#Consultant Reproductive Medicine
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com rank in the US is 25.
Text
#Best Infertility Hospitals in Shivamogga#Best fertility Hospitals in Shivamogga#Dr. Kavya V Pradeep#Consultant Reproductive Medicine#Gynaecologist & Laparoscopic Surgeon Shomogga#Fertility Dotors in Shivamogga#Fertility hospital in Shivamogga#Infertility hospital in Shivamogga#Best IVF Center In Shivamogga#Infertility Treatment Centre Shivamogga#Fertility Centre Shivamogga#Best Fertility Clinics Shivamogga#IVF Centres in Shimoga#Best IVF Treatment in Shimoga#IVF Cost in Shivamogga#Infertility Treatment In Shimoga#fertility specialist in Shimoga#Infertility Treatment in Shimoga#fertility clinic Shimoga#Best Fertility Specialist Near Me#Fertility Doctors in Shimoga#Infertility Doctors in Shimoga#fertility clinic
0 notes
Text
guys hear me out imagine house md veterinary hospital au in which:
house got kicked by a cow during his internship and his leg didn’t heal properly which made him use a cane
he was forced to switch to small animal practice, he still hates clients but his fluffy patients love him for some unknown reason
wilson specialises in equine medicine (wilson is basically a horse girl) and because their hospital doesn’t get much calls for horse consults he spends most of his time being annoyed by house
instead of being exposed to hiv cameron gets bit by a rabid 16 year old yorkshire terrier
a lady comes with an obese labrador and chase nearly gets rabid himself
the ducklings are responsible for restraining first and treating patients second
foreman is afraid of small dogs
chase makes fun of him but he’s terrified as well
cameron has four senior sick rescue cats which seem to be immortal
house is addicted to ketamine instead of vicodin
there’s at least one joke about chase’s interest in bdsm and getting bit
wilson always gets a new golden retriever when entering a new marriage, the dogs always stay with his ex-wives
house constantly remarks that he should change his motorcycle for a horse to wilson’s horror
stevie mcqueen was actually brought to the hospital by a rescue for lab animals, house adopted stevie after his treatment was finished
cuddy specialises in animal reproduction and house constantly tries to win the argument by bringing puppies to her office (she folds on occasion)
house nearly does a necropsy on a goat with anthrax
#house md#gregory house#james wilson#lisa cuddy#eric foreman#allison cameron#robert chase#the ducklings#and of course hilson is included in this au#hilson#i’m currently on season 3 so sorry for not including other characters
373 notes
·
View notes
Text
The Importance of Veterinary Imaging in Modern Animal Healthcare

Understanding Veterinary Imaging
Veterinary imaging encompasses various diagnostic techniques that help veterinarians visualize internal structures of animals without invasive procedures. These imaging techniques include:
Veterinary MRI Services: Ideal for diagnosing neurological disorders, musculoskeletal injuries, and soft tissue conditions.
Veterinary CT Scan Services: Used for detailed cross-sectional imaging of bones, lungs, and complex anatomical structures.
Veterinary Ultrasound: Essential for evaluating soft tissues, abdominal organs, and reproductive health in animals.
Veterinary Radiology Service: Traditional X-rays remain a fundamental tool for detecting fractures, tumors, and internal anomalies.
With the increasing need for precision in veterinary diagnostics, finding a veterinary radiologist near me is becoming a priority for pet owners and veterinary professionals alike.
Why Choose a Veterinary Radiologist?

Benefits of Consulting a Veterinary Radiologist:
Accurate Diagnoses: Specialized training ensures precise interpretation of imaging results.
Advanced Imaging Techniques: Access to cutting-edge imaging technologies for comprehensive evaluations.
Collaborative Approach: Works closely with veterinarians to develop effective treatment plans.
Minimally Invasive Diagnostics: Reduces the need for exploratory surgeries, ensuring animal comfort.
Veterinary MRI: A Game Changer in Animal Healthcare
MRI (Magnetic Resonance Imaging) has revolutionized veterinary imaging by offering high-resolution images of soft tissues, the brain, and the spinal cord. Veterinary MRI services are particularly beneficial for diagnosing conditions such as:
Brain tumors and neurological disorders
Spinal injuries and disc herniations
Joint and ligament injuries
Soft tissue abnormalities
The Role of Veterinary CT Scan Services
Veterinary CT scan services provide detailed three-dimensional imaging, making them invaluable for assessing complex conditions. This imaging technique is commonly used for:
Diagnosing fractures and bone disorders
Evaluating lung diseases and chest abnormalities
Detecting internal tumors and metastases
Planning for complex surgical procedures
For pet owners and veterinarians looking for high-quality diagnostic imaging, veterinary CT scan services are an essential tool in modern veterinary medicine.
The Significance of Veterinary Ultrasound
Veterinary ultrasound is a non-invasive and painless diagnostic tool that helps in real-time visualization of internal organs. It is widely used for:
Monitoring pregnancy and reproductive health
Examining abdominal organs such as the liver, kidneys, and intestines
Detecting fluid accumulation or cysts
Guiding biopsies for accurate sampling
Finding the Right Veterinary Radiology Service
When searching for a vet radiology service, it’s essential to consider factors such as:
Expertise of the Radiologist: Ensure they are board-certified and experienced in interpreting animal imaging.
Turnaround Time: Quick and efficient reporting is crucial for timely treatment.
Availability of Advanced Technology: Clinics with state-of-the-art equipment provide more accurate diagnostics.
Collaboration with Veterinary Clinics: A reliable veterinary radiology service should work closely with general veterinarians to ensure seamless patient care.
Conclusion
Advancements in veterinary imaging have transformed the way veterinarians diagnose and treat animal diseases. Whether you need veterinary MRI services, veterinary CT scan services, or veterinary ultrasound, choosing a qualified veterinary radiologist near me ensures accurate and efficient diagnoses for your pet. With the growing demand for specialized diagnostic services, finding a trusted vet radiology service can make all the difference in ensuring the best possible healthcare for animals.
FAQ
1. What is the difference between veterinary MRI and veterinary CT scan services?
Answer:- Veterinary MRI services are best for imaging soft tissues, the brain, and the spinal cord, making them ideal for neurological and musculoskeletal conditions. Veterinary CT scan services, on the other hand, provide detailed cross-sectional images of bones, lungs, and complex anatomical structures, making them useful for diagnosing fractures, tumors, and lung diseases.
2. How do I find the best veterinary radiologist near me?
Answer:- To find the best veterinary radiologist near me, look for board-certified specialists with experience in interpreting various imaging modalities. Ensure they use advanced technology and provide quick, accurate reports. Collaborating with a reputable vet radiology service can also help ensure high-quality diagnostics.
4 notes
·
View notes
Text
Equine Veterinarian Videography Pro Tips

Dodge embarrassing and irrelevant footage in your equine veterinarian highlight reel. Knowing how a horse veterinarian works to keep them healthy and thriving will help you capture the most compelling vet and horse interaction for a stunning highlight reel.

surroundedmedia.com gathered essential information about what equine veterinarians do, how they diagnose and treat horses, the best interactive moments to capture, and what makes a compelling highlight reel.
What Does an Equine Veterinarian Do?

