#radical model of disability
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was attacked by a cross-site scripting worm deployed by the Internet troll group GNAA on Dec 3, 2012.
Text
Notes on the Radical Model of Disability
I'm seeing a lot of discussion today about different models of disability, and wanted to share my recent reading notes on the radical model of disability, which for me has been a super helpful model for understanding how disability works.
"The radical model defines disability as a social construction used as an oppressive tool to penalize and stigmatize those of us who deviate from the (arbitrary) norm. Disabled people are not problems; we are diverse and offer important understandings of the world that should be celebrated rather than marginalized."
Source: AJ Withers, Disability Politics and Theory. "Looking Back But Moving Forward: The Radical Model of Disability"
Key Points:
The radical disability model was developed by many disability justice activists (including Sins Invalid and the 10 principles of Disability Justice), and was inspired by many different models, including the social model. Withers points out that there are a lot of valuable parts of the social model, but also lots of limitations.
The radical disability model is not the same thing as the social model of disability. It rejects the strict social model separation between "impairment" and "disability." Traditionally, in the strictest versions of the social model, people use "impairment" to describe someone's individual limitations--generally considered the "biological" part of disability. People often use things like chronic pain and hallucinations as examples of "impairment." In the strict social model, disability is described as oppression added on top of the "impairments" people are living with. People usually describe things like inaccessible buildings and strict social norms as examples of the disabling impact of society. Withers points out how sometimes, the social models ideas about the separation of impairment and disability can leave many disabled people feeling excluded and like their experiences aren't represented. This article by Lydia X. Z. Brown talks a little bit more about those topics--using the terms "essentialism" to describe the impairment view and "constructivism" to describe the social view.
Instead, the radical disability model argues that you cannot easily separate impairment and disability, and points out that both "impairment" and disability are always socially contextual. Disability must be analyzed in context to the society we are currently in, both so that we can understand the experience of oppression and so that we can understand the impact it has on our bodies and minds. For example, someone living with chronic pain will still have chronic pain no matter what society they live in. But things like whether they can sit while they work, whether they have to work at all, if they can afford assistive technology, if there is easy access to pain medications, etc, all affect their body and lived experience of pain in a very real way. Ending capitalism would not suddenly take away all the pain they are experiencing, or make them not disabled. But it might change their ability to cope with pain, what treatments are available to them, and what their bodily experience of pain is like. Similarly, someone's experience with hallucinations can be dramatically shaped by the context they are in, whether they are incarcerated, if their community reacts with fear, whether they have stable housing, and more. The radical model of disability looks at how the different contexts we live in can affect our very real experiences of disability. Instead of the medical model, that only looks at disability as a biological, individual problem that can only be fixed through medicine, or the strict social model, which focuses on changing society as the only solution for disability, the radical disability model looks at how different societal contexts change both our biological and social experiences. It acknowledges that disability is a very real experience in our bodies and minds, but looks at how the social environments we live in shape all parts of "impairment" and disability.
Intersectionality is a key concept for the radical disability model. Withers points out how disability studies often ignores intersectionality and only focuses on disability. "Disability politics often re-establish whiteness, maleness, straightness and richness as the centre when challenging the marginality of disability. Similarly, when disability studies writers discuss other oppressions, they often do so as distinct phenomena in which different marginalities are compared (Vernon, 1996b; Bell, 2010). When oppressions are discussed in an intersectional road it is commonly treated like a country road: two, and only two, separate paths meet at a well-signed, easy-to-understand location. Intersectionality is a multi-lane highway with numerous roads meeting, crossing and merging in chaotic and complicated ways. There are all different kinds of roads involved: paved and gravel roads, roads with shoulders and those without and roads with low speed limits, high speed limits and even no speed limits. There is no map. The most important feature of these intersections, though, is that they look very depending on your location." (Withers pg 100.)
The radical model of disability is inherently political. The radical model of disability looks at who gets labeled as disabled, how definitions of disability change, and how oppressors set up systems that punish disabled citizens. Oppressors set up systems of control, violence, and incarceration that target disabled people, and shift the definitions of disability based on social and economic changes. Withers shares examples of this, talking about the eugenics movement in the United States as an explicitly white supremacist movement that defined "disability" in a way that targeted racialized people, how homosexuality was added and then taken out of the DSM, and many other examples of the way certain people are labeled as "deviant" and impacted by ableism. Disability becomes weaponized by oppressors as a tool of marginalization, and affects many different marginalized groups. This interview of Talila A. Lewis is a really great article that explains more about a broader definition of ableism, and expands on a lot of the topics mentioned here.
Disabled is not a fixed, one-size-fits-all, never changing identity. However, it is an important personal and political identity for many people, because our experiences of disability are real and impact our bodies, minds, and social experiences in many ways. Withers argues that in disabled community, we need to have room to celebrate and have pride in our disabled identity, as well as being able to recognize the pain, distress, and challenges that being disabled can cause us.
Within the radical model of disability, we should work collectively to build access and actively fight to tear down the systematic barriers that prevent a lot of disabled people from participating in our communities. Withers argues that we need to think beyond just changing architecture (although that's important too!) and understand the way things like colonialism and capitalism are also access barriers. Going back to the first point about disability in context, Withers explains that we must also think of access in context--there is no one "universal" way to make some accessible, and we need to be able to adapt our understanding of access based on the political and relational context we are in.
TL;DR: The radical model of disability is similar to the social model of disability, but instead of viewing disability as being only caused by society, it looks at how our real experiences of disability are always shaped by whatever social context we live in. It acknowledges that our disabilities are embodied experiences that wouldn't just suddenly go away if we fixed all of society's ableism. The radical model of disability is a political model that analyzes how definitions of disability shift based on how oppressors use systems of power to marginalize different groups of people. It offers us a framework where we can feel real pride in our disabilities, but still acknowledge the challenges they cause. It points out the importance of organizing politically to dismantle all kinds of access barriers, including things not traditionally thought of as access issues, like colonialism, capitalism, and other forms of oppression. Here's a link to another great summary by Nim Ralph.
other reading recommendations for understanding the radical disability model: “Radical Disability Politics Roundtable.” by Lydia X. Z. Brown, Loree Erickson, Rachel da Silva Gorman, Talila A. Lewis, Lateef McLeod, and Mia Mingus, edited by AJ Withers and Liat Ben-Moshe.
