#because as much as what i experience is common and should not be stigmatized
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Total funding amounts to $125.3M.
Text
Sometimes I get to doubting myself and thinking eh I can't be *that* disabled but:
Normal people do not have to sit down in the shower
Normal people do not freak out if they forget to leave their phone next to the shower because what if they pass out in there (for that matter normal people do not prefer to keep a water bottle by the shower in case they need emergency fluids)
Normal people do not keep a bucket beside their bed in case they wake up too sick to move
Normal people do not sleep 12+ hours per day (more than half their life!!) and wake up tired
Normal people can work at jobs outside their house
Normal people do not have to overthink about every move they make and every tiniest decision just to stay at a baseline of stability. Normal people do not use a pulse oximeter as a fidget toy or mobility aids as fashion statements. Normal people get to simply live.
#normal here being non disabled or chronically ill#if you come for me about my phrasing i will bite#because as much as what i experience is common and should not be stigmatized#i do not consider it normal#it is a Bad Part of my life#obscuraposting#i saw obscura vent in medbay
3 notes
·
View notes
Note
Have you ever found it worth floating the possibility to probably autistic people and maskers (close friends, family, etc) that they might be autistic?
I have tried it a couple times and it seems to just make people get really defensive and upset with me (which I can handle), but then also people start to hold me at arms length. My intention is to bring us closer together by talking about our shared struggles and how to improve our lives (which was totally fine in the past talking about our shared traits without the autism label), but attaching the possibility of autism to it has the opposite effect. The people I’m around are VERY adhd-affirming, and I see how having that connection over the mutual struggle brings my adhder loved-ones together, and I really crave that type of connection with the people I already love and have so much in common with.
You shouldn't tell someone what you think their identity ought to be, no matter your intentions.
For one, many people who are masking or undiagosed harbor deeply stigmatized views about what Autism even is, and so they will not take the statement as a positive declaration of belonging, but rather an accusation that they have failed to conceal what is most frightening or vulnerable about themselves. Exposing their most hidden side will make them feel very unsafe and judged, even if your intention is the opposite.
Telling someone that you think they might be neurodivergent also suggests that you know them better than they know themselves, which is untrue, and may feel invasive and unwelcome to hear.
Your friend could be the most obviously Autistic to ever Autistic from your point of view, but the choice of how to self-define still falls solely on them. There are many different ways for a person to interpret their experience, and they might arrive at some other word or concept that better does their experience justice from their perspective.
our identities exist to help us make sense of our lives and express who we are to people, on our terms. Most neurodivergent people are absolutely sick of always getting defined from an external point of view. We don't need member of our own community doing that to us further.
If you have benefitted from coming to understand yourself as Autistic, you can and should speak about that openly and positively. That will be enough incentive for anyone else in your life who is neurodivergent to explore the possibility for themselves. If you vibe easily with someone because you share traits in common or seem to naturally understand one another, let that be enough. Tell the person you feel comfortable around them and that spending time with them helps you to accept yourself. That is a much greater compliment than telling someone who they must be.
209 notes
·
View notes
Text
So how do you change an anti-vaxxer's mind, anyway?
First, understand that sometimes, the answer is simply: you can't. Some people are very firmly entrenched in anti-vax narratives, and will become extremely aggressive in response to challenges.
Second, understand that in this case, saying nothing is better than saying the wrong thing. Becoming hostile, or expressing judgment (no matter how well-deserved) is likely to entrench them more into these conspiracies than it is to make them see reason, making them less likely to be receptive to even gentle challenges in future.
Third, understand that change isn't something that happens after a single conversation. It takes repeated discussions, and a lot of building up trust, to start making people change their minds.
So, then, how do you change an anti-vaxxer's mind?
First step: understand why anti-vaxxers feel this way. This can be summed up in one word: fear. Irrational fear, but fear nonetheless. There are a lot of reasons they may have gotten to this point. They may be deeply distrustful of physicians due to past experiences. People of color in the United States are very prone to vaccine hesitancy and refusal, not because of conservative views, but because of the racist history of the medical institution- in particular, the atrocity known as the Tuskegee experiments. Some, particularly those in the United States, are very prone to distrusting the medical-industrial complex, and extend that skepticism to vaccinations as well. Some may have encountered misinformation, such as the infamous Wakefield farce, which convinced them that children were in danger of being autistic (which is still heavily stigmatized) if they became vaccinated. There are also other reasons, but these are the most common.
And how do we deal with other fears people have? Empathy.
How to have an empathetic conversation about this issue:
First, you need to do just that: have a conversation. Ask open-ended questions, and listen to the answers no matter how much they anger or upset you. The most important and most simple: "what are your reasons for not trusting vaccines?" Other good questions are, "why do you feel this way?" "Are you interested in receiving information about vaccines from me?" "How can I help you work through these difficult feelings?" You need to then tailor your conversation according to how they respond.
You need to build trust with the person you are talking to. If you are in a position of privilege over them, particular if you are white and they are black, you cannot attempt to speak over their concerns about bias in the medical community. This also includes disabled people who no longer trust doctors to have their best interests at heart. Empathize with their concerns, don't erase them, and then segue into the facts. "This is an unfortunate reality, and should never have happened to you. May I share a counterpoint about (specific issue), with the understanding that this does not erase the systemic biases in the medical community?" It is worth noting that breakdowns in trust in the doctor-patient relationship are a key factor that leads to the development of antivax attitudes. This person already feels they can't trust their doctors or the government, and they have, in desperation, turned to a community of other afraid people to be heard. If you remember this, you will have a chance here to gain their trust and be an ambassador for vaccination.
Another way of building trust is to emphasize to them that your goals are aligned. They want what is best for them and their kids, even if they are misguided, and so do you. One rhetorical strategy (that is, incidentally, also used by lawyers in jury trials) is to ascribe positive traits to this person, and then challenge them to live up to it. "I know you love little Tommy very much, and want him to be healthy. I want him to be, too. I am sure, since you care for him deeply, you will look into this issue thoroughly."
That last point is also key. You need to start small, as counterintuitive as it might seem. Don't come right out and say for them and their children to get vaccinated; they need to make that decision by themself. Instead, say that you have information about vaccines that you would like to share with them. It is especially good if you have something saved for a particular claim they made. If, for example, they believed the Wakefield study, there are many refutations out there you can show them. If they are concerned about mercury, you can explain that the kind of mercury in vaccines isn't the "bad" mercury that we find in tuna- and even if it was, there is less mercury in the vaccines than there is in tunafish. Keep it focused, and keep it neutral; one claim at a time.
It is very likely that they will respond to you with a study of their own. Read it carefully before responding. "I noticed that the Wakefield paper has since been retracted. Here is a peer-reviewed study that reaches a different conclusion; it seems worth examining."
You need to show that you are actively listening to what they have to say, and that you appreciate them talking to you. "Thank you for trusting me to talk about this." "Thank you for showing open-mindedness." No vague-posting about anti-vaxxers, no eye-rolling, and no distractions while talking to them.
Another key for showing empathy is to make sure you acknowledge the root of each claim. You don't need to repeat it like a parrot- but for example, using the mercury example above, "it is understandable that you fear mercury! Normally, it is a dangerous substance. Thankfully, there are different kinds of mercury, and the one that can make you sick, methylmercury isn't the same as ethylmercury, which is the one found in vaccines."
Don't start right with debunking myths; always begin with an affirming statement ("that must be scary" or "I know there is a lot of information out there; you must be overwhelmed trying to sort through everything!") before pivoting to correcting misinformation.
Keeping your tone positive in nature is also very helpful. You don't have to be shooting rainbows from your mouth/keyboard, but positive statements help build trust and make people more receptive.
Remember that debunking myths is only one part of what you are seeking to do here. If the person you are talking to starts to feel like you only want to hear their thoughts so you can correct them, they will stop sharing them. No one likes to talk with someone who only wants to be right, even if they ARE right!
Unfortunately, these steps may not work. Sometimes, despite your best efforts, the person won't be receptive. That's okay. Simply tell them again that you are here if they have questions, and you wish for the best for them and their children. Let them come to you if they change their mind.
And please remember, above all else: while these are important conversations, you are never obligated to accept verbal abuse. You have a right to have your boundaries respected just as much as they do. If the person you are talking to name-calls, uses bigoted language, mocks you, wishes bad things on you, etc, it is okay to walk away. Maybe they'll be ready to hear it one day, maybe not, but you don't need to set yourself on fire to keep anyone warm here.
I hope that this guide helps you if you are interested in discussing vaccine hesitancy and refusal! Please let me know if you need anything clarified.
38 notes
·
View notes
Note
if this is too much please don’t feel pressured to answer. i just have a lot of thoughts about antipsychiarty and idrk where i stand
because, like. ive been in really bad places before and then they hospitalized me and like that was *bad*, right, i still believe thats bad
but the hospitalization put me on meds and OBVIOUDLY I DONT THINK PEOPLE SJOULD BE FORCED ON MEDS ITS UP TO THEM but also i consider my meds to be life-saving. because i no longer want to die. because i can stop having panic attacks. because there is an amount of feeling… not even good! just okay! that i never had before
and ive been in therapy that i hated and therapy that didnt work and the hospital doctor called me a “psycho”. but i also have a therapist now that i love. i consider him a friend. they don’t try to fix me or anything but i just, like. i go to therapy and it helps?
and i want to go into psychology. not psychiatry but psychology, because i want to do for other people what my therapist does for me, and i want to help people, and i want to learn about brains- the “normal” (which doesnt really exist) and the abnormal-
and i say that i am a system. and that i am autistic. that i have depression and anxiety. because it helps me to have language to understand myself. to be able to explain certain complixities of my humanity in less words than it should take and yes it misses out on the nuance but it helps, too, i think. learning i was autistic helped me.
so idk. i want to be anti-psych. because of the medical abuse and the usage of diagnoses to undermine people’s feelings. but can i be antipsych and love my medication. can i be antipsych and want to be a therapist. can i be antipsych and enjoy having labels to use for myself because it helps me learn to love whats in the mirror.
and if i cant be antipsych and all these things, then am i propsych? and for the very system that destorys and abuses and traumatizes people?
sorry for all this
im just confused
and scared.
