#so if it's long covid there's the possibility I can return to unstable but not painful leg vs nerve or other tissue damage
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. has $15.1M in annual revenue.
Note
Apologies if this in intrusive, but did you give Wren a bad leg because you also have one? Just curious, because I’m also disabled and pretty much smack my disability on like 60% of my characters
I do! Just not amputated or quite as bad as his (him amputating his is kind of a version of me fantasizing about chopping my own dumbass leg off), I just have to use a cane if I'm walking or upright for too long, like going to the store. Around the house is doable without, maybe with a brace if it's a bad day. My right leg has been weakened after injuries and it keeps getting worse (maybe covid damage mixed with the injuries, general age, and poor genetics?), not specifically and solely due to disease like his is (leg has degraded severely in his case from corprus).
I would probably be a lot happier if I could get it amputated and could summon a leg to replace it too though tbh, he's livin the dream
#I'm kind of hoping we can figure out wtf is happening with my leg but my doctor and I are thinking maybe covid attacked it and preexisting#damaged was compounded by it#so if it's long covid there's the possibility I can return to unstable but not painful leg vs nerve or other tissue damage#though the random losses of balance aren't really explained by that so there might be a cognitive issue along side it#the scans needed to see what my tissue is doing is not covered by insurance so :[ we gotta wait and see#asks#not art
10 notes
·
View notes
Note
How would the batboys react to a female SO with Paranoid Personality Disorder?
Hi there!
Thanks so much for the ask. I hope this is okay :)
-Sky
Bruce
As a person living with paranoid personality disorder, you might be terrified that people are out to harm you. Your place of residence, Gotham city, does nothing but exacerbate your paranoid thought patterns, since criminals run rampant through the streets. It’s hard to distinguish between paranoid thoughts and substantiated concerns. Is that sketchy person with the full face covering one of Black Mask’s False Face Society members sent to abduct you, or are they just a conscientious citizen taking extra precautions to avoid contracting or transmitting the COVID virus? Being in a state of constant fear prevents you from living your life to the fullest. Luckily, your S/O happens to be Batman in his free time.
Bruce eases your mind just with his presence. He’s probably the smartest, strongest, and most resourceful person you know and being with him makes you feel safe. Bruce is the kind of person who you’d blindly listen to during an emergency – if he told you to jump out of a burning plane, you’d do it without a second thought because he’s never let you down in the past and you’re confident that he never will in the future. If you’re feeling fearful in public, Bruce will grab your hand or put an arm around you securely and soothingly whisper in your ear that he’s right here and there’s nothing to worry about. Having paranoid thoughts means that it’s difficult to reason with you, so you probably aren’t convinced that there is no threat, but you do experience some relief from his soft touch and gentle words. He’ll ask if you want to leave and he’ll take you to your safe space. If you’re feeling fearful in private, Bruce will hold you close and rub your back to reduce your anxiety. If you’re by yourself and start to have those racing, panicked paranoid thoughts, you can always call Bruce. He’ll drop whatever he is doing and come take care of you.
Bruce will teach you self defense to help you feel more comfortable around people. He won’t arm you with any dangerous weapons because he doesn’t want an innocent person to get hurt if you get spooked. Bruce will ask if you want to move into the manor since it has strong security and comes with several vigilantes. If you would rather stay at your own place, Bruce will install a variety of safety systems to make you feel protected. He’ll even spend most nights at your place so you can sleep peacefully. Overall, Bruce is like your lifeline. He’ll know just what to do to help you through your difficult thoughts.
Dick
Dick is a social butterfly who’s had his fair share of romantic partners in the past so it’s natural for you to feel jealous when he spends time with other people. Dick will adamantly declare that he’s with you and only you. At first you might try to ignore the prickly feeling of jealousy because you don’t want to come off as a possessive S/O, but the clues accumulate and suggest that he’s cheating on you. For example, he’ll rarely spend the night with you. You’ll catch him sneaking into bed at ungodly hours of the morning. When confronted, he’ll make up an excuse that he just went to get a drink of water or use the bathroom. You’ll spot bruises scattered over his chest knowing you definitely did not leave those there. He’ll play it off as a gym injury.
When you raise your suspicions, Dick is hesitant to explain. You take this as confirmation of infidelity and you’re ready to walk out. At that point, he has no choice but to come clean about his secret identity as Nightwing. That sounds farfetched and you likely think he’s a pathological liar. Finally, Dick proves it to you and explains that he didn’t want you to be dragged into his dangerous nightlife. While you accept that as the truth, you’ll always wonder if he’s hiding more secrets. Furthermore, you’re probably pissed that he was gaslighting you. Dick will do everything he can to make it up to you. He’ll apologize profusely and in extravagant ways, be more transparent, and shower you with excessive love and affection. It might take a long time, but eventually Dick will worm his way back into your good graces.
It doesn’t take long for the green-eyed monster to rear its’ ugly head again. Now that you’re in the know, you’re hyperaware of the attractive vigilantes that Dick works with and it’s emotionally draining to be jealous all the time. You don’t want to be the type of person who tries to control their partner’s life, but when the suffering becomes too much to bear, you might ask him to stop seeing certain people. Dick will calmly assure you that there isn’t anything going on with any of his vigilante friends. If that doesn’t appease you, he’ll suggest that you hang out with the team and get to know them. He hopes that you’ll see that there aren’t any romantic feelings between them. Whatever you do, please don’t force him to choose between you and his hero life. It will tear him apart.
Jason
Trust is very important to Jason. He doesn’t trust many people as it is and needs a S/O who he can trust wholeheartedly and who will trust him in return. He believes that this relationship will fail if you don’t have confidence in each other. He’ll take it personally if you distrust him. Jason will get defensive and frustrated if you accuse him of being unfaithful, especially if you don’t have a shred of evidence to support your claims. He’ll be offended and deeply hurt that you think so negatively of him but once he’s had some time to cool off, he’ll be able to process everything more objectively. He’ll accept that you can’t control the way you feel. You’d explained it to him once that you do trust him, but there’s a separate voice in your head that tells you otherwise. Jason won’t give up on you though. He’ll come up with a proposition - he’ll agree to install a tracking app on his phone so you can monitor his whereabouts if you’ll promise to work on learning to trust him, whether it be via professional psychotherapy or reading self-help books.
On the other hand, if Jason is one of the only people you trust, he’ll be elated to know that you two have built such a strong connection. It’ll be easy to confide in him because he’ll gladly listen to your worried thoughts with no judgement. At first, he’ll reassure you that nothing bad is going to happen to you – he’s Red Hood and nobody is going to pull anything on you if they value their life. Eventually he’ll realize that trying to reason with you isn’t helpful so he’ll stick to active listening when you’re experiencing paranoid thoughts.
However, if Jason is fresh out of the pit and emotionally unstable, you two will probably bond over your mutual distrust and cynicism about the world. Although you and Jason will get along exceptionally well, it’s possible that your irrational thoughts may feed each other’s paranoia and exacerbate the feelings of mistrust and suspicion. If you find yourself unable to let things go, feel free to vent away when you’re with Jason. He is the king of holding grudges, so he’ll probably support you and even join in on trash talking that person with you when you’re angry. Learning to forgive and forget is something you and Jason can work on together. In a way, it brings you two closer together since you understand each other on a level that others can’t begin to comprehend.
Tim
Tim very compassionate and patient; however, he’s afraid of triggering you so he’s often walking on eggshells around you. He just wants to be the perfect supportive S/O for you and doesn’t want to mess up the relationship. His worst offense (in your eyes) is using ambiguous language that lends to multiple interpretations. For example, he might innocently compliment your clothes/hair/makeup and you might assume that he only likes you for your appearance or that he’s implying that you’re vain for wanting to look nice. The moment you shoot him daggers, he’s realized his mistake and starts to furiously backpedal. He tries to explain himself, but he usually ends up digging himself a deeper hole. Eventually, he gets better at expressing his thoughts carefully so that they can’t be misconstrued.
Tim diligently tries to learn your other triggers and how to help. When you’re stuck in a cycle of paranoid thoughts, Tim will get you to focus on what’s real instead of trying to make you see sense. He’ll help you relax by walking you through breathing exercises, playing soothing music, or whatever strategies you find helpful.
Tim isn’t proud of this, but he’s resorted to deceiving you when necessary. For instance, if you’re experiencing paranoid thought patterns and want to be alone, Tim will hesitantly leave, but he’ll probably secretly monitor you only because he’s worried about your safety. If you’re afraid that others are reading your mind, he might pretend that he invented an anti-mindreading helmet to ease your suspicions. He knows you would feel betrayed if you ever found out about his dishonesty, but he reasons that your safety and comfort are more important in the moment.
Damian
Arguments with Damian are brutal. No matter how insignificant the disagreement is, Damian refuses to back down when he believes he’s right. Paired with your own stubbornness and contentiousness, these quarrels generally result in an impasse. Eventually your anger subsides and the depression sinks in. You might assume that Damian doesn’t love you anymore and that fight was the end of your relationship. Maybe you start packing your belongings to move out right away. Damian comes up behind you and asks what you’re doing. When you tell him that you’re leaving because he doesn’t want you anymore, he’s instantly remorseful. He takes your bags out of your hands and proceeds to pull you in close as he tells you how much he loves you. He assures you that two people can disagree and still love each other.
Damian doesn’t want to argue with you and he certainly doesn’t want to see you upset so he’ll always excuse himself before the argument becomes too heated. He hopes that some time apart will allow you both to calm down and come to a compromise, but it’s never that simple. Most of the time, you’ll need a third-party mediator, like a therapist, to resolve your dispute. The act of seeking out a therapist will be a huge accomplishment for your relationship. Damian likes his privacy and doesn’t want someone else in his business and you might be afraid to share intimate information with a stranger in fear that it will be used against you. Nevertheless, you both want to make this relationship work, so you’ll continue to seek help.
Damian has a habit of being blunt. He doesn’t mean to criticize or insult you – in his mind, he is only stating the facts or his opinion for the purpose of helping you improve. Despite his goodhearted intentions, it’s easy for you to take his comments the wrong way and perceive it as a personal attack. If he sees that his remarks have upset you, he’ll acknowledge all the positive aspects of your performance. Still, you might cling to the disparaging comments and ignore the praise. Going forward, Damian will try to be more encouraging and constructive and will only express feedback if you invite him to do so.
#batfam headcanons#batfam x y/n#batfam x reader#batboys headcanons#batboys x reader#batboys x y/n#bruce wayne headcanon#dick grayson headcanon#jason todd headcanon#tim drake headcanon#batfamily headcanons#batfamily x y/n#batfamily x reader#bruce wayne#dick grayson#jason todd#time drake#Damian Wayne#robinchicklets
192 notes
·
View notes
Text
A Guide to Outpatient COVID Treatment: Step-By-Step Doctors’ Plan That Could Save Your Life
Recently, Dr. Peter McCullough, MD, of Baylor University Medical Center in Dallas testified to Texas Senate HHS Committee about how mass media and even some government agencies are silencing clinical outpatient evidence for effective treatment of COVID19 and instead push vaccines only (video shown below).
Treatments like those mentioned by Dr. McCullough can be found in sites like https://c19early.com/ but specifically, McCullough refers to the following Appendix to a document published by Association of American Physicians and Surgeons (AAPSonline.org) as an educational resource. It is based on a paper published in American Journal of Medicine (link), by Dr. Peter McCullough and 22 other clinicians (MDs) and researchers (PhDs).
“Seek early treatment and be your own advocate. All of the physicians contributing to this booklet are on the frontlines treating outpatients at the first signs of COVID illness. Studies in the US and many other countries clearly show that patients who are treated within the first 5 days of symptoms have better outcomes using the combination of medications in the algorithm below.”