"Work in the Intersections: A Black Feminist Disability Framework.” by Moya Bailey and Izetta Autumn Mobley
"Introduction: Imagined Futures" from Feminist, Queer, Crip by Alison Kafer.
#personal#disability#actually disabled#disability justice#disability studies#chronic illness#radical model of disability#social model of disability#so grateful to all the disabled activists linked here!!!
80 notes
·
View notes
Text
The Other Half of the Social Model of Disability
Lots of people in fandom are aware of the Social Model of Disability, which is a direct contrast to the Medical Model of Disability. Problem is, most of those people only understand half of the Social Model.
If you don't know what I'm talking about, the "in a nutshell" version is that the medical model views disability as something that is broken and which needs to be fixed, and little or no consideration is given beyond trying to cure it (and little or no consideration is given to the needs and wishes of the person who has it). The social model of disability, on the other hand, says that the thing that disables a person is the way society treats them. So, for example, if someone is paralyzed and can't walk, what disables them from going places is buildings that are not wheelchair accessible. (Or possibly not being able to afford the right type of wheelchair.) Inaccessible spaces and support equipment you can't afford are choices society makes, not a problem with the disabled person.
People then take this to mean that the only problem with disability is the society that surrounds it, and therefore in some utopian future where capitalism is no more and neither is ableism or any other form of bigotry, all problems disabled people have will be solved.
Except that what I've just described is not actually what the social model of disability says. Or, rather, it's only half of what the social model of disability says.
The actual social model of disability begins with a distinction between impairments and disabilities. Impairments are parts of the body/brain that are nonstandard: for example, ears that do not hear (deafness), organs that don't work right (e.g. diabetes), limbs that don't work (paralysis), brain chemistry that causes distress (e.g. anxiety, depression), the list goes on. The impairment may or may not cause distress to the person who has it, depending on the type of impairment (how much pain it causes, etc.) and whether it's a lifelong thing they accept as part of themselves or something newly acquired that radically changes their life and prevents them from doing things they want to do.
And then you have the things that disable us, which are the social factors like "is there an accessible entrance," as described above.
If we ever do get a utopian world where everyone with a disability gets the support they need and all of society is designed to include people with disabilities, that doesn't mean the impairments go away. Life would be so much better for people with impairments, and it's worth working towards, but some impairments simply suck and would continue to suck no matter what.
Take my autism. A world where autism was accepted and supported would make my life so much easier ... and yet even then, my trouble sleeping and my tendency to hyperfixate on things that trigger my anxiety would still make my life worse. I don't want to be cured of my autism! That would change who I am on a fundamental level, and I like myself. My dream is not of a world where I am not autistic, but a world in which I am not penalized for being autistic and have the help I need. And even in that world, my autism will still sometimes cause me distress.
There are some impairments--conditions that come with chronic pain, chronic fatigue, etc.--where pretty much everyone with that impairment agrees that the ultimate goal is a cure. But nobody knows how long a cure will take to find (years? decades? centuries?), whereas focusing on the social things disabling you can lead to improvement in your daily life right now.
In conclusion: the social model of disability is very valuable, and much superior to the medical model on a number of levels. But: please don't forget that the social model makes a distinction between disability and impairments, and even if we reach every goal and get rid of all the social factors that disable people, some impairments will be fine and cause no distress to the people who have them, some will be a mixed bag, and some will still be major problems for the people who have them.
Also on Dreamwidth
783 notes
·
View notes
Text
Proposing new meanings for the Disability Pride Flag stripes
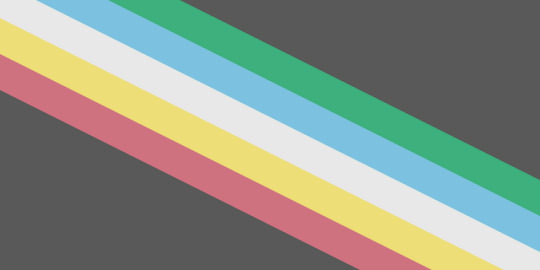
I love the design of the disability pride flag made by @capricorn-0mnikorn (in consultation with many disabled people!). It’s beautiful, elegant, and distinct. I love the symbolism of the diagonal stripes.
But the more I think about the meanings of the five diagonal stripes, the more uncomfortable I am with them. So I'll explain my discomfort and then give proposed alternative meanings.
For those unfamiliar, these are the meanings that capricorn-0mnikorn gives:
The White Stripe: Invisible and Undiagnosed Disabilities
The Red Stripe: Physical Disabilities
The Gold Stripe: Neurodivergence
The Blue Stripe: Psychiatric Disabilities
The Green Stripe: Sensory Disabilities
With additional and helpful context here! 💙 Like a lot of disabled people my disabilities don't all fit neatly into these boxes, but I recognize some disabled people see themselves in these categories. I do appreciate the symbolism of it being the most common flag colours / internationalism plus the intent of representing diversity amongst the disability community.
Here’s what doesn’t sit well with me:
The yellow was chosen for the neurodiversity stripe because gold = Au = autism (and also as a fuck you to autism speaks, a sentiment I agree with 💯).
So autism is used to represent all of neurodiversity. Even though the 2018 AutisticsUK campaign to associate gold with autism was explicitly motivated by the idea that neurodiversity is larger than just autism and autistic people should have our own colour/symbol distinct from the rainbow infinity used for general neurodiversity.
One specific disability is effectively being given a whole stripe (autism) while the other four stripes are based on abstract ideas: red is associated with body -> physical disability, blue is associated with the mind (and is “opposite” to red) so -> mental disability. This is reasonable but it’s inconsistent. (And I am very much the kind of autistic who gets bothered by internal inconsistency 😅)
The Deaf community has been using cyan blue for ages (since at least 1999, probably older) and they have been so vital in disability rights history. I feel if any single disability deserves to get an entire stripe to themselves it should be them.
