#Cell Reports Physical Science
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 411 employees.
Note
hi! i was wondering your opinions on how hrt affects the body? i hold a lot of radfem beliefs but i am trans (taking testosterone). would being a woman to you have to be completely about chromosomes? for example, trans men years on T do not have the same genetic makeup as cis women. same with trans women on E, their genetic makeup would be very different to cis men, and would more correlate to cis women. does this factor in who you consider female/male or having experience as women?
Hi there, thanks for reaching out.
Firstly, I think you may be a bit confused. Taking exogenous hormones does not affect your genetic makeup. Your dna will stay the same unless you're exposed to something extreme like radiation - this is a good thing because dna mutation is bad for you and causes cancer! Your genetic sex is immutable, a person with XY chromosomes cannot have their dna altered to have XX chromosomes instead.
Hormones will affect the expression of your genes, for example turning on facial hair production in women who are taking testosterone. This is why those patterns of facial hair, even in women, differ from person to person. The genes for it were already there, but hormone replacement therapy uses the endocrine system to change what signals get sent to your genes to tell them what features to express.
Beyond chemically induced genetic expression, there are particular physical features in males that do not occur in males, and vice versa. This is a feature of the /ancient/ evolution of sexual reproduction. Despite the variety of metaphysical beliefs about identity and personhood, the truth is that humans evolved to reproduce between two sexes, and human beings cannot change sex. Every cell of your body has your sex encoded within it. This affects us physically in many ways. I and most feminists believe that this fact should be irrelevant to any person's ability to pursue their passion, be themselves, and love who they love. Even so, recognition of biological sex is something important. This is really critical in a medical context. For example: men who receive a blood transfusion from a pregnant or recently pregnant woman have an increased risk of death by transfusion-related lung injury. Another example: tracheostomy tubes differ in size depending on sex due to dimorphism in average tracheal diameter. A women who is reported as a male risks considerable injury by having a male sized tracheostomy tube forced into her windpipe. A considerable amount of medications differ in dose effectiveness and side effects based on biological sex. Something as straightforward as a heart attack has different symptoms depending on if the patient is female or male. Denial of biological sex is dangerous, and as it stands, medical science has not advanced enough to change the biological sex of an individual. If you are born male, you will stay male for your entire life. You say that a transwoman who has taken estrogen is more genetically similar to a woman, I'm sorry but that simply isn't true. A male person will always be more genetically similar to other males than to a female person.
Determination of sex is very simple, it's about the easiest genetic test to do. They have kits for high school classrooms to try out ffs. We need to leave the "meaningful sex change is possible through medical intervention" thing in the past, all we accomplish with that is giving people false hope and an unattainable goal to fixate on. Sex is real and immutable, I wish it didn't matter, but it does.
And why it matters is, maleness and femaleness have become inseparable from certain stereotypes and assigned qualities by societies in human history. Overwhelmingly, the male people subjugate the female people. Since men, male humans, discovered womens' ability to give birth could be taken advantage of, it was capitalized upon. And this is the foundation of patriarchal society. Religions were founded to justify this as the will of god. To deny that women have historically been persecuted due to their sex is, well, misogynistic. There is no "woman feeling" that makes us targets for child marriages, FGM, trafficking/prostitution, and other horrors from the minute we're born and even before. No, it's the sex we were born with that makes the world think it can decide our fate. In fact, the way that people treat male children differently from female children is so different so early, that we are genuinely unable to study human behaviour unaffected by gendered expectations. This is what feminists are talking about when they discuss "socialization". There is not a single man on the planet who knows exactly what it's like to see the world from a woman's eyes, no matter how feminine that man is. Womanhood isn't something you can achieve or acquire through effort: you were either born a woman or you weren't, just like you were either born with detached earlobes or not. It's so simple.
All that to get to my final point: Yes, I believe the definition of womanhood comes down to biology, because anything beyond that is a meaningless stereotype. Women can do anything, be anyone, look any way they want, go through any experience they do. The one thing they have in common is that they are female adult human beings. There is not way to fail at being a woman or do it wrong, you just are. Womanhood is the experience of having been a female person in this world, and nothing else. There are certain things only female human beings need, like abortion and female contraceptive rights, access to spaces where we can be safe from our subjugators (male human beings), and the ability to define ourselves and fight for our collective rights.
(At this point you may object and point out that male people who identify as trans women are also subject to violence and scorn from men: unfortunately that is often the case, but this does not make male people who identify as women, well, female. We need solutions for them that do not involve requiring women to sacrifice our comfort and safety for the sake of a particular subset of men, because of the inherent risks involved and the fact that women do not owe men anything even when those men have it bad.)
One last thing: my opinion is that prescribing exogenous cross-sex hormones is unethical (so are all elective cosmetic medical procedures but that's a post for a different day). I understand the distress that gender dysphoria inflicts on people, however the ill effects of hrt are too numerous to condone. The huge increase in risk of stroke with estrogen, heart disease and uterine atrophy with testosterone, and the way that trans medicine studies are notorious for losing followup with patients after a year or less... it's short sighted and frankly, financially motivated. The amount of trans patients who are prescribed hormones without access to an endocrinologist, it's honestly infuriating. People deserve the best care possible, not lab rat bullshit where they cut you loose when it's not working out. I won't judge anyone for what they do to themselves to cope with distress, but I want everyone, especially girls, to be aware of the lifetime effects medical decisions may have, and that you also can find happiness within yourself without hurting your body.
Thanks again for your question, be well ✌️
212 notes
·
View notes
Text

Researchers discover new mechanism to cool buildings while saving energy
With temperatures rising globally, the need for more sustainable cooling options is also growing. Researchers at UCLA and their colleagues have now found an affordable and scalable process to cool buildings in the summer and heat them in the winter. Led by Aaswath Raman, an associate professor of materials science and engineering at the UCLA Samueli School of Engineering, the research team recently published a study in Cell Reports Physical Science detailing a new method to manipulate the movement of radiant heat through common building materials to optimize thermal management. Radiant heat, which is felt whenever a hot surface warms our bodies and homes and is carried by electromagnetic waves, travels across the entire broadband spectrum at ground level between buildings and their environments, such as streets and neighboring structures. On the other hand, heat moves between buildings and the sky in a much narrower portion of the infrared spectrum known as the atmospheric transmission window. The difference in how radiant heat travels between buildings and the sky versus the ground has long presented a challenge to cooling buildings with less skyward-facing surfaces. These buildings have been hard to cool in the summer as they retain heat from the ground and neighboring walls when the outside temperature is high. They are equally difficult to warm in wintertime as the outdoor temperature drops and the buildings lose heat.
Read more.
38 notes
·
View notes
Text
University of Central Florida College of Medicine researcher Renee Fleeman is on a mission to kill drug-resistant bacteria, and her latest study has identified a therapy that can penetrate the slime that such infections use to protect themselves from antibiotics. In a study published in Cell Reports Physical Science, Fleeman showed that an antimicrobial peptide from cows has potential for treating incurable infections from the bacterium Klebsiella pneumoniae.
Continue Reading.
63 notes
·
View notes
Text
Also preserved on our archive! (Follow the link to read this whole story and over 1,000 other news and opinion articles about covid!)
by Katherine Poinsatte, PhD
Case report 'emphasizes' possible COVID-19 link to autoimmune conditions
A 26-year-old man in Nepal developed pulmonary sarcoidosis after a mild COVID-19 infection, per a new case report that suggests “sarcoidosis as a potential complication of COVID-19,” according to researchers.
The man was initially diagnosed with post-COVID fibrosis, or thickening and scarring of lung tissue following a COVID-19 infection. However, after not improving for three months, clinicians performed additional tests and confirmed his lingering symptoms — including shortness of breath, repeated fevers, and weight loss — were due to sarcoidosis.
“This case report emphasizes the potential link between COVID-19 and autoimmune conditions like sarcoidosis, highlighting the need for a comprehensive diagnostic approach and long-term observation to distinguish between sarcoidosis and post-COVID fibrosis,” the researchers wrote.
The report, titled “Sarcoidosis in a young adult: A rare sequelae of COVID-19 infection,” was published in Clinical Case Reports.
