#medical billing company in new york
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
25% of US internet users with an annual income of $80-100K use Tumblr.
Text

Expert Medical Billing Services Company in New York
RCM Billing Services is a full medical billing company providing services to healthcare providers in New York & Texas. Maximize your revenue and streamline your practice with our comprehensive medical billing services in New Jersey. Our team of experts ensures accurate and timely processing, reducing claim denials and improving cash flow.
#medical billing in new york#medical billing services in new york#medical billing company in new york#medical billing services in new jersey#medical billing in new jersey#medical billing company in new jersey#medical billing company in texas#medical billing services in texas#RCM Billing
2 notes
·
View notes
Text
MedICD specializes as a Medical insurance credentialing company in Georgia
MedICD, a leading medical insurance credentialing company in Georgia, starts your healthcare practice or facility journey right. Our specialists establish strong relationships with insurance companies and patients through expert credentialing services. We secure and update facility and physician contracts, ensuring optimal reimbursement rates. Let us enhance your professional ties and patient care capabilities.
#Medical insurance credentialing company in Georgia#Medical insurance credentialing company in New York#Medical insurance credentialing company in New Jersey#Medical insurance credentialing company in Florida#Medical insurance credentialing company in Texas#Medical insurance credentialing company in California#Medical insurance credentialing company in Arizona#Medical billing company in Florida#Medical billing company in Texas#Medical billing company in New York#Medical billing company in New Jersey#Medical billing company in California#Medical billing company in Georgia#Medical billing company in Arizona
0 notes
Text
Searching Medical Billing Company in New York?

Are You Finding for Medical Billing Services Nyc? Medvantis is Tob Medical Billing Services New York. We Are Providing Enrollment and Credentialing, Eligibility Verification, Claims Transmission, Payment Posting, and Accounts Receivable Follow-up. For More Detail Visit Us!
#medical billing company in new york#medical billing services new york#medical billing services in ny#medical billing services nyc
0 notes
Text
Unfortunately, doing this requires one to ignore ones moral sensibilities and participate in a dreadful realm of business accumen...
this isn't funny anymore I need to find a way to have money without having to work another day in my life
#I have a friend who started a medical billing company and a marketing company and doesn't work anymore#Like oh so you did evil and now you are 40 and work in the community garden and go rock climbing 5 days a week...#go off.. I guess...?#All my other well off friends just work tech in new york which is it's own hell in my opinion
13K notes
·
View notes
Text
Oregon governor Tina Kotek yesterday signed the state's Right to Repair Act, which will push manufacturers to provide more repair options for their products than any other state so far.
The law, like those passed in New York, California, and Minnesota, will require many manufacturers to provide the same parts, tools, and documentation to individuals and repair shops that they provide to their own repair teams.
But Oregon's bill goes further, preventing companies from implementing schemes that require parts to be verified through encrypted software checks before they will function, known as parts pairing or serialization. Oregon’s bill, SB 1596, is the first in the nation to target that practice. Oregon state senator Janeen Sollman and representative Courtney Neron, both Democrats, sponsored and pushed the bill in the state senate and legislature.
“By eliminating manufacturer restrictions, the Right to Repair will make it easier for Oregonians to keep their personal electronics running,” said Charlie Fisher, director of Oregon's chapter of the Public Interest Research Group, in a statement. “That will conserve precious natural resources and prevent waste. It’s a refreshing alternative to a ‘throwaway’ system that treats everything as disposable.”
Oregon's law isn't stronger in every regard. For one, there is no set number of years for a manufacturer to support a device with repair support. Parts pairing is prohibited only on devices sold in 2025 and later. And there are carve-outs for certain kinds of electronics and devices, including video game consoles, medical devices, HVAC systems, motor vehicles, and—as with other states—“electric toothbrushes.”
Apple opposed the Oregon repair bill for its parts-pairing ban. John Perry, a senior manager for secure design at Apple, testified at a February hearing in Oregon that the pairing restriction would “undermine the security, safety, and privacy of Oregonians by forcing device manufacturers to allow the use of parts of unknown origin in consumer devices.”
Apple surprised many observers with its support for California's repair bill in 2023, though it did so after pressing for repair providers to mention when they use “non-genuine or used” components and to bar repair providers from disabling security features.
According to Consumer Reports, which lobbied and testified in support of Oregon's bill, the repair laws passed in four states now cover nearly 70 million people.
272 notes
·
View notes
Text
The Best News of Last Week - March 20, 2023
🌱 - Okra to the Rescue and Other News You Can't 'Lettuce' Miss This Week
1. 4 day work week being pushed in Congress

Progressive Democrats, led by Rep. Mark Takano of California, are pushing for a four-day workweek to give Americans more time for leisure outside of work. The proposed Thirty-Two Hour Workweek Act would amend the Fair Labor Standards Act of 1938 to require overtime pay for any employee working more than 32 hours in a week at a rate of time and a half.
More than 70 British companies have started to test a four-day workweek, and halfway through the six-month trial, most respondents reported there has been no loss in productivity.
2. Governor Walz signs universal school meals bill into Minnesota law

Minnesota just became the fourth state in the US to provide breakfasts and lunches at no charge to students at participating schools! The bill was signed into law by Governor Tim Walz on Friday, and it's set to ease the burden on parents who struggle to provide meals for their children.
The new legislation will cover the cost of meals for all students, regardless of household income. This means that families who don't qualify for free and reduced meals but who struggle to pay for food will also be covered. The bill is also meant to prevent "lunch shaming" practices, where children are denied food or given substitutes that indicate their family is struggling financially.
3. Texas Researchers Use Okra to Remove Microplastics from Wastewater

Researchers from Tarleton State University in Fort Worth, Texas discovered that food-grade plant extracts from okra have the power to remove microplastics from wastewater. Polysaccharide extracts from plants like fenugreek, cactus, aloe vera, tamarind, and okra were found to be effective non-toxic flocculant alternatives to remove microplastics from water.
Polysaccharides from okra and fenugreek were best for removing microplastics from ocean water, while a combination of okra and tamarind worked best for freshwater. Furthermore, plant-based flocculants can be easily implemented in existing water treatment facilities.
4. In the northern California snow, stranded cows are getting emergency hay drops
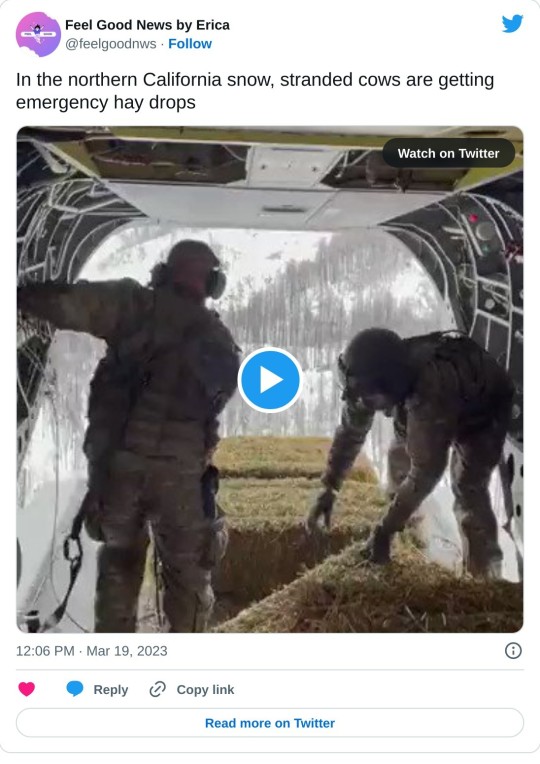
The recent wave of unprecedented snowfall in California has left cattle stranded and starving. When rancher Robert Puga ran out of hay, neighboring Humboldt County officials put together an emergency rescue operation called "Operation Hay Drop." State, federal, and local officials airdropped stranded cattle bales of hay to feed them.
Humboldt County Sheriff William Honsal went to the Coast Guard with the idea of a helicopter rescue, and by midday Sunday, March 5, Operation Hay Drop was underway. So far, Operation Hay Drop has been a success, said rancher Puga. The mission covers about 2,500 head of cattle over several miles.
5. Make-A-Wish Foundation no longer considers Cystic Fibrosis to be automatically qualifying due to improvements in life outcomes for patients