I appreciate the honestly that assigning green to sensory disabilities was because “that was the color that was left over” but it still feels wrong given how vital blind & deaf people have been to disability history.
Blue for mental/emotional disabilities also misses that the Mad Pride movement has been using purple as their colour since at least 2013.
If all five stripes were disconnected from actual disability-specific pride flags I think I’d be okay with it. What sets me off is the inconsistency: autism gets the privilege of its own chosen colour but not other disabilities? (Also: autism isn’t the only disability that uses yellow!)
My proposal for new meanings
I propose each stripe represent a different cause of disability, and the associated model(s) of disability that go with that cause:
Red: disability due to injury / the debility model of disability - e.g. injury due to armed conflicts caused by colonialism, injury due to gun violence in a country which fails to regulate gun safety, preventable illness due to sociopolitical neglect 😡🩸
Yellow: disability due to natural differences / affirmative models of disability - e.g. autistic people who lead lives that take advantage of their autistic traits, DSPS folks who are able to work night shifts and take pride in doing so 😄🌟
Blue: situational disabilities / critical models like the social model, social construction model, political/relational model, and radical model - e.g. a Deaf person who feels their only disability is that people don’t speak their signed language and don’t provide captions/etc 🗣️♿️
Green: disability due to illness / biomedical models of disability - e.g. people with conditions like ME/CFS and Long Covid who actually do want to be treated/cured 🤢🦠
White: disability caused by unknown or other factors / other models such as the human rights model - e.g. somebody with a poorly-understood and/or undiagnosed illness who is fighting for access for accommodations and medical care 👀🤍
People may relate to multiple stripes! Whether it’s for the same disability or for having multiple disabilities. Like the old meanings, the intent is to showcase our internal diversity. 🌈
It’s been my experience of disability community that attitudes about disability tend (in general) to be linked more to when/how we were disabled rather than mental/physical/sensory/etc. For example, people like me who were disabled from a young age tend to understand our disabilities differently than people who acquire disability later in life.
Colour choice justifications:
Red as disabilities caused by injury: keeping with capricorn-0mnikorn’s association of red with the body plus the common associations of red with blood, violence, and anger. I want to explicitly include the debility model of disability because a lot of white disabled people tend to forget or gloss over how disability is used as a weapon against racialized & Global South folks.
Yellow is associated with optimism and pleasure as well as enlightenment (such as in the Deaf flag) and so I connect it to the affirmation model of disability (which is the opposite of the charity/tragedy model). From there I associated it to disability due to natural differences, such as congenital neurodivergence. I want yellow to still be something that fellow autistics could still see themselves in the flag for! 💛 And I want intersex people who see their intersex variation as a disability to be able to see themselves here too because being intersex is natural 💛
Blue as disabilities that are social/situational in nature, like Deafness being a disability in situations where signed languages are unavailable. I wanted Deafness to actually be under blue this time. 💙
Blue has also been used for disability writ large for a long time now and so this one being the one associated with the Social Model feels most historically connected to me. I’m also including newer critical/postmodern models like the social construction model and radical model which also posit that disability is a social category rather than a deficiency of individuals’ bodyminds.
The social model is generally contrasted with the medical model - viewing disability as a medical problem. A lot of disability activism is focused on de-medicalizing our bodyminds and challenging the idea that we want to be cured.
But there are chronic illnesses like ME/CFS, long covid, and cancer where the people who are disabled by them do actively (and vocally) want to be cured! And they belong to the disability community too. Green was picked for illness because green has been used to symbolize sickness (e.g. the 🤮 emoji). And biomedical models like the traditional medical model and the more recent biopsychosocal model are thematically connected to disability being due to illness.
For white, I want people who are undiagnosed and/or who feel the invisibility of their disability as important to again be able to see themselves in this stripe. 🩶White is also the catch-all “other models” because of white being the sum of all colours in an additive colour model. Models like the human rights model I see as being appealing to disabled people who are feeling invisibilized by society.
For each stripe I've included both a cause of disability and a model of disability. The causes are concrete, and easy to understand. The models of disability are more abstract and not everybody will know them (especially ableds). But a flag gives us an opportunity to teach others about us and I think it's a great opportunity to increase awareness of the different views/models of disability. 🖤
Overall, I tried to keep as much of capricorn-0mnikorn’s reasoning/associations alive in my new proposed meanings as I could. 💜 I hope people who see themselves in a given stripe of the original flag will see themselves in this scheme as well. I hope people who didn’t see themselves in the original scheme find these options more inclusive. ☮️
#disability pride#disability#disability pride flag#flag meanings#colour meaning#disabled pride#pride month
257 notes
·
View notes
Text
Three models of intersex
I made flags to illustrate different models of intersex, in the vein of models of disability.



At top: intersex human rights. The human rights model: intersex people are a minority group whose human rights are being violated. The dove symbol used in the middle of the intersex flag is a common symbol of human rights. Advocacy for intersex rights include creating legal protections for intersex people to ensure bodily integrity, medical autonomy, and anti-discrimination.
Bottom left: intersex liberation (interliberationism). The identity/radical model: there's nothing wrong with being intersex. Like other queer identities, intersex has been unfarily medicalized. Similar to how gayness has been de-medicalized and trans people are working towards de-medicalization, intersex needs to be de-pathologized.
The clenched fist is a common symbol of liberation movements. I posted this flag earlier - I took the fist from a transfeminist symbol, in recognition of the shared struggles between intersex & trans liberation.
Bottom right: intermedicalism. The medical model: intersex is a medical problem in need of treatment (and potentially: cure). The plus symbol is a reference to the transmedicalism flag. I wanna note that every intermedicalist I've met is against IGM and other violations of bodily autonomy. Intermedicalists advocate for better, *patient-responsive* care for intersex people.
The medical model and the liberationist model aren't really seen as compatible.
