#like more consistent clusters than mental illnesses
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was created by web developers David Karp and Marco Arment.
Note
how did youknow youbhad bpd? what were the main "symptoms" ?? soryif it comes off as personal or uncomfy you dont hsveto answer
(im rlly rlly rlly autistic abt bpd PREPARE 4 AN ENTIRE BIBLE ABT HOW I DISCOVERED I HAD IT)
ive exhibited symptoms of bpd my entire life (it usually starts 2 present in childhood or early adulthood, it comes from childhood abuse/neglect) i only started 2 notice something was wrong in my tweens/early teens, when malachi became my favorite person and every1 was calling me mentally ill and weird and obsessive. ive known my entire life i was neurodivergent (first started therapy at 6 or 7, diagnosed with bipolar + autism + adhd + depression + anxiety RLLY early on) but there was something else that felt wrong 2 me. at that age i didnt rlly know what 2 search 4 or who 2 talk 2, so i just went on google and searched "love disorders" and obsessive love disorder came up (which isnt even in the DSM iirc) and i posted on google plus saying i likely had that and was shot down IMMEDIATELY 4 "self diagnosing" so i didnt revisit it again until a few years later.
after my breakup in 2021 i felt like it hurt WAY MORE than was normal. i stumbled across a video abt bpd during that time period and it resonated with me way 2 much. im impulsive, i have angry outbursts, im constantly suicidal, i self harm, i have extreme mood swings, i dont know who i am and ive always just mirrored other ppl, i dissociate, i have black and white thinking, i view ppl as all good or all bad and i split, i have consistently unstable relationships, i get attached 2 ppl more than i should be, and i have a paralyzing, nauseating fear of abandonment. i have every symptom in the diagnostic criteria.
i brought up the possibility of me having bpd with my mom i think (i had no one else 2 go 2 becuz all of my friends abandoned me and my parents took away my internet access) and i was shot down again, with my mom saying the CLASSIC "(insert family member) has bpd and shes crazy. ur normal. stop pretending theres something wrong with u. if u had bpd u'd be vindictive and petty and evil. do u think ur those things?"
once i figured out how 2 get my internet access back, maryland dude forced the bpd label on2 me becuz he wanted 2 explain my "abusive" behaviors (he was abusing me but tried 2 gaslight me in2 thinking i had a victim complex and that it was the other way around) and i became uncomfortable with the label becuz he made it seem like if i had bpd then i was a bad person. i continued researching the disorder becuz it still resonated with me even though i was now insecure abt it.
i became comfortable with the label again after he abandoned me, and i brought it up with my therapist. my therapist would HEAVILY DENY that i had bpd, telling me that "if u had bpd u would be attempting suicide 4 attention" "u fit the diagnostic criteria but ur autistic so all of ur symptoms can just be attributed 2 autism srry" "ive had clients with bpd and if u were like them u wouldve had an outburst in my office and be yelling at me by now" and she would even smile at me whenever i brought up my bpd becuz she thought it was funny that i thought i had it, i think. the first time i brought it up with her she told me "its rlly irresponsible 2 self diagnose after reading liek two articles online abt some extreme disorder becuz u think ur broken. ur not broken. dont self diagnose with bpd" and i had to EXPLAIN 2 HER that i wasnt self diagnosing and that id researched it in depth 4 years actually and that she was making assumptions. horribly ableist towards ppl with cluster b disorders, this is a MASSIVE RED FLAG but i didnt switch therapists becuz i was still living with my parents at this point and i felt out of control in every aspect of my life 4 this reason, i didnt even see switching therapists as an option.
then in 2023, while i was homeless, i got evaulated by a psychiatrist. i discussed my bpd with him and finally got diagnosed. i told my therapist i was diagnosed with bpd and she said something like "well im not always gonna be able 2 catch everything" BUT I WAS TELLING U ABT MY BPD 4 MONTHS!!!!! so glad i dont have that therapist anymore but now i dont have one at all, so liek.. hrmmm >:c
im gonna end this by saying.. self diagnosis is valid!!! its so hard 2 get a bpd diagnosis becuz its so demonized and stigmatized, that even those in the mental health system r ableist towards the disorder and those who have it. diagnosis is not always an option with disorders like bpd, and thats so frustrating. its so hard 2 find help becuz every1 thinks ur crazy. but ur not crazy!!! i love all my fellow bpders, i know how agonizing and it is 2 live this tormented life. if u suspect u have bpd, the bpd community welcomes u and supports u!!! and i do 2 :3
140 notes
·
View notes
Text
some of the discourse I've seen on lottie (teen timeline specifically) in the fandom (on the clock app) with people's perceptions of her definitely comes from the lack of understanding and empathy when it comes to psychosis, complex trauma, schizophrenia and cluster b disorders in general. it is also sigh inducing because it is that typical response in media to mystify and vilify personality disorders — especially when delusions and paranoia is involved. so, it's understandable why people automatically see her like a villain due to previous interpretations and one dimensional associations with them being "crazy = evil" characters in media.
(also why are we placing moral views onto the yellowjackets girls when they don't even know what morals to follow either in their little self made society — they literally decide what to do with playing cards).
she's not a villain, she's not evil. they just don't understand her.
heck her biggest fatal flaw is her love. her constant need for validation, acceptance and acknowledgement. she is scared of abandonment, her loneliness being a core character trait and insecurity of hers that follows her everywhere from the narrative to visual composition.
she's a product of her environment. constantly self harms and is unknowingly self destructive. she's literally an isolated, neglected, abused, traumatised, insecure, depressed, unmedicated kid in the worst situation of her life. but, that's still better than being at home constantly having those stressors to fit into what society deems as normal, but never being able to reach what the concept of normal is due to the labelling and stigmatisation surrounding her (people also seem to forget that this is the 90s too. mental health support for complex disorders like this was barely existent. her keeping her diagnosis a secret is understandable).
I have seen people say she "switches up too much"... her "switching up" is actually a part of her fragmented sense of identity, emotional dysregulation, obsessive thoughts, impulsiveness and distorted perception of her reality. she is extremely prone to triggers within her paranoia — paranoid delusions are such an intense experience to cope with and hard to challenge even if you are supported.
stress is a huge factor in her psychosis too and ends up re-triggering her in the recent episodes!
see people function through psychosis differently, but it's such a confusing and overwhelming experience. it's tragic to see that what she thinks she's doing is for everyone's best interest, for their protection and safety is in actuality doing more damage. she has good intentions, she's not inherently bad. it's just the fucked up situation they're in that's heightening all this to the extreme.
(she's not ruled by her disorder either. going through psychosis doesn't completely change your personality — she is still righteous, she is still passionate, she still sympathetic and empathetic).
there's so many layers to her.
that's why I think a lot of people were angry with how sudden she went out, how incomplete it felt. yellowjackets had all the ingredients to create a schizophrenic character that was breaking that one-dimensional model, that actually felt human and not a caricature for crazy. they had it, but dropped the ball in season 3 so badly — opting to go the "mysterious" way with her. having her be the one just consistently punished without some semblance of a rewarding moment for her character in her journey. in the end her illness did define her in a more depressing aspect than insane — she was still called crazy, still alone and was never able to get anyone to truly listen to her in her adulthood...
also! I think the same people who dislike lottie believe in the supernatural theory more than the psychological one. which again can be challenged if you understand what lottie is going through.
the seance scene for example — this can happen within episodic psychosis, people can discover established traits and skills unknown to them consciously while dissociated too. lottie already has prior knowledge in french, so she subconsciously retained more than she (and jackie) was aware of. she was already stressed and placed in a difficult paranoia inducing situation too: the thoughts of the dead man, the place being haunted, the situation being a seance and their location in the wilderness are already established negatively in her mind. all of this is able to create a scenario in her mind that could convince her she is actually possessed. this is also a first insight of how she is trying to disconnect herself from the trauma of the situation too — her schizophrenia infulencing the loss of agency within her own body. self harm while experiencing psychosis is quite common as well (but, that is something she does anyways...). the window was already established as an area of paranoia for her — it would make sense to her to attack it. 'you must spill blood', as mentioned, the connotations of death and doom surrounding the situation she is in are already in her thoughts.
but, yeah it just makes me sigh seeing some of her criticisms as a character come out of people's own lack of knowledge (and/or empathy).
#yellowjackets#lottie matthews#I will always defend lottie matthews#people trying to simplify complex characters *pretends to be shock*
20 notes
·
View notes
Note
You don’t have to respond to this because I know addressing Luna usually ends with your being harassed by lolcow, but thank you for being nice to her. I became familiar with her through lolcow and read her threads consistently up until recently when I realized how it only contributes to her wellbeing in a negative way. Someone’s struggles shouldn’t be other people’s entertainment and I’m so grossed out with myself for being part of that. You are a kind person with a good heart. I’m glad that someone is in her corner rooting for her because she deserves niceness. Luna really is talented and beautiful and I hope that side of the internet goes belly up so she can exist in peace and not under a callous microscope. I wish happiness and success for you too and really enjoy reading your writing. Again, thank you for being nice to her.
No need to thank me we actually have a handful of mutual IRL friends and I genuinely dig her art. For somebody with cluster b struggling so hard to survive if I can provide a dopamine hit with a casual compliment on a hair accessory why would I withhold that? Addiction is a mental health crisis, she’s obviously mentally ill beyond just substance dependance, and mocking her symptoms even the unflattering ones is low hanging fruit it’s laughing at a sick person for being visibly sick there’s not even any cleverness in that. Ive only chatted with her a few times I think to some degree she avoids public interaction with me to avoid lolcow attention but usually responds over dm and idk I’m rooting for the girl I relate to her a lot we just have different preference in chemicals but as a fellow jaded disabled adult who has seen no tangible rewards for the 18 years of strenuous effort I put into maintaining a high academic performance with NPD from the child prodigy treatment who feels like a failure because I was supposed to be famous right now not too disabled to participate in normal society wondering if my work will take off or I’ll die on SSI she and I were from a generation that were lied to and still awaiting payment for the work we already put in OF COURSE were unmotivated to then sign ourselves up for entry level exploitation with the people who dropped out in 9th grade as our equals there’s no reward anymore. What motivation is there to make an effort if there’s literally no reward and every promise of compensation up until this point has been lie after lie how long are we expected to do work with no reward? How long are we expected to feed dollars into a slot machine that hasn’t paid out in a decade? Of course she’s not motivated to get clean and enter the workforce for minimum wage to struggle only slightly less than she’s struggling now for a disproportionate amount of additional effort? Fuck it, I’m on her side, I’d rather rot surviving at a bare minimum level as a disabled person than push my mental capacity to the point where I’m at risk for becoming a public danger due to my symptoms for an extra streaming service and takeout twice more per month and destroy myself in the process. There’s no reward for recovering. There’s no reward for joining the “real world” in 2025. If you’re NOT rotting doing the bare minimum indulging whatever dopamine trigger you can as often as you can you’re a sucker, it isn’t 75 years ago, hard work no longer pays off and there’s no more such thing as upward mobility as a reward for making the right choices. I think a lot of them need to look at Luna to not feel like failures “I’m miserable but I’m putting in EFFORT. I’m also poor and in shot circumstances but I’m DOING THE WORK and BETTERING MYSELF. I’m not seeing any reward for it but I’m MEETING SOCIETAL EXPECTATIONS. I live on TV dinners and wake up every night to panic attacks over my finances despite working but IM NOT ON ILLEGAL DRUGS I just feel bad instead and make a martyr of myself for abstaining from pleasure like a mf catholic” because they have nothing to show for their effort other than the moral superiority they assign to expending it as a late stage capitalist cope. Also their constant comments invalidating her ED are literally dangerous and carry a heavy risk of anti recovery implication and potentially acting as a social contagion with a risk of triggering relapse, as with their display of her self injury photos as being not deep or severe enough to be serious. They’ve move passed bullying moved past harassment this is literally fucking gang stalking at this point idk how it still has not crossed some legal boundary especially given nearly every thread has at least one post that could legally be considered encouragement of suicide which is a criminal offense as was spreading and continuing to spread her paid sw content which is revenge porn aka a literal sex crime
taking a few commissions she became too sick in her addiction to honor isn’t a fantastic career move but it in no way justifies what has been done to her in response.