Given the ongoing life-changing advances in cystic fibrosis, beginning in January 2024, cystic fibrosis will no longer automatically qualify for a wish.
6. 1st woman given stem cell transplant to cure HIV is still virus-free 5 years later

In 2017, a woman known as the "New York patient" underwent a stem cell transplant to treat both her cancer and HIV. Now, about 30 months later, she has been virus-free and off her HIV medication, leading some researchers to suggest that she may have been cured of HIV.
The New York patient, received stem cells taken from umbilical cord blood that also had the HIV-resistance genes. However, it's important to note that there is no official distinction between being cured and being in long-term remission, and the medical team is waiting for longer-term follow-up before making any definitive statements.
7. Cheetahs Back in Wild in India After Seven Decades

Namibian cheetahs have been successfully reintroduced to India after the world's fastest land animal was declared extinct in the South Asian country more than 70 years ago. Two cheetahs, Obaan and Asha, were released into the wild of Kuno National Park after being brought to India last September.
The species is being reintroduced on an experimental basis as part of a major prestige project for Prime Minister Narendra Modi. India aims to bring in about 100 of the big cats over the next decade. The African cheetah is a different subspecies from the extinct Asiatic cheetah, which once roamed the sub-continent in great numbers.
Lastly, I recently opened a Youtube channel. Subscribe for a weekly compilation of feel good videos.
- - -
That's it for this week :) If you liked this post you can support me with a small kofi donation:
Buy me a coffee ❤️
Let's carry the positivity into next week and keep spreading the good news!
640 notes
·
View notes
Text
Your Great-Grandparents Huffed Laughing Gas, And People Paid To See Them Trip
For the height of entertainment, early Cincinnatians enjoyed dropping by one of the local museums to watch their fellow citizens get stoned. The intoxicating agent was not cannabis or opium or shrooms, although all were readily available, but nitrous oxide or “laughing gas.”
The Western Museum started the trend. Founded in 1818 as one of the earliest scientific museums in the United States, the Western Museum is the ancestor of our Museum Center at Union Terminal. Regardless of its heritage, the institution struggled throughout its existence. Although stocked with fossils, minerals, Native American artifacts and animal specimens, the most popular attractions were grotesque wax figures and monstrosities like two-headed piglets and eight-legged lambs.
The museum directors, Robert Best and Joseph Dorfeuille, soon learned that lectures on scientific topics sold more tickets if they tacked a laughing gas demonstration onto the end of the program. An advertisement in the Liberty Hall and Cincinnati Gazette [30 November 1822] is typical:
“Messrs. Best and Dorfeuille will lecture on various departments of Natural History, and Natural Science, the latter to be illustrated by a great variety of amusing and instructing experiments; among others, they will frequently repeat the administration of the Nitrous Oxide, which has always proved in so high a degree interesting.”
By 1834, the Western Museum had replaced laughing gas with a waxworks replica of Dante’s Inferno, and found a young man to spice up the infernal regions with flashpots and fireworks. His name was Samuel Colt, and he would later build a huge firearms company. While he lived in Cincinnati, however, Colt was a 20-year-old hustler fascinated by laughing gas. He billed himself as “the Celebrated Dr. Coult of New York, London and Calcutta,” and pumped nitrous oxide into anyone who paid for a ticket. His on-stage antics here made news far away. The Albany, New York, Argus [30 July 1833] reported:
“A certain Dr. Coult is administering the nitrous oxyde gas at Cincinnati, and by way of making the entertainment ‘peculiarly attractive,’ the gas is inhaled by a ‘curiously deformed black man.’”
The Daily Cincinnati Republican & Commercial Register [6 November 1834] assured readers that Dr. Coult’s exhibitions at Frederick Frank’s art gallery on Front Street contained “not the least shade of impropriety,” and insisted – no matter how entertaining the effects – this was all about science:
“Dr. Coult’s exhibition presents some of the most pleasing and laughable scenes one can well imagine. – Although the peculiar effects of Nitrous Oxide keeps the audience in a state of almost continual merriment, yet there is a great chance for the learned and curious to exhaust all their wits in sober contemplation of the effects of Nitrous Oxide upon the human system.”

Although nitrous oxide had been known and described by English scientists in the 1700s, the gas remained a psychotropic curiosity until its anesthetic properties were discovered in the 1840s. Its potential as an pain reliever was discovered during an on-stage performance by a medical school dropout named Gardner Quincy Colton. Although Colton later built a dental empire by promoting laughing gas for tooth extractions, he stuck with his profitable stage shows for years. In October 1847, Colton filled the auditorium of Cincinnati’s Melodeon Hall over several nights and the Cincinnati Commercial [2 October 1847] reported on the effects of his laughing gas on some selected subjects.
“The effects were different upon different individuals. “A. after the gas bag was removed from his lips, he stood for a moment, staggered about the stage, and finally fell to the floor. “B. commenced dancing a regular hoe-down with arms and legs in the most violent motion, leaping with all his might into the air, and exhibiting the most tremendous strength. This he continued until the excitement wore off. “C., a young merchant on Liberty street, of slight build, at some imaginary insult became enraged and commenced a furious battle upon those on the stage. Small as he was, it took five or six stout men to hold him until the effects of the gas passed away.”
Another subject was rendered “wonderfully polite and self-complacent” and wandered about the stage, rubbing his hands and bowing to the audience, while the next man up erupted in “silly laughter” while staring dumbly at the assembled onlookers. One young lawyer inhaled deeply, then stood in the most erect posture and recited a poem by William Cullen Bryant. According to the Commercial:
“The effects of the Gas lasted from two to five minutes, and seemed to pass off suddenly, dropping the taker of it down from the highest heaven to earth in an instant. We do not know why this gas should be called laughing gas. Most of the persons who took it on Tuesday evening were most solemnly serious. The whole performance passed off remarkably well, nothing occurring of the least unpleasant nature.”
Twenty years later, Doctor Colton was quite successful with his dental franchises, but still presented public demonstrations. On his 1866 tour through the Queen City, Colton not only recruited women as his subjects, but used them to promote his dental practice. An advertisement in the Cincinnati Gazette [17 April 1866] provides a rather shocking description of his show:
“On the above occasion, after the lecture, twelve ladies will inhale the gas, showing its amusing effects. Breathed in small doses, it exhilarates and develops the character. After which Dr. C. will administer it to several ladies in larger doses, producing profound anesthetic sleep during which he will extract their teeth without their knowledge. He will demonstrate that he has ‘a blessing’ to offer to the citizens of Cincinnati.”
Inevitably, once society latches onto some new exhilarant, reports emerge that insanity lurks within the depths of recreational chemistry. Call it the “Reefer Madness” effect. A Mrs. John Boyer of Cumminsville was sent to Cincinnati’s Longview Hospital for the insane in 1871 after weeks of increasingly erratic behavior were attributed to getting a tooth pulled by a Sixth-Street dentist using laughing gas. In 1867, the death of a Mrs. Bolum on Accommodation Street was found, on the result of autopsy, to have been caused by a strangulated hernia, but her family insisted it was dental nitrous oxide. And the Cincinnati Star [30 September 1876] carried this squib:
“There’s a young woman living in Glendale who, her relatives say, has become mildly insane by the use of laughing gas.”
Wasn’t that the whole point of huffing it anyway?

