#Five-element diagnosis
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s reach among the 26-to-35-year-olds in the US is 11%.
Text
hey so. can we all agree to stop saying "asperger's syndrome".
the arguments have been made already for why the term is offensive to autistic people as a general whole, so i'm not going to repeat them here. what i want to focus on is the less talked about issue with the fact that we as a community still use this word.
there is literally no excuse for any person, but especially jewish & romani people, to have their medical condition named after a fucking nazi who tried to genocide their ancestors. ZERO.
and before i get a ton of people in the replies trying to make excuses, let me pre-emptively answer the most common replies i know i'm going to get.
"ohhhh no but it's sooooo hard for me to switch my language, it's only been ten years since the dsm five came out!!!!!"
boo hoo, it's hard for you to use a different word after over ten years of the dsm five removing asperger's as a diagnosis. it must be soooo much more difficult to give a single shit about jews and roma than the experiences of jews and roma who went through a genocide and are still facing violence to this day /s
"but i'm an aspie and i get to reclaim that word if i want!!!!!"
yeah, the term asperger's syndrome is offensive both to autistic people who fall under the criteria and to autistic people that don't. but do you know who else that term is offensive to? the people who went through a genocide. unless you are jewish or romani i don't want to hear it.
"but i was diagnosed with asperger's syndrome before the dsm five came out!!!!!"
see the above two points about how not continuing to glorify genocide is more important than keeping the same words we've always used for things. it's fine to say you were diagnosed with asperger's, but you do not have "asperger's", you have autism (or are autistic if that's the language you prefer).
"but i didn't know that asperger was a nazi!!!"
well, now you do.
"but naming a medical condition after someone doesn't necessarily glorify them!!!!"
would you apply this logic to literally any other field of science? if we decided to name an element after a nazi, people would rightfully be angry. people have been calling for years to rename a beetle named after a nazi. if you name a medical condition after someone, that generally means one of two things: the person was a very important and good researcher in the field, or the person was a notable person who had the medical condition. this might be a hot take, but i don't think that a nazi scientist working for the nazis should ever be considered the best and most important early researcher in any field to be deserving of having a discovery named after them.
"but you can't speak for all jews!!! look, you aren't even jewish yet, it says that on your profile!!!!"
no, i cannot speak for all jews. but i am speaking for myself when i say that all of your (general) excuses have stopped working, and that y'all need to put others' needs above your feelings sometimes. during the writing of this post, i spoke to other jews who have made posts about this before, but y'all continue to ignore jewish voices and make excuses for yourselves when it really isn't that hard to just stop saying a word.
"you're being ableist by telling me, an autistic person, how i can and cannot identify!!!!!"
i'm writing this post as someone who is autistic and would have been diagnosed with "asperger's syndrome" had i gotten my diagnosis before the dsm five came out. being autistic is no excuse for being racist, antisemitic, or any other bigotry. autistic non-jews have continuously spoken over autistic jews on many issues, including this one, and guys, it is not that hard to care about jews and roma enough to make this tiny change to your vocabulary.
i hope all of this has been enough to ward off some of the responses that i'm going to get to this post. i'm willing to engage in good faith if you're genuinely ignorant or confused, but if you have read this post, you no longer get to say that you "didn't know" that hans asperger was a nazi and that we shouldn't name any medical condition, but especially one that many jews and roma have, after people who committed genocide.
175 notes
·
View notes
Note
Hey! Do you have any tips for breaking writers block when you're adhd and/or autistic? Be it your own tips or a link to another post? My friend and I need help haha
Ahh sorry you got buried under spam and old ask game asks. (I... really need to sort my ask box >.<' ). But here we go, a month late, and hopefully better late than never:
Quick ideas for beating writer's block when autistic and/or ADHD
I've got this old post I wrote on writer's block and focus troubles. Ironically, this was before my autism diagnosis but the tips still happen to be things I, an autistic person, did to manage writing when faced with executive dysfunction (except I didn't know what executive dysfunction was at that point lol). I'm linking this with one important caveat, though: if you have ADHD, "stepping away" might do more harm than good; struggling to start tasks is a Big Thing with ADHD, so not starting the task at all is entirely counterproductive. (Unless you're in burnout! Here's a post about the differences between block and burnout with some ideas on what to do for each, in case that's at all helpful to you).
And here's something yoinked from another old ask-answer:
sometimes a break from more “serious” writing is what you need. Maybe try and take the characters from your main project and drop them somewhere else for the hell of it. I like to throw my characters into the MCU without warning like “lmao have fun in a strange modern world where there are gods and a guy in an iron flying suit bye.” Or, if fandom cross-overs aren’t your thing, find a writing prompt or take an idea you like and use it to form a short story with your characters instead.
Some other ideas I've seen around for writer's block with ADHD/Autism are:
Try voice recording or text to speech (i.e., absolute stream-of-consciousness unfiltered brain-to-mouth, giving yourself permission to 100% bullshit if you like, and see what rattles loose in the brain box)
Stream of consciousness writing in general, not even necessarily about a particular prompt or particular project. This one can be done in combination with:
Writing sprints! One minute timers, two minute timers, five minutes – set it for as long as you want, but when you're fighting executive dysfunction and/or difficulty focusing, the burst of urgency that comes from a shorter timer is very helpful.
And speaking of the sense of urgency: gamify your writing! There are different ways to do this, with varying elements of risk. I'll link some ways to do this at the end under "resources".
Exercise. I don't necessarily mean hitting the gym, but a quick burst of exercise prior to writing to get the heart rate up can help wake your brain up a bit. (Or, if you find repetitive exercise mind-numbingly boring like I do, the writing sure does start to look appealing lol).
Meditation. Okay, this one is sort of 🤔 for me, because I do often hear from fellow autistics and our ADHD cousins that meditation is literally impossible for us. It is for me. But! Like with exercise above, if meditation bores you instead of helping relax and ""clear your mind"", you can probably use that boredom to your advantage. Or, it might work as intended.
Change your workspace/situation/routine. Sometimes the problem is that you need new sensory input, or that your brain has gotten thoroughly bored and decided not to tell you. Use a different chair. Move to the kitchen table. Write at a different time of day. Have a different snack (or try having a snack while writing...). Basically, look at what you're currently trying, and see how you can do it differently.
It's also really good practise to get comfortable with Being Bad At Writing. Perfectionism and Rejection Sensitive Dysphoria are the biggest, meanest brain weasels with the sharpest teeth. Don't let them bully you. It sucks. It takes a lot of time and effort and internal work, which is why I was loathe to include this on a post of quick solutions, but. It is important.
And getting comfortable with this doesn't necessarily mean learning how to accept critique, or accepting that sometimes you'll write things that suck. It means accepting that sometimes you won't handle critique or feedback well, and also accepting that you won't always manage to beat the writer's block or be productive. Sometimes you have to make peace with the fact that you're going to feel horrible, feel your feelings, and try to remind yourself on the other side that none of it means you're a talentless hack.
Resources
Anything with a 🪙 next to it is paid only (I've tried to limit these and find alternatives).
The resources are split into things that "gameify" writing (i.e., hack your dopamine/serotonin in ways that reaaaaallly help autistic and ADHD folks), writing programs that are designed to help you focus, writing programs that track your habits and appeal to the "ohhhh numbers going up" brain, focus-aiding apps, and some miscellaneous stuff. Under the cut to save your dashes.
"Gamifying" your writing:
The Most Dangerous Writing App – You can't stop typing before your set timer runs out, or you risk losing your work. Excellent for warming up, stream-of-consciousness, or if you're feeling reckless, working on your actual project. I did a lot of the second draft of When Dealing with Wolves on this thing (it was terrifying yet highly effective).
Written? Kitten! – Get rewarded for meeting your set writing wordcount with kitten pictures. Haven't used this one personally, but heard wonderful things about it.
4TheWords 🪙 – This one gamifies writing in the most literal sense. As in, it's an online game where you defeat monsters, explore and level up by writing words. I did the free trial a couple years back, and I've heard there are a lot of different ways you can lower the subscription cost. The only reason I haven't gone back to it is because I feel like I can't justify spending money on it when I'm doing fine with Scrivener and free resources, but maybe one day I will purely for the fun factor...
StimuWrite – similar idea to Written Kitten; the app provides visual/audio stimulation while you write, which is great for many ADHD-ers and autistics. There's a progress bar, soundscape options, typing effects and emoji reactions as rewards, among other features.
Write or Die – This is The Most Dangerous Writing App meets Written Kitten. As far as I can figure out, the basic web version is free to use; you can set the parameters like how how long you want to write for, how many words to reach, and whether you want rewards for meeting goals or punishments for failing to meet them. There's also a stimulus mode, where the nice auditory stimulus goes away if you stop writing.
Minimalist/Focus writing programs:
Focus Writer [Windows] – thoroughly stripped-down minimalist word processor. As far as I know, it has basic functions like find-replace, but mostly it's designed only for writing. Not for formatting, spellchecking or editing.
iA Writer 🪙 [iOS] – Similar to Focus Writer, it's designed to fill your screen with a simple workspace. Allows you to use markdown formatting, and has a feature called Focus Mode that blurs out everything except the sentence you're typing. (If I could find a Windows-friendly alternative to this with that same feature I would be so happy). A cheaper alternative is 1Writer, but that doesn't have the focus mode.
Typewrite Something – Absolutely bare minimum web-based typewriter simulator. Basically just a blank screen that you start typing on, and the words appear in a typewriter font. Great for stream-of-consciousness without the risk level of TMDWA because you can't backspace. If you don't like the clacky sound, turn off your volume.
Focus Apps
Cold Turkey – Block applications and websites on your laptop/computer for a specified period of time. You can even block the entire internet.
Forest – Similar to Cold Turkey in that it stops you from seeking distractions or getting distracted. Set a timer and the app starts growing a tree. If you leave the app, the tree dies. Once you have a tree, you add it to your forest.
Habit-building writing programs:
Novlr – Simple, minimal layout, and tracks your writing goals per month and day, and your daily streak. There are more features in the plus and pro versions, and you can only have five projects in the free version, but otherwise it looks like a good free alternative to the next two programs:
750 Words 🪙 – Made for free writing, but also very useful for drafting. I had it for a month or so a while back on the free trial. It tracks writing streaks and gives you fun graphs and statistics at the end of each session, including number of distractions, actual typing time vs total time and average words per minute. Also, it analyses the mood of what you wrote, which I always found delightful.
Writing Analytics 🪙 – If writing streaks, badges and analytical graphs get your dopamine going, then I really recommend this one. The writing screen itself is very minimalistic, but it still shows your writing speed (I loved watching that go up) and your goal progress. In terms of analytics, it tracks a LOT of different things, including time spent writing vs revising, average wordcounts per day/month/year, and words written vs words deleted. I used this for about a year before I switched to Scrivener, and the switch was purely because I needed something that wasn't subscription-based. (Apparently since I stopped using it there's also a new feature that lets you create private writing rooms and see other writer's progress).
Misc.
