#research. and talk to a queer doctor or someone you trust. your health is not something to be taken lightly
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has 4 main sources of revenue.
Text

i believe this is what op is referring to. it's not guaranteed and this specific situation is mostly in regards to taking it alongside SSRIs. from what i can tell a lot of people take ashwagandha every day (though the common recommendation is up to 3 months.) the hormone effects are real to my knowledge but long-term safety is unknown. meaning theres no guarantee in either direction. people just have to be safe, talk to your doctor for advice and guidance!
thank you for bringing this to people's awareness op!
here's the article i found: https://www.goodrx.com/well-being/supplements-herbs/ashwagandha-drug-interactions
https://www.goodrx.com/well-being/supplements-herbs/ashwagandha-drug-interactions
and here's another one: https://medlineplus.gov/druginfo/natural/953.html
Don't Fall for this scam.
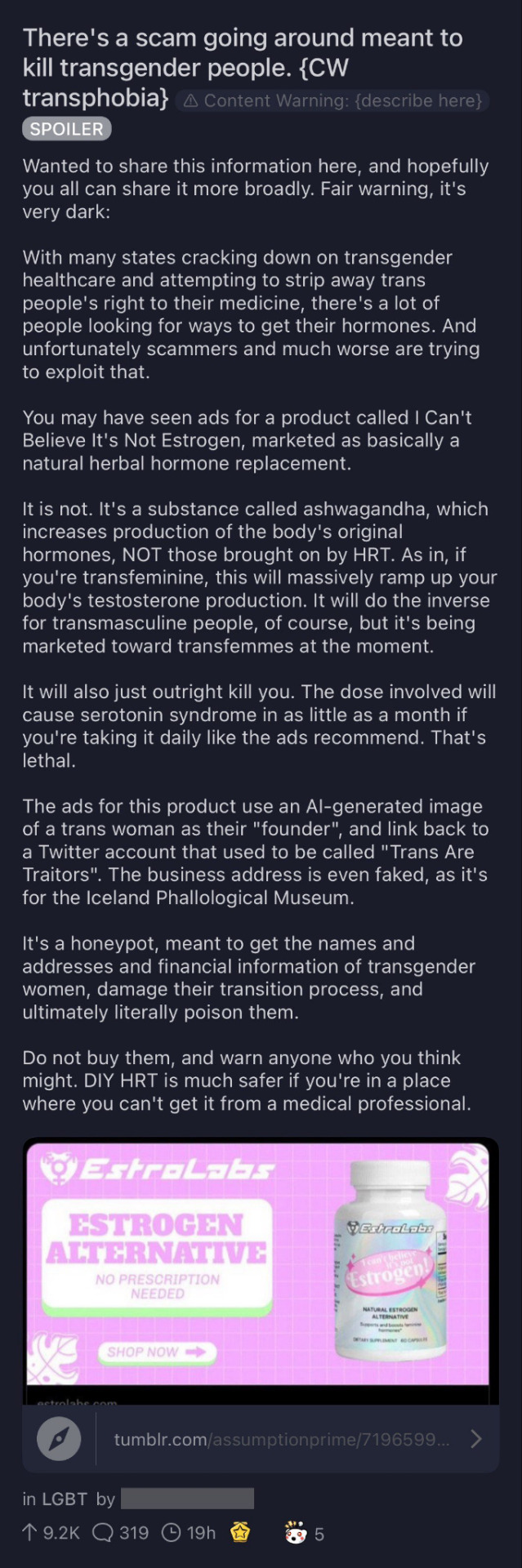
Transgender community, please please please do NOT use this product! It will kill you if used, please do not use it whatsoever.
Please reblog and spread the word
#no hate to anyone i just don't want people to get really scared when scams like this have always been super prevalent. research research#research. and talk to a queer doctor or someone you trust. your health is not something to be taken lightly
21K notes
·
View notes
Note
CW for medical stuff, mother abuse, transphobia, suicide and SH mentions
so i’m doing this whole host of tests in a hospital to figure out if anything besides fibromyalgia is wrong with me. I made the mistake of telling a psychologist that i experience ONE very specific delusion not related to my physical health even tangentially, and next thing I know the doctor diagnoses me with somatic symptom disorder. I experience more than one delusion but even then i knew telling him about the others would be a bad move. (my mom doesn’t i have delusions, so she doesn’t know this could be contributing to the diagnosis) I researched SSD, and I don’t fit the criteria for it in any way other than ‘has anxiety’. It isn’t even germ or illness related anxiety.
anyways, my DEAR, LOVELY mother immediately believes the doctor and I can’t convince her that it’s because of my (professionally diagnosed) fibromyalgia now. She also recently revealed that she’s basically a TERF lite, and I’m nonbinary.
I don’t know how i’m going to survive this, my mom now thinks my chronic illness is all in my head because of an ableist doctor who took advantage of my trust, and she thinks that all of my queer identities are either phases or because ‘‘‘‘being trans is a trend’’’’ and only supports me when we’re in public. She makes a halfhearted attempt when we’re alone but I can’t talk about medical transition because she’ll go on rants about how testosterone is being handed out like candy to 11 year old girls and how there’s a rash of new gender clinic that let children have permanent surgeries in the name of transition.
I don’t want to kill myself, but I suffer from severe depression and self harm, and I’m genuinely scared of harming or killing myself. I have an appointment with my really fucking cool therapist who actually believes me and doesn’t use the fact that I have trauma based delusions against me, but I don’t know if that will help because i haven’t felt this hopeless and in danger in a very long time. I don’t know who else to tell this to, i’m sorry if it’s too much or if i’m just being overdramatic.
Hi anon,
You are absolutely not being dramatic at all. You deserve so much better than this and I’m so sorry that the doctor took advantage of your trust.
I really hope that your appointment with your therapist went well. And even if one session was not helpful, I do think it is possible more sessions would be. While I don’t think she can fix everything, I think that feeling like someone is in your corner can make a world of difference.
Do any followers have suggestions/advice?
#mod april#trauma talks#tw self harm#tw suicide mention#tw transphobia#tw medical#tw abuse#tw mother abuse
4 notes
·
View notes
Text
An ask I got recently:
hi so i’m a transmed and i’m not sure if you’ll answer this because of that but i saw your post about transmedicalism and was wondering if you could expand on that? you seem like a genuinely kind and judgement-free person, thank you darling x
My response:
Heh, you call me “judgement-free” and ask for my opinion on a topic I’ve formed a lot of judgments about… I get it though, I’m not into attacking people for what they believe so much as providing FACTS. As a cis queer, my insight into transmedicalism isn’t really about the innate experience of trans-ness so much as using my education and professional experience to talk about social science research, diagnostic systems, and public health policy.
This ended up really long, so the tl;dr is, I think transmedicalism as I understand it:
Misunderstands why and how the DSM’s Gender Dysphoria diagnosis was written,
Treats the medical establishment with a level of trust and credibility it doesn’t deserve, at a time when LGBT+ people, especially trans people, need to be informed and vigilant critics of it, and
Approaches the problem of limited resources in an ass-backwards way that I think will end up hurting the trans community in the long run.
TW: Transphobia; homophobia; suicide; institutionalization; torture; electroshock therapy; child abuse; incidental mentions of pedophilia.
So first off I’m guessing you mean this post, about not trusting the medical establishment to tell you who you are? That’s what I’m trying to elaborate on here.