Symptoms of COVID-19 infection continued despite treatment An autoimmune disease, sarcoidosis is characterized by an overactive immune system that causes granulomas, or small clumps of inflammatory cells, to form on different tissues and organs.
Sarcoidosis can be triggered by viral, bacterial, and fungal infections. During an infection, the immune system sometimes forms granulomas to surround the threat to the body so the clump of immune cells can destroy it later. In most people, these granulomas naturally go away once the infection is gone. However, when they are long-term, they can cause serious, permanent damage to organs.
In about 90% of cases, patients exhibit some level of pulmonary sarcoidosis, marked by the formation of granulomas on the lungs. These granulomas negatively impact lung function, causing symptoms like shortness of breath, coughing, chest pains, and wheezing. Granulomas can also lead to long-term lung scarring, also known as fibrosis, in which the lung tissue becomes stiff and thick, making it difficult for patients to breathe and reducing the amount of air the lungs can hold.
Infections with COVID-19, caused by the SARS-CoV-2 coronavirus that spread worldwide, can lead to many upper respiratory symptoms, including coughing and shortness of breath. In about 7% of cases, COVID-19 patients will also develop lung fibrosis.
Now, a team led by a researcher at the Nepalese Army Institute of Health Sciences College of Medicine described the case of a young man who had a five-day infection with COVID-19, exhibiting mild symptoms like coughing, fever, sore throat, and muscle soreness.
The man’s fever and cough did not go away, and one month after his initial COVID-19 infection he returned to the clinic. At that time, he tested negative for COVID-19, but his chest X-ray showed signs of lung inflammation and scarring.
He was preliminarily diagnosed with post-COVID fibrosis and prescribed a corticosteroid and a bronchodilator to help reduce inflammation and relax the muscles in the airways.
Further research needed to better understand disease links Despite treatment with those medications, however, the man’s symptoms lingered, leading him to seek medical care again three months after the initial COVID-19 infection. He reported symptoms like low-grade fevers, coughing, shortness of breath with physical activity, and weight loss.
Doctors did additional imaging of the man’s lungs, revealing multiple abnormalities. These included larger than normal lymph nodes, clumps of immune cells, and thickening of the connective tissue around the lung’s blood vessels and bronchi, the airways that lead from the windpipe to a lung.
After ruling out tuberculosis, the doctors analyzed biopsies obtained from the patient’s lymph nodes within the lungs, confirming the presence of granulomas. This led to a confirmed diagnosis of pulmonary sarcoidosis.
“Distinguishing between COVID-19 and sarcoidosis based on clinical and imaging features can be difficult due to significant overlap,” the researchers wrote. “Therefore, for symptomatic patients, obtaining a [biopsy-based] diagnosis of sarcoidosis is crucial to initiate early treatment.”
The patient’s previous treatment regimen was increased. When his cough worsened, the man was temporarily given the oral steroid prednisone until his cough went away. NADI'S NOTE: A recent large study of the effects of general steroids in long covid treatment showed no statistically significant results. Just goes to show you how far behind we are on finding effective treatment for covid and its lingering systems: They just keep cramming the same old chemicals down our throats and expecting different results. It's insanity. (little rant over lol)
At the time of the study’s publication, the patient did not have any sarcoidosis-related symptoms nor was taking any medications. He now has regular follow-up appointments every three months.
“This case report emphasizes that sarcoidosis like many autoimmune conditions arises due to immune system dysfunction following COVID-19 infection,” the researchers wrote.
Additional study is needed to learn more, per the researchers.
“Further research and extended follow-up are necessary to clarify these associations and understand the underlying mechanisms comprehensively,” the team concluded.
Study Link: onlinelibrary.wiley.com/doi/10.1002/ccr3.9445
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
22 notes
·
View notes

Note
Hey please may I ask for dr.stone Gen and Hyoga with a s/o who got badly injured, then being protective perhaps ❣️

thank you for your request! manga spoilers for hyoga’s part- i hope that’s alright!
warnings: blood, stabbing

Though impressed by Gen’s betrayal of the Tsukasa Empire, Hyoga wouldn't allow him to get away with it. He needed to be reminded of the might they had, that they were no fools.
And so when he remembers a comment Gen had made about a certain villager when reporting back to the Tsukasa Empire, he immediately knows how he wants to deliver that reminder.
As if the situation couldn’t have gotten any worse with Hyoga’s attack on the Kingdom of Science, he revealed that his ambush was merely a distraction as his right hand Homura set fire to Ishigami Village. To deal the final blow on not only the double crosser himself but the rest of the villagers, Hyoga caught you when you were off guard staring in horror at the sight of your home being burned down and stabbed you with his spear. As the others dealt with fending off Homura, Hyoga and his men, Gen and the other villagers stayed behind to help tend to your massive stab wound. Suika had run off in an effort to lure the group away from the village, giving the villagers the opportunity to take care of you without having to be on guard. Senku called out some instructions to Gen on how to help with your wound until he got back before running off after Suika with Kohaku. Through shaky hands, Gen immediately got to work.
He was relieved when Senku later did a proper assessment of your condition and assured him that you’d eventually recover. Though horribly wounded, your condition was similar to Gen’s from when he’d been stabbed.
Gen knew better than anyone the pain you were in, being victim of one of Hyoga’s spear assaults himself. It was tremendous, and you were weak in every sense. Just watching you in your frail state made all those feelings wash over him again, and his guilt was just as immense.
He watches you throughout your entire recovery. When you manage to feel well enough to talk, he talks your ear off. He tries to take your mind off your inability to move and redirect your focus to more lighthearted matters, whether it be the Kingdom of Science’s progress in creating cell phones or his magic tricks. Gen’s company helped you pass the time instead of spending it basking in your agony.
When you’re entirely healed, he teaches you some of his own tricks to self defense, such as his fake blood bags, to help keep you even the slightest bit safer in the future. He’s nervous to have you involved in any battles after that, especially against the Tsukasa Empire, but he knows it's unavoidable and that you’ll want to fight. So though he can’t physically protect you himself, he does what he can to keep you safe in the ways he knows how.
In future conflicts, despite his fear, he still puts a protective arm in front of you and tries at all cost to manipulate the battle away from you, so you could stay clear of danger for as long as he could control it.

The Kingdom of Science was backed into a corner- or so the enemy thought. It just so happened that Senku purposely chose the room Hyoga was being held in on the Perseus, and he just so happened to have the last remainder of revival fluid to use on him. Being in the tricky situation they were in, Senku was left with no other option.
As Hyoga emerged from his stone stature and took hold of Kinro’s spear, he surveyed his new surroundings. He quickly understood the dilemma the Kingdom of Science faced and searched for you within the panicked group. His eyes landed on yours, shocked and doubtful, with the slightest sliver of guilt. From the very beginning you had sided with Senku, disgusted over your friend’s cruel vision for the new world and what he was willing to do to bring it to fruition. Having to help take down someone you were so close to hurt your heart, but for the sake of others, you did what had to be done. On the surface, it was as if Hyoga had no room in his seemingly miniscule heart for you anymore, but your dedication was true and your means of protecting others impressive.
Which is why when he was torn between siding with Moz or the Kingdom of Science, his eyes settled on you almost tauntingly, cold steel gaze pinning a sort of blame on you.
But then his eyes trailed downward.
You were hunched over and holding your shoulder with your opposite hand, blood seeping down your arm and all over your fingers and the palm of your hand. You looked tired, presumably from the excessive loss of blood and the need to keep moving in order to stay safe. Yet you stood with your friends once again, not letting yourself submit to Moz’s wrath.
And so Hyoga lunged forward with the golden spear toward Moz, and a fierce battle between the two spearsmen ensued. Senku’s risky “wild card” paid off in the end, as Hyoga was eventually able to bring Moz to his knees and force him to surrender.
His strength and skill is just as admirable as ever, was your final thought before the loss of blood caused you to pass out near the end of the battle.
When you woke, you were met with the sound of incoherent talking and the familiar walls of the Perseus bunker. You slowly blinked as your eyes adjusted to the sight of Senku and Hyoga talking over your body, serious looks etched into their faces and tones as you started to comprehend their words.
