#H1N1 (Swine Flu) Vaccination Market
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr office adopted Tommy, an 11-year-old Pomeranian.
Text
H1N1 (Swine Flu) Vaccination Market : Trends and Future Growth Analysis by 2031

The "H1N1 (Swine Flu) Vaccination Market" is a dynamic and rapidly evolving sector, with significant advancements and growth anticipated by 2031. Comprehensive market research reveals a detailed analysis of market size, share, and trends, providing valuable insights into its expansion. This report delves into segmentation and definition, offering a clear understanding of market components and drivers. Employing SWOT and PESTEL analyses, the study evaluates the market's strengths, weaknesses, opportunities, and threats, alongside political, economic, social, technological, environmental, and legal factors. Expert opinions and recent developments highlight the geographical distribution and forecast the market's trajectory, ensuring a robust foundation for strategic planning and investment.
What is the projected market size & growth rate of the H1N1 (Swine Flu) Vaccination Market?
Market Analysis and Size
The H1N1 flu, sometimes also known as swine flu, is a type of influenza A virus. It was often known as swine flu and was a new combination of influenza viruses that infect pigs, birds and humans. There have been severe cases of influenza in recent times. As per the World Health Organization (WHO), annually, around 3 to 5 million cases of severe illness and approximately 2,90,000 to 6,50,000 respiratory deaths are because of seasonal influenza. Also, increasing levels of respiratory ailments and immune deficient ailments due to the increasing elderly population has further caused huge growth opportunities for the H1N1 (swine flu) vaccination market.
Data Bridge Market Research analyses that the H1N1 (swine flu) vaccination market, which was USD 13.29 billion in 2022, would rise to USD 21.51 billion by 2030 and is expected to undergo a CAGR of 6.20% during the forecast period 2023 to 2030. In addition to the insights on market scenarios such as market value, growth rate, segmentation, geographical coverage, and major players, the market reports curated by the Data Bridge Market Research also include depth expert analysis, patient epidemiology, pipeline analysis, pricing analysis, and regulatory framework.
Browse Detailed TOC, Tables and Figures with Charts which is spread across 350 Pages that provides exclusive data, information, vital statistics, trends, and competitive landscape details in this niche sector.
This research report is the result of an extensive primary and secondary research effort into the H1N1 (Swine Flu) Vaccination market. It provides a thorough overview of the market's current and future objectives, along with a competitive analysis of the industry, broken down by application, type and regional trends. It also provides a dashboard overview of the past and present performance of leading companies. A variety of methodologies and analyses are used in the research to ensure accurate and comprehensive information about the H1N1 (Swine Flu) Vaccination Market.
Get a Sample PDF of Report - https://www.databridgemarketresearch.com/request-a-sample/?dbmr=global-h1n1-swine-flu-vaccination-market
Which are the driving factors of the H1N1 (Swine Flu) Vaccination market?
The driving factors of the H1N1 (Swine Flu) Vaccination market include technological advancements that enhance product efficiency and user experience, increasing consumer demand driven by changing lifestyle preferences, and favorable government regulations and policies that support market growth. Additionally, rising investment in research and development and the expanding application scope of H1N1 (Swine Flu) Vaccination across various industries further propel market expansion.
H1N1 (Swine Flu) Vaccination Market - Competitive and Segmentation Analysis:
Global H1N1 (Swine Flu) Vaccination Market, By Vaccine Type (Intranasal, Conjugate, Attenuated Vaccines, Inactivated Vaccines, Intramuscular, and Toxoid), Type of Brand (Agripal, Fiuarix, Influgen, Influvac, Nasovac, Vaxigrip, and Others) and End User (Hospitals, Clinics, and Others) – Industry Trends and Forecast to 2031.
How do you determine the list of the key players included in the report?
With the aim of clearly revealing the competitive situation of the industry, we concretely analyze not only the leading enterprises that have a voice on a global scale, but also the regional small and medium-sized companies that play key roles and have plenty of potential growth.
Which are the top companies operating in the H1N1 (Swine Flu) Vaccination market?
Some of the major players operating in the H1N1 (swine flu) vaccination market are:
Sanofi (France)
Pfizer Inc. (U.S.)
GSK plc (U.K.)
Novartis AG (Switzerland)
Mylan N.V. (U.S.)
Baxter.(U.S.)
AstraZeneca (U.K.)
Johnson & Johnson Private Limited (U.S.)
Virbac (France)
Vetoquinol (France)
Zoetis (U.S.)
Novavax (U.S.).
Zydus Group (India).
Panacea Biotec (India).
SINOVAC (China).
Abbott (U.S.)
SEQIRUS (U.S.)
Cipla Inc (India)
Short Description About H1N1 (Swine Flu) Vaccination Market:
The Global H1N1 (Swine Flu) Vaccination market is anticipated to rise at a considerable rate during the forecast period, between 2024 and 2031. In 2023, the market is growing at a steady rate and with the rising adoption of strategies by key players, the market is expected to rise over the projected horizon.
North America, especially The United States, will still play an important role which can not be ignored. Any changes from United States might affect the development trend of H1N1 (Swine Flu) Vaccination. The market in North America is expected to grow considerably during the forecast period. The high adoption of advanced technology and the presence of large players in this region are likely to create ample growth opportunities for the market.
Europe also play important roles in global market, with a magnificent growth in CAGR During the Forecast period 2024-2031.
H1N1 (Swine Flu) Vaccination Market size is projected to reach Multimillion USD by 2031, In comparison to 2024, at unexpected CAGR during 2024-2031.
Despite the presence of intense competition, due to the global recovery trend is clear, investors are still optimistic about this area, and it will still be more new investments entering the field in the future.
This report focuses on the H1N1 (Swine Flu) Vaccination in global market, especially in North America, Europe and Asia-Pacific, South America, Middle East and Africa. This report categorizes the market based on manufacturers, regions, type and application.
Get a Sample Copy of the H1N1 (Swine Flu) Vaccination Report 2024
What are your main data sources?
Both Primary and Secondary data sources are being used while compiling the report. Primary sources include extensive interviews of key opinion leaders and industry experts (such as experienced front-line staff, directors, CEOs, and marketing executives), downstream distributors, as well as end-users. Secondary sources include the research of the annual and financial reports of the top companies, public files, new journals, etc. We also cooperate with some third-party databases.
Geographically, the detailed analysis of consumption, revenue, market share and growth rate, historical data and forecast (2024-2031) of the following regions are covered in Chapters
What are the key regions in the global H1N1 (Swine Flu) Vaccination market?
North America (United States, Canada and Mexico)
Europe (Germany, UK, France, Italy, Russia and Turkey etc.)
Asia-Pacific (China, Japan, Korea, India, Australia, Indonesia, Thailand, Philippines, Malaysia and Vietnam)
South America (Brazil, Argentina, Columbia etc.)
Middle East and Africa (Saudi Arabia, UAE, Egypt, Nigeria and South Africa)
This H1N1 (Swine Flu) Vaccination Market Research/Analysis Report Contains Answers to your following Questions
What are the global trends in the H1N1 (Swine Flu) Vaccination market?
Would the market witness an increase or decline in the demand in the coming years?
What is the estimated demand for different types of products in H1N1 (Swine Flu) Vaccination?
What are the upcoming industry applications and trends for H1N1 (Swine Flu) Vaccination market?
What Are Projections of Global H1N1 (Swine Flu) Vaccination Industry Considering Capacity, Production and Production Value? What Will Be the Estimation of Cost and Profit? What Will Be Market Share, Supply and Consumption? What about Import and Export?
Where will the strategic developments take the industry in the mid to long-term?
What are the factors contributing to the final price of H1N1 (Swine Flu) Vaccination?
What are the raw materials used for H1N1 (Swine Flu) Vaccination manufacturing?
How big is the opportunity for the H1N1 (Swine Flu) Vaccination market?
How will the increasing adoption of H1N1 (Swine Flu) Vaccination for mining impact the growth rate of the overall market?
How much is the global H1N1 (Swine Flu) Vaccination market worth? What was the value of the market In 2020?
Who are the major players operating in the H1N1 (Swine Flu) Vaccination market? Which companies are the front runners?
Which are the recent industry trends that can be implemented to generate additional revenue streams?
What Should Be Entry Strategies, Countermeasures to Economic Impact, and Marketing Channels for H1N1 (Swine Flu) Vaccination Industry?
Customization of the Report
Can I modify the scope of the report and customize it to suit my requirements? Yes. Customized requirements of multi-dimensional, deep-level and high-quality can help our customers precisely grasp market opportunities, effortlessly confront market challenges, properly formulate market strategies and act promptly, thus to win them sufficient time and space for market competition.
Inquire more and share questions if any before the purchase on this report at - https://www.databridgemarketresearch.com/inquire-before-buying/?dbmr=global-h1n1-swine-flu-vaccination-market
Detailed TOC of Global H1N1 (Swine Flu) Vaccination Market Insights and Forecast to 2031
Introduction
Market Segmentation
Executive Summary
Premium Insights
Market Overview
H1N1 (Swine Flu) Vaccination Market By Type
H1N1 (Swine Flu) Vaccination Market By Function
H1N1 (Swine Flu) Vaccination Market By Material
H1N1 (Swine Flu) Vaccination Market By End User
H1N1 (Swine Flu) Vaccination Market By Region
H1N1 (Swine Flu) Vaccination Market: Company Landscape
SWOT Analysis
Company Profiles
Continued...
Purchase this report – https://www.databridgemarketresearch.com/checkout/buy/singleuser/global-h1n1-swine-flu-vaccination-market
Data Bridge Market Research:
Today's trends are a great way to predict future events!
Data Bridge Market Research is a market research and consulting company that stands out for its innovative and distinctive approach, as well as its unmatched resilience and integrated methods. We are dedicated to identifying the best market opportunities, and providing insightful information that will help your business thrive in the marketplace. Data Bridge offers tailored solutions to complex business challenges. This facilitates a smooth decision-making process. Data Bridge was founded in Pune in 2015. It is the product of deep wisdom and experience.
Contact Us:
Data Bridge Market Research
US: +1 614 591 3140
UK: +44 845 154 9652
APAC: +653 1251 975
Email:- [email protected]
Browse More Reports:
Global Precision Farming Software Market – Industry Trends and Forecast to 2030
Global Oligosaccharides in Infant Nutrition Market – Industry Trends and Forecast to 2029
Global H1N1 (Swine Flu) Vaccination Market – Industry Trends and Forecast to 2030
Global Airbag Inflator Market - Industry Trends and Forecast to 2028
Global Veterinary Anti-Infective Market – Industry Trends and Forecast to 2029
#H1N1 (Swine Flu) Vaccination Market#H1N1 (Swine Flu) Vaccination Market Size#H1N1 (Swine Flu) Vaccination Market Share#H1N1 (Swine Flu) Vaccination Market Trends
0 notes
Text
0 notes
Photo

H1N1 (swine flu) Vaccination Market expected to grow at CAGR of 17% in the forecast period of 2018 to 2025 |Commonwealth Serum Laboratories, Zydus Cadila, Panacea Biotec, Shanghai Institute Of Biological Products
Get Free Sample Copy of This Report @ https://bit.ly/35fItwz
On the report of the Commercial H1N1 (swine flu) Vaccination Market report, the global market is expected to witness a relatively higher growth rate during the forecast period. H1N1 (swine flu) Vaccination market offers the company profile of major key players including progress trends, competitive landscape breakdown, and key in regions development status.
#H1N1 (swine flu) Vaccination market#H1N1 (swine flu) Vaccination market anlaysis#H1N1 (swine flu) Vaccination size#H1N1 (swine flu) Vaccination share#H1N1 (swine flu) Vaccination trend#H1N1 (swine flu) Vaccination outlook#H1N1 (swine flu) Vaccination insight#H1N1 (swine flu) Vaccination overview
0 notes
Text
Heather Cox Richardson
December 29, 2020 (Tuesday)
There is definitely a feeling of change in the air. For all his continuing insistence that he won the 2020 election, Trump is a lame duck.