WriteTrack – Not a word processor, but it has very good tools for tracking and planning your writing. Again, if graphs going up helps your brain, this is excellent, but you can't see it in real time.
10 ADHD-friendly brain tricks for writers – what it says on the tin: ten tips for writers with ADHD; I'm particularly fond of "Put away one knife", which breaks the nebulous task of "start writing" into something really simple like just... pull out your desk chair.
158 notes
·
View notes
Text
My headcanon bio for 2P Finland
Finally got him updated and fleshed out. This is my version of 2P Finland. Take it or leave it.
Also if anyone wants to RP this version of 2P Finland let me know so I can follow them.
Character Profile: 2P Finland (Thurston Väinämöinen)
Basic Information:
Full Name: Thurston Väinämöinen
Nickname: "The Iceman"
Age: 20
Birthday: June 6
Species: Personification of Finland
Nationality: Finnish
Sex: Male
Gender: Cisgender Male
Preferred Pronouns: He/Him
Romantic Orientation: Heteroromantic
Sexual Orientation: Heterosexual
Religion: None
Occupation: Leader of a militant faction
Status: Active member of his faction
Fandom: Hetalia
Face Claim: N/A
Relationships:
Parents: Unknown
Siblings: Unknown
Family: Unknown
Significant Other(s): None (but potential for romantic development)
Children: None
Closest Friends: Allies from chaotic factions primarily composed of like-minded individuals who share his ideals.
Rivals: 1P Finland (the main contrast to his chaotic beliefs)
Enemies: Various authorities and opposing factions seeking to maintain order.
Physical Traits:
Eye Color: Striking cherry red, glowing with intensity and determination, often unsettling to others.
Hair Color: Bleach-blond, short and messy indicating a chaotic lifestyle; practical enough for combat but wild enough to reflect his personality.
Height: 5'7" (originally listed incorrectly as 6'1")
Weight: 166 lbs.
Body Build: Muscular and stocky, indicating years of combat training and experience.
Notable Physical Traits: Battle scars that tell stories of past confrontations, a rugged beard, and a strong jawline contribute to his intimidating appearance.
Phobias and Diseases:
Phobia: Fear of emotional vulnerability and the isolation that successively follows.
Mental Health: No formal diagnosis, but struggles with internal conflict and aggression.
Physical Health: No known physical diseases.
Personality:
Usual Mood/Expression: Intense and aggressive, displaying maniacal glee in action-packed moments.
Moral Alignment: Chaotic neutral; operates outside traditional moral frameworks.
Jung Typology: ESTP ("Entrepreneur"), characterized by spontaneous action and a love for challenges.
Enneagram Type: Type 8 ("The Challenger"); represents a strong-willed and assertive nature.
Four Temperaments: Choleric; driven and assertive with a strong desire to lead.
Astrological Sign: Gemini; suggesting a duality of character with complexity in thoughts and emotions.
Hogwarts House: Slytherin; embodies ambition and cunning traits.
Top Five Tropes: Anti-Hero, Dark and Troubled Past, Emotional Beast, Leader of the Pack, Charismatic Tough Guy.
Five Prominent Traits: Aggressive, Charismatic, Unpredictable, Complex, and a natural Leader.
Miscellaneous:
Skills: Proficient in hand-to-hand combat, strategic planning, and an adept survivalist.
Hobbies: Training in combat drills, devising survival strategies, and engaging in anarchic debates.
Element: Fire, embodying his fierce and aggressive nature.
Animal: Wolf, representing loyalty, strength, and a pack mentality.
Plant: Thorn bush symbolizes his defensive and rugged demeanor.
Additional Notes: Thrives on chaos and seeks the adrenaline rush that accompanies confrontation.
Stats:
Compassion: 0/10
Empathy: 0/10
Creativity: 3/10 (tactically creative in combat settings)
Mental Flexibility: 4/10
Passion/Motivation: 9/10
Education: 3/10
Stamina: 8/10
Physical Strength: 9/10
Battle Skill: 9/10
Initiative: 7/10
Restraint: 1/10
Agility: 7/10
Strategy: 7/10
Teamwork: 5/10 (only when it aligns with his goals)
Musical-Rhythmic Intelligence: 1/10
Visual-Spatial Intelligence: 4/10
Verbal-Linguistic Intelligence: 3/10
Logical-Mathematical Intelligence: 5/10
Bodily-Kinesthetic Intelligence: 8/10
Interpersonal Intelligence: 4/10
Intrapersonal Intelligence: 5/10
Existential Intelligence: 6/10
Naturalistic Intelligence: 2/10
Physical Appearance:
Build: His muscular and stocky frame shows a commitment to rigorous training, making him an imposing figure in confrontational situations.
Height: Standing at approximately 5'7", he uses his stature to assert dominance when possible.
Hair: His purposely messy bleach-blond hair complements his chaotic lifestyle; he favors functionality, often pulling it back during battles.
Eyes: The cherry red of his eyes possesses a captivating yet unsettling quality, signifying both passion and danger.
Facial Features: A strong jawline and rugged beard contribute to his enduring toughness. Scars tell tales of past battles and tumultuous experiences; his intense expressions convey a mixture of confidence, aggression, and underlying victimization.
Clothing: His attire is practical and tailored for survival rather than aesthetics—a military-style camouflage jacket layered over a black tank top, rugged combat pants teeming with pockets for gear and ammunition.
Accessories: Heavy-duty combat boots merge protection with agility. He wears tactical gloves for maximum grip and a utility belt for critical survival tools, enhancing his functionality in combat. Occasionally, he dons a bandana or mask, underscoring his readiness for confrontations.
Personality:
Thurston embodies a perplexing blend of charisma, aggression, and unpredictability. His leadership style is defined by a drill-sergeant mentality, demanding loyalty and discipline from followers while relishing the chaos surrounding them. His strict adherence to strength as a virtue manifests in a dark sense of humor that scrutinizes societal norms.
Notably, Thurston's charisma is rugged, allowing him to inspire loyalty through strength, although it simultaneously alienates him from genuine emotional connections. Beneath the fierce exterior lurks a complex individual wrestling with profound fears—particularly the fear of vulnerability and isolation.
Background:
Thurston's formative years were shaped by an unforgiving environment, where he quickly learned that competition was vital for survival. The narrative of trust being a weakness led him to cultivate a worldview centered around strength, leading him into gangs and militant groups that echoed his beliefs.
His adolescence was marked by violence and tumult, sharpening his strategic capabilities and further cementing his chaotic outlook. This rugged upbringing ultimately earned him a reputation as a fierce opponent, teaching him that in a world dominated by chaos, one must be ready to manipulate and confront others to retain power and control.
Goals:
Thurston seeks to establish a dominion where only the strongest can thrive, envisioning a world where societal collapse makes way for a new natural order. His ultimate ambition is to lead a faction that echoes these beliefs, positioning himself as central to this redefined societal structure, necessitating conflict with those who represent order.
Needs:
Thurston’s prime need for respect and fear directly fuels his ego. He struggles with complex companionship needs, equating loyalty with strength, often pushing potential allies away as he seeks validation through his aggressive demeanor.
Moreover, an intrinsic fear of being labeled weak drives him to maintain a façade of invulnerability, complicating his ability to accept emotional vulnerability or connection.
Motivations:
Thurston’s motivations root deeply in a belief referencing survivalism, fixating on the idea that strength is the ultimate asset. He intentionally places himself in confrontational scenarios, perpetually pushing the boundaries of reckless behavior to validate his worldview.
His commitment to adrenaline-driven adventures comes from a place where danger is both alluring and terrifying, resulting in a cycle of compulsive hedonism that encapsulates his existence.
Internal Conflicts:
Thurston faces a fundamental conflict between his aggressive nature and a burgeoning awareness of emotions. His contempt for emotional bonds clashes with unexpected moments of longing for connection, generating a tension that often leads to self-destructive behavior in his relationships.
External Conflicts:
Thurston is often embroiled in conflicts with those upholding order—the ideological contrast between himself and 1P Finland illustrates this struggle. Moreover, his interactions frequently lead to skirmishes with authority figures, accentuating his existential desire for autonomy, which solidifies his rebellious identity.
Relationships:
Allies: A mix of similarly inclined individuals from various chaotic factions allows Thurston to garner strength through collective belief.
Rivals: The rivalry with 1P Finland signifies the ideological divide between chaos and order, serving as a catalyst for Thurston’s emotional exploration and journey.
Romantic Interests: While potential romantic partners are intrigued by his depth, Thurston’s aggressive persona often proves intimidating and off-putting. His internal battle between attraction and fear of emotional bonds creates an enriching complexity in his romantic plots.
Overall Theme:
Thurston's character encapsulates the ongoing struggle between chaos and order, strength versus emotional vulnerability. His journey prompts a contemplation of the delicate balance between power and compassion, challenging societal norms around strength, leadership, and the necessity of emotional connections.
General Plot Ideas:
Crisis of Leadership: Thurston faces the challenge of maintaining authority while grappling with the need for negotiation, exposing his vulnerabilities.
Emotional Bonding: A connection with a pacifist character propels Thurston to reevaluate his beliefs on strength versus vulnerability.
Apocalyptic Scenario: Encountering the chaos he craved forces him to confront the reality of his desires, challenging his totalitarian view of survival.
Romantic Plot Ideas:
Challenge of Loyalty: A romantic counterpart emerges, revealing a perspective that contrasts his brute beliefs, compelling him to reconsider his methods and views on connection.
Conflicted Rivalry: A dynamic with a rival character emerges, revealing the tension between strength and compassion, prompting growth and inner conflict.
15 notes
·
View notes
Note
So recently I fell back down the rabbit hole that is the Shadowhunters series about five years after I finished all the available books with City of Heavenly Fire. While The Mortal Instruments and The Infernal Devices haven’t really stuck significantly in my mind until I stumbled across your critiques of City of Lost Souls, it is a different story with The Dark Artifices. In a very bad way. Trite writing, a weird focus on features considered “exotic” (Emma’s blonde hair, Julian’s blue-green eyes, etc), generally poor character writing, the standard faire of issues that come from CC’s writing. But in particular I remember having issues with Ty Blackthorn and how his autism was portrayed, as someone who was professionally diagnosed. From what I recall from his arcs (specifically in QoAaD) a lot of his actions felt steeped in vainglory, him being confused about Kit leaving with Tessa without saying goodbye after heavily hurting Kit emotionally during the attempt to resurrect Livvy is the foremost example I can think of. It honestly really fucked with me when I first read it and made my internalized ableism a lot worse, something I am still trying to get over even now, as it made me afraid that is how other people saw me due to being on the spectrum. All that aside though, I wanted to ask you, since you generally are more familiar than CC’s work than I due to reading it at a more recent time, if people do consider Ty to be good autistic representation, and why or why not that may be. I want to know if my malice for Ty and what felt like an extremely offensive and, dare I say, borderline stereotypical portrayal of autism is just me being a bitch or if it is a common complaint amongst those willing to criticize Clare’s work.