2 notes
·
View notes
Text
It lost popularity because disabled people dont want to bring it up but disability appropriation should be brought back as a term. That's what alot of these muds and pseudo-transabled terms are. You want to have a disorder but dont actually have it so you either pretend you have it or make up a ton of terms that basically are transabled without having to own it with stupid nonsequitors that allow you to claim enterance into our community without ever actually facing our oppression (no, someone calling a slur on the internet and your doctor clocking you for faking is not ablesit oppression.)
No, needing glasses or contacts doesn't make you "basically blind". No, your untreated unmedicated personality disorder is not a mental disability. No, your alter doesn't actually have that mental illness unless you do and you don't, that's just your assumptions about what that illness would look or feel like and has zero bearing on the reality of said illness. At this point y'all are turning the very real term of " atypical dysphoria" into a dog whistle for transid shit. It gets so misused so often and for everything that only really transids and diet rqs use it but expect people to respect you.
The mogai community has been trampling the disabled community forever then wonder why we all leave. We left cause you said you have the right to the word cripple cause the "headmate" you got off a bulid-a-headmate blog "came with a missing leg" and now you "totally understand the experiences of amputees". You have a mental illness, please seek help, it's not normal to want to be a system let alone have a physical or mental disability.
If you want one, either or both of these two things are true: 1. You do not understand the reality of disabled people and thus, believe it's just a cluster of symptoms Instead of the very real class struggles we deal with not just in public but also in private and often results in suicide due to how badly we are treated or 2. You understand the severe and terrible experiences of being disabled and still choose to pretend to have or genuinely want it and do not understand that wanting to be disabled doesn't actually make you disabled and is often a result of a desire to self harm with no outlet. Like... Not hurting yourself in the usual way but wanting to get by a car to be paralyzed is not only not a normal neutral desire but often the symptom of severe mental illness and a desire to self harm.
This is not normal and I don't even mean that in a pro-psych way, you need help. That is just one of many symptoms that can very very easily result in suicide. If you are having those desires consistently, especially if it's something thays consuming you and you think about it every single day and it's one of the few things you can focus on, especially if you want it as a result of an accident to remove personal accountability for causing that injury, that is a sign of something being very very wrong in your mind. This is not normal behavior that harms no one, this very quickly results in people maiming and abusing themselves. The mogai community is so scared of alienating people, they are trying to normalize intrusive thoughts. Yes, they are common in people with Ptsd but are very very often the symptom of a bigger problem and if you have them, get your ass in therapy. Common dosent equal normal and therefore harmless.
Im writing this in big text, Wanting to stab people or yourself or cut off body parts or desire a severe mental illness (often one that isnt invisible and is taken much more seriously than what most people actually have) is a cry for help and signs that you may become a danger to yourself and others. These are not normal and often are a symptom of a much bigger and much more serious problem. They are common and often do not result in anything but they can and are used as hallmarks showing where your head is. Therapists, professionals, use their frequency to measure mental turmoil. People with Ptsd, depression, anxiety, OCD, etc who are in healthy situations and are considered " getting better/ok" do not have these fantasies and intrusive thoughts with any or even semi-consistency.
If you are having these fantasies and desires more than twice a week, please ffs go get help. Especially if they are depressing or scaring you and are either lead or followed by self harm desires and suicidal thoughts. You are not a bad person for having intrusive thoughts and fantasies of disability or severe mental illness, they do not mean your inherently evil, violent or ableist. They do however mean that you may not be realizing how bad your self hate, depression, PTSD, etc are actually getting because these thoughts and desires, especially consistently, are your brain crying for help and considering every option it can to either cope with or escape a situation that's scaring it.
Do not listen to a 16 yr old on here saying it's totally normal to want to kys every 3 days and making flags and identities for wishing they were limbless, these are warning signs to you and others that something must change and you need to get help before the thoughts turn to fantasies and you feel the need to turn them into reality. Most people who actually hurt themselves say it was a passing thought that originally scared them, then became an obsessive fantasy then resulted in them hurting themselves and end up regretting it horribly. Please listen to them. This is not normal and we want you safe, happy and healthy and you are not safe, happy and healthy fantasizing about hurting yourself and trying to make that part of your identity. If you can't stop due to the fact disabled people are telling you they are hurting us and our community, do it for yourself.
#clover speaks#like seriously they are common not normal#and although it may seem cool suffering isnt#please dont ignore and especially dont try to own your body wanting to destroy itself#you do not need to be a completely neurotypical person presenting to be healthy but this is not that#there is a normal healthy level for those struggling with mental illness and that isnt it#please go get help#you are not alone and you are not a freak but this is a very important sign that you are not ok and you need help#this is why antipscyh and radical inclusionism and medpunk are so fuckign dangerous#do not normalize these thoughts they are not your desires and they are not an indication of your morality#but they are not normal and they are ways of your body warning you subconsciously that something is very wrong mentally#im not making this up this is what the professionals say#they know what these often are#please go get help you are not transabled you have a mental illness that is using that term and its normalcy to encourage and excuse sh#please listen to your body and get help
2 notes
·
View notes
Note
do you think jinx is good rep for bpd people? I see many saying she's accurate but I also see others call her terrible rep not bcs inaccuracy but bcs of how violent she is and how she could give a negative impression of bpd
I mean, the use of the good representation casus is usually what I have a problem with because wheat does good representation even mean. I mostly see people judge it on basis of whether the character makes the whole ass community look nonthreatening amd sympathetic which I loathe - to me, it should be judged on character construction level, is this aspect of the character consistent and written with the same attention to emotional beats, inner logic and narrative as everything else? and jinx is because her emotional landscape is key to the show as a whole and is written with the same attention to her humanity as every other character, she is not a caricature
i say this as someone who has bpd and has interacted with bpd communities so many times over the years but bpd does make you a difficult person to form relationships with, if it didn't you wouldn't have bpd khkgkj I realise that when you search bpd you will never find actual resources for people with bpd like you would with depression or anxiety but usually articles written by frustrated dudes who have beef with their crazy exes and people love to chalk everything up to cluster bs being inherently insane or sth. this is why you need to get rid off the black and white thinking that judges people on moral value like they are fictional characters because irl people who you have problems with probably have more going on than meets the eye - which doesn't absolve you of giving other people the same grace you want to be given but it means no one is just evil or not
sometimes mental illness will make you a really shitty friend or partner and recognising how those actions affect people in your life and taking responsibility for them IS part of recovery that is extremely uncomfortable but it doesn't mean its not human and shouldn't be portrayed in media just because its complicated. and sometimes a bitch chooses to remain a cunt kbjbkbj
3 notes
·
View notes
Text
¶ … psychiatric nursing practice in Australian prisons," Doyle (1999) attempts to discern what factors influence psychiatric nursing care. In particular, the researcher attempted to decide what factors may influence a nurse's ability to work effectively under straining circumstances, in this case working with challenging patients in a prison. The problem as the researcher states it is that more than 100,000 patients require treatment while living in prison and correctional institutions. The unique client group presents many challenges to nursing staff including mental illness and developmental disabilities. In addition many patients are emotionally unstable. The author clearly identifies problems associated with providing optimal health care to incarcerated offenders. Also noted are the increased mortality rate and disease rate among this population. Nurses must often face challenging situations. They are often tasked with working with difficult patients. In addition they may face technological obstacles or conflicting values when working in certain settings, or in this case stigma association working with prisoners. It is important nurses overcome these obstacles so they are able to delivery the best quality care to patients regardless of their situation. Study Purpose The purpose of the study is to discern what challenges psychiatric nurses face and what factors may influence the quality of care they bestow on patients in a sub-optimal working environment. The aim of the researcher is to point out the obstacles nurses face in delivery high quality care to patients under trying conditions. Whether nurses work in a psychiatric institute or other institution, they are likely to face similar obstacles. The researcher clearly states the purpose. The author intends to "study issues of concern to nurses delivering mental health care to offenders." Research Question While the research question is not directly stated, the researcher does state his intent to study issues that concern nurse's delivery care to criminal offenders. The question allows adequate exploration from a qualitative perspective. The intent of the research is to study a phenomena, especially through observation, which is supported through qualitative research. Study Design The researcher suggests use of a praxis qualitative research approach, supported by other researchers (Lather, 1991). This type of research is also called applied research. The research design included a focus group of 10 mental health nurses who were interviewed regarding their concerns with patients. This method is supported by other qualitative studies that suggest focus groups and in depth interviews are appropriate (Street & Walsh, 1996; Massarik, 1981). The researcher also elected to use open-ended questioning. The method is appropriate because it is aligned with qualitative investigation. The questionnaire and interview approach allow the researcher to observe the phenomena occurring in their natural state. The study design utilized qualitative textual analysis where the researcher clustered themes of questions for nursing participants to answer. A narrative was subsequently produced describing the problems as described by the subjects interviewed. Subjects and Setting The researcher selected 30 subjects registered as psychiatric mental health nurses whose job was to deliver care to imprisoned men and women in a central industrial prison. Nurses employed for purposes of this study worked 24 hours care shift. The selection of nursing care staff is representative of the nursing population caring for this group at large, thus adequately represented the situation. The setting is appropriate as it examines nurses working in a walled and secure 120-bed prison unit. Data Collection Methods The methods used are consistent with a qualitative examination because they support use of an open-ended questionnaire. Qualitative analysis requires that the research examine a given phenomena and draw conclusions from this information. The researcher does this successfully by analyzing data using a clustered approach. The research gathers similar information to create a narrative exploring the range of problems demonstrated at the prison. The author did not comment on what instruments or disclosures were used to protect the identity of those interviewed. Interviews were taped and recorded. To protect the identity of the participants the researcher should have taken steps to assure anonymity. This may include assigning each participant a code or number to identify them for study purposes. It is possible that despite the lack of information regarding confidentiality, the researcher did take steps to assure anonymity. Data Analysis Procedures The data analysis procedures correspond to other methods adopted by qualitative researchers in the past. The data analysis procedures are consistent with a qualitative approach as the author is using applied research techniques to gather information from which to draw a narrative conclusion. The two major strengths of the study include the researchers directed approach to selecting a target population and use of open ended questions that allow the researcher to gather as much information as possible about the phenomena being investigated. The primary limitation of the study is the small sample size and single location used. It would be impossible for the researchers to generalize their information to the population at large based on this small sample. While the sample may be representative of most nursing situations where nurses work with inmates, it is difficult to assert this without additional studies. The author concludes that the environment in which psychiatric mental health nurse's work is often one dominated by surveillance, control and harsh circumstances. The author further concludes that nurses are often compromised and face resistance when attempting to implement routines and set up priorities. The conclusions are appropriate based on the interview data the researcher gathered from nurses working in the field. Because the nurses directly reported their circumstances and pressures, it is easy for the researcher to draw conclusions. The implications suggests that this research can be used to guide future training and support programs for nurses working in difficult situations. The researcher suggests that the challenges nurse's face in these situations must be acknowledge and recognized so adequate support may be offered nurses working under these conditions in the future. References: Doyle, J. (1999). "A qualitative study of factors influencing psychiatric nursing practice in Australian prisons." Perspectives in Psychiatric Care, 35(1):29 https://www.paperdue.com/customer/paper/psychiatric-nursing-practice-in-australian-67125#:~:text=Logout-,PsychiatricnursingpracticeinAustralianprisonsDoyle,-Length4pages Lather, P. (1991). Getting smart. New York: Routledge. Massarik, F. (1981). The intervening process re-examined. In P. Reason & J. Rowan (Eds.), Human enquiry: A source book of new paradigm research (pp. 201-207). New York: Wiley. Street, A., & Walsh, C. (1996). Community nursing issues in Maori mental health. Australia and New Zealand Journal of Mental Health Nursing, 5, 54-62. Read the full article
0 notes
Text
Just read up DMS-5 over BPD since all my traits™ could be just autism
I do def think my autism played a huge role on it and fortified the development of BPD, but even though there's overlap, the focus of the topics are almost unrelated.
