#The representation of the spectrum
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Premium Tumblr themes are available from anywhere between $9 to $49.
Text
I love that ace representation ranges from this QUEEN

to this THING

#The representation of the spectrum#helluva boss#stolas#blitzo#blitzø#Helluva#octavia#mammon#loona#asexual#ace
116 notes
·
View notes
Text
Writing a Schizophrenic Character: Everything But Hallucinations
Plain text: Writing a Schizophrenic character: Everything But Hallucinations
Hey! Mod Bert here.
So: you’ve decided to write a character with schizophrenia or schizoaffective disorder (there are other disorders on the schizophrenia spectrum but I will be focusing on these for today)
You’ve done it, you have their hallucinations and maybe even delusions picked out. Maybe they are one of many who experience auditory hallucinations or maybe they also have visual hallucinations or a combination. Maybe they have olfactory hallucinations as well. They may have persecutory delusions or delusions of reference or something like Cotard’s delusion or clinical lycanthropy. Awesome, you’ve done it!
What, I hear you say? What do you mean that’s only 2 of the 5 components needed to be diagnosed with schizophrenia? What do you mean, you don’t need to hallucinate at all to be schizophrenic?
What Goes Into a Diagnosis of Schizophrenia
Plain Text: What goes into a diagnosis of schizophrenia
Not a lot of people realize there’s more to schizophrenia and schizoaffective than just hallucinations or delusions. There are 5 diagnostic criterias that are needed for schizophrenia, and only 2 of the 5 are needed for a month, with larger symptoms happening for six months or more. Let’s get into it.
Delusions
Hallucinations
Disorganized speech or thinking*
Disorganized or unusual motor behavior (catatonia)*
Negative symptoms (avolition, anhedonia, flat affect)*
I’m going to focus on disorganized speech/thinking, catatonia, and negative symptoms.
Disorganized Speech/Thinking
Plain Text: Disorganized Speech/Thinking
Schizophrenia and related disorders are often called “thought disorders” for a reason. Speech and thinking can be extremely affected, and for people like me this can be one of the first and most striking examples of an episode coming. Some people will always have disorganized symptoms that will flare during episodes. A myth is that schizophrenia can be indistinguishable with medicine: most people will have some level of symptoms even during moments of peace or “remission”. More on remission later.
So, disorganized speech. Some examples are: word salad (schizoaphasia), thought blocking, poverty of speech (alogia), pressurized speech, clanging, and echolalia.
Word salad: a combination of words that do not make sense together. Often called schizoaphasia for its similarity to jargon in Wernicke’s aphasia, this is instead a disconnection with the brain and not due to damage to the language part of the brain.
(Example: the salad would be yellow in the fat cow).
Thought blocking: A severe loss of thought, often paired with connecting two trains of thought that are not connected
(Example: I went to the………Do you like grapes?)
Poverty of speech: A lack of organic responses to speech or organically speaking, it can be severe enough that a person only responds to questions or in one word responses. Can also happen in severe depression.
(Example: Person A: Did you do anything fun today?
Person B: Yes.
Person A: Oh, what did you do?
Person B: Store
Person A: How was it?
Person B: Fun)
Pressurized speech: A sort of frenzied way of speaking associated with psychosis or mania.
Clanging: Connecting phrases together because of what they sound like instead of meaning
(Example: I went bent tent rent).
Echolalia: Repeating word’s and phrases. Commonly also associated with Autism Spectrum Disorder.
(Example: Person A: I went to the store.
Person B: To the store.)
These are not the only examples but they are some ones I thought I'd highlight, either because they’re well known or I have experience with them, or because they’re famously thought of with other disorders as well and I wanted to point out how things overlap.
Personal experience: I had severe alogia for the duration of my last and worst episode. People thought I was mad at them because of the clipped way I spoke and the lack of really speaking. It got me in a lot of trouble. I didn’t realize what I was saying was different or weird (I have the least insight when it comes to my speaking patterns affected by my schizoaffective, meaning I can’t hear any difference and all of this is from repeated conversations with my mom, who was my caretaker for a bit and knows the most about my speech and what it means). The best solution was talking with people and being honest and educating myself and others. I don’t know about others, but I couldn’t have used AAC at that time.
Catatonia
Plain text: Catatonia
Fun fact: catatonia means unusual motor behaviors! Any unusual motor behaviors mean catatonia. This includes what we think of when we think of catatonia in schizophrenia (inability to move) as well as the opposite (being unable to stop moving) as well as strange movements and ways of holding and moving the body! Catatonia in the DSM-5 includes 3 or more of these 12 behaviors:
-Agitation unrelated to external stimuli
-Catalepsy
-Echolalia
-Echopraxia
-Grimacing
-Mannerism
-Mutism
-Negativism
-Posturing
-Stereotypy
-Stupor
-waxy flexibility
I have some experiences with catatonia-like symptoms but since they were never identified as such I’ll skip those for now. I will say that catatonia is a symptom that can happen in many disorders besides schizophrenia as well.
Negative Symptoms! Yay!
Plain text: negative symptoms! Yay!
So a positive symptom (Hallucinations or delusions) are symptoms that add something to reality or a person. Negative symptoms are symptoms that take away. There are 5 A’s:
-Alogia (Again, poverty of speech, our favorite)
-Avolition (Lack of energy and motivation)
-Affect (Blunted affect, or a flat way of speaking)
-Anhedonia (Lack of pleasure in things that used to bring you pleasure, often thought of with depression)
-Asociality (Lack of interest in social events and relationships)
There are also often cognitive changes including thinking and memory, information recall, understanding, and acquisition, and so forth.
Schizophrenia and schizoaffective often (but not always) happen with what’s called a prodromal period. This period can be months to years (mine was a little less than a year) and mainly consists of negative symptoms. Slowly, positive symptoms are added. There are thought to be stages to schizophrenia including prodrome, active phases, and remission.
I’ll talk about that a little for a second because I’m currently in remission and no one knows what that means. I was diagnosed with schizoaffective depressive type in January 2021. As of February 2024, I no longer qualified to be rediagnosed because my symptoms were strongly under control and no longer severe enough to qualify for a diagnosis. They also didn’t distress me or impact my daily life severely. Day to day now I still have mild symptoms and take my antipsychotics (trying to go off them have made it clear that I still have some symptoms I choose to keep medicating) but I haven’t had a delusion in 2 years and been hospitalized in 3. There’s always a possibility of another episode but I work with my team to keep myself one step ahead if that happens.
What I want from a character with schizophrenia
Plain Text: What I want from a character with schizophrenia
Alright the writing advice part. What do I want from a character with schizophrenia or schizoaffective (which is schizophrenia plus either depression or bipolar).
-Characters with caregivers.
-Characters using coping strategies (recording hallucinations to tell if theyre hallucinations, taking medication, having service animals that greet people so they know if they’re a hallucination, using aids for the cognitive symptoms like sticky notes and organizational tools)
-Characters who know other characters with their disorder, either online or in support group or through running in similar circles
-Characters having autonomy
-Characters who aren’t the killer or horror victim. I know it’s cool to have the schizophrenic protagonist in horror, and I love horror, but I don’t want to read about the horror being symptoms the whole time
-Characters who are in magical scenarios, who are in fantasy and sci-fi. The schizophrenic princess and the schizoaffective robot technician aboard the spaceship.
-Medication and hospitalization treated casually. Sometimes we need higher care. That’s morally neutral
-Characters with negative symptoms and speech symptoms.
-Characters with catatonia!
-Characters with other disorders as well
-characters with side effects from medicine treated casually
-Characters with cognitive symptoms
Thank you for reading this incredibly long thing! Happy writing!
3K notes
·
View notes
Text
if I see one more “straight people on the aromantic and/or asexual spectrum don’t count” I will personally light shit on fire
If you’re heterosexual and aromantic, you’re valid. If you’re asexual and heteroromantic, fuck yeah, you’re valid too. You belong here, in LGBTQIA+ spaces, and I love and accept you here. You belong at the pride parade, you belong in the LGBTQIA+ clubs at your school or university, and you belong in the LGBTQIA+ community.
We love you. You belong. anyone who says otherwise can go fuck themselves.
#asexual#acespec#arospec#aromantism#aro#aspec#asexual awareness week#asexual pride#asexual positivity#asexual representation#asexual spectrum#aromantic#aromantic asexual
3K notes
·
View notes
Text
i will always dislike the stereotype that cisgender men are just beings who only think / care about sex, so my cis men out there who are asexual or just genuinely don't think sex is that important, you are seen and will always be valid :D /gen
#tw sex mention#cisgender#cis man#cis male#cis men#cis#asexual community#asexuality#asexual#asexual positivity#asexual pride#asexual representation#asexual spectrum#actually asexual#ace stuff#ace pride#acespec#ace positivity#ace rep#ace representation#ace spec#ace spectrum#ace umbrella#ace#pride#queer#lgbtq#lgbtqia+#lgbtq+ community#lgbt community
2K notes
·
View notes
Text










Autistic Animated Character Appreciation Post
#autistic representation#luz noceda#the owl house#june chen#the ghost and molly mcgee#dib membrane#invader zim#hank venture#the venture bros#mabel pines#gravity falls#tina belcher#bobs burgers#sterling archer#archer#fred jones#scooby doo mystery incorporated#rick sanchez#rick and morty#deadpool#ultimate spider man#autism#its a spectrum#I wanted to include Ron Stoppable so badly#but I was like nah one will friedle character mention is enough
250 notes
·
View notes
Text
Intersex Guide! (Updated 5/28/2025)
(UPDATED: May 28th, 2025. Please reblog again if you only saw our old versions. Please also reblog if you've never seen this before, to spread awareness.)
Hello and happy pride! We wished to share a passion project we have been working on for months - a guide to intersex traits and variations!
Now, a question that many ask - what is intersex? Well, we will be answering that question for you here! Anything on this post that is written in red is NOT intersex, so if you wish to skip over any of it, you can. And if you wish to get straight into the intersex types, scroll down to the read-more and start from there.
Intersex, also known as The Intersex Spectrum, is a term used to describe when someone's biological sex - as in the sex they are born with/what they naturally develop during puberty - is not clearly aligned with the typical perisex/endosex/dyadic (wolffipathian or mulleripathian) sex traits.
(Note: Wolffipathian is a term to mean "the male sex", while mulleripathian is a term to mean "the female sex." They were created in order to separate the male & female gender from sex, as calling people "males" or "females" could be misgendering them.)
(Intersex does not include someone that is wolffipathian or mulleripathian, and later chose to have their sex traits changed due to being transgender, transsex, or altersex. It also does not include wolffipathians that experienced circumcision/dorsal slits or penis splitting, mulleripathians that experienced genital mutilation, or wollfipathians & mulleripathians that indulged in modifications such as piercings and beading.)
This only applies to primary sex traits - chromosomes, genitals, reproductive organs, hormones, and hormone responsiveness. Atypical secondary sex traits (breasts, muscle tone, body/facial hair, deepness of voice) do not make someone intersex unless it is paired with "abnormalities" in primary sex traits.
Before you can understand what it means to be intersex, first we must clarify what it means to not be intersex.
A typical wolffipathian has XY chromosomes, a moderate (or large) penis, two moderately-sized testicles within the scrotum, an average-sized prostate, two vas deferens, two average-sized seminal vesicles, and (without the influence of HRT) more androgens (mostly testosterone) than mulleripathians. Their androgen levels fall into a typical range compared to other wolffipathians. Upon puberty, they usually experience an increase in muscle mass, higher amounts of body/facial hair, and a deeper pitched voice - however, these traits can vary based on genetics and race, and aren't guaranteed.
