#National Hospital for Neurology
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In Q3 of 2020, 31% of US users access the Tumblr app daily.
Text
Also preserved on our archive
Long Covid, the constellation of long-term health effects caused by SARS-CoV-2 infection, is a significant global health crisis affecting at least 400 million individuals worldwide, with a cost of $ 1 trillion, equivalent to 1% of the global Gross Domestic Product. Long Covid can affect nearly every organ system resulting in various symptoms including fatigue, cognitive dysfunction, post-exertional malaise, autonomic dysfunction, and chronic conditions including new onset diabetes, cardiovascular disease, gastrointestinal and neurologic disorders. Long Covid can affect people across the lifespan and across age, race and ethnicity, and baseline health status.
Chinese scientists were among the first to report Long Covid in people who survived the acute phase of Covid-19. However, these early seminal Chinese studies on Long Covid were exclusively from Wuhan – where the pandemic originated. Because of China’s zero Covid policies, infection rates plummeted quickly in Wuhan and were very low and sporadic outside of Wuhan for much of 2020, 2021, and 2022. However, China relaxed its zero Covid policies at the end of 2022 which led to explosion of cases – hundreds of millions of Chinese got infected with SARS-CoV-2 in the weeks and months following the lifting of zero Covid policies.
Now a report by Qin and colleagues provides insights into the colossal scale of Long Covid that resulted from those infections. Their large-scale survey of 74,075 Chinese participants, one of the largest studies of its kind and the first from China, shows that approximately 10%–30% of survey participants reported experiencing Long Covid symptoms such as fatigue, memory decline, decreased exercise ability, and brain fog. The features of Long Covid in China mirror those observed in studies conducted in other parts of the world. This underscores the consistency of Long Covid features across national borders, cultures and healthcare settings.
Interestingly, the authors show that despite having milder acute symptoms during reinfection, participants who experienced multiple infections were more likely to experience various Long Covid symptoms with greater severity. The authors show that having two infections is risk factor for many long-term Covid symptoms, and the risk increased exponentially when the number of infections exceeded two. These new data on Long Covid risk after reinfection are remarkably consistent with prior studies.
Another critical insight from the study is the protective role of Covid-19 vaccines in reducing the incidence and severity of Long Covid. The data shows that vaccination, particularly with multiple booster shots, significantly decreases the risk of developing long-term symptoms. These findings are consistent with other studies showing that vaccines reduce the risk of Long Covid. Despite this, Covid-19 vaccine policies in much of the world consider effectiveness of vaccines in reducing risks of hospitalization and death during the acute phase of SARS-CoV-2 infection (which are most evident in older adults and people with comorbidities) and ignore their protective effect on Long Covid – a condition that affects people across the lifespan including young adults and children. Consequently, restrictive vaccine policies exclude children, young and healthy adults who may benefit from the beneficial effects of vaccine on Long Covid. Vaccine policies must holistically consider the benefit profile of Covid-19 vaccines including their effects in lowering the risk of Long Covid.
Looking forward, there are several key areas where Long Covid research must focus. There is an urgent need for comprehensive—and globally coordinated—Long Covid research strategy to understand the biological mechanisms, develop diagnostics, test therapeutics, characterize the long-term epidemiology and clinical course, evaluate health care delivery, and assess the impacts of Long Covid on patients, care givers, health systems, economies and societies.
Equally important are policies to prevent Long Covid; support impacted individuals and their care givers; and ensure access, quality and equity of care. Policies are also needed to promote public awareness and facilitate professional training for health care providers.
China, with its rich scientific history, is poised to contribute significantly to solving the puzzle of Long Covid. The international community must come together to identify areas of synergies in research, share data, resources, and expertise to accelerate progress on Long Covid. This includes fostering partnerships between governments, academic institutions, and the private sector, as well as engaging with patient advocacy groups to ensure that research is aligned with the needs and experiences of those affected by Long Covid.
The study by Qin and colleagues offers the first comprehensive view of the state of Long Covid in China. The findings are both sobering and illuminating. Long Covid is clearly a serious public health challenge in China, as it is globally. These insights underscore the urgent need for a coordinated international response to address this significant and growing crisis. The stakes are high. Yet, throughout history, humanity has risen to the challenge of solving complex problems. We must now face Long Covid with the same resolve, ingenuity, and collaborative spirit that have driven our greatest achievements.
#long covid#covid conscious#mask up#covid#pandemic#wear a mask#public health#covid 19#wear a respirator#still coviding#sars cov 2#coronavirus#covid is not over
54 notes
·
View notes
Text
"In the most comprehensive national study since the onset of the COVID-19 pandemic, a team of researchers that includes a Rutgers-organized consortium of pediatric sites has concluded that long COVID symptoms in children are tangible, pervasive, wide ranging and clinically distinct within specific age groups. Results of the study, funded by the National Institutes of Health (NIH), are published in the Journal of the American Medical Association. “We have convincing evidence that COVID-19 is not just a mild, benign illness for children,” said Lawrence C. Kleinman, a professor of pediatrics and population health expert at Rutgers Robert Wood Johnson Medical School (RWJMS) and the study’s third co-author. “There are children who are clearly disabled by long COVID for long periods of time.” In the early stages of the pandemic, a myth arose and was perpetuated suggesting that because children often developed only mild cases of COVID-19, the risks for young patients were not serious. But this conjecture dissipated amid a rash of data demonstrating that a few children infected with COVID-19 will get very sick and others will suffer an array of health complications long after initial exposure. Broadly defined, long COVID includes symptoms, signs, and conditions – such as aches, fatigue, memory loss and stomach pain – that develop, persist or relapse more than a month after a COVID-19 infection. Worldwide, an estimated 65 million people, including children, live with long COVID. Until recently, most research into COVID-19’s lingering effects focused on adults. To quantify long COVID’s impact on children and determine whether symptoms experienced by the youngest COVID-19 patients differ by age group and from adults, Kleinman and more than 140 researchers throughout the United States crunched data from NIH’s Researching COVID to Enhance Recovery (RECOVER) Initiative, a national effort to survey COVID-19’s long-term impact. As part of RECOVER, caregivers for 5,367 children (898 school-aged children and 4,469 adolescents) completed online surveys about their children’s health in time for this data analysis. Roughly 86 percent of the sample had previously been infected with COVID-19, while 14 percent – the control group – had not. The survey assessed 74 known and potential long COVID-19 symptoms across nine domains: eyes, ears, nose and throat; heart and lungs; gastrointestinal; dermatologic; musculoskeletal; neurologic; behavioral and psychological; menstrual; and general. By analyzing the responses, researchers found 45 percent of COVID-19 infected school-age children (ages 6 to 11) reported at least one prolonged symptom after initial recovery versus 33 percent of uninfected children. Thirty-nine percent of COVID-19 infected adolescents (ages 12 to 17) reported one prolonged symptom, compared with 27 percent of uninfected adolescents. These differences implicate the virus as a likely causal factor, rather than just having lived through the pandemic. Long COVID symptoms in children also were clustered in patterns distinct from adults and from each other. For instance, the most common symptom in adolescents was loss of smell and taste, followed by low energy, muscle aches and fatigue. For school-age children, memory and focus issues topped the list, followed by stomach pain, headaches and back or neck pain. Children experienced prolonged symptoms after COVID-19 infection “in almost every organ system, with the vast majority having multisystem involvement,” the authors wrote."
oh hey, remember a couple of years ago during the omicron wave when multisystem inflammatory syndrome was driving a lot of kids to go to the hospital?
29 notes
·
View notes
Text
To my new followers, let me introduce myself.
I'm Buttacake or Auntie.
I have a Bachelors of Arts in History from the University of Illinois at Urbana-Champaign. Primary focus was medieval History. Secondary focus was US Minority History up to 1865.
I have a Juris Doctor, or law degree, from the University of Illinois College of Law. My specialization was Critical Race Theory. Yeah...that boogeyman. I wrote my legal note on tribal sovereignty & enrollment. I am a Cherokee Freedman descendant of the Cherokee Nation and, at that time, the Cherokee Nation had been fighting to exclude Freedman descendants from citizenship. I also have some distant Osage & Chickasaw heritage.
And, I also have a Masters degree in Sociology from Trinity College, Dublin. Specialization was Race, Ethnicity & Conflict. My ethnographic dissertation was on the Tea Party movement & the "origin" of white Christian Nationalism called "Jesus and the White Man".
I have been researching MAGA since 2015 (prior to that, it was the Tea Party movement). I have attended Trump rallies as an observer for years, so I anticipated this move years ago, and was trying to avoid this outcome.
After law school, I worked at Amazon during its growth & expansion early days. I held a Kindle prototype in my hands before it launched. I reported up to Jeff B and had to respond to his emails whenever a customer escalated one of my decisions. I left when co-workers started sleeping under their desks.
I have been a social worker, by craft, for the last decade. First in child welfare. Then, working with young adults with autism. Then, on to working at a psychiatric & forensic hospital.
I'm a former union organizer. Still an activist.
But in 2019, I was assaulted by a patient, and that injury developed into a permanent brain injury. I have Functional Neurological Disorder which means my brain & body miscommunicated.
Add to all of that, I have been a hockey fan for over 30 years, and I discovered my ethnographic training transfers quite well to the world of hockey.
Welcome.
10 notes
·
View notes
Text