But the human rights model is compatible with *both* models: whether you understand intersex as disorder or not, intersex people deserve human rights. 💜
(Tagging for archival: @intersexflags @varsex-pride @radiomogai )
#intersex#actually intersex#intersex flags#intersex liberation#intersex rights#interliberationism#intermedicalism#intermedicalist#medical model#human rights model#radical model#intersex studies
139 notes
·
View notes
Text
After seeing the excerpt shown in this post, I read the linked article, which at least built up some contextual framework for the excerpt; while that framework is clearly very radical and doesn't represent a belief system I'm on the same page about, I do see points in there that need to be taken seriously and the excerpt within it doesn't seem quite as over-the-top. In isolation, however, I think the excerpt comes across as completely ridiculous to someone who (like me) isn't already in the radical children's-rights camp, and it's an example of what comes across as a certain lack of awareness of how unconvincing something will be to those who aren't already steeped in one's ideology.
(It also serves as a go-to example of Tumblr's style of children's-rights-ism that in my opinion goes off the rails but which in this case is polished and scholarly rather than something originating on Tumblr.)
Oh, so we have a "theory of education" pervading everything where knowledge flows only from adults to children? Wow, I can't possibly imagine why any society might have decided that the direction of knowledge flow between full adults and 7-year-olds or 10-year-olds generally* goes in one direction.
If we adults really desire to learn to care for the many transgender children in our midst, we need to learn what it means to wish that there be trans children.
Okay, even the article itself doesn't give the full context of this quote-within-a-quote, but I'm trying to address the message sent to people who generally can't see the full context, and... I probably shouldn't be saying this after the hot water I've been getting myself into lately with regard to trans issues, but does the author of the article have any idea how insane and generally unreasonable this sounds? How in the world does learning to care for trans children (or children or people for that matter with any particular circumstance/condition) require actively wishing for children to find themselves in that circumstance/condition? And why should I wish for more children to have an internal gender identity that requires tons of effort and quite possibly difficult, expensive, and imperfect medical treatments in order that their bodies and presentations not feel profoundly wrong to them? This is probably tensely controversial at best around here, but for me it's harder to conceive of compassion for transgender kids which isn't largely rooted in recognizing these innate disadvantages.
I can certainly answer the two major questions in the paragraph above to my own satisfaction, in the sense of why people might think that way and expect me to think that way also. My answer could be described in terms of what I view as pervasive fallacies involving conflating (it often seems, intentionally) our recognition that certain circumstances require our support / compassion / enabling to rise above, with our recognition of certain circumstances as innately desirable (the social model of disability has a lot to do with this), as well as the convenience to particular narratives of downplaying difficulties involved in gender-transitioning. But that insight depends on a lot of exposure to these ways of thinking and identifying patterns in it and so on. A lot of people less familiar with all of this are just going to dismiss it all as insane. They're going to dismiss the full context of the article as insane as well, but at least the writer very nakedly identifies themself as radical, which helps put things into perspective.
*There are obvious caveats to the point I'm making. I think most of us can agree that the best teachers recognize things they can learn from their students and do learn from their students constantly. I'll never forget how one of my sixth-grade teachers -- the one I felt closest to actually -- wrote in my yearbook something like (quoting as best I can from memory) "Every now and then, we teachers find a student from whom we can learn. Thank you for being that student for me."



From Of Innocence and Of Experience by Sophie Lewis
#not as charitable as i could be#children's rights#trans issues#education#social model of disability#radicalism#i apologize to the mutual i'm directly reblogging this from#who has more personal reasons than most to be bitter#at the power imbalance between parents and their offspring#and to view places like tumblr as a safe haven or even lifesaver
1K notes
·
View notes
Text
it’s crazy to think about how mohamed is chronically ill just like i am. while i an medically gaslit and blamed in american hospitals, he barely has access to care at all. i only need to care for myself and my small household; mohamed has a wife and three children relying on him. he has the same trouble breathing that i do when my illness is at its worst. he has the same pain in his face.
to assist this family is to assist all of us who are abandoned by imperialist models of care; disabled liberations means free palestine. a radical approach to illness is a decolonial approach. please help my friend.
#192 on el-shab-hussein and nabulsi's spreadsheet of vetted fundraisers.
78 notes
·
View notes
Text
Psych Abolition Chat: Harm Reduction for Disorderly Eating

A huge thanks to all the people who came to the first set of Harm Reduction Chats! I really enjoyed spending time with you all + I was surprised by the turnout + delighted by how much everyone had to say.
Some topics we touched on across both sessions:
disability + eating disorders + the ways that those intersect, as well as dealing with grief related to acquiring a disability via an eating disorder
the problems with withholding harm reduction until one's eating disorder has been sufficiently "severe + enduring"; harm reduction as a right for all
harm reduction in restrictive settings like inpatient: is this possible?
abstinence-only care models for eating disorders + the harm they cause
autonomy, choice, + ng tubes; autonomy as the defining factor of positive experiences with all forms of care
the invisible labor of having to teach oneself harm reduction techniques when they aren't widely available
disordered eating, obsessions + compulsions, whether or not disordered eating is a manifestation of obsessions/compulsions
People showed interest in creating or crowdsourcing the following:
more resources on harm reduction for laxative use
basically any harm reduction resources about eating disorders that are actually rooted in radical principles of autonomy
community/social connection for sharing grief surrounding acquired disability from eating disorders
The next set of sessions will be focused on self-injury + presented by Elliott @trans-axolotl + they are on Monday, Sep 16th at 9pm EST + Saturday, Sep 21st at 12pm EST.
The compiled resources from all of the sessions can be found here. I am still looking for more resources, especially pertaining to ED harm reduction!
(img src; Louise Bourgeois, 10 AM is When You Came to Me, 2006)
140 notes
·
View notes
Text
There are three main models of disability that are in common use. The moral model, the medical model, and the social model.