Note: A penis has a phallus, a scrotum beneath the phallus, foreskin protecting the head of the phallus, and a urethra on the tip of the penis. It is straight or slightly curved when erect.
A typical mulleripathian has XX chromosomes, a vulva, two average-sized ovaries, a single average-sized (or large) uterus, two fallopian tubes, and (without the influence of HRT) more estrogen than wolffipathians. Their estrogen levels fall into the typical range compared to other mulleripathians. Upon puberty, they usually (but not always) grow breasts, have widened hips, lesser amounts of body/facial hair, and a higher pitched voice - however, these traits can vary based on genetics and race, and aren't guaranteed.
Note: A vulva has two labia, a single pea-sized clitoris, a single moderate (or deep) vaginal entry, and a urethra above the vaginal entry and under the clitoris.
Here is a list of non-typical sex traits that, by themselves, are not intersex.
Accessory Breasts (Polymastia): Having more than two breasts. Accessory Nipples (Polythelia): Having more than two nipples. Athelia: Having only one nipple, or no nipples at all. Amastia: Having only one breast & nipple, or no breasts & nipples at all. Breast Hypertrophy/Macromastia/Gigantomastia: Having extremely large breasts Gynecomostia: Breasts on a wolffipathian. The reason this is not considered intersex is because all sexes (except for people with amastia) have breast tissue, which can vary in size regardless of sex. Mulleripathians can have small breasts, and wolffipathians can have larger breasts than is expected. Hypotonia: Low muscle tone. Bicornuate Uterus: A heart-shaped uterus. There are exceptions where this diagnosis is considered intersex, if the two sides of the uterus are distinct enough to be two separate spaces (in which case, the term uterus didelphys - which is discussed in the reproductive traits segment - would be more fitting.) Septate Uterus: A uterus that internally has a partition down the middle. There are exceptions where this diagnosis is considered intersex, if the two sides of the uterus are split enough to be two separate spaces (in which case, the term uterus didelphys - which is discussed in the reproductive traits segment - would be more fitting.) Retroverted Uterus: A uterus that is rotated differently than typical. This can sometimes cause a vagina (if one is present) to curve a bit as well. Macropenis: A penis that is 7 inches/17.78 centimeters or larger. Macroorchidism: Testicles that are 4 milliliters or above pre-puberty, and above 30 milliliters as an adult. Macrovagina: A vagina that is deeper than 5 inches/13 centimeters. Labial Hypertrophy: Labia that is longer than average (above 2 inches/5 centimeters)
Now, onto the intersex spectrum! First, some notes.
-An intersex trait is a singular atypical trait. For example, someone with ambiguous genitals, but no other "abnormality" has an intersex trait. -An intersex variation is when multiple atypical traits are present, with at least one of them being an intersex trait. For example, someone with ambiguous genitals and fused kidneys has an intersex variation. Equally, someone with ambiguous genitals and cryptorchidism also has an intersex variation. -CTF stands for "close to female." CTF traits are characteristics that are closely associated with mulleripathians (vulvas, uteruses, ovaries, estrogen as the main sex hormone, breasts, widened hips, XX chromosomes, etc.) CTF people are intersex people who call their body as a whole CTF, due to a majority (but not necessarily all) of their sex traits being CTF (ie; a person with breasts, a uterus, ovaries, and a penis might call themself CTF, even though not all of their traits are CTF in nature.) -CTM stands for "close to male." CTM traits are characteristics that are closely associated with wolffipathians (a penis, testicles, androgens as the main sex hormones, increased hair growth, higher muscle mass, a deepened voice, XY chromosomes, etc.) CTM people are intersex people who call their body as a whole CTM, due to a majority (but not necessarily all) of their sex traits being CTM. -CTA stands for "close to androgynous." CTA traits are characteristics that are predominantly "androgynous", or an equal mix of "feminine" and "masculine" (ie; ambiguous genitals, ovotestes, XXYY chromosomes, etc.) CTA people are intersex people who call their body as a whole CTA, due to a majority (but not necessarily all) of their sex traits being CTA, or they have a near-equal mix of CTF and CTM sex traits. -CTN stands for "close to neutral." CTN traits are characteristics that are predominantly "neutral" (ie; small/absent/blocked off genitalia or reproductive organs, a lack of hormone production, 0X chromosomes, etc.) CTN people are intersex people who call themself CTN, due to a majority (but not necessarily all) of their sex traits being CTN.
Also, when we state that an intersex trait/variation is "fairly common", we mean that it is fairly common amongst the intersex population, not that it is fairly common in the general population. Being intersex is still classified as "rare" statistically speaking (as statistics define "rare" as 1 in 1,000 people.)
So for the sake of this post, here is how we are classifying the following:
"Fairly common" = 1 in every 5,000 (or less)
"Rare" = above 1 in every 5,000, up to 1 in every 100,000
"Extremely rare" = above 1 in every 100,000
Keep in mind that "may co-occur" means that not all of the features will be present on every single person with that variation; in fact, none of the extra features could be present. However, for chromosomal variations specifically, it is highly likely that at least 1-5 (or more) of the listed extra features will be present.
And finally, when we say that "fertility is average", what we mean is that the gonads are fully capable of producing healthy average numbers of sperm/eggs, and/or the uterus is capable of carrying healthy babies. Struggles with the sperm reaching the eggs still might occur, but if direct insemination is done (as in the sperm is directly injected), then pregnancy should occur perfectly fine.
-------------------
Penile Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the penis.
Congenital Chordee: An trait in which an individual is born with a curved penis. This curve may be on its own, or it may be curved due to webbed-skin on the scrotum connecting to the penis and holding it in a curved manner. As a lone variation, those with congenital chordee have XY chromosomes, testicles, and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 200 AMAB births.
-
Penoscrotal Transposition (PST): A trait in which an individual is born with a scrotum that is in front of the penis, rather than beneath it. A Shawl Scrotum/Donut Scrotum is a form of PST where the scrotum completely surrounds the penis like a shawl. As a lone variation, those with PST have XY chromosomes, testicles (possibly cryptorchidism, in which case the scrotum surrounding the penis is full of empty tissue), and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include absent kneecaps, ureter abnormalities, an absent or underdeveloped kidney, heart disease, overgrown/protruding ribs, widely-spaced nipples, an incurved pinkie finger, a small lower jaw, a chin dimple, folded eyelids, a large/protruding back of the skull, cerebral atrophy, and intellectual disability.
-
Diphallia/Bifid Penis: A trait in which an individual has two penises (either next to each other or one on top the other.) These penises could be of the same size, or have a size difference. A urethra may be present on only one penis (possibly with epispadias or hypospadias), both penises, or they may have a single urethra that is in-between both the two penises. Erections may be possible in both penises or only in one. As a lone trait or variation, those with diphallia have XY chromosomes, testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include pubic bone abnormalities, an extra hole (not an anus) that leads into the rectum, an absent anus (which will need surgical intervention in order to pass waste), two colons, an extra ureter, fused kidneys, an extra kidney, a rotated kidney, an inguinal hernia, gastrointestinal abnormalities, an extra gastrointestinal tract, exposed organs on the lower abdomen, heart abnormalities, spinal abnormalities, and an absent thumb.
-------------------
Urethral Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the urethra.
Urethral Duplication/Double Urethra: A trait in which an individual with a singular set of genitals has two urethras. One of the urethras may not fully reach between the bladder and genitals, either cutting off before reaching the bladder (making it visible from the outside, but without a use), cutting off before reaching the genitals (making it connected to the bladder, but not visible or accessible from the outside), or cutting off in the middle (making it connected to the bladder, and visible from the outside, but a blockage existing somewhere in the middle internally.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (usually with epispadias for one or both of the urethras, however the urethras could be side-by-side as well) or clitoromegaly & fused labia, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis (usually with hypospadias or epispadias for one of the urethras, though both can be side-by-side on the penis head), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status of this variation, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include recurring urinary tract infections, an extra ureter, an extra bladder, an extra rectum, an extra colon, an absent kidney, an abnormally-located kidney, kidney cysts, spinal abnormalities, and an opening between the windpipe and the esophagus.
-
Hypospadias: A trait in which an individual with a penis is born with a urethra that is located lower than typical. This could be lower on the head of the phallus than typical, or it could be on the shaft, the scrotum, or even underneath the phallus. As a lone variation, they have XY chromosomes, a penis/micropenis (possibly with chordee or PST), testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 250 AMAB births. Vulval Hypospadias/Hypospadias Feminis is an extremely rare form of hypospadias that occurs on vulvas, in which a urethra opens lower than typical, possibly on the vaginal wall (meaning it may appear as though an individual is urinating out of the vagina.) As a lone variation, those with vulval hypospadias have XX chromosomes, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the rarity, little is known about the fertility status of vulval hypospadias. A common trait/disability that may co-occur (for both forms of hypospadias) is recurring urinary tract infections.
-
Epispadias: A trait in which an individual is born with a urethra that is located higher than typical. On a penis, this refers to a urethra that is located above the typical spot on the penis head. Ona vulva, the urethra is on the stomach or above/in the middle of the clitoris (thus splitting the clitoris into two.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is extremely rare. Common traits and disabilities that may co-occur includes recurring urinary tract infections and exposed organs on the lower abdomen.
-
Urogenital Sinus Anomaly (UGS)/Persistent Urogenital Sinus Anomaly (PUGS): A trait in which an individual has a single opening, which is a combination of both urethral and vaginal tissue, and connects to both the urinary tract and the reproductive tract. This opening could be the size of a typical vaginal entry, the size of a urethra, or somewhere in-between. As a lone variation, those with UGS have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare. A common trait/disability that may co-occur is recurring urinary tract infections.
-
Persistent Cloaca: A trait in which an individual has a single opening for urination, menstruation/sexual output, and feces (being a combination of the urethra, vaginal entry, and anus.) This opening could be the size of a typical vaginal entry, the size of a urethra, the size of an anus, or somewhere in-between. It could be placed anywhere from the crotch to between the buttocks, or somewhere in the middle. Partial cloacas may occur as well, in which the anus and the vagina are combined but the urethra is still separate, or the anus and the urethra are combined but the vagina is still separate. As a lone variation, those with persistent cloacas have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/one ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. If they have a uterus and a partial cloaca, they may have a double cervix, with one cervix in each opening. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare. Common traits and disabilities that may co-occur include recurring urinary tract infections, a dilated colon, a dilated vaginal entry, urine buildup (which may cause a stretched/swollen kidneys or ureter), an absent kidney, an abnormally-located kidney, heart defects, a tethered spinal cord, and an underdeveloped esophagus.
-------------------
Ambiguous Genitals
These are traits in which a person was born with a combination of vulval and penile characteristics. Micropenises are often considered a part of this spectrum.
As a lone trait, this can come in a androestrogenized, estrogenized, or androgenized form.
The androestrogenized form can have any mix of gonads, reproductive organs, hormone production, and puberty. Typically they either have XX or XY chromosomes, however occasionally they may have a chromosomal variation as well.
Those with the estrogenized version have XX chromosomes, two ovaries (or ovotestes), and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips.
Those with the androgenized version have XY chromosomes, testicles (or ovotestes) and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice.
Ambiguous genitals are fairly common, occurring in 1 of every 5,000 births.