Today’s complicated fight in the Senate over the one-time stimulus payment of $2000 illustrated that Senate Majority Leader Mitch McConnell (R-KY), not Trump, now controls the Republican caucus. Trump originally refused to sign the Consolidated Appropriations Act of 2021, the bill that contains the coronavirus relief measures, because he claimed he objected to its meager $600 stimulus payments. Six hundred dollars was the amount his negotiators had demanded, but he suddenly said he wanted them to be $2000. Democrats in the House jumped on Trump’s demand for the higher payment and they passed a measure on Monday to increase the payments.
Trump had attacked the bill largely because he is angry at McConnell and Senate Majority Whip John Thune (R-SD) (a whip keeps party members in line behind the party leader) for acknowledging Biden’s victory in November. He was trying to illustrate his power by refusing to sign the bill at all. But Sunday night he gave in without winning anything. Yet, he continued to say he wanted higher payments. The House was happy to give him what the Democrats had wanted all along; today, Trump lost the showdown in the Senate.
Senate Minority Leader Chuck Schumer (D-NY) introduced the measure, but Senate Majority Leader Mitch McConnell (R-KY) killed it. This enabled the two embattled Republican Senate candidates from Georgia both to support Trump and to claim they wanted higher payments, all without actually having to vote for the higher payments. McConnell bested Trump all around: he had no intention of raising those payments no matter what Trump tweeted... and he didn’t.
Trump’s influence in Washington is waning in other ways, too. Yesterday, the House repassed the National Defense Authorization Act over Trump’s veto. Trump claims to object to the bill for a number of reasons, including that it will require that military bases currently named for Confederate generals be renamed, but this is the measure into which Congress put the Corporate Transparency Act I wrote about a few days ago. It will undercut the country’s plague of so-called shell companies, which enable money laundering and other criminal activity because they are owned and operated in secret. The new measure will require that all owners and operators of such companies be clearly identified.
This will likely impact the Trump family, which uses shell companies.
There were other rumblings today that Trump’s post-presidential life might have some sticky places. The Manhattan District Attorney’s Office has hired forensic accountants to help investigate Trump and his businesses. This investigation is a criminal investigation. New York Attorney General Letitia James is in charge of a civil investigation into Trump’s businesses.
But the big thing which showed momentum is moving away from Trump is that President-Elect Joe Biden is forcefully criticizing the Trump administration for its failure to plan for distribution of the coronavirus vaccine.
With more than 330,000 Americans dead of Covid-19 and infections spiking, Biden today noted that the Trump administration has fallen behind on vaccine distribution. The effort got off to a poor start as the administration delivered fewer doses than it had promised and initially blamed Pfizer for a “miscommunication,” only to have Pfizer state that it had “millions of doses” in a warehouse but had received no information about where to send them.
The administration promised to vaccinate 20 million Americans by the end of December, but yesterday, the Centers for Disease Control and Prevention reported that it had administered just 2.1 million doses in two weeks, although that number is likely somewhat low because of lag times in reporting. At the current rate, Dr. Leana S. Wen writes in the Washington Post, we can expect to achieve herd immunity in 10 years.
The administration at first refused to share information with the Biden camp about distribution, claiming there was a plan, even though, when finally part of discussions in early December, Biden said “[t]here is no detailed plan that we've seen, anyway, as to how you get the vaccine out of a container, into an injection syringe, into somebody's arm.”
Health and Human Services Secretary Alex Azar responded that Biden’s claim was “nonsense.” “[W]e have comprehensive plans from the Centers for Disease Control and Prevention working with 64 public health jurisdictions across the country as our governors have laid out very detailed plans that we’ve worked with them on. We’re leveraging our retail pharmacies, our hospitals, our public health departments, our community health centers.” Azar said the distribution process was being “micromanaged and controlled by the United States military, as well as our incredible private sector. We do hundreds of millions of vaccinations a year. We’re leveraging the systems that are known, and that work here in the United States." Azar assured Fox News Sunday host Chris Wallace that, as soon as the vaccines were approved, the government would be shipping them “to all of the states and territories that we work with. And within hours they can be vaccinating,”
It turns out Biden was more right than Azar. The administration planned simply to get the vaccines to the states, and then leave to them the problem of actually getting the vaccines into people’s arms. But state Departments of Health are strapped for money after trying to manage the pandemic for nine months, and had been allotted only $6 million apiece to make the distributions happen. (The new Consolidated Appropriations Act that Trump just signed has significantly more money in it for distribution.)
“The Trump administration’s plan to distribute vaccines is falling behind, far behind,” Biden said today. “As I long feared and warned, the effort to distribute and administer the vaccine is not progressing as it should.”
Finally stung, Trump tweeted tonight that “It is up to the States to distribute the vaccines once brought to the designated areas by the Federal Government. We have not only developed the vaccines, including putting up money to move the process along quickly, but gotten them to the states. Biden failed with Swine Flu!” (Biden was not in charge of the Obama Administration’s response to H1N1 in 2009, which broke out three months after Obama took office.)
Biden promised to invoke the National Defense Production Act, a law that permits the president to require companies to produce goods at the same time that it guarantees them a market for those goods, to speed up the production of supplies necessary to distribute the vaccine quickly. “I have directed my team to prepare a much more aggressive effort, with more federal involvement and leadership to get things back on track,” he said.
But he warned that we are behind and, breaking with the Trump administration, warned that things are going to get much worse before they get better. The spike in infections along with the fallout from holiday gatherings means we will see high case numbers in January and high death tolls in February. It will be mid-March, he warns, before we see improvement. “The next few weeks and months are going to be very tough, a very tough period for our nation — maybe the toughest during this entire pandemic,” Biden said. “I know it’s hard to hear, but it’s the truth.”
“We are going to get through this. Brighter days are coming,” Biden said. “But it’s going to take all of the grit and determination we have as Americans to get it done.”
4 notes
·
View notes
Photo

I actually had a different multi-page comic prepped for today, but over the weekend I got a wild hare to do something on topic right now. So if you've ever wondered how a disease can jump from other animals to us, now you know!
Species portrayed: Rabies virus (Rabies lyssavirus), SARS-CoV-2, Lyme disease (Borrelia sp.), Ebola (Ebolavirus sp.), human (Homo sapiens), domestic pig, (Sus scrofa domesticus) domestic chicken (Gallus gallus domesticus), domestic dog (Canis lupus familiaris), domestic cow (Bos taurus), masked palm civet (Paguma larvata), Chinese pangolin (Manis pentadactyla), large flying fox (Pteropus vampyrus), domestic cat (Felis catus), Senegal parrot (Poicephalus senegalus), bearded dragon (Pogona sp.), domestic rabbit (Oryctolagus cuniculus domesticus)
(Just a reminder that I have stickers and other fun merch at my Redbubble store, and you can also tip me for my work at my Ko-Fi! Like many people, my income has been pretty badly affected by current circumstances, so every little boost will help.)
Transcript under cut.
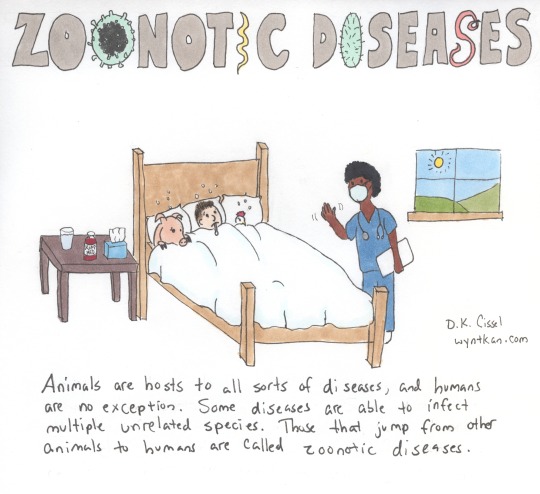
[Title: Zoonotic Diseases - the second O and the I in Zoonotic, and the I and season S in Diseases have been replaced by drawings of bacteria and viruses]
[First panel: A doctor in scrubs and carrying a chart waves to a man, a pig and a chicken all laying sick in bed. A table by the bed holds tissues, cough medicine and a glass of water. The window nearby shows a view out onto a sunny landscape.]
Animals are hosts to all sorts of diseases, and humans are no exception. Some diseases are able to infect multiple unrelated species. Those that jump from other animals to humans are called zoonotic diseases.
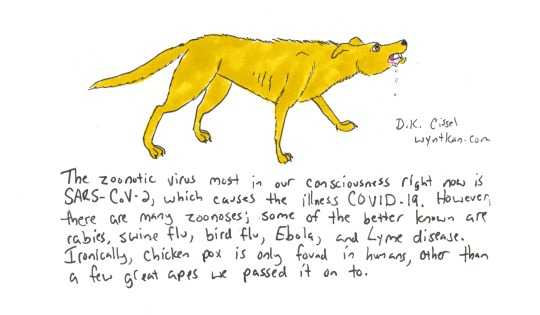
[Second panel: A yellow short-haired dog snarls and foams at the mouth.]
The zoonotic virus most in our consciousness right now is SARS-CoV-2, which causes the illness COVID-19. However, there are many zoonoses; some of the better known are rabies, swine flu, bird flu, Ebola, and Lyme disease. Ironically, chicken pox is only found in humans, other than a few great apes we passed it on to.
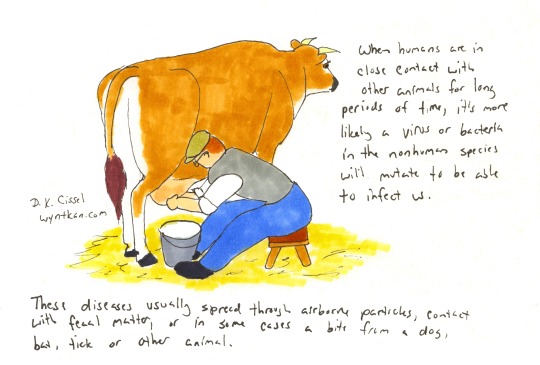
[Third panel: a man sits on a stool while milking a Jersey cow into a pail.]
When humans are in close contact with other animals for long periods of time, it’s more likely a virus or bacteria in the nonhuman species will mutate to be able to infect us. These diseases usually spread through airborne particules, contact with fecal matter, or in some cases a bite from a dog, bat, tick or other animal.
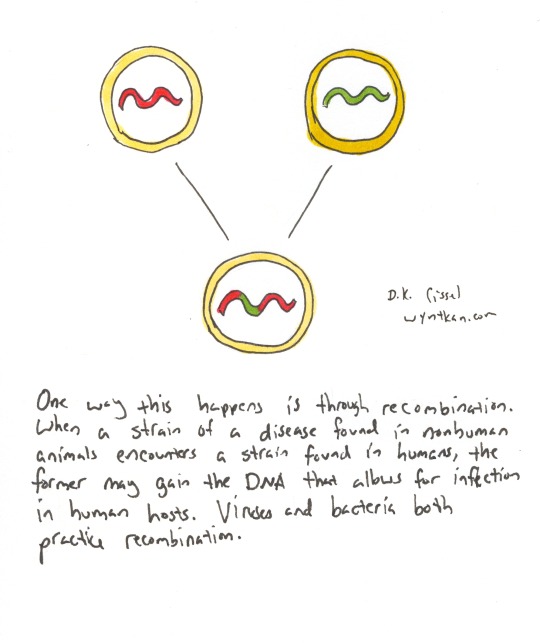
[Fourth panel: Three circles with squiggles inside them represent viruses. One has a red squiggle, another has a green squiggle, and lines from these two point to the third which has a red and green squiggle.]
One way this happens is through recombination. When a strain of a disease found in nonhuman animals encounters a strain found in humans, the former may gain the DNA that allows for infection in human hosts. Viruses and bacteria both practice recombination.