“...no longer has any affiliation with me. Even then, your Kingdom of Science wouldn’t resort to such violent means.”
“And we have no way of knowing you won’t do the same.”
“I see aiding you in your battle was a mistake.”
As you shifted in your bed, both pairs of eyes snapped toward you in surprise. Hyoga’s eyes widened at the same time Senku smirked. “Good morning, sleeping beauty. Feeling well rested?”
You yelped as you attempted to prop yourself up on your injured arm, and Hyoga quickly forced you back to lie down. “Think before you act, you fool.”
His sharp gaze returned to Senku as he narrowed his eyes. “I will look over Y/N alongside you. Whether I have your permission or not doesn’t matter to me.”
Senku shrugged. “I have no problem with that so long as you’re serious.”
An agreement was reached. Hyoga would take over Senku’s place in monitoring your recovery in order for Senku to focus on the next steps the Kingdom of Science should take. Like that, Hyoga had joined the Kingdom of Science.
You did a lot of catching up while under his care. What had you been doing while he was petrified? What was the Kingdom of Science working toward now? What other injuries had you sustained? Why the hell weren’t you more careful? There was a conflicting mix between care and resentment in his questions and comments, the contrast between each putting you on edge. You didn’t know exactly where you stood with Hyoga, and his dual responses made it difficult to deduct where he stood on the matter.
It had to be somewhere neutral, because why else would he be so insistent on looking out for you? Why would he constantly put you down for your mistake if there wasn’t some part of him that still cared about you? Why was he so quick to shield you from the other members of the Kingdom of Science? Why did his eyes hold such strong resentment when you told him of the way Moz hurt you?
In a strange way, you almost felt the need to thank Moz, because you were able to reunite with an old friend and rekindle feelings of something more.
#dr stone x reader#dr stone oneshot#dr stone headcanons#dr stone imagines#dr stone fluff#hyoga x reader#hyoga oneshot#gen asagiri x reader#gen asagiri oneshot#gen asagiri headcanons#dr stone hcs
255 notes
·
View notes
Text
Prompt #9: Interpret the most amazing thing you know about nature
Recently, I learned that trees have the ability to heal both the mind and body by releasing natural chemicals that trigger measurable physiological and psychological benefits! The moment you breathe in that crisp, earthy air, your body responds. Stress fades, your heart rate slows, and your mind clears. This isn’t just a feeling, it’s science!

Figure 1: Here is a picture of people on a simple walk through a forested area, which has the profound ability to strengthen our bodies, refresh our minds, and promote overall well-being.
Trees, particularly pine, cedar, cypress, spruce, fir, and oak, release airborne compounds called phytoncides, which act as a defense mechanism against pests and disease. These chemicals help trees resist harmful bacteria, fungi, and insects. For humans, exposure to phytoncides has measurable health benefits. Studies show that they boost the immune system by increasing the activity of natural killer (NK) cells, a type of white blood cell that helps destroy infected or cancerous cells. They also lower cortisol levels, reducing stress and promoting a state of relaxation. This means that simply being in a forest, surrounded by trees, can actively improve immune function and help regulate the body’s stress response.
A study conducted at Nippon Medical School in Tokyo found that spending just a few hours in a forest increased NK cell activity for up to 30 days (Li, Q. et al., 2008). This suggests that the health benefits of nature extend well beyond the time spent outdoors. Another study compared the effects of walking in a forest versus walking in an urban area. Results showed that those who walked in nature had lower blood pressure and reduced stress levels, indicating that natural environments have a direct calming effect on the body (Park et al., 2010).
When phytoncides are inhaled, they activate the parasympathetic nervous system, which is responsible for relaxation and recovery. This shift counteracts the constant "fight-or-flight" response triggered by daily stressors. As a result, phytoncide exposure reduces anxiety, improves mood, and enhances sleep quality. A research study found that individuals who spent time in forests had lower levels of depression and reported feeling more mentally refreshed compared to those in urban settings (Hansen et al., 2017). These effects suggest that exposure to nature is not only beneficial for short-term stress relief but may also play a role in preventing long-term mental health issues.
The benefits of spending time in nature extend beyond mental well-being to physical health improvements. A study published in the International Journal of Environmental Research and Public Health found that people who spent time in the forest had lower blood pressure, reduced inflammation, and a stronger immune response (Lee et al., 2011). The combination of fresh air, lower stress levels, and increased oxygen intake supports cardiovascular health and reduces the risk of stress-related illnesses. Additionally, the slower breathing and reduced heart rate observed in forest environments help regulate the body’s autonomic functions, promoting overall physiological balance.
Even if you can’t escape to the woods, you can still bring nature’s benefits into your life. A simple walk in the park, keeping houseplants, or even listening to forest sounds can trigger some of the same calming effects.
If spending time in nature has measurable health benefits, should workplaces or schools incorporate outdoor time into daily routines? Why or why not?
References: Li, Q., Kobayashi, M., Inagaki, H., et al. (2008). A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins. International Journal of Immunopathology and Pharmacology, 21(1), 117-127. Environmental Health Prevention Medicine
Park, B.J., Tsunetsugu, Y., Kasetani, T., et al. (2010). The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): evidence from field experiments in 24 forests across Japan. Environmental Health and Preventive Medicine, 15(1), 18-26.
Hansen, M.M., Jones, R., & Tocchini, K. (2017). Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. International Journal of Environmental Research and Public Health, 14(8), 851.
Lee, J., Park, B.J., Tsunetsugu, Y., et al. (2011). Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health, 125(2), 93-100.
5 notes
·
View notes
Text
My first attempt at Fanfic for the Fallen Hero universe. I am a science nerd in healthcare, so I'd like to try the first Dr. Halabi note as a SOAP (physician) note at Dr. Mortum's facility for my Sidestep (Arya).
Arya, as Retribution, is an anarchist set on justice and has been revealed to the Rangers, but Sky-Raider got her out before any of the Rangers could make a move.
__________________________
Note: These records are for internal use ONLY. Disclosure of these forms will be met with swift recourse.
Date: 5-10-21
Facility: Mortum Site 01
Patient #: 2344
Patient Name: Arya Skovsgaard
Gender: Female (She/Her)
Attending: Dr. Halabi, MD
CC: Traumatic MVA
HPI:
Arya Skovsgaard is a 30 y.o. AFAB transferred to Site 01 two days following a motor vehicle accident. Per LDPD reports, the patient was restrained, and airbags were deployed. The patient appeared to be driving down the opposite lane on a two-lane highway and struck an oncoming truck. The larger truck was undamaged, but the vehicle the patient was driving was no longer operable. The patient is a known telepath (T12345678), Alpha level. She is known to be capable of operating other individuals through telepathy. The patient was transferred from the care of the Los Diabolos’ Rangers prior to arrival at Site 01. Previous to this, they were at Memorial Hospital under the care of another, unknown physician, wherein lower extremity injuries were treated. The patient chart was consulted prior to transfer. During their stay at this facility, the patient was discharged to inpatient care with a bilateral tibial fracture along the mid-diaphyseal line and a right femoral fracture at the mid-epiphyseal line. Lastly, physicians at the Ranger facility note left SI joint disjunction. It is not known if the accident was intentional, but the Ranger discharge notes allude to this as a possibility. For this reason, the patient will be under constant security detail.
HPI is incomplete due to the current AMS.
ROS:
Patient arrived to facility in a state of alterted mental status leading to an incomplete ROS
Head: Positive for trauma
ENT: Negative for dental trauma
MSK: Grossly apparent damage to bilateral lower extremities
Integumentary: Positive for abrasions, lacerations, ecchymosis
Psych: Altered mental status
Neuro: Loss of consciousness
Physical Exam:
Physical exam from Dr. Petroza at time of surgery and reconstruction is included as a separate document. Below is Dr. Halabi’s secondary PE upon admission to Site 01.
Head: Trauma noted to bilateral orbitals. Ecchymosis around orbitals with classic appearance of trauma.
Neck: No trauma noted
Lymph: No abormalities noted.
Musculoskeletal: See diagram. Dr. Petroza and team applied bilateral leg casting to patient from femural head distally to ankle. Difficult to assess. Otherwise noted
CV: No murmurs, rubs, gallops. Normal rate, rhythm.