I have to admit, when you say “I’m a transmedicalist” that tells me very little about you, because on Tumblr the term seems to encompass a dizzying array of perspectives. Some transmedicalists believe in what seems to me the oldschool version of “The only TRUE trans people suffer agonizing dysphoria that can only be fixed with surgery and hormones, everyone else is an evil pretender stealing resources and can FUCK RIGHT OFF” and others are like, um… “I have total love and respect for nonbinary and nondysphoric trans people! I qualify for a DSM diagnosis of dysphoria but that doesn’t make me inherently better or more trans than anyone else.”
Which is very confusing to me because according to everything I’ve learned, the latter opinion is not transmedicalism. It’s just… a view of transness that acknowledges current diagnostic labels and scientific research. It’s what most people who support trans rights and do not identify as transmedicalists believe. But I kind of get the impression that Tumblr transmedicalism has expanded well past its original mandate, to the point that if a lot of “transmedicalists” saw the movement’s original positions they’d go “Whoa that’s way too strict and doesn’t help our community, I want nothing to do with it.”.
Okay so. Elaborating on the stuff I can comment on.
1. DSM what?
The American Psychiatric Association publishes a big thick book called The Diagnostic and Statistical Manual of Mental Disorders, called the DSM for short. This is the “Bible of psychiatry”, North America’s definitive listing of mental disorders and conditions. It receives significant revision and updates roughly every 10-15 years; it was last updated in 2013, meaning it will likely get updated sometime between 2023 and 2028.
The DSM lists hundreds of “codes”, each of which indicates a specific kind of mental disorder. For example, 296.23 is “Major depressive disorder, Single episode, Severe,” and 300.02 is “Generalized anxiety disorder.” These codes have information on how common the condition is, how it’s diagnosed, and what kind of treatment is appropriate for it.
Diagnostic codes are the key to health professionals getting paid. If there isn’t a code for it, we can’t get paid for it, and therefore we have very few resources to treat it with. The people who actually pay for healthcare–usually insurance companies or government agencies–decide how much they will pay for each code item to be treated. They’ll pay for, say, three sessions of group therapy for mild depression (296.21), or they’ll pay for more expensive private therapy if it’s moderate (296.22); they’ll pay for the cheap kind of drug if you have severe depression (296.23), but to get the more expensive drug, you need to have depression with psychotic features (296.24).
Healthcare companies, especially in the USA where the system is very very broken and the DSM is written, are cheap bastards. If they can find an excuse not to fund some treatment, they’ll use it. “We think this person who lost their job and can’t get off the couch should pay this $1000 bill for therapy,” they’ll say. “After all, they were diagnosed as code 296.21, and then saw a private therapist for five sessions, when we only allow three sessions of group therapy, and you’re saying they haven’t had enough treatment yet?”
A lot of the advocacy work mental health professionals do is trying to get the big funding bodies to pay us adequately for the work we do. (This is a much easier process in countries with single-payer healthcare, where this negotiation only needs to be done with a single entity. In the USA, it needs to be done with every single health insurance company in existence, as well as the government, sometimes differently in every single state, and then again on a case-by-case basis as well.) Healthcare providers have to argue that three sessions of group therapy isn’t enough, that Medicaid needs to pay therapists more per hour than it costs those therapists to rent a room to practice in, or else therapists would lose money by seeing Medicaid clients. DSM codes exist a tiny bit to let us communicate with each other about the people we treat, and a huge amount to let us get paid. The fact that their existence lets people make sense of their own experiences and find a community with people who share common experiences and interests with them is a very minor side benefit the DSM’s authors really don’t keep in mind when they update and revise different diagnoses.
So when it comes to convincing insurance companies to pay for treatment, humanitarian reasons like “they’ll be very unhappy without it” tend not to work. The best argument we have for them paying for psychological treatment is that it’s economical: that if they don’t pay for it now, they’ll have to pay even more later. If they refuse to pay, let’s say, $2000 to treat mild depression when someone loses their job, and either refuse treatment or stick the person with the bill, then that person’s life might spiral out of control–they might, let’s say, run low on money, get evicted from their apartment, develop severe depression, attempt suicide, and end up in hospital needing to be medically resuscitated and then put in an inpatient psych ward for a month. The insurance company then faces the prospect of having to pay, let’s say, $100,000 for all that treatment. At which point somebody clever goes, “Huh, so it would have been cheaper to just… pay the original $2000 instead so they could bounce back, get a new job, and not need any of this treatment later.”
Trans healthcare can be kind of expensive, since it often involves counselling, years of hormone therapy, medical garments, and multiple surgeries. Health insurance companies hate paying for anything, and have traditionally wanted not to cover any of this. “This is ridiculous!” they said. “These are elective cosmetic treatments, it’s not like they’re dying of cancer, these people can pay the same rate for breast enhancements or testosterone injections as anyone else.”
So when the APA Task Force on Gender Identity Disorder (a task force comprised, as far as I can tell, entirely of cis people) sat down to plan for the 2013 update of the DSM, one of their biggest goals was: Treatment recommendations. Create a diagnosis which they could effectively use to advocate that insurance companies fund gender transition. Like when you go back and read the documents from their meetings in 2008 and 2011, their big thing is “create a diagnosis that can be used to form treatment recommendations.” So that’s what they did; in 2013 they made the GD diagnosis, and in 2014 the Affordable Care Act required insurers to provide treatment for it.
A lot of trans people weren’t happy with the DSM task force’s decisions, such as the choice to keep “Transvestic Fetishism,” which is basically the autogynephilia theory, and just rename it “Transvestic Disorder”. The creation of the Gender Dysphoria diagnosis, basically, was designed to force the preventive care argument. They didn’t think they could win on trans healthcare being a necessity because healthcare is a human right, so they went with: Trans people have a very high suicide rate, and one way to bring it down is to help them transition. One of the major predictors of suicidality is dysphoria. The more dysphoric someone is, the more likely they are to attempt suicide (source). Therefore, health insurers should fund treatment for gender dysphoria because it was cheaper than paying for emergency room admissions and inpatient psychiatric hospitalizations.
I have spoken to trans scientists about what research exists, and my understanding is: The dysphoria/no dysphoria split is not actually validated in the science. That is, when you research trans people, there is not some huge gaping difference between the experiences, or brains, of people With Dysphoria, and people Without Dysphoria. Mostly, scientists haven’t even thought it was an important distinction to study. The diagnosis wasn’t reflecting a strong theme in the research about trans experiences; that research showed that trans people with all levels of dysphoria were helped with medical transition. The biggest difference is just that dysphoria is a stronger risk factor for suicide. Experiencing transphobia is another strong risk factor, but that’s harder to measure in a doctor’s office, so dysphoria it was.
(I’ve seen some transmedicalists claim that dysphoria’s major feature is incongruence, not distress. And I’ll just say, uh… in psychology, “dysphoria” is the opposite of of “euphoria”, literally means “excessive pain”, and is used in many disorders to describe a deep-seated sense of distress and wrongness. As a mental health professional, I just can’t imagine most of my colleagues agreeing that something can be called “dysphoria” if the person doesn’t feel real distress about it. If you want a diagnosis that doesn’t demand dysphoria, you’d need Gender Incongruence in the upcoming version of the ICD-11, which is the primary diagnostic system used in Europe, published by the World Health Organization.)
2. Doctors are not magic
Medicine is a science, and science is a system of knowledge based on having an idea, testing it against reality, and revising that knowledge in light of what you learned. We’re learning and growing all the time.