Equine veterinarians provide essential horse care, ensuring their health, performance, and overall well-being. Capturing their work on video educates viewers and highlights the dedication and skill required in equine medicine. Equine veterinarians perform multiple tasks to keep horses healthy and sound. Here are 15 primary responsibilities:
Conduct comprehensive health examinations
Diagnose lameness and musculoskeletal issues
Administer vaccinations and parasite control treatments
Perform dental care and corrective procedures
Provide reproductive services, including artificial insemination
Carry out emergency care for injuries and illnesses
Prescribe medications and develop treatment plans
Manage colic cases with surgical or non-surgical interventions
Monitor and treat respiratory conditions
Advise on nutrition and weight management
Collaborate with trainers and owners on performance issues
Perform diagnostic imaging such as X-rays and ultrasounds
Implement preventative health programs
Educate owners about proper care and management
Oversee rehabilitation following surgery or injury
Each task requires precision, compassion, and extensive equine anatomy and behavior knowledge.
Diagnosing and Treating Horses

Equine veterinarians utilize traditional clinical methods and advanced diagnostic tools to evaluate a horse's health. A typical diagnosis process includes:
History Taking - Gathering information from owners about a horse’s behavior, diet, exercise routines, and recent changes.
Physical Examination - Assessing vital signs, inspecting limbs, eyes, and respiratory function, and palpating the body to locate pain or abnormalities.
Diagnostic Imaging - Using X-rays, ultrasounds, or endoscopy to view internal structures.
Laboratory Testing - Analyzing blood, urine, or tissue samples to detect infections, metabolic imbalances, or other conditions.

Treatment plans depend on the diagnosis. They might include administering medications, recommending rest or modified exercise, performing surgeries, or suggesting nutritional adjustments. Preventative care, such as vaccination schedules and routine check-ups, is crucial in maintaining a horse's health.
How Often Should Horses Be Visited by a Veterinarian?
Regular veterinary visits are crucial to ensure early detection of potential issues. Ideally, horses should have a comprehensive health check at least once annually. However, more frequent visits might be necessary for performance horses, older animals, or those with chronic conditions. Seasonal check-ups, particularly before and after intense training periods or competition seasons, can help maintain optimal health and performance.
Best Equine Veterinarian Moments to Capture on Video

When creating a highlight reel for equine veterinary work, focus on moments demonstrating skill, compassion, and the human-animal bond. Consider capturing:
Examinations and Diagnostics: Footage of veterinarians performing thorough check-ups, taking X-rays, or conducting ultrasounds.
Emergency Interventions: Dramatic, yet controlled, moments when rapid response saves a horse’s life during a colic crisis or severe injury.
Treatment Procedures: Close-ups of delicate procedures, such as dental work or wound care, highlighting precision and care.
Owner Consultations: Interactions where veterinarians explain diagnoses and treatment options, showcasing empathy and professionalism.
Rehabilitation Sessions: Document progress during recovery, emphasizing improvements and the positive impact of veterinary care.

These interactions educate the public and build trust between veterinarians and the community.
Components of a Compelling Highlight Reel
A high-quality highlight reel should weave together informative and engaging content. Here are key elements to include:
Clear Narration: Use voiceover or on-screen text to explain procedures, diagnoses, and the importance of preventive care. Dynamic Visuals: Combine wide shots of clinical settings with close-ups of detailed procedures, ensuring a balanced visual narrative. Emotional Connection: Capture moments that reveal genuine care, such as gentle interactions with horses or reassuring gestures toward worried owners. Before-and-After Comparisons: Show improvements in a horse’s condition post-treatment to illustrate the effectiveness of veterinary care. Professional Editing: Employ smooth transitions, appropriate background music, and clear labeling of procedures to keep viewers engaged and informed.
Watch this video to see a professionally made equine veterinarian video.
youtube
Preventive Measures in Equine Health

Prevention is a cornerstone of equine veterinary care. Regular check-ups, proper nutrition, and a tailored exercise regimen help maintain a horse's health and prevent many severe conditions. Veterinarians also educate owners on the following:
Maintaining a clean, safe environment
Implementing routine vaccination and parasite control schedules
Monitoring for early signs of lameness or discomfort
Providing appropriate rest periods after strenuous activities
This proactive approach reduces emergency visits and ensures horses perform at their best.
Videography Pro Tips for Equine Veterinarians
In this article, you discovered crucial information about what equine veterinarians do, how they diagnose and treat horses, the best moments to capture, and what makes a compelling highlight reel.
Equine veterinarians are vital to a horse’s health and success, performing responsibilities ranging from routine care to emergency interventions. Capturing their work on video educates audiences and celebrates the artistry and expertise behind equine medicine.
Ignoring the need to educate yourself on equine veterinarian activities and practices will leave you missing out on exceptional footage, resulting in poorly constructed highlight reels or promotional videos.
Sources: pmc.ncbi.nlm.nih.gov/articles/PMC3898908 aaep.org
Surrounded Media LLC
177 Fairway Drive Newnan, GA30265 (770) 727-1577
To see the original version of this article, visit https://www.surroundedmedia.com/blog/equine-veterinarian-videography-pro-tips
#videography#drone videography#drone videography atlanta#professional videography atlanta#cinematic storytelling atlanta#Equine Veterinarian#Horse Vet#Veterinarian Videography#Youtube
2 notes
·
View notes
Text

