#Brain movement disorders
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile US users spent an average of 115.8 minutes on Tumblr app monthly.
Text
What Are Movement Disorders? An Overview of Common Conditions
Movement disorders encompass a range of neurological conditions that impact an individual's ability to control their muscles and movements. These disorders can lead to unusual movements, tremors, stiffness, or lack of coordination. Some common movement disorders include Parkinson's disease, which is marked by tremors and rigidity; essential tremor, which causes uncontrollable shaking; dystonia, characterized by muscle contractions that result in twisting and abnormal postures; and Huntington's disease, a hereditary condition that leads to progressive motor dysfunction. Although the precise causes of these disorders can differ, many are associated with alterations in brain chemistry or damage to the brain regions that govern movement control.
If you or someone you care about is showing signs of a movement disorder, our specialized movement disorders hospital provides tailored care and advanced treatment options aimed at managing symptoms and enhancing quality of life. Our skilled team employs the latest diagnostic tools and custom treatment plans to assist patients in effectively managing their conditions.
0 notes
Text
Brain pathways: an information superhighway
Understanding the neural network
The brain, our body's conductor, is a complex network of billions of interconnected neurons. These neurons communicate with each other via specialized pathways known as nerve tracts. These pathways are essential for transmitting sensory, motor and cognitive information throughout the body.

Main brain pathways
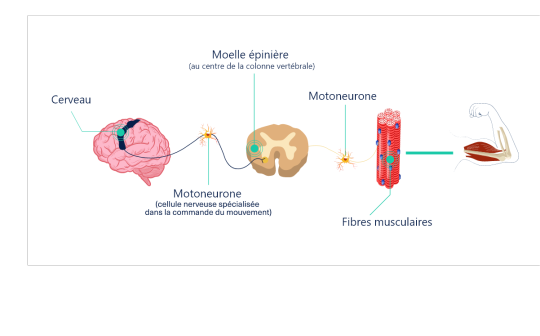
1. The pyramidal pathway
- Role: The pyramidal pathway is primarily responsible for the voluntary control of movement. It connects the primary motor cortex to the motor neurons in the spinal cord, enabling the initiation and control of precise skeletal muscle movements.
- Components: It comprises the corticospinal bundle and the corticobulbar bundle.
- How it works: Nerve signals from the motor cortex travel down this pathway to activate the muscles concerned.
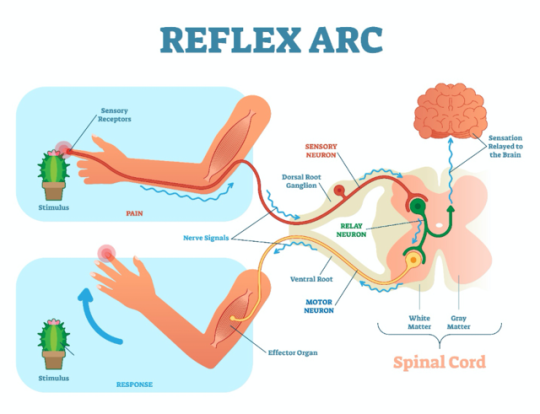
2. Sensory pathways
- Role: These pathways transmit sensory information from the body to the brain.
- Types of sensitivity:
o Tactile sensitivity: Allows us to perceive touch, pressure and vibration.
o Thermal sensitivity: Allows us to perceive heat and cold.
o Deep sensitivity: Allows us to perceive the position of limbs in space (proprioception) and joint movements.
o Pain sensitivity: Allows us to perceive pain.
- Pathway: Sensory information is transmitted by peripheral nerves to the spinal cord, then back to the brain via various ascending pathways.
3. Specific sensory pathways
- Visual: transmits visual information from the retina to the occipital lobe.
- Auditory: Transmits auditory information from the inner ear to the temporal lobe.
- Olfactory pathway: transmits olfactory information from olfactory receptors to the olfactory bulb.