You may not have heard of the moral model before, but if you are disabled, you have felt the impact of it. The moral model is disability as a failure of character. It sources the problem of disability in the character of the disabled person. It's the people who insist that if you just tried harder, were better, had a better attitude, that you would no longer be disabled. It is a model that is used by ableists in order to conceptualize of disability as a failing of the individual. An extreme example of this mindset are the Christian Scientists, who believe that all illnesses and disabilities should be healed by the grace of their god and that if you are not healed, something is wrong with you. It is the the most cruel of the models, and the least successful at assisting disabled people.
The medical model is the model used by the medical establishment and by those who put their stock in medical authority. It sources the problem of disability in the body. It measures disability against a theoretical average person, and seeks to make disabled people match that average person more closely. This model works very well for disabled people with disabilities that can be measured, have a potential treatment plan, and want their disability gone. It does not work very well for people who do not match all three criteria. If they match the first and second but not the third, then strict adherents of the medical model often fall back on the moral model, stating that they are stupid, lazy, or selfish for not being interested in being cured. This also often happens if treatment fails to improve the condition of the disabled person.
The social model is a newer model, largely designed by disability activists and scholars and often defined in opposition to the medical model. It sources the problem of disability in the interaction between the disabled person and their physical and social environment. It argues that the solution of disability is to change the environment so that impairments are no longer an issue. This model works very well for disabled people who consider their disability not to be an issue when fully accommodated. It does not work well for people who consider their disability an inherent impairment and/or desire a cure. Strict adherents of the social model often fall back on the moral model when considering these people, stating that they are short-sighted or that they worship the medical model. These are the people who state things such as that depression would not exist in a world without capitalism.
When a disabled person fails to behave as expected by the model a person has of disability, the moral model is almost always the fallback position, because many people cannot conceive of why someone would disagree with them other than a lack of good character. This is a problem, because the moral model proposes no solution but to ignore or abuse the disabled person until they behave as expected.
Another notable interaction is that adherents of the medical model can often be persuaded to support the more traditional parts of the social model, such as providing large text resources to people with impaired vision, so long as there is empirical research backing it. However, they rarely support more radical arguments that challenge how we define disability and how society should be structured or restructured.
All three models have major failure points. The moral model fails every disabled person it is applied to. The medical and social models both fail different disabled people when adhered to strictly. The best approach at the moment seems to be hybridizing the social and medical models, so that they cover each other's weak points and fit the needs of the widest spectrum of disabled people. The main barrier to this is that they are often defined in opposition to each other.
#I personally adhere to a hybridized model of the medical and social models that I informally call the independence model#If an individual is disabled or not is their personal call#as is what they do about it.#it does need to be acknowledged who is considered disabled by our society and how that will affect someone#even if they do not consider themselves disabled#Medical care and accommodations should be available to whoever wants it#but should never be forced or pressed on anyone#Public spaces and events should be accessible to as wide a variety of people as possible#The main failure point of the independence model is that it does not call for a single clear solution#and basing a model around personal choice makes it difficult to make policy proposals
147 notes
·
View notes
Text
"There are four key concepts in the radical model. Firstly, disability is not separate from other forms of oppression; rather, it is interlocked with and overlaps them. Secondly, what is considered normal is arbitrary and requires deconstruction. Up until this point, all of the models of disability have failed to challenge the supremacy of the norm. Margrit Shildrick and Janet Price (1998: 236) have written, "A more radical politics of disability, then, would disrupt the norms of dis/ abled identity … by exposing the failure of those norms to ever fully and finally contain a definitive standard:' Thirdly, the disability label is used to marginalize specific types of people in order to obtain and maintain power; the classification of disabled is a political determination, not a biological one. Disability is not about whether or not something is "wrong" with someone; it is about the classification of disability, which allows certain people to be marginalized and other people to both benefit from that marginalization and justify it, because the rest of ns are inferior. Lastly, accessibility cannot be addressed universally; rather it must be approached holistically"
-AJ Withers, Disability Politics and Theory. "Looking Back But Moving Forward: The Radical Model of Disability"
#personal#disability justice#disability studies#radical disability model#will post notes on this in a sec. seeing that a lot of ppl are talking about disability models again and i want to share one of#the disability models i find the most helpful for talking about disability#disability#actuallydisabled
44 notes
·
View notes
Text
I read this extremely disturbing article about weight loss “treatment” (drugs and even surgeries) for children. I do not recommend reading it if you struggle at all with internalized sizeism or body image unhappiness. It is extremely upsetting. Really, don’t read it.
The focus of the article is a teenage girl called Maggie who has been pathologized for her weight her entire life, literally since infancy, and then, as a 13 year old, was given weight loss drugs and bariatric surgery. The writer of the article, Lisa Miller, is clearly framing child weight loss as a reasonable medical practice and “radical fat-acceptance advocates” as somehow going too far. Miller is also clearly framing child weight loss interventions as necessary for “health” reasons.
My partner alerted me to a journalistic trend we started noticing around 2015 – when a writer is trying to express that the people they’re writing about have one motivation, but all the actual quotes from the subject express a different motivation. This often happens when a writer is trying to argue that support for a racist/sexist/bigoted policy position or politician isn’t motivated by racism/sexism/bigotry; it’s motivated by Some Other Thing – and then every actual quote from a supporter is some strain of racist/sexist/bigoted (see: almost every mainstream article from the mid-2010s about the alt-right, men’s rights, gamergate, or the Trump movement).
In “Ozempic Era,” Miller is trying to convey that child weight loss interventions are necessary “treatments” for “medical problems,” not the result of forced aesthetic conformity due to systemic sizeism – but the actual parents and kids she quotes all cite aesthetic and social reasons for wanting their children or themselves to lose weight. They talk about fitting in. Fitting clothes. Being accepted. Gaining confidence. Wanting to look like thin, popular kids. One of the parents explicitly rebutted the fat-acceptance movement by saying “The world is not built for overweight people” as though acknowledging and changing that fact isn’t the entire point of the movement.
