#but i don't like. have an actual source of medical advice for this
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
I'm lowkey thinking about quitting my meds again but idk if it's just because I'm frustrated or if there's actual merit to the idea. Like I don't have clear enough evidence that their effectiveness has changed and the sensible thing to do would be still refill them so I have adequate time to decide and then wean off then but i AM frustrated enough to just want to say fuck it.
#i just don't feel like lying to the teledoc and saying they're working so he'll give me more#but i don't like. have an actual source of medical advice for this#like someone who is informed on both my prescription history and my mental health? haven't had that since college#when I've been back on meds the last few years it's just been like 'hey doc I'm depressed' and they say 'try taking lexapro'#the way gps talk about depression it's like they've vaguely heard of it before#they skimmed their textbook and guess on the exam#they're like uhh you get sad sometimes and can't sleep? here u go i guess#i need a mental health professional#wish they were real
0 notes
Text
I don't think there is a significant or notable number of people who believe transmascs are not oppressed.
I feel slightly insane just having to type this out, but this is rhetoric you inevitably come across if you discuss transfeminism on Tumblr.
The mainstream, cissexist understanding of transmasculine people is the Irreversible Damage narrative (one that's old enough to show up in Transsexual Empire as well) of transmascs as "misguided little girls", "tricked" into "mutilating themselves". It is a deliberately emasculating and transphobic narrative that very explicitly centers on oppression, even if the fevered imaginings misattribute the cause. As anyone who's dealt with the gatekeeping medical establishment knows, they are far from giving away HRT or even consults with both hands, and most transfems I know have a hard enough time convincing people to take DIY T advice, leave alone "tricking" anyone into top surgery.
Arguably, the misogyny that transmasculine folks experience is the defining narrative surrounding their existence, as transmasculinity is frequently and erroneously attributed to "tomboyish women" who resent their position in the patriarchy so much they seek to transition out of it. This rhetoric is an invisiblization of transmasculinity, constructed deliberately to preserve gendered verticality, for if it were possible to "gain status" under the sexed regime, its entire basis, its ideological naturalization, would fall apart.
Honestly, the actual discussions I see are centered around whether "transmisogyny" is a term that should apply to transmascs and transfems alike. While I understand the impetus for that discussion, I feel like the assertion that transmisogyny is a specific oppression that transfems experience for our perceived abandonment of the "male sex" is often conflated with the incorrect idea that we believe transmasculine people are not oppressed at all. This is not true, and we understand, rather acutely, that our society is entirely organized around reproductive exploitation. That is, in fact, the source of transfeminine disposability!
I know I'm someone who "just got here" and there is a history here that I'm not a part of, but so much of that history is speckled with hearsay and fabrication that I can't even attempt to make sense of it. All I know is that I, in 2024, have been called a revived medieval slur for effeminate men by people who attribute certain beliefs to me based on my being a trans woman who is also a feminist, and I simply do not hold those views, nor do I know anyone who sincerely does.
If you're going to attempt to discredit a transfeminist, or transfeminism in general, then please at least do us the courtesy of responding to things we actually say and have actually argued instead of ascribing to us phantom ideologies in a frankly conspiratorial fashion. I also implore people to pay attention to how transphobic rhetoric operates out in the wider world, how actual reactionaries talk about and think of trans people, instead of fixating so hard on internecine social media clique drama that one enters an alternate reality--a phantasm, as Judith Butler would put it.
Speaking of which--do y'all have any idea how overrepresented transmascs are in trans studies and queer theory? Can we like, stop and reckon with reality-as-it-is, instead of hallucinating a transfeminine hegemony where it doesn't exist? I'm aware a lot of their output isn't particularly explicative on the material realities of transmasculine oppression despite their prominence in the academy, but that is ... not the fault of trans women, who face extremely harsh epistemic injustice even in trans studies.
The actual issue is how invisiblized transmasculine oppression is and how the epistemicide that transmasculine people face manifests as a refusal to differentiate between the misogyny all women face, reproductive exploitation in particular, and the contours of violence, erasure, and oppression directed at specifically transmasculine people.
You will notice that is a society-wide problem, motivated by a desire to erase the possibilities of transmasculinity, to the point of not even being willing to name it. You will notice that I am quite familiar with how this works, and how it's completely compatible with a materialist transfeminist framework that analyzes how our oppression is--while distinct--interlinked and stems from the same root.
I sincerely hope that whoever needs to see this post sees it, and that something productive--more productive dialogue, at least--can arise from it.
#transfeminism#gender is a regime#materialist feminism#lesbian feminism#sex is a social construct#social constructionism#feminism#transmisogyny#anti transmasculinity#transphobia#erasure#epistemic injustice#epistemicide#queer theory#queer studies#queer academia
2K notes
·
View notes
Text
My dear lgbt+ kids,
It's difficult to write anything about the safety of Pride events without either greatly downplaying or exaggerating the potential risks of attending.
This is, at least partly, an online issue: the internet is international but there’s no international standard of safety for lgbt+ people. Someone reading this blog may be from a country where Pride events are generally safe and counterprotests are uncommon (or at least stay small and nonviolent) - but it'd be grossly negligent of me to pretend that this is true for everyone everywhere.
On top of those differences by country or location, there’s also individual safety concerns. Some things may pose a potential risk to certain groups or individuals while other people are unlikely to be negatively affected by them. This includes factors like crowds, loud music, exposure to alcohol or drugs etc. but also factors like the risk of being seen by someone who knows you or the risk of racist or antisemitic attacks etc.
All this is to say: I will happily share some general advice on safety with you – but if you’re trying to make a personal decision regarding the safety of attending Pride (regardless of whether that is “Is it safe for me to attend an event at all?” or just “How can I prepare for an event, so it’s as comfortable and fun as possible for me?”), don’t rely solely on me… or on any one voice you hear online. They may be in a totally different situation than you and inadvertently give you a totally wrong picture of it!
Tip Number One actually ties in with everything I said above: do you have friends (or other trusted people) who have attended Pride in your area before? If so, they may be a more reliable source of advice than a stranger online! Maybe you could even ask them to come along? Having an experienced Pride-goer with you is one of the best ways to ensure a safe and comfortable experience.
Other tips and pieces of advice that may be helpful:
Look the location up before you arrive: Which public transport stations are nearby? Where would you go if you need to buy a quick snack? Are there public toilets available? Where’s the nearest hospital or emergency room? Also note your surroundings when you arrive: Where are the exits? Are there any easily recognizable spots you could look for if you get lost? Where will you meet up with your friends or group if you accidentally get separated from them?
Make a plan beforehand and share it with at least one trusted person. Let them know where you are going, who you are going with, how you plan to get there and back home (public transit, your own car, your friend’s car etc.) and when you intend to be back home. Make sure to keep them updated on any changes in your plans and ask them to check in regularly. Also agree on what they should do if they haven’t heard from you at the agreed time.
If you go with a friend or a group, agree beforehand how you’ll handle potential scenarios: what if one person wants to go home and the other(s) want to stay? What if one of you gets separated from the other(s)? (Don’t rely solely on texting/calling each other in such cases (phones can unexpectedly die, get lost, get stolen, have no cell service etc.))
Pride events often take place in summer, so make sure to keep sun/heat safety in mind! Wear sunscreen, stay hydrated, don't overexhaust yourself in hot weather and read up on the symptoms of (and first aid for) heat exhaustion.
If you want to stay safe and alert, your best bet is to stay sober. Don’t drink alcohol or take drugs. (If you do plan to do either of these things, then please keep basic harm reduction measures in mind: don’t drink on an empty stomach, don’t mix alcohol and meds, have at least one person in your group who stays sober, don’t drink & drive etc.)
Make sure to take everything with you that you may need, such as a water bottle, snacks, any necessary medications, face masks, first aid supplies, a portable charger for your phone, emergency contact info (written down in case your phone dies), sunscreen etc.
Learn your rights when it comes to getting stopped by police (Make sure that what you read up on is actually true for your country and is up to date).
Read up on safety precautions for chemical irritation if the use of pepper spray/tear gas is a concern in your area. Same goes for active shooter situations. It may be a worst case scenario but it’s better to read up beforehand if it’s something you worry about.
Don’t engage with counterprotesters. Even if they seem nonviolent, keep in mind that they may just be waiting for you to provoke them, so they can “justify” escalating to violence. Just keep your distance, don’t talk to them, don’t let them bait you into conversation.
Lastly, you want to keep everyone else safe too, so: make sure you don’t accidentally out anyone. Pride is supposed to be a safe space. Don’t take pictures of strangers, don’t upload anything on social media that shows anyone’s face or name if you didn’t get explicit permission to do so.
With all my love,
Your Tumblr Dad
239 notes
·
View notes
Text
It's Hurricane Season so I'd like to share some advice as a life-long Floridian who's experienced a few things. This is going to be directed primarily to people living in areas at risk of blackouts which could last several days.
Preparations
Aside from food, water, and gas, some things you'll want to make sure you have are flashlights and batteries. Make sure to refill any medications you might need.
From @dea-certe: Fill up all vehicles and maybe a few gas containers now. Firstly because it will be more expensive in the storm aftermath, but also because it will be harder to find. I went to five different gas stations to find fuel at one point and was kicking myself because I had used so much has keeping the phones charged and keeping the heat going.
Get raincoats in case you need to go outside cause the wind will destroy any umbrellas.. If you can't get one, take a garbage bag and tear a face hole into it and use that.
Also, get bug repellent, especially mosquito repellent. Mosquitos breed around still water and there will be a lot of still water.
And if you have an infant, make sure to stock up on diapers, baby wipes, etc. Even if you don't have an infant, baby wipes can be useful to help keep yourself clean.
You might want to buy some gardening gloves as well to make the post-storm cleanup safer.
SUPER IMPORTANT FOR SANITY AND SANITATION: get caught up on laundry and dishes. No power means no running water. Don't make things worse by not having clean dishes or clean clothes to use. While you're cleaning, change your bed sheets as well. Once you have power, change your sheets again.
Also, download any games, ebooks, shows, etc you can onto any battery-charged electronic devices you have. It will help your sanity when all you can do is wait.
From @metadata-uber-alles: My recommendation re: radio is to make sure you have an actual AM/FM radio, one that can run on batteries. You can probably thrift it if you don't have one already. Most radio stations stream online too, but if the power goes out you'll be rationing your phone battery and may not have internet.