I don’t know if this sounds painfully obvious or totally groundbreaking, but: Basically all medical research is done by people who don’t have the condition they’re writing about. Psychology has a strong historical bias against believing the personal testimonies of people with conditions that have been deemed mental disorders, so researchers who have experienced the disorder they’re writing about have often had to hide that fact, like Kay Redfield Jamison hiding that she had bipolar disorder until she became a world-renowned expert on it, or Marsha Linehan hiding that she had borderline personality disorder until she pioneered the treatment that could effectively cure it. Often, having a condition was seen as proof you couldn’t actually have a truthful and objective experience of it.
So what I’m trying to say is: The “gender dysphoria” diagnosis was written and debated, so far as I can tell, by entirely cis committee members. The vast majority of psychological and psychiatric research about LGBT+ people is written by cisgender heterosexual scientists. Most clinical and scientific writing has been outsider scientists looking at people they have enormous power over and making decisions about their basic existence with very little accountability.
And to show you how far we’ve come, I want to show you part of the DSM as it was from 1952 to 1973. It shows you just why so many older LGBT+ people find it deeply ironic that now the DSM is being held up as definitive of trans experience:
302 Sexual Deviation This category is for individuals whose sexual interests are directed primarily toward objects other than people of the opposite sex, toward sexual acts not usually associated with coitus, or towards coitus performed under bizarre circumstances as in necrophilia, pedophilia, sexual sadism, and fetishism. Even though many find their practices distasteful, they remain unable to substitute normal sexual behavior for them. This diagnosis is not appropriate for individuals who perform deviant sexual acts because normal sexual objects are not available to them.
302.0 Homosexuality 302.1 Fetishism 302.2 Pedophilia 302.2 Transvestitism […]
Yes, really. That is how psychiatry viewed us. At a time when research from other fields, like psychology and sociology, were showing that this view was completely unsupported by evidence, psychiatry thought LGBT+ people were fundamentally disordered, criminal, and incapable of prosocial behaviour.
My favourite retelling of the decades of activism it took LGBT+ people and allies to get the DSM to change is from a friend who did her master’s thesis on the topic, because she leaves in the clown suits and gay bars, which really shows how scientific and dignified the process was. The long story short is: It took over 20 years of lobbying by LGBT+ people who were sick and tired of being locked up in mental institutions and subjected to treatments like electroshock training, as well as by LGBT+ social scientists, clinicians, and psychiatrists, to get homosexuality declassified as a mental illness. And that was homosexuality; the push to change how trans people were listed in the DSM is very recent, as seen in the latest version listing “Transvestic Disorder”, a description very few trans people ever use for themselves.
Here are a few more examples of how people with a condition have had to take an active part in the science about them:
When HIV/AIDS appeared in the USA, the government didn’t care why drug addicts and gay people were dying mysteriously. Hospitals refused to treat people with this mysterious new disease. AIDS patients had to fight to get any funding put into what AIDS is, how it spreads, or how it could be treated; they also had to campaign to change the massive public prejudice against them, so they could be treated, housed, and allowed to live. Here’s an article on the activist tactics they used. If you want an intro to the fight (or at least, white peoples’ experience of it), you could look into the movies How to Survive a Plague, And the Band Played On, and The Normal Heart.
Chronic Fatigue Syndrome (CFS) is a little-understood disease that causes debilitating exhaustion. It’s found twice as often in women as men. Doctors understand very little about what it is or why it happens, and patients with CFS are often written off a lazy hypochondriacs who just don’t want to try hard. There are basically no known treatments. In 2011, a British study said that an effective treatment for CFS was “graded exercise”, a program where people did slowly increasing levels of physical activity. This flew in the face of what people with CFS knew to be true: That their disease caused them to get much worse after they exercised. That for them, being forced to do ever-increasing exercise was basically tantamount to torture, so it was very concerning that health authorities and insurance companies began requiring that they undergo graded exercise treatment (and parents with children with CFS had to put their children through this treatment, or lose custody for “medical neglect”). So they investigated the study, found that it was seriously flawed, got many health authorities to reverse their position on graded exercise, and have made strides into pointing researchers to looking into biological causes of their illness.
Amyotrophic lateral sclerosis (ALS) is a rare but debilitating disease that isn’t researched much, because it affects such a small portion of the population. The ALS community realized that if they wanted better treatment, they would need to raise the money for research themselves. In 2014 they organized a viral “ice bucket challenge” to get people to donate to their cause, and raised $115 million, enough to make significant advances in understanding ALS and getting closer to a cure.
A common treatment for Autism is Applied Behaviour Analysis (ABA), which is designed to encourage “desired” behaviours and discourage “undesired” ones. The problem is, the treatment targets behaviour an Autistic person’s parents and teachers consider desirable or undesirable, without consideration that some “undesired” behaviours (like stimming) are fundamental and necessary to the wellbeing of Autistic people. Furthermore, the treatment involves punishing Autistic children for failure to behave as expected–in traditional ABA, by witholding rewards or praise until they stop, or in more extreme cases, by subjecting them to literal electric shocks to punish them. (In that last case, they’ve been ordered to stop using the shock devices by August 31, 2020. That only took YEARS.) Autistic people have had to campaign loud and long to say that different treatment strategies should be researched and used, especially on Autistic children.
So I mean… I get that the medical model can provide an element of validation and social acceptance. It can feel really good to have people in white coats back you up and say you’re the real deal. But if you get in touch with most LGBT+ and transgender groups, they’d say that there’s still a lot of work to be done when it comes to researching trans issues and getting scientific and governmental authorities to recognize your rights to social acceptance and medical treatment.
Within a few years, the definition you’re resting on will turn to sand beneath your feet. The Great DSM Machine will begin whirring into life pretty soon and considering what revisions it has to make. You’ll have an opportunity to make your voice heard and to push for real change. So… do you want to be part of that process of pushing trans rights forward, or do you just want to feel loss because they’re changing your strict definition of who’s valid and who’s not?
3. Scarcity is not a law of physics
One of the major arguments I see transmedicalists push is that there’s only a limited number of surgeries or hormone prescriptions available, so it’s not okay for a non-dysphoric person to “steal” the resources that another trans person might need more. This makes sense in a limited kind of way; it’s a good way to operate if, say, you’re sharing a pizza for lunch and deciding whether to give the last slice to someone who’s hungry and hasn’t eaten, or someone who’s already full.
When you start to back up and look at really big and complex systems–basically anything as big, or bigger, than a school board or a hospital or a municipal government–it’s not a helpful lens anymore. Because the most important thing about social institutions is that they can change. We can make them change. And the most important factor in how much the world changes is how many people demand that it change.
I’ve talked about this before when it comes to homeless shelters, and how the absolute worst thing they can have are empty beds. I used to work in women’s shelters, which came about when second-wave feminists started seriously looking at the problem of domestic violence in the 1960s and 70s, It was an issue male-dominated governments and healthcare systems hadn’t taken seriously before, but feminists started heck and did research and staged demonstrations and basically demanded that organizations that worked for the “public benefit” reduce the number of women being killed by their husbands. Their research showed that the leading cause of death in those cases were when women tried to leave and their partners tried to kill them, so the most obvious solution was to give them someplace safe to go where their partners couldn’t find them. Therefore the solution became: Women’s shelters. When feminists committed to founding and running these shelters, local governments could be talked into giving them money to keep them running.