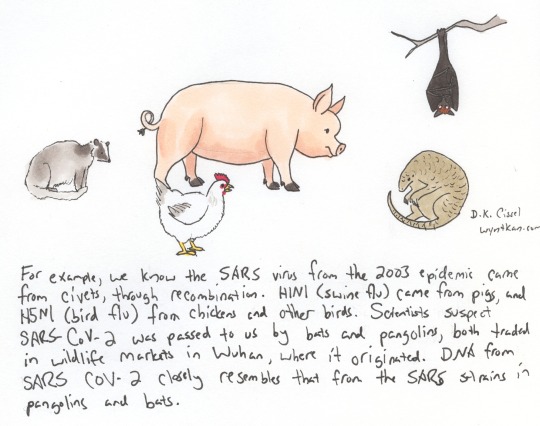
[Fifth panel: Several animals are on a blank background, including a masked palm civet, a domestic pig, a domestic chicken, a Chinese pangolin, and a large flying fox bat.]
For example, we know the SARS virus from the 2003 epidemic came from civets, through recombination. H1N1 (swine flu) came from pigs, and H5N1 (bird flu) from chickens and other birds. Scientists suspect SARS-CoV-2 was passed to us by bats and pangolins, both traded in wildlife markets in Wuhan, where it originated. DNA from SARS-CoV-2 closely resembles that from the SARS strains in pangolins and bats.
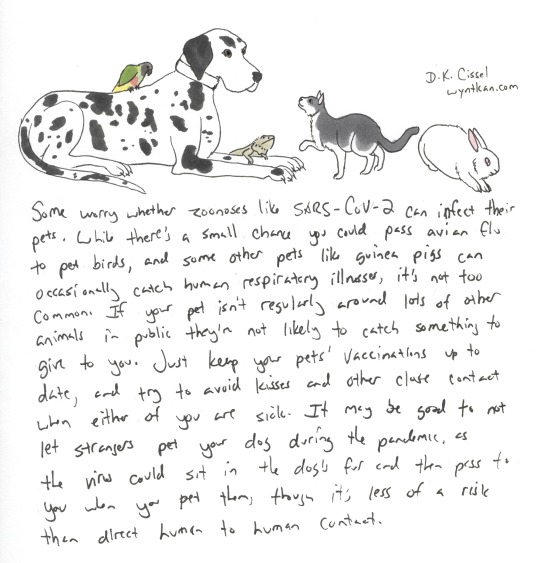
[Sixth panel: More animals on a blank background, including a Senegal parrot sitting on the back of a great dane, a bearded dragon, a domestic cat, and a domestic rabbit.]
Some worry whether zoonoses like SARS-C0V-2 can infect their pets. While there’s a small chance you could pass avian flu to pet birds, and some other pets like guinea pigs occasionally catch human respiratory illnesses, it’s not too common. If your pet isn’t regularly around lots of other animals in public they’re not likely to catch something to give to you. Just keep your pets’ vaccination up to date, and try to avoid kisses and other close contact when either of you are sick. It may be good to not let strangers pet your dog during the pandemic, as the virus could sit in the dog’s fur and then pass to you when you pet them, though it’s less of a risk than direct human to human contact.
[Seventh panel: A golden retriever in green scrubs and a stethoscope sits looking at the viewer. Next to her is a sign that says “Wash hands! Clean everything! Lots of space! Good hygiene! Let wild animals stay wild!”]
How do we prevent zoonoses? By limiting close exposure to wild animals, and keeping all captive animals in clean, uncrowded quarters. Treat sick animals as soon as possible. If you handle animals, even pets, wash your hands thoroughly before eating, drinking, or otherwise putting your hands near your face. Be familiar with zoonoses that the animals in your life may be susecptible to so you can all stay healthy!
35 notes
·
View notes
Link
We have been paying dearly for China's lies.
"This is one of the worst cover-ups in human history, and now the world is facing a global pandemic," said Rep. Michael T. McCaul, the ranking Republican member of the House Foreign Affairs Committee, before the US intelligence community concluded, in a classified report to the White House, that China has concealed the origin and extent of the catastrophic global coronavirus outbreak.
The Chinese Communist Party's "failure has unleashed a global contagion killing thousands", wrote Cardinal Charles Maung Bo, president of the Federation of Asian Bishops' Conferences, on April 1. "As we survey the damage done to lives around the world, we must ask who is responsible?"
"... there is one government that has primary responsibility for what it has done and what it has failed to do, and that is the CCP [Chinese Communist Party] regime in Beijing. Let me be clear — it is the CCP that has been responsible, not the people of China... Lies and propaganda have put millions of lives around the world in danger... In recent years, we have seen an intense crackdown on freedom of expression in China. Lawyers, bloggers, dissidents and civil society activists have been rounded up and have disappeared."
One more person has just disappeared: Ai Fen, a Chinese physician who was head of the emergency department at Wuhan Central Hospital, had worked with the late Dr. Li Wenliang. Ai, who claimed that her bosses silenced her early warnings about coronavirus, appears to have vanished. Her whereabouts, according to 60 Minutes Australia, are unknown. The journalists who saw what happened inside Wuhan have also disappeared. Caixin Global reported that the laboratories which sequenced the coronavirus in December were ordered by Chinese officials to hand over or destroy the samples and not release their findings. "If I had known what was to happen, I would not have cared about the reprimand, I would have fucking talked about it to whoever, where ever I could", Ai Fen said in an interview in March. Those were her last recorded words.
There is no record at all, however, about how this pandemic began. Wet market? A cave full of bats? Pangolins? Or a bio-weapons laboratory? No foreign doctors, journalists, analysts or international observers are present in Wuhan. Why, if the virus came out of a wet market or a cave, did China suppress inquiries to such an extent? Why, in December, did Beijing order Chinese scientists to destroy proof about the virus? Why did Chinese officials claim that US soldiers brought the virus to Wuhan? Why should it be scandalous that a US President calls a virus that began in China a "Chinese virus"?
Who announced on January 11 that Wuhan's wet market was the origin of this epidemic? The Chinese regime. It was later discovered that the first known case of coronavirus traced back to November 17, 2019.
The same Chinese regime later claimed that this coronavirus "may not have originated in China". What respected scientist or institution can now trust anything that comes out of China?
Many leading scientists have dismissed the claim that the Covid-19 virus was an engineered pathogen. This conclusion was seemingly based on the fact that Wuhan has two major virus research labs: the Wuhan Center for Disease Control and Prevention, which is apparently less than a mile from the market, and the Wuhan Institute of Virology, a biosafety level 4 (BSL-4) laboratory, handling the world's most deadly pathogens, located just seven miles from the market. The story was immediately and emphatically trashed as a "conspiracy theory".
Those scientists claim that the virus likely originated among wildlife before spreading to humans, possibly through a food market in Wuhan. They say that, through genetic sequencing, they have identified the culprit for Covid-19 as a bat coronavirus. End of story? Science, thankfully, begins by asking questions and then seeking answers.
Bats were not, it seems, sold at Wuhan's wet market. The Lancet noted in a January study that the first Covid-19 case in Wuhan had no connection to the market. The Lancet's paper, written by Chinese researchers from several institutions, detailed that 13 of the 41 first cases had no link to the market. "That's a big number, 13, with no link," commented Daniel Lucey, an infectious disease specialist at Georgetown University. So how did the epidemic start?
"Now it seems clear that [the] seafood market is not the only origin of the virus, but to be honest we still do not know where the virus came from now", notes Bin Cao, pulmonary specialist at Capital Medical University, and the corresponding author of the Lancet article.
US Secretary of State Mike Pompeo has said that China's Communist Party is withholding information about the coronavirus.
If we do not know, it is necessary be open to all possibilities.
"Less than 300 yards from the seafood market is the Wuhan branch of the Chinese Center for Disease Control and Prevention" wrote David Ignatius of the Washington Post.
"Researchers from that facility and the nearby Wuhan Institute of Virology have posted articles about collecting bat coronaviruses from around China, for study to prevent future illness. Did one of those samples leak, or was hazardous waste deposited in a place where it could spread?".
"Collecting viruses" presumably does not exclude the possibility of a "leaked virus". Worse, if China is not able to protect its laboratories, it needs to be held accountable and made to pay for the devastating global damage.
"Experts know the new coronavirus is not a bioweapon. They disagree on whether it could have leaked from a research lab", stated The Bulletin of the Atomic Scientists. Professor Richard Ebright of Rutgers University's Waksman Institute of Microbiology, and a major biosecurity expert, agreed with the Nature Medicine authors' argument that the coronavirus was not manipulated by humans. But Ebright does think it possible that the Covid-19 started as an accidental leak from a laboratory, such as one of the two in Wuhan, which are known to have been studying bat viruses:
"Virus collection or animal infection with a virus having the transmission characteristics of the outbreak virus would pose substantial risk of infection of a lab worker, and from the lab worker, the public."
Ebright has also claimed that bat coronaviruses are studied in Wuhan at Biosafety Level 2, "which provides only minimal protection" compared with the top BSL-4.
"We don't know what happened, but there are a lot of reasons to believe that this indeed was a release of some sort", China expert Gordon Chang said to Die Weltwoche.
"No one has been able to study it. How can you say it's not a release from a lab if you can't go to the lab? Indeed, we have seen Beijing do its best to prevent virologists and epidemiologists from actually going to Wuhan. The World Health Organization team went to Wuhan for like half a day with only part of the team."
That is another major problem. The potential major investigator of the Wuhan coronavirus pandemic's origin, the World Health Organization (WHO), is now accused of being "China's coronavirus' accomplice". As late as January 14, the WHO quoted Chinese health officials claiming there had been no human transmissions of the coronavirus within the country yet.
China poses a biosecurity risks for the entire planet. One year before the first coronavirus case was identified in Wuhan, US Customs and Border Protection agents at Detroit Metro Airport stopped a Chinese biologist with three vials labeled "Antibodies" in his luggage. According to an unclassified FBI tactical intelligence report obtained by Yahoo News:
"Inspection of the writing on the vials and the stated recipient led inspection personnel to believe the materials contained within the vials may be viable Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) materials."
Why is China trafficking in dangerous viruses in the first place?
According to Yanzhong Huang, a senior fellow for Global Health at the Council on Foreign Relations:
"A safety breach at a Chinese Center for Disease Control and Prevention lab is believed to have caused four suspected SARS cases, including one death, in Beijing in 2004. A similar accident caused 65 lab workers of Lanzhou Veterinary Research Institute to be infected with brucellosis in December 2019. In January 2020, a renowned Chinese scientist, Li Ning, was sentenced to 12 years in prison for selling experimental animals to local markets".
In February, Botao Xiao and Lei Xiao, from Guangzhou's South China University of Technology, wrote in a research paper:
"In addition to origins of natural recombination and intermediate host the killer coronavirus probably originated from a laboratory in Wuhan. Safety level [sic] may need to be reinforced in high risk biohazardous laboratories".
Xiao later told the Wall Street Journal that he had withdrawn the paper because it "was not supported by direct proofs".
Chinese laboratory mistakes have happened before. By 2010, researchers published as fact: "The most famous case of a released laboratory strain is the re-emergent H1N1 influenza-A virus which was first observed in China in May of 1977 and in Russia shortly thereafter". The virus may have escaped from a lab attempting to prepare a vaccine in response to the U.S. swine flu pandemic alert.
In 1999 the most senior defector in the US from the Soviet biological warfare program, Ken Alibek, revealed that Soviet officials concluded that China had suffered a serious accident at one of its secret biological plants, causing two major epidemics of fever that had swept China in the late 1980s. "Our analysts", Alibek stated in his book, Biohazard, "concluded that they were caused by an accident in a lab where Chinese scientists were weaponizing viral diseases".
In 2004, the World Health Organization disclosed that the latest outbreak of "severe acute respiratory syndrome" (SARS) in China involved two researchers who were working with the virus in a Beijing research lab. The WHO denounced Chinese breaches of safety procedures, and director of the Center for Disease Control and Prevention, Li Liming, resigned. Science magazine also stated that "for the third time in less than a year, an outbreak of SARS seems to have originated from a failure in laboratory containment".
Moreover, three years ago, when China opened the laboratory in Wuhan, Tim Trevan, a Maryland biosafety specialist, told Nature that he worried about the safety of the building because "structures where everyone feels free to speak up and openness of information are important." Free speech and open information: exactly what Chinese regime fought against in December and January.