Dave Whammond
* * * *
Person. Woman. Man. Camera. TV. Double Standard.
July 8, 2024
ROBERT B. HUBBELL
JUL 08, 2024
The mainstream media continues its whisper campaign against President Biden, as they report that anonymous “senior leaders” talk “in private” about approaching Joe Biden to urge him to drop out. At least Adam Schiff had the guts to express his qualms in public respectfully, even though I strongly disagree with his views (on this subject).
One evolving narrative among the press is that the Biden administration “concealed” the truth of Biden’s cognitive state—which supposedly justifies their righteous anger. Bull****. This is another example of a double standard applied by a media that is intent on driving Joe Biden out of the race—damn the facts!
Joe Biden has been transparent with the American people about his health—which cannot be said about Trump.
Remember Trump's unexplained visit to Walter Reed for a treatment that remains secret to this day? Or showing up to a debate in 2020 knowing he had tested positive for Covid but concealed that fact from Joe Biden, the debate moderators, and the American public?
Or having a doctor release a statement about Trump's health that was dictated by Trump? Or when the White House physician provided false information about Trump's vital statistics—like his weight—and said that Trump might be the first president to live to be 200?
Amid all the calls for “cognitive tests” for Biden—but not Trump—journalists are committing malpractice by failing to note that President Biden released a detailed summary of his annual physical in February of this year.
The full report is here: Health-Summary-2.28.pdf (whitehouse.gov). The examination included consultations with neurological experts at Walter Reed hospital. I urge you to read the entire report and consider how you would measure up to such a battery of tests!
[...]
So, Biden did have a “detailed neurological exam” four-and-half months ago. The widespread media demands that Biden “take a neurological exam” should be directed to Trump instead.
Predictably, this “proof” won’t be enough for the media. Just as the media refused to accept a certified copy of President Obama’s birth certificate, the goalposts will keep shifting.
The issue is not Joe Biden. It is Donald Trump—and the media’s arrogant refusal to apply the same scrutiny to Trump that it is applying to Biden. If they did, they would be demanding neurological exams of Trump and his withdrawal from the race. So far as we have been informed by Trump, his cognitive test consisted of recalling five objects: “Person. Woman. Man. Camera. TV.” Can you say, “double standard”?
Why isn’t the media making demands that Trump submit to “extremely detailed neurologic testing” by experts from a nationally recognized hospital?
The answer is simple. Trump has quashed dissent within his party. Anyone who dares raise a voice in dissent is the immediate recipient of anonymous death threats and public ridicule on Trump's vanity media platform. And Trump's para-military press surrogates leap into action, declaring that the dissidents are dead to MAGA.
So, the press's application of the same standards to Trump has no upside because it won’t incite the mass panic among Republicans that Democrats are willing to supply by the bucketful.
I accept at face value the good faith of readers who say they have lost confidence in Biden because of the debate or any other reason. That is a personal judgment only you can make. But I again remind everyone that “Biden should withdraw” is not a plan. If you believe a different path to victory is appropriate, then you must devote yourself to that path with all the vigor and financial resources you can muster.
[...]
Timothy Snyder (author of On Tyranny and Substack blog Thinking About), addressed the role that the press has been playing in whipping up “fascist froth” that helps Trump. See Timothy Snyder, Fascism and Fear (substack.com)
There are three tests of good faith for those who are proposing that President Biden step down. The first is recognition that Biden’s first term has been one of extraordinary achievement. The second is a plan for what the Democrats would do, should Biden withdraw, to select a nominee and win the election. The third is recognition that the threat of regime change is what might justify changing the nominee.
If I am right that much of the energy behind the Biden pile-on is displaced fear of a regime change, much of the media will continue to generate fascist froth for Trump, whether or not Biden is the Democratic nominee — unless, of course, journalists confront their fears, and keep the issue of regime change inside the story, and provide a constructive alternative alongside personal criticism.
[I inverted the order of Snyder’s two paragraphs above so they made more sense in a short quotation.]
And, finally, Rebecca Solnit wrote what I wish I had written. See her essay in The Guardian: Why is the pundit class so desperate to push Biden out of the race?
Solnit begins:
I am not usually one to offer diagnoses of people I’ve never met, but it does seem like the pundit class of the American media is suffering from severe memory loss. Because they’re doing exactly what they did in the 2016 presidential race – providing wildly asymmetrical and inflammatory coverage of the one candidate running against Donald J Trump. They have become a stampeding herd producing an avalanche of stories suggesting Biden is unfit, will lose and should go away, at a point in the campaign in which replacing him would likely be somewhere between extremely difficult and utterly catastrophic. They do this while ignoring something every scholar and critic of journalism knows well and every journalist should. As Nikole Hannah-Jones put it: “As media we consistently proclaim that we are just reporting the news when in fact we are driving it. What we cover, how we cover it, determines often what Americans think is important and how they perceive these issues yet we keep pretending it’s not so.” They are not reporting that he is a loser; they are making him one. And so it goes with what appears to be a journalistic competition to outdo each other in the aggressiveness of the attacks and the unreality of the proposals. It’s a dogpile and a panic, and there is no one more unable to understand their own emotional life, biases and motives than people who are utterly convinced of their own ironclad rationality and objectivity, [also known as] pundits.
Here's my advice to everyone—regardless of what side of the issue you take regarding Joe Biden’s continued candidacy. The issue is Trump, not Biden. Whether Biden drops out is not something you or I have control over. (Readers frequently write to me and say, “Please tell Joe Biden . . . .” The only thing Joe Biden knows about me is my credit card number.)
Joe Biden has control over his choices; his close advisors and family have influence; some senior leaders in the Democratic Party have some influence. They are talking amongst themselves. Let them have a rational, private conversation not played out on the front pages of the NYTimes and WaPo minutes after the latest exchange of views.
However, the one institution that has demonstrated it cannot be trusted to deal with this question is the media. They have a perverse financial incentive: Chaos = profit. They are agents of chaos at this moment in pursuit of the mighty dollar.
I believe that Joe Biden is the best candidate to defeat Trump, that replacing him at this point poses unacknowledged and unknowable risks, and that those who advocate a different path have the burden of identifying and funding an alternative candidate.
Our task has not changed. It is our moral and patriotic duty to alert all Americans about the threat posed by Trump and his fascist plan to undermine democracy. We have plenty of work and precious little time left to accomplish our task.
Let us channel all our energy away from debating Joe Biden’s age and health into defeating Trump. In that task, we must speak with one voice.
[MORE]
[Robert B. Hubbell Newsletter]
22 notes
·
View notes
Text