(Men’s rights activists, the misogynist kind, like to whine about “why aren’t there men’s shelters?” and the very simple answer is: Because you didn’t fight for them, you teatowels. Whether a movement gets resources and funding is hugely a reflection of how many people have said, “This needs resources and funding! Look, I’m writing a cheque! Everyone, throw money at this!” In other news, The BC Society for Male Survivors of Sexual Abuse does great work. People should throw money at them.)
When the system in power knows there are resources it wants and doesn’t have, it finds a way to make them appear. For example, in Canada, the government knows that it doesn’t have enough trained professionals living in its far North, where the population is scarce and not very many people want to live. Doctors and teachers would prefer to live in the southern cities. But because it’s committed to Northern schools and hospitals, they create incentives. For example, the government offers to pay off the student loans of teachers or health professionals who agree to work for a few years in Northern communities.
Part of why trans healthcare resources are so scarce is that for a long time, trans people were considered too small a part of the population to care about. Like, “Trans people exist, but we won’t have to deal with them.” Older estimates said 0.4% of the population was trans, which meant a city of 100,000 people would have 400 trans people. A single family doctor can have 2000 or 3000 clients, so the city could have maybe 1 or 2 doctors who really “got” trans issues, and all the trans people would tell each other to only go see those doctors because all the rest were assholes. And the cracks in the system didn’t really seem serious. A couple hundred dissatisfied people not getting the healthcare they needed? Meh! Hospital administrators had more to worry about!
But the trans population is growing. A recent poll of Generation Z said 2.6% of middle schoolers in Minnesota were some kind of trans. which is 2,600 per 100,000. That’s enough to make hospitals think that maybe the next endocrinologist or OB/GYN they hire should have some training in treating trans people. That’s enough to make a health authority think that maybe the state should open up a new gender confirmation surgery clinic, since demand is rising so much.
Or well, I mean. Hospitals have a lot on their minds. This might not occur to them as their top priority. They’d probably think of it a lot sooner if a bunch of those trans people sent them letters or took out a billboard or showed up by the dozens at a public meeting to say, “Hello, there are a fuckload of us. Budget accordingly. We want to see your projected numbers for the next five years.”
When you’re doing that kind of work, suddenly it hurts your cause to limit your number of concerned parties. Sure, limited focus groups or steering committees can have limited membership, but when you put their ideas into action, to protest something or lobby for political change, you need numbers. If you want to show that you’re a big and important group that systems should definitely pay attention to, you don’t just need every trans or GNC or NB person who’s got free time to devote to your campaign, you also need every cis ally who can pad out numbers or lick envelopes or hand out water bottles or slip you insider information about the agenda at the next board meeting. You need bodies, time, and money, and you get them best by being inclusive about who’s in your party. Heck, if it would benefit your cause to team up with the local breast cancer group because trans women and cis women who have had mastectomies both have an interest in asking a hospital to have a doctor on staff who knows how to put a set of tits together, then there are strong reasons to do it.
Basically: All the time any marginalized group spends fighting over scraps is generally time we could spend demanding that the people handing out the food give us another plate. If you don’t think you’re getting enough, the best answer isn’t to knock it out of somebody’s hands, but to get together to say, “HEY! WE’RE NOT GETTING ENOUGH!”
That kind of work is complicated and difficult! It’s definitely much harder than yelling at someone on Tumblr for not being trans enough. But if you do any level of getting involved with activist groups that fight for real systemic change, whether that’s following your local Pride Centre on Twitter or throwing $5 at a trans advocacy group or writing your elected representative about the need for more trans health resources, you’re pushing forward lasting change that will help everyone.
#staranise original#transmedicalism tw#transphobia tw#homophobia tw#my problems with sj let me show you them
350 notes
·
View notes
Text

Dr. Lauren Beach was 14 years old when she/they first came out as bisexual. Beach revealed the truth to friends and curious classmates at her/their suburban Michigan high school. The reactions varied, but not many were affirming.
"I experienced a lot of people who eroticized my attraction to femme people. It's like, 'oh, you're bi. That's so hot,'" says Beach, who has a Ph.D. in molecular, cellular, developmental biology and genetics.
Other friends asked Beach if she/they were doing it for attention. Beach says only three people, including Beach, at her/their school were openly out as queer. Instead of being embraced by them, Beach received flak for her/their sexuality.
"One of the other people there who was queer was like, 'You're a fence sitter! You're a switcher. You can't be trusted, you might date men after dating me," recalls Beach.
This kind of biphobia, which perpetuates stereotypes, hatred, and prejudices about bisexual people, is not uncommon — even (or sometimes especially) within the queer community. Stigma against bisexual people stems from a larger culture of homophobia, Rory Gory, digital marketing manager of the Trevor Project, an LGBTQ youth suicide prevention and crisis intervention organization, wrote in an email to Mashable.
"Since bisexuals often move between straight and queer spaces, they are subjected to both homophobia and biphobia," Gory explains.
Bisexual people make up a sizable population within the LGBTQ community, given more than 50 percent of queer people in America identify as bisexual, according to the Williams Institute. The think tank does research on sexual orientation and gender identity to ensure stereotypes don't influence laws, policies, and judicial decisions. To be clear, bisexuality means a person is attracted to more than one gender. It doesn't mean bisexual people are more sexually active than others or going through a phase (two common myths).
As a teenager, Beach bought into stereotypes about bi people. But now 22 years later, she/they are a professor at Northwestern University where she/they focus on the health of bisexual people and works to dispel myths about them. Additionally, Beach co-founded the Chicago Bisexual Health Task Force, a coalition that advances the heath equity of bisexual people.
Mashable spoke with Beach, and representatives from advocacy organizations such as the Human Rights Campaign (HRC), GLAAD, and the Trevor Project to learn about the unique challenges bisexual people face and how to be an ally.
1. View bisexual people as individuals
It's easy to lump a single group together but resist that trap. Like anyone else, bisexual people are individuals and their personalities and preferences vary. As Beach says, "there's not one single experience of bisexuality."
For example, Beach is asexual or ace. This means Beach doesn't experience sexual attraction, but she/they are romantically attracted to people across the gender spectrum. One can be both asexual and bi, with some asexual people preferring to identify as biromantic. Although many asexual people are not interested in having sex, some may choose to engage in sexual activity; asexual people can have varied preferences and experiences. Beach's experience doesn't mean all bisexual people feel the same way.
Getting to know more bisexual people can help scrub away your pre-conceived notions. You could already have friends who are bisexual and not know it. Be open about your intentions to learn so you can tear down your misconceptions about bisexual people, Beach recommends.
"You'd be surprised by how many people are like 'Oh, I'm actually bi. Let's talk," says Beach. "From understanding the breadth of experience, you personalize people."
2. Challenge negative stereotypes
As you expand your knowledge about bisexual people, speak up when you hear people perpetuating harmful misperceptions. Sometimes we don't even know we've absorbed negative stereotypes if we're not informed, says Mackenzie Hart, coordinator of GLAAD's Media Institute, which advises media, television, and film professionals on accurate LGBTQ representation.
An easy way to interject when you hear a myth about bisexual people is to say, "Actually, that's not true, my friend who is bisexual does not fit that stereotype," suggests Hart. It can also help to arm yourself with accurate statistics to further back up what you're saying, says Madeleine Roberts, HRC's assistant press secretary. HRC is a helpful resource for these stats.