Bifid Scotum: A form of ambiguous genitalia where a penis is present, however the scrotum is separated in a labia-like fashion around the phallus. Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia is fused in a scrotum-like fashion. The fused labia either covers the entirety of the vulva (leaving only the clitoris) exposed, or half of the vulva (leaving the clitoris & urethra exposed, but the vaginal opening mostly or fully hidden.) There may be tissue within the labia that appears like small testicles. Clitoromegaly: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged, being over 1 inch (2.54 centimeters) in diameter. In some cases, it looks like a small penis. Combined Clitoromegaly & Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia fuses to resemble a scrotum and the clitoris is enlarged, creating a structure almost identical to a small penis. The vaginal opening is fully hidden under the labia. Pseudophallus: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged significantly (beyond the typical clitoromegaly expectations) and is merged with labia, creating a significantly-sized penis-like structure. Penis & Vulva Combo 1: A form of ambiguous genitalia where a vulva is present, however the labia stretches up and merges with a penis, becoming the outer skin & foreskin of the phallus. The penis is located where the clitoris usually is (thus replacing the clitoris.) No scrotum or descended testes are present. The urethra is on the vulva, below the penis. There is also a vagina beneath the phallus. The vagina is likely to be shallow (vaginal hypoplasia) and/or the penis is likely to be small (micropenis.) Penis & Vulva Combo 2: A form of ambiguous genitalia where there is a penis (with no scrotum or descended testicles) that has a vulva underneath it. The vulva has labia, which is attached where the scrotum usually would be, and a vaginal opening beneath the phallus. It may or may not also have a clitoris attached to the penis as well, stretching from the glans. The urethra is on the vulva, below the penis. The vagina is likely to be shallow (vaginal hypoplasia) and/or the penis is likely to be small (micropenis.) Penis & Vulva Combo 3: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles), labia stretching from the scrotum, and a vaginal opening beneath the phallus. There is never any clitoris. The urethra can either be on the tip of the penis or on vulva beneath it. The vagina is likely to be shallow (vaginal hypoplasia) and/or the penis is likely to be small (micropenis.) Penis & Vagina Combo: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles) that a vaginal entry tucked beneath the scrotum. The vagina is likely to be shallow (vaginal hypoplasia) and/or the penis is likely to be small (micropenis.)
It is important to note that the term Clitorophallus is often used as an umbrella term to describe micropenises, clitoromegaly, combined clitoromegaly & fused labia, and pseudophalluses.
-------------------
The Agenital Spectrum/Agenital/Agenitalia
These are traits in which a person was born with absent, small, or closed off genitals. Anorchia & Monoorchidism fall under this umbrella as well.
Urethral Agenesis: A trait or variation in which an individual is born without a urethra. It may be visibly absent, or it may appear to be present from the outside, with a blockage of skin being within the first few centimeters or inches internally. A urethra is necessary to be surgically added, as to avoid urine buildup. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include limb deformities, an anus covered by skin (which will need surgical intervention in order to pass waste), urine buildup (which may cause a stretched/swollen kidneys or ureter), an abnormal connection between the bowel and bladder, an absent bladder (which will need surgical intervention in order for urine to have somewhere to be collected), a small kidney, kidney cysts, an underdeveloped lung, an enlarged chamber of the heart, and heart issues.
-
Urethral Hypoplasia: A trait in which an individual is born with a narrow or underdeveloped urethra. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is rare.
-
Vaginal Hypoplasia: A trait in which an individual has a vaginal opening that is small/tight or not very deep. As a lone variation, those with vaginal hypoplasia have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 5,000 AFAB births.
-
Vaginal Agenesis/Vaginal Aplasia: A trait in which an individual has some or all of the external vulva (clitoris, labia, & urethra), but no vaginal opening. As a lone variation, those with vaginal agenesis have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry. Pregnancy is possible if they have a uterus that is present and large enough, however sperm will need to be medically injected (unless they have a vaginal entry created surgically.). If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 4,000 AFAB births.
-
Imperforate Hymen: A trait in which an individual has a hymen that completely covers the vaginal opening. As a lone variation, those with imperforate hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. Pregnancy is possible, however embryos will need to be medically implanted (unless they have the hymen removed surgically.) This trait is fairly common, occurring in 1 of every 1,000 AFAB births.
-
Microperforate Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only one tiny hole in the hymen. Cribriform Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only multiple tiny holes scattered across the hymen. Septate Hymen: A trait in which an individual has a hymen that stretches across the middle of the vaginal opening, making it appear as though there are two (or more) vaginal entries (when in reality, every hole leads to the same vagina.) Sleeve Hymen/Redundant Hymen: A trait in which an individual has a hymen that is thicker than expected, leaving it to fold in on itself. As lone variations, those with microperforate hymens, cribriform hymens, septate hymens, or sleeve hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. All four of these variations are fairly common, with each (separately) occurring in 1 of every 1,000 AFAB births.
-
Vaginal Septum: A trait in which an individual has a vaginal opening that is partially or fully blocked by skin tissue (which is not a hymen.) A Transverse Vaginal Septum (TVS) is when the tissue runs horizontally across or within the vaginal cavity, dividing or blocking it. Depending on how deep or wide this tissue is within the vagina, it may cause the vagina to seem short/small (due to blocking the vagina mid-way), may make the cervix seem absent (due to covering the cervix), could split the vagina into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally), or could be covering the entrance to the vagina altogether. An Obstructed Hemivagina is when the tissue runs vertically across/within the vaginal cavity, and curves to block part (but not all) of the vaginal entrance, leaving one side open. This might cause the vagina to seem short/small, and might cover the cervix. It may be obvious externally or only noticeable internally. This trait almost always partners uterus didelphys, blocking menstrual output from one of the two uteruses. A Longitudinal Vaginal Septum (LVS) is when the tissue runs vertically across/within the vaginal cavity, splitting it into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally.) As a lone variation, those with vaginal septums have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small or absent, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the tissue. This trait is rare.
-
Labial Hypoplasia: A trait in which an individual with a vulva is born without one or both labia. As a lone variation, those with labial hypoplasia have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Clitoral Hypoplasia: A trait in which an individual has a vulva with a small clitoris (under 0.75 inches or 1.90 centimeters.) Clitoral Agenesis: A trait in which an individual has a vulva, but no clitoris. As lone variations, those with clitoral hypoplasia or clitoral agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Penile Agenesis/Penile Aplasia: A trait in which an individual who is expected to have a penis is born without one. They either have urethral agenesis, a lone urethra, or a persistent cloaca. As a lone variation, those with penile agenesis have XY chromosomes, two testicles/one testicle (monorchidism) or anorchia, and a prostate. If they have testes, cryptorchidism is common. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. If testes are present, they can produce semen, but it may not be able to exit the urethra/cloaca depending on its placement and how the testes connect. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include twisted feet, an absent anus (which will need surgical intervention in order to pass waste), anal abnormalities, bladder abnormalities, small kidneys, kidney cysts, urine buildup (which may cause a stretched/swollen kidneys or ureter), a hole between the heart chambers, small lungs, a connection between the windpipe and esophagus, a flat nose, and rotated ears.
-
Micropenis/Microphallus/Penile Hypoplasia: A trait in which an individual is born with a small penis. Micropenises are 0.98 inches/2.5 centimeters or less in infants, and 3.67 inches/9.32 centimeters or less in adults. As a lone variation, those with micropenises have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is rare.
-
Congenital Buried Penis/Congenital Hidden Penis: A trait in which an individual is born with a penis that is mostly or entirely hidden within the skin of the abdomen, thigh, or scrotum. As a lone variation, those with congenital buried penises have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is fairly common, with the exact estimates unknown.
-
Aposthia: A trait in which an individual is born with a penis that has very little or no foreskin. As a lone variation, those with aposthia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Microorchidism/Testicular Hypoplasia: A trait in which an individual is born with one or multiple testicles that are smaller than average. Microtestes are 14 milliliters or less in adults, 3 milliliters or less during puberty, and under 1 milliliter pre-puberty. As a lone variation, those with microorchidism XY chromosomes, two testicles (possibly with cryptorchidism), a penis/micropenis or ambiguous genitals, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than wolffipathians. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome.
-
Cryptorchidism: A trait in which an individual is born with one or multiple testicles that are undescended (within the body, rather than hanging in the genital area.) This trait only counts as intersex if the testicles do not descend within the first 3-6 months after birth. As a lone variation, those with cryptorchidism have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is extremely common, occurring in 1 of every 100 AMAB births, however it can also occur in AFAB and AXAB/UAB individuals too. A common trait/disability that may co-occur is testicular cancer.
-------------------
Gonadal Agenesis
These are traits that cause one or both gonads to be absent.
Common traits and disabilities that may co-occur with gonadal agenesis include an absent kidney, kidney swelling, and kidney stones.
Anorchia/Bilateral Congenital Anorchia/Testicular Agenesis: A trait in which an individual that is expected to have testicles instead has no gonads. As a lone variation, those with cryptorchidism have XY chromosomes, a penis/micropenis or ambiguous genitals (which may have a urogenital sinus anomaly or a hole between the urethra & vagina) or penile agenesis, and a prostate. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile. This trait is rare.
-
Monorchidism/Monorchism/Unilateral Congenital Anorchia: A trait in which an individual is born with a single testicle. As a lone variation, those with monorchidism have XY chromosomes, a penis, possibly cryptorchidism, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is fairly common, occurring in 1 of every 5,000 AMAB births.
-
Unilateral Ovarian Agenesis: A trait in which an individual is born with a single ovary. As a lone variation, those with unilateral ovarian agenesis have XX chromosomes, a vulva, and a uterus/unicornuate uterus or MRKH syndrome. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. They are at a higher risk of infertility. If they are fertile enough, and have a uterus that is large enough, pregnancy is possible. If they are fertile enough, and have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is rare.
-
Ovarian Agenesis/Bilateral Ovarian Agenesis: A trait in which an individual that is expected to have ovaries instead has no gonads. As a lone variation, those with ovarian agenesis have XX chromosomes, a vulva, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile, however if they have a uterus (and it is large enough), they can carry a (genetically unrelated) embryo if it is medically implanted. This trait is rare.
-------------------
Other Reproductive Traits
Gonadal Dysgenesis: A trait in which an individual is born with a gonad (ovary, testicle, or ovoteste) that is full of empty tissue, rather than reproductive tissue. These are known as "streak gonads." If a person has two streak gonads, they will not begin puberty unless they are on HRT, and will have no eggs or sperm. XX Gonadal Dysgenesis/Pure Gonadal Dysgenesis (PGD) is a form of gonadal dysgenesis, in which an individual with XX chromosomes is born with two streak ovaries. They have a vulva or clitoromegaly and a uterus. They will not begin puberty unless they are on HRT. Due to the lack of eggs, they are infertile, however they can carry a (genetically unrelated) embryo if it is medically implanted. Swyer Syndrome and Mixed Gonadal Dysgenesis fall under this umbrella, and Turner Syndrome often does as well. All forms of gonadal dysgenesis are rare, except for when it occurs in Turner Syndrome.
-
Ovarian Hypoplasia/Hypoplastic Ovaries: A trait in which an individual is born with one or multiple ovaries that are smaller than typical. Unilateral Ovarian Hypoplasia is when an individual is born with one ovary that is smaller than typical. Bilateral Ovarian Hypoplasia is when an individual is born with both ovaries being smaller than typical. As a lone variation, those with ovarian hypoplasia have XX chromosomes, a vulva, and a uterus (possibly with fallopian tube agenesis or uterine hypoplasia.) Their menstruation may be irregular or absent. Pregnancy is possible if they have a uterus that is large enough, however they are at a higher risk of infertility and early menopause. If they have eggs and a large enough uterus, they may become pregnant naturally. If they have no fallopian tubes, they may need medical intervention in order to access their eggs. If their uterus is too small, then their eggs can be used to implant an embryo into another carrier. This trait is rare on its own, but fairly common when partnered with Turner Syndrome.