COVID-19 hospitalizations and death can be reduced with outpatient treatment.
Principles of COVID-19 outpatient care include: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, 4) antiplatelet/antithrombotic therapy 5) administration of oxygen, monitoring, and telemedicine.
“For the ambulatory patient with recognized early signs and symptoms of COVID-19, often with nasal real-time reverse transcription or oral antigen testing pending, the following 4 principles could be deployed in a layered and escalating manner depending on clinical manifestations of COVID-19-like illness and confirmed infection: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, and 4) antiplatelet/antithrombotic therapy. Because the results of testing could take up to a week to return, treatment can be started before the results are known. For patients with cardinal features of the syndrome (ie, fever, body aches, nasal congestion, loss of taste and smell, etc.) and suspected false-negative testing, treatment can be the same as those with confirmed COVID-19. Future randomized trials are expected to confirm, reject, refine, and expand these principles. In this article, they are set forth in emergency response to the growing pandemic as shown in Figure 1 .
Treatment algorithm for COVID-19-like and confirmed COVID-19 illness in ambulatory patients at home in self-quarantine. BMI = body mass index; CKD = chronic kidney disease; CVD = cardiovascular disease; DM = diabetes mellitus; Dz = disease; HCQ = hydroxychloroquine; Mgt = management; O2 = oxygen; Ox = oximetry; Yr = year.
The basic groups of prescription medicines and other therapies used in COVID-19:
▪ Combination anti-viral medicines started as soon as symptoms occur ▪ Medicines to decrease inflammation, such as corticosteroids (called immunomodulators)
▪ Anticoagulant therapy to prevent blood-clots that can cause strokes, heart attacks, kidney shut-down, and death.
▪ Non-prescription supportive treatments with zinc, vitamin D, vitamin C, electrolyte drinks such as Pedialyte, and others.
▪ Home-based oxygen support, such as with an oxygen concentrator. These machines are available by physician prescription from home health medical supply businesses and are covered on most medical insurance plans.
I. Antiviral Agents:
These must be started quickly at STAGE I (Days 1-5):
Symptoms include sore throat, nasal stuffiness, fatigue, headaches, body aches, loss of taste and/or smell, loss of appetite, nausea, diarrhea, fever.
These medicines stop the virus from (1) entering the cells and (2) from multiplying once inside the cells, and they reduce bacterial invasion in the sinuses and lung:
▪ *Hydroxychloroquine (HCQ) with azithromycin (AZM) or doxycycline
OR
▪ Ivermectin with azithromycin (AZM) or doxycycline
Either combination above must also include zinc sulfate or gluconate, plus supplemental vitamin D, and vitamin C. Some doctors also recommend adding a B complex vitamin.
Zinc is critical. It helps block the virus from multiplying.
Hydroxychloroquine is the carrier taking zinc INTO the cells to do its job.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 16
II. Anti-inflammatory Agents - Corticosteroids (“steroids”): Oral and Nebulized.
These are started at STAGE II (Days 3-14) to reduce inflammation, the cause of added damage to the lungs and critical organs. Symptoms include worsening cough, difficulty breathing, chest heaviness/tightness or chest pain.
As inflammation damages the airways interfering with normal oxygen-carbon dioxide exchange, blood oxygen levels drop and people experience loss of focus, drowsiness, confusion, difficulty concentrating, low energy and severe fatigue.
The exaggerated Inflammation response in COVID further increases the risk of blood clots.
Prescription medicines and other support added now to Stage I medicines are: ▪ nebulized budesonide to help penetrate the lungs and reduce inflammation ▪ oral prednisone, methylprednisolone, dexamethasone
▪ colchicine – may also be added to reduce inflammation
▪ full strength adult aspirin 325 mg to reduce inflammation and risk of blood clots ▪ home oxygen concentrator may be needed to improve oxygen levels (requires physician prescription)
III. Prescription Anticoagulants (“blood thinners”):
STAGE III (Day 7 and beyond): Symptoms seen in Stage II intensify. Difficulty breathing becomes extreme, oxygen levels drop sharply, risk of heart attack or stroke increases. At this point, people are critically ill.
The medicines to be added to Stage I and II medicines now include:
▪ Aspirin 325 mg unless told not to take by your doctors
▪ And/or low molecular weight heparin injections (e.g. enoxaparin [Lovenox]) OR
▪ apixaban (Eliquis), or rivaroxaban (Xarelto), or dabigatran (Pradaxa) or
edoxaban (Savaysa) in standard doses for 5 to 30 days
If these added steps do not lead to improvement, or the patient becomes unstable, a 911 call is warranted for ER evaluation and hospital admission so that more aggressive IV medications (such as remdesivir, Regeneron, and others) may be considered, and more intensive ventilation regimens are possible in ICU settings.
IV. Vitamins, Supplements, and Oxygen.
▪ Zinc sulfate, gluconate or citrate. These forms are available in pharmacies, health food stores, and sold online. Zinc sulfate 220 mg provides 50 mg elemental zinc, the recommended anti-viral dose. Zinc in the form of zinc picolinate form is not recommended following reports of liver damage and tumors from studies about 20 years ago. Following these reports, the German Commission E that regulates supplements used in medical practice in Germany banned this form of zinc.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 17
▪ Vitamin D3, preferable in oil in capsules for better absorption. Recommended doses for anti-viral benefit vary from 5000 IU or more for 5-30 days
▪ Vitamin C with bioflavonoids for antioxidant, anti-inflammatory effects. Dose
recommendations from our contributors vary from 1000 mg (1 gram) once or twice a day up to 4 or more times a day.
▪ A word about quercetin. Some physicians are recommending this supplement to reduce viral illnesses because quercetin acts as a zinc ionophore to improve zinc
uptake into cells. It is much less potent than HCQ as a zinc transporter, and it does
not reach high concentrations in lung cells that HCQ does. Quercetin may help
reduce risk of viral illness if you are basically healthy. But it is not potent enough to replace HCQ for treatment of COVID once you have symptoms, and it does not
adequately get into lung tissue unless you take massive doses (3-5 grams a day),
which cause significant GI side effects such as diarrhea.
Control of Contagion
A major goal of self-quarantine is the control of contagion. Many sources of information suggest the main place of viral transmission occurs in the home. Facial covering for all contacts within the home as well as frequent use of hand sanitizer and hand washing is mandatory. Sterilizing surfaces such as countertops, door handles, phones, and other devices is advised. When possible, other close contacts can move out of the domicile and temporarily stay with others not ill with SARS-CoV-2. Findings from multiple studies indicate that policies concerning control of the spread of SARS-CoV-2 are effective and extension into the home as the most frequent site of viral transfer is paramount.
Reduction of Self-Reinoculation
It is well-recognized that COVID-19 exists outside the human body in a bioaerosol of airborne particles and droplets. Because exhaled air in an infected person is considered to be “loaded” with inoculum, each exhalation and inhalation is effectively reinoculation. In patients who are hospitalized, negative pressure is applied to the room air largely to reduce spread outside of the room. We propose that fresh air could reduce reinoculation and potentially reduce the severity of illness and possibly reduce household spread during quarantine. This calls for open windows, fans for aeration, or spending long periods of time outdoors away from others with no face covering to disperse and not reinhale the viral bioaerosol.
Combination Antiviral Therapy
Rapid and amplified viral replication is the hallmark of most acute viral infections. By reducing the rate, quantity, or duration of viral replication, the degree of direct viral injury to the respiratory epithelium, vasculature, and organs may be lessened. Additionally, secondary processes that depend on viral stimulation, including the activation of inflammatory cells, cytokines, and coagulation, could potentially be lessened if viral replication is attenuated. Because no form of readily available medication has been designed specifically to inhibit SARS-CoV-2 replication, 2 or more of the nonspecific agents listed here can be entertained. None of the approaches listed have specific regulatory approved advertising labels for their manufacturers; thus all would be appropriately considered acceptable “off-label” use.
Zinc Lozenges and Zinc Sulfate
Zinc is a known inhibitor of coronavirus replication. Clinical trials of zinc lozenges in the common cold have demonstrated modest reductions in the duration and or severity of symptoms. By extension, this readily available nontoxic therapy could be deployed at the first signs of COVID-19. Zinc lozenges can be administered 5 times a day for up to 5 days and extended if needed if symptoms persist. The amount of elemental zinc lozenges is <25% of that in a single 220-mg zinc sulfate daily tablet. This dose of zinc sulfate has been effectively used in combination with antimalarials in early treatment of high-risk outpatients with COVID-19.
Antimalarials
Hydroxychloroquine (HCQ) is an antimalarial/anti-inflammatory drug that impairs endosomal transfer of virions within human cells. HCQ is also a zinc ionophore that conveys zinc intracellularly to block the SARS-CoV-2 RNA-dependent RNA polymerase, which is the core enzyme of the virus replication. The currently completed retrospective studies and randomized trials have generally shown these findings: 1) when started late in the hospital course and for short durations of time, antimalarials appear to be ineffective, 2) when started earlier in the hospital course, for progressively longer durations and in outpatients, antimalarials may reduce the progression of disease, prevent hospitalization, and are associated with reduced mortality. In a retrospective inpatient study of 2541 patients hospitalized with COVID-19, therapy associated with an adjusted reduction in mortality was HCQ alone (hazard ratio [HR] = 0.34, 95% confidence interval [CI] 0.25-0.46, P <0.001) and HCQ with azithromycin (HR = 0.29, 95% CI 0.22-0.40, P <0.001). HCQ was approved by the US Food and Drug Administration in 1955, has been used by hundreds of millions of people worldwide since then, is sold over the counter in many countries, and has a well-characterized safety profile that should not raise undue alarm. Although asymptomatic QT prolongation is a well-recognized and infrequent (<1%) complication of HCQ, it is possible that in the setting of acute illness symptomatic arrhythmias could develop. Data safety and monitoring boards have not declared safety concerns in any clinical trial published to date. Rare patients with a personal or family history of prolonged QT syndrome and those on additional QT prolonging, contraindicated drugs (eg, dofetilide, sotalol) should be treated with caution and a plan to monitor the QTc in the ambulatory setting. A typical HCQ regimen is 200 mg bid for 5 days and extended to 30 days for continued symptoms. A minimal sufficient dose of HCQ should be used, because in excessive doses the drug can interfere with early immune response to the virus.
Azithromycin
Azithromycin is a commonly used macrolide antibiotic that has antiviral properties mainly attributed to reduced endosomal transfer of virions as well as established anti-inflammatory effects. It has been commonly used in COVID-19 studies initially based on French reports demonstrating markedly reduced durations of viral shedding, fewer hospitalizations, and reduced mortality combination with HCQ as compared to those untreated. In the large inpatient study (n = 2451) discussed previously, those who received azithromycin alone had an adjusted HR for mortality of 1.05, 95% CI 0.68-1.62, and P = 0.83.23 The combination of HCQ and azithromycin has been used as standard of care in other contexts as a standard of care in more than 300,000 older adults with multiple comorbidities. This agent is well-tolerated and like HCQ can prolong the QTc in <1% of patients. The same safety precautions for HCQ listed previously could be extended to azithromycin with or without HCQ. Azithromycin provides additional coverage of bacterial upper respiratory pathogens that could potentially play a role in concurrent or secondary infection. Thus, this agent can serve as a safety net for patients with COVID-19 against clinical failure of the bacterial component of community-acquired pneumonia. The same safety precautions for HCQ could be extended to azithromycin with or without HCQ. Because both HCQ and azithromycin have small but potentially additive risks of QTc prolongation, patients with known or suspected arrhythmias or taking contraindicated medications or should have more thorough workup (eg, review of baseline electrocardiogram, imaging studies, etc.) before receiving these 2 together. One of many dosing schemes is 250 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection.
Doxycycline
Doxycycline is another common antibiotic with multiple intracellular effects that may reduce viral replication, cellular damage, and expression of inflammatory factors. This drug has no effect on cardiac conduction and has the main caveat of gastrointestinal upset and esophagitis. As with azithromycin, doxycycline has the advantage of offering antibacterial coverage for superimposed bacterial infection in the upper respiratory tract. Doxycycline has a high degree of activity against many common respiratory pathogens including Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, anaerobes such as Bacteroides and anaerobic/microaerophilic streptococci and atypical agents like Legionella, Mycoplasma pneumoniae, and Chlamydia pneumoniae. One of many dosing schemes is 200 mg po followed by 100 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection. Doxycycline may be useful with HCQ for patients in whom the HCQ-azithromycin combination is not desired.
Favipiravir
Favipiravir, an oral selective inhibitor of RNA-dependent RNA polymerase, is approved for ambulatory use in COVID-19 in Russia, India, and other countries outside of the United States.35 It has been previously used for treatment of some life-threatening infections such as Ebola virus, Lassa virus, and rabies. Its therapeutic efficacy has been proven in these diseases. Like, the antimalarials and antibiotics, favipiravir has no large-scale randomized trials completed at this time, given the short time frame of the pandemic. A dose administration could be 1600 mg po bid on day 1, following by 600 mg po bid for 14 days.
Immunomodulators
The manifestations of COVID-19 that prompt hospitalization and that may well lead to multiorgan system failure are attributed to a cytokine storm. The characteristic profile of a patient acutely ill with COVID-19 includes leukocytosis with a relative neutropenia. These patients have higher serum level of cytokines (ie, TNF-α, IFN-γ, IL-1β, IL-2, IL-4, IL-6, and IL-10) and C-reactive protein than control individuals. Among patients with COVID-19, serum IL-6 and IL-10 levels appear even more elevated in the critically ill. As with any acute inflammatory state, early treatment with immunomodulators is expected to impart greater benefit. In COVID-19, some of the first respiratory findings are nasal congestion, cough, and wheezing. These features are due to excess inflammation and cytokine activation. Early use of corticosteroids is a rational intervention for patients with COVID-19 with these features as they would be in acute asthma or reactive airways disease. The RECOVERY trial randomized 6425 hospitalized patients with COVID-19 in a 2:1 ratio to dexamethasone 6 mg po/IV daily for up to 10 days and found dexamethasone reduced mortality (HR = 0.65, 95% CI 0.51-0.82, P <0.001). One potential dosing scheme for outpatients starting on day 5 or the onset of respiratory symptoms is prednisone 1 mg/kg given daily for 5 days with or without a subsequent taper.
Colchicine
Colchicine is a nonsteroidal antimitotic drug that blocks metaphase by binding to the ends of microtubules to prevent the elongation of the microtubule polymer. This agent has proven useful in gout and idiopathic recurrent pericarditis. The GRECCO-19 randomized open-label trial in 105 hospitalized patients with COVID-19 found that colchicine was associated with a reduction in D-dimer levels and improved clinical outcomes. The clinical primary end point (2-point change in World Health Organization ordinal scale) occurred in 14.0% in the control group (7 of 50 patients) and 1.8% in the colchicine group (1 of 55 patients) (odds ratio, 0.11; 95% CI, 0.01-0.96; P = 0.02). Because the short-term safety profile is well understood, it is reasonable to consider this agent along with corticosteroids in an attempt to reduce the effects of cytokine storm. A dosing scheme of 1.2 mg po, followed by 0.6 mg po bid for 3 weeks can be considered.
Antiplatelet Agents and Antithrombotics
Multiple studies have described increased rates of pathological macro- and micro-thrombosis. Patients with COVID-19 have described chest heaviness associated with desaturation that suggests the possibility of pulmonary thrombosis. Multiple reports have described elevated D-dimer levels in acutely ill patients with COVID-19, which has been consistently associated with increased risk of deep venous thrombosis and pulmonary embolism. Necropsy studies have described pulmonary microthrombosis in COVID-19. These observations support the notion that endothelial injury and thrombosis play a role oxygen desaturation, a cardinal reason for hospitalization and supportive care. Based on this pathophysiologic rationale, aspirin 81 mg daily can be administered as an initial antiplatelet and anti-inflammatory agent. Ambulatory patients can be additionally treated with subcutaneous low-molecular-weight heparin or with short-acting novel anticoagulant drugs in dosing schemes similar to those use in outpatient thromboprophylaxis. In a retrospective study of 2773 inpatients with COVID-19, 28% received anticoagulant therapy within 2 days of admission, and despite being used in more severe cases, anticoagulant administration was associated with a reduction in mortality (HR = 0.86 per day of therapy, 95% CI: 0.82-0.89; P <0.001). Additional supportive data on the use anticoagulants reducing mortality has been reported in hospitalized patients with elevated D-dimer levels and higher comorbidity scores.53 Many acutely ill outpatients also have general indications for venous thromboembolism prophylaxis applicable to COVID-19.
Delivery of Oxygen and Monitoring
Because ambulatory centers and clinics have been reticent to have face-to-face visits with patients with COVID-19, telemedicine is a reasonable platform for monitoring. Clinical impressions can be gained with audio and video interviews by the physician with the patient. Supplemental information, including vital signs and symptoms, will be important to guide the physician. A significant component of safe outpatient management is maintenance of arterial oxygen saturation on room air or prescribed home oxygen under direct supervision by daily telemedicine with escalation to hospitalization for assisted ventilation if needed. Self-proning could be entertained for confident patients with good at-home monitoring.
Many of the measures discussed in this article could be extended to seniors in COVID-19 treatment units in nursing homes and other nonhospital settings. This would leave the purposes of hospitalization to the administration of intravenous fluid and parenteral medication, assisted pressure or mechanical ventilation, and advanced mechanical circulatory support.”
youtube
This is the group’s statement on vaccines:
“Vaccines in Development:
Several vaccine models are being investigated for SARS-CoV-2 (COVID-19) including DNA and RNA vaccines. These vaccines take genetic information from other sources that is introduced into the cells. This information includes instructions to produce a SARS2-like viral antigen itself, and the immune system then reacts to it to develop immunity to the virus.
The most important consideration before approving a vaccine for human use is to make sure that the vaccine is safe and effective. Developing safe and controlled infection models for humans normally takes many years of phased testing in the lab and then in humans. Many physicians and scientists have been concerned that vaccine manufacturers, with government support, are speeding up this process in ways that are not allowing adequate time for the usual phased testing leading up to human clinical trials. Two vaccine manufacturers already have voluntarily paused their clinical trials in people due to serious adverse events.
Currently, there are no RNA-based vaccines approved for human use so it would seem prudent to take the time needed to ensure safety. Vaccines for RNA viruses are notoriously challenging and difficult to develop. We still, after all these years since AIDS emerged in the 1980s, do not have a vaccine for the AIDS virus, or the SARS-1 coronavirus that emerged in 2002-2003, and both are RNA viruses.
Several attempts have been made to create vaccines for coronavirus and other respiratory viruses but none of the vaccines have survived the testing phases. The vaccine trials for SARS-1 from 2003, for example, was shut down because it produced autoimmune hypersensitivity reactions when exposed to the natural virus after immunization in animal studies.
Another problem is that the SARS-2 virus has already shown many mutations. Viruses adapt to the environment to survive. Like the flu virus, it is difficult to predict what mutations will occur and circulate around the world each season. A new vaccine must be reformulated to adjust to the changing genetic makeup of the SARS-2 virus.
Even the best vaccines for flu are only about 30-60% effective. Compare that with an effectiveness for improvement ranging from 64% to more than 90% in more than 100 new studies showing early, outpatient treatment with our existing medications described in chapters.
As research on the vaccine continues, safety and effectiveness are of primary concern. The good news is there are very safe and effective early treatments already available as we described in Chapter 3. Clearly, early, home-based treatment has now been so successful and offers so much hope, there is less urgency to have a vaccine.”
You can sign up to receive the full protocol here: https://aapsonline.org/covidpatientguide/ or find the research paper here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7410805/
5 notes
·
View notes
Text
The Timeline
A year ago in March 2020, I was newly returning back to work after recovering from a severe skin infection. I was on painkillers and several rounds of antibiotics throughout January and February 2020. It was a hard time recovering and for a second there, I thought I was going to die. My blood sugar was through the roof, inflammation and infection were forming a lethal combination. Emergency doctor was grateful I came in when I did because if I had waited any longer I would have lost the battle. My vitals and condition were so unstable that the surgeon did not feel safe operating on me. I had to heal with medicine, quarantine and bed rest.
That took a hard hit to my finances. Behind in rent and bills. In late November in to December 2019 I was just out of work for 2 weeks with an unexplained condition with my lungs. My lungs were inflamed, I had a dry cough but no fluid being brought up. I had terrible night sweats and difficulty breathing. I was given antibiotics, anti-inflammatory medicine and steroids in addition to my daily inhaler and Ventolin inhaler for emergencies. So that's a timeline for ya.
NOV - DEC 2019 Lung Problems
JAN - FEB 2020 Skin Infection
FEB - MAR 2020 Return to Work
MAR 16, 2020 The World Shuts Down.
April comes and I'm hopeful. I begin cutting back on smoking cigarettes. I wasn't a heavy smoker to begin with, but I was definitely smoking 10-15 cigarettes on a bad day; 8-10 on a regular day. I remember saying to Martina and DJ,
"When I take my last puff, that's all it will be. I won't remember the day. I won't say to anyone that I've quit because they will remember. It'll be all they talk about but I don't want to hear any of it. Talking about smoking all the time doesn't help me."
Sometime in late May I took my last puff of a cigarette. I no longer desired to smoke and no longer craved the taste. I told no one and I have successfully overcome my addiction to cigarettes. I enjoyed a quiet birthday on May 29th and was hopeful that Summer would bring some more joy!
Start of Summer in to July 2020... Becoming pregnant should have been a happy occasion for an engaged couple. It wasn't for us. When I learned I was pregnant, my body was in distress. I didn't know what was happening, but my body was in pain. Everyday it got a little bit worse. At this point I had been cigarette free for about 2 months and I had no cycle for 2 months. Extreme Sciatica and Arthritis pain crippled me and suddenly I began seeing spots of blood. I was rushed to the emergency room and learned that I was 14 weeks pregnant. I was ordered to bed rest and limit my movement. We were thrilled but terrified. DJ's hours were cut, but I was working from home. We exhausted our funds to make bed rest as comfortable as possible. Mid July comes and at 16.5 weeks of pregnancy, I miscarried. My sac ripped. I was in so much pain. DJ's heart broke and my heart crumbled. I was looking at a 4 to 6 week recovery but in fact, it took 8 weeks for my body to return to normal. That's a timeline for ya.
APR - MAY 2020 Transition from Moderate to Non Smoker.
JUN - JUL 2020 Becomes Ill, Learns Shes Pregnant!
MID JULY 2020 Suffers Miscarriage
JULY - AUG 2020 Recovery from Miscarriage
SEP 2020 - DEC 2020 I'm recovered and preparing for the next obstacle in my way. My father became ill and was hospitalized. No one could visit him, but suddenly one day, they allowed my mother to go to his room. Nearly two weeks later, my mother tested positive for COVID-19. She battled that for weeks and while all of that was going on Martina had a health scare too in September. Things were going crazy everywhere. As we battled through Autumn, I dealt with my hearing becoming significantly worse. Wisdom Tooth, Jaw Joint and Ear Pain-Infection-Inflammation. Trying to visit a doctor in person was a struggle. I kept being denied an in-person appointment because of my symptoms. I call with symptoms, they make me do a test, I test negative but they would make me quarantine for 14 days and then I call again to make an in-person appointment because my symptoms have worsened... the cycle repeats. I ended up being rushed to the emergency room because I had chills, shakes, sweats and I couldn't hold my head up anymore. 14 days of antibiotics and drops. Finally got some relief.
JANUARY 2021 - CURRENT I was done with 2020. I didn't think things could get any worse until January 30th. My best friend unexpectedly died. Martina and I talked so much about our lives, our goals and our hardships. I always thought that because of my many illnesses that I would leave here first. She hated when we got on that subject but we talked about it in depth many times throughout our friendship. After the miscarriage, I told her I wasn't sure if I would ever become a mother. When Martina passed away after talking with our mutual mentor, confidant and former co-worker Mrs. McCreary, it occurred to me that my life may have an entirely different purpose than how I may have envisioned it to be.
I've spend these days and nights in mourning. The day Martina died, I wasn't aware that she had passed on that day but when I woke in the morning, I felt heavy and full of sorrow. I said to DJ, "Something is wrong but I don't know what it is. I feel it all in my body." At that time, I had no idea my friend had departed but my spirit knew. I spent that entire day focusing on improving what I thought was a mood. I woke up earlier than usual on Monday, preparing to log in for work. I wanted to talk to Martina but I learned she had died. Suddenly everything I felt that Saturday and Sunday made sense.
I talk to Martina out loud every morning, every day now. I know she can't respond but I believe that she can hear me. She always believed in me, even when I didn't believe in myself. The future brings more sorrow for me but also more clarity. Everyday I'm attuning to my goals. I know that I want to live for as long as possible. I want to be available and able; for me, for DJ and for all of our loved ones including Martina. Her children meant the world to her and if any one of them ever needed me for anything... I want to be available and able to be there for them.
I have a timeline for my future but I'm going to take my time, not waste time.
#sad#sad thoughts#depression#grieving#miscarriage#womenshealth#mental health#ripbestfriend#friendship#infection#quitting smoking#cigarettes
1 note
·
View note
Text
A week in the life of the ‘new normal’ sixth form