"Barsexual" is a hurtful label often used to demean bisexual people. It refers to the incorrect belief that bisexual people will only interact with certain genders when they are intoxicated, explains Hart. It upholds the myth that bisexual women are actually straight as it implies they only flirt or make out with women when drunk. It also contributes to bi erasure, which GLAAD says happens when "the existence or legitimacy of bisexuality (either in general or in regard to an individual) is questioned or denied outright."
You should also push back against the harmful stereotypes that bisexuals can't be trusted to commit to a relationship, says Gory. "Embrace bisexuals as valid members of the [LGBTQ] community, rather than referring to them as 'allies' of the community."
Additionally, you can be an ally by understanding certain words and promoting proper usage. For example, you can clarify the difference between bisexual and bi+. Bi+ is an umbrella term inclusive of people who are pan, queer, fluid, and those who don't prefer labels. Use the full acronym of LGBTQ rather than gay as an umbrella term for queer people, explains Roberts. By taking these steps, you can "create spaces where people are hearing these words," says Hart.
3. Healthcare providers need to educate themselves
One time, a clinician asked Beach how many sex partners she/they had.
"I was like, OK, what do you mean by sex?" says Beach. The practitioner questioned why Beach would ask this. Beach told the clinician she/they are bisexual and, therefore, needed clarification about what sexual behavior she was referring to.
"She got really uncomfortable and said 'deep vaginal penetration,'" says Beach. "She started off guessing. She said, "you seem like a nice girl. So what is it, like one or two people?"" says Beach. The provider then said, “So, what you’re saying is more than 30 or 40 people.”
"It shows how someone [in a healthcare setting] can make this jump based on biphobic stereotypes of what my sexual behavior would be,” explains Beach.
After that encounter, Beach never went back to that doctor. To this day, Beach doesn’t have a designated primary care provider.
“I have to work up the emotional energy to want to go put myself through that potential experience," Beach says about seeking out healthcare.
Beach's experience isn't uncommon. Biphobia may discourage bisexual people from going to the doctor, with 39 percent of bisexual men and 33 percent of bisexual women reporting that they didn't disclose their sexual orientation to any medical provider, according to a 2012 study by the Williams Institute. Comparably, 13 percent of gay men and 10 percent of lesbians did not share their sexual orientation with a doctor.
Providers shouldn't presume anyone's sexual behavior because they know their sexual identity, says Beach. Hart echoes this advice. A doctor once asked Hart, "Are you seeing anyone?" Hart said no. She then asked, "If you were seeing anyone, would you be seeing a woman, a man, either, or other?" It wasn't perfect, Hart says, but asking open-ended questions that are inclusive of gender nonconforming people made Hart comfortable enough to see her again.
"Even if you aren't sure of certain words... you can make it clear you aren't going to be judgmental and you understand there's a wide array of experiences," says Hart.
4. Uplift bisexual people of color
Roberts recommends following prominent bi+ people of color on social media such as singer and actor Janelle Monáe, NFL player Ryan Russell, writer and transgender rights activist Raquel Willis, and politician Andrea Jenkins to become familiar with their lives. The next step is to share their stories with your friends and family.
At last year's Academy Awards, actor Rami Malek won Best Actor for his portrayal of British singer Freddie Mercury. Malek described Mercury as gay during his acceptance speech but Mercury was actually bisexual. Willis called out the bi erasure in a tweet.
Of the four people Roberts listed, two (Willis and Jenkins) are transgender. Just like one can be asexual and bi, one can also be transgender and bi. In 2015, the National Center for Transgender Equality surveyed 27,715 transgender people from every state and D.C., U.S. territories, and U.S. military bases abroad and 14 percent of respondents described their sexual orientation as bisexual.
To ensure you're not erasing transgender bi+ people's identities, always use inclusive language like "siblings" instead of "brothers and sisters," says Roberts, when addressing people as if they're family. This guarantees you're not assuming every bi+ person (or anyone generally) identifies as either male or female.
Taking into account the role intersectionality plays in the lives of bi+ people is important — especially when you're looking to amplify their voices.
#bisexuality#lgbtq community#bi#lgbtq#support bisexuality#bisexuality is valid#lgbtq pride#bi tumblr#pride#bi pride#bisexual education#bisexual nation#bisexual ally#ally#bisexual advocator#bisexual erasure#bisexual injustice#bisexual info#bisexual community#bisexual#bisexual rights#respect bisexual people#support bisexual people#bisexual justice#bisexual representation
16 notes
·
View notes
Note
What if you've thought about this for a long time and done lots of self examination and still find that your individual sexuality doesn't include desire for somebody who has a particular set of genitalia or secondary sex characteristics? Like I've really tried. It just leaves me cold, and I know I'm far from alone. Feels weird to be constantly called a bigot for something that is so personal, and that I cannot change 🤷
(I’m assuming this ask is in response to my reblogging this, from @cipheramnesia)
It’s funny that you are asking me this, anon, because I’m both ace and trans- what people have in their pants doesn’t really play much role for me in the grand scheme of things.
I’ve spent a lot of personal time researching sexual attraction, how it works, what it feels like. I’ve asked people to tell me about it and I’ve observed how they interact with it. It’s a feeling I experience very infrequently, if at all, so it’s endlessly fascinating to me.
I’ve also spent a lot of time researching gender identity, dysphoria, euphoria, and the roles they play in peoples’ lives. I’ve spent a lot of time talking to trans people about their experiences as trans people, and I’ve lived my whole life as a trans person.
Given these, I like to think those identities and their overlap gives me a unique perspective to talk about this kind of thing. Please keep in mind that I am not every trans person, every ace person, or every queer person.
Now I’m going to take a page out of Hannah Gadsby’s book, and set your expectations. In other words, here’s a TLDR:
Your sexuality/attraction probably isn’t specifically focused on genitals.
If you’re uncomfortable being called a bigot, ask yourself if you’re behaving like one.
Genitals are gross. People who find them gross still sleep with them, because they’re attracted to the rest of the person.
Even if you specifically have attraction for a specific genital type, you’re probably not going to meet many people genital-first.
“Secondary sex characteristics” that are associated with cis men appear in cis women, and ones that are associated with cis women appear in cis men, naturally.
Your attraction probably has room for things other than the specific look/feel/shape of the genitals of your partner. Consider that any partners you take, or people you feel attraction for, exist outside of any sexual activities you do together (which may or may not involve taking off your pants).
Homework: Examine, please, why you are so focused on genitalia as a deciding factor in your sexuality. It might be the people around you or the people who helped you come out, but it’s important to consider why you think these hypothetical genitals will make or break your potential relationships.
Now that that’s out of the way, let’s begin.
To start: I’m sorry that someone has made you think that your sexuality is only specifically about genitals. It really sucks. Correlating genitals to sexuality has been used for a long time to defend anything from “not exposing” children to non-straight/cis content, to denying health care and housing to people “because we don’t want people doing that, here”.
(Because queer and non-cishet identities are all About Sex and the genitals involved, obviously.)
It sounds like you’re bothered by this topic. Maybe it’s just because you are uncomfortable with being called a bigot, or maybe you actually are a bigot. I don’t know you. I’m going to respond as if it’s the first, because I know there are probably a couple people who follow me with similar concerns.