-
Fallopian Tube Agenesis: A trait in which an individual with ovaries and a uterus is born without one or both fallopian tubes. Unilateral Fallopian Tube Agenesis is when an individual is born with only one fallopian tube. Bilateral Fallopian Tube Agenesis is when an individual is born with no fallopian tubes. As a lone variation, those with fallopian tube agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with fallopian tube agenesis are capable of producing eggs, however only people with unilateral fallopian tube agenesis are capable of being impregnated (as they still have one fallopian tube to transport eggs) meanwhile people with bilateral fallopian tube agenesis are incapable of transporting eggs (as they have no fallopian tubes) and will need medical intervention to access their eggs. This trait is rare.
-
Vas Deferens Aplasia/Congenital Absence of the Vas Deferens (CAVD): A trait in which an individual with testes is born without one or both vas deferens. Unilateral Vas Deferens Aplasia/Congenital Unilateral Absence of Vas Deferens (CUAVD) is when an individual is born with only one vas deferens. Bilateral Vas Deferens Aplasia/Congenital Bilateral Absence of Vas Deferens (CBAVD) is when an individual is born with no vas deferens. As a lone variation, those with vas deferens aplasia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Those with vas deferens aplasia are capable of producing sperm, however only people with CUAVD are capable of releasing it (as they still have one vas deferens to deliver the sperm to the urethra), meanwhile people with CBAVD are incapable of releasing it (as they have no vas deferens) and will need medical intervention to access their sperm. This trait is fairly common, occurring in 1 of ever 1,000 AMAB births.
-
Seminal Vesicle Hypoplasia: A trait in which an individual has a seminal vesicle that is smaller than typical. Unilateral Seminal Vesicle Hypoplasia is when an individual is born with one seminal vesicle that is smaller than typical. Bilateral Seminal Vesicle Hypoplasia is when an individual is born with two seminal vesicles that are smaller than typical. Seminal Vesicle Agenesis: A trait in which an individual that is expected to have seminal vesicles has none, or only one. Unilateral Seminal Vesicle Agenesis is when an individual is born with only one seminal vesicle. Bilateral Seminal Vesicle Agenesis is when an individual is born with no seminal vesicles. As lone variations, those with seminal vesicle hypoplasia or seminal vesicle agenesis have XY chromosomes, a penis, two testicles (possibly with vas deferens aplasisa), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may or may not be capable of producing semen. If they are incapable of producing semen (or have vas deferens aplasia), then they will need medical intervention to access their sperm. These traits are rare. Common traits and disabilities that may co-occur include kidney abnormalities and an absent kidney.
-
Prostate Hypoplasia: A trait in which an individual has a prostate that is smaller than typical. For adults, the mass of a hypoplastic prostate is 10 cubic centimeters or less. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than wolffipathians. They may be capable of producing semen, but are at a higher risk of infertility. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
Prostate Agenesis: A trait in which an individual that is expected to have a prostate instead has none. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than wolffipathians. Their testes typically produce sperm, however the sperm is incapable of leaving the body due to the lack of prostate, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
WNT4 Deficiency: A variation in which an individual with XX chromosomes has a mutation in the WNT4 gene, which causes them to be born with an absent uterus, a vulva with vaginal agenesis or vaginal hypoplasia, and two ovaries. During puberty (without the influence of HRT), they will have hyperandrogenism, leading them to have testosterone as their main sex hormone, and will likely develop clitoromegaly, increased facial/body hair, higher muscle mass, and breasts. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This variation is rare.
-
Mayer–Rokitansky–Küster–Hauser Syndrome (MRKH Syndrome)/Müllerian Agenesis/Müllerian Aplasia: A trait in which an individual that is expected to have a uterus is born with a completely or partially absent uterus. As a lone variation, those with MRKH syndrome have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia) or a urogenital sinus anomaly, and two ovaries (which may be on an atypical spot of the fallopian tubes.) During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring 1 in every 4,500 AFAB births. Common traits and disabilities that may co-occur include a shorter height than average, abnormally located kidneys, an absent or underdeveloped kidney, heart complications, rib abnormalities, spinal abnormalities (possibly scoliosis), a short neck, a low hairline on the back of the neck, and hearing disabilities/deafness.
-
Unicornuate Uterus: A trait in which an individual is born with a uterus that has one side fully developed, while the other side of the uterus is underdeveloped (known as a Hemi-Uterus) or absent. If a hemi-uterus is present, it may or may not be functional. If it is functional, menstrual fluids will be released from it. The hemi-uterus might have a large enough opening that allows the menstrual fluids to leak into the main uterus - however, if the hemi-uterus does not have a wide enough opening, the menstrual fluids may get trapped and buildup could occur, or menstruation could take longer to end. As a lone variation, those with a unicornuate uterus will have XX chromosomes, a vulva, and two ovaries/an ovary (unilateral ovarian agenesis). The ovaries may be on an atypical spot of the fallopian tube(s). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of premature birth, miscarriage, and ectopic pregnancy. This trait is fairly common, occurring in 1 of every 4,000 AFAB births. Common traits and disabilities that may co-occur include kidney abnormalities and kidney cysts.
-
Uterine Hypoplasia/Hypoplastic Uterus: A trait in which an individual is born with a uterus that is smaller than typical. For adults, the length (from top to bottom) of a hypoplastic uterus is 2 inches/5 centimeters or smaller. As a lone variation, those with uterine hypoplasia have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia), and two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. They may have hypogonadism, so their estrogen levels might be lower than mulleripathians. If the uterus is smaller than 1.60 inches/4 centimeters, pregnancy is not possible, however their eggs (if they have an ovary) can be used to implant an embryo into another carrier. If the uterus is 1.60 inches/4 centimeters or larger, pregnancy is possible. however they are at a higher risk of miscarriage and premature birth, and if they have no ovaries, an embryo implant may be the only way to become pregnant. This trait is rare.
-
Cervical Agenesis/Cervical Dysgenesis/Cervical Atresia: A trait in which an individual with a uterus is born without a cervix, leaving the uterus closed off from the genitalia. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a cervix. Pregnancy is possible, however embryos will need to be medically implanted (unless they have a cervix created surgically.) This trait is extremely rare.
-
Cervical Hypoplasia: A trait in which an individual with a uterus is born with a cervix that is smaller than typical. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the cervix being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to expand the cervix. This trait is extremely rare.
-
Cervical Duplication/Double Cervix: A trait in which an individual with a uterus is born with 2 cervixes. As a lone variation, those with cervical duplication have XX chromosomes, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), two ovaries, and a uterus or uterus didelphys. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare on its own, but fairly common when partnered with uterus didelphys.
-
Uterus Didelphys: A variation in which an individual is born with two uteruses. Sometimes people with this variation are diagnosed with bicornuate uterus or septate uterus instead. As a lone variation, those with uterus didelphys have XX chromosomes, possibly cervical duplication, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), and two ovaries (typically one fallopian tube & ovary for each uterus). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average, however there is a higher risk of miscarriage and premature birth. Oftentimes each uterus can be impregnated separately. This trait is fairly common, occurring in 1 of every 3,000 AFAB births. Common traits and disabilities that may co-occur include severe menstrual cramps, heavy bleeding, extra menstruation, sexual dysfunction, and an absent kidney.
-
Fallopian Tube Duplication/Accessory Fallopian Tube: A variation in which an individual is born with three (or more) fallopian tubes. The extra tubes may or may not be attached to the uterus itself. As a lone variation, those with fallopian tube duplication have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however there may be difficulty with eggs reaching the uterus, due to going through one of the extra fallopian tubes, which may not have a connection with the uterus. This gives a higher risk of ectopic pregnancy and miscarriage. This trait is fairly common, with the exact estimates unknown. A common trait/disability that may co-occur is endometriosis.
-
Vas Deferens Duplication/Accessory Vas Deferens: A variation in which an individual is born with three (or more) vas deferens. The extra vas deferens may or may not be attached to the testes or prostate. As a lone variation, those with vas deferens duplication have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include inguinal hernias, an absent kidney, and cystic fibrosis.
-
Seminal Vesicle Duplication: A trait in which an individual is born with three (or more) seminal vesicles. As a lone variation, those with seminal vesicle duplication have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include kidney abnormalities.
-
Polyorchidism: A trait in which an individual is born with three (or more) testicles. These testicles could be descended, or they could have cryptorchidism. As a lone variation, those with polyorchidism have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Accessory Ovary: A trait in which a person has three (or more) ovaries, with the extra ovaries being connected to the other ovaries, the fallopian tubes, or the uterus. Supernumerary Ovary: A trait in which a person has three (or more) ovaries (and possibly extra fallopian tubes), with the extra ovaries (& fallopian tubes) being detached from the reproductive system, located away from the other ovaries. If they are latched onto/pressed against a different organ (ie; the intestines), they may cause abdominal pain. As lone variations, those with accessory ovaries or supernumerary ovaries have XX chromosomes, a vulva, and a uterus (possibly a bicornuate one) or unicornuate uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include extra adrenal glands, an absent kidney, an absent ureter, an extra ureter, and pouches in the bladder.
-
Ovotesticular Syndrome/Bigonadal/Ambigonadal: A variation in which an individual is born with a combination of ovaries and testicles. This could be ovaries and testes as separate gonads, or it could be a unique gonads (Ovotestes) that has both testicular and ovarian tissue within it. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. People with ovotestes have a uterus 90% of the time (possibly with uterine hypoplasia), and they may or may not have a prostate. They may have fallopian tubes, vas deferens, or both. As a lone trait, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes and a vulva or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. Those with the XY form have XY chromosomes, a penis (possibly with chordee or hypospadias) or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. People with both the XX and XY forms are at a higher risk of infertility. However, for those who are fertile, most commonly, the semen is infertile, while the eggs are fertile. However in rarer cases it is the other way around, with the eggs being infertile and the sperm being fertile. This trait is rare. Common traits and disabilities that may co-occur include germ cell tumors and inguinal hernias.
-
Persistent Müllerian Duct Syndrome (PMDS): A variation in which an individual with XY chromosomes is born with a uterus (possibly a hypoplastic uterus or an incomplete one) and possibly fallopian tubes. They usually have a prostate. In some cases, they may have an ovary or ovoteste, however most often they have testicles. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. They will have a penis, micropenis, or ambiguous genitals. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than wolffipathians. They may or may not be fertile, depending on the presence (or lack thereof) of a prostate, the function of their gonads, and the size of their uterus. If they have a prostate and functional testes, they are capable of producing sperm. If they have a large enough uterus, they are capable of pregnancy (however it may need to be medically implanted, depending on whether or not their genitals have a vaginal entry.) If the uterus is large enough to menstruate, the shedding will either exit through the genitals (if there is a vaginal entry or the urethra is connected to the uterus), or it will have nowhere to go. If it has nowhere to go, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry or to remove the uterus. This variation is extremely rare.
-------------------
Hypergonadism
These are traits that cause a person's gonads to produce a higher level of hormones than in wolffipathians and mulleripathians.