BPD Diagnosis Criteria focuses on self image and interpersonal relationships althewhile autism is a Neurodevelopmental Disorder (aka affects basically all parts of your life but mainly learning, behavior and disability needs)
I need to preface DMS-5 doesn't believe in disorders causing others (disorders), even though a lot, and I mean, a lot of mentally ill people have expressed the origins of a disorder comes from another one they already had since childhood (I've seen this on DID, Cluster Bs, PTSD, IED and OCD communities).
Don't "um actually" me in this one this book simply does not cite any disorder or the consequences of it as a cause of another disorder aside from PTSD and drug induced symptoms (note: I did mostly read about the personality, depressive and anxiety disorders)
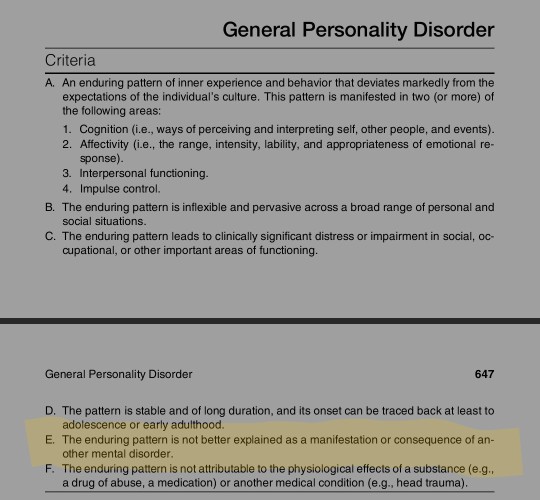
There's two sets of diagnostic criteria for BPD, the one above which is general for any personality disorder, on it, there's a clear overlap with autism.
A. An enduring pattern of inner experience and behavior that deviates markedly from the expectations of the individual’s culture. This pattern is manifested in two (or more) of the following areas: 1. Cognition (i.e., ways of perceiving and interpreting self, other people, and events). 2. Affectivity (i.e., the range, intensity, lability, and appropriateness of emotional response). 3. Interpersonal functioning. 4. Impulse control.
(...)
C. The enduring pattern leads to clinically significant distress or impairment in social, occupational, or other important areas of functioning.
(...)
Reiterating, the above is for ALL personality disorders, including cluster A and C.
Now about the diagnosis for Bordeline.
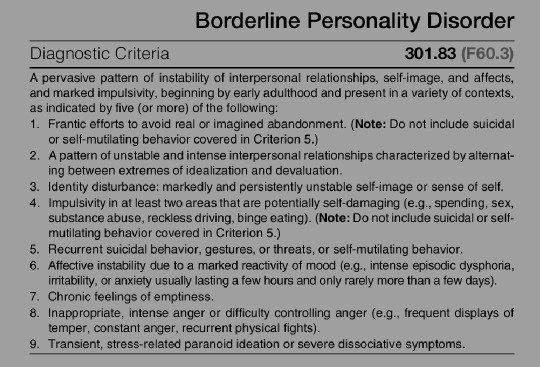
From all of them, I do identify with most besides 3.
I never experienced a lack of self Identity, I know who I am, even though sometimes my masking gets me really confused over it.
4 and 6 and 8 are the closest to autism-like the criteria ever gets. The minimum for the diagnosis is identifying with five of these.
So like, what does this mean for autistic people diagnosed with BPD or with BPD traits? It means there's overlap, after all, 'impulsivity' (the impulsivity one is a stretch bc for each it happens for different reasons) and hardship controlling feelings is real. Well, there's some options.
You either have autism AND BPD, not because of your heightened feelings and impulsivity, but because of your fear of abandonment, the lack of consistency not only on your identity (not like masking, not like DID) but also your views on your loved ones.
Or you were diagnosed by an asshole that has movies and pop psychology as their research.
Research related notes:
The idea that BPD is the worst in its first years (early adulthood) which is when my symptoms got increasingly worse.
The percentage of having a personality disorder gets higher if your parents have it (my dad is diagnosed with BPD, which is when it dawned on me about myself, we are really similar)
Diagnoses happens more on women (75%) and I don't know why that's ALL that it said about it. I don't believe in gender related mental disorders, that sounds ridiculous (although traumas and coping mechanisms will change due to ✨society✨ because I also believe that the environment makes you)
Another topic I want to discuss are symptoms that are clearly not in the diagnostic criteria.
I'm not saying they don't exist and "you have something else actually"™ there's a reason I would research the book first, on individuals second and Google third. Diagnosed people know way more how it is to live with a disorder than a professional who only studies things by other professionals who probably treated us like lab rats.
But it is notable that BPD has nothing about empathy, sympathy and all that shit, althewhile, NPD and ASPD do. Regardless of whether it was said or not, the behavior noted in the book will affect how a pwBPD empathy and sympathy works.
That's all, thanks for coming to my Ted talk, I hope y'all can accept me even tho I'm self diagnosed 🩷
#i hope this helps someone too#cccat vent#actually autistic#bpd#psychology#yes i make everything about me in some way or another im increasingly more self conscious anout it#also DMS-5 is heavily flawed and still has acephobic + kink shaming diagonosis in it
1 note
·
View note
Text
Raiden most definitely has Anti-Social Personality Disorder
— An essay by a fan who also has ASPD
Side note by author: This essay will be updated in the future (a new post will be made). Hello, my name is R and I was diagnosed with Anti-Social Personality Disorder when I was 23 years old back in 2018. I also study in the field of psychology and medicine, so I know a thing or two about mental health. In this essay I want to elaborate why I think that Raiden doesn’t just suffer from (complex) PTSD but also Anti-Social Personality Disorder and I base this interpretation on canon evidence, research I did on the mental health of former child soldiers as well as my own experience with the disorder.
In the following text Anti-Social Personality Disorder will be shortened to ASPD.
What is Anti-Social Personality Disorder?
ASPD, also known as Dissocial Personality Disorder/DSPD in the ICD, formerly known under the name Psychopathy or Sociopathy, is a Cluster B (the ‘dramatic’ type) personality disorder known under the ICD-Code F60.2 or the DSM-V Code 301.7.
The reason why I will not call ASPD Socio- or Psychopathy in this essay is that these terms have been obsolete since the introduction of the DSM-IV in 1994, the disorders have been merged into one disorder as well as the fact that the ASPD community widely regards these terms as the equivalent of a slur (If you do not have the disorder yourself, do not, under any circumstances, use these words. There are words such as ‘asshole’ that describe shitty people better than you being downright ableist in your choice of words. Note that the subreddits r/aspd and r/sociopath are overrun by illness fakers and people who refuse to get better, they do not represent people with the disorder really well).
According to the DSM-V, ASPD is described as the following:
“A. A pervasive pattern of disregard for and violation of the rights of others, occurring since age 15 years, as indicated by three (or more) of the following:
1. Failure to conform to social norms with respect to lawful behaviours, as indicated by repeatedly performing acts that are grounds for arrest,
2. Deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure,
3. Impulsivity or failure to plan ahead,
4. Irritability and aggressiveness, as indicated by repeated physical fights or assaults,
5. Reckless disregard for the safety of self or others,
6. Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behaviour or honour financial obligations,
7. Lack of remorse, as indicated by being indifferent to or rationalising having hurt, mistreated or stolen from another.
B. The individual is at least age 18.
C. There is evidence of conduct disorder with onset before age 15 years.
D. The occurrence of antisocial behaviour is not exclusively during the course of schizophrenia or bipolar disorder.”
What the diagnostic criteria of ASPD does not list is that people with the disorder often times also have low affect, which is indicated by shallow, rather fleeting, inconsistent emotionality as well as a partial or complete lack of affective (emotional) empathy. This is likely caused by chronic emotional dissociation and is irreversible.
People with ASPD are capable of feeling every emotion, but the operative here is can, not will. Often times the emotional experience is reduced to feeling content, bored, apathetic and angry or irritated. Everything else is very much background noise that can be ignored with ease. Also people with ASPD are able to use cognitive (learned) empathy, but often times this is used to manipulate. Some people with ASPD are self-aware, either through diagnosis or life experience. It is possible to have a completely normal life with this disorder and people around the person with ASPD do not notice that they have anything at all, because we are pretty much capable of faking emotions very well thanks to great observational skills. However, this does not apply to every person with ASPD.
ASPD is caused by prolonged abuse, neglect and/or trauma in (early) childhood which likely involved heavy exposure to violence. Poverty is also linked to the likelihood of someone developing it. A genetic link is being researched but has yet to be proven to be able to cause this disorder without any of the aforementioned. The so called ‘warrior gene’ theory is pretty much bullshit, as it is argued that it can only appear in people of European ethnicity. This theory is pretty much racism at its finest and therefore anti-science.