I mean first off Im just one person whos anti psych and everyone whos anti psych will have different opinions on these subjects .
The most common anti psych stance on meds is that we should have full autonomy in choosing to take medication and in choosing not to take any meds. -this is not what reality looks like rn. Especially people with very stigmatized labels like schizophrenia or bipolar disorder are coerced into taking meds /literally forced on meds trough physical violence and coerced into staying on meds that harm them. And then other people -like for example people who are trans or nonbinary who want to transition are put through a dehumanizing process of pathologization of their queerness just to get access to HRT and then theyre still often denied access to gender affirming care . Both is awful . We always know who we are and what we need best. We deserve full autonomy on our decisions,always. You can obviously take meds yourself and be anti psych thats not a contradiction at all.
Also a lot of people who are anti psych reject the biomedical model (=mental health is the same as physical health - this includes words like Symptom/disorder and diagnosis labels like depression anxiety autism schizophrenia etc) since there is no scientific basis for calling our mental distress / neurodivergency a disorder or an illness and our diagnoses are just descriptive labels that say nothing about the cause of our suffering/behavior/feelings/ourselves in general . There has never been found a chemical imbalance, genetic defect or biomarker for our experiences of distress/neurodiversity .they came to These conclusions through their own Research .its insane that the biomedical model is still talked about as If its scientific fact, it is disproven and inherently contradictory . I highly recommend reading into current anti psych/Mad studies literature to understand how this oppressive system of hegemonic psychology operates in our current neoliberal society and why the biomedical model is still used today to diagnose us as "ill" and "treat" us . This is my perspective on the matter.
But honestly, i wont ever tell someone what words to use to describe their own experiences, how they should think about themselves and who they are - thats what psychologists do . Im not interested in doing that at all . Use the language you seem fit to describe yourself - i just recommend reading into different frameworks of interpreting your own experiences before you conclude that the biomedical model is the one that makes the most sense to you.
This is a different framework based on marxist theory
This is a different framework based on the disability rights movement
This is the biomedical model explained
Resources for psych abolition (harm reduction Guides, Mad studies, Zines ... )
This is a PDF to a book that goes in depth about the biomedical model and how the psychiatric system and its ideology is still extremely oppressive today
One thing that i firmly believe, that a lot of other people who are also anti psych dont share the same view on, is that Im convinced that you can not be against psychiatric violence and then become part of this oppressive system yourself. To me thats like becoming a cop to stop police brutality 💀Give me a Break
Thank you for your ask ! I highly highly recommend reading more into the subject of mad studies/psych abolition before dedicating energy time and money into being part of a system that youll probably despise in the end . (💀i have a degree in psychology by the way so i speak from experience)
10 notes
·
View notes
Note
Do you have any advice or specific tips to writing a low/no empathy character? Or a resource to recommend?
Hi nonny! Thanks for asking! I'm going to try my best to answer your question, but keep in mind, this is all based on my own personal experience, and that varies vastly from person to person. (if anyone else experiences low/no empathy, please feel free to add on to this post!)
So, some things to keep in mind:
Why does your character experience low/no empathy? For me, it's a symptom of my autism, but there are multiple reasons a character could have low/no empathy. The most common is probably going to be some form of disability (autism), or disorder (psychopathy), etc. (Be careful while doing research though, especially on disorders like psychopathy! You're going to run into a lot of ableist bullshit. Make sure to look for sources written by people living with these disorders/disabilities.) (If anyone has any resources on other disabilities or disorders that cause low empathy that they personally recommend, please feel free to add links!!!) Whatever the reason, it's not going to only affect their empathy. It's going to affect every part of their life. So make sure to do your research, and write respectfully. If you know someone or follow someone who has a certain condition, ask if they'd feel comfortable answering questions for you. If they aren't, that's fine. If they are, they're going to be a great resource. (I'd also recommend getting a sensitivity reader, particularly when writing about mental disorders that are already frequently stigmatized. You want to make sure you're not promoting harmful stereotypes.) I should note, however, that neurotypical people can also have low/no empathy!!! It just happens to also be a common symptom of various mental disorders.
Consider what kind of empathy does your character lack. There are two kinds of empathy! Emotional (or affective) empathy, and cognitive empathy. Affective empathy is made up of three parts: Feeling the same emotion as someone else, feeling discomfort or stress in response to someone else's suffering, and feeling compassion for or understanding another's emotions. Cognitive empathy is the ability to recognize and understand the emotions of someone else. This includes being to "stand in someone else's shoes", or take another person's perspective, and generally understand what they're feeling. This one has been called more of a "skill", in that it's something people can "learn", where as affective empathy can't be taught or learned. When people talk about having low/no empathy, they are usually referring to lacking affective empathy, but a character might struggle with both!
Not everyone experiences empathy the same. Some people lack empathy in some circumstances, but have it in others. For example, I lack empathy when it comes to human beings, but I am much more empathetic when it comes to animals. A character might only be able to empathize with very specific scenarios or people. (For example, if someone else is going through a very similar scenario to one they have experienced in the past, it may be easier for them to feel empathy. But it might not!) Some people can empathize with certain emotions better than others. (I empathize better with anger, but can't empathize at all with grief.)
Understand that a lack of empathy does not equal a lack of caring. Just because a person doesn't feel the emotions someone else is feeling doesn't mean they don't care. A person with low or no empathy can still be kind and compassionate to others. They might go about trying to cheer people up in a slightly different way (I personally tend to try and go for distractions), but they still care about their friends and loved ones. Even seemingly "uncaring" things said by those who lack empathy do not come from a place of malice. (I can't tell you how many times I've said something well-meaning and had people assume I was being cruel. I wasn't, and I genuinely had good intentions.)
Keep in mind how your character reacts to other's emotions. People with empathy tend to feel similarly to those they empathize with, which generally creates a feeling of connection. (This is part of what leads to that sense of "coming together after tragedy".) A person with low/no empathy might instead feel alienated or uncomfortable when faced with large outpourings of emotions. They might be uncertain how to act or what to do, and they may try and avoid situations with strong negative emotions because of it. (In my case, people crying makes me very uncomfortable, because I don't know how to respond. So I try and keep my distance.)
Think about how your character processes their own emotions. Just because a character doesn't feel empathy for others doesn't mean that they are incapable of feeling those emotions on their own. A character who has no empathy for a grieving friend can still grieve! But chances are they will process that emotion differently than a person with "normal" empathy. They might try to push their emotions away and bottle them up. Or one emotion might transition into one they have an easier time processing. (For me, I don't experience sadness normally. It either transitions to anger, or it is replaced by different thoughts.)
Think about how their lack of empathy influences their life. A person who lacks empathy is not going to experience life the same way as a person with "normal" empathy. They might have a hard time making friends, or they might excel at a job that requires a logical mind. They might give great advice, or their friends might know to never ask them about relationships. They might be great at organizing people, even in times of stress, because their brain compartmentalizes and thinks pragmatically. They might totally shut down when faced with an emotional situation because they don't know how to process it.
Having no empathy can be very alienating. People expect empathy constantly. It's a big part of why people love emotional media, and it's the expected response when someone you know experiences suffering. Not having empathy can mean that you feel disconnected from your loved ones or community as a whole. It might mean biting your tongue and not saying what you think because people would read it as uncaring or cruel.
Remember: Having low or no empathy is not a bad thing. People with low/no empathy are often villainized in media, and the trait is often given to antagonists. But that's a harmful stereotype and harmful belief in general. That's not saying that your character with low empathy has to be "good", but don't use their low empathy as proof that they're a "bad person". Try thinking about situations in which having low/no empathy might be useful! I personally am reminded of the post I saw years ago where someone was saying that if not for their lack of empathy, they probably couldn't do their job. (iirc, they worked handling the bodies of organ donors, some of whom were quite young.)
Okay, that's all I can think of for now, but like I said before, anyone else who experiences low or no empathy is encouraged to reblog this post and add on to it! And if I made any mistakes here, please let me know so I can fix them!!! I tried to base this mostly off of my own experience, so take it all with a grain of salt.