Finally, while you should ideally board up your windows to protect them from debris, make sure at the minimum that all your windows are closed. Wind pressures are going to suck air out of any openings in your home.
Food and Water
First and most important: DO NOT BE A HOARDER!!
Even if your home has no power, that doesn't mean your local grocery store has no power. You can expect some reduced supply due to damaged supply lines and a spike in demand, but you shouldn't be worrying about empty shelves. At worst, have the amount of supplies you might need for 10 days. If you normally go to the grocery store every 2 weeks or longer, just stock up the amount you normally would.
Buy more items that are less likely to spoil and don't need refrigeration. When you have no power, prioritize eating anything which requires refrigeration (milk, cheese, meats) or has a short shelf life (bread).
Demand will be higher in preparation, and supply will be diminished for a bit, but supply issues only become unbearable when people start hoarding.
As for water, you'll need a surplus since you need water for so much. I cannot stress this particular part enough:
You need water to flush your toilet.
If there's somewhere with running water you can go when you need to poop, use that whenever possible, but you need water available at home to refill your toilet's cistern if you don't have that option (either time, distance, etc).
Make sure you have a supply of drinking water. Don't go buying every water bottle you can find (See the bit about hoarding), but you should buy more than you might normally use. Instead, gather water through things like your sink or from a hose into any sealable containers you might have . If you have a bathtub, fill it up just before the hurricane. If you have a pool, that's another source of water. If no debris got in the pool, you can use it for bathing. If you have empty buckets, you can get some additional water during the hurricane by filling them with large rocks or bricks and leaving them out in the open to collect the rain water.
Different water sources will be used for different purposes:
bottled, canned, or other store-bought water: Drinking, cooking, and refrigeration (explained later)
Water in unsealed containers: refill the toilet cistern
Water in a sealed containers: bathing and cleaning (Can also be used for the toilet)
As mentioned with food, supplies at your grocer will be reduced but not necessarily empty. You should be able to buy enough additional drinking water and be able to also use it for cleaning, giving you more water for the toilet. The tip about gathering rain water will only work once. There will likely be no rain for at least a week afterward.
In case you need to evacuate
Keep tabs on whatever emergency alerts are available. Check what your local radio channel is or what sites to check online. Make sure you know how to get to your local shelter, including alternate paths in case a road is inaccessible.
Load your vehicle with anything you might need to bring with you before the storm so you don't have to spend time looking for them and double checking when every minute could count. Pack some pillows, blankets, and extra clothes just in case. Also include anything you cannot risk losing for school or work like laptops.
Refrigeration
Without power, your fridge is now just a giant cooler and a ticking bomb to being a biohazard. Fill it up as much as possible. Cold air escapes easily when you open it and heat disperses fastest throw the air. Remember how I said you should buy extra water? A fridge filled with cold water will stay cooler longer. Any liquid will do. Fill your fridge with water bottles, soda cans, beer, fruit juice, whatever. As long as it doesn't spoil at room temperature. Milk can technically help too, but since it spoils you shouldn't keep much of it and should use it quickly.
Additional things like fruits and veggies will also help. What matters is you want to reduce the amount of empty space and fill it with anything which can keep the temperature down. Put a frozen block of iron in for all I care. Just don't have a super empty fridge.
If you have a generator
Good for you. You're not completely without power now. But you need to set priorities on what to use it for. Generators can only supply so much power at a time so you can't just hook everything to it and expect things to work out.
Top priority is the fridge. Twice a day, morning and evening, plug the fridge to the generator and let it run for two hours to cool things down. Don't hook up the fridge when you don't expect to open it (like when everyone is asleep).
Second priority should be charging cell phones, laptops, and anything else like that. Depending on your circumstances, you can charge them at work, from your car, etc so only hook them up when batteries are low.
Third, comfort. I understand this will be stressful, but hooking up your tv and gaming computer isn't the best idea. If you've done what I suggested earlier, you'll at least have something to watch or do without needing to hook it to your generator. Like with the above electronics, you might be able to find other ways to charge them, but only attach them to your generator when you don't need to worry about necessities.
Finally for the love of god, DO NOT HOOK AN AC TO THE GENERATOR!!. Air conditioners draw a lot of power, especially once the room is hot. But your generator can only do so much. The AC will kill your power supply really quickly. Use a fan or the AC in your vehicle if you need to cool down.
Also worth noting, if you have an electric vehicle, that could potentially be used as well. I don't know specifics, but look into that if you own one.
Final notes
This is not comprehensive and I may be wrong about some things.
Please refer to actual expert sources for comprehensive help.
This is just suggestions from someone who has to deal with this every year and has figured out how to deal with the aftermath. Your living conditions may be different so please check how to handle any concerns unique to you.
Stay safe and do not give up hope.
1K notes
·
View notes
Note
Hi Sam, could you please recommend any resources/websites to learn about ADHD medication? Until reading your post about second-line meds I thought Adderal was the only one
I can definitely talk about it a little! Always bearing in mind that I am not a doctor and this is not medical advice, etc. etc.
So, I've had many friends with ADHD in my life before I got my diagnosis and I picked up some stuff from them even before getting diagnosed; I also spoke with my prescribing psychiatrist about options when we met. If you think your psychiatrist might be resistant to discussing options, or you don't have one, doing your own research is good, but it's not really a substitute for a specialist in medication management. So it's also important to know what your needs are -- ie, "I want help with my executive function but I need something that's nonaddictive" or "I want something nonsedative" or "I don't think the treatment I'm on is working, what is available outside of this kind of medication?"
The problems you run into with researching medication for ADHD are threefold:
Most well-informed sources aren't actually geared towards non-doctor adults who just want to know what their options are -- they're usually either doctors who don't know how to talk about medication to non-doctors, or doctors (and parents) talking to parents about pediatric options.
A huge number of sites when you google are either AI-generated, covert ads for stimulant addiction rehab, or both.
Reliable sites with easy-to-understand information are not updated super often.
So you just kind of have to be really alert and read the "page" itself for context clues -- is it a science journal, is it an organization that helps people with ADHD, is it a doctor, is it a rehab clinic, is it a drug advertiser, is it a random site with a weird URL that's probably AI generated, etc.
So for example, ADDitude Magazine, which is kind of the pre-eminent clearinghouse for non-scholarly information on ADHD, is a great place to start, but when the research is clearly outlined it sometimes isn't up-to-date, and when it's up-to-date it's often a little impenetrable. They have an extensive library of podcast/webinars, and I started this particular research with this one, but his slides aren't super well-organized, he flips back and forth between chemical and brand name, and he doesn't always designate which is which. However, he does have a couple of slides that list off a bunch of medications, so I just put those into a spreadsheet, gleaned what I could from him, and then searched each medication. I did find a pretty good chart at WebMD that at least gives you the types and brand names fairly visibly. (Fwiw with the webinar, I definitely spent more time skimming the transcript than listening to him, auto transcription isn't GOOD but it is helpful in speeding through stuff like that.)
I think, functionally, there are four types of meds for ADHD, and the more popular ones often have several variations. Sometimes this is just for dosage purposes -- like, if you have trouble swallowing pills there are some meds that come in liquids or patches, so it's useful to learn the chemical name rather than the brand name, because then you can identify several "brands" that all use the same chemical and start to differentiate between them.
Top of the list you have your methylphenidate and your amphetamine, those are the two types of stimulant medications; the most well known brand names for these are Ritalin (methylphenidate) and Adderall (amphetamine).
Then there's the nonstimulant medications, SNRIs (Strattera, for example) and Alpha-2 Agonists (guanfacine and clonidine, brand names Kapvay and Intuniv; I'm looking at these for a second-line medication). There's some crossover between these and the next category:
Antidepressants are sometimes helpful with ADHD symptoms as well as being helpful for depression; I haven't looked at these much because for me they feel like the nuclear option, but it's Dopamine reuptake inhibitors like Wellbutrin and tricyclics like Tofranil. If you're researching these you don't need to look at like, every antidepressant ever, just look for ones that are specifically mentioned in context with ADHD.
Lastly there are what I call the Offlabels -- medications that we understand to have an impact on ADHD for some people, but which aren't generally prescribed very often, and sometimes aren't approved for use. I don't know much about these, either, because they tend to be for complex cases that don't respond to the usual scrips and are particularly difficult to research. The one I have in my notes is memantine (brand name Namenda) which is primarily a dementia medication that has shown to be particularly helpful for social cognition in people with combined Autism/ADHD.
So yeah -- hopefully that's a start for you, but as with everything online, don't take my word for it -- I'm also a lay person and may get stuff wrong, so this is just what I've found and kept in my notes. Your best bet truly is to find a psychiatrist specializing in ADHD medication management and discuss your options with them. Good luck!
136 notes
·
View notes
Text
Tips for freshly diagnosed celiac-havers
Someone I knew asked me for advice after getting diagnosed with celiac. I gave her some. I might as well share them with you as well!
I am not a doctor, and not your doctor, I'm just some guy with celiac disease. Ask an actual doctor for help with medical decisions. I'm in the northeastern United States, so you might have to go hunting for equivalent resources if you live elsewhere.
Are you done with testing?
If you had a tTG-IgA blood test with an elevated result, or a doctor just told you you have celiac, but you have not gotten a biopsy via endoscopy to confirm your diagnosis, WAIT! You may not want to stop eating gluten quite yet. You have to be eating gluten for the biopsy test to work.
It is not fun to stop eating gluten, start feeling better, and then have to start eating it again just to prove that you really have celiac disease.
Your choice in this area is personal. If you know you're going to have to wait years to get an endoscopy, it would probably be healthier and more pleasant to stop eating gluten now and then do a "gluten challenge" for a few weeks before your endoscopy.
If it's unlikely you will ever get an endoscopy (too expensive, inaccessible, phobia, etc), there's no point in waiting for something that may never come -- just stop eating gluten now.
But if you can schedule an endoscopy for a month or two from now, it's probably best to keep eating gluten until the endoscopy. Sorry.
Please eat food. Like, enough food.
The most important tip I got early in my diagnosis is that if you stop eating gluten and you start feeling crummy -- dizzy, cranky, tired, etc -- it's not because you're going through "gluten detox" or some shit. It's because you're hungry!