In the past two weeks, high schools, sixth forms and colleges have opened their doors once again to welcome back the whole cohort after, what was practically, a sixth month long holiday. So, what’s changed and what’s stayed relatively the same? And what could recent changes in the UK mean for the future of this academic year?
For all students in the UK, our last day of school came a few weeks into March, and those of us who didn’t return for those few days in the summer (for reasons such as living with vulnerable family members or anxiety over the coronavirus) this September will be our first time physically back in school. (I’ve made two previous blog posts about living as a student during lockdown and the catastrophe that was results day, so if you are interested in those I’ll leave them linked at the end of the post). As if the first day back from summer break didn’t hold enough anxiety for some of us, we have to return into what feels more like a hospital than a school – or so I thought…
New school rules
Due to the current circumstances right now, schools have been told to put protective measures in place in a feeble attempt to follow government guidelines and limit the possibility of a COVID outbreak. I say feeble attempt, as my school at least, doesn’t seem to know exactly what to do at the moment – and the measures in place are not exactly effective or logical. Don’t get me wrong, everyone is just as clueless when it comes to knowing which restrictions are truly effective and which aren’t, so I give the teachers full credit for at least trying to be safe, yet what they are trying seems very contradicting. For starters, each year group is supposed to be one big ‘bubble’. When going outside for break, the younger years are herded into their own ‘factions’ on the school field, in order to stick within their year group bubble. Additionally, students are only ever going to have classes with people in their year group, so the only students they should mix with are others in their year. However, there are two glaring issues with this ‘solution’. Firstly, when students are travelling in the corridors between class, they’re mixing with practically every year group in those claustrophobic, traffic jam prone halls. The one-way system prevents students from facing each other I suppose, but I’ll expand on that later. The other issue with the year group ‘bubbles’ is the fact that if it happens to rain (which trust me is a common problem in Wales, the country in the UK which has the largest rainfall in mm out of the other countries) then the whole cohort will be shepherded in to one of the two dinner halls, where they’ll be forced crowd in one large group and mingle with other years – which obviously completely contradicts the bubble solution altogether.
Now, onto the one-way system as promised. Summed up simply, it really doesn’t make much sense. I understand that in going one way, students are not facing each other so germs are less likely to spread. However, the fact that no students are wearing masks defeats the purpose, as whichever way you’re walking you’re inevitably breathing the same air in close proximity. I doubt that making masks compulsory in the corridors will make much of a difference. Also, there is the fact that no one sticks to the one-way system when there are no chaperones to see you ‘rebel’.
The one thing that I feel like makes sense is wiping down surfaces, computers, chairs, and all communal equipment in general to ensure that everything is as sanitary as possible. Then again, I suppose, it doesn’t make much of a difference when every other rule isn’t being followed. We’re not exactly distancing when we’re sat shoulder to shoulder in lessons.
So, these days it’s hard to know what is within ‘guidelines’ and what isn’t – honestly, most people are just picking and choosing when to follow them. In a way, it’s hardly a ‘new normal’; it’s more like normal with a dash of hand sanitiser.
What does the future of the academic year look like?
Of course, as we’ve seen for six months now, no one is any good at predicting the course of this virus and what glorious surprises it has in store next. Every future plan is unstable at the moment, and that definitely does not exclude education. As numbers and the infection rate is starting to increase again in the UK (despite the deaths not significantly rising too) and we’re approaching a sort of ‘second wave’ of COVID, two week localised lockdowns are looming, and the possibility of exams taking place is on the ropes. Rumour has it is that exam boards are planning to push back exams next year, to allow students extra study time to make up for potentially missing even more of our education. Exam boards have already taken out small portions of exams to lower the content in the course slightly, which I think is definitely a step in the right direction so far. As for my sixth form, we’re being given mini assessments and mocks every few weeks, so in case of the event of cancelled exams again next year, teachers will be able to give the exam boards proof of what level we have been working at all year. Again, even if it will be a bit of a stress to keep up as high-level grades as possible on a weekly or monthly basis, it is also a good tactic for the possibility of predicted grades. So as the future of this academic year is still hazy, I’m trying to prepare for the worst just in case!
My opinion
Thus in my opinion (not that anyone explicitly asked for it) although this year is going to be a bit rocky, I think that we need to just face it head on, and really appreciate the times that we are physically in school. It’s a bit bitter sweet for me really, as I’m in my final year now and, like many others, I feel as if I’m being robbed of all the fun and, as odd as it sounds, the ‘normal’ stress of year 13. In terms of following or not following guidelines, students are less likely to be majorly affected if catching the coronavirus, especially now that it is ‘less deadly’ than it was in the beginning. With that logic, I think that schools can afford to be a bit more lenient with following guidelines, and I think that education should be a priority when looking at what can still go ahead in lieu of the rising cases in the UK. That being said, we should all make sure to stay safe and make logical choices when considering our actions.
What do you think about the guidelines in place at your school or college? Do you agree with them, and are they even being followed? Start a discussion in the comments!
Coronavirus reflection - being a student in lockdown
A level results day 2020... what went wrong?
#school#Sixth Form#college#back to school#Corona#coronavirus#a level exams#exams#student#student life
6 notes
·
View notes
Text
Pluralistic: 21 Mar 2020 (Cool Tools, scientists predict cooperation, Don't Look for the Helpers, after the crisis, a people's bailout, judge vs unicorns, Marc Davis's Haunted Mansion)
Today's links
My appearance on Cool Tools: My favorite gadgets.
UK emergency science panel predicts mass altruism: Reality has a well-known collectivist bias.
Don't Look for the Helpers: The text version of my essay for the new Nightvale anxiety podcast.
After the crisis, a program for transformative change: Pandemic reveals the systems' failures, and what to do about them.
Pandemic stimulus, realpolitik edition: Stephanie Kelton and AOC on a people's bailout.
Beautiful judicial snark: "No, your unicorn trademark is not an emergency."
Marc Davis's Haunted Mansion: What if Marc Davis had sole control over the ride's design?
This day in history: 2005, 2010, 2015, 2019
Colophon: Recent publications, current writing projects, upcoming appearances, current reading
My appearance on Cool Tools (permalink)
This week, I appear on the Cool Tools podcast to discuss my favorite, most indispensible gadgets and services and why I love them.
https://kk.org/cooltools/cory-doctorow-science-fiction-author/
My top picks were my Crkt Snap-Lock knife – a one-handed-opening, lightweight, super versatile pocket knife that I carry everywhere.
https://www.crkt.com/snap-lock.html
I also chose my Chinese OEM underwater MP3 player. I swim every day for my chronic pain maintenance and this is how I make it bearable, getting through 1-2 audiobooks/month.

https://www.amazon.com/exec/obidos/ASIN/B00GWV6GUO/cooltoolsshow-20
My third choice was Libro.fm, the DRM-free, indie-bookseller friendly way to listen to audiobooks. Basically the same catalog as Audible, at the same price, the only difference being that buying from them supports neighborhood booksellers, not Amazon.

It was a really fun! @Frauenfelder and @kevin2kelly are super smart about gadgets.
Here's the MP3:
http://tracking.feedpress.it/link/7810/13374488/779800513-cool-tools-218-cory-doctorow.mp3
UK emergency science panel predicts mass altruism (permalink)
SAGE is the UK Government's Scientific Advisory Group for Emergencies. This is their hour to shine.
They have just published a spectacular, plain-language set of technical reports on the pandemic.
https://www.gov.uk/government/groups/scientific-advisory-group-for-emergencies-sage-coronavirus-covid-19-response
This is the most interesting: "on risk of public disorder."
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/873736/08-spi-b-return-on-risk-of-public-disorder.pdf
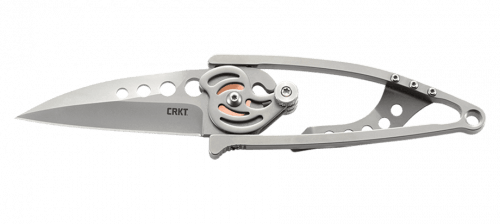
The expert panel affirms the conclusions of Rebecca Solnit in her indispensable book "A Paradise Built in Hell," a closely researched history of disasters that finds that they are the moment in which people spring to the aid of their neighbors.
https://www.newyorker.com/magazine/2009/10/05/a-paradise-built-in-hell
SAGE's expert panel on disasters: "large scale rioting is unlikely. It is rarely seen in these circumstances. Acts of altruism will predominate, and HMG could readily promote and guide these."
"Where public disorder occurs, it is usually triggered by perceptions about the Government's response, rather than the nature of the epidemic. A perception that Government response strategies are not effective in looking after the public may lead to an increase in tensions."
"Promote a sense of collectivism: All messaging should reinforce a sense of community, that 'we are all in this together.'"
For decades, Britain has been poisoned by Margaret Thatcher's sociopathic maxim, "There is no such thing as society."
It turns out that reality (and pandemics) has a well-known collectivist bias.
Don't Look for the Helpers (permalink)
I wrote a short essay about how I'm coping with The Current Situation for Our Plague Year, a new podcast from Joseph Fink of Welcome to Nightvale, called "Don't Look for the Helpers".
https://pluralistic.net/2020/03/17/pluralistic-17-mar-2020/#ourplagueyear
Today, PM Press published the essay in a new digital collection, "All We Have Is Each Other."
https://www.pmpress.org/blog/category/blog/all-we-have-is-each-other/
"Assuming things will break down does not make you a dystopian. Engineers who design systems on the assumption that nothing could go wrong aren't utopians, they're idiots who kill people. 'Nothing could go wrong' is why there weren't enough lifeboats on the fucking Titanic."
"Every disaster ends with mutual aid. By definition. That's the only way a disaster can end: with people pulling together. If there's one lesson to take from Mad Max, it's that pulling apart only deepens the crisis, and the it will not end until we pull together."
"I've been telling stories of humanity rising to crisis for decades. Now I'm telling them to myself. I hope you'll keep that story in mind today, as plutocrats are seeking to weaponize narratives to turn our crisis into a self-serving catastrophe."
https://www.pmpress.org/blog/2020/03/19/dont-look-for-the-helpers-by-cory-doctorow/

