to be their flagship from the market.
Was Baycol/Lipobay so much more dangerous than her sisters from the competitors? “It was a very potent statin,” explains Langsjoen. “But Pfizers’ Lipitor is only a little bit less potent and is thus only killing a little fewer people. A statin is a statin.” After the Baycol/Lipobay incident a group of scientists, lead by the Italian biochemist Gian Paolo Littarru, send a petition to the FDA and to the health authorities from the EU. From this petition: “It is possible that the reported statin related deaths are the top of an iceberg. (….) The extent of the observed statin induced Q10 deprivation should not be underestimated. There are indications that we doctors, with the best intentions, are creating a life-threatening situation in million of healthy patients. Conclusive research shows that supplementing this humble molecule could prevent tremendous suffering and costs.”
Would the pharmaceutical companies, with all the competence and technology they can buy, really not know what individual physicians ascertain with quite simple means? Do they possess unknown information, showing that those worried doctors got hold of the wrong end of the stick?
All too keen curiosity from outsiders is not appreciated in this business. An inquisitive person will not get real information, unless using illegal methods. But we may safely assume that the industry is aware of this hitch. Merck & Co Inc. deposited the patents US 4929437 respectively US 4933165 on the 29th of May and the 12th of June 1990, both stating: A pharmaceutical composition comprising a pharmaceutical carrier and an effective antihypercholerolemic amount of an HMG-CoA reductase inhibitor and an amount of Co-enzyme Q10 effective to couteract HMG-CoA reductase inhibitor-associated skeletal muscle myopathy.Merck claimed the exclusive rights to a combination drug of a statin and Q10. The vital combination was never realised. Apparently Merck didn’t want to make the combination drug, the competitors could not do it.
“We are at the beginning of the biggest medical tragedy that mankind ever witnessed,” cardiologist Langsjoen says. “Never before in history has the medical establishment knowingly created a life threatening nutrient deficiency in millions of otherwise healthy people, only to sit back with arrogance and horrific irresponsibility and watch to see what happens. I cannot help to view my once great profession with a mixture of sorrow and contempt.”
Why does the pharmaceutical industry keep a simple formula that might prevent a disaster and in the worst case does no harm, off the market? Within the relatively small group of independent physicians and scientists discussing this matter openly, one explanation prevails. “A combination pill has to go through all the clinical trials again,” speculates biochemist Christian Allan, former worker on the National Institutes of Health, in the discussion forum of The International Network of Cholesterol Skeptics (THINCS). “They would have to form four groups. One group gets a placebo, one group takes the combination drug, one group gets the plain statin, and one group gets only Q10. Now, smaller studies have shown clear cardiovascular benefits of Q10-supplementation. The trial might thus find that the people in the Q10-only arm do just as fine or even better than the groups taking the combination or the statins.
This must be a nightmare for the industry. They would invest a fortune, only to prove that a ‘useless’ supplement is as effective and above all a lot safer than their multi billion dollar designer drug.” And why would the industry take such a risk? The worried scientists observe a ‘huge professional ignorance’ in the field. A majority of physicians isn’t even aware of the fact that Q10 plays a crucial role in cellular energy production. Cardiologist Langsjoen: “They think it´s some kind of snake oil, in the same category as shark cartilage and apple vinegar.”
To make one thing perfectly clear, statins do offer some protection against our number one cause of death, myocardial infarction. This protection is independent of cholesterol reduction. People with low levels profit just as much as people with high levels, while those whose LDL-levels remain quite high are having the best prognosis.
Coincidentally statins possess strong anti-inflammatory properties and are able to stabilize the atherosclerotic plaques responsible for heart attacks. This does safe lives. But the drug companies really understand the business on the fair. Without lying, they paint a somewhat misleading picture; a matter of playing with numbers. A nice example is WOSCOPS, which examined the effect of pravastatin in healthy people with very high cholesterol levels. In The Netherlands, this group is almost automatically put on lifelong statin therapy. In his ads the manufacturer presents an impressive 25 percent risk reduction.
But what does this imply? Were there 25 more heart deaths in the group not taking the drug? Not at all. After five years 98.8 percent of the patients taking Pravachol were still alive. In the placebo group ‘only’ 98,4 percent was still alive and kicking. The relative risk reduction – the difference between 1.2 and 1.6 – is indeed 25 percent, a difference just being statistically significant. This modest effect is overshadowed by several studies showing a quite sinister cancer mortality in the treated groups.
Notorious is the so-called CARE trial. Twelve women in the statin group developed breast cancer, compared to only one in the control group. Another large study, the EXCEL project starring Merck’s lovastatine, was stopped after only eleven months, when the Mevacor group was producing 275 percent more deaths, mainly from cancer.