Respiratory: Some wheezing. Imaging from Ranger HQ shows no pneumothorax. Brusing to ribs, possibly due to CPR on scene.
GU: No abnormalities noted
Integumentary: Diffuse ecchymosis and bruising to regions visible, patient has [REDACTED] on skin noting them to be [REDACTED].
Psych: Unable to assess
Neuro: Unable to assess. Known telepath.
Assessment:
Agreement with prior disagnosis of bilateral tibial fracture along the mid-diaphsyeal line and right femoral fracture at the mid-epiphyseal line with protrusion from the medial right femur and bilateral media tibia.
Dipostion:
Inpatient discharge.
Progress notes:
5-20-21
2320: Call recieved that patient is en route.
5-21-21
0023: Patient arrives to Site 01.
0024: Dr. Halabi, attending, in room and performing phyical exam.
0100: Patient woke briefly and [REDACTED] attacked them - they were removed from the premises. Security was tightened on the room.
0300: Patient awakens and requests food. Dr. Mortum in room and discussion plan with patient.
0800: Phone call received on patients cell phone from number listed “Julia.” Voicemail left.
TRANSCRIPTION: “Arya, I know you’re out there. I… I’m glad. We’ll talk when you’re ready. I know you don’t want me to be around for this - but we need to talk. I want to help. I had some time to think… you might not have gone about this in the way I would have expected, but I think you have the right idea. Please call me. I love you.”
0830: Patient requesting discharge to their home. The Site will send her with an escort.
Electronic Signature:
Dr. Halabi, MD
This report is to remain within Site 01. If it is found outside of these servers, it should be destroyed, and the aforementioned party should be warned.
25 notes
·
View notes
Text

My name is Dr Jill Simons. I'm a board-certified pediatrician and the executive director for the American College of Pediatricians. Today I'm here alongside my colleagues representing the Coalition of co-signers of the Doctors Protecting Children Declaration. Our coalition consists of physicians together with nurses, behavioral health clinicians, other health professionals, scientists, researchers and public health and policy professionals. And we have serious concerns about the physical and mental health effects of the current protocols promoted for the care of children and adolescents in the United States who express discomfort with their biological sex.
This declaration was authored by the American College of Pediatricians, but really it was developed from the expertise of hundreds of doctors researchers and other healthcare workers and leaders wh, for years have been sounding the alarm on the harmful protocols that continue to be promoted by the medical organizations in the United States. Despite recent revelations from the leaked WPATH Files and the recent release of the final report from the Cass Review, these medical organizations have not changed course.
So, we are calling on these medical organizations of the United States, including the American Academy of Pediatrics, the Endocrine Society, the Pediatric Endocrine Society, the American Medical Association, the American Psychological Association and the American Academy of Child and Adolescent Psychiatry to follow the science and their European colleagues and immediately stop the promotion of social affirmation, puberty blockers, cross-sex hormones and surgeries for children and adolescents who experience distress over their biological sex.
In our declaration, we affirm that sex is a dimorphic, innate trait defined in relation to an organism's biological role in reproduction: male and female this genetic signature is present in every nucleated somatic cell in the body and is not altered by drugs or surgical interventions. Consideration of these innate differences is critical to the practice of good medicine and to the development of sound policy for children and adults alike. Medical decision-making should be based upon an individual's biological sex. It should respect biological reality and the dignity of the person by compassionately addressing the whole person.
We are here defying the claims made by these medical organizations in the US that those of us who are concerned are a minority and that their protocols are consensus. They are not consensus, and we are speaking in a loud unified voice: enough.
[ Full press conference: https://youtu.be/C2tU90XPFlg ]
--
Doctors Protecting Children Declaration
As physicians, together with nurses, psychotherapists and behavioral health clinicians, other health professionals, scientists, researchers, and public health and policy professionals, we have serious concerns about the physical and mental health effects of the current protocols promoted for the care of children and adolescents in the United States who express discomfort with their biological sex.
We affirm:
1. Sex is a dimorphic, innate trait defined in relation to an organism’s biological role in reproduction. In humans, primary sex determination occurs at fertilization and is directed by a complement of sex determining genes on the X and Y chromosomes. This genetic signature is present in every nucleated somatic cell in the body and is not altered by drugs or surgical interventions
2. Consideration of these innate differences is critical to the practice of good medicine and to the development of sound public policy for children and adults alike.
3. Gender ideology, the view that sex (male and female) is inadequate and that humans need to be further categorized based on an individual’s thoughts and feelings described as “gender identity” or “gender expression”, does not accommodate the reality of these innate sex differences. This leads to the inaccurate view that children can be born in the wrong body. Gender ideology seeks to affirm thoughts, feelings and beliefs, with puberty blockers, hormones, and surgeries that harm healthy bodies, rather than affirm biological reality.
4. Medical decision making should not be based upon an individual’s thoughts and feelings, as in “gender identity” or “gender expression”, but rather should be based upon an individual’s biological sex. Medical decision making should respect biological reality and the dignity of the person by compassionately addressing the whole person.
We recognize:
1. Most children and adolescents whose thoughts and feelings do not align with their biological sex will resolve those mental incongruencies after experiencing the normal developmental process of puberty.
Desistance is the norm without affirmation as documented by Zucker in his article “The Myth of Peristence”. (1) Zucker, KJ. The myth of persistence: Response to “A critical commentary on follow-up studies and ‘desistance’ theories about transgender and gender nonconforming children” by Temple Newhook et al. International Journal of Transgenderism. 2018: 19(2), 231–245. Published online May 29, 2018.http://doi.org/10.1080/15532739.2018.1468293 [1]
In the “largest sample to date of boys clinic-referred for gender dysphoria,” there was a desistance rate of 87.8%. (2) Singh D, Bradley SJ and Zucker KJ. A Follow-Up Study of Boys With Gender Identity Disorder. Front Psychiatry. 2021;12:632784. doi: 10.3389/fpsyt.2021.632784
The pro-affirmation Endocrine Society Guidelines (2017) admit: “…the GD/gender incongruence of a minority of prepubertal children appears to persist in adolescence.” (3) Hembree, W., Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: An Endocrine Society clinical practice guideline J Clin Endocrinol Metab. 2017; 102:1–35.
A longitudinal study from the University of Groningen in the Netherlands followed 2772 adolescents (recruited from a psychiatric clinic) from age 11 years through 22 – 26 years. “In early adolescence 11% of participants reported gender non- contentedness. The prevalence decreased with age and was 4% at the last follow-up (around age 26).” Even in this psychiatric patient study group for which interventions were not addressed, but “gender affirmation” is most likely, gender non-contentedness (essentially gender noncongruence) decreased substantially from early adolescence to young adulthood.(4) Rawee P, Rosmalen JGM, Kalverdiijk L and Burke SM. Development of gender non-contentedness during adolescence and early adulthood. Archives of Sexual Behavior. 2024; https://doi.org/10.1007/s10508-024-02817-5
2. Responsible informed consent is not possible in light of extremely limited long-term follow-up studies of interventions, and the immature, often impulsive, nature of the adolescent brain. The adolescent brain’s prefrontal cortex is immature and is limited in its ability to strategize, problem solve and make emotionally laden decisions that have life-long consequences.[2]
3. Sex-trait modification or “Gender affirming” clinics in the United States base their treatments upon the “Standards of Care” developed by the World Professional Association for Transgender Health (WPATH). However, the foundation of WPATH guidelines is demonstrably flawed and pediatric patients can be harmed when subjected to those protocols.
The two Dutch studies that form the foundation for treatment guidelines as documented in the WPATH “Standards of Care” guidelines version 7 (SOC 7) had serious flaws.[3]
These studies did show that the appearance of secondary sex characteristics in adolescents and young adults could be changed by hormonal and surgical interventions, but they failed to demonstrate meaningful long-term improvement in psychological well-being.
Scientific concerns with these studies also include a lack of a control group, small sample sizes, significant numbers of patients lost to follow up, and the elimination of patients who experienced significant mental illness from entering the studies.
It is concerning that the Dutch studies did not address complications and adverse outcome in the adolescent cohort that underwent transition. These complications included new onset diabetes, obesity and one death.[4]
4. There is now sufficient research to further demonstrate the failure of the WPATH, American Academy of Pediatrics and Endocrine Society protocols.