#Anonymous#morrigan replies#writing autistic characters#writing low empathy characters#writing no empathy characters#character development#character inspo#no empathy#low empathy
116 notes
·
View notes
Note
I agree that drugs should be legalised and not stigmatized but you're delusional if you think "most drugs can be consumed completely safely with almost 0 risk to the user"
I think the key here is the word "can" by which I mean that if consumed in safe doses and safe environments and from safe sources etc most like mainstream drugs (I'm thinking of like mdma, LSD, shrooms, ketamine, coke) CAN be consumed safely with very little risks. I know this to be a fact #1. because I've done a lot of actual research on this where I've read numerous sources from scientists doctors and users as opposed to just say taking in the abstinence only information I received during school, reading a couple Tumblr posts and assuming I know everything there is to know about the topic and #2 I've used every drug I just listed and more and never suffered any adverse effects because I did my research, tested them for impurities when appropriate, and took other measures to ensure my safety
there are obviously exceptions and drugs that just shouldn't be fucked with (meth and heroin is what I'm thinking, but I also know people who have consumed these once or twice with 0 repercussions because that's how human experience works), but if you're actually interested in learning more about the many ways in which you were lied to about how "illegal drugs" are somehow automatically much worse for you than prescription drugs or socially acceptable drugs (like caffeine and alcohol) then feel free to either 1. do your own ACTUAL research that does not involve trusting for profit rehab centers and abstinence only educators (I'll even get you started with a couple good resources) or 2. message me off anon to have a real discussion about the mechanisms by which the most common drugs operate and the ways in which they can be consumed as safely as you can consume alcohol cigarettes and energy drinks but sending me your half cocked uninformed and unnecessarily insulting opinion on anon is not exactly productive. additionally, I'm sure you can see why I struggle to see or believe that you ACTUALLY think drugs should be destigmatized and aren't just parroting what you think the correct woke opinion is when you refuse to even take the very first step to destigmatizing drugs, drug use, and drug users and actually unlearn all the stigmatizing things you've been taught
I know that it's a lot easier just to port over all the things you've learned from dubious sources that you trusted implicitly because they claimed to be an authority and not actually do the work required to achieve the goals you claim to support, but easier doesn't mean right
#thanks for trying though#messages like this are so interesting because what are you trying to accomplish here#oh fuck guys someone anonymously called me delusional for stating a fact which i can support with research#guess i better change my whole world view#i guess if im giving you the benefit of the doubt here ill say maybe i used the word 'most' a bit erroneously#considering there are like thousands of prescription and nonprescription drugs#but ironically people always talk about the danger of drugs without actually meaning to invlude prescription drugs#even when theyre talking about things like fentanyl. because prescription drugs are just thought of as safe#in a way that like lsd (which is extraordinarily safe) is not#but even still i feel that the rest of the point of my post shouldve overshadowed what might be somehwat of an exaggeration#youve just ignored the entire rest of the post in favor of supporting your preexisting worldview#so you can feel superior for some reason? like why else would you send this message#fascinating
18 notes
·
View notes
Note
Hi sex witch, I (cis man, late 20s) have a bit of an issue regarding medication and my sex life... I'm hoping you can be a bit of a sounding board for me?
I recently started taking an SNRI to help with anxiety and sleep. It seems to be working (not perfectly, but there's definitely a pretty big improvement).
Currently I'm single and all my sex is solo, but I've noticed that since I started the meds my libido has significantly reduced. It's also more difficult to reach orgasm, and the orgasms feel... different? (Not sure how I feel about that bit...)
My main problem is trying to work out whether I want to raise this with my doctor when I go for my next check-up. I'm not in the market for sex with anyone else right now, so the only person it is affecting is me. The positives in terms of my anxiety are great, and the negatives are more "differences" than actual "negatives".
What do you think? Should I push to try a different medication before I get settled on this one? Or should I spend more time working out whether I'm comfortable with the lower sex-drive? I think both are reasonable, and I would appreciate your opinion - thanks!
hi anon,
PREFACE: I'M NOT ANY KIND OF DOCTOR AND THIS ISN'T MEDICAL ADVICE.
I just want to start by commending you for noting the difference between "different" and "negative." people are often taught to think of any change in their sexual function as automatically bad, when in fact it's often nothing more than a very natural fluctuation within their body.
in your case, that fluctuation is very common; many people report experiencing a decrease in libido after beginning anti-depressants. hormones drive much of our sexuality, and anti-depressants wreak havoc on our the delicate chemical balance in our brain - for the better, of course, because they ideally help bridge the gap for chemical deficiencies in our brains that make us feel Not So Good, but as a side effect functions like the libido can be thrown into a spiral.
it's worth noting that the change often isn't permanent; eventually, your body may very well acclimate to the new hormonal arrangement and gets back to business as usual. I can personally attest that my first year on anti-depressants saw my libido pretty much go dormant, but it eventually came back with a vengeance.
I'm not in any way, shape, or form an expert on how the brain works and how medication works in the long term, but as someone who spends a lot of time talking to people about sex and has been on anti-depressants for years, I have to wonder if part of the sex drive's return has to do with the effectiveness of the medication over time. many people have a hard time fully accessing their sexuality when they're suffering from stress, anxiety, and depression, because being horny - let alone actually having sex - requires an amount of mental space and energy that just isn't there when you're struggling to even perform the basic tasks that let you get through the day. again, speaking from personal experience, I know that before I was medicated, WAAAAAAY too much of my energy was getting burned up by my anxiety and the accompanying physical symptoms; there's not much left over for libido when all of you're exhausting yourself shaking and otherwise being a nervous wreck. turns out being horny is WAY EASIER when you aren't constantly on edge!
I will also point out that sometimes the reason people who aren't doing so great in regards to their mental health masturbate so much is for those sweet little dopamine hits that they're not getting anywhere else, which I don't say to stigmatize jerking off while mentally ill (god knows I can't judge for that) but to point out that after a few months with more managed anxiety, you may not even be as interested in solo sex as you previously were. or you will be, but it will look different thanks to the other positive effects your medication has had. sexuality is a slippery creature, and it's impossible to predict exactly how it will shift throughout our lives.
my point being, if you haven't noticed any other adverse side effects of this medication and you think it's going to help more than hinder you, I would recommend continuing with it for the time. you'll keep reaping the positive benefits in the meantime, and you'll have some time to reflect on those changes as they continue to happen and figure out how this new shape your sexuality has taken can still fit into the overall mosaic of your life. if you ultimately decide that you don't like what's changed, that's fine! but I would broadly advise waiting it out through the most dramatic shifts that will happen early on to get a fuller picture.
42 notes
·
View notes
Note
Hey, I hope your doing ok and I love your posts, even though I don’t have schizophrenia your posts help me see from other perspectives and be more open minded and considerate.
So anyway in the past week I came across two posts from two different people that were on tik tok that said (jokingly) “none of these people know I have schizophrenia” and it was a picture of an empty room.
I felt the need to share this and I was wondering what your opinion on these “jokes” are. but I don’t get how people can say people with schizophrenia are evil and then turn around and make harmful jokes about it.
And I don’t know if you have tik tok or see any posts like these but I was wondering how you deal with them (or how I should deal with them)
I don’t have tik tok and I refuse to download it but posts like these give me anxiety I do try to avoid these posts but when they cross my path I get angry and upset and I wish these people were educated enough to not make these jokes.
I hope this makes sense and I you have a good day
Thank you! I'm always grateful to see nonschizophrenics follow this blog just to get a new perspective, it brings me hope that people without the experience can still have enough respect and understanding to listen to people like me.
And yes, I am very aware of these types of "jokes". It's common enough to have the name "schizoposting" and I hate it so much. That particular joke has been done many, many times, and the punchline is the person with schizophrenia. These types of "jokes" range from making fun of symptoms like hallucinations, making fun of people who take antipsychotics, or triggering delusions just because people think it's funny. (Sidenote a lot of these "jokes" seem to think hallucinations are usually like seeing full people for long enough, and not being scared by them enough that they are your friend, when that actually isn't a very common hallucination at all and I think that idea comes from misrepresentations in the media.)
I hate these "jokes" for a few reasons. First they are making fun of real mentally ill people who can, and do see these posts. I do not see what's funny about making fun of serious symptoms that people actually suffer with. I didn't choose to have these symptoms or this disorder, it's not funny to me at all. I honestly don't see "jokes" at the expense of people with any other mental disorder by people who don't have the disorder nearly as often as I see jokes about schizophrenics by nonschizophrenics. I've never even looked for them and they just show up. My partners TikTok (which they don't use to look up any schizophrenia content) will just have them pop up. And I rarely see any backlash to this content that I would expect in this time where a lot more people are aware of mental illnesses and mistreatment of those who have them. Secondly, these "jokes" seem to assume that actual schizophrenic people won't see them, or they just don't care. Honestly a lot of people don't realize that schizophrenic people actually exist and actually participate in life and online. Thirdly the "jokes" that purposely trigger delusions/unreality can be very harmful to psychotic people. Once again this isn't funny at all. Fourthly this just adds a new layer of stigma to the already highly stigmatized disorder of schizophrenia. We are still seen as dangerous and scary, and also just existing, taking our meds and having symptoms is funny to people who don't experience it. I honestly have very rarely, if ever see people who are not psychotic stand up for psychotic people online, it seems much more people are willing to just laugh at us.
For people like you who are not schizophrenic and see this content online anywhere, please report it as harassment and don't leave a comment/reply. Even if you are commenting to educate, the algorithm will just see this as engagement and possibly push it out to more people.
For anyone reading this who is schizophrenic/psychotic and you see this content, report it if you feel comfortable with that, and block the account.
These "jokes" shouldn't exist, and everyone should be able to see how rude and sanist they are.
For me, when I see these posts I get angry, but I try not to look at them too long, and I don't attempt to educate those people. It's not worth my time or energy and I think if everyone with respect for schizophrenic people just ignored them it would be helpful. Unless you personally know someone who is posting these "jokes" and they can listen to you, you can try to educate them. Honestly it comes down to letting nonschizophrenic people know that schizophrenic people are human beings that deserve basic respect, because they may have never been told that before.