But really, fat acceptance barely got acknowledged at all. The bulk of the contrast, as usual, was between the “judgmental” view that “blames” fat people for being fat, and the supposedly more progressive medical view that blames genetics, environment, and other factors outside an individual’s control for fat people being fat. It’s so much easier to start the conversation at “Whose fault is it that fat people are fat?” and “What’s the best way to make fat people stop being fat?” than to step back and question “Why is being fat a bad thing?”
I don’t even think the parents being interviewed are being disingenuous, necessarily. So often in discussions of fat liberation, disability liberation, mad liberation, neurodivergent liberation, whatever, people clinging to the medical model will insist, as though they’re the first ones to think of it, “What about the problems with being (fat/disabled/etc) that aren’t caused by social factors? What about the suffering intrinsic to the condition itself? Social change wouldn’t fix that!” and then, when asked for examples, will immediately cite examples of problems caused by social factors and systems. Clothes not fitting is a social problem (clothing is made by humans!), not a problem intrinsic to fatness. Bullying is a social problem (humans are the bullies!), not a problem intrinsic to fatness. Fat children lacking self-confidence is a social problem (self-confidence largely comes from relationships!), not a problem intrinsic to fatness. People are really out there trying to come up with non-socially-caused problems intrinsic to fatness and citing “airplane seats” as though airplanes are naturally occurring.
A perfect example of this in Miller’s article is that now that Maggie has lost weight, she can be a cheerleader – she’s still not small enough to be at the top of the pyramid, but she’s strong enough to be at the bottom of the pyramid!
How, exactly, is weight loss necessary for that? There’s no size limit to the bottom of the pyramid! That’s where your heavy people are supposed to go! There are, at least, actual physics-based reasons why a heavy person might not be suited for the top of the pyramid. If the claim were “Before she lost weight, she was on the bottom of the pyramid, but afterward, she’s small enough to be on the top,” that would at least be a change directly connected to her physical weight. But for any physical activity that doesn’t directly involve being lifted, weight should have very little connection to ability. Fat people can and do run, lift, swim, and do every physical activity that thin people do. Of course, various medical conditions and disabilities can affect those abilities (in fat people, thin people, medium-sized people, and everyone else), and not everyone is particularly interested in athleticism, but it’s just dishonest to pretend or imply that thinness is a prerequisite for any kind of athletic activity.
“But, Hypatia,” you, the straw reader who lives in my head, might be saying, “You’re always talking about youth rights and autonomy! If the 13 year old consented to have her body surgically and chemically altered, shouldn’t we respect her choice?”
Great question, straw reader who lives in my head. Consent has to be informed. And uncoerced. I do not believe that a 13 year old who has been pathologized for her weight since she was an infant, who has been told by her parents and doctors and every authority figure in her life that her body is a problem, who has been relentlessly bullied and ostracized for her weight, is making an uncoerced choice. Nor, if she has never been exposed to the fat acceptance/liberation or health at every size models, is she making an informed one. There is no indication that accepting her naturally fat body was ever an option for her.
Regardless, my point isn’t even “13 year olds shouldn’t be prescribed bariatric surgery or weight-loss drugs” (although I absolutely think they shouldn’t, and I wonder where the people who [falsely] think gender-affirming care is “permanent surgery on children” are on this). It’s “We should abolish the pervasive, unquestioned, widespread systemic sizeism that leads people to think fatness is a bad thing.”
87 notes
·
View notes
Text
The ugliest part of the DSM-IlI story is "the people involved," those who practiced what Lewis calls "bad politics" (109). This story is a shocking array of subterfuges and exclusions, with the role of chief villain going to Robert Spitzer, chair of the task force that created DSM-III. Lewis reports that the committee assembled by Spitzer during late 1974 and early 1975 consisted of five psychiatrists who formed an “invisible college” of like-minded researchers" (112) and "carefully eliminated any people with alternative perspectives," including clinicians (114). The task force quickly made major changes to the manual, including its new emphasis on medicalization and classification, and then, for five years, "covered its tracks" by engaging in a long process of "field trials" that, Lewis maintains, "effectively covered over" the fact that a very small group had already made most of the major ideological and procedural changes (114). The DSM-III, Lewis points out, claims that the field trials involved over 12,000 patients evaluated by about 550 clinicians, and lists hundreds of "contributors" (114). But those involved in the field trials "tested the manual according to the rules, norms, and priorities of the initial [five-member] task force" (115). In other words, these "contributors" were "testing" a model that had already been radically shifted; they were not involved in the ideological, rhetorical, and clinical shift itself.
From that point, Lewis's story of "bad politics" grows even more disturbing, citing exclusion of psychologists, social workers, and researchers who attempted to bring feminist perspectives to DSM-III. "[P]retty much anyone who was not a privileged, white, male, academic psychiatrist," Lewis concludes, was "systematically snubbed, ignored, denigrated, and dismissed" (115).
Margaret Price, Mad at School: Rhetorics of Mental Disability and Academic Life
14 notes
·
View notes
Text
Some new, bright variants of the Disability Pride flag (with historic colours)




The diagonal stripe Disability Pride flag design by @capricorn-0mnikorn et al is flexible about the specific colours used for the red, yellow, white, blue, and green stripes - there are a variety of versions ranging from full saturation to reduced saturation.
For fun -- and to lean into my proposal for the stripe colours to be about different models & causes of disability -- I thought I'd make variant versions where the stripe colours come from historic flags and symbols made by disability organizers!
These are intended as supplementary variants of the main versions for circumstances where we want to talk about disability history. (I think the standard, desaturated version is the best general-purpose disability pride flag!)
The versions on the left have a silver grey (#cfd1d0) background from the Eros Recio disability flag. The versions on the right have the original black. The black/grey is to mourn disabled people who have died due to eugenics, violence, neglect, and illness.

Red: disability caused by violence and/or neglect (itself a form of violence). Also models of disability like debility and disabled black feminist theorizing which focus on how disability is used as a tool of violence to enact societal oppression.
The red (#f71d20) comes from the red AIDS ribbons (1991) used to protest the societal neglect of the AIDS pandemic. HIV/AIDS was ignored by governments for years because they either didn't care - or thought it was a good thing - that massive numbers of gay, black & hemophiliac people were dying.