16 notes
·
View notes
Note
The Ken and Stella pregnancy blurb was so good could you write one where they find out that she’s pregnant?
ive been thinking about this scenario a lot and i cant really decide how i want this to go . . .
i think a year or so after they get married (stella is like 30ish) they start to really do their research and find the best fertility clinic in the city. its been almost 20 years since kendall and rava struggled to get pregnant, but still, he's not feeling optimistic.
stella gets a clean bill of health from the doctor, but ken isn't so lucky. just as he suspected, he was the problem. again.
was it the drugs? he was clean now, but he used so much...could he have ruined his chances forever?
stella assures him that it'll be okay, but she never went through what he had to 20 years ago.
they decide on a couple of treatments. they're both taking shots every day and pills at night and its exhausting. most of the meds go to kendall, but stella has to take some too, just in case.
they begin with intrauterine insemination, which is pretty simple and painless, but stella gets her period two weeks later. its hard on both of them, but especially kendall because he knows it's him, not her.
next they try ivf, which is a lot more complicated and expensive (not that money is an issue). now they both have to do injections and stella goes in for her egg retrieval.
the egg retrieval goes better than expected and they're left with 10. ken's sample has some relatively viable sperm so they pull the trigger and try to make some embryos.
the waiting is by-far the worst part, because deep down kendall knows there's no way those embryos are going to get made with his shitty sperm. he's right, unfortunately, and they're back to square one with zero embryos and ten now-frozen eggs.
kendall suggests a donor, like they did with iverson. stella's heartbroken, but they start to look into other options.
because they have the best doctors, however, they get into a trial for a new drug that increases sperm count and viability. stella is thrilled and insists kendall try it, but it's another injection and he's not super happy about it. nothing has ever worked for him, why now?
it's nice to have a break from more intense treatments, so they agree and kendall marks his torso up with injection pricks again.
three months later, ken and stella are enjoying some time off from surgery and tiny, microscopic cells that control their lives. kendall's in new york for the week, working on some financials for their production company (i imagine them making something rival to waystar and completely taking over the media scene), and stella is holding it down in los angeles, or at least trying to.
it's flu season and she's been to so many fancy parties in the last few weeks, stella is sick as a dog. she's a little worried, but the nausea, vomiting and headaches are typical for the flu, right?
she also chalks her late period up to stress. but it's been at least a few weeks...
the day before kendall is supposed to come home, stella drives herself to the hospital after she can't stop throwing up.
"when did the symptoms start?" the doctor asks.
"a week ago, i think, but ive been feeling kind of off for a while."
"and there's no chance you're pregnant? when was your last period?"
stella's heart skips a beat.
"um, i'm not sure. we're trying, uh, but it's been unsuccessful. my period is really irregular and i've been stressed so--" she trails off. "we've been trying for a couple of years."
"and are you taking medication?"
"i did, but it's not really..." she thinks for a bit. "it's not a uterus issue, it's my husband."
"and what is he taking?"
she tells the doctor about the new medication kendall is taking. "it's only been three months, so we're still hopeful. or at least i am."
"i've heard some great things about that new drug. it's really changing people's lives." the doctor smiles, turning away from stella and writing something down. "i'm going to order some tests, but i think you're fine."
------------------
kendall, obviously, sprints to his jet when stella tells him she's sick. she insists she's fine, but wants him to come home as soon as he can, which stresses him out to no avail.
he bursts through the door four hours later, finding stella reading a magazine on the couch.
"stell!" he says, running towards her.
"hey baby." she hugs him, bringing him down to the couch with her. stella presses her lips to his, but kendall is confused.
"aren't you sick?" he pulls away.
her face breaks into a huge smile. "about that..." stella gets up from the couch and walks to the kitchen.
kendall looks at her quizzically, as she comes back with a piece of paper in her hands.
"i have something to show you." she says, holding the paper close to her.
"okay..." kendall smiles at her, utterly confused.
stella carefully sits next to him on the couch. "here."
kendall recognizes the picture immediately. he used to frame them when rava was pregnant with iverson.
"what is this?" he holds up the ultrasound. it's too good to be true, right? tears prick his eyes.
stella is crying already, and takes his hand. "that's inside of me."
he looks down at the black and white photo again. a fuzzy, bean-looking object sits, next to another, smaller object. he's speechless for the first time in his life.
"what is that?" he whispers, pointing to the smaller object on the page.
stella looks at him, and he really can't read her for once.
"this surprise comes with another surprise." she laughs.
kendall's crying, but he takes another look. "is that..."
"yeah."
"two?" he smiles wide.
"i'm pregnant." she finally says, putting her hands on his cheeks. "baby, we're having twins."
they both burst out into crying giggles, hugging. kendall kisses her all over, stopping at her stomach. it's still pretty flat, but he knows her body so well he swears he can see a tiny bump growing.
THIS WAS SO FUN AND LOVELY TO WRITE I LOVE THEM AND I HOPE U DO TOO
25 notes
·
View notes
Note
so i know you mentioned the bros and usagi and co were going to continue protecting new york and the hidden city and stuff, but i can’t imagine a job like that paying much unless they were working for the police or something. so, if you plan on them having jobs other than that, what are they?
side note: i hc leo and mikey work for hueso for at least a little while, bc we know from that one hidden city ep they would make good(ish) servers
I just answered this a bit. As teenagers Usagi, Gen, and Kitsune work for Hueso. He called Leo in when he needs extra help and Mikey on days when his staff won’t come (mob days) Leo used to come whenever he needed a break from his family or a distraction from his thoughts. Now with his boyfriend and friends working there he basically has a part time job with how much he’s there helping out and hanging out with them.
As adults their jobs differ. Yes saving the city doesn’t pay the bills.
Donnie
a software engineer. He has two companies. One that sells hacking equipment and programs and one that sells security. There always seems to be an update in his hacking software right after there is an update in his security programs. There is just enough space for the people doing truly illegal stuff to get caught but never for the people pirating movies to get caught. Does he monitor his hacking programs to see what people are doing and strategically update the security programs just in time to catch career criminals and billionaire doing illegal things, he’s yes he does. - but most of his time is spent building other tech for his family or third business.
Mikey
a chef. I know I said he would study psychology if he could a while ago but his passion is food. He owns the most popular restaurant in the hidden city. The only thing he doesn’t serve is pizza as he doesn’t want to compete with Hueso.
Raph and Kitsune
They runs a non-profit helping people escape from abusive situations. Raph focuses on helping children while Kitsune helps women. They also have resources for men needing help as they know that men can get abused to and they want to help them as well. All of their siblings are the biggest doners to their project.
Leo
He goes into medicine. I think that splinter made all the boys get their education online so Leo was able to go to college/med school in the hidden city. I think he’d specialize in trauma surgery as it’s the closest to battle field medic. (I still haven’t decided his full path)
He does keep a list of doctors and nurses who are kind and treat patients with respect and dignity. He passes the list along to Raph so that he knows which doctors to request when the people he helps need medical care.
April
She becomes a journalist and is a big part of desegregating the hidden city and New York. Her goal is for her family to one day walk above ground without any fear.
Cassie
Brownie empire. She has a choke hold on the industry. She is playing the long game. Anytime April needs sources or Raph needs donations there is a brownie box showing up at the targets house buttering them up for her family to slip in and do what they need to. She still has her long goal, World Domination. As soon as her family is on board they are running this world. Unfortunately her family is not on board. (I will let you guess which members aren’t down with world domination)
Usagi and Gen
Body guard business. Usagi hates how much crime there is in the hidden city so he starts helping people. He gets a reputation of not being scared of any of the crime bosses. One thing leads to another and boom business. They only take jobs from people doing legal activity. Big Mama is not a fan but also wildly impressed. She’s tried to get them under her employment for years.
They get big enough to have other employees and there is always a shift going at Raph and Kitsune’s non-profit. It is the safest in the city as no one gets through their body guards.
They also teach self defense class and will do free ones at the non-profit. The whole family will join in on those.
Casey
Author. I’ve said it before but I’ll say it again, this boy has the most popular young adult novels out there. He is just writing down that happened in his timeline and people are losing their minds. He did it to keep his memory of them alive. Now he gets fan art of him and Master Leonardo when he was growing up in the mail. He also get letters asking how he could kill cheaters off when they were so beloved by fans. (Raph and Donnie’s deaths caused an uproar. His moms was expected as “all parents are dead in these kinds of stories”) When yokai and humans are finally intermixing a picture of Casey and his family comes out and everyone can tell that the characters in his book are based off of the turtles in his life. They all get some weird mail from that.
#a world of samurais and ninjas#asks#leosagi#rise leo#awosan miyamoto usagi#rise donnie#rise raph#rise mikey#rise april#rise cassandra#rise casey#awosan gen#awosan kitsune
75 notes
·
View notes
Text
By: Christina Buttons
Published: Feb 21, 2024
The Arizona Mirror published an article earlier this month titled "The latest GOP anti-trans strategy: Requiring ‘detransition’ services," arguing that legislation aimed at providing healthcare and insurance coverage for detransitioners is unnecessary—it is merely a tactic by Republicans to hassle people who currently identify as transgender. The article was republished under the same title in the Phoenix New Times.
The article focuses on an Arizona senate bill that would make the pathway of detransition easier for those who are struggling to get the healthcare they need. Currently, there are no billing codes for detransitioning, nor is there anything resembling a standard of care for this growing population. Additionally, some insurance companies explicitly exclude gender-reversal procedures.
But you wouldn’t learn any of this from reading the Arizona Mirror. It appears that the author, Gloria Gomez, only writes about the bill in an attempt to discredit it. The articles’ premise is that detransitioners face no difficulties in accessing healthcare and this bill is merely a scheme designed to inconvenience people who currently identify as transgender.
Gomez does not speak to a single detransitioner, opting instead to quote gender activists who argue the bill is “unnecessary” and not a “real issue” because detransitioners’ “medical needs are already covered by insurance.”
The first half of this article will debunk these misleading claims and clarify the purpose and necessity of detransition healthcare bills, offering a new contribution to the discourse. The latter half will counter several common misleading claims about detransition and "gender-affirming care" made by Gomez. For those familiar with my work, I often address these claims, so some of the content may be drawn from earlier writings.