#answered#schizoposting#schizophrenia#schizophrenia jokes#mental illness#nd#schizophrenic#neurodivergent#psychosis#actuallyschizophrenic#mental health awareness#pseriouslypsychotic
80 notes
·
View notes
Text
"A reader asked: Why are there so many Autistic people with narcissistic parents?
Before I get into this topic, here's a content warning. If it helps you feel safe to vilify and dehumanize people with narcissistic behaviors, then you may want to skip this post. I'm here to humanize people, including people with NPD! (And neurotypicals too but that's a topic for another day)
If a compassionate understanding of what causes narcissistic behaviors is likely to trigger you, you can stop reading here. Debate is not welcome on this page: you're of course welcome to disagree, but you don't need to tell me if you disagree.
So, why do so many Autistic people have narcissistic parents? Why do narcissistic traits seem more common in families that also have Autism, ADHD, & HSP neurotypes?
My response: Narcissism is a misguided defense mechanism against overwhelm. NPD is a form of C-PTSD. Narcissistic behaviors can often conceal other forms of neurodivergence.
Parents of Autistics are extremely likely to be Autistic or ADHD themselves because of genetics. I have SO MANY ND peers who have narcissistic parents who are undiagnosed Autistics.
Most people who learned to use narcissistic strategies to feel safe are themselves Autistic, ADHD, or some other form of sensitive neurotype. People who are not as neurally sensitive don't experience such severe reactions to lack of control.
A common core wound in this trauma pattern is experiencing emotional abandonment throughout childhood while having external needs abundantly met. Sensitive ND children who have everything they need EXCEPT emotional connection and co-regulation tend to develop either BPD or NPD depending on their socialization and predisposition.
To use a popular example, Trump grew up with unsupported ADHD and an abusive father, so he learned to use extreme control of others to feel safe. Narcissistic behaviors are subconsciously triggered fight responses that are typically aimed at controlling relational or sensory environments.
To be clear, saying it's a trauma response does not excuse harm! If we hurt someone in a fight response, we are still responsible. If our trauma responses are harming people, we must seek help to integrate the trauma response.
"Narcissists can't heal" is a myth that comes from the fact that the resources necessary for a narcissistic person to heal do not yet exist in most of the world. People with NPD CAN heal if they are supported enough to learn how to use other strategies for building safety in their nervous system. Most professionals refuse clients who have this diagnosis because they aren't trained well enough to be able to help without becoming targets for harmful behavior themselves.
The complex trauma explanation of NPD is one that I learned from ND people who have a NPD diagnosis, are aware of their patterns, and are trying to heal but face enormous challenges around accessing help. "Nothing about us without us" applies to people with NPD as much as any other form of neurodivergence.
Occasionally, people who have experienced relational abuse get really mad at me for saying that people with NPD are neurodivergent or that their lived experience perspective is valuable just like any other group within the neurodivergent umbrella.
I believe stigmatization of narcissistic behaviors actually perpetuates the social conditions necessary for narcissism to thrive. It has been really helpful for my own healing to separate the abuse I experienced from the innate neurodivergence of the people who hurt me.
Edit: An important clarification! Boundaries are essential. Having compassion for someone's pain does NOT mean I should stick around and allow myself to be harmed. We can understand that "hurt people hurt people" while refusing to allow harm to continue. I am not suggesting that people need to accept or forgive their abusers. Also, if someone has hurt you, regardless of the reason, you are not responsible for helping them heal."
_
From the comments:
Sarah Longstaff: “I do want to add to this my plug for an anthropological perspective. The diagnoses in the DSM are all from the outside—they do not rely on open-ended interviewing or lived experience analysis. They were not created cooperatively with people needing help.
They also do not factor in trauma. Complex PTSD has been excluded from the DSM for 3 decades. When I see people throwing out “my relative was diagnosed with___,” I want to point out that diagnosis is extremely subjective—and may be wrong.
Insurance companies do not want to cover long-term trauma therapy. Pills are cheaper. A lot of misdiagnosis has happened in the last 30+ years. I am thrilled that people are talking about trauma again, but remember, trauma therapy is still available primarily for rich people. “Not getting help” is not always a lack of will—it is a lack of affordability and access. Florida Medicaid, for instance, will only cover “crisis management,” not EMDR.
As a victim I too need to protect myself from people and behaviors. But also in the name of compassion and fact and accuracy, we need more people pushing back against categories that aren’t scientific, that don’t include lived experience and collaboration, and that aren’t trauma/nervous-system informed.
Another factor—alexythymia. Alexythymia is neurological—it is an interoception issue. Some people misinterpret feelings, and/or only feel strong emotions and may need to create those. Alexythymia is part of neurodivergence too.
When dealing with my undiagnosed autistic parents’ narcissistic behavior I often ask myself “does my ‘healthy’ approach just not let them access the intensity of emotion that they need to feel? Could this be a factor?”
It helps me take their behavior less personally.”
4 notes
·
View notes
Text
The problem plaguing cishet romance and the biggest advantage queer romance has over it: A sociology of literature analysis on the history and prevalence of the romance genre
I've gotten some feedback where people have expressed that they thought they didn't like romances but later found out they liked queer romances. I thought it would be fun to go over some inherent differences between cishet and queer relationships in fiction and how they came to be. I've chosen to use cishet instead of straight because I want to make it clear that these things don't necessarily apply if someone in a straight romance is confirmed not to be straight, and they definitely don't apply if one or both are trans.
As usual, I hope you enjoy this.
So, what is the biggest problem with cishet romances? Its ubiquity. The type of relationships depicted in those stories wouldn't be half as problematic if they weren't so prevalent. It'd be one thing if a few stories had some questionable, to say the least, relationships portrayed positively. After all, countless stories have some questionable things in them that go unnoticed by the narrative, but that doesn't mean that people who like those stories can't tell that those things aren't commonplace. Nor does it have to mean that there’s any harm in those people believing those things were accurately portrayed. The times this becomes a problem is when the portrayal of something questionable becomes so widespread that people start to think that it's odd for them not to have this thing in their lives or when a popular work inaccurately portrays something that's already poorly understood and highly stigmatized. This, inversely, is also the main argument against setting requirements for one specific story since one story isn't going to change the world, no matter how popular. Storytelling is one of the most collective forms of expression there is, so what really matters is how much effect it has on other storytellers. Not to mention the role fandoms have in normalizing queer identities as someone who has previously been sheltered learns about different people’s experiences through a common interest.
So, how did cishet become so prevalent? Well, for starters, there used to be a time when a man and a woman getting together was seen as a societal obligation, and whether or not the people involved even liked each other wasn't a concern to anyone. There was also some method to their madness, as this sort of arrangement worked quite well for the societal structure at the time. It made sense to create stories where the justification for someone getting together is that they're a boy and a girl because that was the main requirement in the eyes of society. If anything, the stories often portrayed people choosing to marry someone for their personality, which many historians would say wasn't something people did. At least not typically. Though, who's to say? It's a lot easier to find out what people in the past did than why. The bottom line is that cishet relationships were so prevalent in stories because they were stupidly prevalent within society.
Then there’s the way a lot of cishet relationships are depicted in fiction. It tends to imply what a desired relationship should be like, which at best creates unreasonable expectations and sometimes straight up encourages girls and young women to seek out traits in men that ain’t healthy. Some of the most prominent of these are anger issues, controlling behaviors, and possessiveness. This, too, used to serve a function. How good of function that was is debatable, but the point still stands. Portraying these traits as manageable, at the very least, was a way to prepare girls to be married away to someone who might not treat them the best. Stories managed to do this by reassuring them they could tame their new husbands. The whole “I can fix him” mentality evolved from this. Telling someone repeatedly that they can fix someone by making them fall in love with them tends to make them believe it. This somewhat common delusion results from centuries upon centuries of multi-generational gaslighting. Long ago, believing this could be seen as a form of copium since girls at the time usually didn’t have much of a say in who they got promised away to and were stuck with that person until one of them kicked the bucket. Nowadays, in all the places where girls and women, or those perceived as such, ain’t forced into relationships, this mentality causes nothing but trouble. It should go without saying that if someone doesn’t treat others well, they are not relationship material.
However, it’s worth noting that this has become less of an issue in recent years as there has been a decline in romance in pop culture, particularly in movies. There’s also been a rise in queer romances in more wide-reaching stories, and male/female relationships have gotten healthier depictions. Although a lot of those consist of people who are not straight, so they’re technically queer relationships too. The only place those outdated ideas consistently persist is in stories targeted toward people who are already used to those kinds of depictions.
Speaking of queer relationships, when it comes to fiction, they tend to avoid these issues. So, why is that? Well, for starters, despite what some bigots might say, it’s a lot harder to avoid being exposed to straight attraction than gay attraction. Many commercials are, in particular, needlessly straight. Also, there isn’t a precedent for two people of the same gender or anyone who isn’t perceived as a man and a woman to be obligated to get together. This leads to authors being less likely to either write or be asked to write a queer romance for the sake of it, which means that the romances in stories that feature queer relationships tend to be more deliberate. Then there’s the casual sexism that’s often brushed off in cishet romance that will more than likely come off as odd if it appeared in a romance between two people of the same gender. For example, it’s not too uncommon for one of the main characters in cishet romances to have had some unfortunate encounters with someone of a different gender, and the character does that thing where they think everyone within a group is the same. Try having a female character think that all women cheat without guaranteeing that it’s going to give someone pause. Unfortunately, internalized misogyny is very much a thing, but the point is that it’s not something people are just going to shrug off.