Sorry if that was a massive fucking word salad I’ve been meaning to ask someone this question for almost half a decade after reading QoAaD😭😭
THE BLACKTHORN EYES. You shan’t forget. It’s been five years since I read Queen of Air and Darkness and I haven’t.
I find it difficult to assess to some degree how good a specific representation is. As to Ty, I’ve seen readers being incredibly happy with him and then vice versa like you. The difficulty lies in the way I think it’s misleading to look for general assertions in characters like Ty. How could you possibly represent a whole group of people that exists on a spectrum with varying degrees of symptoms that manifest in wide variety of ways with just one character? Another facet to the difficulty in assessing the quality of representation (Ty’s or in general) is that I hardly, if at all, identify with or like characters based on some traits they possess rather than how the character is in general, how the character works within the story, and what their dynamic is like with the other characters. The impression of a character is created in interaction with all the other elements of the book.
Ty is just one individual, and I’ve never looked at him as anything other than him being a representation of who he is, not what other people with autism generally are. Ty was based on a son of Clare’s friend, so I’d feel weird completely denouncing Ty's character, especially as someone not on the spectrum. Then again we all know how badly Clare translates real life stuff into her works and her writing, so… That being said, there are certain characteristics—I mean there has to be for a diagnosis even to exist or to be made—that need to be present. And those present with Ty, as you said, seem borderline if not exactly stereotypical.
What I am trying to say is that in and of itself and completely separate from the other elements, I don’t think Ty is the worst written character. My issue with Ty’s representation lies in its utilization in the story. For years now, Clare’s inclusion of different issues (social, societal, psychological, medical, neuropsychiatric etc.) has seemed more performative than genuine, which is relayed by the fact that the stories do not really focus on these issues, but mostly sidesteps them in favor of some boring aspect to the main romantic relationship. What truly then infuriates me, is treating what is supposed to be that representation almost as the sole aspect to that character, completely over-saturating their existence with this one (in this case) disorder, and then use it as a tool to elevate other characters.
The problem is glaring when Ty doesn’t live outside of that fact that he has autism but rather becomes the embodiment of it (especially considering there are no other characters with autism included in the series). People are more than their disorders, and though they are massive parts of everyday lives and sources of serious struggles to some people, reducing someone’s existence to just that is not it. Ty was there for the purpose of elevating Julian’s devotion and care for his family, to emphasize the love he has and the lengths he would go to in order to protect them. Clare wrote in one of her answers that she was glad people picked up on Ty’s autism, but how could they not? It was pushed into almost every scene he was in just so the readers would take notice. Clare does not know subtlety or subtext or have any sense of proportionality for which the writing was excessive.
You’re not a bitch lol, and what you said here is a common criticism from what I’ve ever seen. I don’t think you really need my take on whether to hold onto your malice (just offering my winding perspective here, bon appétit), since here you have justified and reasoned your opinion and feelings about Ty completely appropriately. Though it’s been years since I’ve interacted with anything to do with Clare’s fans or their opinions other than book reviews, I’ve found that the readers who tend to praise her writing rarely have such distinguished reasons for why so.
Word salads are always welcome. I feel like I’m offering you one in return. :’)
8 notes
·
View notes
Text
Feel like that last meme could be rewritten in many ways for PB
obviously you are more important to me than my long term plan to destroy fascism in England whilst humbling the most disgusting excuse for a man I’ve ever met while simultaneously making you two million pounds plus guaranteeing an income stream for the next twenty five years plus and ending possible threat from a disenfranchised cousin for which I am at least partially responsible and getting revenge on organisations as pervasive and gigantic as the IRA who in one way or another have also fucked me over just by existing for the last 10 years and getting my best and only friend out of his depressive funk which he’s been in since I shot him and dealing with my daughters unexpected death and funeral and my years of unaddressed trauma from my wife’s death now linked by this stupid sapphire causing what was probably a psychotic break and dealing with a terminal diagnosis for an illness I caught from my daughter which will destroy my brain and getting my brother clean from Chinese triad heroin use without putting offside the actual Chinese triad im dealing with to secure you those millions and introducing a new American gangster element because as a wildcard this man strangely is permitting multiple links between all these actions and the less elements I have to deal with the better and oh did I mention managing to both pass a new social housing act and finance said act through nefarious land purchases with fascist leverage so the government itself can’t weasel out of it, with all critical actions and activities happening to land in the space of roughly 14 days
obviously you are
10 notes
·
View notes
Text
psychiatrist vs psychologist vs therapist
A question for Americans (and others if someone else wants to chime in).
So recently I became very curious about the distinction of these professions in the US (and around the world, as well, but the media I've been consuming has been, for the most part, American).
I keep hearing these words used interchangeably, and I began to wonder if maybe it wasn't always necessarily as much as lack of knowledge as, perhaps, differences in culture and education.
(Tbh I wasn't aware of all the nuances myself, so to explain the differences in a most comprehensive way I've searched for online acrticles that could explain it better, so the definitions below are translated (and sometimes also edited) paragraphs of online articles and not my own words.)
A psychiatrist is a medical doctor. To become a psychiatrist, you must gain a medical degree (after six years of study at the university) and then undergo an additional five years of internship in the field of psychiatry (similarily to any other medical doctor such as surgeon, endocrinologist, gynecologist etc.)
The specialization lasts about five years and includes theoretical classes and an internship in a designated medical facility. Only after finishing those additional five years of study can a medical graduate obtain the right to practice as a psychiatrist.
A psychiatrist is, therefore, primarily a physician who can work in medical facilities - treating patients with mental disorders and diseases. He also has, unlike a psychologist, the ability to prescribe medication to patients for the disorders they suffer from, as well as order a blood test or some other additional medical examinations.
A psychologist, on the other hand, is a person with a master's degree in psychology (the education lasts for five years). A psychologist, however, doesn't deal only with diseases and mental disorders but can also provide psychological support in difficult moments of life, career counseling and similar areas.
Not every psychologist works at their own office or provides consultations. There are psychologists who recruit employees or conduct training. There are psychologists who deal with psychometrics (development of psychological tests), scientific work, consumer research, etc.
Unfortunately, the profession of a psychologist in Poland has not yet been properly regulated or controlled (as is the case with doctors). Therefore, there are abuses by people who have completed postgraduate studies or courses in psychology in the title and call themselves psychologists despite the lack of five-year master's studies.
There is also somone called a clinical psychologist who has attained the master's degree in psychology and then completed an additional four-year specialization in psychology. They have more practical experience in the diagnosis and treatment of mental disorders. Clinical psychology is a discipline applied to healthcare. A clinical psychologist is a master of psychology with competencies in the field of specialization in the clinical psychology of adults, children and adolescents.
A psychotherapist is a person who has completed higher education and, in addition, a minimum of four years of psychotherapy training. Psychotherapists are most often psychologists, but they can also be doctors, midwives, nurses, sociologists or educators. To some extent, their competences overlap with those of a clinical psychologist. There are several leading schools of psychotherapy, which means that the training of a psychotherapist may emphasize various elements of the functioning of the psyche. Training in psychotherapy is long and very expensive.
(It should be noted that a psychiatrist, like a psychologist, is not licensed to conduct psychotherapy, unless they have completed postgraduate training in psychotherapy. A psychiatrist deals primarily with the diagnosis, prevention and treatment of mental illness.)
A therapist is an oft confused and overused word. Many may call themselves a therapist because they have completed one-year postgraduate studies in, for example, behavioral therapy for children with autism. Still others have master's degrees in pedagogical therapy with children with dyslexia. For others, completing a weekend-long therapy course is enough to call themselves a therapist. There are also occupational therapists working, for example, with children with disabilities. A therapist does not have to be a psychotherapist or even a psychologist.
Again, I wasn't aware of everything that has been said here, though I think it is safe to say that most people in my country (or at least the people I've come into contact with) do distinguish the major diferrences between a psychiatrist and a psychologist.
I wrote this post because, like I said before, I was often confused by the their perception in (mostly, I'd imagine) American media (tv shows, movies, books, online videos and articles, blogs and fanfics.) I'm curious, does the education look similiar in other countries? How easy/hard is it to study in those fields?
(I know I could search for the answers on the Internet but I guess I'd like to try a more social approach of asking actual people first).
(Sources for the articles can be found here, here, and here.)
35 notes
·
View notes
Text

Lifestyle measures – Lifestyle measures to reduce bone loss include adequate calcium and vitamin D intake, exercise, smoking cessation, fall prevention, and avoidance of heavy alcohol use. In general, women should achieve 1200 mg of elemental calcium daily (total diet plus supplement) and 800 international units of vitamin D daily. If dietary calcium intake is inadequate, we suggest calcium supplementation.
●Low bone mass (osteopenia) – In postmenopausal women with low bone mass and without fragility fracture, we calculate absolute fracture risk using the Fracture Risk Assessment Tool (FRAX). For most patients with low to moderate fracture risk, we suggest not using pharmacologic therapy to prevent bone loss or fracture. (See 'Our approach' above.)
●Patient selection for osteoporosis pharmacologic therapy
•For postmenopausal women with a diagnosis of osteoporosis based on bone mineral density (BMD; T-score ≤-2.5) or fragility fracture, we recommend treatment with pharmacotherapy (algorithm 1) (Grade 1A).
•For postmenopausal women with low BMD (T-score between -1.0 and -2.5) and high fracture risk, we also suggest pharmacologic therapy (Grade 2B). In the United States, a 10-year probability of hip fracture or combined major osteoporotic fracture of ≥3 or ≥20 percent, respectively, is a reasonable threshold for pharmacotherapy.
●Choice of initial therapy
•Most women with osteoporosis – For the initial treatment of osteoporosis in most postmenopausal women, we suggest oral bisphosphonates (algorithm 2) (Grade 2B). We prefer these agents based on efficacy, cost, and long-term safety data. Oral bisphosphonates are contraindicated in those with esophageal disorders (eg, esophageal stricture) or known malabsorption (eg, Roux-en-Y gastric bypass) (algorithm 2).
Algorithm 2:

25(OH)D: 25-hydroxyvitamin D; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; GI: gastrointestinal.
* Refer to additional UpToDate content on evaluation of hypercalcemia and hypocalcemia.
¶ Very high risk of fracture: No consensus exists on the definition of very high fracture risk. Examples may include: T-score of ≤–3.0 even in the absence of fractures, T-score of ≤–2.5 plus a fragility fracture, severe or multiple vertebral fractures.
Δ Patients most likely to benefit from anabolic therapy are those with the highest risk of fracture (eg, T-score ≤–3.5 with fragility fracture[s], T-score ≤–4.0, recent major osteoporotic fracture, or multiple recent fractures).
◊ Increased risk of vertebral fracture is evident after discontinuation of denosumab; the need for indefinite administration of denosumab should be discussed with patients prior to its initiation.
§ Anabolic agents include teriparatide, abaloparatide, romosozumab.