- Taste pathway: transmits taste information from the taste buds to the taste cortex.
4. Proprioception pathway
- Role: Proprioception is the sense that enables us to know our body's position in space.
- How it works: Proprioceptive receptors in muscles, tendons and joints constantly send information to the brain about the state of muscle contraction, joint angle and limb position.
- Importance: Proprioception is essential for movement coordination, balance and posture.
Nerve pathway disorders
Damage to or dysfunction of these pathways can lead to a variety of neurological disorders, such as :
- Hemiplegia: Paralysis of one side of the body.
- Paresthesia: Sensation of numbness or tingling.
- Ataxia: Loss of coordination of movements.
- Blindness: Loss of vision.
- Deafness: Loss of hearing.
In conclusion
Brain pathways are complex networks that ensure communication between the brain and the body. Understanding how they work is essential for grasping the mechanisms underlying many physiological and pathological processes.
Go further
#nerve pathways#brain#neurology#neuroscience#pyramidal pathway#sensitivity#proprioception#nervous system#neuroanatomy#brain health#neurological disorders#brain anatomy#neurons#synapses#cerebral cortex#spinal cord#peripheral nerves#senses#perception#movement#coordination
2 notes
·
View notes
Text
Deep Brain Stimulation - Movement Disorders Treatment in Houston, TX
Dr. Nicolas Nammour specializes in treating deep brain stimulation and movement disorders, offering solutions for improved quality of life in Houston, TX.

0 notes
Text

Understanding the progression of Parkinson's disease is key to providing the right care. This blog explains the 5 stages of Parkinson's disease, from early symptoms to advanced stages. Learn how each stage affects daily life and what to expect as the condition evolves, helping caregivers and families prepare for the future with more awareness and support.
#Parkinsons Disease#Parkinsons Awareness#Neurological Health#Chronic Illness#Stages of Parkinsons#Movement Disorders#Parkinsons Support#Living With Parkinsons#Parkinsons Care#Brain Health#5 Stages of Parkinsons#Parkinson 5 Stages#5 Stages of Parkinson Disease#5 Stages of PD#Stage Five Parkinsons
0 notes
Text
Dr. Sandeep Goel is recognized & one of the best neurologist in Jalandhar, Punjab, India.

Welcome to NeuroCare, where excellence meets experience in neurological care. Dr. Sandeep Goel, our esteemed neurologist, boasts over 30 years of expertise in diagnosing simple and complex neuro problems.

ith over 30 years of specialized neurological care, NHS Neuro Care, led by the esteemed Dr. Sandeep Goel, the best neurologist in Jalandhar, Punjab, India, a dedicated wing of the Department of Neurology that focuses on the advanced, latest procedures and programs to achieve excellence in neurological care, including treatment for Brain, Spine Conditions, and nerve Disorders. Trust in our best neurologist, for unparalleled care in Jalandhar, Punjab, India.
For an Appointment visit: https://nhsneurocare.com/ or Call: +91 9888173033
0 notes
Text
What Is Deep Brain Stimulation How Does DBS Work Deep Brain Stimulation For Movement Disorders - Drkharkar
DBS is the short form of “Deep Brain Stimulation”. DBS is one type of Parkinson’s Surgery.
DBS works by passing a small current into the brain. This current is passed into only to a small part of the brain.
The doctor selects one out of two brain parts (either the GPi or the STN).
DBS works by changing the electrical currents in these areas. At present, we cannot mathematically calculate these changes.
But, empirically (as-seen-with-our-own-eyes) – DBS improves Parkinson’s symptoms.
Let us learn more about these topics:
READ MORE...Best Neurologist In Mumbai, Thane- Dr Kharkar, NeuroPlus Epilepsy & Parkinson's Clinic
0 notes
Text
Expert Neurosurgery Care at HCG Hospitals: Brain, Spine, and Nerve Specialists

Discover leading neurosurgery at HCG Hospitals, offering specialized treatment for brain, spinal cord, and nerve conditions. Our dedicated team provides comprehensive, personalized care, integrating advanced technology and non-surgical approaches for optimal patient well-being and improved quality of life.