The Cass Review was released on April 10, 2024, as an “independent review of gender identity services for children and young people”. The following points are from Cass’s final report:[5]
Commissioned by the National Health Service (NHS) England, and chaired by Dr. Hilary Cass, the 388-page report utilized systematic reviews, qualitative and quantitative research, as well as focus groups, roundtables and interviews with international clinicians and policy makers.
As part of the evaluation, they reviewed the research on social transition, puberty blockers, and cross-sex hormones.
Social transition
“The systematic review showed no clear evidence that social transition in childhood has any positive or negative mental health outcomes, and relatively weak evidence for any effect in adolescence.
However, those who had socially transitioned at an earlier age and/or prior to being seen in clinic were more likely to proceed to a medical pathway.”
Puberty blockers
“The systematic review undertaken by the University of York found multiple studies demonstrating that puberty blockers exert their intended effect in suppressing puberty, and also that bone density is compromised during puberty suppression. However, no changes in gender dysphoria or body satisfaction were demonstrated [emphasis added].”
“There was insufficient/inconsistent evidence about the effects of puberty suppression on psychological or psychosocial wellbeing, cognitive development, cardio-metabolic risk or fertility.”
“Moreover, given that the vast majority of young people started on puberty blockers proceed from puberty blockers to masculinizing/ feminizing hormones, there is no evidence that puberty blockers buy time to think, and some concern that they may change the trajectory of psychosexual and gender identity development.”
Cross-sex hormones
“The University of York carried out a systematic review of outcomes of masculinising/feminising hormones.” They concluded, “There is a lack of high-quality research assessing the outcomes of hormone interventions in adolescents with gender dysphoria/incongruence, and few studies that undertake long-term follow-up. No conclusions can be drawn about the effect on gender dysphoria, body satisfaction, psychosocial health, cognitive development, or fertility.”
“Uncertainty remains about the outcomes for height/growth, cardio-metabolic and bone health.”
The Cass Review further stated, “Assessing whether a hormone pathway is indicated is challenging. A formal diagnosis of gender dysphoria is frequently cited as a prerequisite for accessing hormone treatment. However, it is not reliably predictive of whether that young person will have longstanding gender incongruence in the future, or whether medical intervention will be the best option for them.”
A 2024 German systematic review on the evidence for use of puberty blockers (PB) and cross-sex hormones (CSH) in minors with gender dysphoria (GD) also found “The available evidence on the use of PB and CSH in minors with GD is very limited and based on only a few studies with small numbers, and these studies have problematic methodology and quality. There also is a lack of adequate and meaningful long-term studies. Current evidence doesn’t suggest that GD symptoms and mental health significantly improve when PB or CSH are used in minors with GD.”[6]
5. There are serious long-term risks associated with the use of social transition, puberty blockers, masculinizing or feminizing hormones, and surgeries, not the least of which is potential sterility.
Youth who are socially affirmed are more likely to progress to using puberty blockers and cross-sex (masculinizing or feminizing) hormones.
“Social transition is associated with the persistence of gender dysphoria as a child progresses into adolescence.”[7]
“Gender social transition of prepubertal children will increase dramatically the rate of gender dysphoria persistence when compared to follow-up studies of children with gender dysphoria who did not receive this type of psychosocial intervention and, oddly enough, might be characterized as iatrogenic.”[8]
Puberty blockers permanently disrupt physical, cognitive, emotional and social development.
Side effects listed in the Lupron package insert include emotional lability, worsening psychological illness, low bone density, impaired memory, and the rare side-effect of pseudotumor cerebri (brain swelling).[9]
A coalition of physicians and medical organizations from around the world submitted a petition to the Commissioner of the U.S. Food and Drug Administration requesting urgent action be taken to eliminate the off-label use of GnRH (growth hormone) agonists in children.[10]
Testosterone use in females and estrogen use in males are associated with dangerous health risks across the lifespan including, but not limited to, cardiovascular disease, high blood pressure, heart attacks, blood clots, stroke, diabetes, and cancer.[xi],[12]
Genital surgeries affect future fertility and reproduction.
6. A report from Environmental Progress released on March 4, 2024, entitled “The WPATH Files” revealed “widespread medical malpractice on children and vulnerable adults at global transgender healthcare authority.”[13]
“The WPATH Files reveal that the organization does not meet the standards of evidence-based medicine, and members frequently discuss improvising treatments as they go along.”
“Members are fully aware that children and adolescents cannot comprehend the lifelong consequences of ‘gender-affirming care’ and, in some cases due to poor health literacy, neither can their parents.”
In addition, developmentally challenged and mentally ill individuals were being encouraged to “transition”, and treatments were often improvised.
7. Evidence-based medical research now demonstrates there is little to no benefit from any or all suggested “gender affirming” interventions for adolescents experiencing Gender Dysphoria. Social “affirmation”, puberty blockers, masculinizing or feminizing hormones, and surgeries, individually or in combination, do not appear to improve long-term mental health of the adolescents, including suicide risk.[14]
8. Psychotherapy for underlying mental health issues such as depression, anxiety, and autism, as well as prior emotional trauma or abuse should be the first line of treatment for these vulnerable children experiencing discomfort with their biological sex.
9. England, Scotland, Sweden, Denmark, and Finland have all recognized the scientific research demonstrating that the social, hormonal and surgical interventions are not only unhelpful but are harmful. So, these European countries have paused protocols and are instead focusing on evaluating and treating the underlying and preceding mental health concerns.
10. Other medical organizations are adhering to the evidence-based medicine documented in the Cass Review Final Report.
The constitution of the National Health Service in England will be updated to state, “We are defining sex as biological sex.”[15]
The European Society of Child and Adolescent Psychiatry issued a document titled “ESCAP statement on the care for children and adolescents with gender dysphoria: an urgent need for safeguarding clinical, scientific, and ethical standards.”
In this paper, they stated, “The standards of evidence-based medicine must ensure the best and safest possible care for each individual in this highly vulnerable group of children and adolescents. As such, ESCAP calls for healthcare providers not to promote experimental and unnecessarily invasive treatments with unproven psycho-social effects and, therefore, to adhere to the “primum-nil-nocere” (first, do no harm) principle”.[16]
11. Health care professionals around the world are also acknowledging the urgent need to protect children from harmful “gender-affirming” interventions.
In a letter to the British newspaper, The Guardian, sixteen psychologists, some of whom worked at the Tavistock Center for Gender Identity Development Service, acknowledged the role clinical psychologists played in placing children on an “irreversible medical pathway that in most cases was inappropriate.”[17]
In the United States, a group of psychiatrists, physicians and other health care workers wrote an open Letter to the American Psychiatric Association (APA), calling on the APA to explain why it glaringly ignored many scientific developments in gender-related care and to consider its responsibility to promote and protect patients’ safety, mental and physical health.[18]
12. Despite all the above evidence that gender affirming treatments are not only unhelpful, but are harmful, and despite the knowledge that the adolescent brain is immature, professional medical organizations in the United States continue to promote these interventions. Further, they state that legislation to protect children from harmful interventions is dangerous since it interferes with necessary medical care for children and adolescents.
The American Psychological Association states it is the largest association of psychologists worldwide. The organization released a policy statement in February 2024 stating, “The APA opposes state bans on gender-affirming care, which are contrary to the principles of evidence-based healthcare, human rights, and social justice.”[19]
The Endocrine Society responded to the Cass Review by reaffirming their stance. “We stand firm in our support of gender-affirming care…. NHS England’s recent report, the Cass Review, does not contain any new research that would contradict the recommendations made in our Clinical Practice Guideline on gender-affirming care.”[20]
The American Academy of Pediatrics (AAP) Board of Directors in August 2023, voted to reaffirm their 2018 policy statement on gender-affirming care. They did decide to authorize a systematic review but only because they were concerned “about restrictions to access to health care with bans on gender-affirming care in more than 20 states.”[21]
Of note, Dr. Hilary Cass called out the AAP for “holding on to a position that is now demonstrated to be out of date by multiple systematic reviews.”[22]
In Conclusion
Therefore, given the recent research and the revelations of the harmful approach advocated by WPATH and its followers in the United States, we, the undersigned, call upon the medical professional organizations of the United States, including the American Academy of Pediatrics, the Endocrine Society, the Pediatric Endocrine Society, American Medical Association, the American Psychological Association, and the American Academy of Child and Adolescent Psychiatry to follow the science and their European professional colleagues and immediately stop the promotion of social affirmation, puberty blockers, cross-sex hormones and surgeries for children and adolescents who experience distress over their biological sex. Instead, these organizations should recommend comprehensive evaluations and therapies aimed at identifying and addressing underlying psychological co-morbidities and neurodiversity that often predispose to and accompany gender dysphoria. We also encourage the physicians who are members of these professional organizations to contact their leadership and urge them to adhere to the evidence-based research now available.