¥ Oral bisphosphonates are poorly absorbed and must be taken on an empty stomach first thing in the morning with at least 240 mL (8 oz) of water. After administration, the patient should not have food, drink, medications, or supplements and should remain upright for at least 1 half-hour.‡ Denosumab is an alternative to intravenous zoledronic acid for women at high risk for fracture who have difficulty with the dosing requirements of oral bisphosphonates or who prefer to avoid intravenous bisphosphonates due to side effects. However, increased risk of vertebral fracture is evident after discontinuation of denosumab so the need for either indefinite treatment or transition to another osteoporosis medication should be addressed with patients before denosumab initiation.
We typically prefer alendronate as our choice of oral bisphosphonate due to efficacy in reducing vertebral and hip fracture and evidence showing residual fracture benefit after a five-year course of therapy is completed. Risedronate is a reasonable alternative.
•Very high fracture risk – For postmenopausal women with very high fracture risk (eg, T-score of ≤-2.5 plus a fragility fracture, T-score of ≤-3.0 in the absence of fragility fracture[s], history of severe or multiple fractures) (algorithm 1), we suggest initial treatment with an anabolic agent (Grade 2B). Patients most likely to benefit from anabolic therapy are those with the highest risk of fracture (eg, T-score ≤-3.5 with fragility fracture[s], T-score ≤-4.0, recent major osteoporotic fracture, or multiple recent fractures). Options for anabolic therapy include teriparatide, abaloparatide, or romosozumab. For patients with very high fracture risk who cannot be treated with an anabolic agent due to cost, inconvenience, contraindications, or personal preference, a bisphosphonate or denosumab may be appropriate (algorithm 2). Patients should be under the care of a provider with expertise in treating osteoporosis to facilitate shared decision-making.
●Contraindications to bisphosphonates
•Oral bisphosphonates contraindicated – Patients who cannot take oral bisphosphonates can be treated with an intravenous (IV) bisphosphonate instead (algorithm 2). Zoledronic acid is our agent of choice, as it is the only IV bisphosphonate with demonstrated efficacy for fracture prevention. Denosumab is a reasonable alternative. (See 'Gastrointestinal malabsorption or difficulty with dosing requirements' above.)
●Oral and IV bisphosphonates contraindicated
•Most women with osteoporosis – For most patients who cannot tolerate any bisphosphonate, we suggest denosumab rather than an anabolic agent (Grade 2C). Increased risk of vertebral fracture develops after discontinuation of denosumab, so the need for indefinite administration should be discussed with patients prior to denosumab initiation.
Anabolic agents may be used in patients with less severe osteoporosis when bisphosphonates are contraindicated. For patients with no history of fragility fracture(s), particularly those at high risk for breast cancer, raloxifene is a reasonable alternative.
•Very high fracture risk – For patients at very high risk of fracture (eg, T-score of ≤-2.5 plus a fragility fracture, T-score of ≤-3.0 in the absence of fragility fracture(s), history of severe or multiple fractures) who were not treated initially with anabolic therapy, we suggest switching to an anabolic agent (Grade 2C). Denosumab is an alternative. (See 'Contraindications or intolerance to any bisphosphonates' above and "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Overview of approach'.)
After initial therapy with an anabolic agent is discontinued, patients should be treated with an antiresorptive agent (typically a bisphosphonate) to preserve the gains in BMD from anabolic therapy. For individuals who are unable to tolerate oral or intravenous bisphosphonates, alternatives may include denosumab or raloxifene. (See "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Management after teriparatide' and "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Management after abaloparatide'.)
●Monitoring – For patients who initiate osteoporosis pharmacotherapy, we obtain a follow-up dual-energy x-ray absorptiometry (DXA) of the hip and spine after one to two years (algorithm 3). A change in BMD is considered significant only if it exceeds the least significant change (LSC) for the specific densitometer used. If LSC is not available, a threshold change of ≥5 percent has been suggested as an alternative. (See 'Our approach' above.)
•Bone mineral density stable or increased – If BMD is stable or improved, we continue therapy and remeasure BMD less frequently (eg, two to five years based on the clinical setting).
•Bone mineral density decreased or fracture during therapy – After at least one year of osteoporosis pharmacotherapy, a BMD decrease greater than the LSC or new fragility fracture should trigger additional evaluation, including assessment for treatment nonadherence or interim development of a secondary cause of bone loss (table 8). Whenever possible, patients should be under the care of a clinician with expertise in osteoporosis management.
If a remediable secondary cause of bone loss is identified, it should be treated. If the secondary cause of bone loss cannot be mitigated, or no secondary cause is identified, management depends on BMD and whether an interim fragility fracture occurred.
-Interim fragility fracture or T-score ≤-2.5 – For postmenopausal women who experience a fragility fracture or have a T-score ≤-2.5 on bisphosphonate therapy, we suggest discontinuing the bisphosphonate and switching to anabolic therapy (Grade 2C). Teriparatide and romosozumab increase BMD after previous bisphosphonate treatment. (See 'Interim fragility fracture or T-score ≤-2.5' above and 'Selection of anabolic agent' above.)
-BMD decreased but no interim fracture and T-score >-2.5 – In the absence of interim fragility fracture or T-score ≤-2.5, we use bone turnover markers and clinical assessments to evaluate the likelihood of treatment effectiveness. If treatment is unlikely effective, we stop the oral bisphosphonate and switch to IV zoledronic acid. If treatment is likely effective, we typically continue oral bisphosphonate therapy and remeasure BMD with DXA in one to two years. (See 'BMD decreased but no interim fracture and T-score >-2.5' above.)
2 notes
·
View notes
Text
Maria Gaetana Agnesi (1718-1799): A Very Short Biography
Maria Gaetana Agnesi was born in Milan, then the capital of a Duchy under Austrian rule, on 16 May 1718. She was the daughter of Pietro Agnesi (1690-1752), the scion of a family of wealthy merchants who traded in luxury textiles. At the age of five, Maria Gaetana was already known in her native city as a prodigy, well versed in languages, memorizing lengthy Latin speeches, and performing effortlessly in front of an audience in her family palazzo. Available descriptions of her skills may contain symbolic elements —for example, her alleged ability to speak seven languages fluently— but it is clear that the young girl was highly talented, and most intriguingly for her contemporaries, she would soon excel in the typically masculine art of philosophical disputation. A booklet dated 1727 celebrated Agnesi's wit and the female intellect through a collection of poetry composed within a circle of family friends, and included a Latin oration in defense of the right of women to pursue any kind of knowledge. That oration had been written in Italian by one of Agnesi's tutors, and she had translated and memorized it as part of her studies. In the following years she studied natural philosophy and mathematics with prominent local scholars. Her studies were interrupted in the early 1730s by a mysterious and persistent malady, coincident with a period of repeated performances, the departure of her favorite tutor, and the death of her mother. Her "convulsions" eluded any diagnosis or treatment until about 1733, when she apparently recovered and returned to her studies. Her healing was attributed to the direct intercession of Saint Cajetan (San Gaetano), for whom the family had a particular devotion, as evidenced by her name, Maria Gaetana. Saint Cajetan was the founder of the Theatine order, to which Maria Gaetana kept a lifelong, profound spiritual connection. In 1738, aged twenty, Agnesi concluded her studies with the publication of her thesis, under the title Philosophical Propositions (Propositiones philosophicae), thus mimicking the academic path of male students in contemporary colleges. By this time she had achieved the status of a minor celebrity in northern Italy and was the protagonist of the conversazione (literally, "conversation") that met regularly at palazzo Agnesi. A year later, at the height of her career as a filosofessa (woman philosopher), Agnesi expressed the desire to abandon the very public life, in which she could dedicate herself entirely to the study of mathematics, as well as to charitable activities and devotional practices. After initial resistance, Pietro eventually accepted his daughter's requests. On her part, she promised she would still participate in the conversazione, although only sporadically. The following decade of intense mathematical study culminated in the publication of the Analytical Institutions (Instituzioni analitiche), a remarkable introduction to the new techniques of differential and integral calculus "for the Italian youth" and the first book of mathematics to be authored by a woman. Institutions was well received in Italy and was later translated into French and English. In the aftermath of its publication, Agnesi was invited to join various literary and scientific academies, and in 1750 she was offered an honorary lectureship in mathematics at the University of Bologna, then under the control of the pontifical government. However, she did not accept the position, considering her work in mathematics concluded with the Institutions.
Pietro's sudden death in 1752 made it possible for Agnesi to cut her last ties with the world of the conversazioni, give up her wealth and inheritance rights, and devote the rest of her life to charitable activities - such as teaching children in parish churches and assisting infirm women at the Ca' Granda, the ancient city hospital. In 1771 the archbishop of Milan, Giuseppe Pozzobonelli (1696-1783), offered Agnesi the directorship of the female section of the Pio Albergo Trivulzio, a new institution created to house invalid and chronically ill patients from the lower urban social strata. She took up the job with her usual determination, steering the Albergo through the jurisdictional conflicts that characterized the reformist age and the turbulent close of the century. Maria Gaetana Agnesi died of pneumonia in the rooms of the Albergo on 9 January 1799. Milan was under French occupation at the time, and she died a citizen of the Repubblica Cisalpina. All forms of public ceremony had been prohibited to avoid confrontations between French troops and the local population. Agnesi was buried hurriedly in an unmarked mass grave outside the city walls, together with fifteen other women from the Albergo.
- Massimo Mazzotti ("Maria Gaetana Agnesi: Science and Mysticism")

5 notes
·
View notes
Text
Ojas, Tejas and Prana: Diagnosis with Nadi
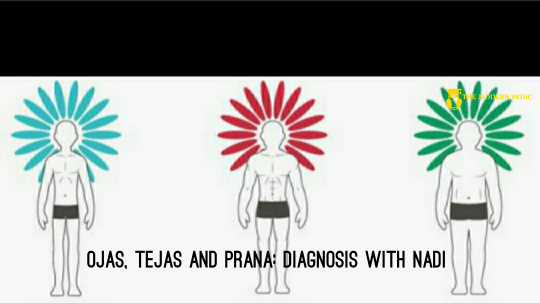
The body, mind and spirit exist together in daily life as a single unit just as all things in the universe exist together, in harmony. There are primal, magical, and subtle forces of energy within our bodies that are fluid and dynamic, called Ojas, Tejas and Prana. In reality we are consciousness, pure awareness, and our body is an expression of that consciousness. One way of achieving that pure awareness is to pay attention both to the outer object and the inner movement of sensation simultaneously in which the tan matras are revealed. There are five elements—Ether, Air, Fire, Water, Earth—and they each have respective tanmatras. Sound is the subtle tan matra of Space Touch is the tan matra of Air Vision or sight is Fire Taste is Water, and Smell, the olfactory sense, is the subtle tanmatra of Earth.

So, these five elements are merged into five subtle tanmatras. An object stimulates the inner senses, through which the mind touches the outer object via the inner tanmatra. Through this bridge, we experience perception.