Similar reds are now used by the Millions Missing (2016) campaigns to advocate for research and treatment for ME/CFS, another disease which disproportionately affects disadvantaged groups (mostly women) that has been widely neglected and dismissed.


Yellow: disability caused by natural differences. Models like the affirmative model and evolutionary models which view disability as providing positive benefits to individuals and/or society.
The specific golden yellow (#FDD70A): comes from the intersex flag (2013). Intersex is an umbrella term for natural bodily variations that don't neatly conform to ideas of "male" or "female". As a result we are medicalized when there is nothing actually wrong with us. (We intersex folks also belong to the queer community because of how we threaten binary ideas about sex/gender.)
Gold also appears on the Eros Recio disability flag (2017). More recently (2018), gold has become associated with autism, another natural difference.


White: disability caused by unknown or other factors. Models like the human rights model, which focus on how disabled people - regardless of how or why they are disabled - are deserving of basic human/civil rights and liberties.
The specific white (#FFFFFF) is from the neurodiversity flag. I have been unable to track down the first one from 2005 but a large variety of rainbow infinities on white backgrounds have been used ever since for neurodiversity.
Neurodiversity is a large umbrella category, and can be caused by many factors.

Blue: situational disabilities. Models like the social model and the radical model which posit there is nothing wrong with us. The problem is how society excludes us.
The specific blue (#009ee0) comes from the Deaf flag (2011). Many Deaf people feel there is nothing wrong with being Deaf, the problem is that the rest of society does not use signed languages, provide captions & transcripts, etc.


Green: disability due to natural illness. By "natural" I mean not socially imposed like how how treatable diseases are allowed to persist due to sociopolitical oppression/neglect. This is associated with medical models of disability.
Honestly I struggled for a historical flag for green - seems green is not a colour that disabled organizers seem to have been using until very recently(?). There are a bunch of green awareness ribbons from the 00s such as for kidney cancer, mitochondrial disease, hepatits B, and lyme disease. But I could not find evidence that any of them were made by the people with the relevant disabilities.
If anybody knows of any disability-led designs that prominently feature green that were used before ~2016 please let me know!
Green has been used as a colour for mental illness since at least 2013, and judging from my google image search results for "green ribbon awareness" this has been the most popular green ribbon awareness campaign.
But everything I can find gives me the impression this green ribbon campaign was created by sane people, though some celebrities who have been open about having mental health problems have backed the campaign.
The green sunflower lanyards used to indicate hidden disabilities started in 2016 in the UK, from which I got this green (#1f9a4b).

Purple: disability as a community. Models like the social construction model which focus on how the category of disability is socially constructed and maintained.
The purple (#82609b) is from the mad pride flag (2013). Mad pride has its origin in the psychiatric survivor movement, which has been critical of how psychiatry defines and punishes madness.
Madness in particularly has a long history of being socially constructed. For example, in how sociopolitical oppression can be twisted into individual pathology: black slaves who fled slavery were diagnosed with "drapetomania" rather than for society to understand slavery as oppression. More recently, terms like "climate anxiety" and "climate grief" have been used to individualize the climate crisis.
Including purple in the place of green in the flag is as a means to include mad pride & mutual aid communities when talking disability history. The five colours of the standard disability pride flag are to symbolize all of humanity, being the most common colours used in national flags.
Swapping out the green for purple for talking about disability history kind of represents how we disabled people have been on our own, not really represented by nation-states.
#disability#disability pride#disability pride month#disabled pride#recoloured flag#flag history#disability history
43 notes
·
View notes
Text
over 20,000 people in the United States died of Covid-19 since the beginning of 2024. Millions who avoided death are nonetheless still living with Long Covid, and this number grows each month. We are still in crisis.
Most importantly, though, implementing accessibility measures during an active pandemic is the right thing to do, as it makes events safer for everyone. Black communities, people of color, the disability community at large, members of the LGBTQIA+ community, and low-income communities continue to be especially hard-hit by the pandemic and the abandonment of Covid-19 precautions. The pandemic reproduces the very forms of ableism, classism, and racism that existed before 2020. There are millions of already systemically marginalized people who are being further pushed out of public life. This is unjust, and we must do better.
[However,] a blueprint for radical inclusion and living a full, safer life within the context of Covid-19 exists.
source

Install HEPA filters in your space. Installing a plug-in air purifier in your space is a great place to begin. Because almost all public spaces currently fall short of the ventilation needed for Covid-19 safety, it’s safe to assume that your space would also benefit from this efficient first step. Make sure it’s appropriately sized for your space and continuously running. If funds allow, upgrade your HVAC system to include HEPA filtration.
Practice mask requirements. Consider requiring and providing high-quality masks for everyone who will be in your space and attending your events. Contrary to popular belief, mask requirements do not deter guests in any meaningful numbers. Clean Air Club has been hosting Covid-safer events in Chicago for over a year, and a majority of the mask-required events sell out every time. If obtaining masks for your event is cost-prohibitive, check in with your local mask bloc for assistance.
Collect and share data on the safety of your space and region. Collect data on the ventilation in your space using a carbon dioxide (CO2) monitor. The higher the number, the more attention you need to pay to improving the ventilation and air purification in the space. Open windows and doors, crank up the HVAC, and plug in another purifier. You’ll know you’ve succeeded when the CO2 levels in your space are close to the levels expected outdoors in fresh air (around 400 ppm). As a bonus, this improved ventilation and purification will remediate poor air quality due to climate-change induced wildfires, improve concentration, and aid in accommodating disabling conditions such as asthma and allergies. Data collection should also include monitoring wastewater data, now our most accurate picture of the true prevalence of Covid-19 and other wastewater-monitored viruses in our population at any given time. We can use this data to increase the number of mitigation strategies adopted when wastewater levels are high. Consider creating an internal chart at your organization that lists protocols associated with different wastewater levels, reducing the burden of communication and oversight during higher periods.