Hyperestrogenism: A trait in which an individual has high levels of estrogen. If they have ovaries, this describes having higher levels of estrogen than mulleripathians do. If they have testicles, this describes having higher levels of estrogen than wolffipathians do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (possibly with labial hypertrophy), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though it will be high), and will likely develop breasts (possibly with breast hypertrophy) and widened hips. Their menstruation could be heavy or irregular. They may also have hypoandrogenism, meaning their testosterone levels might be lower than mulleripathians. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis or micropenis, and two testicles (possibly with microorchidism). During puberty (without the influence of HRT), they will either have estrogen and testosterone at near-equal levels, or have estrogen as the main sex hormone, and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. If estrogen is their main sex hormone, they may also have hypoandrogenism, meaning their testosterone levels might be lower than wolffipathians. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), cold hands/cold feet, weight gain, swollen or tender breasts, bumpy breasts, a higher risk of breast cancer, a low libido, thinning hair, chronic migraines, memory difficulty, sleep disorders, and mood disorders. Aromatase Excess Syndrome (AEXS/AES)/Familial Hyperestrogenism is an extremely rare form of hyperestrogenism, caused by genetic mutations in the CYP19A1 gene, which makes the body convert more androgens into estrogen than is typical.
-
Hyperandrogenism: A trait in which an individual has high levels of androgens. If they have ovaries, this describes having higher levels of androgens than mulleripathians do. If they have testicles, this describes having higher levels of androgens than wolffipathians do. As a lone variation, this comes in both an XX form and an XY form. In 80% of cases the XX form is caused by Polycystic Ovarian Syndrome (PCOS), a genetic condition that causes the ovaries to overproduce hormones, which may cause cysts to develop on the ovaries. Those with the XX form have XX chromosomes, a vulva or clitoromegaly, two ovaries, and a uterus. During puberty (without the influence of HRT), they will either have estrogen and androgens at near-equal levels, or have androgens as the main sex hormones, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breasts and widened hips. If androgens are their main sex hormones, they may also have hypoestrogenism, meaning their estrogen levels might be lower than mulleripathians. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis (possibly a macropenis), two testicles (possible with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypoestrogenism, meaning their estrogen levels might be lower than wolffipathians. They may be capable of producing sperm, but are at a higher risk of infertility. The XX form is extremely common, occurring in 5-10% of AFAB people. The XY form is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), oily skin, higher levels of acne, a high libido, bald patches, high blood cholesterol, diabetes, behavioral disorders, mood disorders, and anxiety disorders. Familial Male-Limited Precocious Puberty (FMPP)/Testotoxicosis is an extremely rare form of the XY form of hyperandrogenism, where puberty-influencing androgen production begins extremely early, causing puberty to begin between the ages of 1-5 years old.
-------------------
Hypogonadism
These are traits that cause a person's gonads to produce a lower level of hormones than in wolffipathians and mulleripathians.
Primary Hypogonadism/Hypergonadotropic Hypogonadism describes when the gonads themselves have low production levels. The brain is still communicating to produce the average wolffipathian/mulleripathian levels of hormones, but the gonads are failing to keep up with the brains-signals.
Secondary Hypogonadism/Hypogonadotropic Hypogonadism/Central Hypogonadism describes when the brain has low levels of communication with the gonads. The brain is failing to send out typical levels of signals to the gonads, and the gonads only produce hormones when a signal is received.
Hypoestrogenism/Estrogen Deficiency: A trait in which an individual has low levels of estrogen. If they have ovaries, this describes having lower levels of estrogen than mulleripathians do. If they have testicles, this describes having lower levels of estrogen than wolffipathians do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone (though it will be low) and have the possibility of developing breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Turner Syndrome or PCOS. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, genital dryness, a higher risk of urinary tract infections, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-
Hypoandrogenism/Androgen Deficiency: A trait in which an individual has low levels of androgens. If they have ovaries, this describes having lower levels of androgens than mulleripathians do. If they have testicles, this describes having lower levels of androgens than wolffipathians do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-------------------
Other Hormonal Variations
Congenital Adrenal Hyperplasia (CAH): A variation in which an individual has adrenal glands that produce low levels of cortisol and/or aldosterone, and as a result, produce extra androgens to make up for it (leading to hyperandrogenism.) Classic CAH is when the symptoms are obvious at infancy, while Nonclassic CAH is when the symptoms occur in later childhood/teen years or adulthood. Classic CAH can be simple-virilizing or salt-wasting. Simple-virilizing CAH is when the aldosterone levels are low, but not dangerous. Salt-wasting CAH is when the aldosterone levels are too low to regulate the salt within the blood, leading to high levels of salt in the urine, which will need supplements and medications to manage. If people with salt-wasting CAH don't get treatment, it can result in low blood sugar, high levels of acid in the blood, dehydration, vomiting, diarrhea, irregular heartbeat, shock, coma, and death. Classic CAH has both an XX form and an XY form. Those with the XX form of classic CAH have XX chromosomes, a vulva (possibly with vaginal hypoplasia or a urogenital sinus anomaly) or ambiguous genitals, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Classic CAH have XY chromosomes, a penis (possibly a macropenis) two testicles (possibly with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Nonclassic CAH has both an XX and an XY form as well. Those with the XX form of nonclassic CAH have XX chromosomes, a vulva (though it may develop into clitoromegaly), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. They might also develop PCOS. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Nonclassic CAH have XY chromosomes, a penis, two testicles , and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Classic CAH is rare. Nonclassic CAH is extremely common, occurring in 1 of every 200-1,000 births. Common traits and disabilities that may co-occur with all forms of CAH include an early puberty (which may lead to a shorter height than average), oily skin, and higher levels of acne.
-
Leydig Cell Hypoplasia (LCH): A variation in which an individual with XY chromosomes is born with testicles (possibly with microorchidism or cryptorchidism), which has underdeveloped or absent leydig cells, resulting in hypoandrogenism and delayed or absent puberty. They have a penis or micropenis (possibly with hypospadias), bifid scrotum, or a vulva. They also have a prostate. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is extremely rare. Common traits and disabilities that may co-occur include a taller height than average, low bone density, and delayed or absent bone maturation.
-
17-Ketosteroid Reductase Deficiency (17 KSR Deficiency): A variation in which an individual with XY chromosomes has a genetic mutation that causes the hormone androstenedione not to convert into testosterone as frequently as it does within wolffipathians, resulting in hypoandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly). They also have two testicles (possibly with microorchidism or cryptorchidism) and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
5α-Reductase 2 Deficiency (5αR2D)/Pseudovaginal Perineoscrotal Hypospadias/PPSH: A variation in which an individual with XY chromosomes has a genetic mutation that causes a lower production of dihydrotestosterone compared to wolffipathians, resulting in hyperandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly.) They also have two testicles (possibly with cryptorchidism) and a prostate (possibly with prostate hypoplasia.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
Aromatase Deficiency: A variation in which an individual's body is incapable of converting androgens into estrogen, resulting in hyperandrogenism and hypoestrogenism. This begins during fetal development, and comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a clitorophallus or fused labia, two ovaries (possibly hypoplastic ovaries), and a uterus (though menstruation does not occur.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. Those with the XY form of aromatase deficiency have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include patches of darker/lighter skin, a taller height than average, low bone density, long limbs, inturned knees, high blood sugar, type 2 diabetes, weight gain, and a fatty liver. A person who is pregnant with a baby that has aromatase deficiency will get secondary effects of the androgens from the fetus within them. They may develop phallus growth, increased body/facial hair, and a deepened voice. These changes typically end once the baby is born.
-
Estrogen Insensitivity Syndrome (EIS)/Estrogen Resistance: A variation in which an individual's estrogen receptors do not respond to estrogen being produced. The estrogen is present, but the body is not fully using it. This may result in high levels of estrogen in the blood (due to estrogen being unused and building up), with the body only using minimal amounts of it. This comes in both an XX and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus (possibly with uterine hypoplasia.) Menstruation is absent or irregular. They may also have hyperandrogenism and experience ovarian cysts. During puberty (without the influence of HRT), if they don't have hyperandrogenism, then they will have estrogen as the main sex hormone, however it will have very little effect on their physical development. If they have hyperandrogenism, then testosterone will be their main sex hormone (or even just equal to estrogen, though the estrogen is being unused), however its effects will be minimal, likely only resulting in severe acne and pubic hair. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include a delayed puberty, a taller height than average, and low bone density.
-
Androgen Insensitivity Syndrome (AIS)/Androgen Resistance: A variation in which an individual with XY chromosomes has androgen receptors that do not respond to androgens being produced. The androgens are present, but the body is not fully using it. This may result in high levels of androgens in the blood (due to androgens being unused and building up), with the body only using minimal amounts of it. This comes in 3 forms - mild, partial, and complete. Those with Mild Androgen Insensitivity Syndrome (MAIS) have a body that is only mildly unresponsive to androgens, meaning that most of it is still in use. They have a penis (possibly with hypospadias), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. Those with Partial Androgen Insensitivity Syndrome (PAIS) have a body that is partially unresponsive to androgens, meaning that a significant amount of it is not in use. They have a penis or micropenis (possibly with chordee or hypospadias), ambiguous genitals, or a vulva with a urogenital sinus anomaly. They have two testicles (possibly with cryptorchidism), and may have a prostate (possibly with prostate hypoplasia) or no prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth and widened hips. They may be capable of producing sperm, but are at a higher risk of infertility (and if they lack a prostate, the sperm will be incapable of leaving, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring.) Those with Complete Androgen Insensitivity Syndrome (CAIS) have a body that is completely unresponsive to androgens. They have a vulva (possibly with vaginal hypoplasia, labial hypoplasia, and clitoral hypoplasia,) and two testicles with cryptorchidism. They have no prostate and no uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone, and will likely develop breasts and widened hips. They are infertile. All forms of AIS are rare. Common traits and disabilities that may co-occur include a taller height than average, large teeth, dry skin, drier eyes than typical, light sensitivity in the eyes, and dry hair.
-
Chromosomal Variations
These are variations that affect a person's chromosomes.
Swyer Syndrome/XY Gonadal Dysgenesis: A variation in which an individual has XY chromosomes, but due to a genetic mutation, they develop an estrogenized appearance. They have a vulva or clitoromegaly, a uterus (possibly with uterus hypoplasia), and two streak ovaries. They will not begin puberty unless they are on HRT. Due to the streak ovaries, they are infertile, however if their uterus is large enough, they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is rare. A common trait/disability that may co-occur is low bone density.
-
Mixed Gonadal Dysgenesis (MGD)/45X-46XY Mosaicism: A variation in which an individual is born with some cells having X chromosomes, and other cells having XY chromosomes. This comes in two forms. Those with the first form have a vulva (possibly with a urogenital sinus anomaly or vaginal aplasia) or ambiguous genitals and ovaries (though one or both will be streak ovaries). They may in some cases have a uterus. If both of their gonads are streak ovaries, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, meaning their estrogen levels may be low), and will likely develop breasts and widened hips. If they have a non-streak ovary, but no uterus, their eggs can create an embryo to be implanted into another carrier. If they have two streak ovaries, but have a uterus, then they can carry a (genetically unrelated) embryo if it is medically implanted. If they have two streak ovaries, and no uterus, then they are infertile. Those with the second form have a penis/micropenis or ambiguous genitals, testicles (though one or both will be streak), and a prostate (possibly with prostate hypoplasia). If both of their gonads are streak testes, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, meaning their testosterone levels may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. If they have a non-streak testicle, they can produce semen - though, if they also have prostate hypoplasia, they are at a higher risk of infertility. If both of their testes are streak, then they are infertile. This variation is rare.