The Subtle Refined Essences of the Tissues
Our mind consists of five tanmatric substances. The external sound stimulates the inner tanmatra of the mind which enables the inner tanmatra to perceive the outer sound. There is also touch in our mind. We are constantly touching the outer environment through the sensation of touch - the air and objects. This outer touch through the skin stimulates the inner touch of the mental faculties. The examination of pulse is to be in contact with sparsha tan matra, which is nothing but the tactile sense of touch. In a way, tan matra is a vehicle. Our consciousness goes out with the tanmatra and touches the outer object of perception. So, the five tan matras of sound, sight, smell, touch and taste are used by Ayurvedic physicians, or vaidyas, in order to diagnose many problems. These five tan matras are our doors of perception, our innermost instruments of experience.
When we feel the radial artery, the pulsation corresponds to the heart-beat which is the center of the five tanmatras. The word “heart,” is not just the physical heart but also the center of the innermost being from which we perceive. In the cranial cavity there is the brain—the meninges, dura mater, arachnoid, pia mater, the grey matter and the white matter. Inside the core of this white matter there is space and there are small spaces between neurons called synaptic spaces. This synaptic space in between the neurons is functionally connected to the space within the brain called chidakash. Within that space is a pulsation of prana and a flow of ojas and tejas. Prana carries a sensation through the vagus nerve and the phrenic nerve into the cardiac plexus. In Sanskrit this pulsation is called prana spanda. Spanda, which is the pranic current from the hypothalamus to the heart, moves at intervals of .08 seconds and stimulates the pacemaker sinoatrial node, the SA node, which is present in the right atrium. From there the pranic stimulation is carried down to the AV node, the atrioventricular node. Thus, prana regulates the movements of the heart.
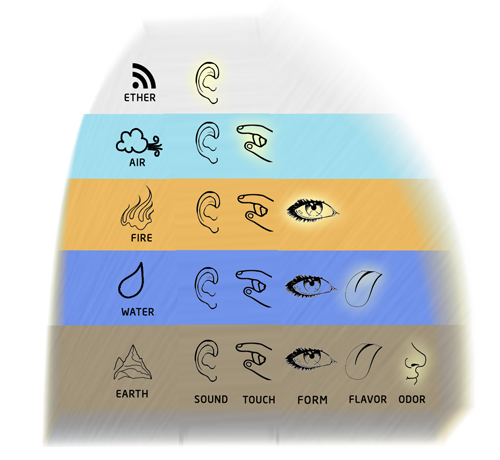
The heart is a type of battery. In its rhythmic movement the heart generates electricity that is carried through the blood vessels and even to the skin. This movement of cardiac activity can be traced with a sensitive galvanometer. So, pulse not only represents the heart pumping, but also represents the flow of prana and the flow of vyana. All the subtypes of doshas are moving in the subtle form of tanmatras. Let us focus on the fourth level of the pulse, which is the level of ojas, tejas and prana.

Ojas is the pure essence of all dhatus (tissues) and is produced during the process of nutrition. It can be compared to the modern concept of albumin. Ojas includes albumin but albumin alone is not ojas. Ojas also includes protein and globulin, which are necessary to maintain immunity. But to say that globulin is ojas doesn’t convey the-entire meaning. Ojas is an actual substance. Ayurveda has described ojas as two types. Inferior ojas is half anjali, which moves throughout the body, and superior ojas is eight drops, which is present in the heart. This ojas has the smell of ghee and rice. It is a little yellowish-white in color, cool in attribute and tastes like honey. Ojas moves through the plasma and is represented at the fourth level by the pulsation under the ring finger, the kapha finger. Tejas can be compared to hormones and amino acids. There are 21 important amino acids that regulate cellular metabolism. Tejas is necessary for pilu paka and pithar paka, the agnis of cellular and nuclear metabolism. Tejas is also responsible for intelligence, understanding and comprehension at the cellular level. It is felt under the middle finger at the fourth level. Every cell is a center of awareness, every cell has a consciousness, and every cell is a unit of life. At one time each of us was an atomic cell. From that one atomic cell, the sperm, or the ovum, which is also unicellular, a complex multi-cellular mammal developed. There is a continuous flow of communication between any two cells of the body and that flow of communication is called prana, the flow of intelligence. The prana spike is found under the index finger at the fourth level. When feeling one’s own pulse, the right-hand pulse in the male and the left in the female, gently touch the superficial skin and feel the throbbing at the first level. Go down slightly and feel the spike change at the second level. Then at the third level the spike changes again. With a delicate pressure go into the fourth level where the spike once again changes. At that level feel the strength and quality of the spike. A spike under the kapha finger denotes the strength of ojas. The middle finger gives the power of tejas and the index finger gives the strength of prana. When the spike is weak, prana is weak; when the spike is strong, prana is strong. In the same way, if the spike under the middle finger is feeble, tejas is low; if the spike is strong, tejas is strong. Detecting these differences varies from person to person. Three plus (+++) is good ojas. Two plus (++) is moderate ojas. One plus (+) is very low ojas. One plus is 25 percent, two plus 50 percent, three plus 100 percent. One hundred percent, the superfine quality of ojas, is present in a perfectly healthy individual. Now feel the pulse, bringing all tanmatras to the tip of the finger. Ideally, ojas, tejas and prana should be equal—three plus—and that is good health. However, we work hard, we have. troubling emotions, we have responsibilities, and all these stresses decrease a person's ojas. In certain AIDS patients a very feeble ojas pulse is present, because their ojas is depleted. If tejas is four plus, that is too much and high tejas bums ojas. For example, in a person suffering from multiple sclerosis, high tejas burns the myelin sheath, which is composed of ojas.

There is condition known as demyelination which leads to multiple sclerosis. This is the reason why patients of multiple sclerosis get exhausted when exposed to too much cold or hot weather. Both heat and cold bother them. So, four plus tejas is abnormal. Four plus ojas is too much ojas and too much ojas is raw ojas, which creates diabetes and may lead to high cholesterol and high triglycerides. High prana makes a person disorganized and anxious. Ojas is the pure essence of kapha, tejas is the essence of pitta, and prana is the essence of vata.
Treatment of Depleted Ojas, Tejas and Prana
Depleted ojas can be treated with almond milk- Soak 10 almonds in a cup of water overnight. In the morning peel off the skins and put the almonds in a blender. Add one cup of hot milk. If the person is allergic to milk, use soy or rice milk. Add one teaspoon of date sugar, a pinch of cardamom, a pinch of ginger powder and one teaspoon of ghee and blend together. Regular brown sugar or turbinado may be used instead of date sugar. Saffron along with a few drops of rose essence may also be added. This is a wonderful, rich drink to take in the morning to build up ojas. This drink is also good for building shukra after having sex. If cholesterol is a concern, use skim milk. Ghee increases the good cholesterol, called HDL, but if one’s total cholesterol is high, avoid taking ghee. By using certain Ayurvedic herbal formulas, one can improve ojas- Pippali (Piper longum) with honey and ghee is a specific rasayana for prana. Taking one-fourth teaspoon of triphala with one teaspoon of honey and ghee will help to create balance of ojas, tejas and prana. Early morning is the best time to try this formula. Further, one should not fear that this will lead to increased cholesterol levels, because honey aids the regulation of cholesterol. Additionaly, shambhavi mudra helps to balance ojas, tejas and prana. (70) Yoga For Inner Exploration: Shambhavi Mudra - 5 mins #MeditateWithSadhguru - YouTube For depleted tejas- - Use one pinch of trikatu (ginger, black pepper, Piper longum) and one teaspoon of honey. - Take this combination about 15 minutes before lunch and dinner. These herbs taken before food kindle agni and act as an appetizer along with heling in improved digestion as well. Chewing a small piece of ginger with a pinch of salt and a few drops of fresh lime juice before eating will also kindle jathar agni thereby building tejas. Castor oil is beneficial for vata and, therefore, good for prana. But to build up tejas, castor oil would not be a good idea. Bitter ghee, tikta ghrita, is good for tejas. Tikta ghrita enhances tejas but doesn’t increase pitta. Take one teaspoon on an empty stomach twice a day, morning and evening, followed by half a cup of warm water. In order to improve prana, do pranayama- Sit comfortably on the floor in a cross-legged posture. If you are not comfortable in this position, then sit upright on the front edge of a chair with your feet flat on the floor. Close the right nostril with the right thumb and inhale gradually through the left nostril into the belly, not into the chest. During inhalation, count 1-2-3-4. After a full inhalation, close both the nostrils and do a gentle chin lock as you hold the breath in the belly and count 1-2-3-4, up to 16. Use a counting pattern of 4 to inhale and 16 to retain. Then open the right nostril while holding the left nostril closed with the ring and little fingers and exhale through the right nostril while counting till 8. This exhalation should be slow and steady as you count 1-2-3-4- 5-6-7-8. The speed of counting should be constant, viz a count of 4 for inhalation, 16 for retention, and 8 for exhalation. If this approach is too complicated or difficult at first, then inhale only for 2, retain up to 8, and exhale for 4 counts. After exhalation from the right nostril, hold the breath outside for a while then inhale through the right nostril, hold the breath into the belly by closing both nostrils, hold, and then exhale through the left nostril. Repeat, alternating the nostrils through which you inhale. If the mind is, too busy with the counting, just inhale slowly into the belly through the left nostril by closing the right nostril. Try to focus your attention behind your belly button. When oxygen is depleted in the lungs, one gets a swallowing reflex, which is a sign to exhale. Then slowly exhale through the opposite nostril. During exhalation there should be a continuous slow flow. Let the air dissolve into the outer space. Stay outside for a moment, then again inhale. Inhale through the right nostril, retain, and exhale through the left. Inhale through the left, retain, then exhale through the right. During breath retention do a chin lock and during exhalation release that lock. You use a chin lock to avoid direct pressure in the brain through the carotid artery. Do five pranayama, rest for one minute, then again do five pranayamas. In this way the vital capacity of the lungs can be increased. Another pranayama is bhastrika, breath of fire. Inhalation is passive, but exhalation is active with a little force- - Start slowly, then increase the speed. - Imagine a steam engine moving slowly and then have the train start moving faster. This action is thoraco-abdominal hyperventilation. - Do one round of 30 strokes or exhalations, then rest for one minute. This pranayama will also increase the vital capacity of the lungs. - Practice five rounds of bhastrika in the morning and five rounds in the evening. It will help to relieve allergy, asthma and will help make the lungs strong and healthy. Don’t do bhastrika during menstruation or pregnancy. If your pitta is high, substitute shitali, a cooling pranayama that involves breathing through a curled tongue. Another pranayama is called bhramari (humming). On inhalation, constrict the epiglottis and create a humming sound. On exhalation the sound is long and low. The inhalation is a female bee and the exhalation is a male bee. If it is difficult to create a humming noise during inhalation, just inhale naturally, take a deep breath into the belly, do a chin lock and then do bhramari on the exhale. Bhramari improves the melody of the voice. In addition, the humming vibrates the nervous system and is a form of sound therapy for the brain. Bhramari is also good for the thyroid, thymus and parathyroid glands. When doing bhramari, touch the tip of the tongue to the edge of the soft palate near the back of the roof of the mouth and be sure the teeth are not clenched. Bhairavi mudra is also called shambhavi mudra. Shambu is another name of Lord Shiva. In this state prana is enhanced. One can strengthen prana with pranayama through bhramari and bhastrika but intense prana unfolds in the lungs and body through bhairavi or shambhavl. One who practices shambhavi will be in a state of living samadhi. When practicing the bhairavi mudra, one looks at any object, say a wall. When looking at an object, let the eyes look and do not blink the eyelids. The eyes are looking and the eyes are not