In animal models statin therapy almost invariably causes cancer and an untimely death, but according to the industry it is impossible to extrapolate such ‘hard endpoints’ to people. The same argument they use with regard to a Swiss study, recently published in Nature Medicine. It showed that Lipitor, Mevacor and Provachol effectively knock out the T-Helper cells, the Special Forces of the immune system. The authors find statins immunosupressive potency so impressive, that they see a role in transplantation patients. Great. For patients receiving a ‘new’ organ. But would a healthy baby boomer with a little high cholesterol happily accept a knocked down defence system? Some cancers love depressed immune systems. In 1996 scientists Newman and Hulley wrote in the Journal of the American Medical Association, regarding the cancer risk: ‘The experiments done to date suggest that statin treatment should be avoided, except in patients with a high and immediate risk of [a heart attack.]’
Dr. Jörgen Vesti-Nielsen, a physician from Karlshamn, Sweden, recently pointed out two possible mechanisms for the suggested cancer-promoting effect. In a discussion with colleagues he states: ‘In a low dose, statins stimulate angiogenesis, the formation of new blood vessels. Tumors need nutrients and thus blood for their growth. They depend on a widespread network of tiny vessels. Without the rapid formation of such a network, a tumour cannot even develop. Any substance stimulating the production of new vessels helps to start and spread cancer.
Moreover, a Finnish study suggests that statins make cells less sensitive to insulin. Who would still deny that insulin resistance is an important mechanism behind several cancer forms?’ Very high doses of statins seem to suppress angiogenesis. However, the vast majority of people with a moderate risk of cardiovascular problems are put on a lifelong low dose treatment.
To his great despair, former astronaut and retired NASA-physician Dr. Duane Graveline from Florida, lost all the memories of his adult life two times. Both times, it happened about five weeks after he was put on Lipitor. The staff in the emergency room told him he had suffered episodes of Transient Global Amnesia, a rare condition, not registered as a side effect of statin use. Graveline became extremely concerned, knowing that his problem could be a sign of a beginning dementia. Until he spoke to Dr. Beatrice A. Golomb, a neuroscientist looking for unknown side effects of statins. She made clear to him that he certainly is not the only statin user who all of a sudden fell into a ‘big black hole for a couple of hours’. Golomb, collecting data on behalf of the National Institutes of Health, will publish the results of an independent study in 2004. After a media announcement Golomb got hundreds of reactions from patients and doctors. She is convinced about a causative relation between the use of statins and TGA and other cognitive problems.
Are Graveline, Golomb and other doctors being haunted by imaginary terrors? In the data the manufacturers have to present if they want approval for a new drug, Transient Global Amnesia is not mentioned. Wouldn’t such a grave problem show up immediately? Biochemist and ‘debunker of fraud in medical science’ Joel M. Kaufmann from the University of Philadelphia (Prof. Emeritus) examined some reports and found a hardly flattering explanation. “Pharmaceutical companies sometimes split up one serious side effect into several minor side effects, in order to prevent their drug from not being approved,” he recently told the audience of a conference. “This is an established method to keep really alarming adverse effects below the 1 percent level.” Transient Global Amnesia can be split into such categories like confusion, memory weakness, senility, dementia and impaired cognitive function. One serious and rather common problem, simply falls apart in several relatively benign side effects. A smart trick that the authorities evidently not always unmask.
To swallow or not to swallow, that’s the question for almost 5 percent of our nation. Nefarma, the Organization for Dutch Pharmaceutical Companies participating in Scientific Research, asserts not to be aware of any prospective problems. When confronted with the alarming petition of biochemist Littarru and colleages, a spokesperson refers to the chief Communications and Public Relations. Why is Merck just ‘sitting’ on these patents for so long? Why doesn’t the industry inform physicians about the potentially harmful effect of blocking the Q10-synthesis? The ‘chief’ still owes an answer. During the weeks we tried to get in contact with her, she had constantly ‘just left the building’. No reaction, not even an e-mail back.
“If your doctor prescribes it, you can be sure the advantages far outweigh the risks,” says a spokesperson for the Dutch Association for Family Physicians. It depends which way around you look at it. Dr. Marshall E. Deutsch, an expert on cholesterol who studied the effect of low fat diets in children, puts it as follows: “The total mortality in the treated groups is – despite all the fuss – not less than in the groups not getting statins. Even in patients with very high cholesterol levels, the gains are meagre. Besides, the available data indicate that total mortality will rise disproportionally after seven years of treatment. If you absolutely don’t want to knock on Petrus’ gate with a heart attack – if you prefer to attend the final party with cancer, chronic heart failure, a stroke, a rope around your neck or whatever ailment – you’d better take statins. If you don’t care how you die, if the quality of your remaining years means more to you, then statins might be a bad idea. To jump out of a plane without a parachute offers excellent protection against cancer. But it has such a devastating effect on total mortality, that no sane doctor will use it as an intervention. I do hope the future will tell us that this comparison was misplaced. But it might not.”
#Statins#statin#controversy#big pharma#pharmacology#side effects#coq10#coenzyme q10#ubiquinol#ubiquinone
0 notes