#HCG Hospitals Neurosurgery#Neurological Conditions Treatment#Brain Tumor Surgery Specialists#Spinal Cord Treatment Hospital#Movement Disorders Neurosurgery#Pediatric Neurology Services#Advanced Neurosurgical Techniques
0 notes
Text
Neurological Disorders: Unraveling the Complexities of the Nervous System
Neurological disorders are a diverse group of medical conditions that affect the nervous system, leading to various impairments in the brain and spinal cord. These conditions can range from mild to severe, causing significant challenges in daily life for affected individuals. In this comprehensive article, we will delve into the world of neurological disorders, exploring their causes, symptoms,…
View On WordPress
#Alzheimer&039;s disease#Amyotrophic lateral sclerosis (ALS)#Brain diseases#Cerebral disorder#Cerebral palsy#Cognitive impairment#Dementia#Epilepsy#Guillain-Barré syndrome#Huntington&039;s disease#Migraine#Movement disorders#Multiple sclerosis#Myasthenia gravis#Nervous system dysfunction#Neurodegenerative diseases#Neurological disorder#Neuropathy#Parkinson&039;s disease#Restless legs syndrome#Seizure disorders#Stroke#Tourette syndrome#Traumatic brain injury (TBI)
0 notes
Text
anyway um. shoutout to disabled people who move their bodies in ways that are considered "wrong" or "abnormal" regardless of the cause or how it's classified. and this isn't limited to just ambulation.
paralysis. dystonia. gait abnormalities. people with muscle weakness and/or atrophy. people with brain damage. rotational differences. clubfoot. knocked knees. other limb and bodily differences. functional deformities that affect movement. tissue contracture. muscular dystrophies. spasticity. impaired proprioception, balance, and/or coordination. chronic pain. spinal disorders. dyspraxia/DCD. apraxia. ataxia. dystaxia. tourette's syndrome and other tic disorders. conversion symptoms. tremors. neurodegenerative disease. degenerative bone diseases. joint instability. myoclonus. parkinsonism. tardive dyskenisia. various other neurological problems.
...and the list goes on.
personally i feel a bit surreal when my body not doesn't always move in the ways i want it to because that straightforward connection that's there for abled people has been disrupted in a myriad of ways. but no one is gross, ugly, or scary for being unable to move their body in ways that society considers "normal" and "healthy." no one deserves to be gawked/stared at or treated like they're subhuman because of the way their body moves.
it's okay for us to exist.
#cripple punk#cripplepunk#cpunk#neurodivergence#disabled positivity#j#idk a better term for 'functional deformity' bc afaik deformity is a term w/ negative associations#affirmations
6K notes
·
View notes
Text
Spasticity
Let's start by clearly defining spasticity:
Spasticity is a neuromuscular disorder characterized by increased muscle tone, stiff, involuntary movements and exaggerated reflexes. It is often associated with lesions of the central nervous system, such as those caused by stroke, multiple sclerosis or spinal cord injury.
Causes of spasticity:
* Cerebral lesions: stroke, head trauma, brain tumors.
* Spinal cord injuries: road accidents, sports injuries, degenerative diseases.
* Neurodegenerative diseases: multiple sclerosis, amyotrophic lateral sclerosis (ALS).
* Other: encephalitis, meningitis, certain infections.
Symptoms of spasticity:
* Increased muscle tone: muscles stiff and difficult to move.
* Involuntary movements: spasms, muscle contractions.
* Exaggerated reflexes: excessive muscular reactions to a stimulus.
* Walking difficulties: stiff gait, leg spasms.
* Pain: muscle contractures, joint pain.
Diagnosis of spasticity :
* Clinical examination: assessment of reflexes, muscle tone, muscle strength.