It's easy to accidentally start eating way less when you start eating gluten free. A celiac diagnosis can make you want to avoid eating because food feels scary and stressful. Cutting a major ingredient from your diet without knowing what to replace it with can also leave you undernourished.
You really need nourishment when you are recovering from celiac! Your body need energy from food to use on healing your intestines. If you've lived with celiac for a long time, you probably have vitamin deficiencies you're trying to bounce back from. The emotional difficulty of adjusting to a new diagnosis is also much easier to face if you're not starving.
All of this advice applies equally regardless of body size. Yes, even if you are very fat. If you're hungry, eat.
Where to find information about gluten-free food
The gold standard for basic celiac info is celiac nonprofits. There's a ton of info about celiac disease and the gluten free diet on their websites. I recommend:
Celiac Disease Foundation
Beyond Celiac
You know what's not a legitimate celiac nonprofit? Gluten Free Society. Do not listen to anything GFS or its founder Peter Osborne have to say. Osborne is not an actual doctor, nor is he doing actual nutrition science. He is a chiropractor (i.e. quack) so bad that his state's board of chiropractors threatened to revoke his license. Don't let anyone tell you celiac means you can't have corn!!! Truly, wtf @ this guy.
Google's AI summaries for searches like "Is XYZ food gluten free" are often inaccurate (because they pick up sites like GFS). I always click through to the source to be sure. "Is XYZ food celiac safe" sometimes gives more useful search results.
I also like this presentation "I Have Celiac" for a super in-depth guide to having and living with celiac. The OP made it to show to loved ones to explain their deal, but it's so thorough that I found it helpful for myself when I got my diagnosis.
I want to buy food that's safe for celiac...how do I do that?
You should be able to find gf food at any supermarket. The selection of baked goods and processed foods may be lacking, depending on where you live, but produce, raw unmarinated cuts of meat, and other whole foods like milk and eggs are generally safe even if not labeled gf.
A lot of supermarkets have an indicator on the price labels to help you -- for example, at Stop and Shop, the labels on the shelf have an orange circle that says "gf" in it under foods that are gluten free. It's best to check the packaging too, since Stop and Shop sometimes gets it wrong!
Something that says "gluten free" or "certified gluten free" on it is safe for celiac*. Something that doesn't say "gluten free" on the packaging may also be safe, so long as it also doesn't contain wheat, barley, or rye, or have a wheat allergy warning under the ingredient list. Here are some tips for what to look for on ingredient labels.
Labels can get real complicated real fast, so just use your best judgment. It's okay if you don't get it right 100% of the time. The goal when living with celiac is to reduce gluten exposure as much as possible, not to hermetically seal yourself in a deep well where a single molecule of gluten can never possibly reach your tongue. You, and only you, get to decide how much exposure risk you're comfortable with.
My favorite grocery store post-diagnosis is Wegmans. My nearest one is a bit of a hike, so I don't go that often, but it's such a treat when I do. Wegmans has a huge gluten free aisle with gf staples and fun snacks, plus lots of food items that can be harder to find gf, like fresh pasta and baked goods.
I also like the online health food store iHerb for finding new gf snacks and ingredients. You can filter the whole store by dietary needs, so you can also find gf skincare/makeup items and supplements if you want. I have a discount link for 20% off: https://secure.iherb.com/rewards/rewards-program?rcode=DRO2876
The best way to find restaurants that can accommodate celiac is Find Me Gluten Free. It's essentially a gluten-free Yelp. People use the site/app to review of restaurants for 1) what cross-contact precautions the restaurant takes and 2) crucially, if the food was good!
Gf food can be expensive, ngl. The National Celiac Association has advice for how to save money on gf food, including a database of food pantries that set aside gf food for people who need it.
GF ~influencers~
If you want to follow some people who Get It, I like:
Phil Hates Gluten (on IG, TT, and YT) has EoE (another gluten-related autoimmune condition). He reviews gf food and restaurants and makes silly videos about the gf experience.
Robyn's Gluten-free Living on YouTube has gf baking videos and advice about traveling, eating at restaurants, saving money on gf food, and more.
Here on Tumblr, @gluttonysansgluten and @certifiedceliac (and I would love more recommendations for celiac related Tumblr accounts!)
Having celiac is really hard. But it does get easier.
I felt overwhelmed and honestly kind of doomed when I got my celiac diagnosis. For the first few months I felt like I couldn't trust any food and I was going to be totally excluded at all social events forever. It sucked. But then I got a lot of practice figuring out which foods were safe for me, advocating for myself at restaurants and when my friends were planning get-togethers involving food, and now things are really not that bad. And I feel way, way less sick.
If you feel overwhelmed or don't know how to interpret the 1 million sources online telling you what's gluten free, I really recommend seeing a dietician. Your best bet is a weight-neutral or HAES dietician who mentions celiac somewhere on their website or online profile. You can generally count on those folks to give you practical information about how to live with celiac, as well as emotional support as you adjust to what is probably a pretty big and stressful change in your life and how you view yourself!
You got this!
*Please do not talk about Cheerios on my post. Make your own.
59 notes
·
View notes
Text
BEWARE OF "body mod advices" - they can be dangerous and LETHAL.
(this post was about a deactivated blog but extends to any possible future blog like it)
edit3 since he deactivated: Red told me in the DMs that he WILL be more careful about all this risk stuff, I believe he is going to do better. Im sure he's a good person and he also was extremely civil in the DMs. Since he's not here to defend himself anymore I'll gladly take his side and say that despite this mess, all Red wanted to do was indeed reduce harm and potentially save lives. Good luck on all your endeavors, Red, I wish you a beautiful and successful career and that you have a great positive impact in the atypical dysphoria community, both on and offline. I don't know how my post truly impacted you, I'm so sorry if you're feeling bad. You acted the best way you possibly could.
Second, if Red comes back, DO NOT HARASS HIM, let him be himself and don't let his past hold them down.
Third, all my points still stand for their deactivated blog and any potential body mod tips blogs in the future. Please everyone, take care, stay safe.
Past edit: DONT HARASS any possible blogs like hers, just REPORT and spread awareness, (also don't make the same mistakes as me: TALK TO THEM FIRST)
Past edit: minors please interact with this post, forget my bio for this one
Past edit: editing editing the post since I talked to Red and he isn't bait. I definitely should have talked to them in DMs first. I sincerely apologize. So sorry Red! To those reading, don't make the same mistake as me, ok? Always talk to people privately first, I genuinely fucked up bad. This mistake of assuming others intentions, can traumatize them. If I were in Red's shoes I'd be traumatized. So yeah, I fucked up bad.
Their intentions are genuine but my point still stands that its extremely dangerous and can't qualify as harm-reduction / end edit note
alright, I'm not transid/radqueer but you guys need to REPORT AND WARN OTHERS of these accounts as soon as they appear. Do not entertain them, no matter how desperate you are to transition. You can become a victim of dangerous charlatanism.
LONG POST AHEAD, VERY IMPORTANT NEVERTHELESS
Archive to what i'm about to post
Red claimed to be "a non-professional surgeon, planning on getting better with practice." Bad move!
Red has told me he's pursuing a medical degree and won't actually do non-qualified surgery.
.
Red: "The blog is centered around an idea of "extreme" body mods that I would like to explore further, [...] things like breaking and re-mending bones, creating new joints, replacing skin, etc."
My point: the road to hell is paved with good intentions, and your blog was unsafe.
.
To any possible counterarguments: "But they (people following/asking advice) know the risks!" That's victim-blaming. Red gave himself the responsibility to give harm-reducing advice, but he didn't do a good job.
"But I know the risks!" You can't possibly know the risks because Red doesn't know either or "kinda knows" but has not properly informed his audience, it didnt give sources, oversimplified their advice and failed to provide accurate information about risk. Or gave plain misinformation.
Again I'm not transid, I can't possibly imagine what you're going through in order to try anything at all to feel better, including trying experimental surgery not legally available or not researched at all. However, please please please do not become a victim of medical deceit or whatever tf it's called. Even if the blog owner tries their best to be reliable.
They might sound confident, but they do not know what they are saying, what they're telling others to do.
.
Ask: "How would I make my skin gray without tattoos?" (DO NOT SHAME THIS USER BTW)
Red: "[...] I assume you want permanent grey. To do this, it's pretty simple, although it'll take a lot of time. Basically, what you want to do is to constantly be exposed to lots of silver. Any product with silver in it like specific lotions and skin creams. also fish, milk, mushrooms, and whole grains tend to have silver in them! So tldr, consume lots of silver!"
STOP!!! DONT FOLLOW THIS ADVICE!!! DONT OVER-EXPOSE YOURSELF TO SILVER!!! "Silver toxicity causes argyria. Silver toxicity occurs when too much silver is in your body." <- from a simple research on "too much silver in blood"
THE RESULT WILL BE ARGYRIA. EVEN IF YOU DO IT SLOWLY, YOU ARE BUILDING UP A HEAVY METAL IN YOUR BODY. THE GREY SKIN IS NOT PRETTY NOR WITHOUT GRUESOME SIDE SYMPTOMS.
Yall. Anything in excess will fuck up your body, including iron, vitamins, and silver.
To whoever asked Red, I don't know your mind, but I'm sure you'd love to live a happy life with grey skin! You'd love to have a body you're comfortable with and looks rad as hell! But you wouldn't be able to enjoy it if you're deeply sick with ARGYRIA, WHICH IS WHAT RED'S ADVICE WILL GIVE YOU!
.
Ask: "How do I get darker skin without going too dark? I’m pale and burn easily, I just want a color similar to Lin Manuel Miranda" (AGAIN DONT HARASS THIS USER)
Red: [...] "expose yourself to the sun more! As you do this, you'll get tan which will protect you from future burns and make your skin slightly darker, do this enough and you can engineer your skin to be as dark as you want!"
THATS MISINFORMATION! Yes you may tan to get darker (Lin's tone may or may not be achievable to you) but one: it's not permanent unless you're constantly going out; two: SKIN CANCER!!!! DONT OVER-EXPOSE YOURSELF TO THE SUN!!!! USE SUNSCREEN!!