Neuron Membrane Shaper
Vital role revealed of a BAR domain protein called FAM92A1 in remodelling neuron membranes during brain development, particularly at synapses, the structure that allows passage of signals from one neuron to another. Insight into the risk of FAM92A1 mutation leading to human neurological disorders
Read the published research article here
Image from work by Liang Wang and Ziyun Yang, and colleagues
Mental Health Center & National Chengdu Center for Safety Evaluation of Drugs, State Key Laboratory of Biotherapy, West China Hospital of Sichuan University, Chengdu, China; Biological & Environmental Sciences, University of Helsinki, Finland
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Nature Communications, July 2024
You can also follow BPoD on Instagram, Twitter and Facebook
16 notes
·
View notes
Note
Sorry for being the bearer of bad news, but we still have, like, three missions to complete before the Despair Sisters return to Japan:
Make sure Tamami and Sophia don't die.
Stop the Holy Salvation Army.
And find Utsuro before either Junko or the Basilisk.

*Wednesday, February 27th, Void Warehouse, morning*

Well...at least we can say with certainty that that's taken care of.
*Emma crosses out one more entry in pen*
February 20-27: Go to National Center of Neurology and Psychiatry (NCNP), stop Tsumugi Shirogane

Yep, no more Shirogane. Thank god.

Not exactly how we wanted it to go, but it's done now. Our most difficult mission's complete, and that just leaves a couple more.

How...How's everyone doing?

...I'm fine.

Well as I can be, I suppose. I'm just glad I could relocate Mizuta's remains.

Anything from the hospital?

Everyone's woken up by now, although Esumi-senpai needs to stay a bit longer. They have some extra tests they need to run.

Oh, but Hajime and Hayase-san should be here soon!

That's great! I can't wait to see them again.

...Perhaps we should be discussing specialization?
What do you mean?

Just what I've suggested. We needn't have this situation repeat itself, thus we should consider how best to specialize what tasks everyone is suited toward from now on.
We still have much else to accomplish, after all.
True, yeah. Has there been any luck with getting in touch with the future?

Still nothing yet. No idea what the problem is, and Setsuka-san doesn't really get it either. We were hoping Hayase could take a look at it.

Well...I'm ready to do my part to help you guys. Mori-san said she is too!

