#sars cov 2 outbreak
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
so they've now found the New Improved monkeypox that WHO has declared a public health emergency outside of Africa- in Sweden and the US so far
heres me thinking we're facing down the next pandemic as This Current Covid Mess vs bird flu but now here comes fucking monkey pox with the steel chair
#i dont even like infectious disease studies im just forced to pay attention bc theres no public health#also fucking bollocks that weve only just started caring about mpox bc its outside africa#but thats a whole different essay#anyways#may the odds be ever in your favour#pandemic#the who#world health organization#monkeypox#mpox#mpox outbreak#mpox virus#bird flu#h5n1#h5n1birdflu#h5n1 virus#covid 19#sars cov 2#sars2#covid isnt over#wear a mask
17 notes
·
View notes
Text
What Is A Tripledemic? Lookout For These Three Viruses That Cause Severe Respiratory Health Issues
As the world continues to navigate post-pandemic life, new health challenges are emerging, particularly with the onset of winter. One of the rising concerns is the tripledemic, a term that has been coined to describe the simultaneous surge of three respiratory viruses—COVID-19, influenza (flu), and respiratory syncytial virus (RSV). These viruses have the potential to overwhelm healthcare systems…
#COVID 19 symptoms#Covid-19#COVID-19 infection#Covid-19 outbreak#flu#flu case#flu symptoms#flu vaccine#health india#immunity boosting food#India COVID-19 cases#india tripledemic#influenza#influenza cases#influenza causes#Influenza Vaccination#Respiratory Health#respiratory health risks#Respiratory syncytial virus#respiratory syncytial virus symptoms#RSV causes#RSV symptoms#SARS-CoV-2 virus#symptoms of COVID-19#symptoms of influenza#tips to boost immunity#tripledemic#tripledemic india#UK tripledemic#viral infections
0 notes
Text
Dr. Robert Malone: "Saya baru pulang dari Tokyo di mana mereka mengadakan perhimpunan 30,000 orang kerana mereka akan melancarkan vaksin RNA yang boleh mereplikasi diri. Jepun digunakan sebagai kelinci percubaan untuk teknologi baru ini di peringkat dunia. Rakyat Jepun memanggil ini bom atom ketiga. Ini dilaksanakan dalam kerjasama antara syarikat AS, Arcturus, sebuah syarikat Kanada, maaf, sebuah syarikat Australia bernama CSL dan sebuah syarikat Jepun.
Kini CEO syarikat Jepun itu baru-baru ini mengadakan sidang akhbar. Apa yang dia katakan? Dia berkata sesiapa yang menyebarkan maklumat salah, kami akan ambil tindakan undang-undang terhadap mereka, kami akan cuba untuk menjatuhkan hukuman penjara ke atas mereka. Jika anda berkata apa-apa yang menentang teknologi vaksin RNA yang boleh mereplikasi diri mereka yang tidak pernah diuji secara ketat, kami tidak tahu jika ia akan menjangkiti orang lain. Kami tidak tahu jika ia akan merebak.
Kami tahu ia akan mereplikasi. Kami tidak tahu jika ia akan masuk ke dalam otak orang tua di Jepun. Tetapi kami tahu bahawa jika kami mengutarakan apa-apa mengenai kebimbangan ini, CEO itu akan mengejar kami dan cuba memasukkan kami ke dalam penjara. Itulah susunan dunia baru. Itulah yang akan kita hadapi. Itulah yang mereka ingin laksanakan ke atas kita.
Mereka ingin menutup suara kita. Mereka ingin menghalang kita daripada bercakap. Mereka mahu mengawal sepenuhnya naratif dan mereka mahu dapat melaksanakan perang psiko terhadap anda semua untuk mengawal anda, untuk melatih anda, untuk menjawab naratif ketakutan tentang influenza burung dan cacar monyet dan apa sahaja yang mereka mahu laksanakan seterusnya untuk mengawal anda, untuk mengajar anda supaya diam, duduk, tinggal di rumah, dan lakukan apa yang disuruh. Saya tidak setuju dengan itu, saya rasa anda pun tidak setuju, dan saya harap anda bergabung dengan kami semua untuk melawan tirani baru ini."
#suntikan vaksin#vaksin99#vaksinasi#vaksin#get vaxxed#get vaccinated#vaccine damage#vaccination#vaccine#vaccines#vaccine genocide#mrna#mrna vaccine#long covid#covid isn't over#covid vaccine#covid 19#covid#still coviding#coronavirus#sars cov 2#monkepox#monkeypox#mpox news#mpox outbreak#mpox#mpox virus#big pharma#cdc#cdc corruption
0 notes
Text
Airborne Risk Indoor Online Calculator (ARIA)
A team of international experts under the World Health Organization (WHO) developed an Airborne Risk Indoor Online Calculator.
ARIA is an online tool that enables users and building managers to assess the risk of SARS-COV-2 (COVID-19) airborne transmission in residential, public, and healthcare settings. The aim is to inform decisions that can significantly reduce the risk of transmission.
A 66-pages document [5.757 MB, English, archived] is available.
#clean air for all#clean air revolution#indoor air quality#COVID#COVID-19#SARS-CoV-2#COVID resources#COVID-19 resources#SARS-CoV-2 resources#online calculator#COVID tools#COVID-19 tools#SARS-CoV-2 tools#CC BY-NC-SA#Attribution-NonCommercial-ShareAlike#creative commons#respiratory aerosols and droplets#respiratory system#respiratory tract infections#risk assessment#risk reduction behavior#sneezing#disinfection#disease outbreaks#infection control#emergencies#delivery of healthcare#virion#referral and consolation#transmission
1 note
·
View note
Text
The next pandemic is inevitable. Australia isn’t ready - Published Sept 23, 2024
(Before you Americans yell at me, It's already the 23rd in Australia. This is very late-breaking)
I thought this was a really good breakdown of the current situation given the government-approved covid denial we live in. Long, but worth a read.
By Kate Aubusson and Mary Ward
Top infectious disease and public health veterans at the nerve centre of the state’s war against COVID-19 are sounding the alarm.
NSW is less prepared today to fend off a deadly pandemic despite the lessons of COVID-19, say top infectious disease and public health veterans at the nerve centre of the state’s war against the virus.
And we won’t have another hundred years to wait.
NSW’s gold standard Test-Trace-Isolate-Quarantine and vaccination strategies will be useless if a distrusting population rejects directives, refuses to give up its freedoms again, and the goodwill of shell-shocked public health workers dries up.
A panel of experts convened by The Sydney Morning Herald called for a pandemic combat agency akin to the armed forces or fire brigades to commit to greater transparency or risk being caught off guard by the next virulent pathogen and misinformation with the potential to spread faster than any virus.
“It’s inevitable,” says Professor Eddie Holmes of the next pandemic. A world-leading authority on the emergence of infectious diseases at the University of Sydney, Holmes predicts: “We’ll have less than 100 years [before the next pandemic].
“We’re seeing a lot of new coronaviruses that are spilling over into animals that humans are interacting with,” said Holmes, the first person to publish the coronavirus genome sequence for the world to see.
“People are exposed all the time, and each time we are rolling the dice.”
The independent review of NSW Health’s response to COVID-19 opened with the same warning: “No health system or community will have the luxury of 100 years of downtime.”
Pandemic preparedness needs to be a “permanent priority”, wrote the report’s author, Robyn Kruk, a former NSW Health secretary, “rather than following the path of those that have adopted a ‘panic and forget strategy,’ allowing system preparedness to wane”.
Why we don’t have 100 years to wait for the next pandemic The World Health Organisation has declared seven public health emergencies of international concern since 2014, including the current mpox outbreak.
Climate change is turbocharging the factors that coalesce to create the perfect breeding ground for a pandemic-causing virus, including population increases, bigger cities, and better-connected global markets and migration.
“Animals will be forced into more constrained environments, and humans that rely on those environments will be again constrained in the same environments. There will be more wet markets, more live animal trade that will just increase exposure,” Holmes said.
“It was clear that we weren’t ready [for COVID],” said Jennie Musto, who, after seven years working for the World Health Organisation overseas, became NSW Health’s operations manager for the Public Health Emergency Operations Centre, the team responsible for NSW’s COVID-19 contact tracing and containment.
“Everyone had preparedness plans gathering dust on a shelf, but no one was actually ready to respond, and so everyone was on the back foot,” Musto said. “Perhaps none of us really thought this was going to happen. We were waiting 500 years.”
Who would willingly become the next doomed whistleblower? Eddie Holmes, known for his repeated assertion that SARS-CoV-2 did not come from a lab, is deeply concerned that when the next pandemic-causing virus emerges, chances are it will be covered up.
“My worry is that if the virus appeared in a small population, say, somewhere in Southeast Asia, the people involved wouldn’t blow the whistle now, given the fact that you would get blamed,” he said.
Li Wenliang, the Wuhan doctor who tried to raise the alarm about a virulent new virus, was reportedly reprimanded by police for spreading rumours and later died of COVID-19.
The global blame game, culminating in a deep distrust of China and accusations that the virus was grown in a Wuhan lab, is why Holmes believes “we’re in no better place than we were before COVID started, if not worse”.
“I work with a lot of people in China trying to keep the lines of communication open, and they’re scared, I think, or nervous about saying things that are perceived to counter national interest.”
From a vaccine perspective, our defences look strong. There have been monumental advancements in vaccine development globally, driven by mRNA technology. In Sydney this month, construction began on an RNA vaccine research and manufacturing facility.
“But the way I see it is that nothing has been done in terms of animal surveillance of outbreaks or data sharing. The [global] politics has got much, much worse,” Holmes said.
Combat force Conjoint Associate Professor Craig Dalton, a leading public health physician and clinical epidemiologist, called for a dramatic expansion of the public health workforce and the establishment of a pandemic combat force that would routinely run real-time pandemic simulations during “peacetime”.
“No one is upset with fire brigades spending most of the time not fighting fires. They train. A lot. And that’s probably how we need to move,” he said.
“We need exercise training units so that every major player in pandemic response is involved in a real-time, three to four-day pandemic response every three to five years at national, state and local [levels].”
The federal Department of Health and Aged Care recently ran a health emergency exercise focused on governance arrangements involving chief health officers and senior health emergency management officials, a spokeswoman for Health Minister Mark Butler said. The outcomes of this exercise will be tested later this year.
Dalton said desktop simulations and high-level exercises involving a handful of chiefs didn’t cut it, considering the thousands of people working across regions and states. He instead suggested an intensive training program run in the Hunter New England region before the 2009 H1N1 pandemic provided a good model.