After the crisis, a program for transformative change (permalink)
The Current Situation has revealed deep cracks in our system: replacing public transit with gig economy drivers who don't get health care or sick leave; the gig economy itself; the lethal inadequacy of private-sector broadband and private-sector health-care, and beyond.
The fact that we can simply abolish data-caps (without networks falling over) and the liquid ban (without planes blowing up) reveals that these supposed existential threats were, in fact, arbitrary, authoritarian, rent-seeking bullshit.
https://pluralistic.net/2020/03/14/masque-of-the-red-death/#security-theater
The people who've spent 40 years convincing us that we're just not free-marketing hard enough continue to insist that all of these problems are merely the result of not having fully dismantled the state (so much for "state capacity libertarianism"):
https://www.bloomberg.com/opinion/articles/2020-03-20/coronavirus-killed-the-progressive-left
They're licking their chops for a 2008-style reboot: eviscerating public services, immiserating workers, fattening plutes and dissolving regulatory safeguards.
It's a playbook developed by Milton Friedman: the scheme to have "ideas lying around" when crisis strikes.
But as Naomi Klein reminds us, the Shock Doctrine cuts both ways. The manifest failures of plutocracy in the Great Depression got us the New Deal and the "30 Glorious Years" of shared prosperity and growth.
https://pluralistic.net/2020/03/17/pluralistic-17-mar-2020/#disaster-socialism
We haven't been idle since 2008. We have "ideas lying around" too. Ideas for a just and resilient society that reorients human life around sustainable and just practices. Motherboard's editorial staff gives us a manifesto for that society, so that this crisis doesn't go to waste:
https://www.vice.com/en_us/article/wxekvw/the-world-after-coronavirus-healthcare-labor-climate-internet
Free and universal healthcare ("healthcare is a basic human right" -B. Sanders)
Abolish ICE and prisons ("ICE is now a public health hazard")
Protect and empower labor ("Without these protections, everyone's safety and health is put at risk")
A healthier climate ("If the 2008-09 financial crash is any indicator, carbon could shoot right back up as soon as the crisis is over")
Fast, accessible broadband ("Community owned/operated broadband networks, long demonized and even prohibited by law are looking better than ever")
Smash the surveillance state ("This pandemic mustn't be used to infringe on the civil liberties and privacy of millions")
Billionaire wealth ("They're sending people to work while jetting off to luxurious doomsday bunkers, getting Covid-19 tests while normal people can't, and also singing 'Imagine' from bucolic getaways.")
Public transit that works ("Congress is poised to prioritize bailing out airlines and the cruise industry before it takes a look at public transit")
The right to repair ("Right-to-repair has become a matter of life and death.")
Science for the people ("We were caught flat-footed by a fixation on 'innovation' and lack of public options")
The future will not be like the past. Whether it is worse or better is our choice to make. It is in our (well-scrubbed) hands.
(Image: Jolove55, CC BY)
Pandemic stimulus, realpolitik edition (permalink)
I've been thinking a lot about what a covid stimulus package could and should look like, and what the possible failure modes and transformative changes could be. Obviously, there's real risk of inflation if handled wrong, because production has halted, so more money could end up chasing fewer goods. That gets ugly quick.
https://pluralistic.net/2020/03/18/diy-tp/#covid-stimulus
Then there's the risk that we just infuse trillions of no-strings-attached dollars into the finance sector, who use it to make our society even more brittle and unstable by hollowing out reeling companies and grinding down brutalized workers.
https://pluralistic.net/2020/03/19/gb-whatsapp/#peoples-bailout
Writing about this stuff in public makes a lot of Twitter people with "investor" in their bios very, very angry. They want giant bailouts for the companies they own stocks in, not transformative change. They use the neolib tactic of throwing out a lot of jargon to instil a sense of your technical illiteracy. Complexity is a con-artist's go-to tactic, after all – it's why proposition bets are so complicated, so you can't do the odds in your head (see also: craps tables).
But not every economist believes that sociopathy is pareto optimal. Leading lights like Stephanie Kelton, the mother of Modern Monetary Theory, who can go toe-to-toe with oligarch-apologists from the Chicago School, explaining how public debt really works.
Kelton and AOC appeared on this week's Deconstructed podcast with Mehdi Hasan to discuss the true scale of the bailout that will be needed (far more than $1T) to get the economy working again. That number can come down (by lowering working peoples' outgoings through rent/mortgage/student loan holidays, etc). But the lesson of 2008 is that to be credible, stimulus must be transparent and aimed at the public good, not the donor-class.
https://theintercept.com/2020/03/20/deconstructed-podcast-alexandria-ocasio-cortez-coronavirus-economy/
https://dcs.megaphone.fm/FLM7803427023.mp3
Otherwise, Congress risks having its hands tied: it might inject an inadequate and corrupt stimulus that benefits its cronies, then be unable to follow that on with a people's bailout that would help us all.
AOC: "Look at this kind of trash pile of legislation the Republicans have just introduced. I've never seen such a thing in my life of, we're going to give the neediest people less. And we're going to give people who are you know, need help but don't need as much help more."
Kelton: "What people mean when they say, you know, oh, Senator Sanders, you want Medicare for All or you want to make public colleges and universities tuition free, you want to cancel student debt, how are you going to pay for it? Where is the money going to come from? What that means in beltway speak is how are you going to offset all of that spending with new revenue from somewhere else, or by spending less in defense or some other category, the budget?"
"When you do a piece of legislation that's 'paid for,' it means you're putting the 50 billion in and it goes to some parts of the economy, and you're taking 50 billion out of some other parts of the economy so that you're not deficit spending."
"We've been so badly educated to respond to deficits as something that's fiscally irresponsible, reckless. It isn't. The government is committing to dropping dollars into the economy without ripping them right back out again. It's exactly what we want them to do right now."
Kelton's work on Modern Monetary Theory is transformative. Her lectures present both a powerful descriptive account of how money works in the economy and a prescriptive account of how we can use that knowledge to make a better, more prosperous world.
https://www.youtube.com/watch?v=WS9nP-BKa3M
She has a new book about this coming in June, The Deficit Myth. This would be a good time to pre-order it. These are scary times for writers with books about to come out (signed, I have three new books out in 2020).
https://stephaniekelton.com/book/

Beautiful judicial snark (permalink)
As Ken "Popehat" White is fond of reminding us, no one snarks quite like a federal judge. And despite being a Trump appointee, Steven C Seeger manages to rip off a couple zingers in this ruling.
http://loweringthebar.net/2020/03/unicorn-case-not-an-emergency.htm
At issue: Art Ask Agency is upset that someone is counterfeiting their unicorn-logo merch, such as this unicorn-scented candle:
https://artaskagency.com/our-licenses/anne-stokes/unicorn-candle/
But Illinois is in covid lockdown, so its case against a bunch of John Doe (alleged) counterfeiters is on hold. Their lawyer has sent a string of motions to the court asking for an emergency hearing so they can proceed, despite the fact that the court clerks are operating on reduced staff and only dealing with matters of the utmost urgency.
The judge is Not Impressed: "At worst, Defendant might sell a few more counterfeit products in the meantime. But Plaintiff makes no showing about anticipated loss of sales. One wonders if fake fantasy products are experiencing brisk sales at the moment."
The judge takes notice of the time a telephonic hearing would consume, "especially given the girth of the Plaintiff's filings."
"Plaintiff argues that it will suffer an 'irreparable injury' if this court does not put a stop to the infringing unicorns and knock-off elves."
"The world is facing a real emergency. Plaintiff is not."
(Image: Karen Neoh, CC BY)

Marc Davis's Haunted Mansion (permalink)
Along with Passport to Dreams Old and New, the Long Forgotten Blog is the best source of information on the history, design, and evolution of Disney theme-parks.
https://passport2dreams.blogspot.com/
But Long Forgotten focuses on a single ride, the glorious, brilliant Haunted Mansion.
The history of the Haunted Mansion was completely upended in late 2019, when Christopher Merritt published his "Marc Davis in His Own Words," a two-volume compendium of journals and interviews with the legendary Imagineer, who was Merritt's mentor.
https://books.disney.com/book/marc-davis-in-his-own-words/
This is probably the best book of Disney/theme-park history ever published, and that's no surprise, as Merritt has already written the definitive history of Knott's Berry Farm:
https://www.angelcitypress.com/collections/authors-christopher-merritt
And Pacific Ocean Park:
https://www.yesterland.com/pacificoceanpark.html
Merritt is an Imagineer, an artist, and a historian, who has direct, lifelong connections with the original Imagineering team. He has unparalleled access, inside knowledge and perspective. So yeah, that is a fucking great book.
Marc Davis was the best character designer in the original Imagineer cohort: he created the Country Bears, the Pirates, and the Haunted Mansion ghosts. He was a spectacular visual gag master, too. And he was one of the (many) legendary Imagineers who had a hand in designing the Haunted Mansion. That ride had so many different iterations, drafts, plans and schemes, and the final product is so wonderful in part because of their remnants.
But Davis actually designed a full-on Haunted Mansion attraction, from start to finish, and those plans are kicking around. Based on those, Long Forgotten has created a narrative account of what it would be like to tour "Marc Davis's Haunted Mansion."
https://longforgottenhauntedmansion.blogspot.com/2020/03/marc-daviss-haunted-mansion.htm
It's…interesting. Davis had some really fun ideas like meeting up with a talking bust (or raven).

And there are great gags (Davis designed the "three-part" stretching portraits, after all).
I mean. this would have been so freaking boss.
But the real meat is something called "The Most Dangerous Ghost":
"The final picture is perhaps behind black drapes which raise as the ghost host calls out attention to it. As the drapes part we see a painting that has everything in it except a figure. There is perhaps a vague image where the figure should be. The ghost host reacts in a frightened manner. He explains that this is terrible because this is the most dangerous ghost in the mansion. When he climbs out of his picture he mingles with the guests until he has turned one of them into a ghost. He describes the ghost's appearance and its omnipotent powers. He suggests again that everyone should stay in a tight group; this evil ghost loves to pick off stragglers. He suggests that the group be wary of sliding panels, gusts of cold air and etc."
Long Forgotten: "The MDG character undercuts the intellectually sloppy notion that all Davis cared about was making the HM funny."
LF goes on to make a good case that Davis wanted to incorporate many of Rolly Crump's gorgeous "Museum of the Weird" designs into his Mansion.
Davis's seance room seems to flirt with MDG some more: "The presence of the villain ghost makes itself felt and these older retired ghosts are frightened. Whatever we have used to indicate the nearness of the villain ghost would be repeated here."
Davis once planned for a Mansion filled with "working class ghosts" (carpenters, soldiers, boxers, etc). The only ones that survived were the coachmen in the graveyard sequence.
And his bride sequence was very explicit about wedding-night murders, culminating with MDG manifesting amid the guests: "He starts a wild mocking laugh. It clouds up outside. The curtains blow inward. It starts to rain along with thunder and lightning. "Outside we see a figure take form and it moves into the room. The rain comes into the room with the figure and a pool of water forms around its feet."
This is gorgeously scary, but as Long Forgotten points out, it has little re-play value (similar to Tomororwland's Alien Encounter): "The gag about the Ghost Host revealing himself as the Most Dangerous Ghost has the obvious disadvantage that it can surprise you only once. Pretty soon everyone knows the 'secret,' and as its usefulness as a genuine shock or scare tactic fades its status as pure camp inevitably increases."
That all said, "We learn what we should already know but sometimes forget: Marc Davis was never an imperious, one-man show. He was a team player. He interacted creatively with the work already done by previous Imagineers, displaying in this outline nothing but respect for what was good in what they had done."