Heads up, guys. They're here.
*The door opens and two familiar faces return*

...H-hey, everyone.

Careful, Haji. Watch your step.

Thank you.
#danganronpa#sdra2#super danganronpa another 2#sdr2#super danganronpa 2#nwpm#neo world program monitor#emma magorobi#hajime hinata#umeko hayase#hibiki otonokoji#nikei yomiuri#estu deguchi#kikue kutsuki#gundham tanaka#hiyoko saionji#mikan tsumiki#hajime makunouchi#a student out of time#DR#Dianthus Memory arc
10 notes
·
View notes
Text
Hello everyone,
I found an interesting about neurodiversity and queerness. According to this article:
Research doesn’t yet offer a clear reason to explain the overlap between the communities. One theory suggests that the greater gender-and-sexual diversity within the neurodivergent population results from challenges in navigating sociocultural norms around mainstream notions of gender and sexuality — like gender roles and expressions, and sexual orientation and attraction. That is, due to the differences in the way a neurodivergent person experiences life, they may struggle to conform to these norms, inspiring them to explore beyond traditions and express themselves in newer ways that resonate with them.
“You could then understand the co-occurrence as perhaps a more honest expression of underlying experiences,” John Strang, director of the Gender and Autism Program at the Children’s National Hospital in Washington, D.C., told Spectrum News.
Further, the struggle to fit within a society that idealizes neurotypical brains can also lead neurodivergent individuals to question a multitude of social norms — including those around gender and sexuality. In other words, the alienation they experience — be it due to autism, a learning disability, a personality disorder, or even bipolar disorder — can cause them to feel like an “outsider” at all times, inducing a greater openness to alternate ideas of gender and sexuality. Upon digging further, they may end up with the conclusion that they are indeed cis-gendered and heterosexual. But in the event that they aren’t, the exploration prompted by the neurological differences that denied one the sense of belonging can inadvertently become the key to discovering their gender and sexuality.
Many neurodivergent people can also feel both sensory and emotional stimuli — including attraction and arousal — more deeply, which can also drive them to explore their sexuality more. While that doesn’t automatically mean they’d turn out to be queer, it does point to them being more open to embracing a queer identity, if their exploration does lead them to that conclusion.
The link to the full article will be below if anyone wants to read more.
Neurodiversity
#neurodivergence#actually neurodivergent#neurodiversity and queerness#lgbtq#feel free to share/reblog#tw bright colors#tw eye strain
86 notes
·
View notes
Note
Thank you for answering, do you think this will be a similar thing to covid? Now I don't have facts or sources other than one disabled advocate on social media but I heard something about one of covids less popularized effects being something about brain degeneration? Or something loosely connected to that. And because of how poorly covid was handled in the US it ended up affecting a lot of people including the children. Or maybe it was something about how the pandemic never truly ended over there and people stopped wearing their masks too soon. I can't remember, but if you know more of it or have any idea what I'm talking about, how comparable do you consider the two situations? Thanks in advance
So I haven't really seen anything about brain degradation, but there is current research into acute covid-19 infections disrupting the blood brain barrier.
It does appear to happen in severe cases, but it's specifically severe cases as far as all of the research I've seen. It's also not really unique to covid-19. To my knowledge, there's a lot of viruses that can trigger a similar response, like Influenza or West Nile. This is generally what causes the most severe forms of these diseases, the BBB gets disturbed, and this triggers inflammation in the brain which fucks with a lot of shit.
This topic is really complicated, and again, research is still ongoing. Part of the current issue with active neurological studies for COVID-19 is kinda similar to CTE research, you can only really tell how bad the neurological damage was after someone's died and you can yoink their brain out to have an in depth look. This means a almost all of the more indepth studies on COVID-19 in brain tissue are from people who are dead. Usually from COVID. So there's a strong bias towards the most severe cases.
That being said, I actually don't think this is particularly comparable to the severity of lead poisoning on people through the 1950s-1980s. Part of which is that children, while they did catch COVID-19, didn't usually get severely sick. They also didn't tend to catch COVID-19 as often in the first place. That's not to say neither happened ever, just that it's comparatively quite rare.
Meanwhile, effectively 100% of children had lead blood poisoning at a level of clinical significance for most of the 1950s-1980s.
Literally, I am not even kidding, this research is from 2015 but it's still extremely informative,
Like, their graphing of blood levels displays this really well,
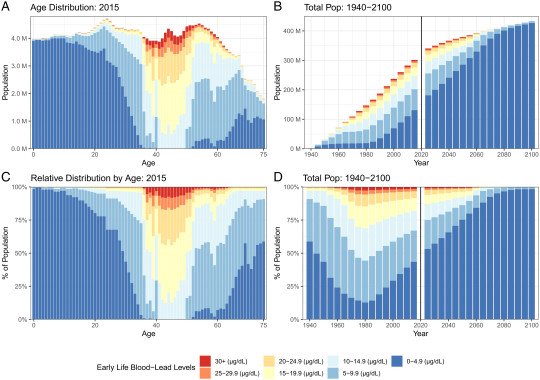
I apologize, you may have to click on it to see, but this is graphing out our entire population in the US and led blood levels in early childhood (note, while people who are old enough to not have been born or been children in the 1950s would not have had CHILDHOOD lead poisoning, they still would've been at high risk for exposure to adult lead poisoning which can still fuck you up). S
For quick reference on blood lead poisoning btw, the CDC level used to be 10 μg/dL (light blue and above), but as since been lowed to 5 and then 3.5 μg/dL as a reference level. This is part of no amount of lead being safe, but above 10 μg/dL is bad. Above 20 μg/dL for children is "hey so we need to do a full medical exam of this child, do an environmental hazard investigation of your home and get a hazard team response specifically to help you get lead of your house". Meanwhile above 45 is "we may need to hospitalize this child".
That's the scale I'm talking about when I say everyone in the 1950s-1980s had childhood lead poisoning. It was everyone. COVID-19, while bad, isn't everyone. It isn't even close. BBB disruption, according to the research I could find, only occurs in some acute illness of infections that happen. This is still bad, but nowhere near the scale of lead poisoning.
12 notes
·
View notes
Text
It is the first gene therapy approved to treat this debilitating and fatal disease found almost exclusively in boys. Emma Ciafaloni is a neuromuscular neurologist with the University of Rochester Medical Center (URMC) neurology department and Golisano Children’s Hospital, and director of the UR Medicine Duchenne Muscular Dystrophy Clinic, which treats boys with Duchenne muscular dystrophy (DMD) from across upstate New York. Ciafaloni has been involved in DMD clinical research for decades and URMC was one of first three sites in the nation to start dosing patients in the phase 3 clinical trial for the new gene therapy. The study, called EMBARK, has since expanded to additional sites in North America, Europe, and Asia. Ciafaloni also served as chair of the independent Data Safety and Monitoring Board for the early phase clinical trials of the therapy. The new drug—delandistrogene moxeparvovec-rokl—is being developed by Sarepta Therapeutics and marketed under the name ELEVIDYS.
Continue Reading
54 notes
·
View notes
Text
Lazarus phenomenon
Autoresuscitation is a phenomenon of the heart during which it can resume its spontaneous activity and generate circulation. It was described for the first time by K. Linko in 1982 as a recovery after discontinued cardiopulmonary resuscitation (CPR). J.G. Bray named the recovery from death the Lazarus phenomenon in 1993. It is based on a biblical story of Jesus’ resurrection of Lazarus four days after confirmation of his death. Up to the end of 2022, 76 cases (coming from 27 countries) of spontaneous recovery after death were reported; among them, 10 occurred in children. The youngest patient was 9 months old, and the oldest was 97 years old. The longest resuscitation lasted 90 min, but the shortest was 6 min. Cardiac arrest occurred in and out of the hospital. The majority of the patients suffered from many diseases. In most cases of the Lazarus phenomenon, the observed rhythms at cardiac arrest were non-shockable (Asystole, PEA). Survival time after death ranged from minutes to hours, days, and even months. Six patients with the Lazarus phenomenon reached full recovery without neurological impairment. Some of the causes leading to autoresuscitation presented here are hyperventilation and alkalosis, auto-PEEP, delayed drug action, hypothermia, intoxication, metabolic disorders (hyperkalemia), and unobserved minimal vital signs. To avoid Lazarus Syndrome, it is recommended that the patient be monitored for 10 min after discontinuing CPR. Knowledge about this phenomenon should be disseminated in the medical community in order to improve the reporting of such cases. The probability of autoresuscitation among older people is possible.
National Library of Medicine
8 notes
·
View notes
Text
Factors associated with outcome in a national cohort of rhinovirus hospitalized patients in Brazil in 2022