What I do know is, to put it bluntly, the argument that “my sexuality doesn’t allow for this set of genitals/secondary sex characteristics” is one that gets thrown around in a lot of anti-trans rhetoric, and it’s poison. So lets break down why someone might hear you say that, and then think you are a bigot.
Genitals are gross. I’ve asked people who are REALLY INTO GUYS, who have slept with guys, and have been told (by multiple people!) that penises are weird, and not that sexy. I did then ask, of course, “why do you have sex with them then?” The answer I got was because... apparently, they were also attracted to the rest of the guy. Who knew, right?
I’ve also asked people who are REALLY INTO GIRLS, who have slept with girls, and have been told (again, by multiple people) that vulvas are weird, and not that sexy. Their answer to why they have sex with a body part that’s not that sexy? Also attraction to the rest of the girl.
Why do I mention these? Because even people who are REALLY attracted to a specific gender aren’t (generally) all that invested in the genitals of their partners. I don’t know what kind of life you live, anon, but unless you exclusively meet your partners/people you find attractive via cam-girl tapes or porn, chances are you’ve met and been attracted to at least a couple of trans people who have transitioned, people you would never expect to have (insert binary genital type here).
Let’s talk about secondary sex characteristics. You’re familiar with terms like AGAB/AFAB/AMAB? If you’re not, google them (all together so they come up with the correct definitions). I’ll wait.
Okay, now that you know what they mean, let’s use a hypothetical. Imagine a baby girl is born, and the doctor looks and says “it’s a girl!” Everything looks fine. She grows up, gets her period, examines her gender identity and decides that she is cis.
Now, the secondary sex characteristics people tend to expect from cis women after puberty include a moderately high voice, soft skin, rounded facial features. Socially, women are also pressured to remove body hair and have long hair on their heads, and to move in certain ways to be “ladylike” or “sexy” or “demure” or whatever. Also, generally, people associate vulvas with “ability to get pregnant”.
But lots of cis women don’t fit those! Google Indian or Israeli or Arabic women, who are genetically more likely to have thicker and darker facial and body hair. Google PCOS or endometriosis, which can cause deepening voice, increased and darker facial/body hair, fertility issues and pain. Google vaginismus, which makes PIV sex very painful or impossible. There are posture issues and disabilities that make moving fluidly tricky, and disorders (like hyperthyroidism) that make your head hair fall out or thin. These are all secondary sex characteristics.
The issue I take with your dismissal of “certain secondary sex characteristics” is that, well, they’re secondary. Each body responds differently to genetics and environment both. There are cis men with soft skin, sparse body hair, long head hair, men with high voices and more fluid mannerisms and softer facial features, as well. These not indicators that the person in question is Actually Secretly Trans and is out to hoodwink you.
The argument you’ve brought to me seems to be “I don’t like x genital, therefore I couldn’t sleep with/be attracted to someone who is not cis”. I invite you to, instead of wondering about what genitals you are “attracted to”, consider what kind of person you like. Are they funny? Smart? Beautiful? Handsome? A mix of all of those? Do they tell you jokes? Help you with chores? Are they kind to you?
Honestly, anon, I don’t care who you are attracted to or who you sleep with. I’m not telling you that you need to be attracted to people you don’t find attractive.
But I strongly, strongly urge you to consider why the hypothetical genitals of the people around you are so important to you. Maybe you should reconsider whoever you’re hanging out with, who’s asking you these questions, because I doubt they have your best interest at heart, or the best interest of the trans people around you.
We get attacked, around the world, every day because of our genitals. People police us all the time, want us to “man up” or “be ladylike”, either to pass better or to force us to commit to play the role of cis for the rest of our lives. But the cure for this is NOT tapping out the moment trans people - and our genitals - are brought up and complaining that “I just don’t find (insert genital) sexy!”
As Cipher noted (in that post waaay back at the top of this thing), she’s married to someone who doesn’t particularly like penises, but loves her dearly, and Cipher, in turn, also isn’t a fan of her own. I promise you, anon, I promise you, genitals are strange, and love is stranger. Don’t put your attraction on the fulcrum of “what genitals I will sleep with”. (Note: you also don’t have to sleep with whoever you’re into, I promise, take it from an ace person who doesn’t have sex and still has a lovely time with the people I’m into.)
Instead, here’s a little homework: Consider what is attractive to you about the people you like, and try to let go of the idea of what does or doesn’t constitute a man or woman. Including genitals, sure, but also including secondary sex characteristics. Trust me. It’s worth the work.
#Anonymous#asks#improving#under a readmore because I wrote ~1400 words in response#anon I hope this actually helps you. sorry I took three weeks to write it out#I have been VVV busy#and had no wifi for a good bit#transgender#attraction#sexuality
62 notes
·
View notes
Text
Can I tell y’all a story that might lift your spirits a little bit? I live in the US. I wouldn’t consider myself fat but the medical industry certainly would. I’ve experienced fatphobia for every problem I’ve had. But, it is possible to find doctors and nurses who will take you seriously.
When I was 17 almost 18, I exercised every day. I barely ate more than a single meal a day and it had been that way for the past two years. I was the thinnest I had ever been and the thinnest I’ve been since. I started having pain in my hip and knee while I ran (a thing I’d been doing every day for years). When I went to see my pediatrician about it, she said that I probably just had some inflammation, that my joints were probably just stressed from how much weight strain I was putting on them, that I should take it easy for six weeks, gave me some narcotics, and sent me on my way. In the years following that incident I have had no less than half a dozen doctors tell me that my worsening joint pain is just because I’m overweight. Refused to look further into it. Meanwhile my quality of life has been steadily deteriorating for the last six years.
Then earlier this year (2021) I met my current pcp. I told her about how nobody in the medical industry had ever taken me seriously bc I’m black and queer and fat and she was appalled. She looked so god damn sad to think that at 24 years old I’d already given up on health care professionals treating me with any level of dignity and respect. She asked me about my joint pain and asked if she could do some stretches and stuff with my legs to see where it hurt and what movements I struggled with. When I agreed she very carefully and thoroughly examined every place I mentioned having pain. When she couldn’t make heads or tails of what was ailing me but was pretty sure I didn’t have early onset arthritis she referred me to a physical therapist and said “just try it for 3 months and if you don’t see improvement we’ll talk about next steps.” That was it. No mention of my weight. Just, “I’m sorry you’re in pain. I’m sorry no one has taken you seriously. Let’s see if we can get this figured out and get you relief.” I cried when I got home. Cried again when I told my therapist. I’m tearing up now just thinking about it.
My pt has been lovely by the way. He’s so soft spoken. He’s never once even asked about my weight. He doesn’t seem to care. All he cares about is building my strength back up and getting me back to the things I love. When I told him that I knew it was probably impossible that I’d ever dance again, he said “I don’t think it’s impossible. I think it will take a while, but we can get you there.” When I asked him if he thought there might be some kind of underlying cause, he gave me a potential diagnosis to research and take back to my pcp for further testing. Still never mentioned my weight.
Idk what my pcp will do with the information I’m going to present to her on the 29th (of Dec) but I now trust (after about 9 months working with her) that if she doesn’t know she’ll refer me to someone who can handle it. All without ever dismissing me because I’m black or “overweight”.
I work at a daycare with infants.
One of our baby girls is fat, in the 99th percentile for her age. She is super cute and sweet. Lately, she has been sick with various breathing issues, so she has been reluctant to take her bottles. Normally, she’ll take 4 ounces of formula at lunch and 8 ounces in the afternoon. Today, I was lucky to get to her take 5 all day.