#Jill Simons#Doctors Protecting Children#American College of Pediatricians#medical scandal#medical malpractice#medical mutilation#medical corruption#WPATH Files#The WPATH Files#Cass review#Cass report#puberty blockers#wrong sex hormones#cross sex hormones#sex trait modification#gender affirming care#gender affirming healthcare#gender affirmation#biological sex#sex is binary#sex binary#religion is a mental illness
18 notes
·
View notes
Text
A-B-O Untitled
Prologue
Dela plucked sample Z- 8-III with sterilized tongs and loaded it into the sequencer, listening as the device starts to hum. They try to ignore the mass of colleagues behind them, eagerly awaiting the results. Everyone else was supposed to be done for the day an hour ago, this is the last of Dela’s samples, but people made excuses to linger, to watch. Ali’s resting his chin on their shoulder, watching the sequencer screen and breathing heavily against their neck.
Distracting.
The device quiets beeped thrice and automatically uploaded the information onto the database whilst spitting out a long summary report. Dela read out the report, the room gradually goes silent, but at the last word they erupt in applause.
Ali hugged them about the shoulders, and partially lifted them of their seat.
Too close.
Dela cleared their throat, and the room gradually fell silent. “Good work everyone! Results will be finalised by tomorrow.” They stand up, partially aided by Ali, who’s still threatening to hoist them into the air again. They grab their crutches and pull themselves up the rest of the way. “Take tomorrow of. We’ve got a shit-tonne of reports to do when you get back.”
More cheers, then everyone begins to filter out. Dela’s the last to leave, Ali by their side. He doesn’t say anything, but Dela can see him scanning the ground ahead to make sure there aren’t any errant pens ready to trip them up.
Self-imposed duty complete, he glanced up and grinned, crooked canine snagging on his bottom lip. Dela dutifully ignores how their heart squeezed. “Congratulations! Think this’ll get you a Lowry Prize?”
“Maybe next year, we’ll probably spend this year defending our work.” It wasn’t uncommon for Lowry prizes to be given late. A year might be optimistic, the record was two decades in physics. “Wish I could be as excited as you and everyone else, but I know the moment the report gets out we’ll, I’ll, be dealing with the vultures.”
As much as they love their work, it’s times like this he can’t stand it. Thankfully, the general public could care less about their typical work (for some reason people don’t find information about uterine cell research exciting) but even the occasional fundraising galas and government meetings they have to go to are cloying.
Dela sighed. “Everyone’s going to want the results to prove their agendas.”
Alis shrugged, then said, as if it’s the easiest thing in the world, “The science will have to speak for itself.”
Note Wrote this while avoiding studying for law school after realizing there are people out there who don't get of to the gender politics comenttary part of A-B-O as much as I do. Don't have a title for this yet.
3 notes
·
View notes
Text
10 shocking stories the media buried today.
The Vigilant Fox
Oct 24, 2024
#10 - Doctors who defied the COVID narrative compile 18 alternative cancer treatments that WORK!
These interventions are not only backed by science, but most of them are affordable or completely free.
The first anti-cancer therapy is glucose management through a ketogenic diet. By drastically reducing carbohydrate intake, the ketogenic diet helps starve cancer cells of their primary fuel source, glucose, according to
The FLCCC Alliance
.
Second on the list is exercise. The report says that regular physical activity boosts immune function (critical for fighting cancer), reduces inflammation, and combats fatigue.
Vitamin D3 is also essential. The report says, “Low levels of vitamin D have been linked to an increased risk of cancer. Supplementing with vitamin D3 may support the immune system and help prevent cancer cell proliferation.”
One of the more interesting items on the list is the inclusion of Ivermectin and Fenbendazole. Ivermectin is believed to “interfere with cellular processes essential for cancer cell viability,” whereas Fenbendazole inhibits cancer cell division and induces cancer cell death.
Here are all 18 therapies ranked in order, as compiled by
The FLCCC Alliance
:
1. Glucose Management & Keto Diet
2. Exercise
3. Stress Reduction, Sleep, and Sunshine
4. Vitamin D3
5. Propranolol
6. Melatonin
7. Metformin
8. Curcumin (Nanocurcumin)
9. Ivermectin
10. Mebendazole/Fenbendazole/Albendazole
11. Green Tea
12. Omega-3 Fatty Acids
13. Berberine
14. Atorvastatin or Simvastatin
15. Sildenafil, Tadalafil, and Vardenafil
16. Disulfiram
17. Ashwagandha
18. Itraconazole
Read the full details about each treatment here.
4 notes
·
View notes
Text
Physiological Effects Of Single Bout Of Moderate And High Intensity Interval Exercise On Selective Attention In Young Adults by Farida ahmad in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Objectives: The primary objective of the study was to determine the effect of moderate intensity exercise and high intensity interval exercise on selective attention.
Methodology: This experimental study was conducted at Khyber Girls Medical College Peshawar from September 2020 to February 2021. A total 34 young adults were recruited who were called for two experimental sessions. During 1st experimental session, participants performed moderate intensity exercise of 15 minutes. Forward digit span test were done both before and after exercise. They were then called after one week for 2nd experimental session. Same steps were carried out but this time they performed high intensity interval exercise. The High intensity interval exercise consisted of one minute of low intensity alternating with one minute of high intensity exercise.
Results: The mean age of participants was 20 ± 2 years, body mass index (BMI) was 23 ± 4 kg/m2 and mean waist hip ratio was 0.81± 0.05. After 15 minutes of high intensity interval exercise, selective attention was significantly improved (P = 0.001).
Conclusions: A single session of High intensity interval exercise was more effective at improving selective attention as compared to moderate exercise.
Key words: High intensity interval exercise, Selective attention, Young adults.
Introduction
Physical exercise (PE) is defined as “ a subset of physical activity that is planned, structured, and repetitive and has as a final or an intermediate objective of improving or maintaining physical fitness” [1]. There are different types of PE, exercise performed at 50 - 63 %, 64 -76 % and 77 – 95% % of heart rate maximum (HR max) are termed low, moderate and high intensity exercises respectively. High intensity exercise has been further classified as continuous, high intensity interval training (HIIT) and sprint interval training [2]. HIIT is a type of exercise characterized by short bouts of high intensity exercise alternating with same duration of rest or lower level of physical exercise [2]. Though PE positively affects selective attention and subsequently memory but unfortunately most of our population is not sufficiently active. A World Health Organization survey shows that 23% of males and 32% of females worldwide do not engage in enough physical activity; only 5% of the adult population worldwide meets the basic recommendations of physical exercise [3]. The situation is even worse in Pakistan, 24.4% males and 43.3% females are not sufficiently active. They consider lack of time, use of internet, cell phones and computers as causes for noncompliance to exercise and sedentary behavior [4, 5]. Luckily HIIT is less time consuming as compared to continuous moderate exercise and is preferred by most people [6-8]. It has recently emerged as an effective exercise paradigm for brain health [9]. The main advantage of HIIT is that it provides strong stimulus for neuronal growth. HIIT is especially beneficial for controlling attention and filtering out unnecessary information when performing any cognitive task[10]. However there are few studies on the effects of HIIT on selective attention.The effects of HIIT on brain health still need to be explored [11, 12]. Our study aims to add to the existing body of evidence by determining the effects of HIIT on selective attention in young adults.