* Medical imaging: MRI, CT scan to identify underlying cause.
* Electromyography: measurement of muscle electrical activity.
Treatments for spasticity :
* Medication: muscle relaxants, baclofen.
* Physical therapy: stretching, muscle-strengthening exercises.
* Orthoses: splints to support joints and improve function.
* Botox: injections of botulinum toxin to reduce muscle spasms.
* Surgery: in the most severe cases, to correct deformities or contractures.
Living with spasticity:
* Adapting to everyday life: technical aids, home improvements.
* Psychological support: to cope with difficulties and improve quality of life.
* Patient associations: to exchange ideas and find support.
Advice for caregivers:
* Training: to understand spasticity and its consequences.
* Get informed: about treatments and available aids.
* Take care of yourself: to avoid exhaustion.
Go further
#spasticity#neuromuscular disorder#central nervous system#muscle tone#reflexes#involuntary movements#AVC : stroke#sclérose en plaques : multiple sclerosis (MS)#spinal cord injury#traumatic brain injury (TBI)#brain tumor#neurodegenerative diseases#encephalitis#meningitis#spasticity diagnosis#spasticity treatment#spasticity medications#physical therapy for spasticity#braces for spasticity#botox for spasticity#spasticity surgery#living with spasticity#caregivers for people with spasticity
0 notes
Text
will shifting ever be scientifically proven? a nerdy investigation. . .
reality shifting exists in a weird twilight zone between mysticism and science. on one hand, shifters claim full sensory experiences in different realities, describing their DRs as just as real—if not more real—than this one. on the other, skeptics dismiss it as intense imagination, an extension of lucid dreaming or dissociation at best.
so, will shifting ever be scientifically proven? will we one day have brain scans, peer-reviewed studies, and neuroscientific validation backing it up? or will it remain in the same category as astral projection and past-life regression—forever debated, never confirmed?
guys, this isn’t just a yes-or-no question. it’s a deep dive into how science deals with the unknown, how history has repeatedly proven skeptics wrong, and whether shifting might be next!!!
what science currently says: shifting vs. similar phenomena
while shifting itself hasn’t been studied in depth (yet), we do have research on similar states of consciousness—lucid dreaming, hypnosis, and even maladaptive daydreaming (to an extent). so, what does science say about these?
1. lucid dreaming: once called “impossible,” now neurologically proven
not too long ago, lucid dreaming was considered pseudoscience. the idea that someone could be conscious while dreaming sounded absurd—until researchers found a way to prove it.
scientists like stephen laberge used fMRI scans and eye movement signals from sleeping participants to confirm that lucid dreamers were indeed aware and controlling their dreams. we now know that lucid dreaming involves a unique interplay between the prefrontal cortex (responsible for self-awareness and decision-making) and the REM sleep stage.
before this research? lucid dreamers were written off as liars, delusional, or mistaking their dreams for something they weren’t. sound familiar?
2. hypnosis: once dismissed, now widely used in medicine
hypnosis was once labeled as stage magic and a party trick. today, it’s an accepted psychological phenomenon used in therapy, pain management, and even surgery (yes, surgery—some patients have undergone operations using only hypnosis as anesthesia).
neuroscientific studies show that hypnosis alters brain activity, shifting people into a highly focused state where the brain processes suggestions as reality. if science could accept that the mind can be influenced to perceive reality differently, why is shifting such a stretch?
3. maladaptive daydreaming: a new but recognized condition
maladaptive daydreaming wasn’t officially named until 2002, when professor eli somer identified it as a distinct phenomenon. before then, people struggling with excessive, immersive daydreaming were misdiagnosed with ADHD, OCD, or dissociative disorders.
now, we have concrete research proving that MD is neurologically distinct from normal imagination, linked to overactivity in the default mode network (DMN)—the brain’s self-referential system.
again, before science caught up, these people were called lazy, unfocused, or simply too imaginative. now? it’s a legitimate condition with ongoing research.
what can we take away from that? well, this formula, probably:
history repeats itself: the cycle of disbelief → proof → acceptance
science has a history of mocking what it doesn’t yet understand. let’s not forget that:
• germ theory was laughed at—until microscopes proved bacteria existed.