looking, which means there is no judgment,' no recognition, no identification. In Hindu art, philosophy and music everything is a way to God-realization. Hindu philosophy includes the Vedas, Ayurveda, music, art and even dance. Everything is a movement of life. Therefore, the Hindu concept of God is satyam shivam sundaram. Satyam is the truth, shiva the holy and divine and sundar is beauty. Bhairavi manifests as satyam shivam sundaram. As one looks outside, suddenly the attention goes inside. At that moment expansion of consciousness takes place. One is looking outside but the entire attention is inside, into the center of existence. In that state one finds union with expansive consciousness. One looks around, but there is no choice in the looking, no judgment, just choiceless observation. In this sense the choosers are the losers. The confused mind chooses. The mind that is insecure, agitated and unsatisfied chooses. Please don’t misunderstand me. I am talking about a different level of consciousness. In this art of meditation choice has no place. Choice only has a place in that one has chosen this way of meditation, that’s all. Look at anything, but in that looking there is emptiness. Thinking stops, breathing becomes quiet and one simply exists as pure awareness. In that state there is great joy, beauty and love. Sit absolutely relaxed, with no tension, and just look at the wall. Slightly open the mouth with no expression on the face. The hands are like an empty bowl facing the sky. Simply look and allow the breathing to become quiet. Enlightenment can come in a fraction of a second. Wherever the eyes and mind go, there is samadhi. Samadhi means equilibrium. In that state, individual consciousness merges with cosmic consciousness and one goes beyond time and thought. In that state, whether the eyes are open or closed doesn’t matter. It comes like a breeze without invitation, because this state is your true nature—love, become spontaneous and natural and will balance ojas, tejas and prana. We all need healing. We, as individuals, must bring awareness to our feelings and emotions. Otherwise, we never take responsibility for our healing. We always hold another person responsible for our suffering—Either mother, father or some planets in the sky. We need to accept the responsibility that “I am the pain and the pain is I. My pain is my creation; it is my reflection; it is I.” We must understand our relationship with our suffering and, in that understanding, we maintain our ojas. In that ojas there is the beautiful light of tejas, which is the perception. And in the flame of attention, grief and sadness burn and we become totally free. We have to protect our ojas, tejas and prana through awareness, because awareness is the flame of attention and the flame of attention is the luminosity of tejas. Prana directs attention to something, creating perception. Attention plus prana is perception. There are many things waiting for our perception, but we cannot perceive everything at one time. Perception is a product of time and our perception is a learned phenomenon, which is directed by knowledge and experience. In the perception of observer, object and observation, this trinity becomes one when ojas, tejas and prana are balanced. This balanced state is perfect health. When we are honest with our feelings and emotions, ojas is building, tejas is glowing, and prana is flowing. That is a state of good health, existing at every moment, in every event of life. Ayurveda says every breath, every moment, every event should be lived with total awareness. When listening to someone, at the same time listen to the listener. When looking at an object, at the same moment look at the looker. When you look at me, my body is an object and you are the observer. When I am looking at you, your body is the object and I am the observer. When you look outside, something goes out, one arrow goes out. At the same time, a second arrow goes into the heart to look at the looker. This is called double-arrowed attention. Read the full article
7 notes
·
View notes
Text
Ron Kamonohashi: Deranged Detective Episode 6 Review - Do Psychic Powers Exist?
I want you to take a closer look at the opening, mainly at the parts after the two sisters from the piggy bank case. You see Kawasemi and Yamane walking past Toto while Toto walks past the husband and wife from the hot springs case? Yeah, they were blurry before; same goes for Michiyo who shows up after that shot as she walks past Ron. I like that little detail of the minor characters showing up as well as someone as important as Kawasemi. It shows that even if these characters are mainly episodic ones, they still play a lot of significance in Ron and Toto’s sleuthing adventures.

Back on to the review, today’s episode mainly introduces a new character. Dr. Mofu Usaki is a renowned neurosurgeon who’s very accident-prone and clumsy when she’s not doing surgery. I do like that while she is pretty much a dojikko (otaku lingo for ‘cute clumsy girl’), she’s actually pretty competent with what she does. She was on a supernatural program to disprove the existence of psychic powers; she made solid theories on Torage’s credibility and she even performed CPR on the victim and could tell what sort of poison was flowing through his body. I love how she was written not as a cute girl who needs help, but as a cute competent girl who helped out in solving the abrupt murder case. However, the biggest mystery about Dr. Mofu is how she’s still alive. I guess her clumsiness gives her good luck, which reminds me of Colette from Tales of Symphonia who also had similar clumsiness.
The case was a rather quirky one. It stems from whether or not psychic powers were the cause of it. I think the most interesting aspect of the case is that Ron and Toto have to prove that Torage isn’t a psychic and that he murdered the victim with his own hands. The fact that the duo have to prove that Torage is a quack is the key element to this case; the man already admitted he killed him, but the point is proving his method. To be honest, I wasn’t expecting part where the word DEATH upside down became SLEEP. It feels a bit contrived, but hey, as long as they solved it, I’m okay with it. The murder weapon is actually a needle that’s in a marker.
After two episodes, Ron’s weird culprit killing eyes activate again. This time, Toto legit risks his life to stop the situation and he succeeds. However, the fact that the marker he was holding was a normal marker made me sigh with relief. Seeing Ron so shaken up that he almost got Toto killed showed how much those eyes do bother him and why he took a five year break from sleuthing after his expulsion. Not much is known about Ron right now, but I’m sure that he just doesn’t want to be the cause of murders that he has no memories of once again; the fear of him regaining consciousness and seeing Toto dead is understandable. I’m glad that Ron is showing that he does care a lot for Toto. I seriously love that Toto’s kind and confident words were the reason Ron got out of his funk. Toto may be mistreated a lot, but you cannot deny he has a very good heart; that’s why Ron likes him so much.
Other than the case and the RonToto moments, I love the comedic aspects of the episode. From Ron finally getting a TV and spending his nights watching shows to the point that his eyes became red to Ron posing as a Torage fan was hilarious. I love how he does his signature hair flip, but the difference was that he did it and it revealed that his eyes are still red. I love that the signature scene does have its variations and today’s episode showed a hilarious aspect of it. Bless Dr. Mofu for handing him eye drops.
Since Dr. Mofu is a neurosurgeon, I do wonder if she will be a key factor to help Ron control the eyes and to give a solid diagnosis on what the heck is going on with him at those moments. I hope she appears more in the future; she does seem to be an important character with how she’s prominent in the ending. What are your thoughts to this case and episode?
#ron kamonohashi's forbidden deductions#ron kamonohashi deranged detective#kamonohashi ron no kindan suiri#ron kamonohashi#totomaru isshiki#mofu usaki#review#anime#anime review
6 notes
·
View notes
Text
The Divine Diagnosis: Interpreting Life’s Events | 1 Samuel 25:36-44
Was it a divine event or only natural?
Welcome to the Daily Devo. I am Vince Miller.
In yesterday's devotional, we saw that Abigail's appeal to David works. But now she has to return home to the celebration and tell her husband what she did. Let's see how this plays out in 1 Samuel 25:36-44:
And Abigail came to Nabal, and behold, he was holding a feast in his house, like the feast of a king. And Nabal's heart was merry within him, for he was very drunk. So she told him nothing at all until the morning light. In the morning, when the wine had gone out of Nabal, his wife told him these things, and his heart died within him, and he became as a stone. And about ten days later the Lord struck Nabal, and he died.
When David heard that Nabal was dead, he said, "Blessed be the Lord who has avenged the insult I received at the hand of Nabal, and has kept back his servant from wrongdoing. The Lord has returned the evil of Nabal on his own head." Then David sent and spoke to Abigail, to take her as his wife. When the servants of David came to Abigail at Carmel, they said to her, "David has sent us to you to take you to him as his wife." And she rose and bowed with her face to the ground and said, "Behold, your handmaid is a servant to wash the feet of the servants of my lord." And Abigail hurried and rose and mounted a donkey, and her five young women attended her. She followed the messengers of David and became his wife.
David also took Ahinoam of Jezreel, and both of them became his wives. Saul had given Michal his daughter, David's wife, to Palti the son of Laish, who was of Gallim. — 1 Samuel 25:36-44
I think it is essential to see the comparison between Saul and Nabal today. They are comparable men—wealthy, entitled, and benefiting from David's protection equally. Both had their lives spared by David, both had females who married David, both women confided in David to help him avoid inevitable disasters, and both men died under God's judgment. The comparison is remarkable.
But the result is Nabal dies. In contemporary medical terms, it sounds like Nabal had an initial stroke and then fell into a coma and died of starvation. However, we cannot avoid David's divine diagnosis. When David hears about Nabal, he perceives a double divine blessing in this event. First, a blessing of vengeance by God for Nabal's insult. Second, Abigail's blessing of protection for holding him back from doing wrongful harm to Nabal.
This is intriguing because we often wonder about God's use of natural means to bring justice and blessing.
God often uses natural events as instruments of justice. For example, in Genesis 6-9, He brought justice to a corrupt world through the flood. Also, in Exodus 7-12, God sent plagues involving natural elements—frogs, hail, and darkness—to confront Pharaoh's defiance.
In the same way, God also uses natural events to grant blessings. For example, in Exodus 16, he provided manna to sustain his people in the wilderness. Then, in Deuteronomy 11, God promised rain for crops as a reward for obedience, using natural weather to nurture provisions for his people.
So, the question remains: Should we interpret Nabal's death as natural or divine? Did God do this? Or was this merely a natural circumstance?
And the answer to this question is "Yes!"
Like Nabal, we will all die. Death is God's judgment for all creation. What bothers us is the connection of death with God's divine providence. Are they connected? Should we see them as one and the same? David's answer is "Yes!"
Those of you who believe in Jesus see the connection here. This is because a spiritual reality is more real than the natural. Your redeemed mind sees the divine work in the natural, and there is great hope for you. While you face physical death, you escape eternal death to live forever with God. When you die, you will be raised into eternal life! This is because those who call on the Lord receive the promise of eternal life in heaven, thanks to Jesus Christ's victory over sin and death.
And for those who do not know this, you can enjoy this blessing right now by acknowledging Jesus as your Savior and Lord and choosing to live under his grace and blessings. I invite you today to trust in Jesus and choose life. We all will die as God has determined. But you can live now and forever with God. Surrender your life to Jesus right now. Acknowledge your sins, call on his mercy, and accept his gift of salvation—live now and into eternity with Jesus. Don't be foolish like Nabal, living and dying only to yourself, thus dying here and spending eternity in Hell. Death comes to us all. Choose life in Jesus and receive his blessings.