Antisocial Behaviour in former Child Soldiers
“Anti-Social and Disruptive Behaviour
PTSD is also significantly associated with negative behaviour against an individual’s own family, the expression of anger and hostility to others, and self-harm (Burton, Foy, Bwanausi, Johnson, & Moore, 1994; Deykin, 1999; Deykin & Buka, 1997; Dodge, 1993; Dutton e al., 2006; Friedman & Schnurr, 1995; Golding, 1999; Joshi & O’Donnell, 2003; Lewis, 1992; Perry & Pollard, 1998). Research shows that former child soldiers have difficulties in controlling aggressive impulses and have little skills for handling life without violence. These children show on-going aggressiveness within their families and communities, even after relocation to their home villages (Wessels, 2006). In a qualitative study, Magambo and Lett (2004) reported that former child soldiers in northern Uganda mainly applied physical violence to resolve conflicts. Although the children sympathised with victims of violence, they could not even think of non-violent alternatives, reflecting an absence of adequate social skills.
Most former child soldiers have spent several critical years of their development in captivity, under the constant threat of abuse and manipulation by their commanders.
Most probably, this period affects the development of a personal and collective identity (Kanagaratnam, Raundalen, & Asbjornson, 2005). In general, children exposed to war and child soldiering show a strong identification with their own group (Gloeckner, 2007; Jensen & Shaw, 1993), and develop a worldview dominated by political and nationalistic categories (Feshbach, 1994). In the Gloeckner (2007) study, it emerged that the longer children had stayed in abduction, the stronger was their rebel-related collective identity. But it may be that their collective identification might occur post hoc after return to their home communities. Gloeckner explained that questions and discussions of family and community members about the cruelty of the LRA’s actions may activate a process of reasoning about what had happened. Former beliefs about ‘right’ and ‘wrong’ actions might clash with current ones, and in order to regain cognitive homeostasis, identification with the rebel group is aspired. Interestingly, this study showed a positive correlation between collective identification and reactive aggression (physical and verbal aggression and anger). In addition, Gloeckner (2007) reported that formerly abducted children with PTSD might be especially vulnerable to accepting simplistic models of ‘good versus bad’ – a black and white worldview, which is a known cognitive distortion. Although a rigid political view might be protective during exposure to war events, it might facilitate violent behaviour after returning from the fighting to individuals’ home communities.
Children living in conditions of political violence and war have been described as ‘growing up too soon’ and ‘losing their childhood’ (Boothby & Knudsen, 2000; UNICEF, 2005, 2006). Levels of conscience seemed to be significantly related to the severity of PTSD symptomatology, but also with negative schematisations of self and others and lower self-efficacy ratings (Goenjian et al., 1999; Joseph, Brewin, Yule, & Williams, 1993; Saigh, Mroueh, Zimmerman, & Fairbanks, 1995).“
- The Psychological Impact of Child Soldiering (by Elisabeth Schauer and Thomas Elbert)
“Behavioral Problems
Former child soldiers exposed to brutal episodes of war-related violence face a range of behavioral problems. In addition, post-conflict factors may contribute to varying degrees of vulnerability to adverse behavioral outcomes. According to Lev Vygotsky the child’s culture and community that he lives in largely affects his development. Vygotsky believed that important learning by the child occurs through social interaction.
For a number of years child soldiers spend time with adult militants under strict rules and regulations. The children were constantly exposed to hostile situations that had negative impact on their psychosocial wellbeing. The children’s thinking pattern and cognitive schemas changed in to more aggressive and violent direction. The children were indoctrinated to perform atrocities without asking questions. They witnessed the gloomy realties of war that made drastic changes in their behavior. The children who had committed atrocities in the past have high risk of developing conduct disorders or anti-social personality disorder and addiction problems if their mental health issues are not appropriately addressed.
In Nepal, Kohrt and his team in 2008 concluded that post-conflict factors such as stigma might contribute to adverse mental health outcomes. Former child soldiers in his sample showed significantly higher symptoms of depression and PTSD compared to matched controls even after adjusting for exposure to traumatic events. In 2010 the researcher Betancourt did a prospective study to investigate psychosocial adjustment in male and female former child soldiers in Sierra Leone using 156 male and female child soldiers. Over the 2-year period of follow-up, youth who had wounded or killed others during the war demonstrated increases in hostility. It has been reported that former child soldiers in Uganda had various behavioral problems and some of them were charged with anti-social activity after their demobilization. Over 70% of prisoners in the juvenile crime unit in the Gulu District, Uganda are former child soldiers, incarcerated on charges of rape, assault and theft.
Social relationships play a key role in child’s behavior as explained by the Psychologist Urie Bronfenbrenner. Nested interacting spheres of social relationships that determine individual behavior and well-being are the fundamental components of analysis in social ecology. When these children were abducted and kept in camps, they had no way of having healthy social relationships.”
- Psychosocial Problems Of Child Soldiers (by Professor Daya Somasundaram and Dr. Ruwan M. Jayatunge)
These to excerpts from two different essays on the mental health of former child soldiers speak for themselves. ASPD is also the only personality disorder that is associated with child soldiers.
Although Raiden had been in treatment when sent to the United States, it doesn’t seem that the treatment had been appropriate enough to prevent him from developing ASPD. It’s mentioned in the Metal Gear wiki that he had at least become ‘outwardly stable’, however, we can see from how he behaves in canon that he hasn’t processed any of his trauma whatsoever. To treat PTSD or any personality disorder, appropriate trauma therapy is required. This has obviously not been the case for him, as he’s incredibly mentally unstable and violent. Even the introduction of nanomachines in his body through the Patriots hasn’t prevented any of his behavioural problems although they did successfully suppress his memories of his trauma, as we learn in MGS2.
The way Raiden shows traits of ASPD
Shallow Affect and Lack of Empathy
Albeit Raiden is portrayed as an emotional person, his emotionality often consists of anger and aggressiveness, and he doesn’t seem to be particularly empathetic either.
In fact, his lack of empathy (and how he justifies his actions to himself) is even being called out by Jetstream Sam in the 4th chapter of Metal Gear Rising. He is also shown to have no reactions to allies dying (Emma Emmerich in MGS2 and Naomi Hunter in MGS4) and is just awkwardly standing there like a cardboard cut-out. While Snake doesn’t show or say anything in these scenes either, his stance is not awkward like Raiden’s.
Raiden is also often told to calm down by various characters throughout the franchise when he is reacting to things with anger or aggression to an almost inappropriate level and he never takes it well. Neither is he good with receiving criticism, and will verbally attack the person who criticised him.
Kevin Washington also calls him creepy for how Raiden describes the cyborgs he is killing like ‘walking vending machines’.
It is also said in the script of MGS2 that Raiden in general has trouble understanding other people’s feelings.
Failure to conform to social norms
“Companies like ours — yours — bend the law as they see fit. Why not bend it when it can save innocent lives?” — Raiden to Boris in MGR
The entire game of Metal Gear Rising basically encompasses this whole part of Raiden. He is seen to be breaking the law out of an emotional urge (which Blade Wolf comments on as well after the awakening of Jack the Ripper) because seeing the children in the lab in Guadalajara being turned into cyborgs against their will triggered him. We learn that he doesn’t act like this because he is some kind of hero protecting the weak (as he is always trying to tell everyone including the player for the first half of the game), he does this out of selfish reasons — to have a reason to kill. His morality is quite grey. Sure, he is on the side of the ‘good guys’ — but his methods are cruel, the style of an anti-hero.
“Not that much of a hero after all, right?” — Raiden to Blade Wolf after killing Monsoon
He shifts his morality as he sees fit — same as the companies he is criticising. Armstrong points out their “kindred spirits” as he is dying at the end of the game as well and we as a player understand that our enemy is right. To achieve our goals, we went overboard with everything and justified our violence — Raiden’s violence — with doing the ‘right’ thing.
Manipulation and Deceitfulness
“So it was artificial on my end too. It was just a game, not the real thing.”
Raiden says this to Rose after she confesses to him that she is a Patriot spy and it almost feels like a confession. The way he says it is very callous, unlike how he talked to her before (and he reverts back to his ‘usual’ self later on anyway), it feels like a ‘mask slip’ where he says what he truly feels. I think about this scene a lot and it makes me believe that Raiden did not truly love Rose until he actually lost her (MGS4). Basically ‘not recognising what you had until you lose it’. People with ASPD often get into relationships to get something out of it – be that getting rid of boredom, money or sex – and they go very far when it comes to faking emotions such as love. It is often said that we cannot love, but this isn’t true. Love to us is more of a conscious choice of committing to someone rather than an emotion and can be very mature when it’s honest. We are also very obsessive lovers, which can turn very toxic very fast if not self-aware and controlled.
Impulsivity and the failure to plan ahead
Stabbing himself to impale Vamp without thinking through that he is going to bleed out, quitting his job at Maverick without thinking through how he is going to pay his bills in the future and the entire ordeal that is the World Marshal incident are what I can list on top of my head where Raiden acts very impulsively.
Aggressiveness, Abusive and Violent Behaviour
In MGS2, Rose mentions that Raiden ‘raised his hand against her’ when she tried to enter his room. This translates to more than just a slap in the face (and even that is horrible behaviour when you are in a relationship) if we look further into Raiden’s behaviour across all the games in which he appears. In the same game we learn that Raiden genuinely enjoys murder. He asks Snake about it, horrified about himself, if he does the same which Snake denies.
In MGS4, Rose talks to Snake about Raiden and why they aren’t together anymore. She speaks about how he became a violent alcoholic (Substance Use Disorder is highly common in people with ASPD) as he was unable to cope with his traumatic memories resurfacing. She implies that he got into regular fights as well, saying so by mentioning that he came home covered in cuts and bruises. We don’t know for sure, but it is likely that Raiden also hit Rose as well but she doesn’t outright say it. She just states that she is scared of him.
“I am worried about him, of course, but… I am also afraid of him.” — Rose about Raiden in MGS4 If you look closely at the scene in which Snake mentions Raiden’s family in MGS4, you get a quick glimpse of Raiden trying to hit Snake — only to break down and fall to his knees, crying. His willingness to physically assault people who are close to him is another one of these signs that speak for ASPD in him.
“Resolving everything with violence, is that it, Raiden?” — Sam to Raiden in MGR
“Feasting on the insides of your enemies?” — Monsoon to Raiden in MGR
Both Sam and Monsoon call out Raiden for his violence in MGR and how he justifies his actions with ‘protecting the weak’ which we learn in the same chapter, is a load of bullshit. Raiden confesses that he fights for the pain he feels — or likely, the adrenaline rushes one gets from it — when being hurt in a fight, that protecting the weak was a lie he told himself to ‘keep himself in check’ and that he thought that he could live a normal life, with his friends and family having his back. However, this didn’t work out and he found himself back on the battlefield and we finally learn why and the reasons are just as shallow as the rest of him.
Reckless disregard of the safety of self or others
Raiden’s recklessness in MGS4 could also be read as suicidal ideation, which is also something a lot but not all people with ASPD experience. Impaling himself and cutting off his own limbs are things I would consider ‘reckless disregard for the safety of self’ as he does this without thinking things through. In his fight with Vamp he definitely didn’t want to die in the end, so I suspect this to be him not thinking things through (which he does a lot, acting on impulses). The same goes for his wish to walk through the microwaves instead of Snake (and god I wish he would’ve gone instead of Snake), which Snake points out is suicidal and that he has a whole life to live still.