Consider additional mitigation layers. Some of the other layers of protection from the swiss cheese model include: pre-event testing, far-UVC lights, providing options for virtual participation, and asking guests to stay home if they’re showing any symptoms of contagious or novel illness. Consider promoting individualized mitigation approaches within your organizations, such as the usage of nasal spray and CPC mouthwash. The key is to remain creative, flexible, and open to adding layers of protection in response to changing risk levels in the environment.
Open up lines of communication. As you implement mitigation layers, communicate them to your community. Ask them how they’ve been impacted by Covid-19 and give people space to share their access needs and ideas. This will provide a crucial why behind your actions and investments. Using the accessibility principle of designing for the highest possible need, your virus safety plan should accommodate the most vulnerable and impacted community members rather than those who have high risk thresholds or behave as though the pandemic is over. Part of effective pandemic communication includes providing accessibility and virus safety information in an Access Note or in an Accessibility Guide. This information should be repeated often in marketing and outreach materials.
Resources
30 notes
·
View notes
Text


(Mis)trust and (ir)responsibility under Empire
Working through trust and responsibility is difficult because both of these words have been so thoroughly colonized by Empire. An important place to begin, we think, is with the ways that Empire sows mistrust and destroys our capacity for collective responsibility by making us dependent on its destructive, depleting, violent ways of life.
Many people’s impulse is to mistrust others from the start, and it makes sense, given that many of us have been living Hobbes’s dream, made real, for centuries. Most everyone we know has been touched by some kind of oppression and abuse, and Empire’s oppressive divisions often lead people to betray even their most intimate relations. For instance, feminists have coined the term “gaslighting” to get at a common patriarchal dynamic that undermines the perceptions of women and femmes by second-guessing, explaining away, and denying their experiences and insights. Gaslighting can be subtle and unintentional, but as feminist writer Nora Samaran explains, it is particularly insidious because it undermines people’s trust in their own capacities:
If you think of the power, the strength, the capacity to effect change that women who trust themselves are capable of, what we are losing when we doubt ourselves is an indomitable force for social change that is significant and therefore, to some, frightening. In other words, our capacity to know ourselves is immensely powerful.[99]
All forms of oppression seem to have this tendency: racism, heteropatriarchy, ableism, ageism, colonization, and other systems of oppression contort people’s insights, experiences and differences into weaknesses or deny them outright. For this reason, the emergence of trust can be a powerful weapon, which is being recovered all the time through struggle.
For many of us, mistrust in ourselves and others started when we were kids, and in a lot of cases in our homes. When they’re really young, kids are curious, open, vulnerable, and capable of radically trusting those around them, and this tends to get sucked out of them from many directions by Empire and the kinds of hierarchical and competitive relationships it promotes. One of the most damaging forms of distrust is built into modern disciplinary institutions, and schooling in particular. As organizer and scholar Matt Hern writes,
At school children are always monitored, and schooled parents believe that they should similarly be constantly monitoring their offspring, in the name of safety. The last decades of this century has seen an exponential growth in concern for children’s daily safety, particularly in cities, and most parents I come into contact with want to keep a very close eye on their kids. This is a laudable concern, and one I share, yet I have a deep suspicion of the equation that safety = surveillance. There is a threshold where our concerned eye becomes over-monitoring and disabling, an authoritarian presence shaping our kids’ lives.[100]
Hern is not singling out certain parents as oppressive, and he implicates himself in this, too. He is pointing to the collective inheritance of a way of life that divorces people from their capacities to trust each other. The model for inculcating these values was (and is) intense discipline and control: kids are encased in concrete for over a decade, trained to sit still, memorize, and obey authority. As the political theorist Toby Rollo has argued, it is no coincidence that colonization, racism, heteropatriarchy, and ableism all tell stories that constitute oppressed and dispossessed people as children.[101] Empire conceives its Others as untrustworthy and lacking maturity, health, morality, knowledge, civilization, and rationality, and so they have all been targets for education, confinement, and control—or for total eradication and genocide.
#joy#anarchism#joyful militancy#resistance#community building#practical anarchy#practical anarchism#anarchist society#practical#revolution#daily posts#communism#anti capitalist#anti capitalism#late stage capitalism#organization#grassroots#grass roots#anarchists#libraries#leftism#social issues#economy#economics#climate change#climate crisis#climate#ecology#anarchy works#environmentalism
15 notes
·
View notes
Text
Undoing Suicidism: A Trans, Queer, Crip Approach to Rethinking (Assisted) Suicide by Alexandre Baril
In Undoing Suicidism, Alexandre Baril argues that suicidal people are oppressed by what he calls structural suicidism, a hidden oppression that, until now, has been unnamed and under-theorized. Each year, suicidism and its preventionist script and strategies reproduce violence and cause additional harm and death among suicidal people through forms of criminalization, incarceration, discrimination, stigmatization, and pathologization. This is particularly true for marginalized groups experiencing multiple oppressions, including queer, trans, disabled, or Mad people.
Undoing Suicidism questions the belief that the best way to help suicidal people is through the logic of prevention. Alexandre Baril presents the thought-provoking argument that supporting assisted suicide for suicidal people could better prevent unnecessary deaths. Offering a new queercrip model of (assisted) suicide, he invites us to imagine what could happen if we started thinking about (assisted) suicide from an anti-suicidist and intersectional framework.
Baril provides a radical reconceptualization of (assisted) suicide and invaluable reflections for academics, activists, practitioners, and policymakers.
#undoing suicidism#undoing suicidism: a trans queer crip approach to rethinking (assisted) suicide#alexandre baril#trans book of the day#trans books#queer books#bookblr#booklr
28 notes
·
View notes
Text
okay. going to go try to work on some of my essays. i know in a pinch i can write a 5 page essay in 30 minutes if i have all the sources already so. i can do this
#personal#half the essays are disability studies essays too so that should be better#can just pretend im penispoasting. one of my essays is about carceral ableism and the radical disability model like.#my favorite fuckign topics#sorry. im so angry a lot of the time right now. i don't have the patience for any of this shit
28 notes
·
View notes