“We were ringing people, actors were getting injections, just like a real pandemic,” said Dalton, who once ordered a burrito in a last-ditch effort to contact a restaurant exposed to COVID-19.
Our heroes have had it The expert panel was emphatic that our pandemic response cannot once again rely on the goodwill of the public health and healthcare workforce.
According to the Kruk review, what began as an emergency response ultimately morphed from a sprint into an ultra marathon and “an admirable (yet unsustainable) ‘whatever it takes’ mindset”.
They were hailed as heroes, but the toll of COVID-19 on healthcare workers was brutal. Workloads were untenable, the risk of transmission was constant, and the risk of violence and aggression (for simply wearing their scrubs on public transport in some cases) was terrifying.
“We got through this pandemic through a lot of people working ridiculous hours,” Dalton said.
“You talk to a lot of people who did that and say they could not do it again.”
Tellingly, several expert personnel who worked at the front lines or in the control centre of NSW’s pandemic defences were invited to join the Herald’s forum but declined. Revisiting this period of intense public scrutiny, culminating in online attacks and physical threats, was just too painful.
So long, solidarity Arguably, the biggest threat to our pandemic defences will be the absence of our greatest strength during COVID: the population’s solidarity and willingness to follow public health orders even when it meant forfeiting fundamental freedoms.
The public largely complied with statewide public health orders, including the stay-at-home directive that became the 107-day Delta lockdown, and other severe restrictions prevented many from being at the bedside of their dying loved ones, visiting relatives in aged care homes and attending funerals.
“My worry is that next time around when those sorts of rules come out, people may say, ‘Well, don’t worry about it.’ They relax it in the future. Why don’t we just not stick to the rules?” said Professor Nicholas Wood, associate director of clinical research and services at the National Centre for Immunisation Research and Surveillance.
“I’m not sure we quite understand whether people [will be] happy with those rules again,” he said.
Dalton was more strident.
“I tend to agree with Michael Osterholm … an eminent US epidemiologist [who] recently said the US is probably less prepared for a pandemic now than it was in 2019, mostly because the learnings by health departments in the COVID pandemic may not make a material difference if faced with a community that distrusts its public health agencies,” he said.
“If H1N1 or something else were to spill over in the next couple of years, things like masks, social distancing and lockdowns would not be acceptable. Vaccination would be rejected by a huge part of the population, and politicians might be shy about putting mandates in.”
As for the total shutdown of major industries, people will struggle to accept it unless the next pandemic poses a greater threat than COVID, said UNSW applied mathematician Professor James Wood.
The risk of the virus to individuals and their families will be weighed against the negative effects of restrictions, which are much better understood today, said Wood, whose modelling of the impact of cases and vaccination rates was used by NSW Health.
“Something like school closure would be a much tougher argument with a similar pathogen,” he said.
A previous panel of education experts convened by the Herald to interrogate pandemic decision-making in that sector was highly critical of the decision to close schools for months during NSW’s Delta lockdown.
Greg Dore, professor of infectious diseases and epidemiology at the Kirby Institute, said the public’s reluctance to adhere to restrictions again may, in part, be appropriate.
“Some of the restrictions on people leaving the country were a bit feudal and too punitive,” he said. “Other restrictions were plain stupid, [for instance] limitations on time exercising outside.”
Meanwhile, the delays to publicly recognise the benefits of face masks and the threat of airborne transmission “ate away at trust”, Dalton said.
“We shouldn’t make those mistakes again,” he said.
Transparent transgressions Uncertainty is not something politicians are adept at communicating, but uncertainty is the only constant during a pandemic of a novel virus.
Vaccines that offered potent protection against early iterations of the COVID virus were less effective against Omicron variants.
“[The public], unfortunately, got hit by a rapid sequence of changes of what was ‘true’ in the pandemic,” James Wood said.
Political distrust can be deadly if governments give the public reason to suspect they are obfuscating.
The expert panel urged NSW’s political leaders to be far more transparent about the public health advice they were given before unilaterally enforcing restrictions.
There was a clear line between public health advice and political decision-making in Victoria. The Victorian chief health officer’s written advice was routinely published online.
In NSW, that line was blurred as Chief Health Officer Kerry Chant stood beside political leaders, most notably former premier Gladys Berejiklian, at the daily press conferences.
Public health experts said that they looked for subtle cues to determine the distinction between the expert advice and the political messaging during press conferences, paying attention to body language, who spoke when and who stayed silent.
“It is fine for public health personnel to have a different view to politicians. They have different jobs. What is not OK is to have politicians saying they are acting on public health advice [when they are not],” he said.
The ‘whys’ behind the decisions being made were missing from the daily press conferences, which created “a vacuum for misinformation”, said social scientist and public health expert Professor Julie Leask at the University of Sydney.
“The communication about what you need to do came out, and it was pretty good … but the ‘why we’re doing this’ and ‘what trade-offs we’ve considered’ and ‘what dilemmas we’ve faced in making this decision’; that was not shared,” Leask said.
The infodemic In the absence of transparency, misinformation and disinformation fill the vacuum.
“We had an ‘infodemic’ during the pandemic,” said Dr Jocelyne Basseal, who worked on the COVID-19 response for WHO in the Western Pacific and leads strategic development at the Sydney Infectious Diseases Institute, University of Sydney.
“The public has been so confused. Where do we go for trusted information [when] everyone can now write absolutely anything, whether on Twitter [now called X] or [elsewhere] on the web?” Basseal said.
A systematic review conducted by WHO found misinformation on social media accounted for up to 51 per cent of posts about vaccines, 29 per cent of posts about COVID-19 and 60 per cent of posts about pandemics.
Basseal’s teenage children recently asked whether they were going into lockdown after TikTok videos about the mpox outbreak.
“There is a lot of work to be done now, in ‘peacetime’ … to get ahead of misinformation,” Basseal said, including fortifying relationships with community groups and teaching scientists – trusted and credible sources of information – how to work with media.
In addition to the Kruk review’s six recommendations to improve its pandemic preparedness, NSW Health undertook a second inquiry into its public health response to COVID-19, which made 104 recommendations.
NSW Health Minister Ryan Park said: “We are working hard to ensure the findings and recommendations from those reports are being implemented as quickly as possible.”
The expert panellists spoke in their capacity as academics and not on behalf of NSW Health or WHO.
The ‘As One System’ review into NSW Health’s COVID-19 response made six recommendations 1. Make governance and decision-making structures clearer, inclusive, and more widely understood 2. Strengthen co-ordination, communication, engagement, and collaboration 3. Enhance the speed, transparency, accuracy, and practicality of data and information sharing 4. Prioritise the needs of vulnerable people and communities most at risk, impacted and in need from day one 5. Put communities at the centre of emergency governance, planning, preparedness, and response 6. Recognise, develop and sustain workforce health, wellbeing, capability and agility.
#mask up#covid#covid 19#pandemic#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
139 notes
·
View notes
Text
"Most of what “public health” does for Americans is taken for granted. Before the Covid pandemic, most people probably didn’t think about it at all. Yet the fact that, in most places in the United States, we can count on the water we drink to be safe, that the food we buy is not contaminated with e-coli or listeria, and that we don’t have to deal with dreaded childhood diseases that ripped through our communities only a few decades ago, is a testament to the tireless work of many, unheralded, often unknown heroes. This invisible safety net has been built up over the years, always underfunded and understaffed, always not-enough, but it’s all we’ve got.
...
By now, we’ve heard Kennedy’s views on everything from fluoride in drinking water to childhood vaccines, to threats to recreate the NIH and FDA in the image of his own quackery. Let’s be clear: Kennedy’s views are not “alternative” to orthodoxy, meant to shake up the system—they are verifiably false. They are nonsense.
Let’s take his claims on fluoride as an example. RFK Jr. wrote on X in early November: “Fluoride is an industrial waste associated with arthritis, bone fractures, bone cancer, IQ loss, neurodevelopmental disorders, and thyroid disease.” Um—no. In high doses over prolonged periods of time—as with many other substances (even water and oxygen!)—exposure to fluoride can be a problem, but not in the small concentrations we see in drinking water. Lest we forget: Fluoride has been a bugaboo of the far right since the 1950s, when fluoridation was supposed to be part of a communist plot to take over America.
And since conspiracy theories know no borders, we can also look at a natural experiment up in Calgary, Canada, for further evidence. In 2011, Calgary’s’s city council banned fluoridation, and now is set to reintroduce it next year. Why? Because since fluoridation ended, cavities in children’s teeth have become more numerous and larger, often requiring treatment under general anesthesia and/or intravenous antibiotic therapy to fight infections associated with tooth decay. As one researcher at the University of Calgary has said, the decision to ban fluoridation had a clear result: It was a source of “avoidable and potentially life-threatening disease, pain, suffering, misery and expense…especially [for] very young children and their families.”
As for vaccination, Kennedy’s views are long-standing and well-known. He has suggested that “there is no vaccine that is safe and effective,” and he still clings to the long-debunked idea that vaccines cause autism. More recently, during the Covid pandemic, he created a multimillion-dollar anti-vaccine juggernaut to dissuade people from getting vaccinated against SARS-CoV-2.
There is no person right now more vital to the anti-vaccine movement than RFK Jr., and his impact has been deadly. By convincing people to forgo routine pediatric vaccinations, he has endangered the lives of thousands of kids, stoked fear in families with autistic children, and in at least once instance was partially responsible for a devastating outbreak of measles. In 2019, 83 people, mostly children, died of the preventable disease in Samoa. While Kennedy has denied that his words and actions were responsible for the outbreak, he has supported anti-vaccination efforts on the islands, written to the nation’s prime minister about the dangers of vaccines, and visited Samoa to meet with anti-vaxxers and subsequently praised them for their work. As Derek Lowe, a columnist from the United States’ leading scientific journal, Science, has said: “Kennedy’s views on science and medicine are not only wrong, they are actively harmful and destructive. He has used them to make a great deal of money, and he has lied about them to interviewers and reporters whenever he finds it convenient.”
...
RFK Jr. is the poster boy for the new Trump administration, a rich man who never has had to worry about a thing in his life, putting the lives of ordinary Americans in jeopardy because he thinks he knows better than scientists. In fact, the man who thought it was a good idea to stage a hit-and-run with a dead baby bear and a bicycle in Central Park has shown a lack of judgment across the board for a long while. But he is part of an emerging kakistocracy-in-waiting that will be run by plutocrats and zealots. Our public health system in America is fragile and shouldn’t be a plaything. Once he’s done with his games, all the king’s horses and all the king’s men may not be able to put our public health infrastructure back together again. The damage may be lasting and profound.