In MGR, Raiden decides to eradicate World Marshal, the largest PMC in the universe at the time of the game, entirely by himself. He raids its Headquarters with total disregard for his own safety or that of others, as he is just ‘lucky’ that the parts of Denver he is getting through, are blocked off from the public. Raiden doesn’t harm civilians — but he doesn’t particularly care if they die either. We know he’s lying to himself about being the good guy. Although his team is unofficially supporting him, he has no backup in case something happens.
Consistent Irresponsibility
Raiden is shown to be consistently irresponsible. He doesn’t hold himself accountable for his actions by lying to himself about his morality and basically gaslighting himself and others about his behaviour. He doesn’t listen to work instructions — Kevin calling him out in the first chapter of MGR for it — and therefore fails missions. He is also shown to constantly argue with the colonel in MGS2, always trying to get out of the situation he is being put into and not taking responsibility.
Lack of Remorse
In MGS2 we learn that Raiden enjoys murder without feeling any particular hard feelings about it. He is terrified about the realisation but doesn’t feel any particular feelings of guilt for it. Neither does he ever mention that he regrets having physically or emotionally harmed Rose in any of the games he appears in (Rose has issues too — they both definitely act like nothing bad ever happened between them at the end of MGS4 and I wish them both a nice stay in the psych ward).
Raiden’s justification to kill in MGR is to ‘protect the weak’ which later turns out to be a complete lie he tells himself and others to seem like the good guy. He’s very much gaslighting himself into believing this throughout the game until Sam and Monsoon confront him about his behaviour and hypocrisy and Raiden drops the mask and reveals his true intentions: that he fights to feel pain in battle, because he gets high on it and that he very much enjoys murder.
“Who protects the weak from the man who ‘protects the weak’?” — Monsoon to Raiden in MGR
In MGR you can also cut off the clothes of civilians you saved. If you do so, your teammates call you out for it. Raiden then does half assed apologies for it, even laughs when being called a nasty creep. He genuinely finds it funny to apparently terrify innocent civilians and doesn’t show any remorse when being called out for it.
Summary
Looking back, Raiden does show many traits of a person with Anti-Social Personality Disorder throughout all the games in which he appears. Although MGR is a lot more “in-your-face” with it, the mainline games show him having those traits very much as well (to be diagnosed one must meet 3 out of 7 listed criteria points, so even if you regard MGR as non-canon, he would still meet the criteria from what we learn from the mainline games). The fact that a lot of former child soldiers struggle with this disorder as adults adds to my theory that he has it. I often see people argue that MGR was not the direction that they would like to see Raiden go and that he is too ‘brutal’. In my opinion, MGR was the more realistic ending for him. I have ASPD and I know that white picket fence home lives just don’t work for people like us. We grow so bored, we start to fuck up shit for ‘fun’ and ruin our lives that way or get addicted to drugs. Raiden choosing the battlefield, finally accepting who he really is (‘Jack the Ripper’), is the more realistic and healthier ending for him than him just lying to himself and being on edge all the time, potentially ruining his marriage that way in the span of a year or two. Love cannot heal extreme childhood trauma, sorry guys. And Raiden seriously needs therapy.
#Raiden#Raiden mgs#Raiden mgr#mgs#mgr#metal gear solid#metal gear rising#mgrr#redrage writing#aspd#anti social personality disorder#antisocial personality disorder#solid snake#rose mgs#golden writing#golden thoughts#golden essays
181 notes
·
View notes
Text
Rules, DNI, Intro, & More!
This is a “x culture is” blog for all neurodivergent folks. So anyone with autism, ADHD, PTSD, dyspraxia, dyslexia, tourette’s, personality disorders, or any other mental illness, psychological/neurological condition, or non-neurotypical neurotype! This includes self-DX folk as well. This was inspired by all the other “x culture is” blogs out there!
This blog is run by Mod Emri (She/They), Mod Aki (He/Him), Mod Milo (they/he/it) and formally Mod Corvid (They&/Them&) and Mod Theseus (voi/voice)!! Queue is currently posting 11 times a day. Asks are always appreciated.
Submission Rules
Please keep your asks to nd culture submissions only, or at the very least being neurodivergent related!! We’d also appreciate it if you didn’t ask for advice as we’re not able to provide help in that department.
Start submissions with “neurodivergent culture is” or some variation (”autism culture is,” “dyspraxia culture is,” “PTSD culture is,” etc.) Asks will be deleted if they don’t follow this.
Keep all fandom/shipping/character talk vague. We do not know every fandom and may not feel comfortable handling specific fandom or media related submissions.
Try to keep your asks free of discourse, we want this to be as positive a place as possible! (Vagueing about your own struggles or life is fine, though.)
Please try to use tone tags if relevant!
DNI
TERFs
transmeds
MAPs/NOMAPs
all queerphobes, including a-spec exclusionists, transphobes, biphobes, panphobes, etc.
Those who believe in cluster B abuse (narcissistic/borderline/anti-social/histrionic)
discourse focused/centered blogs
blogs with minors in their DNI/NSFW blogs
supporters of Autism Speaks
We will try to tag everything appropriately, but please let us know if you want anything tagged that we have not been tagging or forgot to tag! (Things we currently try to tag for.)
If you would like to ask us any questions, please read our FAQ first! It’s underneath the cut. Any questions that have already been answered in our FAQ will be deleted and ignored.
FAQ
What’s the difference between “neurodiverse” and “neurodivergent” and why do you use the term neurodivergent instead of another term?
Despite the term “neurodivergent” seeing some use in modern clinical settings and research, it is not a medical term with a consistent set medical definition, and was not coined in a medical or scientific context. The term “neurodivergent” was coined to describe a broad and generalized community of anyone who in any way does not fit the most common or “average” neurotype. Any situation involving any sort of psychological or neurological “abnormality” or “divergence” as compared to the general population counts under this definition. As mentioned before, it is not a medical term; it is a term which serves the purpose of creating and describing a community which has historically and continuously been marginalized. The term “neurodivergent” has often been conflated with the term “neurodiverse” which is a completely different term with a completely different meaning and context. “Neurodiversity” is a term used specifically to describe ADHD, autism, and in some cases a few other conditions in a small and specific group. It was coined decades ago in the context of education, specifically, but has now seen some use to describe the general community of people with these conditions. All neurodiverse conditions fall under neurodivergence, but neurodivergence is a very broad umbrella term that includes far more than just the conditions classified under neurodiversity. The coiner of the term “neurodivergent” has themselves explained this issue in their own post, here.
We use neurodivergent for a few simple reasons, but the biggest one is that it’s accurate. We’re not just talking about neurodiverse people on this blog, even though all of us are neurodiverse. We’re also talking about everything from epilepsy to CPTSD to depression to NPD. This blog is meant to include the entire community of all neurodivergent people, which means everyone who is not completely neurotypical or of the most common/average neurotype. Though this is our primary reason, there are also others. The term “neurodivergent” was not coined to medicalize or marginalize neurodivergent people, as medical terms and diagnoses historically have. It was coined to describe and unify the broad community of all people who in some way do not fit the neurotypical standard and thus face marginalization based upon lacking that privilege. The term is inclusive and was created by an actual neurodivergent person with the actual community of neurodivergent people in mind.
Us using “neurodivergent” and specifically being a neurodivergent blog and community doesn’t stop anyone from have specific spaces for specific conditions or groups of conditions. If someone wants to make a neurodiverse-culture-is blog, we would gladly support it! We are all neurodiverse, after all. However, we are specifically a neurodivergent blog and community, which means we include all neurodivergent conditions beyond just neurodiverse ones. Broad and inclusive communities and community spaces do not stop more specific ones from existing, they just help unify oppressed people, which is good for more reasons than we can fully list.
Does (insert mental illness/condition/disorder) fall under the neurodivergent umbrella? Do I “count” as neurodivergent if I have/am (insert mental illness/condition/disorder)?
The answer, 99.9% of the time, is yes. If you are in any way, shape, or form not completely neurotypical and of the most common/average neurotype, the answer is always yes.
As discussed in the previous answer, the term “neurodivergent” is a broad community term that describes any person who in any way is not 100% of the most common and average neurotype. This means that any given mental illness or psychological condition, as well as any neurological conditions, fall under this definition. You don’t even have to have a specific label, you just have to fall outside of the average or “default” neurotype in some way. This, again, is all from the exact words of the person who coined the term neurodivergent. It is a term to describe a marginalized community, not a clinical or medical diagnosis or group of diagnoses. That is how it was coined and how it has been used, despite its somewhat significant misuse.
We’ve gotten an absurd amount of questions asking if specific conditions, or even people themselves, “count” as neurodivergent. Unfortunately, the fact that this misinformation and worry is so widespread makes a lot of sense. Not only is there a common misconception that neurodivergent and neurodiverse are synonyms, but there is an immense amount of ableism even within disabled and neurodivergent communities. We’ve gotten seemingly genuine requests before to change our entire blog to exclude people with specific conditions. The fact that some neurodivergent people face much more oppression and stigma than others has created a power imbalance within the community, and some neurodivergent people who face this oppression the most or in the most intense ways lose sight of the fact that those who face less than them still are marginalized on the same basis that they are. After all, we’re all neurodivergent. We all do not have the privilege that fully neurotypical people have. By having broad communities like these, we unite all of the people facing this same struggle and being marginalized on the same basis, even if that marginalization often looks or functions very differently. There can still be, and still are, specific communities for specific identities and experiences. Those who face specific experiences can and do have their own spaces and communities relating to those issues. A broad umbrella for all people who face a certain type of marginalization does not erase these specific, smaller communities, nor does it erase the specific struggles of those who face more marginalization than other marginalized people.
We wish we could take the time to compassionately answer each and every request, but the amount of them is huge and they are all essentially the same, with essentially the same response. You can imagine that gets very repetitive very quickly. If you’re here because you were going to ask whether something (or whether you as a person) “counts” as neurodivergent, this is your answer.
Also, consider that you are not erasing space for others by taking up space in this community. You do not cheapen the struggles of others by also having struggles, even if those struggles are less severe or serious. You still deserve space in our community. If you face any kind of ableism or experience any kind of neurodivergence, no matter how "minor” you or others may think it is, that always matters. We need more voices like yours at the table.
I have a question that wasn’t answered here, where/how can I ask it?
First of all, as respectfully as possible, is this a question you can answer by doing some very simple research? There are some very basic questions people with certain conditions get asked quite a bit, and if Google can easily answer something then you have no reason to ask us. If your question something else (what our personal experiences are, specific advice on your own experiences, complicated or inaccessible information about neurodivergence or specific conditions we have, etc.) then you’re welcome to ask us whatever respectful questions you might have. Keep in mind our rule about advice; this is a submission blog and none of us are professionals. Also note that The Corvidae Collective (Mod Corvid) is always open to answer questions on their& blog @mogai-corvidae about any of their& identities or experiences, which includes general neurodivergence and many specific conditions. If you’re looking for more in-depth answers, that might be a good place to ask.
587 notes
·
View notes
Text

𝔇𝔬 𝔫𝔬𝔱 𝔦𝔫𝔱𝔢𝔯𝔞𝔠𝔱 / 𝔅𝔩𝔬𝔠𝔨𝔩𝔦𝔰𝔱

❥ Yan fetishists / self-proclaimed darlings
❥ Yan roleplayers / writers I don't really mind if you do these things, but if this is the theme of your acc please don't touch my posts. I don't appreciate my struggles being put into a fictional context!