This day in history (permalink)
#15yrsago Disney busts amateur Disneyland tour guide https://web.archive.org/web/20050323133504/http://jimhillmedia.com/mb/articles/showarticle.php?ID=1356
#10yrsago James Randi is gay http://archive.randi.org/site/index.php/swift-blog/914-how-to-say-it.html
#5yrsago Windows 10 announcement: certified hardware can lock out competing OSes https://arstechnica.com/information-technology/2015/03/windows-10-to-make-the-secure-boot-alt-os-lock-out-a-reality/
#1yrago Two arrested for hiding cameras in motel rooms and charging for access to livestreams https://edition.cnn.com/2019/03/20/asia/south-korea-hotel-spy-cam-intl/index.html
Colophon (permalink)
Today's top sources: Ok børge (https://twitter.com/forteller), Beyond the Beyond (http://www.wired.com/category/beyond_the_beyond/).
Currently writing: I've just finished rewrites on a short story, "The Canadian Miracle," for MIT Tech Review. It's a story set in the world of my next novel, "The Lost Cause," a post-GND novel about truth and reconciliation. I've also just completed "Baby Twitter," a piece of design fiction also set in The Lost Cause's prehistory, for a British think-tank. I'm getting geared up to start work on the novel next.
Currently reading: Just started Lauren Beukes's forthcoming Afterland: it's Y the Last Man plus plus, and two chapters in, it's amazeballs. Last month, I finished Andrea Bernstein's "American Oligarchs"; it's a magnificent history of the Kushner and Trump families, showing how they cheated, stole and lied their way into power. I'm getting really into Anna Weiner's memoir about tech, "Uncanny Valley." I just loaded Matt Stoller's "Goliath" onto my underwater MP3 player and I'm listening to it as I swim laps.
Latest podcast: The Masque of the Red Death and Punch Brothers Punch https://craphound.com/podcast/2020/03/16/the-masque-of-the-red-death-and-punch-brothers-punch/
Upcoming books: "Poesy the Monster Slayer" (Jul 2020), a picture book about monsters, bedtime, gender, and kicking ass. Pre-order here: https://us.macmillan.com/books/9781626723627?utm_source=socialmedia&utm_medium=socialpost&utm_term=na-poesycorypreorder&utm_content=na-preorder-buynow&utm_campaign=9781626723627
(we're having a launch for it in Burbank on July 11 at Dark Delicacies and you can get me AND Poesy to sign it and Dark Del will ship it to the monster kids in your life in time for the release date).
"Attack Surface": The third Little Brother book, Oct 20, 2020. https://us.macmillan.com/books/9781250757531
"Little Brother/Homeland": A reissue omnibus edition with a new introduction by Edward Snowden: https://us.macmillan.com/books/9781250774583
16 notes
·
View notes
Text
Year 2 - Initiate
At the time of this writing, I'm sitting in my office on the first day of classes outside of isolation. We've successfully welcome all of our students back to campus, isolated for a week, completed two COVID tests, and had our first full-campus events for the year.
I can't begin to explain how different our family is feeling so far this year. It's a much older family - the kids are 18, 17, 17, 16, 15, 14, and 14 - and this, along with changes in the student constellation - has made a world of difference in how our house and family feels. Though we loved things about our family last year, working with that group was overall a very stressful experience, with more exceptions to rules and expectations that I could possibly count, unstable students who expected the world to revolve around them at all time, and having to mediate often negative interactions between students constantly. This year, our group gets along, and when they disagree, they can calmly discuss the disagreement and compromise with each other. Every student is at least moderately independent and understands that, sometimes, the needs of the group will come before their own personal needs. And, most importantly, they want to connect and see each other as human beings with feelings and needs, instead of someone who is just put in their way to annoy them and make their life harder.
This past weekend, for example, Ryan left to take a large group of new students and helping students to the titidorf, a campground near school, which left me on duty for the house with only four returning students in it. We ate dinner on Saturday night - free seating, so I ate with my teacher friends - and then the kids came back to the house for a bit. Three of the four left for Stuckli, this "dance club" the kids host on some Saturday nights, and one (who is too young to go) stayed behind and relaxed in her room. After Stuckli, one of the kids came in the apartment to tell me he was back and to ask if we could all go stargazing, as the sky was "too beautiful to miss tonight". I said we could, and he rushed off to shower before coming back with the rest of the students a few minutes later. Then, we all went up onto our balcony in the apartment, they climbed on the roof wrapped in blankets, and we just chatted and looked at the stars with the Milky Way in full view. The next morning, we ate brunch - free seating again - and then decided to have family bonding by watching The Green Mile, which was one of the kids' favorite movies. We ate popcorn and ended the movie all crying on the couch, sharing hugs before they went to relax for the rest of their afternoon.
Our family isn't without issue: We have two students who weren't particularly wanted in other families, students with histories of eating disorders, self-harm, anger issues, panic attacks, and 5/7 who go to some kind of therapy or counseling on a regular basis for specific issues and needs. But, when I imagined coming to the Ecole and doing family work, this is what I imagined. A life where I didn't have to feel constantly on guard, constantly ready to fight with a kid about who even knows, constantly ready to put out fires without any student leaders who were able to step in when we needed it. I wanted to be around students who wanted to be around me and who didn't feel in competition with each other for attention, and who were able to work together and collaborate, as well as students who had a genuine interest in each other, their cultures, their experiences, and the things that have brought them here. So far this year, it seems that we have that.
I had a moment last night after our family meeting that I hadn't felt in a long time: At Williams, I struggled with long breaks because I was bored, because I missed the kids, missed Alcala, missed the regularity of my normal life. Last year, I took every opportunity I could to get away from the family because I found it to be so incredibly stressful. This included eating meals and brunch with the family downstairs many weekends and going shopping off campus frequently just to get away. I didn't know what to do with this desire, because I'm so used to really loving my work, and spent much of the year feeling bad about wanting so much distance from a type of relationship that I used to really value. Last night, we made plans for one of our girls to be in charge of brunch this weekend, and after our meeting, I realized that Ryan and I will be off duty this weekend and wouldn't HAVE to go to brunch. For the first time since we came to the Ecole, I felt conflicted because I WANTED to be with the kids instead of doing everything I could to create more space between us. It feels good to be back.
I also had a really interesting first linguistic experience this weekend: While watching the movie, I realized I was the only American there, and Ryan and I are the only American's in the family. One of the characters in The Green Mile is Cajun, speaks French in the movie, and I was asked where he was from and why he sounded like he did. Later in the film, another student asked about John Coffey's accent - "is it old English or bad English". In both cases, I was the one with the cultural context to help them understand the characters and the stigmas behind their accents.
Otherwise, things are moving along! We have a new German Shepherd - we called him Jordy after Jordy Nelson, the former Green Bay Packer who rarely missed a catch - and have made the decision in the last few days to keep him. He's about 14 months old and has much more energy than Al did, and he came from a previous home where he didn't have many rules, so he's severely lacking in manners. But, the kids love him and he loves them, so we'll keep working with him to get his manners in check.
0 notes
Text
Google Explains Featured Snippets Volatility
Google eliminated a lot of highlighted pieces toward the beginning of March 2021 then they returned. Google's John Mueller remarks on why perceivability of highlighted pieces changes.
Included Snippets Search Volatility
Toward the start of March included pieces appeared to vanish from the web index results pages (SERPs). Some were calling it memorable lows.
However up to this point there hasn't been a lot of data from Google. Our Digital Marketing course in Pune gives deeper information about Digital Marketing course.
Google's John Mueller clarified the reasons why highlighted scraps aren't generally steady in a new available time home base. to know more about the Digital Marketing course, go through the course.
Was Featured Snippet Volatility Deliberate?
Somebody inquired as to whether the evacuation of the highlighted pieces was deliberate or if there was something different going on. Typically changes are steady and not so apparently emotional.
The Question:
"Simply contemplating whether that was conscious on Google's side to diminish included scraps from appearing or on the off chance that it was possibly… for another explanation that may be going on?
Simply contemplating whether there's any… reasoning or on the off chance that you know whether… possibly it was a symptom of another change?"
John Mueller didn't remark on the new highlighted scraps unpredictability. However, he offered a clarification of why included pieces can appear to be unstable.
Of interest is the point at which he makes reference to that they are set off and that Google attempts to refresh the "edges" for setting off them. You’ll get the opportunity to enter the IT world through the Digital Marketing course.
Screen capture of Google's Mueller addressing highlighted bits question
John Mueller replied:
"I don't have the foggiest idea. … The highlighted bits and rich outcomes by and large, those sorts of things can vacillate after some time.
What's more, I realize the groups are continually dealing with those highlights and attempting to calibrate the setting off. In Our Digital Marketing course in Pune, We provide Affordable Fees and practical knowledge.
So when we would show them or when we wouldn't show them, in some cases the setting off changes over the long run that we only sort of decrease the edge generally or that we change the center a tad and say like not so much here but rather more here. Here and there that occurs across geologies or dialects.
However, these sorts of changes from our side are basically ordinary natural changes in search, how they can generally occur."
Explanations behind Changes in Search
Natural changes in search can be a wide assortment of things.
As a rule, Google's inquiry center will in general adjust towards:
Degrading manipulative strategies
Fulfilling client assumptions
Showing valuable substance to clients
Reacting to changes in search plan (move in what watchwords mean)
Reacting to changes in client conduct (Covid, travel, telecommute)
We also provide 100% Job to our students with Best Digital Marketing Course.
0 notes
Text
tired and weak
I don’t know if I’m going to be able to bounce back.
I don’t know if I’m stable or functional right now.
I am no longer spending days weeping, getting the violent psychotic meltdowns or other overtly physical symptoms but I don’t think I’m okay.
But I can’t keep myself shut up not doing any of the things I like to do online because isolating myself is not helping me. I only did it because my psychotic episode was causing me to hurt my friends. I did this for them, but it’s not helping me beyond cutting off things that my psychosis could latch onto. It is more than capable of doing it on its own.
I am coming to terms with how my situation is not healthy, it is not sustainable, and it is not safe.
I feel that I am not safe and I do not have anyone I can trust. That my environment is unhealthy and is continuing to retraumatize me and that I am not receiving adequate care.
I am unable at this time to tell how much of this is delusion and how much is that people in my life are actually a danger to me. Psychosis is like that. But things have been getting clearer on many relationships and issues.
My roommate told me that he is going to be writing a letter to the landlord to try and convince them that I need to get my service dog and if that works I wouldn’t need to take it to court. But I can’t tell if that’s just an empty promise. I feel like I am being told what I want to hear in an effort to keep me under control. That I am being satiated just enough so I don’t get violent or kill myself. But that my environment is never going to improve in its current state.
There’s been a lot of empty promises. And with my psychosis makes the already difficult issues impossible to navigate.
I am very disabled. I know I type really well and talk a big game, all bark and no bite though basically. Truth is I am unable to take care of myself. And with covid and me being high risk I don’t know if I am capable to put myself into a new situation/environment where I can thrive at this time. I am at the mercy of whoever I can find as a guardian. This is not healthy, and is something that I cannot yet find an escape from. All that it seems I can do is hold on and wait until an opportunity presents itself, to submit to the freeze and fawn response until I’m able to make my move. A move I will need support that I can’t even begin to wrap my head around to make.
Obviously “cringing and waiting” isn’t something that severe mental illnesses are going to be play nice with. And this is why I am unstable.
I must stress that I am not an independent. I am not functional in society as an independent. And even with my service dog this may stay the same financially. I am stunted, slow, whatever gentle word you want to call mental retardation. And that on top of debilitating mental disorders and trauma disorders prevents me from functioning on my own.
I cannot have a job. I cannot leave the house by my own. I have a learning disability surrounding numbers, time, math, etc. I am slow enough that it is extremely difficult for me to go about daily adult tasks that most people take for granted. My physical body being shit just ads to that and makes me slow in an equally useless and infuriating way.
It is very easy to take advantage of me. And the combination of me being a dependent when combined with that is dangerous for my health.
I will be making a doctor appointment for the explicit purpose of getting a note to try and pressure the landlord. I know that once me and my service dog are a working team more opportunities to become more independent and to get myself out of this situation will be presenting themselves. But nothing can happen immediately, yet at the same time I am suffering from things not being resolved immediately.
I am living in a way that is constantly exposing me to stress and pain. And I have acknowledged I need to get out of it but don’t yet have the means to know how.
I do have friends who may be capable of helping, but the virus has put a roadblock on that help for now.
Things like moving, programs for people with disabilities, hospital visits, etc. have all been made impossible by the virus.
I have ruled out moving back in with my mother. Even though she has improved and I definitely see her as a victim of abuse and living with undiagnosed mental illnesses of her own it just is not safe for me to live with her.
The only thing I can do now is make the effort to try and protect myself from the things that are hurting me emotionally that I am currently incapable of getting away from.
And trying to push towards my dog.
Everything else is waiting for things to be capable of changing.
I have pinpointed what I believe triggered this week’s psychotic break. Residual trauma from the first Christmas spent knowing the holiday killed Zippy, combined with frequent exposure to traumatic stimuli and unhealthy power dynamics, financial and social stress, as well as an increased lack of support regarding being invalid.
I am not in a healthy situation.
I began to sniff out bad people with the intent to keep track of them to make sure they weren’t planning to hurt me. This is the same maladaptive strategy I have been using to make sure my birth father wasn’t planning to kill everyone at my mom’s house way back when. In reality, exposing myself to the evil culture of bad people is not helping me psychologically. And I am powerless to actually kill them like I wish I could. But I felt like I had some level of control knowing their every move after I have no control in the situations I am spending my daily life in. It’s like drinking a poison so you can ignore a gunshot wound. I wish I could treat the wound, but drinking the poison makes me forget about it for a while. Both are unhealthy, but the act of creating a new problem makes it easier to ignore the initial one that I have no ability to change. At the cost of my rapidly fraying mental stability.
My environment is not one that I can control. And it is not one that I can currently fix or leave.
For my safety I am not capable of going into detail about certain people and their effect on my health. Being a dependent means that this directly can threaten me at an already vulnerable time.
I need to get out of my current situation, but am incapable of doing so. This has caused an extreme amount of stress to build up to the point that my antipsychotics weren’t enough to keep me safe. I was told that even being on anti psychotics you can still experience episodes and down periods. Which is scary to think about.
But I have no avenue to change this situation at this time.
I do not know if I am fit to hold communications with people right now. I will not be returning to social groups until I am told explicitly that it is okay to do so. By my primary care physician, by my psychiatrist, and by the people I socialize with themselves. But I will now state that anyone may come to me with the explicit understanding that I don’t know if I am rational or mentally safe right now. You will be communicating with me at your own risk and understand that I may still be experiencing heightened amounts of unreality and delusions.
I am no longer experiencing violent symptoms. I have made the steps to prevent myself from doomscrolling and keeping tabs on my abusers. But I understand that I am not above the possibility of lapsing back into doing this.
I am now on my pain meds again. Being off them for an extended period of time was likely contributing to my psychological pain despite these meds themselves not being addictive, the relief they give me might have been.
I am currently only with 3 dolars in my bank account and 5 dollars cash. I will be getting paid in 12 days. I should have enough food to last me this long. It is stressful, but I was already anticipating this situation to happen at this time.
I am extremely sorry for allowing my delusions and sickness to hurt innocent people. It was not my intent to cause pain to others. Whilst I would like to explicitly remind people that my mental illness directly influences how I perceive reality and this can make it impossible to tell if I am justified in my actions at times, it still doesn’t make up for the pain it may cause in the process.
Friends have expressed pain at me saying that I am not recieving help and nobody is helping me despite them trying to support me online.
Please understand that I appreciate the energy you are sending my way, but I am explicitly venting about my living situation that you nor I have any way of fixing. In the future to help my friends not feel like I am ignoring their attempts at helping me I have created this disclaimer that I will be putting on posts about situations that online friends cannot help or change. I hope this will alleviate the pain of your efforts not solving my problems.

I appreciate everything people try to do for me, even if my mental illness makes me not see it at the time. I understand it is very difficult to be close to someone who doesn’t perceive reality properly all the time, and I may not always show it when I am being helped due to one issue being immediately replaced by another, but I do appreciate.
I have been told that despite me being clingy that I tend to push people away and isolate myself when I am hurting. This is because I was abused and treated badly for expressing clinginess. This included targeted stalking when I was still a minor. My brain had it beaten into me that if I was clingy towards people they would hate me and not want to be my friend. As a result I experience clinginess by violently wishing I could be close to them while trying to hide that from them and give them space. If anything this presents itself as persecutory jealousy. It is something I am trying to stop doing.
I also apologize for friends trying to do things with me, encourage me, socialize with me, and me being too exhausted to appreciate or join in. This is equal parts my distress at my living situation, my mental health, and my physical health. I spend most of my life far too exhausted to consistently socialize except for manic periods where I am desperate to do so. Again, the solution to this issue is post-covid changes to my living situation and the resources I have access to.
The point that I think sums this up though is that I cannot keep living like this. I will continue breaking down, I will continue having episodes, and I will continue lashing out. Violence is and always has been my answer to fear in situations I cannot change or leave.
I don’t know if there’s a way to fix this during covid, but I KNOW there isn’t an immediate way to fix this before I get my service dog.
Additionally: I do not want to be institutionalized, being trapped in a psych ward when you are not explicitly a danger to yourself or someone else will only make you worse, and calling police for “wellness checks” on disabled people who have ugly/scary mental illnesses will get them killed. Please understand that the system itself will not help me. I need to find a different solution. This unfortunately does involve jumping through hoops that I cannot at this time.
Again, I would like to state that I will be trying to return online, but I will not be engaging with people who haven’t explicitly come TO ME until my doctor, my psychiatrist, and those people themselves, let me know that I am allowed to do so. Please be advised that I may not currently be in a safe place mentally.
I will be trying to interact with art and media that I enjoy with minimal social contact with people outside of those who have come to me and are okay with that. Stressful things i will make every attempt to ignore.
0 notes
Text
Triple P: PT School, OP, Pandemic
2020.
Anyone currently living in it, doesn’t need a further description. After CIM in December, I was super motivated to get back into the groove of things. Anxiety beat me down and I didn’t have the marathon my body was capable of. I was in the best shape of my life, so I knew I wanted to take another stab at it as soon as possible. The plan was to run Grandma’s Marathon in June. Then I got into NYC, so I had hoped for a victory lap there. But training through the baseball season sounded unpleasant. I had done this once before, but with more structure and the ability to schedule my days a bit better. So what made me decide to take on the challenge? My first ‘P’
Last year, I felt as though I’d lost control of my life. My family had struggles and my body gave up on me. It was after a cascade of events that I finally broke and decided to apply to Physical Therapy school. I’d have to live on loans, step away from having a steady paycheck for 3 years, and yet again move. But at the age of 30, my priorities in life have changed and I can not achieve them anymore as just an athletic trainer. I needed 3 pre-req classes, which I was able to do completely online through my mom’s college. By the end of summer 2019 I had completed all necessary components of each application. The week before CIM, I received word that I had been admitted into one of those schools. Though it was not my top choice, I was going to PT school! In January I traveled to Colorado Springs and took part in a 2 week volunteer rotation at the US Olympic Training Center. What a fantastic experience, which can be an entirely separate post. Once I returned, I had heard back from all the schools I applied to and had started training for Grandma’s. 2020 was starting off in a very exciting way. And then, the second ‘P’ began.
In the beginning of March I started to experience pains in my lower abdomen and inner thighs. They were strange and weird, pains I had never experienced before. At the start of a run or any time I restarted say after waiting for the light to change, I would have sharp pain and pressure in my lower abdomen that would subside after a few strides. During long runs, in the later miles I would feel a constant sensations as if something was pulling on the bottom of my ‘butt bones’ (gluteal tuberosity for my anatomy nerds). After I ran, my inner thighs (adductors) would be extremely irritated the rest of the day. If I tired to stretch them, I felt nothing but pain. As my training progressed, the pain I felt when restarted caused my to shuffle my feet for some time before the sharp pains subsided. After a run, anytime I went on one leg my hips felt so unstable. I finally decided to seek the help of a pelvic floor PT. To my knowledge, if there is adductor pain the pelvic floor is involved, thus my reason for starting there. I was full functional, things just hurt. It took a while to come to a diagnosis but once she found one, I looked through my textbooks and agreed. I was suffering from Osteitis Pubis (OP). At the moment of diagnosis, I made the decision to stop running. I wanted for this to go away as soon as possible. It was April 29th. I know this because I ran a fantastic 5 mile tempo that still stands as my last activity on Strava. Grandma’s had been cancelled by then so I was doing a long road tempo every 3 weeks and working on shorter intervals on the track. I was back into the rhythm I had been in during the fall. Crushing workouts and loving my fitness. I was so excited to do something great. But I stopped running and took to my Elliptigo, which didn’t cause pain. Now for the sucky part of American medicine. I was loosing my health insurance in a month due to leaving my job. By the time I went to our team physician, I had 1 week left. He was unfamiliar of the condition so unfortunately didn’t offer any help. He advised me to see a specialist but it was too late. I spent the summer at home on the Elliptigo and bike. By the time I went out to school in mid-August, I was attempting to run. But by the time I tried to run a mile, the pain was coming back. I tried swimming but this created so much pain it hurt to walk again. Now having insurance again, I made a PT appointment with a sport specialty PT and an Ortho with a hip specialty. PT was working on progressing activities without pain, but I still felt a lot of abnormal things. The Ortho ordered an MRI and referred the to a specialist to rule out a sports hernia. In that visit, he and the radiology report of my MRI confirmed the OP diagnosis. I was told zero forms of activity for 12 weeks and I received an injection into my pubic symphysis. The injection relived the pain I had when lifting groceries or laundry, so that was a relief. After 12 weeks I could start progressing back. So for the past 2 weeks I have been progressing in time on the bike, every other day. It wasn’t until a few weeks ago that I stopped having bony pain. My hope is to start running at the start of next month, in a very very slow manner. Fingers crossed for me please!
The bright side of all of this, the final ‘P’. 2020 is the year of the pandemic. COVID-19 hit the US in March and our world has been out of sorts ever since. Both of my races were canceled but once I heal and the world heals, I will complete both races. I want to experience NYC as it was, in all its magic. I want a big pace group to crush Grandma’s with. I want to explore Minnesota and go out in public and feel safe on a plane. So this time has allowed me the time to heal. It’s allowed me time to commit to school. Though I am struggling with the appearance of my body, I am trying to be kind to it, with the long term health of my pelvic pubic bones in mind. Many runners careers are ended by OP. But many people are loosing their lives to COVID. I am being patient with my body, with strangers, and with the world. This all is not forever, it’s just now. Time heals all wounds.
To end on a perfect note, look at my mom’s new dog! Meet Tessie.