IVF Specialist in Wakad - Orion Hospital: Your Trusted Fertility Partner
Are you looking for an experienced and reliable IVF specialist in Wakad? Infertility can be a challenging journey, but with the right medical expertise, your dream of parenthood can become a reality. Orion Hospital, a leading healthcare facility in Wakad, offers world-class fertility treatments with advanced technology and experienced specialists.
Why Choose an IVF Specialist in Wakad at Orion Hospital?
Wakad has become a preferred destination for couples seeking fertility treatments due to its well-equipped clinics, modern medical facilities, and experienced reproductive specialists. Orion Hospital stands out as a premier choice for fertility treatment due to the following reasons:
Expertise & Experience: The IVF specialists at Orion Hospital have years of experience in treating infertility cases with a high success rate.
Advanced Technology: The fertility department at Orion Hospital is equipped with state-of-the-art technology, ensuring the best possible treatment options.
Personalized Treatment Plans: Each patient receives customized fertility solutions based on their medical history and needs.
Affordable Treatment Options: Compared to other metro cities, IVF treatments at Orion Hospital in Wakad are cost-effective without compromising quality.
Services Offered by IVF Specialists in Wakad at Orion Hospital
The IVF specialists in Wakad at Orion Hospital offer a wide range of services to address different infertility issues, including:
In Vitro Fertilization (IVF)
Intrauterine Insemination (IUI)
Intracytoplasmic Sperm Injection (ICSI)
Egg Freezing & Embryo Preservation
Male & Female Infertility Treatments
Counseling & Support Services
How to Choose the Best IVF Specialist in Wakad?
Selecting the right fertility specialist is crucial for a successful treatment. Here are some key factors to consider:
Experience & Qualifications: Look for a specialist with extensive experience and relevant certifications in reproductive medicine.
Clinic Success Rates: Check the success rates of the clinic for IVF and other fertility treatments.
Patient Reviews & Testimonials: Reading patient feedback can help you understand the quality of care provided.
Facilities & Technology: Ensure that the clinic has the latest reproductive technology for better treatment outcomes.
Approach & Communication: A compassionate and transparent approach by the specialist can make the journey smoother.
Conclusion
If you are struggling with infertility and seeking an IVF specialist in Wakad, Orion Hospital offers top-notch fertility care with experienced doctors and cutting-edge technology. With advanced treatments, affordable pricing, and personalized care, you can take the first step towards fulfilling your dream of parenthood. Book a consultation with a trusted fertility expert at Orion Hospital today and embark on your journey to parenthood with confidence.
For the best IVF specialist in Wakad, consult Orion Hospital and take the first step towards a joyful future!
4 notes
·
View notes
Text
2023 Reading Log pt 16
The last books I read in 2023, and the least books I've read in a year since starting to keep track. But 80 books is still nothing to sneeze at.
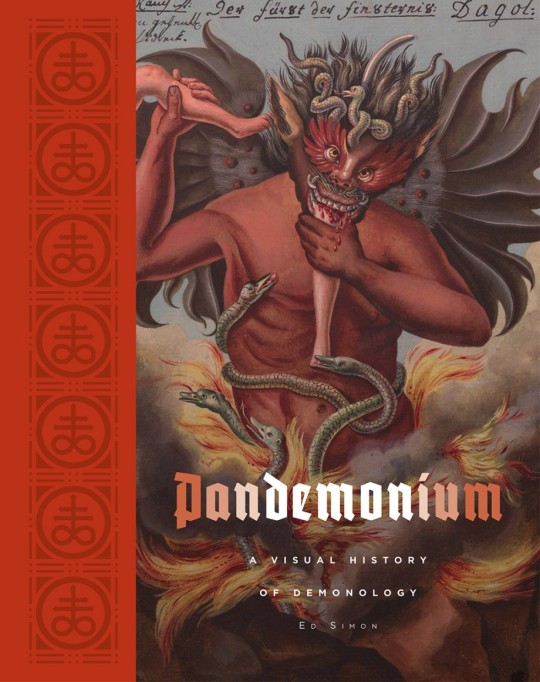
76. Pandemonium: A Visual History of Demonology by Ed Simon. This book rules; it’s up there for best books I’ve read in 2023. As the title suggests, the book is primarily concerned with high quality reproductions of art of demons and hell in the Western tradition, organized by era, with accompanying essays discussing the role played by demons in culture and what they symbolize in literature, religion and art. These build to a crescendo, as the last essays are about the modern era as an Age of Moloch, where destructive, unrelenting consumption is the rule of the elite, which articulates feelings that I have had as a demon-obsessed ex-Christian for some time. It also talks about the Cthulhu Mythos as a post-modern demonology, which probably pisses ST Joshi off something fierce, so I give it props for that as well.
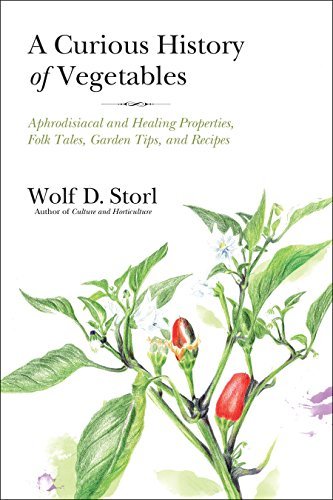
76a. A Curious History of Vegetables by Wolf D. Storl. “Curious” is an excellent word to describe this book, as its author is a nut. We’re talking, “consults astrological charts for planting certain vegetables” nut. Although the cover calls him an “ethnobotanist”, Storl is clearly a crank of the highest order—the introduction includes ranting about how vegetables are full of deva spirits, but GMOs are possessed by rakshasas. I was willing to read along for quite a while with this as a book about the magical properties and beliefs about plants—I got about halfway. But by that point, the author’s continual paranoia about using drugs as medicine, claiming that every vegetable is a panacea, and obvious disdain for scientific curiosity or little things like “evidence” got to be too much for me. That’s not me elevating him into a strawman, BTW. He goes into a lengthy rant about “The Shoemaker and the Elves”, talking about how scientists destroy magic with their curiosity and thus ruin the world. Blech.
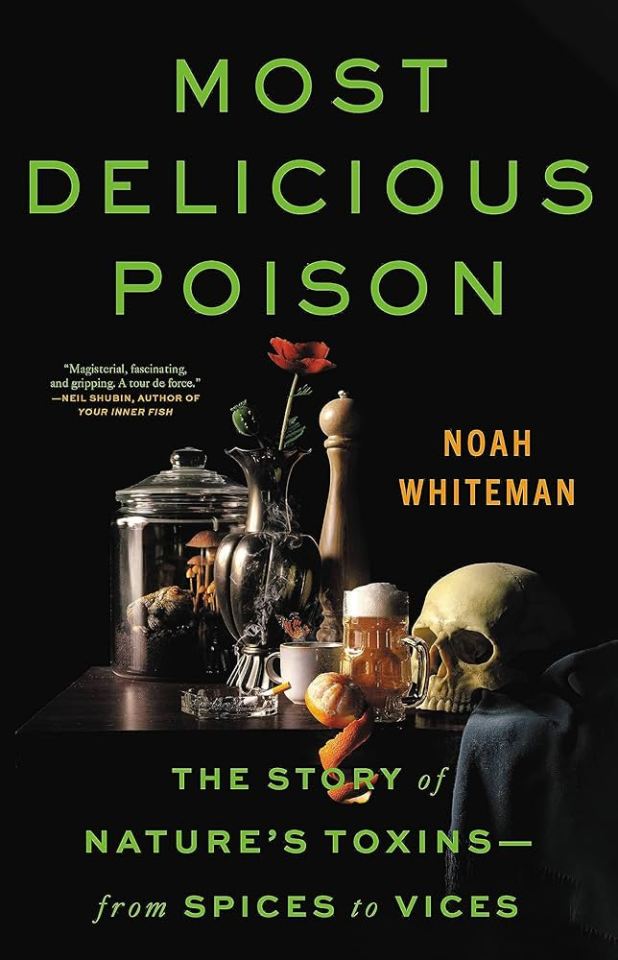
77. Most Delicious Poison by Noah Whiteman. I’m a sucker for books about poison, and this is a good one. I think I’d still recommend Plants that Kill above this, but this is an excellent follow-up for the reader. This book talks a lot more about the modes of action of particular chemicals, and how chemicals fall into families of molecules that often have related properties. The book is one of those part science/part memoir nonfiction books that seem to have grown in popularity. The author was inspired to write it in part by his father’s death from alcoholism. So definitely go into it with a trigger warning in mind.
77a. Sex in the World of Myth by David Leeming. Abandoned after the Greece/Rome chapter. I abandoned it partially because it lumped Greece and Rome together and talked about their views on sex and sexuality as if they were interchangeable and consistent through the thousands of years of their existences, partially because the author is a Freudian. Life is too short to read books by Freudians. The specific line that made me give up was when the author defined all pornography as violent and exploitative. Blanket statement.
78. Household Horror by Marc Olivier. This is a weird one, even by the standards of “scholarly analyses of horror movies”, in that it looks at the horror movies it covers from the perspective of inanimate objects within them. Sometimes literally—the author discusses The Exorcist through the lens of Regan’s bed being possessed before she is—and sometimes figuratively—what does the exact make and model of the typewriter, and the reams and reams of hand typed text, say about The Shining? It’s witty and engaging, and an interesting way to view and review movies that, for the most part, have received a lot of critical attention already.
79. Quackery: A Brief History of the Worst Ways to Cure Everything by Lydia Kang and Nate Pedersen. This is a re-read; I bought this book shortly after it was released in 2017 and read it then. But, the podcast Behind the Bastards did an episode on radium quackery that used it as a source, and I was still stinging from having started and abandoned two crappy books in as many weeks, so I wanted something of a comfort read. Of course, my version of a “comfort read” involves gross medical malpractice and people poisoning themselves and others. I’m strange. The book is organized into chapters by subject (elements, animal products, vegetable poisons, etc), and is very well illustrated with vintage advertisements, engravings and photographs. There are more in-depth books about just about all of the topics covered here, but this is an excellent survey of the more shameful corners of medical history.
80. Words from Hell by Jess Zafarris. It’s a book on etymology! Namely, the etymology of profanity, slurs, sex, violence, drugs, crime, monsters… It’s a bit of a mixed bag in terms of theme, but is organized well within. A recurring topic is the hidden biases built into the English language, from “sinister” meaning “left-handed” to the classism built into words like “rascal” and “villain”. The author is good about discussing multiple hypotheses for word origins, and about when things are uncertain and unknown. And she’s a sex-positive WLW, which goes a long way towards giving me good feelings towards any book (an example joke: when discussing the shared root word of “vagina” and “vanilla”, she quips “no wonder they’re both so fun to lick”).
17 notes
·
View notes
Text
Woman's reproductive rights uk
Below the line for those who are uncomfortable
When I was pregnant my consultant was an abortion specialist and she got very nervous finding out my husband was a a journalist because she'd been secretly recorded once by a woman pretending to want an abortion.
To see if she was following the law.
Which she was because the law in the UK is pretty simple.
The law in the UK is that women can only have abortions for health reasons.
Yet, it's an extremely rare circumstance for a woman to be turned down for an abortion - they have to literally state 'I didn't want a girl' or similar as sex based abortions are illigal.
Now, the reason it's rare is because health reasons in the UK law includes mental health of the mother and there is an understanding a woman who ends up having to go through pregnancy and birth when she is not prepared and does not want to is going to cause her anxiety and depression and this is enough of a health reason to qualify for an abortion, or be past the 24 weeks pregnant mark which with free healthcare and walk in clinics in the UK there are plenty of opportunities to determine - I don't think I've been to a dr's without having to take a pregnancy test in the last year.
When put on the news and asked if she thought she'd asked enough questions to determine if a woman had the right to an abortion under these laws my consultant said (not verbatim because my memory is not that good) 'Abortions are not an easy thing for the mind or body to deal with and I trust that every woman who comes to me has already thought about their situation and made their decision and has not woken up one morning and come into my clinic on a whim. They know their situation better than I do , so they are the best to judge."
That consultant later saved my life from a post-birth complication so I'm glad she was not hounded out of medicine - as she said, she respects women's choices but more than that she had a skill that can save lives.
2 notes
·
View notes
Text
I still haven’t moved on from finding out today that there is a tiktok trend of people INGESTING BORAX.