• deep-sea creatures? dismissed as sailor myths—until we developed better submersibles.
• lucid dreaming, hypnosis, and MD—all called “fake”, until research proved otherwise.
what does this tell us? if shifting is real, the fact that it hasn’t been proven yet doesn’t mean it won’t be. it just means science hasn’t caught up.
but, i like being thorough & unbiased, so i’ll list a few reasons i think or don’t think it’ll be proven!
reasons shifting might be proven
1. brain scans might reveal shifting-specific activity.
• fMRI studies could eventually show unique neurological patterns in shifting states, differentiating it from dreaming or imagination.
2. science is moving towards studying altered consciousness.
• lucid dreaming, astral projection, and out-of-body experiences are getting more attention in neuroscience. shifting could be next.
3. quantum theories suggest consciousness may not be confined to the brain.
• theories like the many-worlds interpretation propose infinite parallel realities—if true, shifting might be tapping into that.
4. hypnosis proves perception can be altered at a deep level.
• shifting might be a self-induced state where the brain accepts a different reality as real.
5. historical precedent shows that dismissed phenomena often get validated later.
reasons shifting might never be proven
1. there’s no scientific method to test it yet.
• unlike lucid dreaming (where we can confirm awareness inside dreams), there’s no current way to measure or prove someone is in a DR.
2. it relies on subjective experience.
• shifting is deeply personal—there’s no external way to prove someone’s consciousness is in another reality.
3. science still struggles to define consciousness itself.
• if we don’t fully understand what consciousness is, proving it can move between realities is even harder.
4. there’s no physical evidence of DRs existing.
• unless we discover parallel realities and a way to interact with them, shifting might remain in the realm of belief rather than science.
5. mainstream science is slow to accept unconventional ideas.
• even if shifting is real, it could take decades—or even centuries—for science to acknowledge it.
my verdict: will shifting ever be proven?
it depends on what shifting actually is.
• if shifting is a genuine form of multiversal travel, it might take quantum physics advancing far beyond what we currently know to validate it.
• if shifting is a unique altered state of consciousness, neuroscience might eventually find evidence through brain imaging studies.
• if shifting is something else entirely—something we don’t even have a framework for yet—it might never be proven in our lifetime.
but history has shown that just because science hasn’t proven something yet doesn’t mean it won’t. skepticism is often just delayed understanding.
so, will shifting be scientifically proven? not tomorrow, not next year—but if history has taught us anything, it’s that the impossible has a habit of becoming reality.
and when that day comes, best believe we’ll be the ones saying “told you so.”
#shifting#reality shifting#shiftblr#shifting community#loassumption#shifting tips#shifting antis dni#shifting script#law of assumption
307 notes
·
View notes
Text
What are some things other psychotics do to differentiate between hallucination and reality? And what are ways some of you hold off symptoms? Looking to get a nice thread for people to help each other going here, this stuff isn't posted about enough.
Ways we prevent symptoms/stop them from progressing:
Make background noise to prevent auditory hallucinations. Most of ours start by hearing something that we can't identify the cause of in the background, and our brain starts the spiral from there. So we listen to music all the time and sleep with a fan on every single night, even in the winter. We just point it away from us if we don't want it making us cold.
Blame the cat (or other pets). Any weird movement, scratching, crunching or thumping? That's just Jerry, don't worry about it. He's a silly cat that does cat things even while we're sleeping. Any noise can be blamed on pets or the wind, which stops the paranoia from setting in and making everything bad.
We also tell ourselves that if there was an actual issue like an intruder or monster, the cat would hiss or scream, and the dog would be barking or making noise. This can be applied to many pets.