TO ANYONE SEEKING A MUCH DARKER TONE: YOU CAN'T "GO AS DARK AS YOU WANT TO" BY TANNING. Just look at people who have lived their whole lives outdoors like farmers! White people can't tan to black! There's a limit to how tan you may get! Are you seriously gonna risk skin cancer for an impossible thing???
.
Red: "Self amputation is really dangerous! You should learn how to use a tourniquet, that way, you can stop the bleeding! [...]" WHERE ARE YOU GETTING YOUR SOURCES, RED?
If anyone reading this is seriously thinking of amputating themselves, and will not change their minds no matter what, please just have someone immediately drive you to the hospital. I do not support such operation and you can still die or get horribly sick even with your best precautions, but you better receive actual medical attention and stay alive rather than trying to heal it yourself. Because what you'll most likely get from following Red's advice is DEATH FROM BLOOD LOSS. Again, if you absolutely cannot get rid of this dysphoria with therapy, or manage it at least, or have a doctor do it for you, I still would NEVER suggest you do it yourself, but IF you end up doing that then at least please go straight to the hospital instead of trying to heal it yourself.
.
Red: "do not try and break your own bones to make modifications! [...] Get another person (Like myself) to help you with the bone breakage instead."
NO ONE KNOWS WTF THEY'RE DOING. YOUR FRIEND DOESN'T. RED DOESN'T (as they advertised in the post). NO ONE IS GOING TO GET MODIFICATIONS LIKE THIS. NO ONE IS GOING TO BE HAPPY. EVERYONE IS GOING TO BE EITHER IN PAIN, RISK OF HORRIBLE INJURIES OR TROUBLE WITH THE LAW. FUCKING AROUND = GUARANTEED BOTCHED OPERATION.
Also, now that Red has clarified she won't perform surgery until having an actual degree, you can't really go to her XD
.
Red: "Some advice for surgery [...] This one's important, make sure your patient is strapped down and properly sedated, if they move, even slightly, you risk hitting a vital artery or organ, if you do hit an artery, don't panic, this is why you learned how to use a tourniquet! if you hit a vital organ though, odds are you won't know how to fix that, so be extra careful with abdomen and face surgery!"
Thats still promoting medical malpractice, mutilating and potentially killing friends, dangerously downplaying surgery so much, this is not harm-reduction
.
Ask: "I want to be blind in one eye, but more-so in the sense of extreme but not total vision loss. I want to do something permanent in the future!" (AGAIN DONT HARASS THIS USER)
Red: Well, a simple fix to your problem is just get some calcium hydroxide in your eye and wash it out a few minutes later, this should lead to permanent, extreme (but not total) vision loss in that eye. Keep it in too long and it can cause total vision loss so be careful!
Ok so, it's great that you're trying to come up with alternative ways for users not to kill themselves by gouging their eyes out, but you've still failed to give them the full picture
From a quick search "calcium hydroxide in the eyes": Exposure to the skin can produce burns, painful irritation and necrosis, and exposure to the eyes may cause severe pain and vision loss that can be temporary or permanent. If calcium hydroxide is exposed to the skin, contaminated clothing should be removed, excess amounts of the chemical should be wiped off and the affected skin should be flushed repeatedly with water. Victims of calcium hydroxide exposure to the eyes should flush their eyes with water continuously for the first 15 minutes, but all cases of external exposure should receive immediate medical care. Inhaling calcium hydroxide through the nose or mouth can also cause immediate, painful and potentially life-threatening complications. Throat and nasal passages may become painful and swollen, and the swelling may restrict airways, making breathing difficult or impossible. If the calcium hydroxide particles are carried all the way to the lungs, this may further complicate breathing. Victims of this type of exposure should be taken immediately to a fresh air environment, and emergency services should be contacted right away. Administration of oxygen and emergency respiratory assistance may be required.
.
Red (answering an ask): "the question shouldn't be what DO people replace their skin with, it should be what CAN they, after all, just because it's never been practiced or very rarely practiced doesn't mean it's bad or impossible! Of course, my personal favorite skin substitutes are rubber and red velvet, I am also a big fan of stainless steel."
(Don't promote such an operation). THIS OPERATION IS BAD AND IMPOSSIBLE TO SUCCEED. SKIN CAN ONLY BE REPLACED WITH SKIN. SKIN IS A LIVING ORGAN. ANY OTHER SUBSTITUTE WILL CAUSE YOU TO LOSE BODY PARTS OR DIE.
YOU KNOW HOW PEOPLE WITH TRANSPLANTS NEED LIFE-LONG MEDICAL ATTENTION SO THEIR BODY DOESN'T REJECT IT? HOW TF WILL YOU DO THIS WITH FUCKING RED VELVET?
YOU WILL FUCK UP YOUR BODY'S IMMUNE SYSTEM A THOUSAND DIFFERENT WAYS.
ANYWAYS. CROSSTAGGING FOR REACH. PLEASE EVERYONE REBLOG. THIS IS SERIOUS SHIT.
#radqueer#rq community#rq 🌈🍓#pro rq 🌈🍓#pro radqueer#transid#transid please interact#transid safe#transabled#transharmful#pro transharmed#pro transid#pro transx#pro transage#pro transabled#radqueer coining#radqueer safe#radqueer please interact#pro radq#rq safe#pro para#pro rq#transid community#transx safe#transid coining#diaracial#pro diarace
81 notes
·
View notes
Text
Disability 101: The language of Disability

Trigger Warning: this post contains discussions of disability slurs (specifically the C and R slurs), and the history of disabled people's use in medical experimentation, including specific (but brief) examples.
Most of the content on my blog is aimed specifically at authors, artists and other creatives, but I've been noticing for a while now, that many of the people who come here to learn about writing and designing better and more compassionate disabled representation are often missing what I would consider to be pretty fundamental knowledge of the disabled community, or have gotten said information from a questionable source, for example, through corporate sensitivity training, who's given them just straight-up incorrect information. This isn't surprising, nor is it really the fault of the people seeking to learn more, rather, it's because of the way society at large talks about (or I suppose, doesn't talk about) disability. However this lack of foundational understanding often leads to creators accidentally including harmful tropes, using damaging or unnecessarily coded language or just including misinformation about our community into their works, often in ways that are quite hard to change by the time they realise there's an issue.
But before we continue:
The disability community is massive and we have a lot of history most people are totally unaware of which influences a lot of these fundamentals. It doesn't help that there are a lot of "allies" to our community who completely ignore and speak over us, many of whom have bigger platforms that actual disabled people, so their advice is seen and shared by more people, muddying the waters even further and making it difficult to discern what is and isn't "good information". Because of that, I understand that it can be hard to know where to start, so while most of my content is dedicated to specifically talking about disability representation in media, and how creators can include better representation in their own works, I also want to take some time to talk about some of the fundamental information about the disabled community I feel everyone (creator or not) should know.
Today I'm going to start on what I think trips people up the most when they're first trying to learn: The language surrounding disability. What terms we (generally) prefer, what terms to avoid, all that. I don't think this is necessarily the most important thing to know right off the bat, but it is probably one of the topics non-disabled people are the most confidently incorrect about, and where general misinformation is the most rampant.
Disclaimer: Before we go ahead, it's important to remember that the disabled community is not a monolith, especially so when we are talking about something like language and preferred terms. This post is designed to be a starting off point, not a rigid set of rules or all-encompassing guide. Different individuals may prefer different terms, possibly even ones listed in this article as words to avoid. Articles like this should always be taken as a general guideline but you should always be respectful of an individual's preference and refer to them how they have asked you to refer to them, even if it goes against general advice you've been given. However, it's important to bear in mind that just because that individual has a preference for a less popular term or even a term others find offensive, doesn't mean every disabled person is ok with it. It's also important to consider that different communities, cultures and countries, as well as people who speak different languages or even dialects of the same language, will have different general preferences, and so it is crucial to do further research on your own.
Disability and disabled are not dirty Words, it's ok to say it
If you grew up in the 1990's or later, like I did, you very likely heard words like "special needs," "differently-abled," "Special education" (often shortened to SPED). There's a very good chance that if you worked in education, healthcare (especially for children), with some disability charities or even if you were the parent of a disabled kid during this time, you were likely told to use these terms as a replacement for words like disabled, because "disability" and specific terms like "autism," "amputee," "downs syndrome," "paraplegic," etc put the focus on the things the person doesn't have or can't do. Calling them "disabled" implies there is something wrong with them, whereas these alternatives put a focus on the idea that folks with these conditions are "different, not less". At least, that's what a lot of people are told.
This is what we call coded language, and it's an issue because a lot of disabled people despise it. There are exceptions, of course, I know a few people who are indifferent, but I honestly can't recall anyone who was disabled themselves who preferred it outside of very young children who's parents insisted it was better (though most chose to move away from it as they got older).
But why? well, because of something that I'm sure you'll notice is going to be a pattern throughout this post: we didn't create these terms, and they weren't made for us, not really.
Most disabled people don't really see using the term "disabled" or any of the modern diagnostic terms (for the most part) as an issue. Yes, many do, by definition, focus on things we don't have, can't do or might struggle with; the definition of an amputee is someone who is missing a limb, the definition of paraplegia is someone who has paralysis in their lower body and legs, meaning they might not be able to or might struggle to move them. The definition of a disability is a little more complex and varies from country to country, but the American CDC defines it as "Any condition of the body or mind that makes it more difficult for the person with the condition to do certain activities and interact with the world around them."
These definitions sound negative, but it's not a bad thing to acknowledge someone doesn't have something most other people possess, or struggles with things others don't. It doesn't make someone "less" to acknowledge they have a barrier others don't. It's just acknowledging a part of our lived experience and acknowledging that our lives, because of these barriers, can sometimes look different, in both big and small ways.
However, a lot of people who are not used to being around disabled people get deeply uncomfortable with this, and this refusal to use straight-forward words like disabled is a symptom of that. This discomfort comes, in my experience, from a lack of understanding of disability as a whole, and potentially misplaced sympathy. They don't know how we do things they see as important, how we could do without the things they have, or what technology or services is available to help us bridge those gaps. This unknown makes a lot of non-disabled people scared, uncomfortable or makes them sad for us, even when it's not necessary. They see that we can't do something they can, like move our legs for example, and make a series of assumptions based on incomplete information. They imagine a life like ours and don't know how it could possibly be fulfilling, because they are missing so many vitally important pieces of information, making our lives look empty, bland and sad.