I ended up going down this rabbit hole to find out where people are getting this information and immediately found this:
https://www.lybrate.com/topic/borax-benefits-and-side-effects


These are real doctors from India with masters who work in the states and such, I did a brief bg check on them. What the fuck? This is the only thing I could find that states borax has “health benefits”. But wait... in the fine print at the bottom:

I kept digging for more and found this article by the Jerusalem Post stating the possible origin of this trend. Dr. Rex E. Newnham has been cited by many tiktokers for having written several papers claiming that borax had health benefits but the research showing results is difficult to find. From these papers, a conspiracy has spawned and now people have become convinced Newnham was onto something and was blocked by big pharma so they could continue making billions.
Now here’s some information you mostly will find online when researching borax:


FUN FACT: Borax is actually banned in several countries because it has been suggested that it can cause cancer and multi-organ accumulation of poisoning. Kids have actually died playing with slime activated by borax. (src)

Studies conducted by NLM (National Library of Medicine) on people who consumed borax show “immune cell proliferation and sister chromatid exchange in human chromosomes”.. In other words: “Toxicity of borax may lead to cellular toxicity and genetic defect in human.” (src)
Here’s what I now know based on most research that can be pulled of borax:
-it is not boric acid, it is also NOT boron. boron is only one component of borax. -classified as a mild skin irritant and can even cause chemical burn -banned by FDA as a food additive. -can be used as a component in pesticides, flame retardant, enamel glazes, glass, ceramics, laundry detergent etc. -has potential to disrupt the reproductive system shown in studies of mice and hemorrhagic gastroenteritis in cattle. (src) -like anything else, bad for you in large quantities or in long-term use but this is actually classified as poisonous and there are more studies that show this than anything opposing. -just because it’s natural doesn’t mean it’s safe for consumption
Folks, if you have joint pain, look into MSM supplements or powder for more potency which is an anti-inflammatory agent that the FDA has recognized as generally safe for consumption under 4000 mg/day with little to no known side effects. You should consult with your doctor before taking any supplements realistically but for the love of god, do not consume borax.
23 notes
·
View notes
Text
#Best Infertility Hospitals in Shivamogga#Best fertility Hospitals in Shivamogga#Dr. Kavya V Pradeep#Consultant Reproductive Medicine#Gynaecologist & Laparoscopic Surgeon Shomogga#Fertility Dotors in Shivamogga#Fertility hospital in Shivamogga#Infertility hospital in Shivamogga#Best IVF Center In Shivamogga#Infertility Treatment Centre Shivamogga#Fertility Centre Shivamogga#Best Fertility Clinics Shivamogga#IVF Centres in Shimoga#Best IVF Treatment in Shimoga#IVF Cost in Shivamogga#Infertility Treatment In Shimoga#fertility specialist in Shimoga#Infertility Treatment in Shimoga#fertility clinic Shimoga#Best Fertility Specialist Near Me#Fertility Doctors in Shimoga#Infertility Doctors in Shimoga#fertility clinic
0 notes
Text
Your Guide to IVF Treatment at Noida's Premier Hospital
Hello and welcome! I'm Dr. Sweta Gupta, and I'm thrilled to share with you the latest insights and information about IVF treatment at our esteemed hospital in Noida. Here at our facility, we are dedicated to providing compassionate care and cutting-edge technology to help couples achieve their dream of parenthood.
About Our Hospital
Located in the heart of Noida, our hospital is renowned for its state-of-the-art infrastructure and world-class facilities. We understand that undergoing fertility treatment can be a deeply personal journey, and our team is committed to supporting you every step of the way.
Meet Dr. Sweta Gupta
As the lead fertility specialist at our hospital, I bring years of experience and a passion for reproductive medicine. My team and I believe in a holistic approach to fertility care, combining advanced medical techniques with personalized attention to address each patient's unique needs.
Comprehensive IVF Services
Our hospital offers a comprehensive range of services to assist you on your fertility journey:
Initial Consultation: A thorough evaluation to understand your medical history and discuss personalized treatment options.
Diagnostic Testing: Advanced diagnostic tests to identify any underlying causes of infertility.
IVF Treatment: Tailored IVF protocols using the latest technology to optimize success rates.
Egg Freezing: Preservation options for women looking to preserve their fertility for the future.
Genetic Testing: Screening options to ensure the health and viability of embryos.
Why Choose Us?
Expertise: Our team comprises skilled fertility specialists, embryologists, and support staff dedicated to your care.
Patient-Centered Care: We prioritize open communication, empathy, and support throughout your treatment journey.
Success Rates: We are proud of our high success rates, which reflect our commitment to excellence in fertility care.
Patient Testimonials
Don't just take our word for it! Read testimonials from our patients who have successfully built their families with our help. Their stories are a testament to our dedication and expertise.
Get Started Today
If you're considering IVF treatment or have questions about your fertility options, we encourage you to schedule a consultation. Our team is here to provide you with the guidance and support you need to make informed decisions about your reproductive health.
Thank you for visiting our blog! Stay tuned for more articles on fertility tips, treatment updates, and patient stories. Remember, at our IVF hospital in Noida, your journey to parenthood is our priority.
For more Information:-
#dr sweta gupta#best ivf doctor in noida#ivf hospital in noida#best fertility doctor in noida#best ivf clinic in noida#best ivf hospital in noida#fertility doctor in noida#best ivf clinic#best ivf centre in noida
2 notes
·
View notes
Text
Miscarriages in Gaza Have Increased 300% Under Israeli Bombing
**And these deaths aren't included in the running count of Palestinians killed**
At Al-Emirati Hospital in Rafah, a woman identified by Doctors Without Borders as Maha sought a delivery room as she began going into labor, but was denied: “All the delivery rooms were full,” an emergency coordinator working with the humanitarian group recounted in a news release published Wednesday. Maha “knew something wasn’t right,” and that she needed care. But without other options, she returned to her tent. Her newborn son died as she gave birth to him in the bathroom near her tent. “Without this war, she would not have lost her son,” the emergency coordinator wrote.
Shortly after Israel’s bombardment of the Gaza Strip began in October, global health groups raised alarms that there was no longer anywhere safe for pregnant women to give birth. More than three months into the siege, conditions have only worsened, and pregnant and menstruating people are especially at risk. Health care workers report a 300% increase in the miscarriage rate among pregnant people in Gaza since Israel’s attacks began three months ago, Nour Beydoun, CARE’s regional advisor on protection and gender in emergencies, told Jezebel.
The lack of supplies due to Israel’s ongoing blockade has resulted in pregnant women struggling to carry healthy pregnancies; higher risk of infection and death after giving birth or having c-sections; increased infant mortality; and a range of other deadly sexual and reproductive health outcomes. Beydoun told Jezebel that CARE has heard about “significant weight loss” among pregnant women “due to the limited access to food, to proper nutrition,” resulting in “poor personal health and also in poor fetal and newborn health.”
Ammal Awadallah, executive director of the Palestinian Family Planning & Protection Association, told Jezebel that “all pregnant women are now at severe risk of delivering in unsafe conditions, being put in situations where they are giving birth in cars, tents, and shelters.” At health centers, pregnant women are only admitted “when fully dilated and are dismissed within a few hours after giving birth, due to the overcrowded facilities and extremely limited resources.” On top of all this, Beydoun said that many women must make the journey to hospitals or health centers—where they could still be turned away due to lack of capacity—on foot.