-
XX-XY Chimerism/46, XX-46 XY Chimerism/XX-XY Mosaicism: A variation in which an individual is born with some cells that have XX chromosomes, and some cells that have XY chromosomes. Those with this variation could have a vulva (possibly with vaginal hypoplasia), a penis/micropenis, or ambiguous genitals. They may have hypospadias, epispadias, or a urogenital sinus anomaly. They can have any of the three gonad types (ovaries, testes, or ovotestes), however in some cases their gonads may also be streak. and may have a prostate, uterus, or both. If they have streak gonads, their puberty may be absent or delayed. If they start puberty naturally, their main sex hormone depends on what their gonads produce more of. They may produce estrogen as their main sex hormone (leading to breast growth and widened hips), androgens as their main sex hormones (leading to increased body/facial hair, higher muscle mass, and a deepened voice,) or a mixture of both - however, hypogonadism is common if they have streak gonads. If they have streak gonads, their fertility may be decreased or (if both gonads are fully streaked) they may be infertile. If they only have non-streak gonads, they may be capable of producing eggs (if they have ovaries or ovotestes) or sperm (if they have testes or ovotestes.) If they produce eggs but have no uterus, than the eggs will need to be extracted in order to create an embryo. If they produce sperm but have ambiguous genitals or a vulva, it may not be capable of being released, depending on how it connects to the genitals, and may need to be extracted in order to create an embryo. If they produce sperm but have a uterus, an embryo implant can be done if they wish to carry a baby. This variation is extremely rare. Common traits & disabilities that may co-occur include asymmetrical features (ie; an asymmetrical face), heterochromia (different colored eyes), and vitiligo.
-
XYY Syndrome/Jacob's Syndrome: A variation in which an individual is born with XYY chromosomes. They have a penis/micropenis (possibly with hypospadias), two testicles (possibly with macroorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism or hyperandrogenism is common, so their testosterone may be high or low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This variation is fairly common, occurring in 1 of every 1,000 AMAB births. Common traits and disabilities that may co-occur include being taller than average, hypotonia, flat feet, abnormal feet patterns, asthma, a large head, low-set ears, flattened cheekbones, dental abnormalities, widely-spaced eyes, night-blindness, tic disorders, seizure disorders, neurodevelopmental disabilities, learning disabilities, and communication disabilities.
-
XYYY Syndrome: A variation in which an individual is born with XYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include being taller than average, hypotonia, fused forearm bones, incurved fingers/toes, radial head dislocation, a short neck, dental abnormalities, a thick lower lip, a flat bridge of the nose, a longer space between the upper lip and nose, folded eyelids, widely spaced eyes, higher levels of acne, and intellectual disability.
-
XYYYY Syndrome: A variation in which an individual is born with XYYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include fused forearm bones, an incurved pinkie finger, facial asymmetry, a smaller than typical jaw, widely-spaced eyes, low set ears, hypertelorism, neurodevelopmental disabilities, and communication disabilities.
-
XXYYY Syndrome: A variation in which an individual is born with XXYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include delayed bone development, abnormal facial features, a small head, and intellectual disability.
-
XXXYY Syndrome: A variation in which an individual is born with XXXYY chromosomes. They have a penis/micropenis or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include being taller than average, delayed bone development, twisted feet, abnormal feet patterns, long legs, long arms, incurved fingers, a slim or underweight body, frequent upper respiratory infections, a narrow chest, a prominent jaw, a small jaw, a wide bridge of the nose, widely spaced eyes, folded eyelids, a prominent forehead, an abnormal face shape, low-set rotated ears, neurodevelopmental disabilities, communication disabilities, and behavioral disorders.
-
XXYY Syndrome: A variation in which an individual is born with XXYY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, flat feet, hip dislocation, inguinal hernias, cardiovascular abnormalities, gastrointestinal disabilities, weight gain , asthma, apnea, frequent upper respiratory tract infections, lymphatic cancer, scoliosis, an incurved pinkie finger, elbow dislocation, fused forearm bones, shoulder abnormalities, a flat back of the skull, a long face, facial asymmetry, a broad jaw, dental abnormalities, a cleft lip, a thick lower lip, widely spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, movement disorders, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
-
Klinefelter Syndrome/XXY Syndrome: A variation in which an individual has XXY chromosomes. They have a penis or micropenis, two testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is extremely common, occurring in 1 of every 500 AMAB births. Common traits and disabilities that may co-occur include a low libido, being taller than average, weak bones, hypotonia, breast cancer, increased body fat, type 2 diabetes, cardiovascular abnormalities, autoimmune disorders, lung disease, narrow shoulders, dental abnormalities, neurodevelopmental disabilities, communication disabilities, learning disabilities, behavioral disorders, depressive disorders, and anxiety disorders.
-
XXXY Syndrome: A variation in which an individual is born with XXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, abnormal shaping at the end of bones, flat feet, twisted feet, hip dislocation, abnormally angled hips, an underdeveloped kidney, inguinal hernias, gastrointestinal disabilities, increased body fat, frequent respiratory tract infections, asthma, cardiovascular abnormalities, scoliosis, elbow dislocation, fused forearm bones, an incurved pinkie finger, low-set sloped shoulders, a short neck, a flat back of the skull, dental abnormalities, a large jaw, a cleft palate, facial asymmetry, a flat bridge of the nose, widely-spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, crossed eyes, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, anxiety disorders, and psychotic disorders.
-
XXXXY Syndrome: A variation in which an individual has XXXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is extremely rare. Common traits and disabilities that may co-occur include being shorter than average, hypotonia, hyperflexible joints, abnormal shaping for the end of the bones, flat feet, a twisted foot, abnormally angled hips, hip dislocation, an absent or underdeveloped kidney, cardiovascular abnormalities, gastrointestinal disabilities, asthma, frequent respiratory infections, scoliosis, an incurved pinkie finger, fused forearm bones, low-set sloped shoulders, a short neck, a flat back of the skull, a prominent jaw, dental abnormalities, a cleft palate, a wide nose, a flat nose, absent olfactory bulbs (resulting in an inability to smell), upslanted eyelids, drooping eyelids, widely spaced eyes, crossed eyes, near-sightedness, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, and communication disabilities.
-
XXXXX Syndrome/Pentasomy X: A variation in which an individual has XXXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include delayed puberty, being shorter than average, short feet, hip dislocation, immune system disorders, cardiovascular abnormalities, a small head, a flat back of the head, a small lower jaw, a flat front face, dental abnormalities, a wide nasal bridge, upslanted eyelids, widely spaced eyes, crossed eyes, low-set rotated ears, and intellectual disability.
-
XXXX Syndrome/Tetrasomy X: A variation in which an individual has XXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is extremely rare. Common traits and disabilities that may co-occur include delayed puberty, hypotonia, hyperflexible joints, hip dislocation, kidney disorders, bladder disabilities, immune system abnormalities, autoimmune disorders, cardiovascular abnormalities, short fingers/toes, an incurved pinkie finger, dental abnormalities, widely spaced eyes, upslanting eyelids, crossed eyes, seizure disorders, learning disabilities, and communication disabilities.
-
Triple X Syndrome/Trisomy X/XXX Syndrome: A variation in which an individual has XXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is fairly common, occurring in 1 of every 1,000 AFAB births. Common traits and disabilities that may co-occur include delayed puberty, being taller than average, hypotonia, hyperflexible joints, flat feet, an absent or underdeveloped kidney, kidney defects, frequent urinary tract infections, autoimmune disorders, a caved-in chest, fused forearm bones, incurved fingers, widely-spaced eyes, folded eyelids, drooping eyelids, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, learning disorders, mood disorders, anxiety disorders, and psychotic disorders.
-
SERKAL Syndrome: A variation in which an individual has XX chromosomes, but due to a genetic mutation in the WNT4 gene, they develop an androgenized appearance. They have a penis or micropenis (possibly with hypospadias or penoscrotal transposition), two testicles or ovotestes (possibly with cryptorchidism), and a prostate. This variation is extremely rare. There is no information on fertility or puberty, as the only three recorded cases of this variation were terminated as fetuses. Common traits and disabilities that may co-occur include a small/underdeveloped bladder, an absent kidney, adrenal abnormalities, non-coiled intestines, small/underdeveloped lungs, heart abnormalities, a diaphragmatic hernia, and an oral cleft.
-
XX Male Syndrome/De La Chapelle Syndrome: A variation in which an individual has XX chromosomes, but due to one of their X chromosomes containing an SRY gene, they develop an androgenized appearance. They have a penis/micropenis (possibly with hypospadias) or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is rare. Common traits and disabilities that may co-occur include a shorter height than average and a low libido.
-
Turner Syndrome/Monosomy X: A variation in which an individual has only one X chromosome and no Y chromosome (0X.) They have a vulva, ovaries (usually hypoplastic ovaries or streak ovaries), and a uterus. Mosaic Turner Syndrome is a type of Turner syndrome where some cells have 0X chromosomes, and other cells have XX chromosomes. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. If one of their ovaries is non-streak, then pregnancy is possible, however they are at a higher risk of infertility and early menopause. If they have two streak ovaries, then they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is fairly common, occurring in 1 of every 2,500 AFAB births. Common traits and disabilities that may co-occur include a delayed puberty, a shorter height than average, vitiligo, moles, birthmarks, skin scarring, low bone density, outturned forearms, nail abnormalities, abnormal feet/hand patterns, flat feet, flexible toe joints, short toes, splayed toes, abnormal shape for the end of the tibia bones, inturned knees, enlarged outer thighbones, hip dislocation, an absent or underdeveloped kidney, fused kidneys, abnormally located kidneys, increased body fat, liver defects, heart defects, autoimmune disorders, thyroid gland inflammation, cystic hygroma, scoliosis, a hunched back, a short sternum, a wide rib cage, a caved-in chest, a broad chest, a broad neck, a webbed neck, a short neck, a low hairline on the back of the head, a small/underdeveloped or absent lower jaw, dental abnormalities, drooping eyelids, folded eyelids, crossed eyes, near-sightedness, prominent ears, frequent ear infections, hearing disabilities, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
_______________________________________________________
_______________________________________________________
_______________________________________________________
And thats all!
Again, please reblog to spread awareness. Intersex people are highly discriminated against. Their bodies are still regularly mutilated at birth or during puberty, and they are still forced into HRT, in order to make them "look right" or "function right."
This medical abuse can cause complete infertility, a loss of sensation in genital areas (making sex unsatisfactory), chronic pain, gender or sex incongruence, and body dysmorphia.
Additionally, intersex children are often bullied at school for looking or sounding "abnormal" for their age/gender. And as they grow up, they face the same difficulties transgender individuals do - judgement for not being a "real man" or "real woman" (or for being non-binary), difficulty dating, struggles finding jobs, complications in receiving proper healthcare, and they are at an increased risk of being abused and assaulted. Many are also left out of sports or kicked out of public bathrooms as well.
This is all due to the lack of education. Tolerance and acceptance needs to be taught to children. Many doctors have no idea how to treat intersex patients, as they didn't learn about their bodies, even in advanced schooling. We need to put a stop to this.
#intersex#intersex spectrum#queer#lgbt#lgbtq#lgbtqia#lgbtqia+#education#educate yourself#educate yourselves#pride month#lgbt pride#happy pride 🌈#queer pride#body diversity#diversity#information#informative#chromosomes#hormones#hormonalhealth#genitals#reproductive rights#reproductive health#representation#reproductive justice#intersex awareness#intersex pride#intersex issues#intersex community
867 notes
·
View notes
Text
This year, I went to two local pride events. It was great, but in both events I noticed something: there was almost no aromantic representation. There were plenty of flags for sale, as well as colored merch and stickers, encompassing a wide range of identities. Not ONE of them was aromantic. The flag banners they'd put up, with a bunch of different LGBTQ+ flags? No aromantic. However, there was an asexual flag as well as other items for sale, which was part of the reason I was surprised by the lack of aromantic flags and other merchandise.