A Chinese video about a key researcher in Wuhan, Tian Junhua, which was released a few weeks before the outbreak in Wuhan, shows Chinese researchers handling bats that contained viruses. In the video (produced by China Science Communication, run by the China Association for Science and Technology), Tian says:
"I am not a doctor, but I work to cure and save people... I am not a soldier, but I work to safeguard an invisible national defense line".
Tian is also reported as having said:
"I can feel the fear: the fear of infections and the fear of getting lost. Because of the fear, I take every step extremely cautiously. The more scared I feel, the more care I take in executing every detail. Because the process of you finding the viruses is also when you can be exposed to them the easiest. I do hope these virus samples will only be preserved for scientific research and will never be used in real life".
For a month, the Chinese Communist Party, instead of fighting the contagion, did everything possible to censor all information about the Covid-19 outbreak. After President Xi Jinping declared "a people's war" on the epidemic on January 20, Chinese security services pursued 5,111 cases of "fabricating and deliberately disseminating false and harmful information". The Chinese Human Rights Defenders documented several types of punishment, including detention, disappearance, fines, interrogations, forced confessions and "educational reprimand".
After that, China lied about the real number of deaths. There are photographs of long lines of stacked urns greeting family members of the dead at funeral homes in Wuhan. Outside one funeral home, trucks shipped in 2,500 urns. According to Chinese official figures, 2,548 people in Wuhan have died of the Covid-19. According to an analysis by Radio Free Asia, seven funeral homes in Wuhan were each handing out 500 funeral urns containing remains for 12 days, from March 23 to the traditional tomb-sweeping festival of April 5, a time that would indicate up to 42,000 urns, or ten times higher than the official figure.
In February, it was reported that Wuhan crematoriums were working around the clock to cope with the massive influx of infected bodies. Wuhan's officials are apparently pushing relatives of the victims to bury the dead "quickly and quietly".
"Natural virus" does not exclude its fallout from a laboratory where pathogens are collected and studied. The Nature Medicine authors "leave us where we were before: with a basis to rule out [a coronavirus from] a lab construct, but no basis to rule out a lab accident", Professor Ebright commented.
"Debate may rage over which center it is, but at this point it seems undeniable that a center has been directly involved with research on viruses, although not necessarily on the creation of a virus" wrote Father Renzo Milanese, a longtime Catholic missionary in Hong Kong.
"In other words, the virus passed from a research center in Wuhan early on. More importantly there is also no question that the authorities were aware of the dangerousness of the virus, that they did not inform anyone and that they tried to keep the facts hidden".
US Senator Josh Hawley has introduced a resolution calling for an international investigation into China's handling of the spread of the virus. According to Hawley:
"The Chinese Communist Party was aware of the reality of the virus as early as December but ordered laboratories to destroy samples and forced doctors to keep silent. It is time for an international investigation into the role their cover-up played in the spread of this devastating pandemic".
Admitting a fault, as the Japanese did after the Fukushima nuclear accident in 2011, might be one way for a country to be accepted again by the international community. Censoring, denying and covering up, as China is doing, will not.
"China claims that the deadly virus did not escape from its biolab," said a China specialist with the Population Research Institute, Steven W. Mosher. "Fine. Prove it by releasing the research records of the Wuhan lab".
27 notes
·
View notes
Text
SEND ONE TO YOUR UK MP NOW
The Vaccine Letter
Dear MP
I write to you today as a concerned constituent.
As we all know there is much talk at the moment of the new coronavirus vaccine. However there are aspects of this conversation that are causing me great concern.
Firstly there is the discussion around mandation and that venues and work places will be able to ask you for proof of vaccination. This is ethically and morally problematic. It is in direct contravention to the Nuremberg Code. The first stipulation of which is “The voluntary consent of the human subject is absolutely essential.” This cannot be given if it is mandated or if people are coerced due to other potential restrictions on their freedoms and liberties eg not being able to go to places of work or leisure.
A petition was started back in August on this matter – https://tinyurl.com/VaccineRestrictions and at the time of writing had over 245,000 signatures. The Government’s response was less than satisfactory. It merely stated that “There are currently no plans to place restrictions on those who refuse to have any potential Covid-19 vaccine.” This response was given on 11th Sept 2020 so is now over two months old and we have recently seen Matt Hancock state that he will not rule out mandating vaccines. However even if the Government does not itself place restrictions upon individuals for choosing to not have the vaccine it ought to be proactively protecting its people from others doing so. The Government do not grant us our rights they are there to protect them, this includes bodily autonomy and freedom from discrimination. Therefore I request you call for this debate to be heard and to do all you can to bring about a Bill preventing discrimination on the basis of vaccine status in any form in the UK including airports, whether this be by bringing forward a Private Members Bill or by lobbying the Government as a matter of urgency.
Please let me know your thoughts and what action you will take on this matter.
Secondly there is talk of shutting down all reasonable debate on the matter of the vaccine under the guise of “anti-vax”. This is a gross overreaction as well as a misnomer. Things based on truth, science and transparency do not fear debate or criticism as they know they will stand the test of time. So therefore why does Parliament fear it regarding the Covid vaccine? Shutting down a debate does more harm than to engage and attempt to rectify the issues. It’s also a huge infringement upon free speech. Surely this is not a path one wants to go down especially not to the point of punitive punishments as has been suggested? This doesn’t just apply to individual members of the public, there are also hundreds of respected doctors who raise concerns over vaccine safety, yet they are shut down and censored. Where is the open scientific debate?
As stated it’s also a misnomer, there are thousands upon thousands of people who have all other vaccines who would choose to not have the Covid vaccine. They are not “anti-vaxxers” and I would again urge Parliament to stop such sweeping statements in an effort to undermine genuine concerns.
Here are a number of concerns that I and many others hold about the Covid-19 vaccine –
These vaccines are being rushed through, therefore it is impossible to know they are safe. Vaccines normally have 5-10 years safety testing.
The last rushed through vaccine was for H1N1 back in 2009 from which people went on to develop debilitating narcolepsy for which the Government paid out £60m in compensation, but some of these symptoms didn’t emerge until 4yrs down the line, giving further weight to the previous point.
The 1976 Swine Flu scare in the US led to 46 million Americans taking a vaccine to avoid a pandemic. That resulted in 4,500 Americans claiming damages of up to $3.4bn. Two thirds of the claims were for neurological damage or death.
Not only is the Pfizer vaccine rushed through, it is also using mRNA technology which is brand new so it is not even comparable to any other vaccine on the market so we cannot expect similar results and may have unexpected long term consequences.
Pfizer has a shocking track record including the largest ever health care fraud payout in the US of $2.3bn. They have also been fined £90m by a competition watchdog for unfair pricing to the NHS by hiking up the cost of Anti epilepsy drug by 2,500 %. Charging the taxpayer an extra £48 million than the actual price which is £2 million per year and we are entrusting them with a new vaccine which they have refused to sell on a non-profit basis?
The MHRA have put out a tender for an AI system to deal with large numbers of expected adverse reactions to the new vaccine.
These are not “conspiracy” nor are they “anti-vax”, they are genuine and valid concerns that many people have. I would be interested in your thoughts on each of the points raised and whether you yourself think on this basis that the vaccine will be safe and if so why? Even if you do believe it’s safe will you make a commitment to allowing reasoned open debate and therefore not voting in support of any legislation brought forward to criminalise any free speech deemed “anti-vax”? As well as doing what you can to bring about
Kind regards,
2 notes
·
View notes
Text
The inclusion of sex-specific information in textbooks is dependent on the availability of sex-specific data, but because women have largely been excluded from medical research this data is severely lacking. Even the very basics of sex determination have a sex data gap: since the landmark 1990 paper that identified the Y chromosome as ‘the’ sex-determining region, the female sex has – the irony – been seen as the default. But in this case, the default didn’t mean we focused on the female. Rather, research instead focused on testes development as the supposedly ‘active’ process, while female sexual development was seen as a passive process – until 2010, when we finally started researching the active process of ovarian determination. Most early research into cardiovascular disease was conducted on men, and women continue to be underrepresented, making up only 25% of participants across thirty-one landmark trials for congestive heart failure between 1987 and 2012.
Women represent 55% of HIV-positive adults in the developing world, and in parts of Africa and the Caribbean women aged five to twenty-four are up to six times more likely to be HIV-positive than young men of the same age. We also know that women experience different clinical symptoms and complications due to HIV, and yet a 2016 review of the inclusion of women in US HIV research found that women made up only 19.2% of participants in antiretroviral studies, 38.1% in vaccination studies and 11.1% in studies to find a cure.
Because of their routine exclusion from clinical trials we lack solid data on how to treat pregnant women for pretty much anything. We may not know how a disease will take hold or what the likely outcome may be, although the WHO warns that many diseases can have ‘particularly serious consequences for pregnant women, or can harm the foetus’. Some strains of influenza virus (including the 2009 H1N1 swine flu virus) have ‘particularly severe symptoms during pregnancy’. There is also evidence that SARS can be more severe during pregnancy. It is of course understandable that a pregnant woman may be reluctant to take part in medical research, but this doesn’t mean that we have to just throw our hands up in the air and accept that we know nothing: we should be routinely and systematically tracking, recording and collating pregnant-women’s health outcomes. But we aren’t – not even during pandemics: during the 2002-4 SARS outbreak in China, pregnant-women’s health outcomes were not systemically tracked and ‘consequently’, the WHO points out, ‘it was not possible to fully characterize the course and outcome of SARS during pregnancy’. Another gender data gap that could have been so easily avoided, and information that will be lacking for when the next pandemic hits.
Like the failure to include women in anatomy textbooks, the failure to include women in medical trials is a historical problem that has its roots in seeing the male body as the default human body, but this traditional bias was radically enhanced in the 1970s, to the great detriment of women’s health, following one of the biggest medical scandals of the twentieth century. In 1960 doctors began prescribing thalidomide to pregnant women who suffered from morning sickness. The drug, which had been available as a mild over-the-counter sedative in many countries since the late 1950s, was considered safe because its developers ‘could not find a dose high enough to kill a rat’. But while it didn’t kill rats, it did affect foetal development (something that in fact the manufacturers knew as early as 1959). Before the drug was taken off the market in 1962, over 10,000 children had been born around the world with thalidomide-related disabilities. In the wake of the scandal, the US Food and Drug Administration (FDA) issued guidelines in 1977 excluding women of childbearing potential from drug trials. This exclusion went unquestioned. The acceptance of the male norm went unquestioned. The male norm continues to go unquestioned by many today, with some researchers continuing to insist, in the face of all the evidence, that biological sex doesn’t matter. One public-health researcher revealed that she had received the following feedback on two different grant applications: ‘I wish you’d stop with all this sex stuff and get back to science’, and ‘I’ve been in this field for 20 years and this [biological difference] doesn’t matter’. It isn’t just anonymous notes, either. A 2014 op-ed published in the journal Scientific American complained that including both sexes in experiments was a waste of resources; in 2015 an op-ed in the official scientific journal of the US National Academy of Sciences insisted that ‘focusing on preclinical sex differences will not address women’s and men’s health disparities’.
Alongside insisting that sex differences don’t matter, some researchers advocate against the inclusion of women in research on the basis that while biological sex may matter, the lack of comparable data arising from the historical data gap makes including women inadvisable (talk about adding insult to injury). Female bodies (both the human and animal variety) are, it is argued, too complex, too variable, too costly to be tested on. Integrating sex and gender into research is seen as ‘burdensome’. It is seen as possible for there to be ‘too much gender’, and for its exclusion to be acceptable on the basis of ‘simplification’ – in which case it’s worth noting that recent studies on mice have actually shown greater variability in males on a number of markers. So who’s too complicated now? Beyond the argument that women’s bodies, with their fluctuating, ‘atypical’ hormones, are simply inconvenient research vessels, researchers also defend their failure to include women in trials by claiming that women are harder to recruit. And it is certainly true that, due to women’s care-giving responsibilities they have less leisure time and may find it harder to make, for example, clinic appointments during the school run. However, this is an argument for adapting trial schedules to women, rather than simply excluding them, and in any case, it is possible to find women if you really want to. While reviews of FDA-mandated medical product trials found that women made up only 18% of participants in trials for endovascular occlusion devices (used if your foetal blood vessel hasn’t closed of its own accord) and 32% of participants in studies on coronary stents (which, incidentally, are another device where women have worse outcomes than men), women represented 90% and 92% of participants in facial wrinkle correction trials and dental device trials, respectively.