Due to limited resources, Awadallah says many c-sections and births “are being performed without basic medical supplies, or anesthesia and without any postnatal care.” Few are able to get or attend appointments with their doctors after giving birth, and many “have no option other than to stay in the overcrowded shelters.” As a result, a lot of “women are being dangerously exposed to infections,” the the risk of maternal mortality is high: “There’s now so much risk of hemorrhaging and infections without the right tools and medicines,” Beydoun said. And the many women forced to undergo emergency c-sections also face cesarean wound infections due to lack of clean medical tools for the procedure.
These conditions are similarly dangerous for newborns, who are “dying from a lack of sterile environment and specialized staff,” Beydoun said.
Of course, this is all assuming that pregnant women are able to be admitted into hospitals at all, where “priority is often not for women going into labor” and beds are rarely available for them, Awadallah said. The conditions at the Al-Emirati field hospital in Rafah demonstrate how overworked hospitals in Gaza have become: Beydoun said the hospital was “initially designed to receive 30 to 40 outpatient consultations from pregnant women on a daily basis—now they handle 300 to 400 cases daily.” The hospital has just one operating room and is “designed to have two to three c-section deliveries per day—now they’re delivering 20 daily.”
In October, it was estimated that at least 50,000 women in Gaza were pregnant. The International Planned Parenthood Federation reported at the time that more women were miscarrying or going into early labor from shock and stress under bombardment. And it’s not yet clear how many of those thousands of pregnant women in Gaza are among the estimated 24,000 Palestinians who have been killed in Israel’s attacks, or among the thousands who remain missing. In its charge of genocide against Israel at the International Court of Justice, South Africa alleges that “two mothers are estimated to be killed every hour in Gaza.” (The Israeli death toll from Hamas attacks on October 7 stands at 1,139. Hamas continues to hold roughly 200 people hostage.)
After months of Israeli bombardment, the health care system in Gaza is “completely collapsing,” Doctors Without Borders warned last month. A CNN investigation published on January 12 found at least 20 of 22 hospitals in northern Gaza had been damaged or destroyed in the first two months of Israel’s war on Gaza, and 14 were directly attacked by Israeli forces. The World Health Organization reported in December that no “functional” hospitals remained in northern Gaza, and only nine out of 36 hospitals in the south were even partially functioning to serve Gaza’s population of 2 million. On Tuesday evening, journalists in Gaza reported that Israeli forces had closed in on and were attacking Nasser Hospital.
Birth complications are just one threat people who menstruate are facing: As the independent Gaza-based journalist Bisan Owda highlighted earlier this month, period supplies are nearly impossible to find. According to Awadallah, few people “can find a pharmacy nearby,” let alone one that still stocks sanitary products. Many are forced to use strips of cloth that they can’t wash due to lack of water, plastic bags in lieu of pads, or, “if they’re lucky enough,” cut-up baby diapers. One hospital worker told Owda that “each day” she encounters “numerous instances of fever directly linked to vaginal yeast infections, arising from inadequate hygiene and the absence of feminine products.” Another told her that the “scarcity of basic products results in more hospital visits, longer hospital stays, and worsened conditions” from infection and disease. Severe water shortages and overcrowded public bathrooms further contribute to “the high number of reproductive and urinary tract infections,” Awadallah said.
On top of that, due to “the suffering, anxiety, and deteriorating psychological status of the women in the [Gaza] Strip,” Awadallah said a large proportion are now “getting their period a number of times during the month” instead of once.
This lack of water and malnutrition as a result of Israel’s blockade have been especially detrimental for nursing mothers: Women are struggling to breastfeed their babies as they aren’t able to produce milk “without having water to drink nor sufficient food to eat,” Awadallah said. In a letter provided by CARE, Alaa, a mother in Gaza, wrote that “no one is eating enough,” and “it is usually the mothers who eat last” in order to feed their children first. “I slept on an empty stomach every night so my children wouldn’t go hungry,” Alaa wrote. Back in October, Al-Aqsa Hospital told the Associated Press that many mothers in Gaza were forced to mix baby formula with contaminated water, “[contributing] to the rise in critical cases” in the hospital’s neonatal ward.
Barriers to basic health care and resources aren’t new for the women and girls of Gaza, Awadallah told Jezebel: “Palestinian women and girls were already living in a severely vulnerable environment, in an area which has been blockaded from essential basic health services and products for more than a decade.” But the crisis has become more dire than ever, and “without a full and immediate ceasefire, and the unimpeded delivery of humanitarian aid across all parts of Gaza, maternal and neonatal deaths will continue to rise.”
#israel is committing genocide#genocide#miscarriage#infant mortality#infection#humanitarian crisis#save palestine#israel is an apartheid state#free palestine 🇵🇸#gaza under attack#illegal occupation#israeli war crimes#ethnic cleansing#apartheid#collective punishment#collateral damage#spread awareness#stand with palestine#stand up for humanity#stolen lives#stolen futures#stolen land#doctors without borders#this was never about hamas
3 notes
·
View notes
Text
Miscarriages in Gaza Have Increased 300% Under Israeli Bombing
At Al-Emirati Hospital in Rafah, a woman identified by Doctors Without Borders as Maha sought a delivery room as she began going into labor, but was denied: “All the delivery rooms were full,” an emergency coordinator working with the humanitarian group recounted in a news release published Wednesday. Maha “knew something wasn’t right,” and that she needed care. But without other options, she returned to her tent. Her newborn son died as she gave birth to him in the bathroom near her tent. “Without this war, she would not have lost her son,” the emergency coordinator wrote.
Shortly after Israel’s bombardment of the Gaza Strip began in October, global health groups raised alarms that there was no longer anywhere safe for pregnant women to give birth. More than three months into the siege, conditions have only worsened, and pregnant and menstruating people are especially at risk. Health care workers report a 300% increase in the miscarriage rate among pregnant people in Gaza since Israel’s attacks began three months ago, Nour Beydoun, CARE’s regional advisor on protection and gender in emergencies, told Jezebel.
The lack of supplies due to Israel’s ongoing blockade has resulted in pregnant women struggling to carry healthy pregnancies; higher risk of infection and death after giving birth or having c-sections; increased infant mortality; and a range of other deadly sexual and reproductive health outcomes. Beydoun told Jezebel that CARE has heard about “significant weight loss” among pregnant women “due to the limited access to food, to proper nutrition,” resulting in “poor personal health and also in poor fetal and newborn health.”
Ammal Awadallah, executive director of the Palestinian Family Planning & Protection Association, told Jezebel that “all pregnant women are now at severe risk of delivering in unsafe conditions, being put in situations where they are giving birth in cars, tents, and shelters.” At health centers, pregnant women are only admitted “when fully dilated and are dismissed within a few hours after giving birth, due to the overcrowded facilities and extremely limited resources.” On top of all this, Beydoun said that many women must make the journey to hospitals or health centers—where they could still be turned away due to lack of capacity—on foot.
Due to limited resources, Awadallah says many c-sections and births “are being performed without basic medical supplies, or anesthesia and without any postnatal care.” Few are able to get or attend appointments with their doctors after giving birth, and many “have no option other than to stay in the overcrowded shelters.” As a result, a lot of “women are being dangerously exposed to infections,” the the risk of maternal mortality is high: “There’s now so much risk of hemorrhaging and infections without the right tools and medicines,” Beydoun said. And the many women forced to undergo emergency c-sections also face cesarean wound infections due to lack of clean medical tools for the procedure.