They don't have the full picture, but ironically, this discomfort stops them from learning more. If you go into a topic like this, assuming it will be depressing and bleak, why would you want to double check? For many, the fact that it doesn't take much for them to become disabled too adds to that feeling of discomfort and fear, so they turn away and try to pretend we're just "different" and insist on replacing the "scary" words that acknowledge the challenges and barriers they too will have to face if they become like us with things that comfort themselves, not us.
All of this is especially important to remember in the cases of disabled people who are severely limited by their disabilities (whether it be due to the disability itself, or the lack of accommodations for it) and who's disabilities do have negative impacts on their lives. It's important to acknowledge that for some of us, the negative stigma around our disabilities is mostly misinformation and an incomplete picture, like I mentioned before, that altering how something is done or approaching things differently can completely remove those barriers for some of us (e.g. like building ramps instead of stairs), but it won't for everyone. terms like "differently abled" completely ignore and dismiss the experiences of this part of the community, all they do is remind the person that you are uncomfortable acknowledging what they are dealing with. "disabled" on the other hand is inclusive of us both.
Person-first vs Identity-first language
Another aspect of the language surrounding disability that causes confusion in a lot of non-disabled people is whether or not you should be using person-first or identity-first language.
Person-first is where you put the person before the name of the disability, for example "Person with a disability," "Person with autism," "person with amputations," etc. Identity-first language, on the other hand, is where you put the person's disabled identity first, so "disabled person," or in the case of some disabilities, you might drop the need to say person at all, so it would be "autistic" and "amputee".
Unlike the last section, the answer to which one you should be using varies a lot on who you ask, and both types of language have their own benefits.
Person-First
Chances are, if you've done any kind of work that would have put you into contact with disabled people in the last few decades or so, you were instructed to use person-first language. weather you are a journalist, a doctor, an educator, a government employee, or were part of many, many other industries, chances are that you were taught to use it.
The reason for this is that, before the introduction and widespread use of person-first language to describe disability, non-disabled people were much less kind in how they spoke about us. Many people openly used slurs, even in formal settings, or referred to us (individually) as "the disabled," "the wheelchair," "the blind," "the downs syndrome," etc. e.g. "the wheelchair over there asked for assistance," or "I'm seeing the downs syndrome at 3pm."
This was especially prevalent in the medical field, with healthcare professionals often exclusively referring to their patients in this (or similar) ways, refusing to acknowledge their personhood, the value of their lives or their lived experiences beyond their disabilities. The medical field often mistreated and abused disabled patients, and before the introduction of laws protecting the rights of disabled people, this was not only completely legal to do, but was sometimes encouraged. On top of general mistreatment, disabled people, specifically, those being kept in mental institutions, asylums, and other places dedicated to their "care" (or containment) were often used as human test subjects.
There are countless examples throughout history, such as when Dr Henry Heiman infected two boys with gonorrhoea without their consent or the consent of their parents in New York in 1895, one of whom was only four years old with epilepsy and the other was 16 years old with unspecified intellectual disabilities. Dr Thomas Francis infected multiple disabled individuals with influenza in 1941, and George L. Fitch who infected six children under 12 living in the "Hawaiian Leper Colony" with what he thought was Syphilis in 1833. The personhood of the victims of these studies were often ignored or downplayed, so it's not too surprising then, that when the disabled community was finally able to start pushing back against their mistreatment in the late 1900's (The specific decade varies depending on which country you're talking about), they advocated for language that put their humanity and personhood first and foremost, making it much harder for people to forget that they were, in fact, still people and deserved to be treated as such.
Today, person-first is still preferred by parts of the community who still face more dehumanisation than most in the disabled community. for example, it's still very popular among people with downs syndrome. Of course, generalisations are just that: generalisations. There are many people with disabilities who experience very extreme dehumanisations, and still prefer not to use person-first, and vice versa.
There are also a number of disabilities that simply don't have names that work using identity-first language for grammatical reasons, such as people with ADHD (though some online communities use "ADHDers" in more informal settings) or people with BPD. Most often these are the disabilities who's names are acronyms, and so person-first is still used, but more out of necessity than genuine preference.
Identity-First
Identity first isn't technically newer than person-first language, but it's use, and it's name, has changed connotations recently as it has begun to become popular in parts of the community.
You see, for some people, their disabilities are an important part of their sense of self, or at the very least, their disabilities are so impactful on their lives, for better or worse, that they feel like they would be a completely different person without them. This is what we mean when we talk about disability as an identity, and what we mean when we say identity-first.
For some folks who prefer identity-first language, they feel like person-first is trying to distance them from their disability, often for the comfort of non-disabled people. It makes a disability sound like something you carry with you and that you could simply leave at the door if you could, not an important part of yourself. It sounds as strange as saying "A person with creativity" as opposed to "a creative person" or, to compare it to another identity of my own, "a person with gayness" instead of "a gay person".
This particular reason is popular among communities such as some parts of the autistic community, as autism impacts their brain, their personality, their interests, the way they communicate with others and more. If they were suddenly "cured" of their autism, they would be totally different people, and so they feel "autistic" is a better descriptor, as they simply can't be separated from their disability. It's a part of what makes them who they are. This is also popular among people born with their disabilities who have only ever known life that way, or those who have had their disabilities for a long time. Their disability, weather directly (such as autism) or indirectly (due to how people treat them, what opportunities or lack there of were available to them, the people they interacted with, etc) has impacted them so much that, once again, if they weren't disabled, they would have become a wholly different person.
Some prefer identity-first because they feel that they should not have to remind others that they are people. They feel it is unnecessary, and that if you need to be constantly reminded that any group of people you don't belong to are still people just because they are different to you, that's honestly just concerning. And then there are some in the community, who just prefer it because it's usually shorter and easier to say.
There's also a lot of people who don't really care either way. Personally, I fall into this category for the most part, as do most people I know. while I do lean more towards identity-first because it's easier to write and say, and because I agree, I think we as a society shouldn't need to be reminded of anyone's personhood so frequently in 2024, I also recognise that unfortunately, some people do still need that reminder.
It's important to note, that calling someone "the wheelchair," "the disabled," "The autistic," etc is not identity-first language, it's typically under the categorisation of objectifying language and you'll be hard-pressed to find anyone who likes or prefers that. Using identity-first language for these disabilities might look like, "Wheelchair user," "autistic/disabled person" or "that person is disabled/autistic". A good rule-of-thumb is to just avoid using "the" when referring to individuals or even groups of people (e.g. the disabled, the elderly, the gays etc).
Slurs
I also want to talk about slurs briefly. A slur, in this context, is defined by Merriam Webster as "an insulting or disparaging remark or innuendo," though it is often used specifically when referring to words of particularly strong impact, often with a lot of history behind why they have that impact.
For the disability community, many (though not all) of our slurs are somewhat unique, in that they were once considered medical diagnoses. While a lot of people do make this argument disingenuously, I do believe there are some people who are genuinely confused about this, which is why I quickly want to bring it up.
Words like "cripple," "retard," and many, many more I am not comfortable saying for a variety of reasons, all started as actual diagnoses. In fact, several of the sources I used even use them in this way, such as the sites and books I found talking about the two boys Henry Heinman infected almost always referring to them as being "mentally retarded" or "experiencing mental retardation".
I've talked about "cripple" specifically in detail before, but in all of these cases, the word went from a neutral descriptor (at least, in theory) to something that was used in increasingly negative ways, both by the medical professionals diagnosing people with these terms, and the general public. In medical settings, these words were often used to justify the horrible treatment directed at people with disabilities (Like we discussed before), and even after protections were put into place, the language kept its associations. In the general public, these words started being used as insults directly, both directed at disabled people and in general. If you went to school in the 2000's, you probably heard "retard" being used as an insult on the playground as a replacement for stupid or ridiculous. You can see how, when a whole generation starts associating a diagnosis with "ridiculous" it starts to become an issue. This would then feed back into how the terms were used medically. As much as we'd like to think of doctors and healthcare professionals as being unaffected by cultural norms, history has proven time and time again that this was not the case. If you'd grown up hearing a real diagnosis as a synonym for an insult, it's not going to make your opinion of the patients you're giving that title to particularly positive unless you're going to spend a lot of time deconstructing those implications, which, in my experience, many do not.
So yes, even though these might have been acceptable terms once, their use in overwhelmingly negative ways has caused a lot of disabled people to become deeply uncomfortable with them, and they have since been deemed slurs.
Of course, not every slur related to disability came from outdated diagnostic terms. The M-slur used against little people, for example, originated during the times where little people's only option for employment was in freak-shows and other demeaning rolls, such as being kept as pets by nobility. The M-slur was used to compare them to a type of small, annoying fly, a midge, as a way to further humiliate and dehumanise them.
There have been movements that attempted or are currently in the process of reclaiming some of these slurs, with notable examples like the "cripplepunk" community for physically disabled people (They do, however, ask that able-bodied people call the movement "c-punk" instead). Though other words like "retard" are more debated, and many people with intellectual and cognitive disabilities (who the slur was usually directed at) feel it is too early to start that process, or feel it should not be reclaimed at all. At the end of the day, it is the people with the disabilities impacted by these terms who get to decide if, how and when a slur is reclaimed, not outside forces and wider society.
Focusing back in on authors and creatives for a moment, if you're writing a disabled character, but you yourself are not disabled, I'd highly recommend against using slurs in your work, even if your character is part of the community that could reclaim it. Even if you are disabled in that same way, I'd recommend caution. I often call myself a cripple in a joking light, but I probably will never feel comfortable including it in any of my work (outside articles like this where we're discussing it, of course). If you really, really must include these slurs, make sure to get input from others in the community.
Outgroup Terms
Finally, one last thing I want to bring up is in reference to the "outgroup terms" disabled people use for people without a disability.
A very common misconception is that if you aren't disabled, you're able-bodied, but this isn't true! Able-bodied (sometimes shortened to A.B.) refers to people without physical disabilities specifically, so you can be able-bodied but still have an intellectual disability or some kind of neurodivergence like autism, dyslexia, or schizophrenia. Likewise, you can be neurotypical - the word for people who aren't neurodivergent - and physically disabled.