When it comes to how healthy queer relationships are depicted, it varies greatly from story to story, but when these relationships are extremely toxic, it’s rarely done by accident. There might be some cases where people who have internalized that guys show affection by easily getting angry and being controlling and possessive could see a man being abusive to another man and not see a problem with it. The stories themselves rarely seem to depict a toxic relationship as anything other than a toxic one.
Lastly, the main characters in queer romances rarely seem to be reluctant to spend time together. That’s not to say they always like these others from the get-go, but that one of them is more likely to contemplate murder than think about how they’ll have to be in the other’s vicinity for an extended period of time. If one or more of them has something against the other, it also tends to last only as long as it takes for them to get to know each other. These characters quickly grow fond of each other compared to their cishet counterparts. Forget about spending half a novel for one of them to find out they were wrong about the other; it usually takes a couple of conversations at maximum before they start to enjoy each other’s company. It’s not clear why this is, but it is hilarious to think about.
#queer romance#relationship representation#even when it comes to creating stories eugenics only makes things worse#yay for diversity
5 notes
·
View notes
Note
hiya, do you have any blanket advice for those looking to do some solid research into self-diagnosis, especially as an autistic? good sources, common mistakes, etc? would appreciate anything because I’ve just had a long few hours of mentally spiralling into the depths of hell over trying to figure out what empathy and remorse actually are
I have posts I will link at the end of this defining remorse that hopefully should help.
Empathy exists in 2 or 3 types, depending on who you ask. Most commonly, you will see 2 types of empathy being spoken about.
Affective empathy (the type people mean when they just say empathy): The ability to recognize other's emotions subconsciously without thinking about it/trying to, and having those emotions mirrored in your own. So (for pwAffective Empathy) if someone is angry, you will feel angry (not at them). If someone is crying, you may want to cry or start crying. If someone is smiling genuinely, you will feel happy. There isn't a qualifier on this. You don't have to know the person at all, let alone care about them, for this to happen if you have affective empathy, but afaik it is stronger in those you're bonded with.
Cognitive Empathy: Being able to intentionally think about "putting yourself in their shoes" and figuring out, based on what you would be feeling/others in previous situations felt, what the person is feeling. This is something that takes some amount of effort and is usually what pwLow/No Empathy learn to do to mask empathy.
The third, that is less talked about as a type of empathy:
Empathic Concern aka Compassion: Seeing someone in a tough situation or going through something that is upsetting (either to them or something generally considered upsetting like de*th) and feeling bad for them (also can include an urge to help them in some way or feeling bad you can't help them).
As for resources, I would say reading the DSM entries is always my first step in the long process of researching a disorder I think I may have. The DSM is thorough, if stigmatizing towards ASPD in some ways, and is the standard to which professionals are held in their diagnoses in the USA.
I also firmly recommend looking into anecdotal experience on tumblr, tiktok, etc etc (besides twitter which imo does not allow enough characters for nuanced discussion of mental health) to see if you relate to how the disorder tends to present. It's especially helpful to try and find pw any comorbid disorders you have talking about their experience. For example, I am AuDHD and have ASPD, which means my experience will be much different than someone with ASPD who does not have autism and/or ADHD. People try and discredit social media representation of mental health, to which I say "screw you, you just don't like that people with mental health disorders don't need to feel isolated and alone and shamed anymore". Obviously, take these as anecdotes, not guarantees on what the disorder looks like, but when you read enough of it, you'll get the vibe of what is controversial vs what most of the community with the disorder experiences.
Common mistakes: beware the loud minority/elitist assholes. There are people who are thoroughly convinced that no one with this disorder is allowed to look different than anyone else with it (Similar to people who say "you can't be autistic bc you don't act like my high support needs 5 year old autistic cousin"). There are people still using the word sociopath in an unironic way (and aren't just reclaiming it). These people will have you believe very ableist things they internalized. Notice them, block them, and move on from it.
Another common mistake is not reading into discourse about the disorder. Discourse can be stressful to read, but if you're looking into if you do or don't have a disorder, it can be very useful to see what is important enough to pw the disorder to be arguing about. You don't have to and maybe shouldn't pick a side while you're still questioning if you have it, but there is info to be gained in respectful discourse posts.
Maybe the most important: reading about stigma and ableism as tagged by people with the disorder. This will help you avoid falling into any internalized ableism and avoid getting blocked by informational accounts that could be beneficial to you learning. Do this before you post (or post again) about the disorder. Learn what is considered harmful, hurtful, ableist, and/or stigmatizing as far as the community of pw the disorder is concerned and keep it in mind in any future posts and irl discussions about the disorder.
Aside from that, I know a great post (not specific to ASPD at all) about the process of self diagnosis that I will link for you under the links to my posts about empathy and remorse. Linking specifically to a reblog with an important addition I touched on here.
I hope this helps!
Links:
It's worth noting that in this last link, OP (not Mental Illness Bingo) repeatedly remarks on it being annoying and/or inappropriate to ask blogs "do you think I might have this", and I personally disagree. That's just a me thing though. I cannot diagnose anyone as I am just a person with a (maybe somewhat worrying) amount of professionally diagnosed mental health conditions, not a professional. Even if I was one, I would not be able to diagnose you bc I am not your professional. I don't mind helping point people in the right direction if they feel I could be helpful though! I do agree that friends may be biased, and I know many other blogs have policies against answering that sort of ask, so know your audience if you ask. Just wanted to make that note here so no one things I'm vagueing them by linking that post. If I am uncomfortable with a certain type of ask, I'll make sure you guys know and probably add it to my pinned post.
Plain text below the cut:
I have posts I will link at the end of this defining remorse that hopefully should help.
Empathy exists in 2 or 3 types, depending on who you ask. Most commonly, you will see 2 types of empathy being spoken about.
Affective empathy (the type people mean when they just say empathy): The ability to recognize other's emotions subconsciously without thinking about it/trying to, and having those emotions mirrored in your own. So (for pwAffective Empathy) if someone is angry, you will feel angry (not at them). If someone is crying, you may want to cry or start crying. If someone is smiling genuinely, you will feel happy. There isn't a qualifier on this. You don't have to know the person at all, let alone care about them, for this to happen if you have affective empathy, but afaik it is stronger in those you're bonded with.
Cognitive Empathy: Being able to intentionally think about "putting yourself in their shoes" and figuring out, based on what you would be feeling/others in previous situations felt, what the person is feeling. This is something that takes some amount of effort and is usually what pwLow/No Empathy learn to do to mask empathy.
The third, that is less talked about as a type of empathy:
Empathic Concern aka Compassion: Seeing someone in a tough situation or going through something that is upsetting (either to them or something generally considered upsetting like de*th) and feeling bad for them (also can include an urge to help them in some way or feeling bad you can't help them).
As for resources, I would say reading the DSM entries is always my first step in the long process of researching a disorder I think I may have. The DSM is thorough, if stigmatizing towards ASPD in some ways, and is the standard to which professionals are held in their diagnoses in the USA.
I also firmly recommend looking into anecdotal experience on tumblr, tiktok, etc etc (besides twitter which imo does not allow enough characters for nuanced discussion of mental health) to see if you relate to how the disorder tends to present. It's especially helpful to try and find pw any comorbid disorders you have talking about their experience. For example, I am AuDHD and have ASPD, which means my experience will be much different than someone with ASPD who does not have autism and/or ADHD. People try and discredit social media representation of mental health, to which I say "screw you, you just don't like that people with mental health disorders don't need to feel isolated and alone and shamed anymore". Obviously, take these as anecdotes, not guarantees on what the disorder looks like, but when you read enough of it, you'll get the vibe of what is controversial vs what most of the community with the disorder experiences.
Common mistakes: beware the loud minority/elitist assholes. There are people who are thoroughly convinced that no one with this disorder is allowed to look different than anyone else with it (Similar to people who say "you can't be autistic bc you don't act like my high support needs 5 year old autistic cousin"). There are people still using the word sociopath in an unironic way (and aren't just reclaiming it). These people will have you believe very ableist things they internalized. Notice them, block them, and move on from it.
Another common mistake is not reading into discourse about the disorder. Discourse can be stressful to read, but if you're looking into if you do or don't have a disorder, it can be very useful to see what is important enough to pw the disorder to be arguing about. You don't have to and maybe shouldn't pick a side while you're still questioning if you have it, but there is info to be gained in respectful discourse posts.
Maybe the most important: reading about stigma and ableism as tagged by people with the disorder. This will help you avoid falling into any internalized ableism and avoid getting blocked by informational accounts that could be beneficial to you learning. Do this before you post (or post again) about the disorder. Learn what is considered harmful, hurtful, ableist, and/or stigmatizing as far as the community of pw the disorder is concerned and keep it in mind in any future posts and irl discussions about the disorder.
Aside from that, I know a great post (not specific to ASPD at all) about the process of self diagnosis that I will link for you under the links to my posts about empathy and remorse. Linking specifically to a reblog with an important addition I touched on here.
I hope this helps!
Links are above, and I have added plain texts to the ones that are mine as well.