Of course, this is all assuming that pregnant women are able to be admitted into hospitals at all, where “priority is often not for women going into labor” and beds are rarely available for them, Awadallah said. The conditions at the Al-Emirati field hospital in Rafah demonstrate how overworked hospitals in Gaza have become: Beydoun said the hospital was “initially designed to receive 30 to 40 outpatient consultations from pregnant women on a daily basis—now they handle 300 to 400 cases daily.” The hospital has just one operating room and is “designed to have two to three c-section deliveries per day—now they’re delivering 20 daily.”
In October, it was estimated that at least 50,000 women in Gaza were pregnant. The International Planned Parenthood Federation reported at the time that more women were miscarrying or going into early labor from shock and stress under bombardment. And it’s not yet clear how many of those thousands of pregnant women in Gaza are among the estimated 24,000 Palestinians who have been killed in Israel’s attacks, or among the thousands who remain missing. In its charge of genocide against Israel at the International Court of Justice, South Africa alleges that “two mothers are estimated to be killed every hour in Gaza.” (The Israeli death toll from Hamas attacks on October 7 stands at 1,139. Hamas continues to hold roughly 200 people hostage.)
After months of Israeli bombardment, the health care system in Gaza is “completely collapsing,” Doctors Without Borders warned last month. A CNN investigation published on January 12 found at least 20 of 22 hospitals in northern Gaza had been damaged or destroyed in the first two months of Israel’s war on Gaza, and 14 were directly attacked by Israeli forces. The World Health Organization reported in December that no “functional” hospitals remained in northern Gaza, and only nine out of 36 hospitals in the south were even partially functioning to serve Gaza’s population of 2 million. On Tuesday evening, journalists in Gaza reported that Israeli forces had closed in on and were attacking Nasser Hospital.
Birth complications are just one threat people who menstruate are facing: As the independent Gaza-based journalist Bisan Owda highlighted earlier this month, period supplies are nearly impossible to find. According to Awadallah, few people “can find a pharmacy nearby,” let alone one that still stocks sanitary products. Many are forced to use strips of cloth that they can’t wash due to lack of water, plastic bags in lieu of pads, or, “if they’re lucky enough,” cut-up baby diapers. One hospital worker told Owda that “each day” she encounters “numerous instances of fever directly linked to vaginal yeast infections, arising from inadequate hygiene and the absence of feminine products.” Another told her that the “scarcity of basic products results in more hospital visits, longer hospital stays, and worsened conditions” from infection and disease. Severe water shortages and overcrowded public bathrooms further contribute to “the high number of reproductive and urinary tract infections,” Awadallah said.
On top of that, due to “the suffering, anxiety, and deteriorating psychological status of the women in the [Gaza] Strip,” Awadallah said a large proportion are now “getting their period a number of times during the month” instead of once.
This lack of water and malnutrition as a result of Israel’s blockade have been especially detrimental for nursing mothers: Women are struggling to breastfeed their babies as they aren’t able to produce milk “without having water to drink nor sufficient food to eat,” Awadallah said. In a letter provided by CARE, Alaa, a mother in Gaza, wrote that “no one is eating enough,” and “it is usually the mothers who eat last” in order to feed their children first. “I slept on an empty stomach every night so my children wouldn’t go hungry,” Alaa wrote. Back in October, Al-Aqsa Hospital told the Associated Press that many mothers in Gaza were forced to mix baby formula with contaminated water, “[contributing] to the rise in critical cases” in the hospital’s neonatal ward.
Barriers to basic health care and resources aren’t new for the women and girls of Gaza, Awadallah told Jezebel: “Palestinian women and girls were already living in a severely vulnerable environment, in an area which has been blockaded from essential basic health services and products for more than a decade.” But the crisis has become more dire than ever, and “without a full and immediate ceasefire, and the unimpeded delivery of humanitarian aid across all parts of Gaza, maternal and neonatal deaths will continue to rise.”
2 notes
·
View notes
Text
Unraveling the Enigma: Exploring the Causes of Infertility in Men and Women