0 notes
Text
the fourth
hi again. it’s 10:41pm.
today was a fucking shit show. like appallingly so. my schedule was supposed to roughly look like this:
6-7am: get up, get ready, go get coffee
8-9: vet appt
9-10: breakfast, clean the kitchen for mom
10-11: post office, quick target run
11.30-4pm: read 2 chapters from textbook
4-5.30: run, shower, etc
5.30-7.30: read half a chapter, take some me time, idk
9pm-11pm: vibe time baybee
here’s how it turned out, roughly.
got coffee, it was very fun. barista is making it very hard to not have a crush on them by simply existing. how rude! took belle to the vet, everything was fine and dandy, as i figured. came home, had a bagel with spinach and eggs, cleaned the kitchen, it was fantastic. my brother ended up needing to ship out his christmas gift to his friend in croatia, but his classes weren’t over until 1:30, so i was like no worries! i’ll just go study for my final till your classes are over, just let me know. i ended up reading absolutely nothing and getting sucked into whatever fucking dumb shit exists on the internet. i also picked 3 therapists from our network and emailed them, introducing myself, and asking for quick interviews next week to see if we’re good fits, because i want to start going to therapy.
i was very excited by this development. it’s taken me over a year of saying i would go to therapy for me to finally get the courage to reach out. at about 12, i went into my parents’ room and said “guess what? i’m finally starting therapy!” and my mother, without missing a beat, says “oh, sorry we did such a bad job raising you. why do you need therapy? i thought we did a great job.” i was fucking stunned. i was like, “woah, no! this isn’t a reflection of you. this is me finally taking care of myself, i have personal things i need to work through. however, i do think that therapy is useful to anyone, and i think everyone should try therapy, at least once,” to which she had the brilliant insight, “there’s nothing wrong with me. should i just make something up about my family and go talk to a stranger about it? is that what you’re doing?” and my dad was like, “hey, that’s not what she’s saying” and my mom basically went off saying that i was weird for thinking that everyone should try therapy, and that i didn’t actually need it, and that it’s weird that i’ve been to therapy twice now, wasn’t complaining to that high school counselor that my parents were so strict enough for me?
those quotes are as close to word for word as i can get, i’m pretty sure it’s exactly what was said. the conversation lasted less than a minute, before i said “i think i need to excuse myself,” and walked away. i came and sat at my desk for i don’t even know how long. i looked at myself in my phone camera, and my face had become so translucent, it was almost green from my blood veins. i walked up to my window and contemplated trying to take the screen out to climb out, but i realized that if i did jump, it would be in my neighbor’s driveway, and that felt really insensitive, so i walked away. i sat back down at my desk and contemplated all the reasons my mom was right, before i realized that she wasn’t right. i have finally realized that i’m not fine.
i’m a depressed, suicidal 20 year old with undiagnosed adhd and ocd, a diagnosed eating disorder, and i’ve been a closeted lesbian for 13 years. i have every right to feel not okay. i didn’t need my mother’s permission to go to therapy, i have my own health insurance and i’m an adult who feels the need to ask for help, and that’s okay.
so i did what i do best, and spewed verbal diarrhea onto my private snap story about what happened and how i’ve been feeling these last few days. my brother’s classes ended early, so i took the opportunity to leave the house as soon as possible, and we took as long as possible to get to the fedex drop box, before i dropped him back at home and kept driving around, trying to process how i felt. i didn’t return either of my textbooks. i think i’m just going to send the one i bought in october after christmas, idk when it’s due but i can’t deal with the fucking lines at the post office anymore. i walked up to the post office, looked at the winding line into a building where the lovely hicks in my hometown refuse to wear masks, decided i wasn’t ready to get covid yet, and went to deposit cash so i could buy weed. i’ll just bite the $40 and buy the one that was due today, maybe i’ll give it to someone next semester.
i got home and responded to my friends’ responses to my story. i got an overwhelmingly positive and loving response from my friends. every single one stuck up for me, supported me, and shared that they’ve been feeling similarly. which is heartbreaking, i can’t believe that all of us have been dealing with this so privately! but anyway, that’s a tomorrow issue.
after i did that, i was ordering my weed when barista texted me, saying they had a question for me, which, when you have a major crush on a coworker with a girlfriend, is a very concerning text to receive. turns out, they just made me earrings! they walked their dog to my house and delivered the insanely cool polymer clay snake earrings. when i greeted them with a hug, they pulled me in so close, literally every part of their body was pressed against mine and my cheek rested on their head so perfectly. they’re on the shorter side, probably 3-4 inches shorter than me, but so strong. the way their arms felt around my back was wild, it was so tight but so gentle but so firm but so, so warm and soft. their hair was soft but frizzy and smelled like them and a little bit like an argan oil shampoo and a little like coffee. their eyes are so much more intensely ice blue in the sun. they hugged me the same way goodbye, and we chatted for a good portion of the evening, about our coworkers and being homeschooled and being nerdy high schoolers and the earrings.
i finally got one chapter done before dinner was ready at 8:30pm, which is late, even by our standards. after dinner, as i was decorating a sugar cookie named gerard, my parents kept making snarky comments about me being a stoner, and i was like yes, bold statements coming from the parents that just used my account to buy a tincture and edibles. anyway, i came upstairs and tried to read more but i’m too emotionally exhausted. eve ended up giving me a call, finally, and filled me in on her life, which is always crazy but i love to hear her voice, so it’s okay. then i learned a tiktok dance, which left me concerningly out of breath, considering it’s only been like 4 days since i ran and i can’t be that out of shape? but i showered and did my skincare routine and made sure my laundry was in the dryer before i sat down to start this.
it’s now 11:20pm, and i’m very proud to report that i am no longer angry with my mother for what she said to me. i’m sad that it’s how she feels, but i recognize that what i’m going through is something she will never understand, as a straight woman who, while prudish, has a healthy relationship with drugs and sex. i love her, and i forgive her, but i’m going to talk to her tomorrow and hold her accountable for gaslighting her already unstable daughter. what she did wasn’t fair, and it hurt. i know she probably feels insecure because she definitely does have things she knows she should go to therapy for, i know for a fact that she faced a lot of childhood and adolescent trauma and i would personally love to make sure she’s in a healthy place with it. but i can’t force her to, obviously, so i have to just hope that she doesn’t project on to me too much in the coming weeks.
i’m exhausted, and i think i’ll go to bed. i feel good about how i handled today, i caught myself in time to think through my actions before i did something completely unwarranted and unhinged. i know that at the time, my brain was in flight mode and i couldn’t cope immediately so i just followed the “i want to die” instinct because it was the strongest, but i still had enough of my logical brain in gear to have forethought. look at you go, prefrontal cortex! knowing that the part of me that is still healthy and wants to live is strong enough to put the kibosh on that maneuver is enough to give me hope that i will be okay someday. i never thought that i would be someone to be experiencing things like this. i really thought that people were being dramatic, if i’m being totally honest. now that i’m experiencing it, i understand. i’m sorry that i didn’t have more empathy.
0 notes
Text
— By Occupy Democrats | May 5, 2020