- Caroline Criado-Pérez’s Invisible Women: Exposing Data Bias in a World Designed for Men
13 notes
·
View notes
Link
* * * *
LETTERS FROM AN AMERICAN
December 29, 2020
Heather Cox Richardson
There is definitely a feeling of change in the air. For all his continuing insistence that he won the 2020 election, Trump is a lame duck.
Today’s complicated fight in the Senate over the one-time stimulus payment of $2000 illustrated that Senate Majority Leader Mitch McConnell (R-KY), not Trump, now controls the Republican caucus. Trump originally refused to sign the Consolidated Appropriations Act of 2021, the bill that contains the coronavirus relief measures, because he claimed he objected to its meager $600 stimulus payments. Six hundred dollars was the amount his negotiators had demanded, but he suddenly said he wanted them to be $2000. Democrats in the House jumped on Trump’s demand for the higher payment and they passed a measure on Monday to increase the payments to $2000.
Trump had attacked the bill largely because he is angry at McConnell and Senate Majority Whip John Thune (R-SD) (a whip keeps party members in line behind the party leader) for acknowledging Biden’s victory in November. He was trying to illustrate his power by refusing to sign the bill at all. But Sunday night he gave in without winning anything, and yet continued to say he wanted higher payments. The House was happy to give him what the Democrats had wanted all along, but today Trump lost the showdown in the Senate.
Senate Minority Leader Chuck Schumer (D-NY) introduced the measure, but Senate Majority Leader Mitch McConnell (R-KY) killed it. This enabled the two embattled Republican Senate candidates from Georgia both to support Trump and to claim they wanted higher payments, all without actually having to vote for the higher payments. McConnell bested Trump all around: he had no intention of raising those payments no matter what Trump tweeted... and he didn’t.
Trump’s influence in Washington is waning in other ways, too. Yesterday, the House repassed the National Defense Authorization Act over Trump’s veto. Trump claims to object to the bill for a number of reasons, including that it will require that military bases currently named for Confederate generals be renamed, but this is the measure into which Congress put the Corporate Transparency Act I wrote about a few days ago. It will undercut the country’s plague of so-called shell companies, which enable money laundering and other criminal activity because they are owned and operated in secret. The new measure will require that all owners and operators of such companies be clearly identified.
This will likely impact the Trump family, which uses shell companies.
There were other rumblings today that Trump’s post-presidential life might have some sticky places. The Manhattan District Attorney’s Office has hired forensic accountants to help investigate Trump and his businesses. This investigation is a criminal investigation. New York Attorney General Letitia James is in charge of a civil investigation into Trump’s businesses.
But the big thing which showed momentum is moving away from Trump is that President-Elect Joe Biden is forcefully criticizing the Trump administration for its failure to plan for distribution of the coronavirus vaccine.
With more than 330,000 Americans dead of Covid-19 and infections spiking, Biden today noted that the Trump administration has fallen behind on vaccine distribution. The effort got off to a poor start as the administration delivered fewer doses than it had promised and initially blamed Pfizer for a “miscommunication,” only to have Pfizer state that it had “millions of doses” in a warehouse but had received no information about where to send them.
The administration promised to vaccinate 20 million Americans by the end of December, but yesterday, the Centers for Disease Control and Prevention reported that it had administered just 2.1 million doses in two weeks, although that number is likely somewhat low because of lag times in reporting. At the current rate, Dr. Leana S. Wen writes in the Washington Post, we can expect to achieve herd immunity in 10 years.
The administration at first refused to share information with the Biden camp about distribution, claiming there was a plan, even though, when finally part of discussions, Biden said “[t]here is no detailed plan that we've seen, anyway, as to how you get the vaccine out of a container, into an injection syringe, into somebody's arm.”
Health and Human Services Secretary Alex Azar responded that Biden’s claim was “nonsense.” “[W]e have comprehensive plans from the Centers for Disease Control and Prevention working with 64 public health jurisdictions across the country as our governors have laid out very detailed plans that we’ve worked with them on. We’re leveraging our retail pharmacies, our hospitals, our public health departments, our community health centers.” Azar said the distribution process was being “micromanaged and controlled by the United States military, as well as our incredible private sector. We do hundreds of millions of vaccinations a year. We’re leveraging the systems that are known, and that work here in the United States.” Azar assured Fox News Sunday host Chris Wallace that, as soon as the vaccines were approved, the government would be shipping them “to all of the states and territories that we work with. And within hours they can be vaccinating,”
It turns out Biden was more right than Azar. The administration planned simply to get the vaccines to the states, and then leave to them the problem of actually getting the vaccines into people’s arms. But state Departments of Health are strapped for money after trying to manage the pandemic for nine months, and had been allotted only $6 million apiece to make the distributions happen. (The new Consolidated Appropriations Act that Trump just signed has significantly more money in it for distribution.)
“The Trump administration’s plan to distribute vaccines is falling behind, far behind,” Biden said today. “As I long feared and warned, the effort to distribute and administer the vaccine is not progressing as it should.”
Finally stung, Trump tweeted tonight that “It is up to the States to distribute the vaccines once brought to the designated areas by the Federal Government. We have not only developed the vaccines, including putting up money to move the process along quickly, but gotten them to the states. Biden failed with Swine Flu!” (Biden was not in charge of the Obama Administration’s response to H1N1 in 2009, which broke out three months after Obama took office.)
Biden promised to invoke the National Defense Production Act, a law that permits the president to require companies to produce goods at the same time that it guarantees them a market for those goods, to speed up the production of supplies necessary to distribute the vaccine quickly. “I have directed my team to prepare a much more aggressive effort, with more federal involvement and leadership to get things back on track,” he said.
But he warned that we are behind and, breaking with the Trump administration, warned that things are going to get much worse before they get better. The spike in infections along with the fallout from holiday gatherings means we will see high cases in January and high death tolls in February. It will be mid-March, he warns, before we see improvement. “The next few weeks and months are going to be very tough, a very tough period for our nation — maybe the toughest during this entire pandemic,” Biden said. “I know it’s hard to hear, but it’s the truth.”
“We are going to get through this. Brighter days are coming,” Biden said. “But it’s going to take all of the grit and determination we have as Americans to get it done.”
—-
LETTERS FROM AN AMERICAN
HEATHER COX RICHARDSON
1 note
·
View note
Text
If Swine Flu Happens During COVID-19, Are We Screwed?
It feels like 2020 can't get any worse, but it always does. Genetic testing of pigs in China from 2011 to 2018 leads us to consider a truly dire possibility: What if we weren't just dealing with one historic and deadly pandemic, but two? Could it even happen?
There’s an outbreak of H1N1, or the “swine flu", running through China’s pig farms right now. According to a study in the Proceedings of the National Academy of Sciences, recent genetic testing of pigs in Chinese farms show genes “similar to [swine flu ‘09] virus,” and has “all the essential hallmarks of a candidate pandemic virus.”
So, how worried should one be about a second pandemic-within-a-pandemic?
As it so happens, the flu is more infectious than even COVID-19, but the world is also better prepared to battle it. It’s been doing so for more than 100 years, after the 1918 pandemic ravaged a world that hadn't yet discovered flu viruses. And the world, if not the U.S., is already at heightened alert for infectious disease. It’d be hard, but not impossible, for two pandemics to run through the world’s population at the same time.
Early warning signals are working
Despite what you may have heard, COVID-19 is not the flu. And the fact that we even know about the possibility of a swine flu outbreak is because experts know all about influenza and take it incredibly seriously. That we are discussing a possible pathogen as it is being reported in academic journals is a good sign. In many ways, health experts are playing catch-up when it comes to Covid-19.
“So what we're seeing a little bit is what public health is constantly doing,” Theresa MacPhail,a medical anthropologist andAssistant Professor at Stevens Institute of Technology, told Motherboard over the phone. MacPhail was in Hong Kong in 2009 during a previous outbreak of H1N1 and worked with the CDC to contain it.
The World Health Organization runs the Global Influenza Surveillance and Response System. (GISRS) Established in 1952, GISRS constantly monitors influenza hotspots and coordinates with healthcare providers and world governments to keep things in check.
“In China, [government officials] regularly sample birds on duck and chicken farms and pigs on pig farms and all the workers who work there for this reason: to see what strains are in circulation to see if there are any potential problems," MacPhail said. "So that's what you're seeing is this particular strain has been in circulation for a while.”
According to MacPhail, there’s good cause to worry, but not to panic, yet. China’s experts sounding the alarm this early is a sign that the system is working as intended. She also said these kinds of alerts and alarms happen all the time. “Most of the time that stuff is ignored by the public,” she said. “You don't know that this is normal.”
Katherine Mason, a medical anthropologist and an assistant professor at Brown University, said that the world is prepared for the flu in a way it wasn’t for the coronavirus. “Everyone always thought the next pandemic was going to be an influenza pandemic,” she told VICE on the phone. “Every year you get news of some new strain of flu … [scientists] have spent a lot of time and resources trying to be able to anticipate the flu, which is partly why Covid-19 caught people off guard.”
Nidia Trovao, a virologist at the National Institute of Health, said she’s watching the new H1N1 strain but isn’t particularly worried about it. “I think the probability of having two pandemics simultaneously is really really low,” she told VICE over the phone. She said that the virus has made the jump from human to pig, but only in the workers in close proximity to the swine. It has yet to move from human to human. “The big evolutionary hurdle is for the virus to gain the capacity for human to human transmission.”
Flu is watched so closely because, in the past, it’s been devastating. The 1918 flu pandemic was a predecessor of H1N1. While it’s often called “the Spanish Flu,” epidemiologists traced its origins to pig farms in Kansas, where it spread through U.S. Army bases and into the wider world. Epidemiologist and historians estimate that the flu killed more than 50 million people worldwide. It was devastating, but scientists learned a lot about how to fight a global influenza pandemic.
The concept of social distancing and wearing masks to prevent the spread of infection were lessons learned during the 1918 pandemic. One of the reasons that the flu spread so fast was because of the close quarters assigned to troops in the U.S. military. Much of the world’s modern health system and America’s modern mliitary’s sanitation practices are direct results of what we learned during the 1918 pandemic.
“This is actually a system that's working that's been in place for a long time,” MacPhail said. “And scientists are relatively on top of it.”
Health measures are already in place
According to MacPhail, the world is better positioned to deal with a flu outbreak than any other infectious disease, even Covid-19. “In some ways, this is the best possible time that's ever been for a new dangerous flu, and this one isn't even that dangerous. It looks like the cases in people are pretty mild,” she said.
She acknowledged that the flu mutates all the time. What seems mild one day may yet turn deadly. But the world is already at least familiar with the measures it needs to take to avoid mass infection. They look a lot like what the world (except much of America) is already doing: masks, shutdowns, social distancing.
“But, say we do have something terrible,” MacPhail said. “We’re already wearing masks…we’re more prepared than we’ve ever been for something like this.”
The GISRS meets twice a year in Geneva to create the seasonal flu vaccines. “This works by having more than 100 laboratires around the world that get samples from these patients with influenza-like illness, then they test for flu using different methods,” Trovao said. “The good thing here is that countries in the Southern hemisphere are currently facing their flu season so we can learn a lot from their experience. We’re seeing lower levels than we usually observe this time of the year. Of more than 2,000 sample tests, only 37 were positive for flu. Those are good results.”
But Trovao those good results should be interpreted with caution. “The pandemic crisis forced us into isolation which will naturally curb transmission,” she said. She also noted that there have been some reports of people getting both the flu and Covid-19 at the same time. “Clinicians should be alert that the positive test for either virus does not rule out the possibility for the other.”
Flu is more transmissible and it evolves more quickly, but the period between contracting the virus and showing symptoms is much lower than Covid-19. We also have vaccines for the flu and systems in place to develop new ones quickly when a new strain appears. According to MacPhail, a new flu vaccine takes roughly 9 months after experts identify a strain. More than 130 separate Covid-19 vaccines are in development currently. The world is spending billions to rush one to market and best estimates say it won’t be available until early next year.
