#FHT
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s reach among the 26-to-35-year-olds in the US is 11%.
Text
I do not give a shit anyome, if you are going to Conan's concert tomorrow London hit me up/reblog me/ find me and kidnap me, I dont care anymore, i just need to enjoy this w someone
#conan gray#Conan#concert#london#london conan#found heaven#found heaven tour#FHT#alley rose#superache#kid krow#sunset season#overdrive#maniac#heather#3rd December#the exit#family line#lookalike
8 notes
·
View notes
Text
I'm on OB rotation again. I asked the attending what are things the PCP should know about prenatal and postpartum pts. Stuff we discussed:
SSRIs can be continued during pregnancy. I often see patients on Zoloft during pregnancy if they need an antidepressant. In fact, I just started a prenatal patient on Zoloft the other day in clinic. It is safe to continue SSRIs during pregnancy because you should treat the patient's depression. Babies can come out sort of jittery because of the SSRI, but that goes away.
Postpartum patients will have bleeding somewhat similar to a menstrual period right after giving birth. It starts to decrease and becomes like a brownish color and can last up to 6 weeks postpartum. Any bleeding beyond that point is abnormal.
There is some evidence that if you have estrogen-containing birth control, it can decrease milk supply. Actually, I had a patient in clinic recently who was seen by an attending and he started her on a progesterone only birth control so that it would not affect her milk supply. Estrogen decreases the patient's milk supply, so patients who plan to breast-feed should not be started on estrogen-containing birth control. Right after giving birth, your body has increased amounts of estrogen, so you would not start estrogen containing birth control until at least 6 weeks postpartum anyway. Increasing estrogen immediately postpartum increases risk of blood clots. For patients who plan to breastfeed and want to be on an oral contraceptive, use progesterone only oral contraceptives until she stops breastfeeding.
If the mother is breastfeeding at least every 4 hours, then this can be used for contraception. It's about 80% effective. Once baby starts sleeping through the night or once baby starts feeding more than every 4 hours, this method won't work! If you go more than 4 hours without breastfeeding, breastfeeding will not protect you from pregnancy! You can also ovulate before your menstrual period returns, so you can't say you can't get pregnant because your period has not returned yet!
I asked the attending I worked with today about how she goes about prescribing birth control. She said she will usually start with Sprintec. It's usually covered by insurance and if it's not covered, it's pretty affordable. She also said Junel is pretty well tolerated. Certain progestins in certain brands of birth control may work better for certain things like acne control, but she didn't have as much knowledge on that. I'll ask another attending again about that. I usually start people on Sprintec as well.
PCP should know that alkaline phosphatase is high in pregnant patients. It comes from the placenta. So don't be freaked out by that.
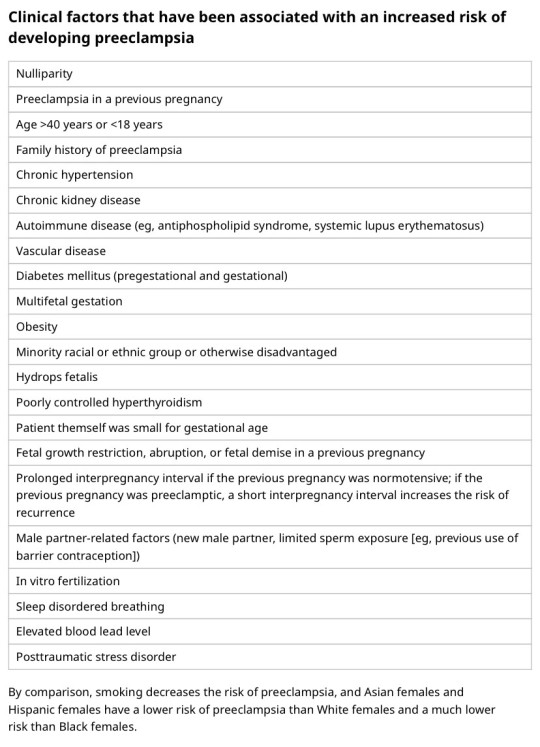
You should know HTN in pregnancy and preeclampsia workup. High BP is 140/90. Severely high BP is 160/110. Swelling occurs in many pregnant pts, but that should also alert you to start preeclampsia workup.