❥ Believe any mental illness is inherently abusive Cluster Bs are more than welcome here. If you don't like them, leave!!!
❥ TERFS / radfems / gender-critical / truscum / transmed / anti-neopronouns / anti-xenogenders
❥ Racists / anti-semites / white supremacists / anti-BLM
❥ Pro-contact paras (big 3) I'm fine with paraphiles being around as long as they are able to recognise what's wrong and don't promote contact
❥ Porn blogs If your blog consistently contains visual NSFW you're likely to be blocked. I'm less strict about textposts but it can still fall under the radar
❥ Blank blogs If you don't have at least a profile/banner or description on your blog, you may appear as a bot and may be blocked as a result

𝔅𝔢𝔣𝔬𝔯𝔢 𝔶𝔬𝔲 𝔣𝔬𝔩𝔩𝔬𝔴
❥ If you dislike people who do "yan stuff" irl then I am not for you. I don't encourage anything without consent but I'm working through some habits and mindsets.
❥ When you follow, your blog will be checked. It will continue to be subject to intermittent checks as long as you remain a follower.
❥ If you've read through this, please send "lichen" to my ask box. It's a way to signal that you acknowledge what's in this post. Liking only shows that you found this, so please spare the extra moment. Your chances of getting blocked increase otherwise.
last updated: January 8, 2025
9 notes
·
View notes
Note
recently one of my siblings got severely (physically) ill, so now everyone is paying attention to them only, and completely ignoring my problems and how i feel and i really feel like im going to lose it. even before i hardly ever got any real attention but now it’s even worse. i don’t even give a fuck about what happens to the sibling but i have to pretend like i do because otherwise i’d automatically be seen as a “bad person”. i’m so sick over this bc like i’m always the one to get ignored and dismissed by the majority of people. idk what to do like i’m considering taking drastic measures like overdosing on drugs on purpose or committing a crime just to make someone notice me - even if in a bad way. i’ve already always hated my siblings because my shitty parents obviously love them more because somehow i’m the only one that had to get all the mental issues. i keep getting into arguments but it doesn’t change anything and then they start insulting me too and i feel even worse. i really don’t know how to go on. i wish i could run away and leave and make them regret how they always treated me but i’m in a situation where i can’t do that at the moment and i’m stuck at home for at least a few more months
hi! i'm so sorry to hear that, not only that your sibling is ill but also that as a result you aren't getting any attention. your problems are real too, and it's awful that they're being ignored. that being said, and i know this is easier said than done, but please keep yourself safe. harming yourself isn't the answer, especially not in the long run. it's incredibly fucked up that they insult you, and i hope that you're able to get out of that situation soon.
you aren't a bad person, the way you're feeling right now is super common with npd/cluster b in general. it's not right that you always get ignored, no one deserves that and it's especially shitty when you have a disorder like this that makes it hurt even more.
if it's at all possible, getting out of the house will be a huge help - even if you can't technically move out yet, just getting away for a few hours each day might prove to be a good idea. especially if you can interact with people who can consistently give you attention in a healthy way, although i do know that this is unfortunately easier said than done. either way, i hope you're able to get out permanently/for good soon.
3 notes
·
View notes
Note
BPD brain anon from this weekend popping in again for an unnecessary update/more inbox rambling, completely unrelated to all the syscourse stuff (which is gross, my heart goes out to OCD anon for their mental illness being used as a talking point).
I'm monoconscious and don't have enough of a sense of self to really recognize any personality changes, beyond any blatantly insane moments (that usually stem from having two Cluster B personality disorders and a cocktail of other mental illnesses). I kind of consider whatever was happening to me this weekend as one of those insane moments, but I DO still think something funky is happening in my subconscious. At the very least, I'm now thinking I'm considerably less "solidly singlet" than I'd thought. I've had a headmate before but I always figured that was more me thought-puppeting responses than an actual headmate.
I could also be doing the BPD brain thing where I convince myself that [thing] is actually a major facet of my identity even though it has literally never come up before, and I, with my lack of consistent self, just go "yeah that looks like it checks out" and adopt it as my identity for YEARS to come. Which is part of why I look back on my previous headmate with suspicion instead of just, accepting that he existed.
I always have a mental dialogue with myself, a back and forth between brain-in-charge and the peanut gallery. Sometimes there is no peanut gallery and my head is void of thought and self. Sometimes there IS a peanut gallery weighing in on my thoughts, and they all speak in my voice. Sometimes I feel like there's a dozen different people saying things but I know they're all the same person, y'know? All NPCs controlled by the same DM. Like this is a game between brain-in-charge and... something submerged in the very back of my brain.
When I was having my Episode, I tried asking myself about it and got some real weird emotional responses, the kind I could feel in my chest and gut even if they weren't really in my brain. I don't remember most of the questions I asked or what caused what responses, but I do remember trying to contact my old headmate. He didn't show up (which I expected, he's been gone for like 12 years), I asked if he was just another puppet, and wham got that gut punch emotional reaction.
Thus: Something Funky Is Happening In My Brain But 🤷♂️🤷♂️IDK What🤷♂️🤷♂️
At this point I am just liveblogging the process of sorting out my feelings into your inbox, sorry about that 😔 I'm defo gonna have a talk with my therapist about this tomorrow though.
No worries, thank you for sharing your experience! It sounds like you're processing a lot, so it makes sense it'd take some time. I'm glad you can talk it through with your therapist tomorrow.
I'll say, I know some people with BPD do consider their plurality to be related or caused by it. Like, considering the lack of consistent self a part of it, instead of a reason to be suspicious of the concept, if that makes sense?
13 notes
·
View notes
Text

I came up with 2 ocs to help me try and visualize how I kind of feel about my gender and myself as a whole (whoever that may be).
First there’s Formless, It’s a Genderfluid gendervoid entity, It is pansexual and panromantic, mute, and an emotional empath to anyone around It. Voids uses the pronouns He/She/They/It/Voids! Voids also is permanently dissociating and always lowkey uncomfortable . It is black with white and tired eyes, with a gradient wispy lower half.
The other oc I made is an android named Cluster. It is agender, asexual, and aromantic. It communicates only through Bleeps and Bloops and no words. It is capable of emotions but is more logic oriented. It is very good at Grounding Formless, and it uses They/It pronouns. It is boxy and grey and has a mouth consisting of 4 sharp angles.
I came up with Formless because I never have truly seen myself as a human, always a formless, shapeless entity with emotions and functioning mental illnesses. I’ve been trying to see myself as more than just a body, more than just a suit of organs, more than just a label of my gender (or a lackthereof?).
I came up with Cluster because when I dissociate (which feels ever present nowadays…) i feel like a robot going through life. The only thing It is better than I am at is Grounding from Dissociation lol
I want to try drawing more of them together, I really love them together. And I hope I can try and discover myself as I draw more of them
#Genderfluid#gendervoid#my ocs#queer oc#ocs#gender identity#gender journey#beginnerartist#amateurartist#original art#dissociation#dpdr#dpdr ocs#mental illness#mental illness ocs#coping ocs#comfort character#oc comfort character#gendervoid art#gendervoid oc#agender#agender artist#genderfluid artist#voidgender#voidgender oc
3 notes
·
View notes
Text
Juniper Publishers- Open Access Journal of Case Studies

A Neurological Presentation of Intravascular Large B-cell Lymphoma: a Rare Cause of Multi-Territory Strokes
Authored by J Newman
Abstract
Intravascular Large B-Cell Lymphoma (ILBCL) affects one in a million people. Here it presented as dysphasia and leg weakness in a forty-five-year-old woman with a history of mental health issues. The initial investigations showed multi-territory infarcts for which we were unable to find a treatable cause. Her condition progressed and she unfortunately died. Although rare, ILBCL ought to be included in differential diagnoses of multi-territory strokes, however, the diagnosis is commonly made post-mortem. Here we discuss common presentations of ILBCL. We note the proximity of her worsening psychiatric symptoms to the time of her death.
Keywords: Lymphocyte cells; Psychiatric symptoms; Intracerebral haemorrhage; Neurological manifestations; Intravascular large B-cell lymphoma
Introduction
Intravascular Large B-Cell Lymphoma is a rare subset of Non-Hodgkin’s Lymphoma that involves the pathological proliferation of lymphocyte cells within capillaries and other small blood vessels [1], causing their occlusion.
As the clonal proliferation is intra-vascular there is relative sparing of the surrounding tissue, making it more difficult to diagnose. The presenting symptoms vary according to the organ affected, although the skin and nervous system are common. When occlusion occurs intra-cerebrally the result is often a stroke.
The importance of identifying the aetiology of stroke in the afflicted patient is well recognised, as it can help direct management and treatment. This is particularly relevant to patients with multi-territory strokes, recurrent strokes, and those who are affected at a young age.
Our patient had worsening psychiatric symptoms leading up to her final admission and diagnosis. We note the proximity of these events, as psychiatric symptoms of ILBCL are poorly documented.
Case Report
A forty-five-year-old Caucasian woman was seen in the emergency department at a tertiary hospital in the UK. She presented with a two-day history of mumbling speech and acting withdrawn, left-sided leg and facial weakness, and right arm spasms. She had a background of depression and had presented acutely to community and hospital psychiatric services 5 months prior to this admission (we do not know the nature of that presentation). Her current medication included olanzapine 10mg daily and venlafaxine MR 300mg daily. Initial examination demonstrated an up-going right plantar response but no other focal neurology.
A CT head scan revealed low attenuation signal changes in the right cerebellar and right frontal lobes. Although her presentation appeared more psychiatric than organic, she was kept in to investigate her symptom complex and CT findings.
A subsequent MRI head demonstrated multiple areas of restricted diffusion in different vascular territories (Figure 1a). There were also foci of high T2 signal changes in the supra-tentorial white matter, with some demonstrating restricted diffusion. Considering the different territories, and different ages of these lesions, a cardio-embolic source was the most likely cause of these infarcts. Her trans-thoracic echocardiogram (TTE) was normal, as was her carotid Doppler. A lumbar puncture showed normal CSF. At this point she developed episodes of seizures corroborated by EEG.
We undertook investigations for lymphoma, and the blood tests showed little except a raised lactate dehydrogenase (LDH 400iU, plasma viscosity normal, blood film normal, haemoglobin 115g/L). We also discussed the possibility of vasculitis. However, her blood results and MR Angiogram did not show any positive findings.
A full-body CT scan was performed to look for other neoplastic lesions, but this was normal. We started high-dose corticosteroids as an empirical treatment for vasculitis.
Two weeks after this, she started to deteriorate. Her seizures became more frequent and her dysphasia more pronounced. A repeat MRI brain (Figure 1b) showed an increase in size of the lesions in the medial frontal and parietal lobes. New lesions in the corpus callosum and left thalamus showed restricted diffusion. The cerebellar, right medial frontal and parietal lesions enhanced with contrast. Long- and short-term MRI head spectroscopy did not show any evidence of a lactate peak to suggest mitochondrial disorder. This picture was consistent with a diagnosis of vasculitis.