“We were not prepared for Coronavirus in the same way,” MacPhail said. “We weren't really surveying Coronavirus the way that we do flu and we don't have the vaccine technology in place already for something like Coronavirus. So that's what we're seeing right now and why this is so bad.”
H1N1 isn’t the only influenza strain on the watchlist. Experts are constantly tracking outbreaks across the globe. “Every day there’s something,” MacPhail said. “Normal people don’t know that there’s a botulism outbreak in cheese in Ireland right now.”
There’s also an ebola outbreak in the Democratic Republic of Congo, cases of bubonic plague in Mongolia, and yellow fever in Ethiopia.
The point is: the world is filled with disease. A new one popping up isn't cause for panic, especially when it's being so closely watched, but it is an opportunity to be vigilant.
But what if it's bad?
These assurances are good reminders of the world’s robust public health system, but they’re cold comfort in the U.S. where COVID-19 infections and deaths rise daily.
In America, and to a lesser extent elsewhere, COVID-19 isn’t just a public health issue, it’s a fiercely political one. State and local officials push back against CDC recommendations, citing economic concerns. Anti-maskers make public scenes that are quickly posted online and go viral. In my own neighborhood message board here in South Carolina, anti-maskers are boasting that they won’t wear a mask under any circumstances. A U.S. passport, once the key to unlocking a world of travel, is now a scarlet letter. So many countries are turning Americans away that it’s easier to list the countries Americans can still travel to than those that block them.
MacPhail initially didn’t think COVID-19 would be that bad, but told VICE after it became a pandemic that she’d been wrong. According to MacPhail, she failed to predict that the U.S. Government would do such a horrible job containing it.
It’s possible, and even likely, that a new round of restrictions based on a new outbreak wouldn’t be enough to convince people to change their opinions on masks and social distancing. They might even double down, at least at first.
Mason said she worries that fighting a second pandemic would be hard, in part, because the flu and COVID-19 have such similar symptoms. “If Covid continues to rage the way it has been here in the states, it’s gonna be very difficult to separate out the appearance of a new flu strain. That’s what I’m worried about.”
Winter is coming, and winter always brings the flu and other respiratory diseases. “I have two kids,” Mason said. “My kids, in the winter, pretty much always have a virus for like four or five months. So it’s going to be hard to differentiate a new one from the one we already have. That’s number one. Number two is the capacity to deal with it which is non existent in the United States at the moment. If the flu started going around, I would be surprised if it made things better rather than worse.”
According to Trovao, the scientific community is already worrying about the flu season. “By itself it already causes high morbidity and mortality,” she said. “I think this is the year where we encourage people even more strongly to get the flu shot, because it lessens the burden on the healthcare system so those beds and capabilities can be directed towards the pandemic.”
“What we are doing to curtail Covid-19, might also curtail the spread of other viruses and reduce transmission of both viruses,” Trovao said. “That’s where we need to focus—keeping people wearing masks and continuing to physically distance and getting the vaccine that we produce every year.”
Anyone can catch COVID-19, but the rates of infection and death are highest among the people at the margins of American society—the elderly and members of racial and ethnic minority groups in particular. This may make it easy for the powerful and privileged to ignore it, and even demand that others risk their lives to provide them with goods and services. A flu with a higher death rate than even Covid-19 (which doctors now believe may cause extensive and life-altering complications even after recovery) would not be so easily mentally sidelined even with the buffers of wealth, power, and even youth.
"I just keep thinking, ‘Thank god [the death rate is] only between one and two percent,’” McPhail said. “But that’s shitty, because that allows us to ignore it for longer. I guarantee you, if a bunch of 20 and 30 year olds were dying right now we would be taking this much more seriously. And if it was killing kids, we’d be on top of this.” (Younger people and children do catch Covid-19 and die, but at rates much lower than older people with underlying conditions.)
“The flu strikes children pretty hard usually,” Mason said. She stressed that every flu strain is different, and affects different groups in different ways. “But if it follows the same pattern as most flu outbreaks, we would be seeing a lot more children dying.”
In particular, Mason pointed to people's reluctance to get flu shots as a reason for its annual death toll. Concerningly, anti-vaccine conspiracies have already begun to circulate regarding a possible Covid-19 vaccine.
“Covid is worse, don’t get me wrong, but the flu is still a big killer every year,” she said. “Part of the reason is people don’t get flu shots even though we have them because they don’t take the flu seriously enough. The flu just spreads like wildfire. If we think Covid spreads easily, if we’re hit with a really serious and deadly flu pandemic it’s going to be even worse.”
According to McPhail, a deadly flu pandemic on top of COVID-19 would be nothing short of a national "reckoning."
“Coronavirus is playing into our worse national traits whereas flu would make us have a reckoning,” MacPhail said. “This is why, traditionally, we’ve been more afraid of the flu. Because it kills indiscriminately across age groups.”
Mason pointed out that even if there’s not a strain of H1N1, seasonal flu on top of the Covid-19 pandemic in the winter, when people get more respiratory diseases, is still concerning.. “[Winter] is going to be really bad. I’m very very concerned about it. If we throw the flu on top of it, even just seasonal flu… nature doesn’t care whether you’ve had enough. It’s gonna do what it’s gonna do. It can get a lot worse.”
Which is why, thankfully, the world's health experts and governments do all they can to contain swine flu. The 2009 H1N1 epidemic began in Central Mexico and spread out of control before global health measures, including a vaccine, brought it under control. The newest outbreak is in China, a country taking active measures to contain and control the virus’s spread.
The pandemics of 1918 and 2020 have taught us a valuable lesson, though: the world's virus response is only as strong as its weakest link, and now as in the past, that weak link is the U.S.
If Swine Flu Happens During COVID-19, Are We Screwed? syndicated from https://triviaqaweb.wordpress.com/feed/
3 notes
·
View notes
Text
Evolution

Image credit: Edel Rodriguez, from Der Spiegel
Donald Trump, World Economic Forum, January 22, 2020: “We have it totally under control. It’s one person coming in from China. We have it under control. It’s going to be just fine.”
Donald Trump, Twitter, January 30, 2020: “Working closely with China and others on Coronavirus outbreak. Only 5 people in U.S., all in good recovery.”
Donald Trump, Fox News, February 2, 2020: “We pretty much shut it down coming in from China. But we can’t have thousands of people coming in who may have this problem, the coronavirus. We’re going to see what happens, but we did shut it down, yes.”
Donald Trump, Twitter, February 24, 2020: “The Coronavirus is very much under control in the USA. We are in contact with everyone and all relevant countries. CDC & World Health have been working hard and very smart. Stock Market starting to look very good to me!”
Donald Trump, New Delhi, India, February 25, 2020: “I have spoken to President Xi, and they’re working very hard. And if you know anything about him, I think he’ll be in pretty good shape. They’re — they’ve had a rough patch, and I think right now they have it — it looks like they’re getting it under control more and more. They’re getting it more and more under control. So I think that’s a problem that’s going to go away.”
Donald Trump, Twitter, February 25, 2020: “CDC and my Administration are doing a GREAT job of handling Coronavirus, including the very early closing of our borders to certain areas of the world. It was opposed by the Dems, ‘too soon’, but turned out to be the correct decision. No matter how well we do, however, the..... ....Democrats talking point is that we are doing badly. If the virus disappeared tomorrow, they would say we did a really poor, and even incompetent, job. Not fair, but it is what it is. So far, by the way, we have not had one death. Let’s keep it that way!”
Donald Trump, White House Press Conference, February 26, 2020: “I don’t think it’s going to come to that, especially with the fact that we’re going down, not up. We’re going very substantially down, not up. ... We have it so well under control. I mean, we really have done a very good job. ... When you have 15 people, and the 15 within a couple of days is going to be down to close to zero, that’s a pretty good job we’ve done.”
Donald Trump, White House Cabinet Room, February 27, 2020: “It’s going to disappear. One day it’s like a miracle, it will disappear.”
Donald Trump, White House South Lawn, February 28, 2020: “We haven’t lost anybody yet. And hopefully, we can keep that intact. We — there have been no deaths in the United States at all. A lot of that is attributable to the fact that we closed the border very early. Otherwise, it could be a different story. So we’ll — we’ll just keep doing a good job. We’re ordering a lot of supplies. We’re ordering a lot of — a lot of elements that, frankly, we wouldn’t be ordering unless it was something like this. But we’re ordering a lot of different elements of medical. We are working on cures and we’re getting some very good results. As you know, they’re working as rapidly as they can on a vaccine for the future.”
Donald Trump, White House Cabinet Room, March 2, 2020: “We will confront this challenge together, and we will continue to do exactly what we’re doing. And we’re going to be very successful. A lot of things are happening. A lot of very exciting things are happening, and they’re happening very rapidly. ... You take a solid flu vaccine, you don’t think that could have an impact, or much of an impact, on corona?”
Donald Trump, Fox News, March 4, 2020: “If we have thousands or hundreds of thousands of people that get better, just by, you know, sitting around and even going to work, some of them go to work, but they get better. ... I will say, though, the H1N1, that was swine flu, commonly referred to as swine flu. And that went from around April of ‘09 to April of ‘10, where there were 60 million cases of swine flu. And over -- actually, it’s over 13,000. I think you might have said 17,000. I had heard it was 13,000, but a lot of -- a lot of deaths. And they didn’t do anything about it. Interestingly, with the swine flu, children were -- in particular, they were vulnerable, sort of the opposite in that respect. But children were very vulnerable to the swine flu. But they never did close the borders. I don't think they ever did have the travel ban. And we did. And, again, they lost at least 13,000. It could be as high as 17,000 people. And we acted much differently.”
Donald Trump, Twitter, March 5, 2020: “With approximately 100,000 CoronaVirus cases worldwide, and 3,280 deaths, the United States, because of quick action on closing our borders, has, as of now, only 129 cases (40 Americans brought in) and 11 deaths. We are working very hard to keep these numbers as low as possible!”
Donald Trump, CDC, March 6, 2020: “As of the time I left the plane with you, we had 240 cases. That’s at least what was on a very fine network known as Fox News. And you love it. But that’s what I happened to be watching. And how was the show last night? Did it get good ratings, by the way? ... I heard it broke all ratings records, but maybe that’s wrong. That’s what they told me. I don’t know. I can’t imagine that. But what happened is, if you look at the number at the time we left, it was 240 cases, Peter, and 11 deaths. That’s what it has been. Now, you look at — throughout the world, I mean, other countries have — South Korea, Italy, and in particular China have many . ... I think, importantly: Anybody right now and yesterday — anybody that needs a test gets a test. We — they’re there. They have the tests. And the tests are beautiful. Anybody that needs a test gets a test. If there’s a doctor that wants to test, if there’s somebody coming off a ship — like the big monster ship that’s out there right now, which, you know — again, that’s a big decision. Do I want to bring all those people on? People would like me to do that. I don’t like the idea of doing it. But anybody that needs a test can have a test. They’re all set. They have them out there. In addition to that, they’re making millions of more as we speak. But as of right now and yesterday, anybody that needs a test — that’s the important thing — and the tests are all perfect, like the letter was perfect. The transcription was perfect, right? This was not as perfect as that, but pretty good. ... I would rather — because I like the numbers being where they are. I don’t need to have the numbers double because of one ship. That wasn’t our fault, and it wasn’t the fault of the people on the ship, either. Okay? It wasn’t their fault either. And they’re mostly Americans, so I can live either way with it. I’d rather have them stay on, personally. ... I think we’re doing a really good job in this country at keeping it down. We’ve really been very vigilant, and we’ve done a tremendous job at keeping to [sic] down. ... You know, my uncle was a great person. He was at MIT. He taught at MIT for, I think, like a record number of years. He was a great super genius. Dr. John Trump. I like this stuff. I really get it. People are surprised that I understand it. Every one of these doctors said, ‘How do you know so much about this?’ Maybe I have a natural ability. Maybe I should have done that instead of running for President.”
Donald Trump, Twitter, March 8, 2020: “We have a perfectly coordinated and fine tuned plan at the White House for our attack on CoronaVirus. We moved VERY early to close borders to certain areas, which was a Godsend. V.P. is doing a great job. The Fake News Media is doing everything possible to make us look bad. Sad!”