The common cold is the primary cause of illness in the community, with over 200 viral strains identified, and rhinovirus infections being the most prevalent. Coronavirus Disease 19 (COVID-19) is also a significant cause of severe illness. The burden of acute respiratory infections has a significant impact on the economy, resulting in absenteeism from work and school. Rhinovirus infections can exacerbate asthma and other chronic diseases, leading to hospitalization. The objective of this study is to investigate the factors associated with death and survival in patients hospitalized for rhinovirus in Brazil in 2022. This is a retrospective cohort study using data from the national surveillance of Severe Acute Respiratory Syndrome (SARS) in 2022 in Brazil, with all the norrifications. We analysed and compared clinical and epidemiological factors and outcomes between survivors and deaths in patients hospitalised for rhinovirus. The absolute and relative frequencies were calculated according to the states. Bivariate analysis was performed using chi-squared test and Fisher’s exact test, while multivariate analysis was performed using COX regression. Out of 8,130 cases of SARS caused by rhinovirus, 291 (3.58%) resulted in death while 7839 (96.47%) patients survived. The factors associated with death were invasive ventilation (p- < 0.001 HR 4.888 CI 95% 3.816–6.262), bocavirus (p- < 0.001 HR 4.204 CI 95% 2.595–6.812), immunodepression/Immunosuppression (p- < 0.001 HR 2.417 CI 95% 1. 544–3, 786), COVID-19 (p- < 0.001 HR 2.167 CI 95% 1.495–3.142), chronic neurological diseases (p-0.007 HR 1.610 CI 95% 1.137–2.280), abdominal pain (p-0.005 HR 1.734 CI 95% 1.186–2.537), age (p- < 0.001 HR 1.038 CI 95% 1.034–1.042). The survival factors identified in this study were dyspnea (p = 0.005; HR 0.683; CI 95% 0.524–0.889), cough (p < 0.001; HR 0.603; CI 95% 0.472–0.769), and asthma (p = 0.052; HR 0.583; CI 95% 0.339–1.004). Additionally, the study found that receiving a COVID-19 booster dose was also a significant survival factor (p = 0.001; HR 0.570; CI 95% 0.415–0.784). The factors associated with death were similar to those in the literature, and the factors associated with survival were also similar, except for the booster dose of the COVID-19 vaccine, which we didn’t find in any studies. Our study is the first to associate the full course of the COVID-19 vaccine with survival in those hospitalized for rhinovirus, regardless of COVID-19 and rhinovirus co-detection.
Read the paper.
#brazil#brazilian politics#politics#science#healthcare#medicine#rhinovirus#image description in alt#mod nise da silveira
2 notes
·
View notes
Text
Also preserved on our archive
DM me if you have access to the attached study: I'd like to read it and it's paywalled.
Researchers at Brigham and Women’s Hospital discovered that individuals exhibiting a wide range of long COVID symptoms were twice as likely to have SARS-CoV-2 proteins in their blood compared to those without such symptoms.
A new study suggests that a persistent infection may be the cause of long COVID symptoms in some people. Conducted by Brigham and Women’s Hospital, a key institution within the Mass General Brigham healthcare system, the research identified signs of ongoing infection in 43 percent of participants who reported cardiopulmonary, musculoskeletal, or neurologic symptoms associated with long COVID. These findings were published today (October 9) in Clinical Microbiology and Infection.
“If we can identify a subset of people who have persistent viral symptoms because of a reservoir of virus in the body, we may be able to treat them with antivirals to alleviate their symptoms,” said lead author Zoe Swank, PhD, a postdoctoral research fellow in the Department of Pathology at Brigham and Women’s Hospital.
Advanced Detection Methods and Study Results The study analyzed 1,569 blood samples collected from 706 people, including 392 participants from the National Institutes of Health-supported Researching COVID to Enhance Recovery (RECOVER) Initiative, who had previously tested positive for a COVID infection. With a highly sensitive test they developed, researchers looked for whole and partial proteins from the SARS-CoV-2 virus. They also analyzed data from the participants’ long COVID symptoms, using electronic medical chart information or surveys that were gathered at the same time as the blood samples were taken.
Compared to people who didn’t report long COVID symptoms, those who reported persisting symptoms affecting heart and lung, brain, and musculoskeletal systems many organ systems were approximately twice as likely to have SARS-CoV-2 proteins circulating in their blood. The research team was able to detect the spike protein and other components of the SARS-CoV-2 virus using Simoa, an ultrasensitive test for detecting single molecules. Commonly reported long COVID symptoms included fatigue, brain fog, muscle pain, joint pain, back pain, headache, sleep disturbance, loss of smell or taste, and gastrointestinal symptoms.
Specifically, 43% of those with long COVID symptoms affecting three major systems in the body, including cardiopulmonary, musculoskeletal, and neurologic systems, tested positive for viral proteins within 1 to 14 months of their positive COVID test. But only 21% of those who didn’t report any long COVID symptoms tested positive for the SARS-CoV-2 biomarkers in this same period.
It’s possible that a persistent infection explains some – but not all – of the long COVID sufferers’ symptoms. If this is the case, testing and treatment could aid in identifying patients who may benefit from treatments such as antiviral medications.
Multiple Causes of Long COVID One of the questions raised by the study is why more than half of patients with wide-ranging long COVID symptoms tested negative for persistent viral proteins.
“This finding suggests there is likely more than one cause of long COVID,” said David Walt, PhD, a professor of Pathology at Brigham and Women’s Hospital and Principal Investigator on the study. “For example, another possible cause of long-COVID symptoms could be that the virus harms the immune system, causing immune dysfunction to continue after the virus is cleared.”
Ongoing Research and Future Directions To better understand whether an ongoing infection is behind some people’s long COVID symptoms, Swank, Walt and other researchers are currently conducting follow-up studies. They’re analyzing blood samples and symptom data in larger groups of patients, including people of wide age ranges and those with compromised immune symptoms. This way, they can also see if some people are more likely to have persistent virus in the body.
“There is still a lot that we don’t know about how this virus affects people,” said David C. Goff, M.D., Ph.D., a senior scientific program director for the RECOVER Observational Consortium Steering Committee and director of the Division of Cardiovascular Sciences at the National Heart, Lung, and Blood Institute (NHLBI), part of NIH. “These types of studies are critical to help investigators better understand the mechanisms underlying long COVID — which will help bring us closer to identifying the right targets for treatment.”
Goff added that these results also support ongoing efforts to study antiviral treatments.
The SARS-CoV-2 blood test developed by Brigham and Women’s researchers is also currently being used in a national study, called RECOVER-VITAL, that is testing whether an antiviral drug helps patients recover from long COVID. The RECOVER-VITAL trial will test the patients’ blood before and after treatment with an antiviral to see if treatment eliminates persistent viral proteins in the blood.
Potential Viral Persistence in Other Diseases The idea that a virus can stay in the body and cause ongoing symptoms months after an infection isn’t unique to COVID. “Other viruses are associated with similar post-acute syndromes,” said Swank. She noted animal studies have found Ebola and Zika proteins in tissues post-infection, and these viruses have also been associated with post-infection illness.
Reference: “Measurement of circulating viral antigens post-SARS-CoV-2 infection in a multicohort study” 9 October 2024, Clinical Microbiology and Infection. DOI: 10.1016/j.cmi.2024.09.001 www.clinicalmicrobiologyandinfection.com/article/S1198-743X(24)00432-4/abstract (PAYWALLED)
#mask up#covid#pandemic#wear a mask#covid 19#coronavirus#public health#sars cov 2#still coviding#wear a respirator#long covid#covid conscious#covid is not over#covid news#covid is airborne#covid isn't over#covid pandemic#covid19#covidー19#get vaccinated
56 notes
·
View notes
Text