Gomez quotes two representatives from the Human Rights Campaign (HRC), the largest LGBTQ political lobbying organization in the United States, which received $50 million in donations in 2023. The HRC regularly protests the New York Times' coverage of detransitioners and the inadequacies of the "gender affirming" model of care.
-
Misleading Claim #1: Detransitioners’ medical needs are “already covered by health insurance”
An emailed statement by Cathryn Oakley, the senior director of legal policy for the Human Rights Campaign (HRC) said:
“This bill is an unnecessary and gratuitous excuse to talk about detransition in an effort to shift the focus from the actual health care that transgender people receive, which is supported by every mainstream American medical health organization, to the care of a very small number of folks whose medical needs are already covered by health insurance.”
For many detransitioners, this is false.
There is significant variability among insurance policies regarding what is covered, leading to disparities in access to care. While some insurers may cover detransition care under certain conditions, others may not, deeming the care not medically necessary.
Had Gomez done any research she’d know some insurance companies explicitly exclude detransition healthcare—like Capital Blue, which has a stipulation in its plans stating gender-reversal surgery is “considered not medically necessary and, therefore, not covered.”
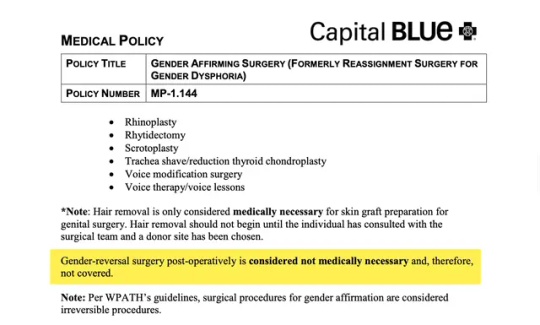
[ Capital Blue ]
…or United Healthcare Community Plan, which excludes “reversal of genital surgery or reversal of surgery to revise secondary sex characteristics.”
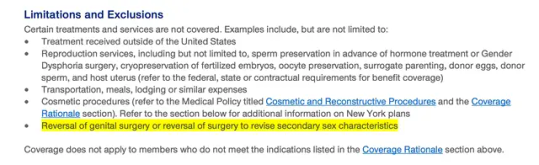
[ United Health Community Plan ]
Others evaluate on a case-by-case basis (California Health & Wellness) or if certain criteria are met (Wellmark), and thankfully, some health insurance companies do cover detransition healthcare (Aetna). These are just a few examples and by no means an exhaustive list. I plan to conduct a much larger overview of insurance providers’ coverage of detransition care in a future investigative article.
-
Misleading Claim #2: Detransitioners receive the same care as those seeking to transition
Bridget Sharpe, the director of HRC's Arizona branch, who responded to the Arizona Mirror's request for comment, said:
“The care for people who detransition is the same as the care for transgender people. Any medical service that affirms someone’s gender includes someone who decides to detransition. If they decide to detransition they are affirming their gender.”
This is not accurate.
Under the current system, when someone transitions, they receive a diagnosis code indicating gender dysphoria. When someone detransitions, they no longer meet the criteria for a gender dysphoria diagnosis. Without a specific diagnosis like gender dysphoria to justify “medical necessity,” obtaining coverage for detransition procedures can be complicated, demonstrating the need for legislation that ensures detransition is covered.
Legislation like SB 1511, which mandates that doctors, health care institutions, or any other licensed health care providers in Arizona offering gender transition procedures must also provide gender detransition procedures. Furthermore, if an insurance policy covers gender transition, it will be required to "provide or pay" for detransition procedures.
A third provision aims to collect information on how many people are requesting detransition procedures by requiring insurance companies to submit a report. Currently, there is no method for tracking detransition, so we don't know how many people are detransitioning.
Gathering more data on detransitioners would aid in the process of acquiring new billing codes from coding authorities. Nine months ago, FAIR in Medicine submitted an application to the Centers for Disease Control and Prevention (CDC) for International Classification of Disease (ICD) diagnosis codes specific to detransition. This application is currently under review. The process to review and approve new ICD diagnosis codes can take over a year and involves several steps, including gathering data, public comment, and revision.
The absence of dedicated medical billing codes for detransition procedures creates a significant barrier for healthcare providers seeking reimbursement for these services. Consequently, they may resort to using inaccurate billing codes.
In practice, healthcare professionals apply their discretion to navigate these challenges. For example, a detransitioned woman who underwent a hysterectomy as part of her transgender experience might be classified similarly to a postmenopausal woman for the purposes of accessing hormone replacement therapy.
An important article by Drs. Aida Cerundolo and Carrie Mendoza on detransition billing codes highlights a case like this: A woman named Katie began taking testosterone at 19, underwent a double mastectomy at 20, and had a hysterectomy at 24. Shortly after, she realized transitioning was a mistake.
Now at 25, Katie is experiencing early menopause and has had significant difficulty obtaining the correct hormone dosage. Even after numerous phone calls, she was prescribed estrogen at a dose typically given to males seeking to become transgender women, which was not suitable for her needs. For obvious reasons, this is not a sustainable solution. We need detransition billing codes.
-
Misleading Claim #3: Detransition healthcare is not a “real issue”
The director of HRC's Arizona branch, Bridget Sharpe, continued her statement by saying:
Instead of resolving a real issue, Sharpe said, the Republican legislation instead seeks to weaponize detransitioning against transgender health care.
It is insulting to dismiss detransitioners’ healthcare needs as not a “real issue.”
Had Gomez interviewed any detransitioners or reviewed research on them, she would understand that many encounter challenges in finding information on detransition or healthcare professionals equipped to address their specific needs.
A 2021 international survey of 237 detransitioners found the support available to detransitioners to meet their medical needs is currently inadequate.
49% seek accurate information on stopping or changing hormonal treatment.
24% require assistance for complications from surgeries or hormonal treatments.
15% need information on and access to reversal surgeries or procedures.
7% provided other responses not listed, such as the need for tests to assess current reproductive health, information on the long-term effects of cross-sex hormones, the health consequences of undergoing a full hysterectomy, and issues related to pain from chest binding.
My preliminary survey of 94 detransitioners and desisters (pending publication) revealed that 72% of those seeking medical assistance faced significant challenges, and 78% of those who sought insurance coverage for detransition services had difficulty accessing it.
I've interviewed several detransitioners who have had immense difficulty in getting insurance coverage for detransition-related needs. One male detransitioner had to wait a full year to have his breast implants removed. Others have turned to crowdfunding to finance their detransition-related procedures.
However, one detransitioner I recently spoke with had no issues in getting insurance coverage for breast reconstruction surgery, which I believe is due to a growing awareness of detransitioners' needs in the last year.
-
Activist-journalism
In the last decade, influential activist organizations, including HRC, GLAAD, ACLU, and SPLC, have collaborated closely to shape the narrative on transgender issues. They provide news outlets with a range of media reference guides, stylebooks, fact sheets, and other resources, equipping mainstream journalists—most of whom are not well-informed on the debate surrounding youth medical transition—with the materials needed to present a biased perspective and label any valid concerns as bigotry. This approach effectively transforms journalists into activists.
Activists rely on propaganda tactics like the illusory truth effect—the tendency for people to believe things that are false after repeated exposure. This strategy of creating a semblance of public agreement benefits from the support of progressive platforms like the Arizona Mirror, which claims to be “an independent, nonprofit news organization” yet serves as an example of political activism masquerading as journalism. Their reporting standards neglect objectivity and thorough research, delivering a skewed narrative that deceives the public.
It seems ironic that progressives who champion “healthcare for all” would try to undermine bills aimed at ensuring a vulnerable group has access to healthcare. And like Pamela Paul pointed out in her recent New York Times op-ed, “These are people who were once the trans-identified kids that so many organizations say they’re trying to protect.”
Activist organizations frequently ignore or downplay the experiences of individuals who have detransitioned, despite these being the same individuals they pledge to support. This neglect is a significant departure from their stated principles. For many, a transgender identity is not a lifelong experience — they need support too.
-
Additional reading:
Misleading Claim #4: Detransition is rare
Gomez states that people who detransition "represent an extreme minority of the transgender experience." To support this statement, she cites the U.S. Transgender Survey of 2015, which is a deeply flawed sample consisting primarily of older adults who transitioned under a medical model vastly different from the current gender-affirmation model concerning youth and young adults.