Infertility, a condition that affects millions of couples worldwide, can be a source of immense emotional distress and frustration. While there are numerous factors that can contribute to infertility, understanding its underlying causes is essential for effective diagnosis and treatment. In this article, we delve into the multifaceted causes of infertility in both men and women, shedding light on the complex interplay of biological, environmental, and lifestyle factors.
Causes of Infertility in Women
Ovulation Disorders: Irregular or absent ovulation can hinder conception. Conditions such as polycystic ovary syndrome (PCOS), thyroid disorders, and premature ovarian insufficiency (POI) can disrupt the ovulation process.
Fallopian Tube Damage: Blockages or damage to the fallopian tubes can prevent the egg from reaching the uterus for fertilization. Previous pelvic infections, endometriosis, or surgery may contribute to fallopian tube issues.
Uterine Abnormalities: Structural abnormalities in the uterus, such as fibroids or polyps, can interfere with embryo implantation and development, leading to infertility.
Age-related Factors: As women age, the quantity and quality of their eggs decline, making conception more challenging. Advanced maternal age is a significant risk factor for infertility.
Causes of Infertility in Men
Low Sperm Count or Quality: Issues with sperm production, motility, or morphology can impair fertility. Factors such as hormonal imbalances, genetic conditions, and lifestyle choices (e.g., smoking, excessive alcohol consumption) can affect sperm health.
Varicocele: A varicocele, an enlargement of the veins within the scrotum, can lead to decreased sperm production and quality. It is a common reversible cause of male infertility.
Testicular Factors: Conditions such as undescended testicles, testicular trauma, or infections can impact sperm production and function, contributing to infertility.
Ejaculatory Disorders: Disorders affecting the ejaculation process, such as retrograde ejaculation or erectile dysfunction, can hinder the delivery of sperm during intercourse.
Seeking Help from a Male Fertility Doctor
For couples struggling with infertility, consulting a male fertility doctor, also known as a reproductive urologist or andrologist, can provide valuable insights and guidance. These specialists are trained to evaluate and treat male infertility issues, offering diagnostic tests, fertility evaluations, and personalized treatment plans to address underlying causes and improve reproductive outcomes.
Conclusion
Infertility can stem from a myriad of factors affecting both men and women. By understanding the potential causes of infertility and seeking specialized care from a male fertility doctor specialist, couples can embark on a journey towards achieving their dream of parenthood. With advancements in reproductive medicine and personalized treatment approaches, there is hope for overcoming infertility challenges and building a family.
2 notes
·
View notes
Text
Embracing Beauty And Wellness: Dr. Manal Younis, The Gynecologist With A Passion For Aesthetics

In the picturesque town of Clonmel, nestled amidst the serene landscapes of Tipperary, Ireland, Dr. Manal Younis has carved her niche in the field of women's health and aesthetics. With a background as a skilled gynecologist and a profound passion for beauty and wellness, Dr. Younis has taken the world of aesthetics by storm, offering a range of innovative treatments that empower her clients to look and feel their best. Let's delve into the journey of this remarkable medical professional and the aesthetic clinic she proudly owns.
A Gynecologist with a Difference
Initially established herself as a trusted gynecologist, specializing in women's health, obstetrics, and reproductive medicine. Her genuine dedication to the well-being of her patients made her a respected name in the community. She worked tirelessly to support women in every stage of their lives, from prenatal care to menopausal health.
As a gynecologist, Dr. Younis realized the inseparable connection between a woman's health and her self-esteem. This realization inspired her to broaden her horizons and offer aesthetic treatments aimed at enhancing her patients' self-confidence and overall well-being.
Beauty in the Heart of Clonmel
In the heart of Clonmel, Dr. Younis opened her own aesthetic clinic, offering a diverse range of beauty treatments. Her clinic is a sanctuary where her clients can escape from the hustle and bustle of daily life and focus on their personal beauty and wellness journey.
Bum Augmentation
The Clinic offers advanced techniques for bum augmentation, giving clients the opportunity to achieve their desired curves. Whether you're looking to enhance your curves or achieve a more balanced figure, her clinic provides safe and effective treatments that cater to your individual needs.
Anti-Wrinkle Injections
Aging is a natural process, but it doesn't mean we have to accept its signs without a fight. Dr. Younis specializes in anti-wrinkle injections that can turn back the clock, smoothing out fine lines and wrinkles to reveal a more youthful, refreshed appearance. These treatments are minimally invasive and can be tailored to target specific areas of concern.
Botox Clinic
Botox Clinic is a household name when it comes to non-surgical rejuvenation. Her clinic boasts a state-of-the-art Botox facility, where clients can achieve smoother, more youthful skin without the need for surgery. Botox treatments are quick, convenient, and deliver impressive results.
The Personal Touch
What sets her apart is her unwavering commitment to providing personalized care to her clients. She understands that every individual is unique, and her approach to aesthetics reflects this belief. Before any treatment, Dr. Younis takes the time to consult with her clients, listening to their concerns and goals. This personalized approach ensures that every treatment plan is tailored to meet the specific needs and desires of each client.
Ensuring Safety and Satisfaction
We prioritize safety above all else. Her extensive medical background as a gynecologist equips her with a deep understanding of the human body, which is crucial when administering aesthetic treatments. She utilizes the latest, FDA-approved techniques and only the highest quality products to ensure her clients receive safe, effective, and long-lasting results.
Client satisfaction is of paramount importance to Dr. Younis. She and her skilled team are dedicated to delivering results that go beyond expectations. Whether it's a subtle enhancement or a more dramatic transformation, the goal is always the same: to empower clients to feel confident and beautiful in their own skin.
Community Involvement
Beyond her clinic, she is an active and compassionate member of the Clonmel community. She takes pride in giving back and supporting local charities and initiatives that promote health and wellness for women in Tipperary.
Conclusion
Dr. Manal Younis, the accomplished gynecologist turned aesthetics specialist, has brought a touch of glamour and empowerment to the picturesque town of Clonmel, Tipperary, Ireland. Her journey from women's health to aesthetic treatments reflects her unwavering commitment to the well-being of her clients. With a personalized approach, a dedication to safety, and a passion for enhancing natural beauty, Dr. Younis's clinic is a beacon of hope for those seeking to look and feel their best.
In a world where self-confidence is the key to success, Dr. Manal Younis provides a gateway to achieving your aesthetic dreams, all within the serene beauty of Tipperary, Ireland.
2 notes
·
View notes
Text
What is IVF?
In recent decades, advancements in medical science have revolutionized the field of reproductive medicine, providing hope and opportunities for couples struggling with infertility. One such groundbreaking technique is In Vitro Fertilization (IVF). In this blog post, we will delve into the intricacies of IVF treatment, exploring what it is, how it works, and the potential it holds for those seeking to build a family.
What is IVF?
In Vitro Fertilization, commonly known as IVF, is a fertility treatment that involves the fertilization of an egg with sperm outside the human body. The process begins by extracting eggs from a woman's ovaries and fertilizing them with sperm in a laboratory dish. Once fertilization occurs, the resulting embryos are then implanted in the woman's uterus with the hope of establishing a successful pregnancy.
Understanding the IVF Process
Ovulation Induction: The first step in IVF involves stimulating the ovaries to produce multiple eggs. Fertility medications are administered to enhance egg production, monitored through ultrasound and blood tests.
Egg Retrieval: Once the eggs are mature, a minor surgical procedure known as egg retrieval is performed. A thin needle is inserted through the vaginal wall to collect the eggs from the ovaries.
Fertilization: The collected eggs are then combined with sperm in a controlled environment, allowing fertilization to occur. This step is closely monitored to ensure the formation of healthy embryos.
Embryo Culture: The fertilized eggs, now embryos, are cultured and monitored for several days. The healthcare team assesses their quality before selecting the most viable embryos for transfer.
Embryo Transfer: In the final step, one or more selected embryos are transferred into the woman's uterus. This is a relatively simple and painless procedure that aims to establish a successful pregnancy.
Success Rates and Considerations
IVF success rates vary depending on several factors, including the age of the woman, the cause of infertility, and the quality of the embryos. While some individuals achieve pregnancy in the first cycle, others may require multiple attempts. It's essential to approach IVF with realistic expectations and to consult with healthcare professionals to understand individual circumstances.
Challenges and Emotional Aspects
Embarking on an IVF journey can be emotionally challenging for couples. The process involves physical, emotional, and financial commitments, and individuals may experience a range of emotions, from hope and excitement to disappointment and stress. Support from loved ones and mental health professionals can play a crucial role in helping individuals navigate these challenges.
Conclusion
In Vitro Fertilization has emerged as a beacon of hope for many couples facing infertility challenges.
Schedule a Consultation with Dr. Sonal Lathi Today If you are considering IVF treatment, Dr. Sonal Lathi is the perfect choice for you. She is a leading expert in IVF, and she is committed to helping couples achieve their parenthood dreams.
#IVF#fertility treatment#reproductive health#in vitro fertilization#family building#infertility#assisted reproductive technology#egg retrieval#embryo transfer#pregnancy journey#parenting hope#medical advancements#healthcare#women's health#parenthood#emotional wellness#support network#family building options#fertility awareness#IVF success#embryo quality#hopeful beginnings#modern medicine#couples' journey#future of reproductive medicine#life through IVF
2 notes
·
View notes
Text
Boost Your Testosterone Naturally with These Simple Tips