Emilia Clarke’s mother has described how her daughter’s brain haemorrhage changed the Clarke family “in an instant”.
Jenny Clarke said it feels like her daughter’s brain haemorrhage – a bleed on the brain – “feels like yesterday” even though it was more than a decade ago.
The incident, which took place when Clarke was working out in a north London gym in 2011, was “completely out of the blue”, Mrs Clarke said.
She said her daughter fought to stay conscious even though she was in “the worst pain she could ever imagine”.
Mrs Clarke told PA: “It feels like yesterday to us really, because it was just such a profound shock.
“She had just started Game Of Thrones, the first season had been filmed and she had just come back from a press tour.
“And then she had her first brain haemorrhage which was completely out of the blue – it was a morning in March and she was in the gym and she suddenly felt this terrible pain in her head – she’s been quoted as saying it was the worst pain she could ever imagine.
“She also realised that something was seriously wrong with her because the pain was so intense.
“So she did her best, as she was lying semi-unconscious on the floor of the gym, to try and make sure she kept a sense of what was around her and she fought to make sure that she didn’t lose consciousness.”
Mrs Clarke added: “When she was rushed to a hospital in London, it was very difficult to establish what has happened to her – and that’s also something that we think is very important; maybe there isn’t enough specialist information and training to actually recognise what happens when you have a brain haemorrhage when you’re young.
“People expect people to have strokes and brain haemorrhages when they’re older, it’s a problem of older age, but Emelia was 23 when she had her first brain haemorrhage, so people didn’t recognise it as a brain haemorrhage.
“So it took a long time before she was admitted to the wonderful Queen Square (the National Hospital for Neurology and Neurosurgery), which is part of University College London Hospitals and literally her life was saved because of an intervention to stop the bleeding.
“But it was three weeks in hospital before we knew whether she was going to have another stroke, and whether she would have different health problems as a result of the brain haemorrhage.”
She added: “Rehabilitation is undervalued and under-prioritised and that’s clearly got to change as a key component of universal health coverage.
“It was such a shock when it happened to us, when Emilia had her brain injury.
“We’ve had thousands of people write to us, and so it’s not just our own lived experience, there’s just not enough provision, not enough services available.
#daenerys defense squad#daenerys appreciation#daenerys deserved better#i stand by daenerys#daenerys stormborn#dragon queen#queen daenerys#emilia clarke#khaleesi#breaker of chains#Sameyou#same you#daenerys#targaryen#Jenny Clarke#game of thrones#game of thrones daenerys#emilia clarke supremacy#emilia clarke ❤️#charity#donate#pro daenerys#pro dany#justice for daenerys
28 notes
·
View notes
Text