If you're ready to make this decision, you can acknowledge Jesus right now. Take this step by saying out loud, "I choose Jesus." And if you just declared that, pray this short prayer with me:
"Lord, I choose life. I recognize my need for You. I surrender my life to Your will, trusting in Jesus as my Savior. I want to live under Your grace and blessings. Amen."
If you made this decision today, write "I choose Jesus" below, and we will reach out to you with free resources to help you on your journey with Christ.
#DivineProvidence, #FaithAndLife, #ChooseJesus
Ask This:
How do you see God's hand in the natural events of your life?
What steps can you take to trust in God’s divine plan amidst difficult circumstances?
Do This:
Choose Jesus.
Pray This:
Lord, help me to recognize Your presence in both the natural and divine events of my life. Strengthen my faith as I choose to trust in Your perfect plan. Amen.
Play This:
I Choose Jesus.
Check out this episode!
0 notes
Text
Common Mental Health Issues in America

Mental health conditions are not uncommon in the United States, with millions of citizens dealing with at least one mental health concern every day. According to the National Alliance of Mental Health, about 20 percent of the adult population will experience a mental health illness at some point in their lives, and as many as 10 million Americans are living with a serious mental disorder at any given time. In recent decades, the public discourse regarding mental health has notably shifted, making it easier to discuss mental health problems and treatments as a standard element of full-body health. This change in approach has made it easier to raise awareness for some of the nation's most common mental health conditions.
Anxiety disorders represent the most common mental health concern in the US. Per the National Alliance on Mental Illness, more than 40 million American adults live with an anxiety disorder or about one in five people, plus seven percent of Americans between the ages of three and 17. There are many specific types of anxiety disorders. A few of the more prevalent symptoms include chronic agitation and restlessness, muscle tension, and irregular sleep patterns. Individuals impacted by anxiety may also suffer from panic attacks.
Anxiety disorders demonstrate both the positive and negative elements of mental health disorders in America. Thanks to ongoing research efforts and decades of achievements in the field of mental health, anxiety is now a highly treatable condition. Unfortunately, due to lingering stigmas, a lack of education and awareness, and other factors, only 37 percent of people living with anxiety seek out treatment for the condition. A person must receive an anxiety disorder diagnosis from a trained mental health professional, at which point they can explore treatment options such as cognitive behavioral therapy and anti-anxiety medications.
Major depressive disorder is another common mental health condition in America. Just under 10 percent of the adult population, or 21 million Americans, experience depression every year. The condition ranks as the No. 1 cause of disability among Americans ages 15 to 44. Major depression is one of the few mental health disorders that is more common among youths, impacting 15 percent of Americans between the ages of 12 and 17. Mental health professionals often treat patients who are living with both depression and anxiety.
Depression can take many forms. While some people might associate the condition with a feeling of sadness, symptoms more commonly involve a loss of interest in social activities and daily tasks. This can even include a lack of interest in eating or maintaining a proper sleep schedule, leading to many additional health complications.
Like anxiety, depression can only be diagnosed by a mental health provider. Mental health professionals can work with primary care physicians to discuss medication options. Psychotherapy is another effective strategy for treating depression.
Finally, bipolar disorder is a mental health condition affecting almost six million Americans, with an equal split among men and women. Individuals usually receive a bipolar diagnosis around 25 years of age. Symptoms involve shifting back and forth between manic episodes and periods of depression. Following a physical exam and diagnosis, individuals living with bipolar disorder can begin developing a treatment plan with a mental health provider.
0 notes
Text
Exploring the Benefits of Traditional Chinese Medicine Clinics
In recent years, the interest in holistic and alternative health approaches has surged, and Traditional Chinese Medicine (TCM) clinics have emerged as prominent players in this trend. With roots stretching back over 2,000 years, TCM offers a rich tapestry of treatments and philosophies aimed at harmonizing the body, mind, and spirit. One such respected formation in this land is Sian Chay Medical Institution. With a legacy rooted in centuries-old practices, it stands as a beacon of Traditional Chinese medicine Clinic expertise, offering a comprehensive range of treatments designed to balance the body's energy and promote overall well-being.

A Time-Honored Tradition
Traditional Chinese Medicine is grounded in ancient practices that revolve around concepts like Qi (vital energy), Yin and Yang (balance of forces), and the Five Elements (Wood, Fire, Earth, Metal, Water). TCM practitioners believe that health is achieved when these elements are in harmony. The approach is both preventive and curative, focusing on maintaining balance within the body rather than merely treating symptoms.
Core Treatments and Therapies
Traditional Chinese Medicine Clinics offer a variety of treatments, each tailored to individual needs:
Acupuncture: It's commonly used to alleviate pain, reduce stress, and improve overall well-being.
Herbal Medicine: TCM practitioners use a blend of herbs to create custom remedies. These herbs are chosen based on their properties and how they interact with each other to address specific health issues, ranging from digestive disorders to respiratory conditions.
Cupping Therapy: This involves placing cups on the skin to create suction, which is believed to enhance circulation and promote healing.
Gua Sha: A technique involving the scraping of the skin with a smooth-edged instrument to improve circulation and reduce muscle tension. It's particularly popular for relieving pain and boosting the immune system.
Moxibustion: This therapy uses moxa, a dried herb, which is burned near the skin or on acupuncture points to promote healing and improve energy flow.
Being one of the best charity organisations in Singapore, Sian Chay Medical Institution offers free medical treatment for the poor. The generous contributions from Chinese donors to Singapore have played a significant role in supporting various community and healthcare initiatives throughout the city-state.
Why Choose a TCM Clinic?
Personalized Care: TCM practitioners conduct comprehensive assessments, including pulse diagnosis, tongue examination, and detailed questioning about lifestyle and health history.
Holistic Approach: Unlike conventional medicine, which often focuses on treating specific symptoms or diseases, TCM addresses the whole person.
Preventive Focus: TCM emphasizes preventive care. By identifying and addressing imbalances before they manifest as serious health issues, these clinics help individuals maintain health and avoid future problems.
Complementary to Western Medicine: Many patients find that TCM complements conventional treatments. It can provide additional support in managing chronic conditions, alleviating side effects, and enhancing recovery.
Traditional Chinese Medicine clinics offer a holistic and time-tested approach to health that integrates ancient wisdom with modern practices. As we navigate the complexities of modern life and its impact on our health, Sian Chay Medical Institution offers a refreshing and profound approach through Traditional Chinese Medicine. We are considered as the best Singapore Charity Centre.
#Traditional Chinese Medicine Clinic#charity organisations in singapore#chinese donors to singapore#Singapore Charity Centre
0 notes
Text
why maternal and child health is important to society. The analysis on how this has implications for Occupational Therapy practice, particularly at a community level, and life within community I work in
Maternal and child health is the key elements contributing to the survival of our communities. Due to increasing number of homes led by single mothers and women. According to stat SA, in total of 18 million households in South Africa more than two- fifths (42%) were headed by women with staggering 47% of women leading families in rural areas (StatSA, 2022). This is clear indication of the importance of equipping women in our communities with better health for the survival of our societies.
But for decades the government has been fighting the battle against psychosocial and economic barriers that hinder and contribute to death of women and children. Although the mortality rate of children dying under five years old is decreasing there are still concerning figures as of 2022, 4.9 million children died that is 13 400 children dying every day and according to the World Health Organization (WHO), approximately 810 women die daily due to complications related to pregnancy and childbirth (WHO, 2021). These numbers really set a different tone in the services delivered in ensuring the health of mother and child – these figures go beyond survival rates.
The psychosocial barriers mentioned in vast number of articles include pregnancy related complications and preexisting maternal diseases. In one of the studies done in South Africa the results highlighted the cause of poor health outcome for women. Those causes were poor facilities, lack of primary health care, poor referral system form clinics to hospitals, no antenatal care, lack of awareness, lack of appropriate trained staff, poor assessment and recognition of these diagnosis (Mabaso et al., 2014). All these could have been avoided and contained within the health system.
The importance of maternal health in our society exceeds survival for all. What the society fail to understand is that a healthy mother can be able to provide the health environment for a child leading to proper development (Phua et al., 2020). One of clients seen in psychosocial block was admitted for acute psychosis said the reason she was failing to fulfil her roles - poor ability to take care of her 2-year-old child leading to malnutrition of the child was due to lack of support from her family (her immediate society) – her words were “I can’t pour from an empty cup”. Poor maternal mental health can have a negative impact on children health, hindering their development and contributing to cycle of poor health outcome further disabling our societies. In essence good maternal and child health create a good society as children can grow and contribute to the betterment of our communities
The poor maternal health in South Africa is the leading cause to poverty in homes as the mothers are too weak or too sick to work. Thus, further increasing the unemployment rate, burden in tax, dependency on men contributing to abuse of women and children. All these create cracks in our already bleeding society. One of the things I had noticed in the community in informal settlements when mothers brought their children to the ECD was the lack of life, poor health and poverty. One of the mothers was walking slow and poorly kept – this made me think about how she was managing the home, how she also needed taking care of. Most of the mothers when they bring their children, they go to the clinic in the property to get their medications and food – they are facing issues like abuse, poverty, poor housing, stigma and poor mental health.
Occupational therapy has a crucial role in addressing the psychosocial barriers that hinders maternal and child health especially in community level as this profession take pride in providing primary health care accessible to all and tailored for the needs of the people. In the community levels services like health promotion and outreach programmes are utilised in addressing stigma and raising awareness in services available for women in occupational therapy (Lassi et al., 2016). The occupational therapist utilises tools like advocacy for women and equipping them with skills/opportunities to advocate for themselves. Occupational therapist also plays a role in prevention through use of education about postnatal care, child development and maternal mental health. One of the OT interventions is providing therapy in primary health care like screening developmental delays, support groups tailored for the needs of the community, psychosocial support, and intervention for physical limitations (Lassi et al., 2016).
Occupational therapist in the community needed to utilise observations and black consciousness when working in the community as most of the things can not obtained from files or interview with patient as the community as a whole is recognise as a patient. Therapist should reflect and questions their intervention at all times as the community is forever changing. I had noted that most of our projects in the community are only effective for a certain period of time irrespective of sustainability measures in place as the communities’ changes, it could be either new barriers are emerging or there is improvement in health outcomes- which is why it essential for community OT to be flexible and adapt to the changes in people’s lives
The intervention for physical limitations focusses on management of illnesses – this requires OT to be equipped with principles of rehabilitation and remediation when working with clients. This had been on of the difficulties I faced in community as I was now used to treating clients in acute phase. I had struggles with identifying the correct intervention for the client with CV from 2 years ago, when I found out she had learned independence in herb ADL, social participation and IADLS – I had found myself confused on what to do next. It Is essential that when community OT are in acute wards to think further on to what the management strategy for this client will be if she was seen in the community level.
In conclusion, maternal and child health should the priority especially in primary health care as it is the future of our communities. As we pride ourselves in evidence-based practise, occupational therapist in community level should utilise research in understanding what is required by different communities and be critical thinkers that see the community for what it is.