If you want to refer to people without any disabilities at all, the most common way to do that, and the term I've been using throughout this post, is just non-disabled. Some people also use the term "abled" but this isn't as widely agreed upon, as many people assume it's just a shortened version of able-bodied.
Conclusion
As I said in the beginning, this post is meant to just be a general guide, not hard and fast rules. The disabled community isn't a monolith, and we don't agree on everything and that's ok. Different people and groups will have different preferences and that's ok too. If you're an outsider to the community and you aren't sure what words or terms to use, just ask (so long as you're polite about it and/or it's relevant to the conversation at hand, it's fine) but always respect an individual's preference over a generic piece of advice like this post. Under no circumstances should you ever correct a disabled person on how they refer to themselves and their own community. If they refer to themselves as disabled, that's great. If they call themselves, a person with a disability, also great! I can not tell you how many non-disabled people who have told me I am "disrespecting myself" for calling myself an amputee, autistic or disabled.
At the end of the day, how any individual wishes to refer to themselves is their choice, but for creatives, especially those of you writing disabled characters as a non-disabled person, it's important to be aware of the reception and implications different words may have with your audience.
[Thumbnail ID: An image of overlapping speech bubbles on a blue background containing several terms, ranging from commonly accepted to offensive, used to refer to disabled people. Some of the more easily visible bubbles say things like "differently abled," "Disabled," "Special Needs," "Person With a Disability," "Special," "Slow" and many more. In the centre, the biggest bubble says "Disability 101: The Language of Disability." /End ID]
#Writing disability with Cy Cyborg#Disability 101#Long Post#Disability#Disabled#Disability Representation#Writing Disability#Writing#Writeblr#Authors#Creators#Writing Advice#Disabled Characters#Disability History#Language#On Writing#Disability in Media
106 notes
·
View notes
Text
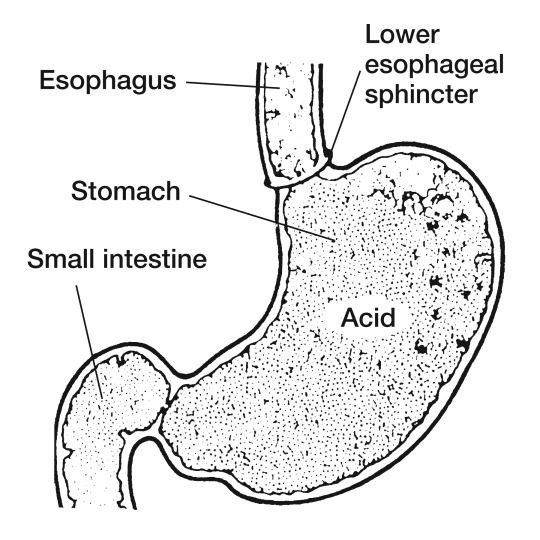
The LES is the laziest bastard
No, not the neighborhood in Manhattan, I am talking about the Lower Esophageal Sphincter. This guy:
I'm having a new case of something like frequent heartburn right now, so in my idle moments of health anxiety I'm looking at fun facts to stress about online.
I'm coming across lots of mentions of what causes GERD (advanced and potentially risky heartburn, basically), and how it's mechanically caused by the Lower Esophageal Sphincter relaxing too much, or not being stalwart enough in its defense against its hapless human host's Bacchanalian eating habits, or against their now-medically-significant-Fatness, or their Unfashionably Tight Pants. Basically, the stomach acid shouldn't be in the esophagus, but this underpaid-security-guard of a structure lets it get into there sometimes. There are some pretty easy-to-predict things that make stomach acid worse. They're obvious if you've ever eaten too much of something that didn't agree with you: rich food, acidic food, spicy food.
But I was surprised by the less-expected mentions of several things that make this flesh ring relax too much. It's PRACTICALLY ALL OF MY HABITS:
Alcohol
Cannabis
Caffeine
Menthol (1)
Antihistamines(2)
Here is the kicker, the thing on the list that will send me into infinite stress spirals if I consider it too much: one of the things that makes this little flesh hole chill out too much is
Anxiety
ANXIETY, the mental state that is famous for tensing muscles, makes this critically important muscle RELAX. I guess the LES is just "not like the other muscles."
========================================
By the way, this post is not a request for advice - I am getting plenty of advice from sources other than Tumblr. Including, if this doesn't let up soon, an actual doctor. Thank you.
And don't worry, I am completely cutting both alcohol and cannabis out of my life right now, until/unless I can figure this out.
Footnotes:===========================
(1) (Inconvenient because menthol is normally useful for treating nausea and sore throats, 2 symptoms of GERD. Also, because I have a habit of constantly chewing sugar-free peppermint gum).
(2) (Inconvenient because they're useful for sleeping through coughing fits, which GERD causes).
#journal#gerd#health anxiety#heartburn#anatomy#acid reflux#middle age#sphincters#why did i tag this sphincter that will not go well
13 notes
·
View notes
Text
Welcome to lovablethings!
inbox: OPEN! Check what's next here: link
This is a blog created by @raygunwestern and his system to reach out to and support the kin community.
How do we intend to achieve this?
Promoting Discords, projects, and other blogs similar to this one!
Offering advice and ideas where I can. (I am NOT a medical professional and cannot and will not provide medical advice or therapy.)
Helping folks get kin calls out there.
And, what you're probably here for- fulfilling requests!
Requests? What requests do you do?
A few kinds. While Raygun is the only mod, the following will be offered:
Name + pronoun ideas
Recipe ideas (PLEASE let me know if you have allergies or specific foods to avoid!)
Shopping / selfcare kits (6 items relating to your kin)
Icons (including pride edits and matching icons)
Sketches or emotes
Read for more info beneath the cut!
What rules do you have?
While not a RULE per se, it should be noted that this blog has a specific focus. The following types of kintypes are welcome to be requested for:
Real animal species, domesticated or wild.
Fantasy animal species in general, such as dragons, unicorns, etc.
Fictional species of animal/monster from media (such as night stalkers from Fallout).
General non-human identities (such as spirits, demons, angels, etc.) including concepts and objects.
Basically, because I admittedly live under a rock and am LARGELY unfamiliar with most sources, I'll be mostly focusing on therians, otherkin, adjacent fictionkin, and the like rather than specific characters. I have nothing against fictionkin! I have many fictionkin types myself, and our system has a couple fictives. I just don't want to disappoint anybody.
If you have a fictionkintype that is an otherwise normal animal (such as Rex from Fallout), if you're willing to give some extra details about what you're looking for, I might be able to help.
On that note, you are very welcome to make requests for your nonhuman alters! Those who don't align themselves with any of these terms but still see themselves as nonhuman in some way are welcome to send in requests, as well, so long as you generally follow the above guidelines.
Furthermore, the actual rules are as follows:
Please have a specific request, at the very least what kind of post you'd like me to make for you! Details relevant to what you're asking for are great, too!
Please be patient. Raygun is the only mod right now and has a brain that beats the hell out of him sometimes.
While I can't control every interaction, it should be noted that trans people are VERY welcome, that BLM and Palestine are supported by the mod, and that I am distinctly not pr0ship.
Please no requests regarding 18+ material of any kind. While the mod is an adult, this blog is intended to be safe for all ages.
All messages regarding any kind of discourse will be promptly deleted.
Why?
lomebly :( and wanted to be helpful,,,
20 notes
·
View notes
Note
Emergency request! (if possible)
I recently found out I have a severe case of anemia (join the club, right? You seem like a pro at dealing with this for quite some time!) It's not just the symptoms like fatigue that bother me, but rather looking as pale as paper. My coworkers even made comments about it in a funny manner.. Could I request a comforting scenario with Dabi and the reader (she/her) after she learns about her diagnosis?
An otherworldly glow - Dabi x Reader
Synopsis: Dabi, and later Toga, both react to your recent anemia diagnosis A/N: hi, sweetheart! No need to stress over that anemia situation. Feel totally free to slide into my DMs, and I'll be your guide through this. I'll dish out some personalized advice – having a doc on call can't hurt, can it? 😅 Maybe I can actually be helpful for once, ha! 😅
MASTERLIST

You step into the League of Villains' hideout, the dim lighting and familiar surroundings providing a sense of comfort amidst the chaos of your recent diagnosis. As you make your way through the corridors, you're greeted by the sounds of hushed conversations in a distance and the occasional clang of metal.
Entering a common area, you spot Dabi sitting on a worn-out couch, his attention focused on a book. He glances up as you approach, his eyes briefly meeting yours before he closes the book and sets it aside.
"You're back finally," he says, his voice carrying a hint of curiosity.
"Yeah, just got back from the doctor's," you reply, offering a tired smile. "Turns out it's quite severe anemia."
Dabi's brow furrows slightly, his concern evident despite his stoic exterior. "Are you alright?"
You nod, taking a seat next to him. "Yeah, I'll manage. It's just been a lot to take in."
He gives a nod of understanding, his gaze softening. "You know, we all have our battles to fight. It's alright to lean on others when you need to. But, of course, don't expect any special or lighter treatment."
You lean back against the couch, appreciating his words. "Thanks, Dabi. It's just… hard sometimes, you know?"
He leans back as well, a thoughtful expression crossing his face. "I get it, doll. Sometimes the world throws things at us that we never signed up for. But it's how we face them that truly matters, isn't it?"
As you sit together, the conversation shifts to lighter topics, Dabi sharing a few anecdotes from his own experiences. You find yourself surprisingly at ease, the tension from earlier gradually melting away.
After a while, Dabi glances at you with a small smirk. "You know, you've got that pale complexion going for you. Guess we'll have to call you our resident ghost now."
You can't help but chuckle, giving him a smack on the shoulder. "Oh great, just what I needed the most – a new nickname, Mr Patchwork. It was rude!"
He smirks back, his tone teasing. "Embrace it. Who needs a tan when you've got an otherworldly glow?"
"Oh, seriously, Dabi?!" Yet your laughter fills the air, and you realize that this interaction, though unconventional, has been a source of comfort.
Amidst the lighthearted banter, you hear a mischievous chuckle from behind you. "Well, well, what do we have here?" The voice belongs to no one else but Toga Himiko.
Dabi rolls his eyes, feigning annoyance. "Just what I needed – a company of the weirdo."