I'm not saying the asexual representation is bad; it's great! It's the lack of representation for aromanticism that is problematic. I'm aroace. I was pissed as HELL because I felt that half of me was underrepresented. I can't imagine how excluded allosexual arospec folk would have felt to know that they had all but been completely erased. The A in LGBTQIA doesn't just stand for asexual; it's for aromantic and agender (which I also noted had no representation) too.
The only mention of aromanticism at all in both pride events was a brief, easy to overlook touch on it at a few stalls. Pride is meant to be inclusive to all. To ALL. Not ALLOROMANTICS ONLY. ALL.
I'm aromantic. I'm not just ace. It took me years to figure out that I was also aromantic, but it doesn't actually make a difference. If I can only find my asexuality shown at pride events then things need to change.
I am aromantic. I'd like for that part of me to be represented. I DEMAND that part of me to be represented.
#screaming at midnight#aromantic#aromantism#aromance#aromantic representation#aromantic pride#aromantic spectrum#aromantic visibility#arospec#aro pride#A IS ASEXUAL AROMANTIC AND AGENDER#REMEMBER THAT#ALWAYS#IT'S NOT JUST ASEXUAL#DON'T FORGET ABOUT THE AROMANTIC AND/OR AGENDER FOLKS#pride is for everyone#pride month#lgbtqia#queer pride#lgbtq#lgbt pride#lgbtq community#queer#pride#queer community#lgbtqiia+
674 notes
·
View notes
Text
Master Chief is Kind of an Asexual Icon and No One Can Change My Mind
Master Chief doesn’t flirt. He doesn’t hook up. He doesn’t even look at people that way.
And yet, he has one of the most powerful, emotionally-charged connections in gaming — with Cortana. It’s deep, loyal, intimate, and completely non-sexual.
That’s ace-coded royalty, right there.
💬 No Romance, No Problem
Across multiple Halo games, novels, and even the show, Master Chief:
Has zero sexual partners.
Doesn’t engage in romantic subplots.
Doesn’t even hint at interest in anyone physically.
He's too busy saving the galaxy — and honestly? He just doesn’t seem to care. That’s not how he connects.
🤝 Loyalty > Lust
Chief shows his love by:
Protecting people with his life.
Trusting Cortana with his every thought.
Staying behind, finishing the mission, never leaving anyone behind.
His version of closeness isn’t about sex or romance — it’s about presence, purpose, and protection. That’s a form of intimacy a lot of aces get.
🛠️ Purpose-Driven, Not Pleasure-Seeking
Everything about Chief’s life is structured around:
Duty
Honor
Survival
There’s no desire for pleasure, seduction, or even flirting. His body is a tool, not a statement. He exists to serve a mission, not to fulfill tropes of sexual masculinity.
🌈 Ace-Coded Masculinity That Hits Different
Where most action heroes are hypersexualized, Chief is:
Quiet
Stoic
Emotionally vulnerable only to those he truly trusts
He’s never reduced to a love interest. Never sexualized. And never portrayed as needing sex to be whole. He’s complete as he is.
💜 Chief x Cortana: Queerplatonic Vibes
They’re not lovers. They’re not just partners. They’re something more rare — deep soul-bonded allies.
It’s not romantic. It’s not sexual. It’s intimate in a way that lives between the lines.
And honestly? That’s one of the most ace-coded dynamics in all of sci-fi.
🏁 TL;DR: Master Chief is ace-coded. He redefines what intimacy, masculinity, and connection can look like — and he doesn’t need sex or romance to do it.
💥 We stan an emotionally armored legend.
#asexual#asexuality#ace headcanon#halo#master chief#cortana#ace representation#nonsexual intimacy#queerplatonic vibes#video game characters#gaming culture#ace spectrum#headcanon
160 notes
·
View notes
Text
I'm just trying to see something. Not sure if this has been done before?
593 notes
·
View notes
Text
"So, you wanna make them ace?"
Asexuality 101: Making your characters asexual
Indroduction: Ok, so, from what I've seen in fandom and in general, most people don't really know how to write an asexual character. Many just quit it and make them allosexual, others just struggle their way without having much of a guide. Prime example is Alastor from Hazbin Hotel, whom many people want to involve in sexual scenarios so they go with the "asexuality is a spectrum" route. Problem is, they don't understand how asexuality is a spectrum exactly and then they just end up writing their characters as allo. Now, how to avoid this? Teaching them!
If you're looking for a good way to get started with your own asexual oc, an ace headcanon or a media charater, I've got you! (i mention sex briefly here in some parts)
My credentials: I'm ace.
The basics
What is asexuality?
Asexuality is a sexual orientation that is generally defined by the lack of sexual attraction, or a very little amount of it. Sexual attraction is many times confused with libido, which is the sexual desire. Sexual attraction is more accurately, "the desire of having sex with this specific person." Therefore, some ace people do have a libido, and do want to have sex, but mostly are just not attracted to a person.
Myths and misconceptions
Asexuals can't have sex - as many shippers say, "asexuality is a spectrum", and while some aces don't have sex indeed, they can want it and have it as well. Person to person scenario
Asexuals don't know nothing about sex - unless the ace in question is a child, they probably may know, in fact, a lot. Many ace people like reading, watching or consuming smut, and by this and other means, even if they don't have sex themselves, they pretty much know how it is and how it works. Sex is everywhere, after all. Hard to miss
Asexuality is caused by trauma - it can be! Just not always, and most aces are simply born this way
Asexuality is a medical condition - much like homosexuality, asexuality is frequently treated as an illnes and many ace people are forced into conversion therapy. Some people also hold the belief that asexuality is caused by an anormality in a person's hormones, a mental illness, etc. But it is not true! Asexual people can obviously also be mentally ill in some way, but these are different things. It is just a sexual orientation like any other!
Asexuality is caused by HRT - hormone replacement therapy, ie. taking testosterone or estrogen, is one of the most common type of medical transition for trans people. Some hold the belief that taking hormones like those can "break" your sexuality (estrogen does sometimes decrease a person's libido, but it depends on the person's organism and it doesn't take your sexual attraction away from you), and turn you asexual
Asexuality is caused by autism - this myth may be originated from the fact that many autistic people are in fact asexual, or by the fact that both asexuals and autistic people tend to be infantilized a lot. However, as much as autistic people are very commonly also ace, asexuality is not, in fact, a symptom of autism
Basic terminology
Ace - short for "asexual".
Aro - short for "aromantic"; someone who experiences little to no romantic attraction, aka typically "doesn't fall in love".
Allo - somebody who does experience attraction. "Allosexual" is someone who is not asexual, and "alloromantic" is someone who is not aromantic.
Aspec - short for "a-spectrum". The a-spectrum is an umbrella term for anyone who is in any way ace, aro, aplatonic, afamilial, or other identities that fit here.
Acespec - short for "asexual spectrum/ace spectrum". It's a part of the a-spectrum and contemplates all asexuality.
Aesthetic attraction - finding someone pretty or beatiful, without necessarily wanting to have sex with them. Many ace people who didn't know they were ace report to having used to mistake it with sexual attraction.
Sensual attraction - similar to sexual attraction; the desire to touch someone, but without wanting to actuall have sex with them. Many ace people also confused this with sexual attraction.
Aphobia - discrimination against aspec people.
Amatonormativity- the belief that everybody is happier in a relationship, wether they want it or not, and should want and seek to be in one, and the general root of aphobia.
The Split Attraction Model
If you are looking on the ace community for a while, you might have heard of the split attraction model--if you haven't, here it is:
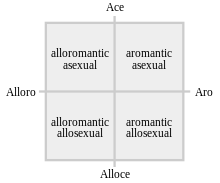
Image description: The Split Attraction Model, a cross chart inside a square, with four ends. The first end of the cross is labelled "ace", its opposite is labelled as "alloce", the third end is labelled as "alloro" and it's opposite is labelled as "aro". The section on the "alloro" and "ace" square is labelled "alloromantic asexual", the section in the "ace" and "aro" part is labelled "aromantic asexual", the section on the "alloro" and "alloce" square is labelled as "alloromantic allosexual" and the section on the "aro" and "alloce" section is labelled "aromantic allosexual". /end ID.
The split attraction model divides all orientations in four groups: The aroaces, the aroallos, the alloaces and the alloallos. It is usually shortened to "SAM".
Many people find this model useful, because it sorts your attraction into two groups: allo- and a-, and yes and no. It's simple and easy.
Many aces do not use this model to explain their attraction/lack thereof though! Hence the first distinction of aces we have here: SAM-aces and non-SAM-aces. Basically aces who use the Split Attraction Model and aces who prefer not to!
A non-SAM ace may define their asexuality as their romantic orientation as well, or label themselves differently altogether. While a SAM ace could call themselves an "asexual aromantic" or an "asexual alloromantic", a non-SAM ace could call themselves just "an asexual". In this case, they can be neither "alloro" nor "aro".
If your character is aware of their sexuality and identifies as ace, it's good to know wether they use the Split Attraction Model for themselves or not.
The spectrum
You may have heard that "asexuality is a spectrum" a thousand times, but what does it mean?
Just like "non-binary", "asexual" can be an identity on its own, but it is actually an umbrella term for a bunch of orientations. When we say that it is a spectrum, we are saying that there is Nuance. "Ace who doesn't date", "ace who dates", "ace who experiences just a little bit of sexual attraction", "aces who like sex" and so on. 'But Angel', you ask me, 'didn't you say that asexuality is when people don't have sexual attraction?' It can be! But there IS nuance, and that's what I am here to tell you.
There are two more factors beyond the SAM that you can consider:
"Are they sex repulsed, sex favorable, or sex neutral?"
Here is the "aces can still have sex" thing. A sex repulsed ace is probably what the majority of people think when they hear "asexual". It is an ace person who doesn't like sex. Doesn't want to have it, is disgusted by it, despises sexual intimacy, etc. They are the aces who tipically just don't want to have sex, and are very happy without it.
A sex favorable asexual is someone who likes it. Sure, they don't feel sexual attraction, but who's letting it stop them, right? They like sexual acts, they are fine and happy with having sex in general, and that's what the "aces can still have sex" point means. Yes, they can, if they want to! Maybe your character themself doesn't define themselves as neither repulsed nor favorable, but it's good to know what their instance on sex is.
Sex neutral asexuals are aces who are not repulsed by it, but are not really into it either. They may have sex, they may be fine with it, they may like it even, but they generally don't have a desire or strong feelings regarding it. It's just sex, after all.
Sex ambivalent asexuals are another thing I want to touch on. They are tipically aces whose instance on sex changes! Sometimes they may feel repulsed by it, sometimes they may want it, sometimes they may not care. They are neither strictly one, nor another. Their feelings change!
It's good to see where in this categorization your character or blorbo would be.
Inside the asexual spectrum, where do they stand?