But we are not powerless. So much of public health happens locally—and we can protect this precious national resource by speaking up and speaking out, at our city or town council meetings, calling and writing our state representatives, our mayors and our governors. This is going to be necessary work. As my Yale colleague Timothy Snyder has said: “Defend institutions.… Institutions do not protect themselves. So choose an institution you care about and take its side.” This may be your local public health department or Planned Parenthood clinic, a mental health clinic or needle exchange program, or services for LGBTQ+ or immigrant populations in your neighborhood.
These are all part of what makes public health happen day in and day out in our communities. Deprive RFK Jr. and Donald Trump of their power; take it away from them with focus and tenacity. Chip away at their campaign to destroy public health in America. These kinds of small acts will add up and will make a difference. If these men are the disease, let us be the cure."
53 notes
·
View notes
Text
H5N1: What to know before fear spreads
What is H5N1?
H5N1 is a 1996 strain of the Spanish or Avian Flu first detected in Chinese birds before spreading globally across various avian species. H5N1 is similar to H1N1, but spreads slower and has a much higher mortality rate.
H5N1 may also be referred to as Influenza A. The American Association of Bovine Practitioners has seen fit to rename H5N1 to Bovine Influenza A Virus, or BIAV, and are encouraging others to use the same terminology.
I would not be surprised if the colloquial name among the public becomes Bovine Flu or American Flu in the coming months, and may be referred to as the Chinese Flu by the same folks who took the spark of the SARS-CoV-2 (COVID-19) pandemic as an excuse to be publicly racist to East Asian people without social repercussions.
BIAV is a virus, meaning that it is a (probably) non-living packet of self-replicating infectious material with a high rate of mutation. BIAV is structured similarly to SARS-CoV-2, having a packet of infectious material encased in a spherical shell with a corona, or crown, of proteins that can latch to living cells to inject RNA.
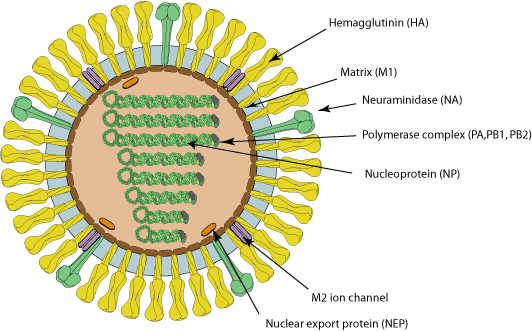
Image source with interactive model: ViralZone - H5N1 subtype
What is the history of BIAV?
In 1996 and 1997, an outbreak of BIAV occurred among poultry and infected 18 people in Hong Kong, 6 of which died. This seemingly isolated incident then infected ~860 people with a >50% death rate.
At the time, BIAV was known as Highly Pathogenic Avian Influenza, or HPAI, and killed nearly 100% of chickens within a 48 hour period.
From 2003 to 2005, continual outbreaks occurred in China and other East Asian countries, before spreading to Cambodia, the Netherlands, Thailand, and Vietnam.
From 2014 to 2016, it began being detected in American fowl, as well as mutating the H5N6 (lethal in birds, no human to human transmission) and H5N8 (largely spread through turkeys, ducks had immunity) viruses.
BIAV has since evolved into a clade known as 2.3.4.4b, and was first detected in 2021 in wild American birds. This then caused outbreaks in 2022 among wild and domesticated birds (such as chickens) alike, but was largely being overshadowed by the pressing SARS-CoV-2 pandemic at the time.
From 2022 to 2023, it was observed to be spreading among various mammals, including humans. Now, in 2024, we're having the most concerning rapid outbreak of BIAV since 2003.
BIAV is known to spread from mammal to mammal, particularly between cows and humans. BIAV may also be spread from cow to cow (highly likely, but not confirmed - this is likely the reason the virus has spread to Idaho from Texan cattle), and is known to be lethal to domestic cats and birds within 48 hours.
How does BIAV spread?
BIAV spreads through fomites - direct contact with infected animals or infected surfaces and then touching parts of your face or other orifices - as well as through airborne particulates, which may be inhaled and enter the sinuses and lungs.
BIAV is known to spread through:
Asymptomatic Ducks, geese, swans, various shorebirds
Symptomatic, may be lethal Foxes, bears, seals, sea lions, polar bears, domestic cats, dogs, minks, goats, cows, (potentially human to human, but unconfirmed - there have only been 8 potential human to human cases in 2024).
How can I protect against BIAV?
As BIAV is a type of Influenza A, existing protocols should do fine.
Current recommendations are to wash your hands vigorously after interacting with birds (I would also recommend doing this with mammals), avoid touching your face or other open orifices, and wear N95 masks.
Avoid sick or dead animals entirely - I would also recommend reporting them to your local Animal Control or veterinary centre and warning them about the infection risk. People who work with animals are recommended to also wear full PPE such as N95 masks, eye protection, gloves, and partake in vigorous hand washing.
If you suspect you've caught BIAV, seek medical attention immediately. Existing medications such as oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil can reduce BIAV's ability to replicate.
Standard flu shots will not protect against BIAV. Remember - symptoms of BIAV may not manifest for between 2 to 8 days, and potentially infected people should be monitored for at least 10 days.
How far has BIAV spread?
BIAV is currently a global virus, though the current infection location of note is the United States.
Image Key: Dark red - Countries with humans, poultry and wild birds killed by H5N1 Deep red - Countries with poultry or wild birds killed by H5N1 and has reported human cases of H5N1 Light red - Countries with poultry or wild birds killed by H5N1
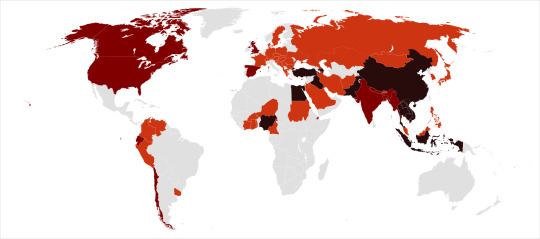
Image source: Wikipedia - Influenza A virus subtype H5N1 - File: Global spread of H5N1 map
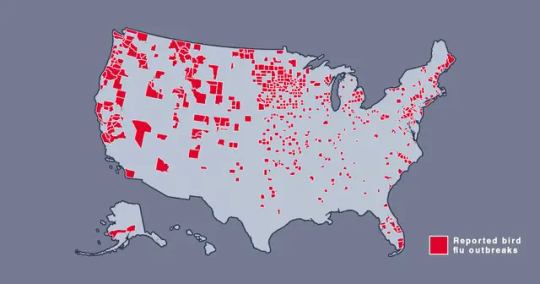
Image source: Metro.co.uk - Map shows where bird flu is spreading in US amid new warning - File: The Centers for Disease Control and Prevention’s H5N1 bird flu detections map across the United States
Should I be afraid?
You needn't be afraid, just prepared. BIAV has a concerningly high lethality, but this ironically culls its spread somewhat.
In the event human to human transmission of BIAV is confirmed, this will likely mainly affect marginalized communities, poor people, and homeless people, who are likely to have less access to medical care, and a higher likelihood of working in jobs that require frequent close human contact, such as fast food or retail jobs.
Given the response to SARS-CoV-2, corporations - and probably the government - may shove a proper response under the rug and refuse to participate in a full quarantine, which may leave people forced to go to work in dangerous conditions.
If this does spread into an epidemic or pandemic, given our extensive knowledge about Influenza, and the US having a backup vaccine for a prior strain of H5N1, a vaccine should be able to be developed relatively quickly and would hopefully be deployed freely without charge - we won't have to worry about a situation like The Stand.
Wash your hands, keep clean, avoid large social gatherings where possible, wear an N95 mask if you can afford them (Remember: Cloth masks are the least protective, but are better than nothing. If you can't afford N95 masks, I recommend wearing a well-fitted cloth mask with a disposable face mask over it to prevent pneumonia from moisture buildup in the disposable mask), support the disabled, poor, and homeless, and stay educated.
We can do better this time.
Further things to check out:
YouTube: MedCram - H5N1 Cattle Outbreak: Background and Currently Known Facts (ft. Roger Seheult, M.D.)
Wikipedia - Influenza A virus subtype H5N1
Maine.gov - Avian Influenza and People
CDC.gov - Technical Report: Highly Pathogenic Avian Influenza A(H5N1) Viruses
Wikipedia - H5N1 genetic structure
realagriculture - Influenza infection in cattle gets new name: Bovine Influenza A Virus (BIAV)
#H5N1#bird flu#avian flu#bovine flu#BIAV#pandemic#epidemic#COVID 19#coronavirus#spanish flu#long post#text post#no id#undescribed#news#politics#us news#us politics#american news#american politics#world news#global news#global politics#world politics#lgbt#lgbtq#queer#trans#communist#socialist
47 notes
·
View notes
Text
Good News - May 1-7
Like these weekly compilations? Support me on Ko-fi! Also, if you tip me on Ko-fi, at the end of the month I'll send you a link to all of the articles I found but didn't use each week - almost double the content!
1. New study says conservation works, providing hope for biodiversity efforts

“A new study published in Science reveals that conservation works, with conservation actions improving or slowing the decline of biodiversity in two-thirds of the cases analyzed.”
2. Monk Seal Pup Debuts in Waikīkī on Lei Day
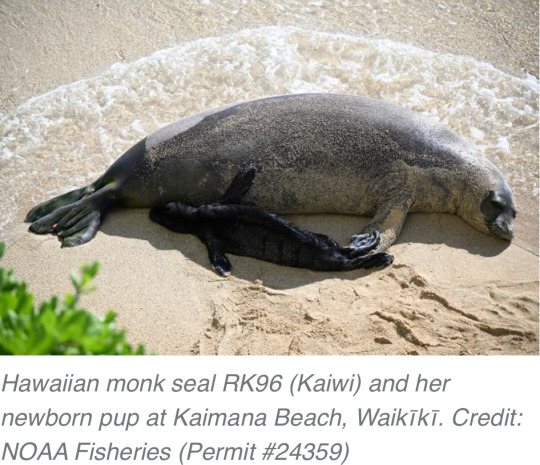
“Endangered Hawaiian monk seal RK96 (Kaiwi) gave birth to her sixth pup on popular Kaimana Beach in Waikīkī, Oʻahu! […] Hawaiian monk seals are one of the most endangered seal species in the world, so each pup represents hope for the species’ recovery.”