Toga ignores his sarcasm and plops down on the couch next to you. "So, what's the diagnosis, cutie? You're not dying on us, are you?"
You chuckle at her bluntness. "No, just severe anemia. Apparently, I've become the resident ghost around here, according to Dabi," you give him a look.
Toga leans in closer with a sly grin, her eyes dancing with mischief. "Hey, you know, I've got this kinda unusual idea to help with your anemia. Have you ever considered… drinking blood?"
You raise an eyebrow. "Wait, seriously?"
Toga nods enthusiastically. "Yeah, think about it – it's like a natural source of iron, right?"
"Oh, wonderful. Now we're not just a villain organisation but we're also giving medical advice. What's next, Toga? Career fucking counseling?" Dabi snorted.
"I'll stick to more conventional methods. Iron supplements and a balanced diet, you know?" You tell her, rubbing your nape.
Toga pouts, crossing her arms playfully. "Well, fine, be boring as Dabi. But just remember, if you change your mind, I'm here with my trusty collection of syringes!"
Dabi lets out an exasperated sigh. "I still can't believe I'm outnumbered by lunatics."
#emergency request#dabi#dabi x reader fluff#dabi x reader#dabi x y/n#dabi x you#mha dabi#mha x reader#mha x you#bnha x fem!reader#bnha x you#mha fluff#himiko toga x reader#toga himiko#himiko toga#bnha dabi#my hero academia dabi#boku no hero academia#divider by cafekitsune#mha fanfiction#mha fic#dabi fic
103 notes
·
View notes
Text
Gender Critical Tesponse
In response to this [Jordan Peterson Video]
About claims made by organizations opposed to trans people existing in general.
Donoharm.com direct quote:
"A reader assumes full responsibility for any actions taken based on information obtained from this website. In particular, we emphasize that the information available through this site should not be interpreted as medical or professional advice. All medical information, from this or any other source, needs to be carefully reviewed with your trusted healthcare provider before being acted upon in any way."
This means that they know that the information itself is inflammatory; and they take no responsibility if you firebomb a healthcare facility based on what you've read.
Now I've browsed the [donoharm] and [stoptheharm] websites and...There's not only browser-data intensive... They're extremely vague for the amount of resources they use to be able to load up into your browser.
It took me several minutes on my high-speed unlimited data mobile pixel 7 to download.
Most, if not all, the articles are targeted and show very little actual information to back up their claims
Instead focusing on the assumption that their position is correct. Anti-dei, anti-trans, generic arguments without substance.
The claims that they make are incredibly alarming; and they need support for such claims. They don't give any....
I could give several supporting documentation off the top of my head; but for some reason... They don't list it there. The assumption is that this is a universal truth everybody knows.
But if you quote certain politicians or conservative interviewers... Nobody ever knew trans people existed a handful of years ago!
So.. does nobody know? Or does everybody? And if it's everybody... Where's the info?
They have some data; limited, extremely limited and cherry picked about who's doing what surgeries to minors and how mental health providers might be doing stuff.
They, however; don't discriminate in their data collection about which gender affirming surgeries are given, or what medication is given for what reason.
For example; how much of those dollars is due to circumcision? Are you focusing on trans people because it's in your best interest not to confront the religious institutions? It'd be much more effective.
Another example; which medications are given out in support of [precocious puberty]? Why isn't this part of your data sets?
And yet another; what about hormones given to out to children that aren't not trans?
Some children have the opposite of [precocious puberty] I've forgotten what they call it; but they give AMAB boys testosterone if it looks like they're not growing fast enough, and they give AFAB girls estrogen if it seems like they're too manly.
And you even avoid data on gender corrective surgery given to infants that are not circumcision.
It seems you avoid those ENTIRELY; because you know it'd put you in league with us; the trans community... Who have had to deal with those cases and are very much against them.
This is a problem.
Because while we seem supportive of the same Goal; you're targeting trans people in general for the issues caused by the "Normal Gender" community.
You've even said something incredibly important; we must stop this need to gender children at birth in order to avoid giving infants those surgeries and children those hormones.
But it certainly most probably isn't the "Trans Agenda" to force children into a scenario where they need to re-transition themselves when they get older and learn just what doctors have done as part of the "cis-normative agenda" that has caused so many problems in the first place.
Stop blaming the trans community for cisgender bullshits.
7 notes
·
View notes
Note
👀 Gordon amputation HCs? (If you don't mind talking about them!)

Y;HES
ok disclaimer: I am not an amputee! I am not a medical professional! I am not a prosthetic maker! I am not an engineer! I am simply an autistic writer and artist who has had a webcomic with an amputee character for 5+ years and I have done my research- but PLEASE if you like these headcanons and use it as advice for writing amputees I would also suggest listening to other sources, too!
The prosthetic:
-the arm ends about maybe like five inches under the wrist- which makes it just enough to get basic prosthetics going. Something a LOT of people don't consider is how much space you need to get robotics in there!
-This is the case for everyones(?i have yet to see otherwise) headcanons whether they know it or not but he specifically has a myoelectric prosthetic- which in itself is an EXTREMELY high-tech one! What it does is it detects electricity(YES! YOUR MUSCLES HAVE ELECTRICITY IN THEM!) from the muscles under your skin and amplifies them to be movement!

I would actually HIGHLY suggest people do research into these prosthetics because they are SUPER cool but also not as good as you think they are! That being said:
-He cannot feel with it and has to guess how hard he has to grip something! There's research for prosthetics like this, but they're extremely faulty and- if anyone wants to correct me on this that's fine but I'm pretty sure- it would need Constant upkeep and repairs, ESPECIALLY if it could feel like a normal hand.
-at first he only used it when he went out and when he was doing something that might need two hands Because of this- he didn't really wear it much around the house. Not to mention like...he went from losing it, to an immediate gun arm, to suddenly having a prosthetic- whiiiich. Isn't good for the psychological part of a traumatic amputation! So yeah he didn't really like it all too much at first. Don't get me wrong it was a great tool and he appreciated it over no hand especially because he could actually properly articulate the fingers but...it also just. Was jarring.
-eventually, he and Dr. Coomer teamed up to make it more adaptable, and by that I mean a fucking pirate-ass thing where he could swap out his hand for other things like forks or electric screwdrivers or like. Anything. They like to get together to make new hands on the weekend. It's enrichment. With these add-ons he wore the prosthetic more, but sometimes he just. prefers taping a fork to his limb and calling it a day.
-^this hc is based off of adaptive devices that people make to work with whats left of the limb instead of trying to replace it! They range from other robotics to something plastic and/or 3d printed that just holds a pencil in place. From what I've researched they tend to be more liked than clunky fingers you cant feel lol
-IF THERE IS ANY ADVICE YOU GLEEN FROM THIS: please please please he doesn't sleep with his prosthetic on he SHOULD NOT SLEEP WITH HIS PROSTHETIC ON. DO NOT SLEEP WEARING YOUR PROSTHETIC- this also goes for just chilling out ect. Do you "chill out" in your jeans with a belt on?
-I've said it a few times already but I DO want to encourage other people who draw art or write fics that it's OKAY if his prosthetic doesn't work like a perfect, new hand and in fact is more realistic and something that should be done more often! It's very common to want to write off an amputees disability with "ok now they have a prosthetic they're all better <3" which isn't true at all and it really IS worth it to do some extra research- I might just have an engineering and medical special interest so it might just be me but its SUPER fun to learn things and it makes it more interesting writing how a character interacts with their disability!
The amputation/specifics(WARNING FOR TALK ABOUT GORE, OBVIOUSLY):
-I usually write/draw it being a combat knife because that's specifically what he mentions was used, but realistically it would've been something that could get through the suit itself. Either way, it was a really slow and painful process. Fun fact- while this is like...a debate in the medical field, the forearm is one of the most painful things in the body to break!
-Continuing from that last part, there ARE a lot of nerves in your forearm(ever hit your funnybone? yeah. yowch), as well as TWO bones. Arms and hands are SUPER complex so injuries are...just As complex!
-In the full VOD in act 3, Gordon mentions his suit cauterized it- which if you dont know what that is- it's basically Burning A Wound Shut. I can see this being the case, actually- seeing as the suit itself detects specific things in the body being injured- electricity IS a way to cauterize something. I want to point out that cauterization, however, is AGONIZINGLY PAINFUL and is SUPER DANGEROUS, even when controlled! He's SUPER lucky he didn't go into shock and die in his sleep lmao.
-Oh speaking of sleep. I said this in another post but it was sunset when they betrayed him- and daytime when he woke up. So he was asleep in the garbage compactor for hours.
-It's implied because he keeps talking about how he's still bleeding, but yeah even with the suit cauterizing the wound it wouldn't be fully shut. So he'd be bleeding a lot- ESPECIALLY if it didn't want to kill the nerves in his arm(which makes prosthesis easier in the future, via the myoelectric method I mentioned earlier).
-Because of this Tommy(and later Dr. Coomer and Bubby) had to make him make-shift wrappings and have him lean on them a lot. He lost a Lot of blood and by the time they found a fully functioning medical station it wasn't able to just...give him more. It could give him iron and such but yeah this guy has anemia.
-this is just a really funny note but in act 4 when he's leaving Darnolds lab in the VOD he goes "well I guess I'm able-bodied again!" NO YOU ARE NOT THAT IS GUNHAND. But anyways because of this statement, I think for the first few days after being without his arm hes like. oh im not really disabled though even though he is like. stereotypically disabled. sir
-Phantom pains and nightmares are. A nearly nightly combo.
-Whether they're triggered by something or not, phantom pains in general suck so so so so much. Just so much.
-He actually took a Long time to go to a doctor for his issues. Gordon. Buddy. Look Me In The Eyes. you can get medicine for your pain. you can take physical therapy. please . He wasnt even trying to like...tough it out like part of him was but it was mostly that he just. didnt know and forgot.
-it took him a really long time to trust Benrey touching where his hand used to be, but once they grew close post-rescas him and Tommy became Gordons go-to for phantom pain/itch help. slap my dumb arm thank you
Aaaand thats all I can think of at the moment! I might add on if I have any like. Sudden crushing things I need to say about him and my amputation hcs!