Donald Trump, Twitter, March 9, 2020: “So last year 37,000 Americans died from the common Flu. It averages between 27,000 and 70,000 per year. Nothing is shut down, life & the economy go on. At this moment there are 546 confirmed cases of CoronaVirus, with 22 deaths. Think about that!”
Donald Trump, White House Press Briefing, March 9, 2020: “We have a great economy, we have a very strong economy, but this came — this blindsided the world. And I think we’ve handled it very, very well.”
Donald Trump, Twitter, March 13, 2020: “For decades the @CDCgov looked at, and studied, its testing system, but did nothing about it. It would always be inadequate and slow for a large scale pandemic, but a pandemic would never happen, they hoped. President Obama made changes that only complicated things further..... .... Their response to H1N1 Swine Flu was a full scale disaster, with thousands dying, and nothing meaningful done to fix the testing problem, until now. The changes have been made and testing will soon happen on a very large scale basis. All Red Tape has been cut, ready to go!”
Donald Trump, White House Press Conference, March 13, 2020: “To unleash the full power of the federal government in this effort, today I am officially declaring a national emergency. Two very big words. ... No, I don’t take responsibility at all, because we were given a — a set of circumstances and we were given rules, regulations, and specifications from a different time. ... If you go back to the swine flu, it was nothing like this. They didn’t do testing like this. And actually, they lost approximately 14,000 people. And they didn’t do the testing. They started thinking about testing when it was far too late. ... [Q: Mr. President, the last administration said that they had tested a million people at this point.] Well, ask them how they did with the swine flu. It was a disaster. Next, please. Next, please. They had a very big failure with swine flu. A very big failure.”
#COVID-19#coronavirus#China#pandemic#national emergency#Trump#Donald Trump#President Trump#Trump quote#alternative facts#Trump lies#LiarInChief#Lying Liars Who Lie#CDC#Centers for Disease Control#flu#influenza#responsibility#finger pointing#scapegoating#Obama#Barack Obama#President Obama#POTUS#Obama administration#H1N1#swine flu
6 notes
·
View notes
Text
COVID-19 Coronavirus “Fake” Pandemic: Timeline and Analysis

On January 30th 2020, the World Health Organization (WHO) declared a Public Health Emergency of International Concern (PHEIC) in relation to China’s novel coronavirus (2019-nCoV) categorized as a viral pneumonia. The virus outbreak was centred in Wuhan, a city in Eastern China with a population in excess of 11 million.
In the week prior to January 30th decision, the WHO Emergency Committee “expressed divergent views”. There were visible divisions within the Committee. On January 30th, a far-reaching decision was taken without the support of expert opinion at a time when the coronavirus outbreak was limited to Mainland China.
There were 150 confirmed cases outside China, when the decision was taken. 6 in the United States, 3 in Canada, 2 in the UK, etc.
150 confirmed cases over a population of 6.4 billion (World population of 7.8 billion minus China’s 1-4 billion).
What was the risk of being infected? Virtually zero.
The WHO did not act to reassure and inform World public opinion. Quite the opposite: A “Fear Pandemic” rather than a genuine Public Health Emergency of International Concern (PHEIC) was launched.
Outright panic and uncertainty were sustained through a carefully designed media disinformation campaign.
Almost immediately this led to economic dislocations, a crisis in trade and transportation with China affecting major airlines and shipping companies. A hate campaign against ethnic Chinese in Western countries was launched, followed by the collapse in late February of stock markets, not to mention the crisis in the tourist industry resulting in countless bankruptcies.
The complexity of this crisis and its impacts have to be addressed and carefully analysed.
What we are dealing with is “economic warfare” supported by media disinformation, coupled with the deliberate intent by the Trump administration to undermine China’s economy. The ongoing economic dislocations are not limited to China.
There are important public health concerns which must be addressed. But what motivated the Director-General of the WHO to act in this way? Who was behind this historic January 30th decision of the WHO’s Director General Tedros Adhanom Ghebreyesus.
Our subsequent analysis (in the timeline below) reveals that powerful corporate interests linked to Big Pharma, Wall Street and agencies of the US government were instrumental in the WHO’s far-reaching decision.
What is at stake is the alliance of “Big Pharma” and “Big Money”, with the endorsement of the Trump Administration. The decision to launch a fake pandemic under the helm of the WHO on January 30, was taken a week earlier at the Davos World Economic Forum (WEF). The media operation was there to spread outright panic.
(Scroll down to Read our Timeline on how these events unfolded)
But this was not the first time that the WHO decided to act in this way.
Remember the unusual circumstances surrounding the April 2009 H1N1 Swine Flu Pandemic.
An atmosphere of fear and intimidation prevailed. The data was manipulated.
Based on incomplete and scanty data, the WHO Director General nonetheless predicted with authority that: “as many as 2 billion people could become infected over the next two years — nearly one-third of the world population.” (World Health Organization as reported by the Western media, July 2009).
It was a multibillion bonanza for Big Pharma supported by the WHO’s Director-General Margaret Chan.
In June 2009, Margaret Chan made the following statement:
“On the basis of … expert assessments of the evidence, the scientific criteria for an influenza pandemic have been met. I have therefore decided to raise the level of influenza pandemic alert from Phase 5 to Phase 6. The world is now at the start of the 2009 influenza pandemic. … Margaret Chan, Director-General, World Health Organization (WHO), Press Briefing 11 June 2009)
What “expert assessments”?
In a subsequent statement she confirmed that:
“Vaccine makers could produce 4.9 billion pandemic flu shots per year in the best-case scenario”,Margaret Chan, Director-General, World Health Organization (WHO), quoted by Reuters, 21 July 2009)
A financial windfall for Big Pharma Vaccine Producers including GlaxoSmithKline, Novartis, Merck & Co., Sanofi, Pfizer. et al.
CORONAVIRUS TIMELINE
September 2019: The official US-WHO position is that the coronavirus originated in Wuhan, Hubei Province and was first discovered in Late December. This statement is questioned by Chinese and Japanese virologists who claim that the virus originated in the US.
A renowned Taiwanese virologist pointed to evidence that the virus could have originated at an earlier stage, stating : “We must look to September of 2019”.
October 18-27 2019: Wuhan 2019: CISM Sport Military World Games
Coronavirus Epidemic: WHO Declares a “Fake” Global Public Health Emergency
Chinese media intimates (without corroborating evidence) that the coronavirus could have been brought to China “from a foreign source” during the CISM Military World Games.
10,000 soldiers from 109 countries will participate
200 American military personnel participated in this 10 day Event.
October 18, Event 201. Baltimore. Coronavirus nCoV-2019 Simulation and Emergency Preparedness Task Force, John Hopkins Bloomberg School of Health Security.
Big Pharma-Big Money Simulation Exercise sponsored by WEF and Gates Foundation
Simulation Exercise of a coronavirus epidemic which results in 65 million dead. Supported by the World Economic Forum (WEF) representing the interests of Financial institutions, the Bill and Melinda Gates Foundation representing Big Pharma:
In October 2019, the Johns Hopkins Center for Health Security hosted a pandemic tabletop exercise called Event 201 with partners, the World Economic Forum and the Bill & Melinda Gates Foundation. … For the scenario, we modeled a fictional coronavirus pandemic, but we explicitly stated that it was not a prediction.
Instead, the exercise served to highlight preparedness and response challenges that would likely arise in a very severe pandemic. We are not now predicting that the nCoV-2019 outbreak will kill 65 million people.
Although our tabletop exercise included a mock novel coronavirus, the inputs we used for modeling the potential impact of that fictional virus are not similar to nCoV-2019.“We are not now predicting that the nCoV-2019 [which was also used as the name of the simulation] outbreak will kill 65 million people.
.Although our tabletop exercise included a mock novel coronavirus, the inputs we used for modeling the potential impact of that fictional virus are not similar to nCoV-2019.”
Several of the occurrences of the nCoV-2019 exercise coincided with what really happened.
In the Event 201 Simulation of a Coronavirus Pandemic, a 15% collapse of financial markets had been “simulated”.
It was not “predicted” according to the organizers and sponsors of the event.
Private sector initiative. Participation of corporate execs, foundations, financial institutions, Banks, Big Pharma, CIA, CDC, No health officials on behalf of national governments or the WHO. The simulation exercise was held on the same day as the opening of the CISM World Militaty Sports Games in Wuhan.
December 31, 2019: First cases of pneumonia detected and reported in Wuhan, Hubei Province. China.
January 1, 2020: Chinese health authorities close the Huanan Seafood Wholesale Market after Western media reports that wild animals sold there may have been the source of the virus. This initial assessment was subsequently refuted by Chinese scientists.
January 7, 2020: Chinese authorities “identify a new type of virus” which was isolated on 7 January. The coronavirus was named 2019-nCoV by the WHO exactly the same name as that adopted in the WEF-Gates-John Hopkins October 18, 2019 simulation exercise.
January 11, 2020 – The Wuhan Municipal Health Commission announces the first death caused by the coronavirus.
January 22, 2020: WHO. Members of the WHO Emergency Committee “expressed divergent views on whether this event constitutes a PHEIC or not”.
January 21-24, 2020: Consultations at the World Economic Forum, Davos, Switzerland under auspices of the Coalition for Epidemic Preparedness Innovations (CEPI) for development of a vaccine program. CEPI is a WEF-Gates partnership. With support from CIPI, Seattle based Moderna will manufacture an mRNA vaccine against 2019-nCoV, “The Vaccine Research Center (VRC) of the National Institute of Allergy and Infectious Diseases (NIAID), part of NIH, collaborated with Moderna to design the vaccine.”
Note: The development of a 2019 nCoV vaccine was announced at Davos, 2 weeks after the January 7, 2020 announcement, and barely a week prior to the official launching of the WHO’s Worldwide Public Health emergency on January 30. The WEF-Gates-CEPI Vaccine Announcement precedes the WHO Public Health Emergency (PHEIC).
January 30, 2020: Geneva: WHO Director General determines that the outbreak constitutes a Public Health Emergency of International Concern (PHEIC). This decision was taken on the basis of 150 confirmed cases outside China, First case of person to person transmission in US is reported, 6 cases in the US, 3 cases in Canada, 2 in the UK.
The WHO Director General had the backing of the Bill and Melinda Gates Foundation, Big Pharma and the World Economic Forum (WEF). There are indications that the decision for the WHO to declare a Global Emergency was taken on the sidelines of the World Economic Forum (WEF) in Davos (January 21-24) overlapping with the Geneva January 22 meeting of the Emergency Committee.
Both WHO’s Director Tedros as well as Bill Gates were present at Davos 2020. Bill Gates announced the Gates Foundation’s $10 billion commitment to vaccines over the next 10 years.
January 30, 2020 The Simulation Exercise Went Live. The same corporate interests and foundations which were involved in the October 18 John Hopkins Simulation Exercise became REAL ACTORS involved in providing their support to the implementation of the WHO Public Health emergency (PHEIC).
January 31, 2020 – One day later following the launch of WHO Global Emergency, The Trump administration announced that it will deny entry to foreign nationals “who have traveled in China in the last 14 days”. This immediately triggers a crisis in air transportation, China-US trade as well as the tourism industry, leading to substantial bankruptcies, not to mention unemployment.
Immediately triggers a campaign against ethnic Chinese throughout the Western World.
Early February: the acronym of the coronavirus was changed from nCoV- 2019 (its name under the October Event 201 John Hopkins Simulation Exercise before it was identified in early January 2020) to COVID-19.
February 28, 2020: A massive WHO vaccination campaign was announced by WHO Director General Dr. Tedros Adhanom Ghebreyesus
Who was behind this campaign: GlaxoSmithKline in partnership with the Coalition for Epidemic Preparedness Innovations (CEPI). It is a Gates-WEF partnership, both of which were sponsors of the October 18, “Simulation Exercise”. The campaign to develop vaccines was initiated prior to decision of the WHO to launch a Global Public Health emergency. It was first announced at the WEF meeting at Davos (21-24 January).