3. West Coast Indigenous-led marine conservation area gets global spotlight

“A coastal First Nation is celebrating global recognition of its marine protected area after recently snagging a “blue park” designation that highlights exemplary ocean conservation efforts around the world. […] Kitasu Bay supports one of the last abundant herring spawns along the central coast, vital to the nation’s communal herring roe on kelp (ROK) fishery - which harvests the protein-rich eggs but leaves the fish alive to flourish and spawn again.”
4. The number of fish on US overfishing list reaches an all-time low. Mackerel and snapper recover

“The report states that 94% of fish stocks are not subject to overfishing, which is slightly better than a year ago. The U.S. was able to remove several important fish stocks from the overfishing list, NOAA said in a statement. […] The removal of species from the overfishing list shows the U.S. is making progress, said Rick Spinrad, NOAA’s administrator.”
5. Researchers Collaborate with the Shipping Industry to Cut Costs, Fuel Consumption and Greenhouse Gas Emissions in Shipping
“Through coordinated ship scheduling and an optimisation of ship operations and port services, the objective is to achieve a substantial increase in energy efficiency and a 10-20% reduction in fuel consumption, consequently resulting in lowered greenhouse gas emissions [and] leading to substantial economic benefits for shipping and environmental advantages for society[….]”
6. The city flower farm that is changing lives

“Heart of BS13 Flowers in Hartcliffe is part of the wider Heart of BS13 charity which tackles food insecurity in south Bristol. Profits from the flower sales to run workshops, offer volunteer and trainee placements, and create education opportunities for people from Hartcliffe.”
7. Four falcon chicks hatch in Glasgow university tower

“Members of the [Glasgow Peregrine] project hope to […] fit [the chicks] with electronic tags that will enable monitoring of their movements. Mr Simpson added: "With the identification tags we can see where they have gone, how high they fly and other information that would be really useful." In recent years the group have held peregrine watches at the university, allowing people to see the birds in their nest.”
8. 'Banana pingers' are saving whales and dolphins around the world

“[T]he Kibel brothers, Pete (a fisheries biologist) and Ben (an engineer) […] have been utilising light to protect turtles, sound to protect porpoises and electro pulses to protect sharks. [… Trials] showed reduced average catch rates of blue shark by 91%, and catch rates of pelagic stingray by 71% […as well as] a fall in the number of sea turtles being trapped by 42%.”
9. New vaccine effective against coronaviruses that haven't even emerged yet
“Researchers have developed a new vaccine technology that has been shown in mice to provide protection against a broad range of coronaviruses with potential for future disease outbreaks -- including ones we don't even know about. […] The new vaccine works by training the body's immune system to recognise specific regions of eight different coronaviruses, including SARS-CoV-1, SARS-CoV-2, and several that are currently circulating in bats and have potential to jump to humans and cause a pandemic.”
10. Grassland birds, Forest birds and Other Migratory Birds to Benefit from More Than $22 Million in Funding Throughout the Americas

“This year, more than $4.87 million in federal funds will be matched by more than $17 million in partner contributions going to 30 collaborative conservation projects in 19 countries across the Americas. “These investments will [… protect] millions of acres of diverse habitats needed by grassland birds, forest birds and shorebirds for wintering, breeding and migration,” said Service Director Martha Williams.”
April 22-28 news here | (all credit for images and written material can be found at the source linked; I don’t claim credit for anything but curating.)
#good news#hopepunk#sorry its late i got distracted lol#biodiversity#conservation#seal#monk seal#hawaiʻi#oahu#first nations#fish#noaa#shipping#climate change#greenhouse gasses#ships#flowers#falcon#glasgow#university#peregrine falcon#birds#whale#dolphin#shark#turtles#vaccine#coronavirus#health#animals
21 notes
·
View notes
Note
When was the last time you and Edward hung out just the two of you?
We have been living on separate continents since the middle of 2020, when I returned to the US to deal with the SARS-CoV-2 outbreaks here and he stayed in the country we had all been living in together prior to the lockdowns. We've visited back and forth for different lengths of time; this summer Esme and I went to visit the children for a little over a month and Edward and I jogged to Portugal and spent a few days in the mountains there.
We mostly lay around in the forest, enjoyed the beautiful sunsets and sunrises, and talked. There was a lot to catch up on. WhatsApp and Facetime only suffice for so much.
23 notes
·
View notes
Text
Master Post: The Yan Papers & Supporting Evidence of an Unrestricted Bioweapon
Yan Reports
Unusual Features of the SARS-CoV-2 Genome Suggesting Sophisticated Laboratory Modification Rather Than Natural Evolution and Delineation of Its Probable Synthetic Route
SARS-CoV-2 Is an Unrestricted Bioweapon: A Truth Revealed through Uncovering a Large-Scale, Organized Scientific Fraud
The Wuhan Laboratory Origin of SARS-CoV-2 and the Validity of the Yan Reports Are Further Proved by the Failure of Two Uninvited "Peer Reviews"
Birger Sørensen, Angus Dalgleish & Andres Susrud
The Evidence which Suggests that This Is No Naturally Evolved Virus: A Reconstructed Historical Aetiology of the SARS-CoV-2 Spike
Steven C. Quay Bayesian Analysis
A Bayesian analysis concludes beyond a reasonable doubt that SARS-CoV-2 is not a natural zoonosis but instead is laboratory derived
Long history of China's CCP and Biowarfare: Analysis from Clare M. Lopez, Director of U.S. Geostrategic Security Issues for the Near East Center for Strategic Engagement (NEC-SE)
The Role of Biological Warfare in China’s Drive for Global Hegemony (Part 1) & How a CCP Operation Ensnared the US Government (Part 2)
Mixed Messaging from U.S. Government on China’s Biological Weapons Program: The involvement of U.S. government entities with Chinese biological weapons scientists and entities is deeply concerning
“Better Late Than Never?”
China’s Biological Warfare Programme: An Integrative Study with Special Reference to Biological Weapons Capabilities by Dany Shoham
This study attempts to profile China’s biological warfare programme (BWP), with special reference to biological weapons (BW) capabilities that exist in facilities affiliated with the defence establishment and the military. For that purpose, a wide variety of facilities affiliated with the defence establishment and with the military are reviewed and profiled. The outcome of that analysis points at 12 facilities affiliated with the defence establishment, plus 30 facilities affiliated with the PLA, that are involved in research, development, production, testing or storage of BW. This huge alignment might be regarded as superfluous, ostensibly; yet, considering the various factors discussed in the present study, the overall derived picture of the Chinese BW-related alignment is not at all surprising. The chances that an outstanding state like China would ignore new avenues of BW designing and deployment are a priori slim, if any. China, in all likelihood, is and will persist as a paramount BW possessor.
‘Virus warfare’ in China military documents
Chinese military scientists discussed the weaponisation of SARS coronaviruses five years before the COVID-19 pandemic, outlining their ideas in a document that predicted a third world war would be fought with biological weapons.
The Secret Speech of General Chi Haotian
The Secret Speech of General Chi Haotian. In 2005, THE EPOCH TIMES acquired a secret speech given by Defense Minister Chi Haotian to high-level Communist Party Cadres sometime before his retirement in 2003. Details given in Chi’s speech coincide with previously unpublished defector testimony on Sino-Russian military plans.
A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence (2015)
The emergence of severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome (MERS)-CoV underscores the threat of cross-species transmission events leading to outbreaks in humans. Here we examine the disease potential of a SARS-like virus, SHC014- CoV, which is currently circulating in Chinese horseshoe bat populations1. Using the SARS-CoV reverse genetics system2, we generated and characterized a chimeric virus expressing the spike of bat coronavirus SHC014 in a mouse-adapted SARS-CoV backbone. The results indicate that group 2b viruses encoding the SHC014 spike in a wild-type backbone can efficiently use multiple orthologs of the SARS receptor human angiotensin converting enzyme II (ACE2), replicate efficiently in primary human airway cells and achieve in vitro titers equivalent to epidemic strains of SARS-CoV. Additionally, in vivo experiments demonstrate replication of the chimeric virus in mouse lung with notable pathogenesis. Evaluation of available SARS-based immune-therapeutic and prophylactic modalities revealed poor efficacy; both monoclonal antibody and vaccine approaches failed to neutralize and protect from infection with CoVs using the novel spike protein. On the basis of these findings, we synthetically re-derived an infectious full-length SHC014 recombinant virus and demonstrate robust viral replication both in vitro and in vivo. Our work suggests a potential risk of SARS-CoV re-emergence from viruses currently circulating in bat populations.
The China-Led WHO Report on Coronavirus Is Deeply Suspect
The China-Led WHO Report on Coronavirus Is Deeply Suspect by Lt. Col. (res.) Dr. Dany Shoham: EXECUTIVE SUMMARY: The WHO’s China-led international investigation into the origins of COVID-19 did not trace either the genomic derivation or the initial contraction of the virus that generated the pandemic. This could be because it did not look for an unnatural scenario or because a natural scenario did not in fact occur. China appears to have essentially dictated the proceedings of the investigation, the findings of which are deeply suspect.
Discovery of a novel merbecovirus DNA clone contaminating agricultural rice sequencing datasets from Wuhan, China
Discovery of a novel merbecovirus DNA clone contaminating agricultural rice sequencing datasets from Wuhan, China
An unreported CoV infectious clone in Wuhan
Csabai et al.
Unique SARS-CoV-2 variant found in public sequence data of Antarctic soil samples collected in 2018-2019
Host genomes for the unique SARS-CoV-2 variant leaked into Antarctic soil metagenomic sequencing data
Project DEFUSE: Defusing the Threat of Bat-borne Coronaviruses
DEFUSE proposal
Nuclear translocation of spike mRNA and protein is a novel pathogenic feature of SARS-CoV-2
The spike (S) protein appears to be a major pathogenic factor that contributes to the unique pathogenesis of SARS-CoV-2. Although the S protein is a surface transmembrane type 1 glycoprotein, it has been predicted to be translocated into the nucleus due to the novel nuclear localization signal (NLS) “PRRARSV”, which is absent from the S protein of other coronaviruses. Indeed, S proteins translocate into the nucleus in SARS-CoV-2-infected cells. To our surprise, S mRNAs also translocate into the nucleus. S mRNA colocalizes with S protein, aiding the nuclear translocation of S mRNA. While nuclear translocation of nucleoprotein (N) has been shown in many coronaviruses, the nuclear translocation of both S mRNA and S protein reveals a novel pathogenic feature of SARS-CoV-2.