[Preeclampsia w/u from UpToDate:
Diagnostic evaluation
•Laboratory – Patients with suspected preeclampsia should have a complete blood count with platelets, creatinine level, liver chemistries, and determination of urinary protein excretion.
•Fetal status – Fetal status is assessed concurrently or postdiagnosis, depending on the degree of concern during maternal evaluation. At a minimum, a nonstress test or biophysical profile is performed if appropriate for gestational age. Ultrasound is used to evaluate amniotic fluid volume and estimate fetal weight, given the increased risk for oligohydramnios and growth restriction.
•Consultation with the neurology service is generally indicated in patients with neurologic deficits/abnormal neurologic examination, which may include ocular symptoms or a severe persistent headache that does not respond to initial routine management of preeclampsia.]
An important thing to review is physiology of pregnancy. Blood volume increases during pregnancy, so there are lots of new RBCs and that will throw off a HgbA1c reading, therefore HgbA1c is not measured during pregnancy and will not be accurate! My attending today told me there was a midwife who offered pts either HgbA1c or oral glucose tolerance tests to screen for gestational DM. The HgbA1c is not accurate in pregnancy, so this should not be done. That would be bad to miss a diagnosis of gestational diabetes. You have to wait until 3 months postpartum to measure HgbA1c to get an accurate reading. Had a pt who did not have a PCP prior to getting pregnant, was on insulin during the pregnancy, and after giving birth, still needs to establish with PCP for diabetes f/u. After you give birth, you insulin needs drastically change, so you don't need as much as you did when you were pregnant. So I stopped her insulin and advised that she f/u with her new PCP for diabetes care.
I still need to review fetal heart tracings. The attending today said the first thing to look at is the baseline (the baseline HR should be about 160 beats/min), then the variability, then look for accelerations and decelerations. If more than 32 weeks GA, accelerations are 15 beats/min above the baseline lasting at least 15 seconds. Early decelerations are representative of compression of the fetal head, which is normal during labor as baby moves down the pelvis/birth canal. Variable decelerations look sharper like a "V" and can represent compression of the umbilical cord. Late decelerations represent placental insufficiency.
ACOG has very helpful practice bulletins.
I can't take screen shots on my work laptop, so I'm just going to summarize gestational HTN w/u from UpToDate:
Gestational HTN: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions 4 hours apart after 20 weeks of gestation in a previously normotensive individual
And:
No proteinuria
No signs/symptoms of preeclampsia-related end-organ dysfunction (eg, thrombocytopenia, renal insufficiency, elevated liver transaminases, pulmonary edema, cerebral or visual symptoms)
Preeclampsia: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions at least 4 hours apart after 20 weeks of gestation in a previously normotensive individual. Patients with systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg should have blood pressure confirmed within a short interval (minutes) to facilitate timely administration of antihypertensive therapy.
And:
Proteinuria (≥300 mg per 24-hour urine collection [or this amount extrapolated from a timed collection], or protein:creatinine ratio ≥0.3, or urine dipstick reading ≥2+ [if other quantitative methods are not available]).
In a patient with new-onset hypertension without proteinuria, the diagnosis of preeclampsia can still be made if any features of severe disease are present.
Preeclampsia with severe features: In a patient with preeclampsia, presence of any of the following findings are features of severe disease:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg on 2 occasions at least 4 hours apart (unless antihypertensive therapy is initiated before this time)
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
Progressive renal insufficiency (serum creatinine concentration >1.1 mg/dL [97 micromol/L] or doubling of the serum creatinine concentration in the absence of other renal disease)
Pulmonary edema
Persistent cerebral or visual disturbances
Eclampsia: A generalized seizure in a pt with preeclampsia that cannot be attributed to other causes.