The study included only those who identified as transgender at the time they took the survey, which, by definition, excludes detransitioners. Gomez overlooks more recent, robust, and representative studies that challenge the notion that detransition is rare, such as a 2022 comprehensive review of medical records that found 30% of teens and young adults discontinued cross-sex hormones after 4 years.
A 2021 study found that 75% of detransitioners did not inform their doctors about their decision to detransition. The rate of detransition remains unknown and is difficult to track, partly due to the absence of specific medical billing codes for detransition procedures.
-
Misleading Claim #5: Youth medical transition is backed by major medical organizations
Gomez relies on an appeal to authority fallacy by stating that puberty blockers and cross-sex hormones for minors are “backed by major medical associations as safe and necessary for the well-being of transgender people.” But these US-based medical organizations are not basing their recommendations on the best available evidence.
Systematic evidence reviews—widely recognized as the gold standard in evidence-based medicine (EBM)—have found that the risks of youth medical transition outweigh any purported benefits.
Public health agencies in Finland, Sweden, England, Denmark and soon Norway have aligned their guidelines with systematic evidence reviews, and have adopted a far more restrictive and cautious approach, one that prioritizes psychotherapy.
Medical authorities in several other countries including France, Ireland, Italy, the Netherlands, Australia, and New Zealand, have begun expressing concerns or are in the process of reevaluating their stance on transitioning minors.
US-based medical organizations in favor of youth medical transition have not aligned their guidelines with systematic evidence reviews, actively resisting such calls for many years. However, just last year, the American Academy of Pediatrics (AAP) finally announced it will be conducting its own systematic evidence review.
The unfortunate reality is that a small, ideologically-motivated group of individuals in charge of US-based medical organizations are acting as political entities that represent specific interest groups and invest heavily in lobbying.
Last year, international experts publicly weighed in on the American debate over "gender-affirming care" for the first time. 21 leading experts on pediatric gender medicine from eight countries wrote a letter expressing disagreement with US-based medical organizations over the treatment of gender dysphoria in youth, urging them to align their recommendations with unbiased evidence “rather than exaggerating the benefits and minimizing the risks.”
Dr. Gordon Guyatt, a clinical epidemiologist at McMaster University and founder of the evidence-based medicine (EBM) movement, who is a highly respected figure in the field of medical research methods and evidence evaluation, has stated that the current guidelines in the US for managing gender dysphoria in adolescents are "untrustworthy" and should not be considered evidence-based.
Guyatt adds that the guidelines fail to offer cautious and conditional recommendations appropriate for the low-quality evidence, highlighting that European policies are ”much more aligned with the evidence than are the Americans.”
-
Misleading Claim #6: Bills aimed at safeguarding youth and vulnerable adults are “anti trans”
Gomez refers to detransitioner Chloe Cole, who transitioned as a minor and spoke in favor of SB 1511, as “a frequent supporter of anti trans legislation.”
Activists and activist-journalists rely heavily on the label “anti-trans,” a strategy referred to as poisoning the well. By branding anyone or anything critical of youth medical transition as motivated by bigotry, they skew the audience’s perception, making them less receptive to other viewpoints.
Legislation aimed at protecting youth (and sometimes vulnerable young adults with psychiatric comorbidities) from a reckless model of care is not “anti-trans,” it is pro-safeguarding. Gender activists have spent years lobbying to remove these protective measures, which they call “gatekeeping.”
Many states that have placed restrictions on medical transition services have not included provisions for detransition or gender-reversal procedures, which is why some are doing so now. Earlier this month, the Tennessee House filed a bill requiring gender clinics to perform detransition procedures.
Do No Harm, an organization dedicated to scientific integrity and ethics in medicine, introduced model legislation last year called the Detransitioner Bill of Rights, which has already been used in several states.
-
Misleading Claim #7: Republicans are the sole proponents of age restrictions on medical transition services
Throughout the article, Gomez repeatedly identifies Republican lawmakers as proponents of "anti-trans legislation," stating, "far-right politicians have latched onto detransitioners to justify their calls to curtail gender-affirming care."
This perspective overlooks the broader context and the international consensus among European countries, arguably more progressive than the United States, that have drastically scaled back on youth medical transition. It also ignores the bipartisan support that opposition to youth transition policies is now receiving in the United States, as groups of Democrats in four states (Louisiana, Maine, New Hampshire, and Texas) have voted against them.
There's also a new organization called Democrats for an Informed Approach to Gender (DIAG), which seeks to organize initiatives for left-leaning individuals that oppose youth transition. Additionally, organizations like Genspect, the Society for Evidence-Based Gender Medicine (SEGM), the LGBT Courage Coalition, the Gender Dysphoria Alliance, and others are non-partisan but primarily consist of healthcare professionals and researchers who identify as liberal or left-leaning, or at least did at some point in time.
Age restrictions on youth medical transition reflect broader public opinion across the political spectrum. A 2023 Washington Post-KFF poll found a majority of adults (nearly 7 out of 10) oppose allowing children aged 10 to 14 access to puberty-blocking drugs, and a similar majority (6 out of 10) opposes cross-sex hormones for 15- to 17-year-olds.
It's regrettable that legislative intervention has become necessary, but as medical organizations continue to let ideologues dictate policies and silence more moderate voices within the profession, lawmakers are left with little choice but to step in.
==
If you haven't already spotted the moral-religious overtones in this ideology, I don't know what more to show you.
The people who insist that "Gender Affirming Treatment" is "healthcare" and "not about you, it's about us and our survival," also want you to believe that care for detransitioners is all about them and attacking them. The narcissism and sociopathy are completely off the charts.
What they're actually afraid of is the scale of this medical scandal. At present, there's no insurance coverage, no billing codes, and limited doctor accountability, which will change as lawsuits proceed. Activists can claim that detransition is "rare" because the medical system doesn't track it. Detransitioners frequently do not return to the same doctor-activist who drugged or carved them up in the first place and are forced to simply "make do." Legal coverage of detransition isn't just a recognition of the phenomenon of detransition and the flaws of simply "affirming" everyone but will also reveal in fine grain detail the extent of it, in a way activists will be unable to continue lie about.
Meanwhile...
#Christina Buttons#detrans#detransition#gender ideology#gender identity ideology#queer theory#medical corruption#medical malpractice#medical scandal#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#religion is a mental illness
11 notes
·
View notes
Text
Profitable Medical billing company in New Jersey USA | MedICD
MedICD is a leading Medical billing company in New Jersey USA, providing highly cost-effective and profitable billing services. Specializing in revenue cycle management, we offer affordable solutions across the entire RCM process, from Eligibility Verification to Denial Management. Choose us for flexible, budget-friendly billing plans tailored to your practice's needs.
#medical billing company in florida#medical billing company in new york#Medical billing company in New Jersey#Medical coding audit checklist#Medical billing company in Florida#Medical billing company in Texas#Medical billing company in New York#Medical billing company in California#Medical billing company in Georgia#Medical billing company in Arizona#Medical insurance credentialing company in New York#Medical insurance credentialing company in New Jersey#Medical insurance credentialing company in Florida#Medical insurance credentialing company in Texas#Medical insurance credentialing company in California#Medical insurance credentialing company in Georgia#Medical insurance credentialing company in Arizona
0 notes
Text
New York Moment
Premise: Max and Sienna get cast as extras on a movie set, and funny antics soon follow.
Book: Open Heart (post series) Pairing: Sienna Trinh x Max Valentine (M!OC) Rating/Category: Teen. Fluff. Words: 1,425
A/N: This fic was requested by @trappedinfanfiction from @creativepromptsforwriting Meet Cute list (prompt 15). Tagging for reblog to @creativepromptfills. I'm using @choicesflashfics week 29, prompt 3 (in bold). Submission for @aprilchallenge prompt "dance"