Late February 2020. Collapse of the stock markets, surge in the value of the stocks of Big Pharma.
Early March devastating consequences for the tourist industry Worldwide.
February 24: Moderna Inc supported by CIPI announced that it experimental mRNA COVID-19 vaccine, known as mRNA-1273, was ready for human testing.
Late February – Early March: China: More than 50% of the infected patients recover and are discharged from the hospitals. March 3, a total of 49,856 patients have recovered from COVID-19 and were discharged from hospitals in China. What this means that the total number of “confirmed infected cases” in China is 30,448. (Namely 80,304 minus 49856 = 30,448 (80 304 is the total number on confirmed cases in China (WHO data, March 3, 2020). These developments concerning “recovery” are not reported by the Western media
March 5, WHO Director General confirms that outside China there are 2055 cases reported in 33 countries. Around 80% of those cases continue to come from just three countries (South Korea, Iran, Italy).
These figures confirm that we are not facing a global health emergency, that the probability of infection is low. And Based on China’s experience the treatment for the virus infection is effective.
March 7: USA: The number of “confirmed cases” (infected and recovered) in the United States in early March is of the order of 430, rising to about 6oo (March 8).
Compare that to the figures pertaining to the Influenza B Virus: The CDC estimates for 2019-2020 “at least 15 million virus flu illnesses… 140,000 hospitalizations and 8,200 deaths. (The Hill)
Early March: IMF and World Bank To the Rescue
The WHO Director General advises member countries that “the World Bank and the International Monetary Fund have both made funds available to stabilize health systems and mitigate the economic consequences of the epidemic”. That is the proposed neoliberal “solution” to COVID-19. The World Bank has committed $12billion in so-called “aid” which will contribute to building up the external debt of developing countries.
March 7: China: The Pandemic is Almost Over
Reported new cases in China fall to double digit. 99 cases recorded on March 7. All of the new cases outside Hubei province are categorized as “imported infections”(from foreign countries). The reliability of the data remains to be established:
99 newly confirmed cases including 74 in Hubei Province, … The new cases included 24 imported infections — 17 in Gansu Province, three in Beijing, three in Shanghai and one in Guangdong Province.
March 10-11 Italy declares a lockdown, followed by several other countries of the EU. Deployment of 30,000 US troops in the EU as part of the “Defend Europe 2020” war games directed against Russia.
March 11: Trump orders the suspension for 30 days of all transatlantic flights from countries of the European Union, with the exception of Britain. Coincides with the collapse of airline stocks and a new wave of financial instability.
March 16: Moderna mRNA-1273 is tested in several stages with 45 volunteers in Seattle, Washington State. The vaccine program started in early February:
“We don’t know whether this vaccine will induce an immune response, or whether it will be safe. That’s why we’re doing a trial,” Jackson stressed. “It’s not at the stage where it would be possible or prudent to give it to the general population.” (AP, March 16, 2020)
Concluding Remarks
We are dealing with a complex global crisis with far-reaching economic, social and geopolitical implications.
We have provided factual information as well as analysis in a summarized “common sense” format.
Is is important that COVID-19 be the object of widespread debate and that the “official interpretations” be forcefully challenged.
We ask our readers to forward this article as well other Global Research articles pertaining to the COVID-19 coronavirus.
The original source of this article is Global Research Copyright ©
Prof Michel Chossudovsky
, Global Research, 2020
4 notes
·
View notes
Text
HOW DOES THE CORONAVIRUS OUTPUT END? WE SHOW YOU HOW TO PLAY SIMILAR EPIDEMICS.
As stock markets crash, travel stops, and new Coronavirus infections are diagnosed in the United States, one question everyone is asking is how the epidemic will end.
No one knows for sure, but virologists say there are signs of similar epidemics. Here are three scenarios:
Coronavirus Is Controlled By Health Officials Through Strict Public Health Measures
When severe acute respiratory syndrome (SARS) first appeared in Asia in 2002, it was quite scary, with a mortality rate of around 10% and without the effectiveness of medications. (The current coronavirus, by comparison, has an estimated mortality rate of less than 1 to 3.4%.) However, within a few months, SARS was controlled and eradicated largely thanks to international collaboration and strict controls. . . Outdated public health measures, such as isolation, quarantine, and contact tracing.

It would be an ideal result. However, the difference is that SARS had more severe symptoms than the current coronavirus, so people went to the hospital shortly after infection.
Coronavirus cases will be more difficult to detect and isolate, said Stuart Weston, a postdoctoral fellow at the University of Maryland. Weston is one of a small group of researchers who have received and is studying samples of coronaviruses. Weston and other experts warn that the epidemic is more widespread than that pursued in the United States and other countries because many people with mild symptoms do not know they are infected.
Coronavirus Affects The Least Developed Countries And Worsens Before Improving
One of the worst lessons of the 2014-2016 Ebola epidemic in West Africa is how an epidemic can develop when it affects countries with poor health infrastructure. For this reason, the World Health Organization and other countries in sub-Saharan Africa have prepared for coronavirus, although only a few cases have been reported so far.
Compared to the coronavirus, Ebola was less contagious and was transmitted primarily through body fluids. Coronavirus can be transmitted by coughing and sneezing droplets of breath that persist on surfaces. However, Ebola has infected more than 28,000 people and left more than 11,000 dead. Ebola is more deadly, and shortages of personnel and supplies, poverty, delays by heads of state, and government mistrust are making the epidemic worse.
WHO heads of state and government have called on countries to prepare. On Friday, the organization raised its coronavirus rating to the highest level. "This is a reality check for all governments on the planet: wake up. Prepare. This virus can be on the move and you must be prepared," said Michael Ryan, WHO Director of Health Emergencies. "Waiting to be complacent, being accidentally caught at this point is not a good excuse."
The New Coronavirus Spreads So Much That It Becomes A Reality.
This is essentially what happened with the 2009 H1N1 epidemic, also known as the swine flu. It spread rapidly and eventually reached around 11-21% of the world population. The WHO declared it a pandemic and fear have spread.
H1N1 flu is milder than originally feared and has caused little more than a runny nose and cough in most people. And H1N1 has become so common that it is simply considered part of the seasonal flu that occurs and occurs every year around the world.
Early mortality estimates for H1N1 were much higher than the 0.01 to 0.03 percent that occurred. However, the Centers for Disease Control and Prevention estimates that H1N1 killed 12,469 people, infected 60.8 million cases, and caused 274,304 hospitalizations in the United States between 2009 and 2010. The actual number is difficult to determine as many die The causes of influenza are not tested for H1N1 flu or any other strain of flu. Seasonal flu has killed at least 18,000 people in the United States this season, according to the CDC.
H1N1 is a particularly good parallel, epidemiologists say, because it has a lower death rate than SARS or MERS, but it is more deadly because of its infectivity and spread.
Not alarming, but another possible parallel could be the 1918 Spanish flu, which had a 2.5% death rate and was incredibly close to coronavirus estimates.
Not alarming, but another possible parallel could be the 1918 Spanish flu, which had a 2.5% death rate and was incredibly close to coronavirus estimates.
Florian Krammer, an influenza virologist, discovered that the world was completely different in 1918.
"We did not have the tools to diagnose diseases or antibiotics to fight secondary infections. Hospitals were places where you died and you did not receive treatment. And in 1918, the world was at war. And many infected people were soldiers in the trenches," said Krammer from the Icahn School of Medicine on Mount Sinai. "Hopefully not."
The number of people who die from a coronavirus ultimately depends on its spread, our preparedness, and the actual death rate of the virus.
Some more important things affect the final phase of the coronavirus
If the coronavirus becomes ubiquitous like H1N1, developing a vaccine is crucial. After the 2009 epidemic, experts developed an H1N1 flu vaccine that was included in the flu vaccines that people received in the following years. This has helped protect particularly vulnerable groups of the population during subsequent waves of infection.
Antiviral drugs may help shortly, and laboratories around the world are testing their effectiveness against coronavirus.
No one knows if the coronavirus will be affected by seasons like the flu, although President Trump says it could "disappear" with warmer temperatures in April.
"We are still learning a lot about the virus," said WHO epidemiologist Maria Van Kerkhove. "At the moment, there is no reason to believe that this virus works differently in different climates. We have to see what will happen later."
Coronaviruses are zoonotic, which means they spread from animals to humans. Experts believe that SARS spreads from bats to civets and humans. Middle East Fatal Respiratory Syndrome (MERS) in 2012 was likely transmitted from bats to camels to humans. With the coronavirus, no one knows which animals have caused the current epidemic. And it's a puzzle that scientists must solve to prevent it from happening again in the future.
A prime suspect is an endangered creature named Pangolin, which resembles a cross between an anteater and an armadillo, and whose scales are traded illegally.
"With SARS, once they found the responsible animals in China, they were able to begin removing them from live markets," said Vineet Menachery, a virologist at the University of Texas Medical Department. "It's like a broken water pipe. You have to find the source to turn it off."
*Precult is the covidcare Prevention. You should visit these sites*
1 note
·
View note
Note
Sorry to bother you, but how do you think the impact of COVID-19 would be on developing countries? And are all the rumours about tropical countries wouldn't get affected much true? And how far is the advance in research about possible cure or vaccine for this (will it be available before huge damage occurs both regarding mortality and economic concerns)?
Not a bother at all! I’ll be up front and say that my healthcare experiences are exclusively US-based and that I have never spent time on a medical mission or done Doctors without Borders or anything like that.
In general, developing countries don’t have the healthcare infrastructure that would be needed to get through COVD-19 at the best-case fatality rate. Their hospitals do not have enough of the equipment, specifically ventilators, needed to support the worst cases through the infection. What is being seen in Italy, where doctors have to decide who gets a ventilator and who gets to die, would absolutely happen there, possibly on a larger scale. I suppose if the country was sufficiently rural, and populations were more isolated, the spread might be slower, but most countries do have an urban center or two, so while certain regions might not be too affected, I think the countries would still feel the impact harshly.
Another factor to consider is that protective equipment (masks, eye gear, gowns) for providers is probably in shorter supply in developing countries. This means that more doctors, nurses, respiratory therapists, etc would probably contract the disease and therefore not be available to help treat and care for the ill. I think developing nations could see a higher fatality rate for COVID-19.
So work is already being done for cures/vaccines, but it will take time to get implemented, I’m going to start with vaccines, since we can use H1N1 as a guidepost. During the swine flu pandemic, a vaccine was able to be implemented with the next year’s flu vaccine. So with creation, testing, and trials, we realistically won’t have a vaccine for about a year. This, of course, only applies to the US. I am not familiar enough with restrictions on clinical trials in other countries to speak to timelines there. It wouldn’t surprise me if other countries start mass vaccination earlier, but just from a development standpoint, it would still probably be months from now. It is also worth noting that a vaccine does nothing for a patient who already has contracted the virus. At the rate this virus can spread through a community, even if we developed a vaccine today and started inoculating people ASAP, the time it takes to roll out a widespread vaccination program to millions of people is probably too slow to actually noticeably slow the rate of spread at this point.
As far as cures go, doctors are trying medications we already have to see if they have any effect, but it’s too early to prove if any medication is actually treating COVID-19. Since this a viral illness, the body will, in the majority of cases, clear it on its own. So if someone gets better after taking a medication typically used to clear influenza quicker or to suppress HIV replication, did they get better because of the treatment or did they get better as they naturally would have on their own? It will require more time and more patients in treatment trials to gather enough data to say for sure whether any of these medications have an effect, but some people are optimistic that antiretroviral meds used to treat HIV are having an effect.
The economic impact is already here en masse. Stock market in the US has crashed hard, which will impact spending for years as people worry about their financial security for retirement. Manufacturing lines in China have been disrupted, so shortages of key industrial and consumer products will inevitably occur over the next weeks to months. Italy, which is one of the 10 largest economies in the world, I believe, has come essentially to a halt. Small businesses will go under in droves. All we can do now is to try and lessen the loss of human life. And at this point, the best way to do this is to slow the inevitable spread (the term here is “flatten the curve.”), and social distancing, frequent hand washing, and self isolation if someone is ill is the best way to do so.
3 notes
·
View notes