SARS–CoV–2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro
Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line
Unnaturalness in the evolution process of the SARS-CoV-2 variants and the possibility of deliberate natural selection
Over the past three years, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has repeatedly experienced pandemics, generating various mutated variants ranging from Alpha to Omicron. In this study, we aimed to clarify the evolutionary processes leading to the formation of SARS-CoV-2 Omicron variants, focusing on Omicron variants with many amino acid mutations in the spike protein among SARS-CoV-2 isolates. To determine the order in which the mutations leading to the formation of the SARS-CoV-2 Omicron variants, we compared the sequences of 129 Omicron BA.1-related isolates, 141 BA.1.1-related isolates, and 122 BA.2-related isolates, and tried to dissolve the evolutionary processes of the SARS-CoV-2 Omicron variants, including the order of mutations leading to the formation of the SARS-CoV-2 Omicron variants and the occurrence of homologous recombination. As a result, we concluded that the formations of a part of Omicron isolates BA.1, BA.1.1, and BA.2 were not the products of genome evolution as is commonly observed in nature, such as the accumulation of mutations and homologous recombinations. Furthermore, the study of 35 recombinant isolates of Omicron variants BA.1 and BA.2, confirmed that Omicron variants were already present in 2020. The analysis we have shown here is that the Omicron variants are formed by an entirely new mechanism that cannot be explained by previous biology, and knowing the way how the SARS-CoV-2 variants were formed prompts a reconsideration of the SARS-CoV-2 pandemic.
Further Supporting Evidence
Anomalies in BatCoV/RaTG13 sequencing and provenance
Time Shows That The ‘Paranoid’ People Were Correct About COVID
Molecular Biology Clues Portray SARS-CoV-2 as a Gain-of-Function Laboratory Manipulation of Bat CoV RaTG13
The genetic structure of SARS-CoV-2 does not rule out a laboratory origin: SARS-COV-2 chimeric structure and furin cleavage site might be the result of genetic manipulation
A look at China’s biowarfare ambitions
Mountains of circumstantial evidence point toward early circulation of SARS-CoV-2
Breaking: SARS-CoV-2 Spike found in bacteria samples taken from China, 2019
Unique SARS-CoV-2 genomes found in Antarctic samples raises questions about SARS-CoV-2 origin, lineages
The Galveston National Lab and Wuhan Institute of Virology
US University Concedes It May Have Broken Law in Contract With Wuhan Lab
Judicial Watch: New Documents Reveal COVID-19 Vaccine Studies Used by HHS were Conducted in China
JW v HHS Wuhan August 31 2021 00696
Flavinkins Archives
THE NATIONAL INSTITUTES OF HEALTH AND ECOHEALTH ALLIANCE DID NOT EFFECTIVELY MONITOR AWARDS AND SUBAWARDS, RESULTING IN MISSED OPPORTUNITIES TO OVERSEE RESEARCH AND OTHER DEFICIENCIES
U.S. Army Medical Research and Development Command (USAMRDC) COVID-19 Common Operational Picture
SELLIN: Is China’s Military Making COVID-19 Variants?
Enhancing Protein Expression by Leveraging Codon Optimization
Engineered bat virus stirs debate over risky research
So, COVID-19 is a Bioweapon After All, The Times ExplainsSars-Cov-2 is a result of bioweapons research, and work of Ralph Baric and Peter Daszak
Journalistic Investigations
The origin of COVID: Did people or nature open Pandora’s box at Wuhan?
What really went on inside the Wuhan lab weeks before Covid erupted?New fresh evidence drawn from confidential reports reveals Chinese scientists spliced together deadly pathogens shortly before the pandemic, the Sunday Times Insight team report
New Emails Chronicle Lab-Leak Coverup in Real Time
Francis Collins and Anthony Fauci emailed about whether NIH funded Wuhan lab before secret call
Pentagon gave millions to EcoHealth Alliance for weapons research program
Leaked Chinese document reveals a sinister plan to ‘unleash’ coronaviruses
BREAKING: DOD CONTROLLED COVID ‘VACCINES’ FROM THE START UNDER NATIONAL SECURITY PROGRAM – LIED THE ENTIRE TIME – Were NEVER ‘Safe and Effective’
The role of the US DoD (and their co-investors) in "covid countermeasures" enterprise.
EVOLUTION OF A THEORY: Unredacted NIH Emails Show Efforts to Rule Out Lab Origin of Covid
The U.S. Keeps Offering China Its COVID Vaccines. China Keeps Saying No
Links between the University of Texas Medical Branch in Galveston and China’s People’s Liberation Army
Broken Bioweapon: Lack of mRNA Integrity in Pfizer Batches: All Regulators Knew This When they "Pretend-Approved" the Shots
Intelligence report warned of coronavirus crisis as early as November: Sources"Analysts concluded it could be a cataclysmic event," a source said
How Did Deborah Birx Get the Job?
Do Governments Track the Injury and Kill Rates from Biowarfare Agents Deployed as mRNA/DNA "Vaccines"?
Lab Leak Most Likely Origin of Covid-19 Pandemic, Energy Department Now Says
FBI Director Says Covid Pandemic Likely Caused by Chinese Lab Leak
Wuhan lab denied BSL4 access for SARS work without clear reasoning
Videos
Proof Government Lab Created COVID, Says Escaped Chinese Virologist Dr. Li-Meng Yan – Ask Dr. Drew
Virologist Dr. Li-Meng Yan Claims Coronavirus Lab 'Cover-Up' Made Her Flee China | Loose Women
The Dr. Jordan B Peterson Podcast, Viral: The Origin of Covid 19 | Matt Ridley | EP 310
Chinese Defector: China’s Weaponization of Covid-19
Was COVID-19 made inside a Chinese lab? | Under Investigation
One Billion COVID Jabs From The CCP? Dr. Naomi Wolf Breaks Down a Disconcerting Timeline
RTE Discussions #16: Examining DoD Involvement in the Pandemic (w/ Sasha Latypova)
Major Evidence China Is Making The Pfizer Vaccine Ingredients!
Naomi Wolf Bombshell: Has China Been Using COVID Vaccines To Decimate Western Democracies?!
LNP/mRNA Is "Natural Born Killer" Says Drug Inventor Dr. Richard Urso w/ Dr Kelly Victory – Ask Dr. Drew
COVID 'Good Material For Non-Traditional Bioweapon' To Ruin Economies: Chinese Virologist
Conversation with Dr. Jane Ruby: We cover the Government-Military-BioPharma Industrial Complex and get into the question Why?
SHOCKING REVELATION - DOCTOR EXPOSES COVID BIOWEAPONS PROGRAM & REVEALS VACCINE WILL KILL MILLIONS
COVID Lab Leak Evidence: Escaped Chinese Virologist Dr. Li-meng Yan & Brian O'Shea
Dr. David Martin: Pandemic Was "Biological Weapon of Genocide" w/ Dr. Kelly Victory – Ask Dr. Drew
Illegal Biolab in CA: Escaped Virologist Warns Of CCP Spy Links w/ Dr. Li-meng Yan – Ask Dr. Drew
Books
What Really Happened In Wuhan: A Virus Like No Other, Countless Infections, Millions of Deaths by Sharri Markson (2022)
Unrestricted Warfare: China's Master Plan to Destroy America by Qiao Liang & Wang Xiangsui (2015)
Podcasts
The Voice of Dr. Yan
Neither Accidental nor Occasional, the History of CCP’s Bioweapon Program Dr. Li-Meng Yan & Clare M. Lopez
No Amnesty Should Be Given Until Investigation of COVID-19 Origin
Pfizer’s Plan of Directed Evolution vs. COVID-19 Predictor in China – Does the Nightmare Become True?
Chinese Spy Balloon is another CCP’s Unrestricted Tactic Against America
CCP promoted novel fabricated data on nature origin of COVID-19
China’s new methodology warfare; Understanding the cognitive war
#covid-19#spike protein#biological WMD#Li-Meng Yan#Yan Papers#covid-19 vaccine#Unrestricted Warfare#fifth generational warfare#fav#save for later#masterpost#most important#important#wuhan institute of virology#wuhan virology lab#furin cleavage site#Clare M. Lopez#Sasha Latypova#virology
92 notes
·
View notes
Text
Toward the end of last year, US health authorities got a tip-off about an upcoming wave of respiratory syncytial virus, a seasonal virus that kills 160,000 people globally every year. Before hospitals reported an uptick in patients, they could see that RSV was more acute in the northeast of the country, with concentrations of the virus ultimately reaching levels more than five times greater than in the western United States. Their early warning system? Wastewater.
By regularly testing virus levels in public wastewater, health institutions are able to target treatments and interventions to the worst-affected areas before doctors on the ground realize something’s going on. “If you can get the information to hospitals or clinics weeks earlier, that gives the opportunity to start thinking about what treatments they might need,” says Marisa Donnelly, senior principal epidemiologist at Biobot Analytics, which helped develop a wastewater surveillance system for the US Centers for Disease Control.
RSV is very common: Every year, 64 million people worldwide get an RSV infection, according to the US National Institute for Allergy and Infectious Diseases—but it’s particularly problematic for the very old and very young. Preventative measures are available, including vaccines and monoclonal antibodies. But often, by the time a community recognizes it has an RSV outbreak, it’s too late to mount the most effective response. Getting hold of enough drugs can also be tricky. “Wastewater analysis gives you better situational awareness of what’s going on and how much it’s fluctuating over time, because we have [historically] very much underdetected RSV cases,” says Bill Hanage, associate director of the Center for Communicable Disease Dynamics at the Harvard T.H. Chan School of Public Health.
The concept of tracking a virus through wastewater came to prominence in the early days of the Covid-19 pandemic in 2020, says Tyson Graber, associate scientist at the Children's Hospital of Eastern Ontario Research Institute, who worked on wastewater analysis as part of Ontario’s Covid response. Initially, researchers weren’t too hopeful. “Nobody thought that you could actually detect bits and pieces of material from a respiratory virus,” says Graber. Yet it proved possible: The scientists were able to detect the presence of SARS-CoV-2, the virus behind Covid-19.
This near-real-time analysis of the virus’s spread helped improve responses to the pandemic not just in Ontario, but worldwide. In the US, the CDC launched its National Wastewater Surveillance System in September 2020.
While each pathogen has its own “predilections and eccentricities,” says Graber, it was possible to adapt the process to look for RSV. Regular RSV testing in wastewater now takes place in the US, Canada, Finland, and Switzerland.