HELLP syndrome: hemolysis, elevated liver enzymes, low platelets. Hypertension may be present (HELLP in such cases is often considered a variant of preeclampsia).
Chronic (pre-existing) hypertension: hypertension diagnosed or present before pregnancy or on at least 2 occasions before 20 weeks of gestation. Hypertension that is first diagnosed during pregnancy and persists for at least 12 weeks postpartum is also consider chronic hypertension.
Blood pressure criteria during pregnancy are:
Systolic ≥140 mmHg and/or diastolic ≥90 mmHg
Prepregnancy and 12 weeks postpartum blood pressure criteria are:
Stage 1 – Systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg
Stage 2 – Systolic ≥140 mmHg or diastolic ≥90 mmHg
Chronic HTN with superimposed preeclampsia*:
Any of these findings in a patient with chronic hypertension:
A sudden increase in blood pressure that was previously well-controlled or an escalation of antihypertensive therapy to control blood pressure
New onset of proteinuria or a sudden increase in proteinuria in a patient with known proteinuria before or early in pregnancy
Significant new end-organ dysfunction consistent with preeclampsia after 20 weeks of gestation or postpartum
*Precise diagnosis is often challenging. High clinical suspicion is warranted given the increase in maternal and fetal-neonatal risks associated with superimposed preeclampsia.
Chronic hypertension with superimposed preeclampsia with severe features:
Any of these findings in a patient with chronic hypertension and superimposed preeclampsia:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg despite escalation of antihypertensive therapy
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
New-onset or worsening renal insufficiency
Pulmonary edema
Persistent cerebral or visual disturbances
A reduction in blood pressure early in pregnancy is a normal physiologic occurrence. For this reason, women with chronic hypertension may be normotensive at their first few prenatal visits. Later in pregnancy, when their blood pressure returns to its prepregnancy baseline, they may appear to be developing preeclampsia or gestational hypertension if there are no documented prepregnancy blood pressure measurements.
BP: blood pressure.
* Blood pressure should be elevated on at least two occasions at least four hours apart. However, if systolic pressure is ≥160 mmHg or diastolic pressure is ≥110 mmHg, confirmation after a short interval, even within a few minutes, is acceptable to facilitate timely initiation of antihypertensive therapy.
¶ The onset of preeclampsia and gestational hypertension is almost always after 20 weeks of gestation. Preeclampsia before 20 weeks of gestation may be associated with a complete or partial molar pregnancy or fetal hydrops. Postpartum preeclampsia usually presents within two days of delivery. The term "delayed postpartum preeclampsia" is used for signs and symptoms of the disease leading to readmission more than two days but less than six weeks after delivery.
Δ Significant proteinuria is defined as ≥0.3 g in a 24-hour urine specimen or protein/creatinine ratio ≥0.3 (mg/mg) (34 mg/mmol) in a random urine specimen or dipstick ≥1+ if a quantitative measurement is unavailable.
◊ Almost all women with the new onset of hypertension and proteinuria at this gestational age or postpartum have preeclampsia, but a rare patient may have occult renal disease exacerbated by the physiologic changes of pregnancy. An active urine sediment (red and white cells and/or cellular casts) is consistent with a proliferative glomerular disorder but not a feature of preeclampsia. Women with chronic hypertension who had proteinuria prior to or in early pregnancy may develop superimposed preeclampsia. This can be difficult to diagnose definitively, but should be suspected when blood pressure increases significantly (especially acutely) in the last half of pregnancy/postpartum or signs/symptoms associated with the severe end of the disease spectrum develop.