"I am a Covid ICU nurse in New York City, and yesterday, like many other days lately, I couldn’t fix my patient. Sure, that happens all the time in the ICU. It definitely wasn’t the first time. It certainly won’t be the last. What makes this patient noteworthy? A few things, actually. He was infected with Covid 19, and he lost his battle with Covid 19. He was only 23 years old.
I was destroyed by his clinical course in a way that has only happened a few times in my nursing career. It wasn’t his presentation. I’ve seen that before. It wasn’t his complications. I’ve seen that too.
It was the grief. It was his parents. The grief I witnessed yesterday, was grief that I haven’t allowed myself to recognize since this runaway train got rolling here in early March. I could sense it. It was lingering in the periphery of my mind, but yesterday something in me gave way, and that grief rushed in.
I think I was struck by a lot of emotions and realities yesterday. Emotions that have been brewing for weeks, and realities that I have been stifling because I had to in order to do my job effectively. My therapist tells me weekly via facetime that it’s impossible to process trauma when the trauma is still occurring. It just keeps building.
I get home from work, take my trusty companion Apollo immediately out to pee, he’s been home for 14 hours at a time. I have to keep my dog walker safe. No one can come into my apartment.
I’ve already been very sick from my work exposure, and I’m heavily exposed every day that I work since I returned after being 72 hours afebrile, the new standard for healthcare workers. That was after a week of running a fever of 104 even with Tylenol around the clock, but thankfully without respiratory symptoms. I was lucky.
Like every other healthcare worker on the planet right now, I strip inside the door, throw all the scrubs in the wash, bleach wipe all of my every day carry supplies, shoes and work bag stay at the bottom of the stairs.
You see, there’s a descending level of Covid contamination as you ascend the stairs just inside my apartment door. Work bag and shoes stay at the bottom. Dog walking shoes next step up, then dog leash, then running shoes.
I dodge my excited and doofy German shepherd, who is bringing me every toy he has to play with, and I go and scald myself for 20 minutes in a hot shower. Washing off the germs, metaphorically washing off the weight of the day.
We play fetch after the shower. Once he’s tired, I lay on the floor with him, holding him tight, until I’m ready to get up and eat, but sometimes I just go straight to bed.
Quite honestly, I’m so tired of the death. With three days off from what has been two months of literal hell on earth as a Covid ICU nurse in NYC, I’m having an evening glass of wine, and munching on the twizzlers my dear aunt sent me from Upstate NY, while my dog is bouncing off the walls because I still don’t have the energy to run every day with him.
Is it the residual effects of the virus? Is it just general exhaustion from working three days in a row? Regardless, the thoughts are finally bleeding out of my mind and into a medium that I’m not sure could possibly convey the reality of this experience.
There’s been a significant change in how we approach the critically ill covid-infected patients on a number of different levels over the last two months. We’re learning about the virus. We’re following trends and patterns. We are researching as we are treating.
The reality is, the people who get sick later in this pandemic will have a better chance for survival. Yet, every day working feels like Groundhog Day. All of the patients have developed the same issues. This 23-year-old kid walked around for a week silently hypoxic and silently dying. By the time he got to us, it was already far too late.
First pneumonia, then Acute Respiratory Distress Syndrome (ARDS), essentially lung failure. Then kidney failure from global hypoxia and the medications we were giving in the beginning, desperately trying to find something that works. Then learning that it doesn’t work, it’s doing more harm than good in the critical care Covid population.
Dialysis for the kidneys. They are so sick that your normal three-times weekly dialysis schedule is too harsh on their body. They’re too unstable. So, we, the ICU nurses, run the dialysis slowly and continuously.
They are all obstructing their bowels from the ever-changing array of medications, as we ran out of some medications completely during our surge. We had to substitute alternatives, narcotics, sedatives, and paralytics, medications we’re heavily sedating and treating their pain with, in an effort to help them tolerate barbaric ventilator settings.
Barbaric ventilator settings while lying them on their bellies because their lungs are so damaged that we have to flip them onto their bellies in an effort to perfuse the functioning lung tissue and ventilate the damaged lung tissue. Ventilator pressure settings that are so high that some of their lungs are being blown out completely in an effort to give them enough oxygen, because lung-protective ventilation measures aren’t working for these patients.
Lungs that are perfused with blood that doesn’t even have adequate oxygen carrying capacity because of how this virus attacks.
Blood that clots. And bleeds. And clots. And bleeds. Everything in their bodies is deranged. Treat the clots with continuous anticoagulation. Stop the anticoagulation when they bleed.
GI bleeds, brain bleeds, pulmonary emboli, strokes. The brain bleeds will likely die. The GI bleeds get blood transfusions and interventions.
Restart the anticoagulation when they clot their continuous or intermittent dialysis filters, rendering them unusable, because we’re trying not to let them die slowly from renal failure. We are constantly making impossible treatment decisions in the critical care pandemic population.
A lot of people have asked me what it’s like here. I truly don’t have adequate descriptors in my vocabulary, try as I might, so I’ll defer to the metaphor of fire.
We are attempting to put out one fire, while three more are cropping up. Then we find out a week or two later that we unknowingly threw gasoline on one fire, because there’s still so much we don’t know about this virus.
Then suddenly there’s no water to fight the fire with. We’re running around holding ice cubes in an effort to put out an inferno. Oh yeah, and the entire time you’ve been in this burning building, you barely have what you need to protect yourself.
The protection you’re using, the guidelines governing that protection, evolved with the surge. One-time use N95? That’s the prior standard, and after what we’ve been through, that’s honestly hysterical. As we were surging here, the CDC revised their guidelines, because the PPE shortage was so critical.
Use anything, they said. Use whatever you have for as long as you can, and improvise what you don’t have.
As we’re discussing medication and viral research, starting clinical trials, talking treatment options in morning rounds for your patient with the team of doctors and clinical pharmacists, suddenly, surprise! Your patient developed a mucous plug in his breathing tube.
Yes, that vital, precious tube that’s connected to the ventilator that’s breathing for them. It’s completely plugged. Blocked. No oxygen or carbon dioxide in or out. It’s a critical emergency.
Even with nebulizer treatments, once we finally had the closed-delivery systems we needed to administer these medications and keep ourselves safe, they’re still plugging. We cannot even routinely suction unless we absolutely have to because suctioning steals all of the positive pressure that’s keeping them alive from the ventilator circuit. One routine suction pass down the breathing tube could kill someone, or leave their body and vital organs hypoxic for hours after.
Well, now they’re plugged. We are then faced with a choice. Both choices place the respiratory therapists, nurses, and doctors at extremely high risk for aerosolized exposure.
We could exchange the breathing tube, but that could take too long, the patient may die in the 2-3 minutes we need to assemble the supplies and manpower needed, and it’s one of the highest-risk procedures for our providers that we could possibly carry out.
Or we could use the clamps that have been the best addition to my every day carry nursing arsenal. You yell for help, you’re alone in the room. Your friends and coworkers, respiratory therapists, doctors, are all rushing to get their PPE on and get into the room to help.
You move around the room cluttered with machines and life sustaining therapies to set up what you need to stave off death. You move deliberately, and you move FAST. The patient is decompensating in the now-familiar and coordinated effort to intervene.
Attach the ambu bag to wall oxygen. Turn it all the way up. Where’s the PEEP valve? God, someone go grab me the PEEP valve off the ambu bag in room 11 next door. We ran out of those a month ago, too. It’s all covid anyway, all of it is covid. Risk cross-contamination or risk imminent death for your patient, risk extreme viral load exposure for you and your coworkers, and most certain death for your patient if you intervene without a PEEP valve.
You clamp the breathing tube, tight. The respiratory therapist shuts off the ventilator, because that side of the circuit can aerosolize and spray virus too if you leave it blasting air after you disconnect. Open the circuit. Respiratory therapy attaches the ambu bag. You unclamp. Bag, bag, bag. Clear the plug. The patient’s oxygen saturation is 23% with a PERFECT waveform. Their heart rate is slowing. Their blood pressure is tanking. Max all your drips, then watch and wait while this patient takes 3 hours to recover to a measly oxygen saturation of 82%, the best you’ll get from them all shift. These patients have no pulmonary reserve.
All of our choices to intervene in this situation risk our own health and safety. In the beginning we were more cautious with ourselves. We don’t want to get sick. We don’t want to be a patient in our own ICU. We’ve cared for our own staff in our ICUs. We don’t want to die. Now? I’ve already been sick. I am so, so tired of the constant death that is the ICU, that personally, I will do anything as long as I have my weeks old N95 and face shield on, just to keep someone alive.
I’ve realized that for many of these patients in the ICU, it won’t matter what I do. It won’t matter how hard I work, though I’ll still work like a crazy person all day, aggressively advocate for my patients in the same way.
My coworkers will go without meals, even though they’re being donated and delivered by people who love and support you. Generous people are helping to keep local restaurants afloat. We can always take the meal home for dinner, or I can devour a slice of pizza as I walk out to my truck parked on the pier, a walk I look forward to every day, because it gives me about eight minutes of silence. To process. To reflect.
I’ll chug a Gatorade when I start feeling lightheaded and I’m seeing stars, immediately after I just pushed an amp of bicarb on a patient and I know I have at least five minutes of a stable blood pressure to step out of the unit, take off my mask and actually breathe.
Every dedicated staff member is working tirelessly to help. The now-closed dental clinic staff has been trained to work in the respiratory lab to run our arterial blood gases, so that the absolutely incredible respiratory therapists who we so desperately need can take care of the patients with us.
Nurses in procedural areas that were closed have been repurposed to work as runners. To run for supplies while the primary nurse is in an isolation room trying to stabilize a patient without the supplies they need, runners to run for blood transfusions.
Physical therapists, occupational therapists, speech and language pathologists being repurposed to be part of the proning teams that helps the nurses turn patients onto their backs and bellies amidst a tangled web of critical lines and tubes, where one small error could mean death for the patient, and exposure for all staff.
Anesthesiologists and residents are managing airways and lines when carrying out these massive patient position changes. Surgical residents are all over the hospital just to put in the critical invasive lines we need in all of our patients.
The travel nurses who rushed into this burning building to help us are easing a healthcare system. The first travel nurse I met came all the way from Texas. Others terminated their steady employment to enlist with a travel agency to help us. Every day there are more travelers arriving.
A nurse from LA came to me after she found out I was part of the home staff, in my home unit, where this all first started in my hospital what feels like a lifetime ago, and said, “I came here for you. For all of the nurses. Because I couldn’t imagine working the way you guys were working for how long you were working like that”. During our surge and peak in the ICU, we were 1:3 ratios with three patients who normally would be a 1:1 assignment. And they were all trying to die at the same time. We were having to choose which patients we were rushing to because we couldn’t help them all at the same time.
The overhead pages for emergencies throughout the hospital rang out and echoed endlessly. Every minute, another rapid response call. Another anesthesia page for an intubation. Another cardiopulmonary arrest. A hospital bursting at the seams with death. Refrigerated trailers being filled.
First it was our normal white body bags. Then orange disaster bags. Then blue tarp bags. We ran out of those too. Now, black bags.
The heartbreakingly unique part of this pandemic, is that these patients are so alone. We are here, but they are suffering alone, with no familiar face or voice. They are dying alone, surrounded by strangers crying into their own masks, trying not to let our precious N95 get wet, trying not to touch our faces with contaminated hands.
Their families are home, waiting for the phone call with their daily update. Some of their loved ones are also sick and quarantined at home.
Can you even IMAGINE? Your husband or wife, mother or father. Sibling. Your child. You drop your loved one off at the emergency department entrance, and you never, ever see them alive again.
Families are home, getting phone calls every day that they’re getting worse. Or maybe they’re getting better. Unfortunately, the ICU in what has quickly become the global epicenter for this pandemic is not a happy place. We are mostly purgatory where I work, so this snapshot may be more morbid than most.
These people are saying goodbye to their loved ones, while they’re still walking and talking, and then maybe a week or two later, they’re just gone. It’s like they disappeared into thin air.
That level of grief is absolutely astounding to me, and that’s coming from a person who knows grief. It changes you immeasurably.
But this grief? This pandemic grief? It’s inconceivable. These families will suffer horribly, every day for the rest of their lives. They might not even be able to bury their loved one. God, if they can’t afford a funeral with an economic shut-down, their loved one will be buried in a mass grave on Hart Island with thousands of others like them. What grave will they have to visit on birthdays and holidays?
Yesterday, I was preparing for a bedside endoscopy procedure to secure a catastrophic GI bleed in this 23-year-old patient.
It was a bleed that required a massive transfusion protocol where the blood bank releases coolers of uncrossmatched O negative blood in an emergency, an overhead page that, ironically, I heard as I was getting into the elevator to head to the fourth floor for my shift yesterday morning; a massive transfusion protocol that I found out I would own as a primary nurse, as I desperately squeezed liters of IV fluids into this patient until we got the cooler full of blood products, and then pumped this patient full of units of blood until we could intervene with endoscopy.
Before the procedure, I stopped everything I was doing that wasn’t life-sustaining. I stopped gathering supplies to start and assist with the procedure.
I told the doctors that I would not do a required “time-out” procedure until I got my phone out, and I facetimed this kid’s mom because I didn’t think he would survive the bedside procedure.
She cried. She wailed. She begged her son to open his eyes, to breathe. She begged me to help her. Ayudame. Ayudame. She begged me to help him. She sang to him. She told him he was strong. She told him how much she loved him. I listened to her heart breaking in real time while she talked to her son, while she saw his swollen face, her baby boy, dying before her eyes through a phone.
Later in the day, after the procedure, his mom and dad came to the hospital. He survived the securement of the bleed, but he was still getting worse no matter what we did. He’s going to die. And against policy, we fought to get them up to see their son.
We found them masks and gowns that we’re still rationing in the hospital, and we let his parents see him, hold him. We let them be with their son.
Like every other nurse would do in the ICU here, I bounced around the room, moving mom from one side of the bed to the other and back again, so I could do what I needed to do, setting up my continuous dialysis machine, with the ONE filter that supply sent up for my use to initiate dialysis therapy. This spaceship-like machine, finicky as all hell, and I had one shot to prime this machine successfully to start dialysis therapy to try to slowly correct the metabolic acidosis that was just ONE of the problems that was killing him as his systolic blood pressure lingered in the 70s, despite maxing all of my blood pressure mediations.
Continuous dialysis started. You press start and hold your breath. You’re not removing any fluid, just filtering the blood, but even the tiniest of fluid shifts in this patient could kill him. But you have no choice.
His vital signs started to look concerning. I could feel the dread in the pit of my stomach, this was going south very quickly. Another nurse and the patient’s father had to physically drag this mother out of the room so we could fill the room with the brains and eyes and hands that would keep this boy alive for another hour.
She wailed in the hallway. Nurses in the next unit down the hall heard her cries through two sets of closed fire doors. We worked furiously to stabilize him for the next four hours.
Twenty minutes before the end of my shift last night, I sat with the attending physician and the parents in a quiet and deserted family waiting room outside the unit. I told his mother that no matter what I do, I cannot fix this. I have maximized everything I have, every tool and medicine at my disposal to save her son. I can’t save her son.
The doctor explained that no matter what we do, his body is failing him. No matter what we do, her son will die. They realized that no matter how hard they pray, no matter how much they want to tear down walls, no matter how many times his mother begs and pleads, “take me instead, I would rather die myself than lose my son”, we cannot save him.
We stayed while she screamed. We stayed until she finally let go of her vice grip on my hands, her body trembling uncontrollably, as she dissolved into her grief, in the arms of her husband.
This is ONE patient. One patient, in one ICU, in one hospital, in one city, in one country, on a planet being ravaged by a virus.
This is the tiniest, devastating snapshot of one patient and one family and their unimaginable grief. Yet, the weight is enormous.
The world should feel that weight too. Because this grief, this heartbreak is everywhere in many forms. Every person on this planet is grieving the loss of something.
Whether that’s freedom or autonomy sacrificed for the greater good. Whether that’s a paycheck or a business, or their livelihood, or maybe they’re grieving the loss of a loved one while still fighting to earn a paycheck, or waiting for government financial relief that they don’t know for certain will come. Maybe they’re a high school senior who will never get to have the graduation they dreamed of. Maybe they’re a college senior, who won’t get to have their senior game they so looked forward to. Maybe they’re afraid that the government is encroaching on their constitutional rights. Maybe it’s their first pregnancy, and it’s nothing like they imagined because of the terrifying world surrounding them.
Or maybe they lost a loved one, maybe someone they love is sick, and they can’t go see them, because there are no visitors allowed and they’re an essential worker. Maybe all they can see of someone they love is a random facetime call in the middle of the day from an area code and a number they don’t know.
Everyone is grieving. We’ve heard plenty of the public’s grief.
I don’t blame anyone for how they’re coping with that grief, even if it frustrates the ever-living hell out of me as I drown in death every day at work. It’s all valid. Everyone’s grief is different, but it doesn’t change the discomfort, the despair on various levels. We are at the bottom of Maslow’s hierarchy of needs. Basic survival, physiological and safety needs. I’ve been here before. I know this feeling. How we survive is how we survive.
Now that I’ve had the time to reflect and write, now that I’ve let the walls down in my mind to let the grief flood in, now that I’ve seen this grief for what feels like the thousandth time since the first week of March as a nurse in a Covid ICU in New York City, it’s time you heard our side. This is devastating. This is our reality. This is our grief."
— Jeannine Nicole
0 notes
Text
Poppies Petals On A Gentle Breeze 🐝
🌴Instead of being upset, anxious and sad about these horrible hours we find ourselves quarantined due to Covid 19, I have decided to pay undiminished attention to the present moment. For all our negative emotions arise from either longing for the past for the way things were; of having jobs, of dressing up for the day with Bulgarian rose perfume and bright pink Schiap lipstick, of farmers markets, birthday parties, concerts and date nights, of frequenting Parisian inspired coffee shops, to eat an almond croissant and a lavender cappuccino while dreaming of the next holiday to the south of France, of collecting handiras, crimson, peach and navy Persian carpets, or barely held together first edition Gallimard books, or visiting dusty and light drenched libraries and the many other, pedestrian activities that evidenced the truest characters of our souls, for these were the pass times that we chose to expend the precious quotas of our lives, but also, the dread we feel today as the weeks merge into a steady river known as corona, can be attributed to the inability to predict things as they will be; of whether we will return to the past way of life, of financial, social, cultural and health security, of being able to travel, to be well and survive the pandemic, and, to be with our loved ones to accomplish our goals and dreams. But, rather, then turn back to the absconding past or to run away prematurely with the unstable future, perhaps it might be more illuminating to remain in the exacting present. For this moment, has its own charms that we may not be seeing, such as the delicate cadence of a string light, hanging like a strand of diamonds over the sweet peas, poppies, cornflowers, borage and lime plant, it may possess, it’s own music, such as a single wind-chime, playing a brief solitary melody, strangely, while the others are still, a message perhaps, that we are usually unable to decipher, it, may have its own taste, such as an English breakfast tea from Connecticut with Scottish shortbread cookies, it may have its personal, signature scent of early April, a mesmerizing prenuptial gift from the blossoms to the moths, of nicotiana, eucalyptus, orange leaves, pineapple sage, burnt palo santo and high scent sweet peas, it has its own touch, of frequented washed, alcohol sanitized hands, reaching to text a friend or comment on a photo, or to harvest cornflowers, nasturtium, violas, California poppies and scarlet sage. So we should quell the nervous aura that attempts to besiege us, just as the virus wrecks its damage upon the lung, we strike at both by breathing slowly and deeply, as possible, into the capillaries, branches and leaves, delivering oxygen and expelling the fear, like a poppy petal that drifts away on a gentle breeze.♾



0 notes
Text
COVID-19: UAE expert tips to protect children from coronavirus, preserve immunity
Picture used for illustrative functions solely Picture Credit score: Pixabay
Dubai: The novel coronavirus illness, COVID-19, appears to be giving children a large berth by way of problems. COVID-19 circumstances worldwide have crossed the 1.5 million mark, claiming over 89,000 lives – as of the time of scripting this story.
Whereas children are usually not immune to getting contaminated by the virus, most reported circumstances are asymptomatic and delicate. That is extensively being attributed to their immunity, which has been all the time stronger and extra resilient than adults.
Nonetheless, there have been a handful of deaths which, although very uncommon, might fear mother and father. We requested a UAE-based physician for her expert opinion and tips on preserving children protected – bodily and mentally.
Dr Rania Ayat Hawayek, Specialist Paediatrician, Medical Director and Founder, Circle Care Clinic and Dyson ambassador answered our most pertinent questions.
What makes children’s immunities stronger than adults?
Why are children at a decrease threat of getting signs?
Children have a sooner cell regeneration fee, and if there’s any harm to a cell of their our bodies it will probably restore a lot better and sooner than in adults. Their our bodies have been topic to far much less free radical harm, their lungs are more healthy, they usually haven’t been consuming extremely processed meals like adults.

Children’s lungs have far much less receptors that the cytokine proteins attributable to the virus…
– Dr Rania Ayat Hawayek, Specialist Paediatrician
Additionally, they haven’t been uncovered to many years of site visitors fumes, air pollution and second-hand smoke, so on the whole, their lungs and our bodies are cleaner and more healthy.
Extra particular to COVID-19 is the truth that children’s lungs have far much less receptors that the cytokine proteins attributable to the virus can latch onto and end in probably critical respiratory problems. This implies they don’t seem to be affected by the respiratory points that adults are inclined to – making them at decrease threat for having extreme signs of the virus.
I’ve to go away dwelling for work
How can I hold my children protected when stepping outdoors for work in an important sector?
For folks who’re nonetheless going out as a result of they’re in one of many very important sectors there are a number of precautions, they’ll take to hold themselves and their households protected upon their return:
• Follow correct social distancing. Don’t instantly hug your children when returning dwelling till you have got taken the mandatory precautions, together with washing your palms totally

Illustrative picture: Do not hug children if you get dwelling, clarify the measures to them
• Assume the garments you put on are contaminated after you come dwelling, so change straight away and the place you possibly can, wash them instantly
• Take off footwear and go away them outdoors in a single day, then clear them earlier than you carry them in
• Put on disposable masks and latex gloves when going outdoors and throw them away as soon as at dwelling. Don’t use the identical masks and gloves once more for they could comprise remnants of the virus in case you have got come throughout an individual with signs
• For these in direct contact with COVID-19 sufferers, resembling healthcare professionals, it’s higher to self-isolate away from the family. If that isn’t attainable guarantee you’re all the time sporting full protecting put on at your workplace
• Set guidelines throughout the family while you’re at work – for e.g. social distancing earlier than dealing with and accepting deliveries, guaranteeing children wash their palms ceaselessly and if they’re stepping out for an emergency ensure they’re geared up with masks and gloves too
Does food plan assist in defending our children?
Which meals gadgets ought to they be consuming proper now to construct resistance in opposition to signs?
A great food plan is essential to defending our children and even us as adults. That’s the reason it is vitally vital to preserve an organised construction day-after-day to proceed to enhance immunity as a preventative measure. Consuming vegatables and fruits is essential, and given the restrictions proper now, it requires us to ahead plan when ordering our groceries to guarantee we all the time have loads of recent fruit and greens at hand.
Moreover, under are a number of the components you should add to the organised routine:
• Children want to keep nicely hydrated, particularly now when they don’t seem to be enjoying outdoors and never feeling very thirsty indoors. Hold their vitamin C consumption excessive. It’s higher if that is via recent fruits however when you’ve got a toddler who’s a fussy eater then dietary supplements are an excellent different.
• Vitamin D can be vital as we’re all spending rather more time indoors and away from direct daylight. Deficiencies of Vitamin D have been linked to decrease ranges of immunity, so do present your little one with a dose of 800IU a day, which is double the traditional day by day dosage of Vitamin D.
• Zinc can be vital in boosting immunity. Among the best sources is nuts. If they don’t seem to be allergic to Brazil nuts, grinding three brazil nuts a day into your little one’s meals is a good way of getting their day by day requirement of Zinc into their food plan.
• Sugar will increase the danger of catching infections, so ensure your loved ones is lowering their consumption of sugar.
Enhancing indoor measures
What measures ought to we take indoors, as well as to sanitising environment?
Enhancing your indoor environment is essential in your children. Now that there are extra family members at dwelling on the identical time, it is important to be additional cautious on the way you clear and rid your house of germs and micro organism.
Deep cleansing permits you to take away dangerous mud from the setting. Correctly sort out mud by washing any tender furnishing gadgets – pillows, curtains, cushions and throws. Different gadgets, resembling mattresses and couches, needs to be cleaned utilizing a strong, absolutely sealed vacuum cleaner with acceptable attachments.
Moreover, take a look at methods to enhance indoor air high quality. The air in our houses can comprise plenty of substances together with mud, germs and micro organism, pet dander, allergens, gases together with unstable natural compounds (VOCs), NO2 and benzene. Now’s the time to put money into an air air purifier that has twin, HEPA filters that may seize pollution, gases and viruses within the air.
Making your house freed from pollution will assist in preserving good immunity in children.
Psychological well being and speaking to children?
What recommendation would you give with regards to safeguarding children’s psychological well being, given the the strict security measures taken by the UAE?
I might advise mother and father to preserve a routine with their children. Children reply nicely to having an ongoing schedule, so that they go to mattress on the identical time and have a construction to their day. Being too versatile of their day-to-day actions tends to make children a bit of insecure and that’s the place they’ll attempt to battle routine and deal with the present scenario as simply an prolonged trip.
Dad and mom ought to keep away from listening and watching the information about COVID-19 and discussing the damaging features of it in entrance of their children. Children take in an awesome deal and rather more than we understand. It’s higher to have a dialog with them concerning the present scenario in easy phrases and ask them what they suppose is occurring.