The Bhopal Tragedy
On the night of December 2nd, 1984, a Union Carbide plant in Bhopal, India, began leaking 27 tonnes of the deadly gas methyl isocyanate. None of the six safety systems designed to contain such a leak were operational, allowing the gas to spread throughout the city of Bhopal. Half a million people were exposed to the gas and 25,000 have died to date as a result of their exposure. More than 120,000 people still suffer from ailments caused by the accident and the subsequent pollution at the plant site. These ailments include blindness, extreme difficulty in breathing and gynaecological disorders. In the Immediate aftermath, the health care system immediately became overloaded. In the severely affected areas, nearly 70% were under-qualified doctors. Medical staff were unprepared for the thousands of casualties. Doctors and hospitals were not aware of proper treatment methods for MIC gas inhalation. There were mass funerals and cremations. Within a few days, trees in the vicinity became barren, and bloated animal carcasses had to be disposed of. 170,000 people were treated at hospitals and temporary dispensaries, and 2,000 buffalo, goats, and other animals were collected and buried. Supplies, including food, became scarce owing to suppliers' safety fears. Fishing was prohibited, causing further supply shortages. Formal statements after a few weeks were issued that air, water, vegetation, and foodstuffs were safe, but people were warned not to consume fish. The number of children exposed to the gases was at least 200,000. Within weeks, the State Government established a number of hospitals, clinics, and mobile units in the gas-affected area to treat the victims. A cohort of 80,021 exposed people was registered, along with a control group, a cohort of 15,931 people from areas not exposed to MIC. Nearly every year since 1986, they have answered the same questionnaire. It shows excess mortality and morbidity in the exposed group. Bias and confounding factors cannot be excluded from the study. Because of migration and other factors, 75% of the cohort is lost, as the ones who move out are not followed. A number of clinical studies are performed. The quality varies, but the different reports support each other. Studied and reported long-term health effects are: Eyes: Chronic conjunctivitis, scars on cornea, corneal opacities, early cataracts Respiratory tracts: Obstructive and/or restrictive disease, pulmonary fibrosis, aggravation of tuberculosis and chronic bronchitis Neurological system: Impairment of memory, finer motor skills, numbness, etc. Psychological problems: Post traumatic stress disorder (PTSD) Children's health: Peri- and neonatal death rates increased. Failure to grow, intellectual impairment, etc. Missing or insufficient fields for research are female reproduction, chromosomal aberrations, cancer, immune deficiency, neurological sequelae, post traumatic stress disorder (PTSD) and children born after the disaster. Late cases that might never be highlighted are respiratory insufficiency, cardiac insufficiency (cor pulmonale), cancer and tuberculosis. Bhopal now has high rates of birth defects and records a miscarriage rate 7x higher than the national average. The site has never been properly cleaned up and it continues to poison the residents of Bhopal.
29 notes
·
View notes
Text