A study of the Ontario experiment in RSV wastewater tracking found that it gives more than a month’s notice in identifying when RSV season begins, and nearly two weeks’ warning of a surge, compared to waiting for people to turn up sick. “We definitely see increases in [RSV in] wastewater starting before we see those same increases in clinical data like hospitalizations,” says Donnelly.
Jasmine Reed, a CDC spokesperson, says that wastewater analysis complements other surveillance systems. “It can capture asymptomatic cases and other cases independent from medical systems, and provides a broader population-level perspective on disease spread,” she says.
The CDC’s program is set up so that, if RSV levels are high in a particular community, local health departments can prioritize interventions, including testing, infection control, and vaccination efforts.
Donnelly envisions wastewater surveillance becoming like a public health “weather app” where communities can check virus activity in their area and make informed decisions on behaviors like masking or vaccination. “We want this system to be expanded across the United States so that everybody has access to wastewater information and add additional tools to keep themselves healthy,” she says. Hanage foresees wastewater analysis being used to track other communicable viruses, like mpox.
While there’s plenty of excitement about the technique, others are more cautious. “It’s one of those sciences that has got a lot of people really excited,” says Paul Hunter, a virologist and professor in medicine at the University of East Anglia. “You either think it’s brilliant or you think it’s pointless, and there’s very little in between.”
Hunter recognizes that wastewater analysis can pick up the spread of disease—and points to evidence that it did so in the Covid-19 pandemic—but questions whether the extra cost is worth the extra insights it provides. “Certainly in Covid, we didn’t think it was [necessary] in the UK, and I think that was the correct judgment,” he says.
But proponents say it’s worth it for RSV—especially given some of the challenges around drug shortages. Last year’s RSV season proved particularly vexing to the US health system, as shortages of nirsevimab, an antibody injection given to infants, were reported across the country.
There’s hope that things will be different when RSV season begins again in the coming weeks. “If you can get the information to hospitals or clinics weeks earlier, that gives the opportunity to start thinking about what treatments they might need,” says Donnelly.
3 notes
·
View notes
Text
Antara mereka yang ditemui mati di rumah dalam 20 hari selepas vaksinasi COVID-19, 71% mempunyai punca kematian yang boleh dikaitkan dengan vaksin tersebut. Ini adalah sesuatu yang membimbangkan dan merupakan panggilan kuat untuk kajian autopsi berskala besar.
#vaksin99#suntikan vaksin#vaksinasi#vaksin#long covid#covid isn't over#covid vaccine#sars cov 2#covid 19#covid#still coviding#coronavirus#pandemic#mpox virus#virus x#x virus#virus#mpox news#mpox outbreak#mpox#monkepox#monkeypox#pfizer#modena#sinovac#astrazeneca#big pharma#new world order#world health organization#cdc
0 notes
Text
Trends in incidence of COVID 19 based on performed Rapid Antigen Test by Piratheep kumar.R in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
The COVID 19 outbreak represents a historically unprecedented pandemic, particularly dangerous and potentially lethal for elderly population. The biological differences in the immune systems between men and women exist which may impact our ability to fight an infection including SARS-2-CoV-2. Men tended to develop more symptomatic and serious disease than women, according to the clinical classification of severity. Age-related changes in the immune system are also different between sexes and there is a marked association between morbidity/mortality and advanced age in COVID-19. This is a single-center, retrospective, data oriented study performed at the private hospital, in Central Province, Sri Lanka. The data of the patients who performed the Rapid Antigen Test (RAT) to know whether they have infected by SARS-CoV-2 or not, were taken for analysis. Test performed date, age, sex, number of positive and negative cases, number of male and female patients were extracted. Finally the data were analyzed in simple statistical method according to the objective of the study. Totally 642 patients performed RAT within the period of one month from 11.08.2021 to 11.09.2021. Among them 426 (66.35%) are male and 216 (33.64%) are female. 20.4% (n=131) of male obtained positive result among the total male population (n=426). Likewise 11.4% (n=73) of female obtained positive result among the total male population (n=216). Large number of positive cases was observed (34.89%) between the age group of 31-40 years in both sexes. The age group of 21-30 and 41-50 years also were shared the almost same percentage (17.13% & 17.75). The large number of positive male patients observed among the age group of 41-50 years. Almost same number of patients was observed in the age group of 21-30 and 31-40. The least number of positive cases (0.7% and 0.9%) observed almost in 0-10 and 81-90 years. When considering the females, large number of positive female patients observed among the age group of 31-40 years.
Key words: Rapid Antigen Test, Covid-19, SARS-CoV-2
Introduction
A rapid antigen test (RAT) or rapid antigen detection test (RADT), is a rapid diagnostic test suitable for point-of-care testing that directly detects the presence of an antigen. It is used to detect SARS-CoV-2 that cause COVID-19. This test is one of the type of lateral flow tests that detect protein, differentiate it from other medical tests such as antibody tests or nucleic acid tests, of either laboratory or point-of-care types. Generally 5 to 30 minutes only will take to get result and, require minimal training or infrastructure, and cost effective (1).
Sri Lanka was extremely vulnerable to the spread of COVID-19 because of its thriving tourism industry and large expatriate population. Sri Lanka almost managed two waves of Covid-19 pandemic well, but has been facing difficulties to control the third wave. The Sri Lankan government has executed stern actions to control the disease including island-wide travel restrictions. The government has been working with its development partners to take necessary action to mobilize resources to respond to the health and economic challenges posed by the pandemic (2) (3).
The COVID 19 outbreak is dangerous and fatal for elderly population. Since the beginning of the actual SARS-CoV-2 outbreak there were an evident that older people were at higher risk to get the infection and develop a more severe with bad prognosis. The mean age of patients that died was 80 years. The majority of those who are infected, that have a self-limiting infection and do recover are younger. On the other hand, those who suffer with more severe disease require intensive care unit admission and finally pass away are older (4).
Sandoval. M., et al mentioned that the number of patients who are affected by SARS-CoV-2 with more than 80 years of age is similar to that with 65–79 years. The mortality rate in very elderly was 37.5% and this percentage was significantly higher compared to that observed in elderly. Further their findings were suggested that the age is a fundamental risk factor for mortality (5).
Since February 2020, more than 27.7 million people in US have been diagnosed with Covid-19 (6). Rates of COVID-19 deaths have increased across the Southern US, among the Hispanic population, and among adults aged 25–44 years (7). Young adults are at increased risk of SARS-CoV-2 because of exposure in work, academic, and social settings. According to the several database of different health organizations young adult, aged 18-29, were confirmed Coid-19 (9).
Go to:Amid of coronavirus disease 2019 (Covid-19) pandemic, much emphasis was initially placed on the elderly or those who have preexisting health conditions such as obesity, hypertension, and diabetes as being at high risk of contracting and/or dying of Covid-19. But it is now becoming clear that being male is also a factor. The epidemiological findings reported across different parts of the world indicated higher morbidity and mortality in males than females. While it is still too early to determine why the gender gap is emerging, this article point to several possible factors such as higher expression of angiotensin-converting enzyme-2 (ACE 2; receptors for coronavirus) in male than female, sex-based immunological differences driven by sex hormone and X chromosome. Furthermore, a large part of this difference in number of deaths is caused by gender behavior (lifestyle), i.e., higher levels of smoking and drinking among men compared to women. Lastly, studies reported that women had more responsible attitude toward the Covid-19 pandemic than men. Irresponsible attitude among men reversibly affect their undertaking of preventive measures such as frequent handwashing, wearing of face mask, and stay at home orders.
The latest immunological study on the receptors for SARS-CoV-2 suggest that ACE2 receptors are responsible for SARS-CoV-2. According to the study by Lu and colleagues there are positive correlation of ACE2 expression and the infection of SARS-CoV (10). Based on the positive correlation between ACE 2 and coronavirus, different studies quantified the expression of ACE 2 proteins in human cells based on gender ethnicity and a study on the expression level and pattern of human ACE 2 using a single-cell RNA-sequencing analysis indicated that Asian males had higher expression of ACE 2 than female (11). Conversely, in establishing the expression of ACE 2 in the primary affected organ, a study conducted in Chinese population found that expression of ACE 2 in human lungs was extremely expressed in Asian male than female (12).
A study by Karnam and colleagues reveled that CD200-CD200R and sex are host factors that together determine the outcome of viral infection. Further a review on association between sex differences in immune responses stated that sex-based immunological differences contribute to variations in the susceptibility to infectious diseases and responses to vaccines in males and females (13). The concept of sex-based immunological differences driven by sex hormone and X chromosome has been well demonstrated via the animal study by Elgendy et al (14) (35). They were concluded the study that estrogen played big role in blocking some viral infection.
The biological differences in the immune systems between men and women may cause impact on fight for infection. Females are more resistant to infections than men and which mediated by certain factors including sex hormones. Further, women have more responsible attitude toward the Covid-19 pandemic than men such as frequent hand washing, wearing of face mask, and stay at home (15).
Most of the studies with Covid-19 patients indicate that males are mostly (more than 50%) affected than females (16) (17) (18). Although the deceased patients were significantly older than the patients who survived COVID-19, ages were comparable between males and females in both the deceased and the patients who survived (18).
A report in The Lancet and Global Health 5050 summary showed that sex-disaggregated data are essential to understanding the distribution of risk, infection and disease in the population, and the extent to which sex and gender affect clinical outcomes (19). The degree of outbreaks which affect men and women in different ways is an important to design the effective equitable policies and interventions (20). A systematic review and meta-analysis conducted to assess the sex difference in acquiring COVID-19 with 57 studies that revealed that the pooled prevalence of COVID-19 confirmed cases among men and women was 55% and 45% respectively (21). A study in Ontario, Canada showed that men were more likely to test positive (22) (23). In Pakistan 72% of COVID-19 cases were male (24). Moreover, the Global Health 5050 data showed that the number of COVID-19 confirmed cases and the death rate due to the disease are high among men in different countries. This might be because behavioral factors and roles which increase the risk of acquiring COVID-19 for men than women. (25) (26) (27).
Men mostly involved in several activities such as alcohol consumption, being involved in key activities during burial rites, and working in basic sectors and occupations that require them to continue being active, to work outside their homes and to interact with other people even during the containment phase. Therefore, men have increased level of exposure and high risk of getting COVID-19 (28) (29) (30).
Men tended to develop more symptomatic and serious disease than women, according to the clinical classification of severity (31). The same incidence also noticed during the previous coronavirus epidemics. Biological sex variation is said to be one of the reasons for the sex discrepancy in COVID-19 cases, severity and mortality (32) (33). Women are in general able to stand a strong immune response to infections and vaccinations (34).