Her condition continued to decline. Her GCS dropped to 7 and did not fluctuate, a repeat CT head revealed a right-sided intracerebral haemorrhage (Figure 2). Given the multitude of insults and progressive nature of her symptoms the difficult decision was taken to adopt a palliative approach for her symptoms. She died a day later.
Discussion
Intravascular Large B-Cell Lymphoma is a rare subset of non-Hodgkin’s lymphoma (NHL), affecting one in a million people [2]. First characterised in 1959 [3], it is known colloquially as “the great imitator” [2] due to its diverse range of presentations. It causes disease by a clonal expansion of lymphocytes within small blood vessels [1] resulting in end-organ damage. In retrospective analyses of case reports, around 90% of intravascular lymphomas are of B-cell origin. Unlike other NHL presentations, there is relative sparing of the lymph nodes [4].
There are two forms of ILBCL, Western and Asian. The former presents, as in this case, with neurological or dermatological symptoms [4]. The Asian variant typically presents with multi-organ failure, pancytopenia, fever and bone marrow involvement.
Common manifestations of the Western variant are dermatological (nodes, plaques, nodules, purpura etc.) and neurological (Table 1). Neurological manifestations are present in two thirds of patients and can include mental status changes, seizures, paralysis, aphasia, dementia, motor deficits, neuropathies, paraesthesias and cerebral haemorrhage as well as many others [5].
One meta-analysis [2] published a table of presenting features from seven major studies. Of the 154 patients, 54% presented with CNS involvement, 45% with cutaneous involvement, and 41% with fever. Two of the most common biochemical findings associated with ILBCL are a raised lactate dehydrogenase (LDH) in up to 90% of cases, and anaemia in two thirds of cases [4]. There may also be a raised erythrocyte sedimentation rate, weight loss or fever.
The diagnosis of ILBCL is made by biopsy [6] of affected tissue, which typically shows malignant lymphoid cells in the lumen of the small blood vessels. One of the difficulties in diagnosing this disease comes from the intravascular location of the pathological cells, and the sparing of surrounding tissue making it difficult to identify pathological cells on biopsy (Figure 2). Bone marrow involvement with positive biopsies have been shown in about one third of patients [4]. There is also evidence that for all presentations, a biopsy of macroscopically normal skin is over 80% sensitive as a test for ILBCL [6], providing an alternative to brain biopsy.
Contrasting theories exist as to why these B-cells have a predilection for capillaries. One theory posits the pathological expression of certain cluster differentiation factors (CD11a and CD49d), which enhances binding to capillary epithelium expressing ligands for these factors (CD54 and CD106) [7]. The other suggests that an absence of surface molecules (CD29 and CD54) disrupts lymphocyte homing and leads to an aggregation in small vessels [8]. It may be that as well as understanding the pathogenesis of this illness, elucidation of any aberrant surface molecule expression may also aid the development of target-specific treatments.
If it is identified early, ILBCL can be treated with anthracycline-based chemotherapy regimens. Typically, cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisolone (CHOP) therapy is used –with rituximab in patients with specific B-cell markers. This shows better response and higher rates of remission than alternative regimes [9]. However, only 33% of treated patients survive 3 years [9].
Cutaneous presentations of ILBCL have a better prognosis than other variants [4]. Factors indicating a poor prognosis include elevated LDH and advanced disease with presence in several sites [10].
When considering differential diagnoses it is important to consider ILBCL as a well-recognised cause of stroke (ischaemic or haemorrhagic) despite its low incidence.
This case is important as it demonstrates a specific neurological presentation of ILBCL and illustrates the difficulty of making a diagnosis, as well as the aggressiveness of the condition. We should also not dismiss worsening psychiatric conditions as being a manifestation of the illness – however unlikely – given the close temporal association.
Learning Points
a) Intravascular Large B-Cell Lymphoma often presents with neurological symptoms (in North America and Europe) and is a rare cause of multi-territory infarcts.
b) The intravascular confinement of the clonal expansion of pathological B-cells causes end organ damage by ischaemia.
c) Diagnosis is made by tissue or bone marrow biopsy; but being intravascular it is usually made post-mortem.
d) Biopsy of macroscopically normal skin also has the potential to be diagnostic.
e) Raised LDH and anaemia are common findings.
To know more about Juniper Publishers please click on: https://juniperpublishers.com/manuscript-guidelines.php
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#Juniper Publishers#juniper publishers journals#Cardio-Thoracic Surgery#Emergency Medicine#General Surgery Genetics#Medicine Neurosurgery
2 notes
·
View notes
Text
¶ … psychiatric nursing practice in Australian prisons," Doyle (1999) attempts to discern what factors influence psychiatric nursing care. In particular, the researcher attempted to decide what factors may influence a nurse's ability to work effectively under straining circumstances, in this case working with challenging patients in a prison. The problem as the researcher states it is that more than 100,000 patients require treatment while living in prison and correctional institutions. The unique client group presents many challenges to nursing staff including mental illness and developmental disabilities. In addition many patients are emotionally unstable. The author clearly identifies problems associated with providing optimal health care to incarcerated offenders. Also noted are the increased mortality rate and disease rate among this population. Nurses must often face challenging situations. They are often tasked with working with difficult patients. In addition they may face technological obstacles or conflicting values when working in certain settings, or in this case stigma association working with prisoners. It is important nurses overcome these obstacles so they are able to delivery the best quality care to patients regardless of their situation. Study Purpose The purpose of the study is to discern what challenges psychiatric nurses face and what factors may influence the quality of care they bestow on patients in a sub-optimal working environment. The aim of the researcher is to point out the obstacles nurses face in delivery high quality care to patients under trying conditions. Whether nurses work in a psychiatric institute or other institution, they are likely to face similar obstacles. The researcher clearly states the purpose. The author intends to "study issues of concern to nurses delivering mental health care to offenders." Research Question While the research question is not directly stated, the researcher does state his intent to study issues that concern nurse's delivery care to criminal offenders. The question allows adequate exploration from a qualitative perspective. The intent of the research is to study a phenomena, especially through observation, which is supported through qualitative research. Study Design The researcher suggests use of a praxis qualitative research approach, supported by other researchers (Lather, 1991). This type of research is also called applied research. The research design included a focus group of 10 mental health nurses who were interviewed regarding their concerns with patients. This method is supported by other qualitative studies that suggest focus groups and in depth interviews are appropriate (Street & Walsh, 1996; Massarik, 1981). The researcher also elected to use open-ended questioning. The method is appropriate because it is aligned with qualitative investigation. The questionnaire and interview approach allow the researcher to observe the phenomena occurring in their natural state. The study design utilized qualitative textual analysis where the researcher clustered themes of questions for nursing participants to answer. A narrative was subsequently produced describing the problems as described by the subjects interviewed. Subjects and Setting The researcher selected 30 subjects registered as psychiatric mental health nurses whose job was to deliver care to imprisoned men and women in a central industrial prison. Nurses employed for purposes of this study worked 24 hours care shift. The selection of nursing care staff is representative of the nursing population caring for this group at large, thus adequately represented the situation. The setting is appropriate as it examines nurses working in a walled and secure 120-bed prison unit. Data Collection Methods The methods used are consistent with a qualitative examination because they support use of an open-ended questionnaire. Qualitative analysis requires that the research examine a given phenomena and draw conclusions from this information. The researcher does this successfully by analyzing data using a clustered approach. The research gathers similar information to create a narrative exploring the range of problems demonstrated at the prison. The author did not comment on what instruments or disclosures were used to protect the identity of those interviewed. Interviews were taped and recorded. To protect the identity of the participants the researcher should have taken steps to assure anonymity. This may include assigning each participant a code or number to identify them for study purposes. It is possible that despite the lack of information regarding confidentiality, the researcher did take steps to assure anonymity. Data Analysis Procedures The data analysis procedures correspond to other methods adopted by qualitative researchers in the past. The data analysis procedures are consistent with a qualitative approach as the author is using applied research techniques to gather information from which to draw a narrative conclusion. The two major strengths of the study include the researchers directed approach to selecting a target population and use of open ended questions that allow the researcher to gather as much information as possible about the phenomena being investigated. The primary limitation of the study is the small sample size and single location used. It would be impossible for the researchers to generalize their information to the population at large based on this small sample. While the sample may be representative of most nursing situations where nurses work with inmates, it is difficult to assert this without additional studies. The author concludes that the environment in which psychiatric mental health nurse's work is often one dominated by surveillance, control and harsh circumstances. The author further concludes that nurses are often compromised and face resistance when attempting to implement routines and set up priorities. The conclusions are appropriate based on the interview data the researcher gathered from nurses working in the field. Because the nurses directly reported their circumstances and pressures, it is easy for the researcher to draw conclusions. The implications suggests that this research can be used to guide future training and support programs for nurses working in difficult situations. The researcher suggests that the challenges nurse's face in these situations must be acknowledge and recognized so adequate support may be offered nurses working under these conditions in the future. References: Doyle, J. (1999). "A qualitative study of factors influencing psychiatric nursing practice in Australian prisons." Perspectives in Psychiatric Care, 35(1):29 https://www.paperdue.com/customer/paper/psychiatric-nursing-practice-in-australian-67125#:~:text=Logout-,PsychiatricnursingpracticeinAustralianprisonsDoyle,-Length4pages Lather, P. (1991). Getting smart. New York: Routledge. Massarik, F. (1981). The intervening process re-examined. In P. Reason & J. Rowan (Eds.), Human enquiry: A source book of new paradigm research (pp. 201-207). New York: Wiley. Street, A., & Walsh, C. (1996). Community nursing issues in Maori mental health. Australia and New Zealand Journal of Mental Health Nursing, 5, 54-62. Read the full article
0 notes
Text
DEATH WILL ONLY BE THE BEGINNING #1
1. The backbone to my emotions
As someone who cannot conceptualise time in any way whatsoever, I want to say sorry to my loved ones. I'm aware I still need to send my friends messages every once in a while and remind them I still want to be their friends and I need to actively work on this. I need to overcome this fear stopping me from being present and accepting peoples love and support. I want to break free from me and I want to feel content being on this earth, I want nothing more than to enjoy experiences with my loved ones. I love you I love you.
I am a young charismatic, creative individual learning to do things differently so I don't always have the same outcomes. I suffer from a Cluster B Personality Disorder; under the same umbrella of mental health I also experience extremely intrusive thoughts on a daily basis, that can become obsessive and compulsively hyper fixated thoughts in an instant. I have anxiety, depression and a lot of the time I’m deeply dissociated to a point where I struggle to believe I’m even real, even when I do know I am real- I have no attachment to my limbs or body as a whole and only feel alive in a spiritual sense or when I self harm. I don't want to get too into my illnesses; as I’m not someone who really likes labels, just know that everyday is a battle and each personality that exists within me is different. I wouldn't say drastically, however its evident for me and living with so many different masks can be intense. Especially when you've tried to convince people that you're just one solid mould in the hopes they don't perceive you as an intense person. I am going to try to take you through a few of my altars and moods starting with the emptiest subconscious alters that I call the backbones of my emotions to the more powerful energetic ones that haven't managed to yet consume me over the years. I hope this can give people an insight.