The streets of Manhattan were teeming under the steaming summer sunshine. Native New Yorkers walked determinedly about their business, and tourists ambled on sidewalks, smartphones in hand, ready to capture their New York moment.
Cars honked, buses wheezed, and people yelled. It was noisy and exciting, annoying and fascinating. It was New York.
Sienna Valentine watched the drama unfold from the relative peace of a shaded sidewalk patio in Greenwich Village, and thought, “I’ve missed this.”
She’d attended medical school at Columbia, and this city had been home for four years. She had so many memories here. Studying in Central Park on a warm spring day. Taking the A Train downtown for a night out with her friends. Ice skating at Rockefeller Center.
Sienna had enjoyed her life in Boston and loved living in DC now. But whenever her husband Max needed to visit New York for work or family, she tagged along if her work schedule allowed.
Luckily for Sienna, Max had no issues making non-work trips either. An overnight trip to watch a Broadway show, a quick day trip to go shopping in Midtown or a romantic weekend getaway.
Life with Max was never dull, Sienna thought dreamily, looking away from the view outside to watch him walking toward her.
“Sorry about that. The guy just wouldn’t stop talking,” Max said, sliding into the chair across from her. He started to reach for his wine glass but suddenly stopped. “Why are you looking at me like that?”
“Like what?”
“Like you want to drag me to the nearest restroom and have your wicked way with me,” he grinned lasciviously.
“I’d rather wait until we get back to our hotel,” she countered with a wink and a smile. “And then I’ll have my wicked way with you. So you might want to load up on carbs.”
“Good plan,” he chuckled. “Check, please!”
Sienna burst into laughter. Definitely not boring, she thought again.
They finished their lunch, talking and just enjoying each other’s company, lingering over their wine. While Max settled the bill, Sienna quickly called their nanny.
“Noah okay?” Max asked, clasping her hand in his as they left the restaurant.
“Yes. Mrs. Banks said he was still asleep and to take our time.”
They started walking east toward Washington Square Park for an open-air concert, passing leafy residential streets lined with brownstones and avoiding the crowds on Bleeker Street by cutting through Cornelia Street.
They were two blocks from the park when they saw steel barricades and a clump of trailers and trucks lined up along one street. Security guards held back crowds as a film crew set up for a shoot outside the park; light stands, cameras and film equipment were everywhere.
“Now what?” Sienna said, disappointed at having their afternoon plans disrupted. It would take time to go around the barricades and crowds.
She turned toward Max, but he was standing a few feet away, reading an information notice taped to the side of a tree trunk.
“Hey, Si? Wanna be an extra in a Hollywood movie?”
When Sienna glanced at him in confusion, he grabbed her hand and pulled her to his side, pointing at the sign.
Intrigued, Sienna read the words block printed on bright yellow paper. “Extras wanted. Couples only. Report to Production Office.”
“Well?” Max smiled, a hint of adventure in his eyes. “It can be our New York Moment.”
“I thought our New York Moment was that extravagant proposal on The Highline?”
“Who says you can only have one?” he challenged, arching his eyebrow.
Intrigued by the idea, Sienna found herself nodding, her apprehension about being on camera carried away by Max’s enthusiasm.
They were outside the production office a short while later, standing in a queue with other couples. A production assistant collected their details and directed them to a trailer for a wardrobe check. That done, they joined the others in a closed-off waiting area near a fountain.
“What kind of movie do you think this is?” Sienna said, craning to see if she could spot any stars.
“Definitely not a porno, given the location,” Max teased, his lips quirked in a half-smile. “I was really looking forward to seeing you in a leather catsuit.”
Sienna snorted. “I don’t have time for your prurient fantasies, Valentine.”
“You say fantasy, I say, meet me at midnight.”
Max took her hand and twirled her into an impromptu dance, their hips swaying to the jaunty tune drifting from a street musician behind the barricade. He tightened his grip on her hand; his other hand splayed across her lower back.
Well used to their rhythm, Sienna readied herself for the backward dip, confident he wouldn’t let her fall. Suddenly, Max tugged at her, and she tripped over her feet, falling against him.
Sienna giggled at her clumsiness, but his smug look and hands cupping her ass made her think it was on purpose.
She locked her hands behind his neck and leaned in, kissing the open space at the base of his throat where he'd left the buttons of his shirt collar undone. She felt his breath hitch before he pulled back slightly. But she wasn’t done.
Sienna stretched on her toes and drew his head down to place her lips against his ear.
“Are you trying to seduce me in public?” she whispered.
He chuckled. “What a thing to say? I’m just rehearsing. For all you know, my character is a suave international spy trying to throw the assassins off his scent by dancing with a beautiful stranger in the park.”
She scoffed. “We’ve both seen that movie, and it usually ends with the spy seducing the woman before jumping out the window.”
“Maybe in this movie, the beautiful woman is the seductress,” he said, amused. “And hopefully she has handcuffs so the spy can’t escape her bed.”
He said the last in such a deadpan manner that Sienna burst into laughter. She laughed so hard she had to wrap her arms around her stomach and gasp for air.
The production assistant walked over, still talking into a headset, clipboard in hand.
“All right, folks. Thanks for your patience,” he said hurriedly. “The AD’s just finishing setting up the shot, and then we’ll escort you to the set. Just some house rules….”
Sienna tried to school her face to pretend interest and attention. It didn’t help that Max moved behind her, wrapped his arms around her waist, and leaned down to speak in her ear, cracking jokes.
“Don’t feed the pigeons? Why would we do that?” Max murmured, deliberately twisting the production assistant’s words about not disturbing the actors.
Sienna covered her mouth with one hand so people couldn’t see her laughing, but there was no hiding the tears spiking her eyelashes.
“Wait? I thought this was a family feature. Why would we be dancing naked in the square with a clown?”
Sienna guffawed, and the production assistant stopped to stare at her. Embarrassed, she pretended to cough and waved a hand in apology. The man continued his instructions, squinting suspiciously at her.
She could feel Max’s body shaking in mirth behind her. As soon as the coast was clear, Sienna slapped the arm around her waist and hissed in annoyance.
“Are you trying to get us kicked off the movie? And you know he didn’t say anything about naked dancing. The extras are supposed to be couples dancing in the park to a summer concert.”
She shivered as Max kissed the sensitive spot behind her ear.
“Tomayto, tomahto,” he said, voice smug. “Want to go back to our hotel for naked dancing?”
Before Sienna could tell him to behave himself, the production assistant announced it was time to head out.
They took their places on discretely placed x-marked spots on the floor. After listening attentively to the director’s instructions, they turned to face each other.
The more it dragged on, the technicians adjusting lighting and whatnot around her, the more nervous Sienna became.
Max placed her hand on his shoulder and put his arm at her waist, ready to swing her into an impromptu dance on a beautiful sunny day. The setup was so similar to what they’d been doing in the waiting area earlier that Sienna’s nerves vanished.
“It’s a good thing we rehearsed earlier,” Max said, a winsome smile hovering on his lips, reading her thoughts perfectly.
Sienna kissed his jaw. “Don’t worry. If you mess up, we can keep practicing back in our hotel. Clothing optional. One more New York Moment.”
“And cut!”
Bonus