The X chromosome is known to contain the largest number of immune-related genes in the whole genome. With their XX chromosome, women have a double copy of key immune genes compared with a single copy in XY in men. This showed that the reaction against infection would be contain both innate and adaptive immune response. Therefore the immune systems of females are generally more responsive than females and it indirectly reflects that women are able to challenge the coronavirus more effectively but this has not been proven (32).
Sex differences in the prevalence and outcomes of infectious diseases occur at all ages, with an overall higher burden of bacterial, viral, fungal and parasitic infections in human males (36) (37) (38) (39). The Hong Kong SARS-CoV-1 epidemic showed an age-adjusted relative mortality risk ratio of 1.62 (95% CI = 1.21, 2.16) for males (40). During the same outbreak in Singapore, male sex was associated with an odds ratio of 3.10 (95% CI = 1.64, 5.87; p ≤ 0.001) for ITU admission or death (41). The Saudi Arabian MERS outbreak in 2013 - 2014 exhibited a case fatality rate of 52% in men and 23% in women (42). Sex differences in both the innate and adaptive immune system have been previously reported and may account for the female advantage in COVID-19. Within the adaptive immune system, females have higher numbers of CD4+ T (43) (44) (45) (46) (47) (48) cells, more robust CD8+ T cell cytotoxic activity (49), and increased B cell production of immunoglobulin compared to males (43) (50). Female B cells also produce more antigen-specific IgG in response to TIV (51).
Age-related changes in the immune system are also different between sexes and there is a marked association between morbidity/mortality and advanced age in COVID-19 (52). For example, males show an age-related decline in B cells and a trend towards accelerated immune ageing. This may further contribute to the sex bias seen in COVID-19 (53).
Hence, this single center, retrospective, data oriented study performed to identify the gender age influences the RAT results and the rate of positive cases before and after the lockdown.
Methodology
This is a single-center, retrospective, data oriented study performed at the private hospital, Central Province, Sri Lanka. The data of the patients who performed the Rapid Antigen Test (RAT) from 11.08.2021to 11.0.2021 to know whether they have infected by SARS-CoV-2 or not, were taken for analysis. The authors developed a data extraction form on an Excel sheet and the following data from main data sheet. Test performed date, age, sex, number of positive and negative cases, number of female patients and number of male patients were extracted. Mistyping of data was resolved by crosschecking. Finally the data were analyzed in simple statistical method according to the objective of the study.
Results and discussion
Totally 642 patients performed RAT within the period of one month from 11.08.2021 to 11.09.2021. Among them 426 (66.35%) are male and 216 (33.64%) are female. Men mostly involved in several activities such as alcohol consumption, being involved in key activities during burial rites, and working in basic sectors and occupations that require them to continue being active, to work outside their homes and to interact with other people even during the containment phase. Therefore, men have increased level of exposure and high risk of getting COVID-19 (28) (29) (30). The present data descriptive study also were supported certain previous research findings.
The number of male patients got positive result in RAT among the total male patients who performed RAT on every day. According to that, 20.4% (n=131) of male obtained positive result among the total male population (n=426). Philip Goulder, professor of immunology at the University of Oxford stated that women’s immune response to the virus is stronger since they have two X chromosomes which is important when talk about the immune response against SARS-Cov-2. Because the protein by which viruses such as coronavirus are detected is fixed on the X chromosome. This is exactly looks like females have double protection compare to male. The present study also showed that large number of RAT positive cases were observed in males compare to females. Gender based lifestyle would have been another possibility for large number of males got positive in RATs. There are important behavioral differences between the sexes according to certain previous research findings (54).
Shows that the number of female patients got positive result in RAT among the total female patients who performed RAT on every day. According to that, 11.4% (n=73) of female obtained positive result among the total male population (n=216).
The relations between the number of positive cases before and after the lockdown. The lockdown declared by the tenth day from the initial day when the data was taken for analysis. The red vertical line differentiates the period as two such as before and after the lockdown. Though there was no decline observed as soon as immediately considerable decline was observed after the 21 days of onset of lockdown. Staying at home, avoiding physical contacts, and avoiding exposure in crowded areas are the best way to prevent the spread of Covid – 19 (54). However the significant decline would be able to see after three weeks only from the date of lockdown since the incubation period of SARS-CoV-2 is 14-21 days. The continuous study should be conducted in order to prove it. However the molecular mechanism of COVID-19 transmission pathway from human to human is still not resolved, the common transmission of respiratory diseases is droplet sprinkling. In this type of spreading, a sick person is exposed to this microbe to people around him by coughing or sneezing. Only the way to prevent these kind of respiratory diseases might be prevent the people to make close contact (54) (55). Approximately 214 countries reported the number of confirmed COVID-19 cases (56). Countries including Sri Lanka have taken very serious constraints such as announced vacation for schools, allowed the employers to work from home and etc. to slow down the COVID 19 outbreak. The lockdown days differ by countries. Countries have set the days when the lockdown started and ended according to the COVID-19 effect on their public. Some countries have extended the lockdown by many days due to COVID-19 continues its influence intensely on the public (57) (58).
The incidence of Covid-19 and age group. Accordingly large number was observed (34.89%) between the age group of 31-40 years in both sexes. The age group of 21-30 and 41-50 years also were shared the almost same percentage (17.13% & 17.75). A study provides evidence that the growing COVID-19 epidemics in the US in 2020 have been driven by adults aged 20 to 49 and, in particular, adults aged 35 to 49, before and after school reopening (59). However many researches pointed out that adults over the age of 60 years are more susceptible to infection since their immune system gradually loses its resiliency.
The relations between the positive number of male & female patients and the age group of total patients. According to that the large number of positive male patients observed among the age group of 41-50 years. Almost same number of patients was observed in the age group of 21-30 and 31-40. The least number of positive cases (0.7% and 0.9%) observed almost in 0-10 and 81-90 years. When considering the females, large number of positive female patients observed among the age group of 31-40 years. In USA Ministry of Health has reported 444 921 COVID-19 cases and 15 756 deaths as of August 31. For men, most reported cases were persons aged 30–39 years (22.7%), followed by 20–29 year-olds (20.1%) and 40–49 year-olds (17.1%). Most reported deaths were seniors, especially 70–79 year-olds (29.5%), followed by those aged 80 years and older (29.2%), and 60–69 year-olds (22.8%). Also found a similar pattern for women, except that most deaths were reported among women aged 80 years and older (44.4%) (60).
Conclusion
The present study showed that the male are mostly got positive in RAT test than female. Further comparing the old age young age group in both sexes were noticed as positive in RAT. Moreover there were no relationship observed before and after the lockdown and trend of Covid-19
The limitations of the study
This study has several limitations.
Only 1 hospital was studied.
More than the absence of specific data on mobility patterns or transportation, detail of recovery, detail of mortality etc.
The COVID-19 pandemic is still ongoing so statistical analysis should continue. There are conflicting statements regarding lockdown by countries on COVID-19.
The effect of the lockdown caused by the COVID-19 pandemic on human health may be the subject of future work.
#Rapid Antigen Test#Covid-19#SARS-CoV-2#jcrmhs#Journal of Clinical Case Reports Medical Images and Health Sciences#Clinical decision making#Clinical Images submissions
4 notes
·
View notes
Text
Also Preserved in our archive (Daily updates!)
What if the pandemic safety net cobbled together in 2020 had been a new beginning?
What if when Joe Biden came into office in 2021, the Covid-19 safety net he was handed had become a new floor?
What if that was his baseline—and the newly elected Democratic president, sold by his most ardent supporters as FDR 2.0, had used our Covid-19 response as the bare minimum of a new social contract with Americans?
What if the caring nature of the best aspects of the US Covid response became the map for international relations—leading not just to international cooperation on infectious disease, but on matters of war, climate and genocide?
What if, instead of dismantling the vaccine-delivery infrastructure—which, at its height, delivered some four million shots in a single day—the Biden administration built upon and made some version of it permanent, so that everyone could easily get annual Covid boosters, annual flu vaccines, or get specialty vaccinations during outbreaks of unusual viruses (such as for mpox during the 2022 summer outbreak among queer men) whenever they needed it?
What if the viral surveillance and communication mechanisms utilized for learning about SARS-CoV-2, treating it and telling the public about it were being used to address H5N1—a virus which has been moving from birds to farm mammals to humans with so little notice that dead cows were killed by the “avian flu” and left on the side of a road in California’s Central Valley, as “Thick swarms of black flies hummed and knocked against the windows of an idling car, while crows and vultures waited nearby—eyeballing the taut and bloated carcasses roasting in the October heat”?What if the leaders of the Democratic party had used Covid as a blueprint to make a national platform based on care?
What if all the ways Covid had made clear how farmers, industrial butchers, kitchen staff and other food workers are the most at risk people amongst us to viral infection led to meaningful, permanent protections, such that they were much less likely to contract not just SARS-CoV-2 but H1N1, H5N1, influenza, or any other existing or novel pathogens?
What if all the all the ways Covid exposed how unsafe industrial food production is (for the workers who make it and the people who eat it alike) had triggered safety reforms, instead of having these warnings ignored and leading towards record numbers of safety recalls for e-coli, Salmonella, and Listeria?
What if an airborne pandemic had led to indoor air being as filtered, treated and regulated as drinking water?
What if everyone with a child was still getting a $300 check from the US treasury, so that having a child was not a gambling-style risk, but a responsibility shared with all of society?
What if the paused-for-years student debts were forgiven, so that young people could actually begin their lives?
What if Biden built on Americans’ experience of just showing up somewhere to get the medical care they needed to create a universal healthcare system?
(What if Kamala Harris built upon Americans’ taste of not getting charged at the point of such service—and campaigned on Medicare for All?)
What if once the link between Covid and homelessness was established, the Democrats had pushed infectious disease as just one reason for an end to evictions and a robust, public-health-backed campaign to end homelessness and stop the United States from having more people living on the streets than any other country?
What if after the link between Covid and incarceration was established, the Democrats had pursued decarceration as a public health measure and—instead of throwing weed and cryptocurrency at us—had made reducing incarceration a centerpiece of the Harris campaign to earn the votes of Black men?
(What if after 100,000 Californians died of Covid and the links between Covid, homelessness and incarceration were clear, residents of the Golden State chose to allow rent control and to abolish legal slavery in prisons—instead of voting to ban rent control and to continue prison slavery?)
What if the leaders of the Democratic party had used Covid as a blueprint to make a national platform based on care?