Stay busy. Focus on something--art, video games, tv shows and films, craft, gardening, anything that keeps you thinking. Don't let the anxiety get to you, just stay focused on your regular life.
Laugh at it. You're hallucinating a monster in your peripheral vision? Name it Fred and tell him to pay rent. You hear weird noises? Tell them to come back with a warrant. For us, treating symptoms like they're jokes or not serious makes us less anxious and therefore makes it easier to get back to a point where we're okay.
Having a friend or a pet near you can help. We feel safer and less alone when we see another living thing near us that's safe. We don't feel as much like we're trapped in another dimension that way.
How we differentiate between reality and unreality:
Touch it. This one only works for things you're not scared of, and if you don't have tactile hallucinations. It's not foolproof! But when we're seeing things like bugs and stuff, reaching out to touch them causes them to fade away so we know they're fake.
Ask friends and other trusted people if they "heard that" or "saw anything". If they're psychosis friendly, feel free to explain and be specific. If not, be vague and keep it to simple things like "hey did you hear anything? I couldn't tell what it was", if that will be safe enough. Having people to ground you can be great.
Look at how others around you are acting. Are they running or interacting with the thing in question in any way? Do they seem to look at it or no? If no one is noticing, it's less likely to be real.
These won't work for everyone and some of these might be harmful to others, but they're helpful to us. You know best what will help you!
Please feel free to add your own! We need more discussion around psychosis that isn't "scary evil person disorder and how to deal with people who have it".
#neurodivergent#actually disabled#disability#disabled#neurodiversity#actually psychotic#actually schizospec#schizoaffective#psychotic#psychosis#schizospec#madpunk#neuropunk#mad pride#endo safe#pro endo#op#martin (he/it)
728 notes
·
View notes
Text
Happy Disability Pride and awareness month! Let's talk about Epilepsy!

Hi there! I got tired of seeing my condition (that impacts my literal every day life) being left out or forgotten about during discussions about disabilities, so I made my own post about it! Let's go!
First Off! What the heck is epilepsy? Epilepsy is the fourth most common neurological disorder in the world, and it's a chronic medical condition. Epilepsy is a brain disorder that causes recurring, frequent, triggered, and unprovoked seizures to occur.
The official Epilepsy Foundation describes seizures as follows: "Seizures are sudden surges of abnormal and excessive electrical activity in your brain, and can affect how you appear or act. Where and how the seizure presents itself can have profound effects...Seizures involve sudden, temporary, bursts of electrical activity in the brain that change or disrupt the way messages are sent between brain cells. These electrical bursts can cause involuntary changes in body movement or function, sensation, behavior or awareness." (Source link)
Sounds like a lot of fun right? This is our life. Even with medication, we can be VERY limited to what can be safe for us. Seizure medications are NOT a cure, they only exist (at least as of now) as a tool to help have your seizures less often, or be triggered less intensely. Even on medication, seizures can still happen.
If you have epilepsy as a child like I did, it impacts your entire growing and developing experience. I spent MANY times as a child in and out of hospitals, neurologist and specialist offices, an getting so many EEG tests done. The pain of scrubbing the glue out of your hair for DAYS is horrible.
At a young age my seizures were so frequent and serious, it impacted my brain's ability to retain information. I had to re-learn the names of things at age 8 and 9. I had to re-learn HOW TO READ at age 10. I had to be home schooled because the public school system of my state at the time refused to work with me. I have VERY distinct and vivid memories of crying over my little baby ABC's book that I needed as a 4th and 5th grader. I knew I should've known this by this age. I knew that at one point I already did, and it was TAKEN FROM ME.