§ Photopsia (flashes of light), scotomata (dark areas or gaps in the visual field), blurred vision, or temporary blindness (rare); severe headache (ie, incapacitating, "the worst headache I've ever had") or headache that persists and progresses despite analgesic therapy; altered mental status. Seizure occurrence upgrades the diagnosis to eclampsia.¥ The differential diagnosis of preeclampsia with severe features includes but is not limited to:
Antiphospholipid syndrome
Acute fatty liver of pregnancy
Thrombotic thrombocytopenic purpura (TTP)
Hemolytic uremic syndrome (HUS)
The laboratory findings in these disorders overlap with those in preeclampsia with severe features. (Refer to table in the UpToDate topic on the clinical manifestations and diagnosis of preeclampsia.) The prepregnancy history, magnitude and spectrum of laboratory abnormalities, and additional presence of signs and symptoms not typically associated with preeclampsia help in making the correct diagnosis, which is not always possible during pregnancy.
In addition, a variety of medical disorders may be associated with hypertension and one or more of the signs and symptoms that occur in women with preeclampsia with severe features. These patients can usually be distinguished from patients with preeclampsia by taking a detailed history, performing a thorough physical examination, and obtaining relevant laboratory studies.‡ In contrast to preeclampsia, gestational hypertension is not associated with end-organ involvement, so neither proteinuria nor the symptoms or laboratory findings of preeclampsia are present.
#OB#OBGYN#birth control#gestational HTN#preeclampsia#eclampsia#breastfeeding#gestational diabetes#fetal heart tracing#FHT
3 notes
·
View notes
Text
shoehorning my interest into practically anything i say or do because why not
#not to people irl#i mwan like i dont interact w anyone fht much but whatveer#talking to myself and saying out loud “hollyyyy shitttt ___ reference?#diary of a dumbass#i WILL find a way to make everything i do connect back to re
3 notes
·
View notes
Text
im just worrrriiiiieeeeerddddddddddddddddddddddd ill never matter to anyone which is stupid because i know i do. but why dont i have any friends at school................... why dont i have any friends i can sgand next to
3 notes
·
View notes
Text
So weird theory but
Is it possible that Blue is in a coma? Or was at one point? And is still in the hospital because of it?
More than once the friends talk about him in the present tense (or at least they do in the subtitles) but the way they talk about him, the words and tone they use, makes it sound like he’s dead.
So coma? Or near-permanent hospitalization?
#for him#for him the series#blue fhts#a bit out there but yeah#maybe?#imma have to rewatch the episodes and pay more attention to how they talk about him to know for sure#but this came to me#i did not expect to have thoughts about this show#after ep1 i was sure it would be my weekly thirst trap show#and yet here i am#cap watches for him#cap speaks
4 notes
·
View notes
Video
youtube
Spinal & Peripheral Joint Manipulation Course 2024
#youtube#backpain manipulation jointpain chiropractor chiropractictreatment backpain spinalmanipulation fht arthritis cpd imm physicaltherapy manual#backpain manipulation jointpain cpd omt omm pyhsicaltherapy maualtherapy
0 notes
Text
Reading this old diary like it’s a manga cuz this is so wild so many twists and turns with the hindsight I have now. Got me on the edge of my seat.
0 notes

Note
WHGHAGSCHSD AWW THANK U MAN

*may i also get a kiss from killz?
YOU MAY, SAEJUN <333

#sid replies#sid rb#it was mostly the colorz#<- its bc i use a colour palette im gonna cry im gonna kill im gonna maim#anyway though ->#and how soft n calmin it was#guyz sid'z art is my therapy#i WILL recognize my therapy art..#what if i HWAI FHT#WHAT IF I DIEE HUH (POS AFF)#IM GONNAJSNDISC#squishing my face and grinning like an idiot omgg#flutters my eyes at u u silly goober
93 notes
·
View notes
Text
Transgender Feminization Steps
Step 1: Mental Health Evaluation and Diagnosis
Consult a mental health professional, such as a psychologist or psychiatrist, who has experience in gender identity issues.
Discuss your gender identity and expression, and receive a diagnosis of gender dysphoria or gender incongruence according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) or the International Classification of Diseases (ICD-11).