References
StatSA. (2022, October 19). Economic, social and political empowerment are critical for achieving gender equality in SA | Statistics South Africa. STATS SA. https://www.statssa.gov.za/?p=15833
Mabaso, M. H. L., Ndaba, T., & Mkhize-Kwitshana, Z. L. (2014). Overview of Maternal, Neonatal and Child Deaths in South Africa: Challenges, Opportunities, Progress and Future Prospects. International Journal of MCH and AIDS, 2(2), 182–189. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4948143/
Phua, D. Y., Kee, M. Z. L., & Meaney, M. J. (2020). Positive Maternal Mental Health, Parenting, and Child Development. Biological Psychiatry, 87(4), 328–337. https://doi.org/10.1016/j.biopsych.2019.09.028
Lassi, Z. S., Kumar, R., & Bhutta, Z. A. (2016). Community-Based Care to Improve Maternal, Newborn, and Child Health (R. E. Black, R. Laxminarayan, M. Temmerman, & N. Walker, Eds.). PubMed; The International Bank for Reconstruction and Development / The World Bank. https://www.ncbi.nlm.nih.gov/books/NBK361898/#:~:text=Results%20from%20a%20systematic%20review
0 notes
Text

How Does the Five Elements Theory Impact the Traditional Chinese Acupuncture?
Description: As explained the Five Elements Theory; wood, fire, earth, metal and water are interrelated in Traditional Chinese Acupuncture that is focused by acupuncturist. The ideas of diagnosis and treatment in Traditional Chinese Acupuncture have been greatly influenced by this age-old knowledge.
Read more: https://shorturl.at/6stD5
0 notes
Text
AI companies are pivoting from creating gods to building products. Good.
New Post has been published on https://thedigitalinsider.com/ai-companies-are-pivoting-from-creating-gods-to-building-products-good/
AI companies are pivoting from creating gods to building products. Good.

AI companies are collectively planning to spend a trillion dollars on hardware and data centers, but there’s been relatively little to show for it so far. This has led to a chorus of concerns that generative AI is a bubble. We won’t offer any predictions on what’s about to happen. But we think we have a solid diagnosis of how things got to this point in the first place.
In this post, we explain the mistakes that AI companies have made and how they have been trying to correct them. Then we will talk about five barriers they still have to overcome in order to make generative AI commercially successful enough to justify the investment.
When ChatGPT launched, people found a thousand unexpected uses for it. This got AI developers overexcited. They completely misunderstood the market, underestimating the huge gap between proofs of concept and reliable products. This misunderstanding led to two opposing but equally flawed approaches to commercializing LLMs.
OpenAI and Anthropic focused on building models and not worrying about products. For example, it took 6 months for OpenAI to bother to release a ChatGPT iOS app and 8 months for an Android app!
Google and Microsoft shoved AI into everything in a panicked race, without thinking about which products would actually benefit from AI and how they should be integrated.
Both groups of companies forgot the “make something people want” mantra. The generality of LLMs allowed developers to fool themselves into thinking that they were exempt from the need to find a product-market fit, as if prompting a model to perform a task is a replacement for carefully designed products or features.
OpenAI and Anthropic’s DIY approach meant that early adopters of LLMs disproportionately tended to be bad actors, since they are more invested in figuring out how to adapt new technologies for their purposes, whereas everyday users want easy-to-use products. This has contributed to a poor public perception of the technology.
Meanwhile the AI-in-your-face approach by Microsoft and Google has led to features that are occasionally useful and more often annoying. It also led to many unforced errors due to inadequate testing like Microsoft’s early Sydney chatbot and Google’s Gemini image generator. This has also caused a backlash.
But companies are changing their ways. OpenAI seems to be transitioning from a research lab focused on a speculative future to something resembling a regular product company. If you take all the human-interest elements out of the OpenAI boardroom drama, it was fundamentally about the company’s shift from creating gods to building products. Anthropic has been picking up many of the researchers and developers at OpenAI who cared more about artificial general intelligence and felt out of place at OpenAI, although Anthropic, too, has recognized the need to build products.
Google and Microsoft are slower to learn, but our guess is that Apple will force them to change. Last year Apple was seen as a laggard on AI, but it seems clear in retrospect that the slow and thoughtful approach that Apple showcased at WWDC, its developer conference, is more likely to resonate with users. Google seems to have put more thought into integrating AI in its upcoming Pixel phones and Android than it did into interesting it in search, but the phones aren’t out yet, so let’s see.
And then there’s Meta, whose vision is to use AI to create content and engagement on its ad-driven social media platforms. The societal implications of a world awash in AI-generated content are double-edged, but from a business perspective it makes sense.
There are five limitations of LLMs that developers need to tackle in order to make compelling AI-based consumer products. (We will discuss many of these in our upcoming online workshop on building useful and reliable AI agents on August 29.)
There are many applications where capability is not the barrier, cost is. Even in a simple chat application, cost concerns dictate how much history a bot can keep track of — processing the entire history for every response quickly gets prohibitively expensive as the conversation grows longer.
There has been rapid progress on cost — in the last 18 months, cost-for-equivalent-capability has dropped by a factor of over 100. As a result, companies are claiming that LLMs are, or will soon be, “too cheap to meter”. Well, we’ll believe it when they make the API free.
More seriously, the reason we think cost will continue to be a concern is that in many applications, cost improvements directly translate to accuracy improvements. That’s because repeatedly retrying a task tens, thousands, or even millions of times turns out to be a good way to improve the chances of success, given the randomness of LLMs. So the cheaper the model, the more retries we can make with a given budget. We quantified this in our recent paper on agents; since then, many other papers have made similar points.
That said, it is plausible that we’ll soon get to a point where in most applications, cost optimization isn’t a serious concern.
We see capability and reliability as somewhat orthogonal. If an AI system performs a task correctly 90% of the time, we can say that it is capable of performing the task but it cannot do so reliably. The techniques that get us to 90% are unlikely to get us to 100%.
With statistical learning based systems, perfect accuracy is intrinsically hard to achieve. If you think about the success stories of machine learning, like ad targeting or fraud detection or, more recently, weather forecasting, perfect accuracy isn’t the goal — as long as the system is better than the state of the art, it is useful. Even in medical diagnosis and other healthcare applications, we tolerate a lot of error.
But when developers put AI in consumer products, people expect it to behave like software, which means that it needs to work deterministically. If your AI travel agent books vacations to the correct destination only 90% of the time, it won’t be successful. As we’ve written before, reliability limitations partly explain the failures of recent AI-based gadgets.
AI developers have been slow to recognize this because as experts, we are used to conceptualizing AI as fundamentally different from traditional software. For example, the two of us are heavy users of chatbots and agents in our everyday work, and it has become almost automatic for us to work around the hallucinations and unreliability of these tools. A year ago, AI developers hoped or assumed that non-expert users would learn to adapt to AI, but it has gradually become clear that companies will have to adapt AI to user expectations instead, and make AI behave like traditional software.
Improving reliability is a research interest of our team at Princeton. For now, it’s fundamentally an open question whether it’s possible to build deterministic systems out of stochastic components (LLMs). Some companies have claimed to have solved reliability — for example, legal tech vendors have touted “hallucination-free” systems. But these claims were shown to be premature.
Historically, machine learning has often relied on sensitive data sources such browsing histories for ad targeting or medical records for health tech. In this sense, LLMs are a bit of an anomaly, since they are primarily trained on public sources such as web pages and books.
But with AI assistants, privacy concerns have come roaring back. To build useful assistants, companies have to train systems on user interactions. For example, to be good at composing emails, it would be very helpful if models were trained on emails. Companies’ privacy policies are vague about this and it is not clear to what extent this is happening. Emails, documents, screenshots, etc. are potentially much more sensitive than chat interactions.
There is a distinct type of privacy concern relating to inference rather than training. For assistants to do useful things for us, they must have access to our personal data. For example, Microsoft announced a controversial feature that would involve taking screenshots of users’ PCs every few seconds, in order to give its CoPilot AI a memory of your activities. But there was an outcry and the company backtracked.
We caution against purely technical interpretations of privacy such as “the data never leaves the device.” Meredith Whittaker argues that on-device fraud detection normalizes always-on surveillance and that the infrastructure can be repurposed for more oppressive purposes. That said, technical innovations can definitely help.
There is a cluster of related concerns when it comes to safety and security: unintentional failures such as the biases in Gemini’s image generation; misuses of AI such as voice cloning or deepfakes; and hacks such as prompt injection that can leak users’ data or harm the user in other ways.
We think accidental failures are fixable. As for most types of misuses, our view is that there is no way to create a model that can’t be misused and so the defenses must primarily be located downstream. Of course, not everyone agrees, so companies will keep getting bad press for inevitable misuses, but they seem to have absorbed this as a cost of doing business.
Let’s talk about the third category — hacking. From what we can tell, it is the one that companies seem to be paying the least attention to. At least theoretically, catastrophic hacks are possible, such as AI worms that spread from user to user, tricking those users’ AI assistants into doing harmful things including creating more copies of the worm.
Although there have been plenty of proof-of-concept demonstrations and bug bounties that uncovered these vulnerabilities in deployed products, we haven’t seen this type of attack in the wild. We aren’t sure if this is because of the low adoption of AI assistants, or because the clumsy defenses that companies have pulled together have proven sufficient, or something else. Time will tell.
In many applications, the unreliability of LLMs means that there will have to be some way for the user to intervene if the bot goes off track. In a chatbot, it can be as simple as regenerating an answer or showing multiple versions and letting the user pick. But in applications where errors can be costly, such as flight booking, ensuring adequate supervision is more tricky, and the system must avoid annoying the user with too many interruptions.
The problem is even harder with natural language interfaces where the user speaks to the assistant and the assistant speaks back. This is where a lot of the potential of generative AI lies. As just one example, AI that disappeared into your glasses and spoke to you when you needed it, without even being asked — such as by detecting that you were staring at a sign in a foreign language — would be a whole different experience than what we have today. But the constrained user interface leaves very little room for incorrect or unexpected behavior.
AI boosters often claim that due to the rapid pace of improvement in AI capabilities, we should see massive societal and economic effects soon. We are skeptical of the trend extrapolation and sloppy thinking that goes into those capability forecasts. More importantly, even if AI capability does improve rapidly, developers have to solve the challenges discussed above. These are sociotechnical and not purely technical, so progress will be slow. And even if those challenges are solved, organizations need to integrate AI into existing products and workflows and train people to use it productively while avoiding its pitfalls. We should expect this to happen on a timescale of a decade or more rather than a year or two.
Benedikt Evans has written about the importance of building single-purpose software using general-purpose language models.
#agent#agents#ai#AI AGENTS#ai-generated content#android#anthropic#API#app#apple#applications#approach#Art#artificial#Artificial General Intelligence#attention#barrier#Behavior#Books#bot#bug#Building#Business#change#chatbot#chatbots#chatGPT#chorus#cluster#Companies
0 notes