As an adult, I'M NOT ALLOWED TO DRIVE A CAR. And I can NEVER go to see a movie in theaters or go to see concerts or live music. There are entire TV shows I don't get to see. I can't go to clubs, arcades, dances, or raves. I miss out on A LOT of fun things. I always do, and I'm WELL AWARE of the fun I'm missing out on. The social, casual, and fun life experiences I'll never get to have. That WE'LL never get to have. And oh yeah! Seizures can KILL SOME OF US. Yep.
And the list goes on, and every person with epilepsy experiences it differently. There are multiple different types of seizures you can have, they're NOT always convulsing on the floor. For example, I have complex-partial-myoclonic-seizures. Meaning my muscles DO twitch when I have seizures, but I'm not always completely unconscious and sometimes I'm even able to stay sitting up. However, I'm still very "off" and can't focus or remember much for a good while after the fact. I can't talk or communicate during one, even with my slight bit of consciousness.
My experiences are not universal, I just wanted to talk about it and bring it up. It helps to talk about it even a little bit. Here's more about different kinds of seizures. Here's more about common seizure triggers. Here's more about CORRECT seizure first aid. And here's more general information/resources.
Please stop leaving us out of disability awareness. Please stop ignoring us or saying we're "not really disabled" or anything else like that. Please. Why does it always feel like the only people who care about epilepsy, are people WITH epilepsy? We're so tired of being ignored by others who don't have our condition.
If you're an epileptic person reading this, I see you. I love you. You're so strong, we all are. I believe in you, I believe in us. We're so much stronger than we get credit for, and it's going to be ok. Your anger and frustration are valid. Your emotions and struggles are real. You're valid, and I see you. Hang in there, we got this.
#epilepsy#epilepsy awareness#actually epileptic#disability pride month#disability awareness month#disability awareness#ok to reblog#disability pride
4K notes
·
View notes
Text
For the purposes of this poll, "mental disability" encompasses anything in the DSM-5, genetic disorders that mess with your brain, and TBIs. (Anon is fully aware not all things in the DSM-5 are mental disabilities (such as intellectual disability or autism).)
Anon is physically and mentally disabled and has been their whole life. They've always been told that only physically disabled people can reclaim "cripple." When they joined the cripplepunk movement in order to find other physically disabled people online, they started seeing posts saying that both physically and mentally disabled people could reclaim cripple and be cripplepunk. They'd like to know what others think.
–
We ask your questions anonymously so you don’t have to! Submissions are open on the 1st and 15th of the month.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#polls about language#submitted mar 1#disability#physical disability#mental disability
151 notes
·
View notes
Note
Hello!!! I hope you don't mind doing this one,
Can you help me write a traumatized person who's having trouble talking because of past trauma? (They can still interact with people, but only with signs and movements, not voice) and also a little anxious
Tell me if you need more details =)
How to Write a Mute / Non-Speaking Character
-> healthline.com
-> verywellhealth.com
-> descriptionary.wordpress.com
Types of Mutism:
selective mutism: having the ability to speak but feeling unable to.
organic mutism: mutism caused by brain injury, such as with drug use or after a stroke.
cerebellar mutism: mutism caused by the removal of a brain tumor from a part of the skull surrounding the cerebellum, which controls coordination and balance.
aphasia: when people find it difficult to speak because of stroke, brain tumor, or head injury.
What Causes Selective Mutism in Adults?
having another anxiety condition, like separation anxiety or social anxiety
experiencing physical, emotional, or sexual abuse
having a family history of selective mutism or social anxiety
having fewer opportunities for social contact
having an extremely shy personality
having a speech or language disorder, learning disability, or sensory processing disorder
parent-child enmeshment, or lack of clear boundaries in the relationship
traumatic experiences
Traumatic Mutism vs Trauma-Induced Selective Mutism
if you have traumatic mutism, you may be unable to talk in all situations following a trauma.
with trauma-induced selective mutism, you may find it impossible to talk only in certain situations-- for example, in front of the person who hurt you or in a setting that resembles the circumstances of your trauma.