------------------
All Fics & Edits: @annfg8 @bluebelle08 @coffeeheartaddict2 @crazy-loca-blog @doriopenheart @genevievemd @headoverheelsforramsey @lucy-268 @jamespotterthefirst @jerzwriter @lady-calypso @mainstreetreader @peonierose @potionsprefect @queencarb @quixoticdreamer16 @rookiemartin @socalwriterbee @takemyopenheart @tessa-liam @trappedinfanfiction
Submissions: @choicesficwriterscreations @openheartfanfics
Max & Sienna only: @aallotarenunelma @storyofmychoices @kyra75
#open heart#open heart choices#choices open heart#open heart fanfics#sienna trinh#open heart fanfiction#choices fanfics#choices fanfiction#choices fic writers creations#cfwc fics of the week#short story#writers on tumblr#sienna trinh x oc#sienna trinh x max valentine
37 notes
·
View notes
Text
Ninjago #1: Ninjago's Potrayal In Webseries
I've actually deliberated over this for a while. Since in the webseries, instead of people sized Lego people, all the characters would be portrayed as human (both because that's always how I've seen them in my head and maybe hopefully Lego Team would consider the change different enough where they won't try and DMCA me) and I was putting Ninjago in the real world instead of its own realm as its portrayed in canon (again, to hopefully dissuade Lego Team from wanting to sue the brakes off my ass and also just because I think it'd be interesting), I thought of just portraying Ninjago City. But well, I've always been a sucker for fantasy, especially urban fantasy. This also gives me a great excuse to learn more about Asia's mythology and how all the different regions and the countries in those regions interpret it! So yay, silver linings!
So, in the webseries, Ninjago would be its own country. I recently got into Ace Attorney (I have the Phoenix Wright trilogy on my Switch and i'm on Bridge to Turnabout) and while looking over the TVTropes page (I do that for all the media i'm into) and watching YouTube videos about Ace Attorney, learned all about the localizations and Japanifornia. So, that's what i'm basing Ninjago off of, which makes sense since, in canon, Ninjago also has western inspiration in addition to the Japanese inspiration. Which brings me to the first fun fact I learned while researching Japan (since Ninjago has a lot of japanese inspiration), I learned that Japan has free healthcare! Well, mostly free, they have to pay 30% of their medical bills themselves, but hey, considering that I live in a capitalist hell state, I'll take it! Also, according to the websites I've looked at for more information, the insurance is provided by the state.
(I now lowkey wonder what kind of insurance the ninja have. It can't be SHI because that's for everyone that's employed full-time by a large or medium company. And last time I checked, none of the ninja work for a medium or large company. Unless Cyrus Borg has them on his payroll and just lies to the government every year that he employs the ninja).
I really loved the realm merge in Dragons Rising and the fact that there were all these different.... races? Species? now in Ninjago because of it and how they had a whole place where all these different cultures could gather and hang out and sell wares and food and clothes and stuff from their home realms and they have contests and events and I just.... I really loved it. Like LOVED it. I just love when they have blended societies in media. Which brings me right back to my love of urban fantasy. I love love LOVE Rise of the Teenage Mutant Ninja Turtles and the whole mystical yokai city under New York they had in the show and how there were hidden hangout places for the yokai up in New York. So, taking elements from ROTTNMT and Dragons Rising, instead of a realm merge, Yokai have been part of Ninjago's history from the start and by modern day have completely integrated into regular society. So, there's shops run by yokai that sell all kinds of mystic stuff as well as restaurants that sell yokai cuisine. Also, dragons have also been part of Ninjago's history since the start and yes, it's pretty much like how Berk from the How To Train Your Dragon Franchise would have been if it was set in the modern day instead of viking times.
There's so much more I want to talk about: how machines and AI like Zane and P.I.X.A.L are viewed, Yokai shops and cuisine, what daily life is like in Ninjago City (Ninjago in general) with dragons flying around, passing through or even just setting up roost there, the Yokai that live in Ninjago and Ninjago City, the gangs that have sprung up over the years (since the webseries would focus on the Ninja's children), how the Serpentine are doing, ect, but this post is already quite long so I'll have to talk about these things in separate posts.
Since I think I've covered all the basics of how I would portray Ninjago in my hypothetical webseries, i'm going to end this post here and share future thoughts I have on Ninjago's portrayal in said hypothetical webseries in future posts. I hope you all enjoyed this post!
5 notes
·
View notes
Note
I don’t know if this has been asked (and I have been meaning to ask) but what does the Turtles, April, Cassandra, Jayden, and everyone else occupation/jobs in SIL? I mean, you gotta have money to pay all the bills and pizzas, right?
Ah! Not a bad question, I did answer this but I can't find it so I'll TLDR it.
Leo: Stay at home dad/At home medical doctor doing diagnosis and paperwork from the med-bay.
Jayden: Part Time Librarian until Lou's birth(really took a toll on them), becomes stay at home parent
Donnie: Sells his tech and runs an at home business. (makes the most money)
Raph: Works in the Mystic Library's kiddy room
Mikey: Professional art therapist
Aiden: Works with his dad's stocks ferm in the Hidden City
April: Freelance reporter for both New York papers and Mystic City papers
Casandra: Runs the Granny Cookie company, especially more behinds the scenes.
3 notes
·
View notes
Text
Hello it's been 7 years on this website and I come with raccoon paws scratching at your window pane.
TLDR: I'm supporting 3- 6 humans, a mortgage, inflated electric bills, student loans, basic needs, and working as the sole provider and now I cannot afford my medicine that prevents my migraines. If you want cheap art I am here hi just remember I'm colorblind so colors won't be perfect.
I take many medications for my migraine condition. I take a daily preventative, an abortive when I have a migraine, and then I have a monthly preventative that is an injectable. I need all of these to get me down to 6 or 8 migraines a month. If it rains I have more but this is with medication. If I do not have one of these medications I have migraines daily and if I encounter a trigger like not getting enough sleep, the weather changing, smoking, etc I'll get knocked out.
Unfortunately I have brainstem migraines which impacts my speech and ability to move in my environment. I continue to work through my migraines because I have literally no choice. I basically look and sound drunk it's horribly embarrassing.
This impacts my ability to drive too. If it strikes at work I need to uber home because my coworkers won't drive me home and no one else has a license.
If I miss one dose of any of my medications it sets off a migraine conga line qs I like to call it and I begin having migraines every 2- 3days and the longer I am off it the more migraines I steadily have.
It's hell.
My migraine medication is 208$. I am currently the only working adult for a household of three and there will soon be three children here for the summer.
Unfortunately I had serotonin syndrome a few weeks ago as some of you know and that had me out of work for a week and a half. Meaning I lost a week and a half pay check. Which may not seem like much but we live in constant poverty and are food insecure.
Literally every dollar counts in our precarious position.
The electricity company in western New York is super charging its customers so a regular electric bill for a house using less electric than average is 300- 500$ a month. Which is just a little less than our mortgage
We currently owe over a 1,000 in back pay, there isn't any relief for individuals who cannot pay the inflated rates. It's totally crazy but I need my medication. I can call the electric company and beg but I can't beg for my medicine.
My field also experiences a drop in attendence in the summer and due to my health my boss I'd trying to reduce my hours to help my body recover. That's great and all but it doesn't help me get the money I need for my injection.
My student loans are 875$ a month and I'm on the lowest payment plan and the government just sold my loans to a private company so I will be paying additional loans soon.
As you can see I have a lot on my plate but I just need that migraine medicine so I can work through it. I do a lot of passive income through survey junkies but I can't do those activities when I'm migraining.
All the images below are works in progress
Basic pencil and ink illustration
Comic book pages 15- 30 depending on content and number of pages.
if you want a comic badly and feel OK with my abilities we can work on a manageable and low price to make multiple pages happen. So bulk pages will be cheaper.