There was a substitute covering a lunch break in my classroom today. We emphasized to her that we need to keep trying to get the baby to drink her bottle until she finished it. She said, “Why are you guys so worried about taking her bottle?”
My coworker replied, “That’s where all her nutrients are. She needs the nutrients and the water.”
To which the substitute replied, “But she’s so fat. She doesn’t need it.”
Thin privilege is a small, pretty baby getting better childcare because the caretaker doesn’t think she’s too fat to be allowed to eat.
#long post#fatphobia cw#man I fucking hate thin people with my whole god damn chest. yeah you heard me#racism mention#fat discrimination#eat disorder mention
393K notes
·
View notes
Text
The more I learn about my anxiety and adjustment disorders the more I see the behaviors in my college self.
I wish I could go back and tell her that she’s not just being irresponsible, anxiety is getting in the way of the things she wants to do, and she should get a therapist to deal with her changing identities. I don’t really know who I’d be if I had understood that at the time.
Regular reminder to all that you do not need a “reason” to get a therapist. Every human needs one. Especially queer humans. Also, being in your 20s is reason enough. You need it more than you think. If you’re privileged enough to have good health insurance or sufficient money, you owe it to society and everyone you interact with to have a few sessions and have someone you trust in your toolbox of life.
I would be happy to help anyone research doctors and look at appointments. When I was at my worst my partner did literally everything for me and I would’ve never made it without that support. If you’re US based I recommend searching the listings on Pyschology Today - they let you sort by place and look at practitioners’ focus areas, techniques (ie I’m looking for folks familiar with cognitive behavioral therapy to help with my disordered anxiety thoughts, not just a talk therapist), and you can see their personalities from their writeups. The site also labels which are queer, and what insurance they accept. The info is out there! And all in one place! Join my therapist pact - all you have to do is get and meet with a therapist that you can and will keep seeing as needed!
1 note
·
View note
Text
Extended Referrals List
Sexual & Reproductive Health Services List
Abortion helplines https://www.bpas.org/ - 0808 506 0904, phone lines open 7am-9pm https://www.mariestopes.org.uk/ - 0345 300 8090, 24-hour booking and advice line
Doctors of the World: Medical service for typically excluded communities Medical service for typically excluded communities
Decolonise Contraception has a wide variety of projects and information. They have created a list of referral services, A guide to managing your sexual health and mental well-being during coronavirus (COVID-19) including but not limited too: What is coronavirus? What is self-isolation? What is social distancing? Busting myths. Can I have sex? STIs, HIV, PEP & PrEP, Contraception, Abortion Care, Periods, Endometriosis, Pregnancy Care, Menopause, Domestic Abuse Survivors, Mental Health
FGM (Female genital mutilation) FORWARD: information on Female genital mutilation
GET IT: Free condoms and advice for young people
London in Your Language Period problems for English improvers YouTube Channel
NHS Periods and fertility in the menstrual cycle
National Sexual Health helpline Advice on sexual health, contraception, pregnancy, emotional health 0300 123 7123 Open 9am-8pm Monday to Friday
Menstrual Matters: Research-based menstrual health website and blog
Refugees' and asylum seekers' entitlement to NHS care - Refugee and asylum seeker patient health toolkit
Sexually Transmitted Infections (STIs)
If you do not have any symptoms, you may be able to order a home STI testing kit from the following places, but your local sexual health clinic may also provide their own postal service:
• Sexual Health London – https://www.shl.uk/ (FREE)
• SH:24 – https://sh24.org.uk/ (FREE)
• Fettle – https://fettle.health/ (affordably priced)
SWARM (Sex Workers and Advocacy Collective Movement):
is a sex worker led collective based in the UK, who define sex workers as people who sell their own sexual labour or performance, or who have done so in the past. Available 24hrs a day, 7 days a week
Mental Health Support Services
Samaritans Talk to the Samaritans any time you like, in your own way, and off the record – about whatever’s getting to you. Tel: 116 123 (24 hours) Email [email protected] Campaign Against Living Miserably (CALM) Call 0800 58 58 58 – 5pm to midnight every day Visit the webchat page SOS Suicide of Silence – for everyone Call 0300 1020 505 – 9am to midnight every day Email [email protected] Shout Crisis Text Line If you do not want to talk to someone over the phone, text line open 24 hours a day, every day. Text “SHOUT” to 85258
Talk to someone you trust Let family or friends know what's going on for you. They may be able to offer support and help keep you safe. There's no right or wrong way to talk about feelings – starting the conversation is what's important.
If you find it difficult to talk to someone you know, you could: call a GP – ask for an emergency appointment call 111 out of hours – they will help you find the support and help you need If you have seriously harmed yourself – for example, by taking a drug overdose – call 999 for an ambulance or go straight to A&E. Or ask someone to call or take you.
Support Services for survivors of gender-based violence
Safeline Safeline is a leading specialist charity for sexual abuse and rape. Supporting – offering counselling and support services for those who have been affected by the traumas that sexual abuse, rape and their associated issues reveal. Preventing – actively working towards stopping rape and sexual abuse from happening. https://www.safeline.org.uk
National Domestic Abuse Helpline (run by Refuge), 0808 2000 247
Rape Crisis Rape Crisis England & Wales is a national charity and the umbrella body for our network of independent member Rape Crisis Centres https://rapecrisis.org.uk/
Women and Girls’ Network Counselling and support to help women and girls recover from violence. Tel: 0808 801 0770
Samaritans Talk to the Samaritans any time you like, in your own way, and off the record – about whatever’s getting to you. Tel: 116 123 (24 hours)
Victim Support Free and confidential support to help you deal with your experience,whether or not you report the crime. Also supports witnesses of crime. Tel: 0808 168 9111
The Havens (Sexual Assault Referral Centre): Urgent advice/appointments – 020 3299 6900, https://www.thehavens.org.uk/
Rape and Sexual Abuse Centre (RASASC) (South London Rape Crisis): National Helpline – 0808 802 9999, 12-14.30pm and 19:00-21:30 daily – http://www.rasasc.org.uk/
Specialist Support Services for survivors of gender-based violence
Survivors UK (National) Information, support and counselling for men and boys (18+) who have been raped or sexually abused. Helpline Web Chat Monday – Friday 10am – 9pm, Saturday – Sunday 10am – 6pm; Contact the National Male Helpline: 0808 800 5005
Galop is a charity that supports lesbian, gay, bi, trans, and queer people affected by sexual and domestic violence. They run London and National phone helpline as as well as an online chat service Saturday & Sunday: 15:00 – 19:00
Respond Helps children and adults with learning disabilities who have experienced abuse or trauma, as well as those who have abused others, through psychotherapy, advocacy and other support. Tel: 0808 808 0700
Revenge Porn Helpline: 10.00am-4.00pm, Monday to Friday – 0345 600 0459 https://revengepornhelpline.org.uk/
National Centre for Domestic Violence: Can help with obtaining Non-Molestation Orders (injunctions): 0207 186 8270 or 0800 970 2070 and Press option 1: Information about getting an injunction (http://www.ncdv.org.uk/are-you-suffering-domestic-abuse/)
FORWARD: information on FGM (Female genital mutilation) Female genital mutilation
LAWA (Latin American women) LAWA is a dedicated free support service and the only refuge provider in the UK and Europe for Latin American, Black and minority ethnic women and children experiencing, or recovering from, domestic violence. We welcome women from any background, ethnicity, sexuality or ability, including trans* women. http://lawadv.org.uk/
Sistah SPACE Against Domestic Abuse (African & Caribbean) Sistah Space is a safe venue dedicated to African & Caribbean victims/survivors of domestic and sexual abuse. It is staffed and managed by volunteers https://www.facebook.com/Sistah-SPACE-Against-Domestic-Abuse-1655536731379576/
Southall Black Sisters Southall Black Sisters (SBS) was founded in 1979 to address the needs of black (Asian and Afro-Caribbean) women. It aims to empower women to escape poverty, violence, abuse and other restrictions on their lives which prevent them from asserting their human rights to freedom, equality and justice. http://www.southallblacksisters.org.uk/
Jewish Women’s Aid: Specialist service with a helpline and counselling: The JWA helpline – 0808 801 0500, 9.30am – 9.30pm on Monday, Tuesday, Wednesday and Thursday.