Different Ways Individuals with Mutism May Choose to Communicate:
Nonverbal Communication: they may rely on facial expressions, gestures, eye contact, and body language to convey their thoughts, emotions, and intentions.
Writing or Typing: they may use a pen and paper, digital devices, or communication apps to write messages, notes, or responses.
Sign Language: they can convey meaning, emotions, and engage in complex conversations through hand signs, facial expressions, and body movements.
Augmentative and Alternative Communication (AAC) Devices: these devices provide individuals with a range of tools and technologies to support their communication needs. They can include speech-generating devices, picture boards, apps, or software that allows users to select words, phrases, or symbols to generate spoken or written output.
Communication Boards and Visual Aids: Communication boards or charts with pictures, symbols, or words can assist individuals in conveying their messages.
Assistive Technology: various assistive technologies, such as speech-to-text apps, text-to-speech programs, or eye-tracking devices that aid individuals with communication.
Tips on Writing a Mute / Non-Speaking Character:
Explore the vast array of nonverbal cues such as facial expressions, body language, gestures, and eye contact. Use descriptions to convey their intentions and reactions.
Utilize internal dialogue. Offer readers a window into their internal thought process, and turn their internal dialogue into a narrative that reveals their inner struggles, triumphs, and complexities so that reader can connect with the character.
Establish a communication system that is unique to your character (Sign language, written notes, telepathy in a fantasy setting, etc.). Having a communication system allows your character to interact with other characters and contribute to the narrative.
Surround them with Understanding Characters that can aid in communcation and fostering meaningful relationships.
Establish the Barriers/Conflicts They'll Experience. Don't forget to be realistic.
Your character is not defined by their inability to speak. Make sure you do not write stereotypes and cliches. Being mute is only one aspect of their identity rather than their defining trait.
Do your research! Seek out firsthand accounts, experiences, and perspectives. Check out online forums and resources to gain insights into their unique challenges, adaptations, and strengths.
If you like what I do and want to support me, please consider buying me a coffee! I also offer editing services and other writing advice on my Ko-fi! Become a member to receive exclusive content, early access, and prioritized writing prompt requests.
#writing prompts#creative writing#writeblr#how to write#writing tips#writing advice#writing resources#writing help#writing tools#how to write a mute character#how to write a non-speaking character#how to write characters
572 notes
·
View notes
Text
do you think the demigods are more likely to be autistic as well
like, the reason they’re canonically more likely to have adhd is bc their brains are hardwired for survival or whatever right, and they’re more likely to be dyslexic bc their brains are hardwired for ancient greek, and anyways that logic is kinda silly but i love it bc rick did it bc of his son’s adhd and dyslexia right. representation
anyways i think it would make sense for them to be more likely to be autistic, too
like, they tend to be more sensitive to their surroundings and pick up on things others don’t, allowing them to see through the mist. it would make sense for their brains to be really hardwired to pick up patterns and maintain strict routines ie training, etc + repetitive movements could help them out on the battlefield in the same way adhd does.
a lot of them have sort of obsessive special interests in things related to their godly parents, like nico w death, annabeth w architecture, percy w the sea, etc. plus, they tend to not feel like they “fit in” or “belong” in the real world, and before they find out abt being a demigod a lot of them think there’s something wrong w them. it’s only once they meet other ppl like them that they realize they aren’t alone
obviously a lot of this is also associated w adhd, but w rick’s logic i think this is fun to think of and makes a lot of sense! plus ✨ comorbidity ✨ exists and ppl w one disorder or condition often have others as well. adhd and autism often go hand in hand!
#kit talks#pjo#percy jackson#hoo#heroes of olympus#rick riordan#annabeth chase#pjo disney+#pjotv#books#nico di angelo#thalia grace#clarisse la rue#silena beauregard#piper mclean#leo valdez#reyna avila ramirez arellano#will solace#frank zhang#hazel levesque#riordanverse#pjoverse#camp half blood
210 notes
·
View notes