Ensure any underlying mental health conditions, such as depression, anxiety, or eating disorders, are well-managed.
Step 2: Hormone Therapy
Begin feminizing hormone therapy (FHT) under the guidance of a healthcare provider experienced in transgender care.
FHT typically involves the use of estrogen (estradiol) and anti-androgens (such as spironolactone) to reduce masculine characteristics and promote female characteristics.
Monitor hormone levels through regular blood tests to ensure they are within a healthy range.
Step 3: Physical Changes
Allow 18-24 months for full physical effects of hormone therapy to manifest.
Expect changes in secondary sex characteristics, such as:
Increased body fat storage in hips, buttocks, and face
Softer skin and reduced facial hair
Breast development
Changes in muscle and body fat distribution
Step 4: Body Feminization Surgery (Optional)
Consider body feminization surgery, such as trunk liposuction and buttocks augmentation, to achieve a more feminine physique.
Choose a surgeon with specialized knowledge and experience in transgender care.
Step 5: Ongoing Care and Monitoring
Schedule regular follow-up appointments with your healthcare provider to monitor hormone levels, physical changes, and overall health.
Address any side effects or complications promptly, and adjust hormone therapy or surgical plans as needed.
Additional Considerations
Social transition: Update your name and pronouns, and adjust your public gender expression.
Voice feminization: Consider voice therapy or surgery to achieve a more feminine voice.
Hair removal: Explore hair removal options, such as electrolysis or laser hair removal, to achieve a smoother, more feminine appearance.
Important Notes
Permanent feminization is a gradual process that requires patience, commitment, and ongoing care.
It is essential to work with healthcare providers experienced in transgender care to ensure safe and effective treatment.
Individual results may vary, and it is crucial to have realistic expectations about the outcomes of hormone therapy and surgery.

19 notes
·
View notes
Note
I dnt know why but, I feel like yujii has very subtle face tattoos and it's the ones beneath his eyes (like where curse Sukuna's eyes supposed to be). He shrugs it off as scars until he confesses to his brother fht he got a tattoo years ago because he looked up to him so much
Oh thats a great hc! Funny thing is, i made sukuna got a face tattoo because of a truth or dare game (he got dared to get a face tattoo while drunk), and yuuji was bewildered like r u for real rn that looks stupid
But yeah, i can see yuuji changed his mind later and got himself one, not too much tho
37 notes
·
View notes
Text

MY GIRL MY SPECIAL GIRL HAS RETURNED TO ME AFTER ALL THIS TIME YES YES YES YES YES YES YES YES YES YES YES YES MY DARLING GIRL YESSSS!!!!! SHAHRA!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! AHHHH!HJKH!GHJ!JH!GJHK!LK:!KLJG!JHG!JHGF!H!FH!!!!HGF!HGFH!!UIKYYU!FHT!FV!HGF!!!!HGF!HF!!UYJ!YHY!FHJ!!JUK!JHG!YG!!!!OOOOHHHHHHHHHH MY GOD SHES S O CUTE LOOK AT HER AND HER TALL HAIR,,,,,,, MY GIRL,,,,,,,,,,,,,,,,,,,,, AHHHHHH
9 notes
·
View notes
Text

FHT Prediction prize 1/3
Lady Amalthea from The Last Unicorn
22 notes
·
View notes
Text
Every time I see people talking about @fandomtrumpshate my mind swaps those last two words. I mean, FHT too but that's not actually what's being said, is it?
FTH Calendar FTH 2025 Groups to Donate to
Can't wait to donate to some of the groups they selected. I've not decided if I'll join the auction or just donate to some of the groups, but either way I'm looking forward to seeing all the fanworks that come out of it.
6 notes
·
View notes
Text
how long do you think it would take dean to notice that sam started FHT
3 notes
·
View notes
Text
hearing theres a new pop song out now about thijnking all your friends are secretly mad at you when they just got their own problems going on MOVE OUT FHT HE WAY its my time baby
5 notes
·
View notes