Introduction
Testosterone is a crucial hormone in the human body, playing a significant role in various aspects of health, including muscle growth, bone density, mood, and even libido. However, as we age, our testosterone levels tend to decrease, which can lead to a range of issues. The good news is that there are natural ways to boost your testosterone levels. In this article, we will explore some simple strategies to increase your testosterone levels, and we'll also introduce you to a product called Alpha Tonic that may aid in this process.
CLICK HERE TO BOOST YOUR HEALTH NOW
Maintain a Healthy Diet

A balanced and nutritious diet is a fundamental factor in maintaining healthy testosterone levels. Include a variety of foods rich in essential nutrients like zinc, vitamin D, and healthy fats. Zinc, found in foods such as lean meats, nuts, and seeds, is essential for the production of testosterone. Vitamin D, obtained from sunlight and foods like fatty fish and fortified dairy products, is also crucial for healthy hormone levels. Make sure to consume enough healthy fats, such as those in avocados and olive oil, which support hormone production.
Exercise Regularly
Regular physical activity is another key to increasing testosterone levels. Engage in both resistance training and cardiovascular exercises. Lifting weights can stimulate the release of testosterone, and high-intensity interval training (HIIT) can also be beneficial. Aim for at least 150 minutes of moderate-intensity aerobic exercise or 75 minutes of vigorous-intensity aerobic exercise each week.
Get Adequate Sleep

Quality sleep is essential for overall health and maintaining healthy testosterone levels. Aim for 7-9 hours of sleep per night, as it helps your body repair and regenerate. Poor sleep can lead to hormonal imbalances and lower testosterone levels, so prioritize a good night's rest.
Manage Stress
Chronic stress can lead to elevated levels of the stress hormone cortisol, which can suppress testosterone production. Practice stress-reduction techniques such as meditation, deep breathing, or yoga to keep cortisol in check and support healthy testosterone levels.
Maintain a Healthy Weight
Being overweight or obese can contribute to lower testosterone levels. Losing excess body fat through a combination of diet and exercise can help increase your testosterone production. It's important to focus on sustainable and gradual weight loss for the best results.
Stay Hydrated

Drinking enough water is crucial for overall health, and it can also help maintain healthy testosterone levels. Dehydration can lead to an increase in cortisol levels, which can negatively impact your hormones.
Limit Alcohol and Avoid Excessive Drinking
Excessive alcohol consumption can lower testosterone levels. If you choose to consume alcohol, do so in moderation to support healthy hormone balance.
Introducing Alpha Tonic

In addition to these lifestyle changes, there are natural supplements like Alpha Tonic that can aid in boosting testosterone levels. Alpha Tonic is a dietary supplement formulated with a combination of ingredients known for their testosterone-boosting properties. It includes ingredients like fenugreek, ashwagandha, and tribulus terrestris, which have been used for centuries in traditional medicine to support male health and hormonal balance.
CLICK HERE TO BOOST YOUR HEALTH NOW
Fenugreek, for example, has been shown to increase testosterone levels while also supporting libido and muscle strength. Ashwagandha is known for its adaptogenic properties, which can help your body manage stress and reduce cortisol levels. Tribulus terrestris has long been used to enhance athletic performance and support male reproductive health.
Before incorporating any dietary supplement into your routine, it's important to consult with a healthcare professional to ensure it's safe and appropriate for your individual needs.
Conclusion
Maintaining healthy testosterone levels is essential for overall well-being and quality of life. By making simple lifestyle changes such as maintaining a healthy diet, exercising regularly, getting enough sleep, managing stress, and staying hydrated, you can naturally increase your testosterone production. Additionally, considering a natural supplement like Alpha Tonic may provide added support in your quest for hormonal balance. Remember that achieving and maintaining healthy testosterone levels is a journey, so be patient and persistent in your efforts to boost your testosterone naturally.
#fitness#health & fitness#health and wellness#nutrition#supplements#libido and desire#testosterone#long life#wellbeing
3 notes
·
View notes