Selective attention permits us to filter out insignificant information and focus on what matters. It also forms the basis for learning of complex material [13]. Unfortunately most of our young adults lose attention within 10 – 20 minutes after the start of a cognitive task[14]. The importance of phonological loop and attention in classroom teaching cannot be underestimated [15, 16]. Moreover it is equally important etiological factor in patients with attention deficit disorders, obsessive compulsive disorders, Alzheimer’s disease and Parkinson disease [17-19]. The amount of attention we pay to a task is controlled by central executive in the frontal lobe of the brain which also has the capability to access long term memory stores so by controlling attention one can enhance memory as well[20].
There are different ways to improve attention and subsequently memory for example environmental modifications, attention process training, self‐regulatory strategies, use of external aids and psychosocial support in adults with attention deficit disorder [21]. In addition , physical exercise is known to improve attention both in healthy and attention deficit population [22, 23].
MATERIALS AND METHODS
This experimental study was carried at the Department of Physiology, Khyber Girls Medical College Peshawar. For the within subject design, sample size was calculated by power analysis and effect size based on previous results of Labban et al.,[24]. Power analysis was calculated by using effect size of 0.50. A sample of 34 participants was enough to get power of .80. After approval from ethical committee of Khyber medical university volunteers were recruited through personal contacts, notices and circulars. Young adult females age 18 – 25, were selected who had no history of psychiatric illnesses, psychiatric medications, smoking, neurological and musculoskeletal disorders. All of them fulfilled the exercise fitness criteria as assessed through physical activity readiness questionnaire [25].
After informed consent, anthropometric measurements of all the participants were taken such as weight, height, waist circumference and hip circumference. Low, Moderate and high intensity of exercise was determined for each individual according to their age. First Maximum heart rate (HR max) was calculated for each individual by the formula 220 – age[26]. Exercise performed at 50 -63 %, 64 -76 % and 77 – 95% % of HRmax was their low, moderate and high intensity levels respectively. High intensity interval exercise comprised of one minute high intensity exercise alternating with same duration low intensity exercise [2]. BMI was calculated by Quetelet’ s formula(weight in Kg/height in meter square [27]. Adopting a within subject design, participants were asked to come for two experimental sessions. Participants were asked to refrain from tea and other caffeinated drinks 24 hours prior to experiment. On first experimental day pre exercise selective attention was assessed through Forward Digit span Test (FDST) which is used extensively throughout clinical and research studies and has high validity and reliability among healthy adults and is a subset of Wechsler’s adult intelligent scale [28]. After this test participant were asked to perform 15 minutes of moderate exercise on tread mill (American Fitness, LK700T CORE) according to their individual levels calculated previously. We were closely monitoring the participants to keep their heart rate within the target ranges of moderate exercise. The subjects were assessed within 5 minutes of finishing exercise for selective attention again through digit span forward test. They were then called after one week for experimental session two. The same steps were carried out but this time they performed high intensity interval exercise for 15 minutes.
RESULTS
The mean age for participants in years was 20 ± 1 SD, mean BMI 23 ± 4 (kg/m2) and mean waist hip circumference ratio was 0.81± 0.05. The average Heart rate of the participants for moderate exercise was between 122 and 152 beats per minute, for high intensity most achieved heart rate of 153 to 190 beats per minute. Data was analyzed by SPSS version 20. Statistical significance was considered at P < 0.05. Shapiro wilk test was used to check the normality of data. Wilcoxon signed rank test for serum FDST showed a positive significant change z = - 1.422, p = .15 with a small effect size (r = .1) and z = - 3.182, p = .001 with a medium effect size (r = .4) for MIE and HIIE respectively.
Forward Digit Span Test Scores before and after exercise FDST = Forward digit span test, M1=before moderate exercise, M2= after moderate exercise, H1= before high intensity interval exercise, H2 =after high intensity interval exercise
Discussion
The objective of this study was to assess the effects of an acute HIT session on one aspect of cognitive function i.e. selective attention in young adults. We used digit span forward test (FDST) to assess selective attention. Moderate exercise did not affect attention while HIIT had a significant effect on selective attention. Mean forward digit span test scores before moderate exercise were 8.41 ± 2 and post exercise they were 8.86 ± 2 (P = 0.15). However HIIT had a significant effect on attention with mean FDST of 8.86 ± 1 and 9.86 ± 1 before and after exercise respectively (P = 0.001).
Results from previous research support our findings. There are several studies demonstrating a positive effect of HIIT on cognition and attention as measured by Victoria Stroop test, Reaction Time test and digit span tests [10, 29, 30]. Walsh et al., 2018 recruited 22 university students, nineteen of the participants were females aged 20 ± 1 year. They were called for two sessions; a HIIT and control visit on separate days. The HIIE session lasted for 11 minutes. Participants completed the d2 test which is another test for measuring selective attention [31]. Effect size analysis revealed a moderate effect size of 0.459 in favor of HIIE with a P = 0.01 [32]. Our effect size was 0.486 and P = 0.001. Another study done at the university of Boston is also in line with our findings who checked inhibitory control, selective attention and declarative memory [10].However Study by Alves et al., 2014 does not match with our findings. They used both Stroop color word test FDST and concluded that HIIT improved the performance in Stroop color word test (P = 0.02) after performing 15 minutes of HIIT on cycle ergometer but no significant effect on FDST which may be attributed to the older age group that they recruited for their experiment i.e. 53 years [33].
Another study by Kao et al demonstrated that HIIT was more beneficial at inhibitory control as assessed by modified flanker task in young adult males and females [10]. A study carried out in children 8 – 10 years of age, also report significant effect after HIIE. Stroop performance was improved after one minute after ( P < 0.01), and improvements were maintained until 30 min after exercise cessation [34].
Tsukamoto recruited 10 males and used felt arousal scale (FAS) to assess arousal level and color word Stroop task for measuring attention and found significant increase after HIIE [35].
Previously it was thought that intensity affects cognition in a U shaped manner, meaning that if we continue to increase the intensity of exercise from low to moderate, cognition will improve but after a high intensity is reached cognition will deteriorate [36]. On the contrary, our and other recent research do not support this hypothesis [33]. In our study the high intensity exercise improved selective attention as compared to moderate exercise. Possible explanation for improved attention can be attributed to psychophysiological mechanisms such as improved cerebral blood flow which provides brain sufficient amount of glucose and oxygen and improved psychological wellbeing [11, 37].
It is also suggested that there is increased levels of epinephrine and nor epinephrine which leads to more arousal and subsequently increased attention [38] .Following exercise there is increased allocation of attention resources [32]. When a person is engaged in any information processing operations involving encoding and decision making he uses attention resources to complete this information processing. Human beings select a limited amount of sensory input to process the information while neglect other unrelated sensory inputs through attention resource allocation [39].
CONCLUSION
Our study validated the previous results and showed that even a single bout of 15 minutes of HIIT improves selective attention and it is more effective as compared to moderate exercise of same duration.
#High intensity interval exercise#Selective attention#Young adults#JCRMHS#Journal of Clinical Case Reports Medical Images and Health Sciences (JCRMHS)| ISSN: 2832-1286#Clinical Images journal
2 notes
·
View notes
Text
An enzyme used in laundry detergent can recycle single-use plastics within 24 hours
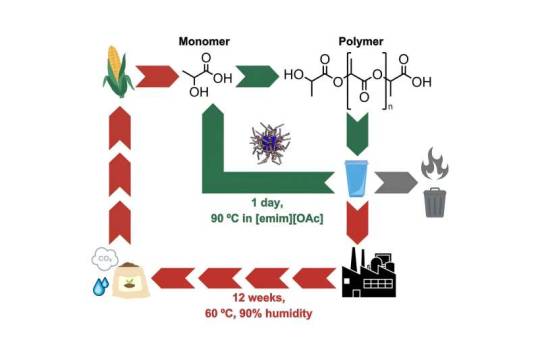
Scientists at King's College London have developed an innovative solution for recycling single-use bioplastics commonly used in disposable items such as coffee cups and food containers. The novel method of chemical recycling, published in Cell Reports Physical Science, uses enzymes typically found in biological laundry detergents to "depolymerize"—or break down—landfill-bound bioplastics. Rapidly converting the items into soluble fragments within just 24 hours, the process achieves full degradation of the bioplastic polylactic acid (PLA). The approach is 84 times faster than the 12-week-long industrial composting process used for recycling bioplastic materials. This discovery offers a widespread recycling solution for single-use PLA plastics, as the team of chemists at King's found that in a further 24 hours at a temperature of 90°C, the bioplastics break down into their chemical building blocks. Once converted into monomers—single molecules—the materials can be turned into equally high-quality plastic for multiple reuse.