Mike Luckovich
* * * *
The New York Times’ conspiracy theory flops spectacularly. White House press corps disgraces itself.
The New York Times ran an article noting that a neurologist from Walter Reed Military Hospital specializing in Parkinson’s Disease had visited the White House on eight occasions over the last eight months. A press briefing at the White House devolved into a shouting match as reporters from the Times and NBC accused White House spokesperson Karine Jean-Pierre of covering up information about President Biden’s health. Or, as the Times described the conduct of the press corps,
The White House briefing room devolved into shouting on Monday as the press secretary, Karine Jean-Pierre, repeatedly dodged and refused to answer questions about the president’s health, and whether visits to the White House by a Parkinson’s doctor were about the president.
The reporters apparently never considered that the Parkinson’s specialist could be treating other White House employees—including 1,000 military personnel—and that Jeane-Pierre was prohibited by federal privacy laws and national security from providing the requested information that might compromise military leaders. Instead, one reporter said the press was “miffed” with Ms. Jean-Pierre and accused her of “dodging questions” to which the press had the absolute right to answers—damn the privacy concerns of possible other patients in the White House.
Late in the day, the President's doctor reaffirmed that the President has been evaluated on three occasions by a neurologist—at each of his annual physicals, including in February of this year. The other visits by the Parkinson’s specialist were to see other members of the White House staff, including military combat veterans—who frequently suffer neurological damage from combat. The letter is here: Letter 7.8.24 - DocumentCloud.
I urge you to read the entire letter. It explains, in relevant part, that the Parkinson’s disease specialist visited the White House as part of a clinic for military personnel:
Prior to the pandemic, and following its end, [the Parkinson’s Disease specialist] has held regular Neurology Clinics at the White House Medical Clinic in support of the thousands of active-duty members assigned in support of White House operations. Many military personnel experience neurological issues related to their service, and Dr. Cannard regularly visits the WHMU as part of this General Neurology practice. We value the contributions he has made across the many patients he has treated in support of the White House and its personnel over these years.
So, the New York Times conspiracy theory went down in flames. But the treatment of Karine Jean-Pierre was despicable. It was racist and sexist. The condescension and wild accusations of a cover up by white male reporters who were “miffed” that a Black woman would not do their bidding is reprehensible.
Each of the reporters who accused Jean-Pierre of a cover-up owes a public apology to her, as do the editors of the New York Times and the other media outlets that allow the journalists to make reckless accusations before researching, considering, and thinking through other innocent explanations.
Robert B. Hubbell Newsletter
+
Amid all the calls for “cognitive tests” for Biden—but not Trump—journalists are committing malpractice by failing to note that President Biden released a detailed summary of his annual physical in February of this year. The full report is here: Health-Summary-2.28.pdf (whitehouse.gov). The examination included consultations with neurological experts at Walter Reed hospital. I urge you to read the entire report and consider how you would measure up to such a battery of tests!
On the issue of Biden’s neurological health, the report states the following:
An extremely detailed neurologic exam was again reassuring in that there were no findings which would be consistent with any cerebellar or other central neurological disorder, such as stroke, multiple sclerosis, Parkinson’s or ascending lateral sclerosis, nor are there any signs of cervical myelopathy. This exam did again support a finding of peripheral neuropathy in both feet. No motor weakness was detected. He exhibits no tremor, either at rest or with activity. He demonstrates excellent fine motor dexterity. But a subtle difference in heat/cold sensation could be elicited as it was last year. This heat/cold sensation deficit was detected a couple inches higher on his ankle/calf this year, which is not unexpected, There may, in fact, be day to day subjective variation of these findings, as during last year’s exam, this area of sensation deficit was actually found to be smaller than the year before.
So, Biden did have a “detailed neurological exam” four-and-half months ago. The widespread media demands that Biden “take a neurological exam” should be directed to Trump instead.
Predictably, this “proof” won’t be enough for the media. Just as the media refused to accept a certified copy of President Obama’s birth certificate, the goalposts will keep shifting.
The issue is not Joe Biden. It is Donald Trump—and the media’s arrogant refusal to apply the same scrutiny to Trump that it is applying to Biden. If they did, they would be demanding neurological exams of Trump and his withdrawal from the race. So far as we have been informed by Trump, his cognitive test consisted of recalling five objects: “Person. Woman. Man. Camera. TV.” Can you say, “double standard”?
Why isn’t the media making demands that Trump submit to “extremely detailed neurologic testing” by experts from a nationally recognized hospital?
[Robert B. Hubbell Newsletter]
#Mike Luckovich#Robert B. Hubbell#Robert b. Hubbell Newsletter#Biden#health documents#detailed neurological exam#double standard
9 notes
·
View notes
Text
An observation as I sit here eating chocolate on my front stoop after a long, grueling day of work; Last year, on the first day of Gemini season, I commented on how relentlessly windy it was. It struck me as funny and somewhat ironic, given that Gemini is an air sign, probably my favorite air sign at that. (Ohhh, how they fan the flames of my lion heart! ....Until they break it, or exacerbate the flames into a raging wildfire, of course.)
Today, Gemini season enters with the exact same powerful energy- stirring up all that's been stuck during Taurus season, and any residual, mucky energy from the winter (which seems to have finally flatlined.)
The sultry heat of our warmest day yet, paired with the ever swirling, cleansing wind, makes me feel mentally stimulated & renewed, and ready to embrace change. (It's also kind of burning my eyes because it's filled with pollen and dust. Things are rarely perfect, but I still fall madly in love with such moments.)
I've always felt that air is very important to my well-being; not only because I have basically NO air elementals in my fiery natal astrology chart to balance everything else. But also due to something deeper and somewhat unexplainable. If you believe in reincarnation and/or karma, perhaps something passed down or carried with me from all the "befores." I was born with my umbilical cord tightly wound around my neck. My Mom said I came out blue, silent, and not breathing. I was put under observation and monitored for a couple of days. It's been thought by mystics/light workers/etc. that we often "come back into the world the same way we went out." Who knows. I've grown more convinced I could be my Grandfather's only brother, reincarnated. He suffered a handful of freak accidents involving trauma to the head/neck before dying in a car crash-which nearly decapitated him-at 18 years old. Up until the moment of my birth, my parents had been expecting a boy, to be named Eric Robert. Alas, they ended up with Jennifer Lynne!
I experienced bouts of fainting from the day I was brought home from the hospital until about age 5, (terrifying my entire family one too many times.) It was eventually determined to be "breath-holding syndrome, temper related" after neurological testing ruled out seizures or anything of the sort.
When those episodes finally stopped, I always remember feeling "breathless" during times of anxiety or upset. My first boyfriend, very young, once fastened a leather bondage collar so tightly around my neck, I had PTSD for weeks. I tried to be tough and never told him how badly it hurt or how uncomfortable I was. To this day, in my adult life, I still get phantom feelings of being choked/strangled when I'm overwhelmed, stressed or emotional. My neck tightens and my pulse pounds, my ears fill up with pressure and I become faint. I can't be in a room with no air movement for more than a couple of minutes; an open door, window, or fan is a must. I just.....NEED AIR, DAMNIT! The human experience is so strange.
Oh, and what are the odds that Avatar The Last Airbender is practically my favorite show of all time? 🌀 (Fire Nation, represent! 🔥)
Thinking I've been alone this whole time, I gaze across the street and see an old man in a wheelchair, parked contently on his driveway, all alone with no lights on, quietly enjoying the gusts of wind and watching the gray clouds sail by above our heads. I tear up a bit, because that's just me, always. I cry to alchemize shit. I cry almost daily. It's how I release the weight of being an empath in this Godforsaken world. (My Mercury in Cancer is showing....)
Anyway, I'm too tired to look for typos, so those are my thoughts for the day. Another neighbor joins the old man to admire the breeze and indulge in a sweet conversation. My heart swells.
Thank you, my beloved moon in Scorpio, for compelling me to write today. My soul is right at home for a couple of days each month when you're in my natal moon sign.
Goodnight wind, goodnight old man, goodnight moon...
And welcome, Mercury-ruled Gemini archetype! ♊️ Here's to endless conversation, communication, spilling the tea, unfinished projects, witty banter, lots of thinking and probably not a lot of sleep! (You crazy, insomniac Gemini fucks!) 😂🩵
#ramblings#thoughts#gemini season#astrology#reincarnation#karma#scorpio moon#air#writers on tumblr#writerscommunity
2 notes
·
View notes