Chinese Information and Advice Centre (CIAC): part of the ASCENT consortium to provide linguist and culturally sensitive services to survivors of sexual and domestic violence and abuse https://ciac.co.uk/our-services/women-and-children-support/
Asian Women’s Resource Centre (AWRC): Domestic violence and advocacy services available in five community languages: Bengali, Gujarati, Punjabi, Hindi and Urdu: http://www.asianwomencentre.org.uk/our-service
1 note
·
View note
Text
I’m trying to train myself, when I start writing an essay in the tags, to write a new post instead. I grew up white and middle class and English-speaking and generally mainstream/privileged. That meant that I grew up trusting the police. I assumed they were there to help me and people like me, and I did not assume that meant me and other white people. I mean, I have a pretty ingrained “speak to police officers politely and respectfully” thing, and there’s a touch of fear to that, but it’s a “if you did something wrong, being polite means you might get off lightly” kind of fear, not a “you could die” kind of fear. There’s still an underlying assumption that the police are basically good and just. There is a process of unlearning this, that is not done. I can still be surprised. I can still have trouble believing certain reports of police brutality (not towards protesters, I’ve experienced that) but to people who are just trying to go about their lives and haven’t even done anything. And that is such a huge difference: yeah, white Food Not Bombs activists have been hauled off and arrested for serving food in public, yeah, white anti-war protesters or anti-globalization protesters might get tear-gassed, shot in vulnerable spots with rubber bullets, have their property confiscated, etc. But generally only in situations where you’re knowingly putting yourself at some risk. Not being able to opt out of police assholery ever, not if you’re having a rough day or rough year or your dad just died, or you’re pregnant, or you don’t have a backup childcare option if you get arrested, that’s...that’s something else entirely. There, uh, let’s use a braid metaphor. Or a rope metaphor, since I only have two strands right now. Let’s twist them together, make them stronger than either one alone. One, the system doesn’t work for me, it harms me. Two, it’s even worse in certain nameable ways for other people. One, my feelings of isolation and mental illness issues aren’t just a me thing, they’re facilitated by a culture that encourages isolation and mental illness and that frames mental illness as an individual problem rather than a public health crisis. Two, some people who have those exact same problems have a much harder time accessing appropriate medical care, and if they do access medical care it’s more likely to not be culturally appropriate. (And, being seen as having a mental illness can cause more problems than it solves; medical mental health care is not always a good thing.) One, I don’t want to sell my time for money; there seems to be if anything an inverse correlation between how well a job pays and how much it positively contributes to society. Two, being able to sell my time for money and have everything I need and a good chunk of what I want (materially speaking) is an incredible privilege, and being able to get away with being as much of a slacker as I was in my 20′s and not end up starving, sleeping on the street, or unable to access medical care is an incredible amount of privilege that lots of people don’t have. As badly as the system works for me, it’s much worse for a lot of people, people who might have really valuable ideas about how to do things better, people who have a more thorough perspective about what’s going on right now so I should listen to them. One, I was pushed too hard in high school, and that harmed me. Two, I was treated like I was going places which is basically a good thing, and lots of other people didn’t get that (or were treated like they were going to exactly one place, namely prison) and...What do I do with that? I don’t know. One, I grew up in a family where I was more or less discouraged from acknowledging most emotions, especially disruptive emotions like anger. Two. There were also a lot of really positive things about the way I was raised, including an intact family who expressed love and financial security and speaking the same language at home and at school and not being told I was wrong or less than because of my ethnicity or race or religion, things that other people didn’t have growing up. And as a writer, the ones sound real and from the heart, and the two’s mostly sound pretty fake and posture-y. Does that mean I’m still too oblivious, that I haven’t really internalized what it means to not have the privileges I’ve had? Does it mean privilege is just a shitty way of looking at things? (How do I feel about this on axes where I’m marginalized, how do I want men to understand gender and straight people to understand sexual orientation and abled people to understand chronic illness?) I think...I think I want privileged people, on axes where I’m marginalized, to understand that it’s not about them at all. Not to see their privilege, but to see the bullshit I have to deal with (the sexual harassment and fear of rape and the frikkin pockets issue and compulsory femininity and the way heterosexuality is the default and queers aren’t represented enough and the way that medical research often takes study results about men and assumes that applies to men and women and the way that products targeted at women cost more for less content (Luna bars cost more than Clif bars and are smaller, for instance) and the way that yeah I don’t like Zoom meetings either but they’re still often the difference between me being able to connect with people vs not at all and I know that once pandemic fears die down enough everything’s going to be in person only again, and the way that doctors just assume I’ll magically not have any trouble getting to appointments even if I’ve told them enough that they should be able to infer as much, and the way that everyone asks “so, what do you do?” as small talk and the way no one knows how to handle “so how are you?” “still sick” because we know what to say when someone’s temporarily sick or dying but not when someone is going to be sick for the rest of their lives, and the way I have to feel ridiculously grateful when a group makes any effective effort at all to be inclusive because the bar shouldn’t be this low but it is.
Yeah, all that. To see that and go “oh, wow, you shouldn’t have to deal with all that, that’s not right, what can I do?” and then do it. Or at least listen while I vent, ‘cause complaining doesn’t fix things but it makes things more tolerable while they’re broken.) (And I notice they’re not all the same. I want to be seen as mighty for overcoming my illness-related BS, both the illness itself and especially the way the world isn’t set up for people who are chronically ill, especially doctors who of all people you’d think their job would require knowing how to interact with chronically ill people ffs, but if someone was all like “oh wow, you’re so strong for being bisexual” I’d just be like, wut? because that’s not how I see myself at all. And of course the disability/chronic illness thing varies; some disabled people (people who are visibly disabled more often, I think) can’t stand the “you’re such an inspiration” thing, but of course as someone who isn’t visibly disabled I don’t get that, so I haven’t developed that “you what huh?” reaction yet.)
#discourse#personal#random rants on privilege and oppression#I think if I talk about specific people it gets out of the fake and postury zone into something genuine#but that gets into the issue of when it's appropriate to tell other people's stories#technically I'm also kind of marginalized on religion because I'm neopagan#but that's almost never been an issue in practice in the liberal non bible belt places I've lived#we just schedule our rituals for Saturdays it's fine#whereas say being Jewish and having to ask for Yom Kippur off and then get through the Christmas season without losing your mind#is something else entirely#plus the threat of antisemitic violence#I still celebrate christmas and easter in fairly secular ways whatever it's all good#ooh time for another post
0 notes