If I were to represent the ace spectrum as a linear thing, I'd do it like this:
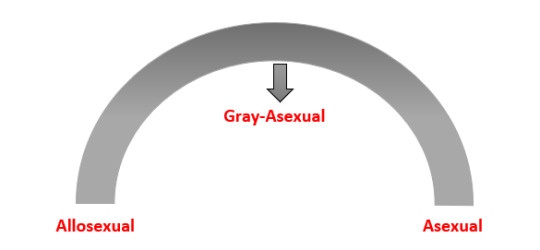
Image description: A linear representation of the asexual spectrum, in the shape of an arch. In one end, it is written "asexual", on the other, it is written "allosexual" and on the very middle, at the top of the arch, it is written "gray-asexual". /end ID.
or like this:
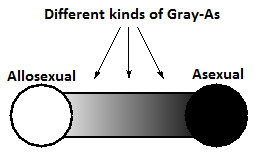
Image description: Another linear representation of the asexual spectrum. One of the ends is a black circle and the other is a white circle. Between them, a gradient goes from one circle to another, passing through different shades of gray. The black end is labelled as "asexual", the white end is labelled as "allosexual", and the gradient with shades of gray is labelled "different kinds of Gray-As". /end ID.
What is graysexual, you ask me? We all know that the world is not black-and-white, and as so, sexuality is also not. Grayace is a term for a person that is also asexual, but not strictly: that is, they are the "feels a little of sexual attraction" part of the spectrum. It is called like that because when we put asexual and allosexual in two ends of a spectrum, graysexuality stands in this gray area.
Gray sexuals may:
Experience sexual attraction only sometimes
Experience light sexual attraction
Experience sexual attraction under certain conditions in certain scenarios, for example, when they are already very intimate with a certain person
And many more! Graysexuality is on itself a spectrum, but having an idea of allosexual -> graysexual -> strictly asexual is already a good guide. Graysexuality can also be described as "having partial sexual attraction".
Fun fact about gray-aces: The asexual flag has four stripes; purple, white, gray and black. The purple stripe is meant to be a color signifier of the community, the white means allosexual, the gray means the gray aces and the black stripe represents people with strictly no sexual attraction. Hence the term "black stripe asexual" (which is not very popular but I personally like).
Micro-labels
You already have a basic understanding of the asexual spectrum and how it works, so you can think on where exactly in the spectrum your character/blorbo is. To help you out further, I present you the microlabels! Much like non binary is an umbrella term with many microlabels like genderqueer, xenogender and demigender, that help one explain their identity with more and more specific explanations, asexuals also have a lot of microlabels! Here are some:
Cupiosexual - asexual person that wishes to have a sexual relationship (example: i am cupioromantic person and i am basically a hopeless romantic and a yearner. cupiosexuality is similar, but with sex)
Gray sexual - asexual person with partial sexual attraction
Demisexual - asexual person who can only be attracted to people they already have a bond with
Abrosexual - person whose sexuality is fluid, and may be asexual at one time, bisexual at another, gay at another, etc.
Aceflux - asexual person whose sexuality changes, like abrosexual, but only between asexual identities
Aegosexual - asexual person who likes the idea of sex or fantasises about it, as long as it doesn't envolve them
Lythosexual - asexual person who is only sexually attracted to people they are not close with, and their sexual attraction fades out once the become closer
Myrsexual - asexual person that uses multiple asexual identities to describe their sexuality
Aroace - aromantic asexual person
Alloace - alloromantic asexual person
Apothisexual - sex-repulsed asexual person
These are not all micro labels in the asexual spectrum, but they are quite a lot. Maybe even if your charater is not sure if they are in a certain label or not, you may find them in some of these descriptions.
Links to resources with more microlabels: Tumblr post by @aroacesafeplaceforall (no images) /
/ A slightly longer list on asexuals.net (undescribed flags) /
/ Another guide for microlabels on lgbtqia.fandom.com (undescribed flags)
Bonus questions
Is it okay if I make my asexual character autistic? Is it not stereotyping? Yes, it's okay. There are actual asexual autistic people, and I'm sure they'd love to get represented as well!
Is it okay if I make my asexual character have sex? Is it not erasure? Yes, you can do that too! As long as it is where they stand in the spectrum (as explained in the topics above), you are doing a good thing by representing sex-favorable asexuals.
Do I have to make a romantic orientation for them too? No. Your character may be a non-sam ace, and identify as ace alone!
I heard that it is erasure if I make smut fanfic of ace character X. I don't get it how! While it is true many ace people have sex, many people when writing that just ignore their sexuality when writing/drawing smut of them! The spectrum is wide, so when you are doing that, remember where they stand on it.
Why can't I headcanon this ace character as allosexual? I headcanon straight characters as gay/bi/pan all the time and nobody says it's wrong! If people don't like my headcanon why can't they just look away? Because asexual people are a marginalized group, unlike straight people, so it is as okay to make them allo as it is to take an asian or black or jewish character and make them white. Because it is not just an individual headcanon; it's a part of a much bigger problem, and by avoiding headcanoning ace characters as allo, you are confronting your own internalized aphobia, which is a good thing! If you still want to make them have sex, well, that's what I made this guide for! So you can make them have sex as you wish without erasing their identity.
I am ace and am basing myself or my own experiences here. Is it okay if I...? The answer is generally yes. If you wanna write about a different ace experience than your own, a little bit of research won't hurt, though!
Is this enough for me to write my ace character? It is a start. This is a general guide, and there are some things I haven't touched on this guide (like aphobia) so I'd advice you to do more in-depth research on topics you want to focus more on, but this should get you pretty far.
Extra
"Is Alastor from Hazbin Hotel canonically ace or aroace?" (slightly related, because some people looking for this guide to write this guy might want to know this too)
Answer: link to a post clearing this up this with some sources. Short answer though, is that he is confirmed to be ace, not aroace.
"If I didn't understand something here, or I have more questions, can I ask you?"
Answer: Yes! You can reblog this post with questions, and my inbox is also open, and I make sure to always let anon on. I will be happy to help if I can.
"One of the image descriptions on this post was off or confusing, can you change it to X so it is better to understand it?"
Answer: Of course! I will need you to signal me in either the notes or in the inbox what I need to change, though.
"Are asexual people queer?"
Answer: Yes! Because the queer community, as the name suggests, is for people who are different, odd, and are not considered "normal" because of that. Asexual people are not a part of "the norm", because we don't feel sexual attraction, and therefore, we, and by extension your ace characters too, are queer.
<2
#writing advice#representation#writing tips#fanfiction#fandom#hazbin alastor#hazbin hotel alastor#radioapple#radiodust#radiohusk#alastor the radio demon#asexual#asexuality#asexual spectrum#non sam ace#aroace#alloace#ace#acespec#ace spectrum#character building#writing asexual characters#queer#writing queer characters#ace characters#asexual characters#shipping#ace alastor#described#sami long post
925 notes
·
View notes
Text
Do You Know This (non-canon) Autistic Character?
Propaganda:
Castiel is an angel, and a classic case of a non-human creature accidentally being portrayed as incredibly autistic. He doesn't understand social cues, he struggles with concepts such as personal space, and has unusual speech patterns and eye contact habits. He also frequently misundertands and misuses pop culture references, even after he is magically given the knowledge of the media others reference. He's also portrayed as unusual among other angels.
As other angels are introduced in the show, many of them do not exhibit Castiel's social difficulties. They also frequently other Cas, saying he doesn't fit in in heaven. He also exhibits some sensory differences, for example he doesn't enjoy eating because he can taste every molecule and finds that overwhelming, though this can be attributed to him being an angel rather than him being autistic.
#Castiel#castiel supernatural#castiel spn#supernatural#autistic representation#autistic characters#poll#polls#tumblr poll#autism#asd#character poll#character polls#autism spectrum disorder#autism in media#autistic spectrum#autistic people#autistic#polls on tumblr#tumblr polls#random polls#fandom polls
147 notes
·
View notes
Text
THIS IS THE FLAG OF MY COUNTRY🗣🗣

#asexual#asexual spectrum#asexual stuff#asexual shitposting#asexual experience#asexual representation#asexual rights#asexual thoughts#asexual things#asexual umbrella#asexual icons#asexual is valid#asexual pride#asexual positivity#asexual post#asexual problems#asexual artist#asexual flag#asexual dinosuars#asexual humor#asexual jokes#asexual lesbian#asexual community#asexual culture#asexual visibility#asexual memes#asexual media#asexual moment#aegosexual#shit post
301 notes
·
View notes
Note
I'm not sure how to write this, but alas.
How would you write a character with Schizophrenia(or any other disorder similar) in a fantasy setting. Say like, Skyrim.
There's quite literally a bunch of supernatural things that happen in that universe that are canon, like ghosts legit exist and what not and you can quite literally talk to gods in there as well. And I know could be seen as a Delusion and what not.
So I'm not sure how to god about respectfully writing one. 😅😅
Hiya! This is one of my absolute favorite topics, and I do this fairly often in my own writing. The best answer is that you blend the two - there is real magic happening and around the character, and they may at times mistake their positive symptoms (hallucinations, delusions, etc) for parts of their world.
An example for skyrim is that maybe they believe their hallucination is a god they have talked to before and when they message the god again they realize the god doesn't understand a reference to the last time "they" talked. Maybe they have a delusion there are demons terrorizing them but it's actually a very sorry ghost. Have fun with the setting and playing with what's reality there and what isn't!
You could also focus on, in terms of delusions, less of talking to gods and demons and ghosts and more on interpersonal delusions. That someone is plotting to kill them, that the world is fake, that someone they've never met is in love with them, that the radio is giving them messages, etc. The big thing to keep in mind is respect for writing characters with schizophrenia and schizophrenia spectrum disorders as well as psychosis in general - they are experiencing a reality that is strong and very real and intense for them. Even if it doesn't overlap with what others experience as reality, the biggest thing is not forcing reality or encouraging the other reality but helping them cope with their reality and stay safe in the episode.
I also encourage you to look at negative symptoms and symptoms of disorganized speech and add that to the character as well, as schizophrenia is more than just hallucinations and delusions. This will help ground your character in the disorder as well even when reality is more fantastical than ours.
I hope this helps, and happy writing! Mod Bert
128 notes
·
View notes
Text
I'm still not over the fact that South Park just casually has the best canonical QPR represention I ever seen. By total accident.

I mean seriously, what the fuck. Tweek and Craig were basically forced to pretend to be together, despite not even being into men, but then they just… continued? Into their adulthood? And it's confirmed to be a platonic relationship. And they act like regular couple, but just not love eachother in romantic or sexual way. They were said by creators to not love eachother in the same way a regular couple would, but still closer than friends or brothers.
I fucking love this. They're the only reason I started watching South Park.
#funny#aromantic#aroace#asexual#aro#ace#qpr#qpr ship#queerplatonic relationship#queer platonic relationship#queerplatonic#aroace representation#aroace spectrum#south park#sp#south park ships#craig x tweek#craig tucker#creek#sp creek#tweek tweak#sp tweek#tweek x craig
219 notes
·
View notes
Text
religious conservatives: no sex before marriage !!
asexuals: okay
religious conservatives: wait no, not like that Σ(゜゜) /hj
#asexual community#asexuality#asexual#actually asexual#asexual pride#asexual representation#asexual spectrum#acephobia#gray ace#ace stuff#ace pride#ace rep#ace representation#ace spec#ace spectrum#ace umbrella#aceflux#acephobia tw#acesexual#acespec#ace#pride#queer#religious conservatives#conservatives#religious#lgbtq#lgbtqia+#lgbtq+ community#lgbt community
2K notes
·
View notes
Text
dragon age lore: half elves just look like humans
dragon age fans:

#the amount of pointy ear alistair art i see gives me life#anyway this was an extremely dumb decision and having a spectrum of half-elf representation would've been far more interesting.#oh well#text post#dragon age#da
959 notes
·
View notes