Read more.
#Materials Science#Science#Enzymes#Plastics#Polymers#Recycling#King's College London#Bioplastics#Biomaterials#Polylactic acid
55 notes
·
View notes
Text
Imagine the possibility of life forms on other planets that don't resemble any on Earth. What might they look like, and why would they be so different? Juan Pérez-Mercader says it may be possible and the answer may be that they developed from a different type of chemistry. For more than 10 years, the senior research fellow in the Department of Earth & Planetary Sciences and the Origins of Life Initiative at Harvard has studied how to produce synthetic living systems—without relying on biochemistry, or the chemistry that has enabled life on Earth. "We have been trying to build a non-biochemical system, which unaided is capable of executing the essential properties common to all natural living systems," Pérez-Mercader explained. The Pérez-Mercader lab's latest study, published last month in Cell Reports Physical Science, even finds such a system engaged in what Charles Darwin called "the struggle for life." The paper features Pérez-Mercader with co-authors Sai Krishna Katla and Chenyu Lin describing how they created two synthetic models (or "species") and observed the ensuing competition between them.
Continue Reading
131 notes
·
View notes
Text
New transistor’s superlative properties could have broad electronics applications
New Post has been published on https://thedigitalinsider.com/new-transistors-superlative-properties-could-have-broad-electronics-applications/
New transistor’s superlative properties could have broad electronics applications
In 2021, a team led by MIT physicists reported creating a new ultrathin ferroelectric material, or one where positive and negative charges separate into different layers. At the time they noted the material’s potential for applications in computer memory and much more. Now the same core team and colleagues — including two from the lab next door — have built a transistor with that material and shown that its properties are so useful that it could change the world of electronics.
Although the team’s results are based on a single transistor in the lab, “in several aspects its properties already meet or exceed industry standards” for the ferroelectric transistors produced today, says Pablo Jarillo-Herrero, the Cecil and Ida Green Professor of Physics, who led the work with professor of physics Raymond Ashoori. Both are also affiliated with the Materials Research Laboratory.
“In my lab we primarily do fundamental physics. This is one of the first, and perhaps most dramatic, examples of how very basic science has led to something that could have a major impact on applications,” Jarillo-Herrero says.
Says Ashoori, “When I think of my whole career in physics, this is the work that I think 10 to 20 years from now could change the world.”
Among the new transistor’s superlative properties:
It can switch between positive and negative charges — essentially the ones and zeros of digital information — at very high speeds, on nanosecond time scales. (A nanosecond is a billionth of a second.)
It is extremely tough. After 100 billion switches it still worked with no signs of degradation.
The material behind the magic is only billionths of a meter thick, one of the thinnest of its kind in the world. That, in turn, could allow for much denser computer memory storage. It could also lead to much more energy-efficient transistors because the voltage required for switching scales with material thickness. (Ultrathin equals ultralow voltages.)
The work is reported in a recent issue of Science. The co-first authors of the paper are Kenji Yasuda, now an assistant professor at Cornell University, and Evan Zalys-Geller, now at Atom Computing. Additional authors are Xirui Wang, an MIT graduate student in physics; Daniel Bennett and Efthimios Kaxiras of Harvard University; Suraj S. Cheema, an assistant professor in MIT’s Department of Electrical Engineering and Computer Science and an affiliate of the Research Laboratory of Electronics; and Kenji Watanabe and Takashi Taniguchi of the National Institute for Materials Science in Japan.
What they did
In a ferroelectric material, positive and negative charges spontaneously head to different sides, or poles. Upon the application of an external electric field, those charges switch sides, reversing the polarization. Switching the polarization can be used to encode digital information, and that information will be nonvolatile, or stable over time. It won’t change unless an electric field is applied. For a ferroelectric to have broad application to electronics, all of this needs to happen at room temperature.
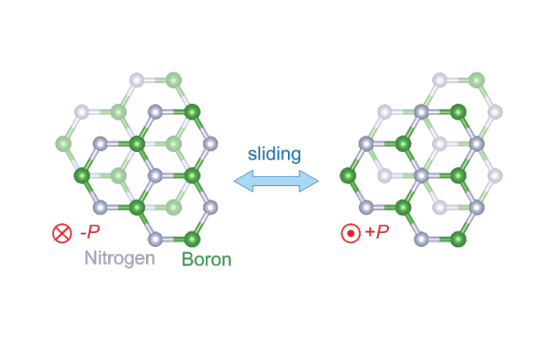
The new ferroelectric material reported in Science in 2021 is based on atomically thin sheets of boron nitride that are stacked parallel to each other, a configuration that doesn’t exist in nature. In bulk boron nitride, the individual layers of boron nitride are instead rotated by 180 degrees.
It turns out that when an electric field is applied to this parallel stacked configuration, one layer of the new boron nitride material slides over the other, slightly changing the positions of the boron and nitrogen atoms. For example, imagine that each of your hands is composed of only one layer of cells. The new phenomenon is akin to pressing your hands together then slightly shifting one above the other.
“So the miracle is that by sliding the two layers a few angstroms, you end up with radically different electronics,” says Ashoori. The diameter of an atom is about 1 angstrom.
Another miracle: “nothing wears out in the sliding,” Ashoori continues. That’s why the new transistor could be switched 100 billion times without degrading. Compare that to the memory in a flash drive made with conventional materials. “Each time you write and erase a flash memory, you get some degradation,” says Ashoori. “Over time, it wears out, which means that you have to use some very sophisticated methods for distributing where you’re reading and writing on the chip.” The new material could make those steps obsolete.
A collaborative effort
Yasuda, the co-first author of the current Science paper, applauds the collaborations involved in the work. Among them, “we [Jarillo-Herrero’s team] made the material and, together with Ray [Ashoori] and [co-first author] Evan [Zalys-Geller], we measured its characteristics in detail. That was very exciting.” Says Ashoori, “many of the techniques in my lab just naturally applied to work that was going on in the lab next door. It’s been a lot of fun.”
Ashoori notes that “there’s a lot of interesting physics behind this” that could be explored. For example, “if you think about the two layers sliding past each other, where does that sliding start?” In addition, says Yasuda, could the ferroelectricity be triggered with something other than electricity, like an optical pulse? And is there a fundamental limit to the amount of switches the material can make?
Challenges remain. For example, the current way of producing the new ferroelectrics is difficult and not conducive to mass manufacturing. “We made a single transistor as a demonstration. If people could grow these materials on the wafer scale, we could create many, many more,” says Yasuda. He notes that different groups are already working to that end.
Concludes Ashoori, “There are a few problems. But if you solve them, this material fits in so many ways into potential future electronics. It’s very exciting.”
This work was supported by the U.S. Army Research Office, the MIT/Microsystems Technology Laboratories Samsung Semiconductor Research Fund, the U.S. National Science Foundation, the Gordon and Betty Moore Foundation, the Ramon Areces Foundation, the Basic Energy Sciences program of the U.S. Department of Energy, the Japan Society for the Promotion of Science, and the Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan.
#2-D#affiliate#applications#atom#atoms#author#billion#boron nitride#career#Cells#change#chip#collaborative#computer#computer memory#Computer Science#Computer science and technology#computing#education#electric field#Electrical Engineering&Computer Science (eecs)#electricity#Electronics#energy#engineering#flash#Foundation#Fundamental#Future#green
2 notes
·
View notes
Text
"I was unsure what the effects of water was going to have on the leaf but overall, it is still science"
"This proves that science can be tested with anything. That is what makes it science!"
"Osmosis is a physical phenomenon that's been used since early mankind"
"This is very impactful to humans because we are made up of cells and molecules, and it is constantly going on in our body right now as you read this"
As per popular demand, here are some of the masterpieces that my students included in their lab reports. Enjoy.
3 notes
·
View notes