Overall I present a pretty confident front, I like to appear like I’ve got my life together even though I’m so far from it, sometimes I’m not sure ill even find the strength to go on long enough in attempt to get my life together, which is a real problem but it's the sad truth. Don't waste time reading this if you're easily triggered as this piece of writing will consist of real and genuine feelings. I’m in no attempt trying to create content for people who enjoy turning blind eyes and wishing they didn’t see this so I’ll give you a fair warning. I'm not responsible for your triggers, whereas I’m responsible for the things I’ve done. I might have cared too much at one point, but I will not hold myself captive to those situations nor will I regret them. I want the lies, deceit and hurt that I’ve committed against loved ones to end, my secrecy has done enough damage and its exhausting pushing people away even though that’s not usually the intent, truth is I am so embarrassed of myself. I'm private, secretive and mysterious but I’ll also talk about my childhood trauma after like 5 minutes. I guess this says I’m happy to talk about my trauma because it's what I know and am comfortable with, I just struggle to tell anyone the real suicidal me behind my problems. I hate that I’m so young and feel like a dead person already.
I tend to act out or distance myself due to fear which isn’t clear at first if you know me, but does become obvious. I might appear as someone with no care in the world, like I’m unbothered, but I assure you that's the African pride combined with the Leo pride. I also don't want people to treat me like a footstool, which has happened when I’ve come off ass too passive. I care so much and over think absolutely everything, it's literally my only way of thinking. I have little to no self esteem and I have no clue who confidence is unless under the influence of something, be it weed, alcohol or psychedelics (which I don't take much of because I enjoy them and don't want to abuse them) I mean I can function sober, I don't even like to be out of control high or drunk, but as Chief Keef once said, I hate being sober. #i'mTrash4thereference. Although I’m not fully healed and functioning yet, I’m a developed character with both positive and negative traits. At the moment I’m going back and fourth between 'just stop trying' and 'you cant give up'. Sometimes depression is kind of like looking at yourself through a window, there’s this part of your brain that understands it'll pass, but you’re so far into despair that its impossible to see the way out, its a lot like being trapped. I am having a bad patch right now, the difference between this one and the last one is I’m more self aware with less of a desire to go on. At least I’m no longer suffering from paranoia and thinking everyone's out to get me all the time or that I’ll get trafficked walking home from somewhere, but depression and mania are so bloody invasive and there’s always that little voice in my head telling me ill never be good enough. Executive dysfunction kills my motivation because I have so many things to do and I cant pick anything to start first, it gets worse when my depression gets worse too. I'm not lonely though; I have a few people who care for me- and while I'm trying to not involve them in the metal episode, they are around to talk to and that means so much. My friends are super encouraging even though I've only briefly mentioned that I'm having a sad time right now, and that's awesome.
I hate that no matter how much better I get there's still this deep desire to get worse. I don't feel like a real person. I just feel like a collection of what people want me to be and various mental disorders. It would be so cool if I could admit to the world I have a personality disorder without feeling disgusting and without fear.
I've had plenty time to reflect upon every bit of thought that created the barbed wire surrounding my logical brain, I want to feel okay to be alive, but I so strongly just want to die. I am tired of fluctuating from feeling extremely vigorously suicidal to passively suicidal; where I just don't have the energy to carry it out myself. It's gotten way past the point that it doesn't matter what kind of day I have, I think about killing myself all day. Sleep is an escape from life and I'm always tired and wanting to 'sleep'. Deep down I feel like I’m waiting for the right time to end my life and it's not the right time yet because I still have a footprint to leave behind, I still have journal pages I want to burn. I cant just jump off the highest accessible building or mall car park I could find just yet- I don’t just want to ruin others by hurting them with my death. It's sad to think I grew into this mindset, waking up wishing I was dead.
Being abandoned by many people in the past made me doubt people and think everyone was out to get me or wanted something from me, it made me feel hurt and lone. So I felt it would be better to let people down before they could hurt me so I wouldn't repeat the same cycle when forming new connections. It wasn't intentional but I could just silence myself due to fear.
I just found myself feeling immensely hopeless, like I was too internally enraged at the external world to be able to trust anything of it. I definitely do want to get better because I’m tired of feeling this way, it's so exhausting and I hate pushing people away from me like I’m poison. I need to allow people to accept all of me.
Before picking up these coping mechanisms when I was younger and more insecure; I wanted to be a part of the world, I had this strong urge to fit in. I had to learn how to manage my anxiety and socialising became more exhausting stemming from my fear of being 'odd' or 'different', I didn’t want to be called out for being different- it was not a compliment at that age, it always felt like a being the joker in the card deck. I was intensely afraid of being judged or labelled as such. Being told I was a 'weirdo' didn't help at all, that type of criticism is what got to me the most. People made me feel like I needed to change, like I was too African, even in a joking manner it didn't help- because although I was okay with who I was, I did feel like I had to change and westernise myself to fit in. I ended up hanging around with people that didn't care, doing stupid things I didn’t even want to do, dating people I didn't connect with. Eventually I got tired of people using me for entertainment, tired of catering to those who refused to understand. I still have to admit there were many periods that I lowered my frequency to be on the wavelength of others that did not match mines at all, I hate that I'm someone who always feels the need to explain myself so people don't think I'm a bad person and even though I don't owe it to everyone and now I am able to make better choices and I'm no longer easily influenced, it still hurts that i was ever around people that made me feel like I was over exaggerating my mental health or uncomfortable to a point where I learned to downplay it or the mention of it. Now as a coping mechanism I’ve become so facetious and sarcastic about my trauma it's a struggle to take myself seriously at times. Users and abusers belittled me to such a point where I felt they'd underestimated my intelligence and most of all humiliated me. It made me tired of justifying myself so now most days I’m just a mute, but I really do finally have good people in my life who deserve some sort of explanation and it's a shame they don't get to be experience a truly present consistent me. It’s just after having the wrong eyes on me, I don’t want anything to see me. I hate attention because I’m so embarrassed of myself I don’t want to be noticed. People looking at me make me want to kill myself.
I've been told to move past my rage, to let go and become a grounded and level headed person. I've been told there is hope for all of us. Must be nice to believe that, all I could wonder was what it was like to get angry without getting homicidal and suicidal. Even on most days where nothing extreme would happen besides negative emotions, my brain still travelled to a dark realm. I've come to a point where I want to live in my daydream universe wile I physically rot away. That's my business. Sometimes I feel as though all my friendships are on a timer, or more so it's that my timer is about to go off, so I subconsciously shy away and make sure i have no deep friendships. Just in case my head decides to do something stupid.
I don't want to have no friends, I want to have friends and I do value friendships so much more than entitled relationships, I just have a difficulty maintaining friendships because it's exhausting for me, it takes a lot of energy to be social and on a level that isn't just superficial where I can just let go and allow myself to fully be. Sometimes I have a hard time relating to other people, and thus I may feel I don’t belong or don’t quite fit in- causing me to feel irritated, paranoid or even in pain during social situations. It's not always this bad, and I don't mean for it to sound dramatic. It's different when In person and I’m really relaxed and comfortable with the company. However virtually socialising and expressing will always be extremely anxiety enducing and its something I need to overcome especially going into this new phase of Artificial Intelligence. So if I start to drift away it most likely isn't a reflection of you. The cycle goes I need alone time to recharge then I realise how long has passed and I just feel so bad I haven’t gotten back, I tell myself I’m an awful friend for dissociating for so long, and then I don’t know how to explain that so my anxiety rises, mood drops and I spiral back into a pit of depression, often wanting to relapse but refraining from doing so. Sometimes I manage to get out of the pit, but by then so much has piled up I don't know where or how to begin again.
I don't feel like I could have a normal friendship as well as romantic relationship. It's hard for me to long term imagine myself being fully relaxed enough to let my guard down and not reluctant to express. I don’t think there’s any condition where ill just be came and enjoy a connection without worrying that the other person isn’t putting in as much effort, or they have an image of me, or that I’ve amplified the emotions and even though I feel them that way do they really understand me or love me as much. Silence is so upsetting and I hate the fact I do it when I'm afraid of myself or don't feel good enough. I never intent for it to become 'the silent treatment' because in reality its not treating anyone, it's more a reflection of what I’m internalizing and not wanting or being unable to project and express those feelings without feeling like party pooper, an attention seeker or 'too deep'. I don't mean to give people false hope, I love the people in my life so much and every one I’ve met on this journey. I'm learning to look at life through a different lens and the people who contributed to my suffering will not be the definition of me. People have led me to believe so much and strung me along, not letting me go- and I realised those entitled controlling abusive relationships were not serving me. I couldn't keep doing it. Now even though I want closeness I end up pushing people away or leaving them in the dark because of fear, especially of something new because I've never experienced anything good and true for a long enough duration of time to rid me of that fear. I also have fear of rejection or hurting, I fear becoming too emotionally invested and becoming co dependant so I end up wanting to avoid the pain than actually wanting to experience the joy and growth the relationship could offer, so I end it before it begins to avoid any possible pain. I feel like I don't deserve these connections,and sometimes the depression runs so deep I have to push people away in case I want to do something stupid- I don’t want them to feel at fault, or obligated to be able to handle me. Sometimes I really can just only be with myself and my thoughts so I hide but it may appear that I’m pushing others away because of my isolation and neglect.
With everyone I know, I get this feeling that they're too good for me, their energy is so radiant and loving but I feel so broken and don’t want to depend on that. I've had perfectly ideal people come into my life and I feel they’re too good for me because I have a lot of work to do on myself first, primarily I need to build up confidence and self esteem because it's the root of most my issues. I want to relate to people, share our deepest fears and wishes without fear of judgement. It's not that I don't want to get better, I simply cannot remember what it was like to have an actual honest to god normal personality. The feeling of being a mentally unstable chameleon is all I have now. I AM my illness, that's the only identifier I have left. I can't remember normality.
I understand that I’m lucky and I’m not ungrateful for the things and people I do have, it doesn’t mean that my life doesn’t suck because of those lucky things. I often think about if someone created technology to transfer life to another, I’d happily give them mine because they'd live it much better than me, I’m not worth anything to myself. I never wanted to be someone to cause pain on the people I love but now I do, even if that’s just through silence. I just disappear when I haven’t been doing well and although I know things get better, recovery isn’t linear and that not all my days are bad, I just have extreme chronic feelings of emptiness.
I struggle to trust people because I don't want to be hurt but I need people so much, I hate feeling unloved. It's so overwhelming because I feel everything so extremely as if I’m going to explode.
My sense of self and reality feels destroyed, my future and dreams are uncertain and it's hard for me to move on, sometimes it scares me what I’m doing to people without the intention of it, being too much or not enough- or at least feeling that way. It's hard for me to give myself a reason and it's not on the people around me to fill my empty void, I hate forcing people to be my friend or understand my illness. I cant expect anyone to want to- it feels like I’m holding their hand while they pull it away; and even though it's not the case I feel awful, I constantly feel like I’m in a more pessimistic head space. I'm worried people will realise I'm as pathetic as I say I am.
3 notes
·
View notes