#hlvrai#half life vr but the ai is self aware#gordon feetman#amputation#asks#goob.txt#anyways. i know its ambiguous if he got his bio hand back or a prosthetic but guys....i promise its not that scary to write....#at least give him like. agonizing problems with his arm coming back if you give him a bio one. but prosthetics are so fun#as well as writing when characters arent wearing them or even just dont like them!!
107 notes
·
View notes
Note
i am https://www.tumblr.com/intersex-support/756014826153771008/i-knew-i-was-intersex-based-on-medical-care-i-got?source=share this anon what was done to me seems to be the kind where they tuck the phallic tissue into the public bone like this (warning medical diagrams of genital surgery): https://www.researchgate.net/figure/Surgical-techniques-of-clitoroplasty-A-recession-clitoroplasty-without-reduction-of_fig1_355550660 at least it was not completely amputated, i guess prior to even knowing this, i had complained to sexual partners after feeling frustrated/unsatisfied many times, that it "feels like my dick is buried in my flesh and i cant get to it, and i have to masturbate in a really weird way for it to work, you have to press spots that arent intuitive" now i'm finding out that is literally what is happening, and its feels crazy in some way i'm interested in if theres any way to undo that too. i want my fuckin dick back and accessible. some people have mentioned there's surgical stuff to undo it, but i don't know where to begin researching, and i don't know specifically what was done to me in order to account for every detail; it seems near impossible in some way.
content note: continued discussion of genitalia, surgery, and sex
Hi anon.
That must have felt absolutely surreal to have described your genitalia in that way to your partners and then to find out that literally was exactly what had happened, and that your intuition and description had been right. Like holy shit, you literally basically described what happened before you even knew what happened.
It's so fucking hard to come to terms with what doctors do to us and how that can affect the rest of our lives and how it can influence things like intimacy, relationships, sex. It never should have happened to you and more than anything I wish there was a way to undo it and get it back.
From what I know about surgery to try to undo it, a lot of it is very dependent on the individual and on what surgical techniques were used, what kind of scar tissue you have, and things like that. Some things are not reversible, because there might have been tissue that they removed that doesn't grow back. But sometimes, there are surgical options that might help with function or sensation. I've really struggled to find resources about this because from what I've seen, it just all is so dependent on individual situations. I have one friend who ended up getting a surgical consult with a surgeon who does gender affirming surgery for trans people who was able to give them an idea for what their particular options would be, and there was a few options in their particular case. But I know that a lot of us just feel like fuck no, we don't want to go to another surgeon and don't even want to explore that as an option which is SO reasonable.
If this isn't helpful for you definitely feel free to ignore, but I think something that helped me come to terms with some of the impacts of medical abuse and navigating intimacy as an intersex person was reading just a bunch of stuff from other intersex people talking about sex. I'll link a few articles here in case that's helpful for you or any other followers. Content note for in depth discussion of genitalia and sex in all the articles, as well as mentions of surgery.
What intersex people want you to know about sex from Teen Vogue
I'm Intersex. Here's how that affects my sex life by Mark Hay.
Honestly I wish I had more resource suggestions for how to figure out how to cope after surgery, possibilities for undoing, how to actually figure out exactly what was done to you. I feel like that can be honestly another layer of injustice that there isn't this information, that we don't have these resources. Coping with medical abuse has definitely felt like a grieving process for me at times, because it is just so, so hard to come to terms with what was done to me, what was irreversible, and how it changed my life. I wish i had better advice or suggestions to give to you, but know that you aren't alone + that I share your anger + that I hope you're able to figure out a way to cope/process/heal in whatever way makes sense to you.
sending so much solidarity and support 💜💜💜
12 notes
·
View notes
Note
I'm so tired. I feel like my whole life I've been fighting to have a healthy relationship with food and my body, and I just can't do it anymore. I can't fight anymore. And it's so, so easy in comparison to restrict and obsess over tracking everything I eat
I'm dealing with symptoms of a currently unknown disability right now, and I'm so tired. I'm tired of doctors saying "wow, I have no idea what's going on, I've never seen labs like this... but I'm sure losing weight will help!" (Or, worse, "looks like everything's fine, just lose some weight!") It's become this belief that if I was skinny my symptoms would be taken seriously. If I was skinny I'd be able to figure out what was going wrong because doctors wouldn't rely on my weight to explain everything. I know logically there are lots of disabled people who are still ignored while being skinny, who still struggle to be taken seriously, but I can't shake this feeling that everything would be easier if I was skinny
It feels like my life is in the hands of people who don't give a shit about me. And they still probably wouldn't give a shit if I was skinny, but maybe they would. I don't know, I've never been skinny, so I can imagine that everything would be perfect if I was
It's definitely at least partially a desire to have control over my body, too. I can't stop my symptoms, I don't have the tools to figure out what's wrong on my own, but I can starve myself! It seems very silly written out, and it is, but knowing it's silly isn't enough
I saw in your about that you've dealt with comorbid chronic illness and eating disorders, so I guess I'm asking... how? That's probably already on your blog somewhere, actually, so I guess I'm just venting more than anything. Advice would be appreciated, though
God, I feel this so hard, anon. So so hard.
First of all, I am so sorry I have taken so long to get to this ask. Work, ny studies, and my personal life have all been overwhelming lately and I’ve been having to focus on some wellness work for myself.
But yeah. What you’re talking about is a REAL problem, and you are not alone. And the constant medical neglect of fat people and the “I’m sure all your mystery symptoms will go away if you just lose weight” is just the cherry on top of the shit sundae that is chronic illness. It hurts peoples’ lives. It can kill. I don’t have a quick fix for this system, anon, but I just wanted to take a moment to validate you because I know that what you’re going through is so frustrating and draining and soul-sucking. I am mentally sending you strength.
First of all, I might have one suggestion for you: lie. Lie to your medical professionals about just one thing, and no other: tell them you are already on a weight-loss journey, even if you are not. If it gets you the help you need in this system - yeah, fib a little. But then, explain to your doctors that the reason you are seeking treatment for your symptoms so proactively is that they are preventing you from doing what you need to do to lose weight. Yes, of course you really want treatment to improve your basic quality of life, but when you’re talking to your doctor, sometimes you gotta frame it in a way they’ll hear. Explain how each symptom has made you unable to pursue an active lifestyle. Or how you’ve been too fatigued to meal prep, or how your symptoms are costing you so much that you are struggling to budget for dietary changes. You don’t have to actually be planning any of these things, but if it gets them to continue pursuing the source of your symptoms, just lie. I know it’s so triggering and awful to have to do this just to get taken seriously, so set aside time to prioritize something that you find self-caring after this.)
I know you say your desire to control your body seems silly written out, but it’s not silly at all. I get it. I really really do because I have the same impulse. When your body keeps acting out of your control in painful ways, it’ll make you desperate. And when you’ve had the message pushed your whole life that being skinny fixes everything, it tends to stick in your mind. You are not alone. You are desperate and being driven by a valid impulse.
Instead of pursuing an eating disorder, remind yourself that eating disorders only give you the illusion of control. Eating disorders only pave the way for the disorder to get more control over you. Not to mention, starving yourself will likely take even more of a toll on your health, doing lasting damage if you lose a significant amount of weight from starving. You are allowed to love yourself more than that. I know it’s hard. I know it’s hard to keep fighting for yourself.
Are you in any chronic illness support groups, online or in person? If you aren’t, I suggest you find some. You may find a good outlet to vent about symptoms, get advice on what got doctors to take other people seriously, and learn more about your own symptoms.
While I don’t recommend starving yourself, you could try tracking your symptoms in relation to certain foods and see if specific food sensitivities worsened them (this was true for me.) For me personally, it helps to remind myself that these foods aren’t “bad” foods - they’re just not good FOR ME, and choosing the ones that make me feel better is a way of taking care of and loving my body. (If you find your symptoms do not change based on dietary experimentation, you can disregard this advice.) For me, it can be really triggering having to avoid certain foods, so I definitely have to take a pause to calm down and talk myself through it sometimes.
Things like meditation exercises, gentle yoga, de-stressing exercises and therapy will not cure your chronic health condition, but may help keep symptoms from spiking as badly because stress is known to exacerbate physical symptoms. (Easier said than done, I know - what you’re going through is stressful. I am not telling you not to feel stressed, just to try and create small pockets of time where you try to give yourself a break from stress, which may not come naturally and may be hard because you cannot go to a place of escaping your symptoms. Just keep trying patiently and be compassionate with yourself.)
Anon, I really really hope this gives you some sort of help and comfort, even though it’s not a cure-all and I did get to it so late. There’s more I could say based on knowing specific symptoms if you’re okay sharing them, but for now I’ll just leave it at this. Feel free to vent in my inbox any time.
8 notes
·
View notes
Note
hi! i don't know how to bring up adhd diagnosis to my parents. they're those "you don't need a label" people. and they're very loving and i know the worst they could say is no, but somehow that feels worse than staying undiagnosed
sorry i don't mean to vent but... any advice?
sounds like you need to convince them of the benefits of you getting a diagnosis.
if you havent already, make yourself an adhd evidence document (i have explained this in previous posts so i wont do it again here, if you havent seen it or need a reminder scroll back through the adhd tag on my blog and you should find it). this should help you to convince them that you have adhd in the first place
then make a list of all of the reasons why you want a diagnosis. this could be accessing reasonable accommodations in school, getting medication, understanding yourself better, or something more personal to you.
if you want to take it a step further, write it like a persuasive essay. you've probably written a bunch of them in English class by now! if you haven't, look up the Point Evidence Explain structure and that should help. find some medical or academic sources to cite if you can!
what you need to help them understand is that its not just about the label, its about what that label opens up for you. tell them how you are struggling (adhd evidence doc) and then show them how a diagnosis would alleviate that (meds, accommodations, etc.)
adhd isnt just "ooh im so quirky- oh look a squirrel!" it has actual detrimental impacts on our school lives, our home lives, and our mental health. but most people just dont know that! explaining all of this to them should increase your chances of convincing them that you need a diagnosis.
if this still doesnt work, look up how old you have to be to have medical autonomy where you live. it might be younger than you think! although i think in most places it is 18. once you reach that age you can take yourself to the doctor and get referred (as long as you aren't in the States and have to pay for it, in that case im sorry)
hope this helps! good luck!!
20 notes
·
View notes