Picture used for illustrative functions: For children their psychological well being is dependent upon how safe they really feel and that is dependent upon how safe their mother and father appear to them.
For instance, my three-year-old son is aware of he can’t go to his grandmother due to the virus, however as soon as that’s cleared, he can see her. On this approach he is aware of it’s due to the virus and never as a result of she doesn’t need to see him. There may be loads of nice digital content material about COVID-19 that has been made for children, which de-mystifies the virus and helps them to higher perceive what’s going on.
Cabin fever: Do children like being indoors?
Children are very adaptable and actually, take pleasure in being indoors. For a lot of of them it’s the first likelihood to be with their mother and father all day, day-after-day.
I discover that it’s the mother and father that have a tendency to get extra of the cabin fever than their children. I might encourage mother and father to make their houses into massive play areas and be inventive in a approach that actually engages with their little one’s creativeness.
For instance, excite them with an indoor treasure hunt by drawing out a map of your house, after which cover the ‘treasure’ elsewhere every time. Alter the problem relying on their age.
For children their psychological well being is dependent upon how safe they really feel and that is dependent upon how safe their mother and father appear to them. So long as you possibly can put a smile in your face, preserve a structured day, and behave usually, they are going to be completely satisfied.
Additionally, don’t really feel pressured to break home guidelines due to the scenario. Be agency with them: when crucial, a no is a no; children get their power and safety from regular and wholesome parenting.
from WordPress https://ift.tt/2UUtK59 via IFTTT
0 notes
Text
Repatriated OFWs resist pandemic’s stresses through family bonds
MANILA — Wilfredo Pamposa’s wallet subdued him yet again, for a fifth straight year. Unpaid salaries and benefits from two bankrupt Saudi Arabian construction firms had long emptied Pamposa’s wallet, almost draining his resilience.
COVID-19 came to the Kingdom of Saudi Arabia mid-March. Pamposa’s iqama (the Kingdom’s permit for employment visa holders) expired. Since 2019 Pamposa and fellow Filipino workers had been economically immobile: “I was on standby for a year, remitting nothing to my family.”
Raising funds through whatever means necessary, Pamposa miraculously paid the penalty for his expired iqama and his exit visa fees. With the help of Philippine diplomatic and labor personnel in Riyadh, Pamposa got repatriated last May.
Pamposa’s eyes and his voice’s tone got hushed as he narrated this story during a webinar on overseas Filipino workers (OFWs) repatriated by the COVID-19 pandemic. During a nine-day quarantine sortie at a small motel in Quezon City, he finally slept on Philippine soil, roused that years of overseas financial agony will finally end.
And when the negative swab test result came out, wife Grace sobbed in glee. What’s important, Grace narrates, “is that he’s back home safe —even without money.” The return trip from the motel in Cubao, Quezon City to the rented apartment in Antipolo City had ceased Pamposa’s years of wallowing in financial despair, before and during the COVID-19 pandemic. Familial love not only saved this breadwinner and his family. I tended to an ihaw-ihaw (grilled street food) stall here, Grace said. Two of their three children stopped schooling since 2019 and they earn from tutoring elementary school children who are their neighbors.
A pandemic pushed OFWs, both with unstable and stable jobs, to the limits. Repatriation saved them, even if quarantine routines and rapid tests back home suspended their excitement to be relieved from the physical, financial and mental stresses of overseas migrant work.
However, the all-enduring Filipino safety net during crises —the family— soldiered migrant breadwinners to confront uncertain economic futures together, with love.
“We’re happy even ‘without money. At least he’s back home [Masaya po kami kahit walang pera. At least nakauwi na],” a teary-eyed Grace Pamposa uttered. “We can earn money once again. What’s important is he’s safe [Iyung pera naman, mapagkikitaan uli iyan. Ang importante, ligtas siya].”
This Filipino safety net calmed the emotions and stresses of some 55,859 repatriated land- and sea-based OFWs who bore the brunt of massive overseas job layoffs. The repatriations continue, possibly reaching 300,000 repatriated OFWs by August, government authorities estimate.
In March, seafarer Archie Arce saw his cruise ship grounded just a month from his return to active duty, with COVID-19 hitting passengers and crew of many luxury cruises. Nobody expected this pandemic to happen, Arce said, “so I wasn’t ready, honestly [hindi ako naging ready, sa totohanan lang].”
Docked for five weeks by required quarantine measures, Arce —now back home— got stomped also by what Caloocan City residents are doing now to survive this pandemic. “I still can’t think of a business until now because many, many people here are now doing business online [Wala kaming maisip na puwedeng business. Dami na kasing nago-online].” Wife Regine (a church volunteer) and a 16-year-old daughter comforted their “sad” father with smiles upon his stepping foot in their humble abode. “Finally [Sa wakas],” Regine said gleefully, “You’re here! We’ll take care of you.” (“Until the financial support comes back,” Grace said their only daughter will skip school this year.)
These tales by the Pamposa and Arce breadwinners reveal a “grieving process” that these returned OFWs have to go through,” veteran OFW counselor Fr. Nilo Tanalega, S.J. of the UGAT Foundation said.
“A job and a dream were both lost,” Tanalega told the OFW couples during a July 10 webinar organized by the Catholic-run nonprofit Scalabrini Migration Center.
Tanalega recommends constant communication for the returned migrant worker and the spouse in these moments of reintegrating back to the country beside quarantines and movement restrictions. This approach, he adds, is a “process that will take time for them to adjust and adapt to family life again.”
Remember, Tanalega explained, “the OFW is accustomed to living alone. Then he or she went back abruptly.”
The pandemic and the resulting quarantines OFWs faced saw them teeter from mental health problems. Recent reports of suicides by Filipino seafarers for example “are serious matters,” Tanalega said.
And now that COVID-19 had grounded Filipino families and livelihoods, Tanalega proffered couples with repatriated OFW breadwinners to ask themselves how they and their families should soldier on.
“It is easy to say that you are now with your families and you should support each other,” Tanalega said. “But they should execute such forms of family support, especially the families’ emotional and relationship needs, at this time.” Economically, for example, Tanalega prodded OFW couples to ask themselves during this pandemic: “How will we know if what we have is enough for us [Paano natin malalaman na sapat na iyan para sa inyo]?”
And with Filipinos still perplexed at the uncertainties their immediate futures hold, 28-year seafarer Teodoro Rosello worries about his next work. Will we get rehired, Rosello asked, “if our companies recover from this pandemic?” But the return home, the Rosello patriarch said, “is freedom from work” for seafarers like him.
Going home to Bacoor City, Cavite is “the happiest part,” and wife Charity made Teodoro’s return happier with a tight hug.
The family’s whole again. I’m seeing my three boys again, Teodoro said. Yet the unseen enemy, COVID-19, pushed the Teodoros mostly inside home even if Cavite’s now on general community quarantine. All plans for out-of-town leisure got cancelled.
But in handling boredom, the family’s up and about to spend happy times. They cook and grill together, singing to their hearts delight, Charity narrates.
Something else held the Teodoros tight in these times. It’s prayer, Charity said. “During this time that we do not know what happens next, we need to cling to prayers. If before we had trust in the Lord, now all the more we need to stick to Him.”
Oops, Charity reminded her hubby: “We have programmed our house chores. Get the broom. Clean the car!” Daily loud serenades by the singing Teodoros pacify the stresses a pandemic continues to bring, and an overseas worker’s fears about the future.
Freelance journalist Kristine Anne Macasiray is a 2019 product of the University of Santo Tomas (UST) journalism program.
Published on The Filipino Connection, Philstar.com, and Tinig-UK.
0 notes
Text
Just really needed to get this theory out there, nature is way more resilient and adaptive than we think
I've had this cool theory for a while which I personally hold true but I'm sure most of you will say is far fetched.
I personally believe that nature is far more adaptable, dynamicly resilient and powerful than we as a society believe. I can't seem to find any articles on the topic because everyone is jaded by the belief that humanity's destruction and eradication of life on earth will bring a collapse to the natural world. This is what I believe is wrong, as we intently destroy the global ecosystem on an unprecedented scale, the overall gene pool of life as a mass will begin to be forced to select for traits that are effective in reducing humanity's stresses and impacts for it's own survival. Many species are evolving to, or are being manipulated into cooperating with humans. But I believe many more species are evolving to directly or indirectly weaken and destroy mankind.
Simply put, life on Earth has constantly evolved and adapted to thrive even through absolute destruction and percievably impossible scenarios. The fact that life came to exist from the most coincidental and bizarre circumstances and has not gone away proves the incredible resilience it holds. We as humans are now constantly destroying and eradicating, forcing nature into extremes to ensure its own survival.
Remember that by nature I mean all cellular and non-cellular life on earth except humanity. Plants, animals, fungi, pathogens, bacteria and everything in between. Particularly I emphasise on microscopic life such as viruses, bacterial and pathogens as these are the fastest to evolve and are thus the most adaptive and resilient of all. Humanity's extortion and destruction is often forcing species to have as profound an impact on humanities prosperity and inevitable survival as possible. The rapidly exponential rate at which life is beginning to cohesively 'jepoardise' humanities prosperity will also be forced to essentially co-operate against mankind and form dynamic direct or indirect systems which make human life more difficult.
Life will constantly try to restore the natural equilibrium that existed before the Anthropocene (human epoch), destroy humankind's existence entirely or force humankind into creating this natural equilibrium which would likely result in various systems of human population control.
I know what many of you are thinking, your probably that humankind possesses the ability to and is essentially acting to destroy the Earth and all life on it. But I simply do not believe we are yet capable of, or never will be capable of destroying life on earth entirely. Not to say if we really tried to say blow the world up by using all nuclear power on earth to creat an exlosion that somehow could break the world in two, of manipulated the trajectory of a meteorite or space Phenomena of some kind to literally disintegrate or split the earth into pieces (with the potential survival of life within the vacuum of space forced to cling in). I simply do not believe we are yet capable or even ever will be capable of the Earth's destruction, mother Earth will likely bring us down first. I f every nuclear warhead on earth were to simultaneously be detonated, extremely catastrophic mass extinction would likely entale and the majority of life will perish. However just as life came to be here life will always remain on earth, and there will always be outliers, enclave, mutated and biologically resistant life that will then flourish and prosper in a new environment with very little competition. In fact the 'eternal' nuclear fallout would dramatically increase the rate of mutation in genetics and life would raidly evolve into a terrifyingly dynamic new reality, or some fungi will just evolve to rapidly detox and irradiate the earth returning it to normal 😂
Now to get back to the point I'm making, humanity must either universally co-operate with the natural world. Or be forced into a position where they are no longer the dominant species. Another species will also likely evolve to be sentient and compete with humanity in a geographically short time period, with many more to follow.
This may all seem like jibber jabber to some of you, it seems that our society's ego has us believe that we are better than nature. We often believe we are not animals and we are so advanced that we have the ability to prosper through anything nature throws at us. But this is simply untrue and mother nature will grab humanity by the balls when she wants to, and her grip is getting tighter.
I don't have any degrees, in fact I don't even have any sources to quote here. There is no reason for you to agree with me, any and all argumant or rebuttal will be great and I would love for someone to raise a point that makes my theory obsolete. I could go on about this with many more intricate predictive theories on the topic, but I have so many more ideas and theories I just need to get out of my head.
Nah, I got a couple other thoughts on this as well. Nature's manipulation of hamnkind may even be completely indirect, we may never now how the natural world can impact our psyche and may simply create an extreme tendency for society to be extremely unstable. The DNA that codes our life may likely select for genes that encourage humans to fight each other as a form of population control, and this may be how an equilibrium could be established. Overpopulation will likely lead to conflict, famine, diseases and all as nature will and always has been thriving for a world of diversity and cohabitation. The environmental recovery caused by the global impact of covid-19 is a great example of how nature indirectly works together against us. Since animals that transmit diseases will often prosper through the lessened impact of humanity in their own lives. Species that can transmit viruses directly or indirectly to humans, will likely thrive, thus selecting for genes which directly or indirectly cause human habitation within their environment to decrease or desist. This will likely lead to a world where animals evolve purely to kill humans, the outcome in only a couple millenia will be scary af.
The problem I see is not animals or plants though, it's pathogens and all the microscopic stuff. When the environment benefits from a virus that impairs humanitys impact, many others will naturally begin to evolve to the benefit of other species in this ecosystem, and diseases will do this first. Viruses and bacteria are of particular concern here since they or the most rapid to evolve and adapt to a change in their environment. Zoonotic viruses that rapidly immobilise humans will have significant benefits to their hosts and ecosystems they are within thus zoonotic viruses that can infect humans will likely be the first step in Earth establishing an equilibrium.
If overpopulation is somehow rapidly addressed this would probably significantly reduce the rate at which this 'theoretical bullshit' may happen. Realised I forgot to mention why I don't have faith in our sciences or doctors to fight spontaneous natural occuring diseases. Viruses/bacteria/pathogens all that, have n essentially infinite ability to evolve, gain resistances and become immune or more severe. It is commonly known that most viruses do not want to kill their hosts, but when the entire global ecosystem benefits from a virus killing it's host, those viruses will begin to occur far more frequently and likely with increasing severity. Sorry if this is scary for you somehow as long as you are young and healthy you will probably be fine but I can't say much about the outcome of a likely upcoming war of significant proportion, likely fought very unconventionally.
TLDR and a lil conclusion: Nature is powerful as heck, in the end we are just another species on this planet and through all the great things we have and will achieve, mother Earth will be able to keep us in check. I don't understand why I am unable to find articles on this, mass extinction does not simply cause life as a whole to perish, it strengthens the gene pool, and by impacting essentially all species of life on Earth; we are essentially creating our own undoing. Overpopulation will likely trigger the most significant mechanisms of 'human eridication'. You can say I'm just a doomsday theorist or something but this will not happen in a couple of years, I believe it has been ongoing ince we first discovered fire and is now taking a drastic step in its inevitable fate. Also not sure if I even mentioned global warming, but the extreme loss and extinction caused by this will likely be short lived, most ecosystems will eventually benefit from Increased temperatures with a global increase in rainfall and water available for evaporation. Fungi and other live organisms will likely evolve systems to reduce harmful gases and elements in the ground and air (as they already do) and filter out the 'toxins'.
I also just want to say that every opinion is biased somehow, of course this for example, but even the most credible articles and studies from prestigious universities or organisations. Simply by thinking that we as humans are top shit, the short term impact of our actions/activities blind us in our judgement of the long term outcome. Nature finds a way, always will and always has, we don't know why or how this occured, but it has clearly proven to be terrifyingly powerful and resilient.
Humanity must lose its ego, we might look like top shit right now but some day or another we will be put in our place. Mother nature is patiently waiting to bitch slap us back into our caves, and it kinda seems that no-one wants to talk about this? Also yes, this is something I thought about on a mushroom trip, but I've formulated the other ideas since. WAKE UP SHEEPLEZ nah jk kidding there's nothing we can do lmao😅
submitted by /u/mrunk0 [link] [comments] source https://www.reddit.com/r/Futurology/comments/hy2tvz/just_really_needed_to_get_this_theory_out_there/
0 notes