#aspd-culture-is#aspd culture is#aspd culture#actually aspd#aspd#aspd awareness#actually antisocial#antisocial personality disorder#aspd traits#anons welcome
13 notes
·
View notes
Note
What made you detransition or rather how did you realize you no longer identify as such? /gen
Well basically I went to a gender therapist per the recommendation of my regular therapist (who fully believed I was trans but she didn't feel comfortable prescribing HRT considering her lack of experience in the field). I had about 20 sessions with him and at one point after about 8 he said that based on the criteria for gender dysphoria he was prepared to write me a prescription for HRT but he wanted to know that I was comfortable with it. I realized I wasn't because giving up the possibility of having biological children hit me like a huge truck. I am aware that some trans men can get pregnant but it's not a sure thing for everyone and also the idea of being perceived as a pregnant man made me very uncomfortable (back then I would have said dysphoric, in reality I'm sure it was just the social stigma), more uncomfortable than the idea of being perceived as a pregnant woman. I am adopted and I have seen firsthand how hard it was for my mom to not have her own bio kids. She still feels sad about it even though I am enough for her. I had always planned on having kids and went through a phase when I was 15 or 16 where I was researching pregnancy in-depth. This should have been another sign I was cis lol.
Anyway so I told my gender therapist I wanted to wait and have a couple kids with a likeminded bisexual cis man or trans woman and then transition. We then spent several sessions talking about other things entirely. In my mind I still identified as a closeted trans man for another year or so but I only told my boyfriend at the time who was bi so he didn't care and I un-came out to my parents - told them it was just a phase and they were relieved. :(
While I was dating that guy, I had a huge crush on a different cis guy who was straight. With this straight guy I would fantasize about having a straight relationship and straight sex, and eventually I did start dating him but didn't really feel the desire to come out to him as trans. I felt weird about having come out to my old bf and I wished that I could just pretend to be a cis woman again to everyone I knew. At some point it occurred to me that while the obvious explanation for this is that trans identity is stigmatized, many trans people do feel relieved when they come out regardless, especially to people that are as supportive as my boyfriend and friends were. It instead occured to me that I wanted to present as a cis woman because I WAS a cis woman but I was still kind of throwing ideas around in my head, not sure what was going on.
Then I happened to go on the subreddit for OCD and they had a bunch of subreddits for specific obsessions listed in the sidebar. I didn't know what /r/tocd stood for so I checked it out and it turns out there is a pretty common subtype of OCD based on the persistent idea that you're trans despite no evidence for this or pre-existing desire to transition (I think the sub is /r/transOCD now). I read through a bunch of posts on there and it basically explained everything I had gone through in the past few years. It was an OCD-based intrusive thought like my old ideas about having to do every problem in the math textbook or having to wear purple to open my crown chakra. Unfortunately this one was spurred on by a bit of social pressure like those posts that are like, "If you even are thinking about being trans, that means you're trans, cis people don't think about this shit" and egg memes on Reddit. Obviously there is also social pressure to NOT be trans but when you've filtered your social circle so stringently that it doesn't include any bigots and therefore anyone who would pressure you to not be trans, the pressure to accept it if you're thinking about it can be stronger in reality.
Like I'm sure that a lot of people who wonder if they're trans are the real deal, a much higher number than the general population, but people with OCD should stay far away from ideas like "If you think about X you are X." OCD makes you fixate on completely random things that have nothing to do with reality, they're not necessarily things you're afraid of, just because you fixate on being trans doesn't mean you're afraid of trans people or dislike them - it just means it's something that your brain has decided to latch onto because it's stuck in a horrible anxiety loop. Maybe I was afraid of being a man in women's spaces and the anxiety that unconsciously provoked in them, or of never coming across as feminine enough, or of my hypersexuality meaning that I was some sort of failed woman. There may very well be a rational root of the obsession but unfortunately TERFs and other people skeptical of trans people existing at all will take that and spin it to be an explanation for everyone who identifies as FTM. I'm sure a lot of trans men had similar feelings to me growing up in a lot of areas but the difference is that they have male brains and I simply don't, they're happier being men socially and physically as much as possible and I am happy with the opposite. So I hope no one takes my personal experience out of its personal context. If you have any more questions feel free to ask and sorry for the novel :)
4 notes
·
View notes
Text
'Is something wrong?' (generic) or 'Did I upset you?' (more direct) while not perfect, I feel like have a better chance of working instead of triggering a knee-jerk 'fuck off' answer. Maybe because these put the person less on the spot.
Let's say they really are angry. Moreover, lets assume the worse that they're mad at us. That sucks, but it happens. Friction is a normal thing in human relationships.
Now, being angry is an extremely vulnerable emotional state. When someone feels vulnerable, pointing that out will, most of the time, make them feel even more vulnerable. And what is one of the most common emotional responses to feeling vulnerable? Yep, jackpot! It's anger.
Other than that, anger is also very heavily stigmatized by society. Showing anger can get you labeled as aggressive, dangerous, abusive, or just straight-up evil. I'm pretty sure almost everyone treats their own anger with some level of internalized shame because of that. Being the first to lose your temper in a conflict will almost exclusively get you shamed for it, and anything others did that got you to that point will be most likely exempted for the sake of your taboo-braking act of showing anger. Angry people will be almost universally shown to be either aggressors, or just too childish to handle the situation as they should, but they almost never, ever will be seen as being right.
So, while wanting to know if you made someone angry is completely reasonable, and asking "are you mad at me?" is supposed to be the best course of action in a perfect world, in our imperfect world it's way too easy to read that as "are you victimizing me with your evil, aggressive emotions?" even if nothing like that even crossed our mind when asking it.
So yeah, if the goal is to de-escalate a tense situation with a loved one, which I'm assuming is the context of the original post, then it's best to avoid wording that points out that they're visibly angry, as it makes them feel less safe, and can evoke situations where they were seen as the bad guy before.
One thing we could ask which does none of that is "Did I do something (wrong)?" and that's already much better than "Are you mad at me?" But it has one flaw - while it has an 'I' it doesn't have a 'you', and thus it only emphasizes our perspective in the situation. Again, that's normal. We all experience life from a first-person view so it's natural that in most cases we want information regarding how things affect us, and how we affect other things. Putting ourselves into someone else's shoes is part of the everyday back and forth between human beings, but when someone is angry, and especially if they're mad at us, they will be much less inclined to view things from our perspective than usual, and asking them to do so might just make them want to end the situation altogether (hence, fuck off reaction)
So waaaaait... we can't emphasize them (since that makes them feel vulnerable and possibly judged) but we also can't emphasize ourselves (since that makes them feel ignored) so what we can say?
"Is something wrong?" is a pretty safe bet. It completely de-emphasizes the participants ('me' and 'you') and takes a holistic approach instead. Is something wrong in this situation? > Is there something we need to fix? >> (Preferably, together?) Zero judgement, maximum productivity - sweet! It's problem is that it's very generic and thus extremely easy to brush off
"Did I upset you?" is much harder to dodge but it's also much more of a gamble too. We're actually asking them here to admit how they feel - wait, wasn't that a big no-no before? Because we don't want them to feel worse and stuff?
Well yeah. But this approach does a lot to soften that blow. First, using the word 'upset' instead of 'mad' or 'angry' already makes it less likely to evoke judgement, even though that wouldn't do much against brushing off on its own.
The big thing here is that we're offering a fair deal. Yes, we ask them to reveal their emotional state to us - which is a big big investment of trust on their part. But we do invest about the same amount of trust in them by suggesting that we might be on the wrong. That's a pretty big thing in interpersonal stuff, even if it's just theoretical! And much more importantly, by framing it that way, we basically promise them a fair trial a healthy discussion where they won't be immediately cast into the bad guy box for the crime of feeling anger.
They should make a "are you mad at me" that is taken neutrally and informationally every time and doesn't make everything worse when you ask it
#tag#idk this post was one#maybe two paragraphs in my head???#i don't what happened and i have no idea how to tag this lol
84K notes
·
View notes
Text
childhood trauma stuff, reducing stigma and all that i guess
didn't want to put it in the tags of that last post bc op and such may not want to see that kind of stuff
but dang i did so much stuff online that was unhealthy and risky as a child in middle and high school. Teaching internet safety to kids is so important to me, I wouldn't want them to do the things I did.
But like, at least by 13 I was talking to adult men online and being very sexual with them. Mostly strangers, but one of them was this teacher I'd had at a computer camp that I started talking to online and had a crush on, and like, at 13 I had no understanding of why that was so inappropriate and damaging to me to be acting on that. I even convinced my mom to go to a store to meet up with him in person, while we were "dating."
My risky behaviors didn't just come out of nowhere. I couldn't manage to tell anyone about this next part until I was an adult, not even my therapist as a teenager-- I didn't think anyone would care, and I was too embarrassed, but not talking about it prevented me from getting help and it made me more vulnerable to being abused by others. Secrecy enables predators, and so the more we bring this uncomfortable stuff to light, the more we can protect each other from them.
But throughout pre-school, daily, I was sa'd by another child, and supposedly no one knew. One of the common symptoms from being sa'd is being hypersexual, but I don't think the adults around me knew that or if they did, didn't notice my behavior. I was also discouraged from talking about my body throughout life. Like, even when I was older and had a period for the first time, my mom just gave me the box of pads, asked if i knew how to use them (i lied and said yes because of the shame that'd been instilled) and that was it.
idk like, even with the metoo movement and the inches society is making toward de-stigmatizing victims talking about their own experiences, it's still hard to talk about it, which kinda means i should get more comfortable talking about it in a healthy way in order to reduce that shame.