Would we be in the lethal position we are now—with a genocide raging abroad, Covid deaths in the hundreds every week at home, a poisoned food supply, $17 trillion in household debt, oligarch goons ready to dismantle government regulations, and a sociopath heading back into the White House—if Covid had been the floor?
#mask up#covid#pandemic#public health#wear a mask#wear a respirator#still coviding#coronavirus#covid 19#sars cov 2#us politics#democratic party#ditch the dems
63 notes
·
View notes
Quote
The US government (USG) funded and supported a program of dangerous laboratory research that may have resulted in the creation and accidental laboratory release of SARS-CoV-2, the virus that caused the Covid-19 pandemic. Following the outbreak, the USG lied in order to cover up its possible role. The US Government should correct the lies, find the facts, and make amends with the rest of the world.
Jeffrey Sachs
3 notes
·
View notes
Text
From the report by Beth Mole, posted 29 Feb 2024:
In a lengthy background document, the agency laid out its rationale for consolidating COVID-19 guidance into general guidance for respiratory viruses—including influenza, RSV, adenoviruses, rhinoviruses, enteroviruses, and others, though specifically not measles. The agency also noted the guidance does not apply to health care settings and outbreak scenarios. "COVID-19 remains an important public health threat, but it is no longer the emergency that it once was, and its health impacts increasingly resemble those of other respiratory viral illnesses, including influenza and RSV," the agency wrote. The most notable change in the new guidance is the previously reported decision to no longer recommend a minimum five-day isolation period for those infected with the pandemic coronavirus, SARS-CoV-2. Instead, the new isolation guidance is based on symptoms, which matches long-standing isolation guidance for other respiratory viruses, including influenza. "The updated Respiratory Virus Guidance recommends people with respiratory virus symptoms that are not better explained by another cause stay home and away from others until at least 24 hours after both resolution of fever AND overall symptom are getting better," the document states. "This recommendation addresses the period of greatest infectiousness and highest viral load for most people, which is typically in the first few days of illness and when symptoms, including fever, are worst." The CDC acknowledged that the eased isolation guidance will create "residual risk of SARS-CoV-2 transmission," and that most people are no longer infectious only after 8 to 10 days. As such, the agency urged people to follow additional interventions—including masking, testing, distancing, hygiene, and improving air quality—for five additional days after their isolation period. "Today’s announcement reflects the progress we have made in protecting against severe illness from COVID-19," CDC Director Dr. Mandy Cohen said in a statement. "However, we still must use the commonsense solutions we know work to protect ourselves and others from serious illness from respiratory viruses—this includes vaccination, treatment, and staying home when we get sick." Overall, the agency argued that a shorter isolation period would be inconsequential. Other countries and states that have similarly abandoned fixed isolation times did not see jumps in COVID-19 emergency department visits or hospitalizations, the CDC pointed out. And most people who have COVID-19 don't know they have it anyway, making COVID-19-specific guidance moot, the agency argued. In a recent CDC survey, less than half of people said they would test for SARS-CoV-2 if they had a cough or cold symptoms, and less than 10 percent said they would go to a pharmacy or health care provider to get tested. Meanwhile, "The overall sensitivity of COVID-19 antigen tests is relatively low and even lower in individuals with only mild symptoms," the agency said. The CDC also raised practical concerns for isolation, including a lack of paid sick leave for many, social isolation, and "societal costs." The points are likely to land poorly with critics. “The CDC is again prioritizing short-term business interests over our health by caving to employer pressure on COVID guidelines. This is a pattern we’ve seen throughout the pandemic,” Lara Jirmanus, Clinical Instructor of Medicine at Harvard Medical School, said in a press release last month after the news first broke of the CDC's planned isolation update. Jirmanus is a member of the People's CDC, a group that advocates for more aggressive COVID-19 policies, which put out the press release. Another member of the group, Sam Friedman, a professor of population health at NYU Grossman School of Medicine, also blasted the CDC's stance last month. The guidance will "make workplaces and public spaces even more unsafe for everyone, particularly for people who are high-risk for COVID complications," he said.
But, the CDC argues that the threat of COVID-19 is fading. Hospitalizations, deaths, prevalence of long COVID, and COVID-19 complications in children (MIS-C) are all down. COVID-19 vaccines are safe and effective at preventing severe disease, death, and to some extent, long COVID—we just need more people to get them. Over 95% of adults hospitalized with COVID-19 in the 2023–2024 respiratory season had no record of receiving the seasonal booster dose, the agency noted. Only 22% of adults got the latest shot, including only 42% of people ages 65 and older. In contrast, 48% of adults got the latest flu shot, including 73% of people ages 65 and older. But even with the crummy vaccination rates for COVID-19, a mix of past infection and shots have led to a substantial protection in the overall population. The CDC even went as far as arguing that COVID-19 deaths have fallen to a level that is similar to what's seen with flu. "Reported deaths involving COVID-19 are several-fold greater than those reported to involve influenza and RSV. However, influenza and likely RSV are often underreported as causes of death," the CDC said. In the 2022–2023 respiratory virus season, there were nearly 90,000 reported COVID-19 deaths. For flu, there were 9,559 reported deaths, but the CDC estimates the true number to be between 18,000 and 97,000. In the current season, there have been 32,949 reported COVID-19 deaths to date and 5,854 reported flu deaths, but the agency estimates the real flu deaths are between 17,000 and 50,000. "Total COVID-19 deaths, accounting for underreporting, are likely to be higher than, but of the same order of magnitude as, total influenza deaths," the agency concluded.
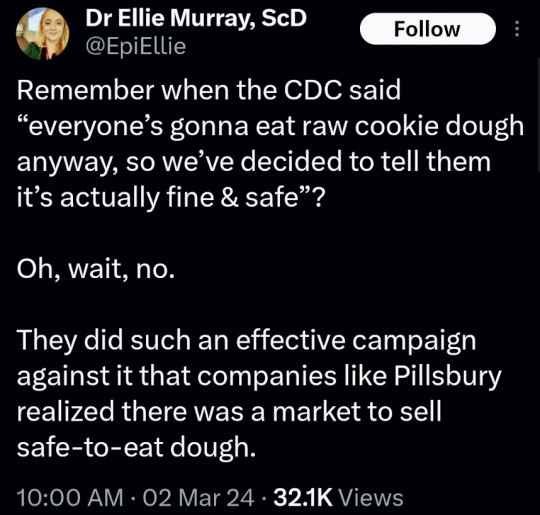
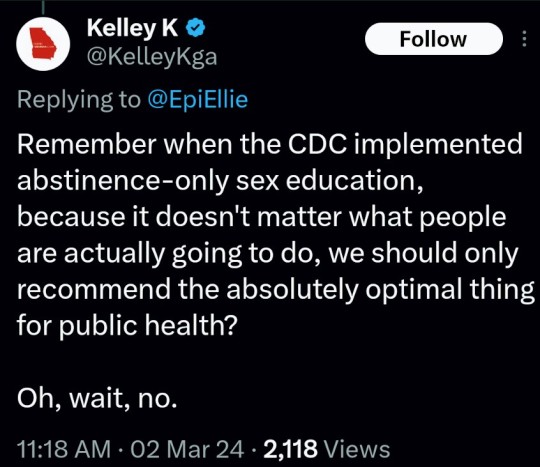
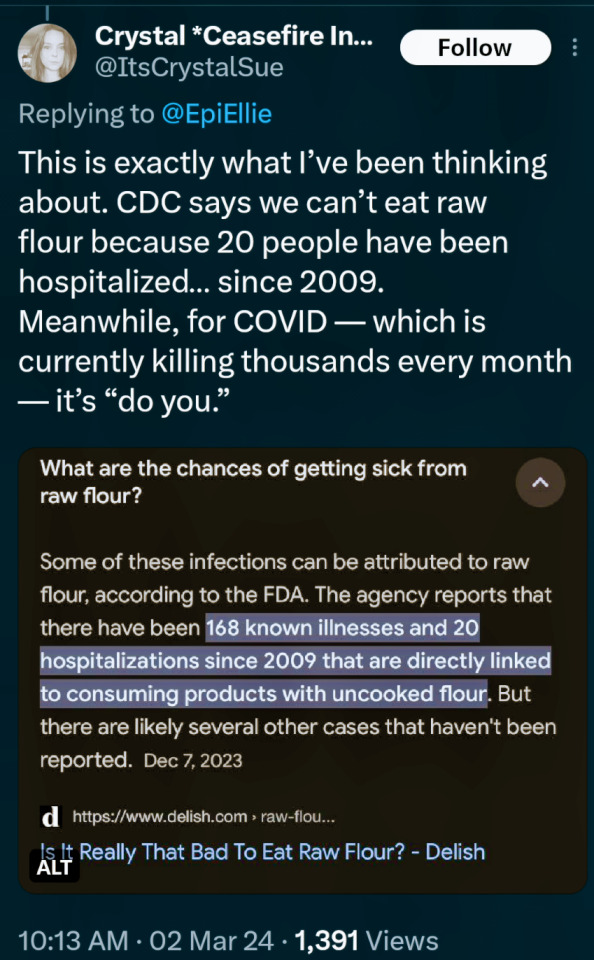
(say no to raw dough: CDC)
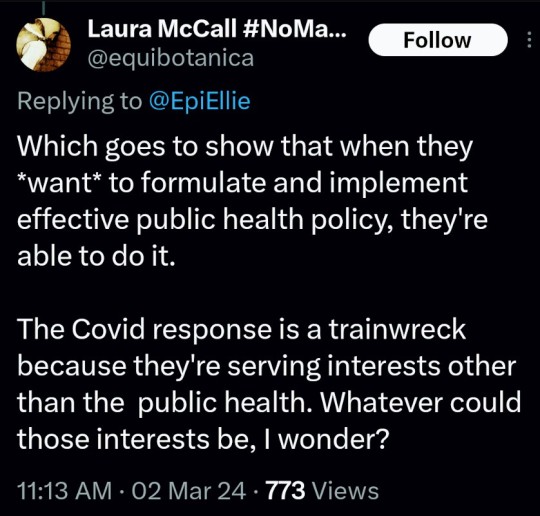
#please stay safe#the vaccines are safe#yes the covid shot is safe#covid is not a hoax#covid causes permanent long term damage to your body even if you're healthy#news#scicomm#science#ars technica#covid--19#coronavirus#beth mole#pandemic#the cdc#centers for disease control#5 day covid isolation#yes you should stay home for at least 5 days if you test positive for covid#Open windows to ventilate indoor space with outdoor air to prevent virus transmission#Wear a mask that doesn't touch your lips#keep distance from others
5 notes
·
View notes