Comic book featured custom outlets??? Just resin customized outlet covers???
Can do
Painting I mean I'm trying it but if you'd like one hmu man
I tinker around with a lot of stuff
I also like to find old toys/statues and remake them so if youre interested in my raccoon art that stuff is up for new homes that will appreciate their unique beauty and love them for who they are.






Thanks for your attention and happy scrolling!!
11 notes
·
View notes
Text
"Sixty percent of insured adults surveyed did not know they had a legal right to appeal."
— Reed Abelson, The New York Times
So what are your Appeal Rights?
When your insurance makes an adverse benefit determination, you have the legal right to appeal that decision. An adverse benefit determination includes denials and any instance where the payment made is less than the amount requested (DOL, C-12). If you think your insurance should have paid more than they did for any reason, you can appeal!
You can also designate a representative to appeal on your behalf, such as your doctor's office. Sometimes this is part of the paperwork you fill out as a new patient, or you may have to fill out a specific form required by your insurance company. These forms typically acknowledge you are aware that a claim is being appealed on your behalf and consent to this use of your appeal rights.
What constitutes an appeal?
Think of your appeal as an argument for why your claim should be paid. To dispute how the insurance processed a charge you will need to identify the claim in question, request that it be reconsidered, and provide supporting documentation, such as chart notes.
Timing
For post-service claims, the insurance company is required to notify you within 30 days of a claim processing if they deny any charges. They are also required to provide you an Explanation of Benefits (EOB) for all claims processed, so the EOB generally doubles as the notification of a denial.
Next you have 180 days to appeal, often counted from the date the claim was processed. I know appealing can be overwhelming, but it's important not to delay, as it may take time to gather supporting documentation. Your appeal can be denied if it is not submitted in time.
After receiving your appeal, the insurance company has 30-60 days to review and respond to it, letting you know whether the denial has been upheld or overturned. An upheld decision means they denied your appeal, while overturning means they approved your appeal and will reprocess the claim.
The timeline for pre-service claims (also known as precertification or prior authorization) can vary depending on the urgency of the service.
What happens if your appeal is denied?
While it's a frustrating situation, don't immediately give up if your appeal is denied!
First-level appeals are reviewed internally by the insurance company. If they agree with their original decision/denial, they should substantiate why the denial is correct. Because the way the legal documents defining your benefits are written can be confusing, this explanation should lend some clarity to why your claim was originally processed as it was. This can inform the next steps you take.
If your insurance plan offers a second-level appeal, they are required to have a different reviewer handle the second appeal (DOL, D-3). Typically you are required to submit this second-level appeal within 60 days from the adverse determination on the first appeal, although this timeframe can vary, so double check!
You also have the right to an external review. In my experience working with employer-based plans, these were always handled by Independent Review Organizations or IROs, but they can also be handled by the Department of Health and Human Services according to Healthcare.gov.
Personal experience & Conclusion
Once, I was diagnosed with a severe vitamin B12 deficiency, and the doctor recommended getting B12 injections in office to get my levels up quickly. Later, my claims were denied. The reason for the denial was that B12 supplements can be purchased over the counter, and over the counter supplies are an exclusion of my medical plan. As soon as I saw the denial on my EOB, I started working on an appeal, and let my doctor's office know that I would be waiting to pay the bill until I knew the results of the appeal process.
In my appeal, I argued that since injectable B12 cannot be purchased OTC the claim should be covered, and as supplemental documentation I provided the chart notes where my doctor noted that injections were recommended over supplements due to the severity of my anemia. My appeal was approved and my claims were reprocessed.
I share my experience to hopefully illustrate some parts of the appeal process discussed above. I luckily understood why my claim was denied and therefore how best to appeal it from my job experience. I knew what I needed to do because I had helped so many people through the process before. Call your insurance company. The person on the other line knows how complicated the system is and are there to help you navigate it. They won't be able to promise any outcomes, but if they've learned something helpful from similar past situations, they'll share it.
1 note
·
View note