Having worked through that trauma, I take all reasonable measures to protect my own kid from ever going through that while careful not to instill an anxiety in her about how she goes through life. Educating her so she knows about her own body and that she can talk about whatever, no topic being off-limits. Educating her about online safety as she starts to interact with people she doesn't know online in slightly less restricted environments. I make sure to check out the environments she'll be in-- my pre-school where I was assaulted had chaotic bathrooms, where there were a few stalls and teachers didn't supervise very well. So this boy was able to force me into a stall every day, and teachers either did not notice (like there were only 3 or 4 stalls, idk why) or didn't think it was a problem). Ugh, and my parents would leave me at his house or have him over on weekends, because they thought we were such good friends. So, when looking for schools, it was always an important thing that they had single person bathrooms where only one kid would be allowed in at a time. And I have to know adults well enough to be able to trust them to be alone with her.
It actually wasn't until I was choosing a pre-school for her that I told anyone what had happened to me. The family kept pressuring me to choose the same pre-school they'd sent me to, and I was like No, I am Not sending her there, imagine how guilty I'd feel sending her to the same place if the same thing that happened to me happened to her? No way. It hadn't even seemed that different, when I visited it again around that time.
Tbh, I don't blame the kid who harmed me; what he did was very likely a result of him having been assaulted, and passing that behavior on because he didn't know it was ok. Like, we were 4 or 5, I don't expect that level of understanding for a child that young. I do think the teachers I had were incredibly irresponsible and put that more on them, than anyone.
1 note
·
View note
Text
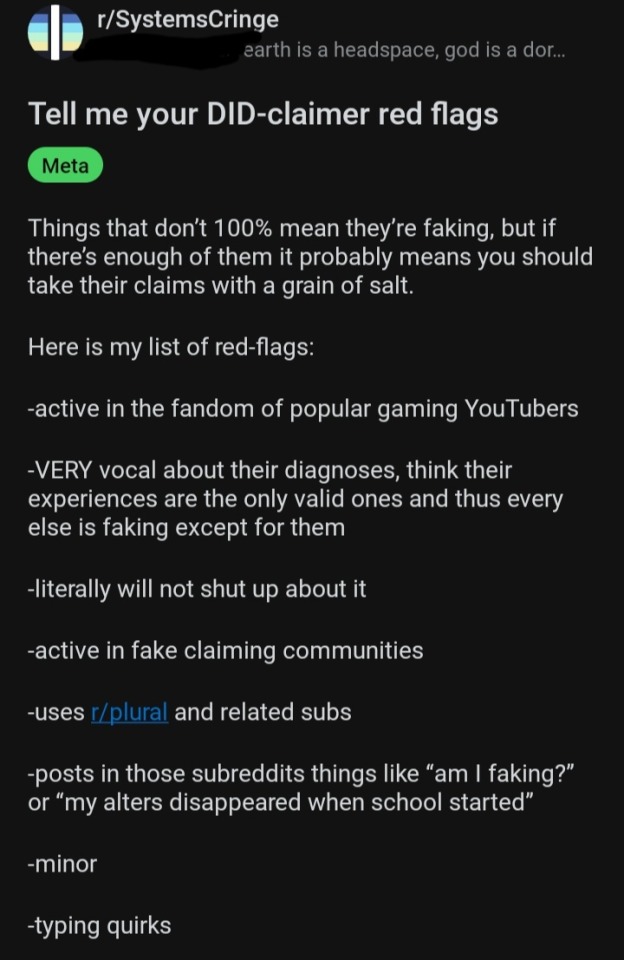

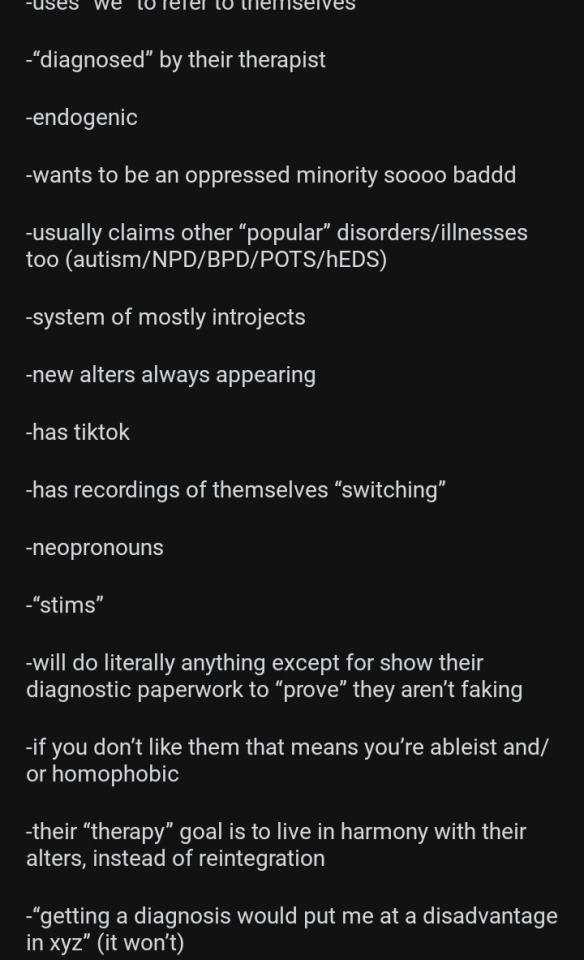

Saw this and it is genuinely one of the worst "DID red flags/DID faker signs" type post I've seen in a while and a few of these genuinely pissed me off so let's unpack these one by one!
!!! Long post !!!
Active in the Fandom of popular gaming youtubers
If it's a large Fandom, it's going to attract more fans. Which also means more disabled people will be in it. Including people with DID.
Certain youtubers yes it could be a red flag to be a fan of them. Isn't related to the person's DID though, it's about them choosing to support a shitty person.
VERY vocal about their diagnosises, think their experiences are the only valid ones and thus everyone else is faking but them
This one I do actually agree with! It absolutely is a red flag to use your diagnosis and how you experience your disorder to put down others!
Literally will not shut up about it
You are probably looking at an account made specifically to be open about DID. Because believe it or not, outside comparatively very small circles on the internet, DID is highly stigmatized. It is hard to find acceptance in real life, so some people go online to look for spaces they can talk about what they can't in the real world. Saying it is a negative thing actively hurts people with DID, because it says that them having spaces to freely exist is bad.
Active in fake claiming communitites
... you haven't been on r/systemscringe very long, have you?
Uses r/plural and related subs
Same point as the 3rd one: DID is highly stigmatized and people with DID are allowed to look for places they can talk about their experiences with DID.
Posts in those subreddits things like "am I faking?" Or "my alters disappeared when school started?"
The first one is actually a rather common thought for a lot of people with DID! For most people with the disorder, it is meant to be covert. Your brain doesn't want you to know you have it because it is trying to protect you from what caused it. So when you do recognize you have the disorder, it is going to try to push you back into denial because it doesn't want you to know you have it.
The second one, while how it is worded certainly could be a red flag as alters don't just disappear, alters seeming to be gone during stressful situations is also actually really common! The entire point of the disorder is to protect a traumatized child from their trauma and future trauma as best as it can. And by extention, it tends to see certain intense emotions as a warning sign, and will lock a particular alter in control to protect as much of the mind as it can from potential trauma.
Minor
It is a childhood trauma based disorder. Every person with DID was a minor with DID at some point.
Typing Quirks
Typing quirks should never have been associated together in the first place. Typing quirks are not a DID thing, or a system thing at all.
I do agree that if they don't have a translation it is a red flag though, it makes it difficult to impossible for multiple groups of disabled people to access.
Pastel or kidcore aesthetic
An aesthetic is not related to DID. At all. Two completely separate things. The only time either of these are a red flag is if the person is using the aesthetic to sexualize things related to children.
Medically recognized
Literally all this means is that a medical professional has agreed that you might have the disorder. Almost everyone now diagnosed at one point was medically recognized, because diagnosis is a process, not a single event.
Makes picrews of their alters
This is literally just like anyone else making a picrew of themselves. Someone making a little character of what they look like (or want to look like in some cases), is not a red flag. It is not uniquely wrong with someone with a specific disorder does this.
Ftm or nonbinary
.... do I even need to spell out how calling being trans a red flag is transphobic?
A-spec
Again, do I really need to spell out how calling someone's orientation a red flag is bigoted....
Dyed hair
See the point on kidcore & Pastel aesthetic: someone's style choices aren't related to any disorder.
Looks like they would microwave their hampster for tik tok clout
Based on physical appearance? No that's not a red flag, because physical appearance is not an actual indicator of what a person is like. Based on personality? Yeah it is a little concerning if that's what you get out of how someone acts.
Furry or furry adjacent
For the last time. People's style choices are not related to their disorder.
Likes east Asian media
Depends. If they're not Asian and like it to an almost obsessive or fetishistic degree, yeah, big red flag. If they're not fetishistic about it or literally Asian themselves? No. People are allowed to like media from other cultures.
I genuinely cannot read most of the next point so I'm not going to try to answer that for now
List of triggers never ends
Personally I think publicly listing triggers in general is a very bad idea, especially for people with disorders that could make them more vulnerable already. So I do for the most part agree with this point.
Probs mentions pro-shippers somewhere
If it's to tell them to stay away/not interact/etc. No. Again, not related to DID, and also a reasonable boundary to have. If it's in support of proshippers, still not DID related, but yeah definitely a red flag in my book.
Fujoshi
If you actually mean non mlm or nblm who fetishize mlm then yeah, that is a red flag. If you mean anyone who liked any mlm ship ever... yeah no. People are allowed to like gay ships. Gatekeeping who can like a ship based on the genders of the characters ends up just othering us.
Username contains words like system/collective/etc
Again, it is probably an account about DID specifically. Not necessarily a red flag for the reasons previously stated.
Uses we to refer to themselves
A lot of people with DID consider alters to be someone else, not themselves. So they see all of them as a group. It's grammatically correct to refer to a group using 'we' instead of 'I'.
"Diagnosed" by their therapist
In a lot of cases, yes. Most therapists cannot diagnose. Certain therapists who are also things like trauma specialists are licensed to, however. It just isn't very common.
Endogenic
I am going to stay out of this one for the most part, as no matter what I answer it will most likely drag me into an argument that detracts from the point of this post. However I do think it is a red flag to claim DID itself can be non traumagenic, it has been proven time and time again to be caused by trauma.
Wants to be an oppressed minority soooo bad
You know, on any topic, I always hated this point. Because nine times out of ten, the person doesn't actually WANT to be an oppressed minority. They just want their struggles as an actual minority to stop being dismissed.
Usually claims other "popular" disorders/illnesses too (Autism/NPD/BPD/POTS/hEDS)
I have a few points for this one.
One, a lot of disorders do actually make it more likely to develop trauma based disorders. Disorders like autism can lower the trauma threshold and make it more likely that dissociation is how the person copes. And disorders, especially physical disabilities, can cause trauma in and of themselves!
Two, these disorders can all be comorbid. Trauma disorders have high comorbidity rates with certain physical disabilities because the stress that caused those trauma disorders puts tangible, physical stress on your body and it's limits. And trauma disorders also have a very high comorbidity rate with other trauma disorders. It's pretty common to have more than one.
Three, NPD most definitely is not a "popular" disorder. Neither is BPD, in my opinion, although the amount of acceptance for it is higher than with NPD. NPD is quite literally one of the most heavily stigmatized disorders. There are articles after articles, entire forums and communities and more, built around calling people with NPD abusers. You look up NPD and you can find page after page after page telling how to spot a narcissist, how to psychologically damage a narcissist, how to hurt one. It is not by any means a "popular" disorder to have.
System of mostly introjects
Current generations literally have the highest amount of access to fictional media in all of recorded history. And when there is more access to fiction, more people will use it to cope. When more people use it to cope, it becomes more common for it to influence how people are. And DID is a disorder highly influenced and tailored by the specific individuals situation.
New alters always appearing
Again, another situation of a person's experiences being misinterpreted: a lot of the time "new" alters aren't actually new. Many alters are hidden from the person for days, weeks, months or even years before they are discovered. And sometimes they don't even realize how long they have been there, because they had no communication with any other alters. Having a poor perception of time is a very common symptom in most dissociative disorders.
Has tik tok
Someone with DID having a social media is not any more a red flag than someone without DID having it. The two are not related.
Has recordings of themselves "switching"
I do personally find this uncomfortable. Especially since, for a lot of people with DID, or OSDD, switching is often completely uncontrollable. A lot of the times it also is uncomfortable or even painful or stress inducing. I can understand how this could be a red flag, although it is not impossible for it to actually happen, especially if someone else is the one filming.
Neopronouns
Points to the previous point about how saying someone's transness is a red flag is transphobic
"Stims"
This one is a grey area. If they are romanticizing them, fetishizing them, treating them like they're cute, spreading misinfo, etc. Then yes. Just showing or talking about stimming in general though? No. That is an actual thing people do, especially people with disorders like ADHD and autism. Calling a symptom associated with disorders a red flag by itself is ableist and harmful to people with those disorders.
Will do literally anything but show their diagnostic paperwork to "prove" they aren't faking
Diagnostic papers are quite literally private medical information. Depending on how they are formated (differs from company to company), they also could include other private information that sharing online could put you in danger. Depending, showing these could literally get a person doxxed. Them keeping themselves safe online is not a red flag, and it is a red flag to demand someone risk their safety to prove their disability to you. Even employers are legally not allowed to demand this information in most cases.
If you don't like them you're ableist and/or homophobic
If said because someone doesn't like them as a person and as a serious thing, then yes. If said because the reason the person didn't like them was because of their orientation or disorder, or as a joke, then no.
Their "therapy" goal is to live in harmony with their alters, instead of reintegration
The thing you are trying to talk about actually has a name! It is called functional multiplicity. And it actually is not "not integrating", it still is a form of integration. Just like final fusion, the goal is to lower dissociative barriers and heal from childhood trauma over time. The only difference is the alters "fusing" or becoming one with one another, is not part of the treatment plan. Functional multiplicity is not the opposite of integration, it is a form of integration in and of itself. People with that goal still want to heal. They just don't feel that final fusion would benefit them. Both are goals approved by many actual professionals.
"Getting a diagnosis would put me at a disadvantage in xyz" (it won't)
Again, this is a grey area and highly depends on the individuals living situation and where they are.
If they are spreading misinformation, like the idea that employers in the U.S. all get to see your diagnosis (again, quite literally illegal for them to try to force you to give them that), then yes, red flag!
However there are certain things that in some places in the world, a DID diagnosis can make harder to access. For instance, it can be harder to get a driver's license in some places.
Additionally, depending on who the person is living with, it could be actively unsafe for them to be diagnosed. Again, in real life, DID is highly stigmatized.
Advocates for self dx
It really depends on how this is gone about. If they are encouraging people to do things like take quizzes or saying "if you do x you have DID" then yes this is a red flag! However, encouraging people to do actual research into the disorder is a good thing! People realizing they have symptoms of something can majorly help them! So can educated self dx, in some cases. It can help them access spaces with resources for people with symptoms like theirs, it can help them learn ways to cope with their symptoms specific to that disorder, it can help them know what to tell their psychiatrist they suspect is going on, and a lot more!
Alters are fully fleshed out characters
Honestly this is another one that rather pissed me off. Alters are not "characters". People with DID are not fictional. These are actual people. As for them being more "fleshed out"... that's part of the point. Again, these are real people. They are going to be complex. Yeah it's rare for ALL alters to be that complex, but the existence of any alters or even multiple alters who are is not a red flag. Distinctly different alters is quite literally one of the symptoms that sets DID apart from other dissociative disorders, like OSDD-1.
Sign offs with alter names
Someone with DID trying to decrease confusion for themselves and those around them is not a red flag by itself. It is literally to help themselves. It is a lot easier to deal with memory barriers if you can look and see something physical telling you what happened and who did it.
Headspace "maps"
Again, this is usually done to help with memory barriers. For a lot of people, DID or not, physically making something to show you what is going on in your head makes it easier to understand for you. Trying to help yourself deal with a damaging symptom of your disorder by giving yourself something to lay it all out is not a bad thing.
Well that was All! Hope that makes sense and cleared some things up.
And before anyone tries to use this to say I'm faking DID: I do not have DID.
239 notes
·
View notes
Text
The difference between Mike and Will’s internalized homophobia
after the one-page script drop yesterday regarding the van scene, it’s easy to take notice that there is more to be unpacked with will as a character, even if it isn’t something we haven’t figured out already. and not to mention mike, who didn’t (suspiciously) have much light shed onto his perspective. so, let’s talk about it!
will is our only canonically gay male character as of now, and i think a lot of people used to gloss over the fact that he does in fact have internalized homophobia just because he has (as well as others) acknowledged his homosexuality, however explicit it may be. will’s sexuality has been very dubious as early as season 1, only just being confirmed recently, without the help of his unsupportive home town and his father in particular. from an early age, his father was already shaming him for his “girlish interests” and calling him names and such. this, accompanied by unkind remarks from classmates throughout his childhood, doesn’t create a healthy outcome for the way will thinks of himself.
will’s experience as a queer person is unfortunately common, which makes the execution of his storyline all the more important. being surrounded by such judgmental and maybe even aggressive views towards queer people is mentally weighing, so it’s no surprise when these negative feelings are turned in on themselves. will’s internalized homophobia isn’t so much about repression, but more of a self-hatred from a lack of inwardly tolerance. will is conscious about his homosexuality, but he accepts societal biases as his own because it’s all he’s known to do. he doesn’t actively try to do anything to make it “go away” while also settling with the idea that he is not allowed to be happy with who he is.
mike is different—while his home life wasn’t necessarily bad, he lacks the emotional support a child requires from the parent(s) (specifically from ted). using context, we can say that his family is inherently conservative so it’s likely he was raised with tainted worldviews (again, mostly having to do with ted). his tendency to bottle up emotions until it all unravels at once is a result of this. naturally, mike keeps these feelings hidden deep down.
unlike will, mike’s internalized homophobia is unconscious, so he represses. heterosexism is another broad term used to describe internally homophobic behaviors, like being unable/unwilling to acknowledge their own sexual orientation and trying to fit heteronormative standards. sound familiar? in a sense, mike moreover “ignores” his same-sex attraction whether he’s aware of it or not. his biases lie a bit more in the “heterosexual = normal” area by a default because it was what he was raised to believe. he should feel ashamed for feeling anything out of the ordinary and that can lead to a fear of others labeling themselves as gay, which then leads to projection (byler rain fight anyone?). he feels threatened but he’s not sure why.
to conclude, the poor boys have fallen victim to society’s rather negative perceptions and have ultimately become stigmatized. someone give them a hug good lord.
#i was gonna upload earlier but i’ve been in the city all day i’m so tired💔#i hope this makes sense#byler#will byers#mike wheeler
34 notes
·
View notes